the heart mary beth vogel, bsn, rn-c. useless facts! the human heart creates enough pressure to...
TRANSCRIPT
THE HEARTMary Beth Vogel, BSN, RN-C
USELESS FACTS!• The human heart creates enough pressure to squirt
blood 30 feet
• There are 60,000 miles of blood vessels in the human body – enough to circle the earth twice!
• The aorta is almost the diameter of a garden hose
• 20% more people die from heart attacks on Mondays than any other day of the week
LOCATION, SIZE, POSITION
• Located in thoracic cavity btwn lungs in mediastinum
• Two thirds to the left of midline and one third to the right
• Apex is just above the diaphragm; base is at the top
• Size and shape of a closed fist
• Apical pulse: btwn ribs 5 & 6, midpt of L clavicle
(5th intercostal space, midclavicular line)
HEART FACTS
• Begins beating at 4 weeks gestation
• Beats over 100,000 times/day
• 72 bpm = 103,680 b/24h and 2,000 gallons of blood daily
• In a 70-year lifetime, an average human heart beats more than 2.5 billion times, pumping approximately 1 million barrels of blood.
• Myocardium: cardiac muscle

HEART ANATOMY

1. MEMBRANES
• Heart is enclosed in pericardial membranes
• Fibrous Pericardium: sac surrounding the heart; outermost layer
• Parietal pericardium: outer layer; lines fibrous pericardium
• Visceral pericardium/epicardium: inner layer ; surface of myocardium
• Serous fluid btwn layers prevents friction
• Why is serous fluid btwn layers important?

• Endocardium: simple squamous epithelial tiss that lines the inside of the hearts chambers
• This smooth tiss prevents clot formation
• Endocardium also lines valves and major vessels that are assoc w/ heart


CARDIAC MEMBRANE DISORDERS
• Pericarditis—inflammation of the pericardium
• Pericardial effusion: accumulation of fluid btwn parietal and visc layers
• Cardiac tamponode—compression of the heart caused by fluid building up between the visceral and parietal pericardium
• Endocarditis: inflammation of endocardium

2. CHAMBERS
• 4 total
• Lined w/ endocardium
• Two upper chambers are called atria (receiving chambers)—right and left atrium
• Two lower chambers are called ventricles (discharging chambers) – right and left ventricle
• Heart is a double sided pump; intercalated discs allow it to pump as a unit
• Wall of each chamber composed of myocardium

3. SEPTUM
• Septum: wall that seperates chambers
• Interatrial: btwn 2 atria
• Interventricular: btwn 2 ventricles
• Septal defects: structural defects of septum; often congenital
• VSD, ASD
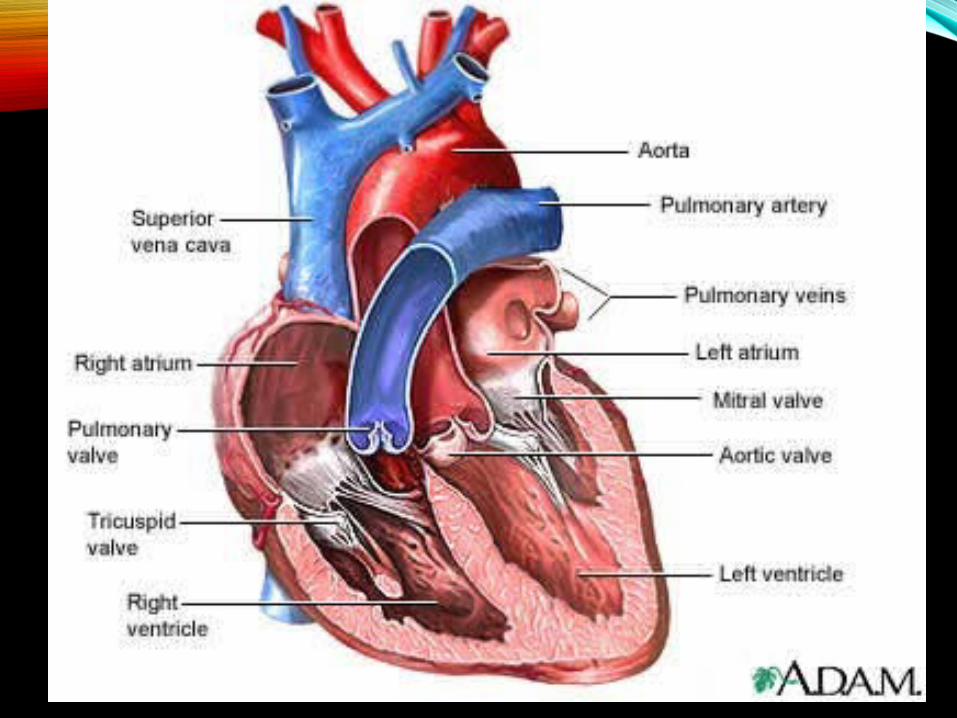

