the cervical aortic knuckle which resembles an aneurysm
TRANSCRIPT
825
THE CERVICAL AORTIC KNUCKLE WHICHRESEMBLES AN ANEURYSM
CECIL LEWISB.Sc., M.Ch. Wales, F.R.C.S.
ASSISTANT IN THE SURGICAL UNIT, ROYAL INFIRMARY, CARDIFF
LAMBERT ROGERS
V.R.D., M.D., M.Sc., F.R.C.S., F.R.A.C.S., F.A.C.S.
PROFESSOR OF SURGERY, UNIVERSITY OF WALES
AN aortic arch may be present in the supraclavicularregion and clinically resemble an aneurysm of the sub-clavian, carotid, or innominate arteries. In mistake forsuch it may be ligated with fatal results, as has probablybeen done on several occasions (Beavan and Fatti 1947).This accident nearly happened in the following case,but fortunately our suspicions were aroused and laterstrengthened by the late C. M. West, then professor ofanatomy at the Welsh National School of Medicine,whom we invited to see the patient and who was present
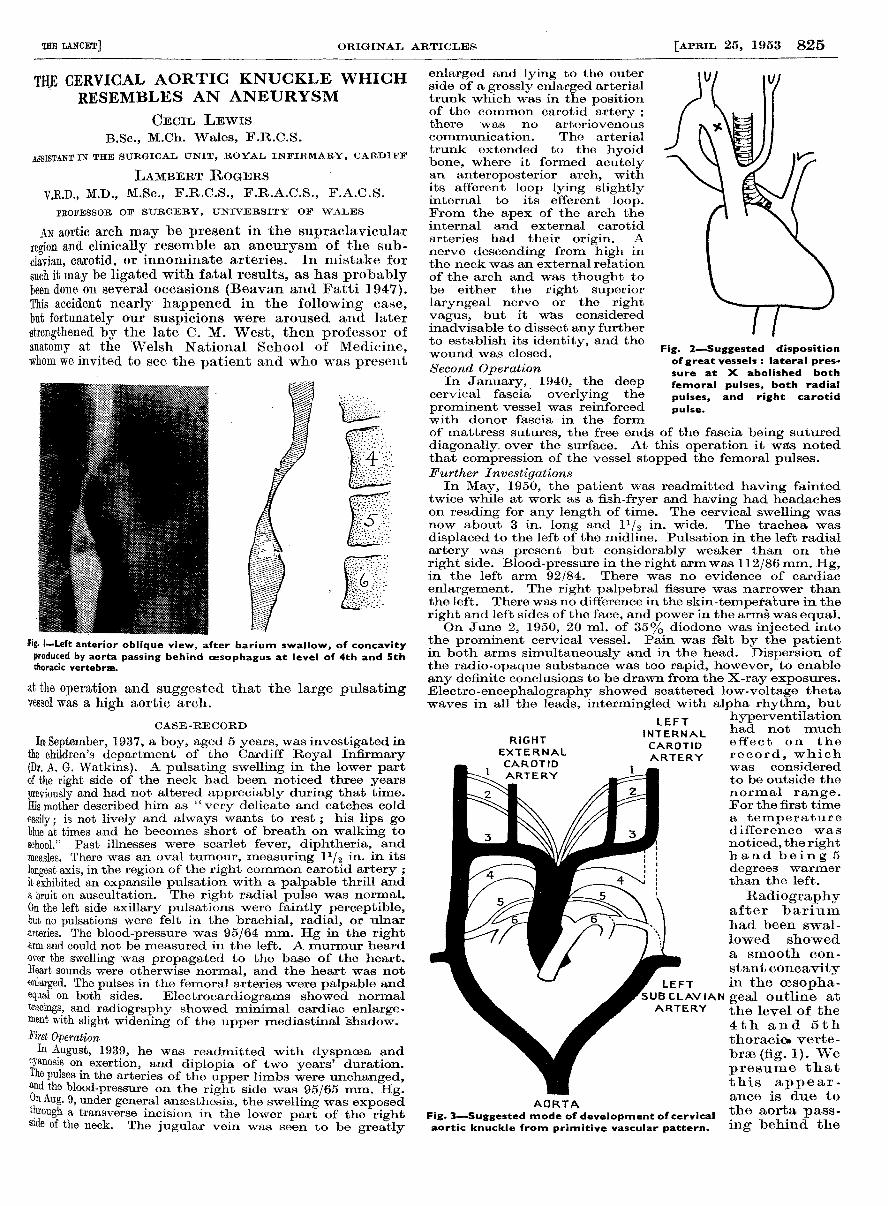
his I-Left anterior oblique view, after barium swallow, of concavityproduced by aorta passing behind oesophagus at level of 4th and 5ththoracic vertebrse.
