solomon islands - who.int · iii foreword the 2011 pharmaceutical country profile for solomon...
TRANSCRIPT

SOLOMON ISLANDS
PHARMACEUTICAL COUNTRY PROFILE
ii
Solomon Islands
Pharmaceutical Country Profile Published by Ministry of Health in collaboration with the World Health
Organization
June 2012
Any part of this document may be freely reviewed, quoted, reproduced, or translated in full or in part, provided that the source is acknowledged. It may not be sold, or
used in conjunction with commercial purposes or for profit.
Users of this Profile are encouraged to send any comments or queries to the following address:
The Director of National Pharmacy Services Division
Ministry of Health and Medical Services PO Box 349, Honiara
Email: [email protected]
This document was produced with the support of the WHO Representative Office in the South Pacific, and all reasonable precautions have been taken to verify the information contained
herein. The published material does not imply the expression of any opinion whatsoever on the part of the World Health Organization, and is being distributed without any warranty of any kind – either expressed or implied. The responsibility for interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising
from its use.

iii
Foreword
The 2011 Pharmaceutical Country Profile for Solomon Islands has been
produced by the Ministry of Health and Medical Services in collaboration with
the World Health Organization.
This document contains information on existing socio-economic and health-
related conditions, resources; as well as on regulatory structures, processes
and outcomes relating to the pharmaceutical sector in the Solomon Islands.
The compiled data comes from international sources (e.g. the World Health
Statistics), surveys conducted in the previous years and country level
information collected in 2011. Some more recent information is also included.
The sources of data for each piece of information are presented at the end of
this document.
On behalf of the Ministry of Health and Medical Services, Solomon Islands, I
wish to express my appreciation to all senior staff] from National Pharmacy
Services Division for their contributions to the process of data collection and
the development of this profile.
It is my hope that partners, researchers, policy-makers and all those who are
interested in the Solomon Islands Pharmaceutical Sector will find this profile
a useful tool to aid their activities.
Timmy Manea
National Pharmacy Services Division, Ministry of Health and Medical Services 28th June, 2012
Signature

iv
Table of content
Introduction ............................................................................................................ 1
Section 1 - Health and Demographic Data ........................................................ 2
Section 2 - Health Services ................................................................................ 6
Section 3 - Policy Issues .................................................................................. 12
Section 4 – Medicines Trade and Production ................................................. 14
Section 5 – Medicines Regulation ................................................................... 16
Section 6 - Medicines Financing ...................................................................... 25
Section 7 - Pharmaceutical Procurement and Distribution in the Public Sector ................................................................................................................. 30
Section 8 - Selection and Rational Use of Medicines .................................... 34
Section 9 - Household Data/Access ............................................................ 3939
1
Introduction
This Pharmaceutical Country Profile provides data on existing socio-economic
and health-related conditions, resources, regulatory structures, processes and
outcomes relating to the pharmaceutical sector of the Solomon Islands. The
aim of this document is to compile all relevant, existing information on the
pharmaceutical sector and make it available to the public in a user-friendly
format. In 2010, the country profiles project was piloted in 13 countries
(http://www.who.int/medicines/areas/coordination/coordination_assessment/e
n/index.html). During 2011, the World Health Organization has supported all
WHO Member States to develop similar comprehensive pharmaceutical
country profiles.
The information is categorized in 9 sections, namely: (1) Health and
Demographic data, (2) Health Services, (3) Policy Issues, (4) Medicines Trade
and Production (5) Medicines Regulation, (6) Medicines Financing, (7)
Pharmaceutical procurement and distribution, (8) Selection and rational use,
and (9) Household data/access. The indicators have been divided into two
categories, namely "core" (most important) and "supplementary" (useful if
available). This narrative profile is based on data derived from both the core
and supplementary indicators. More recent information is also included. For
each piece of information, the year and source of the data are indicated; these
have been used to build the references at the end of the profile; and are also
indicated in the tables. If key national documents are available on-line, links
have been provided to the source documents so that users can easily access
these documents.
The selection of indicators for the profiles has involved all technical units
working in the Essential Medicines Department of the World Health
Organization (WHO), as well as experts from WHO Regional and Country
Offices, Harvard Medical School, Oswaldo Cruz Foundation (known as
Fiocruz), University of Utrecht, the Austrian Federal Institute for Health Care
and representatives from 13 pilot countries.

2
Data collection in all 193 Member States has been conducted using a user-
friendly electronic questionnaire that included a comprehensive instruction
manual and glossary. Countries were requested not to conduct any additional
surveys, but only to enter the results from previous surveys and to provide
centrally available information. To facilitate the work of national counterparts,
the questionnaires were pre-filled at WHO HQ using all publicly-available data
and before being sent out to each country by the WHO Regional Office. A
coordinator was nominated for each of the Member States. The coordinator
for Solomon Islands was Timmy Manea.
The completed questionnaires were then used to generate individual country
profiles. In order to do this in a structured and efficient manner, a text
template was developed. Experts from member states took part in the
development of the profile and, once the final document was ready, an officer
from the Ministry of Health certified the quality of the information and gave
formal permission to publish the profile on the WHO website.
This profile will be regularly updated by National Pharmacy Services Division.
Comments, suggestions or corrections may be sent to:
Timmy Manea
National Pharmacy Services Division , MHMS
PO Box 349
Honiara
Solomon Islands
Honiara Central Post Office

3
Section 1 - Health and Demographic Data
This section gives an overview of the demographics and health status of
Solomon Islands. 1.1 Demographics and Socioeconomic Indicators The total population of Solomon Islands in 2009 was 523,000 with an annual
population growth rate of 2.6%. The annual Gross Domestic Product (GDP)
growth rate is -2.20%. The GDP per capita was US$ 1,257.23 (at the current
exchange ratei).
Of the total population, 39% is under 15 years of age and 5% is over 60 years
of age. The urban population currently stands at 18% of the total population.
The fertility rate in Solomon Islands is 3.8 births per woman. The adult literacy
rate for the population over 15 years is 76.6% (Western Pacific Country
Health Information Profiles, WHO 2010).
1.2 Mortality and Causes of Death
The life expectancy at birth is 69 and 72 years for men and women
respectively. The infant mortality rate (i.e. children under 1 year) is 26/1,000
live births. For children under the age of 5, the mortality rate is 37 /1,000 live
birthsii. The maternal mortality rate is 146/100,000 live birthsiii (The Western
Pacific Country Health Information Profiles, 2010).
The top five diseases causing mortality are:
Disease
1 Cardiovascular diseases
2 Malaria
3 Neonatal causes
4 Neoplasm
5 Respiratory diseases (pneumonia as the leading causes)
i The current exchange rate for calculation is SBD 1 = USD 0.12350 on June 9th, 2011 (http://www.oanda.com/currency/converter/) ii Report on 2009 Population and Housing Census, Solomon Islands iii MDG Goals Progress Report for Solomon Islands, 2010
4
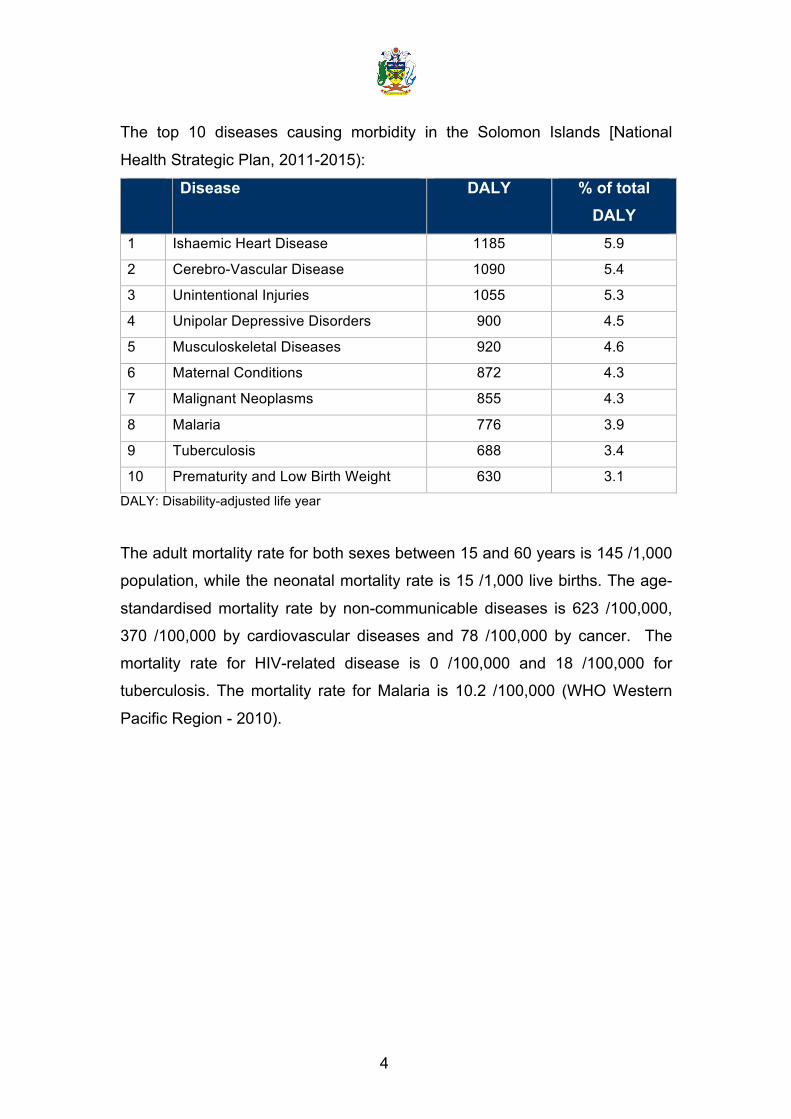
The top 10 diseases causing morbidity in the Solomon Islands [National
Health Strategic Plan, 2011-2015):
Disease DALY % of total DALY
1 Ishaemic Heart Disease 1185 5.9
2 Cerebro-Vascular Disease 1090 5.4
3 Unintentional Injuries 1055 5.3
4 Unipolar Depressive Disorders 900 4.5
5 Musculoskeletal Diseases 920 4.6
6 Maternal Conditions 872 4.3
7 Malignant Neoplasms 855 4.3
8 Malaria 776 3.9
9 Tuberculosis 688 3.4
10 Prematurity and Low Birth Weight 630 3.1
DALY: Disability-adjusted life year
The adult mortality rate for both sexes between 15 and 60 years is 145 /1,000
population, while the neonatal mortality rate is 15 /1,000 live births. The age-
standardised mortality rate by non-communicable diseases is 623 /100,000,
370 /100,000 by cardiovascular diseases and 78 /100,000 by cancer. The
mortality rate for HIV-related disease is 0 /100,000 and 18 /100,000 for
tuberculosis. The mortality rate for Malaria is 10.2 /100,000 (WHO Western
Pacific Region - 2010).

