the elbow fracture
TRANSCRIPT


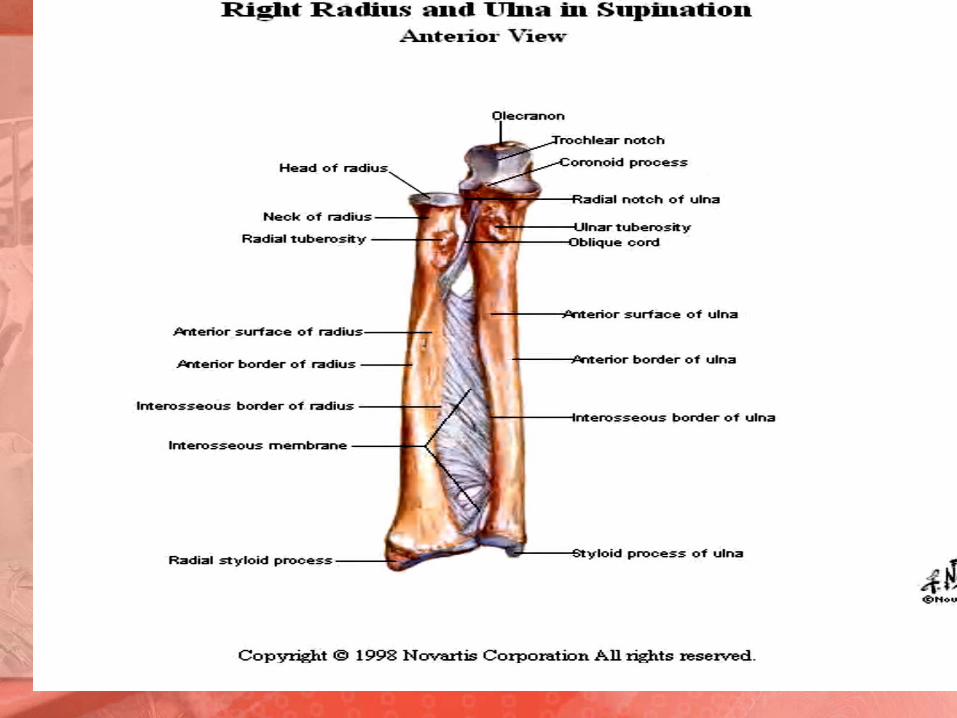
Anatomy of the ElbowIs a synovial hinge joint formed by articulation between the humerus , radius
and ulna.
TrochlearCapitulum
Head of radius Trochlear notch of ulna
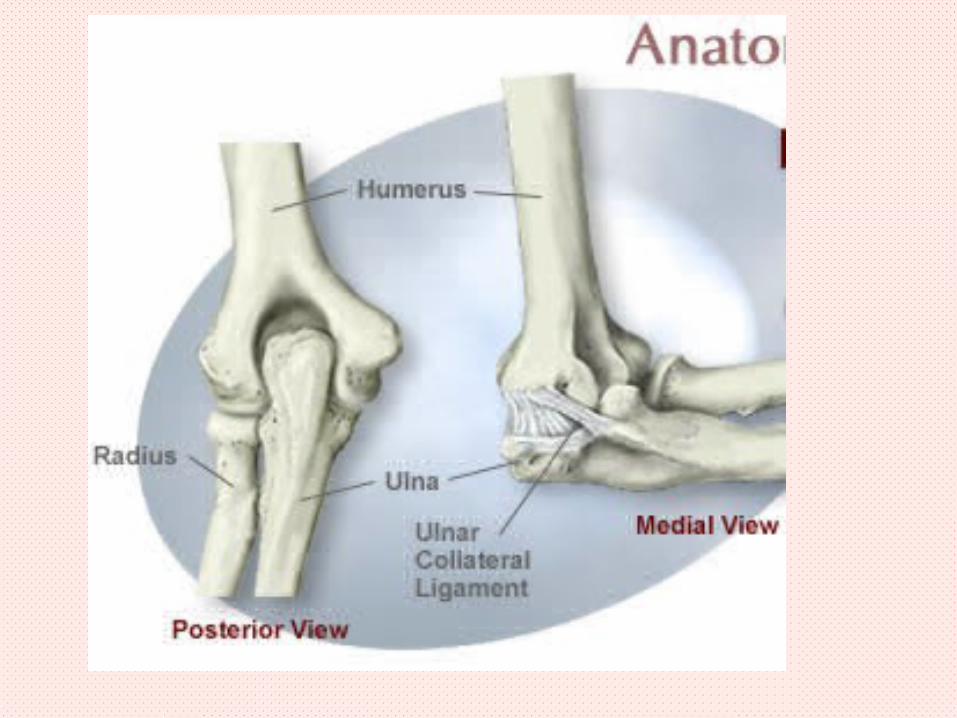

