t ib2miht +f2i - sound pain alliance
TRANSCRIPT

Please Check The Box of Your Clinic Location
BREMERTON2601 Cherry Aver Ste 200,
Bremerton, WA 98310
9927 Mickelberry Road NW,Silverdale, WA 98383
SILVERDALE
ARLINGTON16410 Smokey Point Blvd Ste 210,
Arlington, WA 98223
340 George Hopper Road Ste 1,Burlington, WA 98233
BURLINGTON
4029 Northwest Ave Ste 301,Bellingham, WA 98226
Bellingham
COVINGTON17615 SE 272nd St Ste 109,
Covington, WA 98042
11306 Bridgeport Way Ste D,Lakewood, WA 98499
LAKEWOOD
PUYALLUP
7200 S 180th St Ste 102,Tukwila, WA 98188
120 14th SE Ste D, Puyallup, WA 98371
Tukwila
PATIENT PACKET
Patient Full Name:
Patient DOB:
Primary
Secondary
Work Related?
Automobile Accident?
All of the information I have provided is correct
Patient Information
Last Name: First Name: Middle Initial: ---------- -------- ----Date of Birth: __ / __ / ___ Gender: ____ Social Security#: ________ _
Marital Status (circle one): Divorced / Married / Separated / Single / Widowed
Home Phone: Work: Cell: -------- -------- --------Address: _____________ City: ______ State: __ Zip: ___ _
E-mail:_____________ Employer: _____________ _
Work Status (circle one): Full-time/ Part-time/Not employed/Active military/Student/Retired /Self Emp
Are you on disability? Yes No
GUARANTOR'S INFORMATION SAME AS ABOVE [ ]
Last Name: First Name: Middle Initial: ---------- -------- ----
Date of Birth: __ / __ / __ Gender: ____ Relationship to patient: ________ _
Home Phone: Work: Cell: -------- --------Address: _____________ City: ______ State: Zip: ___ _
INSURANCE INFORMATION
Insurance Co.: __________ Policy#: _____________ _
Insurance Co. Phone: Group#: _____________ _
Subscriber's Name: Date of Birth:_/_/_ Relationship to patient: __ _
Insurance Co.: Policy#: ____________ _
Insurance Co. Phone: __________ Group#: _____________ _
Subscriber's Name: Date of Birth:_/_/_ Relationship to patient: __ _
Yes No Employer: __________ _
City: ________ Claim Manager Name: _______________ _
Date of Injury: __ / __ /__ Claim Manager Phone:_______ Extension: __
Yes [ ] No [ ] Do you had an Attorney? Yes [ ] No [ ]
EMERGENCY CONTACT
Name: Phone: Relationship to Patient: ---------- ------ ------
PHYSICIAN/ PHARMACY INFORMATION
Referring Physician: _______________ Phone: _________ _
Primary Care Physician: Phone: _________ _
Pharmacy: _________ _
PATIENT/ GUARDIAN SIGNATURE: DATE: ------------- ------
[ ] [ ]
Do you have an attorney?
PATIENT INFORMATION
Page 1

Sound Pain Alliance General Policies
Please read the following policies and initial next to each item to indicate your acknowledgment.
Cancellation Policy: Sound Pain Alliance (SPA) requires a 24-hour notice (Mon-Fri) for appointment cancellation. There is a $75.00 fee for follow-up appointments that are canceled without a 24-hour notice. There is a $100 fee for procedures that are canceled without a 24-hour notice. If the patient does not call or show up for their appointment, the same fees apply. If you acquire too many No Call/No Show's you may be discharged from our practice.
Initial Consultation Policy: Your first appointment is a consultation only to discuss your medical needs. Medication, narcotic or non-narcotic, is prescribed at the doctor's discretion and there is no guarantee you will receive a prescription at that visit. A urine drug screen will be collected which can take additional time to process. The results will be reviewed, and a determination made whether to provide medication management.
