the beloved neutrophil: its function in health and...
TRANSCRIPT

The Beloved Neutrophil: Its Function in Health and
Disease

Stem Cell Multipotent Progenitor
Myeloid Lymphoid
CMP IL-3, SCF, GM-CSF CLP MEP GMP
EPO TPO RBC Platelet Neutrophil Monocyte/ Basophil B-cells Macrophage Eosinophil T-Cells Mast cell NK cells
G-CSF M-CSF
GM-CSF, IL-3, SCF
IL-3 IL-5
Committed Progenitor
Mature Cell
SCF
Dendritic cells

PRODUCTION AND KINETICS OF NEUTROPHILS
CELLS % CELLS TIME
Bone Marrow: Mitotic Maturation/ Storage
Myeloblast Promyelocyte Myelocyte Metamyelocyte Band Seg
1 4
16
22 30 21
7 - 9 Days
3 – 7 Days
Vascular: Peripheral Blood Marginating Pool
Seg
2
3
6 – 12 hours
Tissue
Apoptosis and clearance by macrophages
? 0 – 3 days

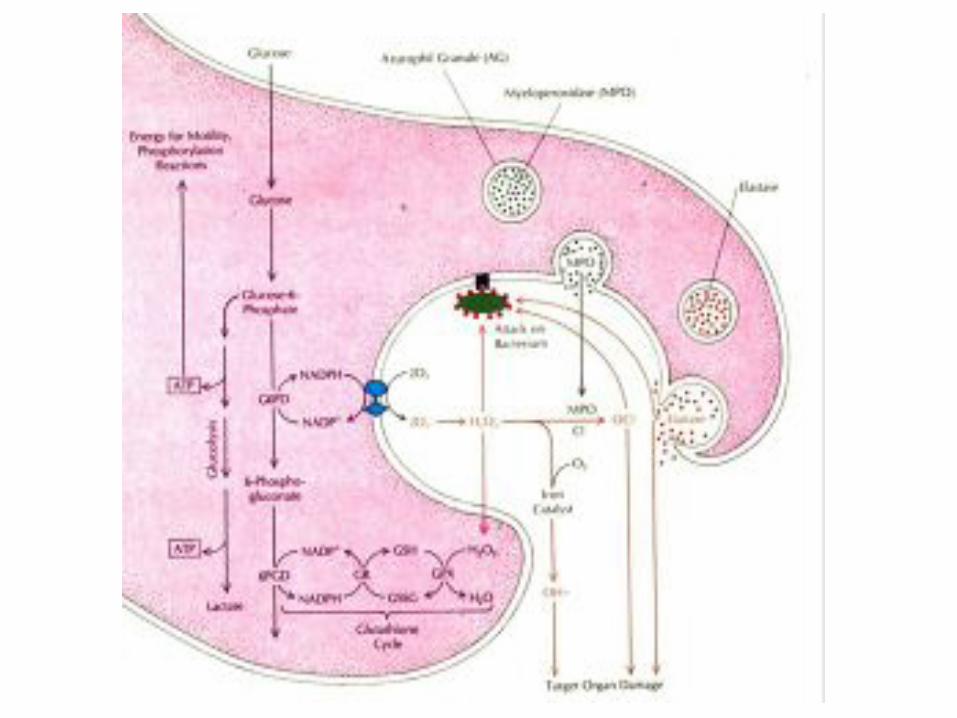
PHAGOCYTOSIS
1. Mobilization 2. Chemotaxis 3. Recognition (Opsonization) 4. Ingestion 5. Degranulation 6. Peroxidation 7. Killing and Digestion 8. Net formation


Adhesion: β 2 Integrins ▪ Heterodimer of D and E chain ▪ Tight adhesion, migration, ingestion, co- stimulation of other PMN responses
LFA-1 Mac-1 (CR3) p150,95 D2E2
D E
CD11a CD18
CD11b CD18
CD11c CD18
CD11d CD18
Cells All leukocytes
PMN, mono/mac, LGL
Dendritic
Mac, mono, PMN, T cell
Ligands ICAMs ICAM-1 C3bi Fibrinogen other
C3bi, other
ICAM-3, other


GRANULOCYTE CHEMOATTRACTANTS
Chemoattractants Source Activators Lipids PAF Neutrophils C5a, LPS, FMLP Endothelium LTB4 Neutrophils FMLP, C5a, LPS Chemokines (D) IL-8 Monocytes, endothelium LPS, IL-1, TNF, IL-3 other cells Gro D, E, J Monocytes, endothelium IL-1, TNF other cells NAP-2 Activated platelets Platelet activation Others FMLP Bacteria C5a Activation of complement

