tb diagnosis: the big picture - teachepi.org · pcr xpert mtb/rif & ultra molecular dst (lpas)...
TRANSCRIPT

TB DIAGNOSIS: THE BIG PICTURE
Madhukar Pai, MD, PhD
McGill University, Montreal

DISCLOSURES
No financial or industry conflicts
I serve as a consultant or advisor to:
FIND, Geneva
TB Alliance, New York
Stop TB Partnership, Geneva

THE PROBLEM

CRITICAL TIME FOR TB
Source: WHO 4

CRITICAL TIME FOR TB
5
2019
DIAGNOSIS: A WEAK LINK IN TB CONTROL
6

MANY TB PATIENTS STRUGGLE TO GET QUALITY DX
Missing patients and major access issues
Long, complex pathways to TB care & diagnostic delays
Broken care cascades
Challenges in getting decentralized care
Limited access to new tools
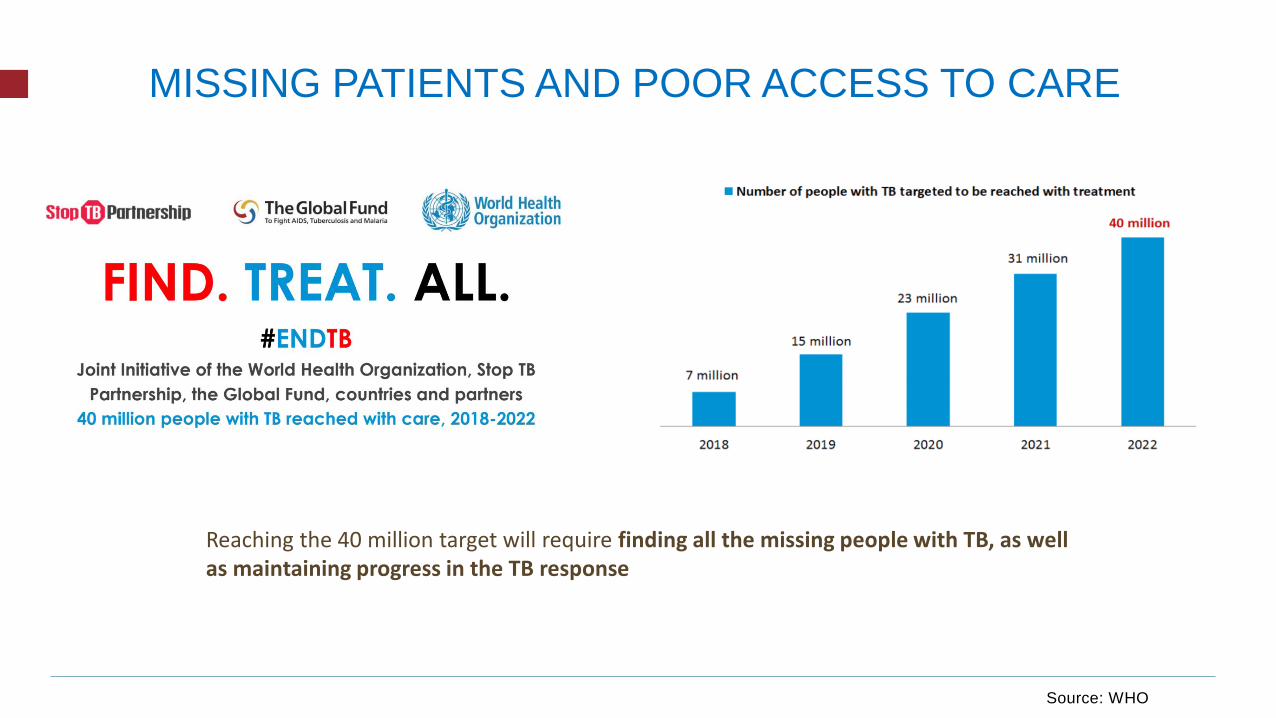
MISSING PATIENTS AND POOR ACCESS TO CARE
Reaching the 40 million target will require finding all the missing people with TB, as well as maintaining progress in the TB response
Source: WHO

