surgical pearls . . . . . . . . . . . . . . . .8 policy and the...
TRANSCRIPT
Editor’s Message . . . . . . . . . . . . . . 3
Washington Medical Matters . . . . .5Policy and the Retina MDWith William L. Rich III, MD
The Road to Recertification . . . . . .6Competencies in Neuro-ophthalmologyBy Nicholas J. Volpe, MD
Surgical Pearls . . . . . . . . . . . . . . . .8The Transition From Fellow toAttending SurgeonBy Omesh P. Gupta, MD, MBA
Break it Down . . . . . . . . . . . . . . .10What Are You Getting With SD-OCT?By Prithvi Mruthyunjaya, MD
Finance Your Life . . . . . . . . . . . . .13Positioning Yourself for Financial SuccessBy Gog Boonswang, CFA;and Lifan Shen, CFA

At the Tip of Performance
works ideally with
e 25+ Probe. Designed for Uncompromising Rigidity and Offering Outstanding Performance.
See the Complete Alcon® MIVS Plus SolutionAvailable in 23 and 25G
Stiffer NeedleUltra-High Speed Cutting Performance up to 5000 CPMImproved Duty Cycle & Higher Aspiration Flow RatesPort Optimization
– Larger Cutting Port Area– Cutting Port Closer to End of Tip
+
+
+
+
25+
25G
Fully Integrated with Grieshaber® DSP 25+ Instruments.
Tip of PerformanceTipTip of Performance
©2009 Alcon, Inc GAU063

As you begin reading this edito-rial, you should be askingyourself, “Why do we needanother journal?” The answeris that New Retina MD is dif-
ferent from other published journals—it wascreated and designed to fill a void in theophthalmic and retina literature. Unlike pub-lications that target the broad community ofretinal specialists, New Retina MD will focussolely on issues that physicians like us, whoare in the first 15 years of their career, face.
Additionally, New Retina MD is geared toward the lives ofretina specialists, not just the practice of medicine.
As readers of the literature, we have noticed that a hostof publications exist that either publish peer-reviewedpapers, summarize the literature, or provide updates onmajor presentations at meetings. We recognized that ahost of topics particular to our needs and interests are leftuntouched. Thus, New Retina MD will pay more robustattention to issues most pertinent to our age cohort and toour day-to-day lives, both clinical and nonclinical.
What’s InsideAs a group, we have unique financial concerns to deal
with in the early part of our careers. Gene Ng, a retinalspecialist who carries an MBA from Harvard, edits our“Finance Your Life” section, which will deconstruct, ana-lyze, and provide insight into the major financial eventsthat you will face in the early part of your career.
Early in our careers, we are in a unique place where weare clinically expert but are still refining our surgical andmedical skills and approaches. New Retina MD will focus on“how to practice” and discuss and help refine clinical skillsappropriate for our stage of practice. Our clinical sectionpresents in-depth interviews with the most accomplishedand recognized retinal specialists who will share their pearlson how to approach a host of problems using the most up-to-date techniques.
Because our age cohort is the first that is required todemonstrate our compentencies in all areas of ophthalmol-ogy every 10 years, New Retina MD will feature a recurring
section, “The Road to Recertification,” which reviews topicsoutside of retina. In this issue, we feature a review of the 10most likely topics to be addressed in neuro-ophthalmology.We will continue to cover similar broad-based topics witheach issue.
Finally, we have assembled an Editorial Board that wellrepresents our cohort’s interests. This dynamic group willcontinue to mold this journal to our needs as a group ofspecialists in the first third of our careers. We welcome yourideas for future issues and encourage your feedback. Thisjournal will continue to evolve and provide needed insightcritical to new retina MDs. NRMD
-Jonathan Prenner, MD; and Richard Kaiser, MDChief Medical Editors
1. John Cleese, from Monty Python’s Flying Circus.
Editorial Advisory Board
Staff Alan B. Guralnick, Publisher484 581 1832; [email protected]
Rachel M. Renshaw, Editor-in-Chief484 581 1858; [email protected]
Adam Krafczek Jr, Esq, Vice President484 581 1815; [email protected]
Barbara Bandomir, Director of Operations484 581 1810; [email protected]
Ron Stender, Director of Art and Production484 581 1864; [email protected]
“And Now for SomethingCompletely Different”1
Diana V. Do, MD
Omesh Gupta, MD, MBA
Prithvi Mruthyunjaya, MD
Eugene W. Ng, MD, MBA
OCTOBER 2010 . NEW RETINA MD 3
Editor’s Message
Richard Kaiser, MD
Jonathan Prenner, MD

©2010CarlZeissMeditec,Inc.CIR.3090.0910.
Cirrus™ HD-OCT gives you a new level of clinical certainty. The latest
features improve your ability to identify pathology and track change
over time.
assessment of the area of interest.
comparison of two retinal exams.
™ ensures accurate registration
and excellent repeatability of macula thickness measurements.
New! Enhanced HD Raster Scan
Carl Zeiss Meditec, Inc. 800 342 9821 www.meditec.zeiss.com/us
Cirrus HD-OCT A new level of clinical certainty.
Visit 1
Visit 2
Visualize change with synchronized B-scans

With William L. Rich III, MD
Washington Medical Matters
OCTOBER 2010 . NEW RETINA MD 5
New Retina MD recently spoke with William L.Rich III, MD, regarding his take on issuesincluding electronic medical records (EMR),physician payments, the Physician QualityReporting Initiative (PQRI), and the effects ofthe health care reform bill. To follow is some
of what he had to say.
New Retina MD: One of the components of the 2009American Recovery and Reinvestment Act that was signedinto law by President Barack Obama is a provision for incen-tive payments that would be awarded to physicians whodemonstrate meaningful use of EMR.
