the eeg in selected generalized seizures - idanda.com ref eeg in generalized.pdfthe eeg in selected...
TRANSCRIPT
REVIEW ARTICLES
The EEG in Selected Generalized Seizures
Richard A. Hrachovy*‡ and James D. Frost Jr.*†
Abstract: This article reviews the ictal and interictal EEG findingsassociated with a select group of generalized seizures. These includeabsence seizures, myoclonic seizures seen in juvenile myoclonicepilepsy, idiopathic generalized tonic clonic seizures, infantilespasms, and atypical absence, tonic, and atonic seizures associatedwith the Lennox Gastaut syndrome.
Key Words: Electroencephalography, Ictal, Interictal, Generalizedseizures, Epilepsy.
(J Clin Neurophysiol 2006;23: 312–332)
The purpose of this article is to briefly describe the inter-ictal and ictal EEG patterns associated with a select group
of generalized seizures. A detailed description of the clinicalmanifestations of the seizures is beyond the scope of thisdiscussion.
IDIOPATHIC GENERALIZED EPILEPSIESOf the various idiopathic generalized seizures, absence,
myoclonic and generalized tonic-clonic seizures will be dis-cussed.
ABSENCE SEIZURES
Interictal EEG FindingsThe background activity is usually normal, although
some degree of slowing of the background rhythms may beseen in up to one third of patients (Sato et al., 1983; Holmeset al., 1987). Paroxysms of rhythmic slow wave activity witha frequency of 2.5 to 3.5 Hz may occur in a generalizedfashion or may be restricted to the occipital derivations (Fig.1). This rhythmic slow activity is generally symmetric andusually blocks with eye opening. It may occur in isolatedruns or may be coupled with the bursts of generalizedspike and wave activity described below (Dalby, 1969;Holmes et al., 1987).
The interictal EEG in patients with absence seizurestypically demonstrates brief bursts of 3 Hz spike-and-wave
activity that are bilaterally synchronous and symmetric(Penry et al., 1975; Holmes et al., 1987). These bursts areusually frontocentral dominant; however, in some patients thebursts are restricted to, or maximally expressed in, the occip-ital regions. The discharges appear and disappear suddenly.The frequency of the spike-and-wave complexes frequentlyvaries slightly during the burst. The first few complexes ofthe burst may occur at a frequency of 3.5 to 4 Hz, whereas,the last few may slow to 2.5 Hz (Niedermeyer, 1972; Daly,1990; Fig. 2). Some of the bursts of spike-and-slow waveactivity may be followed by brief runs of rhythmic 2.5 to 3.5Hz activity in the frontal leads bilaterally (ringing effect). Assoon as the 3 Hz spike-and-wave bursts stop, the backgroundEEG activity immediately returns to the baseline state, withno postictal depression or slowing except for the ringingeffect just mentioned. Three Hz spike-and-wave activityusually becomes more frequent with hyperventilation (Sato etal., 1983) and may be induced by photic stimulation (Wolfand Goosses, 1986).
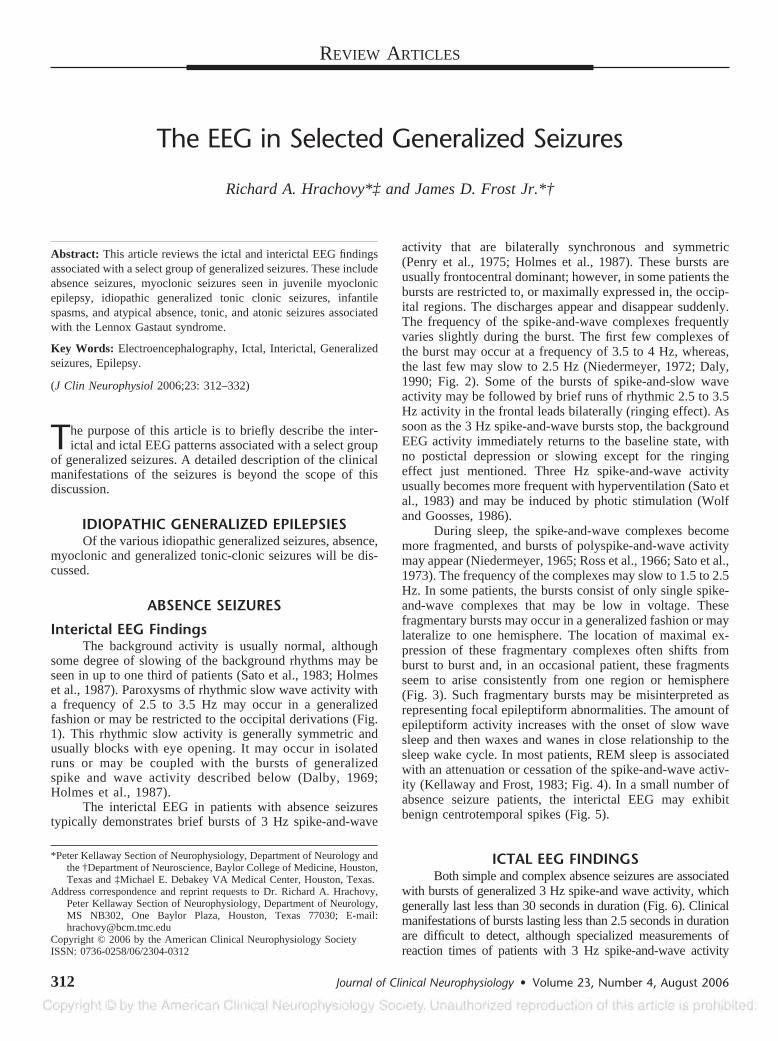
During sleep, the spike-and-wave complexes becomemore fragmented, and bursts of polyspike-and-wave activitymay appear (Niedermeyer, 1965; Ross et al., 1966; Sato et al.,1973). The frequency of the complexes may slow to 1.5 to 2.5Hz. In some patients, the bursts consist of only single spike-and-wave complexes that may be low in voltage. Thesefragmentary bursts may occur in a generalized fashion or maylateralize to one hemisphere. The location of maximal ex-pression of these fragmentary complexes often shifts fromburst to burst and, in an occasional patient, these fragmentsseem to arise consistently from one region or hemisphere(Fig. 3). Such fragmentary bursts may be misinterpreted asrepresenting focal epileptiform abnormalities. The amount ofepileptiform activity increases with the onset of slow wavesleep and then waxes and wanes in close relationship to thesleep wake cycle. In most patients, REM sleep is associatedwith an attenuation or cessation of the spike-and-wave activ-ity (Kellaway and Frost, 1983; Fig. 4). In a small number ofabsence seizure patients, the interictal EEG may exhibitbenign centrotemporal spikes (Fig. 5).
ICTAL EEG FINDINGSBoth simple and complex absence seizures are associated
with bursts of generalized 3 Hz spike-and wave activity, whichgenerally last less than 30 seconds in duration (Fig. 6). Clinicalmanifestations of bursts lasting less than 2.5 seconds in durationare difficult to detect, although specialized measurements ofreaction times of patients with 3 Hz spike-and-wave activity
*Peter Kellaway Section of Neurophysiology, Department of Neurology andthe †Department of Neuroscience, Baylor College of Medicine, Houston,Texas and ‡Michael E. Debakey VA Medical Center, Houston, Texas.
Address correspondence and reprint requests to Dr. Richard A. Hrachovy,Peter Kellaway Section of Neurophysiology, Department of Neurology,MS NB302, One Baylor Plaza, Houston, Texas 77030; E-mail:[email protected]
Copyright © 2006 by the American Clinical Neurophysiology SocietyISSN: 0736-0258/06/2304-0312
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006312

FIGURE 1. Occipital rhythmic in-termittent delta activity (ORIDA) ina 7-year-old patient with absenceseizures.
FIGURE 2. Modulation of the fre-quency of the spike and slow wavecomplexes during a burst of 3 Hzspike-and-wave activity. The firstfew complexes occur at frequency�3 Hz whereas the frequency ofthe later complexes slows to �3Hz.
