the architecture of medical imaging
TRANSCRIPT

The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 9
MRI Safety Planning Implications
MRI suite with 3 scanners
21
Future 4th Scanner
3
Imaging Department
© 2008 Anshen+Allen
ZONE 1
MRI Safety Planning Implications
MRI suite with 3 scanners
21ZONE 2
Future 4th Scanner
3
Imaging Department
© 2008 Anshen+Allen
ZONE 1
MRI Safety Planning Implications
MRI suite with 3 scanners
21ZONE 2
Future 4th Scanner
3
Imaging Department
© 2008 Anshen+Allen
ZONE 1
ZONE 3
MRI Safety Planning Implications
MRI suite with 3 scanners
21ZONE 2
ZONE 4
Future 4th Scanner
3
Imaging Department
© 2008 Anshen+Allen
ZONE 1
ZONE 3
MRI Safety Planning Implications
Secure MRI suite boundary (Zones 3 & 4)
© 2008 Anshen+Allen
MRI Safety Planning Implications
Secure MRI suite boundary (Zones 3 & 4)Secure MRISecure MRI suite door
© 2008 Anshen+Allen

The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 10
MRI Safety Planning Implications
Secure MRI suite boundary (Zones 3 & 4)Secure MRISecure MRI suite door
Through-traffic does not enter MRI suite
© 2008 Anshen+Allen
MRI Safety Planning Implications
© 2008 Anshen+Allen
MRI Safety Planning Implications
One Tech can see 2 MRI rooms
© 2008 Anshen+Allen
MRI Safety Planning Implications
One Tech can see 2 MRI rooms
Both TechsBoth Techs can see entrance to “Security Vestibule”
© 2008 Anshen+Allen
MRI Safety Planning Implications
One Tech can see 2 MRI rooms
Both TechsBoth Techs can see entrance to “Security Vestibule”
Security-controlled Corridor
© 2008 Anshen+Allen
Direction of Door Swing Into Scan Room During a quench, cryogenic gas fills the scan room and depletes 02
© 2008 Anshen+Allen

