supported by the leukemia and lymphoma foundation targeting bcl-2 in cll asher chanan-khan,...
TRANSCRIPT
Supported by The Leukemia and Lymphoma Foundation
Targeting Bcl-2 in CLL
Asher Chanan-Khan, MD Jennifer R Brown, MD PhDProfessor of Medicine Director, CLL Center, DFCIMayo Clinic Florida Associate Professor, Harvard

Bcl-2 (B-cell lymphoma 2)
• First detected in Follicular NHL having t(14;18)
• Translocation results in overproduction of Bcl-2 anti-apoptotic protein
• t(14;18) rarely seen in CLL, though Bcl-2 is overexpressed in ~80% of cases
• Bcl-2 prevents Bax/Bak pro-apoptotic executioner molecules
• Dysregulated expression counters physiologic apoptosis
Bcl-2 protein bound to portion of
Bax
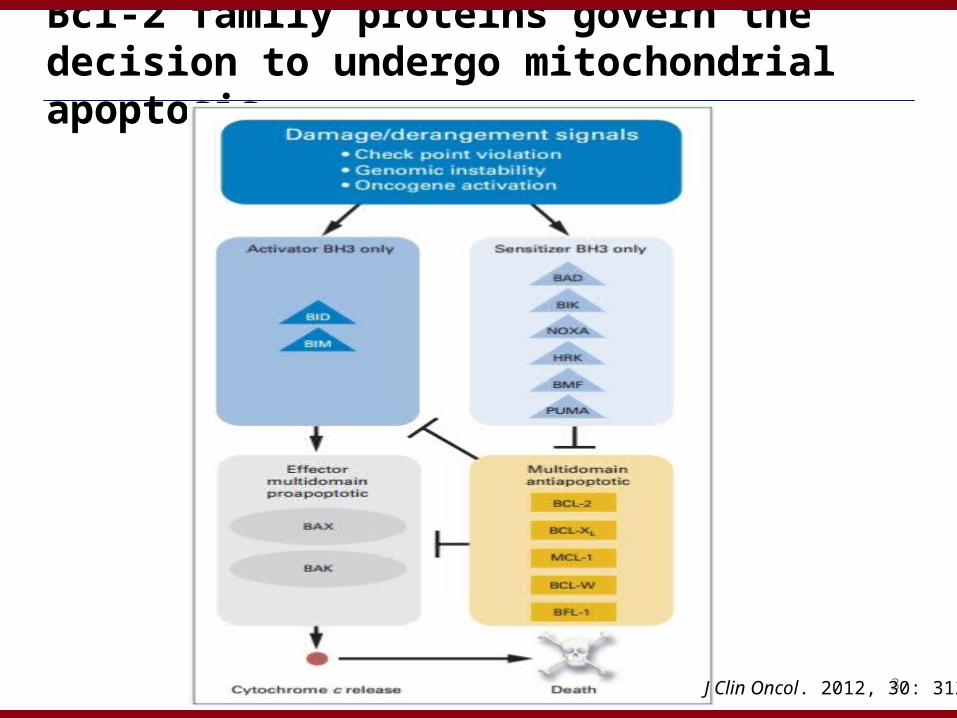
Bcl-2 family proteins govern the decision to undergo mitochondrial apoptosis
3J Clin Oncol. 2012, 30: 3127

4
Displacement of Bim from Bcl-2 induces rapid, irreversible cell death
J Clin Oncol. 2012, 30: 3127

Bcl-2 Is Expressed in Most Types of Cancer
Solid Tumors Hematologic Cancers
Breast Melanoma SCLC CLL Myeloma
LymphomaAMLProstate (HR)Colorectal
1. Lanzafame S et al. Pathol Res Pract. 1998. 2. Yang H-B et al. Anticancer Res. 1999. 3. Jiang S-X et al. J Pathol. 1995. 4. Cerroni L et al. Am J Dermatopathol. 1995. 5. Sullivan GF et al. Clin Cancer Res. 1998. 6. Karakas T et al. Ann Oncol. 1998. 7. Lazaridou A et al. Leukemia Lymphoma. 2000. 8. Chen X et al. Chin J Oncol. 1997. 9. Puthier D et al. Leukemia. 1999.

