spinal tap - sbmu.ac.irinfectious.sbmu.ac.ir/uploads/last_lp_final.pdf · (sle (cva : csf. history...
TRANSCRIPT
SPINAL TAP

-
-
-
-
-
-
--
--
- CSF
CSF
CSF - 40CSF
CSF
CSF
CSF
INDEX 48 history of LP 50 normal CSF
54
abnormal CSF 58 lumbar puncture & indication
62 conterindication 63 procedure
70 complication 72 purpose
74 cross examination & microscopic examination 77- culture
78 latex agglutination 78- PCR 79-LDH
83- after care &risks 85- LP& BRIEF OF THE GUID LINE-

.

:
:
,
,
,
,
:-
,
.
:
.
:
.
:
:
.
,
.

:
:
,
Cauda equine
,

:
Spinal ganglion
,
.

:
(Conus medullaris)
.
:
H
.

:
:
.
.
:
,
,
.
:
.
Error!

(CSF) :
,
,
.
csf
CSF

CSF
CSF
CSF
Mg++ , Ca++ , K++
CSF
CSF -BBB(
CSF
CSF
CSF
CSF
CSF
CSF
CSF
CSF

Spinal Tap
CSF
L1L2
:
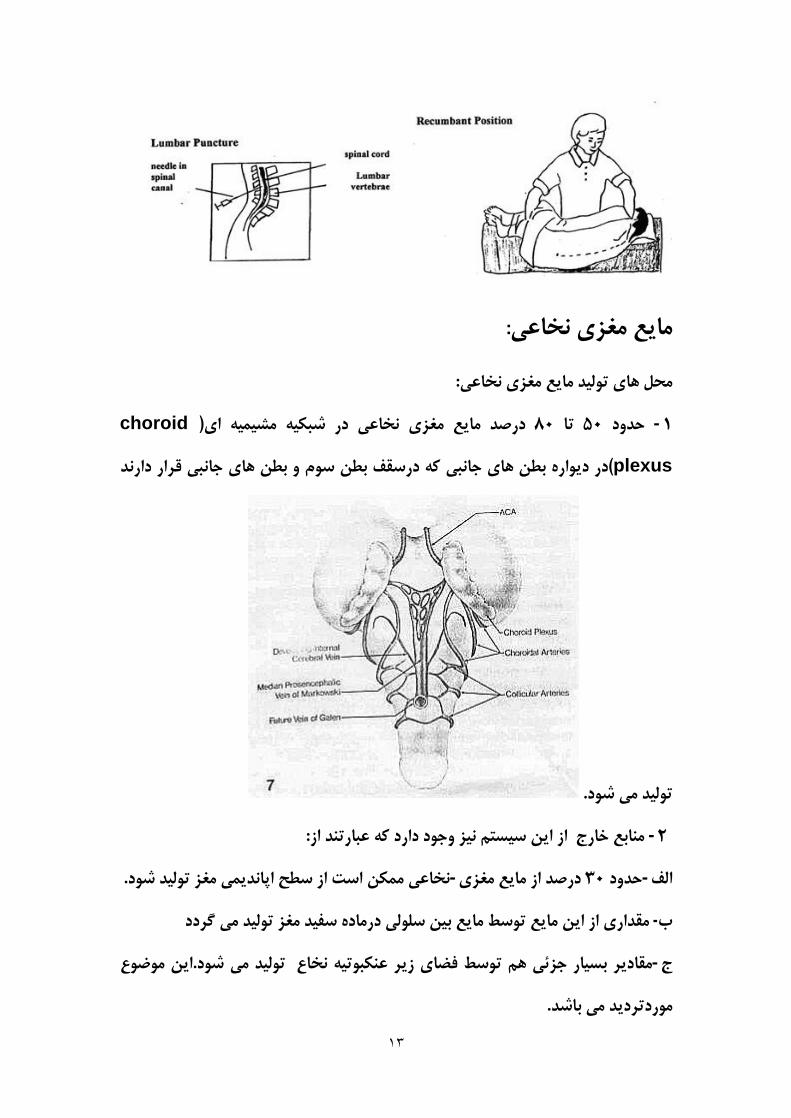
-choroid
plexus
-
--
-
-

-:
----
-

-:
--
-
-
-
:
L2- L1
CSF
CSF
NaclCSF
CSFCSF
CSF
CSF
/
/
cystern magna
)
(

%
/
.
,
,,
sagital
-
.
- WBC
RBCWBC
- CSF
-
-
- LDHCSF
mmol/L

- /
-
CSF
-
LP
RBC
- WBC,RBCCSF
RBCWBC
- CSF
- CSF
- LDHCSF
WBC
SAH

- Na KLPdetect
ReseaRch
CSF
-
RBCWBC
LP
.
- - SAH - TB
--
(--- snakeBite-
-LP
MS
//
-
(

WBC diff
-
.
LP
-TB
caseCSF
LP
-
TB --
LP
TB
CSF
NACL
CSF. CSF

/ CSF,
CSF
CSF
CSF
CSF
.mg , ca , k
CSF
CSF
CSF
CSF
mmH2o
lp
CSF

LP
CSF
CSF
CSF
lp
CSF
-
-
CSF
CSF
CSF :
CSF
/
/ TB /
CSF
CSF
WBC
- LP
-
- CVA
-

-
-
-
-
-
-
WBC
/
-MS
LP
CSF
- MS/-
/-/
- --
CSF
CSF

CSF
MSSLE
csf mmH2O
LP
)
(
CSF
,
CSF,
CSF
CSFLP

CSF :
-
-
-
-
-
-
-
-
-
CSF
:
-
-
-
-
-
CSF :

CSF
CSF
lp
,
,
CSF
LP
LP
CSF
CSF

:
CSF
TB
,

CSF:
CSF

LP
HTLV-III (
MS (
%-
:
MS (

LP:
Error!
CSF
LP:

LP:
CSF

LP:
:
CSF
CSF
CSF

CSF
CSF :
:
CSF
CSF
-
CSF
CSF LP

CSF
CSFmg/dl
CSF :
CSF
CSF
CSF :
LP
:
CSF
BBB
CSF
CSF
CSF :
CSF
CSF
mg/dl (
LP
CSF mg/dl-
CSF
mg/dl (
CSF
mg/dl (
CSF m/dl -
CSF mg/dl-
CSF mg/dl-
«
CSFmg/dl
CSFmg/dl
CSF
CSF :
CSF
CSF
:

CSF
CSF
IgGIgG
IgG
CSF
MS
IgG :
CNS
:

CSF
MSCSF
CNS
LP
MS
CSF
CSF
CSF
MS (
CVA (
:
MS
CSF
:
MS (
SLE (
CVA (
:

CSF

History of lumbar puncture
The first technique for
accessing the Dural
space was described by
the London physician
Dr Walter Essex
Wynter. In 1889, he
developed a crude cut down with cannulation in 4 patients with
tuberculous meningitis. The main purpose was the treatment of raised
intracranial pressure rather than for diagnosis. The tecnique for needle
lumbar puncture was then introduced by the German physician Heinrich
Quincke, who credits Wynter with the earlier discovery; he first reported
his experiences at an internal medicine conference in Wiesbaden in 1891.
He subsequently published a book on the subject.

The lumbar puncture procedure was taken to the United States by Arthur
H. Wentworth M.D., an assistant professor at the Harvard Medical
School, based at Children's Hospital. In 1893, he published a long paper
on diagnosing cerebro-spinal meningitis by examining spinal fluid. His
career took a nosedive, however, when anti vivisectionists prosecuted
him for having obtained spinal fluid from children. He was acquitted, but
he was disinvited from the then forming Johns Hopkins Medical School
where he would have been the first professor of pediatrics.

