the effects of stenting and endothelial denudation on … · the effects of stenting and...
TRANSCRIPT

The effects of stenting and endothelial denudationon aneurysm and branch occlusion in experimentalaneurysm modelsTim Darsaut, MD, Fatiha Bouzeghrane, PhD, Igor Salazkin, MD, Sophie Lerouge, PhD,Gilles Soulez, MD, MSc, Guylaine Gevry, BSc, and Jean Raymond, MD, Montreal, Quebec, Canada
Background: Stents are increasingly used in the endovascular treatment of intracranial aneurysms. We studied the effectsof stenting and endothelial denudation on aneurysm and branch vessel occlusion.Methods: Bilateral lingual bifurcation venous pouch aneurysms were created in eight dogs, surgically scraping theaneurysmal endothelial lining on one side. Both arteries were immediately stented using balloon-expandable stents. Infour other dogs, a wide-neck carotid bifurcation aneurysm was created, with the vein pouch denuded or not (n � 2 each),followed by immediate stenting. Results were compared using angiography and pathology at 10 days (n � 2), 10 (n � 8),and 20 weeks (n � 2). Branch occlusion between initial and final angiograms was recorded. Pathological evaluation ofaneurysms was studied, with attention to neointima formation at the aneurysm ostium and around branch vessel origins.Results: All stented and denuded lingual aneurysms were obliterated compared with two of eight lingual aneurysms thatwere stented alone (P � .007). None of the carotid bifurcation aneurysms became obliterated (0/4), but denudedaneurysms showed partial thrombosis (2/2). Of 68 total stent-covered branches, 5 (7%) were occluded and 17 (27%) hadaltered angiographic flow.Conclusions: Stenting led to suboptimal results in the presence of an intact endothelial layer. Endothelial denudation canpromote aneurysm occlusion when combined with stenting. (J Vasc Surg 2007;45:1228-35.)
Clinical relevance. Following endovascular treatment, cerebral aneurysms are prone to recurrences. Stents are increasinglydeployed as part of the treatment of intracranial aneurysms, but pose risk to perforating vessels crossed by the stent. Themechanism whereby some aneurysms become permanently occluded while other aneurysms recur remains unknown. Thisstudy tests the effects of stenting with and without endothelial denudation on rates of aneurysm healing and branch vesselocclusion. Through further understanding of the factors and forces involved in the formation of durable treatment
results, we hope to develop strategies that will safely decrease the recurrence rate of endovascularly treated aneurysms.Endovascular therapy of aneurysms can improve theoutcome of patients treated after subarachnoid hemor-rhage (SAH) compared with surgical clipping.1 However,this treatment modality is associated with recurrences and aconcern for future hemorrhage.2 Attempts to decrease therecurrence rate have led to several technical and bioengi-neering innovations.3-7 One strategy involves treating theaneurysm as a symptom of the diseased parent vessel, withdeployment of a stent to bridge the aneurysm ostium.Currently, stenting is often combined with coil occlusion,hopefully to modify intra-aneurysmal hemodynamics, pro-voke aneurysm thrombosis, re-establish normal blood flowpatterns within the parent vessel, and perhaps buffer thehemodynamic forces implicated in recurrences.8-12 In ad-dition, the stent may provide a supportive scaffold forneointima deposition at the junction of the parent vesseland aneurysm neck. The major concern regarding thistreatment strategy is the risk of stent-related occlusion ofbranch or perforating vessels and the excessive formation of
From the CHUM Notre-Dame Hospital.Competition of interest: none.Correspondence: Jean Raymond, MD, CHUM Notre-Dame Hospital, Inter-
ventional Neuroradiology, 1560 Sherbrooke East, Suite M-8203, Montreal,Quebec H2L 4M1 Canada (e-mail: [email protected]).
0741-5214/$32.00Copyright © 2007 by The Society for Vascular Surgery.
doi:10.1016/j.jvs.2007.02.0601228
neointima with secondary parent vessel stenosis.13 Further-more, the use of stents alone, particularly if they are de-signed to minimally affect branches and perforators, maynot sufficiently alter hemodynamics to initiate thrombosisand lead to aneurysm healing.14
The defining boundary of the endoluminal space is theendothelial lining, which is comprised of a single layer ofspecialized cells with antithrombotic and thrombolyticproperties important for the maintenance of vessel pa-tency.15 The endothelial lining is responsible for the persis-tence of experimentally constructed aneurysms, for residualflow within the neck of incompletely treated aneurysms andis involved in recanalization following arterial occlu-sion.16,17 Endothelial denudation could be considered as atherapeutic strategy to improve the results of endovasculartreatment of aneurysms.17 However, endothelial denuda-tion in the continued presence of blood flow leads tore-endothelialization.16,18,19 After denudation, hemody-namic changes provoked by stent struts may alter re-endo-thelialization and promote aneurysm thrombosis, organi-zation, and healing in such a fashion as to redefine theboundary of the endoluminal space to one defined by thestent, thereby excluding the aneurysm. The stent may alsolead to increased neointima formation at the site crucial foraneurysm obliteration, at the parent vessel-aneurysm neck
interface.
