sustaining quality of healthcare: institutionalization of...
TRANSCRIPT

Center for Human Services • 7200 Wisconsin Avenue, Suite 600 • Bethesda, MD 20814-4811 • USA • www.qaproject.org
Sustaining Quality of Healthcare:Institutionalization of Quality
Assurance
September 2002
Q A M O N O G R A P H
Q U A L I T Y
A S S U R A N C E
P R O J E C T

The Quality Assurance (QA) Project is funded by the U.S. Agency for International Development(USAID), under Contract Number HRN-C-00-96-90013. The QA Project serves countries eligible forUSAID assistance, USAID Missions and Bureaus, and other agencies and nongovernmental organiza-tions that cooperate with USAID. The QA Project team consists of prime contractor Center for HumanServices; Joint Commission Resources, Inc.; and Johns Hopkins University (including the School ofHygiene and Public Health [JHSPH], the Center for Communication Programs [CCP], and the JohnsHopkins Program for International Education in Reproductive Health [JHPIEGO]). The QA Projectprovides comprehensive, leading-edge technical expertise in the design, management, and implemen-tation of quality assurance programs in developing countries. Center for Human Services, the nonprofitaffiliate of University Research Co., LLC, provides technical assistance and research for the design,management, improvement, and monitoring of health systems and service delivery in over 30 countries.

Sustaining Qualityof Healthcare:Institutionalizationof Quality Assurance
Lynne Miller Franco, Diana R. Silimperi,
Tisna Veldhuyzen van Zanten, Catherine MacAulay,
Karen Askov, Bruno Bouchet, and Lani Marquez
September 2002

iv ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ v
Table of Contents
List of Figures, Boxes, and Tables ........................................................................... v
List of Abbreviations ................................................................................................ vi
Acknowledgements .................................................................................................. vi
Executive Summary ................................................................................................. 1
1 Introduction to Institutionalization ................................................................... 5
1.1 What Is Institutionalization of Quality Assurance? ................................. 5
1.2 Objectives and Organization of the Monograph ..................................... 6
2 Principles of Quality Assurance......................................................................... 9
2.1 What Is Quality of Care? ............................................................................ 9
2.2 Principles of QA for Application in Developing Countries ..................... 10
2.3 The Core Activities of Quality Assurance: The QA Triangle ................... 10
3 A Conceptual Model: What It Takes to Institutionalize
Quality Assurance ............................................................................................. 13
3.1 Overview of the Model ............................................................................. 13
3.2 The Internal Enabling Environment ........................................................ 14
3.2.1 Organizational Policies and Policy Implementation ................ 14
3.2.2 Leadership ................................................................................... 15
3.2.3 Core Values .................................................................................. 16
3.2.4 Resources .................................................................................... 17
3.3 Organizing for Quality: Developing a Structure to
Support QA Implementation ................................................................... 18
3.4 Support Functions ................................................................................... 19
3.4.1 Capacity Building ........................................................................ 20
3.4.2 Information and Communication .............................................. 20
3.4.3 Rewarding Quality Work ............................................................. 22
3.5 Conclusion ................................................................................................ 23

vi ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
4 Understanding the Process of Institutionalization: A Road Map ................. 25
4.1 QA Institutionalization as a Process ...................................................... 25
4.2 The Phases of Institutionalization .......................................................... 25
4.3 Pre-Awareness .......................................................................................... 26
4.4 The Awareness Phase ............................................................................. 26
4.5 The Experiential Phase ............................................................................ 27
4.6 The Expansion Phase .............................................................................. 27
4.7 The Consolidation Phase ........................................................................ 27
4.8 Maturity: Sustained Quality of Care and a Culture of Quality ............. 28
4.9 Conclusion ................................................................................................ 28
5 Moving towards Institutionalization: One Element at a Time ....................... 29
5.1 Policy ......................................................................................................... 29
5.2 Leadership ................................................................................................ 34
5.3 Core Values ............................................................................................... 35
5.4 Resources for QA ...................................................................................... 37
5.5 Organizing for Quality: Creating a Structure for
QA Implementation .................................................................................. 39
5.6 Capacity Building ..................................................................................... 41
5.7 Information and Communication ........................................................... 43
5.8 Rewarding Quality .................................................................................... 44
5.9 Bringing the Elements into Maturity ...................................................... 46
6 Epilogue ...................................................................................................... 49
References .............................................................................................................. 51

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ vii
Figures
Figure 2.1 Dimensions of Quality ................................................ 9
Figure 2.2 Quality Assurance Triangle ....................................... 11
Figure 2.3 Four Steps to Quality Improvement ......................... 12
Figure 3.1 Essential Elements for the
Institutionalization of QA .......................................... 13
Figure 3.2 Institutionalization of Quality Assurance ................ 14
Figure 4.1 The Phases of Institutionalizing
Quality Assurance ..................................................... 25
Boxes
Box 3.1 Quality Policy in Mexico ............................................ 15
Box 3.2 Key Leadership Responsibilities for
Successful QA Implementation ............................... 16
Box 3.3 A Change in Values in Russia .................................. 16
Box 3.4 A Change in Staff Attitudes in South Africa ............ 17
Box 3.5 Core Values that QA Project Experience Has
Shown to Be Critical for Institutionalizing QA ......... 18
Box 3.6 Evolution of the QA Oversight Structure
in Malawi ................................................................... 19
Box 3.7 Key Roles and Responsibilities
for a QA Structure ..................................................... 20
Box 3.8 Capacity Building in Tahoua, Niger ......................... 21
Box 3.9 The Three Types of QA Capacity Building ............... 21
Box 3.10 Sharing Data on Compliance with
Standards in Ecuador ............................................... 22
Box 3.11 Facilitating Information Flow and
Sharing of Lessons in Chile ..................................... 22
Box 3.12 Rewarding High Levels of Quality
and Coverage in Ecuador ......................................... 23
Box 5.1 Evolution of Quality Policies in Malaysia ................ 32
Box 5.2 Top-Level Leadership Support for QA in Chile ........ 34
Box 5.3 Corporate Culture Building in Malaysia .................. 36
Box 5.4 Sustaining the Funding Base for
QA Activities in Chile ................................................. 38
Box 5.5 Structures to Support and Implement QA
in Malaysia ................................................................ 39
List of Figures, Boxes, and Tables
Box 5.6 The Changing Challenges of
Capacity Building in Zambia .................................... 41
Box 5.7 Promoting the National Crusade for
Health Quality in Mexico .......................................... 43
Box 5.8 Rewarding Quality in Malaysia ................................. 45
Tables
Table 4.1 Institutionalization Phase Characteristics,
Strategies, and Indications of Readiness
to Progress ................................................................. 26
Table 5.1 Evolution of QA Essential Elements through
the Phases of Institutionalization ........................... 30
Table 5.2 Illustrative Example of an Organization’s
QA Institutionalization Status .................................. 32
Table 5.3 Possible Activities to Develop the
Essential Element Policy and
Move to the Next Phase/State ................................ 33
Table 5.4 Possible Activities to Develop the
Essential Element Leadership and
Move to the Next Phase/State ................................ 34
Table 5.5 Possible Activities to Develop the
Essential Element Core Values and
Move to the Next Phase/State ................................ 37
Table 5.6 Possible Activities to Develop the
Essential Element Resources for QA
and Move to the Next Phase/State ......................... 38
Table 5.7 Possible Activities to Develop the
Essential Element QA Structure and
Move to the Next Phase/State ................................ 40
Table 5.8 Possible Activities to Develop the
Essential Element Capacity Building and
Move to the Next Phase/State ................................ 42
Table 5.9 Possible Activities to Develop the
Essential Element Information and
Communication and Move to the
Next Phase/State ..................................................... 44
Table 5.10 Possible Activities to Develop the
Essential Element Rewarding Quality and
Move to the Next Phase/State ................................ 45
Table 5.11 Analysis of Each Essential Element in
Zambia’s Quality Assurance Program ..................... 47

viii ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
List of Abbreviations
CBOH Central Board of Health
COHSASA Council for Health ServiceAccreditation of Southern Africa
MOH Ministry of Health
NGO Nongovernmental organization
QA Quality assurance
QD Defining quality
QI Improving quality
QM Measuring quality
USAID United States Agency forInternational Development
Acknowledgements
This monograph has benefited tremendously from thecollective work and thinking of the staff of the QualityAssurance Project, health workers and managers in manydeveloping countries, and James Heiby of the U.S. Agencyfor International Development. The authors want to recog-nize their contributions, without which this monographcould not have been written. We also want to express ourappreciation to Beth Goodrich for her skillful editing of thefinal manuscript.
Recommended citation: Franco, L.M., D.R. Silimperi, T.Veldhuyzen van Zanten, C. MacAulay, K. Askov, B. Bouchet,and L. Marquez. 2002. Sustaining Quality of Healthcare:Institutionalization of Quality Assurance. QA MonographSeries 2(1). Bethesda, MD: Published for the U.S. Agencyfor International Development (USAID) by the QualityAssurance Project.

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 1
I
Executive Summary
MPROVING quality has become a unifying theme acrosshealth programs and countries. Awareness of theimportance of improving healthcare quality is seen in
the rapid spread of evidence-based guidelines, growingattention to patient safety and reducing medical errors,and attempts to reduce waste and inefficiency, to ensurethat scare resources for healthcare are used to derive theirfull impact.
Around the world, impressive efforts are underway inpublic and private organizations to improve the quality ofhealthcare, based on a systematic approach to ensuringthat the details of healthcare are done right—an approachcalled quality assurance. The tools of quality assurance(QA) and quality management, born in manufacturing,have been successfully applied in healthcare in bothdeveloped and less developed countries, and there isgrowing acceptance that QA can improve program andhealth worker performance.
In developing country health systems, the need for higherquality care and health services that are responsive toclients is acute. QA activities have been successfully estab-lished in many developing country settings, but often falterin scaling up or sustaining their achievements. As morenational ministries and other health organizations gainexperience in applying QA approaches, demand has grownfor guidance on the elements and processes that sustainthe quality of healthcare.
The Objectives of This Monograph
This monograph presents a conceptual framework to helphealthcare systems and organizations analyze, plan, build,and sustain efforts to produce quality healthcare. Theframework synthesizes more than ten years of QA Projectexperience assisting in the design and implementationof QA activities and programs in over 25 countries. Thatexperience has shown that the key institutionalizationquestion is often not so much a technical one—how to“do” QA activities—but rather, how to establish a culture ofquality within the organization and make QA an integral,sustainable part of the health system.
As with any kind of organizational change, the road toinstitutionalizing QA can be long and complex. Thismonograph was written to provide practical information to
Ministries of Health and other health organizations in theirquest for sustainable quality of care. It both describes thecomponents necessary to inculcate a culture of qualityand provides practical information on how to facilitate theprocess necessary to reach this goal. A framework of eightessential elements and a phased process for institutional-ization of QA outline the critical aspects and a road mapfor creating a lasting program to improve the quality ofhealthcare. The institutionalization framework drawsheavily on management literature and organizationalchange models, as well as QA program experiences indiverse countries.
The Core Activities of Quality Assurance
At the heart of any effort to institutionalize the delivery ofquality healthcare are three core QA activities: definingquality, measuring quality, and improving quality. Thesecore activities are developed, scaled up, and made integralparts of an organization’s functioning through institutional-ization. Defining quality means developing expectationsor standards of quality, as well as designing systems toproduce quality care. Measuring quality consists of docu-menting the current level of performance or compliancewith expected standards, including patient satisfaction.Improving quality is the application of quality improvementmethods and tools to close the gap between current andexpected levels of quality by understanding and address-ing system deficiencies (as well as enhancing strengths) inorder to improve healthcare processes. These three sets ofactivities work synergistically to ensure quality care as anoutcome of the system. Together they encompass the rangeof mutually supportive QA methodologies and techniques.No core activity alone is sufficient toimprove and maintain quality; it is the interaction andsynergy of all three that sustains high quality healthcare.
A Conceptual Model of QA Institutionalization
Many factors affect a health organization’s ability toinstitutionalize QA and a culture of quality, but we haveidentified eight elements as essential for implementingand sustaining the core QA activities. The first four ele-ments constitute the internal environment conducive toinitiating, expanding, and sustaining QA within the organi-

2 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
zation. Such an enabling environment is comprised of(a) policies that support, guide, and reinforce QA;(b) leadership that sets priorities, promotes learning, andcares about its staff; (c) core organizational values thatemphasize respect, quality, and continued improvement;and (d) adequate resources allocated for the implementa-tion of QA activities. Organizing for quality refers to themapping out of responsibilities and accountability for QAin the organization, including oversight, coordination, andimplementation of QA activities. Three critical supportfunctions sustain implementation of QA and improvedquality of care: (a) capacity building in QA, such as train-ing, supervision, and coaching for healthcare providersand managers; (b) information and communication forthe purposes of sharing, learning, and advocating forquality; and (c) rewarding and recognizing individual andteam efforts to improve quality. Each of these elements isdescribed in depth in this monograph, and the descriptionsare amplified by actual examples from developingcountries.
QA Institutionalization as a Process
While the end goal is to have each of the eight essentialelements fully in place, in reality, the institutionalization ofQA is a process through which an organization continu-
Essential Elements for the
Institutionalization of QA
Internal enablingenvironment:
Policy
Leadership
Core values
Resources
Organizing for quality:
Structure
Support functions:
Capacity building
Information and communication
Rewarding quality
ously moves until QA is fully integrated into its structureand functioning. This process may be thought of as onewhere the organization progresses from having no formalor deliberate QA efforts, to initial awareness, to experimen-tation with QA activities, to expansion, and then consolida-tion of these efforts, until finally reaching a state of fullydeveloped and institutionalized QA activities. At the stateof QA maturity, QA is an integral part of day-to-day opera-tions at all levels; and organizational values, leadership,and policies reinforce a culture of quality.
The pre-existing situation—before an organization beginsto implement any formalized or deliberate QA efforts—ischaracterized by attempts to improve quality that are spo-radic, individual, and informal, rather than part of a deliber-ate, formal QA intervention. The awareness phase is thefirst step on the road to institutionalizing QA; it is charac-terized by individuals (especially organizational leaders)becoming conscious of the need to improve quality of careand of the possibility of doing something deliberate andsystematic about it. The experiential phase is characterizedby the organization starting to implement QA on a smallscale, trying out various QA approaches to learn from theexperience, and developing evidence (documented re-sults) showing that QA leads to improvements in the qual-ity of care. At the end of this phase, sufficient momentumexists for an organization to move into the expansionphase, when there is an increase in scope of QA activities.
The expansion phase is not just a scaling up of QA activi-ties, but also a signal of the strategic expansion of QAimplementation, based on knowledge and experiencesgained in previous phases. This expansion may be geo-graphic, but could also relate to the types of QA activities,the range of facility types or departments involved, or thetypes of health problems being addressed. As expansionstrategies are undertaken, they can precipitate or foster theneed for “taking stock” of QA activities, ushering in a periodof review, refinement, balance, and coordination. Duringconsolidation, existing QA activities and programs aresimultaneously strengthened and anchored into standardorganizational operations, while at the same time beingfortified by addressing lagging or missing activities.
Dividing the institutionalization process into phases re-flects the fact that there is a progression of organizationalcapacity and QA ability that must be developed to sustainthe quality of healthcare. Each phase has specific organiza-tional characteristics and a range of strategies and activi-ties that organizations may use to foster progress to thenext phase. Although it is tempting to assume that progress
QA Project 2000
Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 3
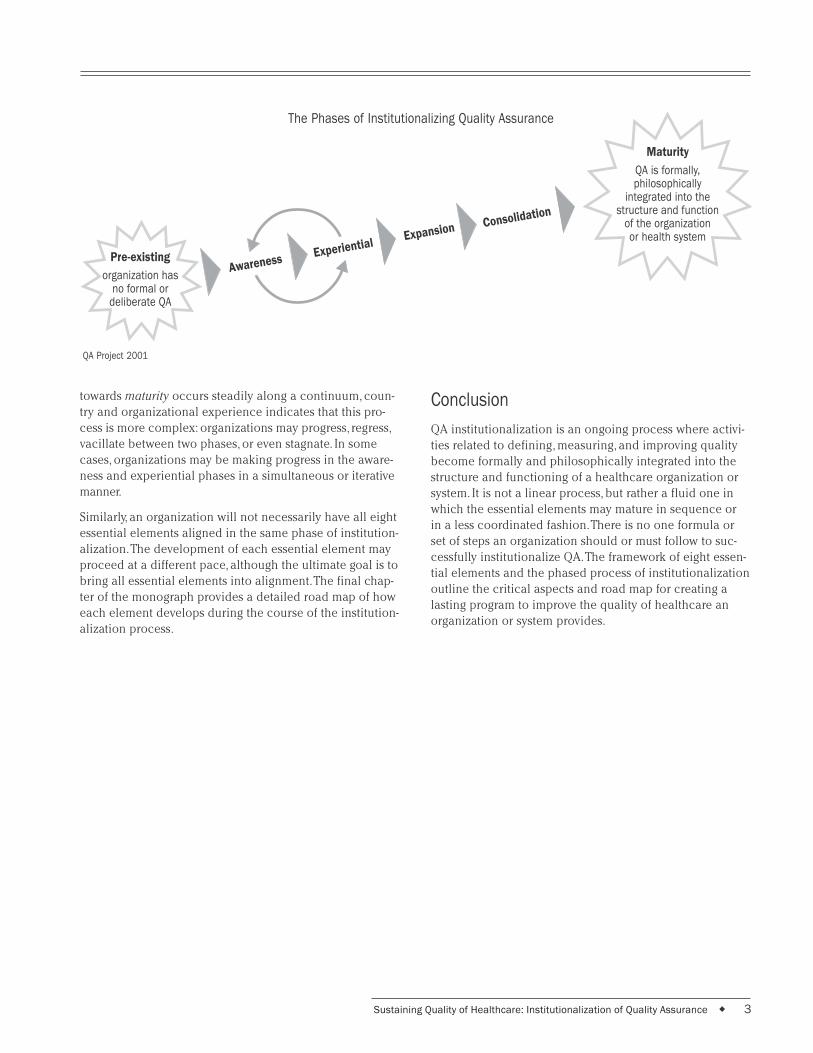
towards maturity occurs steadily along a continuum, coun-try and organizational experience indicates that this pro-cess is more complex: organizations may progress, regress,vacillate between two phases, or even stagnate. In somecases, organizations may be making progress in the aware-ness and experiential phases in a simultaneous or iterativemanner.
Similarly, an organization will not necessarily have all eightessential elements aligned in the same phase of institution-alization. The development of each essential element mayproceed at a different pace, although the ultimate goal is tobring all essential elements into alignment. The final chap-ter of the monograph provides a detailed road map of howeach element develops during the course of the institution-alization process.
Conclusion
QA institutionalization is an ongoing process where activi-ties related to defining, measuring, and improving qualitybecome formally and philosophically integrated into thestructure and functioning of a healthcare organization orsystem. It is not a linear process, but rather a fluid one inwhich the essential elements may mature in sequence orin a less coordinated fashion. There is no one formula orset of steps an organization should or must follow to suc-cessfully institutionalize QA. The framework of eight essen-tial elements and the phased process of institutionalizationoutline the critical aspects and road map for creating alasting program to improve the quality of healthcare anorganization or system provides.
The Phases of Institutionalizing Quality Assurance
Pre-existing
organization hasno formal or
deliberate QA
Expansion Consolidation
Experiential
Maturity
QA is formally,philosophically
integrated into thestructure and function
of the organizationor health system
QA Project 2001
Awareness

4 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 5
Introduction toInstitutionalization
EALTH systems worldwide are recognizing the needto improve quality. Such systems are increasinglyadopting evidence-based guidelines, giving atten-
tion to reducing medical errors, and safeguarding patientsafety. Concern with quality is also expressed in effortsto reduce waste and inefficiency, to ensure that scare re-sources for healthcare are used to derive their full impact.
Why is quality of healthcare important?
Simply stated, healthcare organizations can’t afford not tobe concerned with quality and efficiency. Quality of care isnot a luxury that only wealthy countries can afford; it is animperative for healthcare organizations worldwide. Com-plex health problems that know no national boundaries,such as HIV/AIDS and antibiotic-resistant tuberculosis,demand careful attention to well-designed processes ofcare, based on clinical evidence of effectiveness. The verylimited resources available for publicly funded healthservices in many low-income countries demand that thoseresources be channeled into effective processes of careand that wasteful or ineffective practices be eliminated.
Impressive efforts are underway to improve the quality ofhealthcare being offered to people around the world,based on a systematic approach to ensuring that thedetails of healthcare are done right––an approach calledquality assurance. While the principles and methods ofquality assurance are widely embraced, we know thatre-orienting and reorganizing entire healthcare systems sothat they can consistently offer quality care to all clientsremains a challenge for many countries, especially in thedeveloping world. Quality assurance (QA) activities havebeen successfully established in lower and middle-incomecountries, but often face significant hurdles in scaling upor sustaining their achievements. As more countries gainexperience in applying the methodologies that lead toquality healthcare, demand has grown for guidance on thetotality of the elements and inputs needed to sustain QA.
This monograph presents both a conceptual frameworkand a road map to help organizations create the capacityto plan, build, and sustain efforts to produce qualityhealthcare. We use the term framework to refer to (a) theessential elements an organization must have to institution-alize QA and (b) the phases an organization must passthrough to reach mature institutionalization. The frame-
H1
work incorporates more than ten years of QA Project expe-rience assisting in the design and implementation of QA inover 25 developing country health systems. Other publica-tions by the QA Project provide more general overviews ofquality assurance in healthcare and technical guides tomajor QA interventions (Massoud et al. 2001; BouchetUndated; Rooney and van Ostenberg 1999; Ashton 2001a).Most QA Project publications are available from thewebsite and mailing address on the cover.
1.1 What Is Institutionalization ofQuality Assurance?
The QA Project defines quality assurance as all activitiesthat contribute to defining, designing, assessing, monitor-ing, and improving the quality of healthcare. Whileadequate drug distribution, financing, human resourcesplanning and allocation, and technical and professionaltraining systems contribute to and are necessary for qual-ity care, quality assurance ensures that all processes workeffectively and synchronously to achieve qualityhealthcare.
Our understanding of QA and its use to improve the qual-ity of healthcare in developing countries has grown sub-stantially over the last ten years. One lesson was learningthat having the capacity to carry out technical qualityassurance activities does not ensure that QA is institution-alized within an organization or that QA functions aresustained over the long term. The critical question now isnot so much a technical one, how to “do” QA activities, butrather how to establish and maintain QA as an integral,sustainable part of a health system or organization, woveninto the fabric of daily activities and routine. The process ofachieving this state is what we term “institutionalization.”
Institutionalization is the process through which a set ofactivities, structures, and values becomes an integral andsustainable part of an organization. Institutionalizationmeans that people know what needs to happen to providequality care, they have the skills to make it happen, andthey are committed to making it happen over time withinthe available resources. This notion encompasses abroader set of dimensions than financial sustainabilityalone.

