starget 1 2010 en - straumann.com 03 dearreaders, inoursector,thenamestraumannstandsfor...
TRANSCRIPT

STARGETMAGAZINE FOR CUSTOMERS AND PARTNERS OF STRAUMANN
01 I 2010
FOCAL POINTS
1 Million SLActive®: the success story of Straumann‘s premiumimplant surface
IPS e.max® CAD restorations by Straumann® CADCAM:a highly esthetic solution for single tooth replacement and restoration
New products: Roxolid™ – Straumann® Temporary Abutment
Discussion topic “Cheap Implants“: why the Straumann®
Dental Implant System is a premium brand
Practice benchmarking: discovering and developing unutilizedpotentials for your practice
Straumann and ITI: a high-quality international education program
ITI World Symposium 2010 in Geneva: ”30 Years ofLeadership and Credibility”
STARGET_1_2010_en.indd 1STARGET_1_2010_en.indd 1 21.12.2009 17:34:22 Uhr21.12.2009 17:34:22 Uhr

Imprint: STARGET – An International Magazine for Customers and Partners of Straumann I © Institut Straumann AG I Peter Merian-Weg 12 I CH-4002 Basel IPhone +41 (0)61 965 11 11 I Fax +41 (0)61 965 11 01 I Editors: Roberto González I Mildred Loewen I E-Mail: [email protected] I Internet:www.straumann.com/starget I Appearance: 4 times per year I Layout/Design: EMS & P Kommunikation GmbH, www.ems-p.com I Printing: Dietschi AG IHauptstrasse 22 I CH-4437 Waldenburg
Legal Notice: Exclusion of liability for articles by external authors: articles by external authors published in STARGET have been systematically assessed and carefullyselected by the publisher of STARGET (Institut Straumann AG, Basel). Such articles in every case reflect the opinion of the author(s) concerned and therefore do not neces-sarily coincide with the publisher’s opinion. Nor does the publisher guarantee the completeness or accuracy and correctness of articles by external authors published in
03 Editorial
FOCAL POINTSSLActive®
04 Bone regeneration at BoneLevel implants with SLActive®
surface by F. Schwarz, D.Ferrari, M. Wieland and J.Becker
09 SLActive® launched in SouthKorea
10 Success story of the premiumimplant surface SLActive®
IPS E.MAX® CADRESTORATIONS BYSTRAUMANN® CADCAM12 IPS e.max® CAD restorations
by Straumann® CADCAM
14 The Straumann® CADCAMSolution
Roxolid™18 Roxolid™ – a new material
designed for the specificneeds of implant dentistry
22 Reduced-diameter implantsas a treatment alternative inrisk patients to avoid aug-mentation procedures byHannes P. Schierle, Hans O.Werner, Franziska Nagel
Products26 Exchanging first experiences
with the Straumann® Ana-tomic IPS e.max® Abutment
28 Straumann® TemporaryAbutments
30 New packaging for non-sterile packaged components
32 Expert opinion on the studyby Holger Zipprich et al.
35 Bone Level Implant launchedin Brazil
Clinical Cases36 Synergies for clinical suc-
cess with an osteoconductiveimplant surface and bonereplacement graft, a novelimplant-abutment connec-tion and meticulous occlusaltherapy by Barry P. Levin
41 Regeneration of a periodon-tal defect with Emdogain anda Soft Tissue Level Implant withSLActive® surface, in combi-nation with BoneCeramic byMarlene Teo and Joanne Uy
Simply doing more46 Why the Dental Implant
System is a “premium”solution
53 “Quality and service comeat a price” Interview withSandro Matter
55 Discovering and developingunutilized potentials for yourpractice
58 Literature alerts
Education62 Straumman and ITI:
International educationprogram at a high level
Events64 ITI World Symposium 2010
in Geneva
72 Annual Meeting of the AOin Orlando
74 AEEDC Congress in Dubai
76 Annual Conference of theEAO in Monaco
78 Events overview 2010
TABLE OF CONTENTS
Internet: www.straumann.com/starget or your specific country website www.straumann.(xy)/starget
STARGET_1_2010_en.indd 2STARGET_1_2010_en.indd 2 21.12.2009 17:34:34 Uhr21.12.2009 17:34:34 Uhr

STARGET 1 I 10 03
Dear readers,
In our sector, the name Straumann stands forgenuine and scientifically well-grounded innova-
tions that set standards and open up new possibilities in implant-supportedrestorations.
Even upon its introduction to the market at the EAO 2005 in Munich, theoutstanding osseointegrational properties of SLActive® could be confirmedby numerous studies. Over a million Straumann implants with the SLActive®
surface have been sold since then – proof for us that the experts could beconvinced.
The next major milestone in the story of Straumann products was now pre-sented at the EAO 2009 in Monaco: Roxolid™, the implant material devel-oped specially for the needs of dental implantology. The 3.3mm diameterRoxolid™ implants may enable an implant-borne restoration even in patientswho would otherwise decide against an implant treatment because of adeficiency of available bone and the associated need for augmentation.With Roxolid™ the user can thus reach new groups of patients through time-saving, more cost-effective and less invasive solutions.
And finally, in collaboration with Ivoclar Vivadent AG, Straumann now pro-vides an impressive solution for single tooth restorations with the new “IPSe.max® CAD Restorations by Straumann® CADCAM“.
Another topic that concerns our sector is the discussion of the usefulnessand benefits of cheap implants. In this edition, we would like to illustratewhat Straumann as a premium provider invests and achieves in order to fur-ther develop implant dentistry on a scientific foundation, while continuouslyincreasing treatment safety for patients. We also look at the risks that canresult from using cheap implants.
I hope you find it an interesting read.
Sincerely,Wolfgang Becker
STARGET. The information given in clinical case descriptions, in particular, cannot replace a dental assessment by an appropriately qualified dental specialist in an individualcase. Any orientation to articles published in STARGET is therefore on the dentist’s responsibility. Articles published in STARGET are protected by copyright and may not bereused, in full or in part, without the express consent of the publisher and the author(s) concerned. Third party corporate names and brand names that may be mentionedmay be registered or otherwise protected marks even if this is not specially indicated. The absence of such an indication shall not therefore be interpreted as allowing such aname to be freely used.
Product availability: Certain products and services mentioned in this edition of STARGET may not be available or not yet available in all countries. In case of doubt pleasecontact your local Straumann distributor for information on product availability (addresses of Straumann branches can be found on page 83).
Wolfgang BeckerSenior Vice President Central Europe
EDITORIAL
STARGET_1_2010_en.indd 3STARGET_1_2010_en.indd 3 21.12.2009 17:34:35 Uhr21.12.2009 17:34:35 Uhr

Bone regeneration at Straumann® Bone Levelimplants with SLActive® surface –histological and clinical experiencesby F. Schwarz1, D. Ferrari1, M. Wieland2, J. Becker1
A recent review paper3 has summarized the potential of hydrophilic surface modifications
(Straumann SLActive®) to support tissue integration of titanium dental implants.
Figures 1a–f:Influence of the defect size on bone
regeneration at Straumann® Bone
Level Implants with SLActive®
surface (4.1 x 10mm) after 4
weeks of submerged healing in
dogs without the additional use of
bone grafts or barrier membranes.
White bar:indicates the bottom of the defectYellow bar:indicates the most coronal extent of newlyformed bone in contact with the implant surface
Fig. 1a:Defect length: 7–8 mmPercentage of linear defect fill: 65%Toluidine blue stain (magnification x10)
1Department of OralSurgery, Heinrich HeineUniversity, Düsseldorf,Germany2Institut Straumann AG,Basel, Switzerland
Fig. 1b:Higher magnification (x30) of Fig. 1a
One part of this review paperfocused on the pattern of woundhealing at dehisced implants. Inparticular, previous experimentalstudies performed in dogs havedemonstrated that Straumann® SoftTissue Level implants with SLActive®
surface supported bone regenera-tion in acute-type buccal dehiscencedefects at submerged implantswithout the additional use of guidedbone regeneration or bone augmen-tation procedures.4 At two weeks,newly formed trabeculae of wovenbone, originating from both thelateral walls and the bottom of thedefect areas, started to invade the
dehiscence area. After 12 weeks,SLActive® implants were surroundedby firmly attached, parallel-fiberedwoven bone. The newly formedbuccal aspects of the ridge reachedthe level of the corresponding oralaspects. In contrast, wound healingat SLA® implants was predominantlycharacterized by the formationof dense connective tissue at twoand 12 weeks, without significantincreases in mean new boneheight or bone-to-implant contact.4
Similar results were also observedat non-submerged Soft Tissue Level®
implants with SLActive®.5 In particu-lar, immunohistochemical analysis
1b1a
STARGET 1 I 1004 SLACTIVE® FOCAL POINT
STARGET_1_2010_en.indd 4STARGET_1_2010_en.indd 4 21.12.2009 17:34:35 Uhr21.12.2009 17:34:35 Uhr

Fig. 1c:Defect length: 8–9mmPercentage of linear defect fill: 54%Toluidine blue stain (magnification x10)
Fig. 1d:Higher magnification (x30) of Fig. 1c
Fig. 1e:Defect length: 10mmPercentage of linear defect fill: 57%Toluidine blue stain (magnification x10)
Fig. 1f:Higher magnification (x30) of fig. 1e
1c
after 1 week of healing in dogsrevealed pronounced proliferationof blood vessels adjacent toSLActive® implants, even reach-ing the central compartment of thedefect area. In contrast, at SLA®
implants, the primary meshwork ofnewly formed vascular structureswas located at the bottom and lat-eral aspects of the defect area.Histological and immunohistochemi-cal observations have pointed togreater stabilization of the bloodclot at SLActive® implant surfaces,thus promoting the in-growth of newblood vessels from the adjacentalveolar bone. Basically, the blood
clot acts as a physical matrix thatinduces and amplifies the migra-tion, proliferation and differentiationof endothelial cells, subsequentlyleading to improved angiogenesis.6
Osteogenic cells have also beenobserved to arise from pericytesadjacent to small blood vessels inconnective tissue,7–9 thus explainingthe improved bone formation atSLActive® implants. At 8 weeks,non-submerged and submergedSLActive® implants revealed signifi-cantly higher mean values of newbone height, area of bone forma-tion, and bone-to-implant contactthan corresponding SLA® implants.
However, within the SLActive®
groups, bone regeneration wassignificantly improved at submergedimplants.5
Accordingly, it was concluded thatSLActive® titanium implants support-ed bone regeneration in acute-typebuccal dehiscence defects, and asubmerged healing process furtherimproved the healing outcome.5 Asimilar pattern of bone regenerationwas also observed when Soft Tis-sue Level® implants with SLActiveâwere combined with different typesof barrier membranes or bone sub-stitutes.10,11 Blood vessels and the
1f1e1d
STARGET 1 I 10 05FOCAL POINT SLACTIVE®
STARGET_1_2010_en.indd 5STARGET_1_2010_en.indd 5 21.12.2009 17:34:36 Uhr21.12.2009 17:34:36 Uhr

subsequently formed woven boneinvaded the defect area in a coro-nal direction, primarily along thesurface of SLActive® implants.
Recently, the Straumann® BoneLevel Implant was introduced as atwo-part implant to support bonepreservation for predictable estheticresults.12,13 Its specific macrodesigncoupled with the SLActive® surfacemight provide a promising environ-ment to support bone regenerationeven at advanced defect sites asobserved with Straumann® SoftTissue Level implants with SLActive®.Accordingly, the aim of a veryrecent experimental pilot studyperformed in dogs was to assessthe influence of the defect size onbone regeneration at Straumann®
Bone Level implants with SLActive®.Standardized (width: 4mm; depth:1–2mm) buccal dehiscence-type
defects of different sizes (i.e. height:7–8mm; 8–9mm; and 10mm) weresurgically created following implantsite preparation in the lower jaws ofdogs. After 4 weeks of submergedhealing without the additional useof bone graft substitutes or barriermembranes, dissected blocks wereprocessed for histomorphometricalanalysis (i.e. coronal extent of newlyformed bone in contact with theimplant surface, area of new bonefill, percentage of bone-to-implantcontact in the defect area, and per-centage of linear defect fill).
In general, wound healing wasregarded as uneventful at all sites.There were no signs of any woundinfections or dehiscences. Irrespec-tive of the initial defect size, histo-morphometrical analysis revealed asignificant increase of all parametersinvestigated. The mean percentage
of linear defect fill varied between54 and 65%. In all specimens,the newly formed woven boneextended along the bottom of thedefect in a coronal direction andshowed close contact to the titaniumsurface (Figs. 1a–f). These valueswere within the range of the datareported for either non-submerged/submerged Straumann® Soft Tissueor Bone Level implants with SLActive®
(Table 1). In these studies, however,the defects had a moderate heightof 4mm.
Based on these findings, it might besuggested that Bone Level® implantswith SLActive® surface have a highpotential to support bone regenera-tion even at advanced buccal dehis-cence-type defects. Even though thesurgical creation of standardizeddefects in dogs is a commonly usedmodel to evaluate bone regenera-
Fig. 2b:Compromised implant site in region012. The vestibular bone plate wasalmost completely resorbed.
Fig. 2a:Clinical situation 6 weeks afterextraction of teeth 12 and 22
Fig. 2c:The correct three-dimensional positioningof a Straumann® Bone Level Implant(Ø 4.1, SLActive® 10 mm) was asso-ciated with a large buccal dehiscence-type defect.
Fig. 2d:Guided bone regeneration using acollagen membrane and particulatenatural bone mineral.
Figures 2a–l:Clinical outcome of guided bone regeneration at Straumann® Bone Level implants with SLActive® surface.
2c 2d2b2a
STARGET 1 I 1006 SLACTIVE® FOCAL POINT
STARGET_1_2010_en.indd 6STARGET_1_2010_en.indd 6 21.12.2009 17:34:37 Uhr21.12.2009 17:34:37 Uhr

Fig. 2h:Re-entry at 4 months revealed completedefect fill with newly formed hard tissue.The implant neck was homogeneouslycovered by a thick (2mm) layer ofmineralized tissue.
Fig. 2g:Clinical situation after 4 months
Table 1:Experimental animalstudies reporting on thepercentage of linearbone fill in dehiscence-type defects after 2–4weeks of submergedhealing.
tion at titanium implants, acute-typedefects have a certain tendency tospontaneous healing. Accordingly,from a clinical point of view, thedefect model employed in theseanimal studies on SLActive® implantsmay not reflect the biological situ-ation encountered at chronic-typedefects.
So far, however, clinical experi-ence suggests that a combinationof Straumann® Bone Level implantswith SLActive® and simultaneousguided bone regeneration providesa high level of predictability to sup-port hard tissue formation even atadvanced defect sites (Figs. 2a–l).These findings are also in agreementwith the results obtained previouslywith Straumann® Soft Tissue Levelimplants with SLActive® surface.
Fig. 2e:Double layer technique to increase thestability of the barrier membrane.
Fig. 2f:Tension-free wound closure to ensure asubmerged healing process.
2f 2h2e 2g
References3Schwarz F, Wieland M, Schwartz Z, ZhaoG, Rupp F, Geis-Gerstorfer J, Schedle A,Broggini N, Bornstein MM, Buser D, Fergu-son SJ, Becker J, Boyan BD, Cochran DL.Review: Potential of chemically modifiedhydrophilic surface characteristics to supporttissue integration of titanium dental implants.J Biomed Mater Res B Appl Biomater 2008.4Schwarz F, Herten M, Sager M, WielandM, Dard M, Becker J. Bone regenerationin dehiscence-type defects at chemicallymodified (SLActive®) and conventional SLAtitanium implants: a pilot study in dogs. J ClinPeriodontol 2007;34:78-86.5Schwarz F, Sager M, Ferrari D, Herten M,Wieland M, Becker J. Bone regeneration indehiscence-type defects at non-submerged andsubmerged chemically modified (SLActive®)and conventional SLA titanium implants: animmunohistochemical study in dogs. J ClinPeriodontol 2008;35:64-75.
6Liu HM, Wang DL, Liu CY. Interactionsbetween fibrin, collagen and endothelialcells in angiogenesis. Adv Exp Med Biol1990;281:319-331.7Long MW, Robinson JA, Ashcraft EA, MannKG. Regulation of human bone marrow-derived osteoprogenitor cells by osteogenicgrowth factors. J Clin Invest 1995;95:881-887.8Reilly TM, Seldes R, Luchetti W, BrightonCT. Similarities in the phenotypic expressionof pericytes and bone cells. Clin Orthop1998:95-103.9Rickard DJ, Kassem M, Hefferan TE, SarkarG, Spelsberg TC, Riggs BL. Isolation andcharacterization of osteoblast precursor cellsfrom human bone marrow. J Bone Miner Res1996;11:312-324.10Schwarz F, Herten M, Ferrari D, WielandM, Schmitz L, Engelhardt E, Becker J. Guidedbone regeneration at dehiscence-type defectsusing biphasic hydroxyapatite + beta trical-
Defect Heigth (Healing Period) Implant Type SLActive® SLA®
4mm (2 weeks)4 Tissue Level 34.0–80.0% 0.0%
4mm (4 weeks)5 Tissue Level 69.5–96.1% 37.8±49.1%
4mm (4 weeks)14 Bone Level 48.2– 99.1% not included
STARGET 1 I 10 07FOCAL POINT SLACTIVE®
STARGET_1_2010_en.indd 7STARGET_1_2010_en.indd 7 21.12.2009 17:34:43 Uhr21.12.2009 17:34:43 Uhr

PD Dr Frank Schwarz
Education
1993–1998Dental School, University of Saarland,Homburg/Germany
February 2001Dr med. dent. Thesis: “Periodontaltreatment with an Er:YAG laser”
November 2003Postgraduate Degree Oral Surgery
June 2005Habilitation Priv. Doz. postdoctorallecturer qualification
2k 2l2j2i
Fig. 2k:Placement of an implant in region 022(Straumann® Bone Level Implant, Ø 4.1,SLActive® 10mm) was also associatedwith the occurrence of a dehiscence-typedefect. Note the small decortications priorto the GBR procedure.
Fig. 2j:Adjustment of the healing abutment.
Fig. 2l:Reentry after 4 months of submerged heal-ing also revealed complete defect fill withnewly formed mineralized tissue exceedingand covering the implant neck.
Fig. 2i:Situation subsequent to careful removal ofthe crestal hard tissue bridge.
cium phosphate (BoneCeramic) or a collagen-coated natural bone mineral (BioOss Collagen):an immunohistochemical study in dogs. Int J OralMaxillofac Surg 2007;36:1198-1206.11Schwarz F, Rothamel D, Herten M, WustefeldM, Sager M, Ferrari D, Becker J. Immunohisto-chemical characterization of guided bone regen-eration at a dehiscence-type defect using differentbarrier membranes: an experimental study indogs. Clin Oral Implants Res 2008;19:402-415.12Jung RE, Jones AA, Higginbottom FL, WilsonTG, Schoolfield J, Buser D, Hämmerle CH,Cochran DL. The influence of non-matchingimplant and abutment diameters on radio-graphic crestal bone levels in dogs. J Periodontol2008;79:260-270.13Buser D, Halbritter S, Hart C, Bornstein MM,Grütter L, Chappuis V, Belser UC. Early ImplantPlacement with Simultaneous GBR FollowingSingle-Tooth Extraction in the Esthetic Zone12-Month Results of a Prospective Study with 20Consecutive Patients. J Periodontol (in press).14Schwarz F, Ferrari, Sager M, Wieland M,Becker J. Comparative study on bone regenera-tion in dehiscence-type defects at chemically mod-ified hydrophilic (SLActive®) or nanostructured(NanoTite®) titanium implants. An experimentalstudy in dogs (study finished).
Professional Experience
January 1999–October 2000Department of Periodontology andOperative Dentistry (Prof Dr E. Reich)University of Saarland, Homburg/Germany
November 2000–March 2002Research Associate Department of Oraland Maxillofacial Surgery (Prof DrDr M. Ehrenfeld) Ludwig MaximilianUniversity, Munich/Germany
since April 2002Assistant Professor Department ofOral Surgery (Prof Dr J. Becker),Heinrich Heine University, Düsseldorf/Germany
STARGET 1 I 1008 SLACTIVE® FOCAL POINT
STARGET_1_2010_en.indd 8STARGET_1_2010_en.indd 8 21.12.2009 17:34:45 Uhr21.12.2009 17:34:45 Uhr

STARGET 1 I 10 09FOCAL POINT SLACTIVE®
Spotlight on SLActive® at the31st APDC
This year’s 31st Asia Pacific DentalCongress (APDC) was held in May2009 in Hongkong SAR. At the sem-inar “Current concepts to improveosseointegration of titanium dentalimplants”, guest speakers Prof JürgenBecker and Dr Frank Schwarz fromthe Heinrich Heine University inDüsseldorf (Germany) presentedthe latest scientific research resultsemphasizing the outstanding clinicalbenefits of SLActive®. Furthermore,Prof Urs Brägger from the Univer-sity of Bern (Switzerland) and ProfNiklaus P. Lang from the Universityof Hong Kong SAR were lecturing
SLActive® goes EastSLActive® was launched in South Korea in June 2009 and received the long-awaited approval
by the regulatory authorities in the People’s Republic of China in September 2009.
Dr Frank Schwarz. The hands-on session at the Prince Philip DentalHospital of the University of Hong Kong, oneof the modules in the Speakers DevelopmentProgram.
Regional speakers with Dr Frank Schwarz and Prof Niklaus Lang.
Prof Dr Jürgen Becker at the APDC.
SLActive® Symposium in SouthKorea
The Straumann Symposium onSLActive® was held in Seoul, SouthKorea, on 8 May 2009 with thepurpose to introduce SLActive® tothe about 400 dental professionals.Key opinion leaders from Kyungheeand Yonsei Universities, and dentalclinics attended in order to listenand to meet Dr Schwarz lecturingon SLActive®. The audience wasimpressed by the study results on thecomparison of the surface propertiesbetween SLA® and SLActive® andalso between SLActive® and com-petitors’ surfaces.
Launch in South Korea and product clearance in the People’s Republic of China
about “The impact of CADCAMon dentists, dental technicians andpatients” and “Periodontal careaccording to patient needs” respec-tively in the scientific program.
SLActive® now available in9 Asian countries
Straumann’s premium implant sur-face is now available in 9 Asiancountries: South Korea, Taiwan,Hong Kong, Singapore, Thailand,Malaysia, Indonesia and the Philip-pines. With the product clearancereceived for the People’s Republicof China in September 2009, clini-cians and patients will benefit ofSLActive® in a further country.
Presentation of the Straumann® Dental Implant System in Seoul, South Korea.
STARGET_1_2010_en.indd 9STARGET_1_2010_en.indd 9 21.12.2009 17:34:47 Uhr21.12.2009 17:34:47 Uhr

1 million SLActive® implants sold
The success storyof Straumann’s premiumimplant surface
...over 1 million im
pl
ants
sold
!
Straumann® SLActive
STARGET 1 I 1010 SLACTIVE® FOCAL POINT
STARGET_1_2010_en.indd 10STARGET_1_2010_en.indd 10 21.12.2009 17:34:48 Uhr21.12.2009 17:34:48 Uhr

of the Medicines Authority there inSeptember 2009 and so is aboutto be introduced there (see alsoour report on page 9).
SLActive® – a decision for thehealth of your patients
The broad acceptance of SLActive®
evinced by dentists and cliniciansworking in the area of implant den-tistry is also apparent from the factthat Straumann now supplies onethird of all implants sold with theSLActive® surface. A further majormilestone in the SLActive® story wasreached in September 2009 afterthe 1 millionth SLActive® implant tobe sold was delivered.
firmed clinically. In numerous pre-clinical studies in which SLActive®
was also compared in dehiscencemodels2 and as regards shearstrength3, it proved to be significant-ly better compared to competitors’surfaces.
Awarded the “Medical DeviceTechnology Award 2005“
Because of these features, SLActive®
received the “Medical DeviceTechnology Award“ in 2005, whichis awarded every year by the inter-national market research companyFrost and Sullivan on the basis ofan assessment by an independentexpert committee for outstandingtechnological innovations and theirexemplary introduction.
Gradual worldwide introduction
From 2005 SLActive® was intro-duced gradually in different coun-tries. Since June 2009 cliniciansand patients in South Korea cannow benefit from the advantages.In the People’s Republic of ChinaSLActive® obtained the approval
Innovation and development are the engine that drives progress in
implant dentistry. However, only innovations that involve a genuine
added value and enable the previous range of indications to be
extended have the potential to become successfully established in
practice. SLActive® from Straumann is an example of such added
value.
1Straumann® DentalImplant System: Über-blick wissenschaftlicheForschung. Institut Strau-mann AG.2F. Schwarz, D. Ferrari,M. Wieland, M. Sager,J. Becker. An experi-mental study in dogs:Comparative study onbone regeneration indehiscence-type defectsat chemically modifiedhydrophilic (SLActive®)or nanostructured(NanoTite®) titaniumimplants.3J. Gottlow, S. Barkar-mo, L. Sennerby: Einebiomechanische undhistologische Studie anKaninchen.
Right from the start: clinically doc-umented and setting standards
Straumann® SLActive, the third gen-eration hydrophilic implant surface,has been notably successful sinceit was introduced to the market atthe EAO 2005 in Munich. From thestart, SLActive® was able to con-vince the professional world as itsoutstanding features were alreadyconfirmed by numerous preclini-cal studies when it came on themarket1. The advantages for usersand patients, such as improved pre-dictability and a shortened healingperiod of 3 to 4 weeks with a highsuccess rate, were repeatedly con-
STARGET 1 I 10 11FOCAL POINT SLACTIVE®
STARGET_1_2010_en.indd 11STARGET_1_2010_en.indd 11 21.12.2009 17:34:50 Uhr21.12.2009 17:34:50 Uhr