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 313

FIGURE 3. NREM sleep in a7-year-old patient with absenceseizures demonstrating a burst ofpolyspike-and-wave activity (A) andfragmentary bursts of spike-and-wave activity (B).
FIGURE 4. Time modulation of 3 Hz spike and wave activity. Note the marked attenuation of the spike-and-wave activityduring the REM sleep periods.
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society314
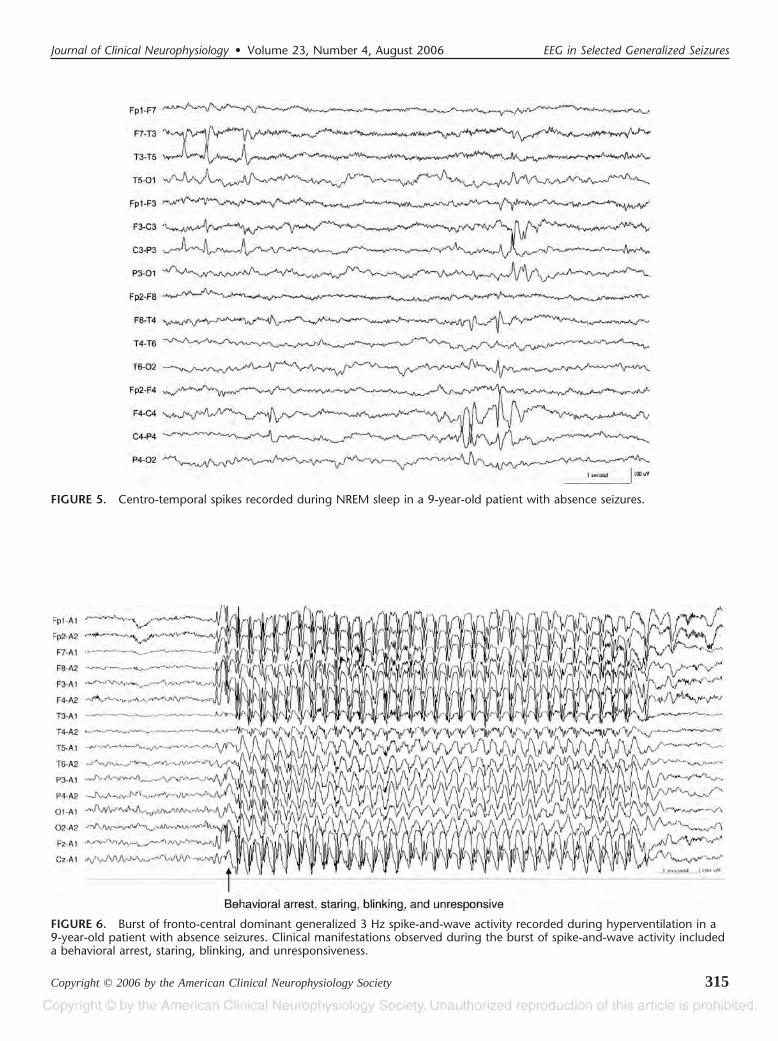
FIGURE 5. Centro-temporal spikes recorded during NREM sleep in a 9-year-old patient with absence seizures.
FIGURE 6. Burst of fronto-central dominant generalized 3 Hz spike-and-wave activity recorded during hyperventilation in a9-year-old patient with absence seizures. Clinical manifestations observed during the burst of spike-and-wave activity includeda behavioral arrest, staring, blinking, and unresponsiveness.
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 315

FIGURE 7. Bursts of 3.5 to 5 Hz spike-and-wave and polyspike-and-wave activity in a 12-year-old patient with juvenile myo-clonic epilepsy.
FIGURE 8. Photoparoxysmal response in a 14-year-old patient with juvenile myoclonic epilepsy.
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society316
have shown that, regardless of its duration, 3 Hz spike-and-waveactivity impairs performance (Mirsky and Van Buren, 1965;Goode et al., 1970; Porter et al., 1973; Browne et al., 1974).Thus, in the clinical setting, the number of absences occurringdaily is often difficult to determine, and a precise count requiresthe use of long-term video/EEG monitoring.
MYOCLONIC SEIZURES-JUVENILE MYOCLONICEPILEPSY
The EEG findings associated with myoclonic seizuresvary depending on the underlying epileptic syndrome. In thissection, only the EEG features associated with the myoclonicseizures seen in patients with juvenile myoclonic epilepsy(JME) will be discussed.
INTERICTAL EEG FINDINGSAs with other idiopathic generalized epilepsies, the back-
ground EEG activity is usually normal. There are bursts offrontocentral dominant generalized spike-and-wave andpolyspike-and-wave activity. The frequency of these burststends to be more irregular than the typical 3 Hz spike-and-wavebursts and varies between 3 and 5 Hz (Janz 1957, 1985, 1989,1990; Tsuboi, 1977; Delgado–Escueta and Enrile–Bascal, 1984;Fig. 7). The polyspikes may occur without the aftercoming slowwave. Frequently these bursts are fragmentary in appearance and
are often restricted to the frontal regions. Typical 3 Hz spike-and-wave activity may occur in JME patients and such patientsusually also exhibit clinical absence seizures.
During sleep, the bursts of spike-and-wave and polyspike-and-wave activity may decrease, particularly during deep slowwave sleep, and the bursts are markedly diminished, or absent,during REM sleep. Fragmentary bursts are frequently seenduring sleep. Arousal from sleep is an extremely potent activatorof spike-and-wave and polyspike-and-wave discharges (Tou-chon, 1982). In some patients, this may be the only timeepileptic activity is seen during a routine 30 to 60 minuteEEG recording. Likewise, clinical seizures often occur onawakening. Hyperventilation may increase or induce epilep-tic discharges (Janz, 1985) and approximately one third ofJME patients are photosensitive (Wolf and Goosses, 1986;Janz, 1990; Fig. 8).
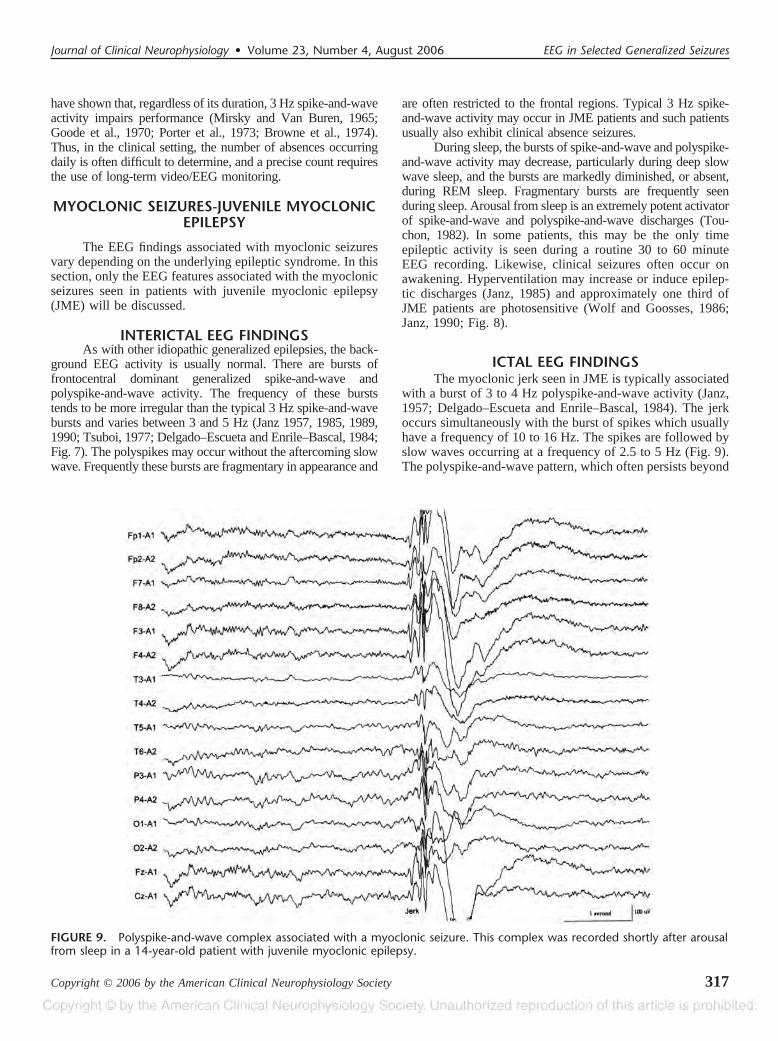
ICTAL EEG FINDINGSThe myoclonic jerk seen in JME is typically associated
with a burst of 3 to 4 Hz polyspike-and-wave activity (Janz,1957; Delgado–Escueta and Enrile–Bascal, 1984). The jerkoccurs simultaneously with the burst of spikes which usuallyhave a frequency of 10 to 16 Hz. The spikes are followed byslow waves occurring at a frequency of 2.5 to 5 Hz (Fig. 9).The polyspike-and-wave pattern, which often persists beyond
FIGURE 9. Polyspike-and-wave complex associated with a myoclonic seizure. This complex was recorded shortly after arousalfrom sleep in a 14-year-old patient with juvenile myoclonic epilepsy.