6 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
QA institutionalization can occur at any organizationallevel—individual healthcare facilities, health networks,intermediate health system structures (such as district orregional health units), national level health systems, orMinistries of Health. When QA is institutionalized into thestructure and functioning of a health system or organiza-tion, QA activities are consistently implemented and sup-ported by an organizational culture1 of quality, as reflectedin organizational values and policies that advocate andsupport quality care.
Quality assurance, as described in this document, is notviewed as a separate vertical program, working indepen-dently from other programs in the organization. The imple-mentation of quality assurance activities does not takeplace in a vacuum, nor should its institutionalization beviewed in isolation. Rather, the goal of QA is to be inte-grated into all programs and activities. Sustaining QA re-quires an environment that enables the initiation, growth,and continuity of QA activities. For this reason, the mono-graph addresses the “enabling” environment internal to theorganization necessary to sustain QA. We also examinepotential opportunities to capitalize on factors or condi-tions in the organization’s environment that might facilitatethe organization’s ability to produce quality healthcareservices.
While quality assurance efforts interact with the largerexternal environment (health sector, as well as other sec-tors that affect health, such as private industry and publicschools), it is beyond the purview of this monograph todiscuss these influences in depth. However, we do pointout opportunities to examine more closely the impact ofthe external environment, such as health sector reforminitiatives in decentralization, financing reform, and re-engineering.2
As with any kind of organizational change, the road toinstitutionalizing QA can be long and complex. Achievingsustained quality healthcare requires organizationalchange to infuse the organization with a culture of quality.This monograph presents a framework of the essentialelements and process necessary to reach the goal of QAbecoming an integral, sustainable part of a healthcareorganization. It also provides practical information on howto facilitate the process. We draw heavily on managementliterature and organizational change models, as well as QAprogram experiences in diverse countries.
1.2 Objectives and Organization of theMonograph
This monograph was written for people who are involvedin the design or improvement of the quality of care in theirorganization or wish to be champions for the introductionof QA into their organization. The framework is valid fororganizations ranging from individual healthcare facilitiesto national Ministries of Health. The monograph’s contentand organization were designed to stimulate reflection andprovide guidance on how best to plan, attain, and maintainquality healthcare.
The monograph has three objectives:
Increase awareness and/or sensitize key stakehold-ers on what it takes to introduce and sustain qualityassurance: The monograph provides information for lead-ers, key decision makers, healthcare practitioners, andother stakeholders about what is involved in implementingand sustaining QA, both the important elements necessaryto sustain QA and strategies for advancing the institutional-ization process. A critical message is that the institutional-ization of QA is a multi-factoral and continual process thatrequires sustained commitment from the leadership. Suchcommitment is worthwhile, as QA has been demonstratedto bring about lasting positive changes in the performanceof healthcare providers, the satisfaction of users, and mostimportantly, the quality of healthcare.
Guide self-assessment of the status of institutional-ization of quality assurance in one’s organization:The monograph can also be used as a guide for assessingthe overall status or to monitor the progress of an organiza-tion with regard to institutionalizing QA. In addition, thedetailed description of the phases of development for eachessential element in the framework can be used to identifywhich elements may need further support in the organiza-tion. The monograph also contains practical examples ofspecific activities and strategies that might be of use dur-ing each phase of institutionalization and to advance eachessential element along the road to maturity.
Facilitate institutionalization of quality assurance inan organization: The discussions of the process of institu-tionalization provide a variety of options an organizationcan consider as it moves through the various phases ofinstitutionalization. While they are not meant to be pre-
1 Organizational culture can be defined as the shared and behavioral expectations that characterize a corporate (or organizational) identity(Grindle 1997).
2 In collaboration with the Pan American Health Organization (PAHO), the QA Project is developing a framework describing the interfacebetween quality assurance and health sector reform. Publication is planned for fall 2002.

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 7
scriptive, these discussions provide guidance on majorsteps and indications of progress that have proven helpfulin developing strong and sustained QA.
The structure of the monograph parallels these objectives.To provide a common background, Section 2 discusses theprinciples and activities that comprise QA efforts and thatlead to improvements in the quality of healthcare. Section3 presents the institutionalization framework, consisting ofeight essential elements that address the internal enablingenvironment, organizing for quality, and the support func-
tions needed to sustain QA. This framework depicts whatthese elements look like when QA is institutionalized.Section 4 addresses the process of institutionalizing QA. Itdescribes the phases an organization passes through onthe road to establishing QA as an integral, sustainable partof the organization. Section 5 describes how each essentialelement of QA institutionalization moves through thesephases. This section also illustrates how one can use thisinformation to plan or improve progress toward institution-alizing QA in one’s own organization.

8 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 9
Principles ofQuality Assurance
2.1 What Is Quality of Care?
The purpose of all quality assurance efforts is to improveand sustain the quality of healthcare. Quality healthcare isthus the ultimate goal of institutionalized QA activities.There are many different definitions for the term “quality”in the context of healthcare:
“…Proper performance (according to standards) ofinterventions that are known to be safe, that are affordableto the society in question, and that have the ability toproduce an impact on mortality, morbidity, disability, andmalnutrition” (Roemer and Montoya-Aguilar 1988).
“The quality of technical care consists in the application ofmedical science and technology in a way that maximizesits benefits to health without correspondingly increasing itsrisks. The degree of quality is, therefore, the extent to whichthe care provided is expected to achieve the most favorablebalance of risks and benefits” (Donabedian 1980).
“Quality is doing the right thing, right, the first time, anddoing it better the next time, with the resource constraintsand to the satisfaction of the community” (Ministry ofHealth and Population of Malawi 1997).
Quality is multi-dimensional, so the QA Project has identi-fied nine dimensions of quality (Figure 2.1) that are impor-tant to a healthcare delivery system’s various internal andexternal stakeholders: individual clients, communities,providers, managers, and payers. Different stakeholdersconsider those dimensions of diverse importance.
Technical performance, one of the more commonly recog-nized dimensions of quality, refers to the degree to whichtasks carried out by health workers and facilities accordwith standards or meet technical expectations.
Access to services reflects a lack of geographic,economic, social, organizational, or linguistic barriers toservices.
Effectiveness of care is the degree to which desired resultsor outcomes are achieved, whereas efficiencyof service delivery relates to the use of resources toproduce those services.
Interpersonal relations refers to effective listeningand communication between provider and client; it isbased on the development of trust, respect, confidentiality,and responsiveness to client concerns.
2
Continuity of services refers to the delivery of careby the same healthcare provider throughout the courseof care (when feasible and appropriate), as well as timelyreferral and communication between providers whenmultiple providers are necessary.
Safety, the degree to which the risks of injury, infection,or other harmful side effects are minimized, is a criticaldimension of quality care and is receiving increasedattention due to the HIV/AIDS epidemic.
The physical infrastructure and comfort dimension is some-times called “amenities”; it includes a facility’s physicalappearance and cleanliness, and the comfort and privacy itaffords clients.
Choice of services refers to client choice of provider, treat-ment, or insurance plan, as appropriate and feasible. Inher-ent in this dimension is client access to information thatallows the client to make an informed choice.
Quality of care refers to the degree to which these ninedimensions of quality are present in the healthcare deliv-ered to a client.
QA Project 1999
Figure 2.1 Dimensions of Quality
Technical performance
Access to services
Effectiveness of care
Efficiency of service delivery
Interpersonal relations
Continuity of services
Safety
Physical infrastructure and comfort
Choice of services

10 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
2.2 Principles of QA for Application inDeveloping Countries
Much of the approach to quality assurance and its institu-tionalization presented in this monograph is built on theteachings and principles of established leaders in the fieldof healthcare quality (Deming 1982; Juran 1988;Donabedian 1980; Berwick 1995; Berwick et al. 1992; Lan-gley et al. 1996). The QA Project has adapted the methods,approaches, and strategies of these leaders for use byhealthcare systems in developing countries. The project’swork includes both traditional QA methodology (e.g.,accreditation, regulation, and standards) as well as newermethods, such as continuous quality improvement.
Our decade of work with hundreds of QA implementationefforts has brought to light a common set of principles that,despite variations among QA programs, lay the foundationfor the institutionalization of QA in any health organizationor system. These principles are the importance of clientperspectives and needs, analyzing systems and processes,the use of data for decision making, and teamwork to solveproblems. These four principles are interrelated and can bedescribed as follows:
Client focus: QA stresses the fact that health services existto meet the health needs of the clients who use them. Byfocusing on serving the needs of clients, healthcare provid-ers and others involved in the delivery of healthcare per-form better. Client focus means caring for the entire personrather than simply addressing an ailment; it means helpingclients not only directly in seeing that they receive thetreatment they should, but also in greeting them with re-spect, helping them find the room or person they need,reducing waiting times, handling their paperwork properly,and numerous other actions that may not be part ofsomeone’s job description but should be part of everyone’sresponsibility.
The principle of client focus distinguishes between “exter-nal” and “internal” clients. The former are generally thepopulation served, including patients, patients’ caretakers,their families, their communities, and even their society. An“internal client” is a particular person’s colleague who mayneed assistance from the person in order to perform a jobfunction. As an example, consider a nurse who needs to beable to access files in order to treat patients. He/she be-comes an internal client to the file clerk when accessing afile. “Focusing on the client” directs our attention to servingclients—both internal and external. A client focus requires
knowing who the clients are while understanding andtrying to meet their needs and expectations.
Understanding work as processes and systems: QArecognizes that unclear, redundant, or incomplete systemsor processes may cause problems in the delivery of qualityhealthcare. Instead of blaming the people working in thesesystems for poor performance, QA activities involve themin the prevention, detection, and resolution of problemswithin processes or systems, in order to improve the qualityof care.
Testing changes and emphasizing the use of data: QAemphasizes the need to improve processes by understand-ing how they function. This principle promotes decisionmaking based on accurate and timely data rather than onassumptions. Understanding and using data also meansunderstanding variation or differences in the output of aprocess or system and determining whether the variationis a normal part of the process or whether it indicates areal change (either as an indication of a problem or of animprovement).
Teamwork: QA focuses on participation and teamwork tosolve problems and implement quality solutions, recogniz-ing that the impact of QA activities is most powerful whenteam members draw on the participation, experience, andknowledge of major participants and stakeholders.
These principles serve as the foundation for QA and reflectthat QA is not just a set of activities, but also a fundamentalset of beliefs and values that should become a “way ofdoing things” in an organization. These principles are inaccord with those espoused in the quality managementliterature (see for example, Berwick et al. 1992; Langley etal. 1996).3 Introducing QA does not necessarily meanchanging the whole way the organization is managed, butimplementing QA according to these principles oftenbrings about positive changes in the management of othercomponents of the health system, such as logistics andfinancial management.
2.3 The Core Activities of Quality Assurance:The QA Triangle
The QA Project approach to improving health servicesperformance encompasses three core quality assuranceactivities: defining quality, measuring quality, and improvingquality. These three sets of activities work synergistically toensure quality care as an outcome of the system and to-
3 The quality management literature often includes leadership as a fifth principle of quality. We include leadership in our framework forinstitutionalization.

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 11
gether comprise the range of various QA methodologiesand techniques used to assure quality healthcare. They arerepresented by a triangle (Figure 2.2) to indicate theirmutually supportive, interactive nature. Each point of thetriangle represents a set of core QA activities, and theunbroken triangle shape suggests that there is not one“correct” or even optimal entry point for initiating QA. Onecould start with making improvements in any problematicarea. At the same time, however, no one core set of QAactivities is sufficient on its own to improve and maintainquality. It is the interaction and synergy of all three thatfacilitate sustainable improvements in healthcare quality.
Defining quality (QD) means developing expectations orstandards of quality. Standards are statements of expectedperformance that define for health workers what consti-tutes quality care. Standards can be developed for inputs,processes, or outcomes; they can be clinical or administra-tive; and they can be applied at any level of a system, froman individual provider to a national department of health.
A good standard is reliable, realistic, valid, and clear, andcan be easily measured. Standards of quality should bebased on the best scientific evidence available and can bedeveloped in accordance with the nine dimensions ofquality discussed above. Stakeholder perception andexpectations of quality (including client and community,
provider, manager, and payer) should also be included inthe definition of quality standards.
Activities other than developing standards that relate todefining quality include designing systems for qualityoutputs; strategic planning; communicating standards; anddesigning various forms of regulation, including accredita-tion, licensure, or certification standards. 4
Measuring quality (QM) consists of quantifying the cur-rent level of performance or compliance with expectedstandards, including patient satisfaction. It involves defin-ing indicators, developing or adapting information systemsto provide data on performance related to the indicators,and analysis and interpretation of results.5
Activities related to measuring quality include routinecollection and analysis of data on adherence to estab-lished standards through supervisory assessments; self-assessment; quality monitoring; and special studies orperiodic assessments, such as audits. Measuring clientsatisfaction is one important form of quality assessment.
Improving quality (QI) refers to the application ofquality management methods and tools to close thegap between current and expected levels of quality byunderstanding and addressing system deficiencies andstrengths to improve, or in some cases, re-design healthcareprocesses. This core QA activity leads to improved perfor-mance according to defined standards of quality.66666
A variety of quality improvement approaches exists, rang-ing from individual performance improvement to redesignof entire systems/processes to organizational restructuring/re-engineering. These approaches differ in terms of time,resources, and complexity, but share the same four stepsin quality improvement: (a) Identify what you want toimprove, (b) Analyze the problem or system, (c) Developpotential solutions or changes that appear likely toimprove the problem or system, and (d) Test and imple-ment the solutions. Step 4 uses the “plan, do, study, act”cycle to determine whether the solutions under consider-ation would really yield improvement and whether theyshould be abandoned, modified, or scaled up. (Figure 2.3presents this approach graphically.)
4 More discussion of the uses and formats of standards in healthcare may be found in Ashton 2001b; more on regulatory approaches is inRooney and van Ostenberg 1999.
5 A systematic approach to measuring the quality of primary and in-patient care is described in Bouchet Undated and Ashton 2001a,respectively.
6 A thorough presentation of approaches to improving quality is in Massoud et al. 2001.
Figure 2.2 The Quality Assurance Triangle
DefiningQuality
Policy Making
Quality (Re)-Designing
Benchmarking
Problem Solving
Management Actions
MeasuringQuality
ImprovingQuality
QualityAssurance
Structural Re-Organization
Incentives
Motivation
Standards Setting
Monitoring Systems
Supervision
QA Project 2000
Quality Regulation Accreditation Audit
Evaluation

12 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Figure 2.3 Four Steps to Quality Improvement
1. Identify Determine what to improve
2. Analyze Understand the problem
3. Develop Hypothesize about what changes will improve theproblem
4. Test/ Test the hypothesized solution to see if it yieldsImplement improvement; based on the results, decide whether
to abandon, modify, or implement the solution
1.
Identify
2.
Analyze
3.
Develop
Plan
Study
Act Do
4.
Test and
Implement
In summary of this section on the principles of qualityassurance, the core QA activities, represented by the QAtriangle, encompass the methods, tools, and approaches anorganization uses to ensure quality care. The rest of thismonograph focuses on how to support and sustain theimplementation of these core QA activities.

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 13
A Conceptual Model: What It Takesto Institutionalize Quality Assurance3
B Figure 3.1 Essential Elements for the
Institutionalization of QA
Essential Elements for the
Institutionalization of QA
Internal enablingenvironment:
Policy
Leadership
Core values
Resources
Organizing for quality:
Structure
Support functions:
Capacity building
Information and communication
Rewarding quality
QA Project 2000
equated with an organization chart or reporting relation-ships. Instead, it refers to the mapping out of responsibili-ties and accountability for QA in the organization,including oversight, coordination, and implementation ofQA activities.
Support functions: Several essential elements are neededto support sustained implementation of QA and improvedquality of care. Three critical support functions are:(a) capacity building in QA, such as training, supervision,and coaching for healthcare providers and managers;(b) information and communication for the purposes ofsharing, learning, and advocating for quality; and(c) rewarding and recognizing individual and team effortsto improve quality.
These three categories are represented in Figure 3.2 as aseries of overlapping concentric circles that work together.At the center is quality healthcare, the desired outcome ofQA. Surrounding the center is the triangle of core QA tech-
EARING in mind that (a) our goal in implementingquality assurance is to improve the quality ofhealthcare; (b) QA and improved quality of care
require not only a technical approach of tools and meth-ods but also a change in attitude; and (c) QA is institution-alized when it is formally and philosophically integratedinto the structure, functioning, and culture of an organiza-tion, we can examine institutionalization more clearly toidentify its “essential elements.” These elements have beenidentified by the QA Project through its international expe-rience in supporting QA activities and programs and fromquality management literature (Baldrige National QualityProgram 2001; Tenner and DeToro 1992; Marszalek-Gaucherand Coffey 1990; Brown 1995; Powell 1995; Shortell et al.1995, among others).
3.1 Overview of the Model
Many factors affect a health organization’s ability toinstitutionalize a change in the way work is approached,especially the key, or essential, elements listed in Figure 3.1.We group them in three categories: internal enabling envi-ronment, organizing for quality, and support functions.These categories are briefly described in the next fewparagraphs; then we describe the role each essential ele-ment plays in institutionalization and how each functionsin a mature organization that can sustain QA.
The internal enabling environment: An internal envi-ronment conducive to initiating, expanding, and sustainingQA is necessary to institutionalize QA. Such a supportive/facilitative environment is comprised of: (a) policies thatsupport, guide, and reinforce QA; (b) leadership that setspriorities, promotes learning, and cares about its staff; (c)core organizational values that emphasize respect, quality,and continued improvement; and (d) adequate resourcesallocated for the implementation of QA activities. The fullimpact of the internal enabling environment is achievedonly through the synergy created among all four of theseelements.
Organizing for quality: Institutionalization requires aclear delineation of roles, responsibilities, and accountabil-ity for the implementation of QA activities. We refer to thisorganization for implementing QA as the essential element,structure. However, in this context structure should not be

14 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Core Values
Leadership
Policy
Resources
RewardingQuality
QD
QMQI
QualityCare
Cap
acity
Build
ing
Structure
Information &
Com
munication
nical activities for improving the quality of care: definingquality (QD), measuring quality (QM), and improvingquality (QI). The impact of these core QA activities willdepend on an enabling environment that encourages aculture of quality and facilitates continued implementa-tion of QA, an appropriate organizational structure forframing effective QA implementation, and the presenceand adequacy of support functions. Developing a cultureof quality requires initiating or strengthening each essen-tial element. Selecting where to begin depends on thesituation, and each essential element—and each categorywhere the essential elements reside—will progress at itsown rate.
Each category of elements is important unto itself, but it isthe combination of elements that facilitates and ensuresinstitutionalization of QA. This model and the ensuingdiscussion of essential elements focus on those elementsthat operate within the organization’s sphere of influence.At the same time, we recognize that every healthcare orga-nization operates within a larger environment that influ-ences its ability to implement QA. For example, somehealthcare organizations approach the institutionalizationof QA within a stable institutional context, while othersoperate in systems undergoing reform. External environ-mental factors create both constraints and opportunitiesfor assuring quality and institutionalizing QA. Health sectorreforms focused on decentralization or new financingmechanisms may provide opportunities for QA to contrib-ute to better health outcomes. By the same token, externalfactors can negatively affect the institutionalization of QA,as is sometimes the case with civil service policies orresource flow to the health sector based on the country’sfinancial situation.
While this model recognizes the influence of externalfactors, it emphasizes the more important role that the
categories of essential elements have in the institutional-ization of QA. The sections that follow describe the roleeach essential element plays in institutionalization andhow they function in a mature organization that is capableof sustaining QA. The elements are discussed by category.
3.2 The Internal Enabling Environment
The internal enabling environment includes thoseorganizational features that encourage the growth ofa sustainable QA program and that senior managersof an organization generally can control or change.
The key elements of the internal enabling environmentfor QA institutionalization are organizational policies,leadership, core values, and commitment to allocate neces-sary resources (human and material) to support QA activi-ties. Regardless of an organization’s level and complexity,these elements are necessary for sustaining QA and for thesmooth functioning of the essential elements in the othertwo categories.
The internal enabling environment operates in the contextof a broader external environment (economic status, politi-cal/administrative structure of the country, political stabil-ity, etc.) that may or may not be enabling. However, muchcan be accomplished to institutionalize QA by strengthen-ing the essential elements in the internal environment.Such strengthening can assist the organization to perseverein sustaining QA activities despite hindrances from theexternal environment. For example, when external fundingended for Chile’s National Quality Improvement Program,it was sustained largely by strong technical leadership andits strategy of decentralizing the planning, direction, andfunding for quality improvement efforts to the level of thecountry’s 27 health services (Gnecco 1999).
Although the internal enabling environment is critical,strengthening it to support QA need not precede efforts todevelop other areas or essential elements. Each elementmay progress at a different rate. Section 5 describes theprocess of strengthening all of the essential elements andthereby moving toward the institutionalization of QA.
3.2.1 Organizational Policies and PolicyImplementation
The term “policy” covers a wide range of organizationaldirectives, from broad policies (like an organizationalmission statement and human resource management) tonarrow policies, such as standard operating proceduresand clinical standards. Policy can be defined as a plan,
Figure 3.2 Institutionalization of Quality Assurance
QA Project 2000