THE NORMAL CSF
The cerebrospinal fluid (CSF)
is produced from arterial
blood by the choroid plexuses
of the lateral and fourth
ventricles by a combined
process of diffusion, pinocytosis and active transfer. by ependymal cells.
The choroid plexus A small amount is also produced consists of tufts of
capillaries with thin fenestrated endothelial cells. These are covered by
modified ependymal cells with bulbous microvilli. The total volume of
CSF in the adult is about 140 ml. The volume of the ventricles is about 25
mi. CSF is produced at a rate of 0.2 - 0.7 ml per minute or 600-700 ml per
day. The circulation of CSF is aided by the pulsations of the choroid
plexus and by the motion of the cilia of ependymal cells. CSF is absorbed
across the arachnoid villi into the venous circulation. The arachnoid villi
act as one-way valves between the subarachnoid space and the dural
sinuses. The rate of absorption correlates with the CSF pressure. CSF acts
as a cushion that protects the brain from shocks and supports the venous
sinuses. It also plays an important role in the homeostasis and metabolism
of the central nervous system
CSF from the lumbar region contains 15 to 45 mg/dl protein (lower in
childen) and 50-80 mg/dl glucose (two-thirds of blood gluCose). Protein

concentration in cisternal and ventricular CSF is lower. Normal CSF
contains 0-5 mononuclear cells. The CSF pressure, measured at lumbar
puncture (LP), is 100-180 mm of H20 (8-15 mm Hg) with the patient
lying on the side and 200-300 mm with the patient sitting up.
Unlike other organs and tissues, brain capillaries show no fenestrations or
pinocytotic (transportation) vesicles and have tight junctions that almost
fuse adjacent cells. This anatomy creates the blood-brain barrier (BBB).
Astrocytic foot processes surround brain capillaries and, during
development, induce brain endothelial cells to develop in this special
leak-proof fashion.
The BBB separates plasma from the interstitial space of the CNS and
affects in a critical fashion the traffic of molecules in and out of the brain.
The ability to exclude certain substances from brain interstitial space has
to do not only with the vascular anatomy, but also with lipid solubility
and selective transcellular transport by endothelial cells. Lipophilic
compounds cross the BBB easier than hydrophilic ones do, and small
lipophilic molecules such as 02 and C02 diffuse freely. Some hydrophilic
compounds, including glucose and amino acids, enter the brain with the
help of transporters, and larger molecules enter via receptor-mediated
endocytosis. The BBB protects the brain from toxic substances but
impedes also the entry of drugs. Hypertonic stimuli and chemical
substances including glutamate and certain cytokines can open the BBB.
HIE and inflammatory mediators produced in sepsis disrupt the BBB.
Blood vessels in GBM and other malignant brain tumors do not have tight
junctions, explaining the fluid leakage and cerebral edema that
accompanies these tumors. The interstitial space of the brain is separated
from the ventricular CSF by the ependymal lining and from the
subarachnoid CSF by the glia limitans. The glia limitans is a thick layer
of interdigitating astrocytic processes with an overlying basement
membrane. This layer seals the surface of the CNS and dips into brain
tissue along the perivascular space (see below). External to it is the pia
matter, a thin layer of connective tissue cells with a small amount of
collagen. The ependymal barrier is far more permeable than the BBB.
The major cerebral arteries and veins traverse the subarachnoid space and
penetrate into the brain, where they branch into smaller vessels and
eventually capillaries. Capillaries are in contact with astrocytic processes.
Vessels larger than capillaries are separated from the surrounding brain
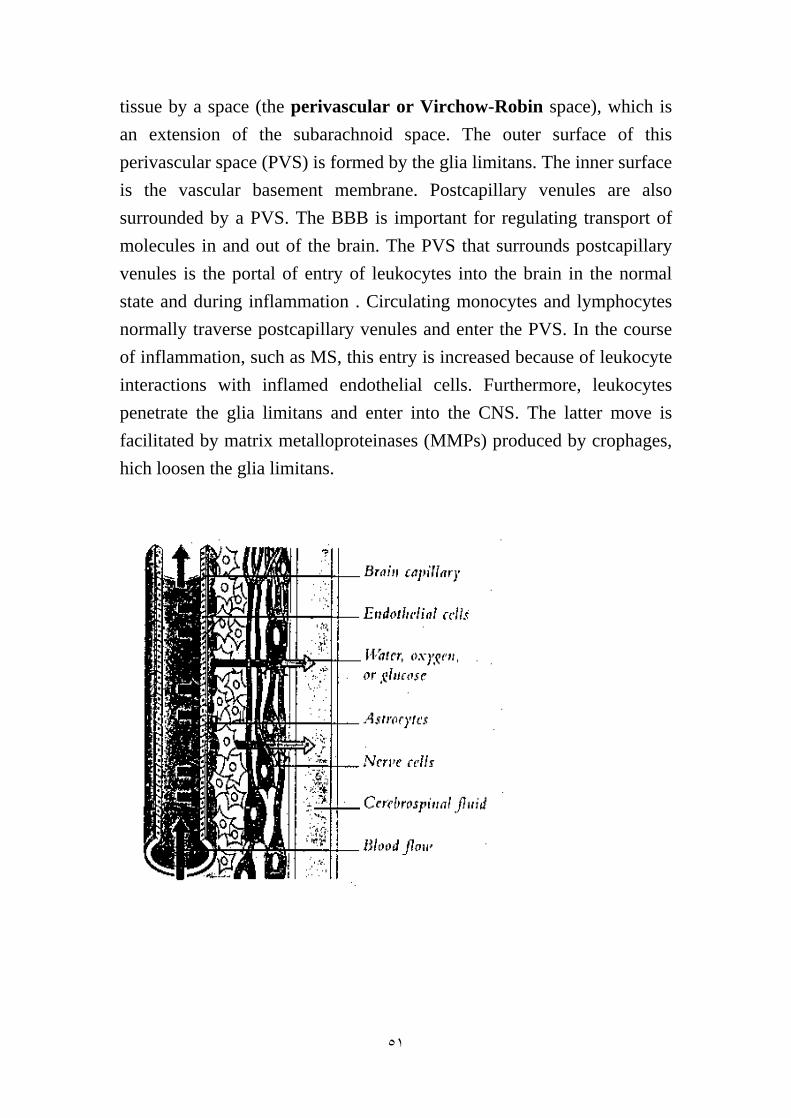
tissue by a space (the perivascular or Virchow-Robin space), which is
an extension of the subarachnoid space. The outer surface of this
perivascular space (PVS) is formed by the glia limitans. The inner surface
is the vascular basement membrane. Postcapillary venules are also
surrounded by a PVS. The BBB is important for regulating transport of
molecules in and out of the brain. The PVS that surrounds postcapillary
venules is the portal of entry of leukocytes into the brain in the normal
state and during inflammation . Circulating monocytes and lymphocytes
normally traverse postcapillary venules and enter the PVS. In the course
of inflammation, such as MS, this entry is increased because of leukocyte
interactions with inflamed endothelial cells. Furthermore, leukocytes
penetrate the glia limitans and enter into the CNS. The latter move is
facilitated by matrix metalloproteinases (MMPs) produced by crophages,
hich loosen the glia limitans.

ABNORMALITIES OF CSF
Blood: Blood may be spilled into the CSF by accidental puncture of a
leptomeningeal vein during entry of the LP needle. Such blood stains the
fluid that is drawn initially and clears gradually. If it does not clear, blood
indicates subarachnoid hemorrhage. Erythrocytes from subarachnoid
hemorrhage are cleared in 3 to 7 days. A few neutrophils and
mononuclear cells may also be present as a result of meningeal irritation.
Xanthochromia (blonde color) of the CSF following subarachnoid
hemorrhage is due to oxyhemoglobin which appears in 4 to 6 hours and
bilirubin which appears in two days. Xanthochromia may also be seen
with hemorrhagic infarcts, brain tumors, and jaundice.
Increased inflammatory cells (pleocytosis) may be caused by infectious
and noninfectious processes. Polymorphonuclear pleocytosis indicates
acute suppurative meningitis. Mononuclear cells are seen in viral
infections (meningoencephalitis, aseptic meningitis), syphilis,
neuroborreliosis, tuberculous meningitis, multiple sclerosis, brain abscess
and brain tumors.
Tumor cells indicate dissemination of metastatic or primary brain tumors
in the subarachnoid space. The most common among the latter is
medulloblastoma. They can be best detected by cytological examination.
A mononuclear inflammatory reaction is often seen in addition to the
tumor cells.
Increased protein: In bacterial meningitis, CSF protein may rise to 500
mg/dl. A more moderate increase (150-200 mg/dl) occurs in
inflammatory diseases of meninges (meningitis, encephalitis), intracranial
tumors, subarachnoid hemorrhage, and cerebral infarction. A more severe
increase occurs in the Guillain-Barre syndrome and acoustic and spinal
schwannoma. In multiple sclerosis, CSF protein is normal or mildly
increased, but there is often an elevation of IgG in CSF, but not in serum,
expressed as an elevation of the CSF IgG/albumin index (normally 10: 1).
In addition, 90% of MS patients have oligoclonal IgG bands in the CSF.
Oligoclonal bands are also seen occasionally in some chronic CNS
infections. The type of oligoclonal bands is constant for each MS patient
throughout the course of the disease. Oligoclonal bands occur in the CSF
only (not in the serum). These quantitative and qualitative CSF changes
indicate that in MS, there is intrathecal immunoglobulin production. In
addition, the CSF in MS often contains myelin fragments and myelin
basic protein (MBP). MBP can be detected by radioimmunoassay. MBP
is not specific for MS. It can appear in any condition causing brain
necrosis, including infarcts.
Low glucose in CSF is seen in suppurative, tuberculous and fungal
infections, sarcoidosis, and meningeal dissemination of tumors. Glucose
is consumed by leukocytes and tumor cells. Lumbar puncture is a very
safe procedure. It is routinely performed without complication. Before the