Bcl-2 expression is increased in and on CLL cells
McCarthy et al Mol Med. 2008 Sep-Oct;14(9-10):618-27
mRNA
A.
B.
C.

High Bcl-2 Expression in CLL Is Associated with Lower Survival
Cu
mu
lati
ve P
rop
ort
ion
Su
rviv
ing
Months0 10 20 30 40 50 60
Faderl et al., Leukemia. 16:1045-1052, 2002.
1.0
0.8
0.6
0.4
0.0
0.9
0.7
0.5
0.3
0.2
0.1
++++ +
+
+++ + ++++++ +
+++++++++++
++ ++ ++++ ++ + +++
++++ ++++ ++ +++++++ +
+
+
++ +
++ +
+++++ +++ +++ + +++ +
+
+++++++
++ + +Bcl-2<3.2>3.2
Pats.11584
P=0.00006
Died2336

Interaction with stromal cells increases anti-apoptotic Bcl-2 proteins in CLL cells
Patel et al Leuk Lymph 2014 Apr;55(4):899-910.
Bcl-2
Bcl-w
Mcl-1
Bcl-xL

Therapeutic strategies to disrupt Bcl-2 function
1. Antisense-based (Oblimersen sodium)
2. Small molecule-based (BH3 mimetics)• AT-101 (Phase II)• Obatoclax – limited efficacy, non-oral availability
• ABT-263 / Navitoclax – increased thrombocytopenia• ABT-199 (Phase III)

Adapted from Zeitlin B D et al. JCO 2008;26:4180-4188
Small-molecule inhibitors of Bcl-2 family proteins
BH3 mimetics

BH3 Mimetics “mimic” BH3-containing pro-apoptotic proteins
• Navitoclax and ABT-199 mainly disrupt Bim:Bcl-2 complexes, not free Bcl-2, Mcl-1 or Bcl-w
• Displaced Bim can antagonize Mcl-1 and/or directly activate Bax/Bak
• Ability to bind Bcl-2 (or other anti-apoptotic Bcl-2 family proteins) with affinities comparable to endogenous ligands likely dictates efficiency to displace Bcl-2 increased Bak/Bax activation apoptosis
Czabotar et al Nat Rev Mol Cell Biol. 2014 Jan;15(1):49-63.

ABT-263
• Oral inhibitor of Bcl-xL, Bcl-2 and Bcl-w
• Binds hydrophobic BH3 binding pocket with high affinity
(Ki ≤ 1 nM)

ABT-737 Induces Apoptosis in Primary CLL Cells
Independent of clinical features:FISH, IGVH,ZAP-70

ABT-263 Induces Reversible Thrombocytopenia: Dog Toxicology Study
Study Day
Dosing
Recovery0
100
200
300
400
500
600
-5 0 15 27 30 34 41
0 mg/kg
1 mg/kg
3 mg/kg
10 mg/kg
20 mg/kg
Pla
tele
t C
ou
nt

Phase 1 ABT-263 in Relapsed CLL: Study M06-873
• Phase I/2a dose-escalation trial– Modified continuous reassessment method
• Eligibility:– Relapsed or refractory CLL and requiring
treatment– Platelets ≥ 75,000/mm3
– Exclusions:• History of immune thrombocytopenia• Prior stem cell transplantation Blood 2009;
114: 883