at the operation and suggested that the large pulsatingvessel was a high aortic arch.
CASE-RECORD
In September, 1937, a boy, aged 5 years, was investigated inthe children’s department of the Cardiff Royal Infirmary(Dr. A. G. Watkins). A pulsating swelling in the lower partof the right side of the neck had been noticed three yearspreviously and had not altered appreciably during that time.His mother described him as " very delicate and catches coldeasily; is not lively and always wants to rest ; his lips goblue at times and he becomes short of breath on walking toschool." Past illnesses were scarlet fever, diphtheria, andmeasles. There was an oval tumour, measuring 11/2 in. in itslongest axis, in the region of the right common carotid artery ;it exhibited an expansile pulsation with a palpable thrill anda bruit on auscultation. The right radial pulse was normal.On the left side axillary pulsations were faintly perceptible,but no pulsations were felt in the brachial, radial, or ulnararteries. The blood-pressure was 95/64 mm. Hg in the rightarm and could not be measured in the left. A murmur heardover the swelling was propagated to the base of the heart.Heart sounds were otherwise normal, and the heart was notenlarged. The pulses in the femoral arteries were palpable andequal on both sides. Electrocardiograms showed normaltracings, and radiography showed minimal cardiac enlarge-ment with slight widening of the upper mediastinal shadow.l’irst OperationIn August, 1939, he was readmitted with dyspnoea and
cyanosis on exertion, and diplopia of two years’ duration.The pulses in the arteries of the upper limbs were unchanged,and the blood-pressure on the right side was 95/65 mm. Hg.On Aug. 9, under general anaesthesia, the swelling was exposedthrough a transverse incision in the lower part of the rightside of the neck. The jugular vein was seen to be greatly
enlarged and lying to the outerside of a grossly enlarged arterialtrunk which was in the positionof the common carotid artery ;there was no arteriovenouscommunication. The arterialtrunk extended to the hyoidbone, where it formed acutelyan anteroposterior arch, withits afferent loop lying slightlyinternal to its efferent loop.From the apex of the arch theinternal and external carotidarteries had their origin. Anerve descending from high inthe neck was an external relationof the arch and was thought tobe either the right superiorlaryngeal nerve or the rightvagus, but it was consideredinadvisable to dissect any furtherto establish its identity, and thewound was closed.Second Operation
In January, 1940, the deepcervical fascia overlying the
prominent vessel was reinforcedwith donor fascia in the formof mattress sutures, the free ends of the fascia being sutureddiagonally over the surface. At this operation it was notedthat compression of the vessel stopped the femoral pulses.Further InvestigationsIn May, 1950, the patient was readmitted having fainted
twice while at work as a fish-fryer and having had headacheson reading for any length of time. The cervical swelling wasnow about 3 in. long and 11/2 in. wide. The trachea was
displaced to the left of the midline. Pulsation in the left radialartery was present but considerably weaker than on theright side. Blood-pressure in the right arm was 112/86 mm. Hg,in the left arm 92/84. There was no evidence of cardiac
enlargement. The right palpebral fissure was narrower thanthe left. There was no difference in the skin-temperature in theright and left sides of the face, and power in the arms was equal.On June 2, 1950, 20 ml. of 35% diodone was injected into
the prominent cervical vessel. Pain was felt by the patientin both arms simultaneously and in the head. Dispersion ofthe radio-opaque substance was too rapid, however, to enableany definite conclusions to be drawn from the X-ray exposures.Electro-encephalography showed scattered low-voltage thetawaves in all the leads. intermingled with alpha rhvthm. but
Fig. 2-Suggested dispositionof great vessels : lateral pres-sure at X abolished both
femoral pulses, both radial
pulses, and right carotid
pulse.
hyperventilationhad not mucheffect on the
record, whichwas consideredto be outside thenormal range.For the first timea temperaturedifference wasnoticed, the righthand being 5degrees warmerthan the left.