5
Further information:
Solomon Islands is in a phase of epidemiological transition. Having to deal with both the control of infectious diseases and an increasing incidence of non-‐communicable diseases, with very limited resources, poses a major challenge for the Government. With the dissipation of ethnic conflict during 1999-‐2003 and with support in 2004 from the Global Fund to Fight AIDS, Tuberculosis and Malaria (the Global Fund), the Australian Agency for International Development (AusAID), the World Bank and Rotary International, progress has been made in malaria control. The malaria burden, measured by annual parasite incidence (API) has been declining steadily over the years. From an API of 167 per 1000 population in 2002, data from 2009 show an API of 74.8 per 1000 population, better than the targeted API of 90 per 1000 population.
The tuberculosis prevalence rate was 70 per 100 000 for 2009, with a 93% cure rate through directly observed treatment, short-‐course (DOTS) therapy in 2008 cohort cases. With the recent approval of the Global Fund submission, the national TB programme is set to make further rapid improvements in TB prevention and control.
There was no major disease outbreak in 2008/2009. However, the worldwide threats of influenza A(HINI) and HIV-‐related disease have resulted in the development of new policies and strategies to strengthen and revitalize disease prevention, control and surveillance, as well as preparedness for action.
Although infectious diseases are still the major causes of morbidity and mortality, there is some evidence that non-‐communicable diseases like cancer (cervical and breast cancers are reported to be the most common, followed by lung cancer), diabetes mellitus, hypertension, tobacco-‐related diseases and mental illness are increasing.
The National Pharmacy Services Division Five-‐Year Strategic Plan (2011-‐2015), highlights key priority areas of i) Essential Medicines Policy and Management; ii) Procurement; iii) Provincial Strengthening and; iv) Rational Use of Medicines.
In particular, Rational Use of Medicines initiatives, led primarily by the Medicines Information Centre, form the forefront of pharmacy division’s response to the epidemiological transition and these are highlighted in the Five-‐Year document.
Key recommendations:
The National Pharmacy Services Division is addressing the epidemiological transition in provisions within their Five-‐Year Strategic Plan (2011-‐2015), which highlights key priority areas of i) Essential Medicines Policy and Management; ii) Procurement; iii) Provincial Strengthening and; iv) Rational Use of Medicines.
In particular, the pharmacy division’s Rational Use of Medicines initiatives, led primarily by the Medicines Information Centre, and initiatives to maintain reliable supplies of appropriate medicines should be vigorously continued in the response to the epidemiological situation.
6
Section 2 - Health Services This section provides information regarding health expenditures and human
resources for health in the Solomon Islands. The contribution of the public and
private sector to overall health expenditure is shown and the specific
information on pharmaceutical expenditure is also presented. Data on human
resources for health and for the pharmaceutical sector is provided as well.
2.1 Health Expenditures
The National Health Accounts (2009) showed that in Solomon Islands, the
total health expenditure (THE) in 2009 was 304 million Solomon Islands
Dollars (SBD) (US$ 37.72 million). The total health expenditure was 5.74% of
the Gross Domestic Product (GDP), equivalent to SBD 581.26 (US$ 72.12)
per capita.
The general governmentiv health expenditure (GGHE) in 2009, as reflected in
the National Health Accounts (NHA) was SBD 285.00 million (US$ 35.36
million). That is, 93.75% of the THE, with a total public health expenditure of
SBD 544.93 (US$ 67.61) per capita. Private health expenditure covers the
remaining 6.25% of the THE. The GGHE represents 16.80% of the total
government budget.
Of the total population, 100% is covered by a public health service, public
health insurance or social insurance, or other sickness funds and 0% is
covered by a private health insurancev.
According to NHA (2009), total pharmaceutical expenditure (TPE) in Solomon
Islands is US$ 2,250,000 which is equivalent to US$ 4.30 per capita. The total
pharmaceutical expenditure accounts for 0.34% of the GDP and makes up
5.97% of the THE (Figure 1). Public expenditure on pharmaceuticals
represents 100% of the total expenditure on pharmaceuticals.
iv According to the NHA definition, by "government expenditure" it is meant all expenditure from public sources, like central government, local government, public insurance funds and parastatal companies. v However, some private companies provide healthcare for their employees
7
Figure 1: Share of Total Pharmaceutical Expenditure as percentage of the Total Health Expenditure. The THE in 2009 was 304 million Solomon Islands Dollars (US$ 37.72 million)
[National Health Accounts, 2009; Ministry of Health and Medical Services]
Social security expenditure makes up 0.0% of government expenditure on
health.
Out-of-pocket expenditure (OOP) as % of private health expenditure is 67.4%.
Premiums for private prepaid health plans are 0.0% of total private health
expenditure.
2.2 Health Personnel and Infrastructure
The health workforce is described in the table below. There are 14 (0.27
/10,000) licensed pharmacists, of which 8 (0.15 /10,000) work in the public
sector. There are 46 (0.88 /10,000) pharmaceutical technicians and assistants
(in all sectors). The pharmacy technicians and assistants are pharmacy
officers, who have undergone a two-year in-country certificate course. They
generally undertake basic functions of dispensing and supply in hospitals and
provincially, whilst several hold senior positions within the National Pharmacy
Services Division, MHMS. There are approximately six times as many
pharmacy officers as pharmacists in the public sector.
There are 89 (1.70 /10,000) physicians and 694 (13.27 /10,000) nursing and
midwifery personnel in Solomon Islands. The ratio of doctors to pharmacists is
6.4 and the ratio of doctors to nurses and midwifery personnel is 0.13.
94%
6%
TPE Other
8
Table 1: Human resources for health in Solomon Islands
Human Resource Licensed pharmacists (all sectors) 14 (0.27 /10,000)
Pharmacists in the public sector 8
Pharmacy technicians and assistants (all sectors) 46 (0.88 /10,000)
Physicians (all sectors) 89 (1.70 /10,000)
Nursing and midwifery personnel (all sectors) 694 (13.27 /10,000)
Figure 2: Distribution of Pharmacy Personnel, Solomon Islands, 2011
In Solomon Islands, there is a Strategic Plan for Pharmaceutical Human
Resource Development in place.
The health infrastructure is described in Table 2 below. There are 11 hospitals
and 732 hospital beds (14 /10,000) in Solomon Islands. There are 310
primary health care units and centres and nine licensed private pharmacies.
Table 2: Health Infrastructure
Infrastructure Hospitals 11
Hospital beds 732 (14 /10,000)1
Primary health care units and centres 310
Private licensed pharmacies 9
23%
77%
Pharmaceutical technicians and assistants Pharmacists

9
The annual starting salary for a newly registered pharmacist in the public
sector is SBD 52,000. The total number of pharmacists who graduated (as a
first degree) in the past two years is six. The Pharmacy Officer Course is run
by the National Training Unit, National Pharmacy Services Division. The
curriculum is regularly reviewed (see box: Further information and key
findings). There are no university-level pharmacy schools in the country.

10
Further information and key findings:
The centrepiece of Pharmacy Training in Solomon Islands is the Pharmacy Officer Certificate course, which has been running since the 1990s and most recently updated in 2008. This most recent update has modernised the programme, making all resources available electronically. The course combines twice-‐weekly tutorials, rotations through all areas of public and private sector pharmacy, provincial experiential placements and ongoing multi-‐faceted assessments. It is two years in length and now entirely run and managed by local pharmacists, who have received training and support from Australian volunteers (through Australian Volunteers International).
Graduates are eligible to work in public pharmacy facilities and carry out most of the functions of qualified pharmacists in remote areas without pharmacists available.
In 2009-‐2010, 10 candidates completed the course. In 2012, a new course commenced with 13 public candidates and six students also participating from the private sector, which is an exciting initiative.
The National Pharmacy Training Unit also runs a 12 month intern course for returning Pharmacy Graduates, which had six participants in 2012, and a basic continuing education program for all staff, consisting of four annual quizzes which are sent to all facilities. This Continuing Education program, called Expansion, is slated for strengthening in the next two to three years.
Solomon Islands’ health care system is organized on a five tier system that shapes its formal health services. The National Referral Hospital is the only tertiary institution in the country. There are eleven provincial hospitals and 316 other health facilities in Solomon Islands that are overseen by the Ministry of Health and Medical Services. Four of the eleven provincial hospitals are operated by churches and report to MHMS , who provide resources and oversight.
Primary Health Care is delivered through a system comprised of provincial hospitals, Area Health Centres (AHC), Rural Health Clinics (RHC), Urban Health Clinics (UHC), and Nurse Aid Posts (NAP). Doctors are available at eleven health facilities in Solomon Islands: the National Referral Hospital in Honiara along with seven public hospitals and three church operated hospitals in the provinces. There is not a doctor resident in Renbel province.
Registered nurses and nurse aides are the front line clinical personnel in health centers, clinics and aid posts. AHCs have four to five staff (Registered Nurses or Nurse Aids, and malaria microscopists) and provide the highest clinic level of primary health care, including outpatient and basic inpatient care. There are 30 AHCs, four UHCs, and five Sub-‐UHCs in the country. Four of the UHCs function as AHCs. RHCs have up to two staff and are smaller than AHCs, but provide similar services. There are 109 RHCs in Solomon Islands.
Nurse Aid Posts are small clinics staffed by one Nurse Aide who is typically a member of the community. Nurse Aides provide first aid, basic primary health care activities, emergency birthing and observation of sick patients before they are referred to a higher-‐level facility. There are 177 NAPs in Solomon Islands. (reference: Solomon Islands Global AIDS Response Progress Report 2012)