What are your thoughts on the adoption of EMR in retinapractices and your interpretation of meaningful use?
William L. Rich III, MD: As far as I am concerned, the mean-ingful-use criteria would preclude the typical ophthalmic EMRfrom qualifying for this program, so I think it would be anegregious mistake to go out and purchase a system now; noone really knows what the final regulations will be. As the cri-teria are currently written, none of us will qualify. They willhave to be adjusted if the Centers for Medicare and MedicaidServices (CMS) wants further adoption of EMR into medicalpractice. Yes, there are potential bonuses and penalties, butno one really thinks it is going to be implemented in its cur-rent form.
NRMD: What are some examples of favorable revisions? Dr. Rich: There must be a greater emphasis on specialty
care. All of the meaningful-use criteria right now deal withclinically ill patients under the care of the primary carephysician, and although we all want coordinated care, thishas to occur between specialties and primary care.
NRMD: How will recent government decisions in pay-ments for physicians and the Patient Protection andAffordable Care Act affect the average retina specialist?
Dr. Rich: First of all, physicians, particularly those practic-ing ophthalmology, will do quite well through 2013. Since2009, ophthalmology receives the highest increase in prac-tice expenses (11%) among all medical specialties. The nexthighest beneficiary gets 5%. Second, liability payments haveincreased—ophthalmology is tied for the highest increase at2%, and there is also a 1% increase because of loss in con-sults. What does this all mean? Between 2010 and 2013, alldoctors are going to see robust increases in payments.
For example, the payments for cataracts will increase 17.5%between now and 2013, and complex retinal detachments will
increase approximately 16% to 18%. Those are hefty increasesafter over a decade and a half of freezes or cuts.
Payment for office procedures, which use a comprehen-sive eye code, will increase 13.6% over the next 3 years. Thein-office diagnostics payment increases are less robust atapproximately 11%. Overall, between now and Jan. 1, 2014,independent of health care reform, things look very good.
Ophthalmologists who do not participate in the MedicarePQRI Eye Program are, in my opinion, foolish. There is a 2%bonus in 2010, 1% in 2011, and 12.5% in 2013, but the prob-lem is that the penalties for nonparticipation after 2013escalate up to 2% per year ad infinitum. The impact is prettydevastating—similar to a negative of compounding interest.
Bonuses for reporting to a registry for Maintenance ofCertification (MOC), which all ophthalmolgists will face, areset at 0.5%.
The real problem with health care reform begins inapproximately 2015. There are 33 million new people whowill eventually be covered under this bill. Twenty million ofthem will be placed into Medicaid. Either a mandate will benecessary to ensure that doctors are accepting thesepatients or we will have to adopt the European model of anAll-Payer system, which is precisely the part of PresidentObama’s bill that will most likely be implemented in 2015 or 2016. In other words, payments from high-end insurancecompanies, such as Blue Cross and Blue Shield, would bebrought down to the Medicare and Medicaid level toensure that there are no financial disincentives for doctorsto accept Medicaid. For the retina specialist, the effect willnot be as significant as other specialties because most reti-na patients are already in the Medicare pool.
In addition to expanding insurance to the uninsured andmaking things more competitive so that people can goonline and pick out a plan and state, there are some otheritems that are mandated. One such mandate is thatMedicare initiate a service called the innovation center,which will calculate alternative methods of payment tophysicians to combat the popular notion that payment ismore closely tied to how many tests and procedures aphysician performs vs quality of outcomes. Additionally,quality of care will be publicly reported, bringing morescrutiny on the medical profession. NRMD
Policy and the Retina MD
William L. Rich III, MD is currently the medical director of health policy for theAmerican Academy Ophthalmology.
6 NEW RETINA MD . OCTOBER 2010
Each year retina specialists willundertake a process to demon-strate their competencies in areasof ophthalmology outside of theirspecialty. The goal of this section is
to highlight these important clinical topics. In each issue, aguest expert in a particular field of ophthalmology will pro-vide a brief summary of subtopics within a specialty. Wewould like to sincerely thank Dr. Nicholas J. Volpe for hiscontributions to this inaugural issue.
- Diana V. Do, MD
Optic Neuritis Optic neuritis is an inflammatory disease of the optic
nerve. Patients are generally younger in age and it ismore common in women. The Optic Neuritis TreatmentTrial (ONTT) showed that patients with optic neuritis who had an abnormal brain MRI scan had a higher risk of developing multiple sclerosis for the subsequent 15 years compared with those with normal brain MRIs.1,2
Thus ophthalmologists have an obligation to be able to recognize optic neuritis, order an MRI scan, and refer appropriate patients to a neurologist or neuro-ophthalmologist for steroid and/or disease-modifyingimmunomodulatory treatment. The ONTT also identifiedsignificant quality-of-life issues that persist in manypatients who otherwise have good recovery from opticneuritis, making referral important for many cases.
Ischemic Optic NeuropathyAnother disease of the optic nerve that retina special-
ists may encounter is ischemic optic neuropathy. Patientsoften present with acutely swollen optic nerves and visionloss. Physicians should be able to distinguish optic neu-ropathy from temporal arteritis, giant cell arteritis, or theidiopathic form. In idiopathic ischemic optic neuropathy,premonitory symptoms include jaw pain and headaches.Diagnostic tests include erythrocyte sedimentation rate(ESR), C-reactive protein (CRP), and platelet counts.Prompt treatment with steroids is indicated when arteriticischemic optic neuropathy is suspected. In idiopathic
cases, patients should be queried to ensure that they arenot taking PDE5 inhibitors (erectile dysfunction drugs), asthere is evidence to suggest that PDE5 inhibitors may beassociated with anterior ischemic optic neuropathy.3
Patients should be screened for history compatible withsleep apnea, another important risk factor, and allpatients with progressive disease should be evaluated foralternative diagnoses with MRI scans and neuro-oph-thalmic consultation regarding possible infiltrative orinflammatory processes. There are some early casereports regarding the use of anti-vascular endothelial growth factor agents and intravitrealsteroids for this indication, but there is no definitive evidence to support their role.