Other Important Receptors on PMNs
x Pattern recognition receptors – Detect microbes � Toll receptor family � Mannose receptor � EGlucan receptor – fungal cell walls x Cytokine receptors – enhance PMN function � G-CSF, GM-CSF � TNF Receptor x Opsonin receptors – trigger phagocytosis � FcJRI, II, III � Complement receptors – x Mac1/CR3 (CD11b/CD18) – C3bi x CR-1 – C3b, C4b, C3bi, C1q, Mannose binding protein


From JG Hirsch, J Exp Med 116:827, 1962, with permission.

CONTENTS OF NEUTROPHIL GRANULES
I. Azurophil granules Functions Acid Hydrolases (glycosidases) Degradation of ingested material Neutral proteases (cathespin G, Destruction of inflamed tissue elastase) Lysozyme Digestion of bacterial cell wall Defensins and bactericidal/proteins Oxygen-independent bacterial killing Myeloperoxidase Oxygen-dependent bacterial killing

CONTENTS OF NEUTROPHIL GRANULES
II. Specific granules Functions Lysozyme Digestion of bacterial cell wall Cobalamin-binding proteins Binding of cobalamin analogues Apolactoferrin Binding of free iron Collagenase Digestion of connective tissue C5a-splitting enzyme Release of C5a Heparinase Digestion of connective tissue Laminin and thrombospondin Adhesion to basement receptors membrane CD11/18 (C3bi) receptor Adhesion to ICAM-1, 2, 3
on endothelium and phagocytosis of C3bi coated particles
Cytochrome B558 Component of NADPH


Infectious complications of phagocyte disorders
(either quantitative or functional)
x Frequent and/or unusually severe bacterial, fungal infections
- Skin, lymph nodes, lungs (portals of entry); other sites via bloodstream or tissue extension
x Unusual site - e.g. liver or brain abscess
x Recurrent/chronic gingivitis, aphthous ulcers
x Staphylococcal common. Also Strep; Gram-negatives, unusual or opportunistic pathogens e.g. Aspergillus, Serratia, B. cepacia, Klebsiella, atypical Mtb

Inherited Defects in Neutrophil Functions
Adhesion: Leukocyte Adhesion Deficiencies (LAD) I, II, III
Chemotaxis: LADI HyperIgE Syndrome Chediak-Higashi Actin defects
Phagocytosis: LADI Chediak-Higashi
Killing: Chronic granulomatous disease Specific granule deficiency Chediak-Higashi MPO deficiency (with DM)


LEUKOCYTE ADHESION DEFICIENCY In Vitro Leukocyte Functional Abnormalities
Clinical Features
x Pediatric age group x Delayed umbilical cord separation x Persistent leukocytosis x Defective neutrophil mobilization
(reduced pus formation) x Impaired wound healing x Recurrent (life-threatening) bacterial
and sometimes viral infections x PMN/Mo adherence and spreading x PMN aggregation

Lekstrom-Himes JA, Gallin JI. Immunodeficiency diseases caused by defects in phagocytes. N Eng J Med 343:1703,2000.

Leukocyte Adhesion Deficiency I (LAD I)
Prevalence Rare Age Usually presents in infancy Genetics AR mutation in CD18 subunit of E2 integrin, leading to complete or partial loss of E2 integrin expression Pathogenesis Defects in adhesion, migration, phagocytosis Clinical Omphalitis, periodontitis, skin/soft tissue infections, pneumonia, sepsis, poor wound healing, delayed cord separation. Staph, gram negatives Labs Neutrophilia, absent CD11/CD18 (including Mac-1) Management HSCT, otherwise supportive care

SUMMARY OF CGD Incidence: 4 per million births Infections: x Pneumonia (70%) Aspergillus x Supportive Adenitis (53%)
Staphylococcus x Subcutaneous Abscess (42%)
Staphylococcus x Liver Abscesses (27%) Staphylococcus x Osteomyelitis (25%) Serratia x Sepsis (18%) Salmonella

