the effect of hypocapnia blood pressure - homepage |...
TRANSCRIPT

The Effect of Hypocapnia on ArterialBlood Pressure
By J. F. BURNUM, M.D., J. B. HICKAM, M.D., AND H. D. MCINTOSH, M.D.In man, hypocapnia induced by hyperventilation causes a drop in arterial pressure. The calculatedperipheral resistance is decreased, indicating a net vasodilatation. The forearm blood flow is mark-edly increased, and the vascular resistance of the forearm is much reduced. Persons with impairedfunction of the sympathetic nervous system continue to show these effects. The increase in forearmflow is not prevented by brachial block. These results suggest that hypocapnia acts directly on bloodvessels to produce a net over-all vasodilatation and fall in blood pressure, and that this effect isnot mediated through the nervous system, as usually supposed.
BREATHING carbon dioxide raises theblood pressure and hyperventilationlowers it in man and experimental
animals. Changes in blood carbon dioxide aresupposed to affect vessels both directly andby way of the vasomotor centers.' Theseactions are thought to be opposite in direction,with the central effect being the stronger.That is, a high carbon dioxide level causes anover-all vasoconstriction because of its effecton the vasomotor centers, even though thedirect action is to dilate vessels. Loss of carbondioxide has opposite effects, both centrally andlocally. These conclusions are based on animalexperiments.
It is the purpose of this paper to describe theeffects on vascular tone of lowering carbondioxide by hyperventilation in (1) normalsubjects and (2) patients in whom portions ofthe nervous system have been destroyed bydisease or surgery or blocked by drugs. Theresults of this study do not support the con-ventional concept of the means by whichcarbon dioxide affects vascular tone.
METHODS
Hyperventilation studies, unless otherwise speci-fied, were conducted on recumbent subjects during
From the Department of Medicine, Duke Univer-sity School of Medicine, Durham, N. C.
This study was aided (in part) by a research grant,Public Health Service H-1370, from the NationalHeart Institute, U. S. Public Health Service, and (inpart) by a grant from the Life Insurance MedicalResearch Fund.
Dr. Burnum was formerly a Life Insurance Med-ical Research Fellow.
Dr. McIntosh is a Research Fellow of the Amer-ican Heart Association.
89
one-minute periods of maximal voluntary forcedbreathing of either room air or a 5 per cent carbondioxide, 21 per cent oxygen gas mixture. Proceduresincluded simultaneous measurements of forearmblood flow by plethysmography, intraarterial pres-sure, pulse rate, cardiac output by dye dilutionmethod2 and arterial blood pH and carbon dioxidecontent;3a4 from the latter blood carbon dioxidetension was calculated. Local forearm vascular re-sistance was calculated as
mean blood pressvre (mm. Hg)forearm blood flow (cc./min./100 cc. tissue)
and over-all peripheral resistance as
mean blood pressvre (mm. Hg)cardiac output (L/min.)
Forearm blood flows at 37 C. with hand excluded,5central venous pressure and intra-arterial pressureswere measured with the use of strain gauges and aSanborn Poly-Viso oscillograph. Single determina-tions of cardiac output were separated by 15-minuteintervals, and the Evans blue dye was injectedthrough a standard cardiac catheter threaded intoone of the intrathoracic great veins (subclavian orsuperior vena cava) or right atrium. Arterial bloodsamples for dye analysis were collected from thebrachial or femoral artery.
Brachial plexus block was achieved by infiltra-tion with 20 cc. of 2 per cent xylocaine containing1:300,000 epinephrine.*
RESULTSControl Subjects
After a period of one minute of forcedbreathing, the arterial blood carbon dioxidetension was commonly halved, falling toaround 20 mm. Hg, and the pH rose to around7.6. Maximal forced voluntary hyperventila-
* Courtesy of Dr. W. K. Nowill, Department ofAnesthesiology, Duke University School of Medicine.
Circulation, Volume IX, January 1954
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

HYPOCAPNIA AND ARTERIAL BLOOD PRESSURE
TABLE 1.-Circulatory Changes during Hyperventilation (Air). Control Subjects
Case no.
