thalassemia: prenatal screening & diagnosis - ogshk.org · copyright © 2016. all rights...
TRANSCRIPT

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Wah Yi Man
Thalassemia:
Prenatal Screening & Diagnosis
• Associate consultant
• Department of Obstetrics & Gynaecology
• Prince of Wales hospital

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Thalassaemia
Most common hereditary disease and single-gene defect in Hong Kong
Lau et al NEJAM 1997
Prevalence of alpha thalassaemia 5%

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Thalassaemia
Most common hereditary disease and single-gene defect in Hong Kong
Lau et al NEJAM 1997
Prevalence of beta thalassaemia 3.1%

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Prenatal Screening and Diagnosis
Pregnant woman
Carrier screen by MCV fetus no risk Mother not carrier
May thal carrier be missed with normal MCV (false –ve)? Possible false -ve: • Single α-globin gene deletion (silent α-carrier; 75%
normal MCV)

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Prenatal Screening and Diagnosis
Pregnant woman
Carrier screen by MCV fetus no risk Mother not carrier
May thal carrier be missed with normal MCV (false –ve)? Possible false -ve: • Single α-globin gene deletion (silent α-carrier; 75%
normal MCV) • Single α –gene mutations
• e.g. Hb Constant Spring, Hb QuongSze
Stop codon mutate

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Prenatal Screening and Diagnosis
Pregnant woman
Carrier screen by MCV fetus no risk Mother not carrier
May thal carrier be missed with normal MCV (false –ve)? Possible false -ve: • Single α-globin gene deletion (silent α-carrier; 75%
normal MCV) • Single α –gene mutations
• e.g. Hb Constant Spring, Hb QuongSze
• Rare silent β-thalassaemia mutation(β++/βN )
chr 11p15.5
5’ 3’ β LCR δ Aγ ε
Gγ

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Prenatal Screening and Diagnosis
Pregnant woman
Carrier screen by MCV fetus no risk Mother not carrier
May thal carrier be missed with normal MCV (false –ve)? Possible false -ve: • Single α-globin gene deletion (silent α-carrier; 75%
normal MCV) • Single α –gene mutations
• e.g. Hb Constant Spring, Hb QuongSze
• Rare silent β-thalassaemia mutation(β++/βN ) • Hb E carrier (50% normal MCV) (mutation in β globin gene)
chr 11p15.5
5’ 3’ β LCR δ Aγ ε
Gγ

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Prenatal Screening and Diagnosis
Pregnant woman
Carrier screen by MCV fetus no risk Mother not carrier
May thal carrier be missed with normal MCV (false –ve)? Possible false -ve: • Single α-globin gene deletion (silent α-carrier; 75%
normal MCV) • Single α –gene mutations
• e.g. Hb Constant Spring, Hb QuongSze
• Rare silent β-thalassaemia mutation(β++/βN ) • Hb E carrier (50% normal MCV) • Hereditary Persistence of Fetal Hb (HPFH) Does it matter to miss the above?
Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
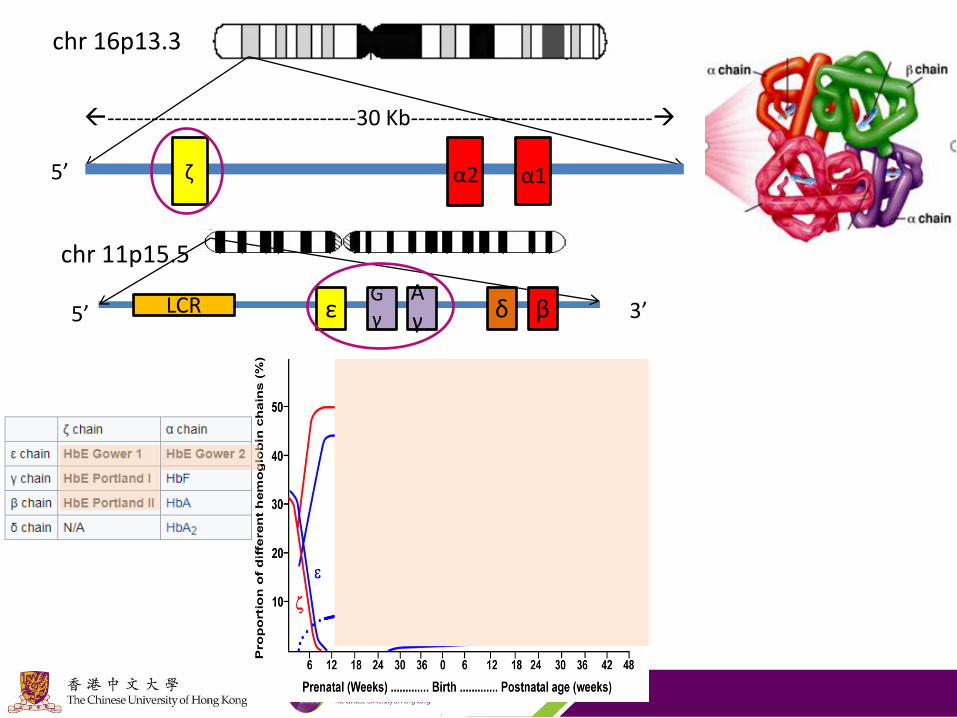
chr 16p13.3
ζ α2 α1 5’ 3’
----------------------------------30 Kb---------------------------------
chr 11p15.5
5’ 3’ β LCR δ Aγ ε
Gγ

