sps texas region clabsi workgroupchatexas.com/wp-content/uploads/2016/11/texas_hac... · •...
TRANSCRIPT

1
SPS Texas Region CLABSI Workgroup

2
The Texas Regional Hospitals
•Baylor Scott & White McLane Children’s Medical Center •Children’s Health, Children’s Medical Center •Children’s Memorial Hermann Hospital •Cook Children’s Medical Center •Covenant Children’s •Dell Children’s Medical Center of Central Texas •Driscoll Children’s Hospital •Medical City Children’s Hospital •Texas Children’s Hospital (Houston) •The Children’s Hospital of San Antonio

3
Beds: 248
Primary Service Area: 46 counties in Central Texas
Inpatient/Observation Admissions 2016: 13,903
Level I Trauma Center
Level IV NICU
Teaching hospital - Dell Medical School
Platinum Certification U.S. Green Building Council
Leadership in Energy and Environmental Design (LEED)
4
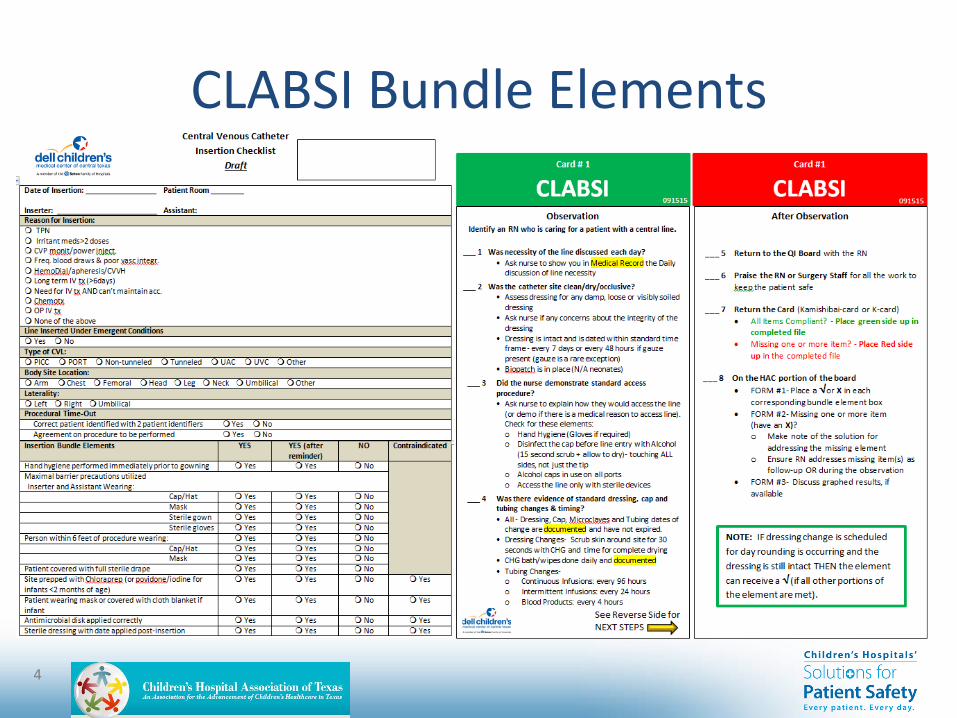
CLABSI Bundle Elements

5
CLABSI Bundle Elements

6
CLABSI Data Collection Methods
• Insertion audits – discontinued a few years ago when compliance was consistently 100%; will be reinstated as checklist in next few months
• Maintenance audits –also stopped a few years ago; restarted with K-card in September 2015 – IP completing monthly point prevalence surveys using
tool shown above
– Unit managers now performing weekly point prevalence surveys using same tool
7
CLABSI Investigative Process 1. All CLABSIs are investigated in detail
2. IP Works up BC, determines if CLABSI criteria met
3. IP & Pedi ID/IP Medical Director discuss
4. SWOT scheduled as soon as possible after IP identifies, unit manager or designee to complete CLABSI data collection form
5. SWOT with
• Unit Manager
• Educator
• VAT nurse (regardless of type of CVL)
• TQM Quality Coordinator
• Staff nurse, if available
• Unit CVL champion
• Others as indicated (IR staff, anesthesia, intensivists)
6. Disseminate findings of SWOT with affected unit and remainder of DCMC

8
CLABSI Investigative Process
SWOT Data Collection Form

9
CLABSI Rate 2015-2016 CVL Utilization Critical Care and Acute combined = .28
NHSN Benchmarks: Pedi M/S ICU = .45; Pedi M/S Acute Care = .19