IPS e.max® CAD restorations byStraumann® CADCAM
The next step in the partnership with Ivoclar Vivadent AG:
Straumann presents the IPS e.max® CAD restorations by
Straumann® CADCAM – a highly esthetic solution for single
tooth replacement and restoration
The IPS e.max® CAD is an innovative lithium-disilicate glass-ceramic fromIvoclar Vivadent AG, an established specialist in ceramic materials andfinal restorations.
1Currently not availablein all countries
STARGET 1 I 1012 IPS E.MAX® CAD RESTORATIONS BY STRAUMANN® CADCAM FOCAL POINT
All-ceramic restorations for efficient estheticsVersatility for easy handlingHigh-strength product designed for reliable restorations
Efficient esthetics
Wide range of translucencies and shadesOptimal tooth design supported by etkon™_visual software(version 5.0 or higher)1 – e.g. Ivoclar Vivadent AG tooth databaseEfficient workflow for high-quality restorations
Easy handling
State-of-the-art software: user friendly and flexible applicationsVarious processing techniques: staining or layering techniqueFlexible cementation: adhesive, self-adhesive or conventional
Designed for reliable restorations
High-strength material: final flexural strength of 360 ± 60MPaCertified industrial milling center applying cutting-edge technologyfor an outstanding quality
STARGET_1_2010_en.indd 12STARGET_1_2010_en.indd 12 21.12.2009 17:34:51 Uhr21.12.2009 17:34:51 Uhr
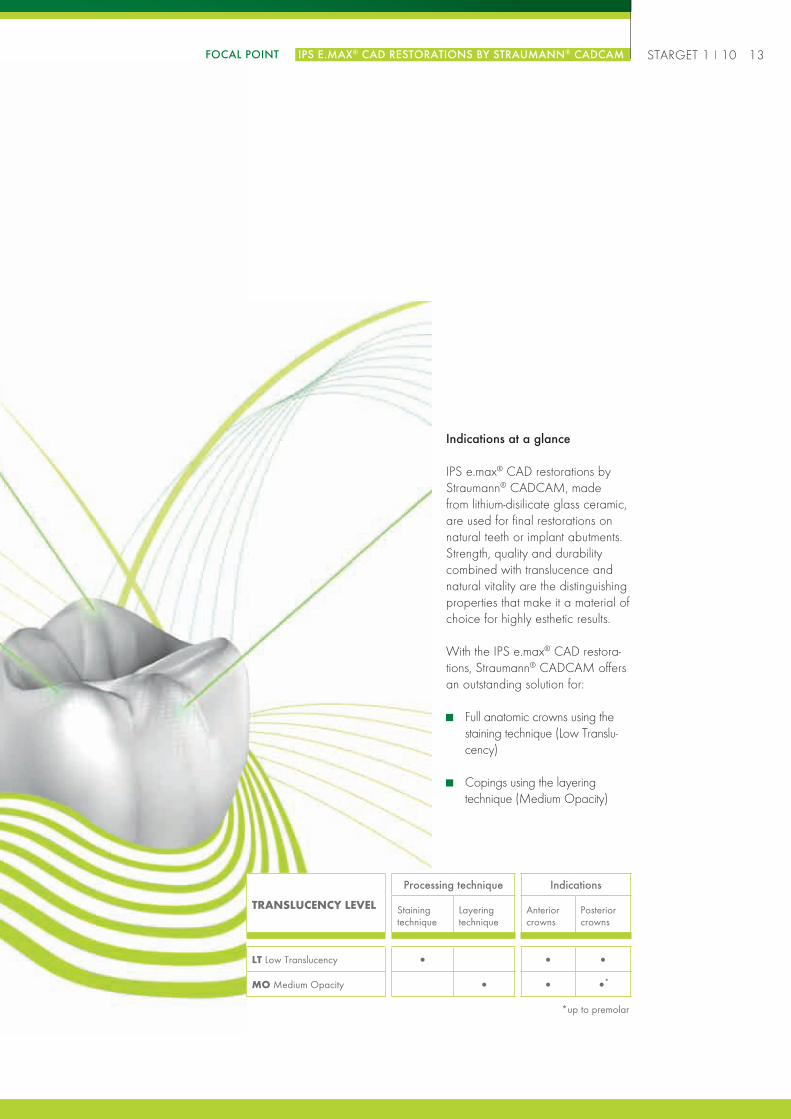
Indications at a glance
IPS e.max® CAD restorations byStraumann® CADCAM, madefrom lithium-disilicate glass ceramic,are used for final restorations onnatural teeth or implant abutments.Strength, quality and durabilitycombined with translucence andnatural vitality are the distinguishingproperties that make it a material ofchoice for highly esthetic results.
With the IPS e.max® CAD restora-tions, Straumann® CADCAM offersan outstanding solution for:
Full anatomic crowns using thestaining technique (Low Translu-cency)
Copings using the layeringtechnique (Medium Opacity)
STARGET 1 I 10 13FOCAL POINT IPS E.MAX® CAD RESTORATIONS BY STRAUMANN® CADCAM
TRANSLUCENCY LEVEL
Processing technique Indications
Stainingtechnique
Layeringtechnique
Anteriorcrowns
Posteriorcrowns
LT Low Translucency • • •
MO Medium Opacity • • •*
*up to premolar
STARGET_1_2010_en.indd 13STARGET_1_2010_en.indd 13 21.12.2009 17:34:52 Uhr21.12.2009 17:34:52 Uhr

In the Lab3D scan of the model anddesign of the restoration
Straumann® CADCAMProduction Center
Milling the framework
Completed frameworkReturned to the lab bylogistic service Scan data transmitted
via Internet
The Straumann® CADCAM SolutionThe 5th generation of the etkon™_visual software features the IPS e.max® CAD restorations by Straumann® CADCAM.
STARGET 1 I 1014 IPS E.MAX® CAD RESTORATIONS BY STRAUMANN® CADCAM FOCAL POINT
1STEP 1: The dental laboratory scans the model.
The etkon™ es1 scanner scans dies and models, acquiring jawand die situation data. With 28,000 precise scanning pointsper second, the etkon™ es1 scanner is highly accurate.
IPS e.max® lithium-disilicate glass-ceramic: excellent clinical performance
Ivoclar Vivadent’s lithium-disilicate glass-ceramic is a significant progress for the dental industry.
At the 39th Annual Session of the American Academy of Fixed Prosthodontics, P.C. Guess, R. Zavanelli, N. Silva, and V.P. Thompson(Researchers in the Department of Biomaterials and Biomimetics at the New York University College of Dentistry)2 presented theresults of their study using the mouth-motion-simulator test to compare the durability of IPS e.max® CAD lithium-disilicate full anatomiccrowns to veneered zirconium dioxide crowns (IPS e.max® ZirCAD/IPS e.max® Ceram).The NYU researchers replicated actual forces exerted in the human mouth to provide a more realistic assessment of how ceramicmaterials hold up to the chewing forces.
The research found that approximately 90% of veneered zirconium dioxide crowns (IPS e.max® ZirCAD/IPS e.max® Ceram) testedshowed chip-off fractures by a force of 350N independent of the number of cycles. None of the IPS e.max® CAD lithium-disilicatefull anatomic crowns showed fracture/chip through the lithium-disilicate crowns below 1,000N and 1 million cycles.As a conclusion, IPS e.max® CAD lithium-disilicate full anatomic crowns demonstrated excellent in vitro performance relative tochipping or fracture in comparison to veneered zirconium dioxide crowns (IPS e.max® ZirCAD/IPS e.max® Ceram).
2Mouth Motion Fatigue and Durability Study Petra C Guess, Ricardo Zavanelli, Nelson Silva and Van P Thompson, New York University, March 2009
STARGET_1_2010_en.indd 14STARGET_1_2010_en.indd 14 21.12.2009 17:34:53 Uhr21.12.2009 17:34:53 Uhr

2
STARGET 1 I 10 15FOCAL POINT IPS E.MAX® CAD RESTORATIONS BY STRAUMANN® CADCAM
Synthetic materials Metals Ceramics
STEP 2: The IPS e.max® CAD restoration by Straumann® CADCAM is designedwith etkon™_visual 5.03
Straumann® CADCAM offers a broad array of materials and an extensive application range.
3Please contact yourregional StraumannSales Point for informa-tion on availability inyour country.
polycon coron ticon zerion IPS e.max ® CAD
With the new module including theIPS e.max® CAD lithium-disilicateglass ceramic from Ivoclar VivadentAG, copings as well as full anatom-ic crowns can be designed easily.The restoration design is further sup-ported by various tooth databases,e.g. Ivoclar Vivadent SR Postarisand SR Vivodent.
To help the dental laboratory achieve an optimal restoration result, the etkon™_visual software supports the den-tal laboratory in producing a design of the IPS e.max® CAD restorations ordered from Straumann® CADCAMthat fulfills the specific guidelines of the material. If the recommended minimum thickness is not respected, thedynamic minimum wall thickness control immediately signals the relevant areas to the user, so that the restorationdesign can be improved easily.
STARGET_1_2010_en.indd 15STARGET_1_2010_en.indd 15 21.12.2009 17:34:54 Uhr21.12.2009 17:34:54 Uhr

STARGET 1 I 1016 IPS E.MAX® CAD RESTORATIONS BY STRAUMANN® CADCAM FOCAL POINT
The software automatically places the restoration in the material blank.Users can select the position of the retention pin, as this one can be ofcritical importance for the further processing and finalization of therestoration.
Once the design of the IPS e.max® CAD restoration by Straumann®
CADCAM is finalized, the restoration can be ordered.
3
4
STEP 3: Milling of the IPS e.max® CAD restorationsin the Straumann® CADCAM productioncentre
Thanks to its rigorous quality management system, continu-ous investment in its state-of-the-art production centers, aswell as development of new technologies, the Straumann®
CADCAM Solution is designed to deliver IPS e.max® CADrestorations of high quality.
STEP 4: Processing in the dental laboratory
The IPS e.max® CAD restorations by Straumann® CADCAM are delivered in their intermediate state(bluish color) to offer high versatility in the processing. Their final strength and esthetic are achieved afterthe crystallization and characterization process in the dental laboratory.
STARGET_1_2010_en.indd 16STARGET_1_2010_en.indd 16 21.12.2009 17:34:59 Uhr21.12.2009 17:34:59 Uhr

STARGET 1 I 10 17
Restoration delivered byStraumann® CADCAM
Restoration delivered by the dentallaboratory to the dental office
IPS e.max® CAD coping by Straumann® CADCAM:
1 million CADCAM elements sold since 2007
A comprehensive service with a full-range portfolio
Meeting international technical standards
Straumann entered the tooth restoration market in2007 through the acquisition of etkon, an emergingCADCAM company. With the global Straumannbrand and presence the business has expanded rap-idly and has now sold over a million elements.Straumann supplies CADCAM copings, crowns andbridges in a range of modern materials including
Straumann provides a comprehensive CADCAMservice, including a full range of CADCAM dentalprosthetics and related technology. The success ofits system is built on innovative CAD software, highprecision milling and powerful laser scanning technol-ogy. Easy to use, the etkon™_visual design softwareenables the dental technician to model prostheticsvia computer. The data are then transmitted via
Straumann® CADCAM is fully integrated and meetsFDA and ISO Medical Device Directive (MDD)
FOCAL POINT IPS E.MAX® CAD RESTORATIONS BY STRAUMANN® CADCAM
Restoration delivered byStraumann® CADCAM
Restoration delivered by the dental laboratoryto the dental office
IPS e.max® CAD crown by Straumann® CADCAM:
zerion™ (ceramic), ticon™ (titanium), coron™ (cobaltchrome), and polycon™ (polymer). The additionof IPS e.max® CAD lithium-disilicate glass ceramicenables the company to offer highly esthetic singletooth restorations in various shades and translucenciessupporting further the success of the Straumann® CAD-CAM solution.
Straumann to a high-speed milling center, which pro-duces the desired prosthetic component and sendsit to the lab for coloring and finishing. Straumann®
CADCAM offers a broad range of modern biocom-patible, durable and esthetic materials, includingstate-of-the-art highly esthetic ceramics such as IPSe.max® CAD restorations by Straumann® CADCAM.
standards, endorsing the high quality, esthetics andprecision for which Straumann is renowned.
STARGET_1_2010_en.indd 17STARGET_1_2010_en.indd 17 21.12.2009 17:35:01 Uhr21.12.2009 17:35:01 Uhr

Pure titanium is known for its bio-logical compatibility, but its strengthis limited. Therefore the clinicalusage of pure titanium implants isrestricted in specific cases. In orderto overcome this strength issueTi-6Al-4V alloys are used as well.These alloys show a better strengthbut they cannot accommodate arough/hydrophilic surface (likeSLA®/SLActive®), due to their metal-lic structure. The osseointegrationof these alloys is compromised asdocumented in various studies7–10.Now, with the combination of theRoxolid™ material and Straumann’s
High strength and excellentosseointegration
Roxolid™ is stronger than puretitanium1,2, the current material ofchoice for implants, and accommo-dates the chemically active surfaceSLActive®. The data gathered fromlaboratory tests and pre-clinicalstudies3,4 as well as the one-yearresults of two human studies5,6 haveunderlined its high strength andexcellent osseointegration proper-ties. The new material is used forStraumann implants with an endo-steal diameter of 3.3mm where
exactly this combination – strengthand osseointegration – is of highestimportance.
More confidence and peace ofmind with small diameter implants
Due to their size, high loads area critical factor for small diameterimplants. Existing approaches offerdifferent, but inadequate materialsolutions in order to meet thesespecific demands: pure titanium orTi-6Al-4V and other Titanium alloyscontaining Aluminum.
Roxolid™ – a new materialdesigned for the specific needsof implant dentistryImplants are exposed to high forces and need to osseointegrate. To meet these constantly increasing
demands in implant therapy, Straumann has developed a new and stronger metallic material with
excellent osseointegration properties: Roxolid™, an alloy of Titanium and Zirconium which was specifi-
cally designed for the needs of implant dentistry.
STARGET 1 I 1018 ROXOLID™
Fig. 1: Schematic depiction of the fatiguetest set-up
1. Block in which the implant is fixed2. Axes of the block3. Implant/abudment/crown system4. Block which creates cyclic force on
the abudmentF. Cyclic force on the system
Bone recession of 3mm is simulated
Biomechanical tests have beenperformed according to the ISO 14801 norm. Within this norm, the long-term survival load of an implant abut-ment system is measured. The systemis exposed to an angle of 30° to acyclic load acting with the frequencyof 15Hz. A worst case scenario issimulated where the implant has abone recession of 3mm. For eachload level 3 systems are tested. Thefatigue strength of a system is theload where three systems survived atleast 5 millions of load cycles withoutany damages.
30°
3Bone
Resorption
F
1
2
3
4
STARGET_1_2010_en.indd 18STARGET_1_2010_en.indd 18 21.12.2009 17:35:02 Uhr21.12.2009 17:35:02 Uhr

Roxolid™ implants have beenused for a wide range of treatmentoptions in a non-interventional study11
where different clinical situationswere treated with a variety of solu-tions. In this study, over 250 patientshave been treated and over 430implants documented. In many ofthese cases, Roxolid™ implants withsmall diameter were chosen due totheir specific benefits. Over 40% ofthese solutions could not be treatedbefore with small diameter implantsbecause the risks would have beentoo high – now, with Roxolid™ thesenew indication possibilities could befully exhausted. Only 2 implant fail-ures were reported to date.
SLActive® surface, a new situationhas been created. The new possi-bilities lead to more peace of mindfor specific treatments where smalldiameter implants have to be used.
Flexibility due to more treatmentoptions: choose the implantyou need, for the best solutionpossible
When treating their patients, clini-cians always want to make surethat they choose the best solutionpossible. This confidence is evenmore important when small diam-eter implants have to be used. WithRoxolid™, the clinician can choosefrom different implant types (softtissue level implants with taperedor with parallel walls and bonelevel implants) and a wide range ofStraumanns’ prosthetic components.
STARGET 1 I 10 19ROXOLID™
Fig. 2: Despite the smaller diameter, Roxolid™implants show higher fatigue strength (long-termsurvival) compared with other implants/abutment.When testing the competitive systems all the oth-ers implants failed(*), whereas with the Roxolid™Straumann® Bone Level Implant only the abut-ment fractured(**).
220
190
160
130
1002.9 3 3.1 3.2 3.3 3.4 3.5 3.6
diameter (mm)
Astra Osseospeed® 3.0S and TiDesign™ Abutment* Astra Osseospeed® 3.5S and TiDesign™ Abutment* NobelActive™ 3.5 andEsthetic Abutment* NobelReplace™ and Esthetic Abutment 3.5* Straumann® Bone Level Roxolid™ and Straumann® Anatomic Abutment**
Fatig
uestr
engt
h(N
)
1Norm ASTM F67 (states minimum tensile strengthof annealed titanium), used for all Straumanntitanium and Roxolid™ implants, data on file2Biomechanical tests performed according to ISO14 801 (15Hz in air, 5 million cycles survival)3Gottlow J et al. Preclinical data presented atthe 23rd Annual meeting of the Academy ofOsseointegration (AO), Boston, and at the 17th
Annual Scientific Meeting of the European Asso-ciation for Osseointegration (EAO), Warsaw4Thoma D et al‚ Evaluation of a new titanium-zirco-nium dental implant. A comparative radiographicstudy in the canine mandible, oral presentation atthe 24th Annual meeting of the Academy ofOsseointegration, San Diego5Stone P, oral presentation at the EAO 2009,Monaco6Al-Nawas B, oral presentation at the EAO 2009,Monaco7Wong M et al. J. Biomed Mater Res 1995;29:1567–15758Stenport VF, Johansson CB. Evaluations of bonetissue integration to pure and alloyed titaniumimplants. Clin Implant Dent Relat Res. 2008,10:191-99Johansson CB, Chong Hyun Han CH, WennerbergA, Albrektsson T. A Quantitative Comparison ofMachined Commercially Pure Titanium and Titani-um-Aluminum-Vanadium Implants in Rabbit Bone.Int J Oral Maxillofac Implants 1998;13:315–32110Steinemann S. “Titanium – the materials of choice?”Periodontology 2000, Vol. 17, 1998, 7-2111Data on file12Data from 2138 referrals in a survey conductedby Prof Gerhard Riegl from the “Institute of Health-care Management” in Augsburg, Germany (seealso p. 55–57)
STARGET_1_2010_en.indd 19STARGET_1_2010_en.indd 19 21.12.2009 17:35:03 Uhr21.12.2009 17:35:03 Uhr

Increasing the patients’ accept-ance by offering a comfortableimplant treatment
As patients’ requirements becomemore complex, dentists strive tooffer them the best solution possi-ble. By meeting the patients’ needs,the dentists can differentiate theirpractice through the benefits provid-ed by small diameter implants. Theyhave many advantages such as theapplication of a minimal invasivesurgery or the removal of only mini-mal bone in cases of an edentulousmandible. They are helpful when
Fig. 3: Only 58% of suitable cases lead into an implant-based therapy.
35
30
25
20
15
10
5
0referred cases suitable cases
Patie
nts
18
31
Clinical situation Implant solution Prosthetic solution Prosthetic options
Fully edentulous 2x3.3mmRoxolid™ implantsor more
Fixed dentureRemovable denture
BarLOCATOR®
Ball AnchorMagnetsSynOcta®
Partially edentulous 2x3.3mmRoxolid™ implantsor more
2 single crowns fordouble tooth gap2 or more unit bridge
Entire Straumann® SoftTissue Level portfolioEntire Straumann® BoneLevel portfolio
Single tooth 1x3.3mmRoxolid™ implant
Screw retained crownsCemented single crown
Entire Straumann® SoftTissue Level portfolioEntire Straumann® BoneLevel portfolio
Treatment options with Roxolid™ Ø 3.3mm implants
the maximization of bone supportand maintaining of the vascularity isrequired. Roxolid™ may offer alsogreater confidence when placingsmall diameter implants in patientswho are sceptical towards implanttreatment.
A market survey12 indicates that,out of all cases suitable, only 58%are treated with implants. With thebenefits offered by small diameterimplants it is now possible to offerto the patients the implant solutionthey were looking for.
STARGET 1 I 1020 ROXOLID™
STARGET_1_2010_en.indd 20STARGET_1_2010_en.indd 20 21.12.2009 17:35:03 Uhr21.12.2009 17:35:03 Uhr

For more information on Roxolid™ see also STARGET 1.2009, p. 4–18. www.straumann.com/starget
A strong scientific program forstrong scientific evidence
It has always been Straumann’smatter of principle that productsundergo a conscientious and
Overview of Roxolid™ lab tests and pre-clinical studies
extended research process startingin the laboratories before they arelaunched. The last step on this wayto marketability is clinical research.Roxolid™ went through a severescientific program with two clinical
studies at launch documenting theproduct with a 1-year follow-up.The entire clinical program forRoxolid™ includes over 400 patientswhich were treated with more than500 Roxolid™ implants.
Content Center(s)Model
indicationStatus
Labo
rato
ry/i
nvi
tro Biomechanical tests Internal Hydropulse Closed (Figure 2)
Corrosion test comparing variousbiomaterials
EMPA Material Closed
Cell culture comparing the osteo-genic and inflammory response ofvarious biomaterials
Internal Cell Closed
Ani
mal
trial
s
Measurements of osseointegrationat 4 wks3
Magneten,Malmö
Mini pigs Closed
Osseointegration at 2, 4 and8 wks4
UniversitySan Antonio
Fox hound Closed
Removal torque measurements fordifferent materials6
Magneten,Malmö
Rabbit Closed
Early bone healing after 3dand 2wks
University ofConnecticut
Mini pigs On-going
Early healing behaviour comparingdifferent materials: tissue morphologyand osseointegration
University of Berne Mini pigs On-going
Clin
ical
stud
ies
Pilot study of implant new material5 2 centers in UK Part. Edentulous 22 patients1 yr FU
Multi Center Study comparingRoxolid™ vs. Ti6
8 centers inEurope
Full edentulous 91 patients1 yr FU
Roxolid™ in the daily practice(NIS)6,11
over 50 centers in EUand US
Various Over 250 patientsRecruitment closed
Show reduced need of augmentati-on and measure quality oflife of patients with hypodontia
University of Cork Hypodontia 20 patientsin preparation
Comparison Roxolid™ 3.3mmvs. Ti 4.1mm
Zurich/Harvard Part. Edentulous 40 patientsRecruitment
Performance of Roxolid™ implantsfor single tooth replacement innarrow spaces
University of Berne Single tooth 40 patientsRecruitment
Performance of Roxolid™ implantsfor the anterior region
Mayo Clinic Various In preparation
STARGET 1 I 10 21ROXOLID™
STARGET_1_2010_en.indd 21STARGET_1_2010_en.indd 21 21.12.2009 17:35:05 Uhr21.12.2009 17:35:05 Uhr

Reduced-diameter implants asa treatment alternative in risk patientsto avoid augmentation procedures
by Prof Dr Hannes P. Schierle, Dr Hans O. Werner, dentist Franziska Nagel
New implant material for extend-ed indication where bone supplyis limited
The ITI began very early on tomake strict demands with regard tothe diameter of implants for treatingdifferent indication classes. On theone hand, this gave the cliniciana certain safety margin as regardsthe employed implant componentsbut on the other hand, a restorationthat complied with the ITI was oftenpossible only after previous andsometimes complex augmentation.With the development of Roxolid™,the new implant material, we are
1 32
Fig. 1:Initial clinical situation.
Fig. 3:OPG with X-ray gauge and drill template.
now able to treat even situationswith a limited bone supply in unu-sual indications without comprehen-sive augmentation measures.
Case description
This case describes the treatment ofa 52-year old patient with severeosteoporosis of the skeletal system,who was on a daily dose of 150mg of Bonviva (oral bisphospho-nate). She was not a smoker.
Her wish was for a fixed dentalprosthesis but this could not be metin the conventional prosthetic way
Fig. 2:Initial radiographic situation.
because of the abutment situation.Because of the previous history,apicectomies had been performedon teeth 24 and 26 and in con-junction with the final extraction ofthe teeth this had led to loss of thebuccal layer of the alveolar proc-ess in this region. Harvesting ofa bone block and other invasivemeasures to prepare the implantsite were declined by the patientout of concern regarding compli-cations because of her existingunderlying disease and medication,and she also declined a two-stageprocedure.
STARGET 1 I 1022 ROXOLID™
STARGET_1_2010_en.indd 22STARGET_1_2010_en.indd 22 21.12.2009 17:35:05 Uhr21.12.2009 17:35:05 Uhr

adequately restored prostheticallyand conservatively. Teeth 16, 15and 45 had had endodontic treat-ment. There were no occlusionproblems and the functional param-eters were in the normal range.
Diagnosis
A saddle area in region 24–26,vertical alveolar ridge atrophy inregion 26, bone deficit in the trans-verse direction in region 24–26with deficit of the buccal layer at24.
Findings
The clinical and radiographicexamination shows moderate gen-eralized horizontal bone atrophy inthe maxilla and mandible and atro-phy of the alveolar process in thevertical dimension of region 26 withloss of the buccal layer at 24–25(Figs. 1, 2).
There was no increased toothmobility and the probing depthswere not in the pathological range.The patient’s oral hygiene at homecould be classified as good andthe reduced residual dentition was
Treatment planning
To restore the saddle area inregion 24 to 26, an implant-bornebridge was planned with implantsin positions 24 and 26. The treat-ment plant provided for sinus flooraugmentation in region 26 via afacial approach. Teeth 24 and26 had been removed approxi-mately 12 weeks before the startof treatment. The residual bonesupply was considered adequateto allow a single-stage procedure.Insertion of a reduced-diameterimplant in region 24 was planned.This was intended to circumvent an
7 8
Fig. 6:Lateral bone window in region 26 for opensinus lift.
Fig. 7:Membrane pushed in on palatal side.
Fig. 8:Membrane only applied.
Fig. 4:Available bone clinically.
Fig. 5:Use of the Safescraper. 54
6
STARGET 1 I 10 23ROXOLID™
STARGET_1_2010_en.indd 23STARGET_1_2010_en.indd 23 21.12.2009 17:35:06 Uhr21.12.2009 17:35:06 Uhr