11
Key recommendations:
Existing policy documents and recommendations relating to this section are in place for the next years.
It is recommended that implementation of the Pharmacy Sector Strategic Plan 2011 – 2015 is continued, especially in regards to:
• Strengthening the Pharmacy Human Resource base throughout the sector • Upgrading training and CE activities as needed • Developing a suitable career structure to retain staff in the public sector • Exploring the issue of partnerships with other organizations; and technical
cooperation for exchange programs involving qualified personnel from other countries whose services can be utilised for a period of time to address unmet training and service delivery needs.
12
Section 3 - Policy Issues
This section addresses the main characteristics of the pharmaceutical policy
in Solomon Islands. The many components of a national pharmaceutical
policy are taken from the WHO publication “How to develop and implement a
national drug policy” (http://apps.who.int/medicinedocs/en/d/Js2283e/).
Information about the capacity for manufacturing medicines and the legal
provisions governing patents is also provided.
3.1 Policy Framework
In Solomon Islands, a National Health Policy (NHP) exists and it was released
in 2011. An associated National Health Policy implementation plan (written in
2011) also exists. An official National Medicines Policy (NMP) document
exists in the Solomon Islands, as detailed in Table 3. It was updated in 2009.
However, a draft of an additional updated version also exists currently. A NMP
implementation plan does not exist, but a Five-Year Strategic Plan for
Pharmacy is available. NMP implementation is regularly monitored/assessed
by the National Pharmacy Services Division and national pharmaceutical
legislation is currently under review, with WHO support.
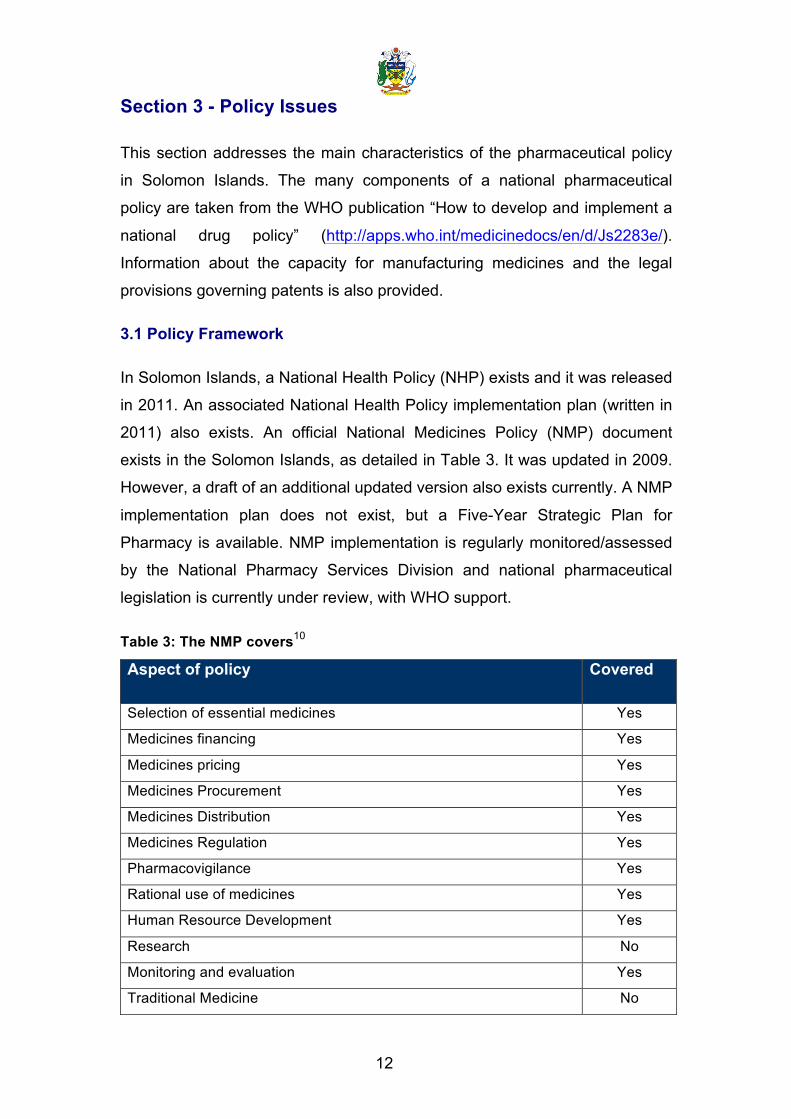
Table 3: The NMP covers10
Aspect of policy Covered
Selection of essential medicines Yes
Medicines financing Yes
Medicines pricing Yes
Medicines Procurement Yes
Medicines Distribution Yes
Medicines Regulation Yes
Pharmacovigilance Yes
Rational use of medicines Yes
Human Resource Development Yes
Research No
Monitoring and evaluation Yes
Traditional Medicine No

13
A policy relating to clinical laboratories is in development. There are official
written guidelines on medicines donations.
A policy is not in place to manage and sanction conflict of interest issues in
pharmaceutical affairs. There is a formal code of conduct for public officials. A
whistle-blowing mechanism that allows individuals to raise concerns about
wrongdoing occurring in the pharmaceutical sector of Solomon Islands does
not exist.
Further information and key findings:
The overall goal of the NMP is:
The development within the available financial and human resources, of the potential that medicines have to contribute to community health within all sectors in the Solomon Islands: the public, private, non-‐government and church sectors.
The four main aims of the NMP are:
1. To ensure the ready and reliable availability of good quality, acceptably safe, and proven effective and affordable essential medicines.
2. To rationalise use of these essential medicines through the provision of improved medicine utilisation information and trained health professionals, and through education of the public in appropriate medicine use and storage with the aim of rationalising medicine supply management, prescribing and dispensing, and improving patient compliance.
3. To inform the National Health Plan on issues related to maintenance of safe and reliable treatment with essential medical supplies.
4. To inform the development of a strategic plan that will set priorities for actions in the short – medium – and long – term.
Key recommendations:
It is recommended that National Pharmacy Services Division Five-‐Year Strategic Plan (2011-‐2015) aimed at implementing components of the NMP continues to be prioritised and implemented.
Activities should be undertaken according to the plan and indicators of their achievement should be monitored to assess implementation and modified if necessary.
14
Section 4 – Medicines Trade and Production 4.1 Intellectual Property Laws and Medicines
Solomon Islands is a member of the World Trade Organization. Legal
provisions granting patents to manufacturers exist. These cover
pharmaceuticals, laboratory supplies, medical supplies and medical
equipment.
Intellectual Property Rights are managed and enforced by the Ministry of
Police and Justice.
National legislation has not been modified to implement the Trade-Related
Aspects of Intellectual Property Rights (TRIPS) Agreement and does not
contain TRIPS-specific flexibilities and safeguards. Solomon Islands is eligible
for the transitional period to 2016.
There are no legal provisions for data exclusivity for pharmaceuticals, patent
term extension or linkage between patent status and marketing authorization.
The country is not engaged in capacity-strengthening initiatives to manage
and apply Intellectual Property Rights in order to contribute to innovation and
promote public health.
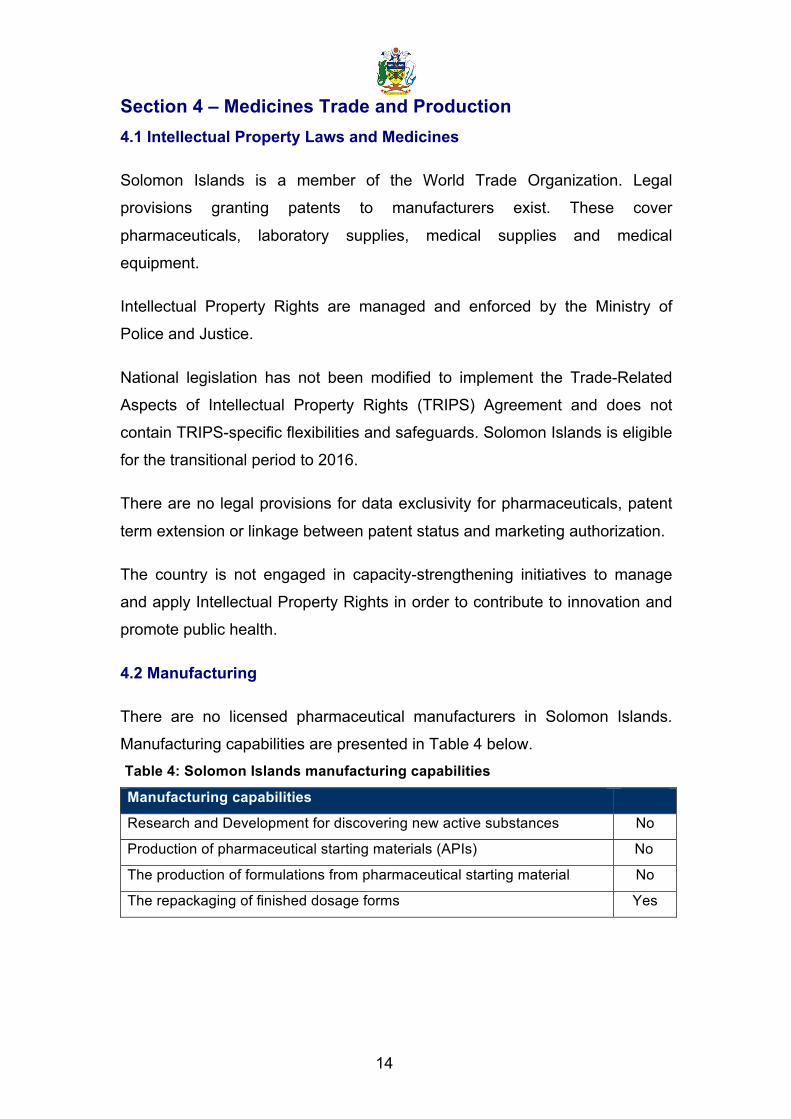
4.2 Manufacturing
There are no licensed pharmaceutical manufacturers in Solomon Islands.
Manufacturing capabilities are presented in Table 4 below. Table 4: Solomon Islands manufacturing capabilities
Manufacturing capabilities
Research and Development for discovering new active substances No
Production of pharmaceutical starting materials (APIs) No
The production of formulations from pharmaceutical starting material No
The repackaging of finished dosage forms Yes