Elbow joint stability
Due to the shape and fit of bones that make joint and the surrounding tissue as
capsular and collateral ligaments:
1 -radial collateral lig.
2 -anular lig. Of radius
3 -ulnar collateral lig.4- transverse lig.
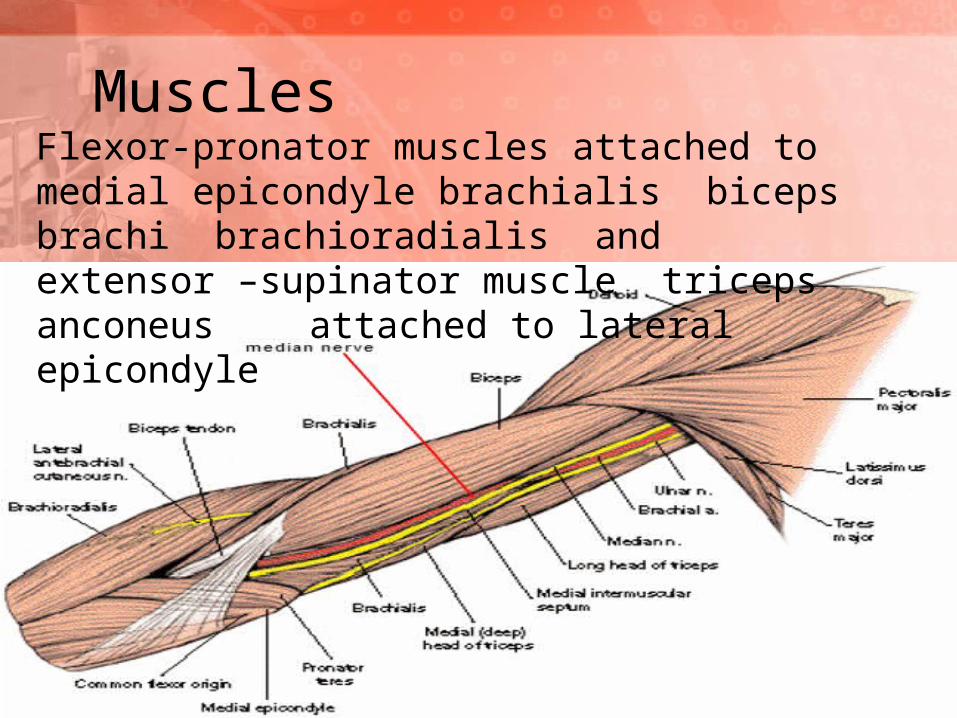
