sponsored by the cma organized medical staff section · the california medical association (cma)...
TRANSCRIPT

Date: October 17, 2013 To: CMA Organized Medical Staff Section From: Yvonne Choong, Staff Coordinator Subject: 2013 OMSS Assembly The California Medical Association (CMA) Organized Medical Staff Section held the 2013 Annual Assembly on Thursday, October 10, 2013 in Anaheim, CA. The CMA House of Delegates (HOD) convened on October 11-13, 2013. The meeting consisted of a business portion--during which proposed resolutions were discussed and a new slate of OMSS Executive Board officers were elected—and an educational portion during which faculty lectured on issues of interest to organized medical staffs (See agenda and speaker presentation slides.) Elections Here is the roster for the OMSS Executive Board for 2013-14: Chair – Damodara Rajasekhar, MD ([email protected]) Vice-Chair – Mel Sterling, MD ([email protected]) Secretary – Joel Velasquez, MD ([email protected]) Delegates – John Luster, MD ([email protected]) & Richard Butcher, MD ([email protected]) Alternate Delegates – Steve Kmucha, MD ([email protected]) & Rosa Rangel, MD ([email protected]) Trustee – Robert Pugach, MD ([email protected]) Status Update: 2013 CMA House of Delegates – Resolutions of Interest to the CMA Organized Medical Staff Section Various resolutions, two of which originated within OMSS, were adopted. The following is a summary of the resolution actions taken related to resolutions discussed at the OMSS Assembly. CMA will be working to implement these resolutions during the next year, as appropriate. SPONSORED BY THE CMA ORGANIZED MEDICAL STAFF SECTION
Resolution Final Language Action Resolution 211-13 ELIMINATION OF CMS OUTPATIENT OBSERVATION STATUS
RESOLVED: That CMA request the Centers for Medicare and Medicaid Services to eliminate Outpatient Patient Observation status for all patients who require care in hospitals.
Substitute adopted

Resolution 613-13 CLINICAL PRIVILEGES AND EXCLUSIVE CONTRACTS
RESOLVED: That CMA support due process rights for all physicians that are on a hospital medical staff regardless of their contractual status with that hospital; and be it further RESOLVED: That CMA support that a decision to terminate an exclusive contract shall not affect the medical staff privileges of medical staff members who were performing services pursuant to that contract.
Substitute adopted
OF INTEREST TO THE CMA ORGANIZED MEDICAL STAFF SECTION
Resolution Final Adopted Language Action Resolution 501-13 NATIONAL HEALTH INFORMATION EXCHANGE AND EHR INTEROPERABILITY
RESOLVED: That CMA support the development of a secure, interoperable, nationwide health information exchange (HIE) network; and be it further RESOLVED: That CMA support efforts to harmonize standards and specifications that would enable usability and interoperability of electronic health records (EHR) systems and facilitate the exchange of health information among health care providers; and be it further RESOLVED: That CMA support improving usability and interoperability of EHR systems with physician input on how they directly impact patient care and physician workflow; and be it further RESOLVED: That CMA support that the Office of the National Coordinator for Health Information Technology (ONC) should address EHR usability and interoperability concerns raised by physicians and add usability and interoperability criteria to the EHR certification process; and be it further RESOLVED: That CMA support legislation to mandate that all electronic health record (EHR) systems must include meaningful interoperability, to be
Substitute adopted for combined resolutions 501-13, 502-13 and 518-13

defined as a user-friendly implementation of ONC standards in a manner allowing the simple electronic transfer of fully structured medical information between EHR users and ensuring the confidentiality of protected patient information.
Resolution 502-13 CALIFORNIA STANDARDIZED ELECTRONIC MEDICAL RECORD SYSTEM
See Resolution 501-13 See Resolution 501-13
Resolution 509-13 RESTRICTIONS ON MARKETING IN HOSPITALS AND MEDICAL CENTERS
RESOLVED: That CMA support policies, duly adopted by a medical staff or facility governing body within its scope of authority: (1) that govern the level and content of contact between physicians and pharmaceutical, device and other medical product representatives in hospital and medical center settings in order to minimize undue external influence over medical judgment and patient care as necessary and appropriate for the particular medical staff or facility; and (2) that promote education, training, operative orientation and coaching as the focus of such contact; and be it further RESOLVED: That CMA urge the California Hospital Association to support such policies; and be it further RESOLVED: That this be referred for national action.
Adopted as amended
Resolution 513-13 AGE DISCRIMINATION AGAINST HEALTH CARE PROFESSIONALS
RESOLVED: That California law be amended to prohibit ageism discrimination explicitly or implicitly in any contract or in any California legislation that specifies an upper age limit; that the federal age discrimination in employment act be fully enacted to cover all health care professionals that practice in the state of California; that mandatory age-based retirement be removed from all health care employee contracts; and that the upper age limits be removed from all state laws affecting health care professionals.
Referred for study and report back

Resolution 517-13 CMA STANCE AGAINST PHYSICIAN INTIMIDATION
RESOLVED: That CMA affirm its strongest determination to protect physicians from interference, harassment, intimidation or retaliation in any form due to their advocacy for patient care and safety; and be it further RESOLVED: That CMA actively encourage physicians to continue undeterred to advocate for patient care and safety as appropriate, and to alert CMA to any cases of whistleblower retaliation, interference, harassment or intimidation.
Adopted
Resolution 601-13 TAXATION OF NOT-FOR-PROFIT HOSPITALS
NONE Not adopted
Resolution 602-13 HOSPITAL FOUNDATION OWNERSHIP OF PHYSICIAN MEDICAL GROUPS
NONE Not adopted
Resolution 603-13 UNIVERSITY HEALTH SYSTEMS AND THE CORPORATE BAR
NONE Not adopted
Resolution 605-13 EMERGENCY DEPARTMENT CONTACT OF APPROPRIATE PHYSICIANS
RESOLVED: That CMA work with hospitals, hospital medical staffs, and other stakeholders to develop a flexible model policy for communication between emergency departments and appropriate physicians, regarding mutual patients, that can be modified to accommodate each hospital’s local needs and resources.
Substitute adopted
Resolution 607-13 MAINTENANCE OF CERTIFICATION AND MAINTENANCE OF LICENSURE PROGRAMS
RESOLVED: That CMA oppose the continuance of the American Board of Medical Specialties Maintenance of Certification and the American Osteopathic Association Osteopathic Continuous Certification programs on the basis that there is no supporting evidence that such programs improve the quality of medical care while placing unnecessary burdens on physicians; and be it further RESOLVED: That CMA oppose any efforts by the Medical Board of California to adopt, use or require the Federation of State Medical Boards
Referred to Board of Trustees for decision

Maintenance of Licensure program as a condition of licensure; and be it further RESOLVED: That this matter be referred for national action.
Resolution 608-13 UNIVERSAL CREDENTIALING SYSTEM
RESOLVED: That CMA support the development of a uniform electronic credentialing system which uses a single application to gather core information on education, training and practice experience that can be supplemented as needed by participating entities.
Substitute adopted
Please contact Yvonne Choong at (916) 551-2884 or [email protected], if you have any questions regarding any items discussed here. We look forward to continuing to work with your medical staff.

2013 OMSS Annual Assembly
Thursday, October 10, 2013 7:30 am – 4:30 pm
AGENDA
7:30 AM – 8:00 AM Registration and Breakfast
8:00 AM – 8:15 AM Welcome and Introductions Richard Thorp, MD Dustin Corcoran, MBA
8:15 AM – 8:45 AM Legal Update Long Do, JD
8:45 AM -10:00 AM CMA-OMSS Business Meeting Resolutions Elections
Lytton Smith, MD
10:00 AM – 11:00 AM Overseeing Physician Contracts with Hospitals
Long Do, JD
11:00 AM – 12:00 PM Non-Physicians on the Medical Staff Astrid Meghrigian, JD
12:00 PM – 1:15 PM Lunch Medical Staff: Open Forum Legislative/Regulatory Update
Juan Torres
1:15 PM – 2:00 PM Medical Injury Compensation Reform Act (MICRA): What it Means for California Physicians
Alicia Wagnon, JD Brett Michelin, JD
2:00 PM – 3:00 PM Aging Physicians William Perry, PhD
3:00 PM – 3:15 PM Physician Health and Wellbeing: Resources for
Medical Staffs Gail Jara
3:15 PM – 4:15 PM Covered California: What Medical Staffs Need to Know
Brett Johnson, JD, MPH
4:15 PM – 4:30 PM Closing Remarks
4:30 PM Adjourn
Meeting Location: Disneyland Hotel, 1150 W Magic Way, Anaheim, (714) 778-6600

Legal Updateg p
CMA-OMSS Annual Assemblyy
Disneyland
October 10, 2013,
LongX.DoLegalCounsel&DirectorofLitigation
CaliforniaMedicalAssociation
Copyright © California Medical Association 2013
California Supreme Court CasesCalifornia Supreme Court Cases
El-Attar v. Hollywood Presbyterian Medical Center56 Cal 4th 976 (June 6 2013)56 Cal. 4th 976 (June 6, 2013)
Fahlen v. Sutter Central Valley HospitalsCal. Supreme Ct. no. S205568 (pending)
Copyright © California Medical Association 2013 2

Other CasesOther Cases
Medical Staff v. Fountain Valley Regional Hosp. & Med. Ctr.Orange County Superior Court no. 30-2013-00649470
Fitzgibbons v. Integrated Healthcare Holdings, Inc.Cal Ct of App (4th Dist ) no G048413Cal. Ct. of App. (4th Dist.) no. G048413
Medical Board v. ChiarottinoCal. Ct. of App. (1st Dist.) no. A138420
Copyright © California Medical Association 2013 3

Long X. DogLegal Counsel & Director of Litigation
California Medical AssociationCalifornia Medical Association
1201 J Street Suite 200
Sacramento, California 95814
(916) 444-5532
Copyright © California Medical Association 2013 4

OMSS Annual AssemblyDisneyland
October 10 2013October 10, 2013
Long X Do EsqLong X. Do, Esq.Legal Counsel & Director of Litigation
CMA Center for Legal Affairs

TOPICS
Part 1 | Reality Check
Part 2 | Legal Constraints| g
Part 3 | Medical Staff Oversight
introduction
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 32

TRADITIONAL HOSPITAL – PHYSICIAN RELATIONSHIP
Voluntary Medical Staff Model
Hospitals Offerp Capital and facilities Up to date equipment Allied health professionals and support staffAllied health professionals and support staff Privileges Centers for quality
Ph i i OffPhysicians Offer Professional services and staffing Emergency call coverageQuality improvement activities Patient admissions
3part 1 | reality check
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 3

HOSPITAL PRACTICE TRENDSState population is growing and aging
37.6M currently, to reach 39.2M in 2015California Medicare eligible – 3.6M in 2000, 6.4M in 2020Low-income population increasing, greater wealth gap
Major financial strains State budget pressures and government reimbursement cuts Tightened credit market constrains access to capitalIncrease in uncompensated care
Cost shifts and pressures to contain costsPublic payors shifting to private managed careFocus on cost containment by public and private payors
Growth in ambulatory surgery centers300% increase in outpatient surgeries since 1996 (CDC)
The Traditional Voluntary Medical Staff Model is Fraying
part 1 | reality check
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 34

PHYSICIAN PRACTICE TRENDS
(FFS R S )
(Practice Costs ↑Medicare Payments ↓ )
(FFS Revenue Stagnant)
(Practice Costs as Percentage of Net Revenue)
part 1 | reality check
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 35

PHYSICIAN PRACTICE TRENDS
Revenue from private payors down
Increased administrative costsIncreased administrative costs
Electronic medical record systems
Payor audits
Quality measurements
Small IPAs most at risk
Groups are merging to increase membership
Public reimbursement down
Physicians Are Feeling Pressure to Change
part 1 | reality check
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 36
REFORMS AND MARKET PRESSURES ARE DRIVING NEW RELATIONSHIPS
New alignments with physicians and other providers and payors
New payment schemes from New payment schemes from volume-based to value-based
EHR and quality measurements
M&As of systems of physician groups and hospitals
part 1 | reality check
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 37

CONTINUUM OF PHYSICIAN/HOSPITAL INTEGRATION METHODS
Degree of Integration
• Physician liaison (VP of Medical Affairs
• ED call coverage agreements
• Real estate/ medical offices
• Office
• Co-management agreements
• Medical foundations
• HospitalMedical Affairs, etc.)
• Service line physician advisory
agreements• Recruitment
assistance• Income
guarantees
• Office timeshare/equipment leases
• Clinical
agreements• Hospital-based
outpatient clinics
• Equity joint
• Hospitalsyndication
• Academic practice
• ACOsadvisory councils
• Medical directorships
guarantees• Physician-
hospital joint marketing
• Hospitalist/
• Clinical institutes/ Centers of excellence
• Gainsharing
• Equity joint ventures
• Clinical integration
• ACOs
• Hospitalist/ intensivist programs
• Gainsharing• MSO/PHO
part 1 | reality check
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 38

BENEFITS OF ALIGNMENT (FOR HOSPITALS)
Assumption by Group/individual of responsibility for effective administration, supervision and coverage;
D l t f ki l ti hi b t th Development of necessary working relationships between the Group/individual and other hospital personnel and departments;
Hospital control over operation of its department;
Assures full-time availability of services;
Lowers costs through standardization of procedures and centralized administration of the departments;administration of the departments;
Allows better scheduling of the use of the facilities;
Assures compliance with the accreditation and licensing i t requirements;
Improves supervision of the support staff and working relations between staff and physicians
part 1 | reality check
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 39

ANTI-KICKBACK LAWS
The offering or acceptance of anything of value for the referral of patients by physicians is prohibited.
• Federal Medicare/Medicaid laws, 42 U.S.C. §1320a-7b• Federal False Claims ActFederal False Claims Act• Cal. Business & Professions Code §650• Cal. Welfare & Institutions Code §14107.2
C l I C d §750• Cal. Insurance Code §750• Cal. Labor Code §3215
part 2 | legal constraints
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 310

STARK LAWS
Physicians are prohibited from referring patients to specified entities in which the physician or a member of the physician's immediate family has a financial interest
42 U S C §1395 • 42 U.S.C. §1395nn
• Cal. Business & Professions Code §§650.01, 650.02
• Cal Labor Code §§139 3 139 31 139 32• Cal. Labor Code §§139.3, 139.31, 139.32
part 2 | legal constraints
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 311

COMMON VIOLATIONS
• Excessive Compensation• Providing Free Services or Staff to Physicians• Paying for Unnecessary Services• Providing Discounts on Items, Such as Leased Space• Failing to Meet Requirements to Fulfill the • Failing to Meet Requirements to Fulfill the
Recruitment Exception in the Stark and Anti-Kickback laws
• Obtaining Preferential Treatment in Return for Referrals
(Ultimately depends on fair market value, applicability of (Ultimately depends on fair market value, applicability of safe harbors or statutory exceptions.)
part 2 | legal constraints
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 312
BAR ON THE CORPORATE PRACTICE OF MEDICINE
“The presence of a corporate entity is incongruous in the workings of a professional regulatory licensing scheme which is based on a professional regulatory licensing scheme which is based on personal qualification, responsibility and sanction, and that the interposition of a lay commercial entity between the professional and his/her patients would give rise to divided loyalties on the part and his/her patients would give rise to divided loyalties on the part of the professional and would destroy the professional relationship into which it was cast.”
65 Ops Cal Atty Gen 223 225 (1982)- 65 Ops. Cal. Atty. Gen. 223, 225 (1982)
part 2 | legal constraints
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 313

BAR ON THE CORPORATE PRACTICE OF MEDICINE
Medical Board Guidance on Activities Violating the Corporate Bar (i.e., control over the physician’s practice of medicine): Ownership is an indicator of control of a patient's medical Ownership is an indicator of control of a patient s medical
records, including determining the contents thereof, and should be retained by a California licensed physician.
Selection (hiring/firing as it relates to clinical competency or Selection (hiring/firing as it relates to clinical competency or proficiency) of professional, physician extender, and allied health staff.
Setting the parameters under which the physician will enter into g p p ycontractual relationships with third-party payers.
Decisions regarding coding and billing procedures for patient care services.
Approval of the selection of medical equipment for the medical practice.
part 2 | legal constraints
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 314

CONTRACT LAW
Courts generally favor enforcement of private contracts, but there are exceptions.
Contracts of adhesion Unduly oppressive or unconscionableUnduly oppressive or unconscionable Violation of law Contracts in contravention of public policy
part 2 | legal constraints
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 315

FUNCTIONS OF THE MEDICAL STAFF
The right and responsibility to be self-governing with respect to the “professional work performed in a h it l ” S B & P f C d §2282hospital.” See Bus. & Prof. Code §2282 Patient welfare depends on ongoing review and improvement of
the quality of care rendered in hospitals The medical staff is the only independent body with the medical
expertise, clinical experience and familiarity with the facilities and personnel involved necessary to conduct effective peer review
The medical staff provides a vital role by using its independent voice to advocate for quality of care
part 3 | medical staff oversight
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 316