JOURNAL OF VASCULAR SURGERYVolume 45, Number 6 Darsaut et al 1229
The present work sought to examine the relationship ofstenting and endothelial denudation to aneurysm andbranch vessel occlusion, as assessed by angiography andpathology, and to explore the potential value of a novelapproach combining both strategies to improve results ofendovascular treatment.
METHODS
Protocols were approved by the Institutional AnimalCare Committee in accordance with the guidelines of theCanadian Council on Animal Care. All procedures wereperformed under general anesthesia. Twelve beagles weigh-ing 8 to 12 kg were sedated with acepromazine (0.1 mg/kg), glycopyrrolate (0.01 mg/kg), and butorphanol (0.1mg/kg), and anesthetized with intravenous thiopental (15mg/kg). Animals were ventilated artificially and main-tained under anesthesia with 2% isoflurane. Postoperativeanalgesia was provided for three days with a 50 �g fentanylpatch.
Surgical techniques. The lingual aneurysm20 and ca-rotid bifurcation aneurysm models21,22 bear resemblanceto human intracranial aneurysms in that they are sur-rounded by branch vessels and occur at vessel bifurcations,respectively. They certainly differ from spontaneous intra-cranial aneurysms but have repeatedly been shown to helpunderstand healing or recurrences after endovascular treat-ment.20-22 Briefly, for the lingual model (n � 8 animals or16 aneurysms), the region of the lingual artery was accessedthrough a midline incision. A portion of the left externaljugular vein was harvested and divided in half to formvenous pouches of equal size. Prior to surgical creation ofthe aneurysm, one of the vein segments was temporarilyinverted and scraped with a scalpel blade to cause endothe-lial denudation, as previously described.17 To evaluate theextent of denudation and damage to the jugular vein seg-ments with this technique, a portion of jugular vein of fourother dogs was harvested and scraped in a similar fashion,fixed in formalin, and processed for factor VIII immuno-staining, Verhoeff, and hematoxylin-phloxine-saffron(HPS) staining. Control non-denuded vein was also har-vested for comparison.
On each side, the lingual nerve was identified andmobilized, and temporary aneurysm clips were applied tobranch vessels. A 4 mm arteriotomy was created on theexternal carotid artery, proximal to the site of the lingualartery origin, which presents a modification from the dis-tally located aneurysm in the originally described model.20
End-to-side anastomoses of the vein segment to the arterywere fashioned, with normal vein on one side and denudedvein on the other. The suture line was sealed with running7.0 Prolene suture, and the aneurysm pouches sealed withhemostatic clips, creating aneurysms 7.1 (�/� 1.3) x 5.7(�/� 1.1) mm with 4.3 (�/� 0.7) mm necks.
For the carotid bifurcation model (n � 4), through amidline incision, both carotid arteries were exposed andtemporarily clipped with aneurysm clips. The left carotidartery was tied off at the origin, mobilized under the
trachea, and anastomosed to the contralateral carotid ar-tery.20,21 A portion of harvested external jugular vein,either normal or denuded, had two slits cut longitudinallyon one side, and was anastomosed to the junction of thetwo carotid arteries, forming wide-neck (7.8 �/� 0.5 mm)bifurcation aneurysms measuring 17.0 (�/� 2.6) x 9.0(�/� 0.8) mm.
Endovascular techniques. The endovascular proce-dure was performed immediately following closure of thesurgical site. Transfemoral access was performed, and fol-lowing angiography, balloon-expandable stents (BX Veloc-ity, Cordis, Miami, Fla for lingual aneurysms; HerculinkPlus, Guidant, Santa Clara, Calif for carotid bifurcationaneurysms) lengths 18 to 28 mm and diameters 3.5 to 4.5mm were deployed bilaterally to bridge the aneurysm neckand lingual artery, or bridging a portion of the aneurysmneck and the origin of the reimplanted left carotid artery forcarotid bifurcations. Stent diameters were chosen followingestimation of the caliber of the parent vessel by digitalangiography, assuring stability by using a stent diameter 0.5mm above vessel diameter. Stents were deployed to nomi-nal diameters using tables provided in the manufacturer’sinstructions (8 atm). Two identical stents were used forpaired aneurysms in each animal. The lengths of stentschosen were variable from one animal to the other; ourgoals were to ensure that the stent bridged the aneurysmostium with a 5 mm “landing zone” on either side todecrease the chance of stent migration. Normotension wasmaintained throughout the endovascular procedure by ti-trating inhalational agents and fluid administration, but wasnot manipulated pharmacologically.