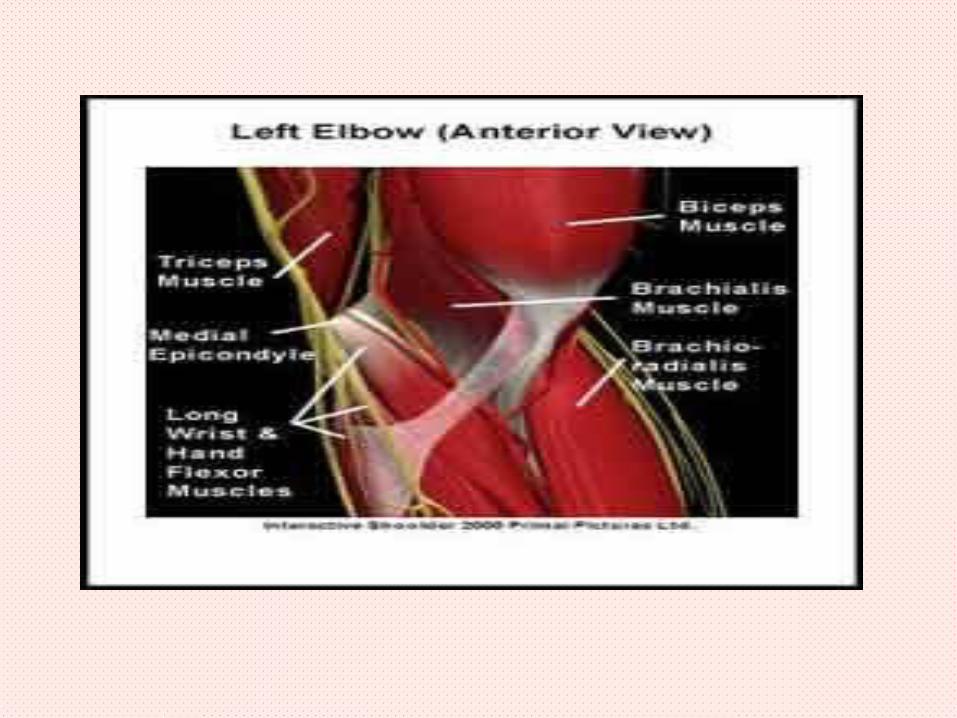
Muscles Flexor-pronator muscles attached to medial epicondyle brachialis biceps brachi brachioradialis and extensor –supinator muscle triceps anconeus attached to lateral epicondyle
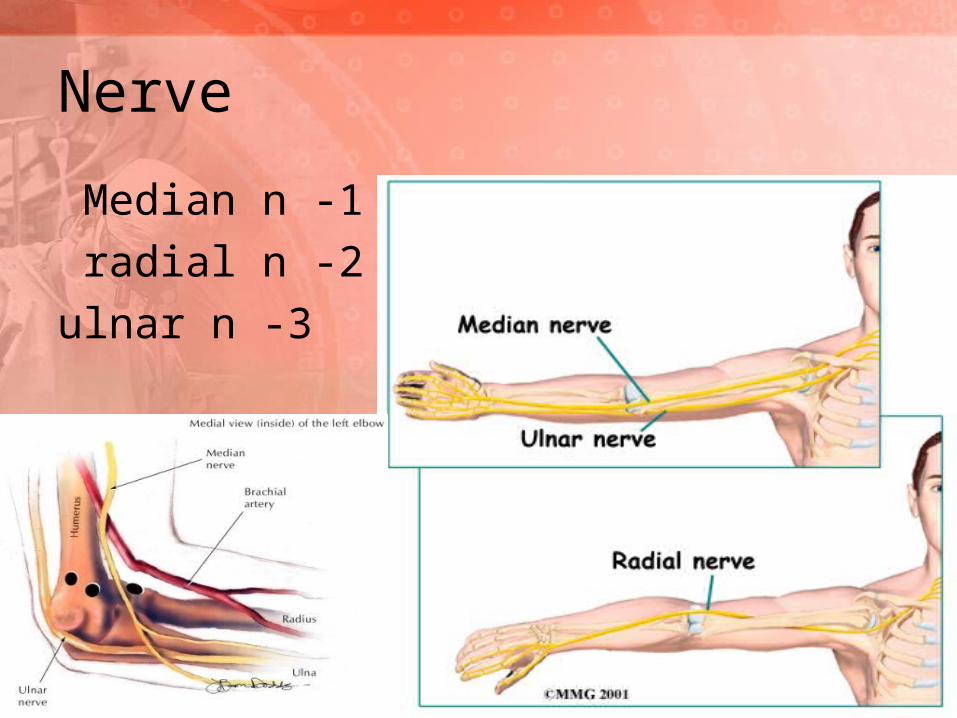
Nerve
1 -Median n
2 -radial n
3 -ulnar n