Idiopathic Intracranial Hypertension Patients with idiopathic intracranial hypertension, also
known as pseudotumor cerebri, present with swollenoptic nerves and elevated intracranial pressure. Whenbilateral disc swelling is present, suggesting elevatedintracranial pressure, it is critical to rule out mass lesionsin the brain, even in patients who are asymptomatic. Allpatients should undergo MRI scanning on an urgentbasis and blood pressure measurement to ensure thatthey do not have malignant hypertension.
The Neuro-Ophthalmology Research DiseaseInvestigator Consortium (NORDIC) is conducting an ongo-ing trial, the Idiopathic Intracranial Hypertension TreatmentTrial (IIHTT) for which enrollment continues to be underway. In this trial, patients are randomized to aggressiveweight loss or treatment with weight loss and acetozo-lamide. In addition to referring patients for enrollment inthis trial, careful monitoring of visual fields remains thestandard of care, along with encouraging weight loss.Patients with progressive vision loss should be referred forconsideration of surgical therapy either with optic nervefenestration or a cerebro spinal fluid shunting procedure.
Transient Monocular Vision LossIn most cases of true transient full field or altitudinal tran-
sient vision loss, artery-to-artery embolic disease is the most
Competencies in Neuro-ophthalmology
The Road to RecertificationSection Editor: Diana V. Do, MD
By Nicholas J. Volpe, MD

likely cause. In addition, transient monocular vision loss canbe a manifestation of temporal arteritis or giant cell arteritis.The recommended diagnostic testing is the same—ESR,CRP, and platelet counts—and patient history is also similar.It is also important to assess the acuity and associated symp-toms in patients with transient monocular vision loss. Forinstance, a series of symptoms that may be harbingers of astroke include recent episodes of convincing transientmonocular blindness and transient hemispheric symptoms,and in these cases patients should be promptly referred foremergency evaluation and treatment. Carotid studies includ-ing an echocardiogram and treatment with aspirin are stan-dard. There is increasing evidence to suggest that patientswith symptomatic significant carotid stenosis may benefitfrom surgical intervention and endarterectomy.4
Orbital Disease Orbital disease, particularly thyroid eye disease, remains
an important diagnosis to consider in all patients with dou-ble vision, particularly those with proptosis or eyelid retrac-tion. Screening for evidence of optic nerve disorder is nec-essary, and clinicians should consider that thyroid eye dis-ease is primarily an autoimmune disease, not directly relatedto thyroid dysfunction, but rather overlapping with a sharedautoimmune haplotype. Idiopathic orbital inflammatory dis-ease or orbital pseudotumor is characterized by a rapidonset of symptoms of proptosis, eyelid swelling, doublevision and the presence of pain, which is usually absent withthyroid disease. Additionally, orbital inflammatory diseaseresponds promptly to systemic steroid treatment, which hasonly mild transient benefit in thyroid disease.
Isolated Optic Atrophy Patients with isolated optic atrophy, or visual field defects,
may present with unexplained vision loss and be recognizedto have visual dysfunction that associates with a pale opticnerve. Patients with symmetric and bilateral central visualloss may suffer nutritional deficiencies, such as B12 or folatedeficiency, or suffer from a hereditary condition. In patientsfor whom visual loss is unilateral or associated with a visualfield defect that respects the vertical meridian, the diagnosisof exclusion is a compressive lesion. In fact, for all patientswith unexplained optic atrophy it is advisable to performimaging studies to rule out a tumor.
Hereditary Optic NeuropathiesHereditary optic neuropathy is a rapidly expanding area
with increasing diagnostic information resulting from theidentification of genetic markers; there are now recognizedloci of genetic defects that are associated with dominantly
inherited optic atrophy, and genetic tests are currentlyavailable to confirm these diagnoses. Hereditary optic neu-ropathy typically presents in children and adolescents withcentral vision loss and is dominantly inherited. Leberhereditary optic neuropathy (LHON) is a mitochondrial dis-order inherited through the mother's lineage, never thefather’s. It generally presents in young men with bilateral orsequential bilateral acute or subacute optic neuropathy.Commercially available genetic analysis will confirm amutation in the mitochondrial genome 90% to 95% of thetime, but unfortunately no treatment is currently available.However, clinical trials using gene therapy to treat LHONare on the horizon.
Cranial Nerve PalsiesPatients with isolated cranial nerve palsies often present
with double vision on a vasculopathic and age-relatedbasis with risk factors such as diabetes and hypertension.The differential diagnosis of vasculopathic palsy includesrecent head trauma, stroke, compressive lesion, or con-genital fourth-nerve palsy with decompensating symp-toms. Most sixth-nerve palsies are vasculopathic, but anMRI scan should be performed to exclude multiple sclero-sis or tumors in patients younger than 55 years. All patientswith third-nerve palsies associated with pupil involvement(given the possibility of intracranial vascular lesion oraneurysm) should be promptly evaluated in the ER by aneurologist or a neuro-ophthalmologist.