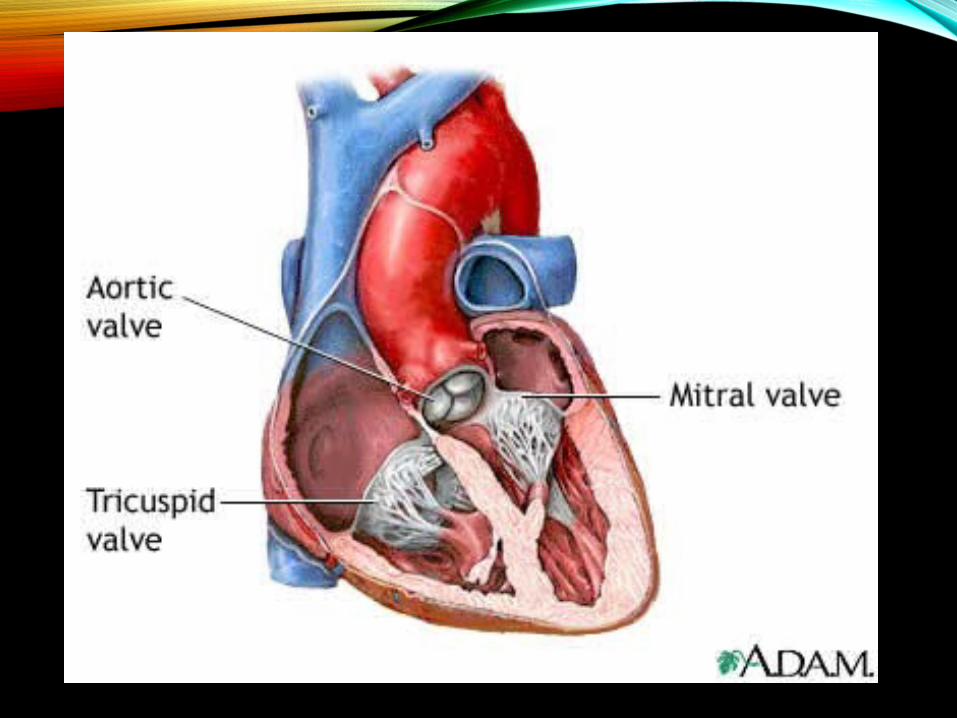
4. VALVES
• Four valves keep blood flowing through the heart; prevent backflow
• Two atrioventricular (AV) and two semilunar (SL) valves
• 2 AV: separate the atria and ventricles:
a. Tricuspid: at the opening from the R atrium into the R ventricle
b. Bicuspid (mitral): at the opening of the L atrium into the L ventricle
• 2 SL: Btwn vent and the major vessels they empty into
a. Pulmonary semilunar: at the beginning of the pulmonary artery
b. Aortic semilunar: at the beginning of the aorta
http://www.getbodysmart.com/ap/circulatorysystem/heart/anatomy/valves/tutorial.html

CARDIAC VALVE DISORDERS
• Incompetent valves: “leak,” allowing some blood back into the chamber from which it came
• Stenosed: narrowed thus decreasing bld flow; cause for murmurs (abnormal, extra sound)
• RHD: strept inf that damages myocardium and/or valves. C/b rheumatic fever 1-5 wks post strept
• MVP: incompetence of mitral valve; edges extend into the left atrium when the left vent contracts