Angiograms were performed immediately followingstent deployment, and at 10 days (n � 2), 10 weeks (n � 8),and 20 weeks (n � 2) poststenting, but interpretation wasperformed in a non-blind fashion. Animals did not receiveany antiplatelet agents or anticoagulants.
Angiographic results were compared using Fisher exacttest, where P � .05 was required for significance. Aneu-rysms were scored in a binary fashion, where a score of 0indicated complete obliteration, and a score of 1 indicatedresidual or recurrent aneurysm. The number of branchescovered by the stent, which varied depending on the lengthof the stent and regional blood vessel anatomy, wascounted on the initial angiogram and compared with thefinal angiogram to determine the incidence of branch oc-clusion. The incidence of hemodynamic alterations, such assluggish blood flow though a branch vessel was also re-corded. The incidence and extent of angiographic in-stentstenosis was determined by measuring the ratio of referencevessel to stent lumen on the same angiogram frame. Signif-icant in-stent stenosis was defined as a reduction of luminaldiameter of greater than 50%.23
Pathology. Animals were sacrificed at 10 days (n � 2with lingual), 10 weeks (n � 4 with lingual and four carotidbifurcation) and 20 weeks (two with lingual aneurysms).Pathological specimens were prepared by cutting the stent/artery complex longitudinally, followed by “en face” micro-photography of the aneurysm and branch vessel ostia,
assessing the extent of neointimal closure of the neck by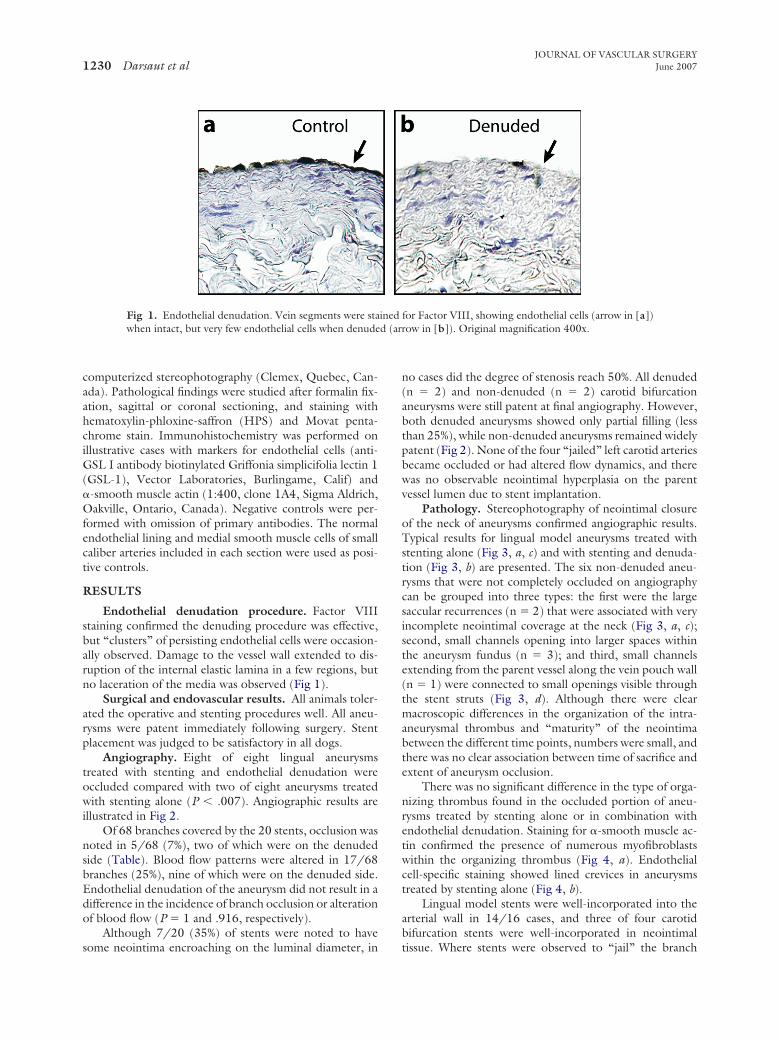
d (ar
JOURNAL OF VASCULAR SURGERYJune 20071230 Darsaut et al
computerized stereophotography (Clemex, Quebec, Can-ada). Pathological findings were studied after formalin fix-ation, sagittal or coronal sectioning, and staining withhematoxylin-phloxine-saffron (HPS) and Movat penta-chrome stain. Immunohistochemistry was performed onillustrative cases with markers for endothelial cells (anti-GSL I antibody biotinylated Griffonia simplicifolia lectin 1(GSL-1), Vector Laboratories, Burlingame, Calif) and�-smooth muscle actin (1:400, clone 1A4, Sigma Aldrich,Oakville, Ontario, Canada). Negative controls were per-formed with omission of primary antibodies. The normalendothelial lining and medial smooth muscle cells of smallcaliber arteries included in each section were used as posi-tive controls.
