some design issues in microbicide trials august 20, 2003 thomas r. fleming, ph.d. professor and...
TRANSCRIPT

Some Design Issues in Microbicide Trials
August 20, 2003
Thomas R. Fleming, Ph.D.Professor and Chair of Biostatistics
University of Washington
FDA Antiviral Drugs Advisory Committee
Selected Design Issues
• Blinding & the Choice of Controls
• Required Strength of Evidence
• Phase 2 vs Phase 2B vs Phase 3
Selected Design Issues
• Blinding & the Choice of Controls
• Required Strength of Evidence
• Phase 2 vs Phase 2B vs Phase 3
Blinding
~ Bias can occur in certain trials if the treatment the patient is receiving is known to:
- the evaluatorseg., subjective endpoints
- the caregiverseg., hospitalization
- the patient/participanteg., pain, efficacy vs effectiveness
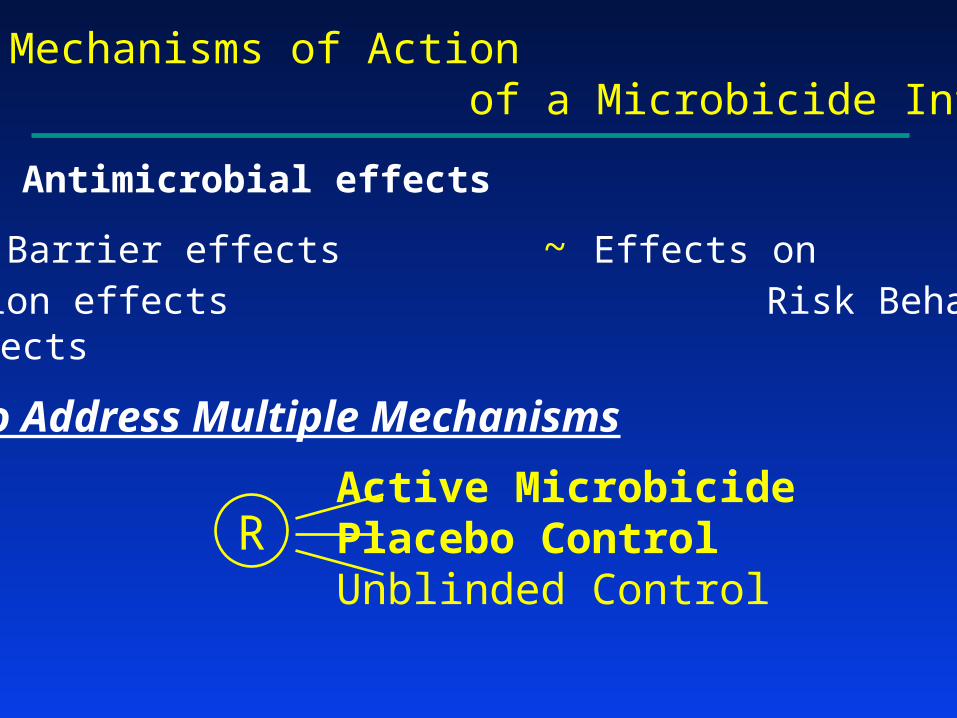
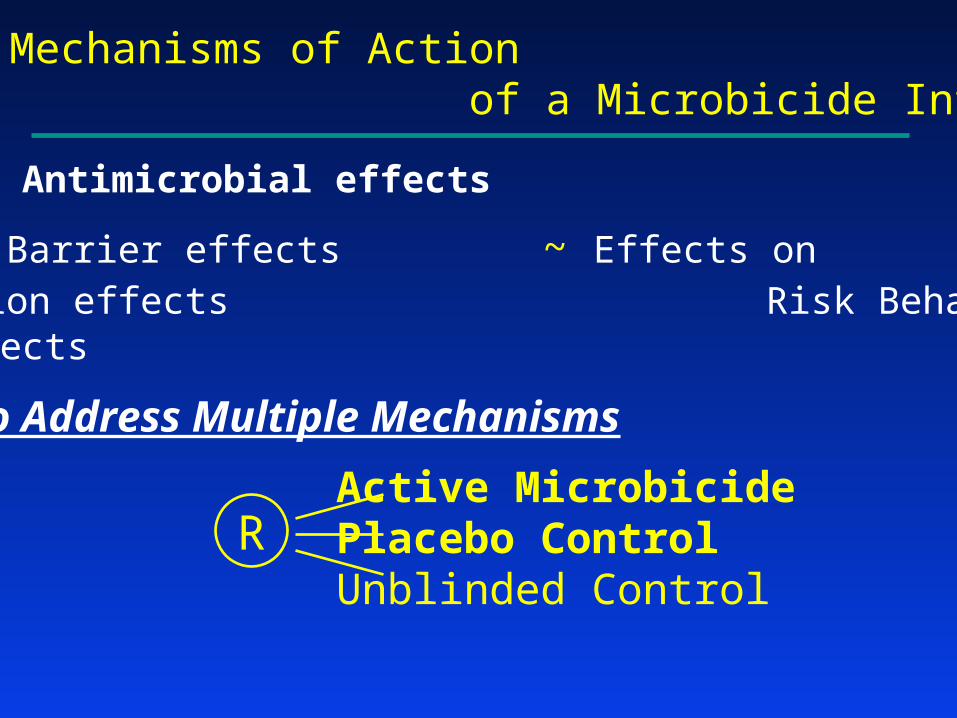
Potential Mechanisms of Action of a Microbicide Intervention
~ Antimicrobial effects
~ Physical Barrier effects ~ Effects on ~ Lubrication effects Risk Behavior~ Other effects
