the kentucky pharmacist vol. 7, #3
DESCRIPTION
May JournalTRANSCRIPT

News & Information for Members
of the Kentucky Pharmacists Association
Vol. 7, No. 3
May 2012
TTHEHE KKENTUCKYENTUCKY
PPHARMACISTHARMACIST
Registration form and
schedule inside! CPE Monitor:
What does it
mean for you?
CE: Compounding
for Scalp
Disorders
Also inside:
Gov. Beshear signs
Pharmacy Audit Bill
2012 Legislative Session Recap, Pg. 12

May 2012
THE KENTUCKY PHARMACIST 2
Table of Contents
Table of Contents
Table of Contents— Oath— Mission Statement 2 President’s Perspective 3 ASCP/HD Smith 4 KPhA Annual Meeting 2012 5 KPhA Invitation for Membership 11 Kentucky Legislative Session Summary 12 May CE—Compounding for Scalp Disorders 16 May Pharmacist/Pharmacy Tech Quiz 24 KPPAC Contribution Form 25 Pharmacy Law Brief 26 CPE Monitor: Change is coming 28 Pharmacy Technician Certification Board 29
Agency for Healthcare Research and Quality 30 Pharmacy Time Capsules 31 KPhA at NASPA Leadership Conference 32 KPhA Government Affairs 33 June CE— Reducing the Burden of ADEs 34 June Pharmacist/Pharmacy Tech Quiz 38 APhA Annual Conference—the Student Perspective 39 Why Do I Need To Be Certified? 40 McWhorter College of Pharmacy 41 Pharmacy Policy Issues 42 Long Term Care CE Event 44 Pharmacists Mutual Companies 45 KPhA Board of Directors 46 Frequently Called and Contacted/Classifieds 47
Oath of a Pharmacist
At this time, I vow to devote my professional life to the service of all humankind through the profession of
pharmacy.
I will consider the welfare of humanity and relief of human suffering my primary concerns.
I will apply my knowledge, experience, and skills to the best of my ability to assure optimal drug therapy
outcomes for the patients I serve.
I will keep abreast of developments and maintain professional competency in my profession of pharmacy.
I will embrace and advocate change in the profession of pharmacy that improves patient care.
I take these vows voluntarily with the full realization of the responsibility with which I am entrusted by the public.
Kentucky Pharmacists Association
The mission of the Kentucky Pharmacists Associa-
tion is to promote the profession of pharmacy, en-
hance the practice standards of the profession, and
demonstrate the value of pharmacist services within the
health care system.
Editorial Office:
© Copyright 2012 to the Kentucky Pharmacists Asso-ciation. The Kentucky Pharmacist is the official journal of the Kentucky Pharmacists Association published bi-monthly. The Kentucky Pharmacist is distributed to KPhA members, paid through allocations of member-ship dues. All views expressed in articles are those of the writer, and not necessarily the official position of the Kentucky Pharmacists Association.
Editorial, advertising and executive offices at 1228 US 127 South, Frankfort, KY 40601. Phone 502.227.2303 Fax 502.227.2258. Email [email protected]. Website http://www.kphanet.org.
The Kentucky Pharmacy Education and Research Foun-
dation (KPERF), established in 1980 as a non-profit sub-
sidiary corporation of the Kentucky Pharmacists Associa-
tion (KPhA), fosters educational activities and research
projects in the field of pharmacy including career coun-
seling, student assistance, post-graduate education, con-
tinuing and professional development and public health
education and assistance.
It is the goal of KPERF to ensure that pharmacy in Ken-
tucky and throughout the nation may sustain the continu-
ing need for sufficient and adequately trained pharma-
cists. KPERF will provide a minimum of 15 continuing
pharmacy education hours. In addition, KPERF will pro-
vide at least three educational interventions through oth-
er mediums — such as webinars — to continuously im-
prove healthcare for all. Programming will be determined
by assessing the gaps between actual practice and ideal
practice, with activities designed to narrow those gaps
using interaction, learning assessment, and evaluation.
Additionally, feedback from learners will be used to im-
prove the overall programming designed by KPERF.

May 2012
THE KENTUCKY PHARMACIST 3
President’s Perspective
As I sit down to write this last article, it’s hard for me to be-lieve that a year has nearly passed, and what a tremen-dous year it has been……A year full of opportunities, chal-lenges, advancements, set-backs, colleagues, students, mentors, old friends and new friends. I can’t tell you how rewarding it has been to be President of your Association, and I thank you for the opportunity.
Over the year, I have harped on the fact that I believe apa-thy has been one of the single largest problems impacting our profession. My goal has been to challenge individuals to say, “Yes I Will,” and be involved. As I’ve stated, leader-ship has to come from a willingness to first be engaged. I’m happy to report that I believe our association and profes-sion have made great strides in being more engaged, yet there is still a tremendous amount to accomplish.
In my many years of involvement with the association, I’ve never experienced a more engaged and active Board of Directors. We have seen an increased activity with our lo-cal associations, as local leaders have stepped up to lead. Individuals not previously engaged with the association have stepped up to serve on or even chair committees. In addition to our standing committees (Organizational, Pro-fessional and Public Affairs), we have very involved and active special called committees, including Government Affairs, Budget and Audit, Contract Review, Policy Review, Past-Presidents, Health Information Technology, and Emergency Preparedness committees. The work these committees are doing is important and is strengthening our association and our profession.
I was inspired by the number of pharmacists and student pharmacists that attended the April 13 and 14 Advancing Pharmacy Practice Summit that KPhA helped sponsor. The event was hosted by UK COP’s Center for Advancement of Pharmacy Practice (CAPP), and in addition to KPhA, APSC, KY BOP, KSHP and SUCOP also sponsored the event. On a weekend in April with many competing hap-penings, almost 100 individuals came from different prac-
tice settings with different pharmacy experience to discuss and plan the path forward for pharmacy. By all accounts, the meeting was a success and proved that a coalition of pharmacists is possible, necessary and meaningful in order to advance our profession. I am not going to attempt to recap the meeting in this article, as the coalition will be de-veloping a report with the proceedings of the summit. How-ever, four broad categories were identified as important in advancing the profession. They include Communication, Redefining the Pharmacist’s Role, Education & Credential-ing and Practice Model.
Go visit Gloria and Lynn’s Kentucky Pharmacy History Mu-seum, and you’ll certainly see that our profession has not been a stagnant one. I don’t know a lot, but I know that change in our profession is destined to continue and it will continue to change at a pace unlike we have seen before. With the changing landscape of healthcare and the contin-ued introduction of technology, the practice of pharmacy, as it stands today, will not be the same tomorrow. Will we internally chart the course for our future, or will we allow outside sources to continue to shape our profession? I hope you will join the coalition in saying, “Yes We Will”, and get engaged. Your next opportunity to get involved with the discussion will occur June 14 at the KPhA annual meeting. Although being held during the KPhA meeting, it will be a continuation of the coalition discussion. Even if you haven’t registered for the meeting, we welcome your attendance and input during this discussion from 8 to 10 pm.
Having said that, I hope you have made plans to attend part – if not all – of the 134
th KPhA Annual Meeting. It will
be held at the Marriott Griffin Gate in Lexington, Ky., on June 13 – 16. If you have never attended, or if you haven’t attended in more than five years or maybe since you were a student, please consider attending. Our association moves forward only through your engagement!
I continue to want to hear from you. If you have a desire to be or questions about how to be involved, please email me at [email protected].
Lewis Wilkerson
PharmD, CGP
KPhA President
2011-2012
KPhA Social Media Links
www.facebook.com/KyPharmAssoc
www.twitter.com/KyPharmAssoc
President’s Perspective
May 2012
THE KENTUCKY PHARMACIST 4
APSC—HD Smith

May 2012
THE KENTUCKY PHARMACIST 5
134th KPhA Annual Meeting
Tentative Program Description
The Kentucky Pharmacists Association supports the pharmacists and pharmacy technicians of Kentucky by providing programming on up-to-date topics faced in pharmacy practice. Pharmacists and pharmacy techni-cians that practice in hospital/health systems, community, retail, consultant, long term care and insurance industries are the targeted audience for this meeting.
Since patient centered care is paramount, this convention targets topics such as diabetes, probiotics and new drugs, as well as topics related to improving patient medication use and safety and more! Attendees will get an update on pharmacy law; fraud, waste and abuse; and drug shortages.
As an ACPE accredited provider, the Kentucky Pharmacy Research and Education Foundation (KPERF) must ensure balance, independence, objectivity and scientific rigor in all its educational activities. Any per-son who is in a position to control the content or direction of a CPE activity must disclose any financial inter-est or other relationship with a commercial interest producing healthcare goods or services that have a di-rect bearing on the subject matter of the programming. Full Disclosure will be given verbally prior to the ac-tivity.
For successful completion of the Knowledge Based CPE activities and subsequent awarding of credit, each participant (Pharmacists and Technicians) must COMPLETE and TURN IN an activity
evaluation form TO THE MODERATOR at the end of each activity.
You will receive your certificates no later than six to eight weeks after the meeting.
Meal functions are open to all registered attendees; name tags required.
Registration is required to attend all continuing education programs.
Meeting attire is casual; President’s Reception and Ray Wirth Banquet are semi-formal.
The Kentucky Pharmacy Education & Research Foundation is accredited by The Accreditation Council for Pharmacy Education as a provider of continuing
Pharmacy education.

May 2012
THE KENTUCKY PHARMACIST 6
134th KPhA Annual Meeting
134th Kentucky Pharmacists Association Annual Meeting Registration Form
June 13-16, 2012 Marriott Griffin Gate, Lexington, KY
Please Type or Print the following:
__________________________________ ________ __________________________
First Name MI Last Name
____________________________________________________ PharmD RPh CPhT Other
Business Affiliation
_____________________________________________ _________________________ ______ _____
Street Address City State Zip
__________________________ _______________________________________________________________
Daytime Phone Email Address
Registration Fees: Please circle applicable Fee
Student- Free Member Non-Member Technician/Resident
Full Registration:
By June 1 $200 $375 $85 $25
After June 1 $250 $425 $110 $35
Single Day Registration:
By June 1 $105 $195 $55 $20
After June 1 $130 $220 $80 $30
Circle Day: Thursday Friday Saturday
Meal Events: Please indicate the total number that will be attending each meal event.
Welcome Luncheon: Thursday ____ yes ____ no _____ additional guest $30
Kroger Luncheon: Friday ____ yes ____ no _____ additional guest $30
Ray Wirth Awards Banquet: Friday ____ yes ____ no _____ additional guest $45
Luncheon: Saturday ____ yes ____ no _____ additional guest $30
Guest Name(s): ______________________________________________________________________________
Please include your guests’ name(s) if you have purchased additional event tickets
Registration $ _______ Additional Meal Tickets $ _______ Total Enclosed $_________
Credit Card Information: AMEX Discover MasterCard Visa
Number: ___________________________________________ Expiration Date:______________
NOTE: If billing address is different than above, please include on back of sheet, or separate sheet.
Please make checks payable to KPhA Annual Meeting.
Mail to: KPhA Annual Meeting 1228 US 127 South Frankfort, KY 40601.
For overnight accommodations: Contact Marriott Griffin Gate via the KPhA custom web reservation site at https://resweb.passkey.com/go/KYPharmacistAssoc, or call1-800-266-9432 and reference Group Code KY Pharmacists Association for the special rate of $129/night. Cut-off for this rate is May 22, 2012. Lodging rate includes parking on site and wireless internet access.
Special Assistance. If you require special assistance or diet to attend, please indicate need on back of this sheet, call 502.227.2303 or email [email protected].

May 2012
THE KENTUCKY PHARMACIST 7
134th KPhA Annual Meeting
7:30 AM Registration
7:30 AM to 9:00 AM Welcome Breakfast (Open to All)
Sponsored By Kentucky Health Information Exchange
8:30 AM to 10:30 AM Quality Medication in the Elderly
Demetra Antimisiaris, Pharm.D., CGP, FASCP, Assistant Professor, Di-
rector of Geriatric Pharmacotherapy, University of Louisville.
10:30 AM to 10:45 AM Refreshment Break
10:45 AM to 11:45 AM
Option 1
Medication Therapy Management Update
Matt Worthy, Pharm.D., Director of Professional and Clinical Services, Rx
Therapy Management.
Christine Richardson, PharmD., Clinical Pharmacist, Rx Therapy
Management
10:45 AM to 11:45 AM
Option 2
Lawsuit Protection
Luke Morgan, J.D., McBrayer, McGinnis, Leslie and Kirkland, PLLC
11:45 AM to 1:00 PM Lunch
Sponsored By University of Kentucky College of Pharmacy
1:00 PM to 2:00 PM CHEST Guidelines Update
Sarah F. White, Pharm.D., Assistant Professor, Clinical and
Administrative Sciences, Sullivan University College of Pharmacy
2:00 PM to 4:00 PM
Option 1
Overview of eHealth in KY: The Impact of HITECH and the Kentucky
Health Information Exchange
Polly Mullins-Bentley, Acting Director, Kentucky Health Information
Exchange
2:00 PM to 4:00 PM
Option 2
Clinical Pearls (Specific topics to be determined)
4:00 PM to 5:00 PM Situation Critical: Managing Drug Shortages
Rola Kaakeh, PharmD, CFPH, Assistant Professor and Founding
Director, International Center for Health Outcomes Policy, Sullivan
University College of Pharmacy
4:00 PM to 5:30 PM House of Delegates Opening Session
5:30 PM to 7:30 PM Grand Opening of Hall of Exhibitors
8 PM to 10 PM Follow-Up for Advancing Pharmacy Practice in Kentucky Summit
10 PM Hospitality Suite
Thursday, June 14, 2012 Tentative Schedule