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 317

the termination of the myoclonic jerk, may last up to severalseconds (Fig. 10). The myoclonic jerks may occur in iso-lation or repetitively. As mentioned above, the arousalmechanism is a potent activator of the myoclonic seizuresseen JME.
IDIOPATHIC GENERALIZED TONIC-CLONICSEIZURES
Interictal EEG FindingsSince idiopathic generalized tonic-clonic seizures may
occur with any of the primary generalized seizure disorders, theinterictal EEG findings associated with these seizures are vari-able (see above). However, in all patients with idiopathic gen-eralized tonic-clonic seizures, the interictal background EEGactivity is usually normal, and the EEG may show brief bursts ofgeneralized 2.5 to 3.5 Hz spike-and-wave and/or polyspike-and-wave activity. In most patients, these bursts last less than 2.5seconds, and such bursts are frequently referred to as “abortive”spike-and-wave activity. It should be remembered that onlyabout one half of patients with primary generalized tonic-clonicseizures will demonstrate spike-and-wave activity on a routineEEG. Conversely, it is also important to realize that not all
patients whose EEG shows abortive generalized spike-and-waveactivity will experience clinical seizures.
As with most primary generalized seizures, the bursts ofspike-and-wave activity observed interictally in patients withidiopathic generalized tonic-clonic seizures typically becomemore frequent with the onset of slow wave sleep. The transitionperiod from wakefulness to drowsiness is particularly importantbecause, in some patients, this is the only time spike-and-waveactivity may appear in a routine EEG. Thus, it is imperative thata sleep EEG be obtained in all patients in whom the diagnosis ofseizures is being considered and that the awake-sleep transitionperiod be recorded. Fragmentary bursts of spike and waveactivity are also common during sleep in this condition.
ICTAL EEG FINDINGSIn the usual clinical setting, the background EEG activity
is obscured by high voltage myogenic artifact during a primarygeneralized seizure. Digital high frequency filtering of the mus-cle artifact allows for adequate visualization of the EEG activityin some patients. The most informative data concerning the ictalEEG changes associated with primary generalized tonic-clonicseizures has been obtained from patients paralyzed with muscle
FIGURE 10. Burst of 4 to 5 Hz spike-and-wave and polyspike-and-wave activity in a 42-year-old patient with juvenile myo-clonic epilepsy. Myoclonic jerks were associated with the first few spike-and-wave complexes.
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society318
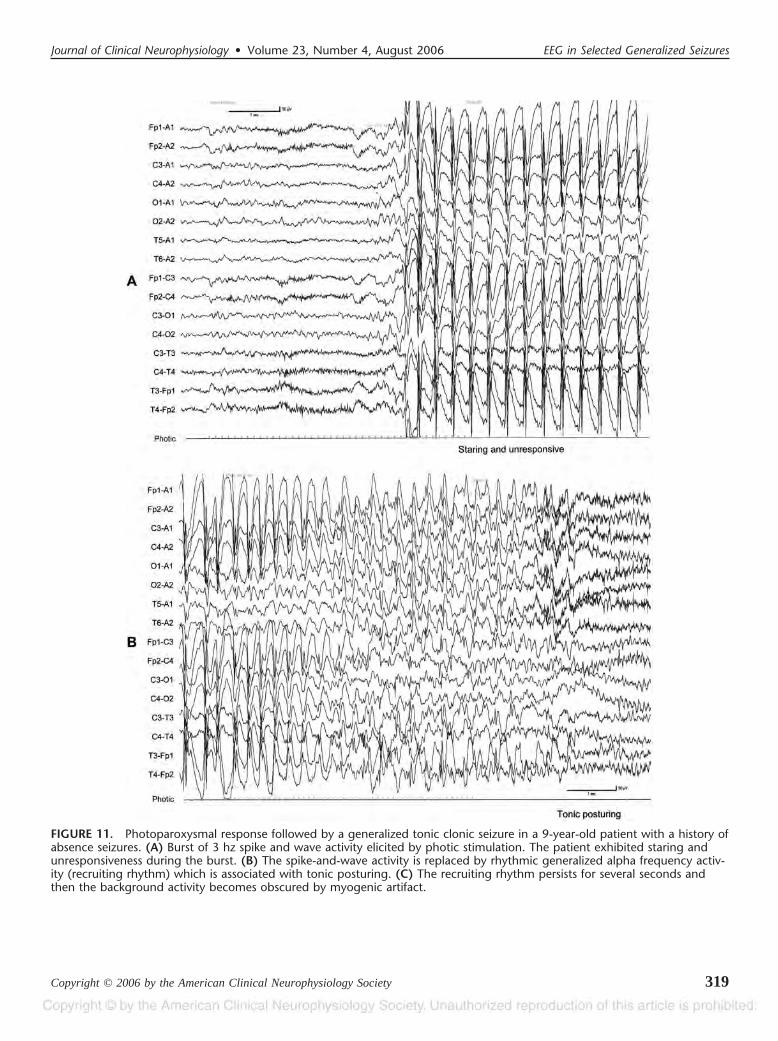
FIGURE 11. Photoparoxysmal response followed by a generalized tonic clonic seizure in a 9-year-old patient with a history ofabsence seizures. (A) Burst of 3 hz spike and wave activity elicited by photic stimulation. The patient exhibited staring andunresponsiveness during the burst. (B) The spike-and-wave activity is replaced by rhythmic generalized alpha frequency activ-ity (recruiting rhythm) which is associated with tonic posturing. (C) The recruiting rhythm persists for several seconds andthen the background activity becomes obscured by myogenic artifact.