test you will have been carefully assessed by your doctor. Basic blood
tests and often a brain scan will have been reviewed. In these
circumstances no serious complications are likely. Headache after
lumbar puncture does occur in a small proportion of cases and its
occurrence appears to be unrelated to how easily the procedure was
performed. It is very rare for this headache to be severe (reported in less
than 5 in 100 procedures in good units) and even rarer for the headache to
be sufficiently prolonged to require readmission to hospital (necessary in
less than 1 in 100 procedures). If this is necessary then you may be given
an infusion of caffeine or the anaesthesist may be asked to perform a
blood patch. (A blood patch is a very simple procedure during which the
anaesthesist will ask you to lie on your side and then inject a small
amount of your own blood into your lower back to seal any site of spinal
fluid leak.) Other complications are usually mild and uncommon. Back
pain may occur but will usually settle. It is extraordinarily unlikely for the
test to cause infection within the nervous system but this is theoretically
possible.

We advise the following:
Lie down flat for at least half an hour (you are in hospital for this time).
Before leaving hospital, get up and walk around to ensure that you are
ready for your journey home. Inform your nurse when you intend to
leave.
Do not drive for the next 24 hours.
Over the next 48 hours, try to drink 3 liters of fluid a day. This helps
replace fluid taken in the procedure.
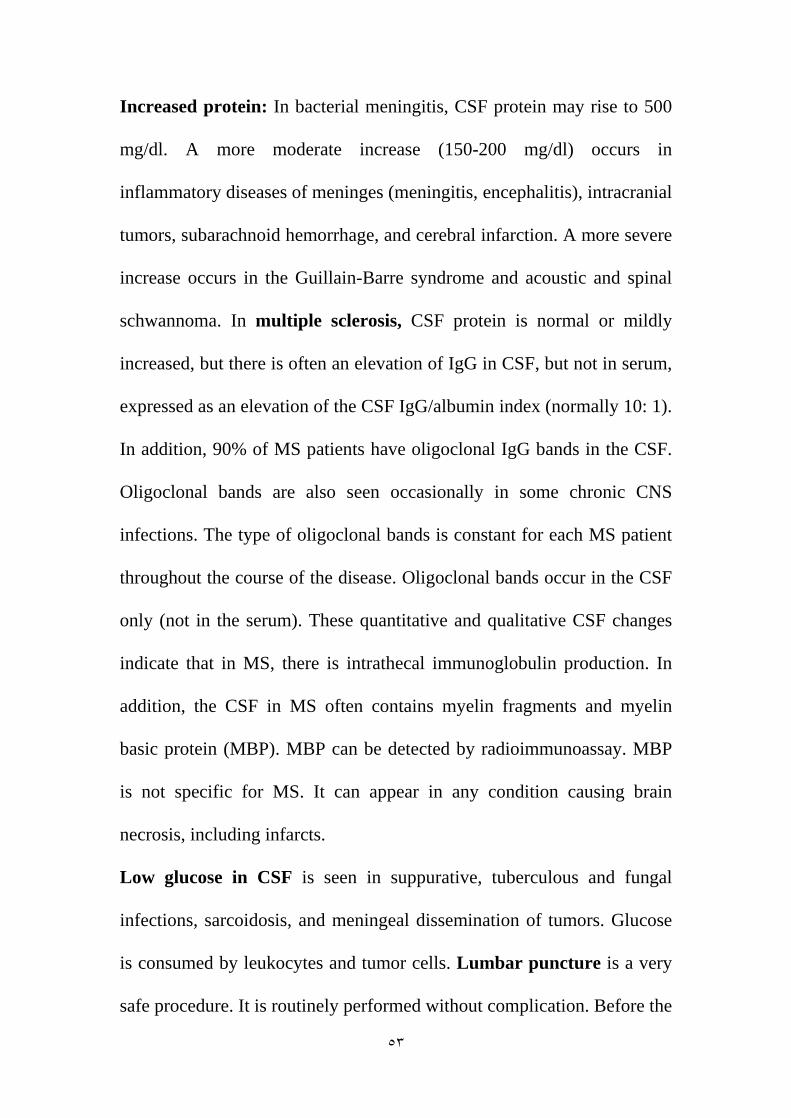
Lumbar puncture
In medicine, a lumbar puncture (colloquially known as a spinal tap) is
a diagnostic and at times therapeutic procedure that is performed in order
to collect a sample of cerebrospinal fluid (CSF) for biochemical,
microbiological, and cytological analysis, or very rarely as a treatment
("therapeutic lumbar puncture") to relieve increased intracranial pressure.
Lumbar puncture is indicated for both diagnostic and therapeutic reasons.
Knowledge of the contraindications, the pertinent anatomy, and the
methods to minimize the risk of complications are necessary for the safe
and efficient performance of the procedure. Risks although rare, can be

substantial and even potentially life-threatening. The risks can be
minimized with an appropriate understanding of the indications,
contraindications, and procedural techniques.
INDICATIONS
Lumbar puncture is used to obtain a sample of cerebrospinal fluid (CSF)
to aid in the diagnosis of infectious, inflammatory, oncologic, and
metabolic processes (Table 1). Therapeutic indications include the
delivery of chemotherapy, antibiotics, and anesthetic agents.

Table 1. Indications and Uses for Lumbar Puncture.
Variable
Diagnostic indications
Infectious disease
Viral. bacterial. or fungal
meningitis
Encephalitis
Inflammatory process
Multiple sclerosis
Guillan-Barre syndrome
Variety of oncologic procedures
Variety of metabolic processes
Therapeutic indications
Numerous procedures requiring
lower-body analgesia
Anesthesia
Narcotics
Bupivacaine
Ventriculitis and some types of
meningitis
Antibiotic administration
Vancomycin
Tests performed on CSF
Cell count, differential count,
measurement of glucose
and protein, cultures
Measurement of myelin basic
proteins, cell counts, cultures
Cell counts. smear on cell
concentrate
Measurement oflactate. pyruvate,
glucose. Protein
Gentamicin
Some leukemias and
lymphomas
Chemotherapy
Methotrexate
Indications
The most common purpose for a lumbar puncture is to collect
cerebrospinal fluid in a case of suspected meningitis, since there is no
other reliable tool with which meningitis, a life-threatening but highly
treatable condition, can be excluded. Young infants commonly require
lumbar puncture as a part of the routine workup for fever without a
source, as they have a much higher risk of meningitis than older persons
and do not reliably show signs of menangeal irritation (meningismus). In
any age group, subarachnoid hemorrhage, hydrocephalus, benign
intracranial hypertension and many other diagnoses may be supported or
excluded with this test.
Lumbar punctures may also be done to inject medications into the
cerebrospinal fluid ("intrathecaly"), particularly for spinal anesthesia or
chemotherapy. It may also be used to detect the presence of malignant
cells in the CSF, as in carcinomatous meningitis or medulloblastoma.

