the prognostic role of immunohistochemistry in...
TRANSCRIPT

THE PROGNOSTIC ROLE OF IMMUNOHISTOCHEMISTRY IN
SARCOMAS
Jason L. Hornick, MD, PhD
March 21, 2010
Department of PathologyBrigham and Women’s Hospital
Harvard Medical SchoolBoston, MA, USA
IMMUNOHISTOCHEMISTRY IN SARCOMA CLASSIFICATION
• IHC plays central role in sarcoma diagnosis
–Confirm histologic impression–Confirm histologic impression
–Distinguish among histologicallysimilar tumors
–Support diagnosis of rare tumor type
–Support diagnosis when tumor arises in unusual location or unusual age group
IMMUNOHISTOCHEMISTRY IN SARCOMA CLASSIFICATION
• Diagnostic IHC markers for sarcomas:
–Markers of differentiation/lineage
»SMA, desmin, caldesmon, myogenin, »SMA, desmin, caldesmon, myogenin, S-100 protein, KIT, EMA, keratins
–Protein correlates of molecular findings
»ALK, MDM2/CDK4, TFE3, INI1, TLE1

Inflammatory WDLPS MDM2
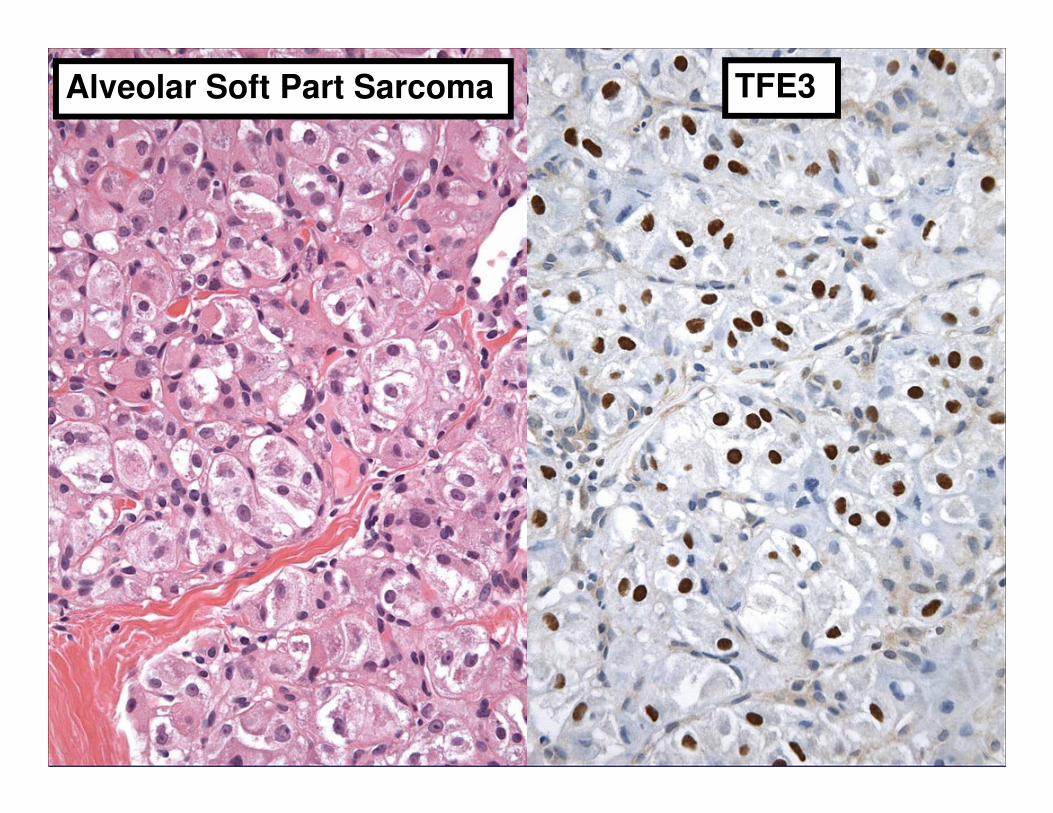
Alveolar Soft Part Sarcoma TFE3
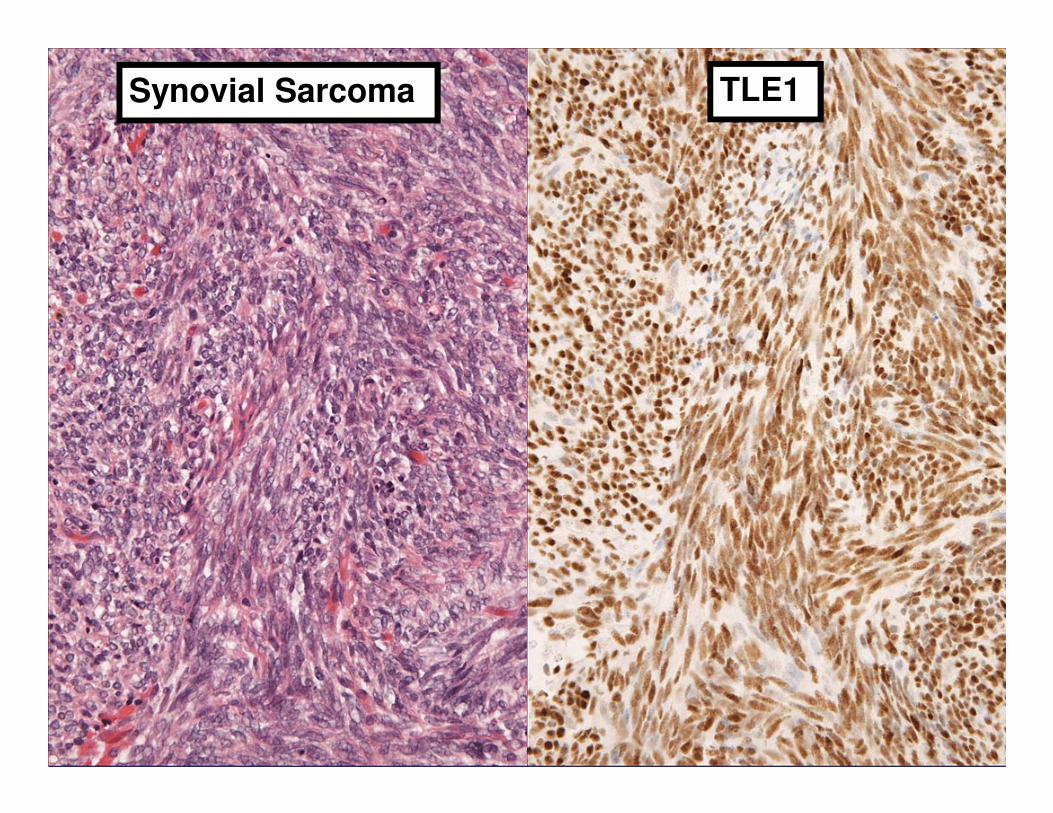
Synovial Sarcoma TLE1
TRADITIONAL PROGNOSTIC MARKERS FOR CANCER
• Tumor size
• Stage
• Lymph node metastases
• Grade
• Vascular invasion
REQUIREMENTS OF NEW PROGNOSTIC MARKER FOR ACCEPTANCE IN CLINICAL
PRACTICE
• Assessment is reproducible and widely available with quality controls
• Substantial added value beyond • Substantial added value beyond established prognostic markers
• Results confirmed by additional independent studies
Simon and Altman. Br J Cancer 1994;69:979-85.