Source: WHO 9

13 country patient-pathways
analysis

Multiple providers are seen before TB is detected
~2 months diagnostic delay in most HBCs
Kapoor et al. PLoS ONE 2012 Mistry et al. PLoS ONE 2016 Veesa et al. PLoS ONE 2018
DELHI MUMBAI TAMIL NADU
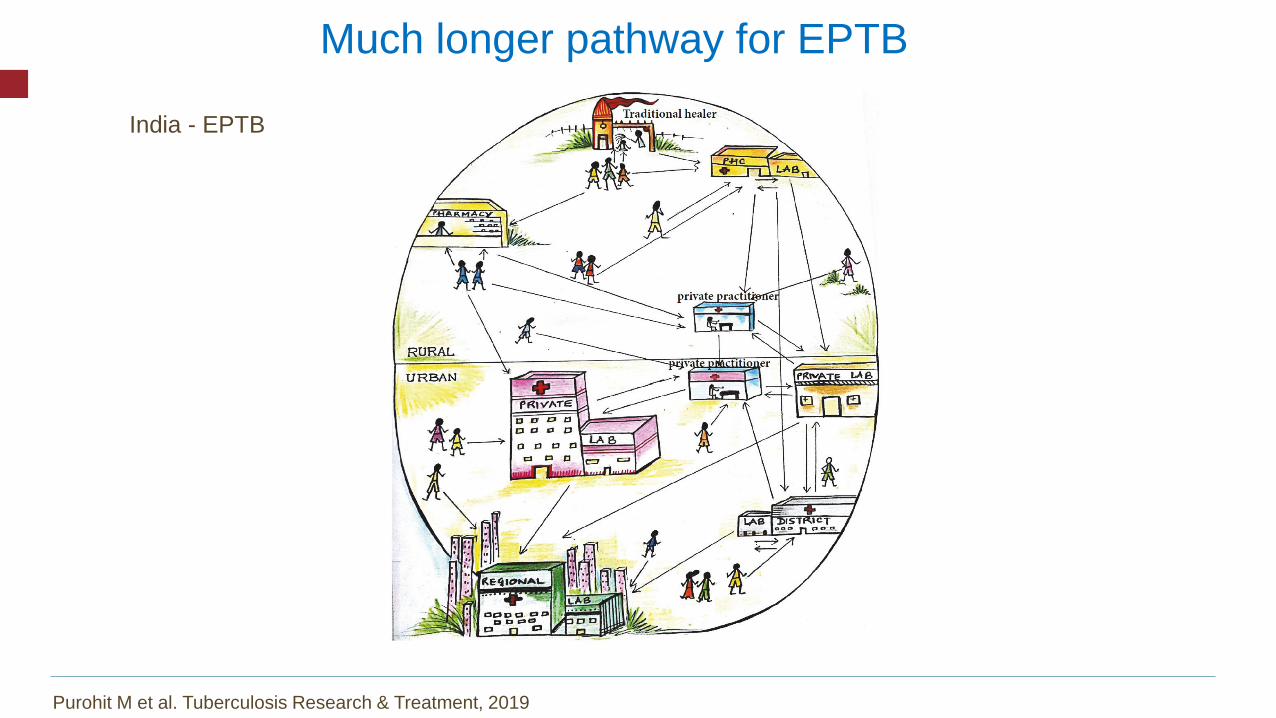
Much longer pathway for EPTB
Purohit M et al. Tuberculosis Research & Treatment, 2019
India - EPTB

Bhattacharya Chakravarty A, Rangan S, Dholakia Y, Rai S, Kamble S, et al. (2019) Such a long journey: What health seeking
pathways of patients with drug resistant tuberculosis in Mumbai tell us. PLOS ONE 14(1): e0209924.
https://doi.org/10.1371/journal.pone.0209924
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0209924
Much longer pathway for DR-TB
India – DR-TB 134 days
7 providers
167 km

Slide courtesy of Guy Stallworthy 14
In 6 of the 7 countries
with most missing cases
(65% of the global total)
private providers account
for 65%-85% of initial
care-seeking …
Percent private primary care
Striking correlation between private/informal care seeking & ‘missing patients’

EVEN WHEN PATIENTS SEEK CARE, WHAT QUALITY DO THEY GET?

30 HBCs
Cascade of care
http://www.jogh.org/documents/issue201901/jogh-09-010423.htm

Global
Cascade of care: DR-TB
Kendall E et al. Int J Tuberc Lung Dis 2019

Cascade of care: Children
https://www.sciencedirect.com/science/article/pii/S2405579417300360
Uganda & Kenya

Cascade of care: Latent TB Infection
Alsdurf H et al. Lancet Infect Dis 2016

Simulated patient studies in 4 countries show that most primary care providers do not manage TB well
www.qutubproject.org 20

SIMULATED PATIENT: CLASSIC CASE OF SUSPECTED TB
(2-3 WEEKS OF PRODUCTIVE COUGH, FEVER, WEIGHT LOSS – “PRESUMED TB”)
www.qutubproject.org 21

RESULTS FROM 4 COUNTRIES
www.qutubproject.org 22Das et al. (2015); Kwan et al. (under review); Daniels et al. (2017); Sylvia et al. (2017); Christian et al. (2018); Daftary A et al. unpublished
Setting - Sector % Correctly Managed % Referred
Delhi, India – private sector 21% 10%
Mumbai, India – private sector 37% 15%
Patna, India – private sector 33% 10%
Nairobi, Kenya – public & private
33 – 40%
Public: 79% asked for sputum test
Private: 36% asked for sputum test
4% - 10%
Rural China (3 provinces) - public
28%, village clinics
38%, township centers
90%, county hospitals
28%, village clinics
18%, township centers
5%, county hospitals
South Africa – public
(Western & Eastern Cape)
43% got TB and HIV tests
84% got sputum TB tests
South Africa – private
(KZN)35% 26%

DOTS coverage What about quality?
MOST TB PROGRAMS STILL FOCUS ON COVERAGE, NOT QUALITY!