Contraindications
Lumbar puncture should not be performed in the following situations
* Idiopathic (unidentified cause) increased intracranial pressure (ICP)
* Rationale: lumbar puncture in the presence of increased ICP may cause
oncal herniation
* Exception: therapeutic use of lumbar puncture to reduce ICP
* Precaution
* CT brain is advocated by some, especially in the following situations
* Age >65
* Reduced GCS or conscious state
* Recent history of seizure
* Focal neurological signs
* Ophthalmoscopy for papiloedema
* Bleeding diathesis
* Coagulopathy
* Decreased platelet count «50 x 1 09/L)
* Infections
Skin infection at puncture site
* Sepsis
* Abnormal respiratory pattern . . .
* Hypertension with bradycardia and deteriorating consciousness.
* Vertebral deformities (scoliosis or kyphosis),
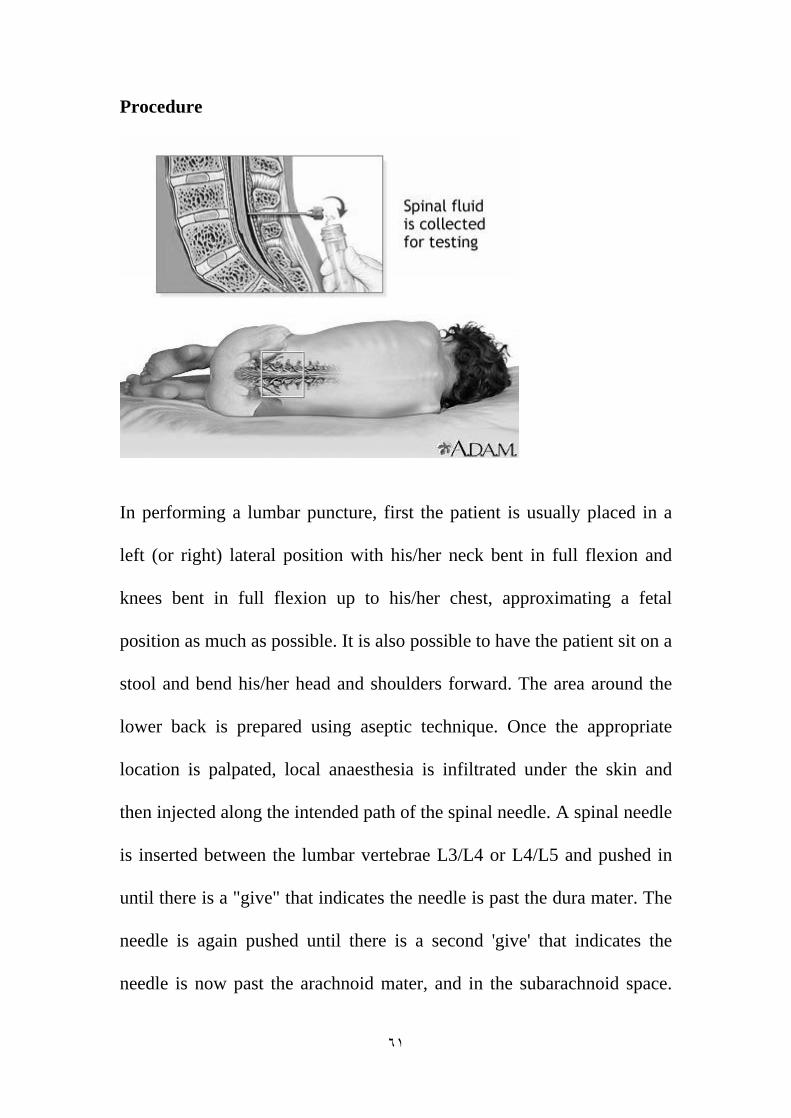
Procedure
In performing a lumbar puncture, first the patient is usually placed in a
left (or right) lateral position with his/her neck bent in full flexion and
knees bent in full flexion up to his/her chest, approximating a fetal
position as much as possible. It is also possible to have the patient sit on a
stool and bend his/her head and shoulders forward. The area around the
lower back is prepared using aseptic technique. Once the appropriate
location is palpated, local anaesthesia is infiltrated under the skin and
then injected along the intended path of the spinal needle. A spinal needle
is inserted between the lumbar vertebrae L3/L4 or L4/L5 and pushed in
until there is a "give" that indicates the needle is past the dura mater. The
needle is again pushed until there is a second 'give' that indicates the
needle is now past the arachnoid mater, and in the subarachnoid space.
The style from the spinal needle is then withdrawn and drops of
cerebrospinal fluid are collected. The opening pressure of the
cerebrospinal fluid may be taken during this collection by using a simple
column manometer. The procedure is ended by withdrawing the needle
while placing pressure on the puncture site. In the past, the patient would
often be asked to lie on his/her back for at least six hours and be
monitored for signs of neurological problems, though there is no
scientific evidence that this provides any benefit. The technique described
is almost identical to that used in spinal anesthesia, except that spinal
anesthesia is more often done with the patient in a sitting position.
The upright seated position is advantageous in that there is less distortion
of spinal anatomy which allows for easier withdrawal of fluid. It is
preferred by some practitioners when a lumbar puncture is performed on
an obese patient where having them lie on their side would cause a
scoliosis and unreliable anatomical landmarks. On the other hand,
opening pressures are notoriously unreliable when measured on a seated
patient and therefore the left or right lateral (lying down) position is
preferred if an opening pressure needs to be measured.
Patient anxiety during the procedure can lead to increased CSF pressure,
especially if the person holds their breath, tenses their muscles or flexes
their knees too tightly against their chest. Diagnostic analysis of changes
in fluid pressure during lumbar puncture procedures requires attention

both to the patient's condition during the procedure and to their medical
history.
blockage resulting in a large pool of CSF, or hydrocephalus associated
with large volumes of CSF. Lumbar puncture for the purpose of reducing
pressure is performed in some patients with idiopathic intracranial
hypertension (also called pseudotumor cerebri.)
The presence of white blood cells in cerebrospinal fluid is called
pleocytosis. A small number of monocytes can be normal; the presence of
granulocytes is always an abnormal finding. A large number of
granulocytes often heralds bacterial meningitis. White cells can also
indicate reaction to repeated lumbar punctures, reactions to prior
injections of medicines or dyes, central nervous system hemorrhage,
leukemia, recent epileptic seizure, or a metastatic tumor. When peripheral
blood contaminates the withdrawn CSF, a common procedural
complication, white blood cells will be present along with erythrocytes,
and their ratio will be the same as that in the peripheral blood.
The finding of erythrophagocytosis where phagocytosed erythrocytes is
observed, signifies haemorrhage into the CSF that preceded the lumbar
puncture. Therefore, when erythrocytes are detected in the CSF sample,
erythrophagocytosis suggests causes other than a traumatic tap, such as
intracranial haemorrhage and haemorrhagic herpetic encephalitis. In

which case, further investigations are warranted, including imaging and
viral culture.
Several substances found in cerebrospinal fluid are available for
diagnostic measurement.
* Measurement of chloride levels may aid in detecting the presence of
tuberculous meningitis.
*
that in the peripheral circulation. A fingerstick or venipuncture at the time
of lumbar puncture may therefore be performed to assess peripheral
glucose levels in order to determine a predicted CSF glucose value.
Decreased glucose levels can indicate fungal, tuberculous or pyogenic
infections; lymphomas; leukemia spreading to the meninges;
meningoencephalitis mumps; or hypoglycemia. A glucose level of less
than one third of blood glucose levels in association with low CSF lactate
levels is typical in hereditary CSF glucose transporter deficiency also
known as De Vivo disease.
* Increased glucose levels in the fluid can indicate diabetes, although the
60% rule still applies.
* Increased levels of glutamine are often involved with hepatic
encephalopathies, Reye's syndrome, hepatic coma, cirrhosis and
hypercapnia.