MITRAL VALVE STENOSIS

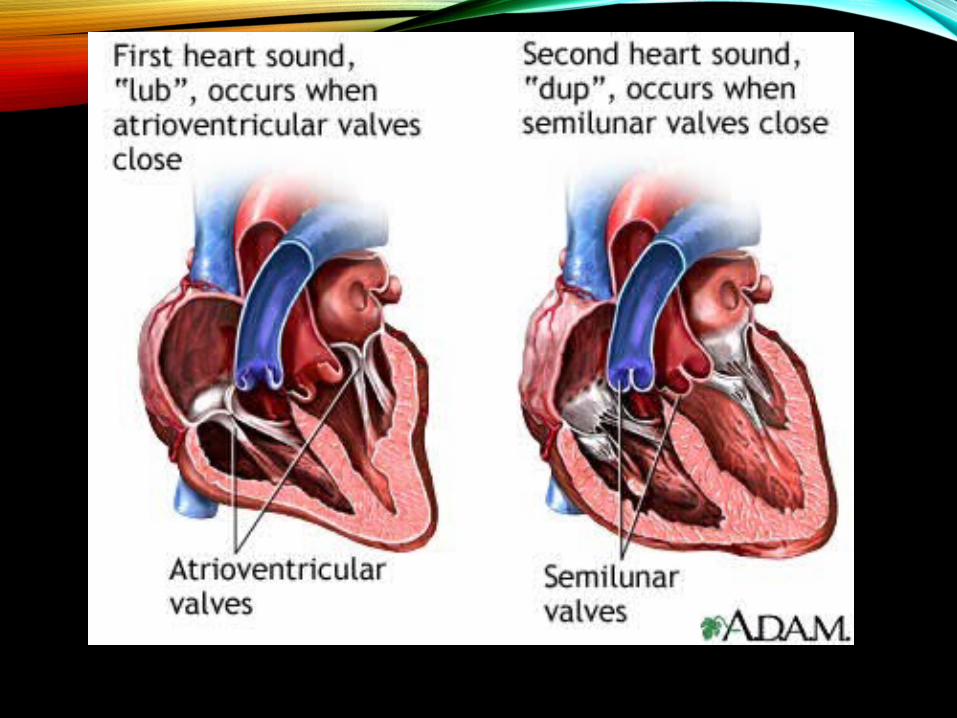
HEART SOUNDS
• Noise prod during cardiac cycle
• Two distinct sounds in every heartbeat: “lub-dub”
• Sound is created by closing of valves
• First (lub) sound is caused by closure of AV valves during contraction of vent (vent systole); longer/louder (aka S1)
• Second (dub) sound is caused by closure of the semilunar valves during relaxation of vent (vent diastole) (S2)
• Pulse deficit: apical – radial (seen in cv disease)

HEART ACTION
• Systole: contraction
• Diastole: relaxation
• Atrial systole is followed by ventricular systole
• Efficient pumping of chambers = rhythmic pumping action
• Valves control direction of bld flow
• Asystole

HEART ANATOMY REVIEW!
• What is the difference btwn epicardium and endocardium?
• Name the structures btwn the 2 atria and ventricles
• Where is apical pulse heard (precisely)?
• Give the names and precise locations of all valves
• Define systole
• What precisely creates the lub dup sounds?

BLOOD FLOW THROUGH THE HEART
• Heart acts as two separate pumps: R atrium and vent perform diff functions from L atrium and vent
• Both sides pump simultaneously
• R side of the heart rec deoxygenated bld from body and pumps it to lungs to pick up O2 and dump CO2
• L side of the heart rec oxygenated bld from the lungs and pumps it to the body
• Both atria contract together; then both vent
• Bld flow is passive from atria to vent but bld is actively pumped from vents to aorta and pul art; thus ventricles are more critical to survival
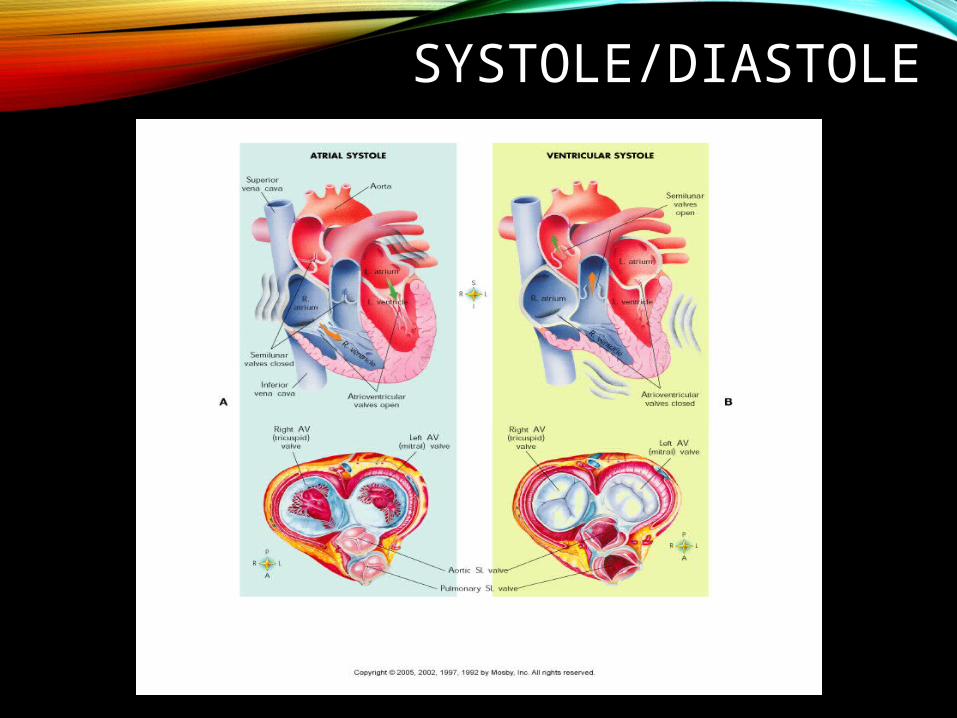
SYSTOLE/DIASTOLE