Enrolled Patient Characteristics
• N=29
• Age: 67 (50-79 y)
• Gender (M:F): 19:10
• No. of prior therapies: 4.5 (1-11)
• Fludarabine refractory: 9 (31%)
• Lymphocyte Count: 15.5 x 109/L (0.8 –
284.3)
• Bulky nodes (> 5cm): 12 (41%)
• FISH: 17p: 11 / 25 (44%)
11q: 5 / 25 (20%)
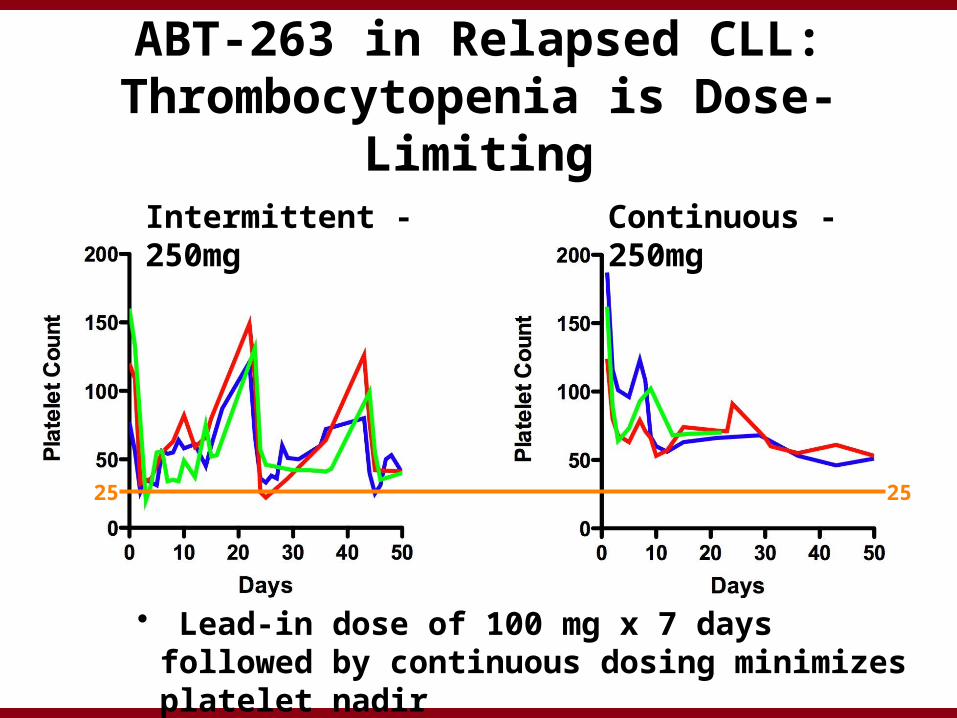
ABT-263 in Relapsed CLL: Thrombocytopenia is Dose-Limiting
Intermittent - 250mg Continuous - 250mg
25 25
• Lead-in dose of 100 mg x 7 days followed by continuous dosing minimizes platelet nadir