COMPONENTS OF SELF-GOVERNANCE
Initiation, development, adoption and amendment of medical staff bylaws, rules and regulations subject to hospital governing board approval (not unreasonably withheld)board approval (not unreasonably withheld)
Selection and removal of medical staff officers Establishment of enforcement criteria for membership Establishment of clinical criteria and standards to oversee and Establishment of clinical criteria and standards to oversee and
manage quality assurance, UR, and other meetings of the medical staff
Assessment and utilization of medical staff duesAssessment and utilization of medical staff dues Establishment of patient care standards Accessibility to and use of independent legal counsel at medical
staff’s expensestaff s expense
- Bus. & Prof. Code §2282.5
part 3 | medical staff oversight
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 317

MEANINGFUL INPUT OVER QUALITY ISSUES
CMA Model Medical Staff Bylaws §7.6-1. Appropriateness of Exclusive Contracts §7 6-3 Department/Service Formation or Elimination§7.6 3. Department/Service Formation or Elimination §11.18. Medical Staff Contracts Review Committee
Key Principles:Key Principles: Reviews to be conducted prior to change in contract/service Hospital is required to consider recommendations and input
from the medical staff Hearing rights preserved for affected physicians Establishes evidentiary standards Medical staffs focus on affect on quality Privileges cannot be tied to a contract (Fountain Valley case)
part 3 | medical staff oversight
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 318

CREDENTIALING, PRIVILEGING AND PEER REVIEW
A primary function of the medical staff is to ensure the competence of its physician members.
Credentialing and privileging (through peer review) is aimed at ensuring the highest quality of care at a hospital, as well as to ensure that physicians’ privileges are not as e as to e su e t at p ys c a s p eges a e otunreasonably or arbitrarily denied.
part 3 | medical staff oversight
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 319

CONFLICT OF INTEREST POLICIES
“For the purposes of these bylaws, CONFLICT OF INTEREST means a personal or financial interest or conflicting fiduciary means a personal or financial interest or conflicting fiduciary obligation that makes it impossible, as a practical matter, for the individual to act in the best interests of the medical staff without regard to the individual's private or personal interest.without regard to the individual s private or personal interest.. . . . A member shall recuse if the member reasonably believes that the member’s ability to render a fair and independent decision is or may be affected by a conflict of independent decision is or may be affected by a conflict of interest. ”
- CMA Model Medical Staff Bylaws §14.6
part 3 | medical staff oversight
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 320

Long X. Do, Esq.
California Medical Association
1201 J Street, Suite 200
Sacramento, CA 95814
(916) 444-5532
end
C a l i f o r n i a M e d i c a l A s s o c i a t i o n © 2 0 1 321

2013 OMSS Annual Assembly
NON PHYSICIANS ON/AND THENON‐PHYSICIANS ON/AND THE MEDICAL STAFF – How Does It All
k?Work?
October 10 2013October 10, 2013 Astridstrid G. Meghrigian, Esq.

What We Will CoverWhat We Will Cover
Non‐Physicians and Current TrendsNon Physicians and Current TrendsWho can be on the Medical Staff and future predictionspredictionsSpecial Considerations Concerning Clinical P h l i ( d P di i )Psychologists (and Podiatrists)
2013 OMSS Annual Assembly 2

What We Will Cover (cont.)What We Will Cover (cont.)
Non‐physicians who are not on the medicalNon physicians who are not on the medical staff:– Who are they? y– How to evaluate which categories will be permitted to practice at the hospital
– What are the scope of permissible activities?– How to credential– Can they admit patients– What type of fair hearing rights?D b k R i– Databank Reporting
2013 OMSS Annual Assembly 3

Current Trends
Growth both numerically and categoricallyGrowth both numerically and categoricallyPopulation GrowthAging populationRetiring WorkforcegLegislative policy (“Access to Care”)
2013 OMSS Annual Assembly 4

Current Trends‐ Legislative Policy and “ l h f i l”“Health Care Professional”
California ExchangeModel ContractFormer Definition of Medically Appropriate
Regulatory Efforts
2013 OMSS Annual Assembly 5
Current Trends‐ Legislative Policy and “ l h f i l”“Health Care Professional”
Scope Expansions SB 494 – Numeric ratios increased where NPs/PAs SB 352 – Medical assistants without MD supervision
AB 1308 No MD supervision for licensedAB 1308 – No MD supervision for licensed midwives
SB 493 – Expansion of pharmacy practicep p y pAB 1000 – Direct access to physical therapistAB 154 – Abortion services
2013 OMSS Annual Assembly 6

Current Trends: Some NumbersCurrent Trends: Some Numbers
More than 400 000 health care jobs added in CA lastMore than 400,000 health care jobs added in CA last decade
CHA estimates it needs an additional 1,000,000 allied h lth f i l b 2030health professionals by 2030
The number of physician assistants in California grew 62% between 2001 and 2009, from 5,000 to 8,000 professionals. The Northern and Sierra region had a greater number of physician assistants per capita than the rest of the state.
Therapist employment in California jumped significantly between 2001 and 2009, with speech‐language pathologists increasing the most (48%) andlanguage pathologists increasing the most (48%) and occupational therapists the least (15%).
2013 OMSS Annual Assembly 7

Current Trends: hThe Categories
Registered nurses AudiologistsNurse midwivesNurse practitioners
Registered dispensing opticians
Nurse anesthetistsVocational nurses
Occupational therapistsDieticians Ph i l th i tPsychoanalysts
Speech‐language pathologists
Physical therapistsPhysical therapy assistantsOptometristspathologists Optometrists
2013 OMSS Annual Assembly 8

Current Trends: h ( )The Categories (cont.)
Hearing aid dispensers Chiropractorsg pPhysicians’ assistantsRespiratory therapists
DentistsClinical psychologistsPodiatrists
PharmacistsPsychiatric technicians
PodiatristsLicensed midwivesPerfusionists
AcupuncturistsMarriage, family and child
l
Licensed Educational psychologists
Licensed Professional counselors
Clinical social workersClinical Counselors
NaturopathsMassage therapistsMassage therapists
2013 OMSS Annual Assembly 9

Examples of Scope of Practice LawsExamples of Scope of Practice Laws
The practice of within the meaning ofThe practice of ______ within the meaning of this chapter means those functions, including basic health care that help people cope withbasic health care, that help people cope with difficulties in daily living that are associated with their actual or potential health or illnesswith their actual or potential health or illness problems or the treatment thereof, and that require a substantial amount of scientificrequire a substantial amount of scientific knowledge or technical skill, including all of the following:following:(B&P 2725) 2013 OMSS Annual Assembly 10
Examples of Scope of Practice LawsExamples of Scope of Practice Laws
”_______” means the application of counseling interventions and psychotherapeuticinterventions and psychotherapeutic techniques to identify and remediate cognitive, mental and emotional issues includingmental, and emotional issues, including personal growth, adjustment to disability, crisis intervention and psychosocial andintervention, and psychosocial and environmental problems.
(B&P 4999.20) 2013 OMSS Annual Assembly 11

Non‐Physicians ON the Medical Staff‐l fCalifornia
M b hi li it d t h i i dMembership limited to physicians and surgeons, dentists, podiatrists and, within the di ti f h f ilit t ddiscretion of each facility not owned or operated by the state, clinical psychologists. (H lth & S f t C d 1316 5 22 C C R(Health & Safety Code 1316.5; 22 C.C.R. 70701.) For state hospitals that offer mental health services, membership for clinical psychologists mandatedRegulatory efforts2013 OMSS Annual Assembly 12
Non‐Physicians ON the Medical Staff‐diMedicare
The governing body must determine inThe governing body must determine, in accordance with State law, which categories of practitioners are eligible candidates forpractitioners are eligible candidates for appointment to the medical staff. 42 CFR482 12482.12– CMS Interpretive Guidelines
• At a minimum must be composed of physicians• At a minimum, must be composed of physicians• Governing body has flexibility to determine others consistent with State law
• Surveyors should review verify that governing body has determined and stated eligible categories2013 OMSS Annual Assembly 13

Non‐Physicians ON the Medical Staff‐di ( )Medicare (cont.)
The medical staff must include doctors ofThe medical staff must include doctors of medicine or osteopathy. In accordance with State law, including scope‐of‐practice laws, the medical staff may also include other categories of nonstaff may also include other categories of non‐physician practitioners determined as eligible for appointment by the governing body. 42 CFR482.22– 2012 Amendment – CMS Rationale –“We believe that the greater flexibility for hospitals– We believe that the greater flexibility for hospitals and medical staffs to enlist the services of non‐physician practitioners to carry out the patient care duties for which they are trained and licensed willduties for which they are trained and licensed will allow them to meet the needs of their patients most efficiently and effectively”….”APRNs, PAs” etc. “have equally important roles to play on a medical staff”
2013 OMSS Annual Assembly 14

Why Does Medicare Matter So Long as We h lif i l ?have California law?
Medicare – Medical staff bylaws must include a requirement that a medical history anda requirement that a medical history and physical examination must be completed by a physician . . . or “other qualified licensedphysician . . . or other qualified licensed individual in accordance with state law and hospital policy.”hospital policy. (42 C.F.R. §482.22)
2013 OMSS Annual Assembly 15

Why Does Medicare Matter So Long as We h lif i l ?have California law?
Former B&P 2472‐ “A doctor of podiatric medicine shall not perform an admittingmedicine shall not perform an admitting history and physical examination of a patient in an acute care hospital where doing soin an acute care hospital where doing so would violate the regulations governing the Medicare program.”Medicare program.
2013 OMSS Annual Assembly 16
Why Does Medicare Matter So Long as We y ghave California law? (cont.)
BPM ‐ ”DPMs are trained and fully licensed under California law to independently perform full‐body history and physical (H&P) examinations in any setting for any patient. With new regulations finalized by the federal Centers for Medicare & Medicaid Services (CMS), there is no longer any conflict with federal criteria.”
2013 OMSS Annual Assembly 17

Why Does Medicare Matter So Long as WeWhy Does Medicare Matter So Long as We have California law? (cont.)
2012 ‐ SB 1236 repeal as “an obsolete provision prohibiting a DPM from performing an admitting history and physical exam at an acute care hospital”
2013 OMSS Annual Assembly 18

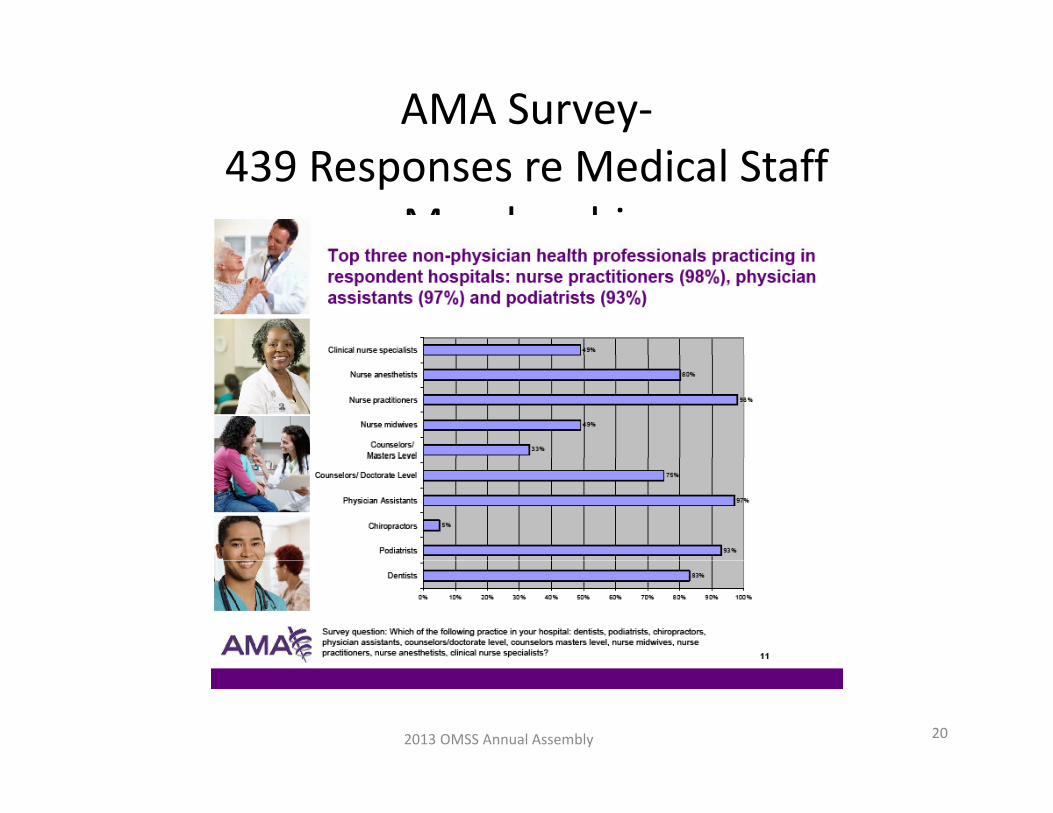
AMA Survey‐439 Responses re Medical Staff
Membershipp(November 2010)
Nurse anesthetists‐ 10%Nurse practitioners‐ 12%Nurse practitioners 12%Nurse midwives‐ 13%Ph i i i t t 12%Physician assistants‐ 12%
2013 OMSS Annual Assembly 19
AMA Survey‐di l ff439 Responses re Medical Staff
Membership
2013 OMSS Annual Assembly 20

AMA Survey‐di l ff439 Responses re Medical Staff
Membership
2013 OMSS Annual Assembly 21

Composition of the Medical Executive iCommittee
If the medical staff has an executive committee, a majority of the members of the , j ycommittee must be doctors of medicine or osteopathy. (42 CFR 482.22) See also, JC p y ( ) ,MS.02.01.01 (same)
2013 OMSS Annual Assembly 22

Who Can Be the Chief of Staff?Who Can Be the Chief of Staff?
Medicare‐ Responsibility must be assigned to:Medicare Responsibility must be assigned to:An individual doctor of medicine or osteopathy.A doctor of dental surgery or dental medicineA doctor of dental surgery or dental medicine, when permitted by State law of the State in which the hospital is locatedwhich the hospital is located.
A doctor of podiatric medicine, when permitted by State law of the State in which the hospital isby State law of the State in which the hospital is located. 42 CFR 482.22
California A physician must have overallCalifornia‐ A physician must have overall responsibility for the medical service 22 CCR 70205
2013 OMSS Annual Assembly 23

Some Special Thoughts on Clinical h l iPsychologists
“If a health service is offered by a health facilityIf a health service is offered by a health facility with both licensed physicians and surgeons and clinical psychologists on the medical staff whichclinical psychologists on the medical staff, which both licensed physicians and surgeons and clinical psychologists are authorized by law toclinical psychologists are authorized by law to perform, the service may be performed by either without discrimination ” HSC 1316 5either, without discrimination. HSC 1316.5“Psychologists may take primary responsibility f d i i di i t t t dfor admission, diagnosis , treatment and discharge of patients.” CAPP v Rank2013 OMSS Annual Assembly 24
Special Thoughts (Cont.)‐hi l?Is this Legal?
The prerogatives of a clinical Psychologist should be to:The prerogatives of a clinical Psychologist should be to:
1) Provide specified patient care services under the supervision or direction of a physician member of the p p yMedical Staff.
2) Exercise independent judgment within the areas of his professional competence and may participate directlyprofessional competence, and may participate directly in the medical management of patients under the supervision of a physician who has been accorded privileges to provide such care and who has ultimateprivileges to provide such care and who has ultimate responsibility for the patient's care,
3) Serve on staff, department and hospital committees,4) Attend meetings of the staff, Department of Medicine and hospital education programs.
2013 OMSS Annual Assembly 25

Medical Staff Obligations for Non‐h h d l ff h hPhysicians Not on the Medical Staff‐Which
Categories
Should not be made on an ad hoc basisDecision must be made as to entire category, not 1 individualShould be based on needs of hospital, the patients and the communityUltimate decision should be made by governing body following a fair process and g g y g pmedical staff input.
2013 OMSS Annual Assembly 26
Which Non‐physicians Can Practice at the p yHospital ‐ Factors in Decision
Must be reasonable and rationale and not for i i ianticompetitive reasons
What is the need?Can this provider type meet the standard of care for the hospital?Is there a closed staff or exclusive contract?
2013 OMSS Annual Assembly 27

Which Non‐physicians Can Practice at the p yHospital ‐ Factors in Decision (cont.)
What type of training was received in hospital setting?setting?What supervision requirements are needed?What type of changes in staffing equipment orWhat type of changes in staffing, equipment or education will be required if category accepted?What are the minimum qualifications?What are the minimum qualifications?
See CMA ON CALL #3075 for a proposed notice andSee CMA ON‐CALL #3075 for a proposed notice and comment procedure
2013 OMSS Annual Assembly 28

What is Scope of Permissible Activities?What is Scope of Permissible Activities?
Legal scope of practiceAvoid making qualifications more stringentAvoid making qualifications more stringent than othersShould be based on recommendations ofShould be based on recommendations of medical staff committee and approved by MEC and governing bodyMEC and governing bodyDelineate activities in a list Bylaws or rules and regs vs. separate document
2013 OMSS Annual Assembly 29