TYPES OF PROGNOSTIC MARKER STUDIES IN CANCER
• Phase I: Exploratory studies (hypothesis generating): seek association between potential marker and disease characteristics that have prognostic importance (grade, stage)
• Phase II: Exploratory studies: evaluate ability of prognostic marker to discriminate between patients at high and low risk of disease progression or death
• Phase III: Confirmatory studies (preferably large, collaborative); independent data sets
Riley et al. Br J Cancer 2009;100:1219-29.
PROBLEMS WITH PROGNOSTIC MARKER STUDIES
• How to determine sample size?
• Cutpoint used to dichotomize continuous marker into “high” (positive) or “low” (negative)?(negative)?
• Multivariable regression including all known prognostic markers/factors (independent significance)
• Publication bias (selective reporting)
• Lack of systematic reviews and/or meta-analyses

PROBLEMS WITH PROGNOSTIC MARKER STUDIES FOR SARCOMA
• Rare diseases – small sample sizes
• Variability in diagnosis/classification among pathologistsamong pathologists
• Variability in treatment among oncologists
• Prospective studies nearly impossible
IMMUNOHISTOCHEMISTRY IN SARCOMA PROGNOSTICATION?
• No currently accepted clinical role, beyond classification/diagnosis (along with grade, most important prognostic factors)factors)
• Numerous “biomarkers” evaluated, most in single retrospective studies
• “Traditional” markers (>20 yrs) such as Ki-67 and p53
• Newer markers identified through gene expression profiling
Ki-67 (MIB-1)
• Recognizes nuclear antigen
• Expressed in proliferating cells
• Preferentially late G1, S, G2, M• Preferentially late G1, S, G2, M
• Not expressed in G0
• Widely used in pathology as marker of proliferation; criterion for malignancy or grade (some organ systems)

p53
• Key role in cell cycle and apoptosis
• Tumor suppressor gene commonly mutated in diverse cancersmutated in diverse cancers
• Wild-type protein weak/negative by IHC
• Mutant protein extended half-life, detectable by IHC (“overexpression”)
• Strong positive staining by IHC reasonable correlation with p53 mutation
OUTLINE
1. Prognostic studies including all types of soft tissue sarcomas
2. Myogenic differentiation in pleomorphic2. Myogenic differentiation in pleomorphicsarcomas
3. Extent of myogenin expression in rhabdomyosarcoma
4. Tumor type-specific prognostic studies
PROGNOSTIC STUDIES INCLUDING ALL TYPES OF INCLUDING ALL TYPES OF SOFT TISSUE SARCOMAS
J Natl Cancer Inst. 1994;86:549-54.Drobnjak et al.
• 174 adult soft tissue sarcomas (heterogeneous types)
• IHC for p53 and Ki-67
• >20% cut-off for each
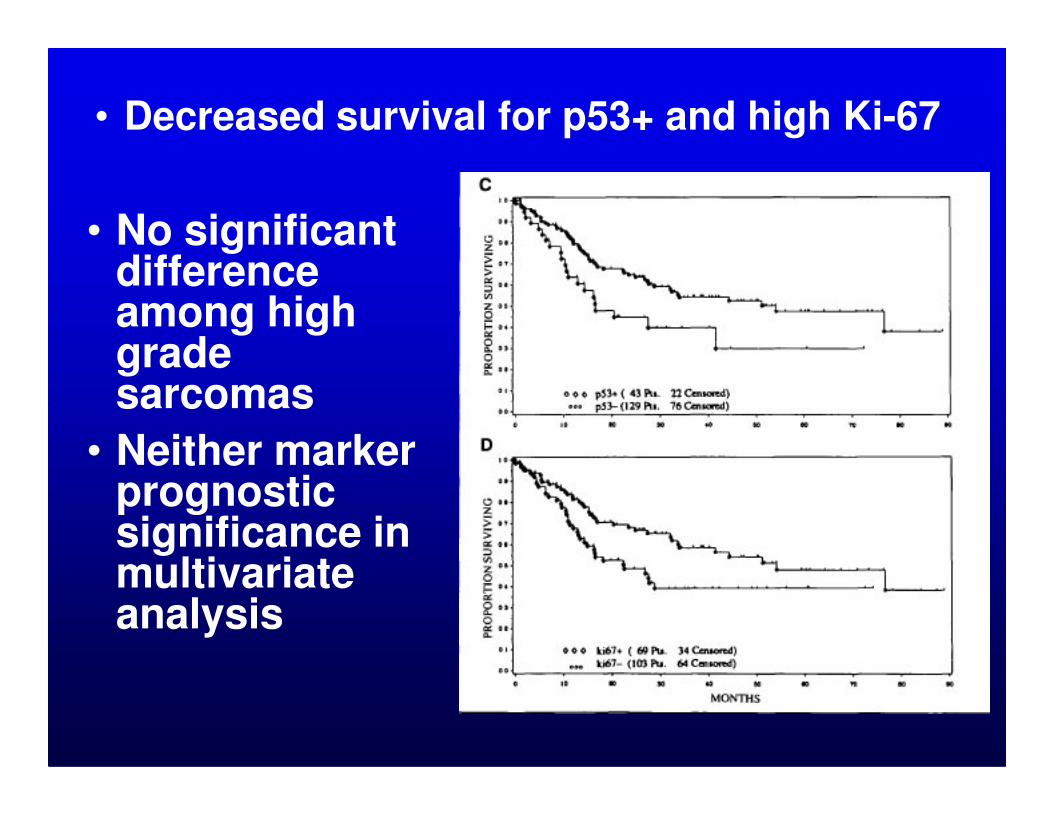
• No significant difference among high grade sarcomas
• Decreased survival for p53+ and high Ki-67
sarcomas
• Neither marker prognostic significance in multivariate analysis
J Clin Oncol. 1997;15:3249-57.Levine et al.