1
State
RestHyperventilation
2 RestHyperventilation
3 RestHyperventilation
4 RestHyperventilation
5 RestHyperventilation
6 RestHyperventilation
7 RestHyperventilation
8 RestHyperventilation
9* RestHyperventilation
Mean B.P. Pulse rate, Cardiacoutput,mm. Hg per. min. L./min.
56 6831 114
89 6463 125
85 8263 160
81 7663 124
91 7070 130
87 9453 160
99 6875 104
93 8076 140
137 90115 140
8.018.7
7.28.1
8.910.1
7.610.0
6.66.8
7.413.9
7.910.4
4.44.8
5.312.0
Forearmbloodflow,
cc./min.!100 cc. arm
Vascular resistance
Over-allPeriph- Forearm,eraT, Mean BP/
Mean BP/ ForearmCardiac flowOutput
12.2 7.0 4.631.0 1.7 1.9
7.5 12.3 11.920.0 7.8 3.8
6.4 9.5 13.38.4 6.2 10.0
11.0 10.7 7.227.3 6.3 2.7
9.7 13.8 9.419.3 10.3 5.4
8.1 11.7 10.820.5 3.8 2.8
11.2 12.5 8.835.2 7.2 3.0
21.115.8
8.3 25.8 16.521.8 9.6 5.3
Mean cir.time,sec.
pH37o pCOsmm. H'g
15.4 7.396.9 7.55
19.2 7.38 40.010.5 7.64 16.8
14.1 7.45 35.58.0 7.62 19.3
14.5 7.39 44.89.3 7.60 22.4
21.1 7.35 45.111.7 7.59 19.0
15.38.4
24.0 7.38 47.013.6 7.56 27.0
15.5 7.39 40.012.1 7.60 20.0
16.5 7.35 41.47.6 7.60 19.2
* Essential hypertension.
tion on 5 per cent carbon dioxide producedlittle or no change in the arterial blood carbondioxide tension. When normal subjects are
allowed to breathe 5 per cent carbon dioxideat will, there is an average increase of approxi-mately 10 mm. Hg in the arterial carbon di-oxide tension. Selected data from eight normalsubjects and one hypertensive patient in whomthe cardiac output was measured are presentedin table 1. Figure 1 shows a schematic summaryof the data pooled from all the control subjects.Mean arterial pressure fell during the period
of one-minute overbreathing in 33 of the 35subjects and was unchanged in two. Theaverage maximal fall was 18 mm. Hg. In some
subjects this fall was transient, with recoveryor even overshoot of the pressure during hyper-ventilation (fig. 2). In other instances recoverywas delayed until after the cessation of the
hyperventilation. In 16 patients forced over-breathing of a 5 per cent carbon dioxidemixture caused no change in pressure. Hyper-ventilation on air caused a striking increasein heart rate; on 5 per cent carbon dioxideonly a moderate increase.The cardiac output during hyperventilation
on air was measured in nine subjects. It in-creased an average of 50 per cent. The circula-tion time was halved (average decrease 43per cent). Measurements were made on threesubjects hyperventilating on 5 per cent carbondioxide; the output decreased in two of thethree subjects and was unchanged in one.
Central venous pressure was measured inthe right atrium or superior vena cava in sevensubjects. There was no change in six and arise of 5 mm. Hg in one.k In 16 subjects hyperventilation on air
90
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

BURNUM, HICKAM AND McINTOSH
(2Z
c4+100LC0I~I,cc +50U-
(2
<Z B.P.(I£ Cordioc Foreorm~- I - Output Flowz
o Ko D:Hypervent. on air O:-50 Overol Ir Hypervent. on 5% CO2 ForeormVosculor Resistonce
FIG. 1. Mean values of circulatory changes duringrecumbent hyperventilation in control subjects arepresented as per cent change from resting measure-ments. During overbreathing on air the blood pres-sure falls and cardiac output and forearm blood flowrise; the calculated over-all and local forearm vascu-lar resistance decrease. During hyperventilation on5 per cent carbon dioxide there is only a small in-crease in forearm flow. These average changes werecalculated from data on blood pressure in 35 subjects,forearm flow in 16 subjects, and cardiac output in 9subjects.