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 319
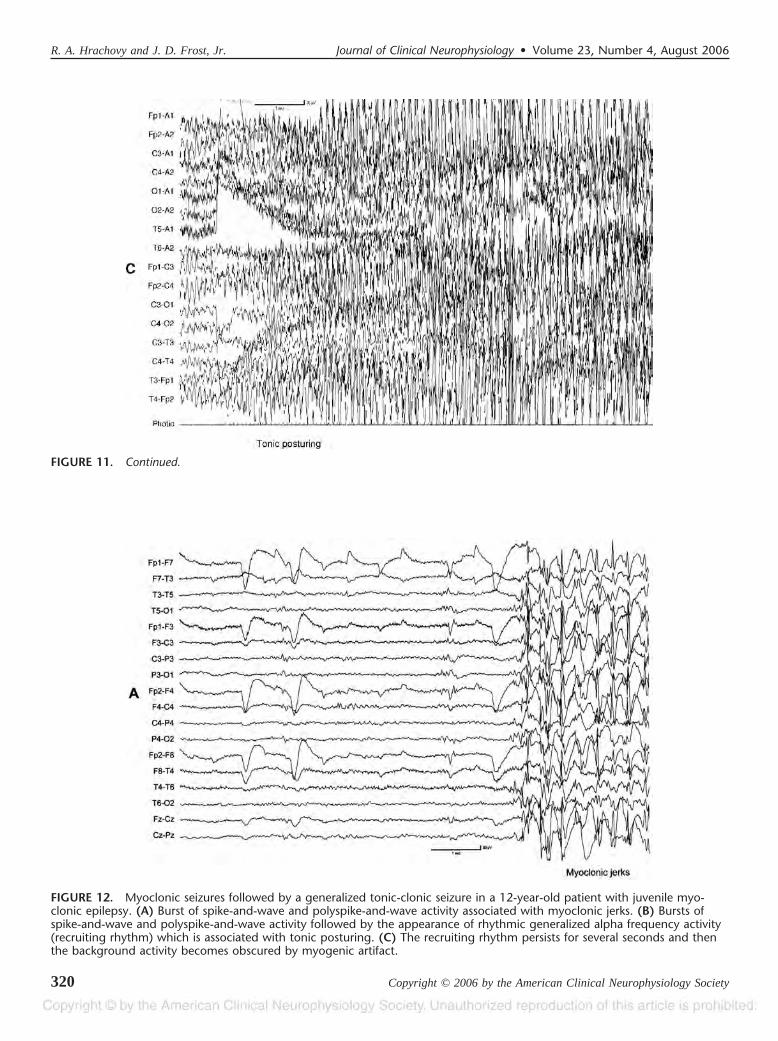
FIGURE 11. Continued.
FIGURE 12. Myoclonic seizures followed by a generalized tonic-clonic seizure in a 12-year-old patient with juvenile myo-clonic epilepsy. (A) Burst of spike-and-wave and polyspike-and-wave activity associated with myoclonic jerks. (B) Bursts ofspike-and-wave and polyspike-and-wave activity followed by the appearance of rhythmic generalized alpha frequency activity(recruiting rhythm) which is associated with tonic posturing. (C) The recruiting rhythm persists for several seconds and thenthe background activity becomes obscured by myogenic artifact.
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society320

relaxants. As the seizure begins, there may be recurrent high voltagepolyspike-and–wave bursts which are associated with myoclonicjerks and/or a cry. Then, the EEG typically shows generalizedvoltage attenuation with superimposed low voltage fast activity(20–40 Hz). This attenuation and superimposed fast activity maynot be seen at the onset of all generalized tonic-clonic seizures. Theattenuation lasts a few seconds and is followed by the appearance of
rhythmic generalized 10 to 12 Hz activity. This rhythmic alphafrequency activity progressively increases in amplitude over thenext 8 to 10 seconds and is associated with the tonic phase of theseizure. Thereafter, the EEG shows generalized slower activity,which increases in amplitude but slows in frequency from 7 to 8 to1 to 2 Hz. When the frequency of these waves reaches 4 to 5 Hz, thewaves become mixed with polyspikes and these polyspike-and-
FIGURE 12. Continued.
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 321

FIGURE 13. Hypsarrhythmia in a 23-month-old infant. (Reprinted from Hrachovy and Frost, 2003, with permission.)
FIGURE 14. Hypsarrhythmia withincreased interhemispheric synchro-nization in a 22-month-old infant.(Reprinted from Hrachovy andFrost, 2003, with permission.)
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society322
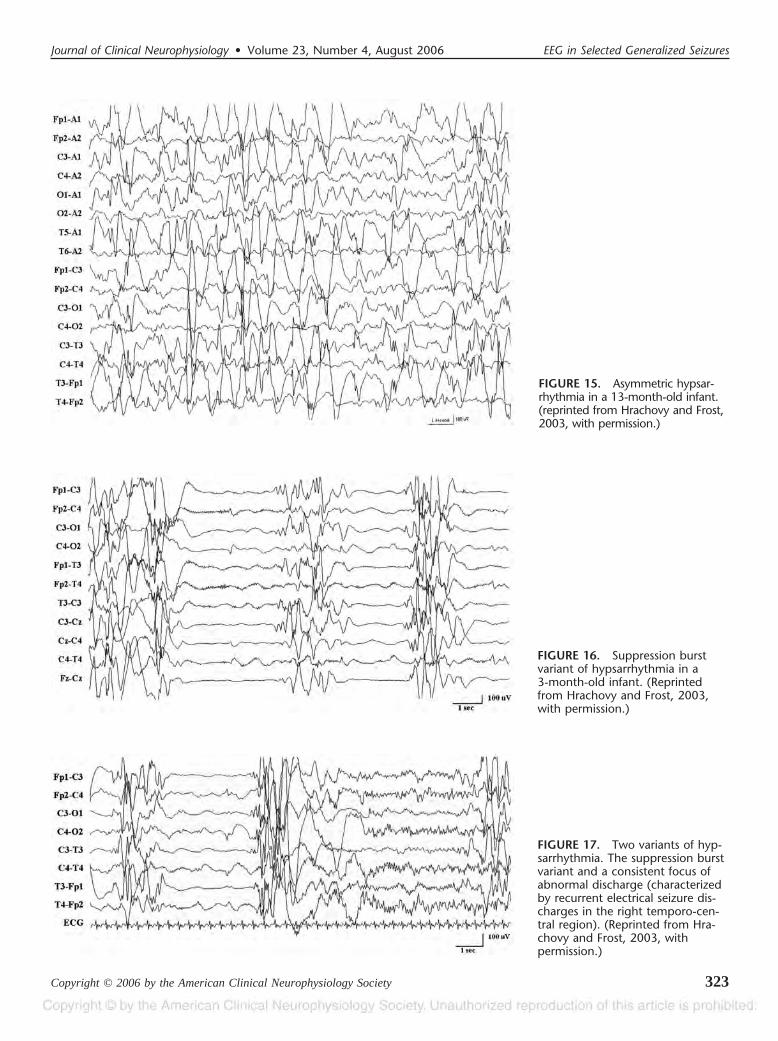
FIGURE 15. Asymmetric hypsar-rhythmia in a 13-month-old infant.(reprinted from Hrachovy and Frost,2003, with permission.)
FIGURE 16. Suppression burstvariant of hypsarrhythmia in a3-month-old infant. (Reprintedfrom Hrachovy and Frost, 2003,with permission.)
FIGURE 17. Two variants of hyp-sarrhythmia. The suppression burstvariant and a consistent focus ofabnormal discharge (characterizedby recurrent electrical seizure dis-charges in the right temporo-cen-tral region). (Reprinted from Hra-chovy and Frost, 2003, withpermission.)
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 323

wave complexes are associated with myoclonic jerks. As the seizurecontinues, the bursts of polyspike-and-wave activity become inter-mittent and between bursts the background EEG activity is sup-pressed. Following the last burst of polyspike-and-wave activity, theEEG shows a generalized voltage attenuation lasting several sec-onds. This attenuation is followed by irregular low voltage deltaactivity which gradually increases in frequency and amplitude(Gastaut and Broughton, 1972; Gastaut and Tassinari, 1975; Nied-ermeyer, 2005). The time required for the EEG to return to thebaseline state is highly variable from patient to patient. The onsetsof two generalized tonic-clonic seizures are shown in figures 11 and12.
In conclusion, although each of the idiopathic gen-eralized seizures is associated with a specific ictal EEGpattern, all of the seizures share two major interictalfeatures: the background EEG activity is usually normaland there are bursts of synchronous and symmetric 2.5 to3.5 Hz spike-and-wave and/or polyspike-and-wave activ-ity. Thus, when a routine EEG shows these two interictalfeatures, it can be strongly suggested that the findings areconsistent with a diagnosis of an idiopathic generalizedepilepsy.