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
chr 16p13.3
ζ α2 α1 5’ 3’
----------------------------------30 Kb---------------------------------
chr 11p15.5
5’ 3’ β LCR δ Aγ ε
Gγ

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
chr 16p13.3
ζ α2 α1 5’ 3’
----------------------------------30 Kb---------------------------------
chr 11p15.5
5’ 3’ β LCR δ Aγ ε
Gγ
At birth: 50-80% HbF Adult Hb pattern at ~ 1 year of life HbF <1.1% HbA ~97% HbA2 <3.5%

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
α- globin gene Deletions

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
α- globin multigene clusters at chromosome 16p13.3: sites of
common Deletions
chr 16p13.3
ζ α2 α1 5’ 3’
----------------------------------30 Kb---------------------------------
--SEA
--FIL
--THAI
--MED
α0(--/)
α+ (-α/)
-α3.7
-α4.2
(normal MCV)
10 different α+ deletion
> 40 different α0 deletion
Normal Silent Minor HbH Hb Barts (αα/αα) > (-α/αα) > (--/αα), (-α/-α) > (--/-α) > (--/--)

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
α- globin gene Mutations

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
α- globin multigene clusters at chromosome 16p13.3:
Mutations
chr 16p13.3
ζ α2 α1 5’ 3’
----------------------------------30 Kb---------------------------------
Mutations affect α2 (αTα/) much more than α1 (ααT/) • At least 90 mutations reported
• e.g. Hb Constant Spring (αCSα/) and Hb Guong Sze (αQSα/) • Produce unstable α- globin chains, worsen phenotype
Normal Silent Minor HbH Hb Barts (αα/αα) > (-α/αα) > (--/αα), (-α/-α) > (--/-α) > (--/--)
(--/αTα) Non-deletional HbH hydrops (αTα/αα)

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
β- globin gene Mutations

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
β- globin multigene clusters at chromosome 11p15.5:
Mutations
chr 11p15.5
5’ 3’ β LCR δ Aγ ε Gγ
• Mutations may cause ↓β- globin production (>300 variants): complete absence (β0/)
severe reduction (β+/) mild reduction (β++/)
Normal Silent Minor Intermedia Major βN/βN > β ++/βN > β0/βN , β+/βN, > β+/β+ > β+/β0 > β0/β0
Coinherited modifying ameliorating genetic factors could result in milder phenotype