Cortical Vision LossFor patients who present with difficulty with their vision,
yet good overall visual acuity and ill-defined symptoms, thepossibility of some type of higher cortical visual processingdisorder should be considered. The most common is a visu-al variant of Alzheimer disease in which patients may have20/20 vision but describe difficulty with reading and recog-nizing objects; however, this is a difficult diagnosis becausethe results of the clinical exam and the patients' visual fielddefects are variable and may often appear normal. Thesepatients should be referred to a neurologist with expertisein cognitive disorders. Rapidly progressive cortical visionloss may be associated with Creutzfeldt-Jakob disease;however, this is a rare diagnosis.
Pupillary DisordersBy far, the most common cause of anisocoria is physio-
logic. For pupils with pronounced anisocoria in scotopicconditions with ptosis, the diagnosis of exclusion isHorner syndrome. Unless associated with pain or otherneurologic symptoms, Horner syndrome is not an urgent
The Road to Recertification
OCTOBER 2010 . NEW RETINA MD 7
(continued on page 9)

8 NEW RETINA MD . OCTOBER 2010
Iam excited to introduce the SurgicalPearls section of New Retina MD. This column is specifically geared tosurgical techniques that we have foundhelpful after fellowship. Although there
are many surgical tools that we learned to use duringfellowship, specific techniques have become extremely valuable.
The first installment focuses on observations that I havemade regarding surgical management since graduatingfrom fellowship. Subsequent issues will feature differentsurgeons and describe their surgical techniques. With eachsubmission, we plan to include surgical images and videosto help illustrate each technique.
- Omesh P. Gupta, MD, MBA
For the entirety of our medical and surgical training, wehave been under the supervision of attendings. Althoughwe have taken mental notes of what they have said anddone, the transition to becoming an attending oneself canbe overwhelming.
Preoperative Evaluation Surgical judgment and management begin with
the preoperative discussion. Selecting the appropriatepatient and surgical case is imperative for early suc-cess. The amount of fellows’ participation in the preop-erative discussion with patients varies among pro-grams. During my fellowship, fellows had an opportu-nity to be actively involved in preoperative decisionmaking with selected patients. Most of the cases inwhich fellows were involved, however, were plannedwithout the fellow present, simply due to the rotationschedule of the program.
As newer attendings, many of us have a tendency to
pursue surgical options sooner than more experiencedsurgeons. This is partly due to our desire to build ourpractices, but is also because we lack the years of per-sonal experience regarding the natural history of reti-nal disorders, which aid in the knowledge of when sur-gical intervention is not necessary. Maintaining a surgically conservative approach early in a career canbe a challenge, but most conditions can be followedfor weeks or months without affecting the ultimatevisual outcome.
To follow are some items that I have learned: • Know the limits of your surgical training.• Identify your strengths and weaknesses and try not
to get involved with any case for which you are notready.
• Manage patient expectations prior to surgery, pro-viding clear details of the surgical process and potentialcomplications.
• Don't be afraid to seek help from your fellowshipmentors or more senior attendings; reviewing a casewith an individual you respect can be incredibly helpful.
In the OR Operating in a new environment can be unsettling.
New nurses, techs, and equipment can easily make acase that was straightforward during fellowship muchmore complicated in a new environment. In my opinion,a physician can never overprepare for surgery days.Particularly in the early stages of one’s career, it isimportant for you to be familiar with the equipment youwill be using. It is also important to know your staff;although you may be comfortable with a particular sur-gery, if your staff is uncomfortable or unfamiliar with theprocedure the case may be much difficult to complete.Make an effort to run through each step of the surgery
The Transition From Fellow to
Attending SurgeonBy Omesh P. Gupta, MD, MBA
Surgical PearlsSection Editor: Omesh P. Gupta, MD, MBA

OCTOBER 2010 . NEW RETINA MD 9
to ensure that all the supplies and equipment are inplace for surgery day. Ask local representatives fromthe pertinent surgical manufacturing companies to bepresent for your first couple days in the operatingroom. These individuals can be incredibly helpful inensuring that your cases run smoothly, and they canalso provide valuable insight into the approaches ofother surgeons who operate at that facility.
It is also beneficial to review all cases before startinga surgery day. During fellowship, we took for grantedthat our attending would have the answer for any prob-lem. Now that we are the attendings, that onus is uponus. Open each chart and remind yourself of the detailsof each surgery. You also might want to put somethought into the surgical order based on your prefer-ences, level of difficulty, necessary equipment, or anes-thesia requirements.
Don't be afraid to ask a more senior member of yourpractice to accompany you to the OR for your first fewcases to reduce your stress level. You may find that yougain some good tips to help make surgery day proceedmore smoothly.
Preparation is Key There is a huge learning curve in the transition from
fellow to attending. This is the first time that most of uswill perform surgery by ourselves in an unfamiliar envi-ronment. Although there is nothing that can fully pre-pare us for those days in the OR, foresight can helpavoid some potential obstacles. NRMD
The Road to RecertificationSurgical Pearls
diagnosis; however, in the presence of neck or face pain,the diagnosis of exclusion is a carotid dissection, andpatients should be sent immediately to the ER with thatdiagnosis in hand. Additionally, neurologic or chestsymptoms suggesting a lung lesion are cause to sendpatients to the ER.
Most Horner syndromes, however, are idiopathic orvasculopathic and not urgent diagnoses. Horner syn-drome can be diagnosed with apraclonidine hydrochlo-ride; instillation will cause a reversal of anisocoriademonstrating denervation sensitivity. Apraclonidinehydrochloride should not be used in children.
For patients with anisocoria that worsens in photopicconditions, it is important to ensure that there is no co-existing ptosis or double vision that may suggest third-nerve palsy. If otherwise isolated, the diagnosis will mostlikely be an Adies tonic pupil, which is an idiopathic cil-iary ganglion disease and does not require further test-ing or workup.