Who is Responsible for Credentialing?Who is Responsible for Credentialing?
Medical staff responsibility to assure quality (22 CCR 70703)p y q y ( ) Interdisciplinary practice committee (established by and
accountable to governing body)– Mandated whenever registered nurses will perform functionsMandated whenever registered nurses will perform functions
according to standardized procedures, or when non‐medical staff members will be granted authorization for the performance of services in the hospital
Allied Health Committee (CMA Model) Joint Commission‐ all licensed independent practitioners
must be credentialed and privileged through the Medical p g gStaff‐ others either through the medical staff process or something that is equivalent– Procedure must be approved by governing body with input from
MEC Ultimately Board decision
2013 OMSS Annual Assembly 30

Composition of Interdisciplinary iCommittee
Th director of nursing The director of nursing The administrator or designee An equal number of physicians appointed by the Executive
C i f h di l ffCommittee of the medical staff Registered nurses appointed by the director of nursing Others who are performing functions (formerly, just physician
assistants)
(When the hospital has a psychiatric unit and one or more ( p p yclinical psychologists on its medical staff, one or more clinical psychologists as appointed by the MEC) 22 CCR 70706
2013 OMSS Annual Assembly 31

Mandated Responsibilities of di i li iInterdisciplinary Committee
Must establish written policies and procedures for theMust establish written policies and procedures for the conduct of its business which must include, but need not be limited to: Provision for securing recommendations from members of the medical staff in the medical specialty or clinical field of practice under review, and from persons in thefield of practice under review, and from persons in the appropriate non‐medical category who practice in the clinical field or specialty under review,
h f fMethods for approving standardized procedures for registered nurses ‐affirmative approval of the administrator and a majority of the physician members j y p yand nurse members of the committee are required,
2013 OMSS Annual Assembly 32

Mandated Responsibilities of di i li iInterdisciplinary Committee
Provision for maintaining clear lines of responsibility of Provision for maintaining clear lines of responsibility of the nursing service for nursing care and the medical staff for medical services, and
Specifying the intended line of approval for each Specifying the intended line of approval for each recommendation of the committee.
Recommending policies and procedures for granting of d d l i il ( d d ti li ) texpanded role privileges (and credentialing) to
registered nurses, whether or not they are employed by the facility, to provide for the assessment, planning and di ti f th di ti d th ti fdirection of the diagnostic and therapeutic care of a patient in a licensed health facility.
(PAs approved by MEC)( pp y )22 CCR 70706(c), 70706.1
2013 OMSS Annual Assembly 33

Credentialing Non‐physicians Who Are Not h di l ffon the Medical Staff
Independent v dependent practitionersBe wary of overly stringent qualifications (e.g., y y g q ( g ,CPR)General qualificationsGeneral qualificationsMaintain supervision requirement as appropriateappropriatePeer references and the Joint Commission‐“ i ll l lifi i ”“essentially equal qualifications”
2013 OMSS Annual Assembly 34
Querying the AuthoritiesQuerying the Authorities
Query State BoardsQuery State Boards– Licentiate" means a physician, podiatrist, clinical psychologist marriage and family therapist clinicalpsychologist, marriage and family therapist, clinical social worker, or dentist under B&P 805
NPDB must query all practitioners on medicalNPDB‐must query all practitioners on medical staff
V l t ti f ll th th h i i d– Voluntary reporting for all other than physician and dentist (45 CFR 60.12)
2013 OMSS Annual Assembly 35

Supervision and the h i iNon‐physician
General Supervision‐– Surgical procedures by dentists and podiatrists‐overall supervision by department chair or designee
Specific supervision‐ dependent practitioners– Qualification of practice prerogative– Physician medical staff members with specific privileges to supervise
• Supervisor Agreement
2013 OMSS Annual Assembly 36
Supervision and the hNon‐physician
Overall Responsibility Medicare Patients mustOverall Responsibility‐Medicare Patients must be under the care of:
A h i i– A physician– A dentistA di i– A podiatrist
– An optometrist– A chiropractor – A clinical psychologist (42 CFR 482.12)
2013 OMSS Annual Assembly 37
Overall Responsibility‐ Joint Commission MS 03.01.03
A patient’s general medical condition isA patient s general medical condition is managed and coordinated by a doctor of medicine or osteopathymedicine or osteopathyThe medical staff determines the circumstances under which consultation orcircumstances under which consultation or management by a physician or other licensed independent practitioner is requiredindependent practitioner is requiredDeemed status hospitals‐ a physician is on call
d ll ior on duty at all times2013 OMSS Annual Assembly 38

AdmissionAdmission
l f h ll b d d l h d d California‐ Patients shall be admitted only upon the order and under the care of a member of the medical staff of the hospital who is a licensed health care practitioner acting p p gwithin the scope of his or her professional licensure. (22 CCR 70717)
M di P ti t d itt d t th h it l l th Medicare‐ Patients are admitted to the hospital only on the recommendation of a licensed practitioner permitted by the State to admit patients to a hospital. If a Medicare patient is admitted by a practitioner not specified above, that patient is under the care of a doctor of medicine or osteopathy. (42 CFR482.12)482.12)
2013 OMSS Annual Assembly 39

Fair Hearing Rights for Non‐PhysiciansFair Hearing Rights for Non Physicians
Generally entitled to fair procedure rights but not the same as medical staff membersException – Marriage and family therapist
Clinical social worker
Joint Commission requires a fair hearing and appeals process for adverse decisions, though pp p , gprocess may differ for non‐members. MS.10.01.01
2013 OMSS Annual Assembly 40

Non‐Physicians Hearing Rights OptionsNon Physicians Hearing Rights Options
1. Same as medical staff member2 Applicants only have an abbreviated2. Applicants only have an abbreviated
process3. Abbreviated for all (CMA?)
2013 OMSS Annual Assembly 41

Steps to TakeSteps to Take
1 Act in the best interests of quality1. Act in the best interests of quality patient care
2 Diligently perform professional2. Diligently perform professional responsibilities
S lf Self‐governance Supervision
3. Align with hospital if possible4. Seek legal counselg
2013 OMSS Annual Assembly 42

The California Medical Association’s 2013 Legislative Wrap-Up
Year of challenges, victories
his year turned out to be a challenging year for the California Medical Association (CMA). We knew going into the legislative session that 2013 would be a historic year, with the implementation of the Affordable Care Act (ACA) and the wave
of legislative freshman. It lived up to our expectations. With the beginning of each session, there are new legislators that come to Sacramento from all walks of life. CMA’s government relations team is challenged with getting to know them, educating them on issues of importance to the physician community and identifying the physicians with whom they have—or should have—relationships. While the Legislature has had up to one third of its members turn over in any given year, this year a majority of legislators were new to Sacramento. The challenging task of educating the new
class was magnified. In addition, 2013 included 12 special elections that resulted from various vacancies created by departures and resignations. CMA faced an unprecedented number of scope of practice expansion bills introduced in the Legislature. These scope bills were painted by supporters as necessary reforms to help implement the ACA. Those who wanted to expand scope had a key message: we need allied health professionals, including nurse practitioners, optometrists and pharmacists, to do more in order to prepare for the many Californians added to California’s health care system through the ACA implementation. Our message was simple: we will not jeopardize patient safety and we need to promote integration of allied health professionals, not fragment them as these proposals suggested.
By Juan Carlos Torres, CMA Vice President of Government Relations

We faced a concerted effort by the nurse practitioners, optometrists and pharmacists who joined together to push their agenda collectively. They put in significant resources to mount a public relations campaign and were actively pursuing newspaper editorial boards across the state to promote their agenda. With the help of our specialty partners and our local medical societies, CMA won the argument in the Capitol. We successfully defeated the attempt by nurse practitioners to gain independent practice in California, as well as efforts by optometrists seeking to diagnose and treat diseases in patients. CMA significantly narrowed the pharmacists’ proposal to ensure that they could provide reasonable services in an integrated and safe manner that promoted collaboration with physicians. CMA also tackled the incorrect perception that physicians are at the center of the opioids overdose crisis occurring in California. Physicians recognize the need to help ensure appropriate prescribing and the need to tackle abuse and diversion of prescription drugs. We helped craft a proposal that will ensure that our state’s prescription monitoring program, CURES, will be upgraded and funded. CMA also secured a streamlined application process for CURES, a requirement that a stakeholders group be consulted as the upgrade and maintenance occurs, and a reduced fee impact on physicians. Most importantly, there will be no mandated participation required of physicians. A proposal that would have given the medical board overly broad power to discipline physicians for inappropriate prescribing was soundly defeated by CMA in an overwhelming fashion on the Assembly floor. CMA was also able to garner amendments to a bill that would have required coroners to report overdose deaths due to controlled substances to the medical board, to ensure that any reports submitted by coroners would remain confidential. (This bill, SB 62, was ultimately vetoed.) In addition, an effort to shift the investigative authority from the Medical Board of California to the Department of Justice was defeated. The trial attorneys’ campaign to eviscerate the Medical Injury Compensation Reform Act (MICRA) was also in full gear this year. Trial attorneys invested heavily in three additional lobbyists and launched a public relations campaign titled “38 Is too Late,” and made several attempts to push a bill through the Legislature. All these efforts resulted in no action in the Capitol, not even the introduction of a bill, a major victory for CMA. While CMA is proud of our legislative victories this year, we understand that these battles will continue next year. Trial attorneys are initiating a ballot fight, allied
health professionals will continue to call for inappropriate scope expansion and legislators will continue to focus on prescription drug abuses. CMA will continue to be the voice of the physician community and is prepared to take on these challenges. Many of our fights garnered significant media attention. The Sacramento Bee outlined the five major battles facing the Legislature in the closing month of session. Of the five battles, CMA was front and center on two—each of which CMA won!
Moving the Physician Agenda Forward
CMA didn’t just play defense. CMA made significant progress in moving our proactive agenda forward this year. After several failed attempts in years prior, CMA partnered with local legislators to successfully secure an annual $15 million appropriation to fully fund the University of California, Riverside School of Medicine, which will be the first new four-year medical school established in California in over 40 years. The effort began this year with two CMA-sponsored bills introduced by newly elected Inland Empire legislators (SB 21 and AB 27), but eventually the conversation shifted to the budget process. Following the approval of the funding in the 2013-2014 state budget, the school welcomed its first class of four-year medical students this fall. The budget also included $3.9 million to upgrade the CURES database, $1.6 million of which was from the Medical Board of California contingent fund (licensing fees). The other professional licensing boards contributed the remainder. The funds are one time in nature and are exclusively for the upgrade of the database platform. While this funding was taken from medical board reserves, we were able to defeat attempts to have new licensing fees pay for this upgrade. We also advanced our efforts to prioritize the need to increase Medi-Cal provider rates. There were two bills introduced in each house that called for this increase. A new coalition, We Care for California, was formed to advocate for that increase. With CMA playing a key role and under the new We Care for California banner, thousands of health care providers from across the state converged on the state capitol in the largest ever health care rally in Sacramento. The historic event, called “WE ARE MEDI-CAL,” included administrators, physicians and frontline health workers from every region of the state. CMA sponsored legislation addressing the need to

provide incentives to encourage physicians to practice in underserved communities. Addressing workforce issues, not scope expansion of allied professionals, is the long term solution to the physician distribution issues faced in California. Two CMA-sponsored bills (AB 565, AB 1288), both signed by Governor Brown, will encourage physicians to locate their practices in the Central Valley, Inland Empire and other underserved regions of our state. There is no doubt that CMA faced a many battles this year, but thanks to the advocacy of the physician community and our government relations team, we won these battles. Bills that we opposed were either defeated or significantly amended to address our concerns. Our sponsored bills, with the exception of two, advanced to the Governor and have been signed. CMA has again demonstrated the important role it plays in shaping health policy in Sacramento. As always, CMA will be prepared to lead our state forward. Below are details on the major bills that CMA followed this year.
CMA-Sponsored Legislation
SB 21 (Roth): UC Riverside Medical School This bill appropriates $15,000,000 annually from the General Fund to the Regents of the University of California for allocation to the School of Medicine at the University of California, Riverside. According to a 2010 report by the California Health Care Foundation, the Inland Empire has the lowest ratio of primary care physicians and specialists of any region in the state. The Council on Graduate Medical Education, a federally funded and authorized group that assesses the physician workforce and reports to federal policymakers, recommends a minimum of 60 to 80 primary care physicians and 85 to 105 specialists per 100,00 people. Sadly, the physician and specialist ratio in the Inland Empire is barely half of that recommended number. The UC Riverside School of Medicine is a critical factor in addressing this need, and consistent state funding is needed for the school to maintain its accreditation.
Status: Signed by the Governor.
SB 640 (Lara): Medi-Cal: Reimbursement Provider PaymentsThis bill seeks to restore the 10 percent Medi-Cal provider rate reductions contained in the 2011-12 state budget.
CMA has built a coalition of different providers who have been impacted by the cuts or who, like CMA, are still in court over their implementation. This bill would both eliminate the retroactive portion of the cuts as well as stop them going forward. This will help provide needed stability to the Medi-Cal system as the state prepares for full federal health reform implementation on January 1, 2014.
Status: Held in Senate Appropriations Committee.
AB 565 (Salas): California Physician Corps ProgramTen years ago, CMA sponsored legislation to create the Steven M. Thompson Physician Corps Loan Repayment Program (STLRP) to increase access to primary care physicians in medically underserved areas. Although the STLRP has awarded more than $17 million to over 220 individuals, the high demand for this program means less than one third of applicants are awarded funding. Given the limited funds in this program, this bill will tighten the eligibility criteria of applicants to the STLRP and help identify gaps in placing physicians in the Central Valley, the Inland Empire and other underserved communities.
Status: Signed by the Governor.
AB 670 (Atkins): Therapeutic SubstitutionsThis bill would prohibit pharmacists from receiving a financial incentive for recommending a patient receive a drug that is chemically different from the one prescribed by the physician, a practice known as therapeutic substitution. There has been an increase in consulting contracts with pharmacists that carve out a separate fee each time a therapeutic substitution is recommended. Though the medicine may treat the same condition, the chemical ingredients are not the same. This often results in adverse side effects or ineffective treatment. Patients who are on medication to treat epilepsy or mental health conditions are particularly vulnerable. Therapeutic substitutions should be based upon the patient’s best interest, not a financial incentive.
Status: Held in Assembly Appropriations Committee.
AB 1003 (Maienschein): Employment of Physical TherapistsCMA and the physical therapists had introduced competing bills this session, which were ultimately combined into one co-sponsored bill (see AB 1000). CMA’s bill would clarify existing law to explicitly authorize medical corporations to hire persons licensed

under the Business and Professions Code, the Chiropractic Act or the Osteopathic Act. In November 2010, the Physical Therapy Board reversed decades-old policy that allowed physical therapy services to be provided by medical corporations. According to the California Employment Development Department, there are over 15,000 practicing physical therapists in California. Furthermore, California adds about 440 new physical therapy jobs each year. Nearly, 80 percent work in medical corporations, hospitals, home health care services and nursing care facilities. As a result, hundreds of physical therapists across California are at risk of losing their jobs.
Status: Assembly Business and Professions Committee – Hearing Postponed.
AB 1288 (V. M. Perez): Physician Workforce: Medically-Underserved CommunitiesAssembly Bill 1288 will require the Medical Board of California and the Osteopathic Medical Board of California to develop a process to give priority review status to the application of an applicant who can demonstrate that he or she intends to practice in a medically underserved area or serve a medically underserved population. AB 1288 will not change the vigorous standards that govern these professions but will instead focus the board’s resources on the areas and populations with the greatest need.
Status: Signed by the Governor.
CMA Co-Sponsored Legislation
SB 191 (Padilla): Emergency Room FundingCo-sponsored by the California American College of Emergency Physicians, this bill extends the sunset date to January 1, 2017. The bill raises approximately $50 million to augment local county emergency medical services funds in order to allow counties, hospitals and physicians to continue providing emergency services in their communities with these desperately needed funds. Emergency care in California is in crisis. In the past decade, more than 65 emergency departments (EDs) have closed; ED visits are up; wait times continue to increase, and hospital diversion is on the rise. Without this bill, the law is set to expire on January 1, 2014.
Status: Signed by the Governor.
AB 1000 (Wieckowski and Maienschein): Physical Therapists: Direct Access to Services and Medical Corporation Employees CMA and the physical therapists had introduced competing bills this session, which were ultimately combined into one co-sponsored bill (AB 1000). The joint bill clarifies an existing ambiguity in the law so that physical therapists can continue to work within the legal boundaries of medical corporations as they have for decades (as was the intention of CMA’s solo bill). The combined bill also gives health care consumers the ability to seek treatment from a physical therapist without a physicians’ consent for a limited period of time. Although CMA had previously opposed attempts to authorize such “direct access,” we believe that the final language is an acceptable compromise. The bill does not expand or modify the scope of practice for physical therapists, including the existing prohibition on a physical therapists diagnosing disease.
Status: Signed by the Governor.
AB 1176 (Bocanegra): Primary Care Access: Residency ProgramsCo-sponsored by the California Academy of Family Physicians, this bill will follow the example of other states and create a funding source for underfunded medical residency training programs by drawing from private payers such as health insurance companies. According to the Council on Graduate Medical Education, 74 percent of California’s 58 counties have an undersupply of primary care physicians, with primary care physicians making up just 34 percent of California’s physician workforce.
Status: Held in Assembly Appropriations Committee.
AB 1208 (Pan): Insurance Affordability Programs: Application FormThe provisions that impacted physicians were deleted. The bill now deals with demographic data collection. Therefore we are no longer co-sponsoring this bill.
Status: Vetoed by the Governor.
Opposed Legislation
SB 117 (Hueso): Integrative Cancer Treatment This bill would prohibit a physician and surgeon, including an osteopathic physician and surgeon, from recommending, prescribing or providing integrative