9 10 11
onlay bone graft in the form of abone plug or extension graft in thisregion. The planning documenta-tion consisted of study models,X-ray gauge and drill template,and orthopantomograph with X-raygauge and drill template (Fig. 3).
Surgical procedure
The bony structures were firstexposed through a ridge incisionwith a mesial relieving incision onthe vestibular aspect, sparing thepapilla distal to 23 and leaving it insitu (Fig. 4). The facial window forsinus augmentation was first dissect-ed extensively with a bone scraper(Safescraper® twist), and the areaof dissection was extended as faras the cranial regions of the zygo-maticoalveolar crest (Fig. 5).
The next step was preparation ofthe lateral window for sinus floorelevation with a spherical diamondbur. The site was prepared for sinusaugmentation by dissecting offthe schneiderian membrane in all
three spatial directions, first fillingthe space palatal to implant 26with bone chips from the zygoma-ticoalveolar crest. With the drilltemplate inserted, pilot holes werethen drilled in regions 24 and 26.Because of the very spongy andsoft type III bone quality, subse-quent preparation of the implantbed was with osteotomes. Aninnovative bone level implant witha reduced diameter (Ø 3.3mm,SLActive® 12 mm) made of titaniumand zirconium (Roxolid™) wasinserted in region 24. A Strau-mann® NC Bone Level Implant wasinserted in region 26 (Ø 4.1mm,SLActive® 10mm). Following inser-tion there was a facial fenestrationdefect in region 24 (Figs. 7, 8).This defect was covered with amixture of autologous bone chipsand blood. The remaining bonechips were used together with ahemostyptic to reinforce the sinusfloor (Figs. 6, 7).
Membrane for GBR technique
An absorbable membrane wasthen applied to the facial bonedefect in region 24 and the accesswindow in region 26 for protec-tion and to stabilize the position ofthe graft (Figs. 7, 8). The woundwas closed with interrupted sutures.The postoperative OPG shows thepositioning of the inserted implants,which corresponds with the optimalprosthetic position given by the drilltemplate.
Exposure
After a healing period of about 10weeks, the implants were exposed.The OPG after exposure showsvery good peri-implant bone, espe-cially crestally in the area of theimplant shoulders (Fig. 11).
Prosthetic restoration
Prosthetic restoration took placeafter an interval of 2 weeks follow-ing exposure. Figs. 12 and 13
Fig. 9:Tight suture closure.
Fig. 10:OPG for postoperative check.
Fig. 11:OPG after exposure of the implants and screwingin the gingiva former.
References
Barter S et al. Clinicalresults presented at the17th annual scientificmeeting of the Euro-pean Association forOsseointegration (EAO),Warsaw, September2008
Gottlow J et al. Preclini-cal data presented atthe 23rd annual meet-ing of the Academy ofOsseointegration (AO),Boston, February 2008,and at the 17th AnnualScientific Meeting of theEuropean Association forOsseointegration (EAO),Warsaw, September2008
Buser D, von Arx Th,ten Bruggenkate Ch,Weingart D. “Basicsurgical principles withITI implants” ClinicalOral Implants Research,Volume 11, Supplement1, Blackwell Publishing,September 2000, pp.59-68(10)
STARGET 1 I 1024 ROXOLID™
STARGET_1_2010_en.indd 24STARGET_1_2010_en.indd 24 21.12.2009 17:35:07 Uhr21.12.2009 17:35:07 Uhr

Fig. 13:Prosthetic restoration II.
Prof Dr H. P. Schierle
Specialist in oral and maxillofacial sur-gery and plastic surgery
Oral surgery practice in Karlsruhe andLandau/Germany
Teaching contract at the Medical Col-lege Hannover/Germany
Director of several postgraduate coursesin oral surgery and implantology
Continuing education consultant
Dr H. O. Werner
Specialist in oral and maxillofacialsurgery
Oral surgery practice in Karlsruhe andLandau/Germany
Continuing education consultant
Franziska Nagel
Specialist resident in oral surgery,Karlsruhe and Landau/Germany
Fig. 12:Prosthetic restoration I.
12 13
show the completed restoration 6months after implant insertion.
Conclusion
The ideal restoration with a fixedimplant-borne dental prosthesis con-
tinues to be based on conditioningthe hard and soft tissue structureswith a view to the final prostheticresult. Deviation from this concept ispossible in special cases in agree-ment with the patient and outsidethe esthetic area. However, in
order to avoid compromises withregard to the long-term stability,the new Roxolid™ implant materialfrom Straumann represents an idealaddition to the Straumann® DentalImplant System.
STARGET 1 I 10 25ROXOLID™
STARGET_1_2010_en.indd 25STARGET_1_2010_en.indd 25 21.12.2009 17:35:08 Uhr21.12.2009 17:35:08 Uhr

STARGET 1 I 1026 PRODUCTS
Exchanging first experienceswith the Straumann® AnatomicIPS e.max® Abutment
Gathering experiences withhighly esthetic, prefabricatedanatomic ceramic abutments
The Straumann® Anatomic IPSe.max® Abutment is a standardizedpremium ZrO2 ceramic abutment,designed for high esthetics andstrength. The abutment featuresa prepared mucosa margin foradaptation to natural soft tissuecontour. Esthetic results are cruciallydetermined by successful soft tissuemanagement. The emergence pro-file of the Straumann® Anatomic IPSe.max® Abutment is in compliancewith the Consistent EmergenceProfiles™ of the Straumann® Bone
Level Implant line. The implant-abut-ment connection of the Straumann®
Anatomic IPS e.max® Abutmentfeatures the Straumann® CrossFit™Connection. The Straumann® Ana-tomic IPS e.max® Abutment is avail-able in 2 shades. It is indicated forcement-retained crowns and bridg-es via mesostructure, and for directveneered screw-retained crowns.With the use of the Straumann®
Anatomic IPS e.max® Abutment therestorative team can apply an ana-tomically formed, ZrO2 abutmentand make first steps and experi-ences with highly esthetic, prefabri-cated anatomic ceramic abutments,which might build the basis for
At the IDS 2009 in Cologne, Straumann introduced the Straumann® Anatomic IPS e.max® Abutment,
the first product resulting of a strategic cooperation between Institut Straumann AG and Ivoclar Vivadent
AG. To generate first clinical experiences and outcomes with this new product, Institut Straumann AG
and Ivoclar Vivadent AG had jointly formed a European Expert Team at the beginning of 2009, com-
posed of Dental Technicians and Prosthodontists. At the end of August, a part of the Expert Team met at
Straumann Headquarters in Basel to exchange first experiences with the new abutment.
EXPERT TEAM MEETING
August 27, 2009 in Basel at Straumann Headquarters
STARGET_1_2010_en.indd 26STARGET_1_2010_en.indd 26 21.12.2009 17:35:10 Uhr21.12.2009 17:35:10 Uhr

STARGET 1 I 10 27PRODUCTS
future use of advanced CADCAMceramic technologies such as theStraumann® CADCAM System.
The expert team
The expert team for the practicaltesting and discussion of theStraumann® Anatomic IPS e.max®
Abutment was formed on the initia-tives of both Straumann and IvoclarVivadent AG. To get an extensiverange of experiences on the broadapplication range of the Strau-mann® Anatomic IPS e.max® Abut-ment, the expert team was com-posed to represent a broad clinicaland technical background. Severalcases were presented at the ExpertTeam meeting at Straumann inBasel in August 2009. The presen-tations included a short overviewof all cases the restorative team
Participants (in alphabetical order): Prof U. Belser, Dr A. Boesch, PD Dr S. Eitner, D. Vinci, Dr J. Wittneben-Matter.
Cases by: Prof U. Belser, V. Brosch, Dr P. Couto Viana, PD Dr S. Eitner, D. Vinci, Prof U. Brägger, A. Bruguera, Dr J. Fabrega,Dr R. di Felice, B. Heckendorn, M. Temperani, Dr J. Wittneben-Matter.
had completed and a detaileddocumentation of one case withmain focus on the case planningand surgical operation as well asdental laboratory procedures andoutcomes.
Summary of the experiencesshared and conclusions
All presenters were greatly satisfiedwith the overall result of the resto-ration. The properties of the abut-ment and the material allow for acomfortable processing which wasdone in the dental lab in all thecases. The anatomically pre-shapedabutment in combination with theStraumann® Bone Level advantagesenabled an efficient preparationprocedure in the dental lab and afamiliar, standardized restorativeworkflow. Both, screw retained and
A selected case from the ExpertTeam with detailed information onthe restorative process, includingan IPS e.max® restoration, will bepresented in STARGET 2.2010.
cemented restorations have beenreported (70% screw-retained,30% cemented) but the result wasidentical: a highly esthetic dentalprosthesis. The shaded MO1colour was more frequently used(80%) than the white MO0 (20%).Thanks to the possibility to selectbetween a white or natural shadecolour in combination with the trans-lucency of the material, estheticwas achieved. The Straumann®
Anatomic IPS e.max® Abutmentoffers user and patients advantageslike higher esthetics, efficiency andthe certainty of predictable results.
STARGET_1_2010_en.indd 27STARGET_1_2010_en.indd 27 21.12.2009 17:35:15 Uhr21.12.2009 17:35:15 Uhr

Straumann® Temporary Abutments
With its narrow diameter, the new Straumann® Temporary Abutment for the Straumann® Bone Level
Implant opens up more restoration possibilities for narrow interdental spaces. For crowns and bridges,
screw or cement-retained in the anterior and posterior region.
Engaging abutments are used forScrew- or cement-retainedtemporary crownsCement-retained temporarybridges
Non-engaging abutments areused for
Screw-retained temporarybridges
STARGET 1 I 1028 PRODUCTS
Your solution for narrow spaces
STARGET_1_2010_en.indd 28STARGET_1_2010_en.indd 28 21.12.2009 17:35:16 Uhr21.12.2009 17:35:16 Uhr
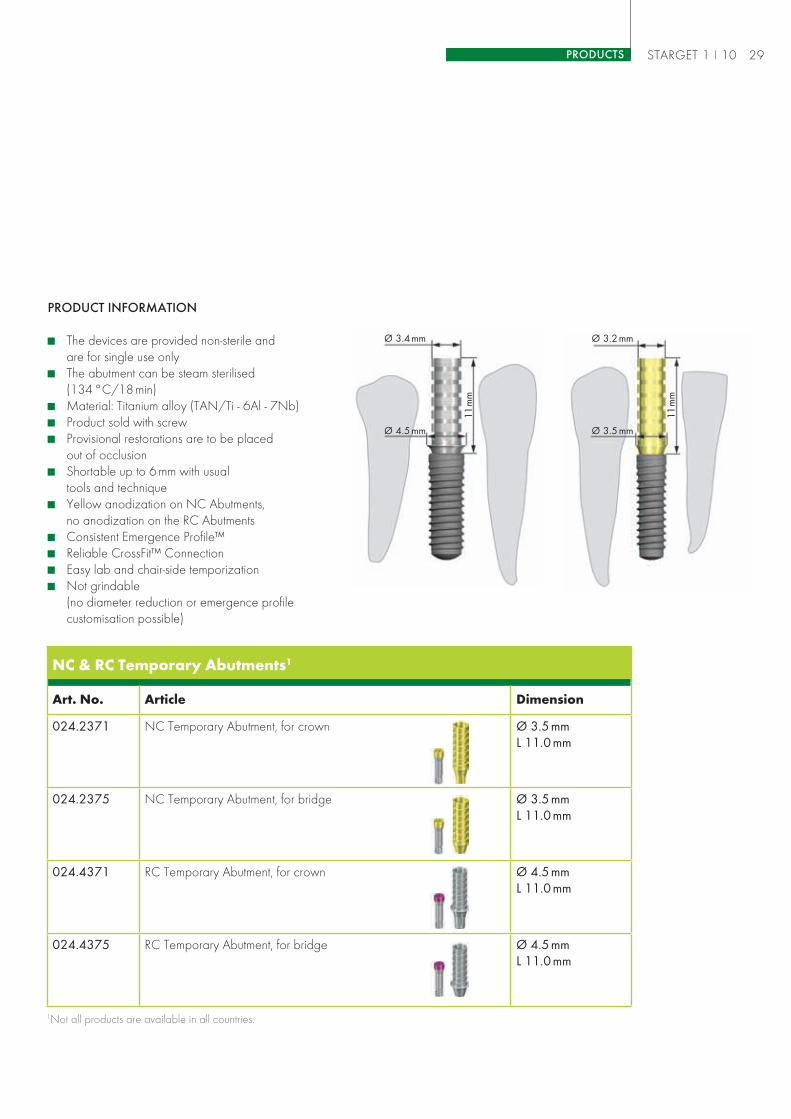
PRODUCT INFORMATION
The devices are provided non-sterile andare for single use onlyThe abutment can be steam sterilised(134 °C/18 min)Material: Titanium alloy (TAN/Ti - 6Al - 7Nb)Product sold with screwProvisional restorations are to be placedout of occlusionShortable up to 6 mm with usualtools and techniqueYellow anodization on NC Abutments,no anodization on the RC AbutmentsConsistent Emergence Profile™Reliable CrossFit™ ConnectionEasy lab and chair-side temporizationNot grindable(no diameter reduction or emergence profilecustomisation possible)
STARGET 1 I 10 29PRODUCTS
NC & RC Temporary Abutments1
Art. No. Article Dimension
024.2371 NC Temporary Abutment, for crown Ø 3.5mmL 11.0mm
024.2375 NC Temporary Abutment, for bridge Ø 3.5mmL 11.0mm
024.4371 RC Temporary Abutment, for crown Ø 4.5mmL 11.0mm
024.4375 RC Temporary Abutment, for bridge Ø 4.5mmL 11.0mm
1Not all products are available in all countries.
Ø 3.4mm Ø 3.2mm
11m
m
11m
m
Ø 4.5mm Ø 3.5mm
STARGET_1_2010_en.indd 29STARGET_1_2010_en.indd 29 21.12.2009 17:35:21 Uhr21.12.2009 17:35:21 Uhr

Be perfectly organized in yourdental lab and practice
STARGET 1 I 1030 PRODUCTS
New packaging for non-sterile packaged components
When dealing with medical devices, both manufacturer and end userare facing specific challenges. In order to completely satisfy these require-ments, we have improved our packaging for non-sterile products.
NEW PACKAGING CONCEPT/STRAUMANN® STORAGE SYSTEM PROSTHETICS
The new blister packaging is stack-able and fits perfectly with the newStorage System Prosthetics.
In accordance to our motto “SimplyDoing More,” our detailed prod-uct documentation on instructionleaflets will now be available in10 languages, the packaging/insert labels in 6 languages. Strau-mann thus addresses the languageguidelines for medical devices byensuring that their products are incompliance with international stand-ards like EN 980 and ISO 15223
and, most importantly, again strivesto satisfy the high demands of itscustomers.
The benefits of this new conceptare a better time management andless expenses in your dental lab orpractice.
Our new packaging offers you some significant advantages:
Quick access to the right productEasier identification due to multi-language labels with pictogramsBetter control of your inventory
STARGET_1_2010_en.indd 30STARGET_1_2010_en.indd 30 21.12.2009 17:35:23 Uhr21.12.2009 17:35:23 Uhr

STARGET 1 I 10 31PRODUCTS
For an even greater increase in efficient organizing, you may also wantto consider the “Straumann® Storage System Prosthetics”.
Product details
L/W/H: 22.6/28/24.8cm
The “Straumann® Storage SystemProsthetics” is delivered with its3 standard drawers. Extra compo-nents can be ordered additionallyaccording to your personal needs.
Product availability
Please ask your Straumann SalesRepresentative on the availabilityof the “Straumann® Storage SystemProsthetics” in your country. He willbe happy to make you an offer.
STARGET_1_2010_en.indd 31STARGET_1_2010_en.indd 31 21.12.2009 17:35:24 Uhr21.12.2009 17:35:24 Uhr

the implant. These assumptions areastonishing and raise the question ofwhy the authors in their evaluationdid not discuss the clinical studiesalready available at that time, allthe more as there are clinicallywell-founded and internationally con-firmed long-term data (> 10 years)for the Straumann® Dental ImplantSystem, which clearly call into ques-tion the findings of the Zipprich study(see box).
In order to assess the relevance ofthe study scientifically, Straumannasked the Dental Faculty of BonnUniversity for an independent expertopinion on Zipprich’s study.
Expert opinion on the study byHolger Zipprich et al.1
Straumann attaches the greatestvalue to the scientifically groundedand clinical testing of all productsand components of the Straumann®
Dental Implant System. As a pio-neer in the field of implant-support-ed restoration, Straumann accord-ingly has comprehensive long-termclinical data on dental implants andthe corresponding prosthetic com-ponents. This applies particularlyto the Straumann® Soft Tissue LevelImplant line, which is among themost frequently employed systemstested in clinical practice world-wide. This implant line is valued bydentists especially because of themany years of clinical evidenceand simplicity.
The in vitro study by Holger Zip-prich was published in 2007 onlyin the German journal “Implantolo-
gie” and since then it has beenpresented repeatedly at industryevents. Interestingly, nothing canbe found in professional journalsabout the corresponding scientificdiscussion with professionals on aninternational level of the methodol-ogy and results.
Subject of the Zipprich study
The in-vitro study in question byHolger Zipprich investigated theconnection between implant andabutment. Because of the move-ments between implant and abut-ment measured in the one-off studydesign in some of the tested implantsystems, the author suppose that themovements between the two com-ponents could have a micro-pumpeffect, which would lead indirectly toincreased bone resorption around
Institut Straumann AG has obtained an independent expert opinion from the Dental Faculty Bonn
on the study by Dipl. Ing. Holger Zipprich et al.
INFORMATION
1Zipprich et al., Erfas-sung, Ursachen undFolgen von Mikrobe-wegungen am Implan-tat-Abutment-Interface(Detection, causesand consequences ofmicro-movements atthe implant-abutmentinterface). Implantologie2007; 15 (1): 31–46.
2Prof. Dr.rer.nat. Dipl.-Phys. Christoph Bouraueland Dr.rer.nat. Dipl.-Math. Ludger Keilig.
3Hermann JS, Buser D,Schenk RK, Cochran DL.Crestal bone changesaround titanium implants.A histometric evaluationof unloaded nonsub-merged and submergedimplants in the caninemandible. J Periodontol2000; 71: 1412-1424.
STARGET 1 I 10 PRODUCTS32
STARGET_1_2010_en.indd 32STARGET_1_2010_en.indd 32 21.12.2009 17:35:26 Uhr21.12.2009 17:35:26 Uhr

Conclusions of the Dental Facultyof Bonn University
The two experts2, both with manyyears of experience in orthodonticbiomechanics and implant andprosthetic biomechanics and materi-als science, came to the followingconclusions in their critical assess-ment of the Zipprich study:
Direct application of the in-vitroresults of the study to clinicalpractice is inadmissible, as men-tioned in the study.
The study design deviates mark-edly from the standards (DIN/ISO 14801) stipulated for test-ing dental implants. Because ofthe great clinical relevance ofthe topic, it is essential that thecomparability (that is, a studydesign in accordance with thestipulated standards) can beguaranteed with further investi-gations.
It is not clear to what extent theinvesting of the implants wasin accordance with DIN/ISO14801, which raises questionswith regard to the applicationof load, in the case of bothsoft tissue level and bone levelimplants.
The spatial resolution of the imag-ing method used in the study was4μm. In the study, a distinction ismade between an undetectablegap and a gap of 0.1–4.0μm.Through this, it is suggested thatconclusions might be drawnabout measurements with anaccuracy of 0.1μm. Correspond-ing interpretations as a result areinadmissible and produce falseideas in the reader.
The study lacks completely acritical consideration of theextent to which the design ofthe crown, the cementing of thecrown or other clinical frame-work conditions can have an
influence on the movementsbetween implant and abutment(gap size).
In summary, the experts foundthat:
“The clinical relevance of the pre-sented results can therefore only bedoubtful, especially as concerns atechnical failure of the implant-abut-ment system or a possible tissuereaction suggested by the authors.Clear evidence of a connectionbetween micro-gaps depending onthe implant-abutment system andtechnical failure or a tissue reactioncannot be identified, especially asthe authors themselves refer to thereports of success in the literature“.
A copy of the expert opinioncan be requested from InstitutStraumann AG.
STARGET 1 I 10PRODUCTS 33
STARGET_1_2010_en.indd 33STARGET_1_2010_en.indd 33 21.12.2009 17:35:27 Uhr21.12.2009 17:35:27 Uhr
STARGET 1 I 10 PRODUCTS34
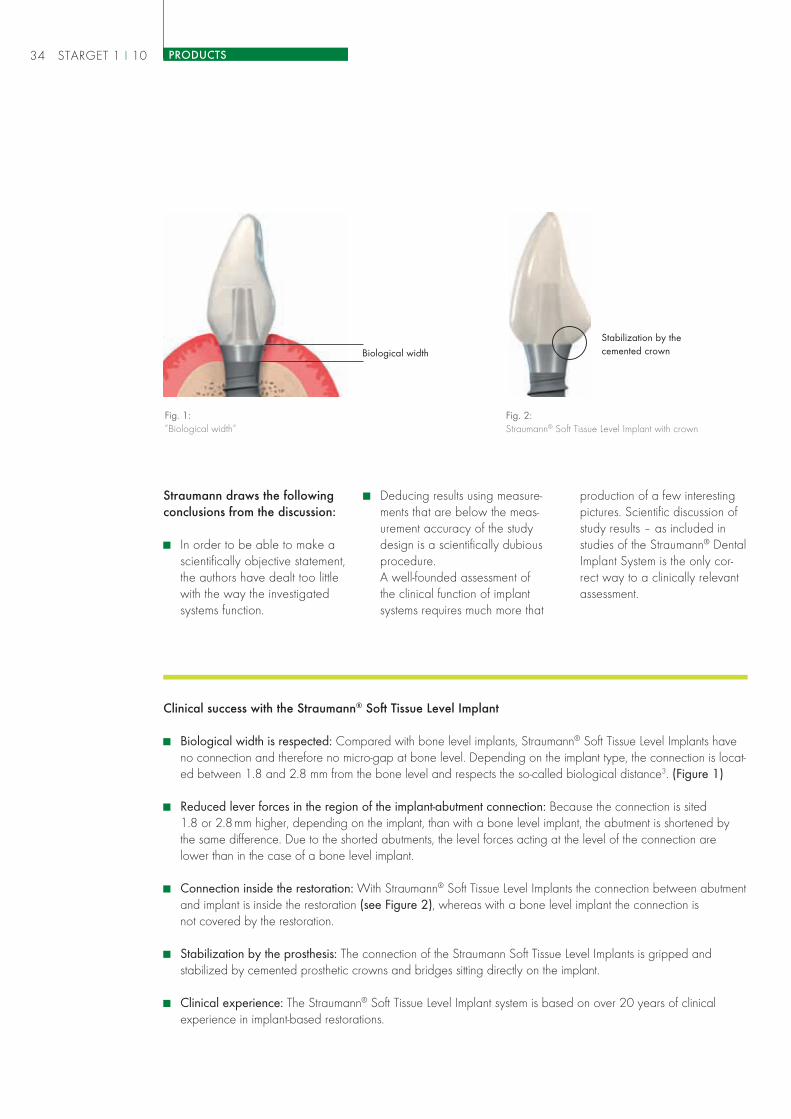
Clinical success with the Straumann® Soft Tissue Level Implant
Biological width is respected: Compared with bone level implants, Straumann® Soft Tissue Level Implants haveno connection and therefore no micro-gap at bone level. Depending on the implant type, the connection is locat-ed between 1.8 and 2.8 mm from the bone level and respects the so-called biological distance3. (Figure 1)
Reduced lever forces in the region of the implant-abutment connection: Because the connection is sited1.8 or 2.8mm higher, depending on the implant, than with a bone level implant, the abutment is shortened bythe same difference. Due to the shorted abutments, the level forces acting at the level of the connection arelower than in the case of a bone level implant.
Connection inside the restoration: With Straumann® Soft Tissue Level Implants the connection between abutmentand implant is inside the restoration (see Figure 2), whereas with a bone level implant the connection isnot covered by the restoration.
Stabilization by the prosthesis: The connection of the Straumann Soft Tissue Level Implants is gripped andstabilized by cemented prosthetic crowns and bridges sitting directly on the implant.
Clinical experience: The Straumann® Soft Tissue Level Implant system is based on over 20 years of clinicalexperience in implant-based restorations.
Fig. 1:“Biological width“
Fig. 2:Straumann® Soft Tissue Level Implant with crown
Biological width
Stabilization by thecemented crown
Straumann draws the followingconclusions from the discussion:
In order to be able to make ascientifically objective statement,the authors have dealt too littlewith the way the investigatedsystems function.
Deducing results using measure-ments that are below the meas-urement accuracy of the studydesign is a scientifically dubiousprocedure.A well-founded assessment ofthe clinical function of implantsystems requires much more that
production of a few interestingpictures. Scientific discussion ofstudy results – as included instudies of the Straumann® DentalImplant System is the only cor-rect way to a clinically relevantassessment.
STARGET_1_2010_en.indd 34STARGET_1_2010_en.indd 34 21.12.2009 17:35:27 Uhr21.12.2009 17:35:27 Uhr

Straumann® Bone Level Implantlaunched in Brazil
Brazil is one of the world’s largestmarkets for many segments of theesthetic health care sector, bothmedical and dental. Therefore, thelaunch of the Straumann® BoneLevel Implant line will close animportant gap for local implanto-logists.
Straumann Brazil gave their targetgroups an opportunity for earlyexperience through a series oflectures throughout Brazil. The“Science and Esthetic” tour, whichstarted in September, is a roadshow that was developed by fiveleading experts of the Straumann®
Dental Implant System (Professors
Alessandro Januário, Julio Joly,Mauricio Araújo, Pedro Tortamanoand Waldemar Polido) and aimsto provide key information to Brazil-ian dental professionals on implantselection criteria, supported withsolid scientific background andlocal clinical cases.
The official launch of the
Straumann® Bone Level Implant
in Brazil was celebrated at the
national congress “Osseointe-
gration – 20 Years of the
Brazilian Experience” on Sep-
tember 3–5 in São Paulo with
over 3,000 guests.
Impressions from the congress“Osseointegration – 20 Years of theBrazilian Experience” in São Paulo.
STARGET 1 I 10PRODUCTS 35
STARGET_1_2010_en.indd 35STARGET_1_2010_en.indd 35 21.12.2009 17:35:28 Uhr21.12.2009 17:35:28 Uhr

Synergies for clinical success with an osteo-conductive implant surface and bone replacementgraft, a novel implant-abutment connection andmeticulous occlusal therapyby Barry P. Levin, DMD
Initial situationThe patient, a 69 year old female with a non-contributory medical history, presented
for a comprehensive periodontal and implant consultation in March of 2008.
Her maxillary molar teeth hadbeen missing for over 5 years afterprevious periodontal therapy wasperformed. Her remaining maxillarydentition demonstrated significantperiodontal attachment loss andmoderate posterior pocketing.Mobility and esthetic compromise
1
3 4 6 85 7
2
STARGET 1 I 1036 CLINICAL CASES
were the patient’s chief complaints(Figs. 1, 2).
The decision was made to extractthe remaining maxillary teeth andplace 6 implants to support a fixedrestoration.
A digital CT scan was taken toassess available bone volume anddensity and assist in implant selection.The cross-sectional slices were alsoused to verify the probability of verti-cal placement and screw retention ofthe provisional prosthesis prior to thestart of treatment (Figs. 3–10).
Fig. 3: Site #4 Fig. 4: Site #6 Fig. 5: Site #8 Fig. 6: Site #9 Fig. 7: Site #11 Fig. 8: Site #13
STARGET_1_2010_en.indd 36STARGET_1_2010_en.indd 36 21.12.2009 17:35:30 Uhr21.12.2009 17:35:30 Uhr