SummaryAlthough these are certainly not all of the topics that
one would want to study in preparation for the practiceemphasis area of neuro-ophthalmology, I believe theyrepresent a good start. More information and completestudy materials can be found on the American Academyof Ophthalmology Web site at:http://one.aao.org/CE/MOC/default.aspx. NRMD
1. Beck RW, Cleary PA, Anderson MM Jr, et al. A randomized, controlled trialof corticosteroids in the treatment of acute optic neuritis. The Optic NeuritisStudy Group. N Engl J Med. 1992;326:581-588.
2. Beck RW, Gal RL, Bhatti MT, et al. Visual function more than 10 years afteroptic neuritis: experience of the Optic Neuritis Treatment Trial. Am JOphthalmol. 2004;137:77-83.
3. Rao AR, Thwaini A, Ahmed HU, Shergill IS, Minhas S. The phosphodi-esterase inhibitors and non-arteritic anterior ischaemic optic neuropathy:increased vigilance is necessary. BJU International. 2007;100:3-4.
4. Rothwell PM, Eliasziw M, Gutnikov SA, Warlow CP, Barnett HJ; CarotidEndarterectomy Trialists Collaboration. Endarterectomy for symptomaticcarotid stenosis in relation to clinical subgroups and timing of surgery.Lancet. 2004;20;363(9413):915-924.
Nicholas J. Volpe, MD formerly Professor and Adele Niessen Chair inOphthalmology at the University ofPennsylvania School of Medicine inPhiladelphia, was recently named the Chair ofOphthalmology at Northwestern UniversityFeinberg School of Medicine in Chicago. He
can be reached at 312 908 8152.
Diana V. Do, MD is an Assistant Professor of Ophthalmology at the Wilmer EyeInstitute, Johns Hopkins School of Medicine, in Baltimore. Sheis a New Retina MD Editorial Board member. Dr. Do can bereached via e-mail at [email protected].
(from page 7)
Omesh P. Gupta, MD, MBA is an Assistant Professor of Clinical Ophthalmology at TempleUniversity School of Medicine in Philadelphia. He is a NewRetina MD Board member. Dr. Gupta may be reached at 215 707 3346; or via e-mail at [email protected].
Don’t be afraid to ask a more
senior member of your practice to
accompany you to the OR for
your first few cases to
reduce your stress level.

10 NEW RETINA MD . OCTOBER 2010
Imagine a world, if you will, where dia-betic macular edema is diagnosed onlywith contact lens biomicroscopy orrecurrent exudation of a choroidal neo-vascular membrane requires repeated
fluorescein angiography before an intravit-real injection. On a routine basis, this would be akin to anepisode of the Twilight Zone. To the majority of us, opti-cal coherence tomography (OCT) has been a vital toolthroughout our residencies and fellowship training.You’ve ordered and interpreted more OCTs in your youngcareer than you have visual fields, ultrasounds, andangiograms combined.
Just as with your personal computer or smartphone,advances in technology have made OCT systems better,faster, and relatively less expensive than early generationmodels used in our training programs. This article willfocus on Fourier-domain, or spectral-domain, OCT (SD-OCT), the latest generation of commercially availableOCT units with image resolution and imaging capabilitiessuperior to earlier generation, time-domain OCT (TD-OCT) units.
Just as with any computer-based technology, yourassessment as to what unit(s) to buy for your new practiceor to upgrade in your existing multispecialty office shouldbe based on understanding the technology, your intend-ed use, ability to integrate into your existing imaging sys-tems, and cost—not just the glitzy bells and whistles.
Why Go Spectral Domain?OCT technology is based on the concepts of coher-
ence and interferometry—light properties that allow theformation of interference patterns and detection of lightechos. In a TD-OCT system, a superluminescent diodelight source is split to a reference mirror and onto theretinal surface. The resultant reflected light waves (indi-vidual A-scans) are combined with the reference signal.The reflected waves are captured as sequential interfer-ence patterns and stored on a computer.1 The result is a2-D, cross-sectional image with an axial resolution of
approximately 10 µm, 400 pixels per A-scan, and scanvelocity of 400 A-scans per second.
With SD-OCT, the mirror is replaced by a spectrome-ter and high resolution charge-coupled device camera.There is electronic, rather than mechanical, separation of the interference patterns that allows simultaneousrather than sequential analysis of all light echos. With SD-OCT images, the axial resolution is typically less than7 µm, 2,048 pixels per A-scan, and a scan velocity ofgreater than 18,000 (up to 55,000) A-scans per second.2
So with SD-OCT, images are captured faster, with higher resolution, and with reduced motion artifact. In addition, there is an incredible amount of image dataobtained at each session, allowing intricate 3-D reconstruction and better point-to-point registration forbetter reproducibility during follow-up scans. Further-more, the density of scans over a given area is greater,resulting in far fewer imaging gaps throughout the poste-rior pole, making one less likely to miss subtle retinalarchitectural changes compared to TD-OCT.
Features to EvaluateAt the time of this printing, there are six US Food and
Drug Administration-approved SD-OCT units on the USmarket, with another three units awaiting approval andavailable outside the United States. When determiningwhich will be the best fit for your practice, there are sev-eral key features to compare (Table 1).