RESULTS
Endothelial denudation procedure. Factor VIIIstaining confirmed the denuding procedure was effective,but “clusters” of persisting endothelial cells were occasion-ally observed. Damage to the vessel wall extended to dis-ruption of the internal elastic lamina in a few regions, butno laceration of the media was observed (Fig 1).
Surgical and endovascular results. All animals toler-ated the operative and stenting procedures well. All aneu-rysms were patent immediately following surgery. Stentplacement was judged to be satisfactory in all dogs.
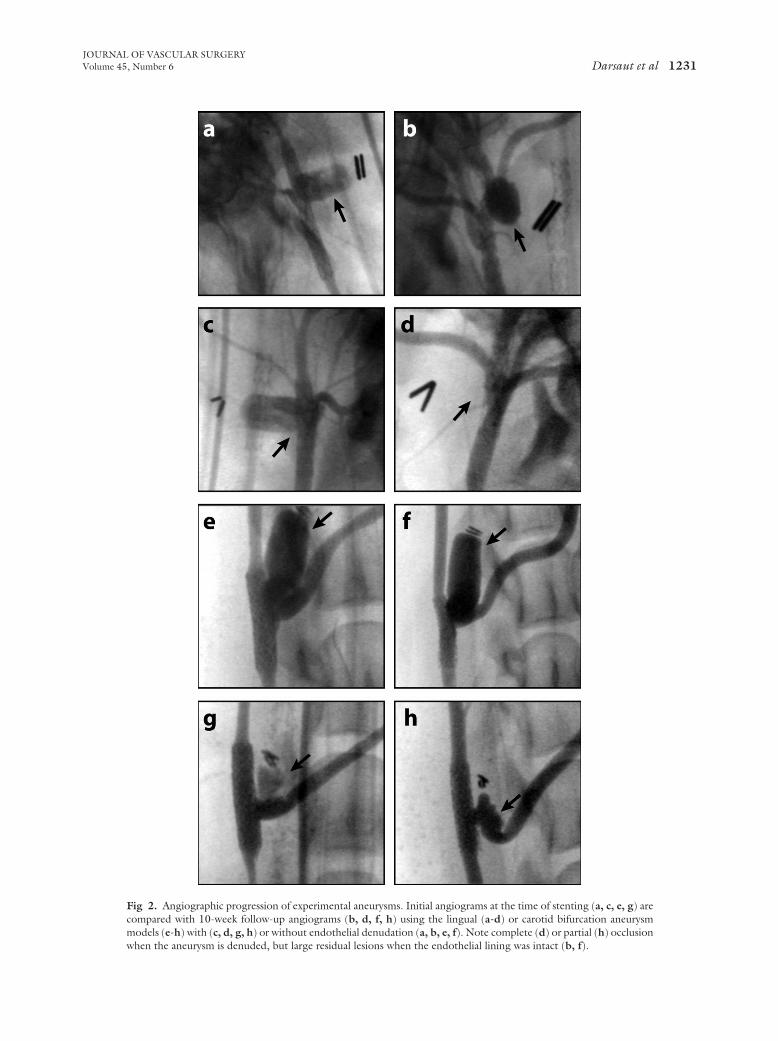
Angiography. Eight of eight lingual aneurysmstreated with stenting and endothelial denudation wereoccluded compared with two of eight aneurysms treatedwith stenting alone (P � .007). Angiographic results areillustrated in Fig 2.
Of 68 branches covered by the 20 stents, occlusion wasnoted in 5/68 (7%), two of which were on the denudedside (Table). Blood flow patterns were altered in 17/68branches (25%), nine of which were on the denuded side.Endothelial denudation of the aneurysm did not result in adifference in the incidence of branch occlusion or alterationof blood flow (P � 1 and .916, respectively).
Although 7/20 (35%) of stents were noted to have
Fig 1. Endothelial denudation. Vein segments were stawhen intact, but very few endothelial cells when denude
some neointima encroaching on the luminal diameter, in
no cases did the degree of stenosis reach 50%. All denuded(n � 2) and non-denuded (n � 2) carotid bifurcationaneurysms were still patent at final angiography. However,both denuded aneurysms showed only partial filling (lessthan 25%), while non-denuded aneurysms remained widelypatent (Fig 2). None of the four “jailed” left carotid arteriesbecame occluded or had altered flow dynamics, and therewas no observable neointimal hyperplasia on the parentvessel lumen due to stent implantation.
