stroke center designation: impact on em e. bradshaw bunney, md, facep
TRANSCRIPT

Stroke Center Designation:Stroke Center Designation:Impact on EMImpact on EM
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Associate ProfessorAssociate ProfessorDepartment of Emergency MedicineDepartment of Emergency Medicine
University of Illinois at ChicagoUniversity of Illinois at Chicago
Our Lady of the Resurrection HospitalOur Lady of the Resurrection Hospital
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Global ObjectivesGlobal Objectives
• Improve patient outcome for both hemorrhagic and ischemic stroke
• EM participation in protocol development
• Hospital financial interest
• Community education

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Session ObjectivesSession Objectives
• Stroke management from community to the ED and beyond
• The history of Stroke Center designation
• EM role in protocol development and Stroke Center designation

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Clinical HistoryClinical History
A 911 call was taken by the Chicago Fire Department dispatch service at 2:25 pm. The caller stated, “My husband is having a stroke and he can not move the left side of his body”. An ALS ambulance arrived at 2:34 pm and found the 67-year-old patient to be sitting in a chair with a BP 140/85, pulse 96, respiratory rate 16 and the inability to move his left arm or leg. His wife also noticed the left side of his face was “flat”. He was able to speak and denied headache, chest pain or shortness of breath.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Clinical HistoryClinical History
He had a history of hypertension, was on Labetalol and Lasix, with no allergies. The paramedics noted the time of onset for the symptoms to be 2:15 pm., which was agreed to by both the patient and his wife. The patient was placed on a cart, an IV was established, oxygen was applied, and glucose was 98. The paramedics called into the base station at 2:48 pm, stating, “We have a probable stroke, with two out of three abnormal on the Cincy scale” and arrived in the ED at 2:52 pm.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Key Clinical QuestionsKey Clinical Questions
• Who, What, Why of Stroke Center designation?• Does my hospital need to become a Stroke
Center?• Does a Stroke Team improve ED care of stoke
patients?• Can an ED use thrombolytics if it is not a
Stroke Center?• What is EMS role in the process?• What are the EM controversies in the care of
stroke patients?