cancer treatment, as defined, to cancer patients unless certain requirements are met. The bill would specify that a failure of a physician and surgeon to comply with these requirements constitutes unprofessional conduct and cause for discipline by the individual’s licensing entity. The bill would require the State Department of Public Health to investigate violations of these provisions.
Status: Author pulled bill from Senate Business and Professions Committee.
SB 266 (Lieu): Health Care Coverage: Out-of-Network CoverageThis bill would prohibit a health facility or a provider group from holding itself out as being within a plan network or a provider network unless all of the individual providers providing services at the facility or with the provider group are within their network, or the provider group acknowledges to the patient in writing or verbally that individual providers within the provider group may be outside the patient’s plan network or provider network and the provider group recommends that the patient contact his or her health care service plan or health insurer for information about providers who are within the patient’s plan network or provider network. Those provisions would not apply to emergency services and care.
Status: Held in Senate Appropriations Committee.
SB 312 (Knight): Absences: Confidential Medical Services: Parent or Guardian ConsentThis bill would require the governing board of a school district to notify pupils in grades 9 to 12 and their parents or guardians, that school authorities may excuse a pupil from the school for confidential medical services who is 16 years of age or older without parental or guardian consent.
Status: Failed in Senate Education Committee.
SB 430 (Wright): Pupil Health: Vision Examination: Binocular Function This bill would, before first enrollment in a California school district of a pupil at a California elementary school, and at least every third year thereafter until the pupil has completed the 8th grade, require the pupil’s vision to be examined by an optometrist or ophthalmologist and require the examination to also include a test for binocular function and refraction and eye health evaluations. The binocular function examination does not need to take effect until the pupil has reached the third grade and
would require the parent or guardian of the pupil to provide results of the examination to the school district.
Status: Pulled by author in Assembly Health Committee.
SB 491 (Hernandez): Nurse Practitioners This bill gives nurse practitioners independent practice. Under this bill, nurse practitioners will no longer need to work pursuant to standardized protocols and procedures or any supervising physician and would basically give them a plenary license to practice medicine.
Status: Held in Assembly Appropriations Committee.
SB 492 (Hernandez): Optometric CorporationsThis bill allows optometrist to practice ophthalmology. Specifically, allows optometrists to (1) treat and diagnose any disease, condition or disorder of the visual system, the human eye adjacent and related structures, (2) prescribe and administer drugs including controlled substances, (3) perform surgical procedures with local or topical anesthetic, (4) order laboratory and diagnostic tests, (5) administer immunizations, (6) diagnose and initiate treatment for any condition with ocular manifestations.
Status: Pulled by author in Assembly Business and Professions Committee.
AB 591 (Fox): Hospital Emergency Room: Geriatric Physician This bill would require each general acute care hospital with an emergency department to have, at all times, a geriatric physician serving on an “on-call” basis to that department.
Status: Pulled by author.
AB 975 (Wieckowski): Health Facilities Community Benefits This bill would declare the necessity of establishing uniform standards for reporting the amount of charity care and community benefits a facility provides to ensure that private nonprofit hospitals and nonprofit multispecialty clinics actually meet the social obligations for which they receive favorable tax treatment.
Status: Failed on Assembly Floor.
ACA 5 (Grove): Abortion: parental notificationThis measure, which would be known as the Parental Notification, Child and Teen Safety, Stop Predators Act, would prohibit a physician and surgeon from performing

an abortion on an unemancipated minor, as defined, unless the physician and surgeon or his or her agent has delivered written notice to the parent of the unemancipated minor, or until a waiver of that notice has been received from the parent or issued by a court pursuant to a prescribed process.
Status: Re-referred to Assembly Health and Assembly Judiciary Committees.
Other Bills of Interest
SB 20 (Hernandez): Health Care: Workforce Training (Support)This bill would transfer all available funds left over in the Department of Managed Health Care’s Managed Care Administrative Fines and Penalties Fund to the Steve Thompson Physician Corps Loan Repayment Program, upon dissolution of the Major Risk Medical Insurance Program.
Status: Held in Assembly Appropriations Committee.
SB 62 (Price): Coroners: Reporting Requirements: Prescription Drug Use (Neutral)This bill would expand those provisions to require a coroner to make a report when he or she receives information that indicates a death may be the result of prescription drug use and to require the coroner to additionally file the report with the Medical Board of California.
Status: Vetoed by the Governor.
SB 47 (Yee): Firearms: Assault Weapons (Support)This bill seeks to reestablish the original intent of the assault weapon ban by slowing down the process of easily reloading a firearm. For several years, gun makers have manufactured assault weapon with a magazine locking device called the “bullet button,” which requires a tool, which may include a tip of a bullet, a magnet, or a glove, to disengage the magazine yet allow for the easy reloading. Since a tool is used to disengage the ammunition feeding device, the firearm’s magazine is not classified as “detachable” and the firearm in question is legal.
Status: Held in Assembly Appropriations Committee.
SB 138 (Hernandez): Confidentiality of Medical Information (Watch)The bill would define additional terms in connection with maintaining the confidentiality of this information, including an “authorization for insurance communications,”
which an insured individual may submit for the purpose of specifying disclosable medical information and insurance transactions and permissible recipients.
Status: Signed by the Governor.
SB 304 (Lieu): Healing Arts: Boards (Neutral)The bill is the sunset extension bill for the Medical Board of California. Significant issues raised by CMA (expert witness, 820 evaluations) were addressed in CMA’s favor. While the proposed transfer to the Department of Justice was rejected, the bill does transfer investigations to the Division of Investigators at the Department of Consumer Affairs.
Status: Signed by the Governor.
SB 352 (Pavley): Medical Assistants:
Supervision (Support)This bill would prohibit a nurse practitioners, certified nurse-midwife or physician assistant from authorizing a medical assistant to perform any clinical laboratory test or examination for which the medical assistant is not authorized.
Status: Signed by the Governor
SB 439 (Steinberg): Medical Marijuana (Watch)This bill codifies the Attorney General’s “Guidelines for the Security and Non-Diversion of Marijuana Grown for Medical Use” and specifies that medical cannabis dispensaries that adhere to the guidelines will not be subject to prosecution for marijuana possession or commerce.
Status: Pulled by author in Assembly Health Committee.
SB 493 (Hernandez): Pharmacy Practice (Neutral)This bill, as introduced, would have expanded the scope of practice for pharmacists to include administering drugs and biological products that have been ordered by a prescriber and expanded other functions pharmacists are authorized to perform. These functions include, among other things, the furnishing of specified drugs including prescription smoking-cessation drugs; ordering and interpreting tests for the purpose of monitoring and managing the efficacy and toxicity of drug therapies; and to independently initiate and administer routine vaccinations. The introduced version of the bill also specified additional functions that may be performed by an advanced practice pharmacist, including performing

physical assessments and certain other functions. The author has accepted numerous amendments offered by CMA, which have the potential to improve access to vaccines for children and access to nicotine based smoking cessation products for adults seeking to end their addiction to tobacco products. The bill requires that all prescriptions be administered under a protocol with a physician. This will help improve the communication and coordination between the patient, their physician and their pharmacists.
Status: Signed by the Governor.
SB 494 (Monning): Health Care Providers: California Health Benefit Exchange (Support)This bill is sponsored by the Physician Assistants and seeks to amend statue to include physician assistants as primary care providers and to increase the number of enrollees assigned to physician assistants in Medi-Cal managed care plans. The bill maintains that physician assistants must operate under the supervision of a physician.
Status: Signed by the Governor.
SB 495 (Yee): Postsecondary Education Employees: Physicians (Support)This bill would require the California State University (CSU) to increase the compensation of physicians employed at student health centers on campuses to be is comparable to the compensation earned at the University of California (UC). The bill would request the UC to increase the compensation of physicians employed at student health centers on campuses of the UC if the compensation of physicians employed at a student health center on a different campus of the UC is increased.
Status: Held at the Assembly Desk.
SB 598 (Hill): Biosimilars (Support)This bill would allow a pharmacist to substitute an interchangeable biosimilar medication when filling a prescription for a biologic medication. SB 598 mirrors California’s patient protections for generic pill substitution and adds a provision that requires a pharmacist to enter information about the substitution into the patient record system or notify the physician within five days after a substitution is made.
Status: Vetoed by the Governor.
SB 615 (Galgiani): Prevailing Wages: California Health Facilities Financing Authority Act (Neutral)
While the bill was moved out of the Assembly Appropriations Committee, the provisions of interest to CMA were removed. As a result, we are no longer co-sponsoring this legislation.
Status: Vetoed by the Governor.
SB 670 (Steinberg): Physicians and Surgeons: Drug Prescribing Privileges: Investigation (Support, after significant amendments)CMA was able to secure amendments that deleted the provisions that would have expanded the Medical Board of California’s authority to limit a physician’s prescribing authority with a lower standard of evidence. With the deletion of these provisions, the bill simply made clarifying improvements to the medical board authority.
Status: Signed by the Governor.
SB 809 (Desaulnier): Controlled Substances: Reporting (Support)This bill would provide ongoing funding for the CURES database by requiring the Medical Board of California and other health professionals’ licensing boards to charge licensees who are authorized to prescribe or dispense controlled substances a fee of $6 annually. The bill also makes changes to the CURES authorizing statute to clarify that the database is a clinical tool and to simplify prescribers’ and dispensers’ enrollment into the database.
Status: Signed by the Governor.
SBX1 1 (Hernandez): Medi-Cal: Eligibility (Support)This bill implements the expansion of federal Medicaid coverage in California (Medicaid is known as Medi-Cal in California) to low-income adults with incomes between 0 and 138 percent of the federal poverty level, establishes the Medi-Cal benefit package for this expansion population, and requires the existing Medi-Cal program to cover the essential health benefits contained in the Patient Protection and Affordable Care Act (ACA). This bill implements a number of the Medicaid ACA provisions to simplify the eligibility, enrollment and renewal processes for Medi-Cal.
Status: Signed by the Governor.
SBX1 2 (Hernandez): Health Care Coverage (Support if Amended)This bill applies the individual insurance market reforms of the Affordable Care Act to health care service plans

(health plans) regulated by the Department of Managed Health Care and updates the small group market laws for health plans to be consistent with final federal regulations.
Status: Signed by the Governor.
SBX1 3 (Hernandez): Health Care Coverage: Bridge Plan (Watch)Requires Covered California (the state’s health benefit exchange) to establish a “bridge” plan product by contracting with Medi-Cal managed care plans for individuals losing Medi-Cal coverage (for example, because of an increase in income), the parents of Medi-Cal or Healthy Families Program children, and individuals with incomes below 200 percent of the federal poverty level. Limits enrollment in bridge plan products only to eligible individuals.
Status: Signed by the Governor.
AB 154 (Atkins): Abortion (Support)This bill would make it a public offense, for a person to perform an abortion if the person does not have a valid license to practice as a physician and surgeon, except that it would not be a public offense for a person to perform an abortion by medication or aspiration techniques in the first trimester of pregnancy if he or she holds a license or certificate authorizing him or her to perform the functions necessary for an abortion by medication or aspiration techniques. With the provisions for training in the bill and the amendments that clarify physician supervision, AB 154 addresses patient safety while expanding access for these services.
Status: Signed by the Governor.
AB 209 (Pan): Medi-Cal: Managed Care: Quality and Accessibility (Support)This bill creates the Medi-Cal Managed Care Health Care Quality and Transparency Act of 2013. The goal of the measure is to require the Department of Health Care Services to develop and implement a plan to monitor, evaluate and improve the quality and accessibility of health care and dental services provided through Medi-Cal managed care. This is meant to emulate the open government approach of the Managed Risk Medical Insurance Board/MRMIB’s operation of the Healthy Families program, which was eliminated in 2012 and all enrolled children were moved into Medi-Cal.
Status: Ordered to inactive file at the request of the author.
AB 361 (Mitchell): Medi-Cal: Health Homes for Medi-Cal Enrollees and Section 1115 Waiver Demonstration Populations with Chronic and Complex Conditions (Support If Amended)Current federal law authorizes a state, subject to federal approval of a state plan amendment, to offer health home services to eligible individuals with chronic conditions. This bill would authorize the Department of Health Care Services, to create a health home program for enrollees with chronic conditions as authorized under federal law.
Status: Signed by the Governor.
AB 446 (Mitchell): HIV Testing (Support)After amendments taken in Senate Health Committee, this bill eliminates the requirement for written documentation of informed consent prior to administering an HIV test in non-clinical settings. Additionally, the bill requires timely delivery of the test results along with other pertinent information, tailored to whether the results are positive or negative, by the medical care provider or the person who administers the test to the patient. The bill no longer requires that every blood draw in emergency departments, public health clinics, or urgent care centers be tested for HIV. Instead, the bill now only requires primary care clinics to offer patients having a blood draw an HIV test. Lastly, the bill allows for the online posting of HIV antibody test results if the results are posted on a secure internet website, which can be accessed only with the use of personal identification number provided the patient at the time of testing.
Status: Signed by the Governor.
AB 459 (Mitchell): Public Contracts: Healthy and Sustainable Food (Support)This bill would clarify and strengthen the state’s existing nutrition guidelines for food and beverages sold in vending machines on state properties. It would also increase incrementally the percentage of foods sold in vending machines that meet the nutrition guidelines from the current 35 percent to 100 percent by January 1, 2017.
Status: Held in Assembly Appropriations Committee.
AB 860 (Perea): Medical School Scholarships (Support)This bill, upon appropriation by the Legislature, would transfer $600,000 in penalty monies levied by the Department of Managed Health Care to fund the Steven M. Thompson Scholarship Program. CMA sponsored AB 589 (Perea) in 2011, which created the scholarship

program, but due to state budget constraints, the bill only allowed for private donations to fund the program.
Status: Held in Assembly Appropriations Committee.
AB 880 (Gomez): Medi-Cal Program Costs (Support)This bill would require large employers of 500 or more employees to pay an “employer responsibility penalty” for each covered employee enrolled in Medi-Cal. The funding generated by the penalty could be appropriated by the Legislature for a variety of different purposes: to increase Medi-Cal provider rates, to provide a supplemental Medi-Cal payment for providers in medically underserved areas, to fund residency programs, to provide payment for the nonfederal share of Medi-Cal, to increase provider reimbursement rates, and to provide reimbursement to county hospitals, community clinics, and other safety net providers. Although the ACA requires employers pay a penalty for employees enrolled in state exchanges (a penalty based on the employers entire workforce, not just the number of individuals enrolled in the exchange), there is no such provision for employers who reduce their employees hours or wages to make them Medi-Cal eligible. Given the current beleaguered state of the Medi-Cal system, coupled with the strains that are expected as a result of the Medi-Cal expansion in 2014, the system will not be able to handle the influx of new lives resulting from large employers cutting employee wages. AB 880 incorporates portions of another CMA-sponsored bill, AB 1176 (Bocanegra), which was held in the Assembly Appropriations Committee earlier this year.
Status: Assembly Inactive File – vote failed.
AB 1139 (Lowenthal): Prescriptions: Biosimilar Products (Watch)This bill would authorize a pharmacist filling a prescription order for a biological product subject to the Federal Food, Drug, and Cosmetic Act to select a biosimilar product, provided that product is deemed by the federal Food and Drug Administration to be interchangeable with the prescribed product.
Status: Assembly Business and Professions Committee hearing postponed.
AB 1263 (Pérez): Medi-Cal: CommuniCAL (Watch)This bill would require the Department of Health Care Services, to establish the Medi-Cal Patient-Centered Communication program (CommuniCal), to be administered by a 3rd-party administrator, to, commencing
July 1, 2014, provide and reimburse for medical interpretation services to Medi-Cal beneficiaries who are limited English proficient.
Status: Vetoed by the Governor.
AB 1308 (Bonilla): Midwifery (Watch)This bill would require the Medical Board of California to, by July 1, 2015, revise and adopt regulations defining the appropriate standard of care and level of supervision required for the practice of midwifery and indentifying complications necessitating referral to a physician.
Status: Signed by the Governor.
ABX1 1 (Pérez): Medi-Cal: Eligibility (Support)This bill enacts statutory changes necessary to implement the coverage expansion, eligibility, simplified enrollment and retention provisions of the Patient Protection and Affordable Care Act of 2010 as amended by the Health Care and Education Reconciliation Act of 2010 related to the Medicaid Program (Medi-Cal in California) and the California Children’s Health Insurance Program.
Status: Signed by the Governor.
ABX1 2 (Pan): Health Care Coverage (Support if Amended)Reforms California’s individual market in accordance with the Affordable Care Act and applies its provisions to insurers regulated by the California Department of Insurance in the individual market; requires guaranteed issue of individual market health insurance policies; prohibits the use of preexisting condition exclusions; establishes open and special enrollment periods consistent with the California health benefit exchange (Covered California); prohibits conditioning issuance or offering based on specified rating factors; prohibits specified marketing and solicitation practices consistent with small group requirements; requires guaranteed renewability of plans; and permits rating factors based on age, geographic region and family size only.
Status: Signed by the Governor.