BLOOD VESSEL ANATOMY/VOCAB
• Arteries: carry oxygenated bld away from heart; elastic and lined w/ smooth musc; distrib nut and O2 to body’s cells
• Arterioles
• Veins: carry deoxygen bld back to heart; 1 way valves prevent back flow; less elasticity than art thus more prone to clots
• Venules

• Capillaries: microscopic vessels connect art/vein and allow for gas/nutrient exchange
• Artery and Vein layers:
• Tunica externa: outer conn tiss layer
• Tunica media: mid layer of sm musc tiss (more in art)
• Tunica intima: endothelial inner layer (simple squamous epithelial tiss)

• Vessel Disorders:
• Aneurysm: abnormal weakening/widening in the wall of an art
• AAA
• Arteriosclerosis: thickening of art wall d/t fat/Ca deposits (hardening of arteries)
• Varicies: varicose veins. Bld pools in superficial veins
• Phlebitis: vein inflamm
• Thrombophlebitis: phlebitis c/b clot (DVT)


PATH OF BLOOD FLOW THROUGH THE HEART:
• http://www.medtropolis.com/VBody.asp
• Venous/deoxygenated blood enters R atrium through sup and inf vena cava
• Deox bld passes from R atrium through tricuspid to R ventricle
• Deox bld passes from R ventricle through pulmonary semilunar valve to pulmonary artery and to lungs

• In the lungs, CO2 is dumped/O2 picked up
• Oxygenated bld travels from lungs to L atrium via 4 pulmonary veins
• Oxy bld passes through bicuspid (mitral) valve to L vent
• Oxy bld in L vent is pumped through aortic semilunar valve into aorta and is distributed to the body

BLOOD FLOW THRU HEART


CIRCULATION
• Systemic Circulation: circ of bld throughout the body
• Aorta: 1st vessel of systemic circ
• Sup/inf vena cava: last vess of sys circ
• Pulmonary Circulation: bld flow to and from lungs
• Pul Art: 1st vess of pul circ
• Pul veins: last vess of pul circ
• Where is B/P highest and lowest?
• Others: coronary, portal, fetal


THE AORTA


BLOOD PRESSURE
• B/P gradient: (aorta=100mmHg; vc=0mmHg) and is impt to maintain circulation
• Factors that influence B/P: bld volume (cardiac output is @ 5L/min), hrt rate, bld viscosity, peripheral resistance
• CVP: B/P w/in R atrium – inf lg periph veins
• HTN: > 140/90 (preHTN = 120-139/80-89); normal = < 120/80
• Risk factors: age, race, genes, obesity, stress, Ca def, smoking, sedentary
CIRCULATORY SHOCK
• Lack of bld flow and delivery of O2 to cells
• Cardiogenic: hrt failure
• Hypovolemic: loss of bld vol
• Neurogenic: widespread vasodilation d/t sympathetic ns disruption
• Anaphylactic: allergy causes vasodilation
• Septic: toxins cause vasodilation