Physical examination:
Inspection look for :
Swelling , muscle wasting
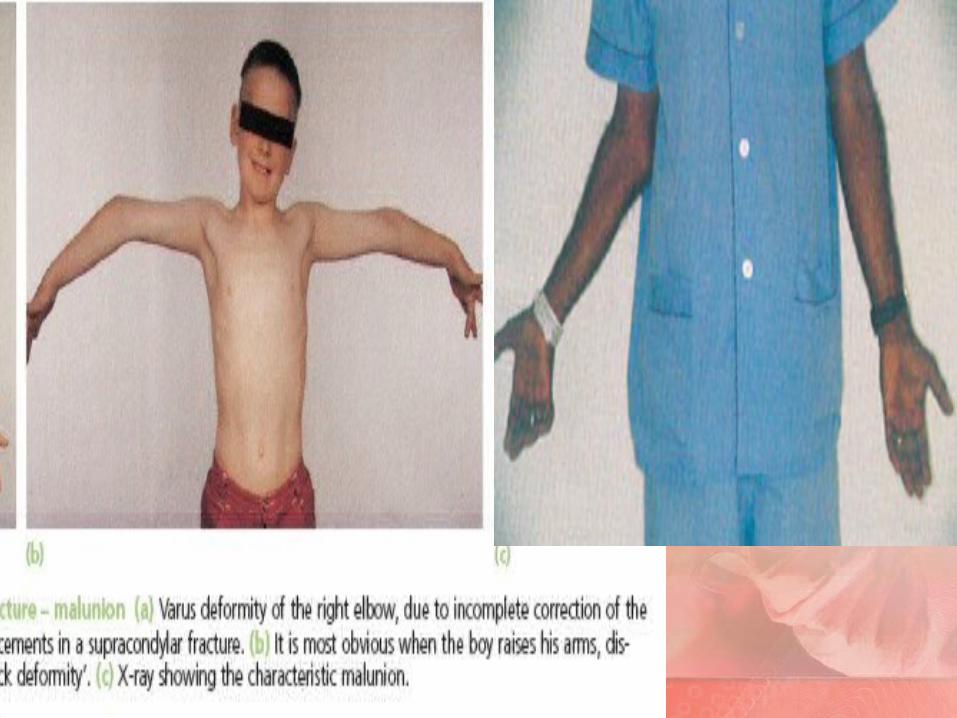
, scare , edema , laceration , deformities , skin change , cubitus valgus , cubitus verus
Palpation:
Soft tissue , posterior aspect , lateral aspect , antreior aspect