• The Medical Injury Compensation Reform Act (MICRA) is California’s medical liability reform law.
• MICRA ensures that injured patients receive fair and full compensation while keeping liability rates from further increasing the cost of health care and limiting a patient’s increasing the cost of health care and limiting a patient s access to care.

MICRA TimelineMICRA Timeline
• Originally passed in 1975Originally passed in 1975.
• Litigated for ten years before taking effect (1985).g y g ( )
• Changed in the famous ‘Napkin Deal’ by the Trial i i ( )Lawyers to increase their percentage take (1988).
• Trial Lawyers unsuccessfully attempted to increase • Trial Lawyers unsuccessfully attempted to increase payouts in 1998, 2000, 2012, 2013.

MICRA ProvidesMICRA Provides• UNLIMITED economic damages for any and all past and g y p
future medical costs.
• UNLIMITED economic damages for lost wages and lifetime g gearning potential.
• UNLIMITED punitive damages for malicious or willful conduct.
• ADDITIONAL DAMAGES up to $250,000 for non-economic ddamages.

MICRA Applies ToMICRA Applies To• Any action for injury against a health care Any action for injury against a health care
provider based on professional negligence
i i i i• Health Care Provider = physician, med student intern, osteopath, dentist, nurse, licensed therapist, psychologist, pharmacist, chiropractor, emergency medical technician, clinic, health facility, health dispensary.health dispensary.
• Professional Negligence = a negligent act or omission to act by a health care provider in the rendering of professional services, which act or omission is the proximate cause of a personal injury or wrongful death, provided that such services are within the scope of services for which the provider is licensed and which are not within any restriction imposed by the licensing agency or licensed hospital.
• Based On = does not include intentional torts eg fraud battery• Based On = does not include intentional torts, eg., fraud, battery

Seven Original Statutory Provisions of MICRA + Punitive Damages+ Punitive Damages
• Limits on Non-Economic Damages: Non-economic damages in a claim against a healthcare provider for medical negligence are limited to $250,000. Economic damages, such as lost earnings, medical care, and rehabilitation costs, are not limited by statute. California Civil Code Section 3333.2.
• Limits on Attorney Contingency Fees: In an action against a health care provider for professional negligence, an attorney’s contingency fee is limited to 40% of the first $50,000 recovered; 33.3% of the next $50,000; 25% of the next $500,000, and 15% of any amount exceeding $600,000. California Business and Professions Code Section 6146.
• Evidence of Collateral Source Payments: Evidence of collateral source payments (such as from personal health insurance) can be considered as they relate to damages. This section helps a jury prevent a double recovery. Civil Code Section 3333.1. y g p j y p y
• Advance Notice of a Claim: To further the public policy of resolving meritorious claims outside of the court system, MICRA requires a claimant to give a 90-day notice of an intention to bring a suit for alleged professional negligence. If the notice is given within 90 days of the expiration of the statute of limitations, the statute is extended 90 days from the date of the notice. California Code of Civil Procedure Sections 364 and 365.
• Statute of Limitations: In California, a claim for alleged medical negligence must be brought within one year from the discovery of an injury and itsnegligent cause, or within three years from injury. Code of Civil Procedure Section 340.5. Minors – within three years of alleged negligent act or by eighth birthday.
• Periodic Payments of Future Damages: A healthcare professional may elect to pay future economic damages, if over $50,000, in periodic amounts to ensure a steady stream of income for the claimant’s current and future needs. Code of Civil Procedure Section 667.7.
• Binding Arbitration of Disputes: Patients and their health care providers may agree that any future dispute may be resolved through binding arbitration. California statute requires specific language for such contracts and also provides that all such contracts be revocable within 30 days. Code of Civil Procedure Section 1295.
• Punitive Damages: Injured patients may claim punitive damages in action against a health care provider upon showing substantial probability of success in establishing that health care provider has committed oppression, fraud or malice. Punitive damages are awarded for the sake of example and by way of punishing the defendant.

MICRA Is ConstitutionalMICRA Is Constitutional• Fein v Permanente Medical Group (1985) 38 Cal.3d 137: California Supreme Court upheld constitutionality of MICRA’s
cap on non-economic damages against due process and equal protection challenges
• Hoffman v US (9th Cir. 1985) 767 F.2d 1431: §3333.2 is consistent with federal Equal Protection Clause
• Yates v Pollock (1987) 194 Cal.App.3d 195: §3333.2 does not violate constitutional right to jury trial
• Hooper v Capobianco (2004 WL 1167395) unpublished: rational basis supports MICRA’s non-economic damage cap not being indexed to inflation; issue for Legislature
V B E (2009 39623 ) bli h d 3333 2 d i l i i l i h j i l i • Van Buren v Evans (2009 WL 1396235) unpublished: §3333.2 does not violate constitutional right to jury trial or separation of powers doctrine; rejected inflation argument
• Stinnett v Tam (2011) 198 Cal.App.4th 1412, rehearing denied 2011, review denied 2011: published opinion: CA 5th
Appellate District Court upheld constitutionality of MICRA’s non-economic damages cap. Court rejected argument that §3333.2 violates Equal Protection b/c insurance crisis & thus rational basis no longer exists; Plaintiff pointed to insurance
fi ’ i i f i j i i iff fcompany profits, Prop 103, DOI’s rate regulation & inflation; Court also rejected argument that §3333.2 deprives plaintiff of Right to Jury Trial
• Hughes v Pham (pending in CA 4th Appellate District Court): Plaintiffs are asserting that MICRA's cap on non-economic damages violates Equal Protection clause of Constitution, their right to jury trial and separation of powers doctrine by impinging on authority of courts to decide cases and enter judgments
• Gavello v Millman (July 9, 2013 WL 3455506) – unpublished: CA 1st Appellate District Court upheld constitutionality of MICRA’s non-economic damages cap and rejected arguments that cap violates Equal Protection and Right to Jury Trial
• Rashidi v Moser (September 23, 2013 WL 5308276) published opinion: CA 4th Appellate District Court upheld constitutionality of MICRA’s non-economic damages cap, rejecting argument that it violates Equal Protection, right to jury y g p, j g g q , g j ytrial and separation of powers doctrine

Th C t Th tThe Current Threat• MICRA is being threatened by the
Consumer Attorneys of California and Consumer Attorneys of California and their front group – Consumer Watchdog.
• Trial attorneys have hired new guns “(including Chris Lehane, “Master of the
Dark Arts” in the Clinton White House) to move the legislature and public on why they believe MICRA needs to be changed.
• Recognizing the high level of support for MICRA and the high opinion of physicians MICRA and the high opinion of physicians held by elected officials and members of the public, the trial attorneys have begun attacking our profession directly to erode this strong support this strong support.
Quotes from Brian Kabateck(President, Consumer Attorneys of California)
• “We are launching this campaign to We are launching this campaign to change the MICRA law as part of a larger campaign about medical safety and about protecting patients in California from doctors…”
• “We must require mandatory drug testing of ll d t ith i il t h it l ”all doctors with privileges at hospitals.”

Other Quotes from the Initiative ProponentsQ p
“This is really all about patients and their allies declaring war on the lack gof accountability for physicians and hospitals in this state”
Jamie Court, President Consumer Watchdog
But the TRUTH Comes Out
“When recoveries are reduced, cases may no longer be profitable from the lawyer’s perspective, and a victim’s ability to retain competent
counsel will be dramatically diminished ”counsel will be dramatically diminished.
Nora Freeman Engstrom, Associate Professor Stanford Law School
MICRA opponents are now mailing toe t t i t d ttags to registered voters.

Trial Lawyer’s Initiative Trial Lawyer s Initiative • Changes the MICRA provision relating to non-g p g
economic damages to say:– On January 1, 2015, the cap on damages shall be adjusted to
fl t th i i i fl ti b d th C P i reflect the increase in inflation based on the Consumer Price Index (CPI) SINCE THE CAP WAS ESTABLISHED.
• NOTE: this will raise the cap to approximately $1.16 Million and i tt ’ f f b $171 000 increase attorney’s fees for same case by $171,000 (from $74,000 to $245,00 just on the non-economic damages).
– The cap will be adjusted annually based on the CPI going forward.
– New pay structure will apply to any suit not resolved as of January 1, 2015.y

Awards Under MICRA Have f iVastly Out-Paced Inflation
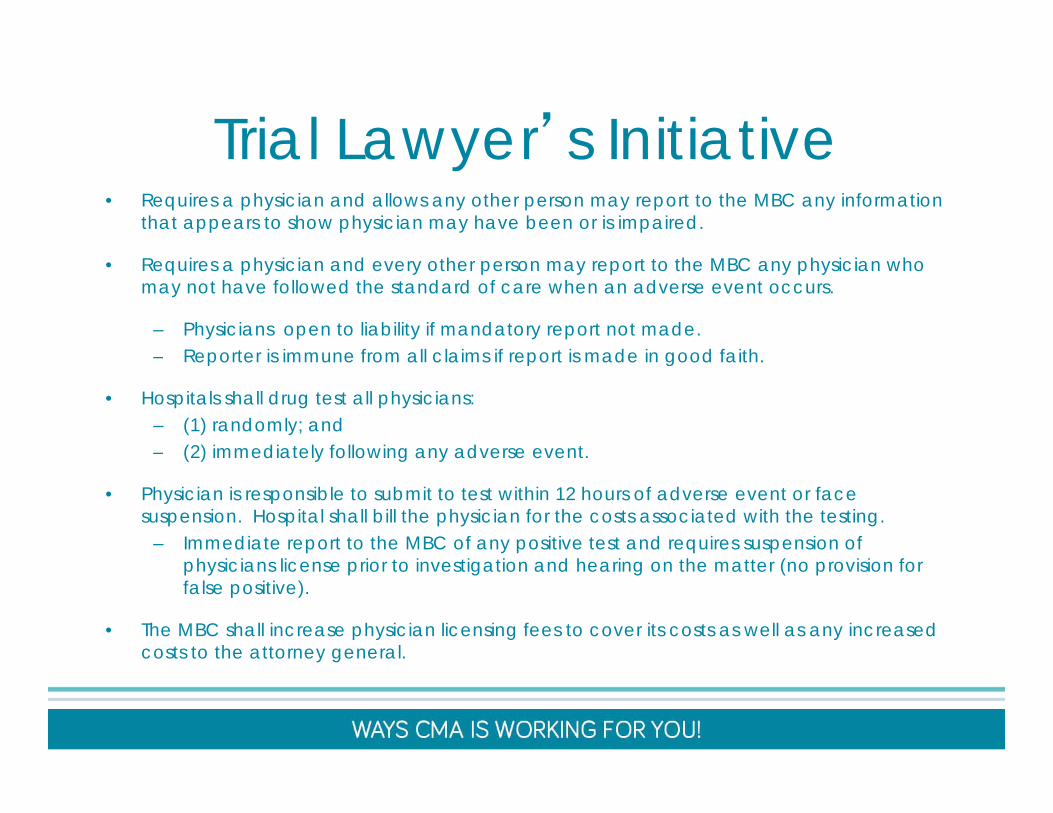
Trial Lawyer’s Initiative Trial Lawyer s Initiative • Requires a physician and allows any other person may report to the MBC any information
that appears to show physician may have been or is impaired.
• Requires a physician and every other person may report to the MBC any physician who may not have followed the standard of care when an adverse event occurs.
– Physicians open to liability if mandatory report not made.Reporter is immune from all claims if report is made in good faith– Reporter is immune from all claims if report is made in good faith.
• Hospitals shall drug test all physicians: – (1) randomly; and – (2) immediately following any adverse event. ( ) ed a e y o o g a y ad e se e e .
• Physician is responsible to submit to test within 12 hours of adverse event or face suspension. Hospital shall bill the physician for the costs associated with the testing.
– Immediate report to the MBC of any positive test and requires suspension of h i i li i t i ti ti d h i th tt ( i i f physicians license prior to investigation and hearing on the matter (no provision for
false positive).
• The MBC shall increase physician licensing fees to cover its costs as well as any increased costs to the attorney general.

Trial Lawyer’s Initiative Trial Lawyer s Initiative • Prior to prescribing or dispensing a Schedule II or Schedule III
controlled substance for the first time to a patient, the health care practitioner shall consult CURES database.
• If the patient has an existing prescription the practitioner shall not prescribe or dispense unless the practitioner determines there is a “legitimate need”legitimate need .
• The practitioner is presumed professionally negligent for failure to The practitioner is presumed professionally negligent for failure to comply with this section and shall be subject to disciplinary action by the MBC.
• NOTE: An accused physician will have the burden of proving compliance.
What’s the cost if this happens?
A 2010 study by the former director of the Legislature’s chief policy analyst predicted that Legislature s chief policy analyst predicted that
simply doubling the cap would result in $9.5 billion in increased health care costs $
in California.
This initiative will quadruple the cap and increase it every year.
b t th d d ’t t th…but the damage doesn’t stop there.
Patient access decreases as health care providers • Patient access decreases as health care providers are forced to limit services or practice in other states if they cannot afford higher malpractice insurance ratesrates.
• Employers are forced to cut health care benefits or require employees to pay more to make up for higher require employees to pay more to make up for higher health care premiums.
• More uninsured Californians increases overall health • More uninsured Californians increases overall health care costs.
Source: HAMM Report 2010Source: HAMM Report 2010
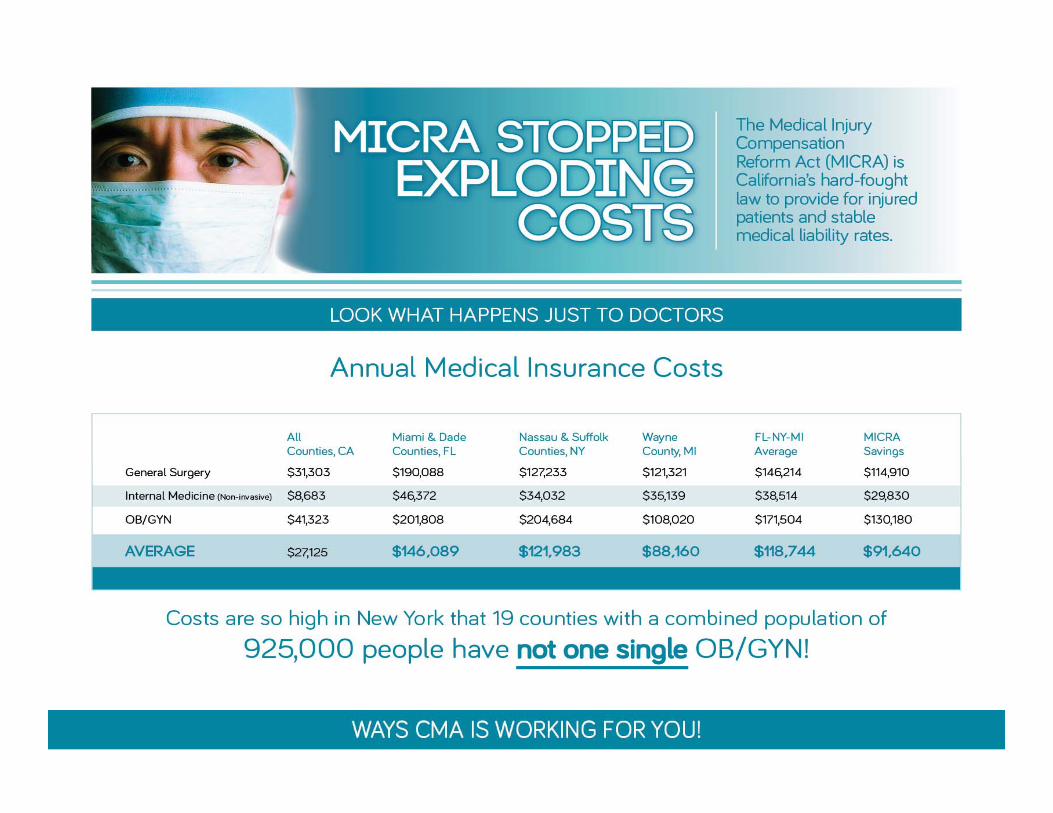

We need your helpWe need your help• By donating to CALPAC, you can help ensure that y g , y p
Pro-MICRA legislators will have the necessary support to stop the Trial Lawyer money grab
through the legislative processthrough the legislative process.
CALPAC – is the primary account utilized by the CMA to elect legislators who hold similar views on the goals and priorities of the medical profession. As any legislative candidate will attest, the first and last goa s a d p o es o e ed ca p o ess o . s a y eg s a e ca d da e a es , e s a d as question of any candidate support interview is what their position on MICRA is. In fact, CALPAC has had such outstanding success in recent years; it is unlikely the Trial Attorneys will make a serious effort to overturn MICRA through the legislature. However, due to term limits, nearly 50% of the legislature will turn-over in just the next two election cycles. CALPAC’s ability to elect MICRA supporting legislators is key to its defense.
As a registered political committee, all contributions to and from the account are publicly disclosed consistent with state law. CALPAC is permitted to contribute to candidates and to other committees that support or oppose candidates. Individual contributions are recommended to go into this account.