INFECTIONS IN CGD Pathogen Presentations
Bacterial � Staphylococcus aureus
Soft tissue infection, Lymphadenitis, Liver Abscess, Osteomyelitis, Pneumonia, Sepsis
� Burkholderia Pneumonia, Sepsis
� Serratia marcescans Pneumonia, Osteomyelitis, Sepsis, Soft tissue infection
� Nocardia species Pneumonia, Osteomyelitis, Brain abscess
Fungal � Aspergillus species � Candida species
Pneumonia, Osteomyelitis, Brain abscess Sepsis, Soft tissue infection, Liver abscess

Lung resection for persistent Aspergillus
Pathology: Chronic inflammatory infiltrate, foci of neutrophils
Silver stain: Aspergillus hyphae
Examples of Infectious Complications of CGD
Impetigo
Lymphadenitis Aspergillus
pneumonia
Lekstrom-Himes and Gallin, NEJM 343, 1703, 2000. � 2000 Massachusetts Medical Society. All rights reserved.


SUMMARY OF CGD
x Other complications: Gastric Outlet Obstruction (15%)
Urinary Tract Obstruction (10%) Colitis (17%) x Cause of Death: Pneumonia/Sepsis, Aspergillus B cepacia


NET C
Yost, C., Cody, M., Harris, E., Thornton, N., McInturff, A., Martinez, M., Chandler, N., Rodesch, C., Albertine, K., Petti, C., Weyrich, A., & Zimmerman, G. (2009). Impaired neutrophil extracellular trap (NET) formation: a novel innate immune deficiency of human neonates. Blood. 113 (25), 6419-6427.

Chronic Granulomatous Disease (CGD)
Pathogenesis Impaired microbial killing due to deficient production of oxidants Clinical a) Lymphadenitis, skin infections, pneumonia, hepatic abscess, pneumonia b) Aspergillus, B. cepacia most problematic; Staph most common. Gram-negative (eg. Serratia). Pathogens often opportunistic or unusual. However, can kill catalase-negative organisms (eg. Strep) using microbial H2O2. c) Granulomatous inflammation, including GI tract Labs Absent or markedly reduced NADPH oxidase activity Management Prophylactic trimethoprim/sulfa, itraconazole, IFNJ; Aggressive/prolonged treatment of infections; Prednisone/ immunisuppr for inflammation

Neutropenia
• Definition: Reduction in the absolute neutrophil count (includes bands and segmented PMNs) below norms for age and ethnic groups in the blood circulation.
• Age-related ANC: Term newborn (1 week): < 1500 Infant (1 month – 4 years): < 1000 Child, adolescent, adult: < 1500
• Ethnicity: < 800

Clinical Risk Assessment
• None: ANC of 1,000 to 1,500/µL
• Moderate: ANC of 500 to 999/µL
• Severe: ANC of 300 to 499/µL
• Very severe: ANC of < 300/µL

Clinical Risk Assessment
• Acute vs. chronic lasting more than three months (ANC < 500/µL).
• Can neutrophils be mobilized from bone marrow?
• Production vs. destruction.
Epidemiology
• Acute neutropenia occurs frequently.
• Congenital neutropenia: ~ 2 per million.
• Cyclic neutropenia: ~ 0.6 per million.

Suspicion of Neutropenia
• Acute severe bacterial infections.
• History of recurrent infections.
• Prolonged or elevated temperature (> 101° F).
• Pneumonia, peritonitis, GU tract infection, buccal and tongue ulcers, chronic gingivitis, cellulitis, perirectal infections.
• Findings associated with a malignancy, immunodeficiency syndrome, viral infection or drug exposure.

Laboratory Evaluation of Neutropenia
• CBCPD and blood smear. • If neutropenia is recurrent, repeat CBCPD 3x/week for 6
weeks. • Coombs test. • Immunoglobulin levels and lymphocyte subsets. • Antineutrophil antibodies. • Serology for viral infections if acute process. • ANA, LDH, uric acid. • Bone marrow exam and cytogenetics.

Antigens
Previous
Names Carrier Glycoproteins
Allele Frequency
(%) Asians*
Allele Frequency
(%) Africans+
Allele Frequency
(%) Whites
Clinical Significance
HNA-1a NA1 FcȣR IIIb (CD16) 88-91 46-66 57-62 AIN, ANN, TRALI
HNA-1b NA2 FcȣR IIIb (CD16) 51-54 78-84 88-89 AIN, ANN, TRALI
HNA-1c SH FcȣR IIIb (CD16) < 1 23-31 5 AIN, ANN, TRALI
HNA-2 NB1 58-64 kDa (CD177) 89-99 98 87-97 AIN, ANN, TRALI, febrile
transfusion reaction,
drug-induced
neutropenia
HNA-3 5b CTL2 (Unknown) nt nt 89-96 ANN, TRALI, febrile
transfusion reaction
HNA-4 HART CR3 (CD11b) nt nt 99 AIN, ANN
HNA-5 OND LFA-1 (CD11a) 81 88 86-92 unknown
Human Neutrophil Alloantigens