Stroke in Perspective: Stroke in Perspective: An Overview An Overview
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Disability Due to Stroke, 1999*Disability Due to Stroke, 1999*†‡†‡
1160
592 567
0
200
400
600
800
1000
1200
1400
All Men Women
Peop
le W
ith D
isab
ilitie
s D
ue to
Str
oke
(100
0s)
Centers for Disease Control (CDC). MMWR. 2001;50:120-125. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5007a3.htm. Accessed December 4, 2003.
*Noninstitutionalized people ≥18 years old.†Total number of people with disabilities=41,168,000.‡Numbers may not add up due to rounding.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Age-Adjusted Stroke Death Rates by Age-Adjusted Stroke Death Rates by Age and Gender, 2001Age and Gender, 2001
59.0 43.4140.4
467.3
1380.2
56.4 32.9109.3
428.6
1550.4
0
200
400
600
800
1000
1200
1400
1600
1800
All Ages* 55 to 64 65 to 74 75 to 84 85 and over
Age in Years
Dea
th R
ate
per
100,
000
Men
Women
National Center for Health Statistics (NCHS). Table 37. In: Health, United States, 2003. Available at: http://www.cdc.gov/nchs/data/hus/tables/2003/03husupdated.pdf. Accessed January 12, 2004.
*Age-adjusted rate calculated using the year 2000 standard population.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Age-Adjusted Stroke Death Rates Age-Adjusted Stroke Death Rates by State, 2001 by State, 2001
Arias E, et al. Natl Vital Stat Rep. 2003;52:1-116. Available at:http://www.cdc.gov/nchs/fastats/stroke.htm. Accessed December 4, 2003.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Age-Adjusted Stroke Death Rates Age-Adjusted Stroke Death Rates by Race and Gender, 2001by Race and Gender, 2001
59.0 56.5
85.4
48.9
56.4 54.5
73.7
41.6
0
10
20
30
40
50
60
70
80
90
100
All Races Caucasian African American Hispanic
Dea
th R
ates
per
100
,000
MaleFemale
National Center for Health Statistics (NCHS). Table 37. In: Health, United States, 2003. Available at: http://www.cdc.gov/nchs/data/hus/tables/2003/03husupdated.pdf. Accessed January 12, 2004.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
$20.2 Billion39.4%
$31.0 Billion60.6%
Direct costs Indirect costs
Estimated Direct and Indirect Estimated Direct and Indirect Costs of Stroke, 2003 Costs of Stroke, 2003
American Heart Association (AHA). Heart Disease and Stroke Statistics — 2003 Update. 2003. Available at: http://www.americanheart.org/downloadable/heart/10590179711482003HDSStatsBookREV7-03.pdf. Accessed October 13, 2003.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Major Causes of Death in the Major Causes of Death in the United States, 2001United States, 2001
247.8
196.0
57.943.7 35.7
0
50
100
150
200
250
300
Heart Disease Cancer CerebrovascularDisease
COPD Accidents
Dea
th R
ates
per
100
,000
Arias E, et al. Natl Vital Stat Rep. 2003;52:1-116. Available at:http://www.cdc.gov/nchs/fastats/stroke.htm. Accessed December 4, 2003.
COPD=chronic obstructive pulmonary disease.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Age-Adjusted Death Rates From Age-Adjusted Death Rates From Stroke: 1950-2001*Stroke: 1950-2001*††
180.7 177.9
147.7
96.2
65.3 63.1 60.9 57.9
0
20
40
60
80
100
120
140
160
180
200
1950 1960 1970 1980 1990 1995 2000 2001
Str
oke
Dea
ths
per
100
,000
*Age-adjusted rates are calculated using the year 2000 standard population.†Data prior to 1970 includes deaths of persons not residents of the 50 states and the District of Columbia.
National Center for Health Statistics (NCHS). Table 37. In: Health, United States, 2003. Available at: http://www.cdc.gov/nchs/data/hus/tables/2003/03husupdated.pdf. Accessed January 12, 2004.
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
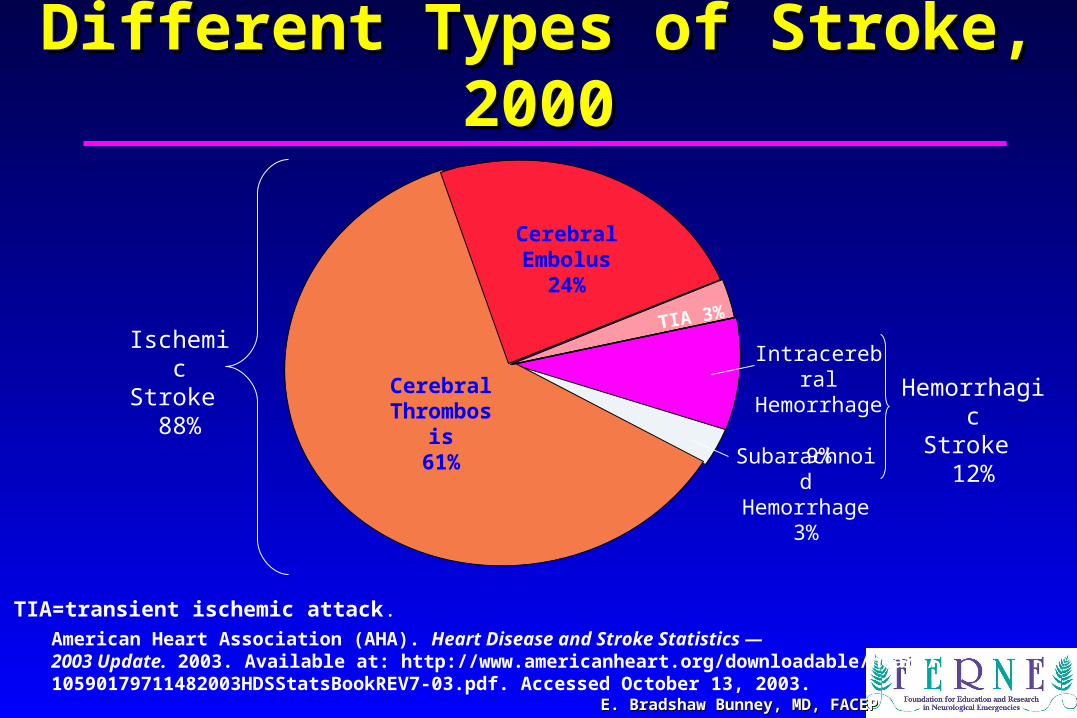
Different Types of Stroke, 2000Different Types of Stroke, 2000
American Heart Association (AHA). Heart Disease and Stroke Statistics — 2003 Update. 2003. Available at: http://www.americanheart.org/downloadable/heart/10590179711482003HDSStatsBookREV7-03.pdf. Accessed October 13, 2003.
TIA=transient ischemic attack.
Ischemic Stroke
88% Cerebral Thrombosis
61%
TIA 3%
Cerebral Embolus
24%
Intracerebral Hemorrhage
9%
Subarachnoid Hemorrhage 3%
HemorrhagicStroke
12%

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
HISTORYHISTORY
• 1995- NINDS- TPA therapy for ischemic stroke• 1996- EM controversy over use of TPA in stroke• 1997- Brain Attack Coalition (BAC) formed• 2000- Primary Stroke Center criteria published• ?- Comprehensive Stroke Center criteria
published

Stroke-site.org

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
BAC MembersBAC Members• NINDS• American Academy of Neurology• American College of Emergency Physicians• American Assn of Neurological Surgeons• American Stroke Association• National Stroke Association • Am Soc of Intervent and Therapy Neuroradiology• American Society of Neuroradiology• Congress of Neurological Surgeons• Stroke Belt Consortium• Veterans Administration• National Association of EMS Physicians• Centers for Disease Control and Prevention• American Assn of Neuroscience Nurses

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Brain Attack CoalitionBrain Attack Coalition
• Stroke scales
• Guidelines
• Pathways
• North Carolina
• Stanford
• Thomas Jefferson
• www.stroke-site.org