• 52 adult soft tissue sarcomas (heterogeneous types)
• IHC for Ki-67
• >40% cut-off = “high”
–84% “low” Ki-67
–16% “high” Ki-67

• Decreased survival for high Ki-67
• Grade not included in multivariate analysis
Histopathology 1998;32:536-46.Jensen et al.
• 216 soft tissue sarcomas (heterogeneous types)
• IHC for Ki-67 and p53• IHC for Ki-67 and p53
• >10% cut-off for p53
• >12% cut-off for Ki-67 (median)
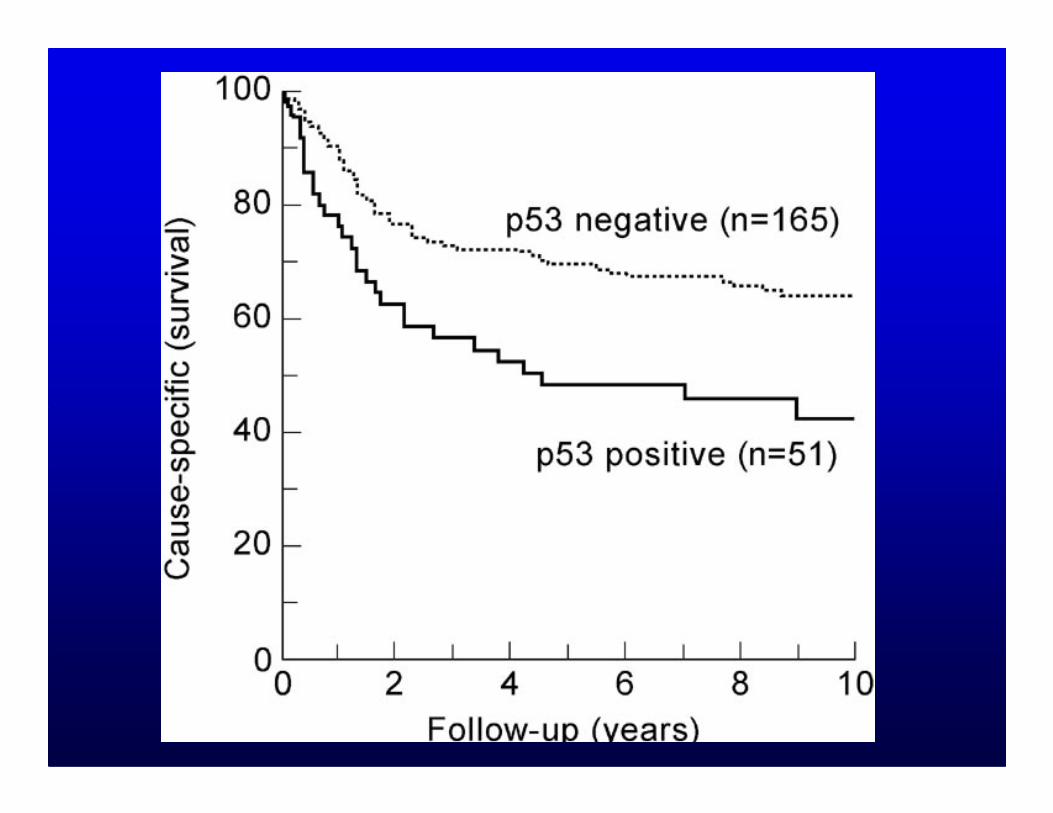
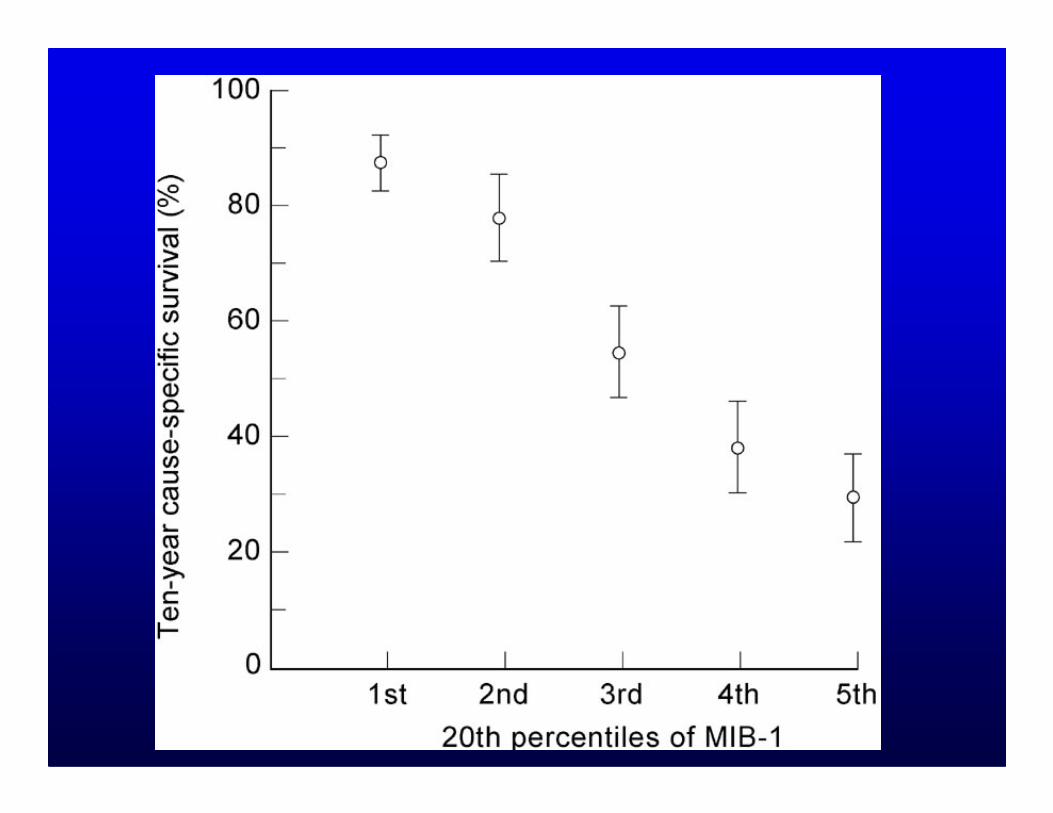
Histopathology 1998;32:536-46.Jensen et al.