Navitoclax induces CLL cell apoptosis in vivo and reduces disease burden
Roberts A W et al. JCO 2012;30:488-496
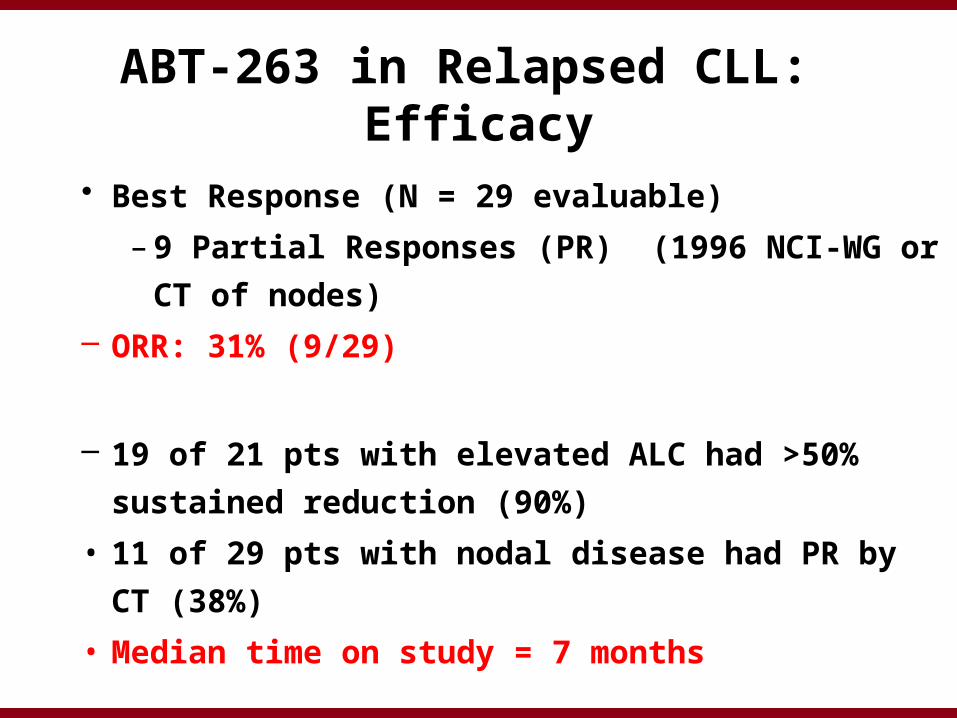
ABT-263 in Relapsed CLL: Efficacy
• Best Response (N = 29 evaluable)
– 9 Partial Responses (PR) (1996 NCI-WG or CT of
nodes)
– ORR: 31% (9/29)
– 19 of 21 pts with elevated ALC had >50% sustained
reduction (90%)
• 11 of 29 pts with nodal disease had PR by CT (38%)
• Median time on study = 7 months
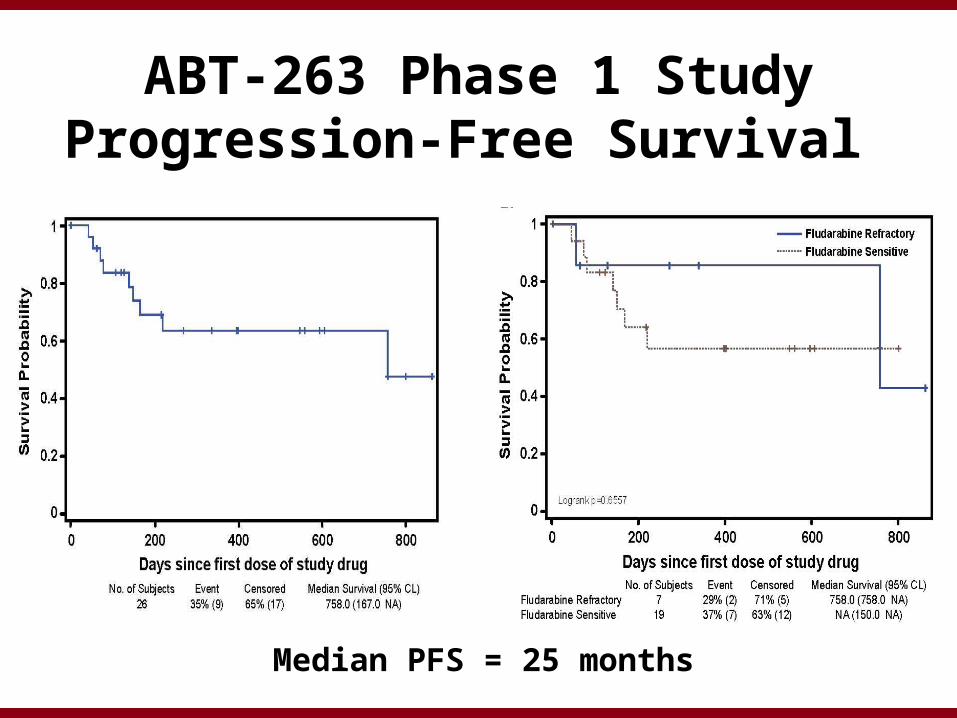
ABT-263 Phase 1 StudyProgression-Free Survival
Median PFS = 25 months