Opioid Therapy Policy: SPA takes a conservative approach to opioid therapy, typically prescribing a lower dose of medications. Research in the amount prescribed, continues to demonstrate that a regimen of a higher dose can result in greater risk of physical dependency, tolerance and addiction, versus a treatment plan that includes lower dosages of opioid medications that result in long- lasting positive outcomes. SPA stringently follows the Federal DEA guidelines in recommendation for prescribing opioid medications.
Disability Forms Policy: In general, as a pain management practice we do not complete disability forms or work release forms. These forms should be completed by your primary care doctor. These forms may be discussed with your provider but please do not expect our office to perform this service for you.
SPA Code of Conduct Pledge: I will always treat the staff with courtesy and respect, I understand SPA has a zero-tolerance policy regarding rude, vulgar, profane or harassing comments or actions to any staff member. This will include repeated phone calls requesting/demanding medications, or early appointments with any staff. I understand if I exhibit any of this behavior, I will be discharge from this practice immediately.
GENERAL POLICIES
Page 2

Assignment of Medical Benefits
I, (Printed legal name of primary Insurance holder), assign all medical and/or surgical benefits to which I am entitled, including private insurance and any other health plan to: Sound Pain Alliance. This assignment will remain in effect until revoked by me in writing. A photocopy of this assignment is to be considered as valid as an original. I hereby authorize said assignee to release all information necessary to secure payment. This may include related drug and/or alcohol abuse treatment, AIDS/HIV, or psychiatric information; including records protected
by federal regulations (42 CRF Part 2) as required to qualify for health benefit payment.
I understand that I am financially responsible for all charges incurred from medical treatment at this facility, whether they are paid by my insurance carrier or not, (public assistance recipients exempt). I also understand that all charges are due upon receipt of statement from this facility unless other arrangements are made with the bookkeeping department. If, for any reason, it becomes necessary for this office to engage an attorney or collection agency to secure payment from me, I agree to pay all reasonable interest charges, attorney fees and/or collection costs.
IF YOUR INSURANCE COMPANY SENDS PAYMENT TO YOU, AND YOU HAVE A BALANCE DUE AT THIS OFFICE, PLEASE ENDORSE THE CHECK AND FORWARD IT ALONG WITH THE EXPLANATION OF BENEFITS WHEN RECEIVED.
PATIENT/ GUARDIAN SIGNATURE: DATE:
ASSIGNMENT OF MEDICAL BENEFITS
Page 3
HIPPA PRIVACY AUTHORIZATION
Please Print Information Here:
Last Name: First Name: Middle Initial:
Date of Birth: / /
I, give my permission to Sound Pain Alliance Member Clinics to release information in regard to appointment dates/times and my protected health information, including but not limited to, insurance, address, phone number(s), test results, health care information and treatment to the following parties:
Name of person: Relationship to Patient:
Name of person: Relationship to Patient:
I understand that:
• I may revoke this authorization at any time, in writing. My revocation will not apply toinformation already retained, used or disclosed in response to this authorization. Unlessrevoked, the automatic expiration date will be 12 months from the date of the signature (unlessotherwise indicated.)
• Unless the purpose of this authorization is to determine payment of a claim or benefits, theprovision of treatment or payment for my care may not be conditioned upon my signing of thisauthorization.
• The information authorized for release may include information which may indicate thepresence of a communicable disease or a noncommunicable disease.
• The information authorized for verbal release also may include protected health informationrelated to mental health (RCW71.05.620)
• The information authorized for verbal release also may include drug/alcohol abuse treatmentrecords (42CFR Part 2). By signing below, I authorize any such records included in my healthinformation to be release.