CRYPTOGENIC OR SYMPTOMATICGENERALIZED EPILEPSIES
The EEG features of infantile spasms and three com-mon seizures associated with the Lennox Gastaut syndrome
(i.e., atypical absence, atonic, and tonic) will be discussed inthis section.
INFANTILE SPASMS
Interictal EEG FindingsThe most common interictal EEG pattern associated with
infantile spasms is hypsarrhythmia. This pattern consists ofgeneralized high voltage, generally asynchronous, slow wavesmixed with random high voltage multifocal spikes and sharpwaves. At times, the spikes and sharp waves occur in a gener-alized fashion, but they do not occur in rhythmic, repetitivesequences such as the slow spike slow wave discharges seen inthe Lennox Gastaut Syndrome (Vazquez and Turner, 1951;Gastaut and Remond, 1952; Kellaway, 1952; Alva–Moncayo etal., 2002; Frost and Hrachovy, 2003). Figure 13 illustrates thetypical hypsarrhythmic pattern. However, in many infantilespasms patients, variations of this prototypical pattern are seen(Hrachovy et al., 1984; Frost and Hrachovy, 2003; Hrachovyand Frost, 2003):
1. Hypsarrhythmia with increased interhemispheric syn-chronization (Fig. 14). In this variant, the diffuse asynchronousslow wave activity and the multifocal spike and sharp waveactivity are mixed with activity that exhibits a significant degreeof interhemispheric synchrony and symmetry. Most commonlythis activity takes the form of synchronous rhythmic frontal oroccipital dominant delta activity or synchronous frontal domi-
FIGURE 18. Hypsarrhythmia comprised of high voltage slow wave activity with little spike or sharp wave activity. (Reprintedfrom Hrachovy and Frost, 2003, with permission.)
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society324
nant slow spike and slow wave activity. This synchronousactivity usually occurs intermittently throughout the record.Most infants with hypsarrhythmia will show some degree ofsynchronization of the background activity if the disorder per-sists for many months, particularly those that transition to theLennox Gastaut syndrome.
2. Asymmetric hypsarrhythmia (Fig. 15). This patternis characterized by the presence of hypsarrhythmia, with aconsistent voltage asymmetry between hemispheres. The pat-tern is also referred to as hemihypsarrythmia or unilateralhypsarrhythmia. This pattern is associated with an underlyingstructural lesion of the brain and may be expressed over eitherthe more normal or abnormal hemisphere.
3. Hypsarrhythmia with episodes of generalized or later-alized voltage attenuation (Fig. 16). This variant is characterizedby a hypsarrhythmic pattern that is interrupted by recurrentepisodes of generalized or lateralized voltage attenuation. Suchepisodes of attenuation are most commonly seen during slow
wave sleep, however, in some patients they occur in a continu-ous, unremitting fashion. In this latter instance, the pattern isreferred to as the suppression burst variant of hypsarrhythmia.The electrodecremental episodes are also one of the ictal EEGpatterns associated with infantile spasms.
4. Hypsarrhythmia with a consistent focus of abnormaldischarge (Fig. 17). In this variant, a consistent focus of spikeor sharp wave activity is superimposed on a hypsarrhythmicbackground. In some patients, focal electrographic seizuredischarges may occur which do not disrupt the ongoinghypsarrhythmic activity.
5. Hypsarrhythmia with little or no spike or sharp waveactivity (Fig. 18). This is the least common of the variants andconsists of asynchronous and synchronous high voltage gen-eralized slow activity with little or no spike/sharp transients.
In addition to these variants, transient alterations occur inthe hypsarrhythmic pattern throughout the day. During slowwave sleep, the voltage of the background activity usually
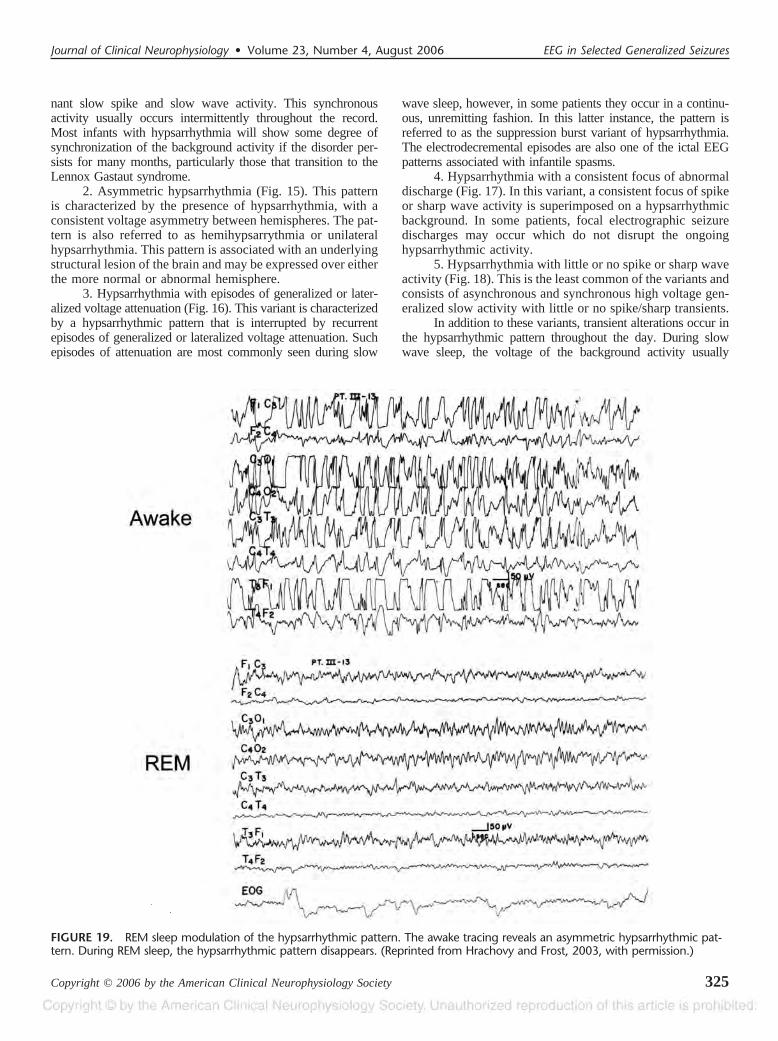
FIGURE 19. REM sleep modulation of the hypsarrhythmic pattern. The awake tracing reveals an asymmetric hypsarrhythmic pat-tern. During REM sleep, the hypsarrhythmic pattern disappears. (Reprinted from Hrachovy and Frost, 2003, with permission.)
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 325
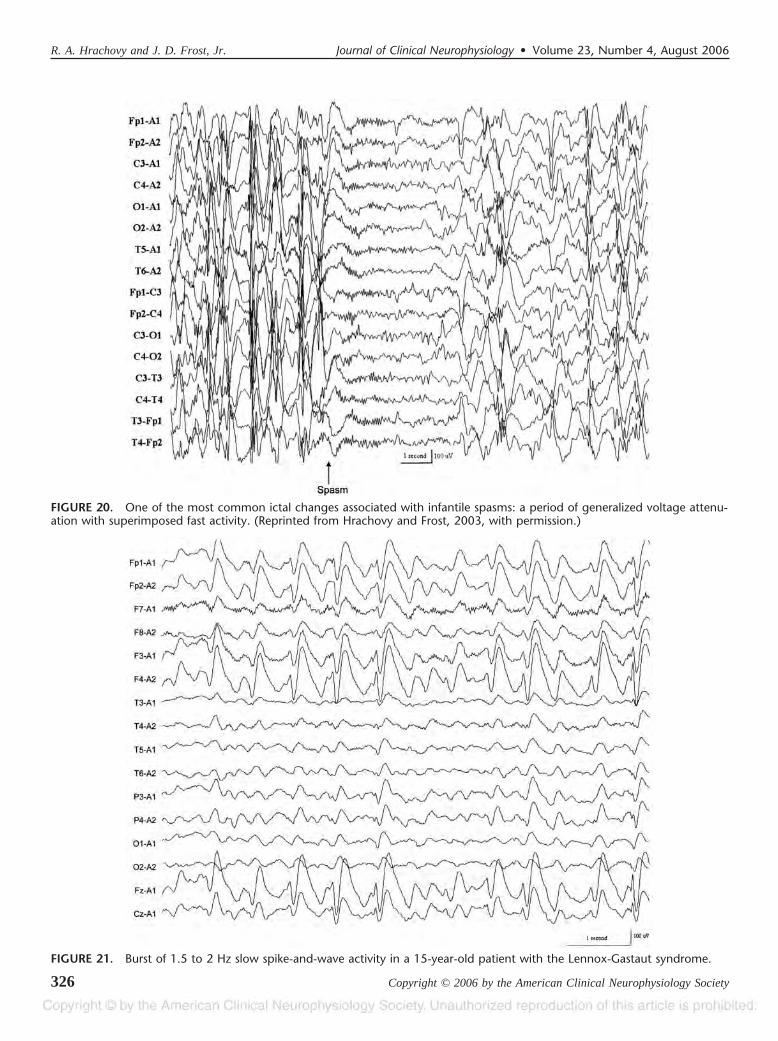
FIGURE 20. One of the most common ictal changes associated with infantile spasms: a period of generalized voltage attenu-ation with superimposed fast activity. (Reprinted from Hrachovy and Frost, 2003, with permission.)