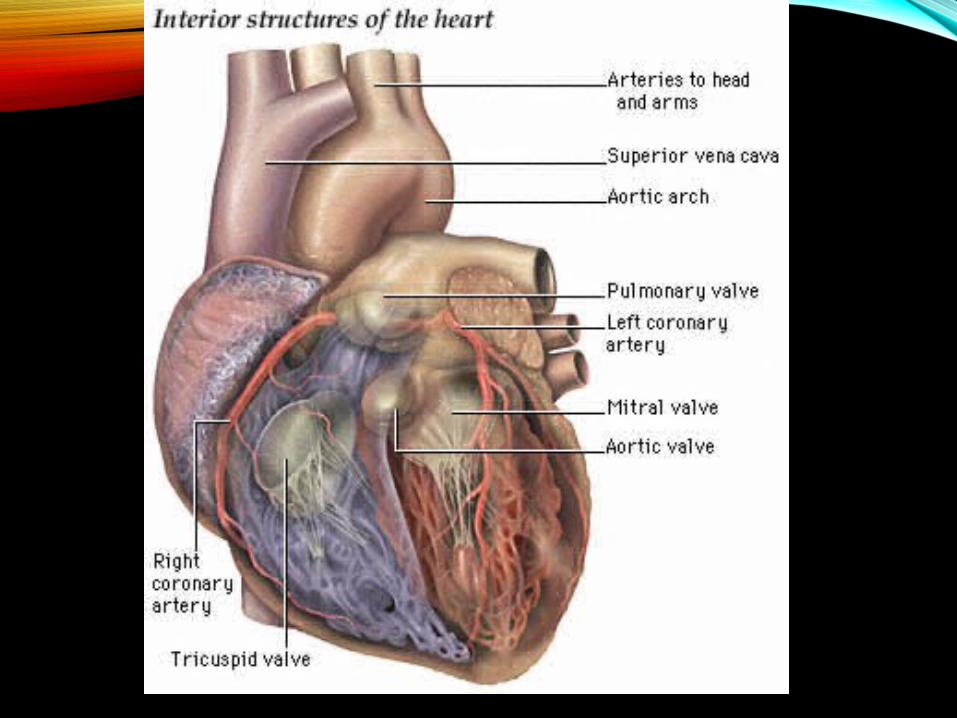
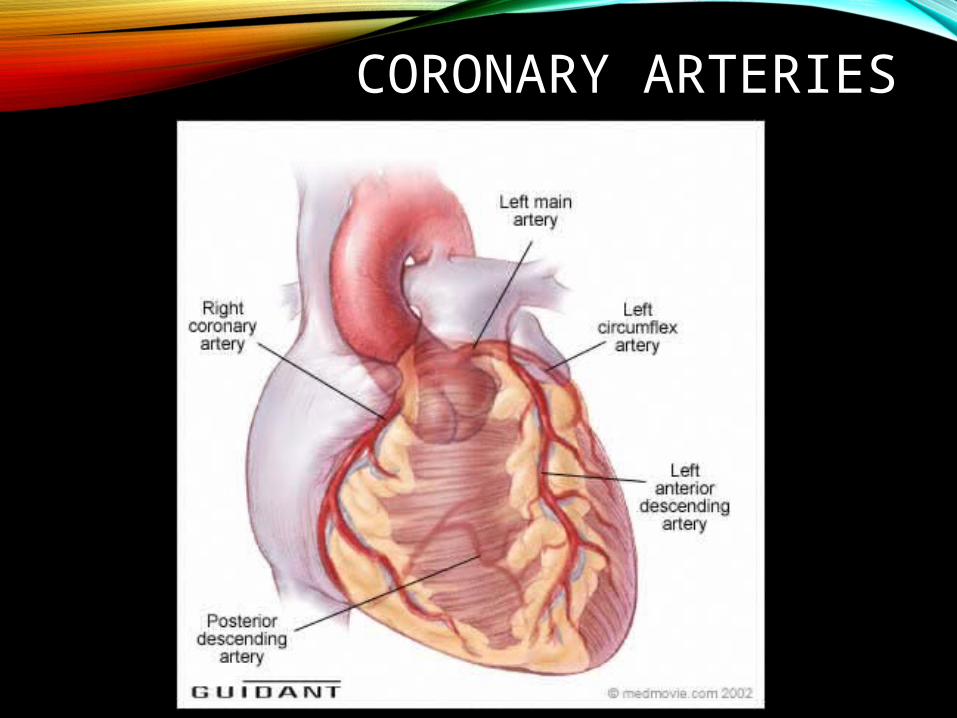
CORONARY CIRCULATION
• Coronary arteries:
• Bld supply for the myocardium
• R&L coronary arteries (R&L main) are 1st branch from aorta
• L Main primary branches: circumflex and LAD
• These are most likely to be affected by coronary artery disease (CAD)
• CAD dx by cardiac cath
• http://www.crozer.org/medinfo/a_playr/player/cath/p_cath.htm#cath_h
CORONARY ARTERIES

• Coronary veins:
• Collect the oxygen-poor blood from myocardium
• Coronary veins empty blood directly into the right atrium through the coronary sinus
• Coronary sinus is a small hole in the right atrium protected by a flap of tissue

CORONARY ARTERIES AND VEINS

CORONARY SINUS


CORONARY ARTERY DISORDERS
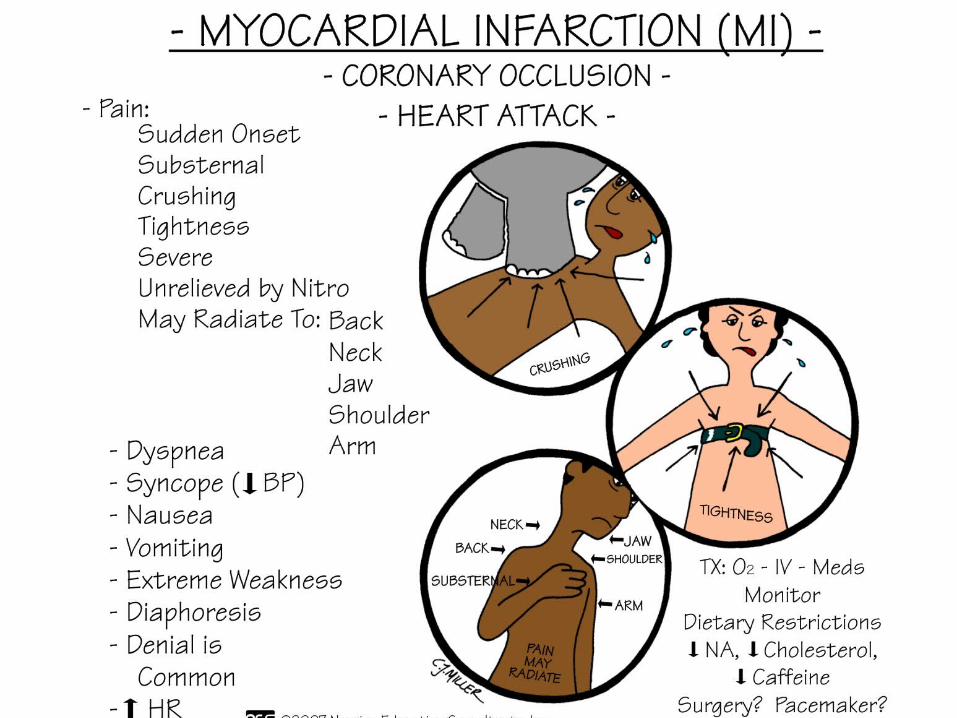
1. MI: blockage of blood flow through the coronary arteries can cause ischemia (lack of O2 causing tiss impairment): prolonged ischemia = infarct (area of necrosis)
• S/S: chest, jaw, shoulder pain, n/v, SOB, diaphoresis
• Tx: prevention, CABG
• Predisposing factors: genes, HTN, DM, smoking, poor diet, high LDL, obesity, sedentary lifestyle