15
Further information and key findings:
Very little work has been done addressing TRIPS compliance; this is likely to be a major issue in the coming three years. It is not expected to impact heavily on the Solomon Islands in the medium-‐term however, as few innovator drugs are currently on the Essential Medicines List.
There are no plans to stimulate local production or manufacture, as the market is small, there is a lack of capacity and funding capital to commence operations, it is difficult to maintain proper manufacturing conditions in this environment and the Solomon Islands is poorly situated for the export market.
Key recommendations:
It is recommended that Trade-‐Related Aspects of Intellectual Property Rights (TRIPS) compliant, health sensitive Laws be developed to enable access to affordable medicines that are needed to address the health problems of Solomon Islands.
§ The Government should take advantage of all the flexibilities and safeguards within the TRIPS Agreement for the promotion of public health and ensuring access to pharmaceuticals.
§ The implications of international trade and other treaties should be studied so as to safeguard the national interest concerning public health and ensure access to pharmaceuticals. In particular, any potential Free Trade Agreement will be examined in detail to ensure that flexibilities available under the TRIPS agreement are not affected.
§ The Ministry of Health and Medical Services should collaborate with the Ministries of Trade and Commerce, Foreign Affairs and External Trade, and other relevant agencies in the area of Intellectual Property Rights in developing a legal framework that enhances access to essential medicines including grant of compulsory licensing and parallel importation and Government Use. Public health and access to pharmaceuticals must remain in the forefront while undertaking and signing any bilateral or international treaties or agreements.
16
Section 5 – Medicines Regulation
This section details the pharmaceutical regulatory framework, resources,
governing institutions and practices in Solomon Islands.
5.1 Regulatory Framework
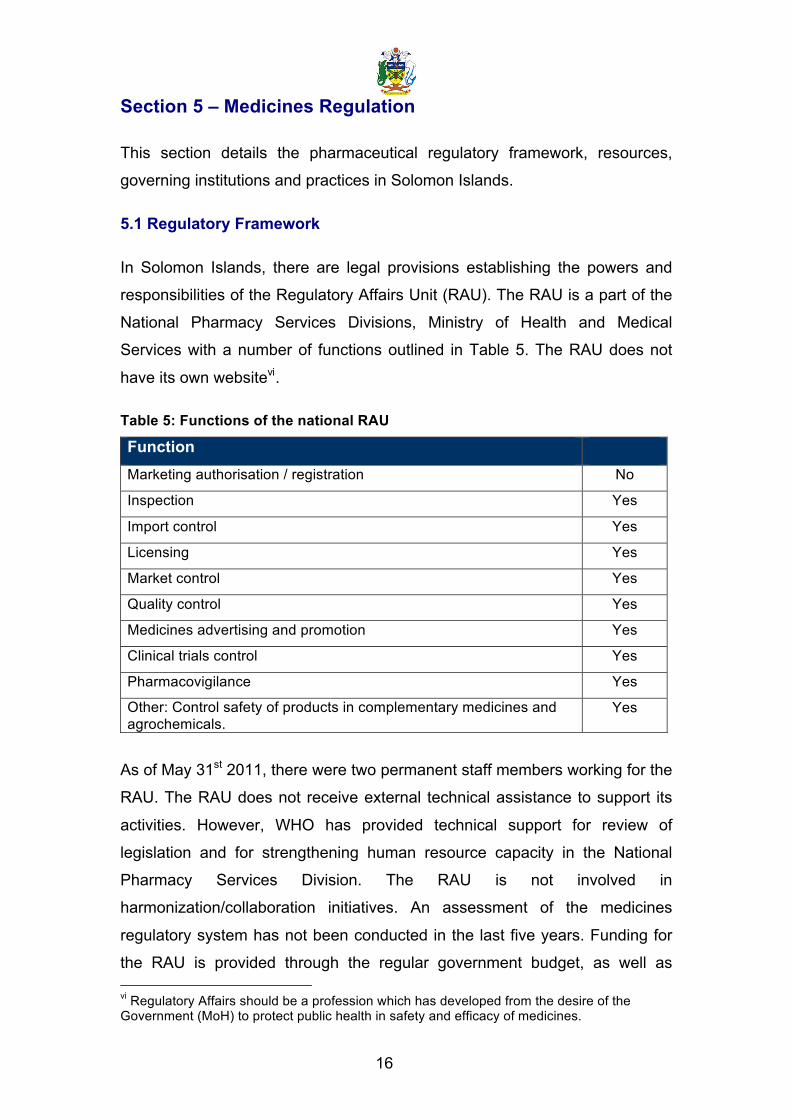
In Solomon Islands, there are legal provisions establishing the powers and
responsibilities of the Regulatory Affairs Unit (RAU). The RAU is a part of the
National Pharmacy Services Divisions, Ministry of Health and Medical
Services with a number of functions outlined in Table 5. The RAU does not
have its own websitevi.
Table 5: Functions of the national RAU
Function Marketing authorisation / registration No
Inspection Yes
Import control Yes
Licensing Yes
Market control Yes
Quality control Yes
Medicines advertising and promotion Yes
Clinical trials control Yes
Pharmacovigilance Yes
Other: Control safety of products in complementary medicines and agrochemicals.
Yes
As of May 31st 2011, there were two permanent staff members working for the
RAU. The RAU does not receive external technical assistance to support its
activities. However, WHO has provided technical support for review of
legislation and for strengthening human resource capacity in the National
Pharmacy Services Division. The RAU is not involved in
harmonization/collaboration initiatives. An assessment of the medicines
regulatory system has not been conducted in the last five years. Funding for
the RAU is provided through the regular government budget, as well as vi Regulatory Affairs should be a profession which has developed from the desire of the Government (MoH) to protect public health in safety and efficacy of medicines.
17
through additional sources. The RAU is primarily funded through the Ministry
of Health and Medical Services and its officers are public servants. Minor
revenues derived from regulatory activities (such as registration fees for
pharmacy professionals and registration of premises) are kept within the RAU
but constitute only a fractional basis of funding. This body does not utilize a
computerized information management system to store and retrieve
information on processes that include registrations, inspection etc.
5.2 Marketing Authorization (Registration)
In Solomon Islands, there are no legal provisions requiring marketing
authorization (registration) for all pharmaceutical products on the market.
Criteria for assessing applications for marketing authorization of
pharmaceutical products do not exist. There are no pharmaceutical products
registered in Solomon Islands. There is a need to support the RAU with
regard to product registration. No registration system currently exists. (See
Box: Further Information and Key Findings at the end of this section for the
current status of pharmacy-related Legislation.)
In the public sector, only those items contained on the Essential Medicines
List are approved for import and supply; the EML is overseen by the National
Drugs and Therapeutics Committee. In the private sector, there is no form of
registration at all; pharmacies are bound by legislation on scheduling of
medicines (and require import permits) but this legislation is out-dated, many
items are not listed on schedules at all and the entire legislation system is
currently under review, with WHO support. It is anticipated that new legislation
and scheduling will go to parliament in 2013.
5.3 Regulatory Inspection
In Solomon Islands, legal provisions exist allowing for appointment of
government pharmaceutical inspectors. Legal provisions permitting inspectors
to inspect premises where pharmaceutical activities are performed exist; such
inspections are required by law and are a pre-requisite for the licensing of
public and private facilities. Where inspections are legal requirements, these
18
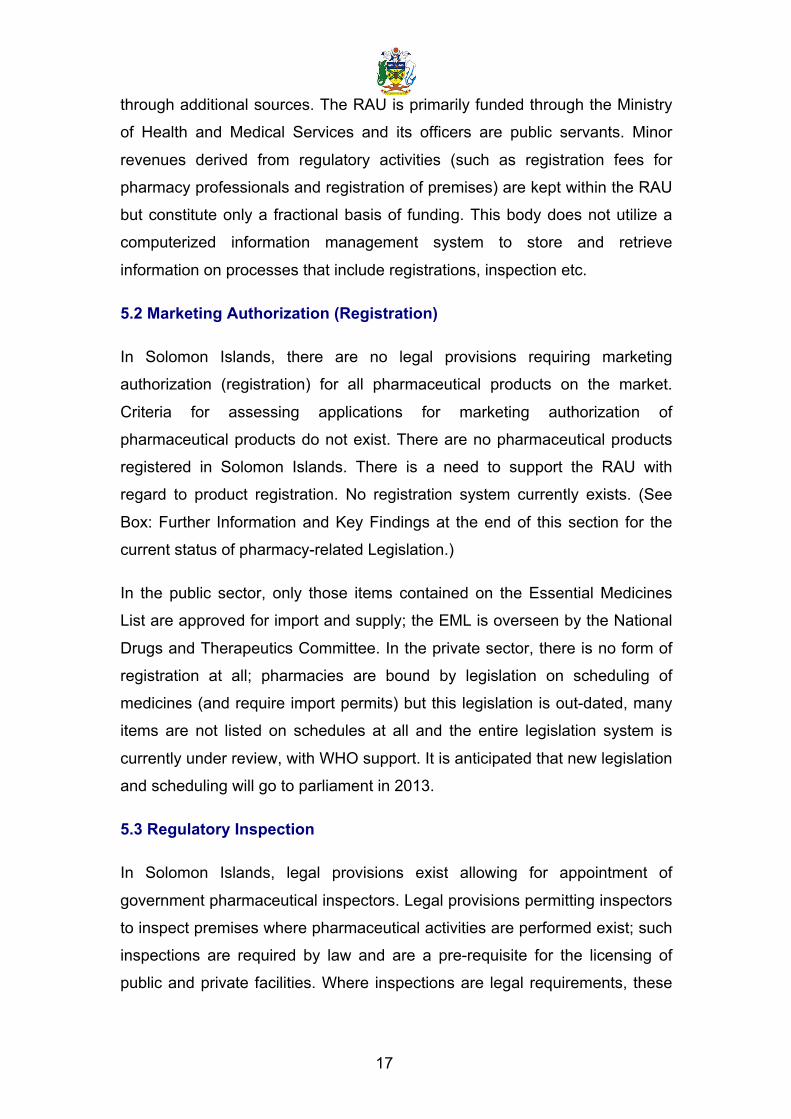
are not the same for public and private facilities. Inspections are carried out
on a number of entities, outlined in Table 6.
Table 6: Local entities inspected for compliance
Entity Inspection Frequencyvii
Local manufacturers No N/A
Private wholesalers Yes Annual
Retail distributors Yes Annual
Public pharmacies and stores Yes Annual
Pharmacies and dispensing points of health facilities
Yes Annual
N/A: not applicable
5.4 Import Control
Legal provisions requiring authorization to import medicines exist. Laws that
allow the sampling of imported products for testing exist. Legal provisions
requiring importation of medicines through authorized ports of entry also exist.
Regulations or laws to allow for inspection of imported pharmaceutical
products at authorized ports of entry exist.
5.5 Licensing
In Solomon Islands, legal provisions requiring manufacturers to be licensed
exist. Legal provisions requiring manufacturers (both domestic and
international) to comply with Good Manufacturing Practices (GMP) also exist.
Good Manufacturing Practices are not published by the government.
Legal provisions requiring importers, wholesalers and distributors to be