FIGURE 21. Burst of 1.5 to 2 Hz slow spike-and-wave activity in a 15-year-old patient with the Lennox-Gastaut syndrome.
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society326

increases and often there is a grouping of the multifocal sharpwave and spike activity, resulting in a quasi-periodic pattern(Hrachovy et al., 1981, 1984; Watanabe et al., 1993). As notedpreviously, episodes of generalized voltage attenuation fre-quently occur during slow wave sleep. Conversely, duringREM sleep there is a marked reduction or total disappearanceof the hypsarrhythmic pattern (Hrachovy et al., 1981, 1984,Fig. 19). Furthermore, on arousal from sleep, the hypsar-
rhythmic pattern is frequently markedly reduced or abolishedand this change may last from seconds to many minutes.Finally, the hypsarrhythmic pattern may also disappear or begreatly reduced during a cluster of spasms, only to returnimmediately after cessation of the spasms (Hrachovy et al.,1984).
Although hypsarrhythmia and its variants are the mostcommon patterns seen with infantile spasms, other interictal
FIGURE 22. Attenuation episodes during NREM sleep in an 11-year-old patient with the Lennox-Gastaut syndrome.
FIGURE 23. Bursts of generalized fast activity during NREM sleep in a 13-year-old patient with the Lennox-Gastaut syn-drome. Such bursts of fast activity may be associated with tonic seizures.
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 327

patterns may be seen. These include diffuse slowing, focalslowing, focal or multifocal spikes and sharp waves, parox-ysmal slow or fast activity, slow spike-and-wave activity, andcontinuous fast and spindling. These patterns may occur inisolation or in various combinations. In rare instances, theinterictal EEG may be normal. This situation is most oftenencountered when hypsarrhythmia disappears followingtreatment, although clinical spasms may continue. However,normal interictal background may be seen shortly after theonset of the disorder. In such instances, hypsarrhythmia willusually be seen on subsequent EEG recordings.
ICTAL EEG FINDINGSVideo/EEG monitoring studies have identified 11
different ictal EEG patterns that occur with infantilespasms (Kellaway et al., 1979; Yamatogi and Ohtahara,1981; King et al., 1985; Donat and Wright, 1991, Fuscoand Vigevano, 1993; Haga et al., 1995a, 1995b; Wong andTrevathan, 2001). These include: (1) a high voltage, fron-tal dominant, generalized slow wave transient; (2) a gen-eralized sharp and slow wave complex; (3) a generalizedsharp and slow wave complex followed by a period ofvoltage attenuation; (4) a period of voltage attenuationonly (electrodecremental episode); (5) a generalized slowwave transient only; (6) a period of voltage attenuationwith superimposed fast activity; (7) a generalized slowwave transient followed by a period of voltage attenuation
with superimposed fast activity; (8) a period of attenuationwith rhythmic slow activity; (9) fast activity only; (10) asharp and slow wave complex followed by a period ofvoltage attenuation with superimposed fast activity; and(11) a period of voltage attenuation with superimposed fastactivity followed by rhythmic slow activity. The mostcommon ictal pattern seen is a period of generalizedvoltage attenuation (Fig. 20). The duration of the ictalevents can range from less than a second to more than 100seconds. There is no close correlation between specifictypes of clinical events (e.g., flexor, extensor, or mixedspasms) and specific ictal EEG patterns. Also, as notedabove, episodes of voltage attenuation frequently occurduring slow wave sleep in the absence of clinical spasms.Also, no significant correlation has been found between thevarious ictal EEG patterns and underlying cause, responseto therapy, or long term developmental outcome (Haga etal., 1995a, 1995b). However, as with the asymmetrichypsarrhythmic pattern, an asymmetric ictal EEG patterndoes correlate with focal or lateralized structural lesions.Asymmetric spasms frequently occur in association withasymmetric ictal patterns (Donat and Lo, 1994; Gaily etal., 1995, 2001).
The ictal discharges frequently occur in clusters near theend of REM sleep periods. If the patient awakens from REMsleep during this cluster, the ictal complexes may becomeassociated with clinical spasms (Hrachovy et al., 1981).
FIGURE 24. Burst of frontal dominant 2 to 2.5 Hz slow spike-and-wave activity associated with an atypical absence seizure,during which time the patient stared and was nonresponsive to name calling.
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society328

FIGURE 25. Generalized voltage attenuation associated with a tonic seizure in a 15-year-old patient with the Lennox-Gastautsyndrome.
FIGURE 26. Generalized voltage attenuation with superimposed fast activity associated with a tonic seizure in a 3-year-oldpatient with the Lennox-Gastaut syndrome.
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 329
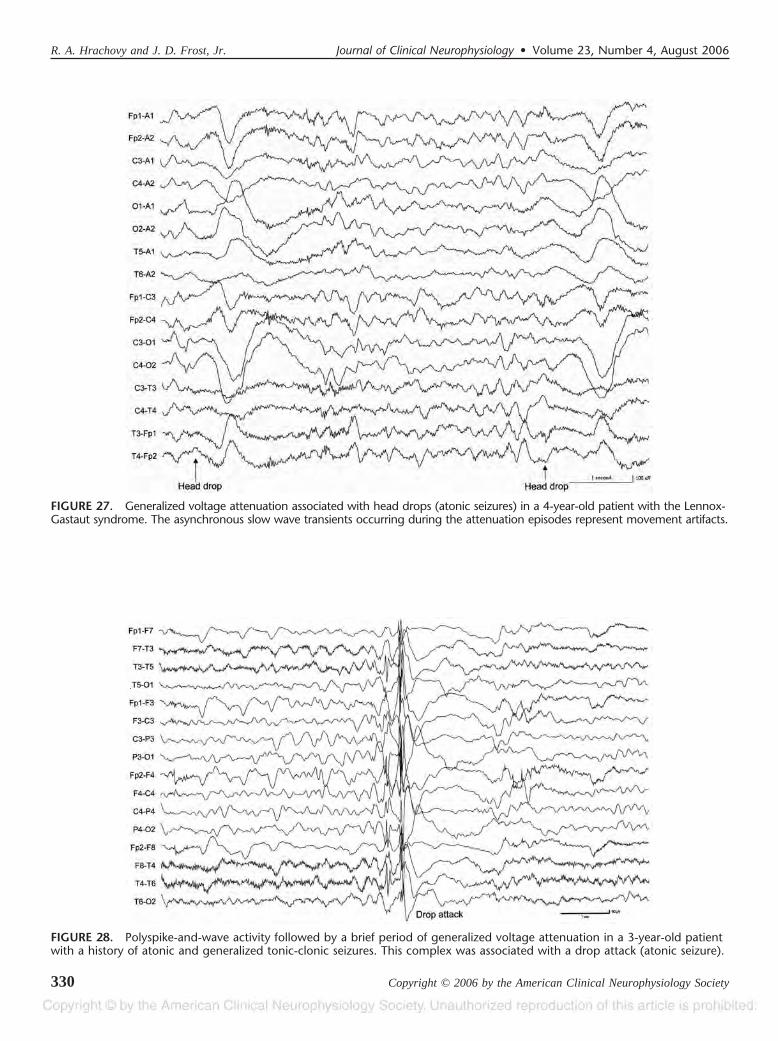
FIGURE 27. Generalized voltage attenuation associated with head drops (atonic seizures) in a 4-year-old patient with the Lennox-Gastaut syndrome. The asynchronous slow wave transients occurring during the attenuation episodes represent movement artifacts.