PATIENT/ GUARDIAN SIGNATURE: Date:
HIPPA PRIVACY AUTHORIZATION
Page 4
PAIN DESCRIPTION
CC: What is your chief complaint today (area of the body)?_______________________________________________
1. List your painful areas (most painful to least painful): _______________________________________________2. Onset: When did the pain start? _______________________________________________3. How did the pain start (ex: injury, accident, no apparent reason)?4. What makes the pain better? (circle those that apply)
alcoholic drinks heat/cold laying down leaning forward/backward sitting standing walking
5. What makes the pain worse? (circle those that apply)
Coughing laying down physical activity laying down leaning forward/backward sitting standing walking
6. Is your pain (check one): Continuous/Constant Intermittent
If Intermittent, what time or day is your pain at its worse? Morning Afternoon Night
7. Please check all the descriptions that fit your current pain:
Sharp Aching Pins/Needles Shooting Heavy Numbness Throbbing Tender Tingling Cramping Splitting Weakness Stabbing Tiring Pulling Gnawing Sickening Hot/Burning Cutting Other: ______________
8. Does your pain travel or radiate to any other part of your body? No Yes, where: _________________9. Do you have any accidental bowel movements or urination due to pain, spine injury or surgery? No Yes10. On a scale from 0 to 10 with “0” representing no pain and “10” representing the most severe pain imaginable (ex: childbirth, broken bones) which number would best describe your pain? Please write a number for each.
Pain Score for TODAY: _________ Pain Score DAILY AVERAGE: ________ Pain Score when most SEVERE _________ Pain Score when pain is LOWEST: ________
11. Have you tried any of the following for your current pain and what relief did it give you?
Chiropractic Therapy Great Relief Short-Term Relief No Relief Massage Therapy Great Relief Short-Term Relief No Relief Physical Therapy Great Relief Short-Term Relief No Relief Acupuncture Great Relief Short-Term Relief No Relief Biofeedback or Mindfulness Great Relief Short-Term Relief No Relief