2. Angina pectoris: chest pain d/t lack of O2 to myocardium. d/t a narrowing of the coronary art from arteriosclerosis
• S/S: usually occurs during exertion, severe emotional stress, or after a heavy meal
• Tx: nitroglycerin
• 3. Arteriosclerosis: hardening/thickening of walls of arteries
• Fatty deposits, calcification of wall of art or thickening of the muscular wall of art from chronic HTN
• Tx: variety of meds
• 4. CHF: heart's function as a pump cannot meet the body's needs
• Causes of CHF: MI, CAD
• Poor bld supply resulting from CHF may cause body's organ sys to fail
• CHF causes blood to back up which can lead to fluid accum in lungs and body tissues
• S/S: edema (systemic and/or pulmonary)
• Tx: meds to improve heart’s pumping ability, diuretics
CARDIAC CYCLE
• Heart beat is regular/rhythmic—each complete beat called a cardiac cycle—adult average is about 72 bpm
• Each cycle, about 0.8 seconds long, subdivided into systole (contraction) and diastole (relaxation)
• Series of events during which electrical imp is conducted thru cardiac structures

• Stroke volume: amt of bld ejected from vent with each beat (@ 60-80ml/beat)
• Cardiac output: amt of bld vent can pump each minute (@ 5 L per minute at rest)
• Stroke vol x bpm or 70ml x 72 bpm
• Athletes have lower hr d/t heart’s ability to pump more bld w/ each beat, thus to have same cardiac output less bpm are required (their stroke vol may be 100ml/beat)
• Starling’s Law of the Heart: the more cardiac musc fibers are stretched, the more forcibly they contract

MURMURS
• Auscultation: assessment of heart sounds
• Heart murmurs—abnormal heart sounds often c/b structural defects
• Stenosed or damaged valves: may allow for leakage of bld or squeezing of bld thru the narrow space create turbulence
• Cause: congenital, RHD, septal defects

CONDUCTION PATHWAY

• Cardiac cycle is a series of mechanical events reg by elec activity of the myocardium
• Cardiac muscle cells have ability to contract spontaneously; the heart generates and conducts its own impulses
• Intercalated discs: link cardiac muscle fibers electrically and mechanically – allow the heart to contract as a unit
• 4 structures in heart generate and conduct imp that allow for atrial and ventricular contraction
• These are:

• 1. SA node: sinoatrial node – “natural pacemaker” – specialized cells loc in the wall of R atrium near the opening of the sup vena cava
• Rapid rate of cont since cells here are very permeable to Na and depolarize quickly which is necessary to initiate a heartbeat
• If there is a defect of SA node the heartbeat can be initiated elsewhere but it will be slower rate

• 2. AV (atrioventricular) node—loc in R atrium along lower part of the interatrial septum
• Imp from SA node travel here to bring about atrial systole
• 3. AV bundle (Bundle of His)—loc in interventricular septum
• Receives imp from AV node
• Transmits imp to last structure
•4. Purkinje fibers—located in walls of ventricles
• Receives imp from Bundle of His
• Imp spreads out to rest of ventricular myocardium to bring about ventricular systole
• This electrical activity and transmission of imp from each of these 4 structures is recorded on an EKG:


• Electrocardiography
• Electrical impulses that generate heart beat can be picked up on surface of body and transformed into visible tracings by an electrocardiogram/electrocardiograph
• EKG has three deflections or waves: P wave, QRS complex
and T wave