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 15
course of action, or a set of regulations adopted by agovernment, business, or institution that is designed toinfluence and determine decisions and procedures(Partnerships for Health Reform Project 2000). Policiesreflect the decisions and actions of an organization’smanagement. Policies written as laws, regulations, plans,and strategy statements constitute official statements ofgoverning principles by which an organization operatesand provides services.
To be effective, policies must be implemented andenforced. When written policies and their mechanism forenforcement incorporate a focus on quality and qualityassurance, they provide sustained guidance for and rein-force the institutionalization of QA, particularly in organi-zations with high turnover at the leadership level.
Policies can be used to highlight an organization’s commit-ment to quality and meeting client needs, to identify prior-ity areas for improvement, and to provide flexibility anddelegation of authority to make improvements (see ex-ample in Box 3.1). Policy development should be based onan orientation to results that reflect real changes in healthstatus and community/client satisfaction.
For organizations embarking on QA, existing policies mighthinder the institutionalization of QA. For example, policiesthat promote highly centralized decision making may limitstaff initiative to make quality improvements. In contextswhere decentralization reforms are being initiated, anopportunity may exist to modify current policies and shiftthe focus to emphasize quality assurance at the local level.In another instance, financing policies may be formulatedto stress cost containment, imposing a culture of efficiencyrather than a culture of quality, at the expense of patientcare. In such a situation, policy dialogue and advocacymay be necessary to incorporate indicators of qualityperformance into financing mechanisms.
Policy is an important link to other enabling environmentalelements. It is often set or influenced by leaders, mayreinforce (or undercut) core values, and determines theresources allocated for QA activities.
3.2.2 Leadership
One definition of a leader is “someone you choose to fol-low to a place you wouldn’t go by yourself” (Barker 1999).Leadership is the ability to motivate, enabling people toachieve results amid challenges and uncertainties (Man-agement Sciences for Health 2002). Leadership is criticalto the institutionalization of QA, because effective QAimplementation requires a change in the way providersand managers work. In many places, health workers aredemoralized after years of working with inadequate
resources, little response or support from higher levels ofmanagement, and little perceived authority to makechanges. Making a shift to instill health workers with thedesire to make improvements and empower them to do soclearly requires leadership.
In the context of QA, leadership relates to an individual’spersonal qualities and actions to support the staff’s abilityto ensure or improve the quality of healthcare. For ex-ample, in Honduras, “active leadership support” was foundto facilitate the speed with which hospital-based qualitydesign teams progressed. Such support was characterizedas keeping up-to-date on the team’s work, maintaining anopen-door policy toward team members, and encouragingthe search for creative solutions to overcome obstacles(Lin 2000). There is no single best leadership style: differ-ent styles are appropriate for different cultures or situa-tions. However, effective leadership for QA involvescreating and communicating a clear vision of what theorganization is trying to achieve; developing the desire toreach that vision among staff; setting priorities to reachthat vision; ensuring that staff have what is needed (flex-ibility, resources, etc.) to reach that vision; and showingcare for staff, thereby building mutual trust (see Box 3.2).
Box 3.1 Quality Policy in Mexico
Improving the quality of healthcare in public andprivate facilities is a major priority of the Governmentof Mexico. In the recently published National HealthProgram 2001-2006, the Secretariat of Health identi-fied “Unleashing a Crusade for Quality” as one of itsmajor strategies, with the following lines of action:
1. Define codes of ethics for health professionals
2. Define and make explicit the rights of healthservice users and healthcare providers
3. Establish a system of follow-up and response tocomplaints and suggestions
4. Establish systems to recognize good performance
5. Develop an information system to link hospitalproductivity and costs
6. Promote the use of clinical guidelines
7. Promote the certification of healthcare providersand facilities
8. Strengthen medical arbitration to resolve conflictsbetween patients and providers
Source: Secretariat of Health, Mexico 2001

16 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Box 3.2 Key Leadership Responsibilities for
Successful QA Implementation
Develop and articulate to the staff a vision for qualityof care—supported by core values and policies toguide standards development—and then allocate theresources to carry out quality assurance activities.
Continually advocate for quality with providers, staff,managers, and members of the community.
Create a synergy between quality words and actions.When leaders/managers advocate for QA in wordsbut not in actions, they signal that quality is not apriority.
Practice and model the four principles central to QA:focusing on clients, systems and processes,decisions based on data, and teamwork.
Use change management strategies to reduceresistance to the changes inevitable when makingimprovements.
Provide resources for QA activities.
Ensure that all operational managers have a workingknowledge of QA approaches and demonstrate acommitment to quality of care.
Empower staff to make improvements.
Ensure staff development to increase QA capacity.
Allocate staff time to participate in QA activities ormake QA part of everyone’s job description.
Adapted from Senge et al. 1994.
This discussion distinguishes between leaders and manag-ers. Every organization has people in charge (managers) ofmaking sure that things get done. Managers plan and orga-nize activities, mobilize resources, and evaluate results.Leaders are individuals who have vision and can motivatepeople to follow and build that vision, who can set anexample for others, and who promulgate the values andgoals of the organization. Leaders see opportunities in theenvironment; develop a vision and direction for the organi-zation; ensure alignment of vision, strategy, systems, andrewards; and motivate others to be creative and innovative.
Institutionalization of QA requires cultivation of leadershipqualities among a range of managers at different levels inthe organization. Not all managers will become leaders,nor will all leaders be managers. However, fostering leader-ship among managers will foster the institutionalization of
QA, since managers have the authority to establish QA asan organizational goal, devise other supporting policies,and allocate (or advocate for) resources to carry out QAactivities. As leaders, these managers will start to model thebehaviors necessary to achieve institutionalization andwill communicate and support organizational core values.Capitalizing on informal leaders who “lead” by virtue oftheir personal strengths facilitates QA institutionalization.
In higher level organizations and more complex inter-organizational collaborations, leadership may come frommore than one front. The vision and direction may comefrom one organization (such as a professional association),while the follow-through and resource allocation maycome from another. In South Africa’s KwaZulu-Natal Prov-ince, for example, the private Council for Health ServiceAccreditation of Southern Africa (COHSASA) providesindividual hospitals with recommendations on how toimprove their performance, while the QA Unit of theprovincial government’s Department of Health providestechnical support to the hospitals to help them implementCOHSASA’s accreditation standards. For successful institu-tionalization the various roles of leadership must beassumed and played out in a coordinated fashion, avoidingcompetition for primacy.
3.2.3 Core Values
The culture of an organization reflects its core values.Ensuring sustained improvements in the quality of carewithin an organization requires shared values that empha-size quality healthcare and responsiveness to clients’needs. Organizational core values manifest themselves inhow individuals in the organization behave individuallyand collectively. They are both a driver of behavior and areflection of what people believe is most fundamental. Toachieve optimal performance, organizational values andthose held by the individuals working in the organizationshould be complementary and aligned to create a synergyof working together towards quality healthcare. Having
Box 3.3 A Change in Values in Russia
“…We are no longer talking about a project. We aretalking about a whole new way of working.”
Dr. Alesander Zoblin, Director of the Tver Oblast Department
of Health, speaking at the launch of the large-scale
implementation of redesigned systems of care, following
the successful pilots
For additional information, see Ethier Forthcoming.

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 17
aligned values means that the core values of the organiza-tion and those of its employees are compatible and con-tribute to the same goals.
Core values do not operate independently within theenabling environment; they are directly connected to theelements of leadership, policy, and resources. Leaders oftenset the tone for organizational core values by modelingbehaviors of respect, caring, and teamwork, and by commu-nicating organizational goals of quality. Policy can estab-lish, communicate, and reinforce the practice of QA as anorganizational core value. The allocation of human andmaterial resources to QA activities sends the message thatquality is valuable to the organization. Core values thatsupport QA promote the development of an environmentwhere people feel they are doing something that matters,both to them personally and to others (see Boxes 3.3 and3.4.).
However, core values are not the result of just leadershipmodeling or resource allocation. Every organization hasvalues in operation, although they are often implicit orunspoken. Institutionalizing QA requires making explicitthose desired values that foster quality care (see Box 3.5).Communicating values clearly and recognizing organiza-tional accomplishments that reflect those values foster aculture of quality essential to sustainable QA.
Box 3.4 A Change in Staff Attitudes in South Africa
“There has been a definite shift in attitudes. Peoplewho may in the past have been ignored in the chainof command are now being given a voice and theyare being heard. This has resulted in a tremendousamount of professional and personal growth and hasbroken down the barriers that often exist betweendoctors, nurses and management. . . . There is morediscussion between patients and staff, and patientsare beginning to feel that their viewpoints are beingtaken into consideration. Nurses are looking morecritically at their activities and at ways to improvetheir performance. Instead of grumbling about asituation, they are now beginning to understand thatit’s better to identify a problem and think of ways tosolve it.”
Miss Joan Maher, Assistant Director of KwaZulu-Natal’s Quality
Assurance and Accreditation Unit, speaking of the changes that
have been noted in the hospitals involved in the COHSASA
accreditation process
Source: COHSASA 2000
Explicit core values also assist in the design of standardsand interventions to improve the quality of care by statingwhat is fundamental to the notion of quality in a particularsetting. For example, at the beginning of a national initia-tive in South Africa to provide adolescent-friendlyhealthcare, a panel of national and international expertsformally talked with young people about their needs andexpectations of clinic services (Dickson-Tetteh et al. Forth-coming). One outcome of the adolescent focus groups wasthe definition of a set of adolescent rights and responsibili-ties. As the standards were being introduced in pilot clin-ics, it became clear that some staff members had difficultyworking with adolescents. Workshops to clarify values forclinic staff focused on the rights and responsibilitiesdefinition and helped staff understand how adolescentsperceived healthcare quality.
In summary, organizational values, when explicitly stated inclear and concrete terms, can motivate change, providedirection, and energize staff. Values serve as a set of guidingprinciples upon which organizational members can buildcommitment to a shared vision of quality.
3.2.4 Resources
Carrying out the daily tasks involved in implementing QAactivities––be they quality improvement activities, design-ing and communicating standards, or monitoring resultsand measuring the success of improvements––requireshuman, material, and financial resources. Resourcesinclude staff time, office supplies, and transportation forQA activities, as well as resources for capacity building andcommunication to support QA implementation. The magni-tude of needed resources may vary over time, with largerinvestments sometimes required initially while capacity isbeing developed. However, even when QA becomes part ofeveryone’s job, resources will be needed to undertake QAactivities, i.e., staff time, designated funds, dedicated materi-als for data collection and interpretation, support to qual-ity improvement teams, and continuing education ofleaders in the science of QA.
Many health systems and organizations have severely lim-ited resources for their programmatic needs. In these cases,the following question should be asked: Within the limits ofthe resources available, how can resources be maximizedto achieve quality care? Without QA, can one be assured ofefficient and effective use of current resources? Researchsuggests that increases in efficiency and effectiveness as aresult of quality improvement initiatives may actually re-duce implementation costs (Atkinson 1990; Abdallah et al.2002).
18 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
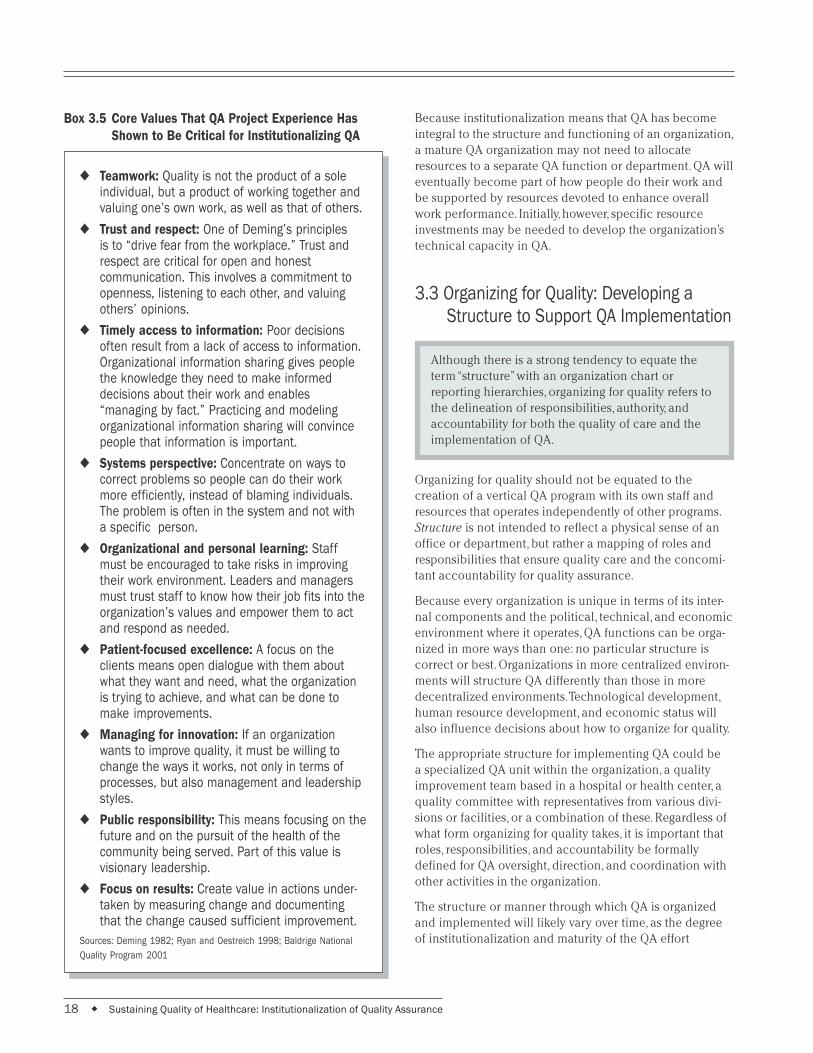
Box 3.5 Core Values That QA Project Experience Has
Shown to Be Critical for Institutionalizing QA
◆ Teamwork: Quality is not the product of a soleindividual, but a product of working together andvaluing one’s own work, as well as that of others.
◆ Trust and respect: One of Deming’s principlesis to “drive fear from the workplace.” Trust andrespect are critical for open and honestcommunication. This involves a commitment toopenness, listening to each other, and valuingothers’ opinions.
◆ Timely access to information: Poor decisionsoften result from a lack of access to information.Organizational information sharing gives peoplethe knowledge they need to make informeddecisions about their work and enables“managing by fact.” Practicing and modelingorganizational information sharing will convincepeople that information is important.
◆ Systems perspective: Concentrate on ways tocorrect problems so people can do their workmore efficiently, instead of blaming individuals.The problem is often in the system and not witha specific person.
◆ Organizational and personal learning: Staffmust be encouraged to take risks in improvingtheir work environment. Leaders and managersmust trust staff to know how their job fits into theorganization’s values and empower them to actand respond as needed.
◆ Patient-focused excellence: A focus on theclients means open dialogue with them aboutwhat they want and need, what the organizationis trying to achieve, and what can be done tomake improvements.
◆ Managing for innovation: If an organizationwants to improve quality, it must be willing tochange the ways it works, not only in terms ofprocesses, but also management and leadershipstyles.
◆ Public responsibility: This means focusing on thefuture and on the pursuit of the health of thecommunity being served. Part of this value isvisionary leadership.
◆ Focus on results: Create value in actions under-taken by measuring change and documentingthat the change caused sufficient improvement.
Sources: Deming 1982; Ryan and Oestreich 1998; Baldrige National
Quality Program 2001
Because institutionalization means that QA has becomeintegral to the structure and functioning of an organization,a mature QA organization may not need to allocateresources to a separate QA function or department. QA willeventually become part of how people do their work andbe supported by resources devoted to enhance overallwork performance. Initially, however, specific resourceinvestments may be needed to develop the organization’stechnical capacity in QA.
3.3 Organizing for Quality: Developing aStructure to Support QA Implementation
Although there is a strong tendency to equate theterm “structure” with an organization chart orreporting hierarchies, organizing for quality refers tothe delineation of responsibilities, authority, andaccountability for both the quality of care and theimplementation of QA.
Organizing for quality should not be equated to thecreation of a vertical QA program with its own staff andresources that operates independently of other programs.Structure is not intended to reflect a physical sense of anoffice or department, but rather a mapping of roles andresponsibilities that ensure quality care and the concomi-tant accountability for quality assurance.
Because every organization is unique in terms of its inter-nal components and the political, technical, and economicenvironment where it operates, QA functions can be orga-nized in more ways than one: no particular structure iscorrect or best. Organizations in more centralized environ-ments will structure QA differently than those in moredecentralized environments. Technological development,human resource development, and economic status willalso influence decisions about how to organize for quality.
The appropriate structure for implementing QA could bea specialized QA unit within the organization, a qualityimprovement team based in a hospital or health center, aquality committee with representatives from various divi-sions or facilities, or a combination of these. Regardless ofwhat form organizing for quality takes, it is important thatroles, responsibilities, and accountability be formallydefined for QA oversight, direction, and coordination withother activities in the organization.
The structure or manner through which QA is organizedand implemented will likely vary over time, as the degreeof institutionalization and maturity of the QA effort

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 19
increases (see example in Box 3.6). During the initial stageof QA institutionalization, some individuals may have to beassigned only to QA, working within a designated QA unit(i.e., a visible organizational location for QA), to boostawareness of QA and its importance to the organization. AsQA becomes more integrated into the routine operationsof the organization and accountability for quality resultsbecomes more embedded, the type of coordination andoversight required may shift, as can its location. Routinemanagement structures may assume daily oversight of QA
Box 3.6 Evolution of the QA Oversight
Structure in Malawi
Malawi’s organization of QA demonstrates how thestructure can change over time and how variousstakeholders for quality have been involved. Duringthe initial stages of developing a country-wide QAplan, a National QA Task Force formed to provideoversight and planning functions. Membershipincluded representatives from the Ministry of Health(MOH), the regulatory boards (medical and nursingcouncils), the teaching institutions (medical schools,nursing schools, and allied health professionalschools), professional associations, the ChristianHealth Association (mission facilities), and privatepractice. The Medical Council housed and providedsupport for this task force.
The success of several quality improvement pilotprojects led to district initiatives in quality, includingthe formation of district and facility QA committees.The organizational locus of the country’s QA activitiesshifted from the national to the district level. Measur-able improvements in the quality of care in the sevenpilot districts led to a decision to reconstitute theNational QA Task Force and shift responsibility for itssupport to the MOH. The reconstituted task forceincluded different members and new responsibilities.
In May 2001, the task force developed a vision forquality, a mission statement, Terms of Reference,and a one-year action plan, which senior MOHmanagers validated at a workshop in July 2001.The action plan clearly delineated the new rolesand responsibilities of the task force and planned atransition of responsibility to a national QA commit-tee. The plan also included capacity building for thetask force and acknowledged the need for developinga cadre of QA experts who could provide coachingand mentoring to others.
For more information, see Reinke et al. 2001.
activities, and the role of a designated QA unit may be-come more narrow and technical in nature (such as focus-ing on development of standards). For example, in Chile,after QA structures in the decentralized health serviceshad attained maturity, the role of the central level QA unitshifted from training and support of quality improvementteams to the development of national technical standardsand quality monitoring tools (Gnecco 1999).
While QA can be implemented at any organizational level(facility, network, district, regional, national), three aspectsof organizing for quality are important, regardless of thetype or level of the organization: oversight, coordinationand support, and conducting QA activities (see Box 3.7).For each of these aspects, roles, responsibilities, and ac-countability must be delineated and delegated within theorganizational framework. The true structure for QA ismanifested in how the roles and responsibilities for per-forming QA activities are divided and/or delegated withinthe organization, how they are implemented, and whetherstaff feel accountable for organizational results (high qual-ity care). As QA becomes institutionalized, every individualbecomes accountable for results and responsible for qual-ity. Eventually, responsibilities for QA will be incorporatedin job descriptions for every staff member, as well as in thescope of work for organizational units. However, specificindividuals or groups must still be assigned responsibilitiesfor oversight, coordination, and support of QA and forconducting QA activities.
3.4 Support Functions
As the name implies, support functions provide“support” for staff to initiate and continue technicalQA activities, and to do them well. Those doing theday-to-day implementation of QA require specifictypes of support beyond those discussed previouslyin the context of the enabling environment orstructure.
Systems to ensure QA capacity building, communication ofQA efforts, and reward for quality work are critical for anorganization to move beyond performing QA as isolatedactivities, to a state of continuously implemented QA, em-bedded in the organizational work ethic. There are manyother support functions, such as logistics and financialmanagement, but these three functions have particularimportance to the institutionalization of QA.

20 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Box 3.7 Key Roles and Responsibilities for a QA Structure
Oversight: Any description of structure must addresswhere the responsibility for oversight of QA activitieslies. This oversight or stewardship for QA includesleadership and political support (developing strategicdirection, setting priorities, follow-up, review ofprogress), as well as technical direction and monitor-ing of QA efforts. Effective oversight structures canvary from designating a senior manager who is wellversed in QA to be responsible, to creating an inde-pendent body of major stakeholders for quality ofcare both within and outside the organization.Whatever the form, oversight responsibilities andaccountability for results must be clearly defined toeffectively implement and sustain QA.
Coordination and support: Responsibility for ensur-ing and coordinating the day-to-day implementationof QA activities must be assigned and accountabilityupheld. The structure must also define how thedifferent components and levels of a QA programfit together and how they will be coordinated andsynchronized. Issues of coordination will vary,depending on the type of organization. For smallerorganizations, coordination across functional divi-sions may be key. In larger or national programs,coordination across geographic units as well asacross broad technical programs will be important.In countries with a decentralized structure forhealthcare administration, coordination becomescrucial for efficient use of resources.
Conducting QA activities (defining, measuring, andimproving quality): Sustainable QA implementationrequires clear delineation of specific duties, lines ofreporting, and accountability for results, as well asallocating time for staff participation in QA. Eventu-ally QA implementation should be part and parcel ofeach individual and team’s job responsibilities andperformance expectations. The nature of QA activi-ties will vary, depending on the level and complexityof the organization. For organizations with moremacro and strategic responsibilities, the focus of QAimplementation may be on regulatory and monitoringfunctions, such as accreditation, development ofquality standards, and monitoring of quality. Forsmaller organizations or organizational units, thefocus may be on quality improvement and localadaptation of standards.
3.4.1 Capacity Building
Capacity building encompasses the whole range of activi-ties that increase QA knowledge, skills, and ability: formalQA training, coaching and mentoring on the job, self- andpeer appraisals, performance improvement, and supervi-sory activities. Ensuring that staff have the necessaryknowledge and skills to carry out their QA responsibilitiesand that they know when and how to best use these skillsis vital for the development of a critical repository of QAtechnical, managerial, and leadership expertise within theorganization.
Doing QA is more than the simple application of technicalmethods. It often requires behavior change––learning towork differently. Traditional approaches to capacity build-ing through one-time classroom training will probably beinsufficient; innovative, alternative modes of learning areuseful, including participatory, performance-based, anddistance learning and mentored on-the-job practice.
Three main types of capacity building are needed forinstitutionalizing QA: basic QA expertise; coaching andmentoring of staff as they implement QA activities; andsupervision and oversight of staff QA efforts. As describedin the example of Tahoua, Niger, in Box 3.8, all three typesare part of a continuum of support that should be providedto staff as they undertake QA activities. These three areas ofcapacity building are not mutually exclusive and may becarried out by a single individual or by a group of individu-als working at different levels.
However they are performed, the ability to carry out thesecapacity-building activities needs to be developed andmaintained in a critical mass of individuals working in theorganization in order to sustain QA. (Box 3.9 details thesemain types of capacity building.)
3.4.2 Information and Communication
Information and communication are critical to efforts toexpand QA and create a learning environment for theorganization and the people working in it. “Information” inthe context of support for QA refers to the gathering ofexperiences and results of QA initiatives. “Communication”is the two-way process of interaction in which availableinformation is shared with various parts of the organiza-tion, with organization staff, with the communities beingserved, and with other stakeholders, including policy mak-ers. Information and communication allow for the identifi-cation of priority areas for quality improvement efforts,reinforcement of core values, recognition of efforts, anddemonstration of results for the purpose of advocacy,benchmarking, and change management.