* Increased levels of lactate can occur the presence of cancer of the
CNS, multiple sclerosis, heritable mitochondrial disease, low blood
pressure, low serum phosphorus, respiratory alkalosis, idiopathic
seizures, traumatic brain injury, cerebral ischemia, brain abscess,
hydrocephalus, . hypocapnia or bacterial meningitis.
* The enzyme lactate dehydrogenase can be measured to help
distinguish meningitides of bacterial origin, which are often associated
with high levels of the enzyme, from those of viral origin in which the
enzyme is low or absent. .
* Changes in total protein content of cerebrospinal fluid can result from
pathologically increased permeability of the blood-cerebrospinal fluid
barrier, obstructions of CSF circulation, meningitis, neurosyphilis, brain
abscesses, subarachnoid hemorrhage, polio, collagen disease or
GuillanBarre syndrome, leakage of CSF, increases in intracranial pressure
or hyperthyroidism. Very high levels of protein may indicate tuberculous
meningitis or spinal block.
* IgG synthetic rate is calculated from measured IgG and total protein
levels; it is elevated in immune disorders such as multiple sclerosis,
transverse myelitis, and neuromyelitis optica of Disc.
* Numerous antibody-mediated tests for CSF are available in some
countries: these include rapid tests for antigens of common bacterial
pathogens, treponemal titers for the diagnosis of neurosyphilis and Lyme
disease, Coccidioides antibody, and others. Reinsertion of the style may
decrease the rate of post lumbar puncture headaches Risks
Post spinal headache with nausea is-the most common complication; it
often responds to analgesics and infusion of fluids. It was long taught that
this complication can often be prevented by strict maintenance of a
supine posture for two hours after the successful puncture; this has not
been borne out in modern studies involving large numbers of patients.
Merritt's Neurology (10th edition), in the section on lumbar puncture,
notes that intravenous caffeine injection is often quite effective in
aborting these so-called "spinal headaches." Contact between the side of
the lumbar puncture needle and a spinal nerve root can result in
anomalous sensations (paresthesia) in a leg during the procedure; this is
harmless and patients can be warned about it in advance to minimize their
anxiety if it should occur. A headache that is persistent despite a long
period of bedrest and occurs only when sitting up may be indicative of a
CSF leak from the lumbar puncture site. It can be treated by more
bedrest, or by an epidural blood patch, where the patient's own blood is
injected back into the site of leakage to cause a clot to form and seal off
the leak.
Serious complications of a properly performed lumbar puncture are
extremely They include spinal or epidural bleeding, and trauma to the

spinal cord or spinal nerve roots resulting in weakness or loss of
sensation, or even paraplegia. The latter is exceedingly rare, since the
level at which the spinal cord ends (normally the inferior border of L 1,
although it is slightly lower in infants) is several vertebral spaces above
the proper location for a lumbar puncture (L3/L4). There are case reports
of lumbar puncture resulting in perforation of abnormal dural arterio-
venous malformations, resulting in catastrophic epidural hemorrhage; this
is exceedingly rare.
The procedure is not recommended when epidural infection is present or
suspected, when topical infections or dermatological conditions pose a
risk of infection at the puncture site or in patients with severe psychosis
or neurosis with back pain. Some authorities believe that withdrawal of
fluid when initial pressures are abnormal could result in spinal cord
compression or cerebral herniation; others believe that such events are
merely coincidental in time, occuring independently as a result of the
same pathology that the lumbar puncture was performed to diagnose. In
any case, computed tomography of the brain is often performed prior to
lumbar puncture if an intracranial mass is suspected.
Removal of cerebrospinal fluid resulting in reduced fluid pressure has
been shown to corelate with greater reduction of cerebral blood flow
among patients with Alzheimer's disease. Its clinical significance is
uncertain.
Diagnostics:
Increased CSF pressure can indicate congestive heart failure, cerebral
edema, subaracnoid hemorrhage, hypo-osmolality resulting from
hemodialysis, meningeal inflanmation, purulent meningitis or tuberculous
meningitis, hydrocephalus, or pseudotumor cerebri.
Decreased CSF pressure can indicate complete subarachnoid blockage,
leakage of spinal fluid, severe dehydration, hyperosmolality, or
circulatory collapse. Significant changes in pressure during the procedure
can indicate tumors or spinal
COMPLICATIONS:
Obese patients may represent a challenge because of difficulty in
identifying landmarks. Osteoarthritis, ankylosing spondylitis,
kyphoscoliosis, previous lumbar surgery, and degenerative disk disease
may make the procedure more difficult. In patients with such conditions,

consultation with an anesthesiologist or interventional radiologist may be
necessary for lumbar puncture to be successful.
Complications from lumbar puncture include herniation cardiorespiratory
compromise, local or referred pain, headache, bleeding, infection,
subarachnoid epidermal cyst, and leakage of CSF. The most common
complication is headache, occurring in up to 36.5% of patients within 48
hours after the procedure. Headaches can be caused by the leakage of
CSF through the puncture site at a rate that exceeds the rate of CSF
production. The incidence increases in relation to the size of the spinal
needles The most serious complication is herniation, which may result
when a large pressure gradient exists between the cranial and lumbar
compartments. This gradient can be increased during a lumbar puncture,
resulting in brain-stem herniation. Patients at high risk for herniation can
be identified by a thorough history- taking and neurologic examination. If
there is still concern about the procedure, CT may be helpful, with the
caveat that these images may not identify pressure elevations. However,
CT is not necessary for all patients, because it could delay diagnosis and
treatment. Bleeding is most likely to occur in a patient with a bleeding
diathesis. The resulting hemorrhage may cause spinal cord compression.
No absolute criteria exist regarding the degree of coagulopathy and the
risk of bleeding, so clinical judgment is necessary. Subarachnoid
epidermal cysts can develop as a consequence of introducing a skin plug

into the subarachnoid space and can be avoided through the use of a
needle with a styll.
Cerebrospinal fluid (CSF) analysis:
Cerebrospinal fluid (CSF) analysis is a set of laboratory tests that
examine a sample of the fluid surrounding the brain and spinal cord. This
fluid is an ultrafiltrate of plasma. It is clear and colorless. It contains
glucose, electrolytes, amino acids, and other small molecules found in
plasma, but has very little protein and few cells. CSF protects the central
nervous system from injury, cushions it from the surrounding bone
structure, provides it with nutrients, and removes waste products by
returning them to the blood. CSF is withdrawn from the subarachnoid
space through a needle by a procedure called a lumbar puncture or spinal
tap. CSF analysis includes tests in clinical chemistry, hematology,
immunology, and microbiology. Usually three or four tubes are collected.
The first tube is used for chemical and/ or serological analysis and the last
two tubes are used for hematology and microbiology tests. This reduces
the chances of a falsely elevated white cell count caused by a traumatic
tap (bleeding into the subarachnoid space at the puncture site), and
contamination of the bacterial culture by skin germs or flora.
Purpose:
The purpose of a CSF analysis is to diagnose medical disorders that affect
the central nervous system. Some of these conditions are:

* meningitis and encephalitis, which may be viral, bacterial, fungal, or
parasitic infections
* metastatic tumors (e.g., leukemia) and central nervous system tumors
that shed cells into the CSF
* syphilis, a sexually transmitted bacterial disease
* bleeding (hemorrhaging) in the brain and spinal cord
* multiple sclerosis, a degenerative nerve disease that results in the loss
of the myelin coating of the nerve fibers of the brain and spinal cord
* Guillan-Barre syndrome, a demyelinating disease involving peripheral
sensory and motor nerves.
Routine examination of CSF includes visual observation of color and
clarity and tests for glucose, protein, lactate, lactate dehydrogenase, red
blood cell count, white blood cell count with differential, syphilis
serology (testing for antibodies indicative of syphilis), Gram stain, and
bacterial culture. Further tests may need 1>0 be performed depending
upon the results of initial tests and the presumptive diagnosis. For
example, an abnormally high total protein seen in a patient suspected of
having a demyelinating disease such as multiple sclerosis dictates CSF
protein electrophoresis and measurement of immunoglobulin levels and
myelin basic protein.

GROSS EXAMINATION:. Color and clarity are important diagnostic
characteristics of CSF. Straw, pink, yellow, or amber pigments
(xanthochromia) are abnormal and indicate the presence of bilirubin,
hemoglobin, red blood cells, or increased protein. Turbidity (suspended
particles) indicates an increased number of cells. Gross examination is an
important aid to differentiating a subarachnoid hemorrhage from a
traumatic tap. The latter is often associated with sequential clearing of
CSF as it is collected; streaks of blood in an otherwise clear fluid; or a
sample that clots.
Microscopic Examination:
Gram stain is positive in 60 to 80 percent of untreated cases of bacterial
meningitis and in 40 to 60 percent of partially treated cases. The
sensitivity according to the causative organism ranges from 90 percent in
pneumococcal or staphylococcal meningitis to less than 50 percent in
Listeria meningitis. Hyphae can occasionally be seen in Candida or other
fungal meningitis cases.
Several factors influence the sensitivity of Gram stain. Laboratory
techniques used to concentrate and stain CSF can greatly influence
reliability. Cytocentrifugation increases the ability to detect bacteria.
Greater numbers of colony-farming units (CFU) per mm' of CSF increase
the likelihood of a positive result. Staining will be positive in 25 percent
of cases if fewer than 1,000 CFU per mm' are present, and
in 75 percent of cases if more than 100,000 CFU per mm' are present.'
Lastly, the experience of laboratory personnel is very important. Up to 10
percent of initial Gram stains are misread."
Acid-fast staining should be done if tuberculosis is clinically suspected.
Only 37 percent of initial smears will be positive for acid-fast bacilli.
This result can be increased to 87 percent if four smears are done."
Sensitivity also can be increased by examining the CSF sediment."
Other stains should be performed if indicated by the situation.
Cryptococcus may be identified up to 50 percent of the time on an India
ink preparation. A tap-water control should always be done to ensure that
the India ink is not contaminated.
Toxoplasmosis can be diagnosed With Wright or Giemsa stain. A simple
wet preparation of CSF under a cover slip can yield positive results in a
variety of protozoan and helminthic infections.
GLUCOSE.: CSF glucose is normally approximately two-thirds of the
fasting plasma glucose. A glucose level below 40 mg/ dL is significant
and occurs in bacterial and fungal meningitis and in malignancy.
PROTEIN.: Total protein levels in CSF are normally very low, and
albumin makes up approximately twothirds of the total. High levels are
seen in many conditions including bacterial and fungal meningitis,
multiple sclerosis, tumors, subarachnoid hemorrhage, and please refer to
page 18