12. Have you had any of the following diagnostic tests regarding your pain? If so, when was it done?EMG: CT Scan: MRI: Myelogram: X-rays:
13. VITALS (FOR OFFICE USE ONLY)
BP.: / Pulse: o2: Resp: Wt:
Page 5
GENERAL MEDICAL HISTORY
1. Please list any prior surgeries with dates:
2. Have you ever tried procedures for the pain? No Yes, what type?(block, steroid shot, Ablation, Stimulator)_____________________________________________________________________________________
3. List any medications allergies:
4. Do you take blood thinners? No Yes, which one?__________________________
5. List all medications you have tried that are helpful:
6. List all medications you have tried that were NOT helpful:
7. Please List all Current Medications with dosages:
8. Other:
9. Other:
10. Other:
Please mark the location and the sensation of pain you are experiencing using the diagram and the symbols below:
+++ Aching XXX Burning /// Stabbing
=== Numbness 000 Pins & Needles
PAIN DIAGRAM
Page 6
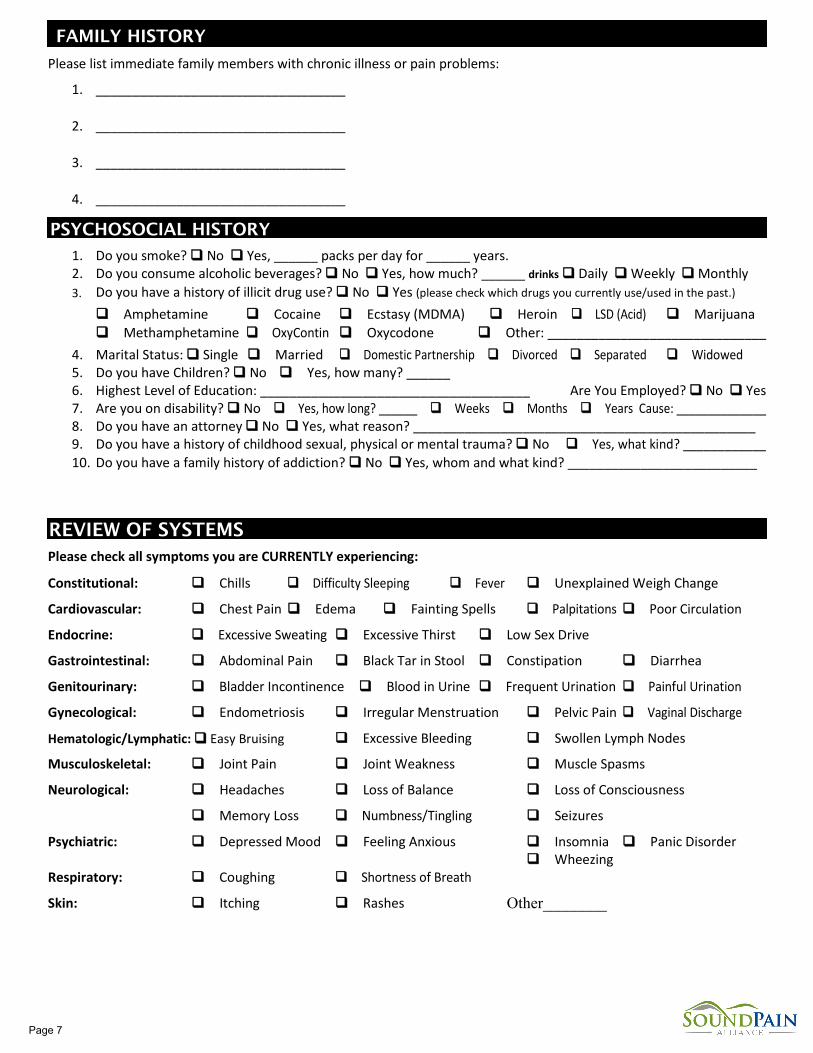
FAMILY HISTORY
Please list immediate family members with chronic illness or pain problems:
1. __________________________________
2. __________________________________
3. __________________________________
4. __________________________________
PSYCHOSOCIAL HISTORY
1. Do you smoke? No Yes, ______ packs per day for ______ years.2. Do you consume alcoholic beverages? No Yes, how much? ______ drinks Daily Weekly Monthly3. Do you have a history of illicit drug use? No Yes (please check which drugs you currently use/used in the past.)
Amphetamine Cocaine Ecstasy (MDMA) Heroin LSD (Acid) Marijuana Methamphetamine OxyContin Oxycodone Other: ______________________________