Design to Address Multiple Mechanisms
Active MicrobicidePlacebo ControlUnblinded Control
R
Should one blind?Some factors to consider (Pocock)
• Practicality Treatments • need to be of a similar nature
• cannot induce obvious side effects• Ethics Blinding should not result in harm/risk
• Avoidance of Bias • Is the placebo truly inert? • How serious is the risk of bias without blinding?
… subjective vs objective endpoints
• Importance of understanding Efficacy vs. Effectiveness
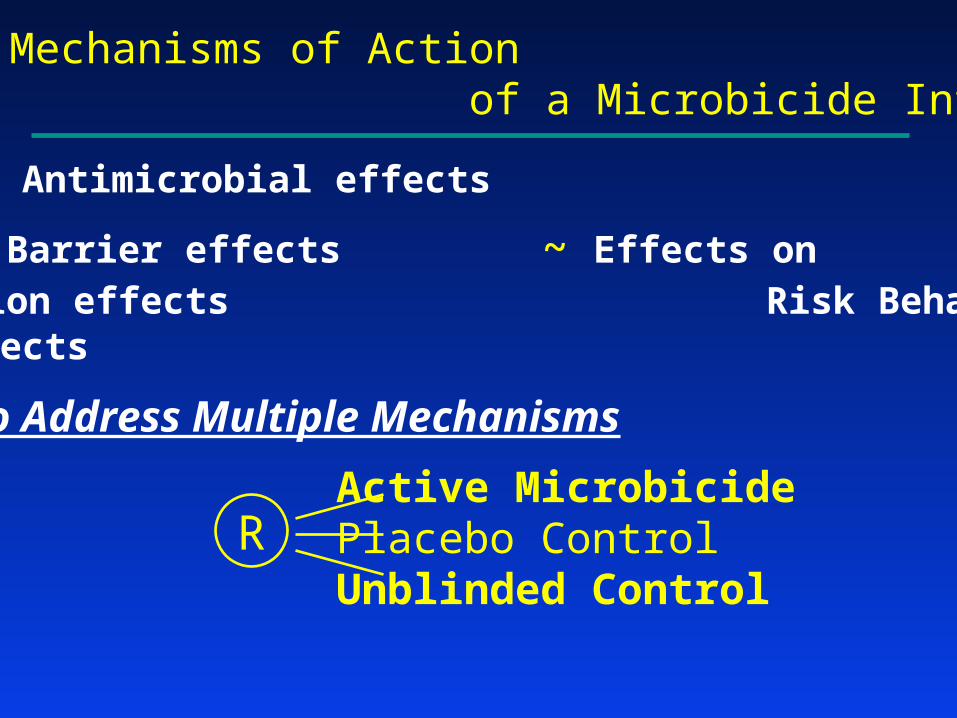
Potential Mechanisms of Action of a Microbicide Intervention
~ Antimicrobial effects
~ Physical Barrier effects ~ Effects on ~ Lubrication effects Risk Behavior~ Other effects
Design to Address Multiple Mechanisms
Active MicrobicidePlacebo ControlUnblinded Control
R
Potential Mechanisms of Action of a Microbicide Intervention
~ Antimicrobial effects
~ Physical Barrier effects ~ Effects on ~ Lubrication effects Risk Behavior~ Other effects
Design to Address Multiple Mechanisms
Active MicrobicidePlacebo ControlUnblinded Control
R