Donate and learn more todayDonate and learn more today
• www.calpac.org
• www.cmanet.org/micra

Assessing the Aging Physician:
Neuropsychological and
Psychological Factors Pertaining
to Fitness for Duty
William Perry, Ph.D.
Jessie Park, Psy.D.
University of California, San Diego

Disclosures
The faculty have nothing to disclose
Objectives
After this presentation you should be able to:
• Determine neuropsychological and personality
changes in the aging physician;
• Understand the implication of aging on clinical
performance;
• Understand the difference between a
neuropsychological assessment and a fitness for duty
(FFD) evaluation.
• Recognize the critical information that needs to be
contained in a FFD report.

The aging physician population
Around the world there are growing concerns
about the dependence on aging medical
professionals.
In Canada, the percentage of doctors aged 65 or
above is expected to reach 20% by 2026.
25% of Australia's medical workforce is at least 55
years old.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Aging Physicians in the United States 42% of the nation's 1 million physicians are older than 55 and 21% are
older than 65, according to the American Medical Association.
Up from 35% and 18%, respectively, in 2006.

Conventional wisdom about physician expertise
generally holds that the longer a physician has
been in practice, the better honed his or her
clinical skills become

Marcus Welby M.D. Welby works with Doctor Steven Kiley, a brilliant young
physician. He has more strait-laced methods and often disagrees
with Welby’s way of thinking but usually ends up seeing the
value in what his partner says. The two work alongside one
another at a private practice in Santa Monica, California.

The 10,000-Hour Rule
• The practice of medicine, like many other areas
of human endeavor, requires considerable
“hands on” experience to achieve mastery. Most
physicians, when asked, indicate that they did
not really feel competent for several years after
they entered practice, which tallies with
estimates from other domains that suggest 10
years or 10,000 hours are required to become
expert (Ericsson KA, 2004).

The aging physician population:
Ageism?
• Hobus et al. (1987) presented two groups of
physicians (novice and expert) with short case
histories each presented on three slides: a
portrait of the patient, the patient chart containing
previous disease history, and a slide with the
presenting complaint.
• The correlation between diagnostic accuracy and
experience was 0.68.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

WHAT ARE THE CONCERNS?

What Are The Concerns?
Choudry, Fletcher & Soumerai Ann Intern Med. 2005;142:260-273.
Physicians with more experience are generally
believed to have accumulated knowledge and
skills during years in practice and therefore to
deliver high-quality care. However, evidence
suggests that there is an inverse relationship
between the number of years that a physician has
been in practice and the quality of care that the
physician provides.
Cannot be reproduced without explicit approval from William Perry, Ph.D.
Systematic Review: The Relationship between
Clinical Experience and Quality of Health Care Choudry, Fletcher & Soumerai Ann Intern Med. 2005;142:260-273
Of 62 published studies that measured physician
knowledge or quality of care and described time
since medical school graduation or age, more than
half suggested that physician performance
declined over time for all outcomes measured
(including screening for cancer, depression
adherence to standards of care).
Only 1 study showed improved performance
for all outcomes measured.
Cannot be reproduced without explicit approval from William Perry, Ph.D.
What are the concerns ?
Waljee and colleagues (2006) found that patients
undergoing a complex operation, such as
pancreas removal or heart bypass, are more likely
to die within 30 days of surgery if the surgeon is 60
or older (Ann Surg;244[3]:353-362).
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Norcini, et al. (2000) Certification and
specialization: do they matter in the outcome
of acute MI?
• Studied 4546 physicians
• They found that patient mortality was negatively
associated with treatment by an attending
cardiologist, who cared for larger numbers of
patients, and was closer to his or her year of
graduation from medical school.
• Acute MI mortality increased by 0.5% for every
year since graduation from medical school.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Surgeon characteristics associated with mortality and
morbidity following carotid endarterectomy. O’Neill L,
Lanska DJ, Hartz A Neurology. 2000;55:773–781
• They studied the relationship between years
since licensure of the surgeon (and other
factors) and death, or complications short of
death, for the procedure of carotid
endarterectomy. The study included 12,725
operations in 284 hospitals. Increased years
since surgeon licensure predicted increased rate
of patient death but did not predict nonfatal
complications.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

So the question has to be asked
WHY?
Errors are part of life
• It was reported in the New York Times that a
Kaiser Foundation health plan medical director
said that “three to five percent of the nation’s
then 425,000 practicing physicians, have an
‘impairment’ of some degree from a wide variety
of causes.”
Cannot be reproduced without explicit approval from William Perry, Ph.D.

If errors are part of life why are
we picking on physicians ?
Added Responsibility when working
in high-risk environment with
unforgiving human error
The commercial airline pilot must have:
• a first class medical certificate every 6 months.
• must submit to random breathalyzer and urine
tests for substance abuse.
• must check out in a simulator at least once a
year, and there are additional checkouts
required by the airline carriers.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Pilots versus Physicians
• The commercial airline pilot must submit to
unannounced checkouts by an air carrier
inspector (FAA).
• The medical evaluation of the commercial pilot is
quite extensive and includes 11 pages in the
FAA manual on the neurologic evaluation alone,
checking for seizures, vertigo, cerebrovascular
accidents, demyelinating diseases, multiple
sclerosis, collagen disease, degenerative
diseases, infections.
• Mandatory retirement at age 65
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Aging and the Brain:
Does age impact competence?

Aging and the Brain
• Brain weight and volume decrease. On average,
the brain loses 5-10 percent of its weight
between the ages of 20 and 90
• A decrease in grey matter volume
• Dendritic spines and cortical neurons decrease
in size and number
• Inflammatory proteins occur in maturing adults (including the hippocampus, responsible for forming new memories)
• Age-related changes in dopamine synthesis
Cannot be reproduced without explicit approval from William Perry, Ph.D.

The Question: Does age effect
competence?
Facts of aging;
• Cardiovascular changes (hypertension)
• Renal Changes (strong relationship BMI and Memory)
• Pulmonary Changes
• Urogenital changes
• Decreased visual acuity
• Often decreased hearing
• Decreased physical strength and stamina
Cannot be reproduced without explicit approval from William Perry, Ph.D.

The Question: Does age effect
competence?
Facts of aging on cognition;
• Decreased reaction time
• Decreased fine motor skills/ dexterity
• Difficulty learning new concepts and skills
• Decreased comprehension of complex
information
• Decreased analytic processing
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Understanding the cognition-
performance link in older physicians

Understanding the cognition-
performance link in older physicians
It is well documented that some (but not all) cognitive abilities
decline with age in adults (Craik & Salthouse,1992).
Information- processing speed, for example, slows, and the
capacity to hold information in working memory may also
decline with age (Cerella, 1994).
Healthy older adults’ memory is preserved for well-learned
material, but ability to process novel information declines.
Cannot be reproduced with explicit approval from William Perry, Ph.D.

Crystalized Abilities
Crystalized abilities increase during the lifespan
through education, occupational and cultural
experience and exposure to culture and
intellectual pursuits.
Crystalized abilities are less affected by aging and
disease and often remain intact in the early stages
of dementia or after brain injury.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Fluid Abilities
• Fluid knowledge involves novel problem solving,
spatial manipulation, mental speed, and
identifying complex relations among stimulus
patterns.
• Fluid abilities peak in the mid 20s and decline
gradually until the 60s when a more rapid
decline takes place.
• Fluid abilities are affected by neurological insult,
genetics and biological aging processes.
Cannot be reproduced without explicit approval from William Perry, Ph.D.
The Aging Physician and Changes in Cognitive
Processing and Their Impact on Medical
Practice Eva & Barnes (2002) Acad Med,77:S1-S
• Analytic processing tends to decline with age
whereas nonanalytic processing remains stable.
• Older physicians tend to do less well when
dealing with novel, conflicting, and complex
patient situations.
• The more individuals rely on their prior
experience, the less of a tendency there will be
to critically incorporate novel conflicting
information.
Cannot be reproduced without explicit approval from William Perry, Ph.D.
Prior experience enables practitioners
to make decisions rapidly
• Expert dermatologists, when they are right, are
quick—an average of 8 seconds. When they are
wrong, it takes them about 12 seconds, and
when they are unsure, they will ponder for 28
seconds on average Norman GR, Rosenthal D, Brooks LR, et al. The development of expertise in dermatology. Arch Dermatol
1989;125:1063–8.

The bottom line is:
• Older expert clinicians frequently arrive at a diagnosis by
mentally comparing the presenting situation to a specific
previous case but are also less likely to give due
consideration to competing diagnoses.
• Although the clinician becomes more and more
accomplished at diagnosis based on pattern recognition
processes with increasing experience, which to some
degree may compensate for failure to keep up in formal
knowledge, it may that the benefits of the strategy come at
the cost of reduced flexibility.

Does the advent of robotics
extend the career of a surgeon?
Study: High-School Video Gamers
Match Physicians at Robotic-
Surgery Simulation • Researchers from University of
Texas - at Galveston tasked
OB/GYN residents and 10th
graders who regularly play
video games to perform tasks
on a robotic-surgery
simulation—like suturing. On
average, the high-school
students, who played two
hours of video games a day,
performed just as well as the
residents.

Assessing the competence of the
aging physician

Impairment vs. Cognitive Weakness

Impairment defined
• Physician impairment is defined by the
Federation of State Medical Boards as “the
inability to practice medicine with reasonable
skill and safety because of physical or mental
illness including, but not limited to aging,
alcoholism, drug dependence, and habitual or
excessive alcohol or chemical use or abuse”
(Rassekh, 1996, p. 213)
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Cognitive Weakness ≠ Impairment
• Cognitive strengths refer to the underlying brain
skills needed for a particular task. These are the
skills that allow us to process the huge influx of
information.
• Imagine trying to run the latest software on an
outdated computer? Or asking a computer with a
small processor or insufficient memory to handle
several complex tasks at once?
• Underlying systems aren't up to speed.
Cannot be reproduced without explicit approval from William Perry, Ph.D.
WEAKNESSES ARE INDEPENDENT
OF AGE AND EDUCATION
In Neuropsychology we
traditionally interpret findings
from an age and education
normative perspective
Cannot be reproduced without explicit approval from William Perry, Ph.D.
Cognitive Weakness ≠ Impairment: The question is not simply impairment or is he/she better than others at
age 70. When it comes to patient health the question is are we providing
optimal care ?
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Do cognitive weaknesses translate to
practice problems ?
A retrospective review of the
neuropsychological test performance of
physicians referred for medical infractions.
Perry W, Crean RD.
Source
Department of Psychiatry, University of California, San Diego, 9500 Gilman Drive, La Jolla, CA
92093-8218, USA. [email protected]
Abstract
Physician-related errors are rising, resulting in an increase in disciplinary actions by licensing
medical authorities. It has been previously reported that cognitive impairment may be
responsible for 63% of all physician-related medical adverse events. In this paper we examine
neuropsychological testing results from 148 physicians referred for assessment by the California
Medical Board (CMB) for various infractions. The neuropsychological test performance of the
physicians was compared to normative reference samples. Overall, they performed in the average
range on most measures; however, they demonstrated relative deficits on tests of sequential
processing, attention, logical analysis, eye-hand coordination, verbal and non-verbal learning.
These findings reveal that this cohort of physicians is performing lower than expected on tests of
intellectual and neuropsychological functioning. Applying a neuropsychological framework to
the assessment of physicians may uncover potential cognitive factors that contribute to medical
practice errors.
Cannot be reproduced without explicit approval from William Perry, Ph.D.
Arch Clin Neuropsychol. 2005 Mar;20(2):161-70
Psychomotor testing predicts rate of skill acquisition for proficiency-based
laparoscopic skills training. Stefanidis D, Korndorffer JR Jr, Black FW, Dunne JB, Sierra R, Touchard CL, Rice DA, Markert RJ, Kastl PR, Scott DJ.
Surgery. 2006 Aug;140(2):252-62
The Relationship between Tests of Neurocognition and Performance on a
Laparoscopic Simulator. Kuzbari O, Crystal H, Bral P, Atiah RA, Kuzbari I, Khachani A, Aslam MF, Minkoff H.
Minim Invasive Surg. 2010;2010:486174.
Visuo-spatial ability in colonoscopy simulator training. Luursema JM, Buzink SN, Verwey WB, Jakimowicz JJ.
Adv Health Sci Educ Theory Pract. 2010 Dec;15(5):685-94.
Laparoscopic performance is related to
Neuropsychological test performance.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

How to detect weaknesses in a
population of “healthy functioning”
individuals

Screening tools: why not screen everyone?
• A screening test is used to look for a disease
when a person doesn't have symptoms. (When a
person has symptoms, diagnostic tests are used
to find out the cause of the symptoms).
• For example, Colorectal Cancer risk.
Current Age 10 Years 20 Years 30 Years
30 0.07 0.32 0.98
40 0.25 0.92 2.10
50 0.69 1.91 3.54
60 1.32 3.08 4.39
70 2.08 3.63 N/A
The table shows the percentage of men who will develop Colorectal Cancer
over 10-, 20, and 30 years.

MicroCog: Assessment of Cognitive
Functioning Powell, D. H., Kaplan, E. F., Whitla, D., Catlin, R., and Funkenstein, H. H. (1993).
Developed by the The Risk Management
Foundation of the Harvard Medical Institutions.
Their original purpose was to produce an
instrument that could screen elderly physicians for
cognitive impairment and thereby reduce their
malpractice liability.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

MicroCog: Brief Description
• Computer-administered and scored test of cognitive
functions.
• Intended as a screening device for cognitive impairment
or diagnostic tool for use as part of a general
neuropsychological examination.
• Designed to be sensitive to detecting cognitive
impairment across a wide age range.
• Takes into account levels of premorbid intellectual
functioning by providing age- and education-level
adjusted norms.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

MicroCog Validity from Powell D. Profiles in Cognitive
Aging. Cambridge, MA (1994)
Cannot be reproduced without explicit approval from William Perry, Ph.D.