24https://naturemicrobiologycommunity.nature.com/users/20892-madhukar-pai/posts/32859-science-of-improvement-tb-cannot-afford-to-lag-behind

TB DX: ACCESS
25

ACCESS TO NEW TOOLS: XPERT MTB/RIF
Cazabon D, Pande T, et al. Gates Open Res 2018

ACCESS TO NEW TOOLS: URINE LAM RAPID TEST
DRC
Nig
eria
4 of 21
countries
are
currently
using LF-
LAM*
DRC
Nig
eria
9 of 21
countries
include
LF-LAM in
a national
policy
DRC
Nig
eria
13 of 21
countries
plan on
using LF-
LAM in the
near
future
*Irrespective of inclusion in national policy
Does your
country’s national
policy include
LF-LAM test in its
TB or HIV
program?
Is your country
currently using the
LF-LAM test?
Do you plan on
using the LF-
LAM test in the
near future?
Singhroy D, et al. Unpublished

TB DX: WHAT ARE THE NEEDS?
28

TOOLS WE HAVE TODAY?
Tuberculin IGRAs
Conventional
microscopyLED/FM
microscopy
Solid cultures Liquid cultures
Conventional
PCR
Xpert MTB/RIF & Ultra
Molecular DST (LPAs)Conventional,
phenotypic
DST
29
TB LAMP
Urine LAM
Included in
1st WHO
Essential
Diagnostics
List

NEEDS ASSESSMENT AND TPPS
Priority needs TPPs
30Kik S et al. ERJ 2014
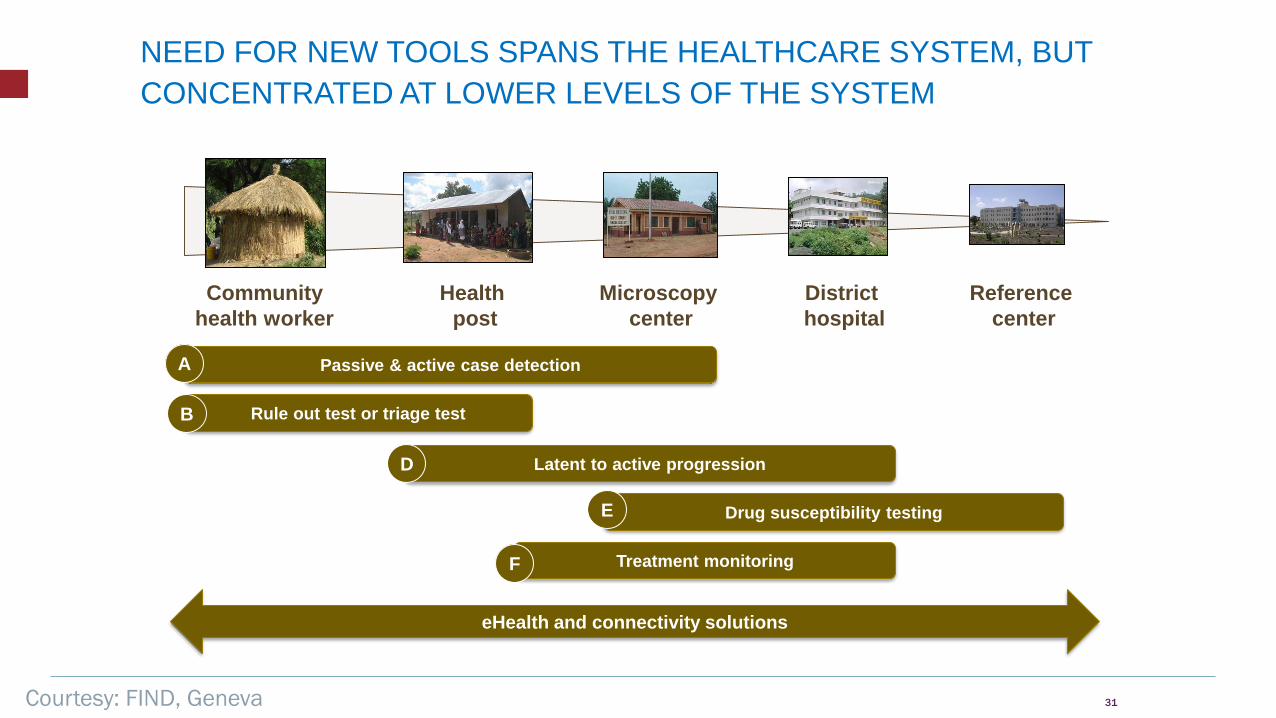
NEED FOR NEW TOOLS SPANS THE HEALTHCARE SYSTEM, BUT
CONCENTRATED AT LOWER LEVELS OF THE SYSTEM
31
Reference
center
District
hospital
Microscopy
center
Health
post
Community
health worker
Passive & active case detection
Rule out test or triage test
Latent to active progression
Drug susceptibility testing
Treatment monitoring
A
B
D
E
F
eHealth and connectivity solutions
Courtesy: FIND, Geneva