Antimicrobial effects vs. Physical Barrier, Lubrication, & Other effects
Annual Risk in: Active / Placebo / Unbl Control
2% / 2% / 3% 3% / 4.5% / 3%
PLA carries full effect Effectiveness << Efficacy~Use PLA in clinical practice ~Avoidable by advocacy
for adherence to condoms
2% / 2.5% / 3% 2.4% / 3.6% / 3%
PLA carries some effect MIC very effective~Use MIC in clinical practice ~Use MIC in clinical practice
(yet Effectiveness < Efficacy)
3% / 3% / 3% 2% / 3% / 3%
No effect MIC very effective
Selected Design Issues
• Blinding & the Choice of Controls
• Required Strength of Evidence
• Phase 2 vs Phase 2B vs Phase 3
Strength of Evidence Guidelinesfor Regulatory Approval
• Two Adequate and Well Controlled Trials
Statistical significance (for each trial) based on strength of evidence corresponding to a one-sided p 0.025
• A Single Pivotal Trial
(Resource intensive trials, with major clinical endpoints)
Strength of evidence (SOE) that would be “robust and compelling”
Proposed Guideline: SOE corresponding to a one-sided p 0.0025-0.005

Illustration: HPTN 035 Design
• Four arms:
– BufferGel
– PRO 2000/5 Gel (P)
– Placebo control
– Unblinded (condom only) control
• 33% effectiveness
• 24 months follow-up

Sample Size (for pairwise comparisons)
• Scenario #1: Statistical significance based on strength of evidence corresponding to a one-sided p 0.025
256 endpoints (4025 participants) required for 90% power to detect 33% effectiveness
• Scenario #2: Statistical significance based on strength of evidence corresponding to a one-sided p 0.0025
405 endpoints (6125 participants) required for 90% power to detect 33% effectiveness

