systemic anti-microbials in periodontal therapy
TRANSCRIPT

Systemic antimicrobials in periodontal therapy

CONTENTS
Introduction
Rationale for use of antibiotics in periodontal therapy
Commonly prescribed antibiotics in periodontal therapy
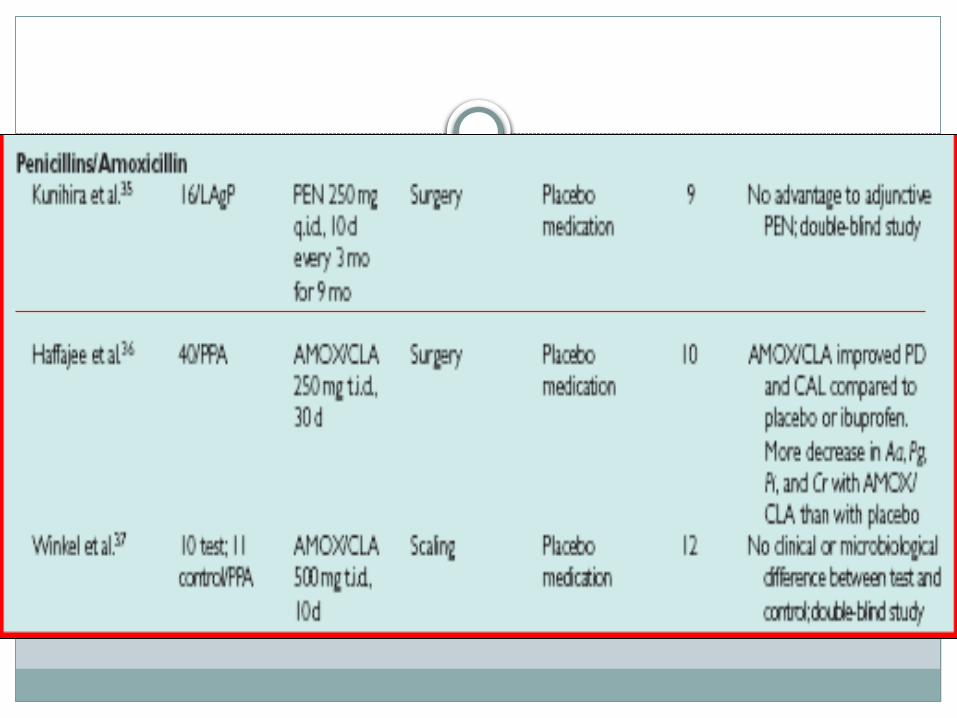
Penicillins (Amoxicillin)
Nitroimadazole (Metronidazole)
Tetracyclines
Macrolides (Azithromycin,Clarithromycin)
Lincomycin derivatives(Clindamycin)
Fluoroquinolones (Ciprofloxacin)
Antibiotic resistance
Conclusion
References

INTRODUCTION
Definition :
Antibiotics may be defined as the substances
produced by the microorganisms, which suppresses
the growth of or kill other microorganisms at very
low concentrations.

CLASSIFICATION A) Mechanism of action :
1. Inhibit cell wall synthesis
• Penicillins
• Cephalosporins
• Vancomycin
• Bacitracin
2. Cause leakage from cell membranes
• Polypeptides – Polymycins, colistin, Bacitracin
• Polyenes – Amphotericin B, Nystatin

5. Inhibit DNA gyrase
• Fluoroquinolones – Ciprofloxacin
6. Interfere with DNA function
• Rifampacin
• Metronidozole
7. Interfere with DNA synthesis
• Idoxuridine
• Acyclovir
• Zidovudine
8) Interfere with intermediary metabolism
Sulfonamides
Pyrimethamine
Ethambutol

B) Chemical structure
1. Sulfonamides and related drugs
• Sulfadiazine and others
• Sulfones – Dapsone (DDS), Paraaminosalicylic acid (PAS).
2. Diaminopyrimidines
• Trimethoprim
• Pyrimethamine
3. Quinolones
• Nalidixic acid
• Ciprofloxacin
• Norfloxacin

4. Tetracycline's
• Oxytetracycline
• Doxycycline etc
5. Nitrobenzene derivative
• Chloramphenicol
6. -lactam antibiotics
• Penicillins
• Cephalosporins
• Monobactams
• Carbapenems

7. Aminoglycosides
• Streptomycin
• Gentamicin
• Neomycin etc
8. Macrolide antibiotics
• Erythromycin
• Roxithromycin
• Azithromycin etc
9. Polypeptide antibiotics
• Polymyxin-B
• Colistin
• Bacitracin

10.Glycopeptides
• Vancomycin
• Teicoplanin
11. Oxazolidinone
• Linezolid
12.Nitrofuran derivatives
• Nitrofurantoin
• Furazolidone
13.Nitroimidozoles
• Metronidozole
• Tinidazole