1311
14
12
15
Figs. 11–13:Lab procedure
Figs. 14–16:Surgial procedure
10
Fig. 10:Axial CT view of maxilla.
9
Fig. 9:Panoramic radiograph.
Lab procedure
Prior to the patient’s surgical appoint-ment, the restorative dentist obtainedstudy models and an occlusalregistration. From these models, amodified maxillary denture and clearacrylic surgical guide were fabri-cated (Figs. 11–13).
Surgical procedure
The stent was utilized to position6 Straumann® Bone Level Implantswith SLActive® surface in the sec-ond bicuspid, canine and centralincisor locations bilaterally. Animplant surface with high surfaceenergy has been demonstrated
16
STARGET 1 I 10 37CLINICAL CASES
in animal and human studies toachieve an accelerated rate ofosseointegration. This providesa shorter healing period duringwhich the patient must demonstratecompliance with a very soft diet.In approximately 3–4 weeks, thepatient may begin gradually incor-porating a more normal dietaryintake. With machined surfaces ormore traditional roughened surfac-es, the time to achieve osseointe-gration may be significantly longer(3–6 months).
Following minor flap reflection, all12 maxillary teeth were carefullyremoved, with great attention topreserving the thin alveolar bone(Fig. 14). Six Straumann® RCBone Level implants (Ø 4.1mm/SLActive® 12.0mm) were placedaccording to the standard protocol,all achieving primary stabilization(Figs. 15, 16).
The voids between the implantbodies and residual socket wallswere obturated with Straumann®
STARGET_1_2010_en.indd 37STARGET_1_2010_en.indd 37 21.12.2009 17:35:33 Uhr21.12.2009 17:35:33 Uhr
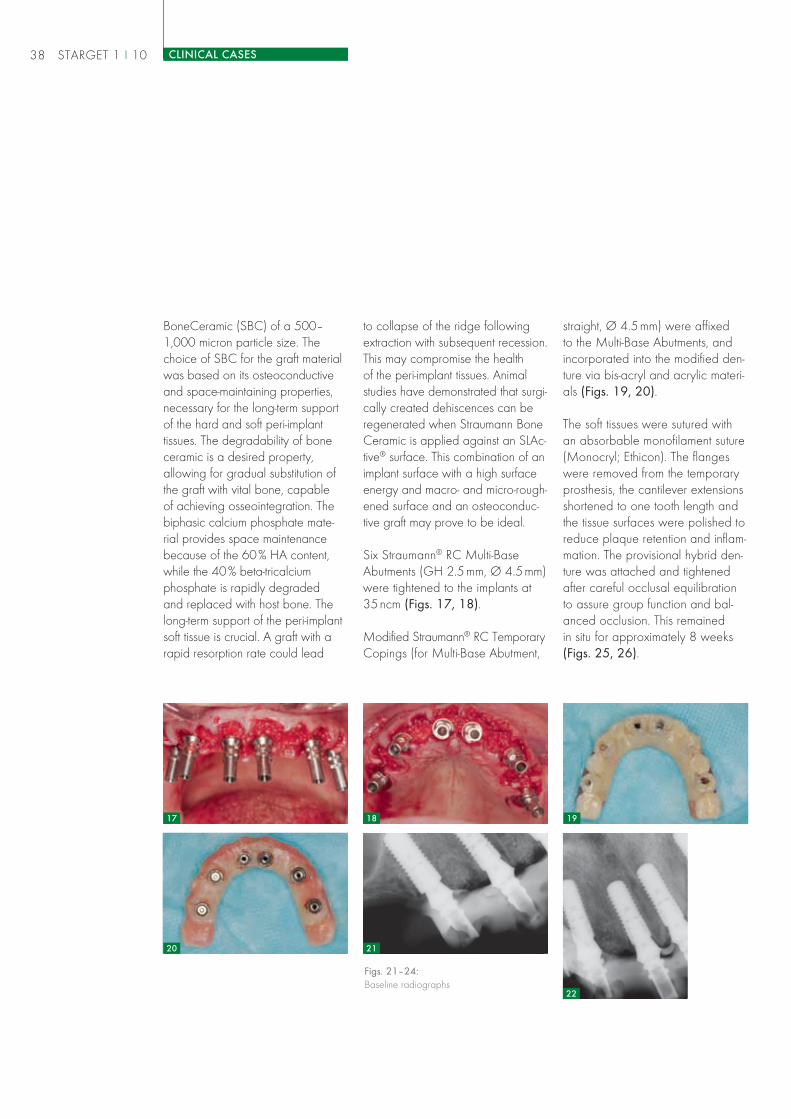
Figs. 21–24:Baseline radiographs
BoneCeramic (SBC) of a 500–1,000 micron particle size. Thechoice of SBC for the graft materialwas based on its osteoconductiveand space-maintaining properties,necessary for the long-term supportof the hard and soft peri-implanttissues. The degradability of boneceramic is a desired property,allowing for gradual substitution ofthe graft with vital bone, capableof achieving osseointegration. Thebiphasic calcium phosphate mate-rial provides space maintenancebecause of the 60% HA content,while the 40% beta-tricalciumphosphate is rapidly degradedand replaced with host bone. Thelong-term support of the peri-implantsoft tissue is crucial. A graft with arapid resorption rate could lead
18 19
20
17
straight, Ø 4.5mm) were affixedto the Multi-Base Abutments, andincorporated into the modified den-ture via bis-acryl and acrylic materi-als (Figs. 19, 20).
The soft tissues were sutured withan absorbable monofilament suture(Monocryl; Ethicon). The flangeswere removed from the temporaryprosthesis, the cantilever extensionsshortened to one tooth length andthe tissue surfaces were polished toreduce plaque retention and inflam-mation. The provisional hybrid den-ture was attached and tightenedafter careful occlusal equilibrationto assure group function and bal-anced occlusion. This remainedin situ for approximately 8 weeks(Figs. 25, 26).
STARGET 1 I 1038 CLINICAL CASES
to collapse of the ridge followingextraction with subsequent recession.This may compromise the healthof the peri-implant tissues. Animalstudies have demonstrated that surgi-cally created dehiscences can beregenerated when Straumann BoneCeramic is applied against an SLAc-tive® surface. This combination of animplant surface with a high surfaceenergy and macro- and micro-rough-ened surface and an osteoconduc-tive graft may prove to be ideal.
Six Straumann® RC Multi-BaseAbutments (GH 2.5mm, Ø 4.5mm)were tightened to the implants at35ncm (Figs. 17, 18).
Modified Straumann® RC TemporaryCopings (for Multi-Base Abutment,
22
21
STARGET_1_2010_en.indd 38STARGET_1_2010_en.indd 38 21.12.2009 17:35:36 Uhr21.12.2009 17:35:36 Uhr

STARGET 1 I 10 39CLINICAL CASES
25 26
27 30
23
28 29
During this healing period, thepatient was advised to maintain avery soft diet, with particular cau-tion during the first 3 post-operativeweeks, to minimize excessiveforces on the implants and facilitateosseointegration.
At the 8-week review, all implantswere immobile and the peri-implantsoft tissues were considered to behealthy and free of frank inflam-mation. The Multi-Base Abutmentlevel impressions were taken and ascrew-retained, fixed partial denture(hybrid prosthesis) was deliveredabout 4 months post-surgery.
24
Final result
Radiographically, there is a strongsuggestion that minimal change hadoccurred from baseline, 5 weekspost-operatively (Figs. 27–30) andafter 8 months of loading (Figs.31–34). This can be attributed to acombination of factors. First, the hori-zontal off-set of the microgap, wherethe prosthetic abutments connect tothe implant, shifts the biologic widthapproximately 0.4mm from thebone crest. Second, the placementof an osteoconductive graft material,such as Straumann® Bone Ceramic(SBC) to obturate the horizontaldefect (HDD) between the fixtureand the residual socket walls wassuccessful in maintaining the bonethickness necessary for long-term
STARGET_1_2010_en.indd 39STARGET_1_2010_en.indd 39 21.12.2009 17:35:38 Uhr21.12.2009 17:35:38 Uhr
osseointegration and tissue support.Third, the Straumann SLActive® surfaceserved to maintain a high level ofcrestal bone to implant contact fromthe time of installation to the deliv-ery of the final prosthesis. Fourth,the provisional FPD was allowedto remain in place for nearly twomonths, facilitating the maturation ofthe supra-crestal, soft tissue attach-ment to the implants before the startof restorative therapy.
Conclusion
This case demonstrates the syner-gies of an implant’s osteoconduc-tive surface, an osteoconductivebone replacement graft, a novelimplant-abutment connectionand meticulous occlusal therapythroughout the completion of care.
Special thanks to Dr Len Fishmanfor the final restorative therapy.
35 36
Fig. 35:Final restoration
Fig. 36:Final restoration
STARGET 1 I 1040 CLINICAL CASES
Barry P. Levin, DMD
Clinical Associate Professor at theDepartment of Periodontics of theUniversity of Pennsylvania
Diplomate of the American Boardof Periodontology
ITI Fellow
3432 3331
STARGET_1_2010_en.indd 40STARGET_1_2010_en.indd 40 21.12.2009 17:35:40 Uhr21.12.2009 17:35:40 Uhr

Regeneration of a periodontal defect withStraumann® Emdogain and a Straumann®
Soft Tissue Level Implant with SLActive® surface,in combination with Straumann® BoneCeramicby Dr Marlene Teo and Dr Joanne Uy
Patient history and findingsA 38 year old Singaporean Chinese woman, non-smoker with no relevant medical history, was
referred for replacement of tooth #14 (FDI) with an implant. It had been extracted 3 months previously
by a general dentist due to a fractured root. She had no other complaints.
At the clinical examination, it wasnoted that tooth #15 had a mobilityof II with 5mm probing depths onthe mid and mesio-buccal aspectsand a 6mm probing depth on thedisto-buccal aspect. There wasinitial caries on the distal aspect of#15. The rest of the probing depthsin the mouth were within normallimits.
The #14 implant site showed goodbucco-lingual and mesio-distal width(Figs. 1, 2) with a slight bone con-cavity apically. The radiographicexamination showed 40% angularbone loss on the mesial and distalsurface of #15 and a healing sock-et at #14. The sinus floor was more
1 2 3
STARGET 1 I 10 41CLINICAL CASES
thus decided that regeneration of#15 with Straumann® Emdogainwould be done simultaneously whenthe implant at #14 was placed.
Surgical procedure
A full thickness flap was raised from#13 to #15. Only a buccal flapwas reflected as the angular defectonly affected the buccal surfaceof #15 and left the palatal surfaceintact.
Granulation tissue was removed and#15 was root planed, leaving a
than 12mm away from the crest ofthe ridge at #14 (Fig. 3). The inter-maxillary relationship was normal.
Treatment planning
The patient was put through initialtherapy with full mouth scaling, andlocalized scaling and root planingwas done on tooth #15. Concen-trated fluoride was applied on #15in an attempt to remineralize thecarious lesion.
Oral hygiene was adequate 6weeks after initial therapy but thelocalized probing depth of 6mm onthe distal aspect of #15 persistedwith bleeding on probing. It was
STARGET_1_2010_en.indd 41STARGET_1_2010_en.indd 41 21.12.2009 17:35:41 Uhr21.12.2009 17:35:41 Uhr

STARGET 1 I 1042 CLINICAL CASES
narrow, 3.5mm deep 3-wall intrab-ony defect on the buccal surface of#15 (Fig. 4).
When the surgical stent was placedat #14, it was noted that the crest ofbone was only 1mm from its futurecervical margin (Fig. 5). Bone wasremoved from the crest (Fig. 6) toensure that the implant would beseated at least 3 mm below thefuture cervical margin.
Implant bed preparation was doneaccording to the Straumann pro-tocol and was restoratively driven,guided by the surgical stent (Fig. 6).
As there was a slight buccal under-cut, the final 3.5mm drill resulted in
an apical perforation of the buccalplate measuring 5mm by 4mm indiameter (Fig. 7).
A Straumann® Soft Tissue LevelImplant (Standard Plus, Ø 4.1mm,SLActive 12mm) was placed in the#14 site in a good restorative posi-tion and with good primary stability(Fig. 8). The Straumann SLActive®
surface was chosen to enhancebone formation during GBR andalso to speed up the osseointegra-tion process for early loading. AStraumann® RN Healing Abutmentwas placed on the implant to allowtransgingival healing.
The buccal plate around theexposed implant threads was then
decorticated to enhance GBR(Fig. 9). Straumann® PrefGel wasplaced on tooth #15 for 2 minutesto treat the root surface, then rinsedoff with saline.
Straumann® BoneCeramic washydrated with saline and placed onthe exposed #14 implant threadsand the decorticated area (Fig. 10).The bone graft area was coveredwith a resorbable collagen mem-brane (Fig. 11).
Straumann® Emdogain was thenmixed with the remaining Straumann®
BoneCeramic. The exposed rootsurface of #15 was coated withStraumann® Emdogain (Fig. 12)and the Straumann® Emdogain/
4 5 6
7
8
9
STARGET_1_2010_en.indd 42STARGET_1_2010_en.indd 42 21.12.2009 17:35:43 Uhr21.12.2009 17:35:43 Uhr
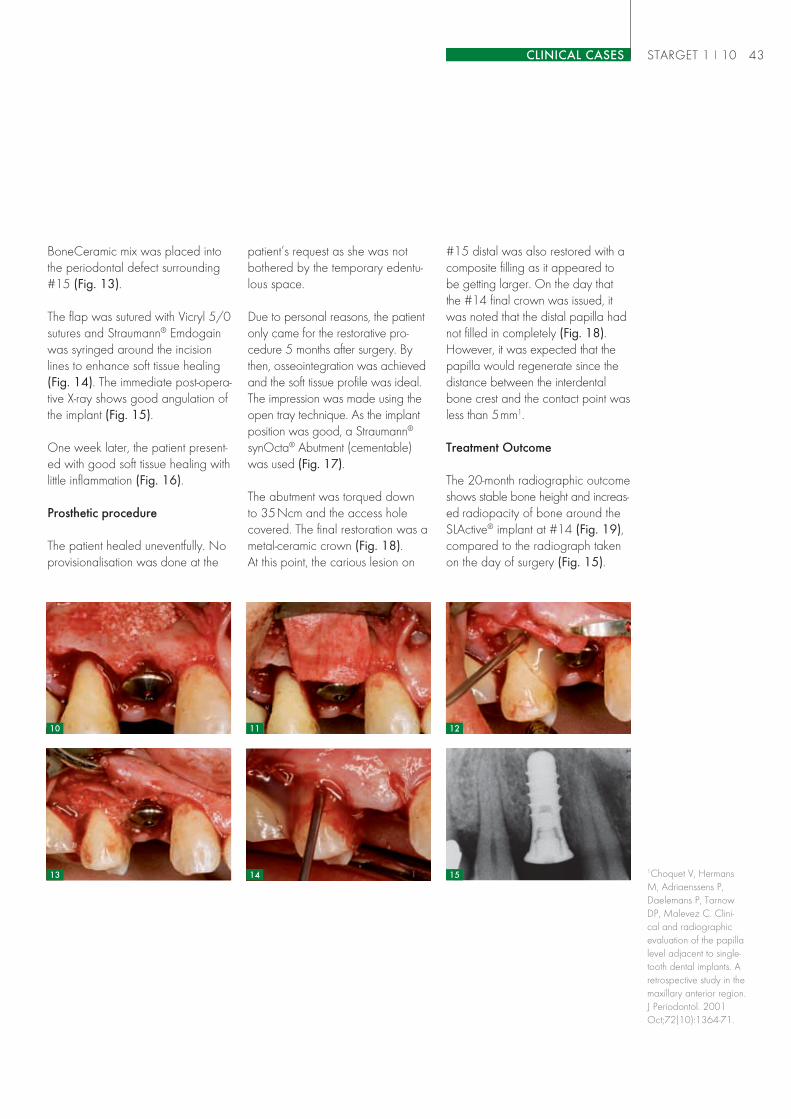
BoneCeramic mix was placed intothe periodontal defect surrounding#15 (Fig. 13).
The flap was sutured with Vicryl 5/0sutures and Straumann® Emdogainwas syringed around the incisionlines to enhance soft tissue healing(Fig. 14). The immediate post-opera-tive X-ray shows good angulation ofthe implant (Fig. 15).
One week later, the patient present-ed with good soft tissue healing withlittle inflammation (Fig. 16).
Prosthetic procedure
The patient healed uneventfully. Noprovisionalisation was done at the
patient’s request as she was notbothered by the temporary edentu-lous space.
Due to personal reasons, the patientonly came for the restorative pro-cedure 5 months after surgery. Bythen, osseointegration was achievedand the soft tissue profile was ideal.The impression was made using theopen tray technique. As the implantposition was good, a Straumann®
synOcta® Abutment (cementable)was used (Fig. 17).
The abutment was torqued downto 35Ncm and the access holecovered. The final restoration was ametal-ceramic crown (Fig. 18).At this point, the carious lesion on
1513 14
1210 11
1Choquet V, HermansM, Adriaenssens P,Daelemans P, TarnowDP, Malevez C. Clini-cal and radiographicevaluation of the papillalevel adjacent to single-tooth dental implants. Aretrospective study in themaxillary anterior region.J Periodontol. 2001Oct;72(10):1364-71.
#15 distal was also restored with acomposite filling as it appeared tobe getting larger. On the day thatthe #14 final crown was issued, itwas noted that the distal papilla hadnot filled in completely (Fig. 18).However, it was expected that thepapilla would regenerate since thedistance between the interdentalbone crest and the contact point wasless than 5mm1.
Treatment Outcome
The 20-month radiographic outcomeshows stable bone height and increas-ed radiopacity of bone around theSLActive® implant at #14 (Fig. 19),compared to the radiograph takenon the day of surgery (Fig. 15).
STARGET 1 I 10 43CLINICAL CASES
STARGET_1_2010_en.indd 43STARGET_1_2010_en.indd 43 21.12.2009 17:35:45 Uhr21.12.2009 17:35:45 Uhr

STARGET 1 I 10 CLINICAL CASES44
also be placed on the exposedimplant threads for Guided BoneRegeneration (GBR) and placed inthe periodontal defect to act as ascaffold for regeneration. Important-ly, this case demonstrates that it ispossible to place an implant with the
Dr Marlene [email protected]
Specialist Periodontist in private practice,Singapore
Diplomate of the American Board ofPeriodontology
Adjunct Lecturer in Preventive Dentistryat the National University of Singapore
Adjunct Assistant Professor at the Univer-sity of North Carolina at Chapel Hill
ITI Fellow
Dr Joanne [email protected]
Specialist Prosthodontist at the NationalUniversity Hospital, Singapore
Assistant Professor of RestorativeDentistry at the National Universityof Singapore
There is also radiographic bone fill ofthe angular defect at #15 (Fig. 19).
Clinically, the distal papilla of #14has filled the interdental space andprobing depths around #15 havedecreased to 3mm and below.Mobility of #15 is now within physi-ologic limits.
The 3-year post-operative examshows stability of the soft tissues(Fig. 20), much like what was foundat the 20-month post-op exam. Thesoft tissue profile of #14 replicatesthat of natural teeth and is sym-metrical with the teeth in the upperleft quadrant (Fig. 21). No 3-yearradiograph was done as the patientwas possibly pregnant.
Conclusions
The placed implant with the Strau-mann SLActive® surface shows goodosseointegration and osteoconduc-tivity. Straumann® BoneCeramic may
20 21
18
19
16 17
SLActive® surface with simultaneousGBR and treat an adjacent toothwith Straumann® Emdogain regener-ation simultaneously. This reduced inthis case the number of surgical pro-cedures. Both procedures provedsuccessful over the span of 3 years.
STARGET_1_2010_en.indd 44STARGET_1_2010_en.indd 44 21.12.2009 17:35:46 Uhr21.12.2009 17:35:46 Uhr

STARGET_1_2010_en.indd 45STARGET_1_2010_en.indd 45 21.12.2009 17:35:50 Uhr21.12.2009 17:35:50 Uhr

Why the Straumann® Dental ImplantSystem is a “premium” solution
Smaller suppliers are increasingly present in the market for dental implants, with cheap implant
products and an aggressive marketing that is targeted at price. Some of these companies would
not even exist without premium suppliers. In this article, Institut Straumann AG would like to
show what premium suppliers do to develop implant dentistry on a scientific foundation and
continuously increase treatment safety, while suppliers of cheap implants are exclusively sales-
oriented organizations with a short-term outlook.
QUALITY AND PRODUCT SAFETY
STARGET 1 I 1046 SIMPLY DOING MORE
What premium brands achieve and why cheap implants cannot be regardedas an option for the patient who wants value for money and peace of mind
STARGET_1_2010_en.indd 46STARGET_1_2010_en.indd 46 21.12.2009 17:35:51 Uhr21.12.2009 17:35:51 Uhr

1Straumann SLActiveScientific Studies ThirdEdition. 2009.
STARGET 1 I 10 47SIMPLY DOING MORE
Years of research, development, and testing precede the launch of a high-end product, such as the excellentimplant surface Straumann SLActive® – with corresponding costs.
manufacturer may compare theprice of its undocumented, second-generation surface with the priceof Straumann’s third-generationhydrophilic SLActive® surface.Endorsed by more than 25 andongoing studies, SLActive® is oneof the best investigated implant sur-faces on the market1.
Price comparisons: SLActive® asan example
It is not uncommon for low-priceplayers to promote their productswith price differences by compar-ing their products against the mostexpensive, high end premiumsolutions. For instance one cheap
The crucial factors of a premiumimplant solution
Without clinical substantiation, lowprice implants simply have no claimto equivalence. Even when it comesto simple design features and finish,the claim that a cheap implant isan equivalent alternative must bebased on comparative long-termdata to support it, which often isnot the case. If a comparison ismade between Straumann’s valueoption, the SLA® surface, and acheap manufacturer, the differencein the overall cost of the treatmentis negliglible. However, the Strau-mann solution offers great flexibility,for example in terms of prostheticrange and planning – with simplehandling and workflow. These arejust two of many elements in ourvalue proposition, which, togetherwith the following factors, explainswhy Straumann is a premiumimplant solution.
SLActive – were price comparisons become difficult
Histological cross-sections show bone defect filled at 12 weeks after implant placement
Straumann7 February 2007
Results from preclinical studies presented by Becker J, Schwarz F (Heinrich-Heine University,Düsseldorf, Germany) at 15th Ann. Sci. Meeting of the EAO, Zurich, 2006
SLA® SLActive®
Newbone
STARGET_1_2010_en.indd 47STARGET_1_2010_en.indd 47 21.12.2009 17:35:52 Uhr21.12.2009 17:35:52 Uhr

STARGET 1 I 1048 SIMPLY DOING MORE
Lasting quality and service
Look-alikes give the clinicians theimpression that they are savingmoney but they don’t talk about thelong-term consequences. As in otherfields, the rule applies: saving moneyat the wrong end can become cost-ly later. A recent comparative studyconducted by the University of Con-necticut reveals how quality stand-ards between premium implants andlook-alikes can differ (see text box).The consequences and costs thatmay result from the usage of suchproducts should therefore be takeninto consideration in advance.
Higher risk of mechanical failure in look-alike implant systems
A study reveals higher risk of mechanical failure in low-cost implantsystems. The study tested the mechanical fracture limit of threeStraumann clone implant systems (IHDE Dental, Bluesky Bio, Lifecore)compared with original Straumann products. The systems testedshowed a significant higher risk of mechanical failure than the origi-nal Straumann implants.
Junghoon Yoo DDS, Robert Kelly DDS, MS, DMedSc: Comparisonof fracture behaviour among different single stage implants undercyclic loading. Reconstructive Sciences, University of ConnecticutHealth Center. Poster presentation at the American College ofProsthodontics, San Diego 2009.
Straumann not only invests in the development of dental implant technology but also in theresearch of pioneering new technologies such as Regeneration and CADCAM.
Cheap implants may not offer flexible solutions for technical matters.But making compromises is not worth even the cheapest price.
STARGET_1_2010_en.indd 48STARGET_1_2010_en.indd 48 21.12.2009 17:35:54 Uhr21.12.2009 17:35:54 Uhr

STARGET 1 I 10 49SIMPLY DOING MORE
An implant is more than a screw
Not only should the dental implantperform functionally and be reliable,it should also last on a long-termbasis – which means that the boneand soft tissues around it need tobe maintained. Comprehensivelong-term clinical studies published inpeer-reviewed journals and present-ed at international scientific meet-ings have always been importantto Straumann and the Straumann®
Dental Implant System is backed byongoing studies assessing estheticparameters over the long term. In2004, an ongoing cohort studywas presented at the 13th ScientificMeeting of the European Asso-ciation of Osseointegration (EAO),which included 12-year data onesthetic parameters of Straumannimplants2. Nine-year data were pub-lished in 20033. Some manufactur-
Premium companies like Straumann offer a large variety of courses worldwide every year to meetthe constantly growing education needs in implant dentistry.
ers of cheap implants were not evenin the business then and still have noclinical program in place.
The question of choice
The implant itself makes up onlya fraction of the overall treatmentcosts. The last thing a patient wantsis to risk failure or jeopardize long-term outcome by trying to save oneor two hundred francs. In a consum-er market, people have a choice asto whether they purchase a premi-um or a cheap product. In dentistry,patients rarely get to choose whichmanufacturers’ products are putinto their mouths. So the patient isunable to make a qualified choiceand has to rely on the prescriberto receive the best treatment andmaterials possible. Thus, if the sup-posed savings are put in relation tothe overall costs of the treatment or
to the costs resulting from implantsor abutments which do not workproperly, it becomes evident thatcheap implants are only supposed-ly cheaper than premium products.
Clinical substantiation
Furthermore, Straumann conductsthorough preclinical and clinicaltests on its products prior to marketintroduction. The results of thesestudies are presented at internation-al scientific congresses and in peerreviewed journals, endorsing thequality of the research. Straumanncurrently has 18 studies running in139 centers in 17 countries andinvolving 2061 patients.
Attention has been drawn to thelack of clinical evidence and long-term data to support cheap implantproducts4. A search for literature
2Belser UC. Longterm sta-bility of esthetic implants.Clin Oral Implants Res2004;15(4):xxiv.3Giannopoulu C et al.:Effect of intracrevicularrestoration margins onperi-implant health: clini-cal, biochemical, andmicrobiologic findingsaround esthetic implantsup to 9 years. J. OralMaxillofac. Implants18(2) 2003: 173-81.4e.g. Buser D in NZZam Sonntag 2009Number 21, p. 45.
STARGET_1_2010_en.indd 49STARGET_1_2010_en.indd 49 21.12.2009 17:35:55 Uhr21.12.2009 17:35:55 Uhr