Glucose Level:
A true normal range cannot be given for CSF glucose. As a general rule,
CSF glucose is about two thirds of the serum glucose measured during
the preceding two to four hours in a normal adult. This ratio decreases
with increasing serum glucose levels. CSF glucose levels generally do not
go above 300 mg
Glucose in the CSF of neonates varies much more than in adults, and the
CSF-to-serum ratio is generally higher than in adults.
CNS infections can cause lowered CSF glucose levels, although glucose
levels are usually normal in viral infections Normal glucose levels do not
rule out infection, because up to 50 percent of patients who have bacterial
meningitis will have normal CSF glucose levels.
Chemical meningitis, inflammatory conditions, subarachnoid
hemorrhage, and hypoglycemia also cause hypoglycorrhachia (low
glucose level in CSF). Elevated levels of glucose in the blood is the only
cause of having an elevated CSF glucose level. There is no pathologic
process that causes CSF glucose levels to be elevated
.

Culture:
Cultures done on 5 percent sheep blood agar and enriched chocolate agar
remain the gold standards for diagnosing bacterial meningitis. Antibiotic
treatment prior to lumbar puncture can decrease the sensitivity of culture,
especially when given intravenously or intramuscularly.
Enterovirus, the leading cause of viral meningitis, can be recovered ill 40
to 80 percent of cases. Culture for herpes simplex virus is 80 to 90
percent sensitive but can take five to seven days to become positive.
Results of viral cultures rarely change the initial management of
meningitis.
Mycobacterium tuberculosis is best grown using multiple large volume
samples of CSF. At least 15 mL and preferably 40 to 50 mL of CSF are
recommended. Culture is positive 56 percent of the time on the first
sample, and improved to 83 percent of the time if four separate samples
are cultured. These cultures often take up to six weeks for positive
identification.
Fungal cultures are positive in more than 95 percent of cryptococcus
neoformans cases and in 66 percent of candidal meningitis cases. Other
fungi are less likely to be culture positive. Similar to tuberculous
meningitis, culture yield in fungal meningitis can be increased by
obtaining large volumes of CSF via repeated lumbar punctures.

Latex Agglutination:
Latex agglutination (LA) allows rapid detection of bacterial antigens in
CSF. Sensitivity varies greatly between bacteria. LA for Haemophilus
illfluenzae has a sensitivity of 60 to 100 percent, but is much lower for
other bacterial. The specificity for LA is very low. However, LA can be
useful in partially treated meningitis cases where cultures may not yield
an organism. Because false positives lead to unnecessary treatment, LA is
not routinely used today. Some experts suggest using LA in cases of
suspected bacterial meningitis if the initial Gram stain and bacterial
culture are negative after 48 hours.
Polymerase Chain Reaction:
Polymerase chain reaction (PCR) has been a great advance in the
diagnosis of meningitis. PCR has high sensitivity and specificity for
many infections of the CNS, is fast, and can be done with small volumes
of CSF. Although testing is expensive, there is a potential for cost savings
by decreasing overall diagnostic testing and intervention.
PCR has been especially useful in the diagnosis of viral meningitis. PCR
of the CSF has a sensitivity of 95 to 100 percent, and a sensitivity of 100
percent for herpes simplex virus type I, Epstein-Barevirus, and
enterovirus. PCR is faster and more sensitive than culture for enterovirus
meningitis. When PCR is positive for enterovirus, it allows earlier
hospital discharge and less intervention.

PCR is the most sensitive means of diagnosing CMV infections of the
CNS, and it has been suggested that PCR should replace brain biopsy as
the gold standard for herpes encephalitis.
PCR has a sensitivity of 54 to 100 percent and a specificity of 94 to 100
percent for tuberculous meningitis, and could replace acid-fast bacillus
smear and culture as the test of choice. PCR is sensitive for acute
neurosyphilis but not for more chronic frms. PCR also is being studied as
a diagnostic tool for bacterial meningitis and other infections of the CNS.
LACTATE:. The CSF lactate is used mainly to help differentiate
bacterial and fungal meningitis, which cause increased lactate, from viral
meningitis, which does not.
LACTATE DEHYDROGENASE:. This enzyme is elevated in bacterial
and fungal meningitis, malignancy, and subarachnoid hemorrhage.
WHITE BLOOD CELL (WBC) COUNT.: The number of white blood
cells in CSF is very low, usually necessitating a manual WBC count. An
increase in WBCs may occur in many conditions including infection
(viral, bacterial, fungal, and parasitic), allergy, leukemia, multiple
sclerosis, hemorrhage, traumatic tap, encephalitis, and Guillain-Barre
syndrome. The WBC differential helps to distinguish many of these
causes. For example, viral infection is usually associated with an increase
in lymphocytes, while bacterial and fungal infections are associated with
an increase in polymorphonuclear leukocytes (neutrophils). The

differential may also reveal eosinophils associated with allergy and
ventricular shunts; macrophages with ingested bacteria (indicating
meningitis), RBCs (indicating hemorrhage), or lipids (indicating possible
cerebral infarction); blasts (immature cells) that indicate leukemia; and
malignant cells characteristic of the tissue of origin. About 50% of
metastatic cancers that infiltrate the central nervous system and about
10% of central nervous system tumors will shed cells into the CSF.
RED BLOOD CELL (RBC) COUNT.: While not normally found in
CSF, RBCs will appear whenever bleeding has occurred. Red cells in
CSF signal subarachnoid hemorrhage, stroke, or traumatic tap. Since
white cells may enter the CSF in response to local infection,
inflammation, or bleeding, the RBC count is used to correct the WBC
count so that it reflects conditions other than hemorrhage or a traumatic
tap. This is accomplished by counting RBCs and WBCs in both blood
and CSF. The ratio of RBCs in CSF to blood is multiplied by the blood
WBC count. This value is subtracted from the CSF WBC count to
eliminate WBCs derived from hemorrhage or traumatic tap.
GRAM STAIN.: The Gram stain is performed on a sediment of the CSF
and is positive in at least 60% of cases of bacterial meningitis. Culture is
performed for both aerobic and anaerobic bacteria. In addition, other
stains (e.g. the acid-fast stain for Mycobacterium tuberculosis, fungal
culture, and rapid identification tests [tests for bacterial and fungal
antigens]) may be performed routinely.
SYPHILIS SEROLOGY.: This involves testing for antibodies that
indicate neurosyphilis. The fluorescent treponemal antibody-absorption
(FTA-ABS) test is often used and is positive in persons with active and
treated syphilis. The test is used in conjunction with the VDRL test for
nontreponemal antibodies, which is positive in most persons with active
syphilis, but negative in treated cases.
Precautions:
In some circumstances, a lumbar puncture to withdraw a small amount of
CSF for analysis may lead to serious complications. Lumbar punctures
should be performed only with extreme caution, and only if the benefits
are thought to outweigh the risks. In people who have bleeding disorders,
lumbar puncture can cause hemorrhage that can compress the spinal cord.
If there is increased spinal column pressure, as may occur with a brain
tumor and other conditions, removal of CSF can cause the brain to
herniate, compressing the brain stem and other vital structures and
leading to irreversible brain damage or death. Bacteria introduced during

the puncture may cause meningitis. For this reason, aseptic technique
must be followed strictly, and a lumbar puncture should never be
performed at the site of a localized skin lesion.
Specimens should be handled with caution to avoid contamination with
skin flora. They should be refrigerated if analysis cannot be performed
immediately.
Description:
Lumbar puncture is performed by inserting the needle between the fourth
and fifth lumbar vertebrae (L4-L5). This location is used because the
spinal cord stops near L2, and a needle introduced below this level will
miss the cord. In rare instances, such as a spinal fluid blockage in the
middle of the back, a physician may perform a spinal tap in the cervical
spine.