May 2012
THE KENTUCKY PHARMACIST 8
134th KPhA Annual Meeting
7:30 AM to 9:00 AM Breakfast/Registration
8:00 AM to 9:00 AM Clinical Services in Community Pharmacy
Amy Thompson, PharmD,.Kroger Pharmacy, D5 Patient Care Specialist
9:00 AM to 9:30 AM Reference Committee
9:00 AM to 11:30 AM
10:15 AM to 10:30 AM
Hall of Exhibitors Open
Refreshment Break in Hall of Exhibitors
11:00 AM to Noon Fraud, Waste and Abuse
Molly Nicole Lewis, McBrayer, McGinnis, Leslie and Kirkland, PLLC
Noon to 1:45 PM KPhA Awards Lunch
Sponsored By Kroger
1:45 PM to 3:45 PM NASPA-NMA Student Pharmacist Self-Care Championship
Endowed by Procter & Gamble
3:45 PM to 4:00 PM Refreshment Break
4:00 PM to 5:00 PM
Option 1
Avoiding Liability Landmines for the Kentucky Pharmacist
Bruce A. Lafferre, Field Representative, Pharmacists Mutual Companies
4:00 PM to 5:00 PM
Option 2
Mythbusters Diabetes Management
Sarah Lawrence, PharmD, MA, Community Pharmacy PGY1 Resident,
Clinical Assistant Professor, College of Pharmacy, Sullivan University
6:00 PM to 7:00 PM President’s Reception
Sponsored By Rx Therapy Management
7:00 PM to 9:00 PM Ray Wirth Banquet
9 PM Hospitality Suite
Friday, June 15, 2012
Saturday, June 16, 2012
7:30 AM to 9:00 AM Continental Breakfast
Sponsored By American Pharmacy Services Corporation
8:00 AM to 10:00 AM New Drugs Update
Trish Rippetoe Freeman, R.Ph., Ph.D., Clinical Associate Professor and Director of Professional Practice Programs, University of Kentucky College of Pharmacy, Department of Pharmacy Practice and Science.
8:00 AM to 10:00 AM Closing House of Delegates
10:00 AM to 10:15 AM Refreshment Break
May 2012
THE KENTUCKY PHARMACIST 9
134th KPhA Annual Meeting
10:30 AM to 11:30 AM
Option 1
Demystifying Probiotics: Role in Health and Disease
Michel Farhat, PhD, Director of Global Professional and Techincal Affairs
at Procter and Gamble Healthcare
10:30 AM to 11:30 AM
Option 2
Preceptor update
Anne Policastri, Pharm.D., MBA, Assistant Director of Experiential Educa-
tion, UK College of Pharmacy.
11:45 AM to 1:00 PM Lunch
Sponsored by Sullivan University College of Pharmacy
1:00 PM to 2:00 PM Kentucky Legislative and Pharmacy Law Update
Ralph Bouvette, B.Sc.Pharm, Ph.D., J.D., Executive Vice-President, Amer-
ican Pharmacy Services Corporation.
2:00 PM to 3:00 PM Business Meetings for Academies
Saturday, June 16, 2012 Continued
Check the KPhA website for
registration forms and more
information updates on the
134th KPhA
Annual Meeting
www.kphanet.org/2012annualmeeting

May 2012
THE KENTUCKY PHARMACIST 10
134th KPhA Annual Meeting

May 2012
THE KENTUCKY PHARMACIST 11
134th KPhA Annual Meeting
$25 Academy for Consultant Pharmacist Member $15 Academy for Compounding Pharmacist Member
CONTACT ME—I want to be involved with KPhA!
Send to: Kentucky Pharmacists Association For more information: www.kphanet.org 1228 US 127 South Phone: 502-227-2303 Frankfort, KY 40601 Fax: 502-227-2258
The Kentucky Pharmacists Association Invitation to Membership Name
Home Address
City/State/Zip
College & Year of Graduation
Home Phone
Home Fax
License Number
Business Name
Business Address
City/State/Zip
Business Phone
Business Fax
Preferred Mailing Address Home Office Charge to my: American Express Discover _MasterCard VISA
Card#
Card Expiration Date
Signature
Membership Investment:
$210 Active Member (licensed in KY) $315 Joint Member (both spouses licensed in KY)
$210 Associate Member (Licensed only in other state or non-pharmacist)
$120 Retired Member $180 Joint Retired $50 Certified Technician
$70 1st Year Tiered $140 2nd Year Tiered

May 2012
THE KENTUCKY PHARMACIST 12
SUMMARY OF PHARMACY ISSUES 2012 Kentucky General Assembly
Prepared by Jan Gould, Gay Dwyer, Bob McFalls and Laura Leigh Goins
Overview: KPhA gratefully acknowledges the en-gagement of pharmacist members throughout the Commonwealth who made legislative advocacy a per-sonal priority during the 2012 regular and special ses-sions. Pharmacists were united in your resolve to make a difference by conducting regular telephone calls and engaging in one-on-one conversations with your state senators and representatives. From the Government Affairs Committee, Chair Richard Slone, and the entire Board of Directors: Give yourself and your colleagues a well-deserved “pat on the back” for your due diligence and commitment. Your advocacy continues to make a difference! KPhA acknowledges and thanks our advocacy part-ners for this session: American Pharmacy Coopera-tive, Inc., American Pharmacy Services Cooperative, EPIC Pharmacies, Inc., Kentucky Independent Phar-macy Alliance, Kentucky Retail Federation National Association of Chain Drug Stores, National Communi-ty Pharmacists Association and HD Smith. Lawmakers adjourned the 2012 General Assembly without resolving two key issues that caused Gover-nor Steve Beshear to immediately call legislators into Special Session on April 16. The legislature ad-journed on April 12 without enacting a budget to im-plement the state road plan and without acting on comprehensive anti-prescription drug abuse legisla-tion. Both issues were on the call and addressed dur-ing the Special Session. KPhA’s “watch list” for the 2012 Session included more than 30 bills and resolutions. Working with its partners and through a concerted effort by engaged pharmacists, KPhA was successful in making signifi-cant changes to the state’s pharmacy audit law, stopped efforts by physicians’ assistants to obtain the ability to dispense drugs and had significant input into the deliberations on the pain clinic/prescription drug abuse issue. While the legislature failed to pass legis-lation addressing the problems with Medicaid man-aged care, the session provided KPhA with many op-portunities to educate legislators about issues with the managed care organizations that now serve the ma-jority of the Medicaid population. These opportunities
will continue during the interim and into the next ses-sion. The following summary provides a narrative regarding the activity on some of the major issues affecting pharmacists that were considered during this year’s legislative session. Visit www.lrc.ky.gov to access complete summaries of the bills prepared by legisla-tive staff on all action taken on the measures, as well as to review the full text of individual bills and resolu-tions. Bills enacted during the 2012 Regular Session will take effect on July 12 unless a specific effective date was included in the legislation or the legislation contained an emergency clause making it effective as soon as it was signed by the Governor. The compre-hensive anti-prescription drug abuse bill enacted in the 2012 Extraordinary Session takes effect July 20. Prescription Drug Abuse/Pain Clinics: Despite spending considerable time this session discussing the issue of prescription drug abuse, lawmakers failed to reach a compromise on legislation to address the issue before adjourning the 2012 Kentucky General Assembly. The issue, however, was on the agenda of the Special Session called by Governor Beshear which began on April 16 where a much-revised ver-sion of HB 1 passed on April 20. Background: While many proposals were filed ad-dressing the prescription drug abuse issue, including the regulation of pain clinics, the major focus was on HB 4 sponsored by House Speaker Greg Stumbo (D-Prestonsburg). As the bill passed the House, it re-quired pain clinics to be owned by physicians or ad-vanced practice registered nurses and placed re-strictions on the dispensing of controlled substances by prescribers. The bill also made significant changes to the state’s electronic prescription reporting system (KASPER). Among the changes was a provision that moved the administration of KASPER from the Cabi-net for Health and Family Services to the Office of Attorney General. It also called for an assessment on prescribers and pharmacists to fund the program and required pharmacists to report data to the KASPER system daily rather than weekly.
Kentucky General Assembly Summary

May 2012
THE KENTUCKY PHARMACIST 13
The Senate passed an amended version of the bill retaining many of the original provisions but also mak-ing some significant changes. The Senate stripped the language in the original bill that established a fee on prescribers and pharmacists to fund KASPER. It also delayed the effective date for the accelerated re-porting of KASPER data until July 1, 2013. Additional-ly, the Senate added several provisions taken from SB 2 that further regulated the activities of pain clin-ics. The Senate passed the revised version of the bill on March 28 but the House failed to concur with the Senate changes. Ultimately the bill wound up in a free conference committee where legislators tried to work out the differences between the House and Senate versions. In the waning days of the session, several draft com-promise proposals were put forward. The initial com-promise included a fee on prescribers and pharma-cists to fund KASPER. The fee, however, was set at $50 annually with allowances for annual adjustments based on inflation. It retained most of the provisions that the Senate added to regulate pain clinics and also retained the requirement that pharmacists enter data into the KASPER system daily rather than on the current weekly schedule with the delayed effective date. The draft added a new provision that placed re-strictions on the dispensing of certain controlled sub-stances by prescribers. Additionally, it prohibited pharmacies from dispensing more than a 30-day sup-ply of Schedule II drugs, Schedule III drugs containing hydrocodone and drugs containing alprazolam, clonazepam or diazepam. This version was never offi-cially acted upon by either chamber. On the last day of the session, another draft compro-mise was put forth that removed the fee language and made other slight modifications to the bill. The legisla-ture adjourned without considering the proposal. During the course of the discussion on prescription drug abuse, KPhA was instrumental in seeking changes to various proposals that surfaced. An early proposal would have required pharmacists to obtain KASPER reports before dispensing any controlled substance. Another proposal would have required pharmacists to obtain photo identification from per-sons picking up controlled substance prescriptions. KPhA effectively worked with lawmakers and its part-ners to get these proposals off the table. Outcome: HB 1 passed the Kentucky legislature as its last act during the Special Session that ended on April 20. In noting its passage, President Lewis D. Wilkerson noted, “KPhA is gratified to see the im-portant issue of prescription drug abuse addressed,
along with the fact that legislators were responsive to hearing and addressing concerns from the pharmacist community as well as those from other provider groups. We remain committed to continuing our work with legislators and other healthcare providers to combat prescription drug abuse, and pharmacists will continue to assure appropriate medication use for our patients." Highlights of the legislation include: The KASPER program is retained in the Cabinet
for Health and Family Services rather than being moved to the Office of Attorney General as origi-nally proposed.
The fee on pharmacists and prescribers was elimi-nated.
Language clarifying who must register for KASPER was added in the Senate.
Language was removed from the original bill tying registration to DEA permits.
Language was removed from the original bill that would have allowed significantly broader access to KASPER reports by law enforcement person-nel.
Pain clinics operating today will be grandfathered from the requirement that pain clinics be owned by physicians.
HB 1 establishes new rules for the operation of pain clinics and, in the future, requires that they be owned by physicians. It requires physicians to obtain KASPER reports before prescribing controlled sub-stances under certain circumstances and limits dis-pensing by prescribers. It requires that pharmacists who are authorized to dispense controlled substances register for a KASPER account but does not mandate that pharmacists obtain KASPER reports. The provi-sion requiring daily rather than weekly reporting of KASPER data by pharmacies is included in the bill, but the effective date for this provision is delayed until July 1, 2013. Also, the penalties for failure to report to KASPER were reduced. Pharmacy Audits: HB 349, a KPhA-backed proposal to revise Kentucky’s pharmacy audit law, was signed into law by Governor Beshear after passing both chambers unanimously. The bill, sponsored by Repre-sentative Tommy Thompson (D-Owensboro), amends Kentucky’s current audit law to address continuing problems faced by pharmacists with audits conducted by insurers and pharmacy benefit managers. HB 349 specifies that an auditing entity may not recoup pay-ments because of clerical errors or omissions, unless there is evidence of fraud or an actual overpayment has been made. Under the provisions of HB 349, re-coupment of overpayments is limited to the actual amount of the overpayment and would not include the
Kentucky General Assembly Summary

May 2012
THE KENTUCKY PHARMACIST 14
dispensing fee. The bill also limits the length of time an auditing entity can require a pharmacy to keep rec-ords. The bill limits record retention to two years or the period of time required by state or federal law.
Another significant provision of HB 349 is the removal of the exemption for managed care organizations (MCOs) serving the Medicaid population. The current law exempted these entities from the audit re-strictions. With the expansion of managed care in the Medicaid program late last year, private companies are now responsible for providing benefits to the ma-jority of the Medicaid population. Implementing improvements to Kentucky’s pharmacy audit law was a legislative priority established by the 2011 KPhA House of Delegates and pharmacists’ ma-jor achievement in this legislative session. Medicaid Managed Care: Despite multiple hearings on the problems with the implementation of managed care for Medicaid recipients, the legislature did not act on any significant legislation addressing Medicaid managed care. Lawmakers were reluctant to inter-vene, citing concerns over the potential budget impact if the Medicaid managed care program was revised. A comprehensive proposal to require the Medicaid man-aged care organizations (MCOs) to comply with pro-vider and patient protections in the insurance code (HB 566) was introduced. Despite being supported by a broad range of patient and provider groups, includ-ing KPhA, the proposal never received a vote in the House. Several bills relating to the pharmacy portion of the managed care program were filed, but all of them ulti-mately stalled. Two bills requiring the MCOs to charge uniform copayments (HB 262 and SB 137) received considerable discussion during the session but both died in the Senate after the MCOs testified that the measures would cause them to open their contracts with the state which would result in additional Medi-caid expenditures. The bills would have increased pharmacy reimbursement by allowing pharmacies to keep the copayments in addition to the contractual reimbursement. A proposal that established guide-lines for the establishment of “maximum allowable cost” pricing mechanisms for not only the MCOs but for all PBMs (SB 125) was introduced. The bill was strongly opposed by PBMs, health insurers, the MCOs and payor groups. SB 125 received a hearing in the Senate Health and Welfare Committee and was approved by the committee. It was later recommitted to the Senate Appropriations and Revenue Commit-tee where it died. Another bill affecting “maximum al-
lowable cost” pricing was filed in the House but failed to receive a hearing.
Significant problems remain for both health care pro-viders and patients in the new Medicaid managed care environment. The issue will no doubt be a major topic of discussion during the interim and KPhA will continue to keep legislators informed about the prob-lems pharmacists are experiencing with the managed care organizations. Therapeutic Shoes: HB 403, a bill that clarified that pharmacy technicians and pharmacist interns can continue to assist pharmacists in the fitting of thera-peutic shoes for diabetics died in the Senate Licens-ing, Occupations and Administrative Regulations Committee. The measure was introduced by Repre-sentative Leslie Combs (D-Pikeville) to address a problem that surfaced with the existing orthotics, pe-dorthics and prosthetics licensing law that is sched-uled to go into effect in 2013. Although the law allows pharmacists to fit therapeutic shoes for diabetics, it restricts the ability of pharmacy personnel to assist pharmacists in the process. Despite unanimously passing the House, the bill never received a commit-tee hearing after a member of Senate leadership ex-pressed concerns about the proposal. Medicaid Fraud: A bill sponsored by House Speaker Greg Stumbo (D-Prestonsburg) proposing to establish the “Kentucky False Claims Act” cleared the House but died in the Senate Judiciary Committee. HB 401 allowed a third party (“whistleblower”) to bring an ac-tion for fraud against anyone doing business with the state. If fraud was found, the whistleblower was enti-tled to a portion of the money recovered. Representa-tive Jimmy Glenn (D- Owensboro) filed a similar pro-posal (HB 51) early in the Session. Glenn’s bill was limited to Medicaid providers and did not receive a hearing in the House committee to which it was as-signed. KPhA was part of a health care provider coali-tion that mounted an aggressive campaign opposed to these bills.
Physicians’ Assistants: Senator Tom Buford (R-Nicholasville) introduced a bill to permit physicians’ assistants to prescribe controlled substances as des-ignated by a supervising physician. SB 96 also would have allowed PAs to dispense all legend drugs. After KPhA objected to allowing PAs to dispense drugs, the sponsor agreed to remove the dispensing language from the bill before it received further consideration. SB 96 received a hearing in the Senate Judiciary Committee but no vote was taken, ending considera-tion of the proposal for the session.
Kentucky General Assembly Summary