STARGET 1 I 1050 SIMPLY DOING MORE
Close interaction with the customers to understand their requirements.
Roxolid™: clinical trials with more than 400 patients and60 centers around the world
In addition to thorough laboratory testing, clinical trials are currently inprogress in more than 400 patients and 60 centers around the worldto ensure that Straumann has independent data substantiating thesafety, performance and benefits of our new high strength material,Roxolid™, before it reaches practitioners and patients. Further stud-ies are planned. Based on current knowledge, Roxolid™ is strongerthan pure titanium5 and preclinical results indicate that it has improvedosseointegration properties compared to titanium6. Straumann’s hopeis that Roxolid™ will lead to smaller diameter implants that may obviatethe need for bone grafting and augmentation in some cases. If so, itcould save patients considerable cost and discomfort. These are justtwo of many reasons why meaningful innovation and research areimportant. Indeed, in contrast to cheap implant suppliers, Straumann isresearching new materials and technologies – such as guided implantsurgery, regenerative materials or CADCAM prosthetics – to addfurther predictability, simplicity, esthetics and reliability to tooth replace-ment procedures.
Look-alikes give the clinicians the impression to save money,but they don’t speak about the long-term consequences.
in PubMed, which includes 18 mil-lion citations from 5,000 journals inMEDLINE, and in Google Scholarhas lead to the result that, for cer-tain manufacturers, there are nopeer-reviewed studies on implantsat all in these two databases.
The costs behind the develop-ment and scientific testing of anext-generation implant surface
Straumann products are backedby clinical studies before they arelaunched. For example more than1,400 implants had been document-ed in clinical trials before our newgeneration bone level implant rangewas put on the market. It took 4years and cost approximately CHF20 million for Straumann to developand test the SLActive® surface tech-nology prior to market introduction.
5Norm ASTM F67(states minimum tensilestrength of annealedtitanium), used for allStraumann titanium andRoxolid™ implants, dataon file6Gottlow J et al. Pre-clinical data presentedat the 23rd Annual Meet-ing of the Academy ofOsseointegration (AO),Boston, and at the17th Annual ScientificMeeting of the Euro-pean Association forOsseointegration (EAO),Warsaw.
STARGET_1_2010_en.indd 50STARGET_1_2010_en.indd 50 21.12.2009 17:35:56 Uhr21.12.2009 17:35:56 Uhr

STARGET 1 I 10 51SIMPLY DOING MORE
Research and development at Straumann: still heading the list ofpriorities even in the recession
Research and development are the basis for launching innovativeproducts and therefore for the company’s future. Even in an economicrockbottom, this budget is not cut at Straumann. Expenditure in thisconnection in the first half of 2009 was over five per cent of turnoverand thus more than in previous years. These investments are madeavailable for basic research, both clinical and preclinical, which playsa central part in product development. Only when convincing scientificevidence has been produced with scientific studies that Straumannproducts are both safe and effective (and furthermore offer clinicaladvantages) are these introduced to the market. Straumann will alsoemploy the necessary means in future to test new products and materi-als before and after market introduction.
Scientifically grounded products– the best investment for doctorand patients
The innovations of Straumann are aresponse to the needs of the steadilydeveloping implant dentistry practice.As the Roxolid™ example shows,an innovative product can signify an
expansion of the range of indicationsfor the dentist working in implantdentistry, that is, the possibility ofreaching new groups of patients inwhom implant therapy was not pos-sible previously for various reasonsor would have involved risks. Thisexpansion of the range of indicationsalso signifies corresponding growth
Peace of mind with premium solutions: they may appear expensiveinitially – but can patients really afford to the possible drawbacks ofcheap alternatives?
for their practice. Straumann custom-ers are among the first who willbenefit directly from the innovative,scientifically founded products thatare designed to last – the outcomeof years of intensive and accordinglyexpensive research.
Training and education:an important element in themarketing mix
Basic training in implant dentistrynow features in under- and post-graduate education. However,there is a huge need for furthereducation, specialization andrefresher courses to ensure thatpractizing dentists, technicians,nurses and other dental profes-sionals are able to offer the lateststandard of care to patients. Pre-mium companies like Straumannoffer a large variety of coursesworldwide every year. These are amajor contribution to raising treat-ment quality and enhancing thestandard of patient care. Although
STARGET_1_2010_en.indd 51STARGET_1_2010_en.indd 51 21.12.2009 17:35:57 Uhr21.12.2009 17:35:57 Uhr
STARGET 1 I 1052 SIMPLY DOING MORE
course participants usually pay acourse fee, the companies incurconsiderable costs for the organi-zation, teaching materials etc.
Direct access to the customersand intense communication
Because Straumann sells directly todentists and dental laboratories, aclose interaction with the customersto understand their requirementsis possible. In addition to provid-ing important information on newproducts and techniques, Strau-mann offers networking and hotlineservices. Our customers thus haveaccess to specialists who can helpwith irregularities and difficult cases.In conjunction with the ITI, broadopportunities for customers to trainfurther and to develop new skillsare offered.
The risk of obsolescence
In times of economic uncertainty,smaller low-margin companies facegreater challenges to survive thanestablished players with large cus-tomer bases. Saving on an implantincreases the patient’s exposure tohaving an unserviceable implant inthe future. Thus, an important ques-tion patients should ask is: ‘Is theimplant system guaranteed?’
The risk of mixing
Cheap implants often do not offerflexible solutions for technical matters.But making compromises is not wortheven the cheapest price. Several lowcost manufacturers sell copycat com-ponents intended for use on premiumbrand implants instead of the moreexpensive original components. Here
Disadvantages and risks you may encounter when using cheap implants:
Lack of clinical studies insecurity in careRestricted implant and prosthetic portfolio restricted treatment optionsCostly fitting inefficient workingCombination with Straumann products loss of Straumann GuaranteeIf problems occur unreliable or no practical onsite serviceUnexpected complications full responsibility passes to the dentistNo guarantee for a long-term market presence of the supplier risk ofno support for phased-out products
again, there is no clinical evidenceto support the claimed compatibility.There is no assurance of the sameprecision or material quality. Further-more, the original manufacturer’sliability for the product is voided andthe dentist is responsible for mixingsystems. As soon as componentsare mixed the Straumann guaranteebecomes void.
The Straumann Guarantee
Quality, education and account-ability come at a price. Short-termsavings can prove painful in thelong term, and although premiumsolutions may appear expensiveinitially, they could well work outcheaper in the long run. The ques-tion is: can patients really afford tothe drawbacks of cheap alterna-tives?
Your benefit when using Straumann products:
The components of the Straumann® Dental Implant System are theresult of more than 20 years of scientific research.Straumann implants and prosthetic components offer an individualvariety of treatment optionsStraumann products are designed for perfectly fitting solutionsStraumann gives a 10-year guaranteeStraumann gives immediate onsite support in problem cases– a call suffices.
STARGET_1_2010_en.indd 52STARGET_1_2010_en.indd 52 21.12.2009 17:35:58 Uhr21.12.2009 17:35:58 Uhr

STARGET 1 I 10 53SIMPLY DOING MORE
Mr. Matter, what are the argu-ments in favor of dental implants?
When a tooth has to be replaced,the dentist chooses either a bridgeor an implant. As regards durability,both implants and bridges come offequally well in a ten-year compari-son. Extrapolated to twenty years,the implants have the advantage.This is because only minor technicalrepairs are needed for implants inthis period. With bridges, the prob-lems are usually much more serious;
In an interview with the Swiss business magazine “Finanz und Wirt-
schaft”1 on the topic of “Cheap implant suppliers versus premium
brands“ Sandro Matter made his position clear, listing the reasons
why, from Straumann’s point of view, such suppliers will not be
successful in the long term and talked about the trends that occupy
the manufacturers.
1Interview: Carla Palm;published in the Swiss“Finanz und Wirtschaft”No. 13 of 18 July 2009,reprinted with the kindpermission of the author.
An interview with Dr Sandro Matter, Head of GlobalProducts at Straumann
“Quality and servicecome at a price”
the entire product then has to bereplaced.
Do these statements apply to allavailable dental implants?
No, the comparison is based onclinical studies with premium implantsfrom Switzerland and Sweden.
How must scientific studies inimplant dentistry be designedif they are to demonstrate thebenefit?
STARGET_1_2010_en.indd 53STARGET_1_2010_en.indd 53 21.12.2009 17:35:58 Uhr21.12.2009 17:35:58 Uhr

STARGET 1 I 10 SIMPLY DOING MORE54
There are different levels of clinicalstudies. The most reliable are rand-omized, controlled multi-center stud-ies, which today are very similar tostudies in the pharma industry. Incontrast, there are individual casedescriptions, which report on thetreatment of individual patients andare published by dentists. Natural-ly, there is an enormous differencebetween the two studies.
I suppose especially in price?
A multi-center study over five yearscosts up to 1 million Swiss francs.At the moment, Straumann has 21clinical studies in the field, and 15of them are multi-center studies.
How can smaller suppliers sellimplants without clinical proof ofthe safety of the products?
These suppliers sell their implantson the basis of the fundamentalrequirements of our sector. Theseinclude the basic biocompatibil-ity of the products, appropriatedesign, mechanical strength andthe company’s quality system. TheEuropean Medical Device Direc-tive does not yet demand any clini-cal evidence for the benefit of theimplants. The companies are onlychecked through a quality audit bythe listed sites.
Is that not frustrating for a marketleader like Straumann, whichinvests several million francs ayear in research and develop-ment?
From 2010 the regulations regard-ing the scope of the clinical evalua-tion for all dental implant supplierswill be intensified. Straumann prod-ucts are already documented byclinical studies although this is notnecessary according to the stand-ards of the sector. However, thisgives us an enormous advantagein the long term in surgical, estheticand long-term comparisons.
Nevertheless, the small suppliersmust be vexatious for the marketleaders.
The small companies like to presentthemselves as Robin Hood andwe big companies are the evilSheriff of Nottingham. That is justso much PR noise and is not true.Just because an implant looks like aStraumann product, it is not equallygood. The products differ consider-ably, ranging from the surface struc-ture through service to the material.Cheap suppliers often use titaniumalloys, which do not osseointegrateas well. In contrast, Straumannworks with pure titanium and thenew material Roxolid™.
The price differences are sub-stantial.
You can’t compare apples withpears. Quality and service comeat a price. If patients knew whatis sometimes implanted, theywould begin to ask questions. Forinstance, when problems arise withimplants that are no longer beingmanufactured.
Let’s stay with the competition.How do you assess the subjectof culturing human teeth fromstem cells?
Admittedly, that is a fascinatingarea of research. However, thebenefit for the dental sector is inthe very distant future. Cell-basedtreatments are currently still veryexpensive. An ordinary dentalimplant treatment costs about4,000 Swiss francs today. On theother hand, patients would haveto come up with many times thatamount for a cultured stem cellsolution; that is still pie in the sky.
“You can’t compare apples with pears. Quality and servicecome at a price. If patients knew what is sometimes implanted,
they would begin to ask questions.“
STARGET_1_2010_en.indd 54STARGET_1_2010_en.indd 54 21.12.2009 17:35:59 Uhr21.12.2009 17:35:59 Uhr

STARGET 1 I 10 55SIMPLY DOING MORE
fessionally analyzed in compliancewith data protection for all thoseinvolved. The aim of the survey isnot to ask referring colleagues orpatients about all of their wishesand then fulfill these but to establishthe leading quality features of thecooperation and then employ thisinformation profitably for one’s ownpractice.
Establishing leading qualityfeatures
The two Straumann initiativesplanned internationally for the startof 2010, “Center of ExcellenceImplantology“ (with the focus onpatients) and “Achieving success inspecialist team” (with the focus onreferring colleagues) are intended
to assist participating Straumanncustomers to obtain new informa-tion about unutilized potentials andassociated forward-looking prac-tice strategies. The surveys will beconducted by the prestigious “Insti-tute for Management in the HealthService“ in Augsburg under Profes-sor Dr Gerhard F. Riegl (see box).The surveys will be used and pro-
Discover and develop unutilizedpotentials for your practice
Implant restorations represent a great future market in the dental sector.1 Any dentist working in
implantology who wants to offer his patients outstanding implant treatment and become successfully
established permanently in this future market must think about his own professional and material
development. Straumann would like to support this process with an excellence initiative.
PRACTICE BENCHMARKING
1See “Dental implantpenetration in leadingmarkets“, Straumannbusiness report 2008p. 21. www.straumann.com/gb2008
The Straumann initiatives “Center of Excellence Implantology“ and “Achievingsuccess in a specialist team”
Team surveyCompares the practice team’s
assessment with the perceptions ofpatients and referring doctors.
“Achieving success in a specialist team“Satisfaction, expectations, wishes andpotential for improvement in the collabora-tion with referring colleagues.
Learning through direct comparisonwith regional colleagues
“Center of Excellence Implantology“Satisfaction, expectations, wishes
and potential for improvement in thetreatment of patients.
Yourpractice
Referring colleagues
Colleague benchmarking
Practice team
Patients
Structure of the bench-marking initiatives: byincluding the practiceteam, patients and com-petitors and comparingthe different perspec-tives, a 360° view ofthe individual situation isobtained.
STARGET_1_2010_en.indd 55STARGET_1_2010_en.indd 55 21.12.2009 17:35:59 Uhr21.12.2009 17:35:59 Uhr

STARGET 1 I 1056 SIMPLY DOING MORE
“Achieving success in a specialist team“: As a specialist workingin implant dentistry, have you ever asked yourself …
… why the referring dentists entrust you in particular withtheir cases?
… whether you know the needs and expectations of yourreferring colleagues?
… how you can offer your referring colleagues more benefitswith small changes?
… what is the basic level of satisfaction of referring colleagueswith the existing cooperation?
… how and by what means can you make yourself and yourpractice stand out from other competitors?
… where you are already outstanding or where improvementswould be appropriate?
… what made you so successful with referring colleaguesand what can you do to develop this success further in thelong term?
“Achieving success in a specialistteam“: how one is perceived byreferring colleagues
An exchange in the spirit of partner-ship about cooperation wishes andthe satisfaction of referring dentistsprovides the surgeon working inimplant dentistry with valuable hintson optimizing potential. This knowl-edge can be an essential key fac-tor for the success of the practice.This is not only a matter of a quan-titative increase in referred patientsbut also of building up long-termlinks to the referring colleagues andextending this network, since it isthe referral of suitable and demand-ing cases for treatment that lays thefoundation for success in implantol-ogy.
Friendliness and atmosphere – two of the factors of patient satisfaction.© Picture: Courtesyof Cyrus Nikkhah,Devonshire House
STARGET_1_2010_en.indd 56STARGET_1_2010_en.indd 56 21.12.2009 17:36:00 Uhr21.12.2009 17:36:00 Uhr

“Center of Excellence Implantol-ogy“: how one is perceived bythe patients
One of the keys to determining anindividual practice’s success formulais a professional patient survey.
STARGET 1 I 10 57SIMPLY DOING MORE
Benchmarking: what is the bestway to differentiate?
The two Straumann initiatives atthe same time represent easily con-ducted regional market research,the results of which can be used forfurther qualification considerations.From the anonymous comparisonwith other colleagues from thesame region, participants find outwhat made colleagues successfuland how they compare with them.
A win-win situation for allinvolved
The excellence initiative describedhere was already carried out suc-
“Center of Excellence Implantology“: As a specialist working in implantdentistry, have you ever asked yourself …
… on what criteria your patients based their choice ofyour practice?
… whether your patients are satisfied and would recommendyou to others?
… what are your patients’ information needs?
… whether your practice team recognizes customer needs correctly?
… what importance your patients attribute especially to the frameworkconditions of your practice which are not relevant to treatment (suchas service, appointment management, friendliness, atmosphere andappearance)?
… how great is the willingness among your patients for tax-deductiblehigh-quality restorations?
cessfully in this form by Straumannin 2008 in one market (Germany),with entirely positive feedbackfrom all involved target groups.Ultimately, everyone benefits fromsuch a survey: the referring den-tist whose wishes are acceptedsystematically and may be imple-mented; the surgeon who canwork toward more referrals andgreater dentist satisfaction throughtargeted changes; and the patientwho obtains optimal treatment dueto the coordination between refer-ring dentists and surgeon. Thus, therecipe for success for a surgicaldental practice is: “If you help thereferring dentist and patient to gain,you gain yourself“.
The “Institute for Management inthe Health Service“ of Prof Dr rer.pol. Gerhard F. Riegl
Straumann’s cooperation partner, the“Institute for Management in the HealthSurface“ of Professor Gerhard Riegl inAugsburg has the expertise of over amillion patient surveys in over 10,000practices. In the dental sector alone, morethan 40,000 patients have been surveyedin over 700 practices. Prof. Riegl’s Instituteis therefore a leader in the area of dentalpatient surveys and is the optimum partnerfor Straumann. Prof. Riegl is regarded inGermany as the “expert in quality assur-ance in medicine“. He is the publisherand author of the first large bestsellerimage and marketing study for dentistsand dental laboratories in German-speak-ing countries under the title: “The DentalPractice as a Center of Excellence“.www.prof-riegl.de
For analyzing the actual situation,it is very instructive to comparethe subjective perceptions of thepatients with the perspective of thepractice owner. One of the result-ing pieces of information might bethat it does not make economic
sense to implement changes (that is,invest time and money), which arenot even noticed by the patient orare classified as minor. The aim ofthis initiative is to be able to set upspecific measures on the basis ofthe obtained data that will increasepatient satisfaction and promoteboth interest in and knowledge ofthe possibilities of modern implantrestorations in the patients.
STARGET_1_2010_en.indd 57STARGET_1_2010_en.indd 57 21.12.2009 17:36:03 Uhr21.12.2009 17:36:03 Uhr

STRAUMANN® DENTALIMPLANT SYSTEM
Cochran DL, Bosshardt DD, Grize L,
Higginbottom FL, Jones AA, Jung RE,
Wieland M, Dard M. Bone response
to loaded implants with non-matching
implant-abutment diameters in the
canine mandible. J Periodontol 2009;
80(4):609-617.
In five dogs, 12 Straumann BoneLevel
Implants per animal were placed after extrac-
tion of all mandibular premolars and first
molars; implants were placed at alveolar crest
level or 1mm above or below. Implants were
submerged on one side of the mandible, while
healing abutments were exposed to the oral
cavity on the other side, and crowns were
placed after 2 months. After 6 months, change
in alveolar bone was -0.34mm, -1.29mm and
0.04mm for implants placed at, below or
above the crestal bone, respectively for sub-
merged implants, and -0.38mm, 1.13mm and
0.19mm for non-submerged implants. There
were no significant differences in bone con-
tact between or within the groups. The bone
loss observed for implants with non-matching
implant-abutment diameters were significantly
less than those reported for similar implants
with matching implant-abutment diameters.
Cochran DL, Nummikoski PV,
Schoolfield JD, Jones AA, Oates TW. A
STRAUMANN® EMDOGAIN
Alhezaimi K, Al-Shalan T, O’Neill R,
Shapurian T, Naghshbandi J, Levi P Jr,
Griffin T. Connective tissue-cementum
regeneration: a new histologic regen-
eration following the use of enamel
matrix derivative in dehiscence-type
defects. A dog model. Int J Periodontics
Restorative Dent 2009;29(4):425-433.
A total of 30 dehiscences were created
on the maxillary canines and second and
fourth premolars of five dogs; Emdogain was
applied in the test group, while no Emdogain
was used in the controls. After 4 months, func-
tional connective tissue fibers in regenerated
cementum (mean amount 3.74 ± 0.43mm)
was found at all Emdogain sites, but no
cementum was formed in the control sites.
Emdogain therefore effectively promotes new
cementum and connective tissue formation.
Cortellini P, Pini-Prato G, Nieri M,
Tonetti MS. Minimally invasive surgical
technique and enamel matrix deriva-
tive in intrabony defects: 2. factors
associated with healing outcomes.
Int J Periodontics Restorative Dent
2009;29(3):257-265.
Minimally invasive surgical technique,
performed using microsurgical instruments
and an operating microscope, was used
to access 40 deep intrabony defects and
apply Emdogain to the root surfaces. CAL
gain after 1 year was 4.9 ± 1.7mm, with
> 4mm gain in 70% of the defects, and was
significantly associated with the depth of the
three-wall component, intraoperative bleed-
ing tendency and its interaction with the
initial amount of bone loss.
Garrocho-Rangel A, Flores H, Silva-
Herzog D, Hernandez-Sierra F, Man-
deville P, Pozos-Guillen AJ. Efficacy of
Emdogain versus calcium hydroxide in
direct pulp capping of primary molars:
a randomized controlled clinical trial.
Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2009;107(5):733-738.
A total of 90 primary molars were treated in
a spilt-mouth design using Emdogain or self-
hardening calcium hydroxide. Internal dentin
absorption, gingival sinus tract, root external
resorption, pain and pathologic mobility
were no significantly different between the
groups; only one treatment in each group
was judged as a failure. The pulp capping
techniques evaluated in this study can there-
fore be recommended on the basis of clini-
cal and radiographic results.
SELECTED LITERATURE OF RECENTLY PUBLISHED JOURNALS1
LITERATURE ALERTS
STARGET 1 I 1058 SIMPLY DOING MORE
1The abstracts ofthe quoted articles arepublicly available fromthe database PubMed
(www.pubmed.gov).The complete articlescan be ordered there
for a fee.
STARGET_1_2010_en.indd 58STARGET_1_2010_en.indd 58 21.12.2009 17:36:03 Uhr21.12.2009 17:36:03 Uhr

237 Straumann implants were placed in 45
patients, and biological, implant and prosthet-
ic parameters evaluated from implant place-
ment up to 5 years. Mean cantilever length
was 15.6mm (range 6 to 21mm). There
were no implant failures, and the prosthesis
survival rate was 95.5%, with a treatment
success rate of 86.7% (six patients did not
meet the criteria for success). The majority of
complications were technical (54/79), and
most of these involved fracture of the acrylic
teeth and base (20/54). Rehabilitation with
mandibular hybrid cantilever prostheses on
implants was therefore a reliable treatment.
Göllner P, Jung BA, Kunkel M, Liechti
T, Wehrbein H. Immediate vs. con-
ventional loading of palatal implants
in humans. Clin Oral Implants Res
2009;20(8):833-837.
From 2000 to 2006, two independent
groups of patients, requiring maximum anchor-
age, were treated using Straumann ortho
implants. Group 1 (n=36) was subjected to
immediate functional loading within the first
24h after insertion while group 2 (n=40)
received conventional implant loading after
12 weeks. The magnitude of orthodontic forc-
es ranged between 1 and 3N. Histological
workup was performed for nearly the last third
of palatal implants removed after treatment.
All implants reached primary stability. How-
ever, 3/36 in group 1 and 1/40 in group 2
Selected literature ofpotential interest fromrecently publishedjournals.
were lost. The remaining implants were clini-
cally stable and no mobility was recognized.
The median BIC rates were 76% in group 1
(n=10) and 84% in group 2 (n=12); the dif-
ference was not statistically significant.
Mericske-Stern R, Probst D, Fahrländer
F, Schellenberg M. Within-subject
comparison of two rigid bar designs
connecting two interforaminal implants:
patients’ satisfaction and prosthetic
results. Clin Implant Dent Relat Res
2009;11(3):228-237.
Patients received an implant-supported over-
denture in the mandible and were randomly
allocated to two groups. Group A received
a standard U-shaped bar (Dolder bar),
AND in group B precision attachments were
soldered distal to the bar copings. After 3
months, patients answered a questionnaire
and the bar design was exchanged. After
a period of another 3 months, the patients
had to answer the same questions; then they
had the choice to keep their preferred bar.
Patients that entered the study with the attach-
ment bar gave slightly better ratings to this
type for four items. At the end of the 6-month
comparison period, all but one patient
wished to continue to wear the attachment
bar. In vivo force measurements of maximum
biting were similar in both bar designs, but
exhibited significantly higher axial forces in
the attachment bar.
prospective multicenter 5-year radio-
graphic evaluation of crestal bone
levels over time in 596 dental implants
placed in 192 patients. J Periodontol
2009;80(5):725-733.
A total of 596 solid screw or hollow cylinder
TPS surfaced Straumann implants placed in
192 patients were evaluated radiographi-
cally at implant placement, prosthesis place-
ment, after 6 months and each year up to 5
years. Significant remodeling was observed
in the first 6 months (mean bone loss of 2.44
± 1.20mm). Mean bone loss from prosthesis
placement to 1 year and from 1 year to
5 years was 0.22 ± 0.42mm and 0.18 ±
0.88mm, respectively; 86% of the total bone
loss over 5 years occurred by the time of
prosthesis placement. The observed trends
were the same when adjusted for implant
design, implant length and type of restora-
tion. There is therefore significant bone
remodeling up to the time of final prosthesis
placement, but minimal bone loss thereafter.
Gallucci GO, Doughtie CB, Hwang
JW, Fiorellini JP, Weber H-P. Five-year
results of fixed implant-supported
rehabilitations with distal cantilevers
for the edentulous mandible. Clin Oral
Implants Res 2009;20(6):601-607.
Implant-supported mandibular hybrid pros-
theses with distal cantilever extensions on
STARGET 1 I 10 59SIMPLY DOING MORE
STARGET_1_2010_en.indd 59STARGET_1_2010_en.indd 59 21.12.2009 17:36:04 Uhr21.12.2009 17:36:04 Uhr
Nedir R, Bischof M, Vazquez L, Nurdin
N, Szmukler-Moncler S, Bernard J-P.
Osteotome sinus floor elevation tech-
nique without grafting material: 3-year
results of a prospective pilot study. Clin
Oral Implants Res 2009;20(7):701-707.
In 17 patients, 25 Straumann implants were
placed (16 molars and nine premolars)
using osteotome sinus floor elevation; 21
of the implants were 10mm long, while
the others were 6mm and 8mm long. The
implants were placed in newly formed bone
tissue. All implants met the survival criteria
after 3 years. Mean endo-sinus bone gain
was 3.1 ± 1.5mm and mean crestal bone
loss was 0.9 ± 0.8mm. Residual protrusion
length decreased from 4.9 ± 2.1mm to 1.8
± 2.1mm. Osteotome sinus floor elevation
was therefore sufficient to gain bone without
graft material.
Nedir R, Nurdin N, Szmukler-Moncler
S, Bischof M. Placement of tapered
implants using an osteotome sinus
floor elevation technique without bone
grafting: 1-year results. Int J Oral Max-
illofac Implants 2009;24(4):727-733.
Osteotome sinus floor elevation without
bone grafting was performed in 32 patients
and 54 Straumann Tapered Implants were
placed in sites with a residual bone height
Selected literature ofpotential interest from
recently publishedjournals.
of between 1 and 6mm (mean height 3.8
± 1.2mm). All implants achieved primary
stability and were loaded after a mean 4.2
± 1.6 months. One-year implant survival
and success rates were 100% and 94.4%,
respectively, and mean bone gain was 2.5 ±
1.7mm and the mean crestal bone loss was
0.2 ± 0.8mm. Primary stability can therefore
be achieved with tapered implants in the pos-
terior maxilla without bone grafting.
Pjetursson BE, Rast C, Brägger U,
Schmidlin K, Zwahlen M, Lang NP.
Maxillary sinus floor elevation using
the (transalveolar) osteotome technique
with or without grafting material.
Part I: implant survival and patients’
perception. Clin Oral Implants Res
2009;20(7):667-676.
A total of 252 Straumann implants were
placed using a modified osteotome tech-
nique in 181 patients between 2000 and
2005. The implant survival rate was 97.4%
for a mean follow-up time of 3.2 years; sur-
vival rates were 91.3% at sites with ≤ 4mm
residual bone height, 90% for sites with
4–5mm residual bone height and 100% at
sites with ≥ 5mm residual bone height. The
survival rate was only 47.6% for 6mm long
implants, compared to 100%, 98.7% and
98.7% for implants 12, 10 and 8mm long,
respectively. Over 90% of patients expressed
satisfaction with the therapy, as measured by
visual analog scale, and the cost of therapy
was considered to be justified.
Pjetursson BE, Ignjatovic D, Matuliene
G, Brägger U, Schmidlin K, Lang NP.
Transalveolar maxillary sinus floor
elevation using osteotomes with or
without grafting material. Part II: radio-
graphic tissue remodeling. Clin Oral
Implants Res 2009;20(7):677-683.
A total of 252 Straumann implants were
placed using a modified osteotome tech-
nique in 181 patients between 2000 and
2005. Deproteinized bovine bone was
used as grafting material for 35% of the
implants, while no grafting material was used
for the remaining implants. Mean residual
bone height was 7.5 ± 2.2mm (range 2
to 12.7mm); the mean residual height at
sites with and without grafting material was
6.4mm and 8.1mm, respectively; the differ-
ence was significant. Mean bone gain with
grafting material was significantly greater
(4.1 ± 2.4mm compared to 1.7 ± 2.0mm
without grafting material). Substantial new
bone gain was therefore observed with
grafting material.
Siciliano VI, Salvi GE, Matarasso S,
Cafiero C, Blasi A, Lang NP. Soft tissue
healing at immediate transmucosal
STARGET 1 I 1060 SIMPLY DOING MORE
STARGET_1_2010_en.indd 60STARGET_1_2010_en.indd 60 21.12.2009 17:36:05 Uhr21.12.2009 17:36:05 Uhr