licensed exist. Legal provisions requiring wholesalers and distributors to
comply with Good Distribution Practices (GDP) exist.
vii Annual inspections for all facilities unless urgent issues arise
19
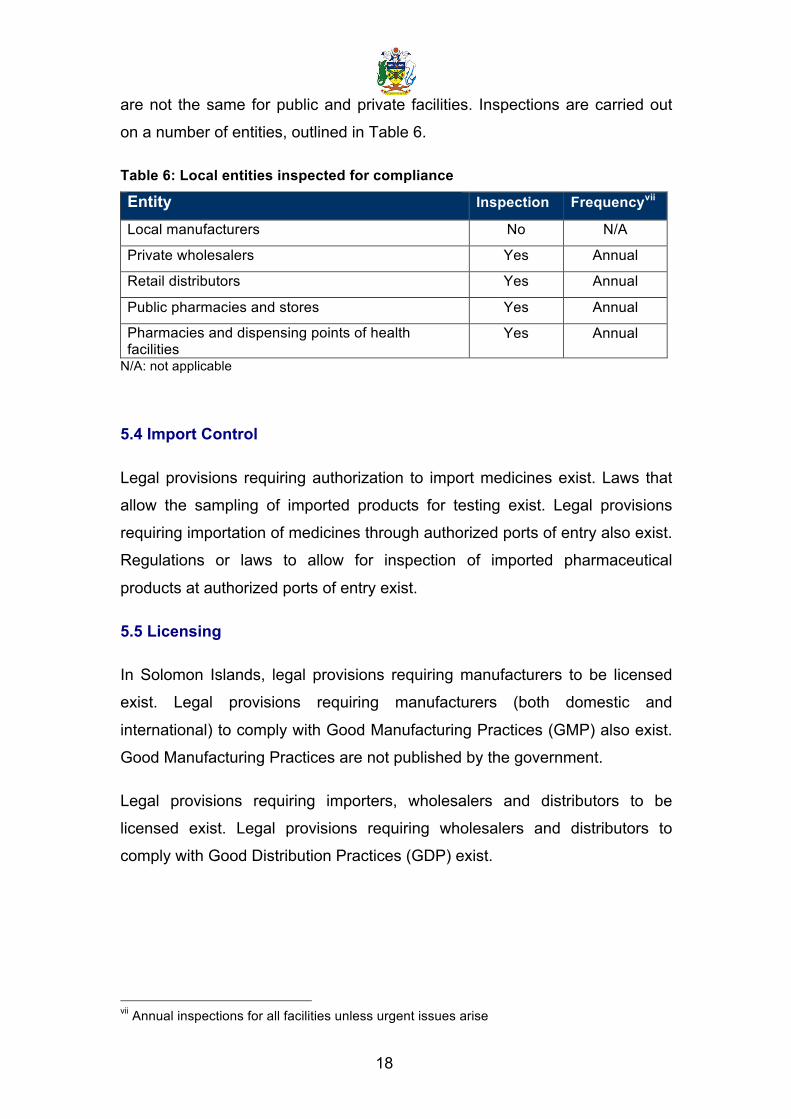
Table 7: Legal provisions pertaining to licensing
Entity requiring licensing Importers Yes
Wholesalers Yes
Distributors Yes
Good Distribution Practices are not published by the government but GDP is
covered in the National Medicines Policy and included in the training
curriculum for Pharmacy Officers.
Legal provisions requiring pharmacists to be registered exist. Legal provisions
exist requiring private, but not public, pharmacies to be licensed. National
Good Pharmacy Practice Guidelines are published by the government. By law,
a list of all licensed pharmaceutical facilities is required to be published.
5.6 Market Control and Quality Control
In Solomon Islands, whilst legal provisions for controlling the pharmaceutical
market exist, quality control testing has not taken place for several years. A
Medicine Quality Control Laboratory does not exist and the MRA does not
contract quality testing services elsewhere. Medicines are visually inspected
in the public sector for a number of reasons, summarised in Table 8.
Table 8: Reason for medicines testing
Medicines tested: For quality monitoring in the public sectorviii Yes
For quality monitoring in the private sectorix No
When there are complaints or problem reports Yes
For product registration No
For public procurement prequalification Yes
For public program products prior to acceptance and/or distribution Yes
viii Routine sampling in pharmacy stores and health facilities ix Routine sampling in retail outlets
20
Samples are not collected by government inspectors for undertaking post-
marketing surveillance testing. The results of quality testing are not publicly
available.
5.7 Medicines Advertising and Promotion
In Solomon Islands, legal provisions to control the promotion and/or
advertising of prescription medicines exist. The Regulatory Affairs Unit is
responsible for regulating promotion and/or advertising of medicines. Legal
provisions prohibit direct advertising of prescription medicines to the public.
Pre-approval for medicines advertisements and promotional materials is not
required. Guidelines and Regulations for advertising and promotion of non-
prescription medicines do not exist. There is a national code of conduct
concerning advertising and promotion of medicines by marketing authorization
holders. The code of conduct applies to both domestic and multinational
manufacturers, for which adherence is voluntary. The code does not contain a
formal process for complaints and sanctions. A list of the complaints and
sanctions for the last two years is not publicly available.
5.8 Clinical Trials
In Solomon Islands, legal provisions requiring authorization for conducting
clinical trials do exist. Approval of clinical trials is undertaken by the National
Ethics Committee within the Ministry of Health and Medical Services.
Clinical trials are required to be entered into an international/national/regional
registry, by law.
Legal provisions do not exist for GMP compliance of investigational products.
Sponsor investigators are not legally required to comply with Good Clinical
Practices (GCP). National GCP regulations are not published by the
Government. Legal provisions do not permit the inspection of facilities where
clinical trials are performed.
21
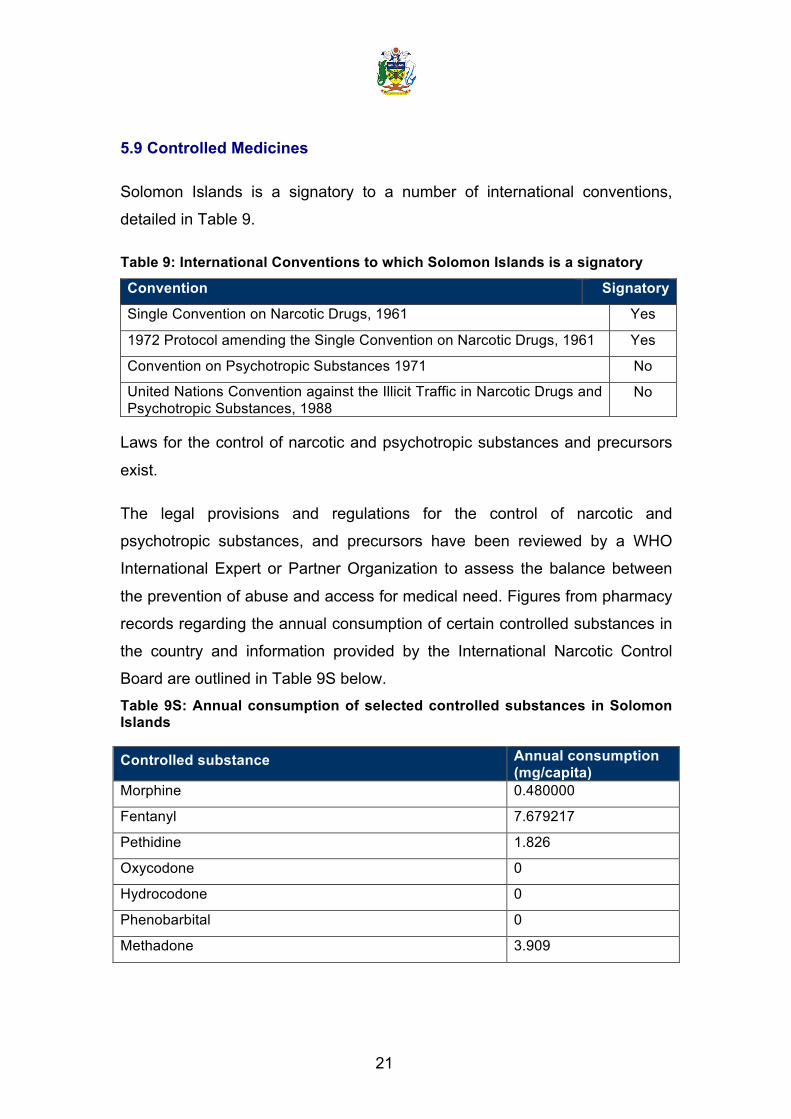
5.9 Controlled Medicines
Solomon Islands is a signatory to a number of international conventions,
detailed in Table 9.
Table 9: International Conventions to which Solomon Islands is a signatory
Convention Signatory
Single Convention on Narcotic Drugs, 1961 Yes
1972 Protocol amending the Single Convention on Narcotic Drugs, 1961 Yes
Convention on Psychotropic Substances 1971 No
United Nations Convention against the Illicit Traffic in Narcotic Drugs and Psychotropic Substances, 1988
No
Laws for the control of narcotic and psychotropic substances and precursors
exist.
The legal provisions and regulations for the control of narcotic and
psychotropic substances, and precursors have been reviewed by a WHO
International Expert or Partner Organization to assess the balance between
the prevention of abuse and access for medical need. Figures from pharmacy
records regarding the annual consumption of certain controlled substances in
the country and information provided by the International Narcotic Control
Board are outlined in Table 9S below. Table 9S: Annual consumption of selected controlled substances in Solomon Islands
Controlled substance Annual consumption (mg/capita)
Morphine 0.480000
Fentanyl 7.679217
Pethidine 1.826
Oxycodone 0
Hydrocodone 0
Phenobarbital 0
Methadone 3.909
22
5.10 Pharmacovigilance
In Solomon Islands, there are no legal provisions in the Drugs and Poisons
Act that provide for pharmacovigilance activities as part of the MRA mandate. Legal provisions requiring the Marketing Authorization holder to continuously
monitor the safety of their products and report to the MRA do not exist. Laws
regarding the monitoring of Adverse Drug Reactions (ADRs) do not exist in
Solomon Islands. A national pharmacovigilance centre linked to the MRA
exists. The Pharmacovigilance Centre has one staff member, who is also
responsible for the Medicines Information Centre. The Centre has not
published an analysis report in the previous two years and it does not publish
a regular ADR bulletin; it undertakes only fledgling pharmacovigilance and will
require strengthening in the next two to three years.
An official standardized form for reporting ADRs is used in Solomon Islands.
Feedback is not provided to reporters. Information pertaining to ADRs is not
stored in a national ADR database.
There is no national ADR or pharmacovigilance advisory committee able to
provide technical assistance or causality assessment, risk assessment, risk
management, case investigation and, where necessary, crisis management
including crisis communication in Solomon Islands. A clear communication
strategy for routine communication and crises communication does not exist.
ADRs are monitored in some public health programs (for example
tuberculosis, HIV-related disease, malaria). A number of steps are being
considered in order to enhance the pharmacovigilance system. For example,
funding exists for a consultant to review the pharmacovigilance mechanisms
in the country with a view to establishing a database for at least some drugs
(e.g. anti-malarial drugs). A standardised form is already in place but this
requires promotion and staff are not currently available to undertake this.
Medication errors (MEs) are not reported. A risk management plan is not
presented as part of the product dossier submitted for Marketing Authorization.