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
β- globin multigene clusters at chromosome 11p15.5:
Mutations
chr 11p15.5
5’ 3’ β LCR δ Aγ ε Gγ
Normal Silent Minor Intermedia Major βN/βN > β ++/βN > β0/βN , β+/βN, > β+/β+ > β+/β0 > β0/β0
Clinical severity depends on the extent of alpha/nonalpha globin chain imbalance Ameliorating genetic factors • Reduce alpha chain output
Co-inherited alpha thalassaemia • β0/β0 plus -α/-α or ααT/αα more likely thalassaemia
intermedia phenotype • β0/β0 plus -α/αα more likely thalassaemia major phenotype
• High HbF production • Deltabeta thalassaemia, beta promoter deletion • Hereditary persistent fetal haemoglobin
Involve hematologist for counselling
Milder phenotype resulting from coinherited modifying ameliorating genetic factors

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
β- globin multigene clusters at chromosome 11p15.5:
Mutations
chr 11p15.5
5’ 3’ β LCR δ Aγ ε Gγ
• Mutations may cause ↓β- globin production (>300 variants): complete absence (β0/)
severe reduction (β+/) mild reduction (β++/)
• Mutations may produce abnormal or unstable Hb variants, e.g. HbE (βE), Hb Lepore (δβ+ thal)
Normal Silent Minor Intermedia Major βN/βN > β ++/βN > β0/βN , β+/βN, > β+/β+ > β+/β0 > β0/β0
50% HbE/βN 50% HbE/HbE> HbE/β+ HbE/β0
may need repeated transfusion in childhood,phenotype become more stable later in adolescent

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
β- globin gene Deletions

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
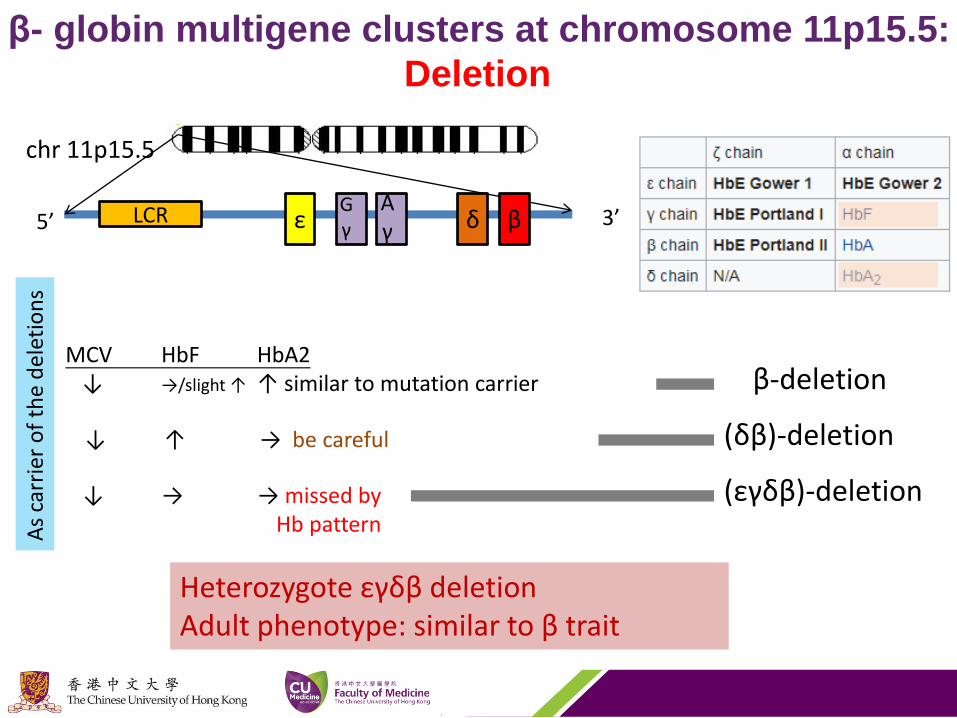
β- globin multigene clusters at chromosome 11p15.5:
Deletion
β-deletion
(δβ)-deletion
(εγδβ)-deletion
chr 11p15.5
5’ 3’ β LCR δ Aγ ε
Gγ
(δβ)0: increased HbF, reduced HbA2
MCV HbF HbA2 ↓ →/slight ↑ ↑ similar to mutation carrier
↓ ↑ → be careful
↓ → → missed by Hb pattern A
s ca
rrie
r o
f th
e d
elet
ion
s
Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
β- globin multigene clusters at chromosome 11p15.5:
Deletion
β-deletion
(δβ)-deletion
(εγδβ)-deletion
chr 11p15.5
5’ 3’ β LCR δ Aγ ε
Gγ
(δβ)0: increased HbF, reduced HbA2
MCV HbF HbA2 ↓ →/slight ↑ ↑ similar to mutation carrier
↓ ↑ → be careful
↓ → → missed by Hb pattern A
s ca
rrie
r o
f th
e d
elet
ion
s
Heterozygote εγδβ deletion Adult phenotype: similar to β trait