MOVEMENT OF ELBOW
Flexion ( Brachioradialis , biceps )
Extension ( Triceps)
Supination (biceps , supinator )
Pronation ( pronator teres , pronator quadratus ).

Movement of elbow

Ossification of the elbow bones
Ossification in menemonic critoeCapitulum ossified at 2 years of ageThe medial epicondyle ossified at 6 years
Trochlea at8 years of age Olecranon at 10 years of age
Lateral epicondyle at 12 years of age So we cant detect fractures of this part before this age but by special technicality such as baumanns angle which subtended by the longitudinal axis of humerus shaft and line through the coronal axis of the capitellar physis it is normal less than 80 degree it is important to be sure that the distal fragment is reduced.
Fracture around the elbow




Fracture of the condoyle
Mechanism of injury High energy injutry except in osteoportic
clincly
pain swelling check pules
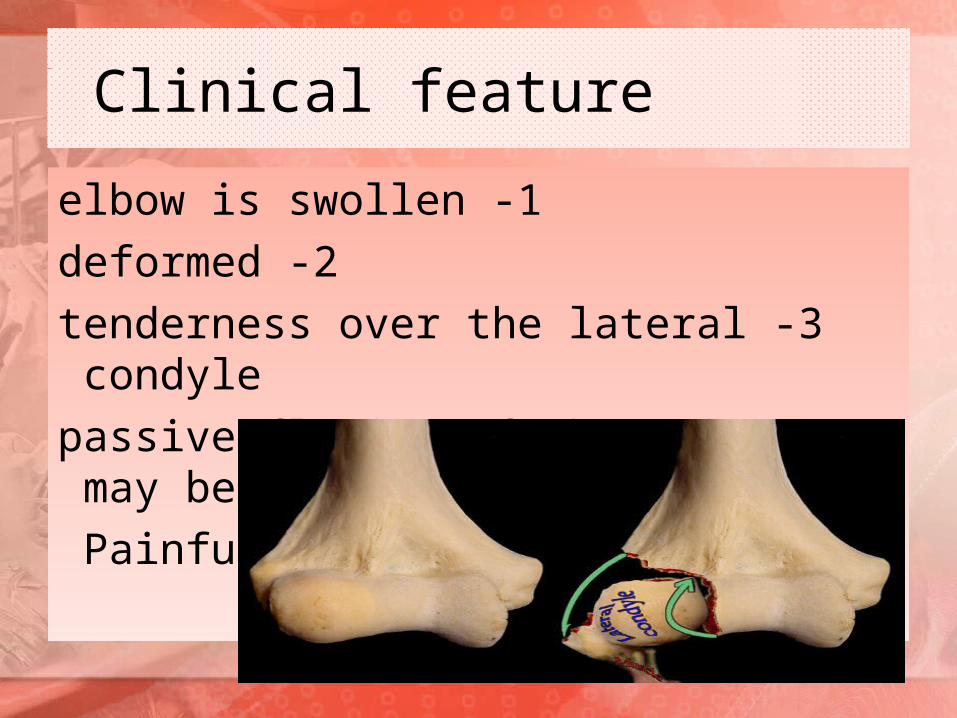
Clinical feature
1 -elbow is swollen
2 -deformed
3 -tenderness over the lateral condyle
4 -passive flexion of the wrist may be
Painful

X-ray fracture extend from lower humerus to elbow joint its difficult to tell whether one or both condyle involved spcialy if it
undisplaced condyler fracture
treatment
A- if there is no displacement The arm can be in a bakslab with elbowFlexed 90 x-ray to exclud late displacment gentel movment after one week
B-displaced fracture open reduction and internal fixation throgh postiror approach

•Ulner nerve should be identifide and protacted from injury
•Fregment reduce and held temporary with k wirs if fracture small fregment unicondyler
and not commented it fixed with screws
•Large fregment do plate to prevent displacment
•Bicondyler and commented do double plate and screws fixation

•And somtime bone graft in the gaps
•Postoprtive movment encouraed but not forced
•Healing in about 8weeks
•In olde pt elbow replacment is more relible option
complication
Vasculer injery nerve injery usually median and ulner
nerve staffnes
hetrotopic ossification process form bone tissue outside skeleton

Inter condyler fracture
•T or y shaped fracture
•Mechanism fall into the elbow medial
•And latral condyle sepreted from each other and rotated downword outword duto
effect of flexor and extensor muscle l
treatment
One of the most difficult to treat
Functional result without reduction are generaly poor and even when
accurately reduced some residual loss of function is usuall
Open reduction and internal fixation requir high dgree of skills its indicated in yonge
adult
•Treatment by early activity is suitable in old pt and function result are satisfactory
•Some surgeons do skeletel traction through the olecranon as alternative open
reduction Its easier and safer but functional result not good
of medial epicondyle Avulsion fracture
•Avulsion of epiphysis of medial epi condyle is common duto strain applid to
elbow with force of flexor group of muscle
•Position of avulsed fregment may rang from minimal sepration to gross
displacment and displacment with the epicondyle being pulled into the joint and trapped between humerus and olecranon

treatment
•Minor sepration no reduction but elbow should be rested incollar and cuff for 3
weeks
•Gross displacement or epicondyle trapped in joint reduction by manipulation is
sometimes successful but if fails open reduction and internel fixation is indicated
epicondyle Avulsion of lateral
•LESS COMMON
-14 year 11
duto traction of extensor muscle from varus strain of the joint may avulse latral
epicondyl
Since the latral epicondyler epiphysis is not constant and even appear separately it
exists only for 1-2 year
Fracture of proximal end of radius
•Commn yonge adult and children mechanism fall on outstretched hand
with elbow extended and forarm pornated of head aginst cpitulum coused impact
•Fracture of head of radius common in adult
•Fracture of neck of radius common in children
•Articular cartlage of captulium may affected
•Spcial features
•Following fall on outstretched arm the patint complain of pain and local
tenderness posterolatraly over proximal end of radius and marked pain in
supination and pronation