May 2012
THE KENTUCKY PHARMACIST 15
PSE Regulation: A compromise proposal restricting the sale of products containing pseudoephedrine (PSE) passed the legislature this year and was signed into law by the Governor. SB 3 allows an individual to purchase up to 7.2 grams of PSE per month with a maximum annual limit of 24 grams without a prescrip-tion. Sales limits would be monitored by the current MethCheck (NPLEX) system. Once that amount is exceeded, a prescription would be required. Gel caps and liquid preparations are exempted. The bill also incorporates provisions of other bills introduced this session that would block sales of PSE to persons convicted of meth-related offenses. The regulation of PSE has been a much-debated issue for several years as legislators grappled with the growing prob-lem of illegal methamphetamine production. SB 3 was one of many bills introduced this session that dealt with the issue.
DME Licensing: Anoth-er new licensing re-quirement was passed in HB 282 that calls for the Board of Pharmacy to license providers of home medical equip-ment and services. Un-less the equipment and related services are provided through a sep-arate legal entity, li-censed pharmacies that sell, rent or lease dura-ble medical equipment (DME) are not required to obtain the new li-cense. Neither are equipment manufacturers or wholesale distributors that do not deal directly with the patient. The bill authorizes licensees to provide home medical equipment and services that require a pre-scription or order from a practitioner. Prescription Drug Disposal: Representative Joni Jenkins (D-Shively) filed legislation (HB 238) estab-lishing a disposal program for unused prescription drugs. The bill easily passed the House but died in the Senate Veterans, Military Affairs and Public Pro-tection Committee. The bill called for the Energy and Environment Cabinet to work with local governments to set up collection points for unused prescription drugs in unopened containers. APRN Prescribing: The APRN association sought legislation this session to eliminate the requirement
that APRNs have a collaborative practice agreement with a physician in order to prescribe non-controlled drugs. While the bill (SB 187) never received a hear-ing in the Senate Judiciary Committee, its provisions were added to HB 512 in the House. HB 512 passed the House but died in the Senate Judiciary Committee as well.
A competing proposal backed by the Kentucky Medi-cal Association was also introduced but likewise failed to pass. SB 190 sought to place additional require-ments on APRNs wishing to prescribe drugs. It out-lined specific elements required to be in collaborative practice agreements and gave the Board of Medical Licensure more oversight of these agreements, Mail Order Pharmacy: The House unanimously
adopted HR 198 urging the Personnel Cabinet, the Kentucky Retire-ment System and the Kentucky Teachers’ Re-tirement System to evaluate the policies of the mail order pharma-cy benefit programs they provide to make sure the policies are compliant with state laws requiring that local pharmacies have the opportunity to partici-pate. As a simple reso-lution, it required no ac-tion by the Senate.
Other Pharmacy Issues: Legislation to place re-strictions on e-prescribing systems has been signed by the Governor (SB 144). The bill prohibits e-prescribing systems from being designed to limit a physician’s choice of drug and calls for the state to incorporate national standards once they have been developed. The Governor also signed SB 114, a bill placing restrictions on the use of step therapies for drugs by insurance companies. The legislature failed to pass HB 377, a bill essentially prohibiting generic substitution for tamper-resistant opioids. It was ap-proved by the House Health and Welfare Committee but was later recommitted to the House Appropria-tions and Revenue Committee. A measure to prohibit the sale of products containing dextromethorphan as the only active ingredient to anyone under age 18 was introduced in the House but HB 106 was not consid-ered in the House Judiciary Committee.
Kentucky General Assembly Summary

May 2012
THE KENTUCKY PHARMACIST 16
May 2012 CE-Compounding for Scalp
Compounding for Scalp Disorders
and Conditions By: Y. Pramar, Ph.D., Professor of Pharmaceutics
Xavier University of Louisiana, College of Pharmacy, New Orleans, Louisiana.
Reprinted with permission of the author and the Louisiana Pharmacists Association where this
article originally appeared. This activity may appear in other state pharmacy association journals.
There are no financial relationships that could be perceived as real or apparent conflicts of interest.
Universal Activity # 0143-9999-12-005-H04-P
1.5 Credit Hours (0.15 CEUs)
Goals: The goals of this article are to provide information on the physiology and disorders of the scalp, and typical
drug therapy used to treat these disorders.
Objectives: At the conclusion of this lesson, the reader should be able to:
1. Discuss the physiology of the scalp and the function of the sebum, sweat glands and pores.
2. List at least five disorders/conditions of the scalp.
3. Describe different treatment approaches used in scalp disorders.
4. Become familiar with various formulations used in the treatment of seborrheic dermatitis, dandruff, psoriasis, hair
loss, lice and ringworm.
KPERF offers all
CE articles to
members online at
www.kphanet.org
Introduction
Scalp disorders may be painful, annoying, unsightly
and embarrassing. Scalp problems may require short-
term treatment, but many of them need long-term
therapy over months, and sometimes years. Com-
pounding pharmacists have a significant role in
achieving successful therapeutic outcomes in this
emerging field.
Anatomy and Physiology
The scalp consists primarily of the skin, sweat glands,
sebaceous glands, hair shafts and hair. When these
appendages are not functioning properly in harmony
with one another, various scalp disorders can occur.
Scalp: The scalp is the portion of the body consisting
of skin and subcutaneous tissue normally containing
hair that covers the neuro-cranium. It is especially rich
in blood vessels; therefore, profuse bleeding may oc-
cur with scalp injuries. The functions of the scalp
(skin) include protection and excretion. It secretes
metabolic waste materials and toxins in order to rid
the body of them. It also secretes sweat to cool the
body, and sebum to protect the skin.
Skin: Each layer of the skin (epidermis, dermis, sub-
cutaneous) has a specific function. Included in the
skin are the sebaceous glands that produce sebum
and secrete it through the sebaceous ducts into hair
follicles where it migrates to the surface of the skin.
This flow of sebum removes dead skin cells that flake
off from inside the hair follicle. Sebum consists of fatty
acids and other substances and protects the skin by
reducing the evaporation of water from the skin and
blocks the penetration of excess water into the skin.
This sebum is one of two constituents making up the
lipid film present on the skin surface, the other being
the lipids of the epidermal cells.
Pores: The pores in the skin are where the hair folli-
cles reside. The pore size is related to sebaceous
gland size. Pores enlarge to accommodate a greater
oil flow. Acne caused by blocked pores often clears
up when the pores enlarge allowing unimpeded
movement of sebum through the pore.
Sweat Glands: Sweat glands consist of a single tube,
the lower portion of which is coiled into a ball and the
upper part (the duct) opens onto the surface of the
skin. There are two types of sweat glands, the eccrine

May 2012
THE KENTUCKY PHARMACIST 17
May 2012 CE-Compounding for Scalp
and the apocrine. The eccrine sweat glands, distribut-
ed all over the body, primarily regulate body tempera-
ture and eliminate toxic substances and waste prod-
ucts; the perspiration is clear and consists of traces of
salt, carbohydrates, protein and oil. The sweat they
produce is primarily odorless. The apocrine sweat
glands are primarily in the underarm area, around the
nipples and in the genital area. They are stimulated
by the same hormones that stimulate hair growth in
the underarms and genital area. The fluid they se-
crete is milky and rich in organic material that is sub-
ject to bacterial decay, causing body odor. The hair
entraps both sweat and bacteria.
Sebum: When the sebum gets stuck in the pores,
whiteheads, blackheads, papules, pimples and cysts
can ultimately occur. It is a result of the sebum getting
blocked during its transport and clumping with dead
skin cells, being acted upon by bacteria and ultimately
blocking the opening to the skin surface. If pressure
builds up, pustules and cysts result.
Hair: Hair grows on the scalp and each hair filament
originates in a deep hair follicle which penetrates into
the dermis. At the base of the follicle is the papilla
which is the center of hair growth containing the capil-
laries and nerves that supply the hair. As new cells
are formed and older cells are pushed upward, they
gradually die and harden into a hair shaft, consisting
of two layers, the cuticle and cortex. The outer layer,
the cuticle, consists of flat, colorless, overlapping
cells. The cortex contains pigment and a tough pro-
tein called keratin, forming the bulk of the hair shaft.
Coarse hair, as on the scalp, contains an additional
inner core called the medulla. The hair is lubricated by
sebaceous glands that are located in the hair follicle.
In general, human scalp hair is shed every two to four
years; body hairs are shed more frequently.
Hair growth: Hair growth is cyclical, consisting of three
phases. The growing phase is the “Anagen” phase;
about 90 percent of scalp hairs are in the anagen
phase at any point in time. On a daily basis, about 50
to 100 scalp follicles go into the resting phase, or the
“Catagen” phase, which involves 1 percent of the
hairs daily. The shedding phase is the “Telogen”
phase and approximately 10-20 percent of scalp hairs
may be in the telogen phase at any point in time.
SCALP DISORDERS AND THEIR TREATMENT
Seborrheic Dermatitis and Dandruff
Description: Seborrheic dermatitis is an acute or
chronic papulosquamous dermatitis presenting with
dry scales and underlying erythema. In some cases
pruritis is present. Dandruff occurs when there is a
mild scaling without any erythema, and can occur if
the scalp is dry or oily. It may be the result of several
factors, including hormonal imbalance, impaired met-
abolic nutrition, diet, tension, increased bacterial and
fungal activity, biochemical changes in the scalp, the
use of topical medications and cosmetics. Seborrheic
dermatitis occurs when there is general erythema
without tight, thick, silvery scales. Psoriasis is evi-
denced by the presence of well-demarcated red
plaques.
Treatment: Routine treatment for seborrhea of the
scalp involves a shampoo that may contain tar, zinc
pyrithione or selenium, used daily if necessary. A ke-
toconazole 1 percent or 2 percent shampoo can be
used twice weekly. If needed, solutions or lotions of
topical corticosteroids can be used twice daily.
Psoriasis
Description: Psoriasis is an inflammatory skin disease
that may be based upon a genetic predisposition.
When the skin is injured or irritated, it tends to induce
lesions of psoriasis at the site. There are several vari-
ants of psoriasis, with the most common being the
plaque type. Psoriasis presents as silvery scales on
bright red, well-demarcated plaques that may be ac-
companied by itching.
Treatment: The treatment selected for psoriasis of the
scalp is based on its extent and severity. Therapy can
be initiated using a corticosteroid preparation. Other
measures include tar preparations, such as coal tar
solution (LCD, Liquor Carbonis Detergens), anthralin,
calcipotriene and tazarotene. Treatment can be initiat-
ed with a tar shampoo used daily. For thick scales on
the scalp, a 6 percent salicylic acid gel, or a phenol :
mineral oil : glycerin mixture can be used. Alternative-
ly, fluocinolone acetonide 0.01 percent in oil can be
applied under a shower cap at night followed by tar
shampoo in the morning. Corticosteroids such as tri-
amcinolone, fluocinolone, betamethasone dipropio-