Response Correlates with Low MCL-1 and High BIM:MCL-1 or BIM:BCL-2 Ratios
MCL-1 BIM:MCL1 Ratio
BIM:BCL2 Ratio

ABT-263 Slightly Less Potent than ABT-737: Likely Insignificant
S KhawD HuangAW Roberts

Apoptosis In Vitro Is Inhibited in Whole Blood, by Albumin Binding
CCR 2010; 16: 4217
10mM ABT263
1mM

Co-Culture with CD154+ Fibroblasts Leads to ABT-737 Resistance
CLL Cell Viability after 24 hr. Co-Culture
Vehicle
ABT-737
0
20
40
60
80
100Parental
CD154+
p < 0.001
% v
iab
ilit
y b
y A
nn
ex
in-P
I
M Davids, J Brown, A Letai, unpublished data

ABT-199: Selective Bcl-2 small molecule inhibitor
• Developed by structure-based NMR-guided design using ABT-263 as a scaffold
• Potently binds Bcl-2 with a Ki of 0.010nM
• Causes less thrombocytopenia than ABT-263 (due to less selectivity for Bcl-xL)
• Oral availability (daily dose schedule)
• Currently being investigated in phase III trials in CLL, Non-Hodgkin's lymphoma and multiple myelomaABT-199
ABT-263
Bcl-2
Souers AJ et al. Nat. Med. (Vol.19) 2013; Seymour JF et al. ASCO 2013, Abstract #7018

ABT-199 Dosing SchemaDaily ABT-199 doses increased weekly to the designated cohort dose (DCD)
Initial Ramp-Up Schema: Dose Escalation
Ramp-Up Schema: Expanded Safety Cohort
* 3 patients (1 each in cohorts 2, 3, & 5) received ABT-199 20 mg as initial dose** Step-up doses range from 100 to 400 mg # DCD ranges from 150 to 1200 mg

Patient Characteristics (n=105)Characteristics All CLL/SLL
Age, y Median 66 [36 – 86]
Bulky nodes, n (%) ≥5 cm 58 (55)
≥10 cm 17 (16)
Number of prior therapies
Median 4 [1 - 11]
IGHV mutation status Unmutated 36/48 (75)
17p Status Deleted 23 (22)
Not Deleted 49 (47)
Missing 9/24 (31)
Fludarabine, n (%) Prior Treatment 87 (83)
Refractory 62 (59)

Adverse EventsAll Grades≥20% of pts
N=105n (%)
Diarrhea 42 (40) Neutropenia 38 (36) Nausea 37 (35) Upper respiratory tract infection 35 (33) Fatigue 27 (27) Cough 21 (20)
Grades 3/4 ≥ 5% pts n (%)
Neutropenia 35 (33) Anemia 10 (10) Febrile neutropenia 7 (7) Thrombocytopenia 7 (7) Hyperglycemia 7 (7) Tumor lysis syndrome (TLS) 7 (7) Hypokalemia 5 (5)

Presentation Title | Date xx.xx.xx | Company Confidential © 2013 29
Serious Adverse Events (SAEs) Possibly or Probably Related to ABT-199
SAEs (≥ 2 pts) N=105n (%)
Febrile neutropenia 4 (4)
Tumor lysis syndrome (TLS)* 3 (3)
• Other SAEs (n=1): sudden death* (in the setting of TLS)
As of April 9, 2014, in the 49 patients treated since modifications were made to the dose ramp-up scheme as well as the tumor TLS prophylaxis and monitoring schedule, no additional events of clinical TLS (or SAEs of TLS) have been reported.