Fractured neck of radius
Mechanism of injuryA full on the outstretched
hand forces The elbow into valgus and pushed
the radial head against the capitulum Clinical feature
#Pain in the elbow #Localized tenderness over radial head
#Pain on rotating the forearm
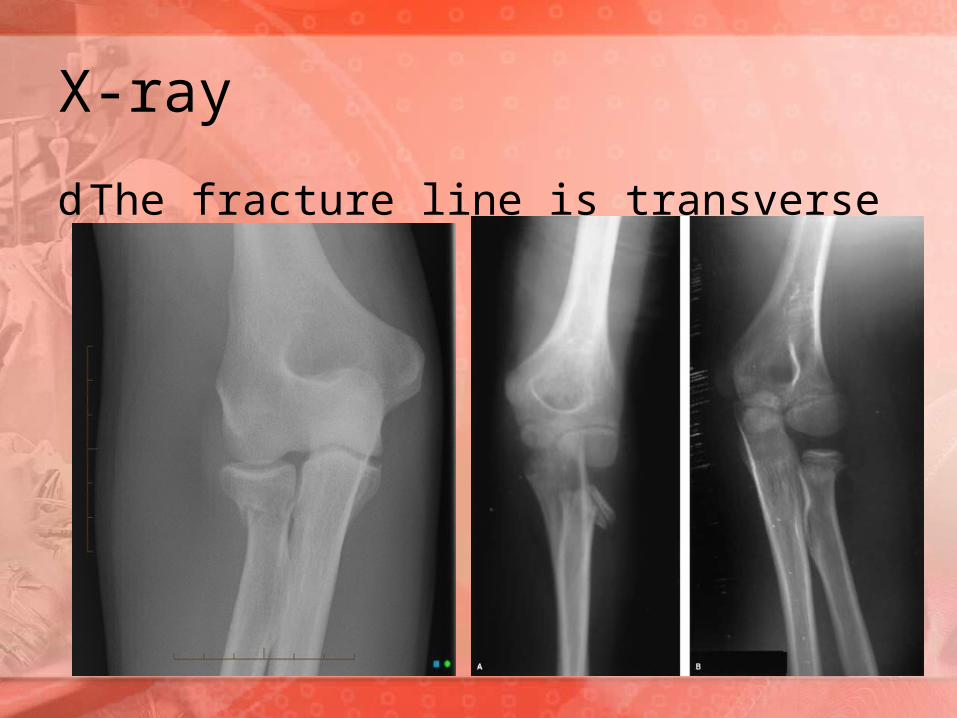
X-ray
d The fracture line is transverse

Treatment
Up to 30 degree of radial head tilt and up to 3mm of transverse displacement are acceptable. The arm is rested in a collar and cuff and exercise after week Displacement of more than 30 degree should corrected pt elbow extended traction and varus force are applied the surgeon then push displaced radial
fregment by thumb
•If this fails open reduction performed no need internal fixation following opration
elbow splinted 90 flexion for1-2weeks
Fracture that seen one week or longer after injury should be un treated except light
splitage

Fracture of head of radius . this this could A-vertical spilt undisplaced, this can be treated rest on coller and cuff for 2-3 weeks then active exercise . B-single fragment displaced of the lateral portion of the head broken off and usually displaced distally . This is treated open reduction and fixation by pinning back the fragment with a kirschner wire or small screw . C- comminuted fracture –this is best treated by early excision of the head, this usually gives an simple excision on radial head is
Now should replaced by metal prosthasis adequate.
•The wrist also shold be very carfuly examined to exclude concomitant injury of distal radioulner joint called essex lopresti
lesion
complications
•Joint staffness may involve both elbow and radioulner joint
•Recurrent instablity can occure if medial collatral ligement was injered and radial
head excised
•Osteoarthritis of radiocapitellar joint is late complication it may call for excion head

Fracture proximal ulna
Fructure cronoid proces
bony insirtion of brachalis muscle so fracture usually avoltion