May 2012
THE KENTUCKY PHARMACIST 18
May 2012 CE-Compounding for Scalp
nate, fluocinonide, amcinonide, or clobetasol in solu-
tion form can be used twice daily.
Hair Loss
I. Description: Pattern, or androgenetic baldness, is
the most common form of alopecia. It is of genetic
predetermination with the earliest changes occurring
on the front sides of the scalp and at the crown of the
skull. The extent of hair loss is variable and unpredict-
able, but may be experienced by approximately 80
percent of all men.
Treatment: A 5 percent solution of minoxidil alone or
in combination with other active ingredients can be
used in both male and female patients, generally
twice daily. Those that respond are usually less than
five years into their hair loss.
II. Description: Alopecia areata is believed to be the
result of an imuunologic process. Typically, there are
patches that are smooth, without scarring. Tiny hairs,
generally 2-3 mm in length, may be seen. In some
cases, all the scalp hair may eventually be involved.
Alopecia areata is a self-limiting disease where there
may be complete re-growth of hair in about 80 per-
cent of cases. In some cases, mild alopecia areata is
resistant to therapy.
Treatment: Severe forms may be treated by systemic
corticosteroids; however, recurrences generally occur
when therapy is discontinued. Corticosteroids can
also be administered intralesionally; for example, tri-
amcinolone acetonide 2.5 to 10 mg/mL can be inject-
ed in aliquots of 0.1 mL every 1 to 2 cm in the in-
volved areas. The total dose should not exceed 30
mg per month for adults. Another treatment includes
daily use of anthralin 0.5 percent ointment.
Other therapeutic approaches involve the use of topi-
cal diphenylcyclopropenone and squaric acid dibutyl
ester. These agents serve to sensitize the skin; this is
followed by application of progressively weaker con-
centrations designed to produce a slight dermatitis.
This results in hair re-growth in 3 to 6 months in some
patients.
III. Description: Drug-induced alopecia may result
from thallium, excessive vitamin A, retinoids, antimi-
totic agents, anticoagulants, antithyroid drugs, oral
contraceptives, trimethadione, allopurinol, proprano-
lol, indomethacin, amphetamines, salicylates, gen-
tamicin and levodopa. Drug-induced alopecia is very
disconcerting to the patient, but it is reversible when
the causative agent is discontinued.
Treatment: No real treatment is indicated in such cas-
es, other than discontinuation of the causative agent.
Lice
Description: Pediculus humanus var capitis (the head
louse, approximately 3-4 mm long) is the causative
agent for pediculosis of the skin of the scalp. It is pre-
sented as pruritis with excoriation and the presence
of nits on hair shafts; they are easiest to see above
the ears and at the nape of the neck. Head lice can
be spread by individuals sharing hats or combs and it
is epidemic among children of all socioeconomic clas-
ses, especially in elementary schools. Adults in close
contact with children may also get the infestation.
Treatment: Options for treating head lice include iver-
mectin 0.8 percent lotion, malathion 0.5 percent or 1
percent lotion, permethrin 1 percent cream rinse and
pyrethrins 0/17 percent to 0.33 percent. The ivermec-
tin lotion is left on for 8 to 12 hours prior to rinsing off.
The malathion is applied to the scalp and left on for
about 12 hours. The permethrin cream rinse is left on
from 30 minutes to 8 hours prior to rinsing off and
treatment is repeated in one week. Following applica-
tion of these preparations, it is important to meticu-
lously remove the nits with a fine-tooth comb.
Ringworm
Description: Ringworm presents as a ring-shaped le-
sion with an advancing scaly border and central
cleared area, or as scaly patches with a distinct bor-
der on the skin or scalp. The affected areas may also
itch. Trichophyton rubrum is the most common causa-
tive agent.
Treatment: Many of the topical antifungal agents can
be used, including miconazole, clotrimazole, ketocon-
azole, econazole, sulconazole, oxiconazole, ciclopir-
ox, butenafine and terbinafine. Topical dosage forms
commonly used include creams, solutions and gels.
If the product is expected to be exposed to a wet en-
vironment, an ointment would be more appropriate.
Treatment should be continued up to two weeks after
symptoms have resolved.
May 2012
THE KENTUCKY PHARMACIST 19
May 2012 CE-Compounding for Scalp
References
1. ‘A practical guide to contemporary pharmacy prac-
tice’ by Judith E. Thompson, Third Edition. Lip-
pincott, Williams & Wilkins. 2009
2. ‘Pharmaceutical Dosage Forms and Drug Delivery
Systems’ by Howard C. Ansel, Nicholas G. Popo-
vich, and Loyd V. Allen, Jr. Ninth Edition. Lip-
pincott, Williams & Wilkins. 2011.
3. ‘The Art, Science, and Technology of Pharmaceu-
tical Compounding’ by Loyd V. Allen, Jr. Third Edi-
tion. American Pharmacists Association. 2008.
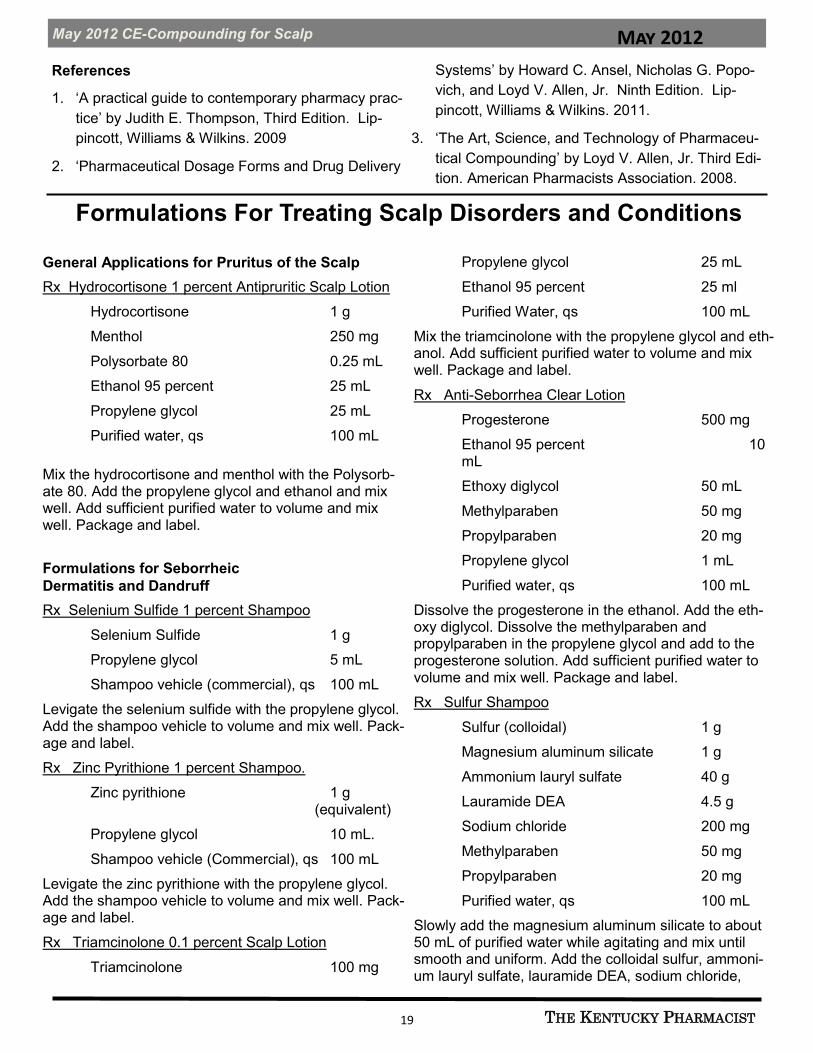
General Applications for Pruritus of the Scalp
Rx Hydrocortisone 1 percent Antipruritic Scalp Lotion
Hydrocortisone 1 g
Menthol 250 mg
Polysorbate 80 0.25 mL
Ethanol 95 percent 25 mL
Propylene glycol 25 mL
Purified water, qs 100 mL
Mix the hydrocortisone and menthol with the Polysorb-ate 80. Add the propylene glycol and ethanol and mix well. Add sufficient purified water to volume and mix well. Package and label.
Formulations for Seborrheic
Dermatitis and Dandruff
Rx Selenium Sulfide 1 percent Shampoo
Selenium Sulfide 1 g
Propylene glycol 5 mL
Shampoo vehicle (commercial), qs 100 mL
Levigate the selenium sulfide with the propylene glycol. Add the shampoo vehicle to volume and mix well. Pack-age and label.
Rx Zinc Pyrithione 1 percent Shampoo.
Zinc pyrithione 1 g (equivalent)
Propylene glycol 10 mL.
Shampoo vehicle (Commercial), qs 100 mL
Levigate the zinc pyrithione with the propylene glycol. Add the shampoo vehicle to volume and mix well. Pack-age and label.
Rx Triamcinolone 0.1 percent Scalp Lotion
Triamcinolone 100 mg
Propylene glycol 25 mL
Ethanol 95 percent 25 ml
Purified Water, qs 100 mL
Mix the triamcinolone with the propylene glycol and eth-anol. Add sufficient purified water to volume and mix well. Package and label.
Rx Anti-Seborrhea Clear Lotion
Progesterone 500 mg
Ethanol 95 percent 10 mL
Ethoxy diglycol 50 mL
Methylparaben 50 mg
Propylparaben 20 mg
Propylene glycol 1 mL
Purified water, qs 100 mL
Dissolve the progesterone in the ethanol. Add the eth-oxy diglycol. Dissolve the methylparaben and propylparaben in the propylene glycol and add to the progesterone solution. Add sufficient purified water to volume and mix well. Package and label.
Rx Sulfur Shampoo
Sulfur (colloidal) 1 g
Magnesium aluminum silicate 1 g
Ammonium lauryl sulfate 40 g
Lauramide DEA 4.5 g
Sodium chloride 200 mg
Methylparaben 50 mg
Propylparaben 20 mg
Purified water, qs 100 mL
Slowly add the magnesium aluminum silicate to about 50 mL of purified water while agitating and mix until smooth and uniform. Add the colloidal sulfur, ammoni-um lauryl sulfate, lauramide DEA, sodium chloride,
Formulations For Treating Scalp Disorders and Conditions

May 2012
THE KENTUCKY PHARMACIST 20
May 2012 CE-Compounding for Scalp
methylparaben and propylparaben and mix well. Add sufficient purified water to volume and mix well. Pack-age and label.
Rx Phenol, Glycerin and Mineral Oil Shake Lotion
Phenol 1 g
Glycerin 10 mL
Purified water 20 mL
Methylparaben 50 mg
Propylparaben 20 mg
Mineral Oil, Light, qs 100 mL
Dissolve the phenol, methylparaben and propylpara-ben in the glycerin. Add the purified water and mix well. Add the mineral oil and agitate. This is not an emulsion, but is an immiscible shake-type lotion.
Formulations for Psoriasis
Rx Coal Tar Shampoo
Coal tar solution 2.8 g
Polysorbate 80 5 mL
Shampoo vehicle (commercial), qs 100 mL
Mix the coal tar solution with the polysorbate 80. In-corporate the shampoo vehicle and mix well. Pack-age and label.
Rx Coal Tar and Salicylic Acid Scalp Lotion
Coal tar solution 10 mL
Salicylic acid 6 g
Polysorbate 80 1 mL
Ethanol 95 percent 20 mL
Propylene glycol, qs 100 mL
Mix the polysorbate 80 with the coal tar solution. Mix the salicylic acid with the alcohol and about 60 mL of the propylene glycol. Add the coal tar solution mixture slowly with mixing to the propylene glycol mixture. Add sufficient propylene glycol to volume and mix well. Package and label.
Rx Anthralin 1 percent and Coal Tar 1 percent Ointment
Anthralin 1 g
Coal tar 1 g
Polysorbate 80 2 g
Aquaphor, qs 100 g
Mix the coal tar with the polysorbate 80 and incorpo-rate the anthralin. Incorporate into the Aquaphor and mix until uniform. Package and label.
Rx Anthralin 1 percent Medication Stick
Anthralin 200 mg
Polyethylene glycol 3350 6.5 g
Polyethylene glycol 300 15 mL
Mix the polyethylene glycols together by heating to a temperature of about 550C. Incorporate the anthralin and mix well. Pour into medication stick molds and allow to cool. Package and label.
Rx Calcipotriene 0.003 percent Lotion
Calcipotriene 0.005 percent Cream 60 g
Propylene glycol, qs 100 mL
Mix the commercial calcipotriene 0.005 percent cream with sufficient propylene glycol to make 100 mL. Package and label.
Rx Fluocinolone Acetonide 0.01 percent in Oil
Fluocinolone acetonide 10 mg
Vegetable oil, qs 100 mL
Incorporate the fluocinolone acetonide into a vegeta-ble oil, such as sesame oil, or almond oil, and mix well. Package and label.
Formulations for Hair Loss
Rx Minoxidil 5 percent and Retinoic Acid 0.01 percent Scalp Lotion
Minoxidil 5 g
Retinoic acid 10 mg
Propylene glycol 20 mL
Ethanol 95 percent, qs 100 mL
Mix the minoxidil and retinoic acid with the propylene glycol. Add sufficient ethanol to volume and mix well. Package and label.
Rx Minoxidil 2 percent and Finasteride 0.1 percent Scalp Lotion
Minoxidil 2 g
Finasteride 100 mg
Propylene glycol 20 mL
Ethanol 95 percent, qs 100 mL
Pulverize the required number of finasteride tablets and mix with about 75 mL of ethanol in a covered con-
May 2012
THE KENTUCKY PHARMACIST 21
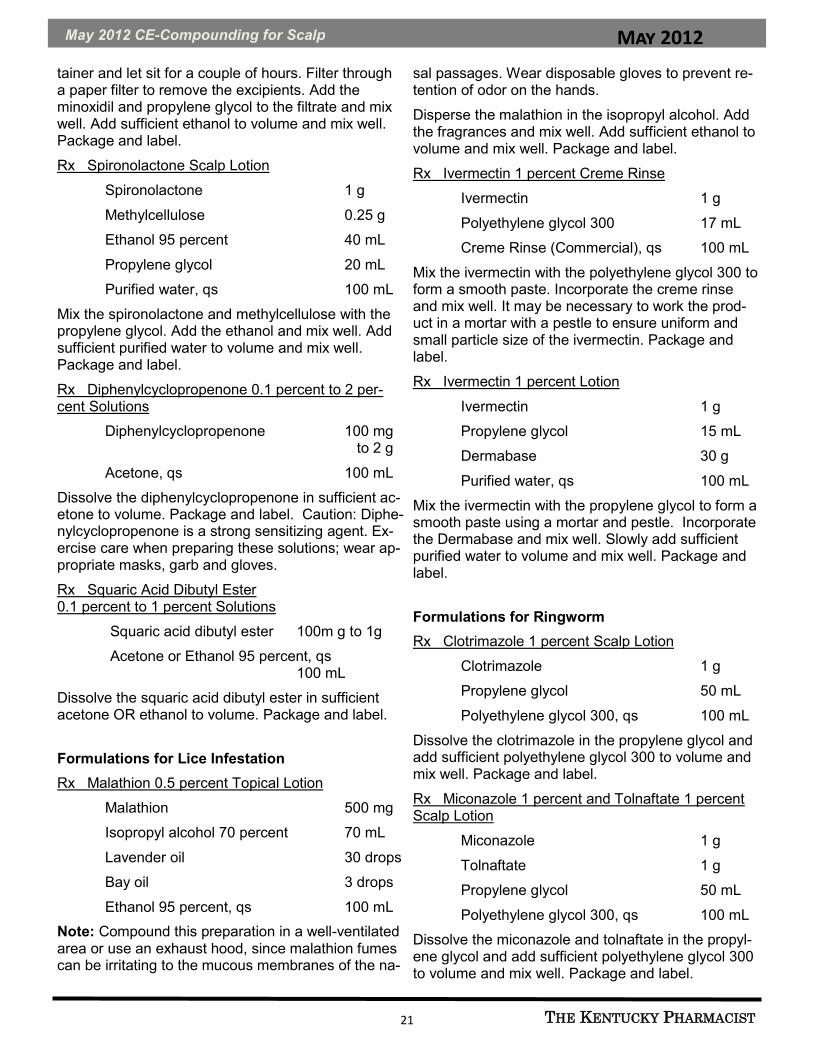
May 2012 CE-Compounding for Scalp
tainer and let sit for a couple of hours. Filter through a paper filter to remove the excipients. Add the minoxidil and propylene glycol to the filtrate and mix well. Add sufficient ethanol to volume and mix well. Package and label.
Rx Spironolactone Scalp Lotion
Spironolactone 1 g
Methylcellulose 0.25 g
Ethanol 95 percent 40 mL
Propylene glycol 20 mL
Purified water, qs 100 mL
Mix the spironolactone and methylcellulose with the propylene glycol. Add the ethanol and mix well. Add sufficient purified water to volume and mix well. Package and label.
Rx Diphenylcyclopropenone 0.1 percent to 2 per-cent Solutions
Diphenylcyclopropenone 100 mg to 2 g
Acetone, qs 100 mL
Dissolve the diphenylcyclopropenone in sufficient ac-etone to volume. Package and label. Caution: Diphe-nylcyclopropenone is a strong sensitizing agent. Ex-ercise care when preparing these solutions; wear ap-propriate masks, garb and gloves.
Rx Squaric Acid Dibutyl Ester 0.1 percent to 1 percent Solutions
Squaric acid dibutyl ester 100m g to 1g
Acetone or Ethanol 95 percent, qs 100 mL
Dissolve the squaric acid dibutyl ester in sufficient acetone OR ethanol to volume. Package and label.
Formulations for Lice Infestation
Rx Malathion 0.5 percent Topical Lotion
Malathion 500 mg
Isopropyl alcohol 70 percent 70 mL
Lavender oil 30 drops
Bay oil 3 drops
Ethanol 95 percent, qs 100 mL
Note: Compound this preparation in a well-ventilated area or use an exhaust hood, since malathion fumes can be irritating to the mucous membranes of the na-
sal passages. Wear disposable gloves to prevent re-tention of odor on the hands.
Disperse the malathion in the isopropyl alcohol. Add the fragrances and mix well. Add sufficient ethanol to volume and mix well. Package and label.
Rx Ivermectin 1 percent Creme Rinse
Ivermectin 1 g
Polyethylene glycol 300 17 mL
Creme Rinse (Commercial), qs 100 mL
Mix the ivermectin with the polyethylene glycol 300 to form a smooth paste. Incorporate the creme rinse and mix well. It may be necessary to work the prod-uct in a mortar with a pestle to ensure uniform and small particle size of the ivermectin. Package and label.
Rx Ivermectin 1 percent Lotion
Ivermectin 1 g
Propylene glycol 15 mL
Dermabase 30 g
Purified water, qs 100 mL
Mix the ivermectin with the propylene glycol to form a smooth paste using a mortar and pestle. Incorporate the Dermabase and mix well. Slowly add sufficient purified water to volume and mix well. Package and label.
Formulations for Ringworm
Rx Clotrimazole 1 percent Scalp Lotion
Clotrimazole 1 g
Propylene glycol 50 mL
Polyethylene glycol 300, qs 100 mL
Dissolve the clotrimazole in the propylene glycol and add sufficient polyethylene glycol 300 to volume and mix well. Package and label.
Rx Miconazole 1 percent and Tolnaftate 1 percent Scalp Lotion
Miconazole 1 g
Tolnaftate 1 g
Propylene glycol 50 mL
Polyethylene glycol 300, qs 100 mL
Dissolve the miconazole and tolnaftate in the propyl-ene glycol and add sufficient polyethylene glycol 300 to volume and mix well. Package and label.