Strokeassociation.orgStrokeassociation.org

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
American Stroke American Stroke AssociationAssociation
• Acute Stroke Treatment ProgramAcute Stroke Treatment Program
• Operation StrokeOperation Stroke
• Get with the Guidelines-StrokeGet with the Guidelines-Stroke
• Stroke Center CertificationStroke Center Certification
• www.strokeassociation.orgwww.strokeassociation.org

Stroke.org

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
National Stroke AssociationNational Stroke Association
• Public Health Stoke Summit• CDC sponsored
• Increase public awareness
• Develop state programs to decrease the incidence and death rate
• National Tutorial on Stroke

Why Were Stroke Centers Why Were Stroke Centers Developed?Developed?
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

TIME IS BRAINTIME IS BRAIN
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Time is BrainTime is Brain
• Narrow therapeutic window• t-PA within three hours of
symptom onset
• Rapid identification, transport, diagnosis and treatment
• Stroke “chain of survival” (AHA)

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Trauma Center ModelTrauma Center Model• Military experience with rapid evacuation• 1966: Accidental Death and Disability: The
neglected disease of modern society• National Academy of Sciences document• Strong government leadership proposed• Called for improved training, education, and research• Role of prehospital care emphasized
• Radio communication• EMS training
• Categorize hospital capabilities: 4 categories• Resulted in the National Highway Safety Act

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Trauma Center ModelTrauma Center Model• 1993 report: 20 states had trauma systems
with legal authority• 5 States had full implementation: many states
failed to enforce limitations on the number of centers based on need (due to political obstacles
• Financial Crisis: decreased federal support, managed care, DRGs, staff retention
• Trauma center implementation has provided an infrastructure for the provision of emergency care
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Who is Designating Stroke Centers?Who is Designating Stroke Centers?
• American Stroke Association
• Joint Commission

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
ASA GWTG MeasuresASA GWTG Measures• Acute Stroke Treatment:
• Time of symptom onset
• Time from EMS receiving call to EMS arrival
• Time patient arrived at Emergency Department (ED)
• Time of CT/MRI Scan
• Time of thrombolytic therapy
• Ischemic Stroke Prevention:
• Smoking Cessation Counseling
• Lipid Lowering Therapy
• Blood Pressure Treatment
• Weight and Exercise Management
• Diabetes Management
• Atrial Fibrillation Management
Focus is quality of careFocus is quality of care
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Disease Specific Care CertificationDisease Specific Care Certification• Premise is that certification process will drive
quality measures and improve outcomes• No emergency medicine society has endorsed this
initiative• t-PA controversy• Overcrowding• Medical legal implications
JCAHO JCAHO

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
• Accreditation• Surveys are organization-based, focused on quality and
safe care processes and functions• Traditional JCAHO evaluation product• 50 years establishing expertise in evaluating health care
organizations
• Certification• Reviews are service-based, focused on quality, safety,
and outcomes of improving clinical care • Voluntary—not an add-on to accreditation
Accreditation vs. CertificationAccreditation vs. CertificationJCAHO JCAHO

Brain Attack CoalitionBrain Attack Coalition
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Recommendations for Recommendations for Developing Primary Stroke CentersDeveloping Primary Stroke Centers
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Major Elements Major Elements
• Patient care areas• Acute stroke teams• Written care
protocols• Emergency medical
services• Emergency
department• Stroke unit• Neurosurgical
services
• Support services• Stroke center director• Neuroimaging
services• Laboratory services• Outcome and quality
improvement activities
• Continuing medical education
Alberts MJ, et al. JAMA. 2000;283:3102-3109.
of a Primary Stroke Centerof a Primary Stroke Center

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Anticipated BenefitsAnticipated Benefits
• Increased patient-care efficiency• Fewer peristroke complications• Increased use of therapies for acute stroke• Decreased morbidity and mortality• Improved long-term outcomes• Decreased costs to the healthcare system• Improved patient satisfaction
Alberts MJ, et al. JAMA. 2000;283:3102-3109.
of a Primary Stroke Centerof a Primary Stroke Center