• Grade strongest predictor of survival
• No effect of Ki-67 on survival for “MFH”
• Among high grade sarcomas other than • Among high grade sarcomas other than “MFH”, Ki-67 strong independent predictor of survival
Oncogene 1998;16:1183-5.Würl et al.
• 86 primary extremity soft tissue sarcomas (heterogeneous types)
• IHC for p53 and MDM2
• >10% cut-off for each
– 57% positive for p53
– 70% positive for MDM2
– 46% positive for both

Cancer 1998;83:490-7.Heslin et al.
• 121 localized high grade soft tissue sarcomas of extremities (heterogeneous types)(heterogeneous types)
• IHC for Ki-67 and p53
• >20% cut-off for each
–Ki-67 “increased” in 69%
–p53 “positive” in 9%
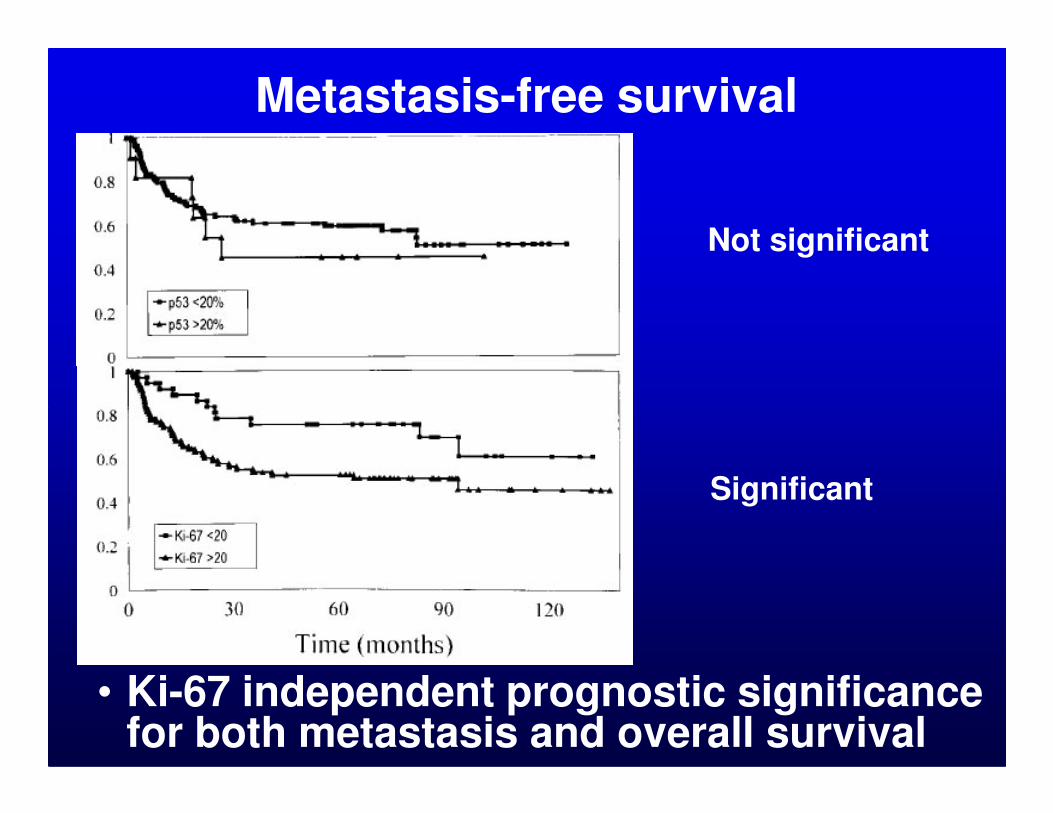
Metastasis-free survival
Not significant
• Ki-67 independent prognostic significance for both metastasis and overall survival
Significant
Comments
• Ki-67 not a replacement for grading
• Ki-67 may be prognostic for (some) high grade sarcomas
• p53 aberrations nearly exclusive to high grade sarcomas
• Given marked differences in behavior for sarcoma subtypes, difficult to draw meaningful conclusions
MYOGENIC DIFFERENTIATION IN PLEOMORPHIC
SARCOMASSARCOMAS

J Clin Oncol. 2001;19:3045-50.Fletcher et al.
• 100 “MFH” of extremities/trunk wall re-classified
• Upon re-review:
–29 myxofibrosarcomas
–20 leiomyosarcomas
–30 overall some form of high grade myogenic sarcoma

Myogenic tumors (stage II/III) worse metastasis-free survival

Cancer 2003;98:805-13.Deyrup et al.