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 21
Box 3.8 Capacity Building in Tahoua, Niger
The QA Project provided long-term technical assis-tance to the Department of Health of Tahoua, Niger,to institutionalize QA in the decentralized manage-ment of health services in the region. Training andon-site coaching were the central strategies used toenable health workers at the regional, district, andfacility levels to apply QA concepts and methods.
The Tahoua QA project first trained health workerswho had been selected for the regional and district-level quality improvement teams in each of theregion’s seven districts. Training gave participants aframework and skills to systematically solve quality-related problems using methods adapted to localconditions. During the training workshops, partici-pants chose a problem, drafted a definition state-ment, and began preliminary problem analysis beforeleaving training.
The QA Project’s resident advisor gave the teamssupport, visiting each team regularly to motivateteam members and help them apply the QA method-ology. This follow-up support was found to be criticalto teams’ ability to move through the problem-solvingcycle, since QA required very different attitudes andskills than what Tahoua health workers were accus-tomed to. Members of the district managementteams and supervisors were also trained in coachingand team-building skills to enable them to train andsupport facility-level quality improvement teams.
Source: QA Project Undated
Box 3.9 The Three Types of QA Capacity Building
Providing basic QA expertise: Institutionalization ofQA requires that health providers and managersreceive initial and continuing knowledge and skilldevelopment in QA techniques and methods. Asappropriate, the ability to manage QA activities mightalso be included. Developing basic QA expertiseshould ultimately be integrated into the pre-serviceand in-service training systems. Training activitiescan be on- or off-site, in the context of the job, orusing distance learning. Staff needs will change overtime, so training should be tailored to evolving QAresponsibilities and related learning needs. QAProject experience has shown that training is mosteffective when it is “just in time”—i.e., when staff andproviders need the information.
Ongoing coaching and mentoring: Coaching andmentoring provide ongoing technical and motiva-tional support to facilitate the behavior changesneeded to undertake and sustain QA activities inthe routine working environment, while simulta-neously encouraging the development of a “cultureof quality.” The term “coach” refers to an individualwho is well versed in QA techniques and principlesand can provide on-the-job technical support to staffimplementing QA activities. In contrast, a “mentor” issomeone who acts as a guide or advisor. A mentordoes not need to be a QA expert, but must be ableto know when additional intervention or expertisewould be useful and facilitate connection with anappropriate resource person.
Supervision: Staff also need day-to-day support andcorrection as they undertake QA activities. Achievingsupportive supervision of QA requires enhancing thesupervisor’s facilitative role; assuring that supervi-sors have a foundation of QA expertise; and teachingsupervisors how to observe, assess a situation, andgive constructive and immediate feedback forimprovement.
Ensuring the timely flow of information is critical to effec-tive implementation of QA and thus to improvements inthe quality of care. Formal mechanisms to assure the com-munication of new standards, policies, and improvementefforts increase the likelihood of acceptance and compli-ance with these QA activities. Communication reinforcesthe notion that QA is everyone’s business, that successesshould be publicized, and that lessons should be sharedeven when things do not go as planned.
Successful information and communication support forQA includes:
Recording improvements and changes, using both data todemonstrate results that have been achieved and storiesabout how these results were achieved (see example inBox 3.10).
Sharing what has been achieved and how it was done,with the organization’s staff, the community it serves, andothers who might learn from it and become motivated by itto improve their own services (see Box 3.11).
Using the results for advocating policy changes andresources: when activities are well documented with sup-porting data, it is easier to convince decision makers.

22 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Box 3.10 Sharing Data on Compliance with
Standards in Ecuador
As part of a QA intervention to improve compliancewith maternal and child care standards in hospitalsin Ecuador, data on monthly compliance with thestandards are posted in each hospital’s public areasfor staff and clients to see. Monthly staff discussionsof the trends in compliance with standards havegenerated collective self-supervision, creating theopportunity to discuss causes for problems andpotential interventions and heightening awarenessamong staff of their role in quality improvement.
Hermida and Robalino. Forthcoming
Box 3.11 Facilitating Information Flow and
Sharing of Lessons in Chile
The national quality unit in Chile’s Ministry of Health(MOH) has played the lead role in coordinating thedissemination of information on QA interventions andresults from quality improvement activities carriedout in the Health Services. Approaches used include:
National “Quality in Healthcare Month”: Since1994, the MOH has designate October “Quality inHealthcare Month” to stimulate health professionalsthroughout the country to come together to sharesuccesses and promote quality through specialevents.
Bi-monthly newsletter: In the first three years of theprogram, the quality unit published and distributedthroughout the country a newsletter reporting onadvances by local quality improvement projects,training activities, and formation of quality commit-tees. The newsletter ceased publication in 1995because circulation had become too large and fundsceased. Instead, the central team now contributesQA information to bulletins published by the healthregions.
National Resource Center: The quality unit houses aresource center on QA methods and experiences. Thematerials are available to quality monitors and teamsthroughout the country and to self-organized QAstudy groups.
National Quality Assurance Conference: Since1995, the MOH has sponsored an annual conferencefeaturing presentations of quality improvementprojects, regional quality plans, and technicaldiscussions of QA issues. The average attendanceis 250 participants, drawn from the health services,universities, and the private sector.
Gnecco et al. 1999
When QA is institutionalized, the organization has beentransformed into a learning environment. Yet, withoutaccess to information, it is difficult to learn, so gatheringand communicating information are essential supportfunctions.
3.4.3 Rewarding Quality Work
In addition to having the capacity to do QA and havinginformation available about what can be achieved, staffalso need to see that their QA efforts are important to theorganizational leadership and the communities served.Providing individual, group, or organizational recognitionor rewards can reinforce interest in QA endeavors and helpto align staff values with organizational values relating toquality.
Every organization has implicit, if not explicit, incentivesthat influence staff behavior. Institutionalization requiresdeveloping mechanisms to stimulate and reward workersfor striving to provide quality services. Incentives canbe material—such as in Zambia, where some districtsrewarded their best staff with bicycles or sewingmachines—or non-material—such as public recognitionof staff. In Costa Rica and Niger, the best QA teams wereselected to attend a conference, thus serving the dualpurpose of rewarding staff while continuing their skilldevelopment. These practices boost employee self-esteemand encourage continual efforts.
There are many ways to recognize and reward individualsand teams for QA efforts that do not necessarily requireadditional resources: featuring the work of quality improve-ment teams in meetings or newsletters, publicly recogniz-ing an “employee of the month” for outstanding clientfocus, posting displays on QA efforts in healthcare facili-
ties, and honoring individuals and teams with symbolicawards. Quality improvement efforts, commitment to QAgoals, or quality work can also be recognized in the regularperformance appraisal system.
Rewarding quality work can also be done through higherlevel interventions, such as changes in financing systemsor in civil service human resource management policies(see example in Box 3.12).

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 23
Staff also find rewards and gratification when managersremove disincentives or barriers to quality. For example,quotas on the number of patients a provider must see maydiscourage adherence to guidelines or adequate patientcounseling. Lowering such quotas gives employees anopportunity to experience the satisfaction of providingquality care. Similarly, lack of responsiveness by manage-ment to staff suggestions for quality improvements willdiscourage staff from making such suggestions. Rewardingquality requires managers to identify and reduce or elimi-nate barriers to quality at every level of the organization.
3.5 Conclusion
These eight essential elements—policy, leadership, corevalues, resources, structure, capacity building, informationand communication, and rewarding quality—are key tounderstanding what is needed to sustain QA interventionsand continuous improvement in the quality of care deliv-ered.
The framework presented here describes the internal ele-ments around which an organization must focus its effortsto institutionalize QA. These elements do not appear spon-taneously; they must, each in its own right, be developedand nurtured. Institutionalization of QA requires a long-term vision, because it can be a lengthy and sometimescomplex process. Section 4 describes the dynamic processthat organizations go through as they embark on the roadtowards QA institutionalization and continuous quality ofcare.
Box 3.12 Rewarding High Levels of Quality and
Coverage in Ecuador
In 2000, the Ministry of Health of Ecuador (MOH)introduced a new program, called “Free Maternity,” toimprove maternal and child health care. An importantfeature of this program was to change the mecha-nism by which health districts would be funded and tointroduce a financial incentive for districts to providetargeted maternal and child services, such as prena-tal consultations, normal deliveries, management ofobstetrical complications, family planning, and carefor children under five.
Besides assigning funds through annual budgets,under the new program the MOH pays participatinghealth districts based on the number of priority ser-vices provided and on meeting quality standards inthe provision of those services. The terms of paymentand quality standards are defined through formalmanagement agreements between the national FreeMaternity Coordination Unit and the municipality inwhich the district lies. Quality teams in the facilitiesmonitor and continuously improve their compliancewith approximately 30 maternal and child healthclinical standards on a monthly or bimonthly basis,under the supervision of the district managementteams and provincial MOH office. The facilities alsoregularly measure client satisfaction through exitinterviews conducted by community members.
In 2002, the Free Maternity program proposed twonew elements in the payment scheme to rewardquality, client-focused care. First, the MOH wouldpay a 2 percent premium above the agreed-uponpayment amount to districts that achieve particularlyhigh levels of quality, coverage, and client satisfac-tion. Data on compliance with clinical quality stan-dards and coverage levels would determine eligibilityfor the premium. Second, users’ committees (madeup of clients of facilities in the district) would reviewquality of care information, including client satisfac-tion, and advise the program on paying the premium.
After more than a year of pilot testing in eightdistricts, the QA component of the program is beingprogressively extended to the entire country. One-third of Ecuador’s 217 municipalities have signedmanagement agreements. Introduction of theproposed premium and users’ review is expected in2003.
Source: Jorge Hermida, personal communication with L. Marquez,
September 2002

24 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 25
Understanding the Process ofInstitutionalization: A Road Map
4.1 QA Institutionalization as a Process
The preceding section focused on the eight essentialelements for institutionalizing QA and what they look likewhen QA is institutionalized; in other words, it was a staticdepiction of their “end state.” In reality, the institutionaliza-tion of QA is an evolving process, where organizationalchanges take place continuously while QA becomes for-mally and philosophically integrated into an organization’sstructure and functioning. This section examines this pro-cess of institutionalizing QA within an entire organizationwithout looking at each individual element (as notedearlier, an organization may be a facility, a network ofhealth centers, a district, or a regional or national system).The next section presents the process for each elementseparately.
The process of institutionalization can be described as apassage through a series of phases, between an initial stateof pre-awareness of QA and the end state of mature QAfunctions and structure. The QA Project has identified fourmain transitional phases: awareness, experiential, expan-sion, and consolidation. The phases and their descriptionswere derived from QA Project experience in developingcountry health systems and are consistent with conceptsin the organizational development literature (Renzi 1996;United States Agency for International Development 2000).The characteristics, strategies, and activities depictedfor each phase are illustrative and are not meant to beprescriptive.
Although institutionalization is a continuum, subdividing itinto four distinct phases helps to map out the process that
4organizations are likely to experience. Such a road mapcan assist healthcare organizations to assess their ownlevel of QA development and to make decisions (humanresource, financial, and technical) on how best to furthertheir organization’s advancement toward incorporating QAas part of day-to-day operations.
4.2 The Phases of Institutionalization
The phases of institutionalization reflect the degree oforganizational commitment and capacity to do QA and theextent to which QA activities are implemented within theorganization. Figure 4.1 depicts the phases an organizationpasses through as it moves towards QA maturity, when QAis formally and philosophically integrated into the way theorganization functions. Although the figure depictsprogress through the phases as linear, different reasonsmay cause actual progress to include reverting to an ear-lier phase. Furthermore, some phases (e.g., awareness andexperiential) often occur simultaneously or in an iterativefashion, as suggested by the curved arrows.
Table 4.1 lists the characteristics, strategies, and indicationsof readiness to progress for each phase. Organizationalleaders and managers can use this table to determine theirorganization’s location on the institutionalization con-tinuum, either as a whole or at the level of each essentialelement. The description of potential strategies and activi-ties in each phase provides guidance for planning how tomost efficiently move toward QA maturity by helpingleaders visualize where the organization should go andhow to get there.
Figure 4.1 The Phases of Institutionalizing Quality Assurance
Pre-existing
organization hasno formal or
deliberate QA
Expansion Consolidation
Experiential
Maturity
QA is formally,philosophically
integrated into thestructure and function
of the organizationor health system
QA Project 2001
Awareness
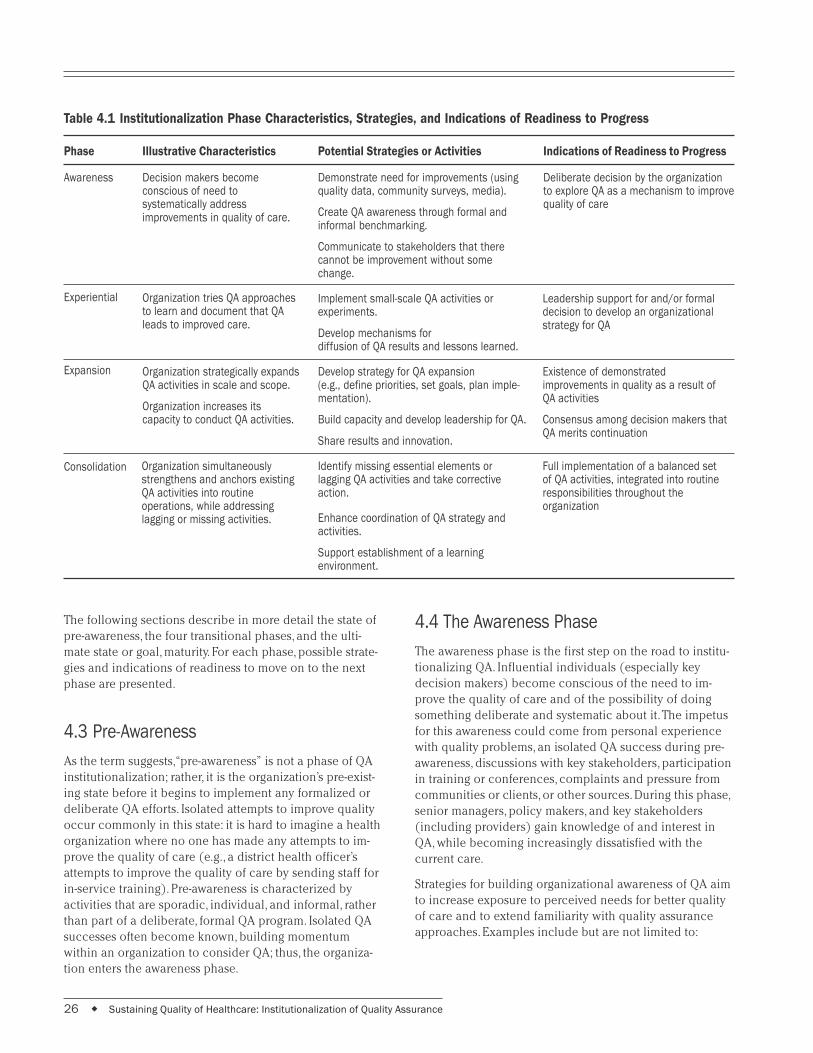
26 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Phase
Awareness
Illustrative Characteristics
Decision makers becomeconscious of need tosystematically addressimprovements in quality of care.
Potential Strategies or Activities
Demonstrate need for improvements (usingquality data, community surveys, media).
Create QA awareness through formal andinformal benchmarking.
Communicate to stakeholders that therecannot be improvement without somechange.
Implement small-scale QA activities orexperiments.
Develop mechanisms fordiffusion of QA results and lessons learned.
Develop strategy for QA expansion(e.g., define priorities, set goals, plan imple-mentation).
Build capacity and develop leadership for QA.
Share results and innovation.
Identify missing essential elements orlagging QA activities and take correctiveaction.
Enhance coordination of QA strategy andactivities.
Support establishment of a learningenvironment.
Indications of Readiness to Progress
Deliberate decision by the organizationto explore QA as a mechanism to improvequality of care
Organization tries QA approachesto learn and document that QAleads to improved care.
Experiential Leadership support for and/or formaldecision to develop an organizationalstrategy for QA
Organization strategically expandsQA activities in scale and scope.
Organization increases itscapacity to conduct QA activities.
Existence of demonstratedimprovements in quality as a result ofQA activities
Consensus among decision makers thatQA merits continuation
Expansion
Consolidation
Table 4.1 Institutionalization Phase Characteristics, Strategies, and Indications of Readiness to Progress
The following sections describe in more detail the state ofpre-awareness, the four transitional phases, and the ulti-mate state or goal, maturity. For each phase, possible strate-gies and indications of readiness to move on to the nextphase are presented.
4.3 Pre-Awareness
As the term suggests, “pre-awareness” is not a phase of QAinstitutionalization; rather, it is the organization’s pre-exist-ing state before it begins to implement any formalized ordeliberate QA efforts. Isolated attempts to improve qualityoccur commonly in this state: it is hard to imagine a healthorganization where no one has made any attempts to im-prove the quality of care (e.g., a district health officer’sattempts to improve the quality of care by sending staff forin-service training). Pre-awareness is characterized byactivities that are sporadic, individual, and informal, ratherthan part of a deliberate, formal QA program. Isolated QAsuccesses often become known, building momentumwithin an organization to consider QA; thus, the organiza-tion enters the awareness phase.
4.4 The Awareness Phase
The awareness phase is the first step on the road to institu-tionalizing QA. Influential individuals (especially keydecision makers) become conscious of the need to im-prove the quality of care and of the possibility of doingsomething deliberate and systematic about it. The impetusfor this awareness could come from personal experiencewith quality problems, an isolated QA success during pre-awareness, discussions with key stakeholders, participationin training or conferences, complaints and pressure fromcommunities or clients, or other sources. During this phase,senior managers, policy makers, and key stakeholders(including providers) gain knowledge of and interest inQA, while becoming increasingly dissatisfied with thecurrent care.
Strategies for building organizational awareness of QA aimto increase exposure to perceived needs for better qualityof care and to extend familiarity with quality assuranceapproaches. Examples include but are not limited to:
Organization simultaneouslystrengthens and anchors existingQA activities into routineoperations, while addressinglagging or missing activities.
Full implementation of a balanced setof QA activities, integrated into routineresponsibilities throughout theorganization
Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 27
◆ Using comparative data to demonstrate the need forimprovement, i.e., comparing health status indicatorsfor the population served by the organization withregional, national, or international statistics
◆ Examining and discussing a critical incident, such asan avoidable death or other tragedy in the organization
◆ Conducting formal or informal QA sensitizationsessions for a variety of stakeholders and organiza-tional leaders to introduce QA approaches in health
◆ Benchmarking (through site visits to other organiza-tions or countries) to increase awareness of “otherways of doing things” that may be more effective
◆ Assessing the level of quality to demonstrate thecurrent state of care provided by the organization
The main indication for organizational readiness to moveon to the experiential phase is the deliberate decision bythe organization or system to explore the use of QA as ameans to improve quality of care.
4.5 The Experiential Phase
This phase is characterized by the organization undertak-ing specific QA activities and trying out various QAapproaches to learn from the experience, while it developsevidence (documents results) that QA does make a differ-ence and leads to improvements in the quality of care.
Strategies of most use during the experiential phaseinclude:
◆ Implementing small-scale QA activities or experimentsto demonstrate results and “learn by doing”
◆ Documenting experiences from these small-scaleefforts in terms of results and establishing processesfor organizational learning
◆ Developing or strengthening mechanisms for thediffusion and exchange of QA experiences andknowledge
The awareness and experiential phases often overlap. Insome organizations, these phases may happen concur-rently in different parts or levels of the organization, ratherthan sequentially. The combined result of these two phasesis the organization’s decision to embrace QA as an organi-zational strategy and expand its implementation. In Malawi,awareness strategies were implemented and followed by aperiod of experimentation at nine pilot sites, but certainstakeholders still needed additional awareness to be readyto support broader organizational strategies to institution-alize QA.
At the end of the experiential phase, sufficient momentumexists for the organization to move into the expansionphase. Indications of such readiness include increasedleadership support and a formal decision to develop anorganizational strategy for QA. This decision indicates thatthe organization has enough knowledge and experiencewith QA to be convinced of its benefits and is committedto extending QA in the organization.
4.6 The Expansion Phase
As the name implies, the most obvious characteristic ofthis phase is expanding implementation of QA activities.This phase is not simply a scaling up of activities orstraightforward replication of positive results across theorganization but rather the strategic expansion of QAimplementation, based on knowledge and experiencesgained in previous phases. Expansion may be geographic,but could also be an expansion in scope (engaging inmore types of QA activities) or in coverage (covering awider range of facility types or departments). Other charac-teristics of this phase are an increasing organizationalcapacity to conduct QA activities and the development/use of a formal QA strategy that includes priorities andimplementation plans. Learning and trying new thingscontinues in the expansion phase.
Strategies of most use during the expansion phase arethose that facilitate expanded implementation, such ascapacity building in QA, diffusion of innovation and results,and leadership development. Two key indications of orga-nizational readiness to move into the consolidation phaseinclude the existence of demonstrated improvements inthe quality of care as a result of the QA strategy/activitiesand a consensus among decision makers and stakeholdersthat QA merits continuation and further consolidation.
4.7 The Consolidation Phase
The boundary between the expansion and the consolida-tion phases is a fine one. As expansion strategies are under-taken, they can precipitate or foster the need for takingstock of QA activities, ushering in a period of review, refine-ment, adjustment, and coordination. During consolidation,the organization is simultaneously strengthening and an-choring existing QA activities and programs into routineoperations, while making its QA effort more comprehen-sive by addressing lagging or missing activities.
Consolidation is thus the natural successor of expansion.For example, during the expansion phase, there may bedisproportionate emphasis on certain essential elements,

28 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
while others are neglected. Similarly, one QA activity (e.g.,setting standards) may be very successfully expanded inscope or geography, while another (e.g., measuring compli-ance) may be lacking. During consolidation, the organiza-tion seeks to initiate any previously undeveloped core QAactivities and bring the weaker essential elements up tospeed. Thus, key strategies for the consolidation phasefocus on refinement and equilibrium to ensure that allessential elements and core QA activities are fully devel-oped and scaled up throughout the organization. Consoli-dation strategies ensure the full implementation of QAplans and the continuity of the gains made during expan-sion. Indications that an organization has reached maturityare the full implementation of a balanced set of QA activi-ties covering the entire organization and integrated intothe responsibilities of all personnel.
4.8 Maturity: Sustained Quality of Careand a Culture of Quality
Maturity is not a phase, but rather a state where QA isformally and philosophically integrated into the structureand function of the organization. With maturity, QA is anintegral part of day-to-day operations at all levels. Organiza-tional values, leadership, policy, and resources reinforce aphilosophical and practical culture of quality. Other indica-
tions of maturity are the full implementation of a balancedQA plan that includes all three core QA activities (definingquality, measuring quality, and improving quality). In addi-tion, each essential element has also reached a state ofmaturity, ensuring that the organization can sustain thequality of healthcare provided.
4.9 Conclusion
QA institutionalization is a process through which an orga-nization integrates a focus on quality into how it definesitself and its mission. The preceding pages describe thevarious phases of QA institutionalization in which an orga-nization or health system might find itself. The importantorganizational elements necessary for institutionalizationalso progress through this same series of phases. Just asinstitutionalization itself is not a linear process, the devel-opment and maturation of each of the eight essential ele-ments may or may not evolve in a synchronized fashion.The overall level of QA institutionalization within an orga-nization depends on how well each of the eight essentialelements has been developed. Section 5 discusses theprocess of institutionalization for each essential elementand suggests strategies to facilitate progress through eachphase.