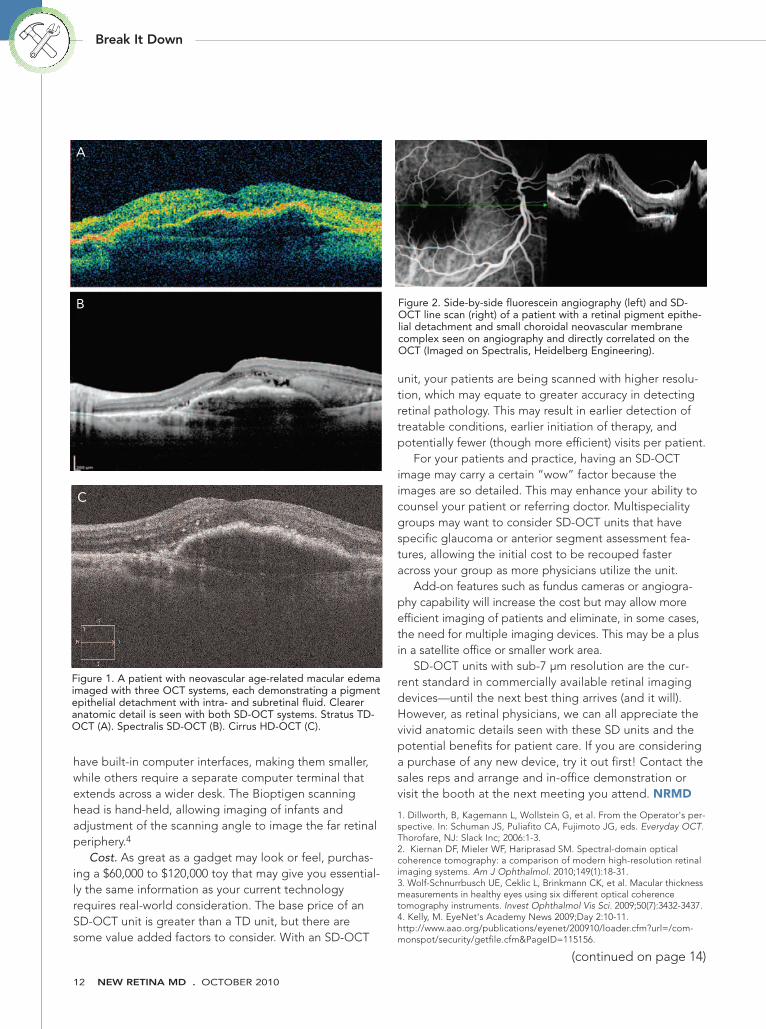
Axial resolution. Current SD-OCT units have optical axialresolutions ranging from 4 µm (HHP SDOCT, Bioptigen,Research Triangle Park, NC) to 7 µm (Spectralis, HeidelbergEngineering, Vista, CA), though the latter provides a 3.5 µm“digital” resolution. Higher resolution produces greaterscan density resulting in greater definition of retinal struc-tures and less motion artifact. When reviewing differentimages, it is helpful to turn off the automatic color functionand look at the grayscale images. Similar to a multiplemegapixel digital camera, it is difficult to find one unit thatis superior to the rest; all provide superb detail of the reti-nal layers—far superior to any TD-OCT image (Figure 1).
What Are You GettingWith SD-OCT?
Break It Down
By Prithvi Mruthyunjaya, MD
Section Editor: Prithvi Mruthyunjaya, MD

OCTOBER 2010 . NEW RETINA MD 11
Macular thickness. All units have the ability to calculatecentral retinal thickness. Numerous studies have attempt-ed to correlate thickness measurements among differentunits, but the fact remains that each unit has a unique seg-mentation algorithm that defines the inner and outer reti-nal layers differently.3 This results in a subtle (within 30 to70 µm) variation between certain units, but enough thattreatment decisions may be incorrectly altered if these vari-ations are not taken into consideration. Most have a nor-mative database to compare your patient’s scan measure-ments and will calculate change in thickness between serialvisits. The high resolution reduces image artifacts com-pared with TD units, and some units allow manual adjust-ment of the inner-outer retinal markers allowing for greateraccuracy in thickness measurements.
Ocular motion tracking. This feature allows a moreexact point-to-point registration of fundus landmarks,ensuring that scans will encompass the same retinaregion in the same eye over different scan sessions. Thepresumed advantage is that specific abnormalities can beimaged reproducibly to observe changes over time, help-ing in diagnosis or in monitoring of treatment effects.Even without this feature, the high scan resolution proba-bly will not miss most macular pathologies, and manualregistration options would allow you to reproduce scansin a particular region if needed.
Fundus image registration. The OCT unit may have atrue or pseudo-fundus camera built into the unit.Compared with TD units, which had live video feeds thatwere often very grainy images, SD units can provide acrisp view to directly compare points on the OCT with
fundus red-free, autofluoresence, angiogram, or indocya-nine green images. Some units have a scanning laserophthalmoscope or digital fundus cameras, providingdetailed images, while others use a sum voxel OCT fun-dus representation that has lower but adequate resolu-tion fundus details. With the fundus image on the samescreen, one can decide if the scan is capturing the fundusabnormality in question (Figure 2).
Software and accessibility. A user-friendly interface isimportant if your practice utilizes different staff members toobtain OCT images. I find that most units are easy to use,but not all interfaces are intuitive. All systems will have theirown viewer where you will be able to perform real-timeimage processing. These functions are fantastic but requiregood understanding of your unit’s capabilities and likelysome extra time. In a busy clinic, you may consider settingup default views. Some units, such as the Cirrus HDOCT4000 (Carl Zeiss Meditec, Dublin, CA), allow segmenta-tion of specific retinal layers (so called C-scan) that can pro-vide a topographic view in isolation or very pretty 3-D pro-jections (Figure 3) that can be rotated on screen.
If you are using electronic medical record or imagemanagement software, be sure the SD-OCT device iscompatible. Viewing prior TD-OCT images may be achallenge if you switch platforms to another company.For example, the 3D-OCT 1000 (Topcon) has a built-inStratus (Carl Zeiss Meditec) TD OCT reader. SD-OCTimages are also very large and require appropriate back-up and storage protocols.
Footprint. A practical consideration is the size andportability of the unit as it fits in your office. Some units
Break It Down
Table 1.