STARGET 1 I 10SIMPLY DOING MORE 61
implants placed into molar extrac-
tion sites with buccal self-contained
dehiscences. A 12-month controlled
clinical trial. Clin Oral Implants Res
2009;20(5):482-488.
Straumann Tapered Effect (TE) implants
were immediately placed in molar extrac-
tion sockets with buccal bone dehiscence in
15 patients, and peri-implant defects were
treated by a guided bone regeneration
technique. In addition, 15 tapered effect
implants were placed in healed molar sites in
15 patients (control group). After 12 months,
implant healing was uneventful in all cases,
and there were no implant failures. Probing
depth and CAL values were significantly
higher around the test implants, indicating
that immediate placement in molar extraction
sites with wide and shallow dehiscences may
result in less favorable outcomes.
Zijderveld SA, Schulten EAJM, Aartman
IHA, ten Bruggenkate CM. Long-term
changes in graft height after maxillary
sinus floor elevation with different graft-
ing materials: radiographic evaluation
with a minimum follow-up of 4.5 years.
Clin Oral Implants Res 2009;20(7):691-
700.
Maxillary sinus floor elevation was performed
in 20 patients with either autogenous bone
or -tricalcium phosphate; patients were
examined radiographically at least five times
in a 4-5-year period and measurements were
taken for BIC distally at the second most
posterior implant, halfway between this and
the posterior implant, and 5 mm distally to
the posterior implant. Vertical bone height
was significantly reduced at all locations,
with no significant differences between the
groups. A reduction in millimeters per month
was observed at all three locations, but there
was no significant difference in height reduc-
tion for vertical bone height and graft height
between the three locations.
STRAUMANN® SLACTIVE
Roccuzzo M, Wilson TG. A prospec-
tive study of 3 weeks’ loading of
chemically modified titanium implants
in the maxillary molar region: 1-year
results. Int J Oral Maxillofac Implants
2009;24(1):65-72.
Implant site preparation in 35 patients was
performed using osteotomes, with minimal
drilling, and Straumann® SLActive surface
implants were subsequently placed in the
maxillary molar area, with abutment connec-
tion and provisional restoration in occlusion
after 3 weeks. Pain was reported for six
patients after 3 weeks, so provisionalization
was postponed for another 4 weeks. There
were no implant failures or patient drop-
outs after 12 months, and there were no
significant differences in clinical parameters
between baseline and 12 months. Three-
week occlusal loading can therefore be suc-
cessfully performed with SLActive® implants.
Schätzle M, Männchen R, Balbach U,
Hämmerle CHF, Toutenburg H, Jung
RE. Stability change of chemically modi-
fied sandblasted/acid-etched titanium
palatal implants. A randomized control-
led clinical trial. Clin Oral Implants Res
2009;20(5):489-495.
Straumann® Orthosystem palatal implants
with either an SLA® or an SLActive® surface
were placed in 40 patients. Resonance
frequency analysis was performed at implant
placement and up to 84 days later. There
were no significant differences in implant
stability between the groups at placement
(ISQ 73.8 ± 5 and 72.7 ± 3.9 for SLA and
SLActive, respectively). ISQ values decreased
thereafter in both groups, increasing again
after 28 days in the modified SLA group and
after 35 days in the SLActive group, returning
to baseline values after 42 and 63 days,
respectively. Stability was significantly higher
in the SLActive group after 12 weeks.
STRAUMANN® BONECERAMIC
Jensen SS, Bornstein MM, Dard M,
Bosshardt DD, Buser D. Comparative
study of biphasic calcium phosphates
with different HA/TCP ratios in man-
dibular bone defects. A long-term
histomorphometric study in minipigs.
J Biomed Mater Res B Appl Biomater
2009;90(1):171-181.
Defects were prepared in the mandibles of
24 minipigs and treated with hydroxyapatite/
tricalcium phosphate in three different ratios
(20/80, 60/40 and 80/20) compared to
autogenous bone, deproteinized bovine bone
mineral (DBBM) or coagulum as controls.
Bone formation and filler degradation of HA/
TCP 20/80 was similar to autogenous bone,
while HA/TCP 60/40 and 80/20 were simi-
lar to DBBM. For all three test materials, bone
formation and filler degradation was inversely
proportional to the HA/TCP ratio. At all time
points (4, 13, 26 and 52 weeks), autogenous
bone showed the highest fraction of filler
surface covered with bone, while the fraction
was higher for DBBM than HA/TCP 80/20
and 60/40 in the early healing phase.
Schwarz F, Sager M, Ferrari D,
Mihatovic I, Becker J. Influence of
recombinant human platelet-derived
growth factor on lateral ridge augmen-
tation using biphasic calcium phosphate
and guided bone regeneration: a histo-
morphometric study in dogs.
J Periodontol 2009;80(8):1315-1323.
Lateral ridge defects in eight dogs were treated
with biphasic calcium phosphate plus collagen
membrane, with or without recombinant human
platelet-derived growth factor-BB (rhPDGF-BB)
and assessed after 3 weeks. Comparable
bone and blood vessel formation was observed
in both groups, but greater transglutaminase II
activity was observed in the rhPDGF-BB group,
resulting in significantly higher mean augment-
ed area and mineralized tissue.
Selected literature ofpotential interest fromrecently publishedjournals.
STARGET_1_2010_en.indd 61STARGET_1_2010_en.indd 61 21.12.2009 17:36:05 Uhr21.12.2009 17:36:05 Uhr

International education programat a high level
“Simply doing more“ applies to Straumann in education, too. In collaboration with the ITI and its
fellows it offers a broad range of high-quality international training and continuing education courses
on the most varied topics in implantology, prosthetics and oral tissue regeneration. This article gives
a brief overview of some of these and indicates where you can obtain further information or register
for one of the numerous events.
Transnational communication ofknowledge
For many years now, Straumannand the ITI (International Team forImplantology) have been highlysuccessful in organizing interna-tional continuing education courseson different topics in the area of
dental implantology and oral tis-sue regeneration. This internationalrange is an ideal complement tothe national courses available. Itenables practitioners to extendtheir knowledge and professionalnetwork purposefully in a globalcontext with top speakers andinstructors.
From theory to practice withnew information and modernequipment
In order to ensure constantly highcourse quality, Straumann and theITI rely on cooperation with expe-rienced and internationally well-known speakers and on courses
STRAUMANN AND ITI
STARGET 1 I 1062 EDUCATION
STARGET_1_2010_en.indd 62STARGET_1_2010_en.indd 62 21.12.2009 17:36:05 Uhr21.12.2009 17:36:05 Uhr

designed to cover all the relevantaspects of comprehensive and in-depth continuing education. Thecontents of the events are charac-terized by a balanced mixture ofscientific, medical and technicaltopics. The discussion of cases fromclinical practice along with the lat-est evidence-based medical infor-mation for treating them successfullyis supplemented optimally by livesurgeries and practical exercises.This is an optimal way to commu-nicate the translation of theory intopractice and it offers the possibilityof applying the acquired knowl-edge under expert instruction.
Broad range of topics
The spectrum of contents offeredinternationally and locally extendsfrom courses on regenerativeperiodontal surgery, GBR, implantsurgery and prosthetics to techni-cal and scientific subjects such asthe optimal use and integrationof CADCAM in practice and the
employment of implant-based treat-ment concepts with a view to opti-mal cost effectiveness for clinicianand patient.
Highlights with attractive frame-work programs
This international continuing educa-tion program contains highlightsthat are impressive not only withregard to the contents and highscientific level: the “ITI EducationWeeks“ at the universities of Bern,Stuttgart and Hong Kong, the suc-cessful “Icelandic Week“, whichwill take place for the third time in2010, the cadaver course at theUniversity of Vienna with its uniquepremises or the course on “ClinicalExperience in Advanced Surgery“in Brazil, which allows surgicaltechniques to be employed onpatients directly. These events com-bine education at the highest levelwith a framework program that willprovide their participants with last-ing memories.
Modular concept in accordancewith SAC guidelines
The range of courses is modularand structured in accordance withthe “SAC Classification in ImplantDentistry“1 guidelines. The treat-ment complexity of clinical casesand the associated treatment risksare classified into the three stagesS (Straightforward), A (Advanced)and C (Complex).
You will find more informationabout the international and localcourses on offer on the homepageof your regional Straumannbranch, in the current internationalcourse brochure, also availablethrough your regional Straumannpartner, or at www.iti.org.
STARGET 1 I 10 63EDUCATION
1 A. Dawson, S. Chen,D. Buser, L. Cordaro,W.Martin, U. Belser.„The SAC Classificationin Implant Dentistry“.Quintessence PublishingCo, 2009. ISBN 978-1-85097-188-7.www.quintessenz.de,www.quintessencepublishing.co.uk,www.quintpub.com.
Live-operation of Prof Daniel Buser at the University of Bern/Switzerland.
STARGET_1_2010_en.indd 63STARGET_1_2010_en.indd 63 21.12.2009 17:36:07 Uhr21.12.2009 17:36:07 Uhr
publications and events. The 2010Symposium motto reflects this his-tory: “30 Years of Leadership andCredibility.”
Much informative and livelydebate and incisive discussionsguaranteed
The faculty for the World Sympo-sium is made up of leading thinkersand opinion leaders in the field ofimplant dentistry from all over theworld and their presence promisesmuch informative and lively debateand incisive discussion. The care-fully balanced scientific programas well as the newly introducedpre-symposium courses and theprogram of social activities avail-able ensure that the ITI World Sym-posium 2010 will be the implantdentistry event of 2010 and onethat should not be missed underany circumstances.
A special year in ITI history
As one of the biggest events in theimplant dentistry calendar, the ITIWorld Symposium justly enjoys anexcellent reputation thanks to itstradition of focusing on cutting-edgeissues and providing clinicians withsolid information as well as theopportunity for discussion with opin-ion leaders from all over the world.The upcoming ITI World Symposiumin Geneva promises to fulfill expec-tations for an incisive and challeng-ing scientific program coupled witha strong practice-oriented approach.2010 is a special year for the ITIas it will be celebrating its 30th anni-versary.
From visionary pioneeringwork to a leading, internationalorganization
As an independent, multidisciplinaryacademic organization, the Inter-national Team for Implantology hasgrown from a small group of vision-ary pioneers in implant dentistry toa leading international organizationwith more than 6,000 Fellows andMembers and national sections in24 countries. The ITI’s mission: “topromote and disseminate knowl-edge on all aspects of implantdentistry and related tissue regen-eration” lays particular emphasis oneducation to ensure that practition-ers are able to deliver optimal treat-ment to their patients. Throughout its30 years, the ITI has led the wayin implant dentistry, taking scientificrigor as its touchstone, and thispervades every aspect of its profes-sional activities, including its many
“30 Years of Leadership and Credibility”ITI WORLD SYMPOSIUM 2010
Further information, registration & accommodation:Internet: www.iti.org/worldsymposium2010E-Mail: [email protected]: +49 89 5482 3462Fax: +49 89 5482 3443
STARGET 1 I 1064 EVENTS
15 – 17 April 2010 in Geneva/Switzerland at the Palexpo Conference Center
STARGET_1_2010_en.indd 64STARGET_1_2010_en.indd 64 21.12.2009 17:36:08 Uhr21.12.2009 17:36:08 Uhr

STARGET 1 I 10 65EVENTS
An interview with Prof Dr Daniel Buser and Dr Stephen Chen
on the ITI World Symposium 2010 in Geneva, Switzerland
“We want to give ourparticipants a greateducational experience”
INTERVIEW
Dr Chen, you are the first Austral-ian Chairman of the ITI WorldSymposium Scientific ProgramCommittee. The symposium willbe held in Geneva, Switzerland– a bit far from Australia. WhyGeneva?
Stephen Chen: We chose Genevabecause it is a central locationfor most of our ITI Members andFellows, and is easy to travel to.Geneva has outstanding infrastruc-ture and exhibition facilities withexcellent accommodation andquality hotels in the vicinity – and itis a beautiful and picturesque city.The other very important point isthat 2010 marks the 30th anniver-sary of the ITI. Although the ITI is aninternational organization, it wasfounded in Switzerland and wewould like to bring this event backto Switzerland to celebrate this30th birthday in the ITI’s birthplace.
Prof Buser, as the new ITI Presi-dent and as a member of theScientific Program Committee, youwere strongly involved in design-ing the program. The theme of theITI World Symposium is “30 Yearsof Leadership and Credibility”.Can you explain to our readerswhat stands behind this claim?
Daniel Buser: With this title wewould like to reflect the leadershipthe ITI has provided in all theseyears. When you analyze thecurrent state of implant dentistryand the milestones achieved, youcan easily recognize that the ITIhas had an impressive influenceover the progress and the futuredevelopment of implant therapy.That involves such topics as thenon-submerged healing modalityand the discussion on surfacetechnologies and biologic width.All these aspects have beenstrongly influenced by the ITI.
Geneva, a beautiful and historiccity in the heart of Europe, is theideal location for the ITI WorldSymposium. This choice wasbased on the excellent infra-structure offered by the PalexpoConference Center, which willprovide the best possible condi-tions for both participants andexhibitors. With its Riviera-likeatmosphere, Geneva has areputation for shopping, bankingand elegance as well as beingthe center for a number of impor-tant, international organizations.The city nestles at the foot of themountains while the lake spreadsout its sparkling expanse infront of it before receding in thedistance to the jagged line ofsnowy white peaks on the hori-zon that are the Alps.For more information visitwww.geneva-tourism.ch
STARGET_1_2010_en.indd 65STARGET_1_2010_en.indd 65 21.12.2009 17:36:09 Uhr21.12.2009 17:36:09 Uhr

STARGET 1 I 1066 EVENTS
The title may not sound too modestbut, in my opinion, it clearly reflectsour pride.
OVERALL, IT IS A STRONG PROGRAM AND EVERY SESSION AND ALL THE SPEAKERS
ARE GOING TO PROVIDE US WITH THE BEST AND MOST UP-TO-DATE INFORMATION
ABOUT THE TOPICS THAT THEY HAVE BEEN ASSIGNED TO. Stephen Chen
novel procedures and how theymight fit into the practice of implantdentistry. The third day reflects avery important and growing areain implant dentistry: namely the rec-ognition that complications are areality of daily practice. Therefore,this day will be devoted to lookingat the different aspects of complica-tions, from surgical and biologic totechnical and, importantly, estheticcomplications. So there is a natu-ral progression through the threedays which I think should be well-received by the audience. Person-ally, I have no favourites amongstthe topics. Overall, it is a strongprogram and every session and allthe speakers are going to provideus with the best and most up-to-dateinformation about the topics thatthey have been assigned to.
Prof Buser, who should attend theITI World Symposium? Is this eventintended only for ITI Fellows andMembers or Straumann users?
Dr Chen, what will be the maintopics and especially the high-lights of the upcoming sympo-sium? What will be your ownfavourites among the presenta-tions?
Chen: The scientific program com-mittee decided to structure the threedays of the Symposium accord-ing to specific themes that reflectclinical practice. On the first day,new clinical methods of diagnosisand treatment planning will bepresented and discussed. The sec-ond day is devoted to treatmentprocedures – not just proven treat-ment procedures but also new and
STARGET_1_2010_en.indd 66STARGET_1_2010_en.indd 66 21.12.2009 17:36:09 Uhr21.12.2009 17:36:09 Uhr

STARGET 1 I 10 67EVENTS
Dr Stephen Chen
Dr Chen is a specialist periodontist in privatepractice in Melbourne, Australia and SeniorFellow at the School of Dentistry, Universityof Melbourne. He graduated from the Uni-versity of Malaya and obtained the MDScdegree from the University of Melbourneand FRACDS. Dr Chen is a Fellow of the ITI,Chairman of the Australasian ITI Section andalso Chairman of the ITI Education Commit-tee and Education Core Group.
Prof Dr Daniel Buser
Prof Dr Daniel Buser is Professor and Chair-man of the Department of Oral Surgery andStomatology at the University of Bern, Swit-zerland. He has been an ITI Fellow since1986 and a member of various committees,most recently Chairman of the EducationCommittee, as well as taking on numerousadditional functions within the organization.Since August 2009, Daniel Buser has beenPresident of the ITI.
Buser: In general, it is intended toattract dentists with an interest inimplant dentistry. Of course we willsee a high share of participantswho are ITI Members and Fellows.But it certainly will be a very instruc-tive experience for non-ITI partici-pants, too.
Dr Chen, the last ITI World Sym-posium in 2007 in New YorkCity set a new record with about3,000 participants. How manyparticipants do you think willshow up in Geneva, also consid-ering these economically chal-lenging times?
Chen: I am very confident that wewill exceed those numbers in Gene-va. Much has been said about thecurrent economic challenges andthe global downturn but the truthof the matter is that dentists willalways seek out quality in continu-ing education. If we put on a strongprogram, irrespective of the eco-nomic times, people will come fromfar and wide.
Prof Buser, you have attendedand lectured at many congressesand symposia all over the world.What makes the ITI World Sym-posium unique?
Buser: I see three reasons forthe uniqueness of the ITI WorldSymposium. Firstly, we alwayshave focused on two topics anddiscussed them very thoroughly.Secondly, it is a truly internationalconference. We had more thansixty nations represented at the lastITI World Symposium in New Yorkin 2007 and I think that this stronginternational touch is an important
factor. And thirdly, the programsof ITI symposia have always beenof an excellent quality which hasled to a first-class reputation that isrecognized by the scientific com-munity.
Dr Chen, as a novelty, the ITIWorld Symposium will featurePre-Symposium Courses? Whatis the intention behind these newevents?
Chen: We want to give ourparticipants a great educationalexperience. The Scientific ProgramCommittee decided to hold twoPre-Symposium Courses that will
address two areas of implantdentistry in detail. The first courseis a bone grafting course for sitedevelopment. The speakers willreport on the latest techniques andprocedures to augment a site priorto implant placement. The secondcourse is a very interesting andtopical one: it deals with soft tis-sue management and conditioningaround implants with the focus onesthetics.
Dr Chen, Prof Buser, many thanksfor the conversation. We wishyou and your team a successfulITI World Symposium 2010 inGeneva, Switzerland.
STARGET_1_2010_en.indd 67STARGET_1_2010_en.indd 67 21.12.2009 17:36:10 Uhr21.12.2009 17:36:10 Uhr

STARGET 1 I 10 EVENTS68
Soft tissue management and conditioningaround implants in the esthetic zone.
Lecture Speakers9:15 Welcome and introduction
Chairmen: Luca Cordaro (ITA), Dean Morton (USA)9:30 Soft tissue conditions for peri-implant tissue health and optimum esthetics Mario Roccuzzo (ITA)
10:10 Ridge preservation: Does it affect soft tissues and esthetic outcome? Paolo Casentini (ITA)10:50 Coffee break11:10 Soft tissue augmentation at the time of implant placement or at second surgery Anthony Sclar (USA)11:50 How do provisional restorations influence our esthetic outcome? Daniel Thoma (SUI)
Are they always needed?12:30 Lunch13:30 Artificial gingiva in the aesthetic zone: a defeat or the most predictable Francesca Vailati (SUI)
and durable aesthetic outcome?14:10 Soft tissue contouring in the provisional phase for multiple missing teeth. Javier Fabrega (ESP)
Different options with transmucosal or bone level implants14:50 Treatment of mucosal recession affecting implant restorations Rino Burkhardt (SUI)15:30 End of pre-symposium
Wednesday, April 14, 2010
Bone grafting for implant site development.
Lecture Speakers9:15 Welcome and introduction
Chairmen: Hideaki Katsuyama (JPN), Gerhard Wahl (GER)9:30 Dimensional and positional requirements of bone for optimum James Ruskin (USA)
function and esthetics10:10 Harvesting of autologous bone – indications for selection of donor sites, Timothy Head (CAN)
morbidity and complications10:50 Coffee break11:10 Procedures for lateral and vertical augmentation of ridges Hendrik Terheyden (GER)
using autogenous bone blocks11:50 Allografts and xenografts Jürgen Becker (GER)12:30 Lunch13:30 Sinus floor grafting using the lateral window technique Hideaki Katsuyama (JPN)14:10 Sinus floor grafting using the transalveolar technique Paul Fugazzotto (USA)14:50 Distraction osteogenesis Paul Rousseau (FRA)15:30 End of pre-symposium
PRE-SYMPOSIUM COURSE 2
PRE-SYMPOSIUM COURSE 1
STARGET_1_2010_en.indd 68STARGET_1_2010_en.indd 68 21.12.2009 17:36:10 Uhr21.12.2009 17:36:10 Uhr

STARGET 1 I 10EVENTS 69
Thursday, April 15, 2010
New Clinical Methods for Diagnosisand Treatment Planning.
Lecture Speakers9:00 Opening of the scientific meeting Daniel Buser (SUI),
Stephen T. Chen (AUS)9:15 Keynote Address: Pioneering a more sustainable future Bertrand Piccard
Session 1: Computer-based diagnostic and planning tools for implant dentistryModerators: Anthony Dickinson (AUS), Johannes Kleinheinz (GER)
10:00 Improving the reliability of computerized reformatted radiological images William Scarfe (USA)10:30 Has cone beam CT made conventional CT obsolete? Bernard Koong (AUS)11:00 Coffee break11:30 From planning to surgery: a critique of guidance Ronald Ernst Jung (SUI)
and navigation techniques12:00 Implant treatment planning software: an essential tool or gadgetry? Daniel Wismeijer (NED)12:30 Panel discussion13:00 Lunch
Session 2: The impact of new technologies on treatment planningModerators: Tom Taylor (USA), Ray Williams (USA)
14:30 Periodontal regenerative procedures in the era of implant dentistry Nikos Donos (GBR)15:00 Choosing the implant design: soft tissue level or bone level? Christoph Hammerle (SUI)15:30 New narrow body implants – expanded treatment opportunities? Paul Stone (GBR)16:00 The SLActive surface – new promise for compromised sites? Frank Schwarz (GER)16:30 Panel discussion
Session 3: Limited Attendance Session (5 parallel presentations)Diagnosis and planning Moderator: Merete Aaboe (DEN)
17:00 3A Planning for patients with hypodontia and anodontia Nadine Brodala (USA)17:25 3A CT evaluation – when, where and how? Robert A. Jaffin (USA)17:50 3A Soft tissue visualization by CT Alessandro Lourenço
Januário (BRA)18:15 3A Anatomy as a risk factor Andre van Zyl (RSA)
Surgery Moderator: Christiaan ten Bruggenkate (NED)17:00 3B Immediate implant placement in the esthetic zone Ken Akimoto (USA)17:25 3B Ridge expansion – esthetic and surgical outcomes Dehua Li (CHN)17:50 3B Computer-guided implant placement Ali Tahmaseb (NED)18:15 3B Replacement of hopless teeth in the esthetic zone Farhad Boltchi (USA)
Restorative procedures Moderator: Eiji Funakoshi (JPN)17:00 3C Attachment systems for implant overdentures Arne Boeckler (GER)17:25 3C Immediate loading of full-arch restorations Jeffrey Ganeles (USA)17:50 3C Immediate loading of two implant overdentures Geert Stoker (NED)18:15 3C Transitional appliances for immediate function of distally tilted implants Sergio Piano (ITA)
Restorative procedures Moderator: Javier Fabrega (ESP)17:00 3D Provisionals and soft tissue management Diego Bechelli (ARG)17:25 3D Abutment material and mucosal color Diego Lops (ITA)17:50 3D Cement vs. screw-retained restorations John Lucas (AUS)18:15 3D Implants and orthodontics Wolfgang Trumm (GER)
Outcomes Moderator: Philip Freiberger (GBR)
STARGET_1_2010_en.indd 69STARGET_1_2010_en.indd 69 21.12.2009 17:36:10 Uhr21.12.2009 17:36:10 Uhr