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Acute Stroke TeamAcute Stroke Team• Personnel with expertise in diagnosing and treating
cerebrovascular disease (may include neurologist or neurosurgeon)1
• Minimum team would include a physician and another healthcare provider (nurse, physician’s assistant, nurse practitioner)1
• National Stroke Association (NSA) organizational recommendations2
• Stroke center team should include a specialist and support in:• Neurology, neurological surgery, neuroradiology, as well as emergency
medicine and rehabilitation medicine• Stroke center team should include, on an as-needed basis, a specialist
and support in:• Cardiology, critical care, gastroenterology, hematology, infectious disease,
internal medicine, pathology, primary care, and vascular surgery
1. Alberts MJ, et al. JAMA. 2000;283:3102-3109.2. Furlan AJ, et al, 1997. Available at http://199.239.30.192/NR/rdonlyres/exkgdlqimjxtunrlwtsd7tpge3i23nwqm5r5uxw3cby4zk6fe3t3ubvtek2kpnp5ocmymjutwyyofb/StrokeCenterRecommendatio.pdf.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Acute Stroke Team (cont’d)Acute Stroke Team (cont’d)• Someone from the team should be available 24/7
• Need system for quick notification and activation of the team
• One member of the team should see patient within 15 minutes
• Written document should be developed to provide information on stroke team guidelines
• Logbook should be established to document call and response times, diagnoses, treatments, and outcomes
Alberts MJ, et al. JAMA. 2000;283:3102-3109.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Written Care ProtocolsWritten Care Protocols• Reduce tPA–related complications• Protocols should include
• Emergency care of ischemic and hemorrhagic strokes• Stabilization of vital functions• Initial diagnostic tests• Initial use of medications
• Protocols should be available any place where patients with stroke may be evaluated or treated
• Should be reviewed and updated once per year
Alberts MJ, et al. JAMA. 2000;283:3102-3109.
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Emergency Medical ServicesEmergency Medical Services• Assigned a high priority • EMS should be integrated with the stroke center• During transportation, EMS and the stroke
center need to communicate• Quickly triage patients with a stroke upon arrival• Educational activities should include stroke
center and EMS staff and occur at least twice a year
Alberts MJ, et al. JAMA. 2000;283:3102-3109.
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Emergency DepartmentEmergency Department• ED personnel should be trained to diagnose and
treat all types of acute strokes• ED staff should access the stroke team • Communicate with EMS and be prepared for
arrival of stroke patients• Written protocols for stroke management and
triage• Educational activities should occur at least twice
a year to reinforce stroke diagnosis and treatment
Alberts MJ, et al. JAMA. 2000;283:3102-3109.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Additional Hospital Units and ServicesAdditional Hospital Units and Services
• Stroke Unit• Does not need to be a distinct unit in the
hospital
• Personnel should have expertise in managing cerebrovascular disease
• Additional infrastructure includes: continuous telemetry, written care protocols, and ability to continuously, noninvasively monitor blood pressure
Alberts MJ, et al. JAMA. 2000;283:3102-3109.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
• Neurosurgical Services• Neurosurgical care should be available
within 2 hours of determination that surgery is necessary (patients can be transferred)
• Hospitals providing the neurosurgical care should have 24-hour–staffed operating room
Alberts MJ, et al. JAMA. 2000;283:3102-3109.
Additional Hospital Units and ServicesAdditional Hospital Units and Services

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Additional Hospital Units and ServicesAdditional Hospital Units and Services
• Neuroimaging (CT or MRI) Imaging within 25 minutes• Image evaluation within 20 minutes
• Standard laboratory tests should be available 24/7
Alberts MJ, et al. JAMA. 2000;283:3102-3109.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Outcomes and Quality ImprovementOutcomes and Quality Improvement
• Database or registry of all stroke patients
• Benchmarks for comparison • Can be selected from treatment guidelines
• Each year, at least two patient-care issues
• Pre-specified committees meet at least three times a year to review and modify practice patterns
Alberts MJ, et al. JAMA. 2000;283:3102-3109.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Educational ProgrammingEducational Programming
• Stroke center staff should earn at least 8 hours of CME credit per year related to cerebrovascular disease
• The stroke center should hold at least two programs per year to educate the public• Prevention and recognition of stroke
symptoms• Availability of acute treatments
Alberts MJ, et al. JAMA. 2000;283:3102-3109.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Stroke Center CertificationStroke Center Certification• Certification review will assess
• Compliance with consensus-based national standards
• Effective use of primary stroke center recommendations and clinical practice guidelines to manage and optimize care
• Performance measurement and improvement activities
• Certification for a 1-year period• A 1-year extension is available
Joint Commission Joint Commission on Accreditation of Healthcare Organizations (JCAHO). Disease-Specific Care: Update [JCAHO Web site]. Issue 1, June 2004. Available at: http://www.jcaho.org/dscc/dsc/dsc+update/dsc_update.htm. Accessed September 15, 2004.
JCAHOJCAHO

Does my Hospital Have to Does my Hospital Have to Become a Stroke Center?Become a Stroke Center?
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Opportunity ExistsOpportunity Exists

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Hospitals That are Stroke CentersHospitals That are Stroke Centers
• Approximately 5,000 hospitals in the US
• As of Feb. 2005 there are 88 certified Stroke Centers
• 50 more in the pipeline
• California, Florida, Ohio and Pennsylvania each have 7
• State certification in Massachusetts and New York

Do Stroke Teams Do Stroke Teams Improve Outcomes?Improve Outcomes?
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

Stroke Team Stroke Team vs vs
Stroke CenterStroke Center
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

TIME IS BRAINTIME IS BRAIN
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Importance of Rapid Identification and TriageImportance of Rapid Identification and Triage
• Intervention in acute ischemic stroke requires the rapid and careful • Assessment• Selection• Treatment • Within 3 hours of symptom onset
• Multiple disciplines and departments• Pre-hospital responders and in-hospital care
providers• Perceptions, attitudes, and behavior of the public
• Warning signs of stroke • Need for rapid and immediate action
of Emergency Stroke Patientsof Emergency Stroke Patients