Illustration:HPTN 035 Trial
Illustration: Percent Reduction in HIV Risk
Scenario #1: One-sided 0.025; 256 endpoints
.025 .0025 .0005
0% 17.5% 21.5% 24% 27% 29.5% 33%
.025 .0025 .0005
Scenario #2: One-sided 0.0025; 405 endpoints
Illustration: Targeted Strength of Evidence
• Setting: Dual Control Arms
– Microbicide Regimen
– Placebo control
– Unblinded (condom only) control
• Illustration of Target Strength of Evidence
– one-sided p 0.025 for both comparisons
and
– one-sided p 0.0025 for ≥ 1 comparison
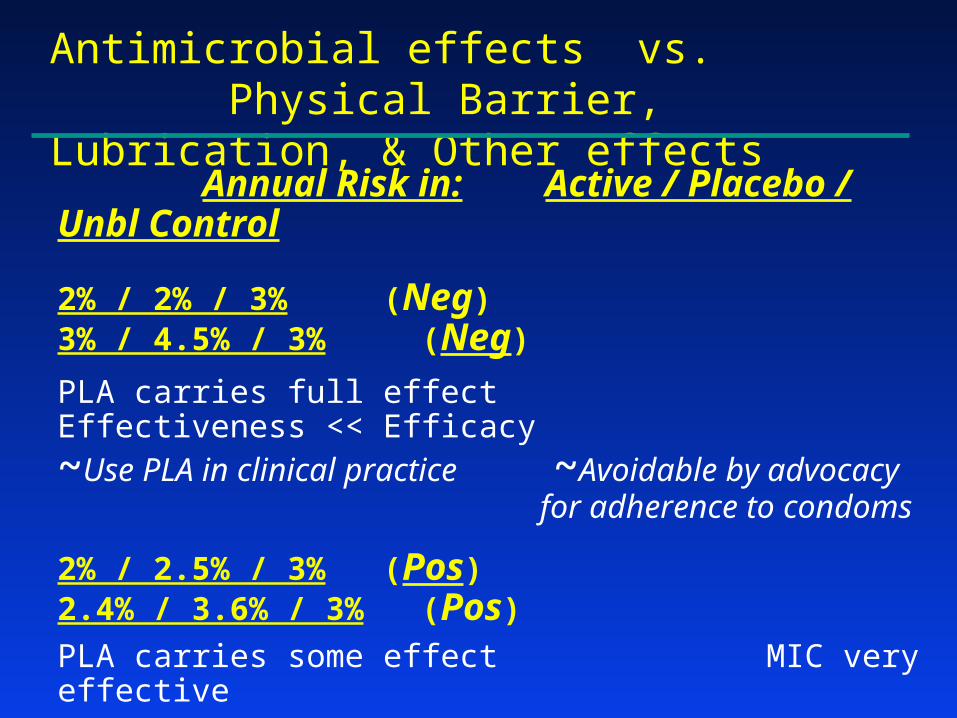
Antimicrobial effects vs. Physical Barrier, Lubrication, & Other effects
Annual Risk in: Active / Placebo / Unbl Control
2% / 2% / 3% (Neg) 3% / 4.5% / 3% (Neg)
PLA carries full effect Effectiveness << Efficacy~Use PLA in clinical practice ~Avoidable by advocacy
for adherence to condoms
2% / 2.5% / 3% (Pos) 2.4% / 3.6% / 3% (Pos)
PLA carries some effect MIC very effective~Use MIC in clinical practice ~Use MIC in clinical practice
(yet Effectiveness < Efficacy)
3% / 3% / 3% (Neg) 2% / 3% / 3% (Pos)
No effect MIC very effective
Selected Design Issues
• Blinding & the Choice of Controls
• Required Strength of Evidence
• Phase 2 vs Phase 2B vs Phase 3

Development Strategies
After Phase 1: What should be the next step?
~ Phase 2
~ Phase 2B (Intermediate Trial)
~ Phase 3

Why Conduct a Phase 2 Trial?
Obtain improved insights:• Safety and biological activity
• Refinements in dose/schedule
• Improving adherence to interventions
• Improving quality of trial conduct- Timely accrual
- High quality study implementation
- High quality data, including retention
Development Strategies
After Phase 1: What should be the next step?
~ Phase 2
~ Phase 2B (Intermediate Trial)
~ Phase 3
The Randomized Phase 2B “Intermediate Trial”
Illustration: HPTN 035 Intermediate Trial
Primary endpoint: HIV-1 Infection Rate
100 endpoints (per pairwise comparison)
Notation:• : True % Reduction
in risk of HIV-1 infection
• : Trial estimate of
^