Pathology. Stereophotography of neointimal closureof the neck of aneurysms confirmed angiographic results.Typical results for lingual model aneurysms treated withstenting alone (Fig 3, a, c) and with stenting and denuda-tion (Fig 3, b) are presented. The six non-denuded aneu-rysms that were not completely occluded on angiographycan be grouped into three types: the first were the largesaccular recurrences (n � 2) that were associated with veryincomplete neointimal coverage at the neck (Fig 3, a, c);second, small channels opening into larger spaces withinthe aneurysm fundus (n � 3); and third, small channelsextending from the parent vessel along the vein pouch wall(n � 1) were connected to small openings visible throughthe stent struts (Fig 3, d). Although there were clearmacroscopic differences in the organization of the intra-aneurysmal thrombus and “maturity” of the neointimabetween the different time points, numbers were small, andthere was no clear association between time of sacrifice andextent of aneurysm occlusion.
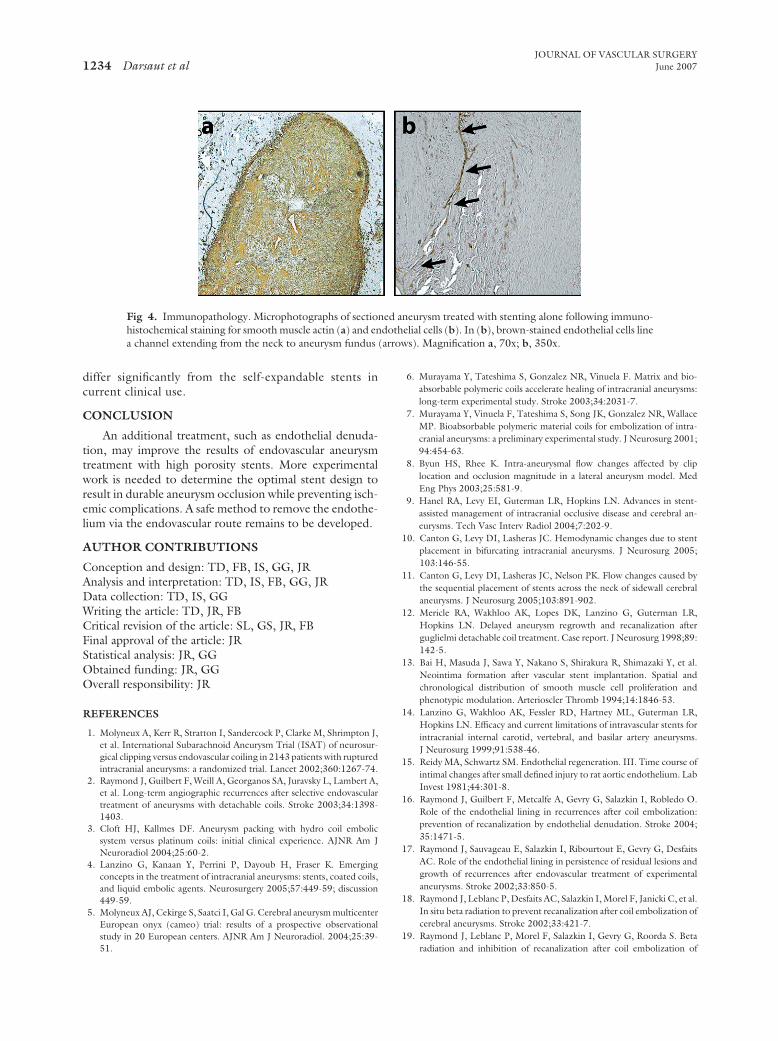
There was no significant difference in the type of orga-nizing thrombus found in the occluded portion of aneu-rysms treated by stenting alone or in combination withendothelial denudation. Staining for �-smooth muscle ac-tin confirmed the presence of numerous myofibroblastswithin the organizing thrombus (Fig 4, a). Endothelialcell-specific staining showed lined crevices in aneurysmstreated by stenting alone (Fig 4, b).
Lingual model stents were well-incorporated into thearterial wall in 14/16 cases, and three of four carotidbifurcation stents were well-incorporated in neointimal
for Factor VIII, showing endothelial cells (arrow in [a])row in [b]). Original magnification 400x.
ined
tissue. Where stents were observed to “jail” the branch
JOURNAL OF VASCULAR SURGERYVolume 45, Number 6 Darsaut et al 1231
Fig 2. Angiographic progression of experimental aneurysms. Initial angiograms at the time of stenting (a, c, e, g) arecompared with 10-week follow-up angiograms (b, d, f, h) using the lingual (a-d) or carotid bifurcation aneurysmmodels (e-h) with (c, d, g, h) or without endothelial denudation (a, b, e, f). Note complete (d) or partial (h) occlusion
when the aneurysm is denuded, but large residual lesions when the endothelial lining was intact (b, f).