2 sec.
increased the blood flow in the forearm to anaverage of 2.5 times the control level. Hyper-ventilation on 5 per cent carbon dioxide alsoincreased the flow, but the increase averagedonly a third as much as when hypocapnia wasallowed to develop. This effect on forearm flowis similar to that recently reported by Clarke.6
Comment. In normal subjects overbreathingon air causes tachycardia, fall in arterialpressure, increased cardiac output and in-creased forearm blood flow. The increase incardiac output in the presence of a reducedmean blood pressure indicates an over-all fallin peripheral resistance. The forearm is one ofthe areas where the resistance is lowered.These data are in general agreement with
those in the literature. Henderson7 pointed outthat Ewald in 1873 produced hypotensionand apnea in dogs by hyperventilation, andMosso found the same effects in man. Thelatter coined the word "acapnia" from theGreek kcapnos meaning "smoke." Hendersonshowed that the fall in blood pressure in both
5% CO2FIG. 2. Continuous intra-arterial pressure tracings during recumbent hyperventilation in normal
subjects. During hyperventilation on air the arterial pressure falls but may tend to recover whileoverbreathing continues, top record, or not until later, middle record. On 5 per cent carbon dioxideno significant fall occurs. (Arrows indicate period of hyperventilation.)
91
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

HYPOCAPNIA AND ARTERIAL BLOOD PRESSURE
dog and man was prevented by breathing acarbon dioxide mixture instead of air.Roomes overventilated dogs in a Drinker
respirator and demonstrated that the fall inarterial pressure resulted from over-all pe-ripheral vasodilation and was prevented bybreathing carbon dioxide. The cardiac outputwas measured by the direct Fick method.
Dale and Evans found in the cat that hyper-ventilation hypotension was largely preventedby overventilation on 5 per cent carbondioxide and that acutely raising the pH withsodium bicarbonate to levels attained duringhyperventilation on air did not cause a fall inpressure. They postulated that loss of carbondioxide caused the fall in pressure and thatthis effect of low carbon dioxide was a centralone since hyperventilation on air after destruc-tion of the spinal cord caused a small rise inpressure, supposedly due to the now unveiledperipheral effects of hypocapnia.
Standard physiology texts have acceptedDale and Evans' explanation that lowering ofthe arterial carbon dioxide tension tends tocause vasoconstriction through local effecton vessels, but this effect is not demonstrablein the intact animal because of vasodilatationinduced by the central effects of the low carbondioxide tension. If this explanation is correctfor man, one would expect the vasodilator
2 sec.
effects of a low carbon dioxide tension to belessened or absent in patients with a largeportion of the vasomotor nerves destroyed bydisease or blocked by suitable drugs. Thishypothesis has been tested on appropriatepatients.Patients with Postural Hypotension
Observations were made on three subjectscomplaining of postural fainting. Two subjectshad the classic syndrome of orthostatic hypo-tension with fixed pulse, impotence and im-paired sweating as described in the classicpaper of Bradbury and Eggleston.1'0 The thirdpatient was incapacitated 12 months afterbilateral lumbar sympathectomy. The disturb-ances in reflex regulation were so marked thatwe believed she might have had poor posturalregulation before operation. In each instance,at least partial paralysis of the vasomotornerves was present. The Valsalva maneuvercaused a major fall in arterial pressure andupon release of the strain, no overshoot inpressure occurred.
Hyperventilation on air in the recumbentposition caused a large fall in arterial pressurewith delayed recovery and no overshoot ofpressure upon resumption of normal respira-tion (fig. 3). The cardiac output and forearmblood flow tended to increase, the circulation
5% C02FIG. 3. Continuous intra-arterial pressure tracings in orthostatic hypotension during recumbent
hyperventilation on air and 5 per cent carbon dioxide. A mean blood pressure fall of 60 mm. Hg oc-curs during overbreathing on air with a delayed recovery after resumption of normal respiration.No change occurs if hyperventilation is conducted on 5 per cent carbon dioxide. In both instancesthe pulse rate is fixed. (Arrows indicate period of hyperventilation.)
92
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from
BURNUM, HICKAM AND McINTOSH
z
w +100
0
wLI.J 0 B |.P.