14.Nicotinic acid derivatives
• Isoniazid
• Pyrazinamide
• Ethionamide
15.Polyene antibiotics
• Nystatin
• Amphotericin-B
• Hamycin
16.Azole derivatives
• Miconazole
• Clotrimazole
• Ketoconazole

C) Type of organisms against which primarily active
1. Antibacterial • Penicillins• Aminoglycosides• Erythromycin
2. Antifungal • Griseofulvin• Amphotericin B• Ketoconazole
3. Antiviral• Idoxuridine• Acyclovir• Zidovudine

4. Antiprotozoal
• Chloroquine
• Pyrimethamine
• Metronidazole
• Diloxanide etc
5. Anthelmintic
• Mebendazole
• Pyrantel
• Niclosamide
• Diethyl carbamazine

D) Spectrum of activity
1. Narrow spectrum
• Penicillin G
• Streptomycin
• Erythromycin
2. Broad spectrum
• Tetracyclines
• Chloramphenicol
E) Type of action
1. Primarily bacteriostatic
• Sulfonamides
• Tetracyclines
• Chloramphenicol
• Erythromycin
• Ethambutol
2. Primarily bactericidal
• Penicillins
• Aminoglycosides
• Rifampin
• Cotrimoxazole
• Cephalosporins
• Vancomycin
• Nalidixic acid
• Ciprofloxacin

F) Antibiotics are obtained from
1. Fungi
• Penicillin
• Cephalosporin
• Griseofulvin
2. Bacteria
• Polymyxin B
• Colistin
• Bacitracin
• Tyrothricin
3. Actinomycetes
• Aminoglycosides
• Tetracyclines
• Chloramphenicol
• Macrolides
• Polyenes

RATIONALE
Bacterial deposits periodontal infections
Mechanical treatment
Inability to eliminate pathogens like A. actinomycetemcomitans
Recolonization by pathogens residing in non – dental sites (Dorsum of Tongue, Tonsils)
Adjunctive systemic antibiotics
(Van winkelhoff AJ,Rams TE, Slots J.Periodontol 2000 1996;10:45-78)

Acute periodontal infections associated with systemic manifestations
Prophylaxis in medically compromised patients
Recurrent periodontitis

Ideal antibiotic for use in periodontal disease should be:
1. Specific for periodontal pathogen
2. Non-toxic
3. Substantive
4. Not in general use for treatment of other diseases
5. Inexpensive
(Gibson W,1982)

GUIDELINES
1. Clinical diagnosis—patients diagnosis can change over time
2. Continuing disease activity
3. Selection based on patients medical, dental status, current
medications and microbial analysis
4. Microbiologic plaque sampling
--method
--indications: aggressive forms of disease, disease refractory to
standard mechanical therapy, periodontitis with systemic
condition

5. Reduce need for periodontal surgery in chronic periodontitis patients
(Loesche 1992)
6. Antibiotics as monotherapy not recommended --disruption of biofilm physically (Greenstein
2005)7. Slots et al 2000-- regenerative healing--start antibiotics 1-2 days prior to surgery continue for 8
days--not well documented

8. Meta-analysis( Haffajee and Socransky 2003)--similar effects for all antibiotics--aggressive periodontitis patients benefited more--overall factors


COMMON ANTIBIOTICS USED FOR TREATMENT OF PERIODONTAL DISEASES

Tetracyclines
widely used in the treatment of periodontal diseases.
--used in treating refractory periodontitis; including localized
aggressive periodontitis.
ability to concentrate in the periodontal tissues and inhibit the
growth of A. actinomycetemcomitans.
---anticollagenase effect that can inhibit tissue destruction and
may aid bone regeneration.

Pharmacology: produced naturally from certain species of
Streptomyces or derived semisynthetically.
--bacteriostatic and are effective against rapidly multiplying bacteria.
--more effective against gram-positive bacteria than gram-negative
bacteria.
insoluble complexes by chelation

concentration in the gingival crevice is 2 to 10 times that in
serum (Bader and Goldhaber 1968.)
low gingival crevicular fluid concentration (2 to 4 µg/ml) are
very effective against many periodontal pathogens.
(Gordon et al
and Pascale et al)

Side effects
contraindicated during pregnancy
cross the placenta and form a stable calcium complex in
bone forming tissue which can result in retardation of
skeletal development
not given to nursing mothers

Clinical Use:
localized aggressive periodontitis (LAP).
Systemic tetracycline can eliminate tissue bacteria and has
been shown to arrest bone loss and suppress A.
actinomycetemcomitans levels in conjunction with scaling
and root planing (Slots et al 1983)
Increased post treatment bone levels

Specific agents
Tetracyclines:
--administration of 250 mg qid.
Minocycline:
-- suppresses spirochetes and motile rods as effectively as scaling
and root planing, up to 3 months after therapy.
-- twice a day
--less photo and renal toxicity
-may cause reversible vertigo.