• P wave: depol of atria and transmission of imp from SA to AV node (atrial systole)
• QRS complex—associated with depol of vent as imp spreads from Bundle of His to Purkinje fibers (vent systole)
• During QRS complex, atria repolarize but this does not appear as a separate wave since it is such a small wave and is hidden by the lgr QRS wave
•T wave— repol of the vent

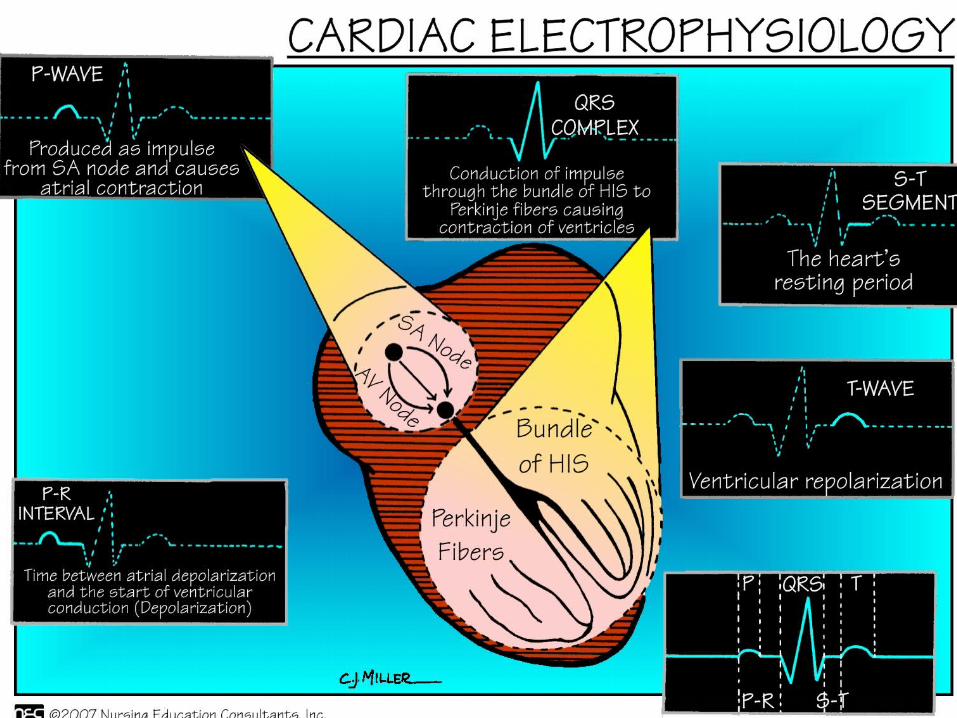

• The length of each wave and the spacing inbetween is clinically significant

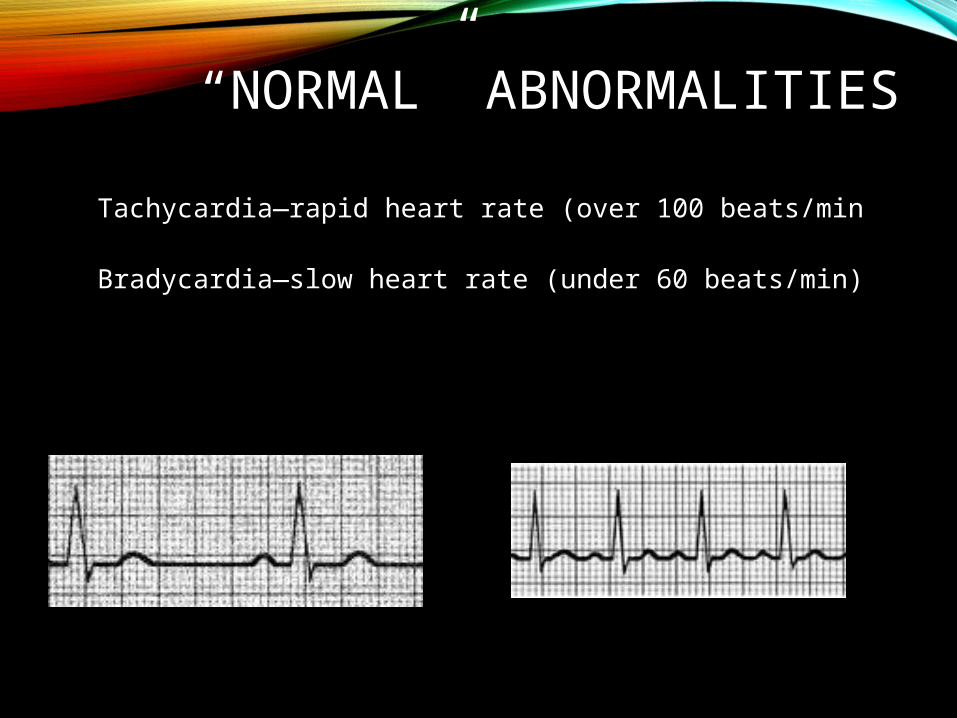
“NORMAL” ABNORMALITIES
Tachycardia—rapid heart rate (over 100 beats/min
Bradycardia—slow heart rate (under 60 beats/min)