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Factors Potentially Delaying Factors Potentially Delaying Response Times in StrokeResponse Times in Stroke
• Inadequate public/patient awareness of signs and symptoms and need to call EMS early
• Strokes don’t cause pain• The need for time urgency for emergency
stroke patients by prehospital and healthcare professionals
• Modification of existing EMS programs for rapid identification, triage, treatment, and transport of emergency stroke patients
EMS=emergency medical services.
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
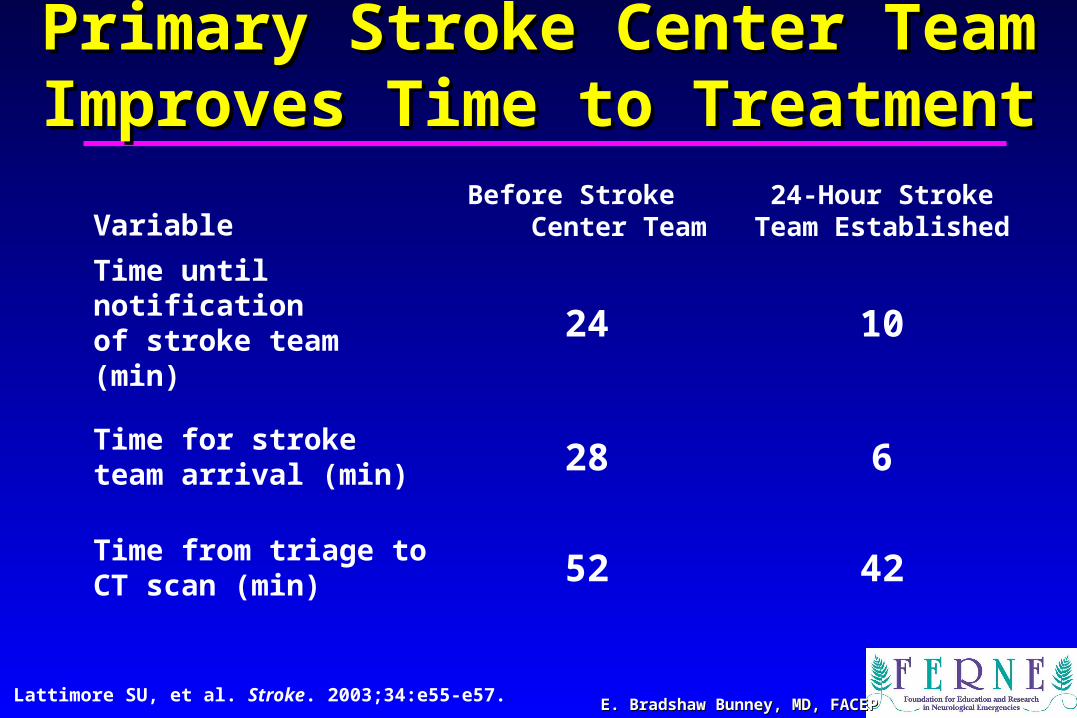
Primary Stroke Center Team Primary Stroke Center Team Improves Time to TreatmentImproves Time to Treatment
VariableBefore Stroke
Center Team24-Hour Stroke Team
Established
Time until notification of stroke team (min) 24 10
Time for stroke team arrival (min) 28 6
Time from triage to CT scan (min) 52 42
Lattimore SU, et al. Stroke. 2003;34:e55-e57.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Stroke Teams and Establishment Stroke Teams and Establishment of Acute Stroke Pathwaysof Acute Stroke Pathways
• One ED’s 2-year experience • St. Joseph’s Hospital
• A 467-bed institution located in Phoenix, Arizona• Includes a neurologic institute and level I trauma center
• Before a stroke team was established, stroke patients:
• Waited an average of 33 minutes for a physician examination
• CT scan took an average of 55 minutes to be completed• An additional 10 to 15 minutes passed until the CT scan
was interpreted
Jahnke HK, et al. J Emerg Nurs. 2003;29:133-139.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Improved Approach to Assessment Improved Approach to Assessment
• St. Joseph’s Hospital developed a stroke team and a written acute stroke pathway
• The acute stroke pathway included a standardized set of orders and instructions for the management of acute ischemic stroke
• Acute stroke pathway goals to improve the quality of patient care:• Decreased length of stay• Increased use of select medications and treatment• Improved patient assessment• Reduced unnecessary testing
Jahnke HK, et al. J Emerg Nurs. 2003;29:133-139.
of Stroke Patientof Stroke Patient

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Acute Stroke Pathway:Acute Stroke Pathway:
• Triage nurses assign stroke patients to “Stroke Team One” or “Stroke Team Two” • Stroke Team Onepatients <6 hours since onset of symptoms• Stroke Team Twopatients >6 hours since onset of symptoms OR
patients whose symptoms have resolved (due to transient ischemic attack)
• ED nurses perform brief neurologic exams every 15 minutes following patient arrival• Orientation, motor skills, sensory abilities, speech, and vision
• NIHSS score determined by stroke neurologist, neurology resident, or stroke research nurse
Jahnke HK, et al. J Emerg Nurs. 2003;29:133-139.
A Two-Armed ApproachA Two-Armed Approach