May 2012
THE KENTUCKY PHARMACIST 22
May 2012 CE-Compounding for Scalp
CPE Monitor:
Information for Pharmacists and Pharmacy Technicians
What is CPE Monitor?
CPE MonitorTM is a national, collaborative effort by the Ac-creditation Council for Pharmacy Education (ACPE) and the
National Association of Boards of Pharmacy (NABP) to provide an electronic system for pharmacists and pharmacy technicians to track their completed continuing pharmacy education (CPE) credits. It will also offer boards of pharmacy the opportunity to electronically authenticate the CPE units completed by their licensees, rather than requiring pharmacists and pharmacy technicians to submit their proof of completion statements (i.e. statements of credit) upon request or for random audits.
How CPE Monitor Works
Pharmacists and pharmacy technicians will receive a unique identification number (ID), known as the NABP e-Profile ID, after setting up their e-Profile with NABP (see How to Register for CPE Monitor). Many ACPE-accredited CPE providers are now requiring pharmacist and pharmacy technician participants to provide their NABP e-Profile ID and date of birth (DOB in MMDD format) to the ACPE-accredited provider when they register for a CPE activity or submit a request for credit. It will be the responsibility of the phar-macist or pharmacy technician to provide the correct information [i.e. ID and DOB (in MMDD format)] in order to receive credit for participating in a CPE activity.
The CPE Monitor system will direct electronic data from ACPE-accredited providers to ACPE and then to NABP, ensuring that CPE credit is officially verified by the providers. Once information is received by NABP, pharmacists and pharmacy technicians will be able to log in to access information about their com-pleted CPE activities.
How to Register for CPE Monitor
Pharmacists and pharmacy technicians are asked to obtain their NABP e-Profile ID now at www.MyCPEmonitor.net to ensure their e-Profile is properly setup prior to implementation of CPE Monitor. As ACPE-accredited providers begin transitioning their systems to CPE Monitor throughout 2012, the e-Profile ID and DOB in MMDD format will be required by those providers to receive credit for any ACPE-accredited CPE activities. By the end of 2012, all ACPE-accredited CPE providers will require the e-Profile ID and the DOB in MMDD format to receive CPE credit.
NABP Customer Service [email protected] Tel: 847-391-4406 Fax: 847-391-4502 Hours: M-F, 9 AM to 5 PM central
Attention all Pharmacists and Pharmacy Technicians!!!!
You MUST sign up for a NABP e-Profile ID to receive CE credit from KPERF or any
other ACPE Provider as of this year. Visit www.kphanet.org/CPEMonitor for more.
Rx Ketoconazole 2 percent Solution
Ketoconazole 2 g
Polyethylene glycol 300 80 mL
Propylene glycol 20 mL
Dissolve the ketoconazole in the polyethylene glycol 300 and propylene glycol and mix well. Package and
label.
Note: With the exception of a few formulations con-taining drugs such as triamcinolone, fluocinolone ace-tonide, spironolactone, finasteride, and squaric acid dibutyl ester, the remaining preparations can be dis-pensed over-the-counter.

May 2012
THE KENTUCKY PHARMACIST 23
May 2012 CE-Compounding for Scalp
May 2012 — Compounding for Scalp Disorders and Conditions
1. Components of the scalp include:
A. Skin
B. Sebaceous glands
C. Hair shafts
D. Sweat glands
E. All of the above
2. Common disorders of the scalp include all of the fol-lowing, EXCEPT:
A. Hyperhidrosis
B. Dandruff
C. Seborrheic dermatitis
D. Lice infestation
E. Ringworm
3. All of the following may be used to treat psoriasis, EXCEPT:
A. Coal tar solution
B. Anthralin
C. Minoxidil
D. Fluocinolone acetonide
E. Clobetasol
4. Individuals may have a genetic predisposition to:
A. Ringworm
B. Lice
C. Dandruff
D. Psoriasis
E. Seborrheic dermatitis
5. Which of the following should be used to treat ring-worm?
A. Coal tar solution
B. Miconazole
C. Hydrocortisone
D. Anthralin
E. Malathion
6. All of the following may be used to treat a lice infes-tation, EXCEPT:
A. Terbinafine
B. Malathion
C. Ivermectin
D. Permethrin
E. Pyrethrins
7. Squaric acid dibutyl ester can be used in the treat-ment of:
A. Seborrheic dermatitis
B. Dandruff
C. Psoriasis
D. Alopecia
E. Lice
8. Seborrhea of the scalp may be treated with:
A. Zinc pyrithione
B. Selenium
C. Ketoconazole shampoo
D. Topical corticosteroids
E. All of the above
9. Select the FALSE statement about lice infestations from the following:
A. It is epidemic among children of all socioeconomic
classes.
B. It presents with dry scale and underlying erythema.
C. It is spread by sharing hats or combs.
D. The nits on hair shafts are easiest to see above the
ears and at the nape of the neck.
E. Adults in close contact with children may also get the infestation.
10. Special precautions are required when dealing with the following drugs:
I. Malathion
II. Diphenylcyclopropenone
III. Coal tar
A. I only
B. III only
C. I and II only
D. II and III only
E. I, II and III

May 2012
THE KENTUCKY PHARMACIST 24
May 2012 CE-Compounding for Scalp
May 2012 — Compounding for Scalp Disorders and Conditions Universal Activity # 0143-9999-12-005-H04-P PHARMACISTS ANSWER SHEET Name ________________________________________________ KY Lic. # __________________________________ Address ________________________________________________________________________________________ PLEASE CIRCLE THE APPROPRIATE ANSWERS: 1. A B C D E 3. A B C D E 5. A B C D E 7. A B C D E 9. A B C D E 2. A B C D E 4. A B C D E 6. A B C D E 8. A B C D E 10.A B C D E Information presented in the activity: Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes ___No Was well written ___Yes ___No Commercial bias was present ___Yes ___No Is relevant to my practice ___Yes ___No Unmet Objectives:______________________________________________________________________________ I hereby certify that I completed this self-study program independently and without assistance from any other party. Signature _________________________________________________ Date _________________________________
NABP #_________________________________ Birthdate _______________________(MM/DD)
This activity is a FREE service to members of the Kentucky Pharmacists Association. The
fee for non-members is $30. The fee for duplicate certificates is $5. Please send a self
addressed, stamped envelope to KPERF, 1228 US 127 South, Frankfort, KY 40601.
The Kentucky Pharmacy Education & Research Foundation is accredited by The Accreditation Council for Pharmacy Education as a provider of continuing Pharmacy education.
Expiration Date: May 15, 2015
Successful Completion: Score of 80 percent will result in 1.5 contact hours or 0.15 CEUs.
Participants who score less than 80 percent will be notified and permitted one re-examination.
May 2012 — Compounding for Scalp Disorders and Conditions TECHNICIANS ANSWER SHEET. Universal Activity # 0143-9999-12-005-H04-T Name _______________________________________________KY Cert. # __________________________________ Address ________________________________________________________________________________________ PLEASE CIRCLE THE APPROPRIATE ANSWERS: 1. A B C D E 3. A B C D E 5. A B C D E 7. A B C D E 9. A B C D E 2. A B C D E 4. A B C D E 6. A B C D E 8. A B C D E 10.A B C D E Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes ___No Was well written ___Yes ___No Commercial bias was present ___Yes ___No Is relevant to my practice ___Yes ___No I hereby certify that I completed this self-study program independently and without assistance from any other party. Signature _________________________________________________ Date _________________________________
NABP #_________________________________ Birthdate _______________________(MM/DD)_
May 2012
THE KENTUCKY PHARMACIST 25
KPPAC Contribution
Name: _________________________________ Pharmacy: __________________________________________
Address: _________________________ City: ___________________ State: _________ Zip: ____________
Phone: ________________ Fax: _________________ E-Mail: ______________________________________
Contribution Amount: $_________ Check ____ (make checks payable to KPPAC)
Credit Card (AMEX; Discover; MasterCard; VISA)
Account #: ____________________________________________________________ Expiration date: _______
Address to which credit card statement is mailed (if different from above)
____________________________________________________________________________________________
CONTRIBUTION LIMITS
The primary, runoff primary and general elections are separate elections. The maximum contribution from a PAC to a
candidate or slate of candidates is $1,000 per election. Contributions from a PAC to a school board candidate are limited to $200 per election.
Individuals may contribute no more than $1,500 per year to all PACs in the aggregate.
In-kind contributions are subject to the same limits as monetary contributions.
Cash Contributions: $50 per contributor, per election. Contributions by cashier’s check or money order are limited to
$50 per election unless the instrument identifies the payor and payee. KRS 121.150(4)
Anonymous Contributions: $50 per contributor, per election, maximum total of $1,000 per election.
(This information is in accordance with KRS 121. 150)
Mail to: Kentucky Pharmacists Political Advocacy Council, 1228 US Highway 127 South, Frankfort, KY 40601
KPPAC Contribution Form
Support the Candidates who Support YOU!
Make your Donation Today!

May 2012
THE KENTUCKY PHARMACIST 26
Pharmacy Law Brief
Pharmacy Law Brief: Importation of Prescription Drugs
Author: Joseph L. Fink III, B.S.Pharm., J.D., Professor of Pharmacy Law and Policy, Department of Pharmacy Practice and Science, UK College of Pharmacy
Question: What is the current status of the law with regard to prescription medications entering the coun-try, both when brought in by a patient and when shipped from outside the country to a patient? I seem to re-call that there even were some programs sponsored by a number of states to facilitate their citizens getting medications from sources in Canada. Response: The federal law in this area is unchanged and has been the same for quite some time. Suc-cinctly stated, it prohibits anyone, including an individual private citizen or a business organization, from bringing into the country an unapproved new drug product that violates the Federal Food, Drug and Cosmetic Act. It does not matter whether the products are for personal use or for resale. The legal position is that the category of unapproved new drugs includes “any drugs, including foreign-made versions of U.S. approved drugs that have not been manufactured in accordance with and pursuant to an FDA approved process.” A number of studies have documented that pharmaceuticals coming into the US and purporting to have been made in one country really come from manufacturers based in other lands. Products labeled to appear to have been manufactured in Canada have been found to originate in Brazil or any number of African nations. It is important to bear in mind that the highly controlled system of drug product approval, manufacturing and distribution was put in place over the past century with the goal of having only approved drug products availa-ble for use by those in the U.S. Some measure of validity attached to the notion of importing medications for personal use from Canada arose when several states launched initiatives to encourage their citizens to take advantage of potential sav-ings claimed to exist. Probably the highest profile initiative of this type was “I-Save Rx” promoted by the now-discredited Gov. Rod Blagojevich of Illinois. This program used both Canadian sources as well as ones in Eu-rope. At least four other states joined the effort but the program died when the Canadian supplier withdrew, claiming that the states had not adequately promoted the program to their citizens. All this being said, the U.S. Food and Drug Administration has the same enforcement discretion as does any law enforcement agency. Just like the state trooper who pulls over a speeding motorist and then decides to issue a warning rather than a ticket, the FDA has some latitude in how it approaches enforcement of the stat-utes and regulations under its jurisdiction. As a general rule, FDA does not bring its enforcement might to bear on individual patients who are importing medications for personal use. The agency has bigger fish to fry,
Resources for further information:
APhA, Drug importation: The realities of safety and security.
http://www.pharmacist.com/AM/Template.cfm?Section=Home2&CONTENTID=17842&TEMPLATE=/CM/
ContentDisplay.cfm
FDA, Information on importation of drugs.
http://www.fda.gov/ForIndustry/ImportProgram/ImportPolicyandInformationbyProduct/default.htm
FDA, FDA operation reveals many drugs promoted as “Canadian” products really originate from other countries.
http://www.fda.gov/NewsEvents/ Newsroom/ Press Announcements/2005/ucm108534.htm.
FDA, Importing prescription drugs: Letters to state and local officials.
http://www.fda.gov/Drugs/DrugSafety/ucm170594.htm.