Severe Chronic Neutropenia
• Heterogeneous group of disorders of myelopoiesis
• Associated with - decreased production of neutrophils - recurrent bacterial infections
• Severity of disease related to degree of neutropenia

Severe Congenital Neutropenia (SCN)
• Early childhood onset with ANC < 200
• Bone marrow shows maturation arrest at promyelocyte-myelocyte stage
• Recurrent life-threatening bacterial infections
• Associated with ELANE (ELA2) mutations

Clinical Issues in SCN
• 10% – 30% risk of evolving into MDS/AML
• HCT should be considered in G-CSF non responders to • > 20µg/kg/day or converting to MDS/AML
• Need for annual bone marrow to survey for cytogenetic changes
• Patients remain at risk for infection because of impaired
neutrophil function

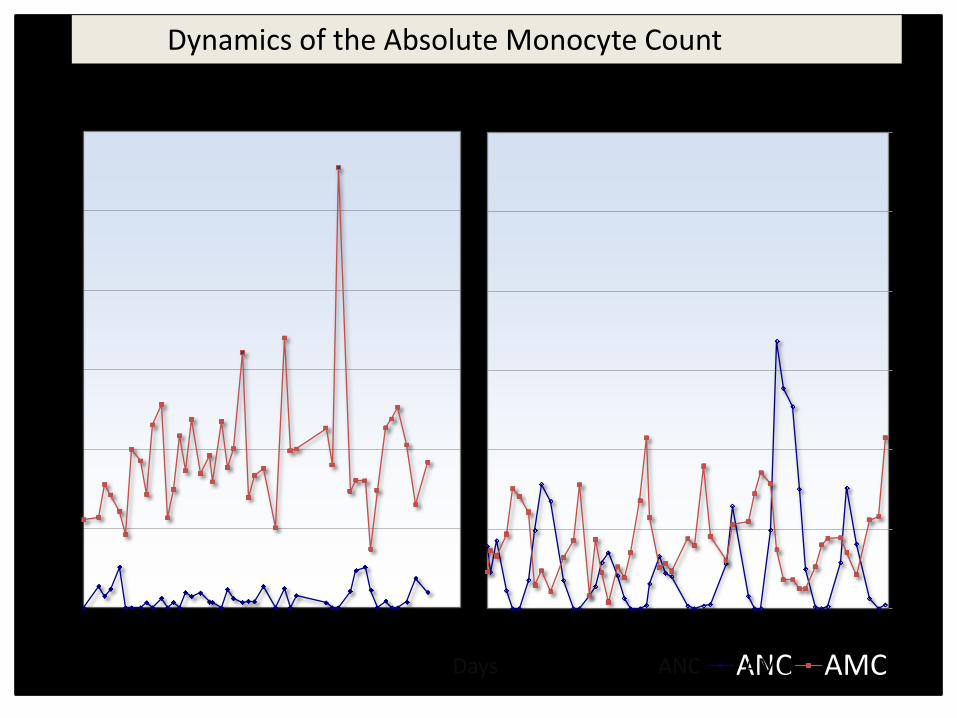
Cyclic Neutropenia
• Dominantly inherited
• Cycle of neutropenia q 21 days
• Marrow during neutropenia: myelocyte arrest
• Stem cell regulatory defect

Cyclic Neutropenia
• Like autosomal dominant SCN, cyclic neutropenia has been linked to mutations in neutrophil
elastase
• ELANE (ELA2) mutations found in essentially 90% of cyclic neutropenia
• NOT associated with an increased risk of AML
0
1000
2000
3000
4000
5000
6000
0 21 42 63 84 105 126
Congenital Neutropenia
0
1000
2000
3000
4000
5000
6000
0 21 42 63 84 105 126
ANC AMC
Cyclic Neutropenia
AMC
Peri
ph
eral
Leu
kocy
te C
ou
nt
(co
un
ts/µ
l)
Dynamics of the Absolute Monocyte Count
Days ANC