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 29
5 Moving towards Institutionalization:One Element at a Time
HE institutionalization of QA is a complex process,as is institutionalizing any change in how anorganization operates. The eight essential ele-
ments of QA all contribute to an organization’s ability toinstitutionalize QA, yet the degree of development of eachessential element will vary within an organization and willvary over time. Each element must go through the sameseries of transitional phases as QA institutionalizationitself: it is unlikely that an organization embarking on QAwill develop all the policies, leadership, values, structure,and support functions all at once. This section discusseshow each element can progress from its current status tomaturity, to fully contribute to the organization’s overallefforts to institutionalize QA. Just as the aggregate viewprovides guidance for overall planning and assessment,looking at each element individually provides concreteideas on how to facilitate its development.
Table 5.1 describes, for each element, the conditions thatsignal an organization’s readiness to move on to the nextphase of institutionalization. Organizations can use thistable to help gauge where they are in the continuum foreach element with respect to each phase of QA develop-ment and identify where QA institutionalization effortsshould focus next.
Table 5.2 provides an illustration of how the status of eachessential element might look for a hypothetical organiza-tion. The shading in each cell shows, at a particular pointin time, the phase that the hypothetical organization hasreached in the institutionalization process for that essentialelement. Looking at the progress of each element relativeto the others would enable the organization to understandthe extent to which its QA development is balanced andcomplete. In this example, it would be appropriate for theorganization to now focus relatively greater efforts on de-veloping the essential element of rewarding quality as itshighest priority and then to strengthen policies, core val-ues, and information and communication. With time, theorganization should reassess the strength of each element,revise the table, and act to strengthen the weakest ele-ments.
The next few pages discuss each essential element indi-vidually, describing its role in facilitating the institutional-ization of QA and how each element develops on the roadto maturity. A table suggests possible activities that an orga-nization might undertake to develop each element and
move the whole organization closer to QA institutionaliza-tion. These strategies should not be seen as prescriptive;they are illustrative and meant to encourage new ideas.The abundance of information is meant to serve as acomprehensive reference, rather than as a “how-to” manual;readers may find it useful to refer to the specific phasesand essential elements that are most relevant to them atthe moment, based on a self-assessment using Table 5.1.
5.1 Policy
Organizations have internally set policies at every level toguide organizational efforts. QA policies provide a frame-work and goals for the development of QA efforts withinan organization. They define the organization’s QAmandate and guide the setting of objectives, allocation ofresources, and implementation of activities to ensurequality healthcare.
While the essential element policy can lend vital directionto an organization’s QA efforts, the development of policystatements about QA are not necessarily effective in initiat-ing QA activities in a country. Policy statements alone,without supportive structures and staff empowered andmotivated to undertake QA, are not sufficient to makequality assurance happen. Similarly, efforts to legislate ordecree quality, without creating the conditions to under-take and sustain QA activities, are doomed. Consequently,the development of explicit national QA policies, as illus-trated in the case of Malaysia in Box 5.1, often occurs yearsafter major QA efforts are underway, thus allowing theorganization to develop policies based on its ownexperience.
It is also important to keep in mind that every healthcaresystem/organization operates in a larger national policyenvironment that may influence organizational QA effortsbut over which the organization may have little influence.For example, national health policies may constrain what aregional health office can do to implement QA. Alterna-tively, the larger policy environment can facilitate the de-velopment of QA policies. Such facilitation occurred inChile in 1989 when its newly elected democratic govern-ment made improving the population’s health status a toppriority in its social policies. This emphasis gave rise to theMinistry of Health’s quality improvement initiative in 1991(Gnecco et al. 1999).
T

30 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Phase of
Institutional-
ization
Awareness
Table 5.1 Evolution of QA Essential Elements through the Phases of Institutionalization
Essential Element
Policy
Key decision makers arewilling to allowexperimentation outsideexisting policies for learningabout QA.
Leadership
Senior decision makersapprove the start of QAexperiments.
Key leaders emerge who arewilling to support QA in theorganization.
Core Values
Key decision makers areaware of the advantages ofexplicit organizational corevalues.
Decision makers indicate awillingness to createmechanisms to reinforcecore values.
Core values that reflect aculture of quality are madeexplicit and accepted by theorganization’s leadership.
Resources for QA
Resources are allocated tosupport initial QAexperiences.
Resources are committed tofinance QA expansion costs.
Budget lines are added forQA activities or resources areallocated for QA withinexisting budgets.
Several operational andsenior managers displayleadership qualities.
Authority to expand QAactivities has been delegatedand the necessary resourcescommitted.
Consensus exists among keystakeholders and decisionmakers about theimportance of putting qualityand support for QA clearlyinto organizational policies(and any reform agendas).
Quality and QA are includedin sector reform agenda.
Policies that support QAcapacity building aredeveloped.
Policies exist that encouragemeasurement andcontinuous improvement.
Experiential
Policies supportingmeasurement andcontinuous improvementhave been written and fullycommunicated.
Resources are available andcore values are aligned withpolicies.
A critical mass exists ofoperational and seniormanagers who displayleadership qualities.
Organizational, unit, andindividual worker goals arealigned.
Staff can articulateorganizational core values.
Core values guide programdevelopment and strategicdecisions.
Realistic budgets for QAactivities are developedbased on awareness of thetrue costs of doing QA.
Decision makersdemonstrate a willingnessto consistently allocateadequate resources for QA.
Expansion
Operational and seniormanagers feel accountablefor quality, provideleadership to QA activities,and advocate for QA.
The organizationdemonstrates a sustainedcommitment of resourcesfor QA.
QA is supported throughoutthe organization at all levels.
Staff feel ownership ofresults and empowered tomake improvements incollaboration with others.
Staff and leaders’ dailyperformance reflects corevalues.
Rewards and programs are inplace to support core values.
Sufficient resources areallocated to support ongoingquality initiatives.
Estimated QA resourceneeds are incorporated intoannual operating budgets.
Consolidation
Explicit core values arereinforced by policies,rewards, and leadershipstyles.
Managers use core values toguide program developmentand their own and theirstaff’s behavior.
QA resource needs areroutinely identified,quantified, and incorporatedinto annual operatingbudgets.
Resources for QA areconsistently made available.
Organizational policiesidentify quality as an explicitgoal and QA as an importantmechanism for reaching thatgoal.
Organizational policies arefully communicated andactively used by leaders toset goals and guideimplementation.
Maturity

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 31
Phase of
Institutional-
ization
Awareness
Essential Element
Structure
Organizational leaders havedecided to further exploreQA.
Responsibility is assigned foroversight, technical support,and implementation of initialQA experiences.
Capacity Building
Key leaders, decisionmakers, and stakeholdersexpress a need for QA andare interested in exploring itfor their organization.
The organization sponsorsQA awareness or trainingevents.
The organization hassupervisors, coaches, andleaders with knowledgeand skills to support andexpand QA efforts.
Consensus exists oncapacity building strategiesfor expansion.
Information and
Communication
Key stakeholders arecommitted to exploring QA.
Information about problemswith quality of care andpossible approaches toimprove quality isdisseminated within theorganization.
Those experimenting withQA regularly document theiractivities and share thisinformation with others,both inside and outside theorganization.
Rewarding Quality
The organization’sleadership recognizes theneed to develop mechanismsor processes for rewardingquality work and QA effortsamong staff.
Managers understand whatimpedes quality work andwhat motivates workers andteams to pursue quality.
Incentive packages tomotivate quality work aredeveloped and tested.
Leaders recognize theneed for clear oversight,coordination, andaccountability for QAexpansion.
Consensus exists withinthe organization as toappropriate and effectivestructures for QA expansion.
Experiential
Responsibility for QAactivities is formally assignedwithin the organization.
QA strategies are refinedbased on an assessment ofQA “structure.”
Mechanisms and systemsare established for routinedocumentation and sharingof results and lessonslearned.
Documentation informationis continually used for QAadvocacy.
Organizational leadersexpress commitment torewarding quality.
Incentive packages thatpassed testing are in place.
Staff are knowledgeableabout incentive andperformance managementsystems.
Staff believe that rewardsystems are fair andmeaningful.
Mechanisms exist forcommunity input into thereward/incentive package.
There is a critical mass ofcompetent staff to supportongoing QA efforts.
Leaders and managersmodel QA values andprocesses.
All staff can accuratelydescribe their ownresponsibilities to contributeto quality of care.
QA content is integrated intoother training curricula.
A mechanism exists tosustain a critical mass ofQA expertise within theorganization.
Systems for documentation,sharing, and advocacyoperate routinely.
Expansion
Consolidation
QA is integrated into jobdescriptions.
Roles, responsibilities, andaccountability for QA areclearly delineated andoperational.
Mechanisms exist for regulardocumentation and sharingof experiences.
Information aboutimprovement areas andbetter practices is used fordecision making at policyand operational levels.
QA capacity building isintegrated into pre-serviceand continuing educationand supported continuouslyby coaching, mentoring,and supervision.
Formal or systematicprocesses exist forrecognizing staff andmanagers who performhigh quality work.
Incentive systems thatreward continuousimprovement are integratedinto the personnel system.
Maturity
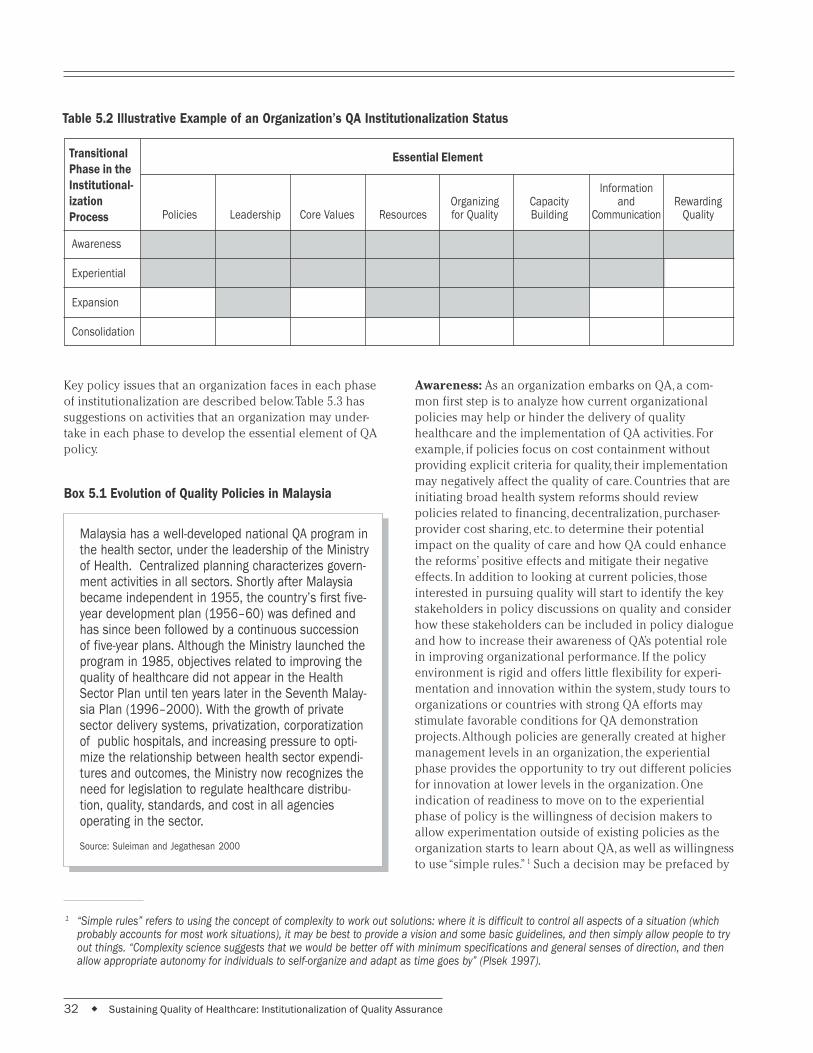
32 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Box 5.1 Evolution of Quality Policies in Malaysia
Malaysia has a well-developed national QA program inthe health sector, under the leadership of the Ministryof Health. Centralized planning characterizes govern-ment activities in all sectors. Shortly after Malaysiabecame independent in 1955, the country’s first five-year development plan (1956–60) was defined andhas since been followed by a continuous successionof five-year plans. Although the Ministry launched theprogram in 1985, objectives related to improving thequality of healthcare did not appear in the HealthSector Plan until ten years later in the Seventh Malay-sia Plan (1996–2000). With the growth of privatesector delivery systems, privatization, corporatizationof public hospitals, and increasing pressure to opti-mize the relationship between health sector expendi-tures and outcomes, the Ministry now recognizes theneed for legislation to regulate healthcare distribu-tion, quality, standards, and cost in all agenciesoperating in the sector.
Source: Suleiman and Jegathesan 2000
Table 5.2 Illustrative Example of an Organization’s QA Institutionalization Status
InformationOrganizing Capacity and Rewarding
Policies Leadership Core Values Resources for Quality Building Communication Quality
Awareness
Experiential
Expansion
Consolidation
Key policy issues that an organization faces in each phaseof institutionalization are described below. Table 5.3 hassuggestions on activities that an organization may under-take in each phase to develop the essential element of QApolicy.
Transitional
Phase in the
Institutional-
ization
Process
Essential Element
Awareness: As an organization embarks on QA, a com-mon first step is to analyze how current organizationalpolicies may help or hinder the delivery of qualityhealthcare and the implementation of QA activities. Forexample, if policies focus on cost containment withoutproviding explicit criteria for quality, their implementationmay negatively affect the quality of care. Countries that areinitiating broad health system reforms should reviewpolicies related to financing, decentralization, purchaser-provider cost sharing, etc. to determine their potentialimpact on the quality of care and how QA could enhancethe reforms’ positive effects and mitigate their negativeeffects. In addition to looking at current policies, thoseinterested in pursuing quality will start to identify the keystakeholders in policy discussions on quality and considerhow these stakeholders can be included in policy dialogueand how to increase their awareness of QA’s potential rolein improving organizational performance. If the policyenvironment is rigid and offers little flexibility for experi-mentation and innovation within the system, study tours toorganizations or countries with strong QA efforts maystimulate favorable conditions for QA demonstrationprojects. Although policies are generally created at highermanagement levels in an organization, the experientialphase provides the opportunity to try out different policiesfor innovation at lower levels in the organization. Oneindication of readiness to move on to the experientialphase of policy is the willingness of decision makers toallow experimentation outside of existing policies as theorganization starts to learn about QA, as well as willingnessto use “simple rules.” 1 Such a decision may be prefaced by
1 “Simple rules” refers to using the concept of complexity to work out solutions: where it is difficult to control all aspects of a situation (whichprobably accounts for most work situations), it may be best to provide a vision and some basic guidelines, and then simply allow people to tryout things. “Complexity science suggests that we would be better off with minimum specifications and general senses of direction, and thenallow appropriate autonomy for individuals to self-organize and adapt as time goes by” (Plsek 1997).

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 33
discussions with various stakeholders (leaders, providers,clients, and communities) about the kinds of policiesneeded to support core values and advance quality initia-tives.
Table 5.3 Possible Activities to Develop the
Essential Element Policy and
Move to the Next Phase/State
Awareness Analyze existing health policies in terms ofaddressing quality and supporting or constraining QA
Assess impact of proposed healthcare reforms onquality
Review and catalog existing quality standards toidentify gaps
Visit other organizations/countries to study their QApolicies
Convene stakeholders to elicit their perspectiveson quality and generate consensus on the need toinclude quality within organizational policy
Develop standards for priority areas where clearperformance expectations are lacking
Disseminate and discuss findings from analysis (fromawareness phase) of the impact of existing policieson healthcare quality; make recommendations foramending or changing policies that hinder quality
Develop an ongoing mechanism for reviewing newpolicies and analyzing impact on healthcare qualityand QA activities prior to their approval
Review human resource policy for impact on qualityof healthcare services
Analyze staffing patterns to delineate feasible,realistic QA implementation plan
Set up a process to update or adapt existingstandards and assess the need for new standardsand related indicators for monitoring the quality oforganizational performance (in terms of healthcareresults)
Implement communication plan to inform allstakeholders of policy
Refine existing QA written policy and institutemechanism to assure regular review/updating
Review policy to assure that it is addressingresources for QA; amend if needed
Analyze resources (human and financial) needed forsupporting QA
Experiential
Expansion
Consolidation
Experiential: During the experiential phase, the content ofpolicies is often built from the bottom up, based on localexperiences and needs to support QA implementation andimprovements in the quality of care. For example, a qualitypolicy or plan developed by a pilot region might serve as amodel for the development of a national quality policy. Keyindications of readiness to move on include consensusamong key stakeholders and decision makers in the orga-nization about the importance of putting quality and sup-port for QA clearly into organizational policies and intoany reform agendas.
Expansion: As an organization moves towards expansion,the need for more specific, operational policies increases.With expansion comes increased scope and coverage ofQA activities. This requires clarity but also flexibility in theimplementation and delegation of authority to makeimprovements. During this phase, the organization maymodify existing policies that hinder quality (or causedisincentives for quality). The organization may need todevelop policies related to capacity building, communica-tion, and rewards that support core values. In particular, ifthe organization is involved with health sector reform,organizational leaders can ensure that quality and QA areincluded in reform policies and plans. A key indication ofreadiness for consolidation in the policy arena is the pres-ence of policies encouraging measurement and continu-ous improvement.
Consolidation: As the organization moves into consolida-tion, it is important to review policies and their impact onstaff’s sense of direction, motivation, and ability to perform.This is also the time to ensure that mechanisms are inplace to regularly review policies and to make changes asneeded to maintain the quality of care. During consolida-tion, increasing alignment between formal and informalpolices takes place, especially with regard to desiredresults, core values, and mechanisms to implement QA.Indications of moving to maturity include the existence ofa written QA policy that is widely communicated through-out the organization, leadership support for QA policy, andalignment of resources and core values with policies.
Maturity: An organization that has reached the state ofpolicy maturity has specific policies supporting qualityhealthcare as an explicit goal of organizational perfor-mance and QA as an important mechanism for reachingthat goal. In addition, these policies are fully communi-cated throughout the organization and to stakeholders.
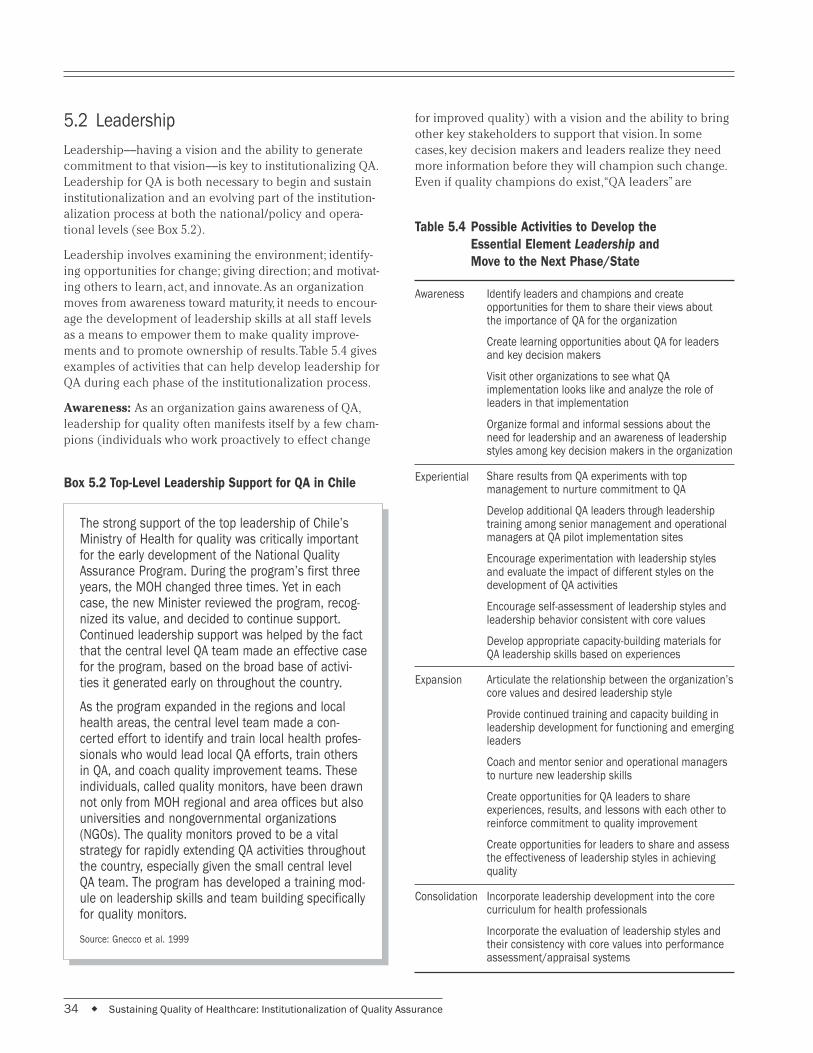
34 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
5.2 Leadership
Leadership––having a vision and the ability to generatecommitment to that vision––is key to institutionalizing QA.Leadership for QA is both necessary to begin and sustaininstitutionalization and an evolving part of the institution-alization process at both the national/policy and opera-tional levels (see Box 5.2).
Leadership involves examining the environment; identify-ing opportunities for change; giving direction; and motivat-ing others to learn, act, and innovate. As an organizationmoves from awareness toward maturity, it needs to encour-age the development of leadership skills at all staff levelsas a means to empower them to make quality improve-ments and to promote ownership of results. Table 5.4 givesexamples of activities that can help develop leadership forQA during each phase of the institutionalization process.
Awareness: As an organization gains awareness of QA,leadership for quality often manifests itself by a few cham-pions (individuals who work proactively to effect change
Box 5.2 Top-Level Leadership Support for QA in Chile
The strong support of the top leadership of Chile’sMinistry of Health for quality was critically importantfor the early development of the National QualityAssurance Program. During the program’s first threeyears, the MOH changed three times. Yet in eachcase, the new Minister reviewed the program, recog-nized its value, and decided to continue support.Continued leadership support was helped by the factthat the central level QA team made an effective casefor the program, based on the broad base of activi-ties it generated early on throughout the country.
As the program expanded in the regions and localhealth areas, the central level team made a con-certed effort to identify and train local health profes-sionals who would lead local QA efforts, train othersin QA, and coach quality improvement teams. Theseindividuals, called quality monitors, have been drawnnot only from MOH regional and area offices but alsouniversities and nongovernmental organizations(NGOs). The quality monitors proved to be a vitalstrategy for rapidly extending QA activities throughoutthe country, especially given the small central levelQA team. The program has developed a training mod-ule on leadership skills and team building specificallyfor quality monitors.
Source: Gnecco et al. 1999
Table 5.4 Possible Activities to Develop the
Essential Element Leadership and
Move to the Next Phase/State
Awareness
Experiential
Expansion
Consolidation
Identify leaders and champions and createopportunities for them to share their views aboutthe importance of QA for the organization
Create learning opportunities about QA for leadersand key decision makers
Visit other organizations to see what QAimplementation looks like and analyze the role ofleaders in that implementation
Organize formal and informal sessions about theneed for leadership and an awareness of leadershipstyles among key decision makers in the organization
Share results from QA experiments with topmanagement to nurture commitment to QA
Develop additional QA leaders through leadershiptraining among senior management and operationalmanagers at QA pilot implementation sites
Encourage experimentation with leadership stylesand evaluate the impact of different styles on thedevelopment of QA activities
Encourage self-assessment of leadership styles andleadership behavior consistent with core values
Develop appropriate capacity-building materials forQA leadership skills based on experiences
Articulate the relationship between the organization’score values and desired leadership style
Provide continued training and capacity building inleadership development for functioning and emergingleaders
Coach and mentor senior and operational managersto nurture new leadership skills
Create opportunities for QA leaders to shareexperiences, results, and lessons with each other toreinforce commitment to quality improvement
Create opportunities for leaders to share and assessthe effectiveness of leadership styles in achievingquality
Incorporate leadership development into the corecurriculum for health professionals
Incorporate the evaluation of leadership styles andtheir consistency with core values into performanceassessment/appraisal systems
for improved quality) with a vision and the ability to bringother key stakeholders to support that vision. In somecases, key decision makers and leaders realize they needmore information before they will champion such change.Even if quality champions do exist, “QA leaders” are