FIGURE 28. Polyspike-and-wave activity followed by a brief period of generalized voltage attenuation in a 3-year-old patientwith a history of atonic and generalized tonic-clonic seizures. This complex was associated with a drop attack (atonic seizure).
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society330

LENNOX GASTAUT SYNDROME
(Atypical Absence, Tonic And Atonic Seizures)Interictal EEG Findings
The EEG usually shows moderate to severe slowing ofthe background activity (Gastaut et al., 1966; Chevrie andAicardi, 1972; Markand, 1977, 2003; Bauer et al., 1983). Thecharacteristic interictal EEG pattern in the Lennox Gastautsyndrome is the slow spike-and-wave discharge. Althoughthe frequency of this discharge may vary from 1 to 4 Hz, thetypical frequency is 1.5 to 2.5 Hz (Blume et al., 1973;Markand, 1977, 2003; Fig. 21). The frequency, amplitude,distribution, and morphology often vary between bursts andduring bursts of slow spike-and-wave activity. Shifting asym-metries of the discharge are common. If patients have largeunilateral hemispheric lesions, the slow spike-and-wave ac-tivity is generally higher over the good hemisphere withcorresponding suppression of the background activity overthe abnormal hemisphere (Markand, 1977, 2003).
There is a marked variation in the duration of the slowspike-and-wave bursts between patients and across serialEEGs in a given patient. Bursts may last only a few secondsor they may occur in long runs. In some patients, the dis-charge may be virtually continuous and it is often difficult todetermine in such patients whether the discharge is associatedwith a clinical seizure (Gastaut et al., 1966; Blume et al.,1973; Markand, 1977, 2003).
Slow spike-and-wave activity is generally not influ-enced by hyperventilation or photic stimulation. However,slow wave sleep dramatically increases the number ofbursts and duration of the discharges and the slow-spike-and-slow-wave complexes frequently become intermixedwith polyspikes. Electrodecremental periods lasting from 2to 4 seconds may occur during slow wave sleep and, ifprominent, may produce a suppression burst pattern(Gastaut et al., 1966; Blume et al., 1973; Markand, 1977;Fig. 22). Also common in Lennox Gastaut syndromepatients is the presence of bursts of fast activity duringslow wave sleep (Gibbs and Gibbs, 1952; Brenner andAtkinson, 1982; Beaumanoir and Dravet, 1992; Markand,2003; Fig. 23). The frequency of this fast activity is 10 to25 Hz, and it is typically generalized, although it is usuallymaximally expressed in the frontal and central regions.These bursts of fast activity may last up to 10 seconds andmay be associated with tonic seizures (see below). DuringREM sleep, the bursts of slow spike-and-wave activity aregreatly diminished (Blume et al., 1973; Amir et al., 1986;Horita et al. 1987).
In addition to the generalized slow spike-and-wave dis-charges, focal, or multifocal spike and sharp wave dischargesmay be seen (Blume et al., 1973; Markand, 1977, 2003).
Ictal EEG FindingsPatients with Lennox Gastaut syndrome experience
multiple seizure types, both generalized and focal. The ictalEEG changes associated with three generalized seizures com-monly encountered (atypical absence, tonic, and atonic) arebriefly discussed here.
Atypical Absence SeizuresAtypical absence seizures are accompanied by bursts of
high amplitude generalized 1.5 to 2.5 Hz activity basicallyindistinguishable from that seen interictally (Markand, 1977;Fig. 24). Less commonly, bursts of fast activity (10-20 Hz) havebeen reported to accompany atypical absence seizures (Blume etal., 1973, Markand, 2003). In general, the impairment of con-sciousness that occurs with atypical absence seizures is progres-sive and not abrupt like that which occurs with 3 Hz spike-and-wave activity. Likewise, recovery of consciousness at the end ofthe seizure is gradual. Thus, in severely retarded individuals, thedetection of atypical absence seizures at bedside may be ex-tremely difficult. The occurrence of drooling, changes in pos-tural tone and myoclonus of the eyelids or perioral musculaturemay aid in the clinical identification of the seizures. However, inmany patients, long runs of slow spike-and-wave dischargesfrequently occur without any apparent change in the patient’sclinical state.
Tonic SeizuresThe EEG during tonic seizures may show generalized
voltage attenuation or so-called electrodecremental change,bursts of rhythmic fast activity (15-25 Hz), or attenuationfollowed by rhythmic fast activity (Gastaut and Tassinari,1975; Markand, 1977; Horita et al. 1987; Figs. 25, 26). Ageneralized slow spike-and-wave complex may precede theseictal patterns. Following the ictal event, the EEG may showgeneralized delta activity for several seconds before returningto the baseline state (Markand, 2003). As mentioned previ-ously, bursts of fast activity frequently occur during slowwave sleep and may or may not be associated with clinicalseizure activity. Some of the clinical seizures occurringduring sleep are subtle (e.g., eye opening and minimal up-wards eye deviation) and may be easily missed withoutvideo/EEG monitoring.
Atonic SeizuresAtonic seizures have been associated with a variety of
ictal EEG patterns (Markand, 2003) including generalizedspike-and-wave activity, generalized polyspike-and-wave ac-tivity, generalized voltage attenuation (Fig. 27), and runs oflow or high voltage fast activity. These patterns can occuralone or in various combinations (Fig. 28).
REFERENCESAlva-Moncayo E, Diaz-Leal MC, Olmos-Garcia de Alba G. Electroencepha-
lographic discoveries in children with infantile massive spasms inMexico. Rev Neurol. 2002;34:928–32.
Amir N, Shalev RS, Steinberg A. Sleep patterns in the Lennox-Gastautsyndrome. Neurology. 1986;36:1224–6.
Bauer G, Aichner F, Saltuari L. Epilepsies with diffuse slow spikes andwaves of late onset. Eur Neurol. 1983;22:344–50.
Beaumanoir A, Dravet C The Lennox-Gastaut syndrome. In: Roger, J,Bureau M, Dravet C, Dreifuss FE, Perret A, Wolf P, eds. Epilepticsyndromes in infancy, childhood and adolescence. London: JohnLibbey, 1992:115–32.
Blume WT, David RB, Gomez MR. Generalized sharp and slow wavecomplexes: associated clinical features and long-term follow-up. Brain.1973;96:289–306.
Brenner RP, Atkinson R. Generalized paroxysmal fast activity: electroen-cephalographic and clinical features. Ann Neurol. 1982;11:386–90.
Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006 EEG in Selected Generalized Seizures
Copyright © 2006 by the American Clinical Neurophysiology Society 331

Browne TR, Penry JK, Porter RJ, Dreifuss FE. Responsiveness before,during, and after spike-wave paroxysms. Neurology. 1974;24:659–65.
Chevrie JJ, Aicardi J. Childhood epileptic encephalopathy with slow spike-wave: a statistical study of 80 cases. Epilepsia. 1972;13:259–71.
Dalby MA. Epilepsy and 3 per second spike-and-wave rhythm. Acta NeurolScand Suppl. 1969;45:1–183.