23
In the last two years there has not been a regulatory decision based on local
pharmacovigilance. There are no training courses in pharmacovigilance.
Further information and key findings:
With WHO support, pharmaceutical legislation was reviewed in Solomon Islands. The Pharmacy Practitioners’ Act and Pharmacy & Poisons Act were re-‐drafted, along with subsidiary regulations to be reviewed by the Pharmacy Board following a period of stakeholder consultations. After presentation to the Attorney General’s office, presentation to parliament is expected in 2013.
Very little work has been done addressing TRIPS compliance; this is likely to be a major issue in the coming three years. It is not expected to impact heavily on Solomon Islands in the medium-‐term however, as few innovator drugs are currently on the Essential Medicines List.
There are no plans to stimulate local production or manufacture, as the market is small, there is a lack of capacity and funding capital to commence operations, it is difficult to maintain proper manufacturing conditions in this environment and Solomon Islands is poorly situated for the export market.

24
Key recommendations:
TRIPS
It is recommended that Trade-‐Related Aspects of Intellectual Property Rights (TRIPS) compliant, health sensitive laws be developed to enable access to affordable medicines that are needed to address the health problems of Solomon Islands.
§ The Government should take advantage of all the flexibilities and safeguards within the TRIPS Agreement for the promotion of public health and ensuring access to pharmaceuticals.
§ The implications of international trade and other treaties should be studied so as to safeguard the national interest concerning public health and ensure access to pharmaceuticals. In particular, any potential Free Trade Agreement will be examined in detail to ensure that flexibilities available under the TRIPS agreement are not affected.
§ The Ministry of Health and Medical Services should collaborate with the Ministries of Trade and Commerce, Foreign Affairs and External Trade, and other relevant agencies in the area of Intellectual Property Rights in developing a legal framework that enhances access to essential medicines including grant of compulsory licensing and parallel importation and Government Use. Public health and access to pharmaceuticals must remain in the forefront while undertaking and signing any bilateral or international treaties or agreements.
Regulatory Affairs
There is a need to support the Regulatory Affairs Unit with regard to product registration. Regulatory Affairs should strengthened to protect public health in safety and efficacy of medicines. The MRA should be strengthened to cover licensing and control of importation and monitoring of medicines throughout the system, including public, private, non-‐government and faith based organisations, to ensure adherence to quality standards and specifications. It should include capacity for investigation within different phases of importation, quality control, distribution and use of medicines.
Pharmacovigilance and medication errors
A pharmacovigilance system with ADR monitoring capacity should be developed as a priority, possibly within a strengthened Medicines Information Unit with strong links with the National Drugs and Therapeutics Committee. A system for reporting and dealing with medication errors should be included.
25
Section 6 - Medicines Financing
In this section, information is provided on the medicines financing mechanism
in Solomon Islands, including the medicines coverage through public and
private health insurance, use of user charges for medicines and the existence
of public programmes providing free medicines. Policies and regulations
affecting the pricing and availability of medicines (e.g. price control and taxes)
are also discussed.
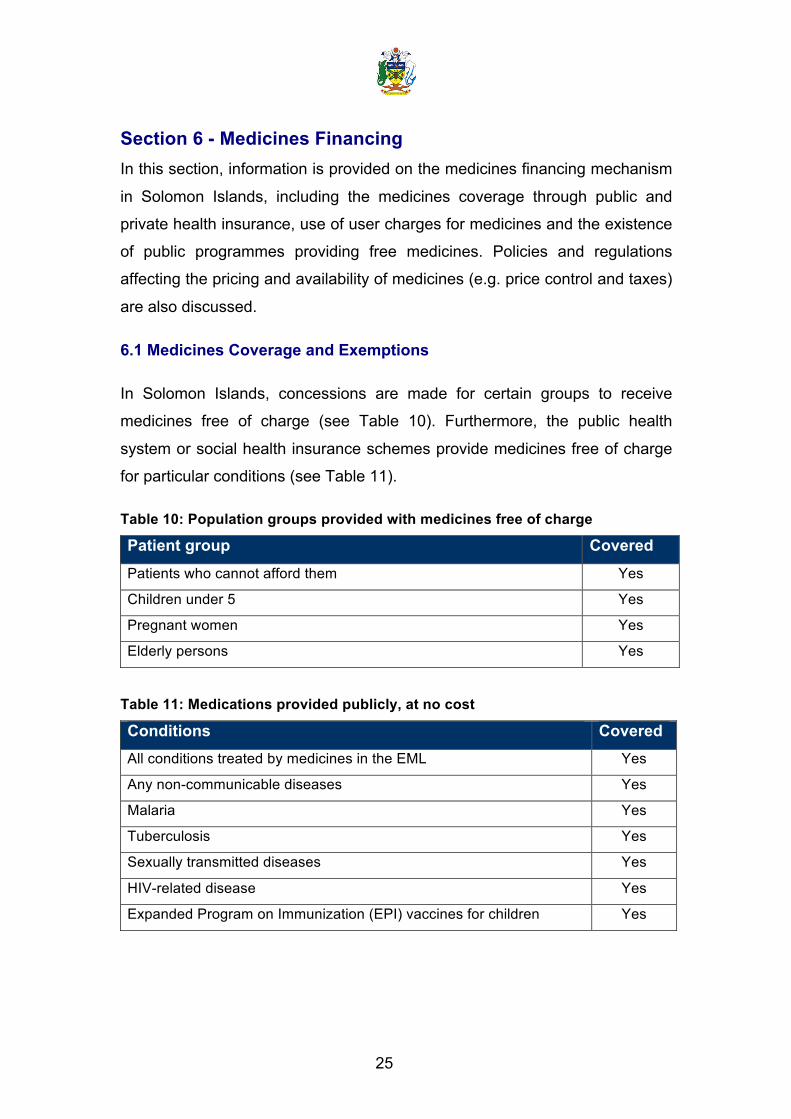
6.1 Medicines Coverage and Exemptions
In Solomon Islands, concessions are made for certain groups to receive
medicines free of charge (see Table 10). Furthermore, the public health
system or social health insurance schemes provide medicines free of charge
for particular conditions (see Table 11).
Table 10: Population groups provided with medicines free of charge
Patient group Covered Patients who cannot afford them Yes
Children under 5 Yes
Pregnant women Yes
Elderly persons Yes
Table 11: Medications provided publicly, at no cost
Conditions Covered All conditions treated by medicines in the EML Yes
Any non-communicable diseases Yes
Malaria Yes
Tuberculosis Yes
Sexually transmitted diseases Yes
HIV-related disease Yes
Expanded Program on Immunization (EPI) vaccines for children Yes
26
A public health service provides coverage for medicines that are on the
Essential Medicines List (EML) for inpatients and outpatients. Furthermore, all
patients (except foreign nationals) receive all medicines free of charge;
foreign nationals are provided free medical services and drugs in emergency
situations, under an informal system. Only medicines on the EML are
available within the public sector.
Private health insurance schemes do not provide medicines coverage. Some
private companies do provide healthcare to their employees but they do so at
their own expense and generally within the restrictions of the EML.
6.2 Patients Fees and Co-payments
Co-payments or fee requirements for consultations are levied at the point of
service delivery. However, there are no co-payments or fee requirements
imposed for medicines. Whilst there is officially no co-payment system, many
clinics will request a 'donation' or contribution for medical consultations or
medicines. Most often, these contributions go towards infrastructure or local
medical transport costs. However, there is no evidence to suggest they are
being used for staff wages or payments.
6.3 Pricing Regulation for the Private Sectorx
In Solomon Islands, there are no legal or regulatory provisions affecting
pricing of medicines.
The government does not run an active national medicines price monitoring
system for retail prices. Regulations do not exist mandating that retail
medicine price information should be publicly accessible.
x This section does not include information pertaining to the non-profit voluntary sector

27
6.4 Prices, Availability and Affordability of Key Medicines
There has not been a WHO/HAI pricing survey conducted in the Solomon
Islands and there would be limited benefit in doing so; the private sector is
very small and heavily concentrated in the capital, Honiara.
6.5 Price Components and Affordability
In the past five years, there has not been a survey on medicine price
components conducted in Solomon Islands.
6.6 Duties and Taxes on Pharmaceuticals (Market)
Solomon Islands does not impose duties on imported active pharmaceutical
ingredients (APIs) in the public sector and duties on imported finished
products are also not imposed.

28
Further information and key findings:
Currently, the Australian Agency for International Development (AusAID) funds roughly 90% of the entire drugs budget for the public sector and pressure will continue to be applied to reduce this donor burden. Given likely increases in the national drug budget, due to the continuing health transition increasing the burden on non-‐communicable diseases and increasing public expectations, medicines financing is likely to become increasingly difficult in the next five years.
It is difficult to properly assess improvements in coverage over the last ten years, given a paucity of evidence but anecdotal reports suggest that medicines coverage has markedly improved in the last five years. Improvements have been particularly strong at the national level.
Several disease areas continue to suffer from chronic under-‐funding; these include but are not limited to mental health, oncology and palliative care. The availability of commodities and expertise in these programs is sadly lacking.
There is no political will to introduce co-‐payments for medicines and little evidence to support this policy, in a society that is still primarily subsistence based. Roughly 80% of the population live in rural areas, largely outside the cash economy and international evidence suggests that even minor payment schemes would reduce access for the most vulnerable populations. It is extremely unlikely that any co-‐payment system for medicines in the public sector will be introduced in the next five years.
Informal payments are still requested by some clinics in rural areas; usually these are to support community-‐based projects to improve local health facilities. There has been no study assessing the impact of these informal payments but it is unlikely they have reduced access to medicines for any group.
The largest barrier to access remains geographic factors; by far, the greatest cost for accessing healthcare is transport to the nearest health facility. There is no clearly defined strategy for addressing this within the pharmacy division.
There has been no formal study of the affordability of medicines in the private sector but given the relatively small size of the market, this is not a priority. The private market is estimated to represent between 5 and 10% of the overall pharmaceuticals market in the country, though there has been no assessment of the market.