Best Percent Change from Baseline in Blood Lymphocyte Count and Nodal Mass by CT Scan
Nodal Mass by CT Scan (n= 93)• The median time to 50% reduction 1.4
months, range [0.65 – 13.7]*• 78 (84%) evaluable patients had at least a
50% reduction in sum of the product of diameters (SPD) of nodal masses
*coincides with first protocol specified CT scan at 6 weeks.
30
Blood Lymphocytes (n=60)
• Median Time to 50% reduction: 14 days, range [1 – 49]
Data represents patients with lymphocyte count >5 x 109/L at baseline
% C
ha
ng
e f
rom
Ba
se
line
-100
-75
-50
-25
0
25
200 800600 400 Safety Expansion150 400300 1200
Cohort Dose (mg)Cohort Dose (mg)

Best Percent Change from Baseline in Bone Marrow Infiltrate (n=51)
• Median time to 50% reduction: 5.5 months, range [1.9 – 17.4]*
• 46/51 (90%) evaluable patients have had at least a 50% reduction.
Anti-tumor activity of ABT-199 was observed in all tumor compartments.
# ^
# Patient had 70% infiltrate at baseline and at Week 24 ^Patient did not have CLL infiltrate at baseline.

Objective Responses of ABT-199 Treated Patients
ResponsesAll
n (%), n = 78del (17p)
n (%) , n = 19F-Refractoryn (%), n =41
IGHV Unmutatedn (%), n =24
Overall response 60 (77) 15 (79) 31 (76) 18 (75)
Complete response (CR/CRi)# 18 (23) 5 (26) 9 (22) 7 (29)
Stable disease 10 (13) 2 (11) 7 (17) 2 (8)
Disease progression 2 (3) 1 (5) 1 (3) 2 (8)
• The median duration of response has not yet been reached based on current patient enrollment numbers.

Current Status of Enrolled Patients (n=105; April 9, 2014)
Median Time on Study
Dose Escalation Patients (all dose levels): 17.1 months, range [0.06 – 29.7]
Safety Expansion Patients: 4.7 months, range [0.52 – 9.3]
Discontinuations
As of April 9, 2014, 105 patients are enrolled and 37 have discontinued for the following reasons:
• 22 Progressive Disease (of which 15 were from Richter’s)
• 12 Adverse Events
• 3 other (1 need for Coumadin, 2 proceeded to alloSCT)
Based on the preliminary safety and efficacy profile of ABT-199, 400 mg is currently being explored as the safety expansion dose.

Progression Free Survival (PFS) at 400 mg or Higher
• Median PFS for patients treated at or above 400 mg has not yet been reached (median follow-up of 5.3 months, range [0.03 – 22])
• As of April 9, 2014, the median PFS for all patients is approximately 18 months

BH3 Profiling provides functional confirmation of on target Bcl-2 antagonism and may predict depth of clinical response to ABT-199
Davids, Deng, Letai (unpublished data)
ABT199 iBH3- BAD 80
ABT199 iBH3 1uM
BA
D 8
0
0 20 40 60 80 1000
20
40
60
80
100
BAD 80
p=0.0001
% cyto C releaseABT-199 1 uM
%cy
to C
rel
ease
BA
D 8
0 u
M
BAD vs. ABT-199 Mitochondrial Depolarization
R square=0.7465