Minocycline --200 mg per day for I week
•reduction in total bacterial counts,
•complete elimination of spirochetes for periods of up to 2 months
•improvement in all clinical parameters.
(Ciancio 2000)

Doxycycline
-- same spectrum of activity as minocycline
-once daily,
Compliance --its absorption from the gastrointestinal tract is
not altered by calcium, metal ions, or antacids, as is
absorption of other tetracyclines.
--100 mg twice daily the first day, then 100 mg once daily
--subantimicrobial dose to inhibit collagenase, it is
recommended in a 20mg dose twice daily.
Penicillins
Pharmacology : natural and semi-synthetic derivatives of
broth cultures of penicillium mold
basic structure-- thiazolidine ring fused with a beta lactam
ring
inhibit bacterial cell wall production-- bactericidal.
Substitutions and modifications on the acyl side chain ---semi
synthetic penicillins-- enhanced antimicrobial properties such
stability to gastric acids, resistance to hydrolytic enzymes
The side chain also determines the stability of the penicillin
against degradation by gastric acid and by enzyme
penicillinase (beta lactamase)

Amoxicillin: semisynthetic penicillin
extended antimicrobial spectrum --gram-positive and gram-
negative bacteria.
excellent absorption after oral administration
susceptible to penicillinase,.
Amoxicillin may be useful in the management of patients with
aggressive periodontitis, both in the localized and generalized
forms.
Jorgensen slots (2000) Recommended dosage is 500 mg tid for 8
days.

Amoxicillin-Clavulanate :
management of patients with refractory or localized aggressive
periodontitis.
Bueno and co-workers arrested alveolar bone loss in patients with
periodontal disease that was refractory to treatment with other
antibiotics including tetracycline, metronidazole, and clindamycin.
Side effects
Allergic reactions(10%)

Metronidazole
Pharmacology: Metronidazole is a Nitroimidazole compound
developed in France to treat protozoal infec tions
bactericidal to obligate anaerobic organisms
disrupt bacterial DNA synthesis in conditions in which a low
reduction potential is present.

Absorption, fate and excretion:
•rapidly and almost completely (80%) absorbed from the small bowel
•Food does not affect its bioavailability.
•The drug is metabolized mainly in liver
•The drug crosses the placental barrier and is present in the milk.

Metronidazole is not the drug of choice for treating A.
actinomycetemcotnitans infections
Rams and Slots 1992 showed, it is effective against A.
actinomycetemcomitans when used in combination with other
antibiotics.
Greenstein in 1993 showed that Metronidazole is also
effective against anaerobes such as P. gingivalis and P.
intermedia.

Clinical Usage: Metronidazole has been used clinically to
treat, acute necrotizing ulcerative gingivitis, chronic
periodontitis, and aggressive periodontitis.
Studies have suggested that when combined with amoxicillin
or amoxicillin -clavulanate potassium ---localized aggressive
or refractory periodontitis.

Dosage :500mg tds for 8 days
Loesche 1992---> 20% spirochetes anaerobic infection
reduced need for surgery
Side Effects:
antabuse effect when alcohol is ingested
inhibits warfarin metabolism---inc prothrombin time

Cephalosporins:
Pharmacology:
similar in action and structure to peni cillins. They are frequently
used in medicine and are resistant to a number of beta-
lactamases
Clinical Usage: not generally used to treat dental-related
infections
penicillins are superior to Cephalosporins in their range of
action against periodontopathic bacteria.

Side Effects: Patients allergic to penicillins must be considered
allergic to all beta-lactam products
Rashes, ur ticaria, fever, and gastrointestinal upset

Clindamycin
Pharmacology: effective against anaerobic bacteria.
--patient is allergic to penicillin.
Clinical Usage: Clindamycin has shown efficacy in patients with
periodontitis refractory to tetracycline therapy. Walker and co-
workers have shown aid in stabilizing refractory patients.(150 mg
qid for 10 days.)
Jorgensen and Slots have recommended a regimen of 300 mg
twice daily for 8 days.