4. Marital Status: Single Married Domestic Partnership Divorced Separated Widowed5. Do you have Children? No Yes, how many? ______6. Highest Level of Education: _____________________________________ Are You Employed? No Yes 7. Are you on disability? No Yes, how long? ______ Weeks Months Years Cause: ______________8. Do you have an attorney No Yes, what reason? _______________________________________________9. Do you have a history of childhood sexual, physical or mental trauma? No Yes, what kind? ____________10. Do you have a family history of addiction? No Yes, whom and what kind? __________________________
REVIEW OF SYSTEMS Please check all symptoms you are CURRENTLY experiencing:
Constitutional: Chills Difficulty Sleeping Fever Unexplained Weigh Change
Cardiovascular: Chest Pain Edema Fainting Spells Palpitations Poor Circulation
Endocrine: Excessive Sweating Excessive Thirst Low Sex Drive
Gastrointestinal: Abdominal Pain Black Tar in Stool Constipation Diarrhea
Genitourinary: Bladder Incontinence Blood in Urine Frequent Urination Painful Urination
Gynecological: Endometriosis Irregular Menstruation Pelvic Pain Vaginal Discharge
Hematologic/Lymphatic: Easy Bruising Excessive Bleeding Swollen Lymph Nodes
Musculoskeletal: Joint Pain Joint Weakness Muscle Spasms
Neurological: Headaches Loss of Balance Loss of Consciousness
Memory Loss Numbness/Tingling Seizures
Psychiatric: Depressed Mood Feeling Anxious Insomnia Panic Disorder
Respiratory: Coughing Shortness of Breath Wheezing
Skin: Itching Rashes Other________
Page 7
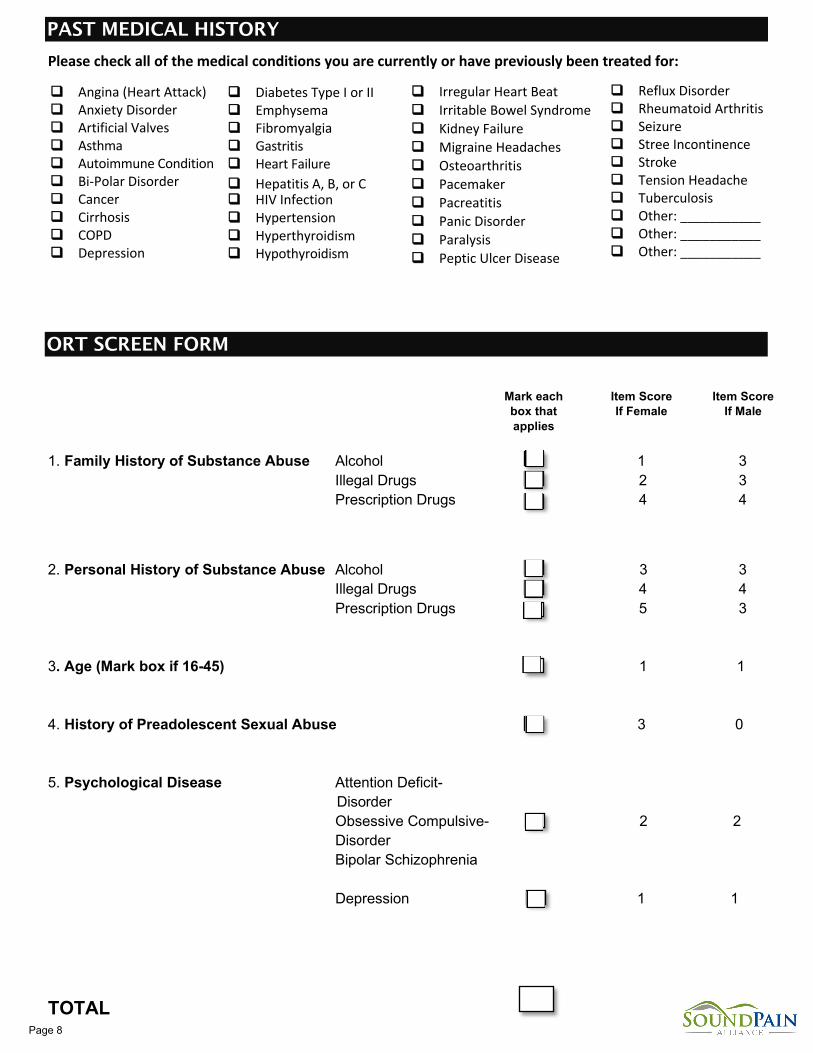
Please check all of the medical conditions you are currently or have previously been treated for:
PAST MEDICAL HISTORY
(f{@a A Di A I Val
Autaimmu e C~ndiliio11 - - I ol r o.rd r
Cancer , rrhoir ,copo D.ep:ress·on
I:
□ F C C H
H or · H
1-1
C Ii-try nthyroldlsm □ 11-'a ra ly.sis
B~ t :S. drum
I□ ypi, ','ll'i□ -d"sm · pt:i UlrtJ!r Di~~
~DPAIN - ALLIANCE -
Angina (Heart Attack) Anxiety Disorder Artificial Valves Asthma Autoimmune Condition Bi-Polar Disorder Cancer Cirrhosis COPD Depression
Diabetes Type I or II Emphysema Fibromyalgia Gastritis Heart Failure Hepatitis A, B, or C HIV Infection Hypertension Hyperthyroidism Hypothyroidism