10
CLABSI Increase • August 2015-December 2016
– 29 CLABSIs (and additional 8 MBI-BSI) • 11 in cardiac patients
– 10 in PICU; 1 in IMC
» 7 CLABSIs in 5 patients d/t Enterobacter cloacae PFGE dendrogram of 3 patients showed cluster was not a single source; one of the patients with two E. clo CLABSIs 2 months apart had similar patterns between the 2 isolates
» Only commonality of 29 factors investigated was same cardiac surgeon
• No E. clo since surgeon left

11
CLABSI Investigation-Discovery • Tracheal colonization of E. clo of some but not all patients
• Respiratory therapy supplies and equipment repeatedly found on sink-side of plexiglas dividers
• RT feedback on potential causes of tracheal colonization- incorrect trach care technique observed of nursing
• No changes to equipment or products for more than 6 months
• Audits on alcohol cap compliance found about 90% compliance
• Oral care – good compliance
• Housekeeping issues- FTEs have been cut back – No dedicated housekeeper in Critical Care; assigned housekeepers intimidated by
equipment, avoided complicated patients’ rooms
– Overflowing trash, cleanliness issues
– Tops of warmers not getting cleaned by housekeepers when patient is in bed

12
CLABSI Investigation-Discovery • SWOTs identified a gap in CHG bathing and/or documentation
• Multidisciplinary focus group revealed wide variation with nurses’ CVL care practices, despite knowing the policy
• Review of 100 cardiac patients showed the recent patients with E. cloacae as being of much higher acuity
• Issues identified with ICU Medical blue Microclaves – septum found to remain depressed on multiple patients
• IP point prevalence surveys on CVL maintenance bundle show poor compliance

13
CLABSI Best Practice Recommendations
• Respiratory therapy completed 3 months of audits to ensure clean equipment not found near sink – between 90% and 100% compliance
• IMC and PICU staff received trach care re-education and training
• Workgroup of RNs and RTs standardized locations of supplies kept in the room; developed individual trach supply bags for new trach patients
• CVL champion identified in PICU, began CVL care observation and 1-on-1 peer coaching of nurses’ practice
• Housekeeping issues addressed with EVS director, requested dedicated housekeeper for Critical Care
• Cardiac council officially recommended dedicated housekeepers for Critical Care areas
• Warmers/isolettes/cribs/beds to be changed out every month to allow thorough cleaning and align with NICU practices
• Monitoring of CVL bundle compliance was begun using new interactive process with a tool called “K cards”

14
CLABSI Best Practice Recommendations
• Monthly DCMC CVL team meetings reinstated
• Spring Nursing Competencies added:
– Reeducation of staff regarding the CHG daily bathing guidelines during Spring competencies
– CVL maintenance bundles part of Spring competencies for Critical Care nurses
• Changed to larger alcohol wipes after complaints smaller ones not wet enough for adequate hub scrubbing
• Moved diaper scales from patient room counter to bathroom
• Dedicated drying stations for RT equipment moved away from sink
• Scrub-the-hub campaign started using reminder stickers on clocks
• Sent all tubing components/connectors currently used at DCMC to ICU Medical for Microclave compatibility testing
• Trialed clear Microclaves in PICU and later changed

15
CLABSI Best Practice Recommendations
• Developed process to take mixing of probiotic away from bedside and into the nutrition room or breast milk room
• Plan developed for improvement of CVL maintenance bundle compliance • Beginning with January of IP’s monthly point prevalence survey, units not
scoring at or above 90% compliance will begin a weekly audit for a minimum of 3 months
• At the end of 3 months of sustained 90% compliance per IP’s point prevalence surveys, weekly audits stop.
• If, at the end of the first 3 months, the unit has not achieved and sustained a 90% compliance, weekly audits will continue until the unit demonstrates 3 months of sustained compliance at or above 90%.
• The clinical manager will submit an additional action plan to IP for improving CVL maintenance compliance
• Results of weekly audits will be shared monthly at the Medical Council

16
Bard All-Points Program
June 2016 – January 2017 Bard All-Points Program
• June - Bard introduced their program
• July – Bard completed a gap analysis comparing policy against the governing standards for dressing changes, blood draws, hub maintenance and medication administration
• July – Bard rounded on all central lines
• July – Bard audited nursing staff performing dressing change, blood draws, hub maintenance and medication admin in a simulated patient room
• August - Data compiled by BARD and presented to leadership
• August - Unit champions trained by Bard
• September - Unit champions educated remainder of staff within 30 days
• Site-rounding and staged assessments repeated 30 days after staff trained
• January 13 - Final presentation

17
SWOT Learnings Spread
All-Teach, All-Learn
Poster Distributed to site staff
18
CLABSI Requests for Assistance

19
QUESTIONS?