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Improvement in Patient CareImprovement in Patient Care
Adapted from Jahnke HK, et al. J Emerg Nurs. 2003;29:133-139.
10
33
7
45
88
44
60
111
77
0
20
40
60
80
100
120
Established NINDSGoals
2000 Data 2001 Data
Tim
e (m
in)
Arrival to Doctor
Arrival to Completed CT
Total Door-to-Needle Time
Since Implementation of Stroke Team Since Implementation of Stroke Team and Acute Stroke Pathwayand Acute Stroke Pathway

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
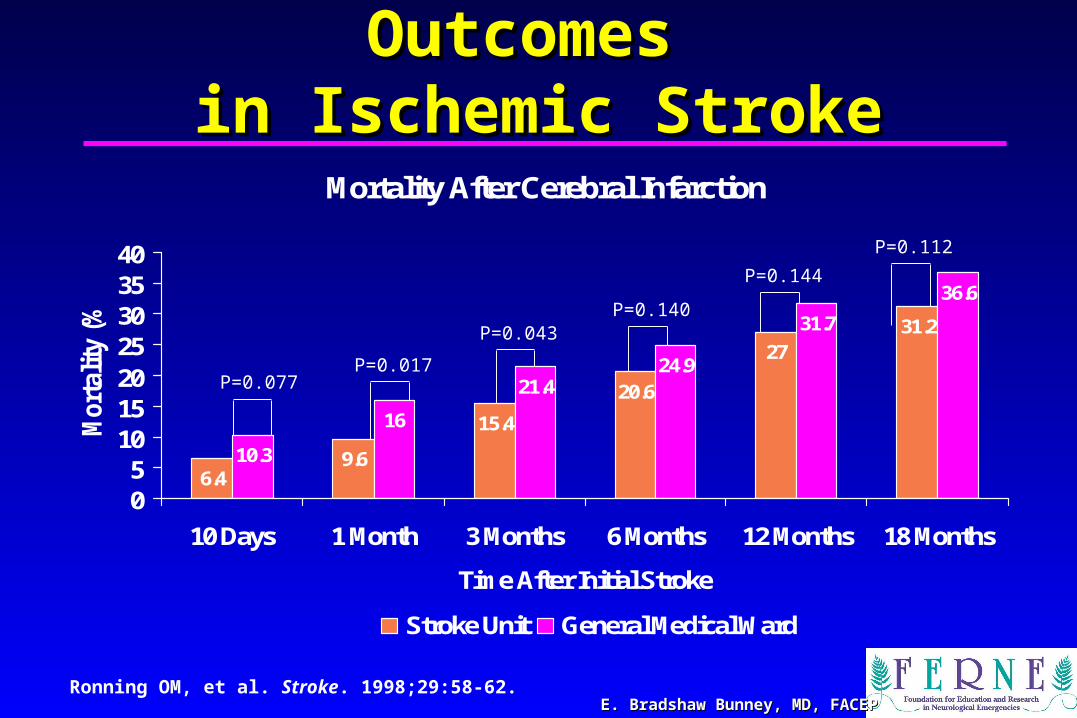
Stroke Units Improve OutcomesStroke Units Improve Outcomes
• Study included 802 patients admitted with a stroke diagnosis to a hospital in Norway
• Study patients arrived within 24 hours of stroke onset and were at least 60 years old
• Patients were treated in the stroke unit or in the general medical ward
• Stroke outcomes were assessed
Ronning OM, et al. Stroke. 1998;29:58-62.
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Stroke Units Improve Outcomes Stroke Units Improve Outcomes in Ischemic Strokein Ischemic Stroke
P=0.077P=0.017
P=0.043P=0.140
P=0.144
P=0.112
Mortality After Cerebral Infarction
6.49.6
15.4
20.6
2731.2
10.3
16
21.424.9
31.7
36.6
05
10152025303540
10 Days 1 Month 3 Months 6 Months 12 Months 18 Months
Time After Initial Stroke
Mor
talit
y (%
)
Stroke Unit General Medical Ward
Ronning OM, et al. Stroke. 1998;29:58-62.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Stroke Units Improve Outcomes Stroke Units Improve Outcomes in Hemorrhagic Strokein Hemorrhagic Stroke
P=0.0291P=0.0041 P=0.0143 P=0.0104 P=0.0205 P=0.0217
Mortality After Intracerebral Hemorrhage
24.5
37.7 39.645.3
52.856.6
51.658.1 61.3 62.9
69.4 71
01020304050607080
10 Days 1 Month 3 Months 6 Months 12 Months 18 Months
Time After Intial Stroke
Mor
talit
y (%
)
Stroke Unit General Medical Ward
Ronning OM, et al. Stroke. 1998;29:58-62.