MicroCog scores of working and retired
MDs
Cannot be reproduced without explicit approval from William Perry, Ph.D.
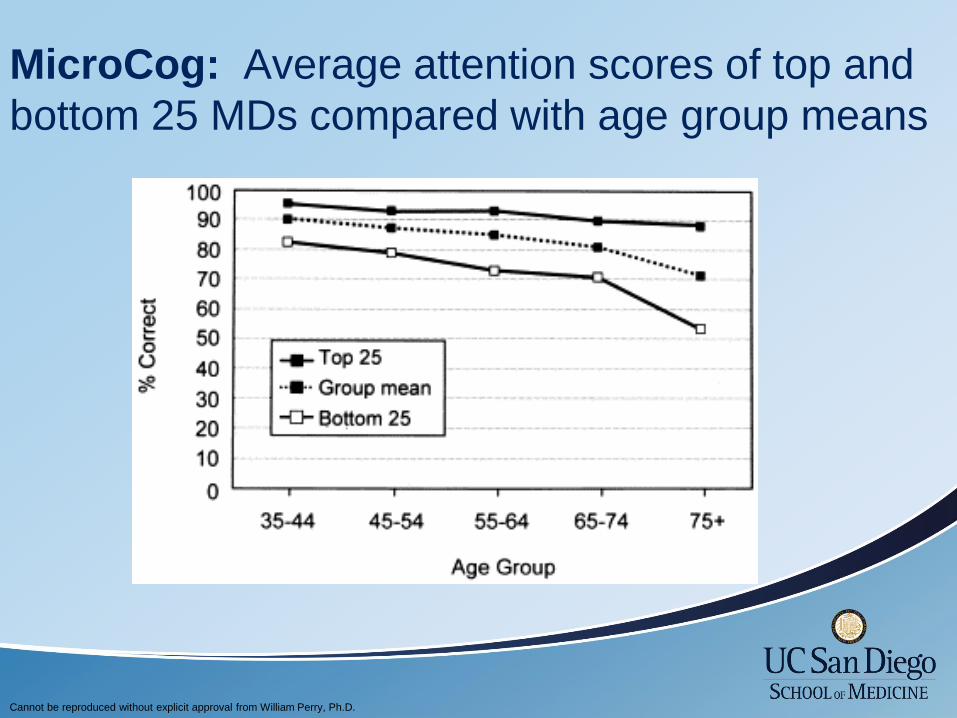
MicroCog: Average attention scores of top and
bottom 25 MDs compared with age group means
Cannot be reproduced without explicit approval from William Perry, Ph.D.
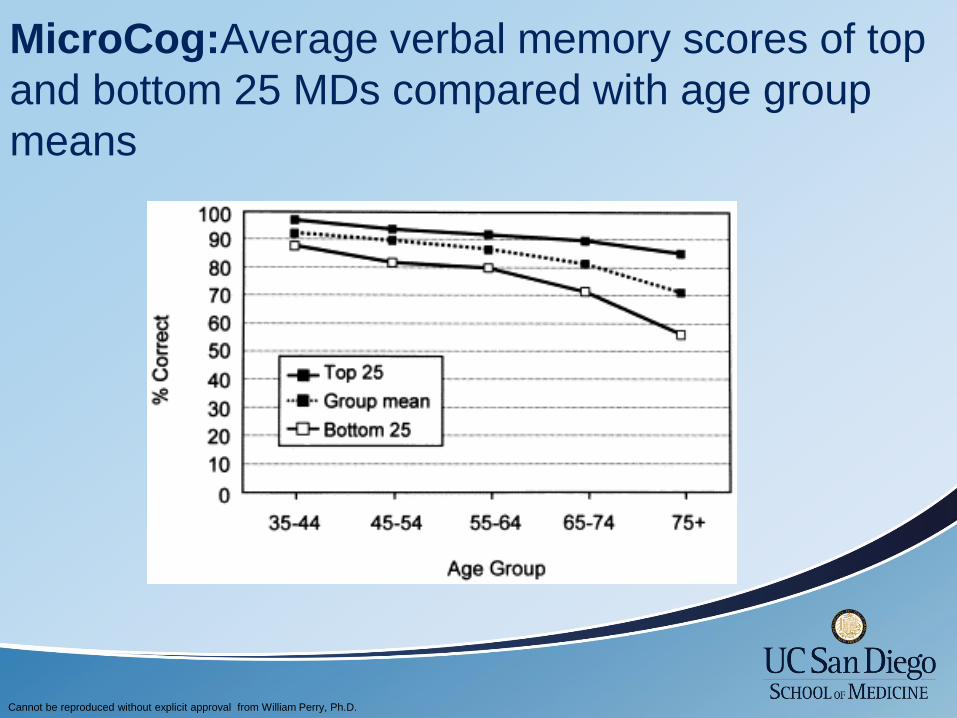
MicroCog:Average verbal memory scores of top
and bottom 25 MDs compared with age group
means
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Cognitive functioning, retirement status, and age: results from the
Cognitive Changes and Retirement among Senior Surgeons study. Drag LL, Bieliauskas LA, Langenecker SA, Greenfield LJ.
J Am Coll Surg. 2010 Sep;211(3):303-7
• They concluded that the majority of practicing senior
surgeons performed at or near the level of their younger
peers on all cognitive tasks, as did almost half of the
retired senior surgeons. This suggests that older age
does not inevitably preclude cognitive proficiency.
Number
of tests
Age group
60–64 65–69 70–74 75+ Total
n % n % n % n %
0 43 78 14 48 7 47 2 22 66
1 10 18 11 38 7 47 7 78 35
2 2 4 4 14 1 6 0 7
3 0 0 0 0 0
Total 55 100 29 100 15 100 9 100 108
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Why do we need neuropsychological
assessment anyway? Can’t we just
talk to peers?
Cannot be reproduced without explicit approval from William Perry, Ph.D.


Features of a full
Fitness for Duty Evaluation
• Thorough Medical Examination (pre- or post-
diagnosis)
• Specialty Medical Evaluation Based on Health
Concern (e.g. Neurology, Cardiology, PM&R,
Psychiatry)
• Occupational Medicine Testing
• Simulated Procedural/Skills Evaluation
• Neuropsychological Testing

Goals of a Neuropsychological/Fitness
for Duty Evaluation • To aid in diagnosing a neuropsychological/neurological
condition (dementia, Mild Cognitive Impairment, Significant
Attentional Disorder). One in eight people aged 65 and older (13%) have
Alzheimer’s disease (Alzheimer’s Association, 2013).
• To determine if a primary health condition (cardiovascular
/pulmonary/ hepatic and renal changes) is impacting his/her
cognitive functioning.
• To determine if cognitive traits or deficits, personality traits or
stress reactions are causing or contributing to problem
behavior or substandard performance.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Cognitive difficulties can
manifest as behavioral problems

Personality changes in the aging physician:
what does the research tell us
• In a large sample of generally healthy individuals
followed for almost five decades, longevity was
associated with being conscientious, emotionally
stable, and active.
• However when there are salient behavioral
changes this can be a signal of health or
emotional problems.

• The maintenance of appropriate social behavior
is a very complex process with many
contributing factors. Social and moral judgments
rely on the proper functioning of neural circuits
concerned with complex cognitive and emotional
processes.

Behavioral signs of possible
cognitive difficulties
• Anger outbursts
• Impulsive gestures
• Increased frustration intolerance
• Paranoia
• Indifference
• Poor hygiene and grooming
• Socially inappropriate comments:
– Off Color humor
– Sexually offensive comments

Assessment of Cognitive Abilities:
determining competence using
neuropsychological assessment
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Neuropsychological Domains and its
Relationship to Medical Practice
Neuropsychological
Function
Premorbid intelligence
and reading skills
Medical Practice
• Indication of a decline in
function over time.
• The ability to profit from
continuing education.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Neuropsychological Domains and its
Relationship to Medical Practice
Neuropsychological
Function
Attention
Medical Practice
• The ability to attend and determine
what is critical and salient.
• To sustain auditory and visual
attention over a sustained period of
time.
• The ability to inhibit incorrect
responses.
• Ability to simultaneously attend to
multiple processes.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Neuropsychological Domains and its
Relationship to Medical Practice
Neuropsychological
Function
Learning and
Memory
Medical Practice
• The ability to learn and
integrate new information
and draw from past
experience.
• The ability to recognize and
recall information efficiently
and quickly, without
irrelevant information
impeding.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Neuropsychological Domains and its
Relationship to Medical Practice
Neuropsychological
Function
Perceptual-motor
skills
Medical Practice
• The ability to perform
physical tasks.
• Eye-hand coordination.
• The ability to manipulate
instruments with fine-
accuracy
Cannot be reproduced without explicit approval from William Perry, Ph.D.

Neuropsychological Domains and its
Relationship to Medical Practice
Neuropsychological
Function
Executive Function
Skills
Medical Practice
• The ability to recognize the
significance of unexpected
situations in order to quickly
make alternative plans
when unusual events arise.
• Planning or decision making
abilities.
• Error correction or
troubleshooting.
Cannot be reproduced without explicit approval from William Perry, Ph.D.

CASE EXAMPLES

Questions?
CALIFORNIA PUBLIC PROTECTION & PHYSICIAN HEALTH CO O R D I N A T I N G P H Y S I C I A N H E A L T H A C T I V I T I E S I N CA L I F O R N I A
California Public Protection & Physician Health (CPPPH) was formed shortly after the Medical Board of California closed its Diversion Program for Physicians. Its mission is to develop a comprehensive physician health program for the state so that California does not remain one of the few states without such a resource.
CPPPH is an independent, non-‐profit public benefit corporation established in 2009 to carry out the steps necessary to create a physician health program. Its activities are based in the understanding that having such a program available contributes to public safety by providing services for physicians who face medical, substance use, psychological, behavioral and/or emotional issues that, if left unaddressed, could adversely impact their ability to deliver safe patient care.
CPPPH is a collaborative effort with funding from many medical organizations including specialty societies, county medical societies, the hospital association, liability carriers and medical groups. It is governed by a Board comprised of leaders from organizations with a long-‐standing involvement with physician health, namely the California Society of Addiction Medicine, the California Psychiatric Association, the California Medical Association and the California Hospital Association.
Goals And Activities of CPPPH • To collaborate with physicians, physician groups and entities
responsible for quality patient care in defining an optimum physician health program for California
• To provide consultation, education and assistance to strengthen the network of services available in California
• To develop guidelines and standards for physician health service providers
• To create a statewide program that coordinates all the services needed to address the spectrum of physician health issues
For information about CPPPH Regional Networks and other details, see www.CPPPH.org.
BOARD OF DIRECTORS James T. Hay, MD, Chair California Medical Association
Marvin Firestone, MD, JD California Psychiatric Association
Lisa Folberg, MPP California Medical Association
Randall Hagar California Psychiatric Association
David Pating, MD California Society of Addiction Medicine
David Perrott, MD California Hospital Association
Lee T. Snook, Jr., MD California Medical Association
Caroline Stewart, LCSW A New Path
Gail Jara Executive Director (510) 547-6989 Sandra E. Bressler Organizational Consultant (916) 548-1896 Janis Thibault, MFT Program Consultant (916) 952-7982 Olma T. Madrid Administration (415) 764-4822 [email protected] Dedicated to public safety and the health and well-being of California physicians

CPPPH Regional Networks
CPPPH mission o To promote a healthy physician workforce o To assist the institutions, organizations and individuals responsible for the quality
of medical care o To establish a statewide physician health program (PHP) in California o To identify, evaluate and address a full spectrum of physician health issues including physical and
mental health, behavioral issues, or addiction issues in individual physicians that may lead to practice impairment and threaten patient safety if left unaddressed
CPPPH regional networks o Deliver practical information, education and training for committees
and persons currently doing physician health work in California. At workshops offered every four months in each region, topics are covered in depth with ample opportunity for questions and information sharing
o Provide the structure for ongoing communication and statewide information sharing
o Identify and share information about the resources that the committees currently use
o Identify needs for CPPPH to address as it develops plans for a statewide program
o Contribute to CPPPH’s voice to speak for physician health in California
Participation is by invitation of CPPPH. The workshop is designed for members and staff of physician health committees in hospital medical staffs, medical groups, county medical societies and specialty societies.
CPPPH regions o Bay Area (Alameda, Contra Costa, Marin, Monterey, Napa, San
Benito, San Francisco, San Mateo, Santa Clara, Santa Cruz, Solano, Sonoma) – Gary Nye, MD
o Sierra Sacramento Valley (Amador, Butte, El Dorado, Nevada, Placer, Plumas, Sacramento, San Joaquin, Sierra, Stanislaus, Sutter, Tuolumne, Yolo, Yuba) – Tom Specht, MD
o Los Angeles (Los Angeles, Orange, Santa Barbara, Ventura) – Ira Lesser, MD
o San Diego (Imperial, Riverside, San Bernardino, San Diego) -‐ Richard Payne, MD
o Humboldt Del Norte o All California medical schools – Karen Miotto, MD For materials from past workshops, see www.CPPPH.org
For other information, contact Gail Jara at [email protected]
C O O R D I N A T I N G P H Y S I C I A N H E A L T H A C T I V I T I E S I N C A L I F O R N I A WWW.CPPPH.ORG
From Bay Area Excellent and perceptive questions and responses. Session brought up several very significant issues. Appreciate specific recommendations and suggestions. Very helpful handouts; will compare them to the forms we use.
From Sierra Sacramento Valley Thank you for putting together top-‐level panelists. Great concept. Keep it going. All chairs of hospital WBC should attend.
Great workshop. So glad the organization CPPPH exists. Awesome meeting. I am extremely excited about CPPPH and what it has to offer many.
From Los Angeles Excellent presentations from expert. I like the idea of being part of the network and that I will get more information on resources for the future.
From San Diego Helpful stimulating discussion. Absolutely worth my time! Group interaction was the best part. Excellent offering; much needed, especially in a local setting. Thankful for this organization.
Regional Workshops:
November 16 – San Diego January 25, 2014 – San Francisco Bay Area
February 8, 2014 – Los Angeles
Guidelines: • Guidelines for Selecting Physician
Health Services • Guidelines for Evaluations of Health
Care Professionals • CMA: Guidelines for Physician Well-‐
Being Committees Policies and Procedures
Download copies from www.cppph.org
California Medical AssociationPhysicians dedicated to the health of Californians
Brett JohnsonAssociate Director, Center for Medical and Regulatory Policy
California Medical AssociationPhysicians dedicated to the health of Californians

Overview
• Basic components of the Exchange p g
• Essential health benefits
Potential impact of the Exchange in California• Potential impact of the Exchange in California
• Exchange’s push for performance
• Potential barriers to care
• Physician issues to watchPhysician issues to watch
• Exchange’s 2013 timeline
California Medical AssociationPhysicians dedicated to the health of Californians
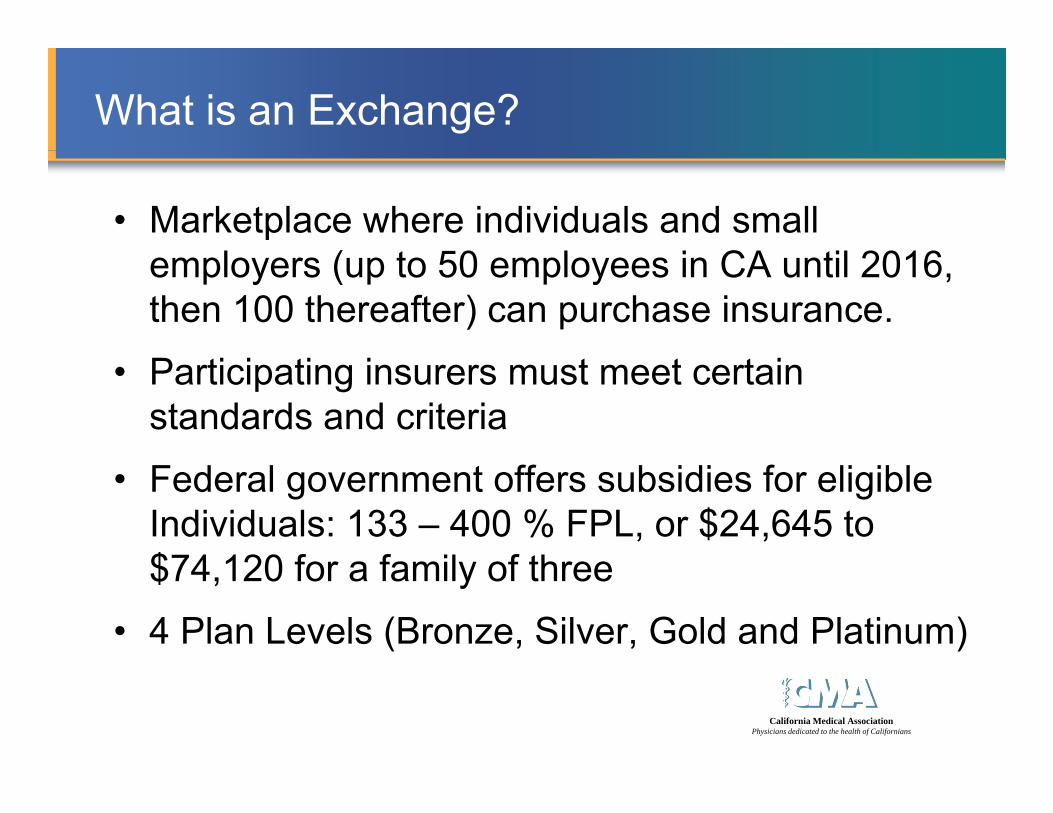
What is an Exchange?
• Marketplace where individuals and small l ( t 50 l i CA til 2016employers (up to 50 employees in CA until 2016,
then 100 thereafter) can purchase insurance.
• Participating insurers must meet certain standards and criteria
• Federal government offers subsidies for eligible Individuals: 133 – 400 % FPL, or $24,645 to $74 120 f f il f th$74,120 for a family of three
• 4 Plan Levels (Bronze, Silver, Gold and Platinum)
California Medical AssociationPhysicians dedicated to the health of Californians

Basics on the California Exchange
• California’s Exchange is an independent public entity within state governmententity within state government
• Consumer interface modeled on Travelocity site
• Governed by a five-member board appointed by the Governor and Legislature
• CA will be an active purchaser state– Similar to Massachusetts
– Unlike Utah (open marketplace)
California Medical AssociationPhysicians dedicated to the health of Californians
Essential Health Benefits (EHB)
What is EHB?
EHB is a minimum set of benefits (broadly outlined• EHB is a minimum set of benefits (broadly outlined by the feds and specifically named by the State) that must be offered by plans in the Exchangethat must be offered by plans in the Exchange.
Why does EHB Matter?• Exchange plans must offer same benefits outside Exchange
• Large group plans may not set annual or lifetime benefit caps on benefits within the EHB
• Medi-Cal expansion covers EHB+
California Medical AssociationPhysicians dedicated to the health of Californians

EHB: Kaiser Small Group HMO
• California has adopted the Kaiser Small Group HMO as its benchmark for the scope of benefits (NOT cost-sharing)p ( g)
• Above average scope of services for patients to utilize: ABA autism therapy as a healthcare service rendered by a– ABA autism therapy as a healthcare service rendered by a licensed provider
– Acupuncture for pain managementp p g
– Smoking cessation drugs
– Surgically implanted hearing devicesg y p g
– Broad substance abuse and non-severe mental illness services covered
California Medical AssociationPhysicians dedicated to the health of Californians
– 100 days skilled nursing facility coverage