29
Key recommendations:
The Ministry of Health and Medical Services should effectively advocate for budgetary allocations from the Solomon Islands Government and donor partners, including vertical programs, which should increasingly look to incorporate parallel funding systems into an integrated national pharmacy budget.
Transport and distribution costs must be included in the national pharmacy budget. An improved system of record keeping linked to appropriate quantification of medicines needs at all health facility levels, in line with the National Pharmacy 5 Year Strategic Plan, would provide information concerning coverage with essential medicines.
30
Section 7 - Pharmaceutical Procurement and Distribution in the Public Sector
This section provides a short overview on the procurement and distribution of
pharmaceuticals in the public sector of Solomon Islands.
7.1 Public Sector Procurement
The public sector procurement is centralized under the responsibility of
National Medical Store (NMS), which is a part of the National Pharmacy
Service Division, MHMS. Pharmaceuticals and medical supplies procured by
National Medical Store are distributed through its Provincial Medical Stores to
primary healthcare facilities.
Tender documents can be obtained from the mSupply data base system used
for procurement. The mSupply system generates reports on all awards and
they are publicly available. Hard copies can be obtained from the NMS.
Procurement is based on the prequalification of suppliers. Prequalification is
performed through the World Bank Prequalification exercise; selection of bids
is based on prior performance, quality assurance, lead times and price
according to the National Medical Stores Procurement Plan and Tender
Guidelines.
There is a written policy for public sector procurement. This policy was
approved in 2010. Legal provisions that give priority to locally produced goods
in public procurement do not exist, as there is no local pharmaceutical
manufacturer. The National Medical Stores Procurement Plan and Tender
Guidelines were approved in 2012.
A Pharmaceutical Tender Board (PTB) performs selection and awards. The
awards are then sent to the Medical Tender Board (MTB) which is the contact
for the Central Tender Board. These two boards approve awards for specific
pharmaceutical supplies or rubber stamp them, because the technicalities
associated with pharmaceutical procurement are performed by the PTB. The
31
PTB is separate but includes a person from the MTB for transparency
requirements.
A process exists to ensure the quality of products that are publicly procured.
Explicit criteria and procedures for prequalification of suppliers exist and a list
of prequalified suppliers and products is publicly available.
In accordance with Solomon Islands Government Financial Instructions, all
major tenders are required to be approved by the Central Tender Board,
within the Ministry of Finance & Treasury.
The tender methods employed in public sector procurement include
international competitive restricted tenders and direct purchasing; Standing
Offer Arrangements for all products are established following each annual
tender, reducing the requirement for non-competitive direct purchasing or
onerous Request-for-Quotations needing to be separately issued. All
purchasing is now done using prequalified suppliers.
7.2 Public Sector Distribution
The National Pharmacy Service Division, MHMS has a Central Medical Store
(called “National Medical Store”) at the national level. There are 14 public
warehouses (Second Level Medical Stores or Provincial Medical Stores) in
the secondary tier of the public sector distribution. There are no national
guidelines on Good Distribution Practices (GDP) but there are National
Pharmacy Standards defining the role, function and infrastructure
requirements of Second Level Medical Stores. A licensing authority that
issues GDP licenses does not exist so a list of GDP certified warehouses or
distributors does not exist in the public sector.
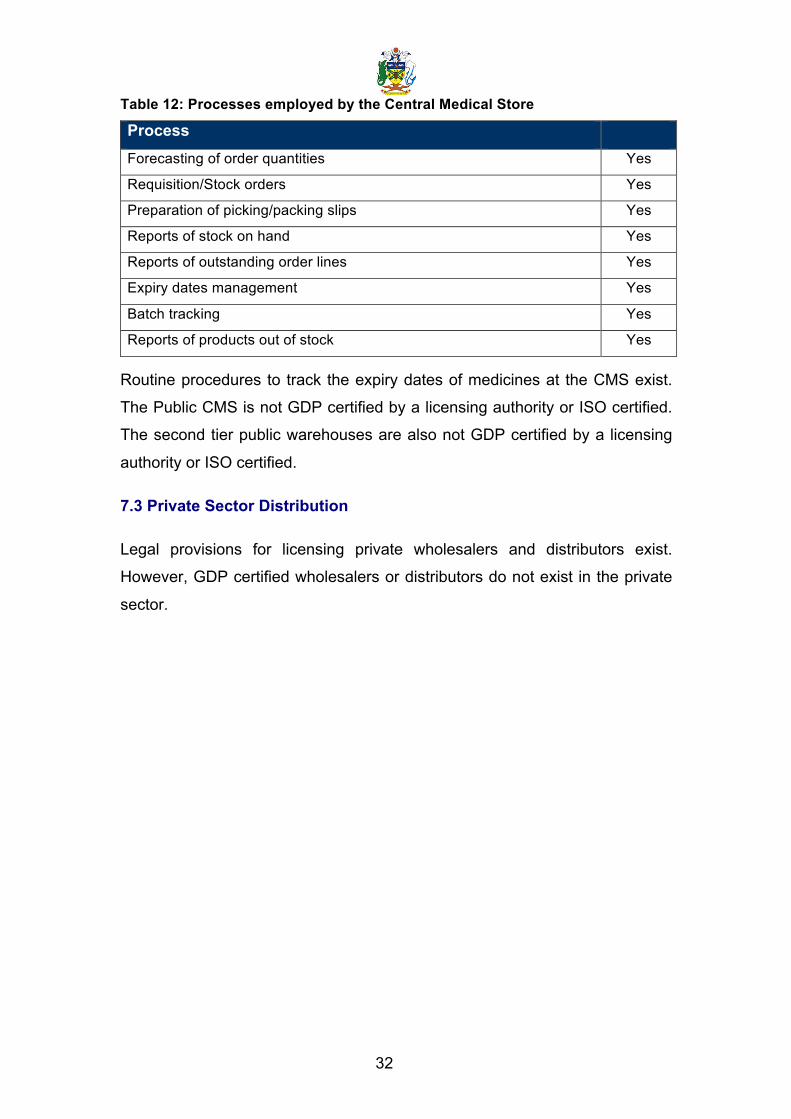
A number of processes are in place at the CMS as detailed in Table 12.
32
Table 12: Processes employed by the Central Medical Store
Process
Forecasting of order quantities Yes
Requisition/Stock orders Yes
Preparation of picking/packing slips Yes
Reports of stock on hand Yes
Reports of outstanding order lines Yes
Expiry dates management Yes
Batch tracking Yes
Reports of products out of stock Yes
Routine procedures to track the expiry dates of medicines at the CMS exist.
The Public CMS is not GDP certified by a licensing authority or ISO certified.
The second tier public warehouses are also not GDP certified by a licensing
authority or ISO certified.
7.3 Private Sector Distribution
Legal provisions for licensing private wholesalers and distributors exist.
However, GDP certified wholesalers or distributors do not exist in the private
sector.