Intermediate Trial Design
Phase 3 Trial Design
-33% 0% 33% 44% 67%
FurtherStudies Positive
-17% 0% 17% 33% 50%Positive
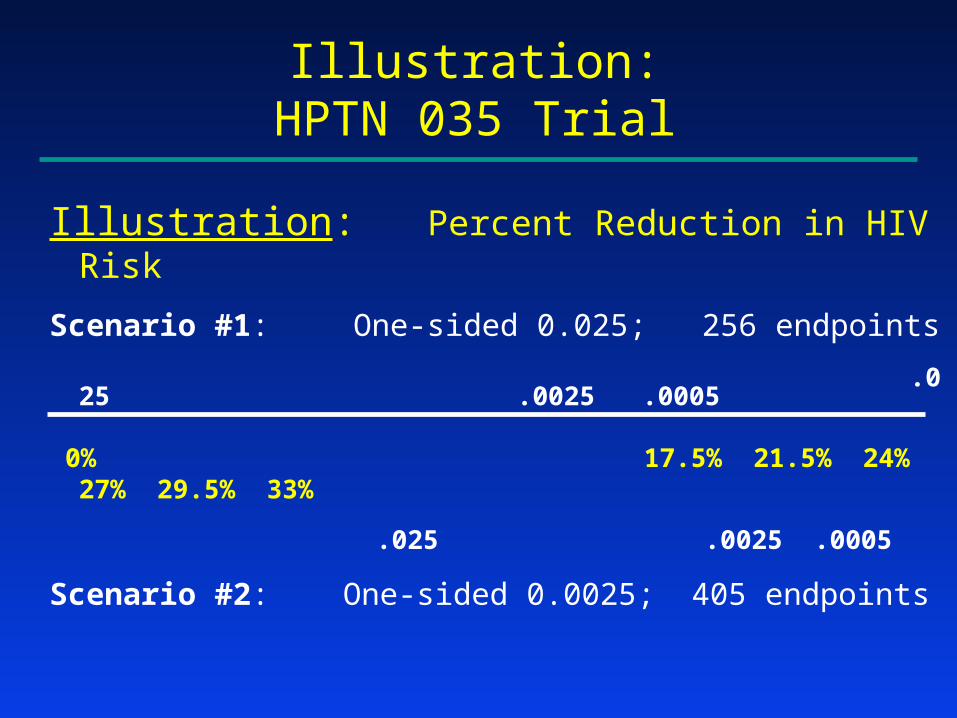
Illustration:HPTN 035 Trial
Illustration: Percent Reduction in HIV Risk
Scenario #1: One-sided 0.025; 256 endpoints
.025 .0025 .0005
0% 17.5% 21.5% 24% 27% 29.5% 33%
.025 .0025 .0005
Scenario #2: One-sided 0.0025; 405 endpoints