JOURNAL OF VASCULAR SURGERYJune 20071232 Darsaut et al
vessel origins, in cases where the ostium was patent, one oftwo patterns of neointima deposition was observed. Some-times the stent struts were devoid of neointima, while inothers, the neointima covered portions of the stent struts,with the ostium patent underneath. In some cases, theneointima was seen to have grown over and occluded thebranch vessel origin (Fig 3, e, f).
Both non-denuded wide-necked carotid bifurcationaneurysms remained widely patent, but aneurysms partiallyoccluded with organized clot were observed in both casestreated with stenting and denudation (Fig 3, g).
DISCUSSION
The use of stenting alone was ineffective at totallyoccluding both lingual and carotid bifurcation aneurysms,at least with the devices we used. Although blood flowpatterns were sufficiently modified to provoke thrombosisand clot organization within the lingual aneurysms, the useof the stent alone did not produce a solid organized struc-ture completely obliterating the aneurysm. When the en-dothelial lining was preserved, small endothelial-lined crev-ices, which have been associated with recurrences16,17 wereobserved in most cases. These results confirm our previousexperiments using radioactive or nonradioactive stents inthe treatment of experimental aneurysms.19 However,when stenting was combined with endothelial denudation,occlusions were more often complete, and aneurysm morecompletely filled with organized tissues. Removal of theendothelial lining may incite a more vigorous thromboticreaction by exposing a collagenous surface. Alternatively,the removal of endothelial signaling may limit or preventthe formation of recurrent crevices.16,17 In the future,endothelial denudation could theoretically be accom-plished with mechanical, physical, or chemical means. Al-though denudation removes parietal endothelial cells, cir-culating endothelial progenitor cells have been described,and likely participate in the repopulation of the maturingthrombus.24
Denudation of the endothelial lining may favor throm-bosis but in the presence of unaltered blood flow, it is mostcommonly followed by re-endothelialization.16,17 Thecombination of stenting and denudation led to improvedresults in the lingual aneurysm model. Attempts to replicatethe results of the lingual model in high-flow wide-neck
Table I. Angiographic results: Stent-related branchocclusion and altered flow dynamic rates with stentingalone and with stenting and denudation
Treatment
Stenting aloneStenting �denudation P value
Occluded aneurysms 2/8 (25%) 8/8 (100%) .007Occluded branches 2/32 (9%) 3/36 (7%) 1Altered blood flow 9/32 (26%) 8/36 (27%) .917
bifurcation aneurysms were unsuccessful. Notably, the
stent does not completely cover the aneurysm ostium inthis model, and the thrombus is exposed to greater hemo-dynamic forces. These conditions seem unfavorable for theformation and organization of intra-aneurysmal clot. An-eurysms such as these may require new devices such asbifurcated stents with asymmetrical cells or different thera-peutic strategies for definitive treatment.
One difficulty with the use of intracranial stents arisesfrom the conflicting goals of provoking aneurysm throm-bosis while sparing adjacent branches. Ideally, the por-tion of the stent covering the aneurysm would be of lowporosity, with minimal blood flow into the aneurysm,with the remainder of the stent comprised of high po-rosity stent cells. Smaller pore sizes may protect theorganizing clot from hemodynamic forces and promoteneointimal proliferation up to the boundary created bythe stent, permitting greater neointimal formation at thejunction of the parent vessel and aneurysm neck. High-porosity stents such as those currently available for intra-cranial use are more likely to preserve perforating vessels,but require an additional treatment, usually coiling, toocclude the aneurysm.
The varying observations at the level of the stentstruts crossing branch vessel ostia may represent threedifferent pathological outcomes: (1) branch vesselthrombosis without recanalization, with dense neointi-mal coverage; (2) branch vessel thrombosis with recana-lization, with nonuniform tissue strands covering thestent struts; and (3) branch vessel remains patent, withbare stent struts crossing a vessel origin. In this series, theuse of stents led to branch occlusion in 7.3% of cases, andendothelial denudation of the aneurysm did not worsenthis rate. However, stent-related blood flow alterationswere observed in 25% of cases, which raises concernsabout stent-related tissue ischemia or infarction. Thefinding of exposed portions of the stent crossing vesselostia further stresses the importance of compliance withlong-term platelet therapy following stenting.
Although in-stent stenosis was not observed with thestents we used, this occurrence is known to vary withtime, and clinical reports of this complication mandatecontinued surveillance until the natural history of intra-cranial stenting is better delineated.25
Experimental limitations. Insights gained regard-ing the effects of stents on aneurysm and branch occlu-sion may provide experimental data to guide treatingphysicians regarding the now-common clinical practiceof deploying stents to treat intracranial aneurysms.