Irregular Heart Beat Irritable Bowel Syndrome Kidney Failure Migraine Headaches Osteoarthritis Pacemaker Pacreatitis Panic Disorder Paralysis Peptic Ulcer Disease
Reflux Disorder Rheumatoid Arthritis Seizure Stree Incontinence Stroke Tension Headache Tuberculosis Other: ___________ Other: ___________ Other: ___________
1. Family History of Substance Abuse Alcohol 1 3 2 3 Illegal Drugs
Prescription Drugs 4 4
2. Personal History of Substance Abuse Alcohol 3 3 4 4 Illegal Drugs
Prescription Drugs 5 3
1 1
3 0
3. Age (Mark box if 16-45)
4. History of Preadolescent Sexual Abuse
5. Psychological Disease
2 2
Attention Deficit- Disorder
Obsessive Compulsive- Disorder Bipolar Schizophrenia
Depression 1 1
TOTAL
Mark each box that applies
Item Score If Female
Item Score If Male
ORT SCREEN FORM
Page 8
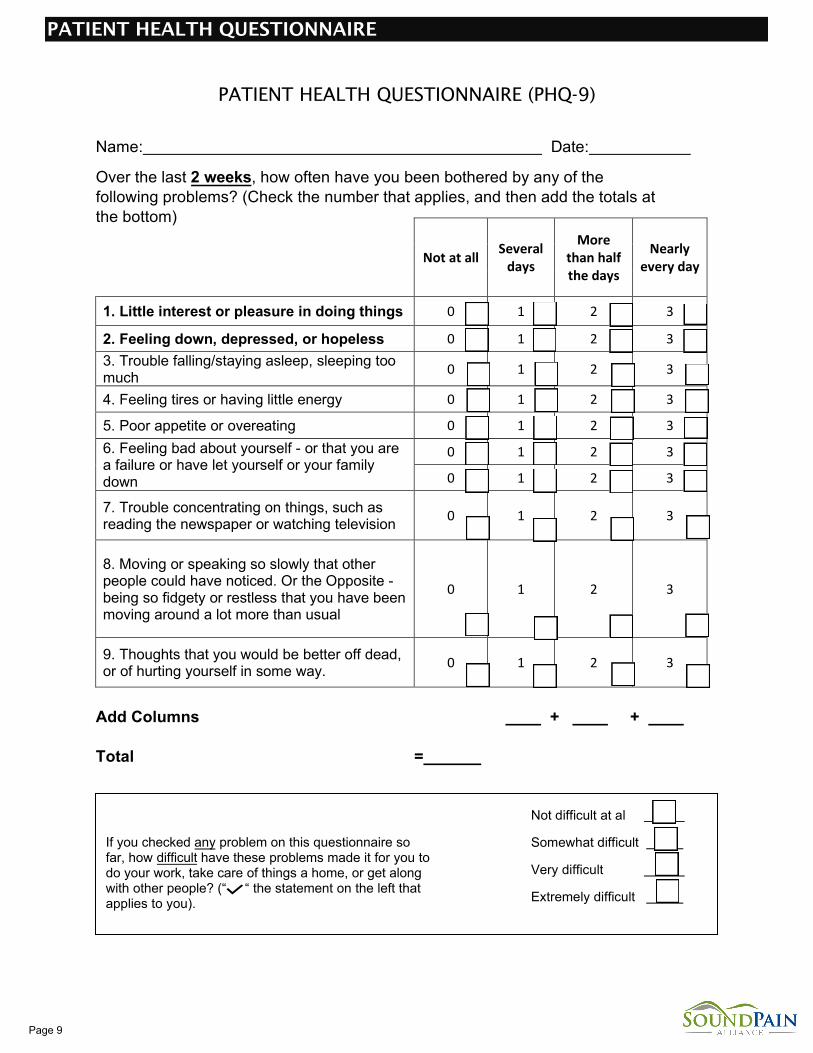
PATIENT HEALTH QUESTIONNAIRE (PHQ-9)
Name: Date:
Over the last 2 weeks, how often have you been bothered by any of the following problems? (Check the number that applies, and then add the totals at the bottom)
Not at all Several days
More than half the days
Nearly every day
1. Little interest or pleasure in doing things 0 1 2 3
2. Feeling down, depressed, or hopeless 0 1 2 3 3. Trouble falling/staying asleep, sleeping toomuch 0 1 2 3
4. Feeling tires or having little energy 0 1 2 3
5. Poor appetite or overeating 0 1 2 3 6. Feeling bad about yourself - or that you area failure or have let yourself or your familydown
0 1 2 3
0 1 2 3
7. Trouble concentrating on things, such asreading the newspaper or watching television 0 1 2 3
8. Moving or speaking so slowly that otherpeople could have noticed. Or the Opposite -being so fidgety or restless that you have beenmoving around a lot more than usual
0 1 2 3
9. Thoughts that you would be better off dead,or of hurting yourself in some way. 0 1 2 3
Add Columns + +
Total =
If you checked any problem on this questionnaire so far, how difficult have these problems made it for you to do your work, take care of things a home, or get along with other people? (“ “ the statement on the left that applies to you).