STARGET 1 I 10 EVENTS70
New and Proven Treatment Procedures.
Lecture Speakers
Session 4: Limited Attendance Session (5 parallel presentations)Risk factors Moderator: Alex Tsai (TPE)
8:00 4A Critical factors for esthetic stability Akshay Kumar (USA)8:25 4A Risk markers for oral bisphosphonate-related osteonecrosis Yong-Dae Kwon (KOR)8:50 4A Excess cement and peri-implant disease Thomas Wilson (USA)9:15 4A Osteoporosis as a risk factor for implant failure Cermal Ucer (GBR)
Surgery Moderator: Juan Carlos García Lara (MEX)8:00 4B Minimally invasive sinus lift procedures Lars Ake Johansson (SWE)8:25 4B Vertical augmentation of the atrophic posterior mandible Waldemar Polido (BRA)8:50 4B Vertical and lateral bone augmentation using biphasic calcium phosphate Andres Stricker (GER)9:15 4B Distraction osteogenesis in partially dentate patients Eppo Wolvius (NED)
Surgery Moderator: Gerrit Wyma (RSA)8:00 4C Microvascular bone transfer for ridge augmentation Alexander Gaggl (AUT)8:25 4C Piezoelectric bone surgery in implant dentistry Nathan Hodges (USA)8:50 4C Prosthodontically-driven tissue engineering George Sandor (CAN)9:15 4C Post-extraction implants and immediate loading Juan Blanco Carrión (ESP)
Restorative procedures Moderator: Richard Leesungbok (KOR)8:00 4D Occlusal reconstruction based on maxillofacial skeletal morphology Masaaki Hojo (JPN)8:25 4D Combining pink acrylic and porcelain in the estetic zone Steven Present (USA)8:50 4D Prosthetic reconstruction of the resected mandible Robert Lee Schneider (USA)9:15 4D Principles of Attachment Selection in Overdenture Treatment Siegfried Heckmann (GER)
Outcomes Moderator: Timothy W. Head (CAN)8:00 4E Immediate non-functional loading of implants in the posterior maxilla Jonathan Mark Korostoff
(USA)8:25 4E Ridge preservation Nikolaos Mardas (GBR)8:50 4E After implant placement and loading – what then? Per Nygaard-Ostby (NOR)9:15 4E Immediately temporized implants in the esthetic zone Barry Levin (USA)9:40 Coffee break
Session 5: Surgical proceduresModerators: Steve Barter (GBR), David Cochran (USA)
10:00 Bone grafting for localized defects – simultaneous or staged? Thomas von Arx (SUI)10:30 Sinus floor augmentation Matteo Chiapasco (ITA)11:00 Short implants – what is short and what is not? Franck Renouard (FRA)11:30 Flapless surgery Stephen T. Chen (AUS)12:00 Panel discussion12:30 Lunch
Friday, April 16, 2010
17:00 3E 10-year outcome of SLA implants in the edentulous maxilla Kerstin Fischer (SWE)17:25 3E Reduced diameter implants in the posterior maxilla João Garcez Filho (BRA)17:50 3E Soft tissue stability around immediately placed and restored implants Pedro Tortamano Neto (BRA)18:15 3E Esthetic outcomes with bone level implants Chris Evans (AUS)18:40 End of day 1
STARGET_1_2010_en.indd 70STARGET_1_2010_en.indd 70 21.12.2009 17:36:11 Uhr21.12.2009 17:36:11 Uhr

STARGET 1 I 10EVENTS 71
Lecture Speakers
Session 6: Treatment procedures – prosthetic and technicalModerators: Frauke Müller (SUI), Tony Dawson (AUS)
14:00 Bone and tissue level implants – prosthetic implications Will Martin (USA)14:30 From casting to CAD/CAM: navigating the technologic advances affecting Brody Hildebrand (USA)
clinicians today15:00 Evolution of loading protocols in oral implantology German Gallucci (USA)15:30 The technicians’ viewpoint – material and technical evolution Michel Magne (USA)
in implant dentistry16:00 Panel discussion
Session 7: ITI Research Competition16:30 Oral presentations (5 categories)
(10 minutes speaking time, 2 minutes for questions + answers per presentation)18:30 End of day 2
Saturday, April 17, 2010
Complications in Implant Dentistryor Dealing with Reality.
Lecture Speakers
Session 8: Surgical and biologic complicationsModerators: Joseph Fiorellini (USA), Erik Hjørting-Hansen (DEN)
9:00 Complications – introduction and overview Niklaus P. Lang (HKG)9:30 Peri-operative complications – occurrence, prevention, and handling Simon Storgård Jensen (DEN)
10:00 Biologic complications – prevention and management Giovanni E. Salvi (SUI)10:30 Coffee break
Session 9: Management of technical complicationsModerators: Andrea Mombelli (SUI), Steven Eckert (USA)
11:00 Technical complications – implant-related Bjarni Elvar Pjetursson (ICE)11:30 Technical complications – prosthesis-related Dean Morton (USA)12:00 Panel discussion12:30 Lunch14:00 ITI Award Ceremony
Session 10: Esthetic complicationsModerators: Lisa Heitz-Mayfield (AUS), Hans-Peter Weber (USA)
14:30 Surgical and prosthodontic management of esthetic complications Daniel Buser and Urs Belser (SUI)15:30 Interactive case discussion
Restorative Dentist – Frank Higginbottom (USA)Periodontist – Luca Cordaro (ITA)
Maxillofacial Surgeon – Dieter Weingart (GER)Technician – Alwin Schönenberger (SUI)
16:30 Closing remarks Daniel Buser (SUI)16:45 End of ITI World Symposium 2010
STARGET_1_2010_en.indd 71STARGET_1_2010_en.indd 71 21.12.2009 17:36:11 Uhr21.12.2009 17:36:11 Uhr
4–6 March 2010 in Orlando/Florida
“The Formula for Predictable ImplantSuccess” – 25th Anniversary Annual Meetingof the Academy of Osseointegration
The Academy of Osseointegration (AO) is celebrating 25 Years of
excellence in education and development of implant technology
and clinical-surgical practice. Throughout the last quarter-century,
the AO has come together to discover and share new ideas,
approaches and technology that have guided dental implant
arena into the 21st century. This year’s Annual Meeting continues
the tradition of promoting professional excellence and fellowship
in the beautiful city of Orlando in Florida.
Straumann at the AOJoin Straumann at booth #419 to learnabout Straumann’s formula – innova-tion and scientific evidence – for pre-dictable implant success. ExperienceRoxolid™ and Straumann guided sur-gery through hands-on at our booth.
On Thursday, March 4, from8:00am–12:00 noon, Straumannwill sponsor a Corporate Forumwith lectures of five internationally-renowned speakers.
PREVIEW
STARGET 1 I 1072 EVENTS
© Orlando pictures:Orlando/Orange Coun-ty Convention & VisitorsBureau, Inc.
Session 1AEvolving treatment options
in GBR – Evidence oftodays techniques and
future perspectives
Christoph Hämmerle
DMD, Prof. Dr. Professor and Chairmanof the Department of Fixed and Remo-vable Prosthodontics and Dental MaterialScience, University of Zurich, Switzerland.
STARGET_1_2010_en.indd 72STARGET_1_2010_en.indd 72 21.12.2009 17:36:11 Uhr21.12.2009 17:36:11 Uhr

OrlandoThe 2010 Annual Meeting ofthe AO will be held at the WaltDisney World Dolphin Resort®
in Orlando, Florida. A recipientof the prestigious Meetings &Conventions Hall of Fame Award,the Walt Disney World DolphinResort® is a respected and recog-nized leader in the US conven-tion resort arena. Ideally locatedin the heart of the Walt DisneyWorld®, guests enjoy immediateaccess to all adjacent themeparks and attractions. Experiencethe exclusive Disney Differences,sophisticated guest rooms featur-ing Westin Heavenly Beds®,the luxurious Mandara Spa and17 world-class restaurants andlounges. For more information visit:www.orlandoinfo.com anddisneyworld.disney.go.com
STARGET 1 I 10 73EVENTS
For more information visit the AO website:www.osseo.org
Session 1BRoxolid™ – more treatment
options in placingsmall diameter implants
Session 2ADigital Interdisciplinary Implant Dentistry – Part I
Session 2BDigital Interdisciplinary Implant Dentistry – Part II
DDS, Diplomate, American Board ofPeriodontology, Clinical AssociateProfessor, Dental School, Universityof Texas at San Antonio, BaylorCollege of Dentistry
Thomas G. Wilson, Jr.
CDT, Founder of Singler DentalCeramics, Inc. with focus on com-plex restorative cases and implantrestorations.
Jeff Singler
DMD, PhD, Sweden
Jan Gottlow
DDS. Clinical Associate Professor,Department of Oral and Maxiol-lofacial Surgery and Pharmacology,Restorative Sciences and GraduateProsthodontics, Baylor College ofDentistry; Clinical Associate Profes-sor, Department of Periodontics,University of Texas San Antonio
Frank L. Higginbottom
STARGET_1_2010_en.indd 73STARGET_1_2010_en.indd 73 21.12.2009 17:36:13 Uhr21.12.2009 17:36:13 Uhr
9–11 March 2010 at the International Convention & Exhibition Center in Dubai
14th Annual UAE International DentalConference & Arab Dental Exhibition (AEEDC)
The AEEDC Conference is a key platform for exchanging knowledge and information among dental
colleagues and experts in the Gulf, Middle East and North Africa regions. Over the 3-day conference
and exhibition, 20,000 visitors are expected. The conference will cover numerous topics highlighting
the advances in dentistry and many other dental techniques essential to dental practice and the satis-
faction of the entire dental sector. A comprehensive scientific program is provided for the education
and enhancement of dental practices. The scientific conference within the event will host international
and regional experts around the globe to present a series of lectures and specialized courses based
on the latest researches and clinical experiences.
DubaiIn addition to an appealing business envi-ronment, Dubai has something to offer foreveryone. For example perfect winter climate,superb beachside resorts, world class shop-ping, spectacular beaches, lush green parks,great facilities for a variety of sports and leisureactivities. For centuries hospitality has beenDubai’s tradition, nowadays Dubai extends thiswelcome to holiday makers as well as businessvisitors, offering facilities of the highest interna-tional standards combined with the charm andadventure of Arabia – an exceptional blendof modern city and timeless desert. For moreinformation visit www.dubaitourism.ae
PREVIEW
STARGET 1 I 1074 EVENTS
STARGET_1_2010_en.indd 74STARGET_1_2010_en.indd 74 21.12.2009 17:36:15 Uhr21.12.2009 17:36:15 Uhr

Also visit the Straumann booth and learn more about Straumann’s latestinnovations, such as Straumann® Roxolid™ (see p. 18–25).
Straumann at the AEEDCOn Wednesday, March 9 in the scientific program, three speakers will present their experiences withthe Straumann® Dental Implant System.
STARGET 1 I 10 75EVENTS
Dr Joe Bassil
Private practice in Beirut/Lebanon
Oral surgeon at the Lebanese ArmyHospital in Beirut
Senior Lecturer at the Department ofOral Surgery of the Saint JosephUniversity in Beirut
ITI Fellow
Dr Dr Frank Palm
Specialist in oromaxillofacial surgery
Chief of the Oromaxillofacial SurgeryDepartment at Klinikum Konstanz/Germany
Professor of implantology and oralsurgery at the University of Pisa/Italy
ITI Fellow
Ass. Prof Dr Dr Bilal Al-Nawas
Specialist in oromaxillofacial surgery
Chief of the Oralmaxillofacial SurgeryDepartment at the University HospitalMainz/Germany
ITI Fellow
Bone Level implantsand tissue level implantsused in atrophic jaws –2 different implant philo-sophies with 2 different
treatment concepts
Small diameter implants –where advanced materials
make a difference
Reconstruction of theseverely resorbed max-illa with a combinationof sinus augmentation,
onlay bone grafting, andimplants for patients with
Ectodermal Dysplasia
AEEDC 2010March 9–11, 2010Dubai International Convention & Exhibition CenterTuesday – Thursday: 10:00 am–6:00pmRefer to program for detailsUSD $220 (before December 31, 2009)USD $270 (after December 31, 2009)(USD $435 (on site registration))
www.aeedc.com
OVERVIEWDates:Venue:
Exhibition hours:Conference hours:
Admission fees for conference:
Information and registration:
STARGET_1_2010_en.indd 75STARGET_1_2010_en.indd 75 21.12.2009 17:36:16 Uhr21.12.2009 17:36:16 Uhr

30 September – 3 October 2009 at the Grimaldi Forum in Monaco
“Guidelines for the Practitioner” –18th Annual Conference of the EAO
REVIEW
STARGET 1 I 1076 EVENTS
Official Roxolid™ launch
The 18th Annual Conference of theEuropean Association for Osseointe-gration, one of the world’s biggestand most important internationalmeetings in implant dentistry, attract-ed over 3,000 dental profession-als from 71 countries. Althoughthe Mediterranean atmosphere ofMonaco and the beautiful weatheroffered a lot of distraction, thescientific sessions were very well
attended throughout the conference.Straumann officially launched itsnew innovative implant materialRoxolid™ in the European market(see p. 18–21).
Straumann Satellite Symposium
In the Straumann Satellite Sympo-sium, Prof Bilal Al-Nawas gavea lecture on Roxolid™ and in thisconnection presented the latestresults from the various pre-clinical
and clinical studies and the ben-efits especially in cases of narrowbone ridges. His presentation andthose of Dr David Schwab, Dr LucaCordaro, Dr Ronald Jung and DrJavier Fábrega can be reviewedonline at www.straumann.com/eao_monaco
STARGET_1_2010_en.indd 76STARGET_1_2010_en.indd 76 21.12.2009 17:36:17 Uhr21.12.2009 17:36:17 Uhr
STARGET 1 I 10 77EVENTS
Preview: EAO 2010 in GlasgowThe next EAO conference will be held in the historic city of Glasgow,Scotland (UK), 6 –9 October 2010. Don’t miss the StraumannSatellite Symposium scheduled for Thursday, 7 October 2010 from11:00 am to 1:00 pm. Should you wish to be kept informed aboutStraumann activities at the EAO Glasgow, please send an e-mail [email protected]. For updated program information & regis-tration, visit the official EAO website: www.eao.org
The “Armadillo”, part of SECC, the Scottish Exhibition&Conference Centre
STARGET_1_2010_en.indd 77STARGET_1_2010_en.indd 77 21.12.2009 17:36:19 Uhr21.12.2009 17:36:19 Uhr
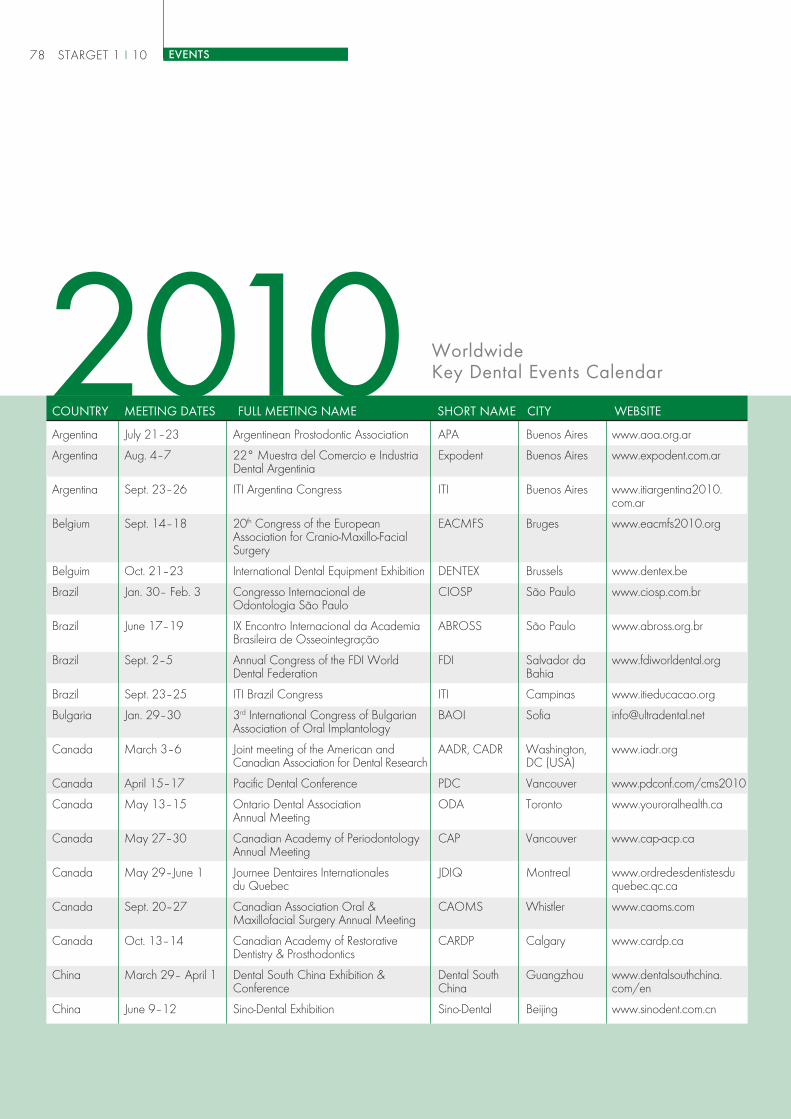
LAND
Argentina July 21–23 Argentinean Prostodontic Association APA Buenos Aires www.aoa.org.ar
Argentina Aug. 4–7 22° Muestra del Comercio e Industria Expodent Buenos Aires www.expodent.com.arDental Argentinia
Argentina Sept. 23–26 ITI Argentina Congress ITI Buenos Aires www.itiargentina2010.com.ar
Belgium Sept. 14–18 20th Congress of the European EACMFS Bruges www.eacmfs2010.orgAssociation for Cranio-Maxillo-FacialSurgery
Belguim Oct. 21–23 International Dental Equipment Exhibition DENTEX Brussels www.dentex.be
Brazil Jan. 30– Feb. 3 Congresso Internacional de CIOSP São Paulo www.ciosp.com.brOdontologia São Paulo
Brazil June 17–19 IX Encontro Internacional da Academia ABROSS São Paulo www.abross.org.brBrasileira de Osseointegração
Brazil Sept. 2–5 Annual Congress of the FDI World FDI Salvador da www.fdiworldental.orgDental Federation Bahia
Brazil Sept. 23–25 ITI Brazil Congress ITI Campinas www.itieducacao.org
Bulgaria Jan. 29–30 3rd International Congress of Bulgarian BAOI Sofia [email protected] of Oral Implantology
Canada March 3–6 Joint meeting of the American and AADR, CADR Washington, www.iadr.orgCanadian Association for Dental Research DC (USA)
Canada April 15–17 Pacific Dental Conference PDC Vancouver www.pdconf.com/cms2010
Canada May 13–15 Ontario Dental Association ODA Toronto www.youroralhealth.caAnnual Meeting
Canada May 27–30 Canadian Academy of Periodontology CAP Vancouver www.cap-acp.caAnnual Meeting
Canada May 29–June 1 Journee Dentaires Internationales JDIQ Montreal www.ordredesdentistesdudu Quebec quebec.qc.ca
Canada Sept. 20–27 Canadian Association Oral & CAOMS Whistler www.caoms.comMaxillofacial Surgery Annual Meeting
Canada Oct. 13–14 Canadian Academy of Restorative CARDP Calgary www.cardp.caDentistry & Prosthodontics
China March 29– April 1 Dental South China Exhibition & Dental South Guangzhou www.dentalsouthchina.Conference China com/en
China June 9–12 Sino-Dental Exhibition Sino-Dental Beijing www.sinodent.com.cn
WorldwideKey Dental Events Calendar2010
COUNTRY MEETING DATES FULL MEETING NAME SHORT NAME CITY WEBSITE
STARGET 1 I 1078 EVENTS
STARGET_1_2010_en.indd 78STARGET_1_2010_en.indd 78 21.12.2009 17:36:22 Uhr21.12.2009 17:36:22 Uhr

SHORT NAME CITY WEBSITEMEETING DATES FULL MEETING NAMECOUNTRY
China Oct. 27–30 13th China International Exhibition & DenTech China Shanghai www.dentech.com.cnSymposium on Dental Equipment,Technology & Products
Denmark April 15–17 Scandinavian Dental Fair SCANDEFA Copenhagen www.scandefa.dk
Finland March 20 Apollonia Symposium 2010 Apollonia Tampere www.apollonia.fi
Finland Nov. 12–14 Finnish Dental Congress and Exhibition Odontologi Helsinki www.apollonia.fi
France Feb. 4–6 Dental Forum Dental Forum Vincennes www.dentalforum2010.com
France Nov. 23–27 Congrès de l‘Association Dentaire ADF Paris www.adfcongres.comFrançaise
Germany May 12–14 Jahrestagung der Arbeitsgemeinschaft AgKiefer Bad Homburg www.ag-kiefer.deKieferchirurgie
Germany May 26–29 Jahrestagung der Deutschen DGMKG Munich www.mkg-chirurgie.deGesellschaft für MKG-Chirurgie
Germany June 3–5 Jahrestagung der Arbeitsgemeinschaft ADT Stuttgart www.ag-dentale-Dentale Technologie technologie.de
Germany Nov. 10–13 Deutscher Zahnärztetag ZÄ-Tag Frankfurt www.dzaet.de
Germany Nov. 24–27 Jahrestagung der Deutschen DGI Hamburg www.dgi-ev.deGesellschaft für Implantologie
Indonesia April 29–May 1 Pertemuan Ilmiah dan Teknologi Gigi PITEKGI Jakarta pitekgi.moestopo.ac.idKedokteran
Ireland May 12–15 Irish Dental Association Annual IDA Galway www.dentist.ieConference
Israel Feb. 3–4 The Annual Meeting of the Israel Perio Tel Aviv www.perio.org.ilPeriodontal and Osseintegration Society
Italy Feb. 5–6 Congresso Internazionale SIO SIO Rome www.osteointegrazione.it
Italy April 16–17 Meeting Mediterraneo AIOP SICOI AIOP - SICOI Riccione www.sicoi.it
Italy May 8 Corso di aggiornamento SIO – SIO Bologna www.osteointegrazione.itAlternative terapeutiche a confronto:rapporti costi-benefici
Italy Oct. 8–9 SICOI Congresso Nazionale SICOI Milan www.sicoi.it
Japan May 14–15 ICOI Japan Advanced Implant ICOI Yokohama www.icoi.jpSymposium
Japan June 12–13 The Academy of Clinical Dentistry ACD Tokyo www.ago.ac
STARGET 1 I 10 79EVENTS
STARGET_1_2010_en.indd 79STARGET_1_2010_en.indd 79 21.12.2009 17:36:22 Uhr21.12.2009 17:36:22 Uhr