May 2012
THE KENTUCKY PHARMACIST 27
Pharmacy Law Brief
The Kentucky Renaissance Pharmacy Museum offers several ways way to show support of the
Museum, our state's leading preservation organization for pharmacy.
While contributions of any size are greatly appreciated, the following levels of annual giving have
been established for your consideration.
Friend of the Museum $100 Proctor Society $250 Damien Society $500 Galen Society $1,000
Name_________________________________ Specify gift amount________________________
Address ______________________________ City____________________Zip______________
Phone H_______________W____________ Email___________________________________
Employer name_____________________________________________for possible matching gift
Tributes in honor or memory of_____________________________________________________
Mail to: Kentucky Renaissance Pharmacy Museum, P.O.Box 910502, Lexington, KY 40591-0502
The Kentucky Renaissance Pharmacy Museum is a non-profit 501(c)(3) business entity and as such donations are tax
deductible. A notice of your tax deductible contributions will be mailed to you annually.
Questions: Contact Lynn Harrelson @ 502-425-8642 or [email protected]
e.g., tracking down the source of the counterfeit Avastin® that recently made its way into the nation’s drug supply. Some of the factors the FDA will weight when deciding whether to pursue enforcement in a given case have been laid out by the agency this way: The intended use of the imported product is unapproved, and it is for a serious condition which has no
approved treatment in the U.S. There is no known commercialization or promotion of the product to U.S. citizens by those distributing the
product. The product is not deemed to pose an unreasonable risk. The individual affirms in writing that it is for personal use, supplies the name and address of the U.S.-
based physician responsible for supervising use of the product, or provides evidence the product being imported is for continuation of a treatment regimen begun abroad.
For the pharmacist an important consideration is that when patients procure medications from a foreign source they may be reluctant to report that to their local pharmacist or physician. Hence, those health profes-sionals may have an incomplete picture of the medications actually being used by the patient. Given the re-luctance of patients to volunteer such information and their hesitance to inquire about the desirability of drug importation from their trusted pharmacist who may be their traditional source for drug products and infor-mation about them, the local pharmacy practitioner may be unaware of the extent of such activities in his or her area.
Disclaimer: The information in this column is intended for educational use and to stimulate professional discussion among colleagues. It should not be construed as legal advice. There is no way such a brief dis-
cussion of an issue or topic for educational or discussion purposes can adequately and fully address the mul-tifaceted and often complex issues that arise in the course of professional practice. It is always the best ad-vice for a pharmacist to seek counsel from an attorney who can become thoroughly familiar with the intrica-
cies of a specific situation, and render advice in accordance with the full information.
Submit Questions: [email protected]

May 2012
THE KENTUCKY PHARMACIST 28
CPE Monitor
CPE MONITOR:
Change is coming By: Scott Sisco, Director of Communications and Continuing Education
Change can be good. Change can
be easy. Change can be challeng-
ing. Change can be scary, but it
doesn’t have to be.
CPE Monitor is a
change. For some phar-
macists and certified
pharmacy technicians
(yes techs, this includes
you), this is a welcome
change that will simplify
one aspect of your pro-
fessional life. For those
who are not as technol-
ogy friendly, this
change will require
some assistance from your tech-
savvy associates.
CPE Monitor was developed
through collaboration between the
Accreditation Council for Pharmacy
Education (ACPE) and the National
Association of Boards of Pharmacy
(NABP) to create an electronic sys-
tem for pharmacists and certified
pharmacy technicians to track com-
pleted continuing education credits.
Since the initial launch of the CPE
Monitor service in March 2011,
more than 93,100 pharmacists and
36,500 pharmacy technicians set
up NABP e-Profiles to prepare for
the shift to electronic tracking of all
ACPE-accredited CPE units.
The continuing education programs
you attend and journal articles you
read WILL NOT change. The Ken-
tucky Pharmacy Education and Re-
search Foundation (KPERF), and
all other ACPE CE Providers, will
continue to offer quality, education-
al programs. The way you earn
your CE will not change.
CPE Monitor only changes how the
certification of your CE is delivered.
No longer will you have to snail
mail a self-addressed stamped en-
velope with your journal answer
sheets. For those over-worked
pharmacists and technicians who
send in that last CE at the end of
the year, this eliminates the wait
time to receive the certificate in the
mail.
Instead, you will be able to go to
your computer and print out either
a list of the CE activities you com-
pleted or certificates for those activ-
ities. You won’t have to keep your
binder of certificates in your phar-
macy. If the Board of Pharmacy
audits your license, your CPE units
will be authenticated electronically
by the investigator.
You may have noticed the new
lines on the answer
sheets for the CE articles
in The Kentucky Pharma-
cist in 2012 requesting
NABP # and Birthdate.
These lines were added
in anticipation of
KPERF’s changeover to
CPE Monitor later this
year. And ladies, you only
have to provide month
and day on the birthdate.
We don’t have to know how old you
are, just the month and day you
were born. ALL ACPE Providers
will completely implement CPE
Monitor by the end of 2012 and will
be requiring this information.
Your first step in this process is to
sign up for your NABP eProfile ID
at www.nabp.net. Click on the CPE
Monitor logo, and it will take you to
the sign up page. NABP Customer
Service is available to answer your
questions at [email protected] or
on the telephone Monday through
Friday 9 a.m. to 5 p.m. Central
Time at 847-391-4406.
Watch this journal and email mes-
sages from KPhA for updates on
CPE Monitor. Updates will also be
posted at www.kphanet.org/
CPEMonitor.

May 2012
THE KENTUCKY PHARMACIST 29
Pharmacy Technician Certification Board
May 2012
THE KENTUCKY PHARMACIST 30
The Federal Agency for Healthcare Research and
Quality (AHRQ) launched a nationwide initiative to
raise awareness of patient-centered outcomes re-
search and to encourage its use. AHRQ provides
pharmacists, other clinicians and patients free re-
sources and tools that objectively summarize current
clinical evidence on various treatment methods to in-
form health care decision making. KPhA is partnering
with AHRQ to provide our members quick access to
these materials and to announce new products as
they become available.
Patient-centered outcomes research informs health
care decision making by comparing the evidence on
the effectiveness, benefits and harms of different
treatment options for common health conditions.
Many of the research studies compare medication
therapies used to treat a wide range of conditions,
including cancers, cardiovascular diseases and relat-
ed conditions, diabetes, arthritis and mental health
disorders.
In conducting systematic reviews, researchers synthe-
size the available evidence on drugs, medical devic-
es, tests, surgeries or ways to deliver health care. The
research findings are translated into practical re-
sources, including:
Clinician research summaries (most are two pag-
es)
Plain language patient research summary bro-
chures (in English and Spanish)
Accredited CME/CE modules (including several
accredited for pharmacists)
Faculty slide presentations
All of these tools are designed to encourage and sup-
port shared decision making between clinicians and
patients, with a goal of better care and increased pa-
tient satisfaction. Clinician materials provide clinical
bottom line information, citing research gaps, when
applicable. Patient materials are written in plain lan-
guage and contain an overview of the condition in ad-
dition to the comparative effectiveness information.
These unbiased resources can help pharmacists:
Identify issues to discuss with patients.
Talk about side effects.
Analyze treatments and assess benefits and
harms for patient outcomes.
Examples of currently available titles include:
Treating Cholesterol With Combination Therapy
Comparing Medications for Adults With Type 2
Diabetes
ACEIs, ARBs or DRI for Adults With Hypertension
Analgesics for Osteoarthritis
To view or download AHRQ resources, visit
www.EffectiveHealthCare.ahrq.gov. To order free
printed copies of the clinician or patient research sum-
maries, including bulk quantities, call the AHRQ Publi-
cations Clearinghouse at 1-800-358-9295 and provide
the code C-02.
For more information about this initiative, contact Vic-
toria McGhee in AHRQ’s Atlanta Regional Office at
404-836-2303 or [email protected].
KPhA partners with AHRQ to offer
free resources for members, patients
Watch your email box for updates on
new information in eNews!
Agency for Healthcare Research and Quality

May 2012
THE KENTUCKY PHARMACIST 31
You MUST sign up for a NABP
e-Profile ID to receive CE credit from KPERF
or any other ACPE Provider.
Visit www.kphanet.org/CPEMonitor for more.
Pharmacy Time Capsules 1987—Twenty-five years ago:
Petition requesting recognition of Nutrition Support Pharmacy Practice as a specialty was submitted to the Board of Pharmaceutical Specialties.
1962—Fifty Years Ago:
New England College of Pharmacy affiliated with Northeastern University.
The Indian Hospital at Crow Agency, Montana began filling outpatient pre-scriptions directly from the patient’s medical record. This was eventually adopted throughout the Indian Health Service.
1937—Seventy-five Years Ago:
National Cancer Institute was established to conduct and support research relating to the cause, diagnosis, and treatment of cancer.
1912—One hundred Years Ago:
Public Health and Marine Hospital Service was renamed the Public Health Service (PHS) and the mission was expanded to include communicable diseases field investigations, navigable stream pollution, and infor-mation dissemination.
APhA House of Delegates was established as a forum for all branches of the profession to have a voice.
By: Dennis B. Worthen
Lloyd Scholar, Lloyd Library and Museum, Cincinnati, OH
One of a series contributed by the American Institute of the History of Pharmacy, a unique non-profit society dedicated to assuring that the contributions of your profession endure as a part of America's history. Mem-bership offers the satisfaction of helping continue this work on behalf of pharmacy, and brings five or more
historical publications to your door each year. To learn more, check out: www.aihp.org
Pharmacy Time Capsules

May 2012
THE KENTUCKY PHARMACIST 32
NASPA Leadership Conference
President-Elect Kimberly Croley and
Executive Director Robert McFalls at-
tended the National Alliance of State
Pharmacy Association Leadership Con-
ference sponsored by Pharmacists Mu-
tual Companies April 29-May 1 at U.S.
Pharmacopeia in Rockville, Md. Associ-
ation directors and president-elects
learned leadership skills and shared
ideas to solve problems faced by many
of the state pharmacy associations.
Pictured are leaders from Georgia, Ex-
ecutive Jim Bracewell and President-
Elect Robert Hatton; Alabama Execu-
tive Louise Jones; NCPA President-
Elect Donnie Calhoun; and McFalls and
Croley.
KPhA at NASPA Leadership Conference
sponsored by Pharmacists Mutual Companies
UKCOP student shares study-abroad experience
Katy Monson, a fourth-year pharmacy and MPA stu-
dent in the Martin School of Public Policy & Admin-
istration at the University of Kentucky, is studying on
a six week experiential education rotation in Ecuador.
She is blogging about her experiences there -
http://pharmdstudentinecuador.blogspot.com/.
KPhA sends email announcements weekly.
If you aren’t receiving:
eNews, Legislative Updates, Grassroots Alerts and
other important announcements, send your email
address to [email protected] to get on the
distribution list.
May 2012
THE KENTUCKY PHARMACIST 33
KPhA Government Affairs
Contribution
Name: _________________________________ Pharmacy: ___________________________________
Address: ____________________________________________________________________________
City: _______________________________________________ State: _________ Zip: ____________
Phone: ________________ Fax: _________________
E-Mail: ______________________________________________________
Contribution Amount: $_________ Check ____ (make checks payable to KPhA Government Affairs)
Credit Card (AMEX; Discover; MasterCard; VISA)
Account #: ____________________________________________________ Expiration date: _______
Address to which credit card statement is mailed (if different from above)
___________________________________________________________________________________
Mail to: Kentucky Pharmacists Association
1228 US Highway 127 South Frankfort, KY 40601
Support the Candidates who Support YOU!
Make your Donation Today!
KPhA Government Affairs Contribution

May 2012
THE KENTUCKY PHARMACIST 34
June 2012 CE—Reducing the Burden of Adverse Drug Events
Reducing the Burden
of Adverse Drug Events By: Lewis Wilkerson, PharmD, CGP
M. Trent Blacketer, MBA, PharmD candidate at University of Kentucky College of Pharmacy
There are no financial relationships that could be perceived as real or apparent conflicts of interest.
Universal Activity # 0143-9999-12-005-H04-P
1.0 Credit Hours (0.1 CEUs)
Objectives
- Discuss the scope of Adverse Drug Events in practice and the importance of prevention - Identify the drug classes most at risk for Adverse Drug Events - Assess patient characteristics that may increase the risk for Adverse Drug Events - Recognize the need for complete patient analysis
KPERF offers all
CE articles to
members online at
www.kphanet.org
Background
Adverse Drug Events (ADEs) are one of the leading
causes of preventable morbidity in our healthcare
practices. A review of studies assessing the incidence
of ADEs in inpatient and outpatient settings reveals
disturbing results for providers. The median ADE prev-
alence rate was 9.5 percent within analysis of pro-
spective studies. ADEs have the potential to elevate
costs within the healthcare system as well, most nota-
bly when leading to unnecessary hospitalizations.
Studies have shown that nearly 5 percent of ADEs will
lead to an additional hospitalization for our patients.1, 2
It has also been exposed that more than 20 percent of
all ADEs could have been prevented if medications
were prescribed and monitored correctly. Prevention
and timely recognition of potential ADEs will help to
improve patient and medication safety within our prac-
tices.3,4
This article will discuss drug classes common-
ly leading to ADEs, as well as patient characteristics to
make ourselves more aware of, in hopes of decreas-
ing the troubling ADE rates encountered today.
Common Drug Class Offenders
A substantial portion of the ADEs encountered by pro-
viders are caused by a limited number of drug classes.
Analgesic, cardiovascular, and hypoglycemic agents
combine to account for more than 85 percent of ADEs.
Opioids and NSAIDS are the obvious offenders in the
analgesic class. Many cardiovascular agents have a
high potential to cause ADEs ranging from diuretics to
anticoagulants. Some diabetic agents merit concern
due to their potential for hypoglycemia. Hypoglycemic
agents do not result in a large majority of the ADEs
that we come across, but a higher percentage of the
events are of serious nature and therefore lead to
more hospitalizations. This explains why they are in-
cluded on most high-risk drug lists. Table 1 lists drug
groups that most commonly led to ADEs in a recent
prospective study.5
As illustrated in the table, NSAIDs should be of utmost
concern for pharmacists when verifying and monitor-
ing patient therapies. Past histories of bleeding or ul-
ceration, as well as potential for renal impairment, are
important factors to be proactive about when providing
care for patients. The other drug group of high con-
cern with nearly 30 percent of ADE cases is diuretics.
Over- or under-diuresing a patient can lead to a num-
ber of avoidable effects, such as hypotension or elec-
trolyte imbalances. Stressing the importance of accu-
rate dosing and frequency of diuretics are necessary
steps in preventing negative outcomes.5
The potential ADE risk drops significantly for anticoag-
ulants when compared to the NSAIDs and diuretics.
This is most likely due to the attitude that clinicians