Aftercare:
After the procedure, the site of the puncture is covered with a sterile
bandage. The patient should remain lying down for four to six hours after
the lumbar puncture. Vital signs should be monitored every 15 minutes
for four hours, then every 30 minutes for another four hours. The
puncture site should be observed for signs of weeping or swelling for 24
hours. The neurological status of the patient should also be evaluated for
such symptoms as numbness and/ or tingling in the lower extremities.
Aftercare:
After the procedure, the site of the puncture is covered with a sterile
bandage. The patient should remain lying down for four to six hours after
the lumbar puncture. Vital signs should be monitored every 15 minutes
for four hours, then every 30 minutes for another four hours. The
puncture site should be observed for signs of weeping or swelling for 24
hours. The neurological status of the patient should also be evaluated for
such symptoms as numbness and/ or tingling in the lower extremities.
Risks:
The most common side effect after the removal of CSF is a headache.
This occurs in 10-30% of adult patients and in up to 40% of children. It is
caused by a decreased CSF pressure related to a small leak of CSF
through the puncture site. These headaches usually are a dull pain,
although some people report a throbbing sensation. A stiff neck and
nausea may accompany the headache. Lumbar puncture headaches
typically begin within two days after the procedure and persist from a few
days to several weeks or months.
Normal results:
Gross appearance: Normal CSF is clear and colorless.
CSF opening pressure: 50-175 mm H 2 0.
Specific gravity: 1.006-1.009.
Glucose: 40-80 mg/ dL.

Total protein: 15-45 mg/ dL.
LD: 1/10 of serum level.
Lactate: less than 35 mg/ dL.
Leukocytes (white blood cells): 0-
30/microL (newborns).
Differential: 60-
macrophages; other cells 2% or less. Monocytes and macrophages are
somewhat higher in neonates.
Gram stain: negative.
Culture: sterile.
Syphilis serology: negative.
Red blood cell count: Normally, there are no red blood cells in the CSF
unless the needle passes through a blood vessel on route to the CSF.
Lumbar Puncture (LP)brief of the guide line
Indications:*
1. Diagnostic aid (infection, hemorrhage, leptomeningeal carcinomatosis,
multiple sclerosis, Guillain-Barre .syndrome, inflammatory conditions, to test for
therapeutic response in NPH, normal pressure hydrocephalus, before shunting)
2. Therapy for idiopathic intracranial hypertension
3. Infusion of anaesthetic ("spinal"), chemotherapy, or agents (contrast myelography

Contraindications:
- INR > 1.4 or other coagulopathy
- platelets < 50
- infection at desired puncture site
- obstructive / non-communicating hydrocephalus
- intracranial mass
- high intracranial pressure (ICP) / papilledema (relative contraindication
, depends on etiology, especially with intracranial mass lesion secondary
to the increased risk of tran stentorial or cerebellar herniation)
- focal neurological symptoms/signs, decreased level of consciousness
- partial/complete spinal block
- acute spinal trauma
Complications:
Relatively common
1) Post LP headache (rates vary from 1-70%, probably <5% for persistent
troublesome headache, "low pressure headache" i.e. headache increases
when upright and diminishes when supine, occasionally associated with
nausea, vomiting and tinnitus, onset within 1-3 days and usually lasts
<5d)
2) Post LP back pain «1/3 of patients, due to local soft tissue truma
Rare
3) Infection e.g. spinal abcess, meningjtis (estimated at 0.2%)

4) Spinal subdural/epidural hematoma (predominantly in patients with a
coagulopathy)
5) Nerve root or spinal cord injury (transient nerve root irritation much
more common than persistent injury)
6) Epidermoid tumor implantation (very low risk if needle advanced only
with stylet in place)
7) Transtentorial or cerebellar herniation (risk 0-5% in patients known to
have an intracranial mass and high ICP)
8) Complications secondary to low intracranial pressure
a) Hearing loss, CNV1 paresis
b) Intracranial subdural hygroma 1 hematoma
10) Complete spinal block (in patients willl partial spinal block)
11) Pachymeningeal enhancement may be seen on gadolinium-enhanced
MRI of head or spine after a lumbar puncture (may be related to low
pressure) CT scanning of the head before LP in suspected meningitis:
- The most worrisome contraindication to lumbar puncture is the
suspicion of increased ICP due to a cerebral mass lesion. Performing a
lumbar puncture in these patients may lead to either trans-tentorial or
uncal herniation and acute neurological deterioration.
- The absence of allthese features makes a significant lesion precluding
LP very unlikely
1) Age> 60 yrs
2) Immuno-compromised state
3) History of CNS disease (eg. grand mal seizures, brain tumour,
hydrocephalus, multiple sclerosis)
4) Seizure within one week of presentation
5) Abnormal LOC
6) Unable to answer two questions correctly or follow two commands
7) Abnormal neurological examination
. An LP may safely be performed without first doing a CT head in a
young previously healthy patient with no history of seizures, a normal
level of consciousness and a normal neurological exam.
Anatomy - Spinal cord usually terminates at L 1 or L 1/L2 in adults (-
95% of adults)
- Thecal sac terminates at -S2
- Intercristal line is an imaginary line that connects the superior border of
the iliac crests
- L4/5 interspace is the first interspace caudal to the intercristal line

Materials:
- sterile gloves and mask
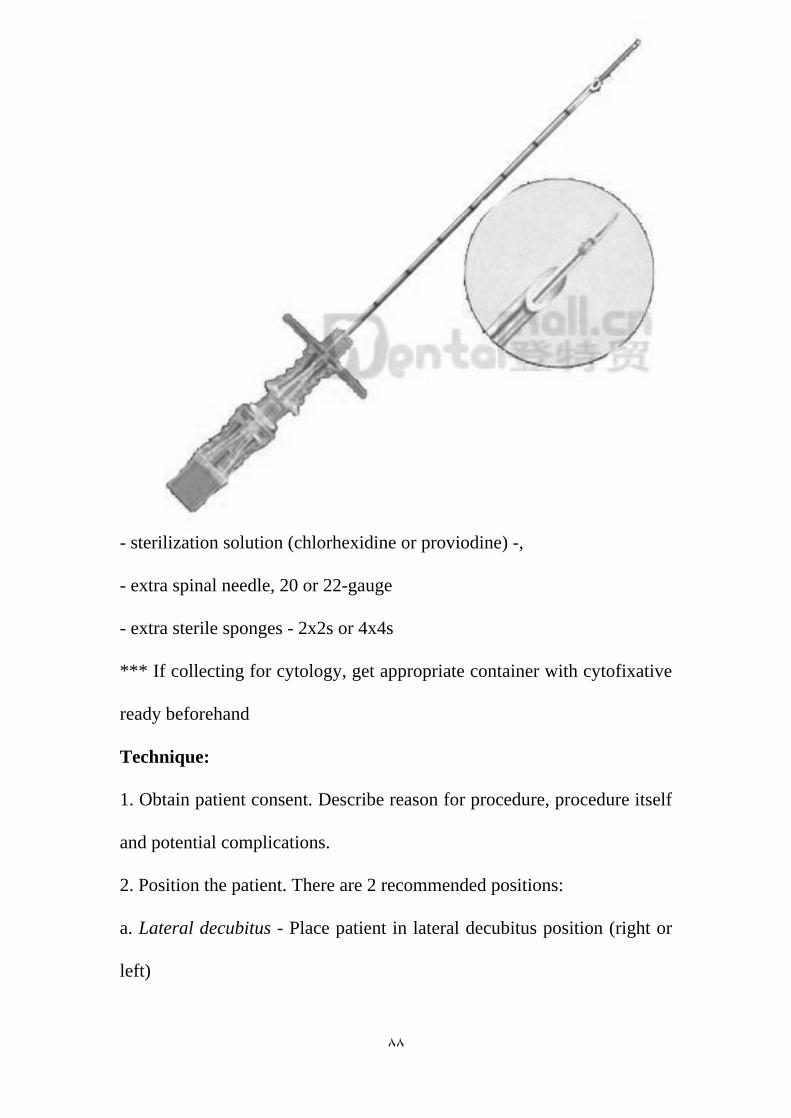
- LP kit (contains: syringe, 25 and 22G needles, 1 % lidocaine, sterile
drapes, sponges and gauze, 22G LP needle, stopcock and manometer, 4
collection tubes and band-aid)
- sterilization solution (chlorhexidine or proviodine) -,
- extra spinal needle, 20 or 22-gauge
- extra sterile sponges - 2x2s or 4x4s
*** If collecting for cytology, get appropriate container with cytofixative
ready beforehand
Technique:
1. Obtain patient consent. Describe reason for procedure, procedure itself
and potential complications.
2. Position the patient. There are 2 recommended positions:
a. Lateral decubitus - Place patient in lateral decubitus position (right or
left)