• 92 pleomorphic sarcomas of extremities
• IHC for SMA, MSA, desmin, • IHC for SMA, MSA, desmin, myoglobin
– 42 positive for at least 1 marker
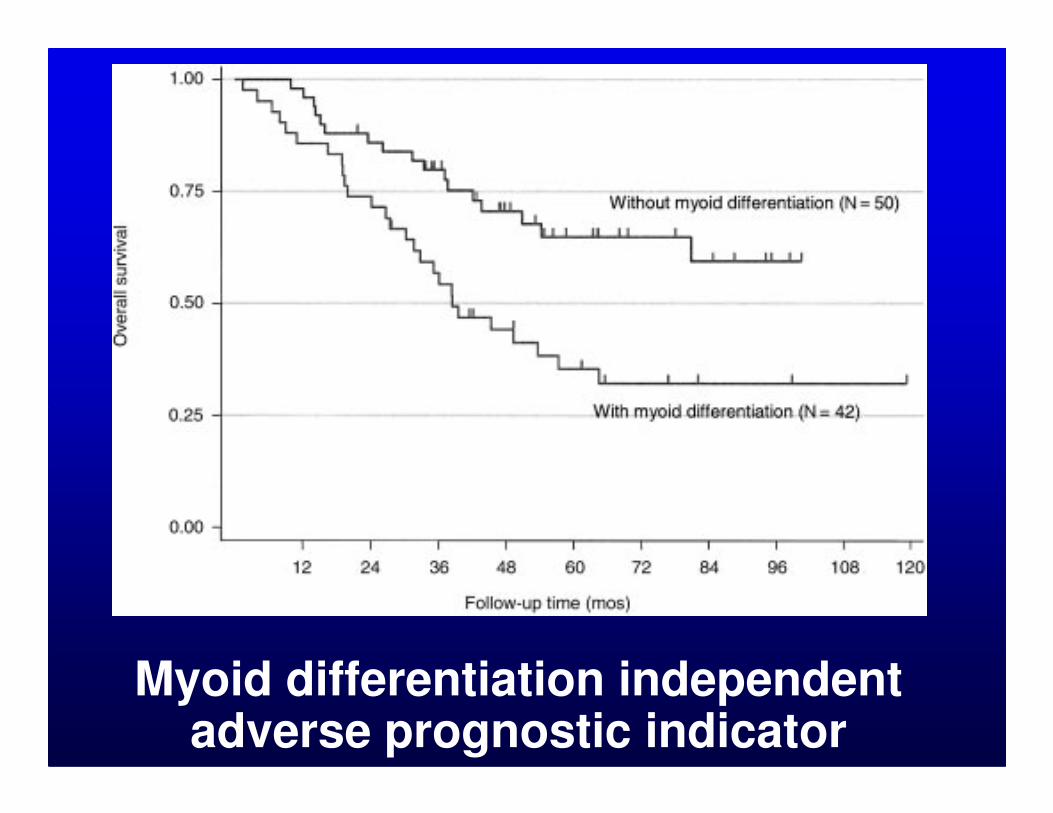
Myoid differentiation independent adverse prognostic indicator
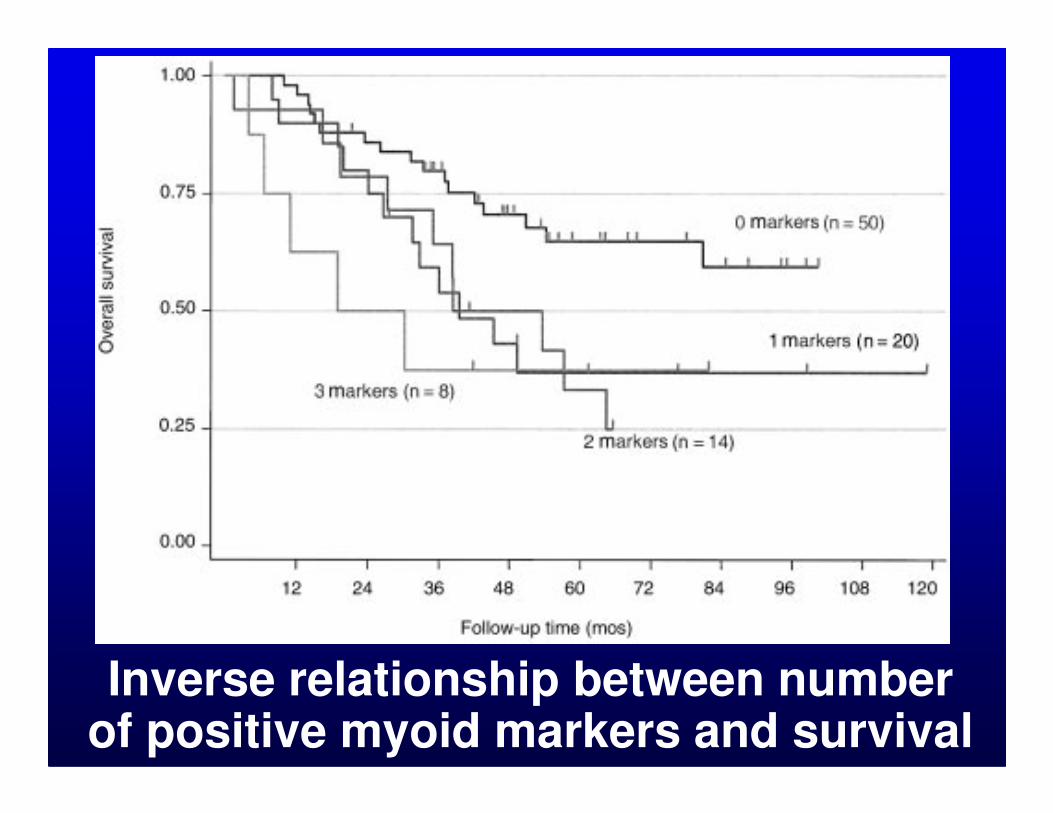
Inverse relationship between number of positive myoid markers and survival
Eur J Surg Oncol. 2004;30:1131-6.Massi et al.