Model
Axial Resolution (µm)
Speed (A-scan x 1000/s)
Thickness maps
Thickness change
3-D reconstruction/
en face image views
Ocular motion tracking
Fundus image registration
Other features
HHP SDOCT
4
17-20
Yes
No
Yes
No
Yes
Hand-held,
Doppler OCT
Cirrus
5
27
Yes
Yes
Yes
No
Yes
Layer
segmen-
tation
Spectralis
7
40
Yes
Yes
Yes
Yes
Yes
FA/ICG/FAF,
wide field
imaging
OPKO SpectralOCT/SLO combo system
5
27
Yes
Yes
Yes
No
Yes
Micro-
perimetry
OPKOInstrumentation/OTI
Optovue
Adapted from Kiernan DF et al. Am J Ophthalmol 2010, and Kelly M, AAO 2009.
Topcon
Medical
Heidelberg
Engineering
Carl Zeiss
Meditec
Bioptigen
RTVue-100
5
26
Yes
Yes
Yes
No
No
Ganglion cell
and corneal
analysis
3D-OCT 1000
6
27
Yes
No
Yes
No
Yes
12 megapixel
nonmydriatic
fundus photos
12 NEW RETINA MD . OCTOBER 2010
have built-in computer interfaces, making them smaller,while others require a separate computer terminal thatextends across a wider desk. The Bioptigen scanninghead is hand-held, allowing imaging of infants andadjustment of the scanning angle to image the far retinalperiphery.4
Cost. As great as a gadget may look or feel, purchas-ing a $60,000 to $120,000 toy that may give you essential-ly the same information as your current technologyrequires real-world consideration. The base price of anSD-OCT unit is greater than a TD unit, but there aresome value added factors to consider. With an SD-OCT
unit, your patients are being scanned with higher resolu-tion, which may equate to greater accuracy in detectingretinal pathology. This may result in earlier detection oftreatable conditions, earlier initiation of therapy, andpotentially fewer (though more efficient) visits per patient.
For your patients and practice, having an SD-OCTimage may carry a certain “wow” factor because theimages are so detailed. This may enhance your ability tocounsel your patient or referring doctor. Multispecialitygroups may want to consider SD-OCT units that havespecific glaucoma or anterior segment assessment fea-tures, allowing the initial cost to be recouped fasteracross your group as more physicians utilize the unit.
Add-on features such as fundus cameras or angiogra-phy capability will increase the cost but may allow moreefficient imaging of patients and eliminate, in some cases,the need for multiple imaging devices. This may be a plusin a satellite office or smaller work area.
SD-OCT units with sub-7 µm resolution are the cur-rent standard in commercially available retinal imagingdevices—until the next best thing arrives (and it will).However, as retinal physicians, we can all appreciate thevivid anatomic details seen with these SD units and thepotential benefits for patient care. If you are consideringa purchase of any new device, try it out first! Contact thesales reps and arrange and in-office demonstration orvisit the booth at the next meeting you attend. NRMD
1. Dillworth, B, Kagemann L, Wollstein G, et al. From the Operator's per-spective. In: Schuman JS, Puliafito CA, Fujimoto JG, eds. Everyday OCT.Thorofare, NJ: Slack Inc; 2006:1-3.2. Kiernan DF, Mieler WF, Hariprasad SM. Spectral-domain opticalcoherence tomography: a comparison of modern high-resolution retinalimaging systems. Am J Ophthalmol. 2010;149(1):18-31.3. Wolf-Schnurrbusch UE, Ceklic L, Brinkmann CK, et al. Macular thicknessmeasurements in healthy eyes using six different optical coherencetomography instruments. Invest Ophthalmol Vis Sci. 2009;50(7):3432-3437.4. Kelly, M. EyeNet's Academy News 2009;Day 2:10-11.http://www.aao.org/publications/eyenet/200910/loader.cfm?url=/com-monspot/security/getfile.cfm&PageID=115156.
Figure 1. A patient with neovascular age-related macular edemaimaged with three OCT systems, each demonstrating a pigmentepithelial detachment with intra- and subretinal fluid. Cleareranatomic detail is seen with both SD-OCT systems. Stratus TD-OCT (A). Spectralis SD-OCT (B). Cirrus HD-OCT (C).
Figure 2. Side-by-side fluorescein angiography (left) and SD-OCT line scan (right) of a patient with a retinal pigment epithe-lial detachment and small choroidal neovascular membranecomplex seen on angiography and directly correlated on theOCT (Imaged on Spectralis, Heidelberg Engineering).
Break It Down
(continued on page 14)
A
B
C

Finance Your Life
OCTOBER 2010 . NEW RETINA MD 13
As young retina specialists, weare fortunate to be in a pro-fession that has great poten-tial for financial success. Toachieve such financial suc-
cess, however, it is important to take own-ership of our financial lives. With an understanding ofthe key issues and a proper advisory team in place, reti-na specialists can achieve financial freedom. In this firstof a series of articles, I have invited Gog Boonswangand Lifan Shen, experienced private wealth managersat JP Morgan Securities, to lend their insights on aseries of tasks they believe must be addressed to reachyour financial goals. Each installment of Finance YourLife will serve as an item on a comprehensive checklistof key issues for managing your financial life. This firstinstallment describes the initial step of putting an advi-sory team in place in order to manage your financiallife. With each subsequent article, we will delve deeperinto each of the subsequent key tasks that should beaddressed.