ARRYTHMIAS/DYSRHYTHMIAS
• Abnormality of heart rhythm
• Both are terms for an irregular heartbeat d/t a damaged conduction system/pathway
• There are many types of arrhythmias (based on location)
• General s/s: palpatation, vertigo, syncope, chest pain, SOB

• Tx: varies acc to the specific arrhythmia but generally the goal is to medically control the rhythm and anticoagulation
• Cardioversion:
restore NSR thru
defibrillation

TYPES OF ARRHYTHMIAS
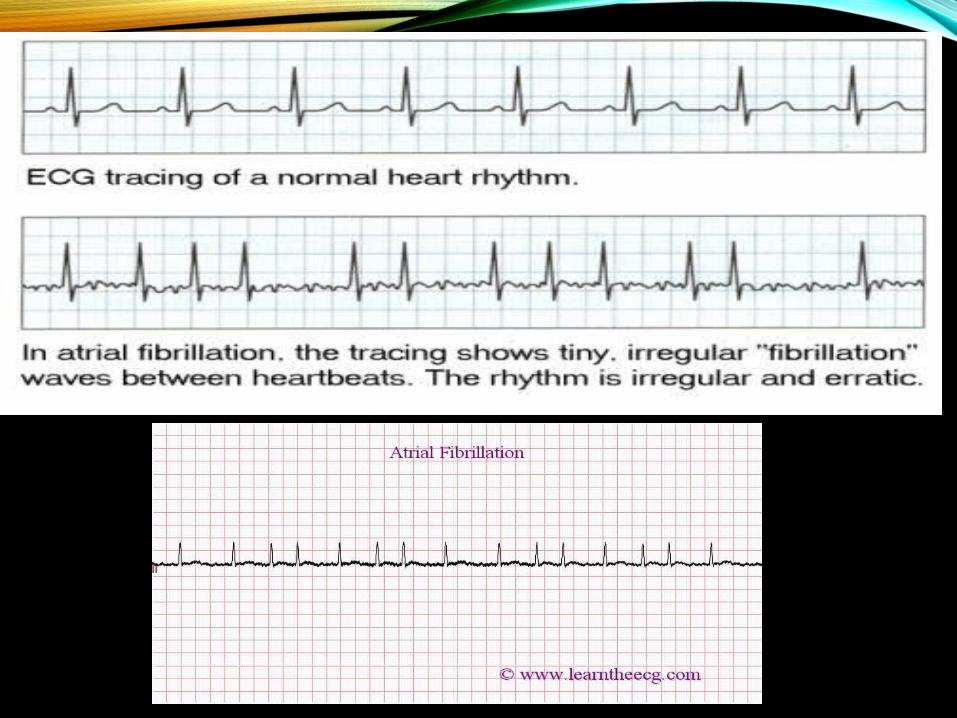
• 1. Atrial fibrillation: the atria quiver btwn 300 and 600 times per minute, never fully contract, so some bld may stay in the atria with each beat
• Pooled bld could clot thus inc risk of CVA
• Tx: meds: beta blockers(Lopressor, Inderal), Ca channel blockers (Cardizem), Digoxin and anticoags (ASA, Coumadin)
• 2. Atrial flutter: atrial tachycardia; less common than a-fib

• 3. Premature ventricular contraction: vent depol occurs too early; wide/early QRS on EKG; if frequent they can be precursor to v tach or v fib. Tx: meds if > 6 PVCs / min
• 4. Ventricular tachycardia: originates in Av bundle; > 100 bpm
• 5. Ventricular fibrillation: rapid depol of vent, loss of cardiac output and B/P; CPR and defib necessary

• NSR with PVC

• Ventricular Tachycardia or “V Tach”

• Ventricular fib or “V Fib”

MORE PROBLEMS
• Heart block: conduction of impulses is delayed/blocked
• Classified by location
• Causes dysrrhythmias
• Tx: pacemaker

CHF
• Heart’s ability to pump is ineffective
• Causes: MIs, HTN, cardiomyopathy, valve disorders, Infection, congenital defects, lifestyle
• S/S: fatigue, edema, SOB, DOE
• TX: meds, lifestyle (decrease Na intake)

HEART FAILURE
• Heart failure—inability to pump enough bld to meet metabolic needs of body tissues; many causes (cardiopyopathy, valve disorder, diseased hrt tiss)
• Right-sided heart failure—rt side of the heart unable to pump, usually d/t lung disease obstructing pul bld flow
• Left-sided heart failure —inability of the left vent to pump, resulting in congestion of the sys and pul circulations
• Tx: may inc transplant

CHF