Potential Impact of the Exchange
• Up to 4.4 mil enrolled by the end of 2016:Reform related outlays: ~$700 mil for exchange operations– Reform-related outlays: ~$700 mil for exchange operations in 2013 & 2014; $300 mil on ACA marketing & outreach
• What happens in the Exchange won’t stay thereWhat happens in the Exchange won t stay there
• One of Exchange’s six guiding values: “The Exchange will be a catalyst for change in California’s health care system, using its market role to stimulate new [care delivery] strategies . . .”[ y] g
• Claim that 80% of ALL practicing physicians & acute care hospitals contracted = Inaccurate
California Medical AssociationPhysicians dedicated to the health of Californians
ca e osp ta s co t acted accu ate

California’s Statewide Average Unsubsidized Premium Rates Among the 12 Exchange Plans
Plan Metal Tier Lowest Cost Plan 2nd Lowest Cost 3rd Lowest Cost
BRONZE $219 $234 $236BRONZE $219 $234 $236
SILVER $304 $325 $335
Silver Plan Premiums for a 40 Year Old Single Individual after SubsidiesSilver Plan Premiums for a 40 Year‐Old Single Individual after Subsidies
Plan ≤ 150% FPL ≤ 200% FPL ≤ 250% FPL > 250% FPLLowest Cost $35 $98 $170 $271Lowest Cost $35 $98 $170 $271
2nd Lowest Cost $57 $121 $193 $294
3rd Lowest Cost $68 $127 $199 $301
150% FPL = $17,235 for individual; + $6,030 for each dependent
California Medical AssociationPhysicians dedicated to the health of Californians
200% FPL = $22,980 for individual; + $8,040 for each dependent250% FPL = $28,725 for individual; + $10,050 for each dependent

Developing the Provider Networks in California
• Networks due to regulators before most contracts went out
• Many physicians unclear whether contracted for exchange• Many physicians unclear whether contracted for exchange
• Very little in contracts thus far – much likely to come in the form of administrative and policy manual amendmentsform of administrative and policy manual amendments
• Offered rates are all over the map– Public statements suggesting averages of 10% below commercial for gg g g 0%
hospitals and 20-30% below commercial for physicians
• Plans still filling in the gaps
• Narrow and tiered networks will abound– E.g., Blue Shield at one-third to half its traditional PPO network
California Medical AssociationPhysicians dedicated to the health of Californians
9
Performance at the Forefront
• Plans and providers given performance ratingsp g p g
• Recently announced a delay until 2016 on rating plans on NCQA-used HEDIS & CAHPS measuresplans on NCQA used HEDIS & CAHPS measures
• 2016+: Assess provider data & rate individuallyU l t di l l l lit i f– Use complementary medical group-level quality info
– Cultural competency/interpreter services
– Personal health management services
– Assess quality down to individual providers
California Medical AssociationPhysicians dedicated to the health of Californians
q y p
– Member decision support tools
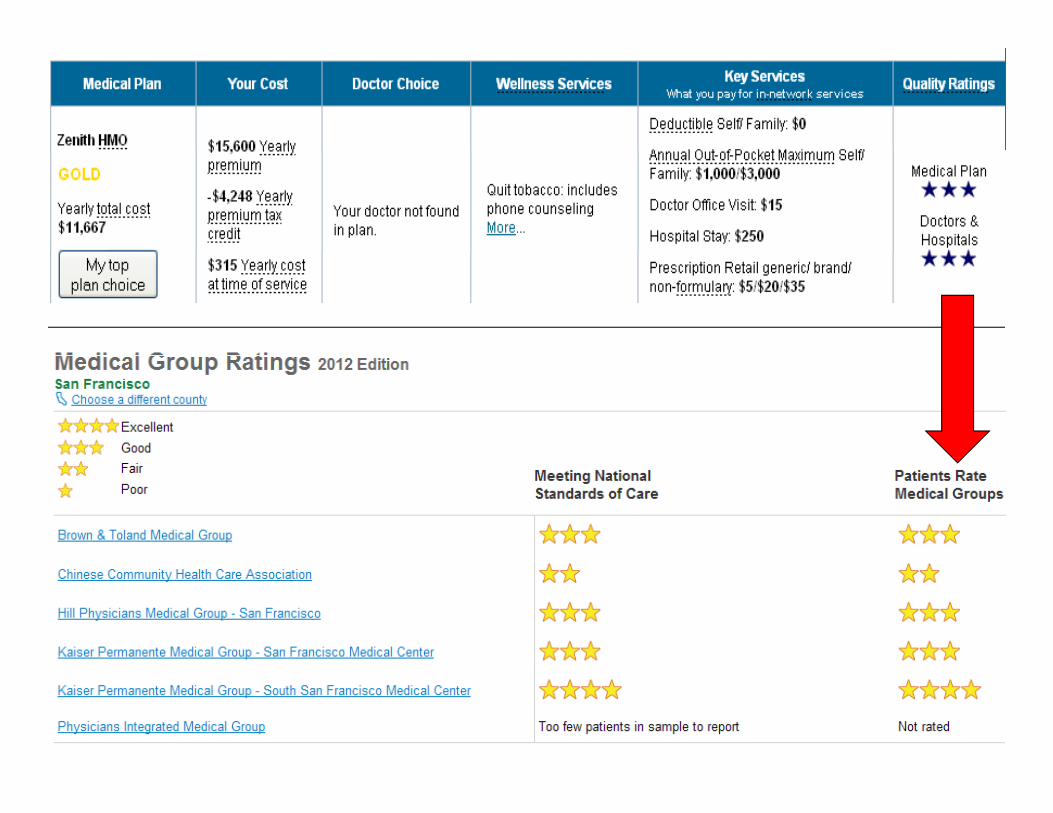
California Medical AssociationPhysicians dedicated to the health of Californians
Barriers to Care with Exchange Products
• Safety net issuesy
• Network inadequacy
Significant patient cost sharing• Significant patient cost-sharing
California Medical AssociationPhysicians dedicated to the health of Californians

Barriers: Safety Net Issues
• Networks must include essential community providers (ECP)
• ECPs include:• ECPs include: – 340B &1927(c) listed providers (ACA req’d; CA = 15% 340B);
DSH facilities & certain state recognized clinics; and– DSH facilities & certain state-recognized clinics; and
– Private physicians with approved applications for the HI-TECH Medi-Cal EHR Incentive Program. g
• Plans are encouraged to include FQHCs in the network
• Some ECP concerns moving forward:Some ECP concerns moving forward:– Adequate ECP networks for underserved communities
– Increased coordination with private providers
California Medical AssociationPhysicians dedicated to the health of Californians
Increased coordination with private providers
– Competition for newly insured and funding
Barriers: Network Inadequacy
• Exchange intends to rely on current agency monitoring of plan directoriesp
• CDI & DMHC do no verification of directories
• Regulators looking at new resourcesRegulators looking at new resources
• Exchange has pledged to explore an expanded role in the verification of provider directories should issues arise
• Model contract proposes a centralized Exchange provider directory with quarterly updating
• Concerns: Use of two+ tier networks, centers of excellence, and reliance on volume providers
California Medical AssociationPhysicians dedicated to the health of Californians

Barriers: Patient Cost-Sharing
California Medical AssociationPhysicians dedicated to the health of Californians

Barriers: Patient Cost-Sharing
• Much of Exchange’s offerings are catastrophic coverage
• Standard cost-sharing caps: $6 350 indiv ; $12 700 familyStandard cost sharing caps: $6,350 indiv.; $12,700 family
• Cost-sharing reductions available to those ≤ 250% FPL enrolling in silver plans and no cost preventive careg
• ER services cost-share (deductible applies): Silver plans = $25 - $250; Bronze plans = $300 or 40%; waived if admitted
• Cost-sharing challenges for patients:
– Significant co-pays for specialist services and imaging
– High brand drug deductibles– Inexperience with premiums & cost-sharing
California Medical AssociationPhysicians dedicated to the health of Californians

Barriers: Patient Cost-Sharing
Service Category Patient Co-PayStandard Silver Standard Bronze
Hospital Stay 20%* (physician services exempted from deductible)
30%*
ER Services $250* $300*
Specialist Visit $65 $70*
X rays and Diagnostic $65 30%*X-rays and Diagnostic Imaging
$65 30%*
Imaging (CT/PET, MRIs) 20%* or $250 30%*
“Integral Part” of a Preventive Care Service
No patient cost share across all plans.
$
California Medical AssociationPhysicians dedicated to the health of Californians
DEDUCTIBLES*Deductible applies.
Medical = $2,000; brand drugs = $250
Medical & drug integrated (inpatient, ER, drugs) = $5,000

Barriers: Patient Cost-Sharing
• On premiums, will the young and healthy sign up?– “Affordable” = $25-50 for individuals; $100-150 for familiesAffordable $25 50 for individuals; $100 150 for families
– Only the lowest cost bronze and silver plans for those making no more than $17,235 fit the focus groups’ view of “affordable.”
• Will high cost-sharing serve as a rate reduction for physicians?– Standard cost-sharing caps: $6,350 self; $12,700 family
– Cost-sharing reductions available to those ≤ 250% FPL enrolling in silver plans and no cost preventive care is available to allsilver plans, and no cost preventive care is available to all
• How will physicians respond to greater pressure to consider costs to patients in the treatment plan?
California Medical AssociationPhysicians dedicated to the health of Californians
consider costs to patients in the treatment plan?

Physician Issues
• Extent of administrative demands still uncertain
R f i ifi l b l i l• Reports of significantly below commercial rates– Will these rates be used elsewhere?
– Why does the Exchange want access to the rates?
• Provider directories still being finalized
• Many plans intending to build networks without new contracts or substantial amendments– “All products” clauses
– Amending policy manuals
California Medical AssociationPhysicians dedicated to the health of Californians
Amending policy manuals
– “All or nothing” amendments
Physician Issue #1: Grace Period
• ACA: 3-month grace period for premium delinquency• Plans must cover 1st month
• May pend then deny all claims in months 2 & 3
• Applies to enrollees receiving federal tax subsidies
• CA Model Contract: Plans must provide15 calendar• CA Model Contract: Plans must provide15 calendar days notice before month #2, but only to:
• Physicians submitting claims on patient in previous• Physicians submitting claims on patient in previous 2 months and the patient’s assigned PCP.
S i f i CACalifornia Medical Association
Physicians dedicated to the health of Californians
• Suspension of coverage now in CA
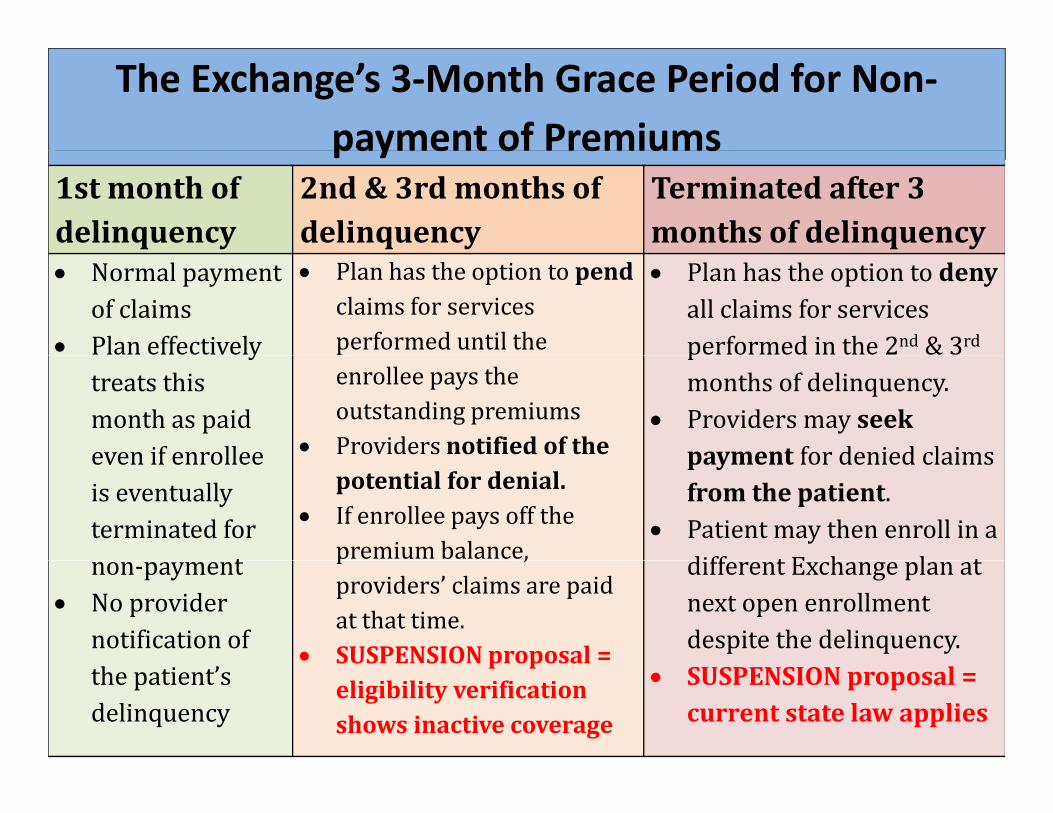
The Exchange’s 3‐Month Grace Period for Non‐payment of Premiumspayment of Premiums
1stmonthofdelinquency
2nd&3rdmonthsofdelinquency
Terminatedafter3monthsofdelinquency
Normalpaymentofclaims
Planeffectively
Planhastheoptiontopendclaimsforservicesperformeduntilthe
Planhastheoptiontodenyallclaimsforservicesperformedinthe2nd &3rdy
treatsthismonthaspaideven if enrollee
enrolleepaystheoutstandingpremiums
Providersnotifiedofthe
pmonthsofdelinquency.
Providersmayseekpayment for denied claimsevenifenrollee
iseventuallyterminatedfor
t
potentialfordenial. Ifenrolleepaysoffthe
premiumbalance,
payment fordeniedclaimsfromthepatient.
Patientmaythenenrollinadiff t E h l tnon‐payment
Noprovidernotificationof
p ,providers’ claimsarepaidatthattime.
SUSPENSION proposal =
differentExchangeplanatnextopenenrollmentdespitethedelinquency.
California Medical AssociationPhysicians dedicated to the health of Californians
thepatient’sdelinquency
SUSPENSIONproposal eligibilityverificationshowsinactivecoverage
SUSPENSIONproposal=currentstatelawapplies

Physician Issue #2: Out-of-Network Services
• Exchange hostile towards out-of-network care
• Plans must disclose what it will pay on out-of-network, non-emergent services to an enrollee
• In-network physicians must disclose the use of or referral to an out-of-network provider or facility– “In a manner that allows the enrollee the
opportunity to act upon . . . the recommendation”
• Physician may rely upon plan-published information sources for contract status
California Medical AssociationPhysicians dedicated to the health of Californians
Physician Issue #3: Admin Burdens
California Medical AssociationPhysicians dedicated to the health of Californians

Physician Issue #3: Admin Burdens
• More than 70 reports required of exchange plansf– Extent of added burden on providers still unclear
• Referral coordination with safety-net providers– Networks must include “essential community providers”
• Push for plans to adopt value-based payment and participate in host of quality initiativesparticipate in host of quality initiatives
• Physicians must report use of shared decision-making t ltools.
• And don’t forget about the ICD-10 transition next year.
California Medical AssociationPhysicians dedicated to the health of Californians

Exchange TimelineExchange Timeline 2013-2014
Provider networks submitted to regulators 2/28/13gFinal QHP Model Contract released 5/8/13Tentative QHP certifications and initial 5/23/13contract agreement with prospective QHPs
Reasonableness rate review by regulators 5/23 – 6/30/13
Individual QHP contracts signed and networks finalized with regulators
Before 7/30/13et o s a ed t egu ato s
Exchange provider database made public Before 7/31/1310/X/13?10/X/13?
Initial Exchange open enrollment period 10/1/13 – 3/31/14
California Medical AssociationPhysicians dedicated to the health of Californians
Exchange coverage begins 1/1/2014
CMA Can Help: FREE member benefits!• CMA’s Reform Essentials – free e‐publication
– sign up by calling (800) 786‐4CMA (4262)
• CMA Practice Resources (CPR) ‐ free monthly e‐publication– sign up by completing subscription form today!
CES b it f t l d f b !• CES website – free tools and resources for members!– www.cmanet.org/ces
• CMA’s members‐only reimbursement helplineCMA s members only reimbursement helpline– (888) 401‐5911 or [email protected]
• CMA’s Center for Economic Services website:– www.cmanet.org/ces
• CMA’s member services helpline (800) 786‐4CMA (4262)
ll l bCalifornia Medical Association
Physicians dedicated to the health of Californians
• CMA On‐Call Legal Library www.cmanet.org

Subscribe to CMA’s Reform Essentials
Brett Johnson JD MPH MSBrett Johnson, JD, MPH, [email protected](916) 551-2552( )
California Medical AssociationPhysicians dedicated to the health of Californians