Radiographyafter bariumhad been swal-lowed showeda smooth con-stant concavityin the cesopha-
v geal outline atthe level of the4th and 5ththoracic. verte-
brae (fig. 1). Wepresume thatthis appear-ance is due tothe aorta pass-ing behind the
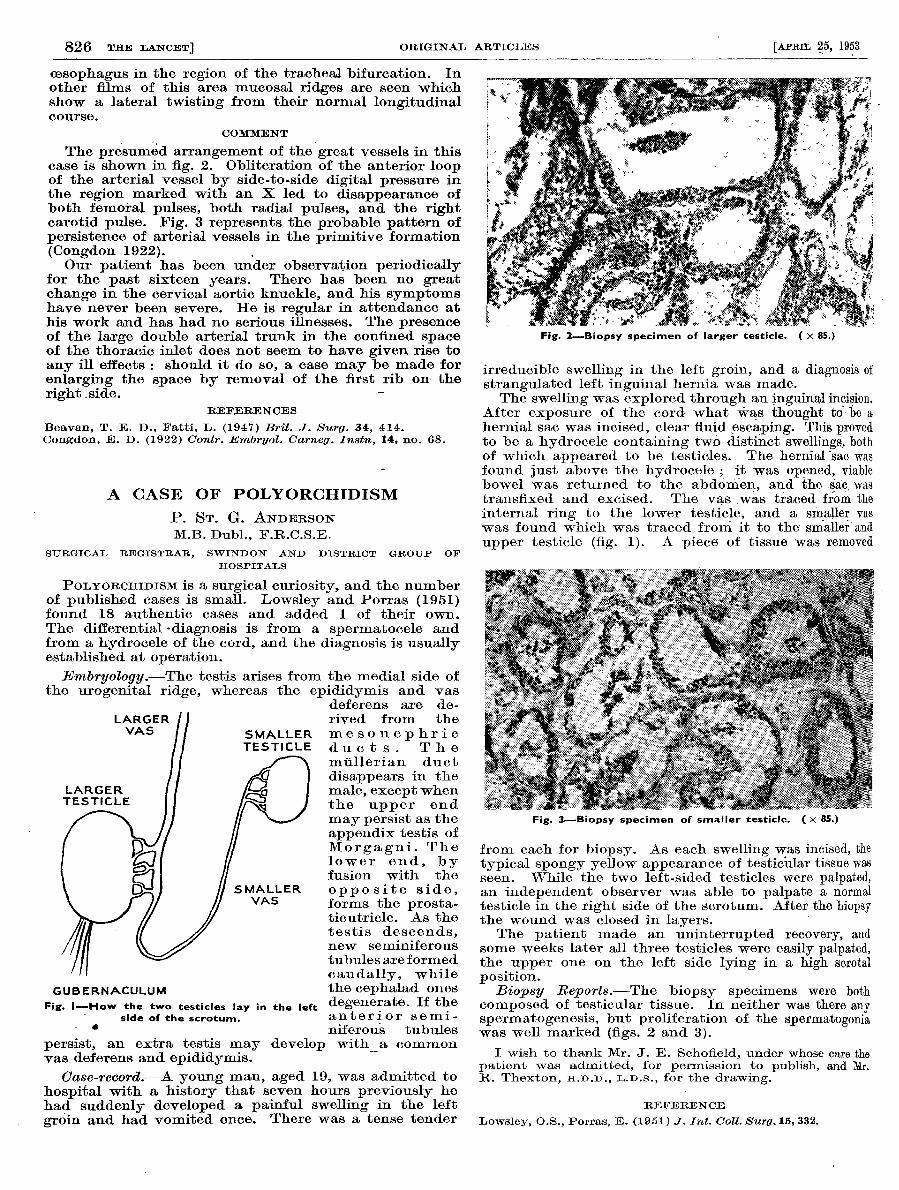
Fig. 3-Suggested mode of development ofcervicalaortic knuckle from primitive vascular pattern.