Not difficult at al
Somewhat difficult
Very difficult
Extremely difficult
PATIENT HEALTH QUESTIONNAIRE
Page 9
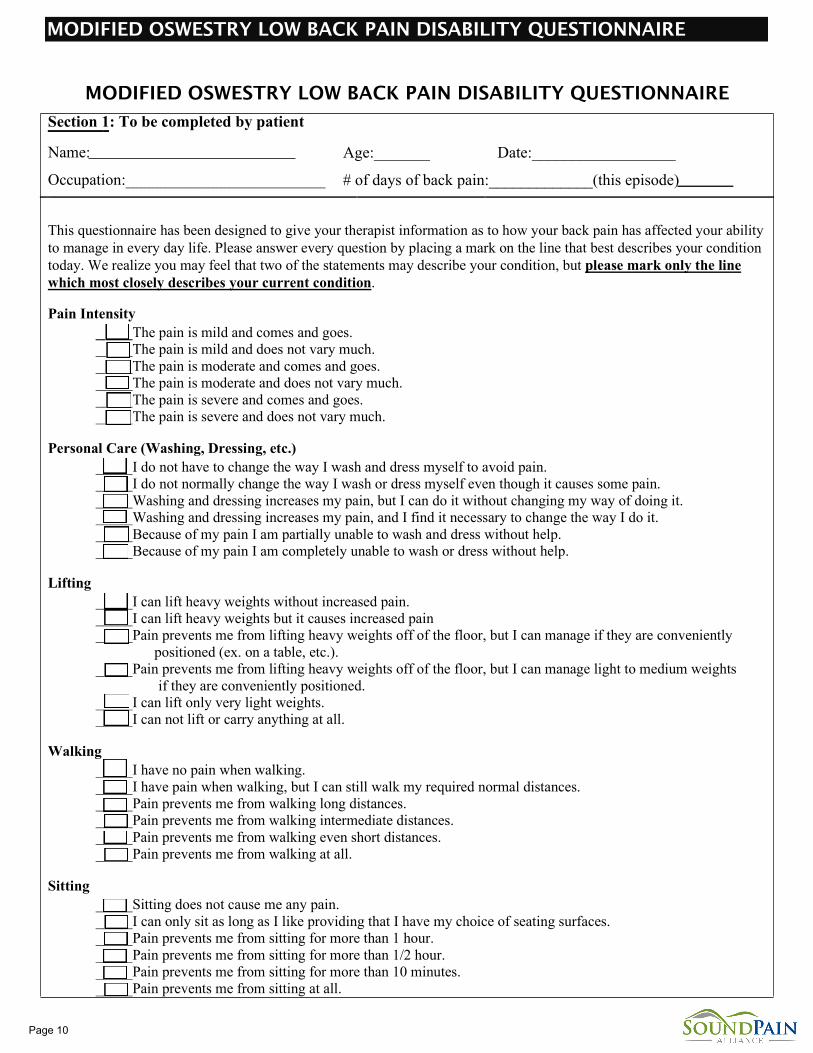
MODIFIED OSWESTRY LOW BACK PAIN DISABILITY QUESTIONNAIRE
Section 1: To be completed by patient
Name:
Occupation:_________________________
Age:_______ Date:__________________
# of days of back pain:_____________(this episode) Section 2: To be completed by patient
This questionnaire has been designed to give your therapist information as to how your back pain has affected your ability to manage in every day life. Please answer every question by placing a mark on the line that best describes your condition today. We realize you may feel that two of the statements may describe your condition, but please mark only the line which most closely describes your current condition.