The advantage of the lingual aneurysm model is thepresence of multiple branch vessels that resemble manyintracranial aneurysms. Aneurysm flow velocities were notmeasured in this study, and differences in hemodynamicforces experienced by these aneurysms may be an importantfactor limiting generalization of our results. Because weused a surgical denuding technique, endovascular treat-ment has to be performed acutely, before a maturation
period to prevent re-endothelialization before stenting.
JOURNAL OF VASCULAR SURGERYVolume 45, Number 6 Darsaut et al 1233
Venous pouches certainly differ from naturally occur-ring aneurysms, in their cellular composition but perhapsalso in their biological reaction. The location of the exper-imental aneurysm within the soft tissues of the canine neckalso represents a different microenvironment comparedwith the CSF space.
Other limitations include the small number of ani-
Fig 3. Macroscopic photography. Typical results for anshown as “en-face” view of aneurysm ostia, (a), and sagittlingual artery ostium (L) in (c) and the patent channel co(arrow in d). “En-face” view of completely occluded anein (b) for comparison. Neointima formation over branchit spared the ostium of the lingual artery in (f). Partiendothelial denudation and stenting is shown in (g) (CCT, organized thrombus; R, residual aneurysm).
mals used, the absence of a control group with denuded
aneurysms without stents in aneurysms of this size andon parent vessels of this caliber, and the absence of along-term follow-up group. The animals in this studywere not treated with antiplatelet agents, as is usuallydone in the clinical setting, due to the more frequentlocal femoral complications that have previously beenencountered with such a treatment in this small animal
ms treated with stenting alone at 10 weeks (a, c, d) aretions through aneurysm remnant (c, d). Note the patentnicating with an open space within the aneurysm fundus
ostium treated with stenting and denudation is shownls is shown to be almost completely occlusive in (e) whileccluded wide-neck carotid bifurcation aneurysm aftermon carotid; LC and RC, left and right carotid arteries;
eurysal secmmuurysmvesseally o, com
model. Finally, the stents used in these experiments
(arrow
JOURNAL OF VASCULAR SURGERYJune 20071234 Darsaut et al
differ significantly from the self-expandable stents incurrent clinical use.
CONCLUSION
An additional treatment, such as endothelial denuda-tion, may improve the results of endovascular aneurysmtreatment with high porosity stents. More experimentalwork is needed to determine the optimal stent design toresult in durable aneurysm occlusion while preventing isch-emic complications. A safe method to remove the endothe-lium via the endovascular route remains to be developed.
AUTHOR CONTRIBUTIONS
Conception and design: TD, FB, IS, GG, JRAnalysis and interpretation: TD, IS, FB, GG, JRData collection: TD, IS, GGWriting the article: TD, JR, FBCritical revision of the article: SL, GS, JR, FBFinal approval of the article: JRStatistical analysis: JR, GGObtained funding: JR, GGOverall responsibility: JR
REFERENCES
1. Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J,et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosur-gical clipping versus endovascular coiling in 2143 patients with rupturedintracranial aneurysms: a randomized trial. Lancet 2002;360:1267-74.
2. Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A,et al. Long-term angiographic recurrences after selective endovasculartreatment of aneurysms with detachable coils. Stroke 2003;34:1398-1403.
3. Cloft HJ, Kallmes DF. Aneurysm packing with hydro coil embolicsystem versus platinum coils: initial clinical experience. AJNR Am JNeuroradiol 2004;25:60-2.
4. Lanzino G, Kanaan Y, Perrini P, Dayoub H, Fraser K. Emergingconcepts in the treatment of intracranial aneurysms: stents, coated coils,and liquid embolic agents. Neurosurgery 2005;57:449-59; discussion449-59.
5. Molyneux AJ, Cekirge S, Saatci I, Gal G. Cerebral aneurysm multicenterEuropean onyx (cameo) trial: results of a prospective observationalstudy in 20 European centers. AJNR Am J Neuroradiol. 2004;25:39-
Fig 4. Immunopathology. Microphotographs of sectiohistochemical staining for smooth muscle actin (a) and ena channel extending from the neck to aneurysm fundus
51.
6. Murayama Y, Tateshima S, Gonzalez NR, Vinuela F. Matrix and bio-absorbable polymeric coils accelerate healing of intracranial aneurysms:long-term experimental study. Stroke 2003;34:2031-7.
7. Murayama Y, Vinuela F, Tateshima S, Song JK, Gonzalez NR, WallaceMP. Bioabsorbable polymeric material coils for embolization of intra-cranial aneurysms: a preliminary experimental study. J Neurosurg 2001;94:454-63.