O Cordiac ForearmtE ~I ~~~Output FlowOL
a. -50a r'"0 Normal Overall Forearmt Orthostotic Hypotension Vasculor Resistance
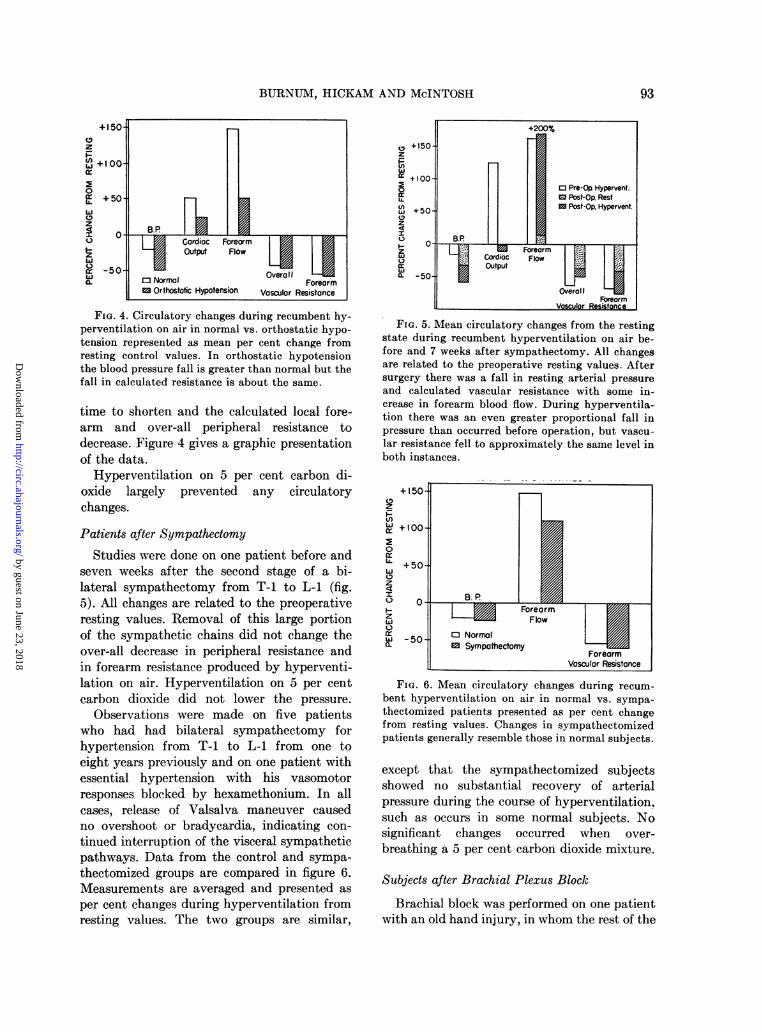
FroIG. 4. Circulatory changes during recumbent hy-perventilation on air in normal vs. orthostatic hypo-tension represented as mean per cent change fromresting control values. In orthostatic hypotensionthe blood pressure fall is greater than normal but thefall in calculated resistance is about the same.
time to shorten and the calculated local fore-arm and over-all peripheral resistance todecrease. Figure 4 gives a graphic presentationof the data.
Hyperventilation on 5 per cent carbon di-oxide largely prevented any circulatorychanges.Patients after Sympathectomy
Studies were done on one patient before andseven weeks after the second stage of a bi-lateral sympathectomy from T-l to L-l (fig.5). All changes are related to the preoperativeresting values. Removal of this large portionof the sympathetic chains did not change theover-all decrease in peripheral resistance andin forearm resistance produced by hyperventi-lation on air. Hyperventilation on 5 per centcarbon dioxide did not lower the pressure.
Observations were made on five patientswho had had bilateral sympathectomy forhypertension from T-l to L-l from one toeight years previously and on one patient withessential hypertension with his vasomotorresponses blocked by hexamethonium. In allcases, release of Valsalva maneuver causedno overshoot or bradycardia, indicating con-
tinued interruption of the visceral sympatheticpathways. Data from the control and sympa-thectomized groups are compared in figure 6.Measurements are averaged and presented as
per cent changes during hyperventilation fromresting values. The two groups are similar,
(9 +-IU-Vz_
a +1000: Pre-Op Hypervent.