““Drip and Ship”?Drip and Ship”?
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Is There a Role forIs There a Role for

Strict Protocol is the Strict Protocol is the
KEYKEY
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Rural Nevada Rural Nevada
• One designated stroke center
• 8 rural EDs
• One protocol agreed to by all hospitals
• Managed through the central stroke team
• Site visits to confirm protocol adherence and promote team approach

Role of Community Role of Community EducationEducation
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Can Community-Based Education Can Community-Based Education Improve Knowledge? Improve Knowledge?
Becker KJ, et al. Cerebrovasc Dis. 2001;11:34-43.
• Objective• Assess if the knowledge deficits regarding
stroke signs, symptoms, and risk factors could be improved
• Methods• Telephone interviews used to assess effect
• Several media resources used
• May to September 1998

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Community-Based Education Community-Based Education Improves Knowledge: ResultsImproves Knowledge: Results
Becker KJ, et al. Cerebrovasc Dis. 2001;11:34-43.
• What organ is injured during a stroke?• Prior to the campaign, 45.2% of respondents knew that the
brain was injured, after the campaign, 49.5%• Can’t easily teach old dogs new tricks• Sustained media education• Begin education earlier in life
• Effect of education campaign• Respondents were 52% more likely to know a risk factor of
stroke (P=0.005)• Respondents were 35% more likely to know a symptom of
stroke (P=0.032)

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Community-Based Education Community-Based Education Improves Knowledge: ConclusionImproves Knowledge: Conclusion
Becker KJ, et al. Cerebrovasc Dis. 2001;11:34-43.
• There is a severe knowledge deficit about stroke that is greater in those at a high risk for stroke, including:• Elderly• Less educated• Persons with low income• Men• Asian Americans
• Knowledge deficit can be improved through community-based education, particularly through public service announcements on television

EMSEMSFront and CenterFront and Center
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Paramedic Quick ScreenParamedic Quick Screen• Paramedic Quick Screen
• Focal neurological symptoms including:• Unilateral weakness• Numbness• Blindness • Loss of speech • Loss of balance
• Well-established time of onset less than 3 hours
• Age >18 years • Notify Base Station to activate Code Stroke
on potential patients during transport
1. Lyden PD, et al. J Stroke Cerebrovasc Dis. 1994;4:106-113. 2. Rapp K, et al. J Neurosci Nurs. 1997;29:361-366.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
University of CincinnatiUniversity of CincinnatiPrehospital Stroke ScalePrehospital Stroke Scale
• Facial Droop (Patient shows teeth or smiles):• Normal (Both sides of face moves equally well)• Abnormal (One side of face doesn’t move as well as other side)
• Arm drift:• Normal (Both arms move the same OR both arms don’t move at all)• Abnormal (One arm either doesn’t move OR one arm drifts down
compared to the other)
• Speech (The patient says “The Cubs aren’t going to the playoffs”):• Normal (Patient says correct words with no slurring of words)• Abnormal (Patient slurs words, says the wrong words, or is unable
to speak)
Source: Adapted from Kothari R, et al. Acad Emerg Med. 1997;4:986-990

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
AHA-Recommended Assessment of a Person AHA-Recommended Assessment of a Person With Suspected Stroke by EMS PersonnelWith Suspected Stroke by EMS Personnel• Assure adequate airway
• Monitor vital signs
• Conduct general medical assessment
• Evidence of trauma to head or neck
• Cardiovascular abnormalities
• Ocular signs
• Conduct neurological examination• Prehospital assessment (eg, Cincinnati Prehospital Stroke Scale)
• Level of consciousness (Glasgow Coma Scale)
• Pupils: size, equality, reactivity
• Presence of seizure activity
• Prearrival notification: estimated time of onset, Glascow Coma Scale score
AHA. BLS for Healthcare Providers. 2001:36-47.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Assessing the Role of Paramedic Assessing the Role of Paramedic Diagnosis and ED Efficiency Diagnosis and ED Efficiency
• Houston study• Performance data from paramedics and 6 hospital EDs• Data collected from 446 patients with suspected acute
stroke• Data were used to assess the effect of:
• Establishing emergency stroke centers• Paramedic education program
• Target treatment times were based on ASA standards• Unenhanced CT scan of the brain within 30 minutes• Maximum of 60 minutes for initiation of tPA
Wojner AW, et al. Am J Crit Care. 2003;12:411-417.
ASA=American Stroke Association.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Effectiveness of Paramedic Diagnosis Effectiveness of Paramedic Diagnosis and ED Treatment Patterns and ED Treatment Patterns
• Stroke diagnosis 321/446 (72%) cases• Onset of signs/symptoms 359/446 (80.5%)
patients• Of these 359 patients, 210 (58.5%) arrived
at the ED within 120 minutes of onset• There were 319 case report forms submitted
with thrombolysis data; 195 of these cases had acute ischemic stroke diagnosed; hospitals 3 and 6 did not administer thrombolytics
Wojner AW, et al. Am J Crit Care. 2003;12:411-417.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
EMS and ED Stroke Care Are EMS and ED Stroke Care Are Improved With EducationImproved With Education
• Houston paramedics are able to diagnose stroke• Aggressive stroke education initiative during the
NINDS study• Close interaction between paramedics and hospital
• Community awareness of signs/symptoms• Allowed >65% of patients with confirmed stroke to
arrive in the emergency department within 3 hours
• ASA standards can promote uniform stroke assessment and treatment processes
Wojner AW, et al. Am J Crit Care. 2003;12:411-417.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
ED Stroke ProtocolED Stroke Protocol• All very similar
• Specific to nuances within the specific hospital
• Must be strictly followed
• Must be implemented in ALL appropriate patients