LAND SHORT NAME CITY WEBSITEMEETING DATES FULL MEETING NAMECOUNTRY
Japan Sept. 17–19 Japanese Society of Oral Implantology JSOI Sapporo www.jsoi.org
Japan Oct. 8–10 Quintessence World Dental Show 2010 QU Yokohama www.quint-j.co.jp
Japan Oct. 17–18 Japanese Society of Oral and JSOMS Chiba www.jsoms.or.jpMaxillofacial Surgeons
Korea March 28 Korean Academy of Oral & KAOMI Seoul www.implant.or.krMaxillofacial Implantology
Korea April 9–11 Korean Academy of Prosthodontics KAP Seoul www.kap.or.kr
Korea May 28–29 Korean Academy of Periodontology – KPERIO Seoul www.kperio.orgSpring Meeting
Korea June 25–27 Seoul International Dental Exhibition & SIDEX Seoul www.sidex.or.krScientific Congress
Korea Nov. 27–28 Korean Academy of Periodontology – KPERIO Seoul www.kperio.orgAutumn Meeting
Malaysia Nov. 26–29 9th Asian Congress on Oral & ACOMS Kuala Lumpur www.acoms2010.orgMaxillofacial Surgery
Norway Jan. 7–10 Vestlandsmøtet VESTLANDS- Bergen www.tannlegeforeningen.noMØTET
Norway May 6–8 SFOMK Congress Oslo NFOKOM Oslo www.kjevekirurgi.org
Norway April 22–24 Midt Norge Møtet MNM Trondheim www.tannlegeforeningen.no
Norway Oct. 14–16 Nordental NORDENTAL Lillestrøm www.tannlegeforeningen.no
Singapore April 16–18 International Dental Exihibition and IDEM Singapore www.idem-singapore.comMeeting
South Africa July 9–10 University of Pretoria and the ITI – UP ITI 2010 Pretoria www.itisouthafrica.orgLatest Developments in Implant Dentistry
South Africa Oct. 29–Nov. 1 South African Dental Association SADA IDEC Durban www.sadaidec2010.co.zaInternational Dental Exhibition andCongress
Spain March 11–13 11th Expodental EXPODENTAL Madrid www.expodental.ifema.es
Spain May 20–22 44th Reunión Española de la SEPA Girona www.sepa.esSociedad Española de Periodonciay Osteintegración
Spain July 14–17 88th General Session & Exhibition IADR Barcelona www.iadr.orgof the International Association forDental Research
Sweden Sept. 1–3 Annual Meeting of the Swedish KKF Uppsala www.kkf.nuAssociation of Oral and MaxillofacialSurgeons (KKFs årsmöte)
Sweden Sept. 15–17 Annual Meeting of the Swedish Society SFOP Halmstad www.sfop.sefor Prosthodontics (Tylösandsdagarna)
STARGET 1 I 1080 EVENTS
STARGET_1_2010_en.indd 80STARGET_1_2010_en.indd 80 21.12.2009 17:36:23 Uhr21.12.2009 17:36:23 Uhr
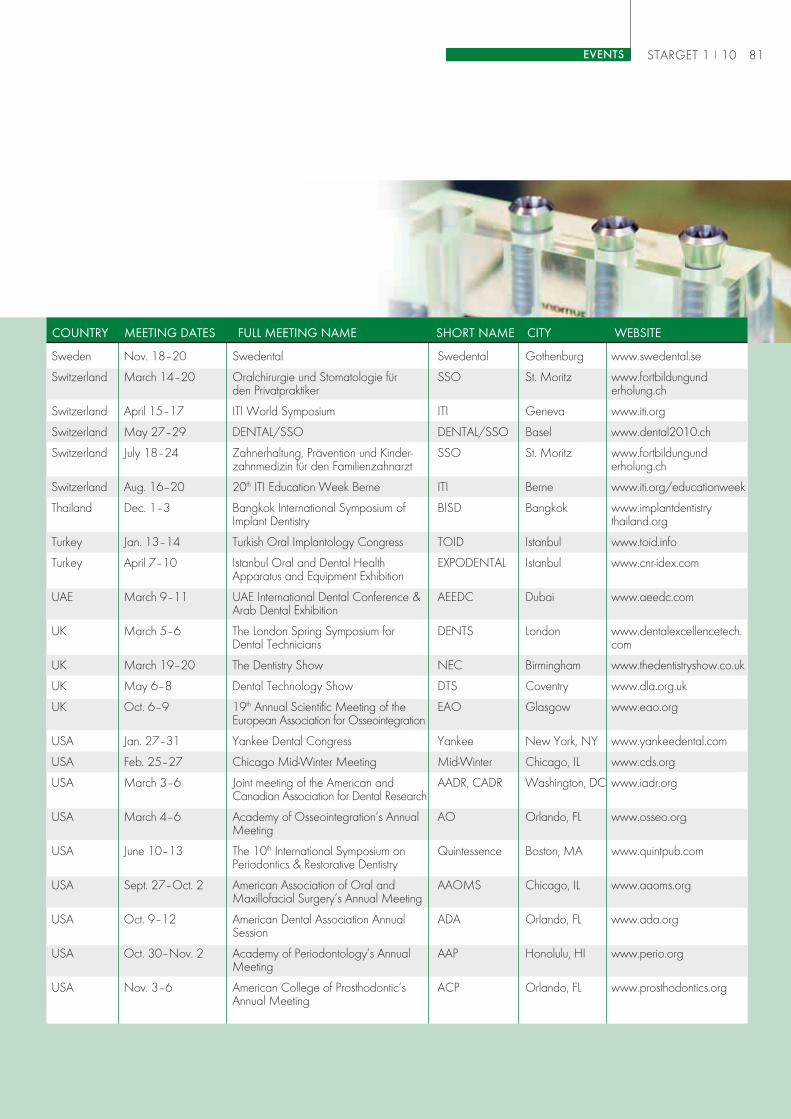
STARGET 1 I 10 81EVENTS
SHORT NAME CITY WEBSITEMEETING DATES FULL MEETING NAMECOUNTRY
Sweden Nov. 18–20 Swedental Swedental Gothenburg www.swedental.se
Switzerland March 14–20 Oralchirurgie und Stomatologie für SSO St. Moritz www.fortbildungundden Privatpraktiker erholung.ch
Switzerland April 15–17 ITI World Symposium ITI Geneva www.iti.org
Switzerland May 27–29 DENTAL/SSO DENTAL/SSO Basel www.dental2010.ch
Switzerland July 18–24 Zahnerhaltung, Prävention und Kinder- SSO St. Moritz www.fortbildungundzahnmedizin für den Familienzahnarzt erholung.ch
Switzerland Aug. 16–20 20th ITI Education Week Berne ITI Berne www.iti.org/educationweek
Thailand Dec. 1–3 Bangkok International Symposium of BISD Bangkok www.implantdentistryImplant Dentistry thailand.org
Turkey Jan. 13–14 Turkish Oral Implantology Congress TOID Istanbul www.toid.info
Turkey April 7–10 Istanbul Oral and Dental Health EXPODENTAL Istanbul www.cnr-idex.comApparatus and Equipment Exhibition
UAE March 9–11 UAE International Dental Conference & AEEDC Dubai www.aeedc.comArab Dental Exhibition
UK March 5–6 The London Spring Symposium for DENTS London www.dentalexcellencetech.Dental Technicians com
UK March 19–20 The Dentistry Show NEC Birmingham www.thedentistryshow.co.uk
UK May 6–8 Dental Technology Show DTS Coventry www.dla.org.uk
UK Oct. 6–9 19th Annual Scientific Meeting of the EAO Glasgow www.eao.orgEuropean Association for Osseointegration
USA Jan. 27–31 Yankee Dental Congress Yankee New York, NY www.yankeedental.com
USA Feb. 25–27 Chicago Mid-Winter Meeting Mid-Winter Chicago, IL www.cds.org
USA March 3–6 Joint meeting of the American and AADR, CADR Washington, DC www.iadr.orgCanadian Association for Dental Research
USA March 4–6 Academy of Osseointegration‘s Annual AO Orlando, FL www.osseo.orgMeeting
USA June 10–13 The 10th International Symposium on Quintessence Boston, MA www.quintpub.comPeriodontics & Restorative Dentistry
USA Sept. 27–Oct. 2 American Association of Oral and AAOMS Chicago, IL www.aaoms.orgMaxillofacial Surgery‘s Annual Meeting
USA Oct. 9–12 American Dental Association Annual ADA Orlando, FL www.ada.orgSession
USA Oct. 30–Nov. 2 Academy of Periodontology‘s Annual AAP Honolulu, HI www.perio.orgMeeting
USA Nov. 3–6 American College of Prosthodontic‘s ACP Orlando, FL www.prosthodontics.orgAnnual Meeting
STARGET_1_2010_en.indd 81STARGET_1_2010_en.indd 81 21.12.2009 17:36:24 Uhr21.12.2009 17:36:24 Uhr

STARGET_1_2010_en.indd 82STARGET_1_2010_en.indd 82 21.12.2009 17:36:24 Uhr21.12.2009 17:36:24 Uhr
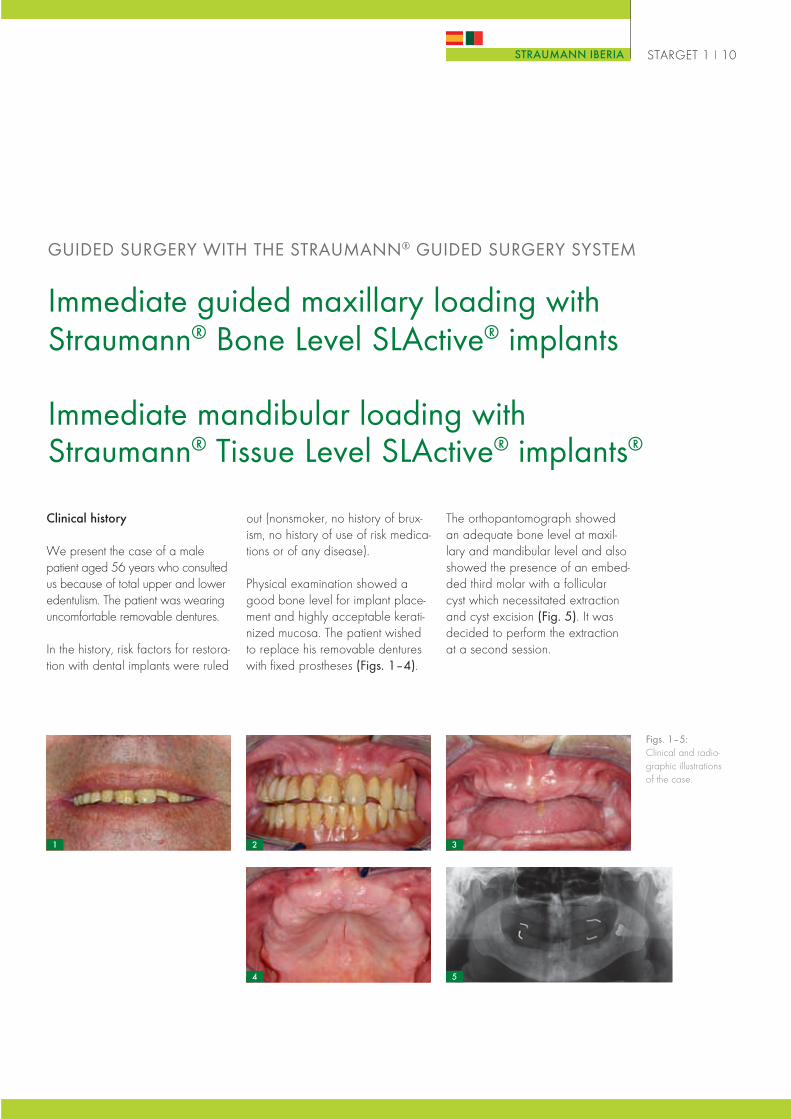
STARGET 1 I 10STRAUMANN IBERIA
Immediate guided maxillary loading withStraumann® Bone Level SLActive® implants
Immediate mandibular loading withStraumann® Tissue Level SLActive® implants®
GUIDED SURGERY WITH THE STRAUMANN® GUIDED SURGERY SYSTEM
Clinical history
We present the case of a malepatient aged 56 years who consultedus because of total upper and loweredentulism. The patient was wearinguncomfortable removable dentures.
In the history, risk factors for restora-tion with dental implants were ruled
Figs. 1–5:Clinical and radio-graphic illustrationsof the case.
out (nonsmoker, no history of brux-ism, no history of use of risk medica-tions or of any disease).
Physical examination showed agood bone level for implant place-ment and highly acceptable kerati-nized mucosa. The patient wishedto replace his removable dentureswith fixed prostheses (Figs. 1–4).
The orthopantomograph showedan adequate bone level at maxil-lary and mandibular level and alsoshowed the presence of an embed-ded third molar with a follicularcyst which necessitated extractionand cyst excision (Fig. 5). It wasdecided to perform the extractionat a second session.
1 2 3
54
ES_Teil_A4_ENGLISCH.indd 1ES_Teil_A4_ENGLISCH.indd 1 22.12.2009 15:54:41 Uhr22.12.2009 15:54:41 Uhr
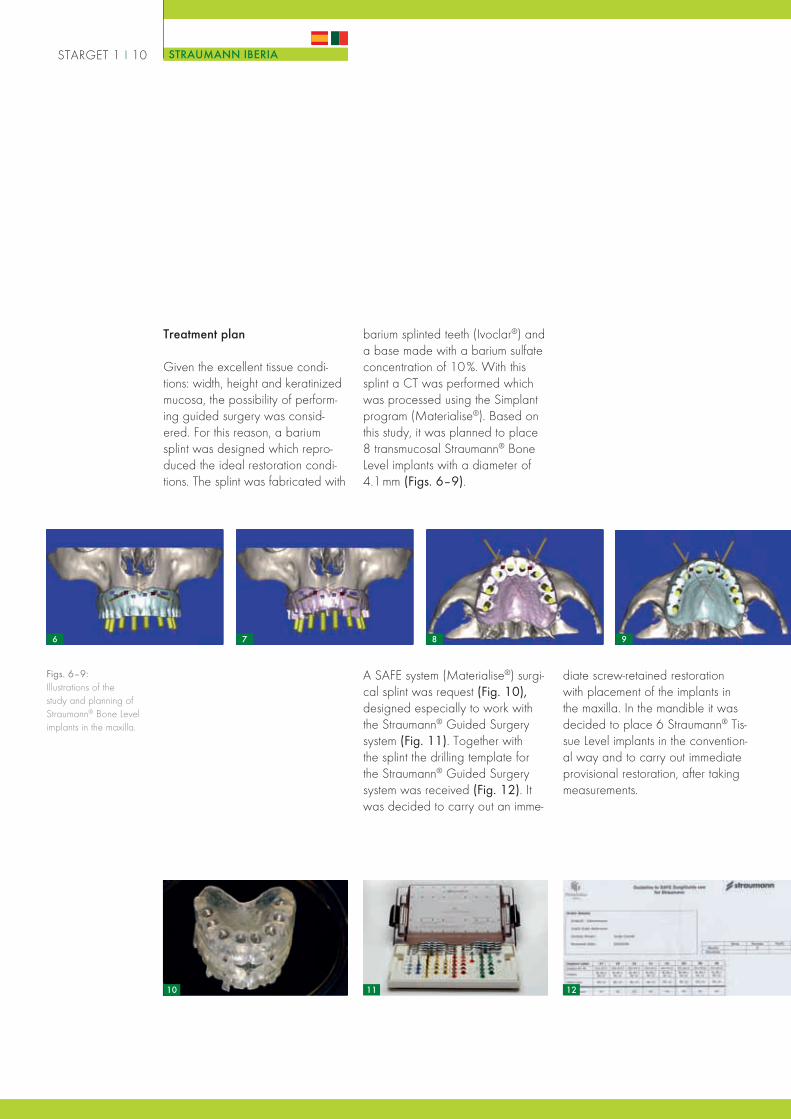
A SAFE system (Materialise®) surgi-cal splint was request (Fig. 10),designed especially to work withthe Straumann® Guided Surgerysystem (Fig. 11). Together withthe splint the drilling template forthe Straumann® Guided Surgerysystem was received (Fig. 12). Itwas decided to carry out an imme-
barium splinted teeth (Ivoclar®) anda base made with a barium sulfateconcentration of 10 %. With thissplint a CT was performed whichwas processed using the Simplantprogram (Materialise®). Based onthis study, it was planned to place8 transmucosal Straumann® BoneLevel implants with a diameter of4.1mm (Figs. 6–9).
10 11 12
Treatment plan
Given the excellent tissue condi-tions: width, height and keratinizedmucosa, the possibility of perform-ing guided surgery was consid-ered. For this reason, a bariumsplint was designed which repro-duced the ideal restoration condi-tions. The splint was fabricated with
Figs. 6–9:Illustrations of thestudy and planning ofStraumann® Bone Levelimplants in the maxilla.
diate screw-retained restorationwith placement of the implants inthe maxilla. In the mandible it wasdecided to place 6 Straumann® Tis-sue Level implants in the convention-al way and to carry out immediateprovisional restoration, after takingmeasurements.
STARGET 1 I 10 STRAUMANN IBERIA
6 7 8 9
ES_Teil_A4_ENGLISCH.indd 2ES_Teil_A4_ENGLISCH.indd 2 22.12.2009 15:55:10 Uhr22.12.2009 15:55:10 Uhr

that two implants had to be insertedtwo millimeters deeper. A good fitbetween the preformed prosthesisand the implant emergence waschecked (Fig. 15). 6 Straumann®
Tissue Level 4.1 x12 mm implantswere placed in the mandible inpositions 42, 43, 46, 32, 33 and36 using a conventional surgicalsplint (Figs. 16–17). In five of thesea suitable insertion torque for animmediate screw-retained restora-tion was obtained (except for theimplant in position 42, which wasleft unloaded). The postoperativeorthopantomograph showed cor-rect distribution of the implants inthe maxilla and mandible (Fig. 18).
Surgical procedure
Under local anesthesia and seda-tion the SAFE surgical splint wasfixed with 1.6 mm internal fixationmicro-screws (Mincro Osteoplac®
system) 12 mm in length (Fig. 13).Using the Straumann® GuidedSurgery system drilling template, 8Straumann® Bone Level SLActive®
4.1 x 12 mm implants were placedin positions 17, 15, 13, 11, 21,23, 25 and 26. Good primarystability was achieved with all ofthem and they were placed with aninsertion torque greater than 35N/cm (Fig. 14). The depth of insertionwas confirmed with a postoperativeorthopantomograph which showed
13 15
17
14
16 18
STARGET 1 I 10STRAUMANN IBERIA
ES_Teil_A4_ENGLISCH.indd 3ES_Teil_A4_ENGLISCH.indd 3 22.12.2009 15:55:29 Uhr22.12.2009 15:55:29 Uhr

Restoration procedure
After the implants were placed, theBone Level abutments were placed(Figs. 19–20) so that the provision-al upper denture could be screwedon to them (Fig. 21). Relining andadjustment were carried out, show-
ing very good adaptation betweenthe provisional prosthesis and theabutments (Fig. 22). An hour afterthe conclusion of the procedure,the provisional upper prosthesiswas screwed to the 8 implants sta-bly and precisely (Fig. 23–26).
19 20 21 22
23 24 25 26
27 28 29 30
In the mandible, impressions were taken with the aim of screwing on theprovisional restoration 24 hours after the procedure (Figs. 27–30).
STARGET 1 I 10 STRAUMANN IBERIA
ES_Teil_A4_ENGLISCH.indd 4ES_Teil_A4_ENGLISCH.indd 4 22.12.2009 15:55:52 Uhr22.12.2009 15:55:52 Uhr

31
24 hours later, the provisional lower denture was placed on 5 ofthe 6 implants (Figs. 31–34).
32 33 34
35 36
38
Patient’s appearance 24 hours after the procedure (Figs. 35–36).
Initial clinical and radiographic situation with the removable dentures(Figs. 37–38), situation 24 hours after the procedure (Figs. 39–40) andsituation 8 weeks later when the provisional dentures were replaced withthe final prostheses (Figs. 41–42).
37
STARGET 1 I 10STRAUMANN IBERIA
39 40
ES_Teil_A4_ENGLISCH.indd 5ES_Teil_A4_ENGLISCH.indd 5 22.12.2009 15:56:30 Uhr22.12.2009 15:56:30 Uhr

Dr Jorge Caubet [email protected]
Doctor of medicine and surgery
Specialist in oral and maxillofacialsurgery
Professor of the University Master’sDegree in Implantology of the BalearicIslands
Fellow of the European Board ofOral and Maxillofacial Surgery
ITI Fellow
Private practice in implant dentistryand preprosthetic surgery, GBCOM(Balearic Oral Surgery and Maxillo-facial Group), Palma de Mallorca
Collaborators:
Dr Jacobo Sanchez Mayoral,dentists and oral and maxillofa-cial surgeon, GBCOM
Dr José Ignacio Iriarte Ortabe,oral and maxillofacial surgeon,GBCOM
Dr Miguel Morey Más, oral andmaxillofacial surgeon, GBCOM
Dr Bahzad Aghaei, dentist,Palma de Mallorca
Dr Marina Muñoz, dentist,Palma de Mallorca
Mr. Alberto Tomás, dentaltechnician, Dentathlon, Palmade Mallorca
Mr. Ignacio Barceló, dentaltechnician, Dentathlon, Palmade Mallorca
Conclusions
The advantages of computer-guided surgical procedures havebeen published in the literature byauthors such as Sarment and vanSteenberghe. On the one hand,precise planning is achieved fromthe anatomical aspect. On theother hand, the possibility of havingstereolithographic surgical splintsallows a very exact approximationof the provisional restoration to beobtained. Transmucosal surgeryprovides excellent results in terms ofspeed and morbidity, with no post-operative inflammation and pain.
The SLActive® surface providesgreater security when placing animmediate provisional restorationso that it is very suitable in theseprocedures.
The Straumann® Guided Surgerysystem offers the possibility ofperforming these guided surgeryprocedures with the majority ofStraumann implants.
42 43
STARGET 1 I 10 STRAUMANN IBERIA
41
ES_Teil_A4_ENGLISCH.indd 6ES_Teil_A4_ENGLISCH.indd 6 22.12.2009 15:57:10 Uhr22.12.2009 15:57:10 Uhr

ES_Teil_A4_ENGLISCH.indd 7ES_Teil_A4_ENGLISCH.indd 7 22.12.2009 15:57:16 Uhr22.12.2009 15:57:16 Uhr
STARGET 1 I 10 STRAUMANN IBERIA
More than 170 people attendedthe talks given by two experts inimplant dentistry, Professor DanielBusel, chairman elect of the ITI, andProfessor Juan Blanco, current chair-man of SEPA.
On Friday 12 June, Prof. Blancoexplained the new SAC clas-sification to the participants. Thisnew classification represents anindispensable reference tool for
SEPA – Straumann meeting IREVIEW
Professor JuanBlanco, Professor
Daniel Buser
The SEPA-Straumann meeting I took place on last June 12 and 13 in the headquartersof the COEC, Colegio Oficial de Odontologos y Estomatologos de Cataluña (OfficialCollege of Dentists and Stomatologists of Catalonia).
clinicians when making decisionsregarding what treatment to use. Inaddition, among other topics, Prof.Blanco explained the most recentloading protocols according to thelast ITI Consensus that took placein Stuttgart.
On Saturday 13 June, the top-ics discussed by Prof. D. Buserincluded the principal risks whenchoosing a specific treatment and
also the selection of biomaterials incases requiring bone regeneration.
Next year, SEPA and Straumannwill again offer all clinicians theprincipal innovations in periodontaltreatments. Here at Straumann, wewould like to congratulate SEPA onits 50th anniversary.
ES_Teil_A4_ENGLISCH.indd 8ES_Teil_A4_ENGLISCH.indd 8 22.12.2009 15:57:18 Uhr22.12.2009 15:57:18 Uhr

ES_Teil_A4_ENGLISCH.indd 9ES_Teil_A4_ENGLISCH.indd 9 22.12.2009 15:57:31 Uhr22.12.2009 15:57:31 Uhr

STARGET 1 I 10 STRAUMANN IBERIA
Straumann present at SEPA Las PalmasREVIEW
The 43rd annual meeting of SEPA, the Sociedad Española de Periodoncia y Osteointegración(Spanish Periodontal and Osseointegration Society), took place in the Alfredo Kraus Auditoriumin Las Palmas, Gran Canarias, on 12, 13 and 14 November.
Straumann as platinum sponsor ofSEPA took part in the recent mee-ting with a 24 m2 stand located inthe “Expoperio” exhibition of theauditorium, where Straumann hadan opportunity to tell the professio-nals who attended the conferenceabout the latest innovations inimplant dentistry, tissue regene-ration and CADCAM solutions,for instance, Roxolid™, the newand innovative material for smalldiameter implants, the StraumannIPS e.max® Anatomical Abutments,which is the latest innovationfrom Straumann for highly estheticrestorations, and the syntheticbone substitute Straumann Bone-Ceramic®.
Straumann itself took part in thescientific program of the congresswith a presentation on “Effectivebony regeneration: experience withnew materials” given by Prof. LucaCordaro; in addition, Straumannsponsored the Clinical Commu-
nications competition, won by DrDaniel Rodrigo, and the party thatfollowed SEPA’s 50th anniversarygala dinner. Straumann would liketo take this opportunity to congra-tulate SEPA again on its 50th anni-versary.
ES_Teil_A4_ENGLISCH.indd 10ES_Teil_A4_ENGLISCH.indd 10 22.12.2009 15:57:33 Uhr22.12.2009 15:57:33 Uhr

■
■
■
■
■
■
■■ ■
■■
■
■ ■ ■■
■ ■
■
■
■
■ ■■
■
■
■
■
■
■
■
■
■■
■
■
■■
■
■■
■
■
■
■
■■
■■
■■
■■ ■
■ ■■
■
■
■
■
SwitzerlandInstitut Straumann AGPeter Merian-Weg 124002 BaselTel. +41/61 965 11 11Fax +41/61 965 11 01
Subsidiary companies:
Australia/New ZealandStraumann Pty. Ltd.7 Gateway CourtPort Melbourne 3207VictoriaTel. +61/39 64 67 060Fax +61/39 64 67 232
Austria/HungaryStraumann GmbH AustriaFlorido TowerFloridsdorfer Hauptstr. 11210 WienTel. +43/12 94 06 60Fax +43/12 94 06 66
BelgiumStraumannBelgicastraat 31930 ZaventemTel. +32/27 90 10 00Fax +32/27 90 10 20
BrazilStraumann Brasil LtdaRua Funchal 26304551-060 São PauloTel. +55/11 30 89 66 83Fax +55/11 30 89 66 84
CanadaStraumann Canada Ltd.4145 North Service RoadSuite 303Burlington/ON-L7L 6A3Tel. +1/905 319 29 00Fax +1/905 319 29 11
Czech RepublicStraumann s.r.o.Na Žertvách 2196180 00 Prague 8Tel. +420/284 094 650Fax +420/284 094 659
DenmarkStraumann Danmark ApSHundige Strandvej 1782670 GreveTel. +45/46 16 06 66Fax +45/43 61 25 81
FinlandStraumann OyFredrikinkatu 48A 7 krs.00100 HelsinkiTel. +358/96 94 28 77Fax +358/96 94 06 95
FranceStraumann France3, rue de la Galmy - Chessy77701 Marne-la-Vallée cedex 4Tel. +33/164 17 30 00Fax +33/164 17 30 10
GermanyStraumann GmbHJechtinger Straße 979111 FreiburgTel. +49/76 14 50 10Fax +49/76 14 50 11 49
Great BritainStraumann Ltd.3 Pegasus Place, Gatwick RoadCrawley RH109AY, West SussexTel. +44/12 93 65 12 30Fax +44/12 93 65 12 39
ItalyStraumann Italia s.r.l.Viale Bodio 37a20158 MilanoTel. +39/02 39 32 831Fax +39/02 39 32 8365
JapanStraumann Japan K.K.3-231-3 Hamaderakoen-choNishi-ku, Sakai-ShiOsaka, Japan 592-8346Tel. +81/722 64 18 82Fax +81/722 64 18 24
MexicoStraumann México SA de CVRubén Darío # 281 int. 1702Piso 17Col. Bosque de Chapultepec11580 México DF.Tel. +52/55 5282 6262Fax +52/55 5282 6289
NetherlandsStraumann B.V.Postbus 3383400 AH IJsselsteinTel. +31/30 60 46 611Fax +31/30 60 46 728
NorwayStraumann ASP.O.Box 1751 Vika0122 OsloTel. +47/23 35 44 88Fax +47/23 35 44 80
South KoreaStraumann South Korea(formerly: B.I. Trading Co. Ltd.)1467-75, Seocho3 -Dong,Seocho-Gu, SeoulTel. +82/72 265 8777Fax +82/72 265 8797
Spain/PortugalStraumann S.A.Edificio Arroyo - AAvda. de Bruselas, 38Planta 128108 Alcobendas (Madrid)Tel. +34/902 400 979Fax +34/913 449 517
SwedenStraumann ABFabriksgatan 1341250 GöteborgTel. +46/31 708 75 00Fax +46/31 708 75 29
USAStraumann USA, LLC60 Minuteman RoadAndover, MA 01810Tel. +1/800 448 8168
+1/978 747 2500Fax +1/978 747 2490
■
■ Subsidiary companies
Distributors
STARGET 1 I 10WORLD-WIDE NEAR TO CUSTOMERS 83
STARGET_1_2010_en.indd 83STARGET_1_2010_en.indd 83 21.12.2009 17:36:27 Uhr21.12.2009 17:36:27 Uhr

www.straumann.com
01/1
015
2.50
0e
STARGET_1_2010_en.indd 84STARGET_1_2010_en.indd 84 21.12.2009 17:36:29 Uhr21.12.2009 17:36:29 Uhr