• 65 pleomorphic sarcomas of extremities re-evaluated
• Upon re-review:• Upon re-review:
–22 leiomyosarcomas
–13 myxofibrosarcomas
–9 other myogenic sarcomas

Myogenic differentiation only independent predictor of overall survival
Comments
• Subclassification of pleomorphicsarcomas clinically significant
• IHC plays important role identify/ confirm myogenic sarcomasconfirm myogenic sarcomas
• Pleomorphic sarcomas with myogenic differentiation (not only LMS, RMS) higher metastatic potential
EXTENT OF MYOGENIN EXPRESSION IN
RHABDOMYOSARCOMARHABDOMYOSARCOMA
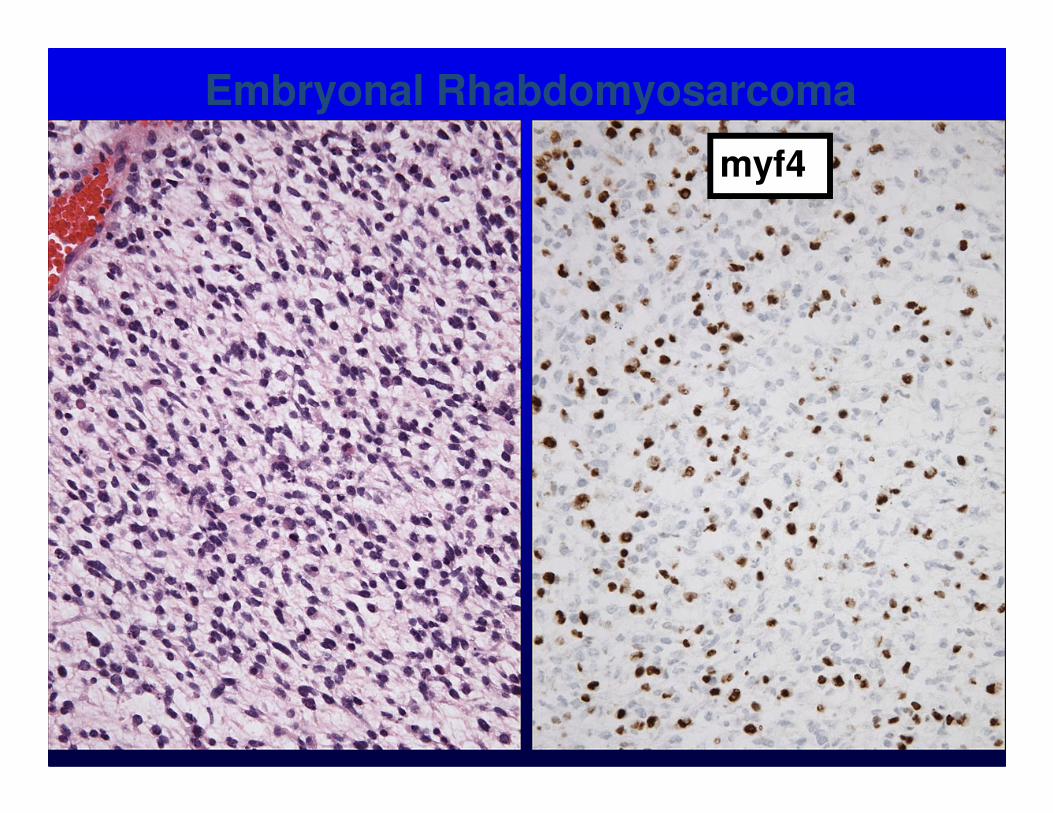
Embryonal Rhabdomyosarcoma
myf4

(Solid) Alveolar Rhabdomyosarcoma
myf4
Am J Surg Pathol. 2008;32:1513-22.Heerema-McKenney et al.
• 71 pediatric rhabdomyosarcomas
• IHC for myogenin (myf4)
• <80% = “focal”• <80% = “focal”