- Lumbosacral area should be as close to edge of bed as possible
- Pillow under head and between legs
- Head flexed and legs curled up towards chest ("fetal" position)
- Shoulders and hips must be perpendicular to bed / floor
b. $itting up
- patient sitsup and leans over a table, resting head and arms on a pillow
- the back of the patient's legs should be resting against the edge of the
bed
- torso / spinal column should be perpendicular to the bed / floor
- ask patient to bulge out lumbosacral spine
3. Landmark. Identify intercristal line and the L4/L5 interspace. Mark this
interspace by making an impression on the patient's skin with the tip of a
pen.
4. Carefully open LP kit and put cleaning solution in reservoir.
5. Put on mask and sterile gloves.
6. Sterilize the field using the sterilizing solution and sponges provided.
Clean a 6 inch area around the desired entry site, proceeding outward in
concentric circles. Do this 3 separate times. Place sterile drape over the
field.
7. Ensure all items in LP tray are ready for use. Eg. 1 % or 2% lidocaine
loaded into syringe, collection tubes open, test to see that the stylet slides

in/out of LP needle easily, stopcock and manometer for opening pressure
measurement ready.
8. Local anaesthesia. Using a 25G needle, inject 1 % or 2% lidocaine
under the skin at the desired entry site. A small bleb under the skin is
sufficient. Switch the needle tip to the 22G needle and anaesthetize
deeper structures by inserting the needle further, injecting lidocaine while
proceeding forward.
9. Insert LP needle. The bevel should be parallel to the spinal column.
Always advance the needle with the stylet in place. Aim needle in the
midline, slightly cephalad, towards the patient's umbilicus. Advance
needle slowly until it is inserted 2-3 cm, then withdraw the stylet to check
for CSF return. Continue to advance the needle,
periodically checking for CSF return. Often a "pop" is appreciated as the
needle pierces the dural membrane. If the needle meets bone or if blood
returns (hitting the venous plexus anterior or posterior to the spinal
canal), withdraw the needle to the skin and redirect the needle
10. Once CSF flow is obtained, measure the opening pressure by
attaching first the stopcock to the LP needle and then the manometer to
the stopcock CSF pressure measured in this way is only accurate with
patient in lateral decubitus position and relaxed (Neck not flexed, legs
extended, no valsalva).

11. Collect CSF fluid into sequential tubes ·1-2 ml in each tube is
sufficient for basic investigations. More fluid will need to be collected for
special tests e.g. viral PCR, cytology etc. 12. Reinsert stylt. Withdraw
needle Place'band-aid over insertion site.
Tips:
1. Position, position, position
2. Try one level above or below (adults)
3. Try 20G needle
4. Ask someone else to try
5. If you can't get it .. abort and order LP under fluoroscopy
Post-LP mobilization and dural puncture headache
- A. period of bed rest along willl supplementary fluids has traditionally been
recommended post-LP to decrease the risk of post-dural puncture headache
- There is no good evidence that either of these recommendations alters the risk
of post-dura1 puncture headache

What to order:
The basics
Tube #1 Cell count and differential
Tube #2 Chemistry (protein, glucose)
Tube #3 Culture and Gram stain
Tube #4 Cell count and differential
Other tests to consider:
- Will need to collect extra fluid for these tests in tube #3 or #4.
India ink and I or Cryptococcal Ag (for Cryptococcus neoformans)
AFB and or PCR for TB
Viral PCR (includes HSV, CMV, EBV)
arbovirus WNV, echovirus
VDRL
fungal culture
viral culture
PCR and or antibody titers for Lyme ds.
oligoclonal banding (3-4 ml)
IgG index, IgG :albumin ratio
cytology (must be collected in cytology fixative) (8-10ml)
flow cytometry (3-4 Inl) (NOT in fixative)

How much CSF to withdraw?
- CSF is produced at a rate of 0.3 ml/min in adults or 450 ml/24t1
- CSF volume is approximately 150 ml in an adult
- For basic investigations, only require 4-8 ml
- May require more volume for special tests (see above). Maximum to be
removed at one time should probably not exceed 20 Ill!.
- 20-30 ml can be removed in case of NPH "tap test" to gauge response.
Normal values:
- Opening pressure 5-20 cm water (oilly valid in lateral decubitus
position)
- Appearance: clear, colorless
- Nucleated cells. <5 per µl
- RBC: <5 per µl.
- WBCRBC ratio. 1 :700 (. For every additional 700 RBCs seen due to
presumed traumatic tap, one WBC is expected)
- Glucose: 2/3 serum value - Protein: 200-450 mg/L
CSF Findings:
Traumatic tap (TT) VS. SAH?
Supernatant:Clear in TT In SAH, expect to see xanthochromia (yellowish
discolouration). NOTE: Xanthocromia takes time to develop. Seen in%
70 by 6h , 90% by12h after SAH.

- RBC count: Declines as CSF drains in TT, therefore compare tube #1 to
tube #4. Does not decline in SAH
- WBC.RBC ratio.' Similar to peripheral blood in TT (. 1 :700). SAH
usually promotes a leukocytosis.
Cloting of fluid May clot in TT if RBC count high. Usually does not clot
in SAH, since there are no clotting factors in CSF.
- Protein.' In TT, increase of approx. 1 mg per 100 RBC. Levels are
greater than this in SAH.
- Opening pressure Usually normal in TT and usually elevated in SAH
- Repeat LP' Usually clear in TT and still bloody xanthochromic in SAH
(CSF taken at a different spinal level)
DDx of CSF hypoglycacrnia
Infectious - Bacterial meningitis TB, Fungal, Cysticercosis, Amoebic,
Syphilis, Trichinosis, Mumps (25%), HSV, VZV
Inflammatory
Sarcoidosis
neoplastic LM carcinomatos and
VASCULAR-SAH(4-8days post bleed and metabolic du to
hypoglycemia

Refrence 1-laviR,yarnitskyD,ROWEJM,weissmanA,segal D.standard vsatramatic Whitacre needle for diagnostic lumbar puncture :arandomized trial .neurology .Oct24 2006:67(8):1492-4 2joffeAR. Lumbar puncture and brain herniation in acute bacterial minangitis:areview.j intencsive care med.jul-aug2007:22(4):194-207 2-roosKL(march 2003)lumbar puncture,semin neural23(1):105-14. 3- how do I perform alumbar puncture and analysis the result to diagnose bacterial meningitis JAMA296(16):2012-22 (OCTOBER2006) 4-leeLC,sennetM erikson JM.prevention and management of post lumber puncture head ache in pediatric oncology pation .jpediate oncol nurs .jul-aug 2007:24(4):200 5- ahmedSV, jayawarena c,judeE.post lumber puncture head ache:diagnos and management .post grade medj.NOV 2006:82(973):713-6 6-springgs DA.BURNDJ.frenchJ, etal .is bed rest useful after diacnostic lumbar puncture post grade med j .jul1992:68(801):581-3 7-aronsonPL ,zonfrilloMR .epidural cerebrospinal fluid collection after lumbar puncture pediater emerging care.jul2009:25 (7):467
-schmidex&sweet operation neurosurgical techniques indication methods and result copyright 2000 by w.b. sanders company page 1103 -2269
-merritt,s neurology twwefth edition page 310-317 10-principal neurology adam,s and victor,s 8 th 2005page 11-12 147-54211- cerospinal fluid j neuro neurosurgerypsychiatry 59-349 .1995

LUMBAR PUNCTURE
By : Dr . M . Besharat
SBMU
IDTMRC Loghman Hospital

This document was created with Win2PDF available at http://www.daneprairie.com.The unregistered version of Win2PDF is for evaluation or non-commercial use only.