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 35
needed throughout the organization to begin institutional-izing QA. Thus, an important set of activities during theawareness phase is to generate awareness of what leader-ship is, why it is important, and how it can be further devel-oped. Indications of leadership readiness to move on tothe experiential phase include the existence of several keyleaders (beyond the initial champions) willing to supportQA in the organization and the approval of senior decisionmakers to start experimental QA activities.
Experiential: During the experiential phase, leaders sup-port staff who are implementing QA by facilitating identifi-cation of opportunities for improvement, providingguidance and feedback, ensuring the flexibility for innova-tion, and rewarding achievements (demonstrated results).At the same time, these QA experiences offer opportunitiesto develop leadership skills and new QA leaders. Suchleadership development might include skills in changemanagement, exploring how current management/leader-ship styles inhibit or facilitate the achievement of quality,working with/empowering teams, and strategic planning.The experiential phase also provides an excellent opportu-nity to experiment with different leadership and manage-ment styles even while trying out various technicalcomponents of QA. Indications of readiness to move on tothe expansion phase include a growing number of indi-viduals at the operational and senior management levelswho display leadership qualities, are aware of leadershipstyles, and delegate authority for quality improvements.
Expansion: During expansion, leadership is critical toarticulate and communicate the quality vision the organi-zation is trying to achieve and to motivate more of theorganization to move towards that vision. Thus, not onlymust leadership continually support expansion, but thenumber of leaders must continually expand as well. Train-ing and cross-fertilization among managers is especiallyimportant during this phase. Training in leadership skillswill broaden to new areas of expansion (geographical,scope, etc.) and focus heavily on change management andalignment with core values as increasing parts of the orga-nization take on new roles related to QA. Cross-fertilizationcan be achieved through the creation of communicationopportunities for leaders to share and assess theirstrategies to support and inspire quality improvement.Indications of readiness to move on to consolidation are asignificant portion of managers throughout the organiza-tion who display leadership qualities and the increasingalignment of organization, unit, and individual workergoals.
Consolidation: Creating an ongoing pool of leaders whocan support QA efforts over time can be achieved by incor-porating leadership development into core curricula athealth professional training institutions. During this phase,
leaders continue to model behaviors and practice qualitymanagement, inspiring others to become leaders in qualityhealthcare. They help assess how well the organization isachieving its quality goals and have developed the habit oflooking for changes needed in strategies for QA implemen-tation. Indications of readiness to move forward to leader-ship maturity include the presence throughout theorganization of senior and operational managers who feelaccountable for quality within their area of responsibility,who advocate QA, and who ensure continued commitmentof resources for QA. Management accountability wouldalso be reflected in staff accountability for quality.
Maturity: In an organization that has reached maturity, acritical mass of leaders exists who embrace a quality cul-ture. The vision and commitment to quality endure, despiteturnover among managers or decision makers, becausestaff feel ownership of organizational results (quality ofcare) and feel motivated to make improvements to achievedesired results.
5.3 Core Values
Every organization has values that are reflected in organi-zational behavior. While many organizations do not haveexplicitly formulated core values, implicit organizationalvalues influence management decisions, management-staffinteraction, and provider-client interaction. For QA to trulyspread and become integrated into the structure and func-tioning of an organization, organizational values mustfoster attention to the needs of the client and facilitateefforts to make improvements in the way things are doneto improve quality. As seen in the case of Malaysia (seeBox 5.3), core values provide a very important foundationfor the institutionalization of QA by promoting a positivework culture that emphasizes quality. Positive core valuesbecome a source of pride and a guide to action when theyare explicit (i.e., written and communicated) and are rein-forced by policies, rewards, and leadership styles. Althoughthe core values in an organization that has institutional-ized QA may vary from one place or culture to another,there will be striking similarities between them: teamwork,trust and respect, support of learning, and openness tochange. Table 5.5 suggests activities that may be appropri-ate to help an organization develop core values to supportquality at each phase of institutionalization.
Awareness: A key to developing organizational values thatcan foster improvements in quality is the examination ofcurrent organizational values, whether implicit or explicit.Are they in alignment or in conflict with those necessaryfor achieving high quality care and the implementation ofQA? Formal exercises to examine organizational valuesand compare them with those of other organizations that

36 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Box 5.3 Corporate Culture Building in Malaysia
In 1991, Malaysia’s Ministry of Health embarked ona formal national effort at building a culture of excel-lence and quality, spurred by a general governmentmovement and led by the Prime Minister, to create a“culture of work excellence” in the public sector. Afterstudying factors underlying the success of variouscorporations, the MOH leadership recognized that aprerequisite for a quality-mature organization is tohave a vision and mission that describe theorganization’s goals and objectives. The followingstatement was developed:
“The Vision is of a nation of healthy individuals,families and communities enjoying an enhancedquality of life. In its corporate Mission, the Ministry ofHealth strives to provide quality health care to all ofits customers through high Quality services,continuing education and research.”
Three core values related to this statement were thenidentified: caring services, teamwork, and profession-alism. Various means were used to communicatethese values and inculcate them in both professionaland nonprofessional staff, including special trainingmodules on core values and reinforcement of theconcept of a quality culture at all opportunities wherestaff met with senior management, such as atassemblies and meetings. Pledges, wearing ofuniforms, and singing of quality-related anthems arealso widely practiced.
The national quality evaluation, conducted in 1997,found that staff knowledge of the core values wasgood, especially among the professional group andthat the main sources of information about the corevalues of the MOH were meetings and briefings. Themajority of staff said that they believed the initiativehad helped them to improve the quality of their workand patient satisfaction.
Source: Suleiman and Jegathesan 2000.
have embraced a culture of quality may be useful, aswould be other efforts to raise leadership’s awareness ofthe benefits of defining and communicating quality values.Indications of readiness to move on include key stakehold-ers, especially decision makers, who are aware of the ad-vantages of explicit core values and of their importance toQA and who are willing to facilitate the formulation andreinforcement of core values.
Experiential: During the experiential phase, an organiza-tion needs to develop mechanisms to facilitate the inter-nalization of core values. This could be done within thecontext of teams that are working on QA experiences (e.g.,quality improvement, standards development, monitoringof quality), which will become microcosms for developingand testing positive core values. They can then demon-strate the kinds of results (organizational behavior) thatemerge from these values. The range of values examinedshould reflect the various levels of interpersonal interac-tions: management-staff, staff-clients, and staff/manage-ment-community. One indication of core value readiness tomove onto the expansion phase is the presence of an ini-tial set of explicit core values that reflect a culture of qual-ity and are accepted by leadership.
Expansion: During this phase, the challenge is to broadenexposure to the newly developed core values amongmembers of the organization and to reward behaviors thatreflect those values. Managers and leaders need to discusscore values with staff and explain how these values influ-ence daily work. One mechanism to reinforce core valuesis their inclusion in formal performance appraisals, i.e., toevaluate how well individual behavior and performancereflect such values. This is also valid for performanceappraisals at the organizational level: How well has theorganization met the needs and expectations of its clients?Indications of readiness to move on to consolidation arethat a large number of staff can articulate theorganization’s core values and that these values guideprogram development and strategic decisions.
Consolidation: During the consolidation phase, a systemmust be developed to assure that organizational standardsand priorities are based on and continually aligned withcore values supporting both high quality healthcare andQA implementation. Indications for readiness to move onto the state of maturity include leaders, staff, and stakehold-ers who can articulate organizational values and whosedaily performance reflects those values. In addition,rewards and other programs that support the core valuesare in place.
Maturity: Maturity is reached when the organization hasexplicit core values that reflect multiple dimensions ofquality and when those values are aligned with efforts forquality improvement. Leaders and managers use theorganization’s core values as the foundation for programdevelopment and to guide their own behavior, and staffthroughout the organization are conscious of the corevalues and apply them in their daily work. Incentive pro-grams express the organization’s recognition that values-based performance contributes to its worth. Disincentivesto such performance are continuously sought out andeliminated.

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 37
Initiate discussion with key policy makers andstakeholders about the importance of core valuesand the kinds of core values that the organizationmight want to consider adopting
Study or visit organizations that have successfulQA programs and study their core values
Develop a plan to work with quality teams toformulate relevant core values, as pertinent to thesuccessful institutionalization of their work
Write out core values and discuss them with healthpersonnel, clients, and other stakeholders
Promote information sharing and education aboutexplicit core values for all staff and organizationalunits
Facilitate inclusion of core values in policystatements, performance systems, etc. and reinforcethem at every opportunity (staff meetings, trainings,ceremonies, etc.)
Assess barriers to change and develop strategies toreduce resistance and overcome barriers
Assess organizational units and staff to verify whetherthey are aware of the organization’s core values andapply them in daily work
Work with human resources and policy makers toincorporate core values into job descriptions andperformance assessments
Eliminate any remaining disincentives that preventthe organization’s core values from being reflected inevery staff member’s daily work
Table 5.5 Possible Activities to Develop the
Essential Element Core Values and
Move to the Next Phase/State
Awareness
Experiential
Expansion
Consolidation
5.4 Resources for QA
When an organization has institutionalized QA, theresources necessary to optimize quality (within the fiscalconstraints of the organization) are available. Althoughallocation of some resources for QA is essential for itsinstitutionalization, it is how the organizational leadersmake use of these resources—rather than the level ofresources—that drives the institutionalization process.Resource requirements for QA will vary as the organizationgoes through the various stages of institutionalization, as avariety of investments is needed to reach maturity (e.g.,capacity building, experimentation, and the time oforganizational leaders to support the institutionalizationprocess), and the magnitude of these investments changesover time.
An important issue during institutionalization is the sourceof resources for QA. QA programs that are entirely depen-dent on donor resources tend to contract after outsidefunding ends. Committing the organization’s own resourcesfor QA activities by incorporating funding for QA intooperating budgets is thus a key milestone on the road toinstitutionalization. Box 5.4 describes how the ChileanMOH addressed this problem with its national quality as-surance program. Table 5.6 suggests other ways to ensurethat adequate resources are available for QA at each phaseof institutionalization.
Awareness: Senior healthcare decision makers maybelieve that improvements in quality are unaffordable,because they see advanced technology as the most prom-ising source of improvement. In fact, QA can lead to manyimprovements in clinical and organizational quality with-out necessarily using more resources. It commonly savesmoney or reduces costs through the elimination of errors,duplication, and inefficiency. Initiating QA activities willrequire some additional resources, but the actual costsrelated to QA will depend on how much staff time is freefor such endeavors and how much capacity for QA alreadyexists in the organization. In the awareness phase, re-sources are needed for capacity building, advocacy andcommunication, and learning about what others havedone. During this phase, it is useful to hold discussionswith leaders, decision makers, and stakeholders regardingthe costs (and savings) of QA, as well as exploring the linkbetween policies supporting QA and resource allocation.Indications of readiness to move on to the next phaseinclude allocation of resources to support initial QAexperiences.
Experiential: Resources needed for the experientialphase include capacity building efforts, time for staff towork on QA activities and documentation, and resourcesfor measuring results, as well as resources to support anyQA structures (oversight and coordination) in place.Resource use for this phase should be evaluated forestimating future costs of QA activities, costs related toimprovements, and cost savings related to demonstratedresults. Indications of readiness to move to expansioninclude readiness to add budget lines for QA activities orallocation of existing budgets to QA and the investmentcosts of expansion.
Expansion: Resource needs in the expansion phaseinclude capacity building, communication mechanisms,reward systems, and leadership development. Many ofthese expansion costs are related to initial investment, sothey will be reduced over time. For example, the allocationfor QA capacity building will decline as it becomes

38 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Box 5.4 Sustaining the Funding Base for
QA Activities in Chile
The MOH of Chile initiated its national qualityassurance program in 1991, supported by a two-year grant from USAID. A team of four central levelstaff was designated to direct the program, provideQA training, and initiate quality improvement activi-ties in the health regions and areas. Yet the fourmembers of the central team realized that theywere too few to provide the level of coaching andtraining needed to support QA implementation inthe country’s 29 health areas. They soon adopteda strategy of stimulating the creation of localquality committees to direct all QA activities andtrain local quality monitors to provide hands-ontechnical support.
In 1993, when external funding ceased, the MOHshifted funding for the central team’s salaries,travel expenses, and other direct costs to itsregular budget. The MOH decided that all othercosts of QA training and implementation, includingtraining materials, participant travel, and per diemexpenses, would be borne by the health regionsand areas themselves, out of their decentralizedoperating budgets. A 1999 study found that thehealth areas were allocating an amount totalingUS$ 85,000 (around US$ 3,000 per health area)to support QA efforts. In addition, over 500 qualitymonitors were volunteering technical support.
In 1996, budget cuts led the MOH to reducestaffing of the central QA team to one full-timeprofessional, who works closely with the heads ofmajor technical programs and units in the MOH todevelop quality standards and monitoring tools thatare implemented throughout the country.
Sources: Gnecco et al. 1999; Legros et al. 2000
integrated into pre-service curricula, ongoing coaching,and supervision. Throughout this phase, it is especiallyimportant to document costs and cost savings related toQA activities, as such information is needed for both plan-ning and advocacy purposes. Indications of readiness tomove on include adequate allocation of resources for QAactivities in the expansion phase, budgets for QA activities,and awareness among decision makers of the true costs ofdoing QA.
Consolidation: A system for monitoring QA implementa-tion costs should be refined and fully functioning in order
to assure that resources allocated for QA are efficientlyand appropriately used. During this phase, more attentionis directed to process improvements to save costs. A moni-toring system should thus be in place to capture cost sav-ings as well as expenditures. The ability to document andanalyze costs with effectiveness measures or costs withoutcome improvements is increasingly important as moreQA resources are budgeted for sustaining quality care. Anindication that the organization is moving toward maturityis the availability of sufficient resources to support ongo-ing quality initiatives and the explicit incorporation ofthese resources for quality in the annual operating budget.
Table 5.6 Possible Activities to Develop the
Essential Element Resources for QA and
Move to the Next Phase/State
Awareness
Experiential
Expansion
Consolidation
Present examples to stakeholders and policy makersof the costs of poor quality and the potential costsavings through reduction of waste or inefficiency, aswell as QA implementation costs
Document existing resource allocations for QA
Identify existing policies that support or could beused to support resources (human, material, andfinancial) for QA
Try out different approaches to measuring the costsand savings of QA activities
Analyze broad staffing requirements and staff timeneeded to implement QA activities
Set up an expenditure tracking system for all QAmaterial investments
Based on results from trial costing methods, expandtheir implementation
Analyze staffing requirements to implementexpanded QA activities
Identify capacity building needed to enable staff toundertake expanded QA
Identify sources for additional staff or expertise
Identify resource needs for new QA activities beingimplemented (e.g., adding self-assessment ormonitoring of performance according to standards,after having developed standards)
Refine the cost-monitoring system for capturing QAexpenditures as well as cost savings
Develop annual and long-term human resourcesplans to address staffing requirements to undertakeand sustain expanded QA
Broker partnerships or intersectoral collaborations asadditional resources to sustain QA activities

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 39
Maturity: As QA becomes a “way of doing business,” cer-tain costs will be reduced. Nevertheless, for QA to be fullyinstitutionalization, resources to support quality initiativesmust be routinely identified, quantified, and incorporatedinto annual operating budgets.
5.5 Organizing for Quality: Creating aStructure for QA Implementation
As Chapter 3 points out, organizing for quality refers to thecreation of structures or mechanisms to provide oversight,coordination, and technical support for QA and to imple-ment QA activities. No single QA structure or organizationis appropriate for all organizations; rather, each organiza-tion must define the structure that best meets its needs andsituation. Regardless of what the structure looks like, whenQA is fully institutionalized, the oversight, coordinationand support, and implementation functions will be inte-grated into the job descriptions and behaviors of staffthroughout the organization. At such point, roles and re-sponsibilities for QA, as well as accountability for qualityof care, are clearly delineated for all staff, so that continualimprovements are made to meet the needs of clients.
Organizing for quality is both a goal and a means to thatgoal, and in this light, it must be flexible over time, as staffbecome increasingly accountable for the quality of theirwork and their quality assurance efforts. The QA structuresthat are developed will change as the organization pro-ceeds through the various phases of institutionalization, asthe organization’s needs, capabilities, and staff change anddevelop. Box 5.5 describes the creation of QA structures inMalaysia, and Table 5.7 identifies steps to facilitate thedevelopment of this essential element through the phasesof institutionalization.
Awareness: During awareness, two types of activitiesrelated to QA structure are taking place: (a) raising aware-ness of the need to structure or organize for quality, and(b) building structures to facilitate awareness of the needfor quality care and for QA. Although a single individual orsmall group may initially champion QA awareness activi-ties, involvement of a wider group of stakeholders willfacilitate commitment over time. At this stage, these con-cerned stakeholders can be an informal group or a formaltask force. Their role is to provide oversight and coordinatevarious communication and capacity-building activities.
Stakeholders should realize that the need for structuredoes not necessarily mean that a vertical program must becreated; furthermore, the appropriate structure for qualitywill probably change over time. The awareness phase isalso a good time to examine other structural changes or
Box 5.5 Structures to Support and Implement
QA in Malaysia
The MOH of Malaysia began experimenting withstructures to assure quality even before the creationof a formal QA program. Quality control circles wereintroduced throughout the civil service in the early1980s. When the national QA program was launchedin 1985, a national level steering committee wasestablished for the program. All service divisions andtechnical programs within the MOH eventually devel-oped their own QA program committees on a stag-gered basis. Also, each state and district has createda QA committee, as have many hospitals. The hospi-tal and district QA committees develop standards andundertake quality initiatives to address locally identi-fied areas of concern. Lastly, quality control circles—problem-solving teams of 6–10 workers from thesame unit or facility—are widespread in the Ministry.
Source: Suleiman and Jegathesan 2000
reforms that may be occurring in the health sector, such asdecentralization. QA can be built into such health sectorchanges, and appropriate opportunities to do so may ariseat this point. A key indication of readiness to move to thenext phase is that organizational leaders have decided tofurther explore QA and have assigned responsibility forimplementation, technical support, and oversight of pilotQA experiences.
Experiential: This phase presents two structural issues:creating structures to facilitate experimentation with QAand trying out various possible ways to organize for quality.Assigning responsibility for QA implementation, coordina-tion of experiential activities, and oversight becomes moreurgent as the organization experiments with QA. As QAtechnical activities are implemented experimentally on asmall scale, the various roles and responsibilities for QA atthe local levels, as well as mechanisms for coordinationand accountability for results, can be explored. Such explo-ration may be done through the structures establishedduring the awareness phase, but these structures will likelybecome larger and more inclusive in this phase. Expansionof stakeholder involvement ensures support for the initialQA experiences and for establishing a learning environ-ment.
In this phase, it becomes even more important to under-stand the relationship of QA efforts to other organizationalchanges that may be occurring in the health sector. Under-standing those relationships will help QA champions find