33
Further information and key findings:
The National Essential Medicines List is overseen by the National Drugs & Therapeutics Committee, although under its current mandate, this is an advisory body only; all decisions can technically be over-‐ruled by the Ministry of Health Executive (though this power has never been exercised).
National Medical Stores is then charged with procuring and distributing all essential medicines through the public sector. It does this through prequalified suppliers; the prequalification criteria has recently been re-‐drafted, using the WHO Prequalification questionnaire templates.
Three major documents have been developed in recent years to improve procurement and distribution systems:
1. SI National Pharmacy Standards: These standards, believed to be amongst the first of their kind in the developing setting, establish uniform criteria for all provincial Second Level Medical Stores across 11 functional areas, including HR, Infrastructure, Stock Management, Dispensing etc. Each facility is assessed annually by senior staff within Pharmacy Division.
2. Standard Operating Procedures for National Medical Stores: The NMS SOPs establish all processes within the NMS facility, across core and supplementary activities such as Goods Receipt, Dispatch, Inventory Management, Waste Disposal etc.
3. National Procurement Plan and Annual Tender Guidelines: This combined document sets out the framework by which procurement is undertaken by the National Pharmacy Services Division and also establishes a step-‐by-‐step plan on how to undertake an annual tender, from budgeting and planning, through quantification, bid evaluation etc.
At the primary healthcare level, stock-‐outs of critical items are still common. Plans are currently in place to further strengthen provincial distribution through the development and implementation of a national distribution plan and the modernising of distribution systems, using increasing IT functionality. The Division is working with software partner Sustainable Solutions to implement these improvements.
Key recommendations:
In addition to training and application of the National Pharmacy Standards, the SOPs for National Medical Stores and the National Procurement Plan and Annual Tender Guidelines efforts should be focussed on the primary level where stock-‐outs are still common.
Introduction of SOPs and standard Order Forms relevant for the stock appropriate for each particular health service should be introduced to maintain reliable supplies of essential medicines and avoid stock-‐outs. Training associated with adherence to STGs and maintenance of records of use should be linked to appropriate quantification of medicines needs at all health facility levels, in line with the National Pharmacy 5 Year Strategic Plan.
34
Section 8 - Selection and Rational Use of Medicines
This section outlines the structures and policies governing the selection of
essential medicines and promotion of rational medicines use in Solomon
Islands.
8.1 National Structures
A National Essential Medicines List (EML) exists in Solomon Islands. The
EML was lastly updated in 2010 and is publicly available. There are currently
475 medicines on the EML. Selection of medicines for the EML is overseen by
the National Drugs and Therapeutics Committee through a written process. A
mechanism aligning the EML with the Standard Treatment Guidelines is in
place.
National Standard Treatment Guidelines (STGs) for most common illnesses
are produced and endorsed by the Ministry of Health and Medical Services in
Solomon Islands. These were last updated in 2011. Specific STGs cover
primary care (updated in 2011) and paediatric conditions (updated in 2009).
Of the public health facilities, 100% have a copy of the EML and 100% have a
copy of the STGs.
There is a public or independently funded national Medicines Information
Centre (MIC) providing information on medicines to prescribers, dispensers
and consumers. Public education campaigns on rational medicine use topics
have been conducted in the last two years. A survey on rational use of
medicines has not been conducted in the previous two years. There is a
national programme and committee, involving government, civil society and
professional bodies, to monitor and promote rational use of medicines.
The MIC printed and launched the 2013 update of the Solomon Islands
Essential Medicines List. They have also developed and are rolling out a
package of interventions to improve the availability and usage of priority
medicines for mothers and children. Interventions include research on zinc
sulphate and ORS for child diarrhoea. In 2012 a comprehensive pilot study
35
was undertaken in one province to ascertain the availability of zinc sulphate in
health facilities, staff knowledge of the rationale for its use and correct use of
zinc sulphate with ORS for diarrhoea. It was demonstrated that it is possible
to increase the availability and comprehension of zinc sulphate for use in
children with diarrhoea, with a series of low-cost, contextually appropriate
interventions. This pilot study will now be rolled out across all provinces;
further work may also focus on all 30 WHO Priority Medicines for Mothers &
Children. This work is likely to be reproducible in similar settings across the
Pacific but more methodological rigour is needed in larger studies. The report
of the study is available from the Pharmacy Services Division.
Other activities carried out by the unit are: two-way radio programs with
nurses in rural areas, printing of special bulletins and Pharmacy Newsletters
that contain information on various drugs, targeting irrational use of medicines
and focus on changes in treatment such as the use of artemesinin compound
treatment for malaria and other current areas of concern.
A written National Strategy for Containing Antimicrobial Resistance does not
exist.
The Solomon Islands’ EML includes formulations specifically for children.
Criteria for the selection of medicines in the EML are explicitly documented. A
formal committee for the selection of products on the EML exists. Conflict of
interest declarations are not required from members of the national EML
committee. A national medicines formulary does not exist.
A funded national inter-sectoral task force to coordinate the promotion of the
appropriate use of antimicrobials and prevention of the spread of infection
does not exist. A national reference laboratory or other institution does not
have responsibility for coordinating epidemiological surveillance of
antimicrobial resistance.
36
8.2 Prescribing
Legal provisions exist to govern the licensing and prescribing practices of
prescribers. Furthermore, legal provisions restricting dispensing by
prescribers exist. Prescribers in the private sector dispense medicines.
There is a National Drugs and Therapeutics Committee (NDTC), as mandated
by the Ministry of Health and Medical Services that oversees the development
and revision of the Essential Medicines List and all Standard Treatment
Guidelines. Provincial Hospitals do not have separate DTCs; the NDTC is
based at the only referral hospital in the country.
Mandatory continuing education that includes rational use of medicines is
required for doctors and nurses, but not for paramedical staff.
Prescribing by INN is obligatory in the public sector, but not in the private
sector. Of the medicines prescribed in the outpatient public health care
facilities, 100% are on the national EML.
A professional association code of conduct which governs the professional
behaviour of doctors exists. Similarly, a professional association code of
conduct governing the professional behaviour of nurses also exists.
8.3 Dispensing
Legal provisions in Solomon Islands to govern dispensing practices of
pharmacy personnel exist. The basic pharmacist training curriculum includes
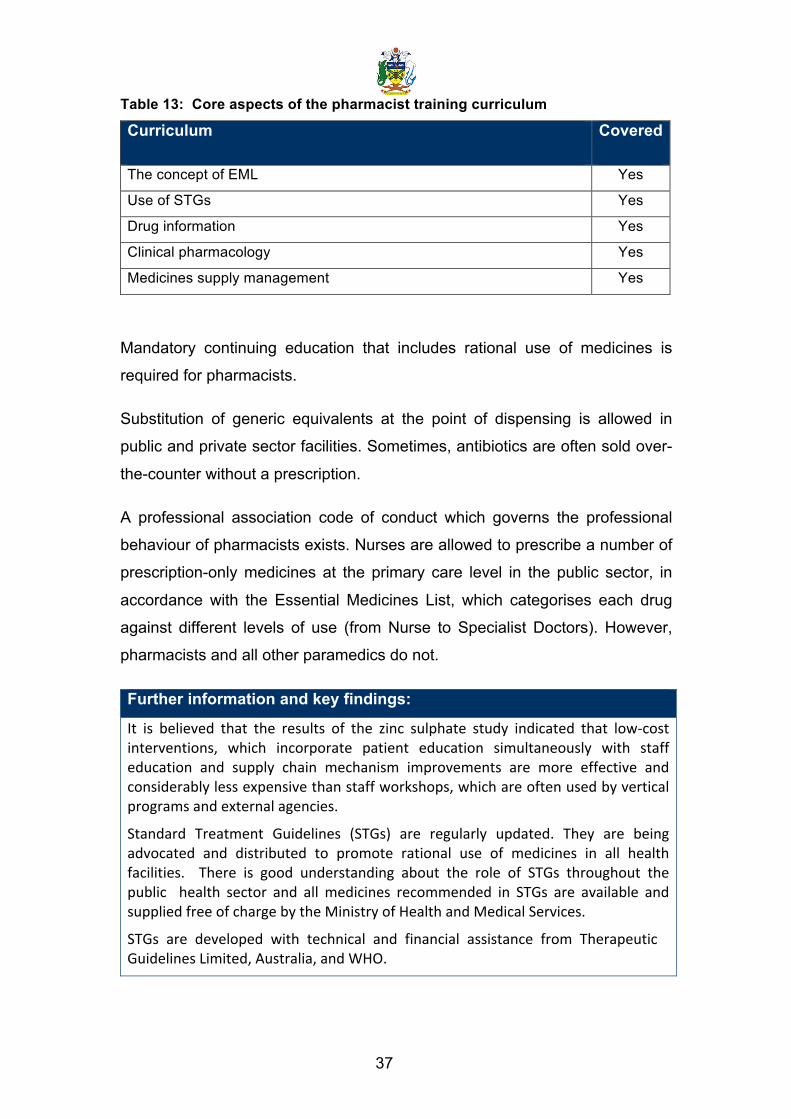
a spectrum of components as outlined in Table 13.
37
Table 13: Core aspects of the pharmacist training curriculum
Curriculum Covered
The concept of EML Yes
Use of STGs Yes
Drug information Yes
Clinical pharmacology Yes
Medicines supply management Yes
Mandatory continuing education that includes rational use of medicines is
required for pharmacists.
Substitution of generic equivalents at the point of dispensing is allowed in
public and private sector facilities. Sometimes, antibiotics are often sold over-
the-counter without a prescription.
A professional association code of conduct which governs the professional
behaviour of pharmacists exists. Nurses are allowed to prescribe a number of
prescription-only medicines at the primary care level in the public sector, in
accordance with the Essential Medicines List, which categorises each drug
against different levels of use (from Nurse to Specialist Doctors). However,
pharmacists and all other paramedics do not.
Further information and key findings:
It is believed that the results of the zinc sulphate study indicated that low-‐cost interventions, which incorporate patient education simultaneously with staff education and supply chain mechanism improvements are more effective and considerably less expensive than staff workshops, which are often used by vertical programs and external agencies.
Standard Treatment Guidelines (STGs) are regularly updated. They are being advocated and distributed to promote rational use of medicines in all health facilities. There is good understanding about the role of STGs throughout the public health sector and all medicines recommended in STGs are available and supplied free of charge by the Ministry of Health and Medical Services.
STGs are developed with technical and financial assistance from Therapeutic Guidelines Limited, Australia, and WHO.

38
Key recommendations:
Activities defined in the Pharmaceutical Service Division 5 Year Strategic Plan 2011 – 2015 will address outstanding issues associated with rational use of medicines. These activities should be supported so they can be undertaken in a timely manner. Among others, activities are defined to strengthen:
• The roles of the Drugs and Therapeutics committee • The maintenance of an updated EML • Training for rational use of medicines; prescribing and dispensing • Patient compliance and self-‐medication • Adverse medicines reaction reporting and response • Medicines Information
Each edition of Standard Treatment Guidelines should be updated every 5 years to maintain currency.
39
Section 9 - Household Data/Access In the past 5 years, no household surveys have been undertaken to assess
the access to medicines.
40
List of key reference documents: International Narcotics Control Board (INCB) (1982). Website: http://www.incb.org/
MDG Goals Progress Report for Solomon Islands, 2010. Available from the Ministry of Health and Medical Services
Ministry of Health, Unpublished data (2010).
Ministry of Police and Justice, Registrar-General's Office, P.O. Box G 15 Honiara, Guadalcanal, Solomon Islands
National Good Pharmacy Practice Guidelines. Available from Pharmacy Services division.
National Health Accounts (NHA) Country Information, “Solomon Islands - National Expenditure on Health (Solomon Dollar) 2009”. Available online: http://www.who.int/nha/country/slb/en/
National Malaria Treatment Guidelines (2009). Available from Pharmacy Services Division.
National Pharmacy Division, “Solomon Islands Essential Medicines List 2010”, Ministry of Health and Medical Services. Available online: http://www.who.int/selection_medicines/country_lists/slb_eml_2010.pdf
National Pharmacy Services Division Complete Five Year Strategic Plan 2011-2015. Available from the National Pharmacy Services Division. .
National Procurement Plan and Annual Tender Guidelines. Available from the National Pharmacy Services Division
Regulatory Affairs, National Pharmacy Division, PO Box 349, Honiara, Solomon Islands
SI National Pharmacy Standards. Available from the National Pharmacy Services Division
SI National Pharmacy Officer Training Curriculum. Available from the Pharmacy Services Division.
Solomon Islands Essential Medicines List, 2010. Available online http://apps.who.int/medicinedocs/documents/s19524en/s19524en.pdf
Solomon Islands Government, “National Health Strategic Plan 2011-2015”, The Ministry of Health & Medical Services, March 2011. Available online: http://www.wpro.who.int/health_services/solomon_islands_nationalhealthplan.pdf
Solomon Islands Guidelines for Donations of Medicines. Available from the Pharmacy Services Division.
Solomon Islands National Medicines Policy. Available from Pharmacy Services Division.
Standard Operating Procedures for National Medical Stores. Available from the National Pharmacy Services Division
Standard Treatment Manual for Adults (2011). Available from Pharmacy Services Division.
Standard Treatment Manual for Children, 3rd Edition, 2009. Available online http://apps.who.int/medicinedocs/documents/s17086e/s17086e.pdf
WHO Solomon Islands Country Profile. Available online http://www.who.int/countries/slb/en/
41
World Bank data (2009). Website: http://data.worldbank.org/
World Health Organization (WHO) (2007), “WHO Level I survey”, Geneva
World Health Organization (WHO) (2009), “World Health Statistics 2009”, WHO Press, Geneva. Available online: http://www.who.int/whosis/whostat/2009/en/index.html.
World Health Organization (WHO) (2010), “World Health Statistics 2010”, WHO Press, Geneva. Available online: http://www.who.int/whosis/whostat/2010/en/index.html.
World Health Organization (WHO) (2011), “World Health Statistics 2011”, WHO Press, Geneva. Available online: http://www.who.int/whosis/whostat/2011/en/index.html
World Health Organization (WHO) Western Pacific Region (2010), “Achieving the Health-Related MDGs in the Western Pacific Region”, Progress Report 2010, WHO Press, Geneva. Available online: http://www.wpro.who.int/health_information_evidence/documents/MDG_Progress_2010_11.pdf
World Health Organization (WHO) Western Pacific Region (2010), “Country Health Information Profiles (CHIPS)”, 2010 Revision, WHO Press, Geneva. Available online: http://www.wpro.who.int/publications/CHIPS2010.pdf
World Health Organization, Western Pacific Region (2010), Consultant's report on National Laboratory Policy and Plan.
World Trade Organization (1996). Available online: http://www.wto.org/english/thewto_e/countries_e/solomon_islands_e.htm