Dosing Schedule of ABT-199 and Rituximab – Cohorts 3 - 6
OR: if one or more electrolytes meet Cairo-Bishop criteria and/or if there is ≥ 30% decrease in ALC with first dose
• 400mg, 500mg, 600mg and safety expansion cohorts dosed with this schedule
37
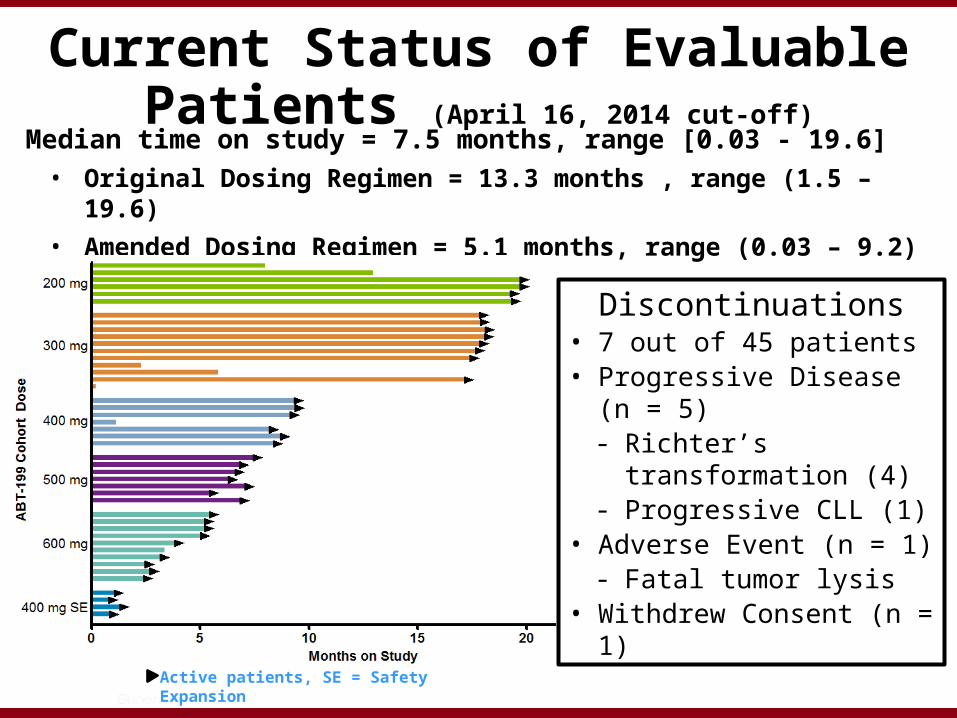
Current Status of Evaluable Patients (April 16, 2014 cut-off)
Median time on study = 7.5 months, range [0.03 - 19.6]
• Original Dosing Regimen = 13.3 months , range (1.5 – 19.6)
• Amended Dosing Regimen = 5.1 months, range (0.03 – 9.2)
Active patients, SE = Safety Expansion
Discontinuations• 7 out of 45 patients • Progressive Disease (n = 5)- Richter’s transformation
(4)- Progressive CLL (1)
• Adverse Event (n = 1)- Fatal tumor lysis
• Withdrew Consent (n = 1)

Responses of Patients treated with ABT-199 and Rituximab
ResponseEvaluable Patients
n=25 (%)
Overall Response 21 (84)
CR (n=4)/ CRi (n=5)* 9 (36)
Disease progression 1 (4)
Discontinued prior to M7 assessment # 2 (8 )
• Of the 20 patients on study < 7 months (still receiving combination):5 have a PR, 6 have a PR at first CT; 9 have not yet been evaluated

Presentation Title | Date xx.xx.xx | Company Confidential © 2013 39
Minimal Residual Disease (MRD)MRD was assessed by local lab using 4 color flow cytometry in 8/9 CR/CRi patients and 6 patients with a PR (based on available data)
Patient Response Source Sensitivity MRD
1 CR Bone Marrow 10-4 Negative
2 CR Peripheral Blood 10-3 Negative
3 CR Bone Marrow 10-3 0.20%
4 CR Bone Marrow 10-3 Negative
Peripheral Blood 10-3 Negative
5 CR Bone Marrow 10-4 Negative
6 CR Bone Marrow 10-4 Negative
7 CR Bone Marrow 10-4 0.02%
8 CR Bone Marrow 10-4 Negative
9 PR Bone Marrow 10-4 Negative
10 PR Bone Marrow 10-4 < 1%
11 PR Bone Marrow 10-4 Negative
12 PR Peripheral Blood 10-4 Negative
13 PR Bone Marrow 10-4 Negative
14 PR Bone Marrow 10-4 Negative