• >80% = “diffuse”
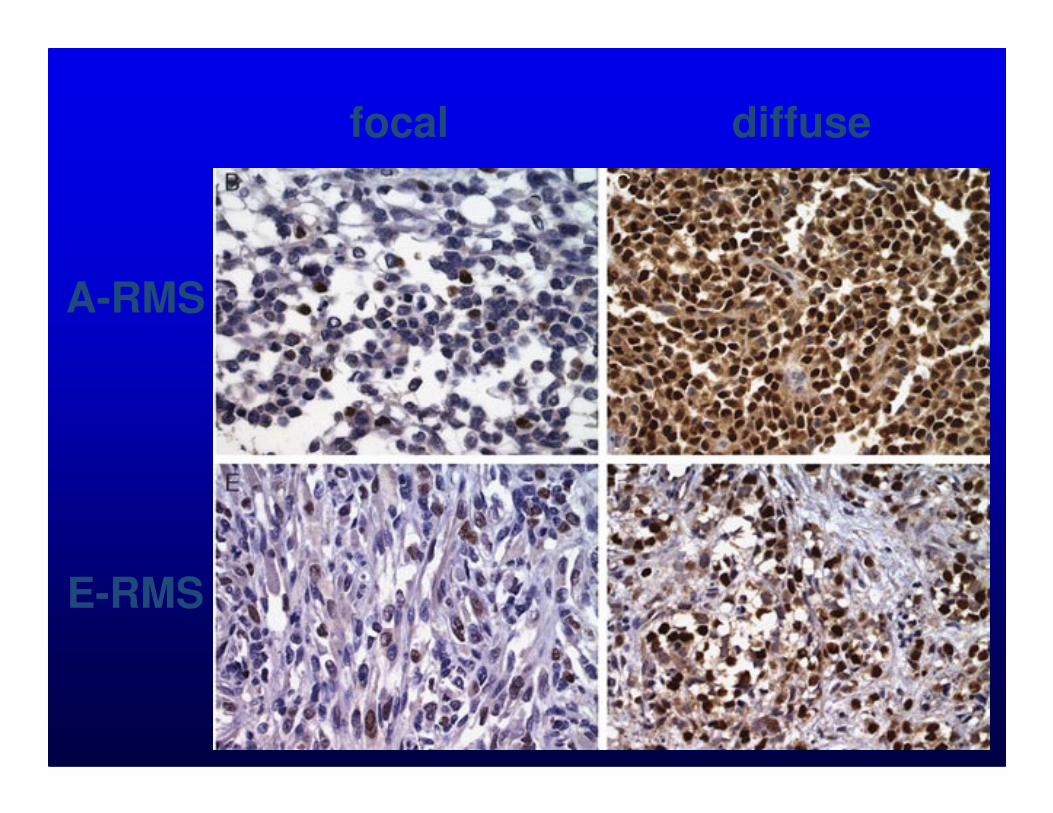
focal diffuse
A-RMS
E-RMS
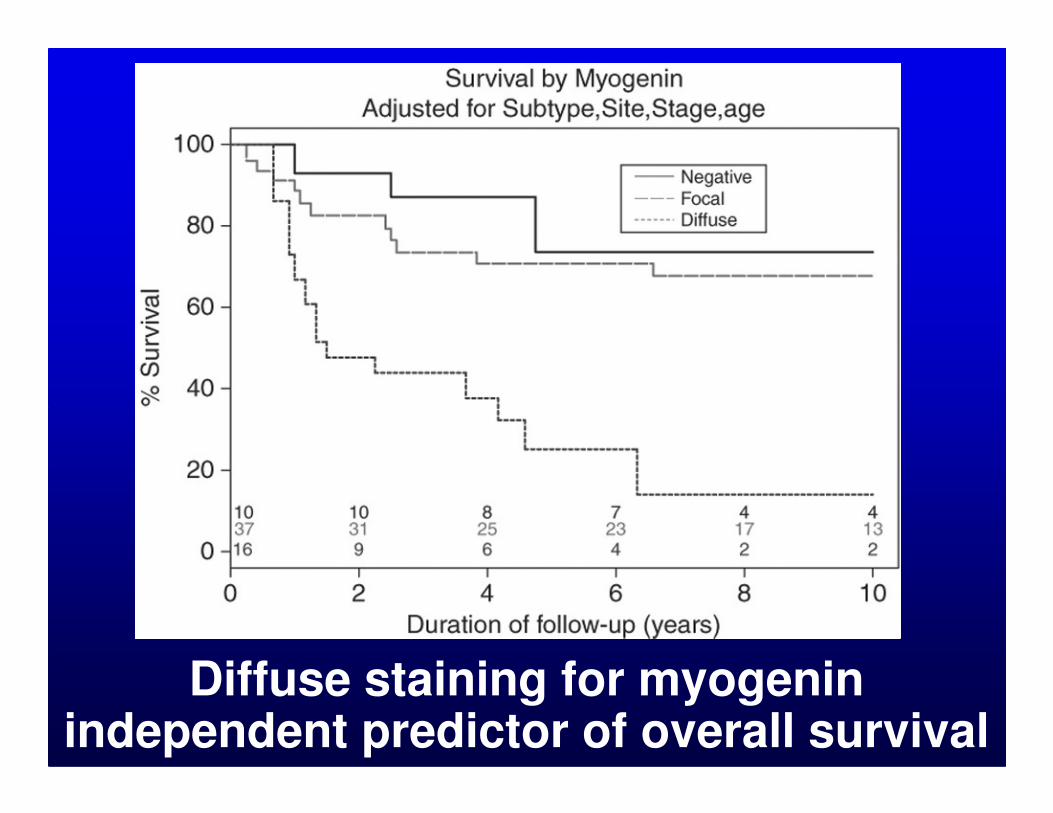
Diffuse staining for myogeninindependent predictor of overall survival
INDIVIDUAL TUMOR TYPE-SPECIFIC PROGNOSTIC SPECIFIC PROGNOSTIC
STUDIES
Mod Pathol. 1997;10:91-7.O’Reilly et al.
• 35 patients with extra-uterine leiomyosarcoma
• IHC for p53 and Ki-67
• No correlation between staining for p53 or Ki-67 and overall or recurrence-free survival
Br J Cancer 1999;80:1809-14.Skytting et al.
• 86 patients with primary localized synovial sarcoma
• IHC for p53 and MIB-1• IHC for p53 and MIB-1
• >10% cut-off for MIB-1
• >25% cut-off for p53
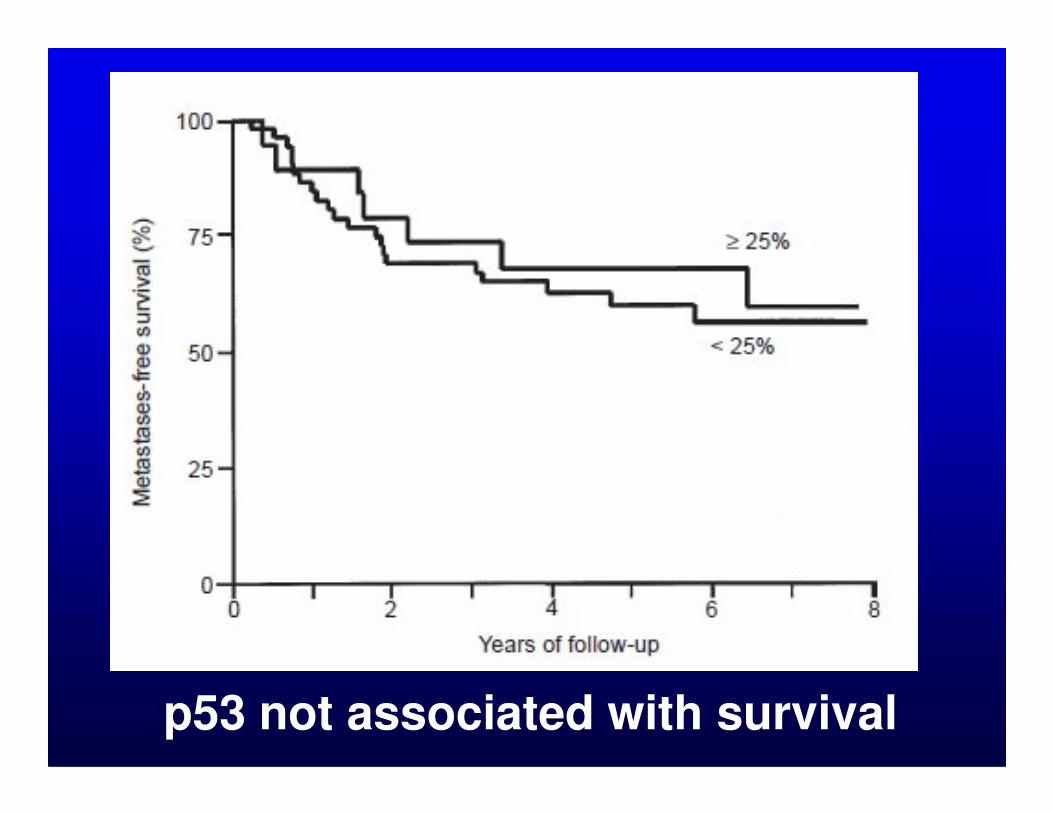
p53 not associated with survival

MIB-1 index significantly associated with metastasis
Am J Pathol. 2000;156:977-83.Antonescu et al.