Intermediate Trial Design
Phase 3 Trial Design
-33% 0% 33% 44% 67%
FurtherStudies Positive
-17% 0% 17% 33% 50%Positive
An Illustration of the Useof an Intermediate TrialBefore a Definitive Trial
Surgical Adjuvant Therapyof Colorectal Cancer
5-FU + LevamisoleLevamisoleControl
R
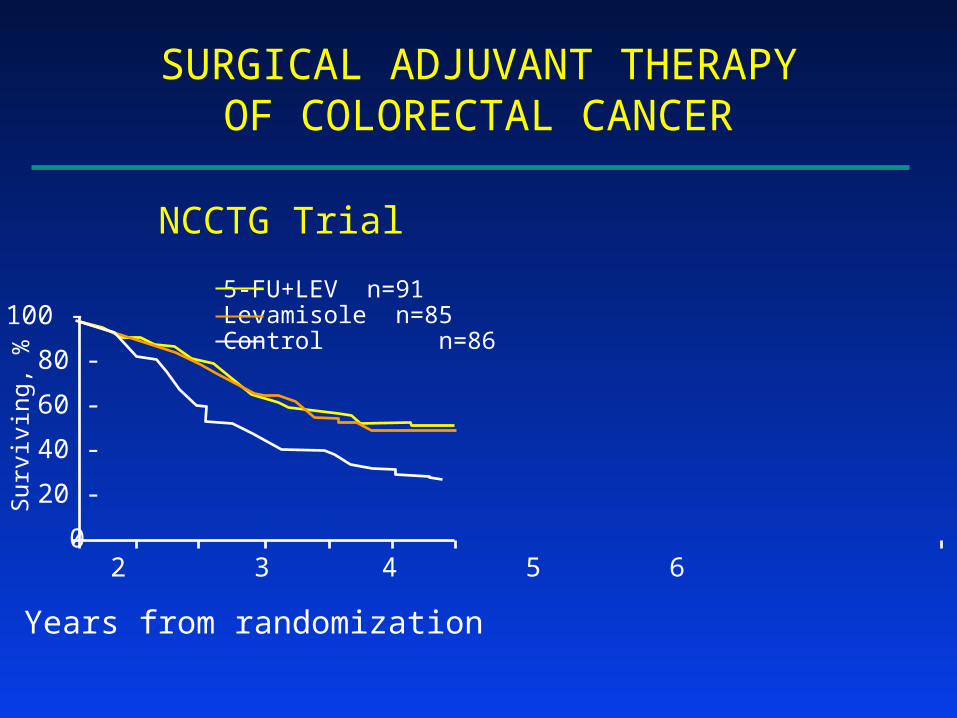
SURGICAL ADJUVANT THERAPYOF COLORECTAL CANCER
Surv
i vin
g, %
0 1 2 3 4 5 6
100 -
80 -
60 -
40 -
20 -
0
Years from randomization
NCCTG Trial
5-FU+LEV n=91Levamisole n=85Control n=86
SURGICAL ADJUVANT THERAPYOF COLORECTAL CANCER
Surv
i vin
g, %
0 1 2 3 4 5 6
100 -
80 -
60 -
40 -
20 -
0
Years from randomization
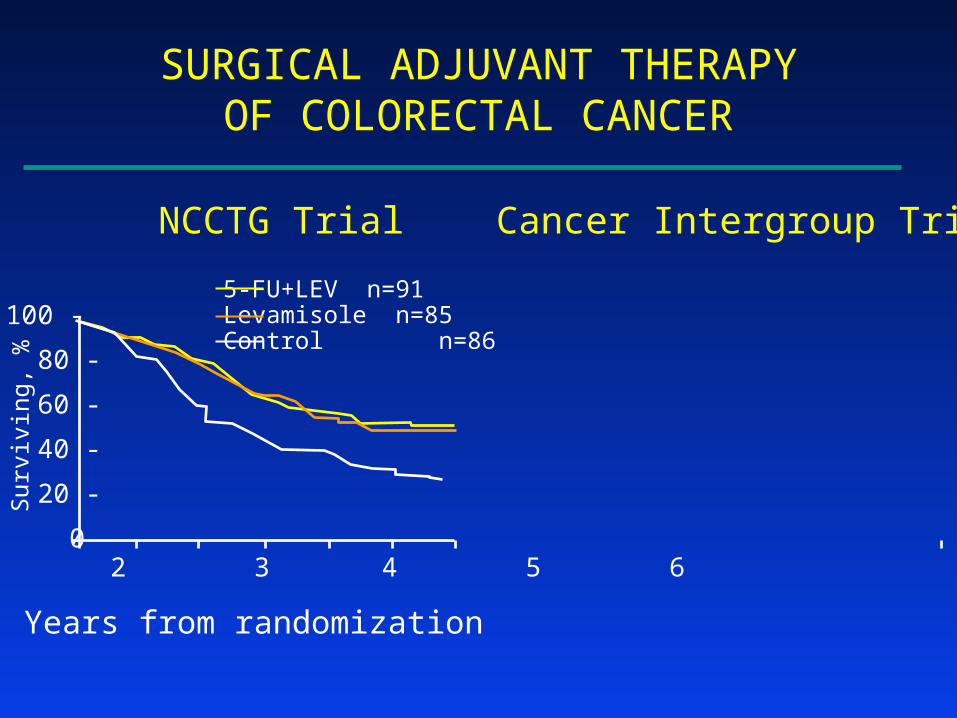
NCCTG Trial Cancer Intergroup Trial
5-FU+LEV n=91Levamisole n=85Control n=86
SURGICAL ADJUVANT THERAPYOF COLORECTAL CANCER
Surv
i vin
g, %
0 1 2 3 4 5 6
100 -
80 -
60 -
40 -
20 -
0
Years from randomization
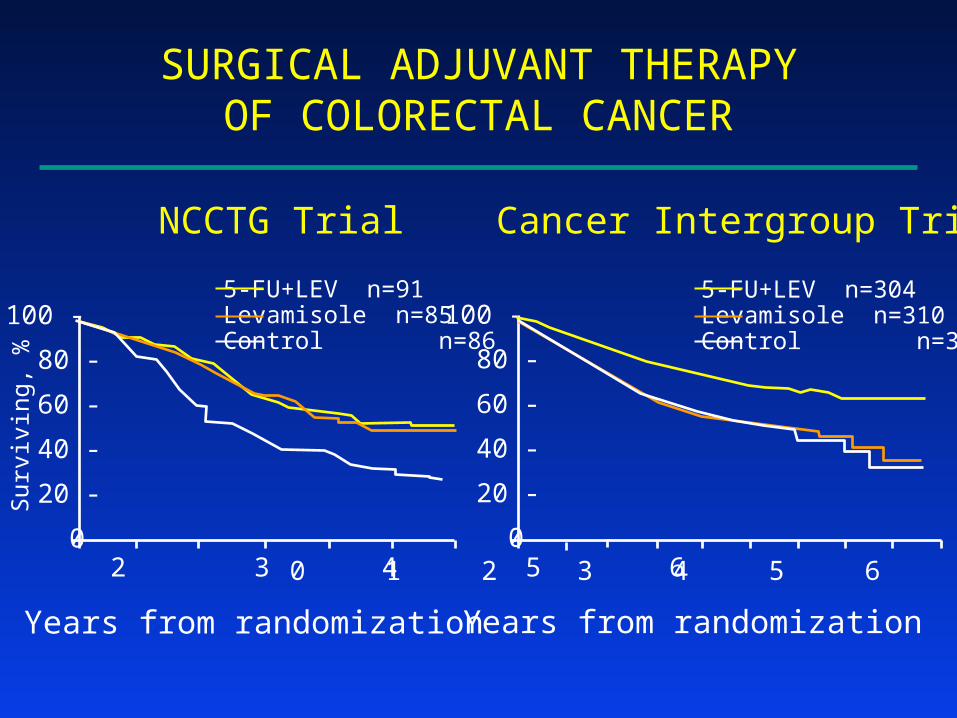
NCCTG Trial Cancer Intergroup Trial
0 1 2 3 4 5 6 7 8 9
100 -
80 -
60 -
40 -
20 -
0
Years from randomization
5-FU+LEV n=91Levamisole n=85Control n=86
5-FU+LEV n=304Levamisole n=310Control n=315
Important Observations
• Confirmatory trials of promising results from Intermediate Trials can be performed successfully
• Confirmatory trials- can reveal true positives (eg, 5-FU+Lev)- can reveal true negatives (eg, Levamisole)