Table 3: Classification of Congenital Neutropenia Disorders
Main hematologic Other clinical Gene Disease (inheritance) features features (chromosomal location)
Disorders of Myelopoiesis -Cyclic neutropenia (AD) Periodic neutropenia None ELANE (19q13.3) -Severe congenital neutropenia (AD) Neutropenia, MDS/AML None ELANE (19q13.3) -Severe congenital neutropenia (AD) Neutropenia, MDS/AML None Gfi1 (1p22) -Severe congenital neutropenia (AD) Neutropenia None G-CSFR (1p35 34.3) -Severe congenital neutropenia (AR) Neutropenia, MDS/AML Neurologic HAX1 (1q21.3) or Kostmann disease impairment Disorders of ribosomal and telomere dysfunction -Shwachman-Diamond (AR) Neutropenia Exocrine SBDS (7q11.22) Aplastic anemia pancreas deficiency MDS/AML Metaphyseal dysostosis -Dyskeratosis congenita (XLR) Pancytopenia Abnormal skin pigmentation, DKC1(Xq28) -Dyskeratosis congenita (AD) MDS/AML nail dystrophy, TERC (3q26)* -Dyskeratosis congenital (AR) oral leukoplakia, TERT (5p33)* epiphora, pulmonary fibrosis, TINF2 (14q11.2) short stature, hair loss, NOP10 (15q14-q15) developmental delay, NHP2 (5q35.3) squamous cell carcinoma of TCAB1(17q13.1) head and neck
Disorders of Metabolism -Reticular dysgenesis (AR) Neutropenia Sensorineural hearing loss AK2 (1p31-p34) Lymphopenia -Barth syndrome (XLR) Neutropenia Cardiomyopathy TAZ1 (Xq28) -Glycogen storage disease type 1b (AR) Neutropenia Hypoglycemia, G6PT1 (11q23) hyperlipidemia, hyperuricemia, growth retardation, osteopenia, renal hypertrophy -Glucose-6-phosphatase Neutropenia Cardiac abnormality, G6PC3 (17q21) catalytic subunit 3 (AR) Thrombocytopenia prominent superficial venous pattern, hepatosplenomegaly, cryptorchidism, microcephaly -Pearson syndrome (mitochondrial) Neutropenia Vacuolization of erythroid Mitochondrial DNA Pancytopenia and myeloid precursors deletion Ringed sideroblasts

Table 3: Classification of Congenital Neutropenia Disorders Cont.
Main hematologic Other clinical Gene Disease (inheritance) features features (chromosomal location)
Disorders of vesicular transport -Chediak-Higashi syndrome (AR) Neutropenia Pigmentary dilution affecting LYST/CHS (1q42.1- Platelet and NK cell hair, skin and ocular fundus, q42.2) dysfunction risk for hemophagocytic syndrome -Cohen syndrome (AR) Neutropenia Developmental delay, facial COH1 (8q22-q23) dysmorphism, retinitis pigmentosa
-Griselli syndrome type II (AR) Pancytopenia Pigmentary dilution of the skin RAB 27A (15q14.1) and hair -Hermansky-Pudlak type II (AR) Neutropenia Oculocutaneous albinism AP3B1 (5q14.1)
-p14 deficiency (AR) Neutropenia, Short stature, MAPBPIP (1q21) Decreased B&T hypopigmentation lymphocytes, hypogammaglobulinemia
Disorders of Immune Function -Cartilage-hair hypoplasia (AR) Neutropenia Short-limbed dwarfism, RMRP (9p21-p12) Lymphopenia fine hair, immodeficiency, Macrocytic anemia increased risk of malignancy -Hyper-IgM syndrome (XLR) Neutropenia Defective humoral immunity CD4OLG (Xq26) -Schminke immuno-osseous dysplasia (AR) Neutropenia Spondyloeiphyseal dysplasia, SMARCAL1 (2q34-36) Pancytopenia nephrotic syndrome, Lymphopenia defective cellular immunity -WHIM syndrome (AD) Neutropenia Warts, hypogammaglobulinemia CXCR4 (2q21) Lymphopenia Infections, myelokathexis Neutrophil hyperplasia in the bone marrow, neutrophil nuclear hypersegmentation with thin filaments connecting pyknotic-appearing lobes -Wiskott-Aldrich syndrome (XLR) Neutropenia Increased risk for acute WAS (Xp11.22-Xp11.3) Lymphopenia myeloid leukemia, Monocytopenia diminished cellular immune function
*AD= autosomal dominant, AD dyskeratosis dyskeratosis congenita disorders are identified in italics; AR= autosomal recessive