Treatment
•By rest in sling is method of choice except
•When large fregment result in elbow instablity then open reduction and internal
fixation is indicated

Fracture of the olecranion .the olecranon is subject to both direct and indirect
trauma because of its superficial position .the most frequent in adult and the elderly patient
diagnosis . Pain graze or bruise over the elbow sugest commented ,in displaced transvers fracture the olecranion may be felt in the lower arm and agape may be palpable the patient unable to extent the
elbow .
Tow types. 1-commented fracture duto dirct truma •2-clean transvers fracture duto traction when the pt
fall •onto hand while triceps m contracted
•X-ray latral veiw show details of fructure
•Treatment1-undisplaced transvers fracture
•Immbolization elbow weth castabout 60degree flexiton for 1 week then exercise
2-displaced transversmay do splintage in stright position but staffness occure so
opretive treatment is prefer we have three methods
•1-fixation with long cancellous screws inserted on tipe
•2-tention band wiring
•3 -contoured plate and screws
•Complication
•Staffness and malunion
•Osteoarthritis in articuler surface of trochlea treated by cortisone and modification activity

Bruise in olecranon fracture
Complication of olecranon fracture /stiffness ,non union , ulnar nerve injury osteoarthritis is a late
complication.
Fracture of capitulumMechanism of injuries-fall on the hand with the elbow straight
Clinical features -fullness in front of the elbow the lateral side of elbow is tender and flexion is grossly restritced
Xray -lateral view capitulum or part of it seen in front of lower humerus and radial head away from it
treatment.1-undisplaced fracture/treated by simple splintage or sling for 4-5 days
2--displaced/oprtive reduced and internal fixation or if proves difficult excised.


Dislocation of the elbowSeprted 2 articuler surface ulna and radies seprated as one unite
Displacement postirory -antirorly-medialy or latraly
40 asscited with fracture of close structure as avulsion of medial epicondyle in child and olecranon –captulium –head of radius – cronoid process fracture
See in any age presented as
1-shorted forarm
2-promenant olecranon p
3-disterbance in triangel
Diagnosisclincly
•x-ray
•Nurovasculer exam

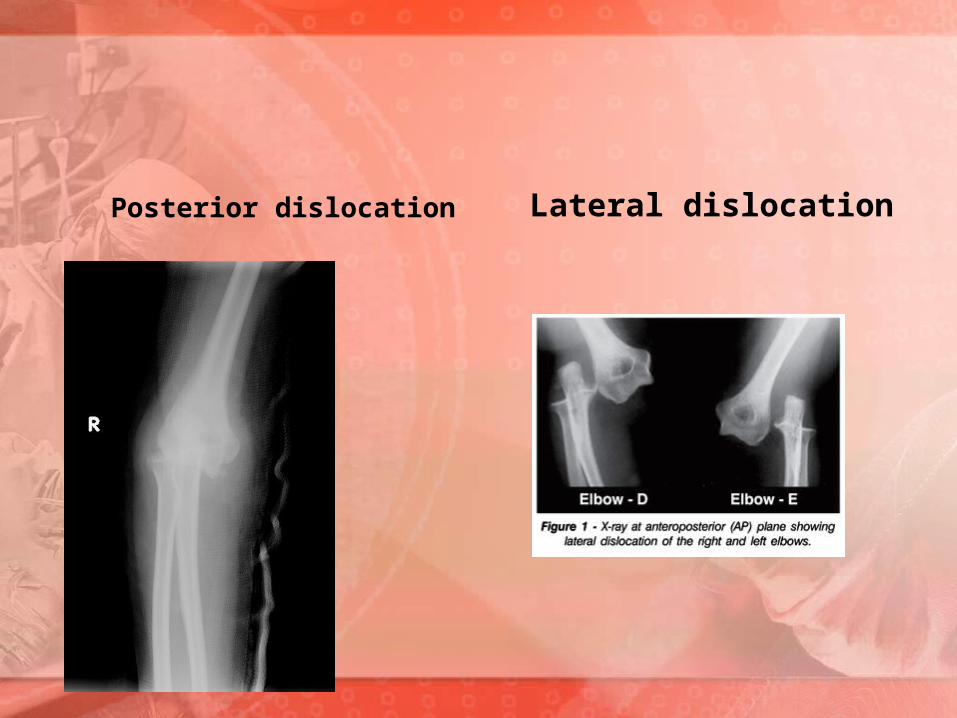
Posterior dislocation Lateral dislocation