L. E3 Post-Op. Rest) +50. I Post-Op. Hypervent.
B.P
ForeormwLu Cardioc Flow |LOQa -50
OverollFbreorm
Voscular Resistonce
FIG. 5. Mean circulatory changes from the restingstate during recumbent hyperventilation on air be-fore and 7 weeks after sympathectomy. All changesare related to the preoperative resting values. Aftersurgery there was a fall in resting arterial pressureand calculated vascular resistance with some in-crease in forearm blood flow. During hyperventila-tion there was an even greater proportional fall inpressure than occurred before operation, but vascu-lar resistance fell to approximately the same level inboth instances.
+15(9Z
I-
+5w
rr +10
0
Z
I
ZLu
0O
-5a.
FIG. 6. Mean circulatory changes during recum-bent hyperventilation on air in normal vs. sympa-thectomized patients presented as per cent changefrom resting values. Changes in sympathectomizedpatients generally resemble those in normal subjects.
except that the sympathectomized subjectsshowed no substantial recovery of arterialpressure during the course of hyperventilation,such as occurs in some normal subjects. Nosignificant changes occurred when over-
breathing a 5 per cent carbon dioxide mixture.
Subjects after Brachial Plexus Block
Brachial block was performed on one patientwith an old hand injury, in whom the rest of the
0- B.P . |S
0
-F0w
0 Normal0 Sympathectomy
ForeormVosculor Resistance
93
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

HYPOCAPNIA AND ARTERIAL BLOOD PRESSURE
extremity was normal, and on one normalsubject. In each case the effectiveness ofsympathetic block was indicated by the skinof the arm becoming hot, dry and flushed. Thearm was anesthetized and almost totally para-lyzed. In addition there was a Horner's syn-drome and phrenic paralysis on the blockedside in one case. The data are summarized intable 2. In both cases before block, hyper-ventilation on air produced the usual fall inblood pressure, rise in forearm blood flow andfall in forearm resistance. After block theresting forearm flow increased, but not to theextent of that produced by preblock hyper-ventilation. After block, during overbreathingthe blood pressure fell as usual, and the fore-arm flow increased and the local resistance fellto precisely the same levels reached beforeblock.
COMMENT
These data indicate that in man a loss ofcarbon dioxide from overbreathing has anover-all vasodilating effect. In normal subjectsthe fall in pressure is restricted by a combina-tion of an increase in cardiac output and theexpected effect of vasoconstriction in variousareas secondary to the fall in arterial pressure.These are the familiar homeostatic adjustmentswhich keep the arterial pressure at its sur-prisingly constant level. The importance ofthese adjustments for regulating the arterialpressure is well shown in the patients withsymptoms of postural hypotension and in thepatient with the recent extensive sympathec-tomy, who had greater and more prolongedfalls in pressure during hyperventilation thandid the normal subjects. The fact that a fallin carbon dioxide tension causes a marked fallin peripheral resistance in patients withdestruction of a large portion of the autonomicnervous system argues against a central effectand suggests that lowering carbon dioxidetension causes vasodilatation because of adirect effect on certain vessels. Brachial blocksestablished the fact that at least in the forearma lowering of carbon dioxide tension causedvasodilation by local action.
These data are not to be interpreted asmeaning that lowering of the arterial carbondioxide tension causes vasodilatation in all
TABLE 2.-Effect of Brachial Plexus Block
MeanMean Forearm Forearm
Subject State blood flow, resistance,mm.BPH cc./min. Mean BP/mm 00cc.g arnm forearm flow
A ControlRest 101 6.5 15.6Hypervent. 80 23.4 3.4
BlockRest 107 16.5 6.5Hypervent. 93 24.8 3.7
B ControlRest 86 6.3 13.7Hypervent. 76 20.0 3.6
BlockRest 89 13.2 6.7Hypervent. 82 22.0 3.7
organs. It is well known that in the cerebralvessels where vasomotor activity is low,acapnia causes a rise in resistance. It doesappear that the sum of all the changes inresistance add up to vasodilation and that ifthe nervous system is not working properlythis vasodilation is sufficient to cause a markedfall in arterial blood pressure.
Neither do these data shed any light on theeffects of high carbon dioxide tension on theblood vessels. The fact that a low carbondioxide tension causes a fall in peripheralresistance does not mean that sufficientlyhigh carbon dioxide tension might not havethe same effect. For example, both too muchpotassium and too little potassium causeparalysis.These data are convincing evidence that the
role of carbon dioxide tension in arterialpressure homeostasis needs further investiga-tion.