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
β- globin multigene clusters at chromosome 11p15.5:
Deletion
β-deletion
(δβ)-deletion
(εγδβ)-deletion
chr 11p15.5
5’ 3’ β LCR δ Aγ ε
Gγ
(δβ)0: increased HbF, reduced HbA2
MCV HbF HbA2 ↓ →/slight ↑ ↑ similar to mutation carrier
↓ ↑ → be careful
↓ → → missed by Hb pattern A
s ca
rrie
r o
f th
e d
elet
ion
s
more than 40 types of deletion
→ ↑ → Hereditary Persistence of Fetal Hemoglobin (HPFH)
↑γ-expression (Not deletion)

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
β- globin multigene clusters at chromosome 11p15.5:
Deletion
β-deletion
(δβ)-deletion
(εγδβ)-deletion
chr 11p15.5
5’ 3’ β LCR δ Aγ ε
Gγ
(δβ)0: increased HbF, reduced HbA2
MCV HbF HbA2 ↓ →/slight ↑ ↑ similar to mutation carrier
↓ ↑ → be careful
↓ → → missed by Hb pattern A
s ca
rrie
r o
f th
e d
elet
ion
s
more than 40 types of deletion
→ ↑ → Hereditary Persistence of Fetal Hemoglobin (HPFH)
↑γ-expression (Not deletion)
Homozygote δβ-thalassemia 100% HbF Phenotype: thalassemia intermedia rather than thalassemia major Homozygote HPFH Phenotype: benign

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Prenatal Screening and Diagnosis
Pregnant woman
Carrier screen by MCV fetus minimal risk Mother not carrier
Hb pattern, Fe status, Father of preg Hb status
Not carriers of the same type
fetus no risk
May thalassaemia carrier be missed by Hb pattern?
May miss rare types of thalassaemia carriers that may cause fetal anaemia, and thalassaemia intermedia postnatally

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
‘Hb Pattern’
High-performance liquid chromatography (HPLC)
Hb Electrophoresis

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
H Inclusion bodies
• Inclusion bodies = HbH:β4 – β chains excess relatively to α chains
• Presence of HbH indicates α-thal carrier (3 genes or 2 genes deletion) – in HK: mostly (--/αα), less likely (-α/-α)
• Absence of HbH inclusions does not preclude α-carrier state
– 1 gene deletion, mutation, or even in 2 genes deletion, esp in Fe deficiency
– αβ carrier (in 7% of β carrier): no relative β chains excess
• Specific but not very sensitive

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Hb Electrophoresis
Barrett et al Best Pr OG 2017
Cellulose acetate Citrate agar
• Different hemoglobins run at different
speed under different electrophoresis
HbA2 false –ve • Fe def may mask β carriers • (δβ)-deletion carriers (HbF ↑) • (εγδβ)-deletion carriers (HbF→) • β++ (silent carrier) benign • HPFH (HbF ↑) benign

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Maternal Paternal Fetus Remark
α MCV=N α-carrier / N If paternal αTα: fetal (--/αTα)
α α α-major / carrier / N
α β Carrier of either α, β, or αβ / N
If paternal αβ carrier: fetal ¼ α-major; So need paternal α-gene study
α Inconclusive α-carrier / N If paternal (αTα/αα) : fetal (--/αTα)
β MCV=N β-carrier / N If paternal HbE: fetal HbE/β0 If maternal αβ carrier, Paternal αTα: fetal (--/αTα)
β β β-major / carrier/ N Rarely both αβ carriers (7%*7%),* ¼ α-major
β α Carrier of either α, β, or αβ / N
If maternal αβ carrier: fetal ¼ α-major; So need paternal α-gene study
β Inconclusive β-carrier / N If paternal (εγδβ)0-carrier: fetal ¼ β-major If paternal (αTα/αα) + maternal αβ carrier: fetal (--/αTα)
Inconclusive: low MCV but no inclusion bodies and HbA2 / HbF not increased, no Fe def