The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 11
Direction of Door Swing Into Scan Room During a quench, cryogenic gas fills the scan room and depletes 02
If the door swings in, i dincreased room pressure can make it difficult to exit quickly.
© 2008 Anshen+Allen
Direction of Door Swing Into Scan Room During a quench, cryogenic gas fills the scan room and depletes 02
If the door swings in, i dincreased room pressure can make it difficult to exit quickly.
If the door swings out it will be easier to exit.
© 2008 Anshen+Allen
“Handed” vs. “Mirrored” Rooms “Handed” Inpatient Rooms
Designed for safety because everything is in the same place
Do providers get disoriented (which patient)?patient)?
Need to provide distinguishing visible landmarks
Where is the evidence?
© 2008 Anshen+Allen
“Handed” X-ray Rooms
Designed for safety because everything is in the same place
Do providers get disoriented (which patient)?patient)?
Need to provide distinguishing visible landmarks
Where is the evidence?
© 2008 Anshen+Allen
“Mirrored” X-ray Rooms
Designed for safety because one technologist can supervise multiple rooms
Staff travel distancesStaff travel distances tend to be shorter than with “handed rooms”
Where is the evidence?
© 2008 Anshen+Allen
The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 12
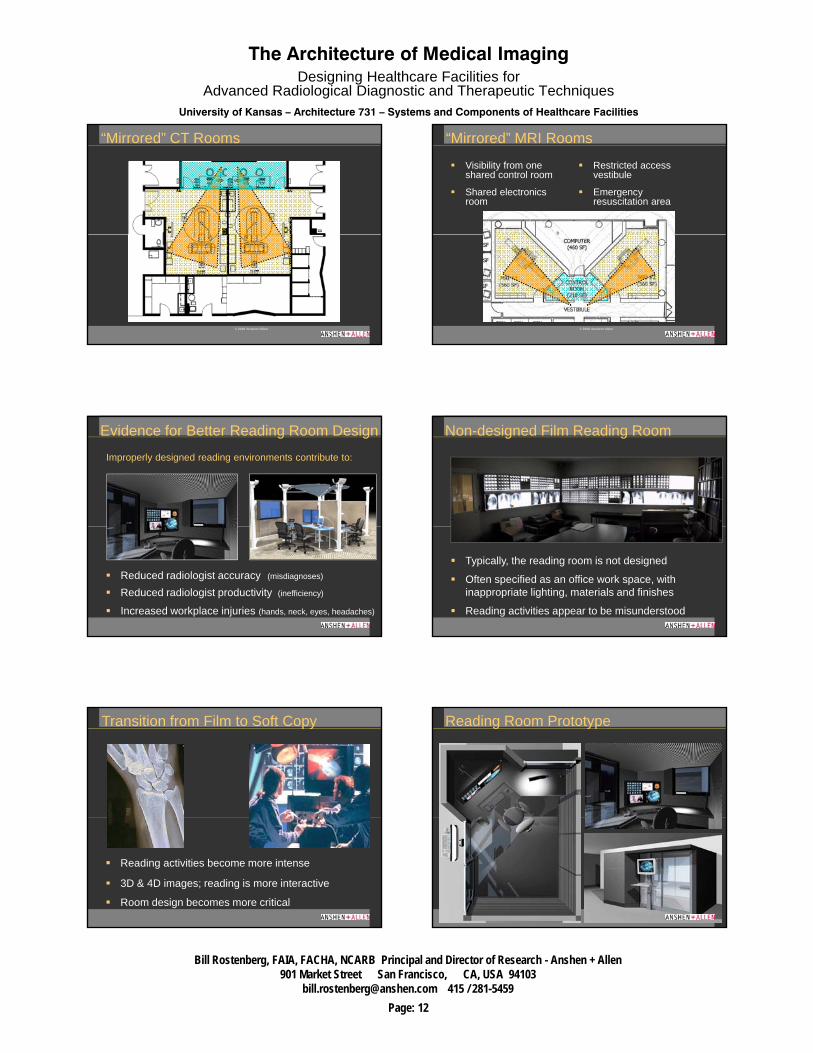
“Mirrored” CT Rooms
© 2008 Anshen+Allen
“Mirrored” MRI Rooms
Visibility from one shared control room
Shared electronics room
Restricted access vestibule
Emergency resuscitation area
© 2008 Anshen+Allen
Improperly designed reading environments contribute to:
Evidence for Better Reading Room Design
Reduced radiologist accuracy (misdiagnoses)
Reduced radiologist productivity (inefficiency)
Increased workplace injuries (hands, neck, eyes, headaches)
Non-designed Film Reading Room
Typically, the reading room is not designed
Often specified as an office work space, with inappropriate lighting, materials and finishes
Reading activities appear to be misunderstood
Transition from Film to Soft Copy
Reading activities become more intense
3D & 4D images; reading is more interactive
Room design becomes more critical
Reading Room Prototype

The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 13
1200
Reading Room Prototype – “COTS”(Commercially off-the-shelf)
Questions??
Convergence of Imaging Convergence of Imaging and Surgeryand Surgery44
Does Form Follow Function?
Surgical and interventional radiology procedures have changed dramatically in recent decades and in many ways are
iconverging
Why do the designs of “surgical” suites and “interventional” suites remain so different?
© 2008 Anshen+Allen
Minimal surgical incisions
Redefinition of “Sterile Field”
Increased reliance on
Surgery Has Become Less Invasive
image guidance
Many surgical procedures similar to interventional radiology and interventional cardiology
Historic IR room utilization: 60-70% = diagnostic procedures
Many diagnostic IR procedures now replaced by less-
IR Has Become More Interventional
p yinvasive modalities (CTA, MRA, SPECT, PET, Hybrids, etc.)
Future IR room utilization will focus on more interventional procedures