May 2012
THE KENTUCKY PHARMACIST 35
June 2012 CE—Reducing the Burden of Adverse Drug Events
have adopted regarding warfarin monitoring. The
medication itself is just as dangerous, if not more so
compared to the aforementioned drug groups, but
comprehensive anticoagulant follow-up has become
standard practice today. This likely decreases the
amount of ADEs that warfarin causes and is a testa-
ment to the effect that pharmacists contributions can
have.
The remainder of the drug classes noted in the study
caused less than 10 percent of the total reported
ADEs.5 The data in Table 1 clearly demonstrates that
a small subset of the total number of drug groups lead
to an overwhelming majority of the ADEs that we en-
counter within our healthcare practices. By digesting
this evidence based knowledge and using it to direct
our efforts toward these concerning classes, the total
number and impact of ADEs could be significantly re-
duced. Assessing the appropriateness of medications
within these drug classes is a great place to start. Al-
ways be alert and consider if the benefits outweigh
the risks before exposing patients to the potential
harmful effects of medications.
Patient Characteristics Predicting Risk
Now that we have discussed which drug classes are
most likely to lead to ADEs, we next must determine
which patients have the highest potential for develop-
ing ADEs. Focusing on statistics regarding patient
demographics helps signify what a high-risk patient
may appear like to us as healthcare providers.
ADEs vary widely in prevalence between different age
groups. A review of multiple studies, looking at differ-
ent age brackets, found that the median prevalence
rates ranged from 2.45 percent for children, to 5.27
percent for adults, and up to 16.1 percent for the el-
derly population. Pediatric patients normally have a
lower patient/healthcare provider ratio and are always
under close supervision, which explains their lower
rate of ADEs. Additionally, the trend shows that as a
patient becomes older they seem to be more suscep-
tible to ADEs.6 As providers, we need to recognize
this and prioritize our elderly patients in order to pre-
vent their higher ADE rates. The Beers’ criteria are a
great resource for clinicians to use for uncovering po-
Table 1: Drug Groups Commonly Leading to Adverse Drug Events
Drug group percent of ADE
cases Individual drugs Adverse reactions
NSAIDs 29.6 Aspirin, diclofenac, ibu-profen, rofecoxib, celecox-ib, ketoprofen, naproxen
GI bleeding, peptic ulceration, haemor-rhagic cerebrovascular accident, renal impairment, wheezing, rash
Diuretics 27.3 Furosemide, bumetanide, spironolactone, amiloride, metolazone, indapamide
Renal impairment, hypotension, elec-trolyte disturbances, gout
Anticoagulants 10.5 Warfarin GI bleeding, haematuria, high INR, haematoma
ACE inhibitors/ARB 7.7 Ramipril, enalaparil, cap-topril, lisinopril, irbesartan, losartan
Renal impairment, hypotension, elec-trolyte disturbance, angioedema
Antidepressants 7.1 Fluoxetine, paroxetine, amitriptyline, citalopram, lithium, venlafaxine
Confusion, hypotension, constipation, GI bleed, hyponataemia
β blockers 6.8 Atenolol, propranolol, so-talol, bisoprolol, metopro-lol, carvedilol
Bradycardia, heart block, hypotension, wheezing
Opiates 6.0 Morphine, dihydrocodeine, tramadol, fentanyl
Constipation, vomiting, confusion, uri-nary retention

May 2012
THE KENTUCKY PHARMACIST 36
June 2012 CE—Reducing the Burden of Adverse Drug Events
tential medication threats in elderly patients. The re-
cently updated criteria can be found on The American
Geriatrics Society website, which is linked in the refer-
ences section .10
Patient demographics other than age do not tend to
reveal such dramatic statistical variances with respect
to ADE rates, but there are some others worth noting.
With respect to gender, females tend to present with
more ADEs in comparison to males. One specific study
focusing on ADEs leading to emergency room visits
found that 60 percent of all ADEs are from the female
population.7 This could be attributed to differing severity
tolerance levels of the events. Race is also a demo-
graphic that has shown to present with differing ADE
rates. Non-Hispanic whites tend to have the lowest
ADE rates, with Hispanics and Blacks having a higher
adjusted risk ratio.8
Past medical history is a characteristic of patient health
that can further inform providers of possible ADE risks.
Comorbid disease states are too often overlooked
when dispensing and monitoring a patient’s therapy.
Medications that are beneficial in treating one condition
can be extremely dangerous when exposed to a patient
with secondary conditions. Secondary disease states
such as cancer or even an acute infection can signifi-
cantly alter the pharmacokinetics of drug therapies.11
Analyzing how comorbid disease states may affect
medications in our patients will undoubtedly reduce the
occurrence of ADEs in our practices.
Another section of patient health that is frequently
skipped over when reviewing for potential ADEs is so-
cial history. Diet and exercise routines, as well as to-
bacco and recreational drug use, are important aspects
to be informed about for proper medication evaluation.
It is well known that certain food and supplements have
the potential to cause drug interactions, yet practition-
ers monitoring regimens often have no knowledge re-
garding their patients diets. Vigorous exercise has the
potential to alter metabolism and excretion of medica-
tions. Additionally, knowing about a patients tobacco
and recreational drug use is extremely valuable when
assessing therapies, especially concerning cardiovas-
cular agents. Social history can sometimes seem like
insignificant information, but the risk for ADEs can defi-
nitely be affected by our patients daily habits.
Another key to assessing patient’s for adverse drug
events is to do a thorough medication review. This in-
cludes medications that they might obtain via another
pharmacy, samples, and OTC’s or supplements. Phar-
macists should also be on the alert when patients have
multiple prescribers as this increases the risk of poten-
tial drug-drug or drug-disease interactions and potential
adverse events.
Health literacy is not often a topic associated with re-
ducing ADEs, but many health safety experts believe it
should be. Recent studies have shown that around 20
percent of Americans read at or below a fifth grade
level, yet package inserts and other health information
data are often written at or above the 10th grade level.9
It is reasonable to assume that many ADEs could be
prevented if patients simply understood what their med-
ications are for and exactly how and when they are
supposed to use them. Understanding the health
literacy gap between providers and patients, and taking
steps to assure patients are well informed about their
regimens may result in reductions in ADEs.
Conclusion
Improving health safety and decreasing the burden of
ADEs for patients requires constantly addressing medi-
cation risks versus benefits. We must not only deter-
mine the appropriateness of physicians prescribing de-
cisions, but also focus on recognizing and preventing
unseen ADEs before they occur. Simply glancing over
a patient’s profile for drug interactions needs to be-
come a routine of the past. Instead, we need to im-
prove quality and outcomes by actively monitoring,
managing, and reassessing all aspects of our patients
health. Diminishing the prevalence of ADEs will elimi-
nate the excess costs from our healthcare system and,
most importantly, improve our patients’ lives.
References
1. Miller GC, Britth HC, Valenti L. Adverse drug events in general practice patients in Australia. Med J Aust. 2006 Apr 3;184(7):321-4.
2. Thomsen LA, Winterstein AG, et al. Systematic re-view of the incidence and characteristics of preventable adverse drug events in ambulatory care. Ann Pharma-cother. 2007 Sep;41(9):1411-26. Epub 2007 Jul 31.
3. Kanjanarat P, Winterstein AG, et al. Nature of pre-ventable adverse drug events in hospitals: a literature review. Am J Health Syst Pharm. 2003 Sep 1;60(17):1750-9.

May 2012
THE KENTUCKY PHARMACIST 37
June 2012 CE—Reducing the Burden of Adverse Drug Events
4. Von Laue NC, Schwappach DL, et al. The epidemi-ology of preventable adverse drug events: a review of the literature. Wien Klin Wochenschr. 2003 Jul 15;115(12):407-15.
5. Pirmohamed M, James S, et al. Adverse drug reac-tions as cause of admission to hospital: prospective analysis of 18,820 patients. BMJ. 2004 July 3; 329(7456): 15–19.
6. Tache SV, Sonnichsen A, Ashcroft DM. Prevalence of adverse drug events in ambulatory care: a systemic review. Ann Pharmacother. 2011 Jul;45(7-8):977-89. Epub 2011 Jun 21.
7. Sikdar KC, Alaghehbandan R, et al. Adverse drug events in adult patients leading to emergency depart-ment visits. Ann Pharmacother. 2010 Apr;44(4):641-9.
Epub 2010 Mar 16.
8. Metersky ML, Hunt DR, et al. Racial disparities in the frequency of patient safety events: results from the National Medicare Patient Safety Monitoring Pro-gram. Med Care. 2011 May;49(5):504-10.
9. Safeer RS, Keenen J. Health literacy: the gap be-tween physicians and patients. Am Fam Physician. 2005 Aug 1;72(3):463-8.
10. The American Geriatrics Society. AGS Beers Cri-teria pocket card. http://www.americangeriatrics.org/files/documents/beers/PrintableBeersPocketCard.pdf.
11. GR Robertson, C Liddle, SJ Clarke. Inflammation and Altered Drug Clearance in Cancer: Transcription-al Repression of a Human CYP3A4 Transgene. Clini-cal Pharmacology & Therapeutics (2008); 83, 6, 894–897.
June 2012 — Reducing the Burden of Adverse Drug Events
1. What was the median ADE prevalence rate within the analysis of prospective studies discussed in the article?
A. 5.4 percent
B. 9.5 percent
C. 14.0 percent
D. 25.5 percent 2. What percent of ADEs are found to lead to additional hospitalizations?
A. 1 percent
B. 3 percent
C. 5 percent
D. 12 percent 3. What percent of ADEs have the potential to be pre-vented if monitored correctly?
A. 5 percent
B. 10 percent
C. 15 percent
D. 20 percent
4. Which three drug classes account for over 85 percent of all ADEs?
A. oncologic, antipsychotic, cardiovascular
B. hypoglycemic, immunosuppressant, oncologic
C. analgesic, cardiovascular, and hypoglycemic
D. analgesic, antipsychotic, cardiovascular
5. Which two drug groups each account for more than 25 percent of the total ADEs respectively?
A. NSAIDs and diuretics
B. antidepressants and anticoagulants
C. opiates and diuretics
D. β blockers and NSAIDs
6. What should every healthcare provider conclude be-fore exposing patients to the potential harmful side ef-fects of medications?
A. Side effects are mild in nature
B. Benefits will outweigh risks
C. Patient is a non-smoker
D. Patient has no other common disease states
7. Which age group tends to encounter ADEs at the highest rate?
A. Infants
B. Pediatrics
C. Adults
D. Elderly
8. True or False: Males present with more ADEs than females.
A. True
B. False 9. Which race demographic has the lowest ADEs rates?
A. Asians
B. Blacks
C. Hispanics
D. Non-Hispanic Whites
10. Health information data is often written at or above which grade level?
A. 3rd grade
B. 6th grade
C. 10th grade
D. 12th grade