40 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
opportunities to integrate QA into other managerialresponsibilities at both the central and local levels, ratherthan creating separate organizational structures.
A key indication of readiness to expand QA structures andefforts is the explicit recognition of the need for clearoversight, coordination, responsibility, and accountabilityfor the expansion of QA implementation. By the time anorganization is ready to move on to expansion, an appro-priate and effective structure for QA within the organiza-tion is clear.
Expansion: As an organization moves into the expansionphase, the manner of organizing for quality becomesexplicit, with clear delineation of structure at all levels.Decisions made during this phase about structure for QAimplementation have implications for other essential ele-ments because the expansion requires a concerted effortto build QA capacity, broaden communication, refinereward systems, and strengthen leadership to support abroader, larger-scale implementation of QA. In many cases,expansion of QA may require short-term assignment ofindividuals solely devoted to carrying out the supportivefunctions for expanding QA implementation. At the sametime, the need continues for a clear assignment of techni-cal oversight and leadership, stakeholder involvement, andcoordination of QA activities throughout the organization.
During expansion, the long-term vision of QA roles, respon-sibilities, and accountability among all staff in the organi-zation becomes more fully developed. This includesdesigning staff performance measures that reflect their QAinvolvement and responsibilities, and orienting staff tothose roles. As time goes on, the effectiveness of the struc-tures for ensuring ongoing use of information for decisionmaking, involving stakeholders, and getting results shouldbe evaluated. A key indication of readiness for consolida-tion is the formal assignment of QA activities and responsi-bilities within the organization. Another indication isconducting a formal assessment of the QA structure torefine QA strategies.
Consolidation: As the organization moves towardsconsolidation of structure, people feel increasinglyaccountable for organizational goals. The need for an arrayof individuals solely responsible for QA activities willdiminish, because in this phase, QA is part of daily opera-tions, the “way things get done.” However, there will becontinuing need for oversight, coordination, and ensuringa learning environment related to QA. The QA structureundergoes refinements or modifications based on experi-ence and assessment. During this phase, mechanisms arefully implemented to ensure that all staff receive trainingand orientation to their QA roles, responsibilities, and new
Identify key stakeholders to participate in initialQA awareness activities
Create a working group or task force to provideoversight of QA awareness activities in theorganization
Visit other organizations to see how they haveorganized themselves to implement quality assuranceactivities
Develop consensus on appropriate structures to tryas the organization embarks on experiences with QAimplementation
Examine broader health system or organizationalreforms to see where QA could be integrated
Test out different models for organizing at theoperational level
Advocate the need for clear oversight, coordination,implementation, and accountability for QA
Review how well the structure for oversight andcoordination is working
Ensure adequate information sharing withstakeholders
Develop consensus on appropriate structures forexpansion
Outline the structural elements at all levels as partof the strategic plan for QA implementation
Delineate and communicate specific QA roles andresponsibilities for all staff
Outline staff performance measures that include orreflect involvement in QA
Ensure adequate orientation and capacity buildingfor new roles and responsibilities at all levels (and foroversight, coordination, and implementation)
Assess the effectiveness of QA structures at all levelsof the organization
Refine or modify QA structures in light ofassessments of how well they facilitate achievingquality care
Continue to work with staff on change managementand communicating their roles and responsibilities
Reinforce roles and responsibilities through rewardsand recognition
Ensure that QA responsibilities are incorporated intoall job descriptions
Table 5.7 Possible Activities to Develop the
Essential Element QA Structure and
Move to the Next Phase/State
Awareness
Experiential
Expansion
Consolidation

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 41
QA techniques and approaches. All staff have QAresponsibilities, and as such, QA training is inte-grated with general training and orientation forany position. An indication that the organizationis moving toward structural maturity is that eachstaff member can accurately describe his or herresponsibilities for achieving quality care.
Maturity: Maturity finds less need for specificvertical or other structures to support QA. How-ever, some independent structures may still havea role, as certain functions—such as QA over-sight and coordination within the organizationand with outside stakeholders––remain promi-nent, even at maturity. Thus, the evolution of theQA structure reflects the increasing integrationof quality into the daily operations of the organi-zation. Nonetheless, even in maturity, the QAstructure may continue to change, responding tochanges in the environment and vision of theorganization.
5.6 Capacity Building
Capacity building plays a very important role infacilitating the institutionalization of QA by en-suring knowledge and skill development in thetechnical implementation (standards develop-ment, process improvement, etc.) and manage-ment (leadership, planning, monitoring, etc.) ofQA activities. Expansion and consolidationrequire a critical mass of QA expertise, and orga-nizations may use many different strategies tobuild and sustain this capacity. Box 5.6 describesthe challenges Zambia has faced in building andsustaining QA capacity. Table 5.8 lists activitiesthat may strengthen QA capacity building ateach stage of institutionalization.
Awareness: To raise awareness among key deci-sion makers about QA as a general strategy toimprove quality of care, capacity building activi-ties focus on providing knowledge about qualityand QA. Such activities may even include sitevisits or study tours to other organizations thathave already implemented QA. The key to capac-ity building during QA awareness is to preparethe ground for change by identifying problemswith the current situation and effective, feasiblealternatives that could be implemented. A keyindication that awareness has been achieved is
Box 5.6 The Changing Challenges of Capacity Building in Zambia
In the early 1990s, Zambia’s political and health sector reformsfocused on improving the quality of healthcare. The health min-istry became aware of QA during an international conferenceand made the commitment to explore QA. Two senior staff weresent for special QA training and study tours; in 1993, these staffconstituted the QA Unit within the Health Reforms Implementa-tion Team. The unit developed sensitization materials—fordistrict and provincial staff—to foster awareness about problemswith quality of care and the need to address client needs. Theunit quickly realized they could not be the sole entity dissemi-nating this information and began encouraging district andprovincial staff to use these materials to more broadly conductsensitization training. They also soon recognized that a singleexposure to QA sensitization materials could not build anindividual’s capacity to guide healthcare improvements at thefacility level. They developed consensus around a comprehen-sive training and mentoring plan that included awareness,standards setting, problem solving, coaching, and QA commit-tee development. QA coaches were developed among thosealready sensitized to QA; they became responsible for furtherdissemination and for guiding local QA work. External assistancethen provided mentoring to the QA Unit to increase its capacityto lead the QA effort.
As Zambia’s QA program entered the expansion phase, coachesshowing skill in this role received instruction as QA trainers.They independently identified groups needing QA training andstarted QA work without involving the QA Unit. QA capacitybuilding expanded from districts to hospitals, and new coachesand trainers were developed specifically for hospital work. Thus,Zambia created a critical mass of trainers and coaches compe-tent to lead QA work, while at the same time creating a criticalmass of staff who could define, measure, and improve qualitycare. Meanwhile, the QA Unit has downsized, causing increasedreliance on the QA trainers and coaches to continue capacity-building activities.
As the Central Board of Health (CBOH) moves QA toward consoli-dation, QA capacity is being integrated into pre-service trainingfor many technical cadres and post-basic training for clinicalofficers and nurses involved in specialized training. Also, plansmust be made to reliably provide ongoing capacity building tocreate more coaches and QA trainers, and to address staffreassignment and attrition at all levels, from facility to topleadership. The consolidation phase will also require the CBOHto consider how it will continue to provide capacity building forits most experienced QA staff: getting them additional learningexperiences through international conferences, courses,professional materials, or other means is becoming animportant challenge.
Source: Askov et al. Undated

42 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
when leaders, decision makers, and stakeholders expressthe need for QA and are interested in exploring what itmeans to implement QA within their organization.
Experiential: Capacity building also has a key role insuccessful experiences with QA implementation that dem-onstrate results, i.e., that show that change is possible andbeneficial. During this phase, capacity-building activitiesfocus on developing (a) specific QA technical skills in acritical mass of practitioners, and (b) the necessary leader-ship and support skills (planning, coaching, etc.) amongthose implementing QA activities. At the end of this phase,a key indication of successful capacity building is that theorganization has a group of supervisors, coaches, and lead-ers with the knowledge and skills not only to support thecurrent level of QA, but also to expand it. In addition, theorganization has an understanding of what kinds of capac-ity-building approaches are most appropriate and consen-sus on strategies for expanding QA capacity buildingwithin the organization.
Expansion: When the organization is ready to expand thescope of QA implementation, capacity building is againcritical by providing and reinforcing QA knowledge andskills to an even broader group of individuals. Duringexpansion, QA capacity building might include training,on-the-job learning, mentoring, coaching, computer-basedlearning, and other forms of learning. For maximaleffectiveness, capacity-building activities for QA must beintegrated with other organizational capacity-buildingactivities. During this phase, QA training and support mate-rials must be compiled or revised as necessary. Capacitymust be developed at several levels: staff with QA leader-ship skills that can facilitate the work of QA teams, QAexperts who can foster the continuous development of QAstrategies and techniques, and staff with QA coaching andmentoring skills who can provide ongoing support to theexpanding QA implementation. These QA staff are not asmall group of exclusive QA experts, but rather a growingproportion of staff with QA skills. The skills of the expand-ing pool of QA coaches, mentors, and master trainersshould be validated at this point and the effectiveness ofQA training evaluated. A key indication of readiness tomove on to the next phase is the creation of a critical massof competent staff to support ongoing QA efforts. Anotherindication is the presence of leaders and managersmodeling QA values and processes.
Consolidation: At this phase, capacity-building plans areintegrated into ongoing staff training and developmentplans. The content and methods of training and othercapacity-building efforts are monitored for their effective-ness. Competency and performance are evaluated on aregular basis, and the results are used to direct improve-ment or enhancement of capacity. Diverse approaches to
Table 5.8 Possible Activities to Develop the
Essential Element Capacity Building and
Move to the Next Phase/State
Awareness
Experiential
Expansion
Consolidation
Undertake QA awareness and sensitization sessionsfor selected stakeholders and decision makers
Explore various perspectives about quality healthcare(manager, provider, client, payer, community)
Perform site visits to facilities reputed to be highquality
Arrange study tours to other countries or regions tobroaden perspectives on quality
Hold workshops on best practices
Study adverse events
Implement quality assessments, includingmeasurement of client satisfaction
Review existing health statistics and epidemiologicaldata
Establish skill development training for supervisorsand coaches, including on-the-job mentoring andevaluation
Introduce self-assessment and monitoring exercises
Conduct leadership training
Develop performance indicators andperformance-based evaluation of training
Test alternative training modalities (e.g., computer-based learning, problem-based learning, mentoring)
Develop a formal QA capacity-building plan
Develop a system for tracking staff training in QA andongoing, performance-based evaluation of trainingeffectiveness
Develop a formal training program for QA mentorsand coaches that includes on-the-job learning
Validate the competence of QA mentors, coaches,and supervisors
Explore whether computer-based learning couldexpand access to QA information to privatepractitioners and remote staff
Develop and implement a leadership trainingcurriculum
Develop a mechanism for an annual QA capacity-building needs assessment, strategic planning ofspecific QA topics, and development of appropriatetraining strategies to address each
Refine the performance-based evaluation system
Refine the process for maintaining a critical numberof competent coaches and mentors
Implement a training strategy to maintain criticalmass of QA practitioners and champions

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 43
capacity building are used, such as self-assessments andon-the-job learning. Additional indications of consolidationinclude having a QA curriculum that is being integratedinto other training curricula, such as pre-service training athealth professional schools and universities, and includingQA in in-service training for specific health interventions.Finally, a key characteristic of this phase is the existence ofa process or mechanism to maintain a critical mass of QAcapacity. Once a critical mass of QA practitioners andsupporters exists along with a strong system to maintainboth numbers and skills, maturity is close at hand.
Maturity: At maturity, capacity building for QA is fullyintegrated into the pre-service and continuing educationcurricula for healthcare providers and managers, and issupported on a continuous basis by coaching, mentoring,and supervision. Thus, the organization has a mechanismto develop and update QA capacity at all levels, includingthe maintenance of a critical mass of experts, coaches, andpractitioners.
5.7 Information and Communication
Information and communication play a key support rolein each phase of the QA institutionalization process. Thisrole encompasses gathering all relevant information aboutdirect QA activities and the other essential elements (suchas policy development) and sharing it with all those whocan learn from it or who need it to further the institutional-ization effort. Information and communication are thusimportant not only to facilitate QA implementation butalso for advocacy and to boost awareness and recognitionof the value of QA. Whether defining, measuring, or improv-ing quality, documenting and sharing results are crucial.Working in teams can successfully take place only if teammembers share (communicate) the information they havewith others on their team. This information is part of thedata collected and used to make decisions for programplanning and improvement. Communication is also theprocess by which clients can provide their input andexpress their satisfaction or dissatisfaction with theservices they receive (see example in Box 5.7).
Each phase of the institutionalization process presentsdifferent communication challenges. A simple planningprocess can establish an effective information and commu-nication mechanism. Such a process includes: defining thespecific goals of information gathering and communica-tion for that phase; identifying any obstacles in meetingthose goals; developing profiles for the different targetgroups (audiences) to be reached with the information;segmenting and prioritizing the target audiences; selectingappropriate communication messages, materials, and chan-
nels for each group; developing and pre-testing materials;assessing effectiveness; and using feedback to refine thecommunication program (Center for Substance AbusePrevention 1997). Activities to develop information andcommunication functions during each phase of the institu-tionalization process are listed in Table 5.9.
Awareness: In the awareness phase, an organization inter-ested in implementing QA may not have full support fromrelevant stakeholder groups. Thus, in conjunction withcapacity-building activities to increase knowledge andawareness, communication’s key role is to advocate for QA,explain why QA is necessary, show that QA can success-fully address quality of care issues, and strengthen commit-ment to implement quality assurance programs. Giving keystakeholders information about quality problems that hasbeen generated from research studies, assessments, orother sources is also useful, as is sharing results from QAefforts in other organizations.
Experiential: During the experiential phase, the organiza-tion usually starts to experiment with ways of generatinginformation about both the process and results of QA
Box 5.7 Promoting the National Crusade for Health
Quality in Mexico
Reflecting the top priority given to improving thequality of healthcare (see Box 3.1), the NationalCrusade for Quality, led by the Secretariat of Healthof the Mexican government, created a national com-munication initiative to promote quality in the healthsector. The campaign has been widely publicizedthrough the mass media and promotional materialssuch as posters and pamphlets. A key campaignobjective is to ensure that improvements inhealthcare quality are clearly perceived by the popu-lation. In addition, a statement of health client rightshas been developed and is being introduced in allhealth facilities. The campaign has created a websiteand a national quality hotline to allow Mexicancitizens to report concerns or problems with healthservice quality.
Another proposed aspect of the campaign is todevelop a system of incentives to improve the perfor-mance of individual providers and healthcare organi-zations. The Secretariat is developing incentives onan experimental basis to determine what combina-tions of incentives would be effective and economi-cally feasible for public sector institutions.
Source: Secretariat of Health, Mexico 2001

44 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
efforts, in order to advocate for an expansion of QA efforts.Organizations at this phase need to develop and testmechanisms for both documenting the results of QA effortsand for sharing this information with decision makers,communities, other teams and facilities, and other stake-holders. Indications of readiness to move on to the nextphase include regular documentation by those experi-menting with QA and sharing of experiences across numer-ous target audiences. Also, mechanisms are in place toensure that improvements, successes, and failures made inone department or division are communicated to otherunits.
Table 5.9 Possible Activities to Develop the Essential
Element Information and Communication and
Move to the Next Phase/State
Awareness
Experiential
Expansion
Consolidation
Gather all information available on QA activitiesoccurring in the organization
Collect information about relevant QA activitiesoccurring in other organizations, regions, or countries
Organize internal and external forums to advocate fora focus on quality and QA
Develop guidelines and formats for QA teams todocument their work
Provide support to QA teams with documentation oftheir work
Organize regular meetings or other venues for QAteams to share their results
Develop a communication plan with key decisionmakers or leaders in QA to help them garner moresupport and consensus about expansion
Foster a culture of open communication ofsuccesses and opportunities to learn from lesssuccessful efforts
Monitor and evaluate ongoing documentation andcommunication processes
Continue to organize or facilitate regular meetingsor other venues for QA teams to share their results
Continue advocacy efforts
Support dissemination of QA experiences andlessons with other organizations both domesticallyand internationally
Evaluate documentation and communicationactivities with a view toward their sustainabilitywithin the organization
Work with human resources and policy makers toincorporate responsibility for documentation andcommunication in job descriptions
Expansion: Once expansion begins, whether it is a geo-graphic expansion or an expansion in scope, informationand communication efforts are needed to help buildconsensus among more stakeholders. This phase calls forperhaps the most aggressive communication effort. Previ-ous awareness-raising interventions may have createdheightened expectations from consumers, providers, andother regions or departments, and criticism of the effortmay have surfaced. As the organization embraces broaderimplementation of QA, information and open communica-tion will facilitate this transition. The documentationprocesses established for the awareness and experientialphases will serve as a foundation for this phase andprovide data to demonstrate improvements in the qualityof care. Benchmarking successful QA efforts, both withinand outside the organization, may be helpful. Indicators ofreadiness to move on to the consolidation phase includemechanisms and systems for routine documentation offindings and lessons learned, regular dissemination andsharing of results, and habitually using information forcontinued advocacy.
Consolidation: Communication activities in the consoli-dation phase should contribute to the diffusion of qualitygoals, objectives, and core values throughout the organiza-tion. Information should continue to feed into the decision-making and policy processes. The mechanisms andsystems set up for documentation, sharing, and advocacyduring the expansion phase are routine, and responsibili-ties for these activities are incorporated into staff jobdescriptions.
Maturity: At maturity, mechanisms for regular documenta-tion and sharing of QA experiences are well established.Improvements made in one part of the organization areshared with other parts and stakeholders. Documentationand data are used routinely for decision making at boththe policy and operational levels to identify areas forimprovement as well as best practices.
5.8 Rewarding Quality
Recognizing and rewarding quality are two of the mosteffective ways to motivate health staff and managers tocontinue and persevere in their efforts to meet client needsin the most effective and efficient manner. The goal ofinstitutionalizing the element of rewarding quality is tocreate an organizational culture where efforts to improveor assure quality are recognized, appreciated, and re-warded and where staff take pride in the quality of theirwork. It is important to note that in addition to tangible andintangible incentives to promote the pursuit of quality,

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 45
institutionalization of QA will require removal of disincen-tives that discourage and prevent behaviors not explicitlyaimed at providing quality healthcare or that ignore clientneeds.
Box 5.8 describes one mechanism for rewarding qualityapplied in Malaysia. Activities to develop rewards for qual-ity during the institutionalization process are presented inTable 5.10.
Awareness: The first step in developing mechanisms forrewarding quality is to develop awareness of both the needfor incentives to improve quality and for removing disin-centives to quality. Initially, the organization must reachconsensus on what constitutes quality in its work. Areefforts focused primarily on efficient use of resources, orare improvements in clients’ health and satisfaction impor-tant for the organization as well? In order to focus rewardsand use reward systems as an incentive to build a cultureof quality, staff must clearly understand the direction ofquality efforts and about performance expectations.Another critical aspect is awareness and understanding ofhow the current human resource management systemcontributes to or hinders rewarding quality. An indicationthat an organization is ready to move to the next phase isthe recognition by leadership of the need to developmechanisms or processes for rewarding quality work andQA efforts among staff.
Experiential: This phase offers opportunities to exploredifferent ways of recognizing and rewarding quality, experi-ment with removing disincentives or barriers to producinghigh quality care, and create disincentives for poor perfor-mance. While incentives used by other organizations mayprovide valuable ideas, each organization will have tolearn what works best and is affordable within its context.
Box 5.8 Rewarding Quality in Malaysia
Innovations to increase productivity and improvequality have been documented in Malaysia’s Ministryof Health since the 1960s. However, they receivedno formal recognition until a 1991 government-widedecree called for the recognition of formal innovationprojects and for the creation of a national innovationaward. Innovations were defined as “new ideas inall aspects of work to produce quality service andimprove productivity as well as to enhance clientsatisfaction.” Several health sector innovationprojects have subsequently won the award.
A 1997 evaluation of the national health sectorquality improvement effort found that while the ideaof innovation was widely accepted in the MOH, itspractice was not uniform throughout the country:some states were much more proactive than others.The evaluation recommended that innovations bemore widely publicized throughout the country tostimulate interest and help others to learn fromsuccessful improvements.
Source: Suleiman and Jegathesan 2000
Visit organizations that have reward or performancemanagement systems in place to encouragequality-focused work
Assess whether all staff have a job description andwhether job descriptions include explicit performanceexpectations
Identify any disincentives in the system thatcontribute to lack of attention to quality among staff
Develop job descriptions for all categories of staff
Begin experimenting with different incentives toreward quality initiatives in the organization
Consider and test a modification of the performanceevaluation system
Organize meetings with managers at differentlevels of the organization to discuss incentives anddisincentives for quality work
Work closely with those developing new organizationalpolicies to harmonize efforts and develop jointimplementation strategy to reorient the organizationtoward quality work
Work with human resources and policy makers toincorporate incentives for quality into staffperformance evaluations
Develop supervisors’ capacity to give feedback andmotivate staff to improve quality
Initiate the development of mechanisms to solicitinput from communities and clients for the incentivesystem
Assess staff satisfaction with incentives and rewardsfor quality
Analyze whether any disincentives to quality workendure in the organization and identify strategies toremove them
Assess whether all parts of the organization and allstaff are included in the new incentive system
Eliminate any remaining disincentives
Conduct a formal evaluation of the effectiveness ofincentives and rewards for quality
Table 5.10 Possible Activities to Develop the
Essential Element Rewarding Quality and
Move to the Next Phase/State
Awareness
Experiential
Expansion
Consolidation

46 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
During this phase, an organization may experiment withvarious packages of incentives and disincentives or chang-ing certain human resource management practices. Thecreation of incentives for communicating results mightalso be analyzed. Key indications of readiness to move onto the expansion phase of rewarding quality include: thepresence of a clear understanding about what impedesquality work and what can motivate workers and teamstowards quality and the implementation of tested incentivepackages.
Expansion: During expansion, the organization movestowards aligning individual staff performance with theorganizational objectives of high quality care. This mightbegin with a system with clear expectations for perfor-mance and work behavior, in which performance is regu-larly assessed, good performance is reinforced, and poorperformance is explicitly discouraged. Mechanisms forrewarding quality work and QI efforts begin to becomeincorporated into the overall QA strategy and are intro-duced at various levels: individual, team, and organiza-tional. Indications for readiness to move to theconsolidation phase include increased levels of staffawareness of incentives and rewards for quality perfor-mance.
Consolidation: During consolidation, the human resourcemanagement system has transparent short- and long-termrewards for individual quality performance and QA efforts.The organization has also implemented rewards for effec-tive team work as well as excellence in the performance oforganizational units. When an organization is ready to beconsidered mature, staff believe that the system of rewardsand incentives is fair and meaningful.
Maturity: Even when an organization reaches a maturestate of QA, it still needs to have formal or systematic pro-cesses for recognizing staff and managers who performtheir work in a quality manner, including incentive systemsthat support continuous improvement. Another indicationthat an organization has a mature reward element is ameans for community input into mechanisms to rewardquality work. In this state, quality is promoted andrecognized by leaders and stakeholders, including thecommunity.
5.9 Bringing the Elements into Maturity
Our description of the process of institutionalization foreach essential element indicates that an organization willnot necessarily have all elements in the same phase at anypoint in time. Because progress is not necessarily uniformacross the range of elements, it is important to examineeach element’s progress and determine how to best directresources and energies to develop each element. Theultimate goal is to bring all elements into maturity—or asclose to that state as possible—and each element is criticalin making that happen. Unless all eight elements are inplace and close to maturity, sustaining QA is difficult.
Determining where each element is in its developmenttakes careful analysis. We reviewed Zambia’s institutional-ization status as of August 2002 to offer an example. As Box5.6 states, Zambia’s Central Board of Health has been de-veloping its QA program since 1993. At a recent meeting ofQA link facilitators and trainers (four local coaches, fiveprovincial level clinical specialists, and 13 national leveltrainers) who are supporting QA activities throughout thecountry, a QA Project staff member participated in analysisof the program. Table 5.11 summarizes the participants’conclusions on each essential element and the actionsthat will move Zambia’s health system forward in itsinstitutionalization.
The analysis of QA institutionalization in Zambia pre-sented in Table 5.11 suggests that a focus on the elementsof policy, core values, information and communication, andrewarding quality would best help to bring the overall QAeffort into alignment. As the framework suggests, theseelements cannot be addressed without leadership support.Therefore, an appropriate next step in Zambia would be tocommunicate this analysis to the senior CBOH leaders togain their support for its recommendations. When QApractitioners regularly inform the organizational leader-ship of the results and benefits of QA activities, their workto institutionalize QA is more likely to succeed.
In summary of Section 5, institutionalization of QA is anongoing process where activities related to defining, mea-suring, and improving the quality of care become formallyand philosophically integrated into the structure and func-tioning of an organization or health system. Institutional-ization is not a linear process of going from point A topoint B but a fluid process where the essential elements ofquality assurance may or may not mature sequentially. Noone path exists for all organizations, but the framework ofeight essential elements and the phased process of institu-tionalization outline the needed aspects and generalroadmap to creating a lasting program to improve thequality of healthcare an organization provides.