Complete Remission: Discontinuation of ABT-199
• 3 patients have discontinued ABT-199 after achieving CR/CRi (2 with MRD negativity)
• Patients had 1, 3, and 4 prior therapies; one had fludarabine refractory disease– Patients are continuing follow-up on study– Patients remain in CR at the time of this analysis (8.6, 8.8, and 11.6
months after cessation)

Ongoing Clinical Trial
1. Phase III, randomized study in relapsed/refractory CLL to evaluate the benefit of ABT-199 + rituximab vs. BR.
2. Phase 2 study of ABT-199 in patients with relapsed or refractory CLL harboring 17p deletion.
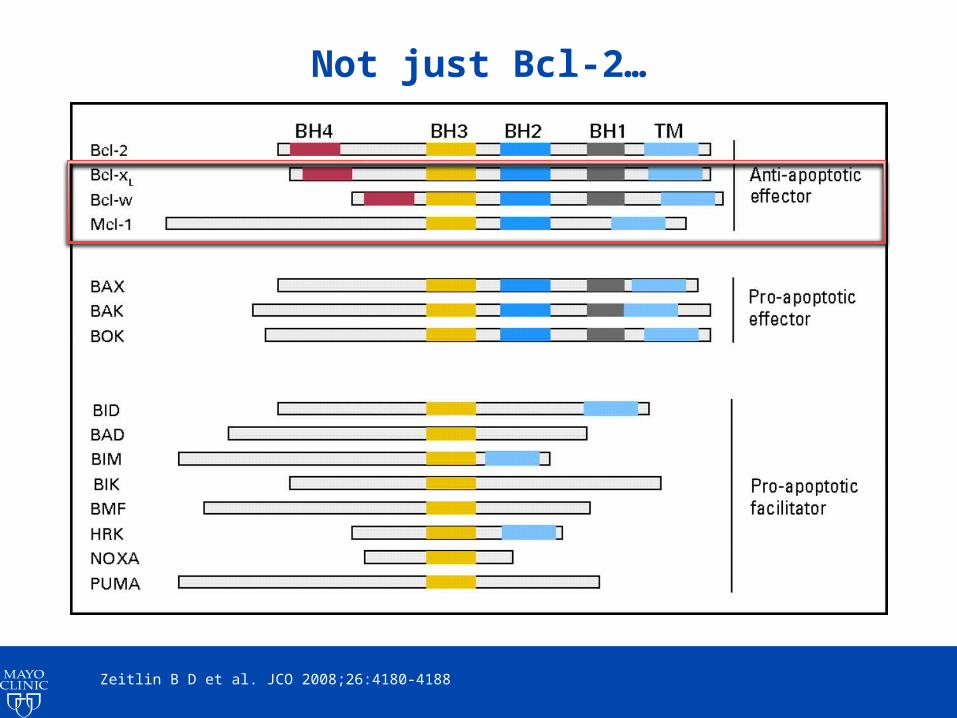
Not just Bcl-2…
Zeitlin B D et al. JCO 2008;26:4180-4188

Potential mechanisms of resistance to ABT-199
• Mcl-1 upregulation
• Stromal mediated resistance
• Mutations in BCL2 or BAX
ABT199 alone
(Low BCL2/MCL1 ratio)
Touzeau et al Leukemia (2014) 28, 210–212; Soderquist et al J. Biol. Chem. 2014, 289:16190-16199; Fresquet et al Blood 2014 Jun 26;123(26):4111-9.

Summary
• BCL-2 is a critical survival pathway in CLL
• BCL-2 family interactions are complex – influenced by multiple family members and the microenvironment– Targeting BCL-XL is problematic in CLL patients
• ABT199 has profound clinical activity, including in bone marrow clearance– Clinical care required due to TLS
• Resistance likely to emerge– ? Early signal of excess Richter’s transformation