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Unusual Case 1
Wife: low MCV; confirmed alpha thal carrier
Husband: normal MCV
Fetal cardiomegaly; anaemia (increased MCA-PSV)
• DDx: – Husband not the father
– Other causes of fetal anaemia / cardiomegaly (Rh, Parvovirus etc)
– Husband is non-deletional a thal carrier (constant spring / QuongSze) with normal MCV
– Uniparental disomy (chr 16)
Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
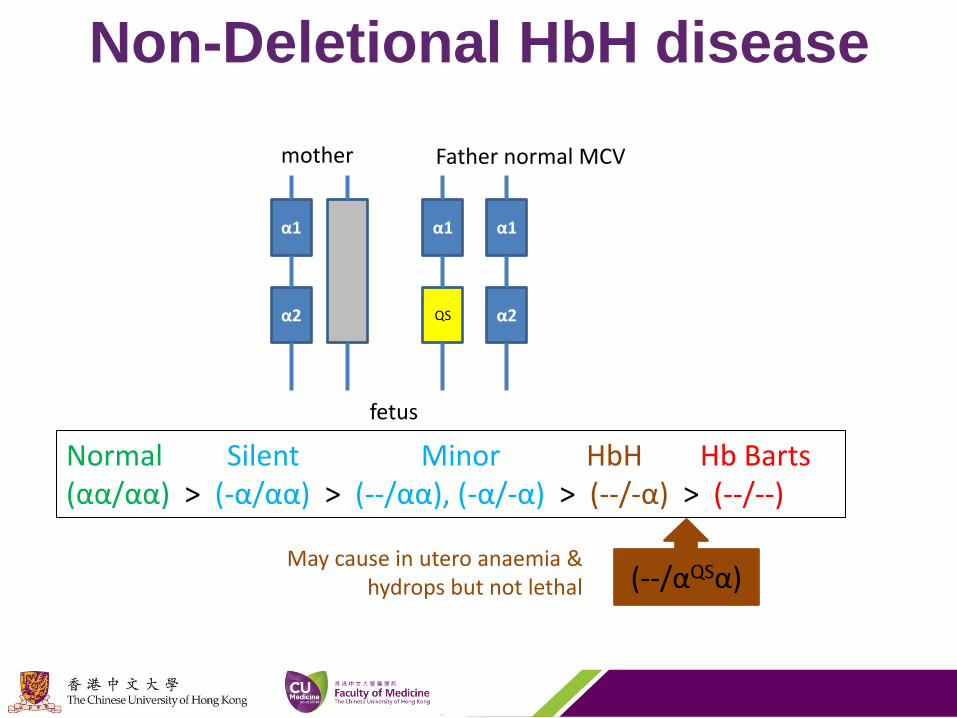
Non-Deletional HbH disease
α1
α2
α1
QS
α1
α2
Father normal MCV mother
fetus
(--/αQSα) May cause in utero anaemia &
hydrops but not lethal
Normal Silent Minor HbH Hb Barts (αα/αα) > (-α/αα) > (--/αα), (-α/-α) > (--/-α) > (--/--)