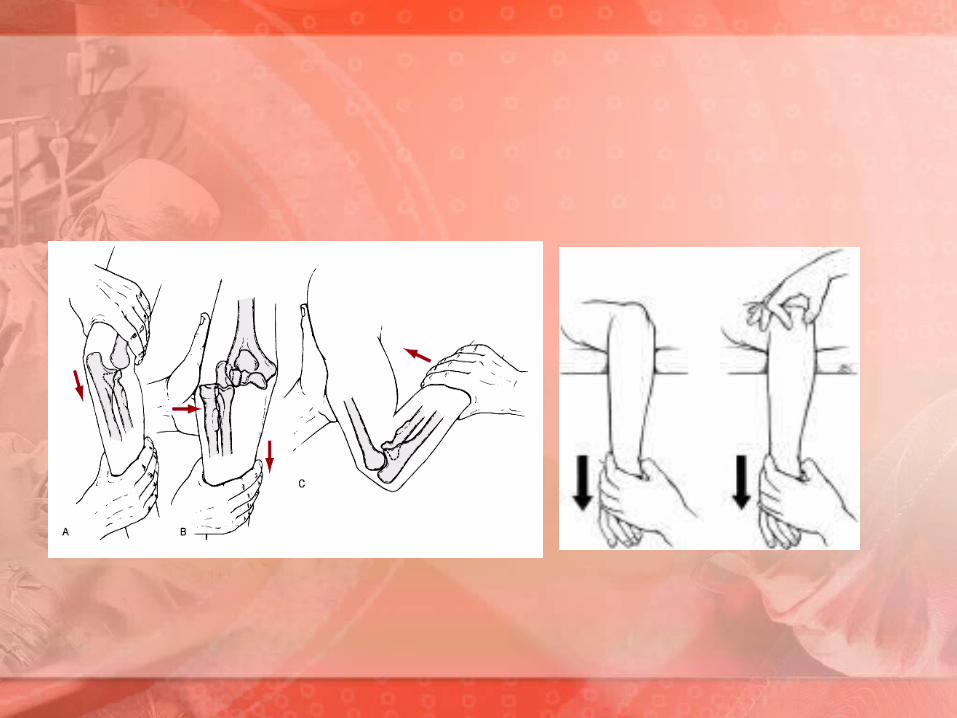
TreatmentAnatomical reduction is essential should be soon as possible . the majority of cases are treated conservatively . surgical intervention may be indicated fore the associated fractures . a-reduction by traction on the forearm in the position in which it lies ,in order to over com biceps and triceps shorting , at the same time the olecranon is pushed forward by thump whilst the elbow is slowly flexed . the stability is then checked by gently moving the elbow through its normal range .b-immobilization . this can be achieved by collar and cuff with or without a posterior slab for 3 week with elbow at 90 flexed .c-rehabilitation Shoulder and finger exercise should command at once .while genteel active . elbow exercise should
common after on week .
Complications • vascular injury of brachial artery may occur but with a
lesser frequency than in cases of supracondylar fracture . • nerve injury . the medial ulnar nerve may be
affected .c/myositis ossification ,which is more common if passive exercise is inflicted on the patient.
• Recurrent of the dislocation may occur if the bony , ligamentous, and muscular support structure are disrupted sufficeintly.
• late complications 1/stiffness 2/heterotopic ossification 3/unreduced dislocation 4/recurrent dislocation 5/osteoarthritis after sever fracture dislocation.
Pulled elbow- subluxation of head of radius this conation occur in
infancy and early childhood .
Mechanism of injury is a traction force applied to the elbow in pronatione leading to subluxation of the head which becomes impacted in the
orbicular ligament .
this condition responds dramatically to quick movement of the forearm in to full supination.

Mechanism of pulled elbow not the radial dislocation

Full supination for mangmente of pulled elbow