SURGICAL ADJUVANT THERAPYOF COLORECTAL CANCER
Surv
i vin
g, %
0 1 2 3 4 5 6
100 -
80 -
60 -
40 -
20 -
0
Years from randomization
NCCTG Trial Cancer Intergroup Trial
0 1 2 3 4 5 6 7 8 9
100 -
80 -
60 -
40 -
20 -
0
Years from randomization
5-FU+LEV n=91Levamisole n=85Control n=86
5-FU+LEV n=304Levamisole n=310Control n=315

RAZT Labor/Delivery/1 wk to I
NVP Single doses to M/I
Illustration of an Intermediate Trial with “Compelling” Results: HIVNET 012
• 8/99 Results Lancet 1999; 354: 795-802
MCT of HIV N 6-8 wks 14-16 wks
AZT 302 59 (21.3%) 65 (25.1%)
NVP 307 35 (11.9%) 37 (13.1%)
1p = 0.0014 1p = 0.0003

Intermediate Trial Design
Phase 3 Trial Design
-33% 0% 33% 44% 67%
FurtherStudies Positive
-17% 0% 17% 33% 50%Positive

Conclusions: Selected Design Issues
• Blinding & the Choice of Controls
• Required Strength of Evidence
• Phase 2 vs Phase 2B vs Phase 3