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
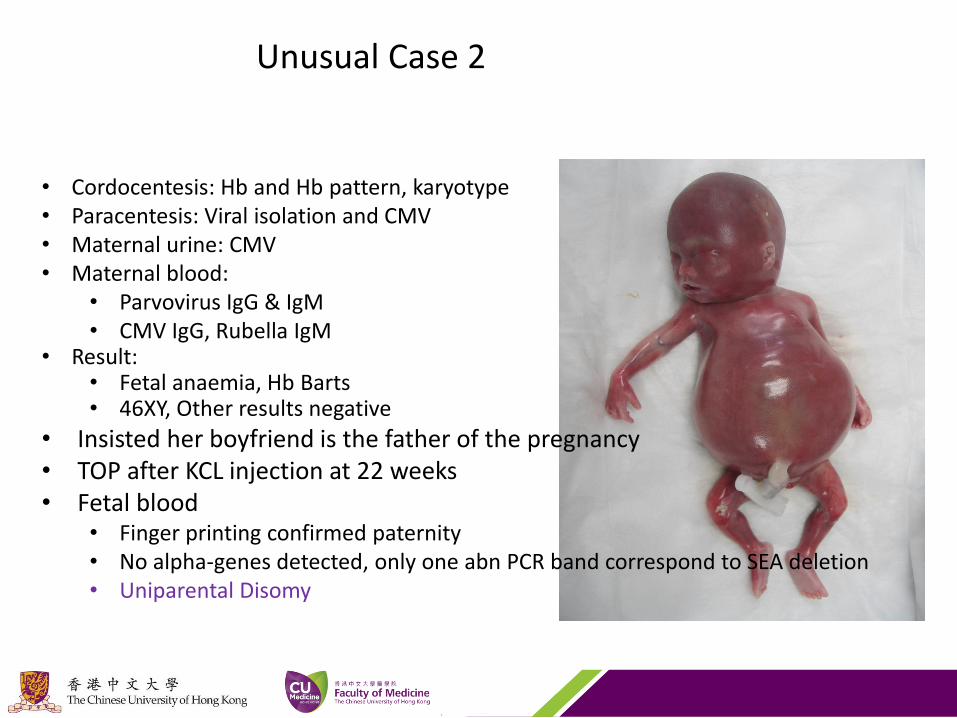
Unusual Case 2
30 year old P0, single and unemployed Mother: alpha-thal carrier but ‘father of pregnancy’ ’s MCV normal Fetal hydrops at 20 weeks
Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Unusual Case 2
• Cordocentesis: Hb and Hb pattern, karyotype • Paracentesis: Viral isolation and CMV • Maternal urine: CMV • Maternal blood:
• Parvovirus IgG & IgM • CMV IgG, Rubella IgM
• Result: • Fetal anaemia, Hb Barts • 46XY, Other results negative
• Insisted her boyfriend is the father of the pregnancy • TOP after KCL injection at 22 weeks • Fetal blood
• Finger printing confirmed paternity • No alpha-genes detected, only one abn PCR band correspond to SEA deletion • Uniparental Disomy

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
• One parent is (--/αα) while other is normal • Transmission from the carrier-parent the abnormal chromosome (--),
which then duplicate, but not from the normal parent • Chr 16 is a common site for trisomic rescue and UPD
Uniparental Disomy chr 16
α1
α2
α1
α2
father mother
fetus
α1
α2
UPD

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
• 29 year old P0, normal MCV, Rh+ve • 20wk USG: Fetal cardiomegaly, high MCA PSV • Further maternal Ix:
– Hb pattern normal – Kleihauer-Betke test, screening for parvovirus, CMV and toxoplasmosis all –ve
• Father of pregnancy: – Unremarkable prenatal course, age 13 incidental finding of low MCV – Hb A2 2.8%, Hb F 0.8%, but no Hb H inclusion bodies were identified ; could not rule out a-thal – No alpha gene deletion or mutation
• Amniocentesis: CMA deletion:
Unusual case 3
chr 11p15.5
5’ 3’ β LCR δ Aγ ε Gγ
εγδβ0/βN carrier: fail to produce enough fetal Hb, need in-utero transfusion After birth: beta minor only (inherited from father)
Hui et al hematol 2017

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Conclusion
Primary carrier screening base on MCV level
May miss rare types of thalassaemia carriers which may
cause fetal anaemia, and thalassaemia intermedia
postnatally
Secondary screening by Hb pattern
Need parental genetic studies to rule out occult carrier
status in some special conditions
Inconclusive Hb pattern result may miss rare types of
thalassaemia

Copyright © 2016. All Rights Reserved. Faculty of Medicine, The Chinese University of Hong Kong
Thank you