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 47
Table 5.11 Analysis of Each Essential Element in Zambia’s Quality Assurance Program
Essential Element
Policy
Status in August 2002
Zambia’s policy environment is moving from experientialto expansion. Policies that support QA capacity building,performance measurement, and continuous improvementare embedded within general management, data manage-ment, and clinical policies and guidelines. Health/manage-ment information system indicators are used for local aswell as national quality assessment and guide improve-ment efforts. The QA implementation plan is part ofstrategic and action planning at all levels (local, district,
province, national). To develop further, staff plan to docu-ment guidelines to formally define the roles and responsi-bilities related to quality for all staff, guide QA committees,and broadly explain the communication/reporting system.Developing an overall QA policy that links all types of QAefforts, including regulatory approaches such as accredita-tion, would also facilitate the expansion of QA activities inZambia.
Zambia is moving into the expansion phase in terms ofleadership. Key leaders at all levels have the authority toexpand QA activities, allowing for creative and individual-ized approaches to measuring and improving quality atdifferent levels of the health system. Some districts andhospitals already have a critical mass of leaders who are
Leadership accountable for quality, lead QA activities, and have pro-vided sustained support and resources for QA work, butthis is not consistent across the country. To move to thenext level, QA coaches are involving a wider variety ofsenior leaders in QA sensitization, to gain their supportand assistance in leading QA efforts.
“The vision of health reforms is to provide quality, cost-effective healthcare as close to the family as possible.”This statement reflects core values held by the Zambianpublic sector health system, placing it in the experientialphase. Staff and leaders are acutely aware of barriersthat limit the achievement of this vision, but the CBOH
continues to include these values in performance assess-ment, supervision, policy development, and strategicdecision making. As they solidify this phase, leaders mayconsider whether the vision and strategic planning implyother important values; if so, these leaders could makethese additional themes explicit.
Core Values
Resources to do QA in Zambia are in the expansionphase. Realistic budgets and other resource documentsat the facility, district, and province levels identifyhuman, financial, and material resources needed toprovide quality healthcare. In many cases, QA is inte-grated with other activities, so a budget for introducing anew service, for example, would include resourcesneeded for standards setting and communication, imme-diate post-intervention quality measurement, and longer-term monitoring. Local budgets define requirements for
capacity building (clinical, QA, health/management infor-mation system, etc.), staffing levels, and priorities forclinical improvements. As activities mature, the CBOHlooks forward to having more of the country incorporateQA resource needs into routine budgets and anticipateshaving sufficient resources to fund all levels at theamounts they have budgeted. Assuring adequate re-sources for national and local level support for the QAprogram would signal an important step towardconsolidation.
Resources
The CBOH is in the consolidation phase vis-à-vis organiz-ing for quality. The assessment concluded that currentorganizational structures do not support communicationabout quality or effective mentoring and monitoring ofQA work by the national level. With a new service qualityspecialist taking over the senior technical QA role inSeptember 2002, an opportunity exists to redefine
roles and responsibilities related to quality and QA at alllevels. As job descriptions are being written, responsibilityfor quality is included. In addition, specific responsibilitystatements for province clinical specialists, QA commit-tees, QA coaches, and national trainers are being revised.
The CBOH is in the expansion phase for capacity building,moving into consolidation. Formal QA capacity building hasoccurred or is ongoing in every district and at each level 2and 3 hospital, and competent coaches are available atmost districts and each hospital. Many, but not all, facili-ties have at least one QA-trained person. Capacity buildinguses standard materials and qualified trainers. Trainingeffectiveness has been routinely evaluated by nationaltrainers, resulting in changes in technical approaches and
coaching training. QA coaches and national trainers havebeen regularly validated with competency-based assess-ment by senior QA practitioners. Training materials havebeen developed for several pre-service and post-basicschool environments in technical clinical programs andnursing. Plans have been made to train additional coachesand national trainers to address attrition and reassign-ment, to ensure a critical mass of QA expertise.
Organizing for Quality
Capacity Building
continued on page 48

48 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Table 5.11 Analysis of Each Essential Element in Zambia’s Quality Assurance Program (Continued)
Essential Element
Information andCommunication
Status in August 2002
This element had been at a consolidation level in pastyears. However, the mechanisms previously establishedfor communication from the field to national level, throughcoaches and national trainers, were recently evaluatedand found flawed. Consequently, this element is seen ascurrently in the experiential phase. Some districts andprovinces do hold regular meetings to discuss qualityissues and review quality efforts. To advance this element,information from these meetings should be regularlycommunicated up to the national level and routinely used
for QA advocacy. Another advance will be to encouragesupervisors to routinely report quality information to theirsupervisors, so more people than just the QA coaches arecommunicating about quality. The most effective methodof communication has been through link meetings—national-level meetings of QA national trainers, provincialclinical specialists, and selected local coaches. Whilebudgets for these meetings are routinely provided, thefunding is insufficient, so ongoing attention is needed toensure that they are conducted routinely.
Zambia is at an experiential level in terms of formalrewards for quality. Job descriptions are not yet developedfor all staff, though job expectations do exist for catego-ries of staff. The system has assumed that workers will beof high quality and has not envisioned a role for rewards orpunishments based on quality performance. At thenational level, leaders are discussing ways to evaluate and
reward quality work. At local levels, where QA efforts aresustained, people are rewarded for quality in several ways:personal recognition by supervisors, formal awards onLabour Day, recognition of “best ward” or “best nurse,”ability to use saved funds on priority needs, and personaladvancement due to knowledge of quality and qualityassurance.
Rewarding Quality
Source: Reinke 2002

Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 49
Epilogue
HE QA Project has now completed ten years of workto support lower- and middle-income countries inimplementing QA in national, regional, and local
healthcare systems. This monograph highlights our under-standing of what is needed to sustain QA in a healthcaresystem or organization over time.
Leadership, both at the facility and the political levels, isperhaps the most critical element in improving andsustaining the quality of care and moving forward in insti-tutionalization. In addition, clear policies that link QA tothe organization’s overall mission and that define the QAroles and responsibilities of coaches, trainers, quality com-mittees, and supervisors must be in place. While our fieldexperience shows that it is possible to implement QAactivities with good results, without overall policies thatsupport QA, such activities are rarely, if ever, sustained.Leadership, policies, and core values that support QA helpsustain health worker motivation to persist in deliveringquality care despite the difficulties they face daily inresource-constrained environments.
Building QA capacity at the facility, district, regional, andnational levels for large-scale implementation is anotherbig challenge, and one that demands further insights inhow to undertake it with the least investment of resources.We know that organizations that are serious about qualityassurance must allocate sufficient resources to develop acadre of QA experts who can train, coach, and mentorothers. Frequent turnover of health personnel calls fordiverse strategies for developing and maintaining QA skillsafter initial waves of QA training. Alternatives to traditionaltraining merit wider application: self-learning, peermentoring, and job aids, as well as mechanisms to reachwould-be healthcare providers during basic education andduring service through professional organizations.
While the eight essential elements and the phases for insti-tutionalization are the central issue of this monograph, it’simportant to keep the principles of QA in mind while insti-tutionalizing QA. For instance, the principle of focusing onthe client, as noted in Section 2, keeps healthcare workersperforming at their best and clients satisfied with the ser-vices they are receiving. Such performance feeds into afocus on results that will resonate with health authorities,who are responsible for improving outcomes for priorityhealth problems and efficiency, and for reducing costs.Providing objective evidence of improvement demon-
6T strates to health decision makers, on an ongoing basis, that
investments in QA produce results. The development ofquality indicators and monitoring systems that capture andcommunicate such results is essential to this end.
The QA Project enters its second decade with a clear un-derstanding of the elements of QA institutionalization anda need to learn how to most efficiently support their devel-opment and scale-up. While a few countries have movedrapidly to expand QA to entire districts or provinces, manycountries become mired in the expansion phase, strugglingwith the challenges of scaling up successful pilot or dem-onstration experiences. We need to learn more about howQA activities in a small number of sites can be efficientlyexpanded to cover all or most of a healthcareorganization’s operations.
No single approach to scaling up fits all countries andcontexts, and we need to increase our understanding ofthe range of expansion strategies and the different condi-tions under which various strategies would work. FocusingQA activities on priority health problems is one model thatcan be effective in rapidly expanding QA efforts. The selec-tion of what to improve determines much of the initialenthusiasm and leadership buy-in to the improvementeffort. It is critical to select important health priorities;doing so will make the effort worthwhile and generatesupport for more improvement. This has the double benefitof achieving measurable results to persuade decision mak-ers that QA activities are worthwhile and providing positivereinforcement to the health providers who undertook theQA activity. Replicating successful interventions or expand-ing work to other clinical areas then serves as the vehicleto spread QA concepts and methods to a larger area or toapply them to other problems.
Another promising approach for building up and sustain-ing QA efforts is creating demand for improved quality ofcare from forces external to the healthcare organization.This external demand for quality may come from clientsand communities (such as the users’ committees or com-munity health boards) or through the healthcare financingsystem, as in the approach of tying payment or reimburse-ment to meeting minimum quality standards. Attention toaddressing client needs and expectations can help lay thegroundwork for greater community involvement in andsupport for QA efforts.

50 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Finally, the growing emphasis on health sector reformthroughout the world provides “fertile soil” for institutional-izing QA. Many countries are currently undergoing majorchanges related to health reform, such as decentralization,integration of private sector in primary care, moderniza-tion, and health insurance diversification. For QA to be partof a national agenda and progress beyond the awarenessand experiential phases, it needs to be linked to theagenda of health system reforms and not work in isolation.
QA is a dynamic field, with new ideas and tools continu-ally being developed. The institutionalization framework
was designed to help healthcare decision makers identifyconcrete actions to further the institutionalization of QA intheir organization or health system. It has been used inLatin America and Africa to assist Ministries of Health toplan and focus efforts and resources to strengthen QAprograms. Responding to requests from country programs,we are now developing self-assessment and monitoringinstruments, based on the framework, to help healthcareorganizations to analyze their QA institutionalizationprogress more systematically over time.
Sustaining Quality of Healthcare: Institutionalization of Quality Assurance ◆ 51
ReferencesAbdallah, H., O. Chernobrovkina, A. Korotkova, R. Massoud,
and B. Burkhalter. 2002. Improving the Quality of Carefor Women with Pregnancy-Induced HypertensionReduces Costs in Tver, Russia. Operations ResearchResults 2(4). Bethesda, MD: Published for the UnitedStates Agency for International Development (USAID)by the Quality Assurance Project.
Ashton, J. 2001a. Monitoring the Quality of Hospital Care.Health Manager’s Guide. Bethesda, MD: Published forthe United States Agency for International Develop-ment (USAID) by the Quality Assurance Project.
Ashton, J. 2001b. Taxonomy of Health System Standards.Project Report. Bethesda, MD: Published for the UnitedStates Agency for International Development (USAID)by the Quality Assurance Project.
Askov, K., C. MacAulay, L. M. Franco, D. Silimperi, and T.Veldhuyzen van Zanten. Undated. Institutionalizationof Quality Assurance. Project Report. Bethesda, MD:Published for the United States Agency forInternational Development (USAID) by the QualityAssurance Project.
Atkinson, P.E. 1990. Creating Cultural Change: The Key toSuccessful Total Quality Management. Toronto: Pfeiffer &Company.
Baldrige National Quality Program. 2001. Health CareCriteria for Performance Excellence 2001. Gaithersburg,MD: Baldrige National Quality Program.
Barker, J.A. 1999. Leadershift: Five Lessons for Leaders in the21st Century. West Des Moines, IA: American Media Inc.
Berwick, D.M. 1995. Improving Health Care Quality. Boston,MA: Institute for Healthcare Improvement.
Berwick, D.M., A. Enthoven, and J.P. Bunker. 1992. Qualitymanagement in the NHS: The doctor’s role–II. BritishMedical Journal 304:304–08.
Bouchet, B. Undated. Monitoring the Quality of PrimaryCare. Health Manager’s Guide. Bethesda, MD: Publishedfor the United States Agency for International Develop-ment (USAID) by the Quality Assurance Project.
Brown, L.D. 1995. Lessons learned in institutionalizationof quality assurance programs: An internationalperspective. International Journal of Quality HealthCare 7(4):419–25.
COHSASA (Council for Health Service Accreditation ofSouthern Africa). 2000. Encouraging progress inKwaZulu-Natal. COHSASA NEWS 1(1).
Center for Substance Abuse Prevention, Substance Abuseand Mental Health Services Administration, U.S. Depart-ment of Health and Human Services. 1997. “Identifyingthe Target Audience.” Technical Assistance Bulletin.June.
Deming, W.E. 1982. Quality Productivity and CompetitivePosition. MIT Center for Advanced Engineering Study:Cambridge, MA.
Dickson-Tetteh K., A. Ashton, D. Silimperi, W. Moleko, and S.Ladha. Forthcoming. Developing a Focused Accredita-tion Model to Improve the Quality of AdolescentHealth Services. Quality Assurance Project Case Study.Bethesda, MD: Published for the U.S. Agency forInternational Development (USAID) by the QualityAssurance Project.
Donabedian, A. 1980. Explorations in Quality Assessmentand Monitoring. Volumes I, II, and III. Ann Arbor, MI:Health Administration Press.
Ethier, K. Forthcoming. Working title: “Empowered byQuality Improvement: A Qualitative Look at theSuccesses of the Quality Assurance Project in Russia,”submitted for presentation at the 8th European Forumon Quality Improvement in Health Care, Bergen,Norway; May 2003.
Gnecco, G. 1999. Making a commitment to quality:Development of the quality assurance programme inChile, 1991–1999. International Journal of QualityHealth Care 11(4):443–45.
Gnecco, G., S. Lucero, A. Bassi, R. Loncomilla, and L.D.Brown. 1999. Making a Commitment to Quality:Development of a National Quality Assurance Programin Chile 1991–1998. Country Report. Bethesda, MD:Published for the United States Agency forInternational Development (USAID) by the QualityAssurance Project.
Grindle, M.S. 1997. Divergent cultures? When publicorganizations perform well in developing countries.World Development 254:481–95.
Hermida, J., and M.E. Robalino. Forthcoming. Increasingcompliance with maternal and child care qualitystandards in Ecuador. International Journal for Qualityin Health Care. 14(6) Supplement.
Juran, J.M. 1988. Juran’s Quality Control Handbook (FourthEdition). USA: McGraw Hill, Inc.
Langley, G.J., K.M. Nolan, T.W. Nolan, C.L. Norman, and L.P.Provost. 1996. The Improvement Guide: A PracticalApproach to Enhancing Organizational Performance.San Francisco, CA: Jossey-Bass Publishers.

52 ◆ Sustaining Quality of Healthcare: Institutionalization of Quality Assurance
Legros, S., R. Massoud, O. Urroz, and E. Kelley. 2000. The ChileQuality Assurance Program: Final Evaluation. TechnicalReport Summary 1(2). Bethesda, MD: Published for theUnited States Agency for International Development(USAID) by the Quality Assurance Project.
Lin, Y. 2000. Designing Quality Essential Obstetric CareServices in Honduras. Quality Assurance Project CaseStudy. Bethesda, MD: Published for the United StatesAgency for International Development (USAID) by theQuality Assurance Project.
Management Sciences for Health. 2002. Developing manag-ers who lead. The Manager 10(3).
Marszalek-Gaucher, E., and R.J. Coffey. 1990. TransformingHealthcare Organizations: How to Achieve and SustainOrganizational Excellence. San Francisco, CA:Jossey-Bass Publishers.
Massoud, R., K. Askov, J. Reinke, L.M. Franco, T. Bornstein, E.Knebel, and C. Macaulay. 2001. A Modern Paradigm forImproving Healthcare Quality. QA Monograph Series1(1). Bethesda, MD: Published for the United StatesAgency for International Development (USAID) by theQuality Assurance Project.
Ministry of Health and Population of Malawi. 1997. NationalQuality Assurance Plan (draft). Lilongwe, Malawi.
Partnerships for Health Reform Project. 2000. Glossary ofHealth Reform Terms for Translators: A Working List forUse by Translators and Health Systems Specialists.Bethesda, MD: Partnerships for Health Reform Projectin cooperation with the Ministry of Health andPopulation, Egypt.
Plsek, P.E. 1997. “Working Paper: Some Emerging Principlesfor Managers of Complex Adaptive Systems (CAS).”<www.directedcreativity.com/pages/ComplexityWP.html>. Uploaded to Internet 5 November1997.
Powell, T.C. 1995. Total quality management as competitiveadvantage: A review and empirical study. StrategicManagement Journal 18:15–37.
QA (Quality Assurance) Project. Undated. “Niger CountryReport: Tahoua Project.” Quality Assurance MethodologyRefinement Series. Bethesda, MD: Published for theUnited States Agency for International Development(USAID) by the Quality Assurance Project.
Reinke, J.M., L. Malianga, and M. Mchombo. 2001. Malawi:May 21–June 7. Trip Report.
Reinke, J.M. 2002. Zambia: August 4–September 1. TripReport.
Renzi, M. 1996. An integrated tool kit for institutionaldevelopment. Public Administration and Development16:469–83.
Roemer, M.I., and C. Montoya-Aguilar. 1988. Qualityassessment and assurance in primary health care.WHO Offset Publication No.105. Geneva, Switzerland:World Health Organization.
Rooney, A., and P. van Ostenberg. 1999. Licensure,Accreditation and Certification: Approaches to HealthServices Quality. Quality Assurance MethodologyRefinement Series. Bethesda, MD: Published for theUnited States Agency for International Developmentby the Quality Assurance Project.
Ryan, K., and D.K. Oestreich. 1998. Driving Fear out of theWorkplace: Creating a High-Trust, High-PerformanceOrganization, 2nd Edition. San Francisco, CA:Jossey-Bass Publishers.
Secretariat of Health, Mexico. 2001. National HealthProgram 2001-2006: The Democratization of Health inMexico. Mexico City.
Senge, P.M., A. Kleiner, C. Roberts, R.B. Ross, and B.J. Smith.1994. The Fifth Discipline Fieldbook: Strategies andTools for Building a Learning Organization. New York,NY: Doubleday.
Shortell, S.M., J.L. O’Brien, J.M. Carman, R.W. Foster, E.F.X.Hughes, H. Boerstler, and E.J. O’Connor. 1995. Assessingthe impact of continuous quality improvement/totalquality management: Concept versus implementation.Health Services Research 30:377–401.
Shortell, S.M., C.L.Bennett CL, Byck GR. 1998. Assessing theimpact of continuous quality improvement on clinicalpractice: What will it take to accelerate programs. TheMilbank Quarterly 76:593–624.
Suleiman, A.B., and M. Jegathesan. 2000. Health inMalaysia–Achievements and Challenges. Malaysia:Ministry of Health.
Tenner, A.R., and I.J. DeToro. 1992. Total QualityManagement: Three Steps to Continuous Improvement.Reading, MA: Addison-Wesley Publishing Company, Inc.
USAID (United States Agency for International Develop-ment). 2000. “Measuring Institutional Capacity.” USAID/CDIE TIPS Number 15. Washington, DC: USAID.
Wagner, C., D.H. DeBakker, and P.P. Groenewegen. 1999. Ameasuring instrument for evaluation of quality systems.International Journal of Quality Health Care 11:119–30.