Pain Intensity _____The pain is mild and comes and goes. _____The pain is mild and does not vary much. _____The pain is moderate and comes and goes. _____The pain is moderate and does not vary much. _____The pain is severe and comes and goes. _____The pain is severe and does not vary much.
Personal Care (Washing, Dressing, etc.) _____I do not have to change the way I wash and dress myself to avoid pain. _____I do not normally change the way I wash or dress myself even though it causes some pain. _____Washing and dressing increases my pain, but I can do it without changing my way of doing it. _____Washing and dressing increases my pain, and I find it necessary to change the way I do it. _____Because of my pain I am partially unable to wash and dress without help. _____Because of my pain I am completely unable to wash or dress without help.
Lifting _____I can lift heavy weights without increased pain. _____I can lift heavy weights but it causes increased pain _____Pain prevents me from lifting heavy weights off of the floor, but I can manage if they are conveniently
positioned (ex. on a table, etc.). _____Pain prevents me from lifting heavy weights off of the floor, but I can manage light to medium weights
if they are conveniently positioned. _____I can lift only very light weights. _____I can not lift or carry anything at all.
Walking _____I have no pain when walking. _____I have pain when walking, but I can still walk my required normal distances. _____Pain prevents me from walking long distances. _____Pain prevents me from walking intermediate distances. _____Pain prevents me from walking even short distances. _____Pain prevents me from walking at all.
Sitting _____Sitting does not cause me any pain. _____I can only sit as long as I like providing that I have my choice of seating surfaces. _____Pain prevents me from sitting for more than 1 hour. _____Pain prevents me from sitting for more than 1/2 hour. _____Pain prevents me from sitting for more than 10 minutes. _____Pain prevents me from sitting at all.
MODIFIED OSWESTRY LOW BACK PAIN DISABILITY QUESTIONNAIRE
Page 10
Section 2 (con’t): To be completed by patient
Standing _____I can stand as long as I want without increased pain. _____I can stand as long as I want but my pain increases with time. _____Pain prevents me from standing more than 1 hour. _____Pain prevents me from standing more than 1/2 hour. _____Pain prevents me from standing more than 10 minutes. _____I avoid standing because it increases my pain right away.
Sleeping _____I get no pain when I am in bed. _____I get pain in bed, but it does not prevent me from sleeping well. _____Because of my pain, my sleep is only 3/4 of my normal amount. _____Because of my pain, my sleep is only 1/2 of my normal amount. _____Because of my pain, my sleep is only 1/4 of my normal amount. _____Pain prevents me from sleeping at all.
Social Life _____My social life is normal and does not increase my pain. _____My social life is normal, but it increases my level of pain. _____Pain prevents me from participating in more energetic activities (ex. sports, dancing, etc.) _____Pain prevents me from going out very often. _____Pain has restricted my social life to my home. _____I have hardly any social life because of my pain.
Traveling _____I get no increased pain when traveling. _____I get some pain while traveling, but none of my usual forms of travel make it any worse. _____I get increased pain while traveling, but it does not cause me to seek alternative forms of travel. _____I get increased pain while traveling which causes me to seek alternative forms of travel. _____My pain restricts all forms of travel except that which is done while I am lying down. _____My pain restricts all forms of travel.
Employment/Homemaking _____My normal job/homemaking activities do not cause pain. _____My normal job/homemaking activities increase my pain, but I can still perform all that is required of me. _____I can perform most of my job/homemaking duties, but pain prevents me from performing more physically
stressful activities (ex. lifting, vacuuming) _____Pain prevents me from doing anything but light duties. _____Pain prevents me from doing even light duties. _____Pain prevents me from performing any job or homemaking chores.
Section 3: To be completed by provider
SCORE:___________
adapted from Hudson-Cook N, Tomes-Nicholson K, Breen A. A revised oswestry disability questionnaire. In: Roland M, Jenner J, eds. Back Pain: New Approaches to Rehabilitation and Education. New York: Manchester University Press; 1989. p. 187-204. [Prepared May 1999]
Page 11