The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 14
Surgical-quality Heating, Ventilation and Air Conditioning (HVAC) requirements
“Surgical-like” restricted workflow requirements
IR Requires a Surgical-like Environment
Increased Prep / Recovery needs
© 2008 Anshen+Allen
Operating Rooms often have sub-optimal lighting conditions
Surgeons may need to view & interact w/ medical images
Design Implications
Surgery Relies on Image Guidance
from a distance
As image guidance become more complex new personnel (radiology techs, IT specialists, etc.) will need to participate in procedures without entering the OR
Design Implications
PACS and Image Guidance in the OR
Green theatrical gels placed over ambient lighting tubes
Information Technology in the OR
Design Implications
MRI in the OR
Design Implications
MAGNET TYPES
StationaryPivoting TravelingPortable
ROOM TYPES
Single RoomDual Room Many Rooms
Design for MRI safety (ACR safety guidelines)
Locate MRI for either “scrubbed” or “ t t l th ”
MRI in the OR
Design Implications
“street clothes” access
Protect against RF and/or magnetic interactions with adjacent occupants
Increase structural, air and cooling capacities
© 2008 Anshen+Allen

The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 15
ORs With Control Rooms
© 2008 Anshen+Allen
ORs With Control Rooms
© 2008 Anshen+Allen
Supplies
Scrubbed TeamSupport Team Patient
ORs With Control Rooms
Control Room
Sub-sterile
© 2008 Anshen+Allen
Definition: The consolidation of various interventional services within a common area and operated as an integrated program.
The Integrated Interventional Suite
Endoscopy IR / Cath Surgery
Level 2Recovery
PACU
Intake/Prep
Shared prep/recovery
© 2006 Anshen+Allen
Kingdom of
Surgery
Kingdom of
Imaging
Kingdom of
Cardiology
Challenges:
The Integrated Interventional Suite
Collective vision to minimize turf battles
Differing protocol for infection control in Surgery, Interventional Radiology and Interventional Cardiology
Lower middle image, courtesy of: Center for Integration of Medicine and Innovative Technology / Massachusetts General Hospital - Operating Room of the Future (ORF) Reuben Mezrich, MD, PhD; Nat Sims, MD
Interventional Cardiology
Contiguous space for multiple services
Cross-training for some support staff
Cost of excess infrastructure capacity for future areas of change
ORsORsIR / CCL / IR / CCL / EP / ShellEP / Shell
Level 2 – IR: 2; EP: 1 Cath Labs: 2; Shell: 1 ORs: 12; Endo: 3; Prep / PACU beds: 53 (2.5:1)
The Integrated Interventional Suite
EP / ShellEP / Shell
Endo
Endo PrePre-- Op / Op /
PostPost--OpOp
© 2008 Anshen+Allen Associated Architects for Palomar Pomerado Health

The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 16
Approach: Flexible Planning ModulesThe Integrated Interventional Suite
© 2008 Anshen+Allen Associated Architects for Palomar Pomerado Health
Room Size:
Room Configuration:
Universal vs. Dedicated:
<600 NSF; 600-750 NSF; > 750 NSF
Square; rectangular; “handed” vs. mirrored
A question of flexibility
Design Considerations:Universal Procedure Rooms
Table Orientation:
Orientation of patient’s head:
Room “zoning” and workflow:
Parallel; perpendicular; diagonal to corridor
Head to corridor; feet to corridor; head to side
Sterile; circulation; anesthesia; documentation zones
© 2008 Anshen+Allen
Approach: Flexible Planning Modules
The Integrated Interventional Suite
© 2008 Anshen+Allen Associated Architects for Palomar Pomerado Health
Approach: Surgery - Clean Core / IR - Staff Core
The Integrated Interventional Suite
© 2008 Anshen+Allen Associated Architects for Palomar Pomerado Health
Approach: Collaborative Cath/IR Staff Core
The Integrated Interventional Suite
© 2008 Anshen+Allen
© 2008 Anshen+Allen
Approach: “Virtual” Red Line
The Integrated Interventional Suite
OR OR OR
OR OR OR
EP
CATH
IR
IR
OR OR OR
OR OR OR
© 2008 Anshen+Allen Associated Architects for Palomar Pomerado Health
OR OR ORCATH IR
OR OR OR