Side Effects:
pseudomembranous colitis
Diarrhea or cramping that develops during the use of
clindamycin may be indicative of colitis --should be
discontinued.
Ciprofloxacin
Pharmacology: Ciprofloxacin is a quinolone active against
gram-negative rods, including all facultative and some
anaerobic putative periodontal pathogens.
Chelation –cations --Decreased absorption
Clinical Usage:
minimal effect on Streptococcus species---facilitate the
establishment of a microflora associated with periodontal
health.
only antibiotic in periodontal therapy to which all strains of A.
actinomycetemcomitans are susceptible.
used in combination with metronidazole. (Slots et al 1992)

Side Effects: Nausea, headache, and abdominal discomfort have been
associated with ciprofloxacin.
-inhibit the metabolism of theophylline, and caffeine and concurrent
administration can produce toxicity.
---enhance the effect of warfarin
---NSAIDS--- Increased risk of central nervous system stimulation

Macrolides
Pharmacology: Macrolide antibiotics contain a many-membered
lactone ring to which one or more deoxy sugars are attached.
inhibit protein synthesis
bacteriostatic or bactericidal, depending on the concentration of
the drug and the nature of the microorganism.
Clinical Usage:
Erythromycin does not concen trate in gingival crevicular fluid,
and it is not effective against most putative periodontal
pathogens. For these reasons, it is not recommended as an
adjunct to peri odontal therapy

Azithromycin
member of the azalide class of macrolides.
effective against anaerobes and gram-negative bacilli
500 mg once daily for three consecutive days.
Concentration in tissue specimens from periodontal lesions is
significantly higher than that of normal gingiva

--penetrates fibroblasts and phagocytes in concentrations 100
to 200 times greater than that of the extracellular
compartment.
actively transported to sites of inflammation by phagocytes
and then released directly into the sites of inflammation as
the phagocytes rupture during phagocytosis.

Drug interactions
Methylprednisolone ---Increased steroid concentration
Nonsedating antihistamines (terfenadine, astemizole)
Increased antihistamine concentration--with the risk of life-
threatening arrhythmia
Theophylline---- Increased serum levels



Metronidazole ---P.g, P.i
Clindamycin ---peptostreptococcus,ß-hemolytic
streptococcus,gram –ve anaerobic rods
Eikenella corrodens
Tetracyclines ---A.a
Selection of antibiotics

Fluoroquinolones(ciprofloxacin)--- enteric
rods,pseudomonas, Staphylococcus,A.a
Azithromycin ---
Enterococcus, Staphylococcus,Eikenella corrodens,
Fusobacterium nucleatum,Peptostreptococcus
Metronidazole +Amoxicillin---A.a,P.g Metronidazole +Ciprofloxacin---substitute
(Position Paper:Systemic Antibiotics in Periodontics; J Periodontol 2004;75:1553-1565.)

SERIAL AND COMBINATION ANTIBIOTIC THERAPY
why combination?
1)Synergism
2)Reduction in severity/incidence of adverse effects
3) Prevent emergence of resistance
4)Broaden spectrum of activity

Rams and Slots metronidazole along with amoxicillin and
ciprofloxacin.
metronidazole-amoxicillin combinations provided excellent
elimination of many organisms in adult and localized
aggressive periodontitis that had been treated unsuccessfully
with tetracyclines and mechanical debridement.
Metronidazole-ciprofloxacin
effective against A. actinomycetemcomitans. Metronidazole
targets obligate anaerobes, and ciprofloxacin targets facultative
anaerobes.
This is a powerful combination against mixed infections. Studies
of this drug combination in the treatment of refractory
periodontitis have documented marked clinical improvement.
therapeutic benefit --reducing or eliminating pathogenic
organisms prophylactic benefit --predominantly streptococcal
microflora.

Metronidazole + amoxicillin 250 mg/t.i.d./8 days of each drug
Metronidazole + ciprofloxacin 500 mg/b.i.d./8 days of each
drug
Antibiotic resistance
indiscriminate use
Cross Resistance: Microorganism are resistance to particular drug frequently are
resistance to other chemically related antimicrobial agent
organisms growing in biofilms are more resistant to
antibiotics than the same species growing in a planktonic
(unattached) state
slower rate of growth of bacterial species in biofilms
(Ashby et al
1994)
The growth rates of these deeper cells decreased allowing
them to survive better
the slower-growing bacteria often over express ‘‘nonspecific
defense mechanisms’’

ion-exchange resin
extracellular enzymes such as b-lactamases, formaldehyde
lyase and formaldehyde dehydrogenase may become trapped
and concentrated in the extracellular matrix, thus
inactivating susceptible, typically positively charged--
hydrophilic antibiotics.
Super-resistant bacteria
Quorum sensing
Conclusion

Position Paper:Systemic Antibiotics in Periodontics. J Periodontol
2004;75:1553-1565.
Systemic antibiotics in the treatment of periodontal diseaseJørgen slots& Miriam ting, Periodontology 2000, Vol. 28, 2002, 106–176
Clinical periodontology: Carranza 10th edition
Dental biofilms:difficult therapeutic targets Periodontology 2000, Vol. 28, 2002, 12–55
References

References
Essentials of medical pharmacology: K.D Tripathi,5th edition

Thank you!