Daly DD Epilepsy and Syncope. In: Pedley, TA, Daly DD, eds. Currentpractice of clinical electroencephalography, 2nd edition. New York:Raven Press, 1990:269–334.
Delgado-Escueta AV, Enrile-Bacsal F. Juvenile myoclonic epilepsy of Janz.Neurology. 1984;34:285–294.
Donat JF, Lo WD. Asymmetric hypsarrhythmia and infantile spasms in Westsyndrome. J Child Neurol. 1994;9:290–6.
Donat JF, Wright FS. Unusual variants of infantile spasms. J Child Neurol.1991;6:313–8.
Frost JD Jr., Hrachovy RA. Infantile spasms. Boston: Kluwer AcademicPublishers, 2003.
Fusco L, Vigevano F. Ictal clinical electroencephalographic findings ofspasms in West syndrome. Epilepsia. 1993;34:671–8.
Gaily E, Liukkonen E, Paetau R, et al. Infantile spasms: diagnosis andassessment of treatment response by video-EEG. Dev Med Child Neu-rol. 2001;43:658–67.
Gaily EK, Shewmon DA, Chugani HT, Curran JG. Asymmetric and asyn-chronous infantile spasms. Epilepsia. 1995;36:873–82.
Gastaut H, Broughton, R. 1972. Epileptic seizures. Springfield, IL: CharlesC. Thomas.
Gastaut H, Remond A. Etude electroencephalographique des myoclonies.Rev Neurol. 1952;86:596–609.
Gastaut H, Roger J, Soulayrol R, et al. Childhood epileptic encephalopathyof children with diffuse slow spike-waves (otherwise known as “petitmal variant”) or Lennox syndrome. Epilepsia. 1966;7:139–79.
Gastaut H, Tassinari CA. The Ictal and Interictal EEG in different types ofepilepsy. In: Handbook of electroencephalography and clinical neuro-physiology, vol. 13A: The epilepsies. Amsterdam: Elsevier, 1975:1–104.
Gibbs FA, Gibbs EL. Atlas of electroencephalography, vol. 2. Epilepsy.Cambridge, MA: Addison-Wesley, 1952.
Goode DJ, Penry JK, Dreifuss FE. Effects of paroxysmal spike-wave oncontinuous visual-motor performance. Epilepsia. 1970;11:241–54.
Haga Y, Watanabe K, Negoro T, et al. Do ictal, clinical, and electroencepha-lographic features predict outcome in West syndrome? Pediatr Neurol.1995a;13:226–9.
Haga Y, Watanabe K, Negoro T, et al. Ictal electroencephalographic findingsof spasms in West syndrome. Psychiatr Clin Neurosci. 1995b;49:S233–4.
Holmes GL, McKeever M, Adamson M. Absence seizures in children:clinical and electroencephalographic features. Ann Neurol. 1987;21:268–273.
Horita H, Kumagai K, Maekawa K. Overnight polygraphic study of Lennox-Gastaut syndrome. Brain Dev. 1987;9:627–35.
Hrachovy RA, Frost JD Jr. Infantile Epileptic Encephalopathy with Hypsar-rhythmia (Infantile spasms/West syndrome). J Clin Neurophysiol. 2003;20:408–25.
Hrachovy RA, Frost JD Jr., Kellaway P. Hypsarrhythmia: variations on thetheme. Epilepsia. 1984;25:317–25.
Hrachovy RA, Frost JD Jr., Kellaway P. Sleep characteristics in infantilespasms. Neurology. 1981;31:688–93.
Janz D. Epilepsy with impulsive petit mal (juvenile myoclonic epilepsy).Acta Neurol Scand. 1985;72:449–59.
Janz D Juvenile myoclonic epilepsy. In: Dam M, Gram, L, eds. Comprehen-sive epileptology. New York: Raven Press, 1990;171–85.
Janz D. Juvenile myoclonic epilepsy: Epilepsy with impulsive petit mal.Cleve Clin J Med. 1989;56(Suppl. 1):S23–33.
Janz D, Christian W. Impulsiv-Petit mal: Dtsch Z Nervenheilk 1957;176:348–86.
Kellaway P. Myoclonic phenomena in infants. Electroencephalogr ClinNeurophysiol. 1952;4:243.
Kellaway P, Frost JD Jr. Biorhythmic modulation of epileptic events. In:Pedley, TA, Meldrum BS, eds. Recent advances in epilepsy. Churchill-Livingstone: Edinburgh, 1983;139–54.
Kellaway P, Hrachovy RA, Frost JD Jr., Zion T. Precise characterization andquantification of infantile spasms. Ann Neurol. 1979;6:214–8.
King DW, Dyken PR, Spinks IL Jr., Murvin AJ. Infantile spasms: ictalphenomena. Pediatr Neurol. 1985;1:213–8.
Markand ON. Lennox-Gastaut syndrome childhood epileptic encephalopa-thy. J Clin Neurophysiol. 2003;20:426–41.
Markand ON. Slow spike-wave activity in EEG and associated clinicalfeatures: often called “Lennox” or “Lennox-Gastaut” syndrome. Neu-rology. 1977;27:746–57.
Mirsky AF, Van Buren JM. On the nature of the absence in centrencephalicepilepsy. Electroencephalogr Clin Neurophysiol. 1965;18:334–48.
Niedermeyer E Epileptic seizure disorders: In: Niedermeyer, E, Lopes DaSilva F, eds. Electroencephalography: Basic principles, clinical appli-cations and related fields, 5th edition. Philadelphia: Lippincott Williamsand Wilkins, 2005:505–619.
Niedermeyer E. The generalized epilepsies. Charles C. Thomas, Springfield,IL, 1972.
Niedermeyer E. Sleep electroencephalograms in petit mal. Arch Neurol.1965;12:625–30.
Penry JK, Porter RJ, Dreifuss FE. Simultaneous recording of absenceseizures with videotape and electroencephalography. A study of 374seizures in 48 patients. Brain. 1975;98:427–40.
Porter RJ, Penry JK, Dreifuss FE. Responsiveness at the onset of spike-wavebursts. Electroencephalogr Clin Neurophysiol. 1973;34:239–45.
Ross JJ, Johnson LC, Walter R. Spike and wave discharges during stages ofsleep. Arch Neurol. 1966;14:399–407.
Sato S, Dreifuss FE, Penry JK. The effect of sleep on spike-wave dischargesin absence seizures. Neurology. 1973;23:1335–45.
Sato SS, Dreifuss FE, Penry JK, et al. Long-term follow-up of absenceseizures. Neurology. 1983;33:1590–5.
Touchon J. Effect of awakening on epileptic activity in primary generalizedmyoclonic epilepsy. In: Sterman, MB, Shouse MN, Passouant P, eds.Sleep and epilepsy. New York: Academic Press, 1982.
Tsuboi T. Primary generalized epilepsy with sporadic myoclonias of myo-clonic petit mal type. Stuttgart: Thieme, 1977.
Vazquez HJ, Turner M. Epilepsia en flexion generalizada. Arch ArgentPediatr. 1951;35:111–41.
Watanabe K, Negoro T, Aso K, Matsumoto A. Reappraisal of interictalelectroencephalograms in infantile spasms. Epilepsia. 1993;34:679–85.
Wolf P, Goosses R. Relation of photosensitivity to epileptic syndromes.J Neurol Neurosurg Psychiat. 1986;49:1368–91.
Wong M, Trevathan E. Infantile spasms. Pediatr Neurol. 2001;24:89–98.Yamatogi Y, Ohtahara S. Age-dependent epileptic encephalopathy: a longi-
tudinal study. Folia Psychiatr Neurol Jpn. 1981;35:321–32.
R. A. Hrachovy and J. D. Frost, Jr. Journal of Clinical Neurophysiology • Volume 23, Number 4, August 2006
Copyright © 2006 by the American Clinical Neurophysiology Society332