Treatment of Stroke Patients Treatment of Stroke Patients Following Admission to the Following Admission to the
Hospital Hospital
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Admission to the Hospital Admission to the Hospital and Complicationsand Complications
• Approximately 25% of patients can worsen during first 24 to 48 hours after stroke • DVT/PE• Pneumonia/aspiration• Neurological complications
• Most to a monitored setting• OT/PT are essential
Adams HP, et al, a scientific statement from the Stroke Council of the American Stroke Association, approved by the American Heart Association Science Advisory and Coordinating Committee. Stroke. 2003;34:1056-1083.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Recommendations for Stroke Care Recommendations for Stroke Care Following Admission to HospitalFollowing Admission to Hospital
• Admission to a stroke unit with comprehensive rehabilitation for patients
• Frequent neurological status checks and vital signs during the first 24 hours
• Early mobilization and measures to prevent stroke complications• Aspiration, malnutrition, pneumonia, deep vein thrombosis
(DVT), pulmonary embolism, pressure sores, orthopedic complications, and contractures
• Prophylactic treatment to prevent DVT • Treatment of infectious complications with antibiotics• Treatment of concurrent medical conditions

EM Controversies EM Controversies
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
in Stroke Managementin Stroke Management
ACEP.org

SAEM.org

AAEM.org
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
EM ConcernsEM Concerns• Internal and external validity of the NINDS trial
• Single trial (two parts)• Treated group not as sick as the placebo group• Hemorrhage rate• Neuroradiology interpretation
• Infrastructure needed to provide timely care• EMS not prepared for their role• Hospitals not prepared for their role
• Medical legal concerns in the emergency medicine and neurology communities
• Reimbursement issues

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
EM Role in the Process and CenterEM Role in the Process and Center• A hospital can not embark on
becoming a stroke center without EM participation
• Models exist where EM has taken the lead role in developing the stroke team• Conversely, models exist where EM has
blocked the initiative

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
ACEP and Stroke CentersACEP and Stroke Centers• October 2003: ACEP Council and Board of Directors
unanimously adopted a resolution to monitor the progress of any federal stroke legislation and dedicate resources to make members of Congress aware that:• Standards of care in stroke treatment remain controversial• The designation of stroke centers based on their ability /
willingness to adhere to such standards of care may have many unintended negative consequences

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
SAEM: MAY 18, 2004SAEM: MAY 18, 2004• Background
• Policy statements: Andy Jagoda• American Stroke: Ellen Magnis
• Panel Presentations• American Stroke: Mark Alberts• ACEP: Brian Hancock• SAEM: Jim Adams• NAEMSP: Robert O’Connors• JACHO: Maureen Connors Potter
• Panel Discussion

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Where do We go From Here?Where do We go From Here?• Work with the Brain Attack Coalition• Educational programs
• Medical students• Residents
• Implementation packets for stroke center certification• Pathways, protocols, tools
• Focus on future therapies and having systems in place to facilitate utilization

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Clinical CourseClinical Course
The patient was met by a nurse, a doctor and an EM tech and taken to the resuscitation room. They confirmed the onset time of 2:15pm. Vital signs were BP 142/88, P 98, R 16, T 99.2 F. HEENT: eyes were deviated to the right but came back to midline with command, PERRL, Ears clear, neck supple. Heart, lungs and abdomen were normal. Neurological exam: CN mild left facial droop, strength 5/5 R arm and leg, 1/5 L arm and leg, no light touch or pin prick sensation in the L arm and leg. NIHSS=17-18.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Clinical CourseClinical Course• The stroke team was called at 3:05pm • Labs were drawn and sent. • The patient went to CT at 3:20 pm and
returned at 3: 41pm.• The stroke team assessed the patient on
return from CT and agreed with the diagnosis of CVA and NIHSS=18.
• Head CT reading was “negative for bleed, normal brain” at 4:03pm.

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Clinical CourseClinical Course• The patient was felt to be a good candidate for
thrombolytics. The patient was advised of the risks and benefits.
• The patient, along with his wife refused thrombolytic therapy, stating “I want nature to take its course”.
• The patient was given 325 mg. of aspirin and admitted to the hospital.
• His 24 hour NIHSS=14.• On discharge, 5 days later, NIHSS=10.
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Key Learning PointsKey Learning Points• JACHO Stroke Center certification requires
multi-disciplinary cooperation with one central champion
• Strict adherence to stroke protocols improves outcomes in these patients
• EMS plays a KEY role in maximizing the management of stroke patients
• The EM community has numerous concerns about the Stroke Center designation concept

E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, FACEP
Questions??Questions??
[email protected]@ferne.org
E. Bradshaw Bunney, MD, FACEPE. Bradshaw Bunney, MD, [email protected]
312 413 7484formatted_bunney_strokecenter_aaem_2005.ppt 2/11/2005 7:32 PM