SUMMARY AND CONCLUSIONS
1. Hypocapnia, induced by voluntary hyper-ventilation, causes a substantial decrease inthe peripheral vascular resistance and bloodpressure of normal subjects, and a substantialincrease in forearm blood flow.
2. These effects of hypocapnia persist insubjects who have extensive loss of functionof the sympathetic nervous system, resultingfrom disease, surgery, or the use of autonomicblocking drugs.
3. Brachial block does not substantially
94
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

BURNUM, HICKAM AND McINTOSH
change the response to hypocapnia of forearmvascular resistance and forearm blood flow.
4. It is probable that vasodilatation pro-duced by hypocapnia in man is the net resultof direct action on the vessels in differentvascular areas and is not mediated by thenervous system.
SUMARIO EsPAmOLEn el hombre la hipocapnia inducida por la
hiperventilaci6n causa un decremento en pre-si6n arterial. La resistencia perif~rica calculadaesta disminuida, indicando una vasodilataci6nneta. La circulaci6n del antebrazo es marcada-mente aumentada, y la resistencia vascularmuy reducida. Personas con funci6n deterio-rada del sistema simpgtico continuan demos-trando estos efectos. El aumento en circula-ci6n del antebrazo no se evita por medio deun bloqueo braquial. Estos resultados sugierenque la hipocapnia actua directamente en losvasos para producir una vasodilataci6n netay un decremento en presi6n arterial, y queeste efecto no es mediado por el sistema ner-vioso como se habia supuesto.
REFERENCES1 BEST, C. H., AND TAYLOR, N. B.: The Physio-
logical Basis of Medical Practice, ed. 5. Balti-more, Williams & Wilkins, 1950.
2HAMILTON, W. F., MOORE, J. W., KINSMAN, V.M., AND SPURLING, R. G.: Studies in circula-tion. IV. Further analysis of the injectionmethod and of changes in hemodynamics underphysiological and pathological conditions. Am.J. Physiol. 99: 534, 1931, 1932.
3PETERS, J. P., AND VAN SLYKE, D. D.: Quantita-tive Clinical Chemistry. Vol. II. Methods.Baltimore, Williams & Wilkins, 1932.
4 VAN SLYKE, D. D., AND SENDROY, J., JR.: Studiesof gas and electrolyte equilibria in blood. XV.Line charts for graphic calculations by theHenderson-Hasselbalch equation, and for cal-culating plasma carbon dioxide content fromwhole blood content. J. Biol. Chem. 79: 781,1928.
5GRANT, R. T., AND BRUCE PEARSON, R. S.: Theblood circulation in the human limb; observa-tions on the differences between the proximaland distal parts and remarks on the regulationof body temperature. Clin. Sc. 3: 119, 1938.
6 CLARKE, R. S. J.: The effect of voluntary over-breathing on the blood flow through the humanforearm. J. Physiol. 118: 537, 1952.
7HENDERSON, Y.: Acapnia and shock. I. Carbondioxide as a factor in the regulation of the heartrate. Am. J. Physiol. 21: 126, 1908.
8 ROOME, N. W.: The cardiac output in hyperven-tilation by external alternating pressure. Am.J. Physiol. 104: 142, 1933.
9 DALE, H. H., AND EVANS, C. L.: Effects on thecirculation of changes in the carbon dioxidecontent of the blood. J. Physiol. 56: 125, 1922.
10 BRADBURY, S., AND EGGLESTON, C.: Postural hy-potension; a report of three cases. Am. Heart.J. 1: 73, 1925.
95
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from

J. F. BURNUM, J. B. HICKAM and H. D. MCINTOSHThe Effect of Hypocapnia on Arterial Blood Pressure
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1954 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.9.1.89
1954;9:89-95Circulation.
http://circ.ahajournals.org/content/9/1/89the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document.
Permissions and Rights Question and Answer Further information about this process is available in therequested is located, click Request Permissions in the middle column of the Web page under Services.the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 23, 2018http://circ.ahajournals.org/
Dow
nloaded from