826
oesophagus in the region of the tracheal bifurcation. Inother films of this area mucosal ridges are seen whichshow a lateral twisting from their normal longitudinalcourse.
COMMENT
The presumed arrangement of the great vessels in thiscase is shown in fig. 2. Obliteration of the anterior loopof the arterial vessel by side-to-side digital pressure inthe region marked with an X led to disappearance ofboth femoral pulses, both radial pulses, and the rightcarotid pulse. Fig. 3 represents the probable pattern ofpersistence of arterial vessels in the primitive formation(Congdon 1922).Our patient has been under observation periodically
for the past sixteen years. There has been no greatchange in the cervical aortic knuckle, and his symptomshave never been severe. He is regular in attendance athis work and has had no serious illnesses. The presenceof the large double arterial trunk in the confined spaceof the thoracic inlet does not seem to have given rise toany ill effects : should it do so, a case may be made for
enlarging the space by removal of the first rib on- theright side. -
REFERENCES
Beavan, T. E. D., Fatti, L. (1947) Brit. J. Surg. 34, 414.Congdon, E. D. (1922) Contr. Embryol. Carneg. Instn, 14, no. 68.
A CASE OF POLYORCHIDISM
P. ST. G. ANDERSONM.B. Dubl., F.R.C.S.E.
SURGICAL REGISTRAR, SWINDON AND DISTRICT GROUP OF
HOSPITALS
POLYORQHIDISM is a surgical curiosity, and the numberof published cases is small. Lowsley and Porras (1951)found 18 authentic cases and added 1 of their own.The differential -diagnosis is from a spermatocele andfrom a hydrocele of the cord, and the diagnosis is usuallyestablished at operation.Embryology.-The testis arises from the medial side of
the urogenital ridge, whereas the epididymis and vasdeferens are de-rived from the
mesonephricducts. Themullerian duct
disappears in themale, except whenthe upper end
may persist as theappendix testis ofMorgagni. Thelower end, byfusion with the
opposite side,forms the prosta-ticutricle. As thetestis descends,new seminiferoustubules are formedcaudally, whilethe cephalad onesdegenerate. If theanterior semi-niferous tubules
persist, an extra testis may develop with a commonvas deferens and epididymis.
-
Case-record.-A young man, aged 19, was admitted tohospital with a history that seven hours previously hehad suddenly developed a painful swelling in the left
groin and had vomited once. There was a tense tender
Fig. 1-How the two testicles lay in the leftside of the scrotum.
- a
Fig. 2-Biopsy specimen of larger testicle. ( x 85.)
irreducible swelling in the left groin, and a diagnosis ofstrangulated left inguinal hernia was made.The swelling was explored through an inguinal incision.
After exposure of the cord what was thought to be ahernial sac was incised, clear fluid escaping. This provedto be a hydrocele containing two distinct swellings, bothof which appeared to be testicles. The hernial -sac wasfound just above the hydrocele ; it was opened, viablebowel was returned to the abdomen, and the sac wastransfixed and excised. The vas was traced from theinternal ring to the lower testicle, and a smaller vaswas found which was traced from it to the smaller andupper testicle (fig. 1). A piece of tissue was removed
Fig. 3-Biopsy specimen of smaller testicle. ( X 85.)
from each for biopsy. As each swelling was incised, thetypical spongy yellow appearance of testicular tissue wasseen. While the two left-sided testicles were palpated,an independent observer was able to palpate a normaltesticle in the right side of the scrotum. After the biopsythe wound was closed in layers.The patient made an uninterrupted recovery, and
some weeks later all three testicles were easily palpated,the upper one on the left side lying in a high scrotalposition.
Biopsy Reports.-The biopsy specimens were bothcomposed of testicular tissue. In neither was there anyspermatogenesis, but proliferation of the spermatogoniawas well marked (figs. 2 and 3).
I wish to thank Mr. J. E. Schofield, under whose care thepatient was admitted, for permission to publish, and Mr.R. Thexton, H.D.D., L.D.S., for the drawing.
REFERENCE
Lowsley, O.S., Porras, E. (1951) J. Int. Coll. Surg. 15, 332.