The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 17
Approach: Flexible Pre-op / PACU
The Integrated Interventional Suite
© 2008 Anshen+Allen Associated Architects for Palomar Pomerado Health
Approach: Flexible Pre-op / PACUThe Integrated Interventional Suite
© 2008 Anshen+Allen Associated Architects for Palomar Pomerado Health
Design and ExperienceDesign and Experience55
Intra-operative and Diagnostic MRI Suite
IntraIntra--operative operative MRIMRI (1)(1)
Diagnostic Diagnostic MRIMRI (7)(7)
© 2008 Anshen+Allen
Intra-operative MRI
© 2008 Anshen+Allen
Diagnostic MRI
© 2008 Anshen+Allen
The Architecture of Medical ImagingDesigning Healthcare Facilities for
Advanced Radiological Diagnostic and Therapeutic TechniquesUniversity of Kansas – Architecture 731 – Systems and Components of Healthcare Facilities
Bill Rostenberg, FAIA, FACHA, NCARB Principal and Director of Research - Anshen + Allen901 Market Street San Francisco, CA, USA 94103
[email protected] 415 / 281-5459Page: 18
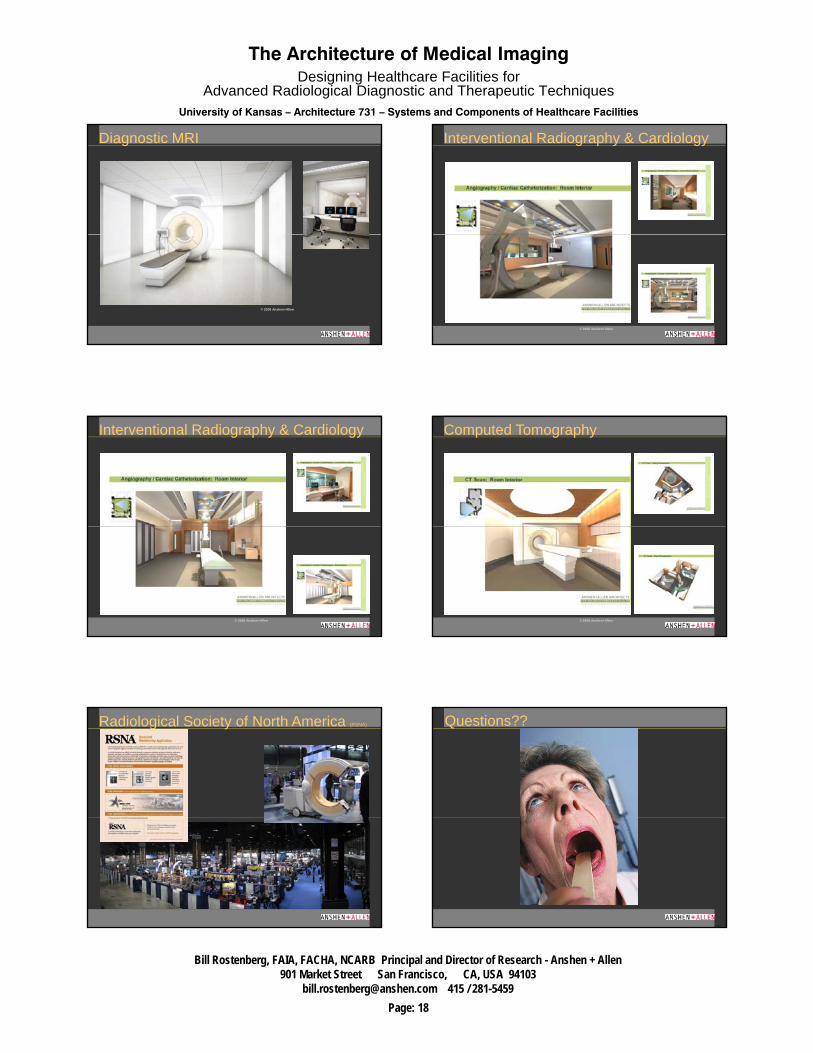
Diagnostic MRI
© 2008 Anshen+Allen
Interventional Radiography & Cardiology
© 2008 Anshen+Allen
Interventional Radiography & Cardiology
© 2008 Anshen+Allen
Computed Tomography
© 2008 Anshen+Allen
Radiological Society of North America (RSNA) Questions??