8. Byun HS, Rhee K. Intra-aneurysmal flow changes affected by cliplocation and occlusion magnitude in a lateral aneurysm model. MedEng Phys 2003;25:581-9.
9. Hanel RA, Levy EI, Guterman LR, Hopkins LN. Advances in stent-assisted management of intracranial occlusive disease and cerebral an-eurysms. Tech Vasc Interv Radiol 2004;7:202-9.
10. Canton G, Levy DI, Lasheras JC. Hemodynamic changes due to stentplacement in bifurcating intracranial aneurysms. J Neurosurg 2005;103:146-55.
11. Canton G, Levy DI, Lasheras JC, Nelson PK. Flow changes caused bythe sequential placement of stents across the neck of sidewall cerebralaneurysms. J Neurosurg 2005;103:891-902.
12. Mericle RA, Wakhloo AK, Lopes DK, Lanzino G, Guterman LR,Hopkins LN. Delayed aneurysm regrowth and recanalization afterguglielmi detachable coil treatment. Case report. J Neurosurg 1998;89:142-5.
13. Bai H, Masuda J, Sawa Y, Nakano S, Shirakura R, Shimazaki Y, et al.Neointima formation after vascular stent implantation. Spatial andchronological distribution of smooth muscle cell proliferation andphenotypic modulation. Arterioscler Thromb 1994;14:1846-53.
14. Lanzino G, Wakhloo AK, Fessler RD, Hartney ML, Guterman LR,Hopkins LN. Efficacy and current limitations of intravascular stents forintracranial internal carotid, vertebral, and basilar artery aneurysms.J Neurosurg 1999;91:538-46.
15. Reidy MA, Schwartz SM. Endothelial regeneration. III. Time course ofintimal changes after small defined injury to rat aortic endothelium. LabInvest 1981;44:301-8.
16. Raymond J, Guilbert F, Metcalfe A, Gevry G, Salazkin I, Robledo O.Role of the endothelial lining in recurrences after coil embolization:prevention of recanalization by endothelial denudation. Stroke 2004;35:1471-5.
17. Raymond J, Sauvageau E, Salazkin I, Ribourtout E, Gevry G, DesfaitsAC. Role of the endothelial lining in persistence of residual lesions andgrowth of recurrences after endovascular treatment of experimentalaneurysms. Stroke 2002;33:850-5.
18. Raymond J, Leblanc P, Desfaits AC, Salazkin I, Morel F, Janicki C, et al.In situ beta radiation to prevent recanalization after coil embolization ofcerebral aneurysms. Stroke 2002;33:421-7.
19. Raymond J, Leblanc P, Morel F, Salazkin I, Gevry G, Roorda S. Beta
neurysm treated with stenting alone following immuno-elial cells (b). In (b), brown-stained endothelial cells lines). Magnification a, 70x; b, 350x.
ned adoth
radiation and inhibition of recanalization after coil embolization of

JOURNAL OF VASCULAR SURGERYVolume 45, Number 6 Darsaut et al 1235
canine arteries and experimental aneurysms: how should radiation bedelivered? Stroke 2003;34:1262-8.
20. Raymond J, Salazkin I, Metcalfe A, Robledo O, Gevry G, Roy D, et al.Lingual artery bifurcation aneurysms for training and evaluation ofneurovascular devices. AJNR Am J Neuroradiol 2004;25:1387-90.
21. Raymond J, Salazkin I, Metcalfe A, Guilbert F, Weill A, Roy D.High-concentration ethylene-vinyl alcohol copolymer and endovascu-lar treatment of experimental aneurysms: feasibility of embolizationwithout protection devices at the neck. AJNR Am J Neuroradiol2003;24:1778-84.
22. Raymond J, Salazkin I, Georganos S, Guilbert F, Desfaits AC, Gevry G,et al. Endovascular treatment of experimental wide neck aneurysms:comparison of results using coils or cyanoacrylate with the assistance ofan aneurysm neck bridge device. AJNR Am J Neuroradiol 2002;23:
1710-16.23. Wakhloo AK, Tio FO, Lieber BB, Schellhammer F, Graf M, HopkinsLN. Self-expanding nitinol stents in canine vertebral arteries: hemody-namics and tissue response. AJNR Am J Neuroradiol 1995;16:1043-51.
24. Moldovan NI, Asahara T. Role of blood mononuclear cells in recanali-zation and vascularization of thrombi: past, present, and future. TrendsCardiovasc Med 2003;13:265-9.
25. Fiorella D, Albuquerque FC, Deshmukh VR, McDougall CG. In-stentstenosis as a delayed complication of neuroform stent-supported coilembolization of an incidental carotid terminus aneurysm. AJNR Am JNeuroradiol 2004;25:1764-7.
Submitted Dec 11, 2006; accepted Feb 18, 2007.