May 2012
THE KENTUCKY PHARMACIST 38
June 2012 CE—Reducing the Burden of Adverse Drug Events
June 2012 — Reducing the Burden of Adverse Drug Events Universal Activity # 0143-0000-12-006-H04-P PHARMACISTS ANSWER SHEET Name ________________________________________________ KY Lic. # __________________________________ Address ________________________________________________________________________________________ PLEASE CIRCLE THE APPROPRIATE ANSWERS: 1. A B C D 3. A B C D 5. A B C D 7. A B C D 9. A B C D 2. A B C D 4. A B C D 6. A B C D 8. A B 10.A B C D Information presented in the activity: Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes ___No Was well written ___Yes ___No Commercial bias was present ___Yes ___No Is relevant to my practice ___Yes ___No Unmet Objectives:______________________________________________________________________________ I hereby certify that I completed this self-study program independently and without assistance from any other party. Signature _________________________________________________ Date _________________________________
NABP #_________________________________ Birthdate _______________________(MM/DD)
This activity is a FREE service to members of the Kentucky Pharmacists Association. The fee for non-members is $30. The fee for duplicate certificates is $5. Please send a self
addressed, stamped envelope to KPERF, 1228 US 127 South, Frankfort, KY 40601.
The Kentucky Pharmacy Education & Research Foundation is accredited by The Accreditation Council for Pharmacy Education as a provider of continuing Pharmacy education.
Expiration Date: May 15, 2015 Successful Completion: Score of 80 percent will result in 1.0 contact hours or 0.1 CEUs.
Participants who score less than 80 percent will be notified and permitted one re-examination.
June 2012 — Reducing the Burden of Adverse Drug Events TECHNICIANS ANSWER SHEET. Universal Activity # 0143-0000-12-006-H04-T Name _______________________________________________KY Cert. # __________________________________ Address ________________________________________________________________________________________ PLEASE CIRCLE THE APPROPRIATE ANSWERS: 1. A B C D 3. A B C D 5. A B C D 7. A B C D 9. A B C D 2. A B C D 4. A B C D 6. A B C D 8. A B 10.A B C D Met my educational needs ___Yes ___No Figures and tables were useful ___Yes ___No Achieve the stated objectives ___Yes ___No Posttest was appropriate ___Yes ___No Was well written ___Yes ___No Commercial bias was present ___Yes ___No Is relevant to my practice ___Yes ___No I hereby certify that I completed this self-study program independently and without assistance from any other party. Signature _________________________________________________ Date _________________________________
NABP #_________________________________ Birthdate _______________________(MM/DD)_
May 2012
THE KENTUCKY PHARMACIST 39
Student Perspective at APhA
APHA ANNUAL CONFERENCE—THE STUDENT PERSPECTIVE
APhA Annual Meeting and Exposition Not Just for Practicing Pharmacists
By: Amanda Jett, Sullivan University College of Pharmacy PharmD Candidate 2013
This was not my first APhA Annual Meeting. With that being said, my expectations of what I would learn were not as high as when I attended last year’s meeting in Seattle. Having served as the President of the Sullivan University College of Pharmacy’s chapter of APhA-ASP for almost a year, I thought I was pretty well set in my knowledge of how to run a chapter, ideas for member recruitment, how to get members interested and involved in advocacy, as well as all of the other responsi-bilities that come with being a chapter president. However, when I arrived in New Orleans and attended the first ASP workshop, I immediately knew it was going to be a long and exhausting, yet extremely rewarding weekend.
Despite the meeting occurring during finals week, SUCOP was able to send four members of our current Executive Committee to New Orleans. The first event we attended was the Executive Committee Leadership Workshop, sponsored by Tar-get. At this workshop national leaders from Target spoke on ways of effective communication within an organization and addressed the issue of smart decision-making. Questions based on hypothetical business scenarios were posed to the chapter committees, and groups had to work together to come up with acceptable answers. While it seemed as though this workshop was geared more toward leading a business, it still challenged our group to communicate with each other and make decisions that would affect our “business.”
The four of us then went our separate ways to attend our respective positions’ workshops. Although I attend-ed the President-Elect workshop last year, I went again with my current President-Elect to share examples of what our chapter has accomplished over the past year. I was sure that I would receive the same information and ideas that were discussed previously, and that this would be a waste of an hour and fifteen minutes. While our chapter has been very successful in recruiting and maintaining members this year – due in part to the ideas I received at the last APhA Annual Meeting – we took pages and pages of notes on ways that other chapters recognize outstanding members and boost morale. We were even able to share some of our ways to make sure that committee leaders can be held accountable for responsibilities and deadlines of which oth-er chapters had not thought. The other members of our group came back from their workshops with some great ideas as well to implement next year.
My favorite portion of the meeting was the House of Delegate sessions and the meetings on proposed resolu-tions. These events gave our chapter members an opportunity to hear several of the current issues surround-ing our profession, our education and the way in which pharmacists interact with other healthcare providers. Again, we were challenged to sit down together and discuss what we as a chapter felt were the best deci-sions to make to lead the future of our profession. Even though most groaned when they were told to attend a three-hour session, I could tell by the end of the weekend that the House of Delegates sessions were others’ favorites as well, as it was exciting to watch our chapter’s opinion of an issue be supported or opposed.
Although I will not be leading our chapter next year, I am still excited to see the progress our new executive committee will make having had an opportunity to attend the APhA Annual Meeting. After returning from this trip, I believe that you cannot attend too many of these types of events, as they all have something unique and new to offer.
Editor’s Note: Amanda
is a recipient of the Dr.
Ralph Bouvette KPhA
Student Leadership
Institute Scholarship to
attend the APhA Annual
Conference.
May 2012
THE KENTUCKY PHARMACIST 40
Pharmacy Technicians
I teach an annual 5-month pharmacy technician certifi-cation class for GrandView Pharmacy, which is cur-rently in session. One of the questions I receive from prospective students, employees or from the public, is, “Why do I need to be certified?” “What’s in it for me?” While many answers have come to mind, over the years, I have gleaned down my responses to those below. Certification is a quality indicator. Indiana currently does not require a pharmacy techni-cian to become certified, only licensed*. Many states, 17 in total (34 percent of the US), require certification by one of the certifying bodies. However, whether or not you need to be certified to work in your state is im-material, because certification is about so much more than entrance into your profession—it’s a very clear way to demonstrate to employers, customers and peers that your professional knowledge and skills meet nationally recognized standards. In discussions with hundreds of pharmacists in the last five years, all have commented on how much they rely on their certified technicians because of the level of knowledge and credibility they bring into the clinical practice. Dr. Lisa O’Hara, Director of Pharmacy Services at GrandView Pharmacy, states, “Any technician that is willing to learn to the level of national certification exemplifies a commitment to personal growth. Individuals that are committed to personal growth do better work. I need to know that the pharmacy technicians that I trust with my license are willing to go to that level”. Certification leads to increased job prospects. The employment rate for pharmacy technicians is ex-pected to increase 31 percent by 2018.** What’s also interesting about this promising number is that, as the Bureau of Labor Statistics notes, “job prospects are expected to be good, especially for those who are cer-tified.” Essentially, adding a CPhT designation to your resume can mean having an advantage in the job mar-ket when it comes to finding a job, commanding a high-er salary and being considered for promotions. Certification increases patient care. Another important reason to consider certifying is be-cause of the effect it can have on the quality of patient care you provide. As a pharmacy technician, one of
your main duties is to prepare prescription medications under the supervision of a licensed pharmacist. These medications are critical to the management of a vast array of conditions, and staying on top of the latest technological advances in pharmaceuticals can prove critical to how well you serve your customers. Once you become a certified pharmacy technician, you will re-certify every two years. The continuing education requirement requires you to keep up with the changes in our industry that occur every day. You must com-plete a minimum of 20 hours of continuing education with at least one hour in pharmacy law. This continued learning can facilitate the extended pharmaceutical knowledge that will prove valuable to your patients. Certification is attainable. You can choose to prepare for the certification exami-nation in one of three ways—on your own with study material you’ve purchased from an organization, at work in an employer-sponsored training program or through a pharmacy technician program at an accredit-ed school. Pharmacy technician programs typically range from six months to two years, depending on which level of education you pursue (certificate, diplo-ma, or associate’s degree). Through classroom instruc-tion and hands-on laboratory experience, you can learn everything from pharmaceutical calculations, terminolo-gy, and recordkeeping to the laws and ethics related to the pharmacy technology field. Many of these pro-grams also include internships in professional pharma-cies, which provide you with a valuable opportunity to practice your skills and network with potential employ-ers. Certified pharmacy technicians collaborate as co-professionals with pharmacists to ensure that the medi-cations dispensed in a variety of practice settings are of the highest quality in the most efficient ways possi-ble. Pharmacists depend on CPhTs to help them serve their patients. CPhTs increase quality while earning more money than their uncertified counterparts. The decision is easy and the path clear, now go get certi-fied! * Kentucky requires technicians to register with the Kentucky Board of Pharmacy. ** Bureau of Labor Statistics, U.S. Department of Labor, Occupa-tional Outlook Handbook, 2010-11 Edition, web site accessed on Nov. 12, 2010.
Why Do I Need To Be Certified? What’s In It For Me?
Article written by Mark Prifogle, 2011 President of the Indiana Academy of Pharmacy Technicians (IAPT), an academy of the Indiana Pharmacists Alliance (IPA). Reprinted with permission. Original article appeared in the Indiana Pharmacist (Vol. 92, No. 3), third quarter, 2011.

May 2012
THE KENTUCKY PHARMACIST 41
McWhorter School of Pharmacy

May 2012
THE KENTUCKY PHARMACIST 42
Pharmacy Policy Issues
PHARMACY POLICY ISSUES: Behind-the-Counter (BTC) Medication - A New Third Class
By: Tam N. Ho
Author: Tam N. Ho is a 2012 Pharm.D. graduate of the UK College of Pharmacy who is now practicing
pharmacy with RiteAid. A native of Ho Chi Minh City, Viet Nam, she earned a B.S. in Biology at the University of Kentucky prior to beginning pharmacy school.
Issue: Should a new category of medications be established based on an intermediate level of consumer access?
Discussion: The nomenclature “Behind-the-Counter” (BTC) signifies an intermediate class of medications that falls between the relatively more widely established classes of prescription medications and over-the-counter (OTC) medications. Consumers can purchase BTC medications without the need to visit a physician; however, a pharmacist’s intervention is required prior to dispensing of any BTC products. The concept of an in-termediate drug class was established in an effort to mitigate controversial issues surrounding the potential for improper use of medications such as pseudoephedrine, Plan B, and dextromethorphan by patients, where such products were previously available OTC or by prescription.
This third class of medications (BTC) has found widespread use interna-tionally in Europe, and in countries such as Australia, Canada and New Zealand. International implementations of BTC programs highlight the po-tential need to establish an official third class of medications in the United States. Specific drug products that have been suggested for inclusion in BTC programs in the United States are medications that treat chronic con-ditions such as asthma, diabetes, hypercholesterolemia, hypertension, osteoporosis and urinary inconti-nence.
Arguments for and against the relatively new concept of a category of BTC medications are numerous. Pro-ponents for a third class of medication (i.e., proponents for BTC programs) assert that such implementations could increase drug availably to patients, especially those patients from underserved populations, e.g., those who are uninsured, underinsured and those with limited access to primary care providers. Further, within the context of administering BTC products, it is argued that pharmacists are well qualified to do so, given that pharmacists generally possess thorough knowledge of drug information. Additionally, pharmacists have typi-cally undergone patient-focused training. With increased interaction between pharmacists and patients through BTC programs, increases in patient adherence rates and ultimately improved health outcomes are anticipated.
Opponents argue that the adoption of the BTC classification for administering selected medications could potentially decrease drug availability to consumers, especially if there is a lack of adequate communication regarding which medications are available through the BTC program. Also, there are concerns that since community pharmacists are generally fully occupied while managing the activities in the pharmacy, fulfillment of such duties may not leave sufficient time to provide high quality intervention services to patients. Lastly, it is argued that BTC programs may lead to patients not being treated properly, i.e., treated for symptoms while undue attention is not provided to treating the underlying illness.
Have an Idea?:
This column is designed to address timely and practical
issues of interest to pharmacists, pharmacy
interns and pharmacy technicians with the goal
being to encourage thought, reflection and exchange
among practitioners. Suggestions regarding topics
for consideration are welcome. Please send them

May 2012
THE KENTUCKY PHARMACIST 43
Pharmacy Policy Issues
Do you have a
story to tell?
Coming in future editions of
The Kentucky Pharmacist
My Story: A Profile of a
KPhA Member
The Kentucky Pharmacists Association is
looking for members with a story to tell.
Have a patient success story to share?
Find a new way to provide a service to the
community?
What makes you stand out in a crowd?
Why did you become a pharmacist?
If you would like to be featured in The
Kentucky Pharmacist, email Scott Sisco at
[email protected] with a brief descrip-
tion of your story.
WANTED:
Blood Glucose Test Strips
I buy unopened, unexpired
diabetic test strips.
The following brands are what I look for
Accu Chek Aviva
Accu Chek Compact Accu Chek Active plus
Bayer Contour Bayer Breeze2 Freestyle lite
One Touch Ultra Blue
Please contact Tim at Green Horseshoe Healthcare
at 502 287 2763.
Check the KPhA website for
registration forms and more
information updates on the
134th KPhA Annual Meeting www.kphanet.org/2012annualmeeting
Prior to the implementation of BTC classifications, some issues pertaining to costs, pharmacists and infra-structure must be addressed. Pharmacist-related issues include defining the role, responsibility, liability and additional training that may be required. Potential cost-related issues include insurance coverage for such products, reimbursement for pharmacists’ services, and possible out-of-pocket cost for consumers. Last, in-frastructure-related issues include providing sufficient lab data regarding patient health status with due regard for patient privacy.

May 2012
THE KENTUCKY PHARMACIST 44
KPhA Academy of Consultant Pharmacists -KY ASCP CE Event
KPhA's Academy of Consult-
ant Pharmacists and the
Kentucky Chapter of ASCP
held a joint continuing educa-
tion program, April 29, 2012
at the Kentucky Renaissance
Pharmacy Museum. Several
new members were added to
both the KY-ASCP Chapter
and KPhA's Academy. The
group raised several hundred
dollars for the Museum. The
meeting organizers, Leah
Tolliver, Jason Baker, Rob
Godwin and Kim Croley,
hope that this meeting will
spark a Renaissance in op-
portunities to educate and
learn how the practice of
consultant pharmacy can
positively influence the
health of all Kentuckians!
Long Term Care
Continuing Education
For more information
For KY-ASCP Chapter: http://www.kyascp.com
Or contact: Leah Tolliver at [email protected] or (859) 333-4748
For KPhA Academy: Go to http://www.kphanet.org
Photos by
Jason and Jennifer Baker

May 2012
THE KENTUCKY PHARMACIST 45
Pharmacists Mutual Companies
May 2012
THE KENTUCKY PHARMACIST 46
KPhA BOARD OF DIRECTORS
Clay Rhodes, Louisville Chairman
[email protected] 502.476.1796
Lewis Wilkerson, Frankfort President
[email protected] 502.695.6920
Frankie Hammons, Barbourville Secretary
[email protected] 606.627.7575
Duane Parsons, Richmond Treasurer
[email protected] 502.553.0312
Kimberly Croley, Corbin President-Elect
[email protected] 606.304.1029
Leon Claywell Past President
Kelley Ratermann Student Representative
Amanda Jett Student Representative
Amanda Burton, Lexington
Chris Clifton, Erlanger
Trish Freeman, Lexington
Joey Mattingly, Prospect
Matt Martin, Louisville
Jeff Mills, Louisville
Glenn Stark, Frankfort
Sam Willett, Mayfield
Leah Tolliver, Lexington
Richard Slone, Hindman
HOUSE OF DELEGATES
Tyler Whisman, Florence Speaker of the House
Matt Martin, Louisville Vice Speaker of the House
KPERF ADVISORY COUNCIL
Ann Amerson, Lexington
Kim Croley, Corbin
KPhA/KPERF HEADQUARTERS
1228 US 127 South, Frankfort, KY 40601
502.227.2303 (Phone) 502.227.2258 (Fax)
www.kphanet.org
www.facebook.com/KyPharmAssoc
www.twitter.com/KyPharmAssoc
Robert McFalls
Executive Director
Matt Worthy, PharmD
Director of Professional & Clinical Services
Scott Sisco
Director of Communications and Continuing Education
Kelli Sheets
Office Manager
Christine Richardson, PharmD
Clinical Pharmacist
Darcie Nixon
Administrative Coordinator & Billing Specialist
Nancy Baldwin
Receptionist/Office Assistant
KPhA Board of Directors

May 2012
THE KENTUCKY PHARMACIST 47
Kentucky Pharmacists Association 1228 US 127 South Frankfort, KY 40601 (502) 227-2303 www.kphanet.org Kentucky Board of Pharmacy State Office Building Annex, Ste. 300 125 Holmes Street Frankfort, KY 40601 (502) 564-7910 www.pharmacy.ky.gov Pharmacy Technician Certification Board 2215 Constitution Avenue Washington, DC 20037-2985 (800) 363-8012 www.ptcb.org Kentucky Society of Health Systems Pharmacists 1501 Twilight Trail Frankfort, KY 40601 (502) 223-5322 www.kshp.org
Kentucky Regional Poison Center (800) 222-1222
American Pharmacists Association (APhA) 2215 Constitution Avenue NW Washington, DC 20037-2985 (800) 237-2742 www.aphanet.org
National Community Pharmacists Association (NCPA) 100 Daingerfield Road Alexandria, VA 22314 (703) 683-8200 [email protected]
Drug Information Center Sullivan University College of Pharmacy 2100 Gardiner Lane Louisville, KY 40205 (502) 413-8638 www.sullivan.edu
Frequently Called and Contacted
Frequently Called and Contacted
KPhA Remembers KPhA desires to honor members who are no longer with us.
Please keep KPhA informed by sending this information to [email protected].
Deceased members for each year will be honored permanently at the KPhA office with a White Coat.
KPhA Classifieds
Western Kentucky Pharmacist available for relief/part-time work. Experienced in retail, long-term care, home IVs, hos-pital and consulting. Willing to drive. Respond to The Ken-tucky Pharmacist ([email protected]) or cell (270-625-2434.)
Director of Pharmacy
75-bed hospital in South-central KY seeking pharmacist director. Doctorate of Pharmacy or 10 years experience as Registered Pharmacist. KY license. Hospital experience, preferred. Ability to develop/implement policies/processes consistent with hospital, state and federal regulatory guide-lines and maintain continuous compliance. Email [email protected] resume and salary require-ments.

May 2012
THE KENTUCKY PHARMACIST 48
THE
Kentucky PHARMACIST
1228 US 127 South
Frankfort, KY 40601
134th KPhA Annual Meeting
June 13-16, 2012
Griffin Gate Marriott Resort and Spa
Lexington, KY
Visit www.kphanet.org for updates.
Look inside for a tentative schedule!