WE NEED BETTER TOOLS FOR LATENT TB
Pai M, et al. Nature Rev Dis Primer 2016 32

© Bill & Melinda Gates Foundation | 33

TB DX: WHAT IS THE CRITICAL PATHWAY?
34

THE IDEAL: SINGLE, LINEAR VALUE CHAIN


VALLEYS OF DEATH!
http://gbchealth.org/crossing-the-valleys-of-death-in-tb-from-development-to-roll-out/
UPSTREAM CHALLENGES: BIOMARKER DISCOVERY AND VALIDATION
38
https://www.bm2dx.org/

DOWNSTREAM CHALLENGES: PRODUCTS TO IMPACT
39Schumacher S et al. PLOS ONE 2016.
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0151073

IN MONTREAL, XPERT MTB/RIF HAD LITTLE IMPACT
“Limited potential impact of Xpert testing in high-
resource, low-incidence ambulatory settings due to
lower sensitivity in the context of less extensive
disease, and limited potential to expedite diagnosis
beyond what is achieved with the existing, well-
performing diagnostic algorithm.”
CID 2014:58 (1 April)
40

IN IQALUIT, XPERT MTB/RIF HAD A POSITIVE IMPACT
“In a predominantly Inuit population …where the burden of TB
is high and no TB testing facilities are available, on-site Xpert
was feasible, accurate and shortened time to TB treatment
initiation.”
Alvarez G et al. CHEST 2015 41

SO, OUR MONTREAL GENEXPERT MACHINE IS NOW SERVING PATIENTS IN RURAL INDIA!

CAN WE RE-IMAGINE TB CARE*?
*ONGOING WORK WITH STOP TB PARTNERSHIP43

44https://www.huffingtonpost.ca/dr-madhukar-pai/tuberculosis-cure-treatment-research_a_23449596/?utm_hp_ref=ca-blogs

ACTIVE TB CARE: REIMAGINED
Presumed TB
Rapid Triage Rapid Dx & DST Sequencing
confirmation
Short drug regimensPatient support & benefits,
adverse event management
Test for treatment
response & cure
eTB ICT
& dashboardNew vaccine
Early care
seeking &
clinical
assessment
Systematic
screening

CHILDHOOD TB CARE: REIMAGINED
Possible TB
Rapid Triage Sputum and non-sputum
based rapid Dx & DST for
PTB and EPTB
Sequencing
confirmation
Short drug regimens
Child-friendly formulationsAdherence, nutritional & family supportTest for treatment
response & cure
eTB ICT
& dashboardNew vaccine
Early care
seeking &
clinical
assessment
Contact & systematic
screening

LATENT TB CARE: REIMAGINED
At risk for infection
&/or progression Diagnosis of infection Rule out disease
Short drug regimens
eTB ICT
& dashboardVaccine to
prevent infection
Risk & clinical assessment
1HP
3HP
4R
Risk/benefit
assessment
Vaccine to
stop
progressionPredictive
correlate of
risk signature
Test for treatment
response & cureClient support & benefits,
adverse event management

VaccinationEarly care seeking
TriageSample
transport & diagnostics
SequencingNew drug regimens
Adherence
Patient Support &
Direct Benefits
ICT, dashboard
& AI
PRODUCT ECOSYSTEM

TB CARE TODAY IS DESIGNED FROM A
PUBLIC HEALTH APPROACH & IS
AIMED AT ‘DISEASE CONTROL’

HUMAN-CENTERED DESIGN TO IMPROVE
TB CARE

PATIENTS’ WISH LIST FOR TB CARE
Active side effects
monitoring
High quality clinical care
Short & sweet
regimen
Targeted information
Peer based counselling
Treated with dignity
Access to mental
health care
Family involvement
Skills building activities
Legal and social
protection
1-stop shop services
Post survival support

11 YEARS TO 2030!
52