- Gene Ng, MD, MBA
SETTING UP THE OPTIMAL ADVISORY TEAM The optimal advisory team includes a private
banker, tax advisor, and trust and estate attorney.Because each role is distinct and complementary, it isimportant not only that each advisor excels in his orher discipline, but that the team works together tomake sure nothing slips through the cracks. An opti-mized team is made up of sophisticated advisors whounderstand the role of each of the other advisors, cre-ating a system of checks and balances. Although hav-ing sophisticated advisors who are able to work closelyand ask good questions of the other members of theteam is helpful, it is dangerous for one of your advisorsto formally take on another advisor’s role (ie, a taxadvisor who makes direct investments in addition toproviding tax advice).
Private Banker/Private Wealth Manager/FinancialAdvisor/ Financial Planner/Broker
A sophisticated private banker typically serves as the“quarterback” of the advisory team. In this role, thebanker works with the client to make all investmentdecisions, provide access to credit, advise on all aspectsof the surgeon’s nonmedical life, and work closely withthe tax advisor and trust and estate attorney to ensureinvestments are optimized on an after-tax basis.
Engaging a private banker can be challenging, asthere is a wide range of sophistication in this profession,making it difficult to differentiate between a sophisticat-ed advisor and a salesman. Thus, due diligence isrequired when looking for a sophisticated banker.Criteria include experience, consistency in career,schooling, professional designations, and highvolume/high profile clientele.
Tax Advisor/Accountant/Business ManagerThe tax advisor’s primary role is to provide tax advice,
work with the banker to optimize investments on anafter-tax basis, and file tax returns. Similar to the privatebanker role, there is a wide range in levels of sophistica-tion. Because it is important for the tax advisor to workclosely with the banker, many times bankers will haverecommendations for top tax advisors with whom theywork, and likewise, tax advisors are often able to recom-mend top bankers. Because there are fewer professionaldesignations, requiring a CPA is a good starting pointwhen looking to engage a tax advisor. More sophisticat-ed tax advisors may advise on corporate structuring andother tax strategies and can offer insight regarding theintricacies of running a private office.
Trust and Estate AttorneyThe trust and estate attorney’s primary role is to draft
the necessary documents to optimize a personal estateand work with the banker to implement the desired gen-erational planning strategy. This includes creating wills,
Positioning Yourself forFinancial Success
By Gog Boonswang, CFA; and Lifan Shen, CFA
Section Editor: Eugene W. Ng, MD, MBA

14 NEW RETINA MD . OCTOBER 2010
Prithvi Mruthyunjaya, MD, is an Assistant Professor of Ophthalmology, VitreoretinalSurgery, and Ocular Oncology at Duke Eye Center in Durham,NC, and is a New Retina MD Editorial Board member. Dr.Mruthyunjaya has no financial interest or conflict of interest withthe imaging technologies discussed. He performs non-spon-sored clinical research with the Spectralis, Cirrus, Stratus andBioptigen imaging systems. He can be reached via e-mail [email protected].
Figure 3. 3-D representations of the lesion in Figure 1 usingsoftware reformatting of SD-OCT images. Spectralis providesan underlay of either a sum voxel projection retinal image orangiography/ICG image (A). Cirrus shows colorization of thevarious retinal layers (B).
Acknowledgements: Michael P. Kelly, Duke Eye Imaging, Durham, NC, and GregoryC. Hoffmeyer, Carl Zeiss Meditec, Dublin, CA, assisted in thepreparation of this manuscript.
Break It Down Finance Your Life
philanthropic entities, and trusts to optimize genera-tional planning. A sophisticated banker should be ableto walk you through the key issues of trust and estateplanning and lead meetings with the attorney to ensurekey goals are properly planned for. This ensures theinvestment plan is optimized with regard to the trustand estate plan and also saves legal fees. Money canbe left to the next generation, a philanthropic entity, orthe Internal Revenue Service; proper trust and estateplanning will ensure this is optimized based on thewishes of the prior generation.
Compiling a world-class team of advisors who worktogether is a key element of achieving financial suc-cess. Future installments of this column will addressadditional key issues including trust and estate plan-ning; insurance and philanthropy; optimizing your per-sonal balance sheet; understanding your investments;retirement planning; and preparing for your children’seducation. NRMD
Gog Boonswang, CFA is a Managing Director with JP Morgan Securities and hasbeen advising high-net-worth families and foundations for 10years. Prior to joining JP Morgan, Boonswang was a FoundingPrincipal of Summit Rock Advisors, a multifamily office thatadvises families with greater than $100 million in investableassets. Prior to joining Summit Rock, Boonswang advisedwealthy families working in the Private Wealth ManagementGroups at Goldman, Sachs & Co., and Morgan Stanley.Boonswang holds an MBA from Harvard Business School anda BA from Princeton University. He can be contacted at 212272 6702; or via e-mail at [email protected].
Lifan Shen, CFA is an Investment Professional with JP Morgan Securities andhas been advising high-net-worth families and foundations for10 years. Prior to joining JP Morgan, Shen was a Vice Presidentat Goldman, Sachs & Co., where he spent 6 years activelymanaging fixed-income and equity portfolios in the PrivateWealth Management Group. In addition to working with exter-nal clients, Shen was responsible for advising more than 50 ofthe most senior Goldman Partner Managing Directors on theirpersonal investments. At the time of his departure, Shen andhis team managed a business with $8 billion of client assets.Shen holds an MBA from the Wharton School of Business andan BA from Dartmouth College. He can be contacted at 212 272 1099; or via e-mail at [email protected].
Eugene W. Ng, MD, MBA is a vitreoretinal surgeon at the Retina Institute of Hawaii. Dr. Ng has no financial interests in the product, or companiesmentioned in this article. Dr. Ng is a New Retina MD EditorialBoard member. He may be reached at 808 955 0255; or via e-mail at [email protected].
(from page 13)(from page 12)
A
B

ad_temp 8/2/10 1:59 PM Page 83