• 49 patients with localized synovial sarcoma of extremities
• IHC for cell cycle-associated • IHC for cell cycle-associated proteins, p53 and Ki-67
• >20% cut-off for Ki-67 (59% +)
• >10% cut-off for p53 (16% +)
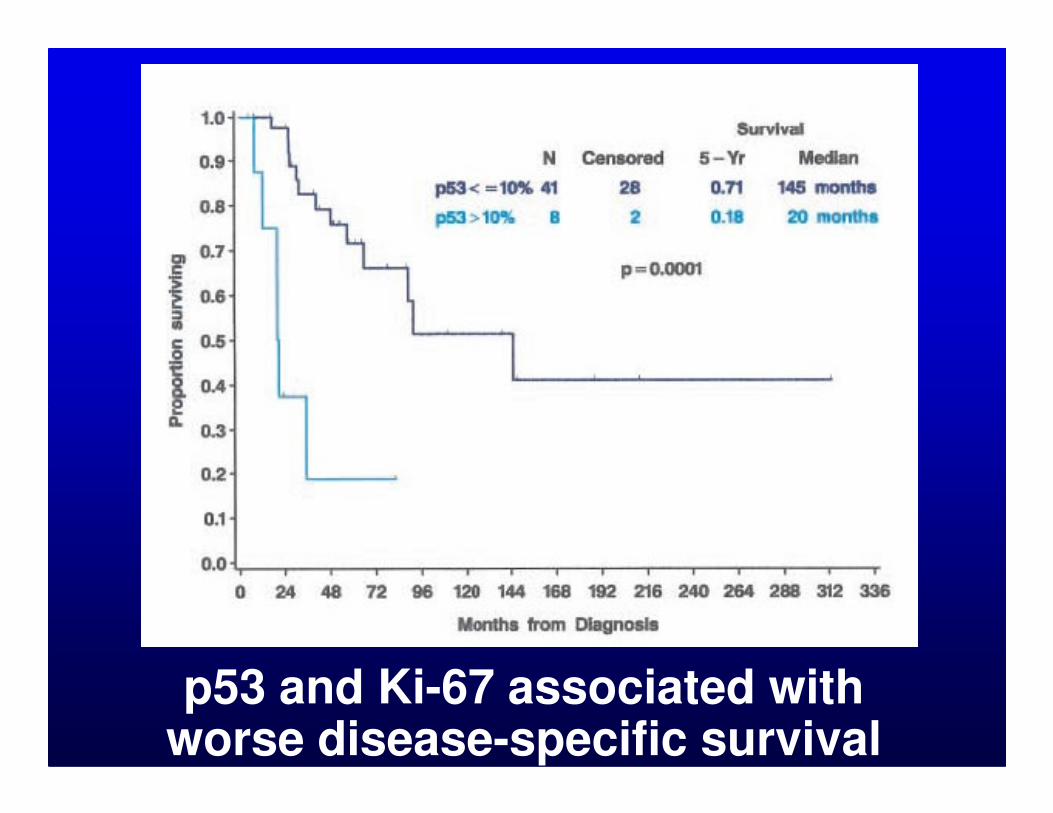
p53 and Ki-67 associated with worse disease-specific survival
Clin Cancer Res. 2001;7:3977-87.Antonescu et al.
• 71 patients with myxoidliposarcoma
• IHC for p53 • IHC for p53
• >10% cut-off (17% positive)
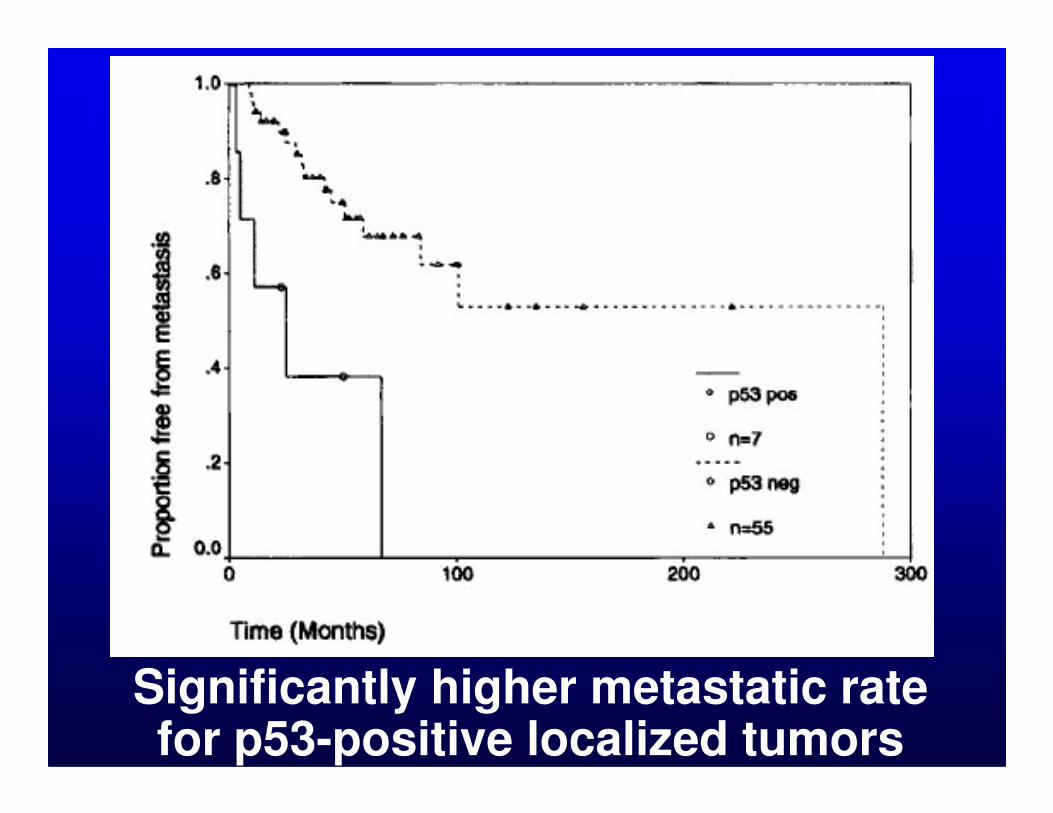
Significantly higher metastatic rate for p53-positive localized tumors
Hum Pathol. 2009;40:1244-51.Cheng et al.
• 32 patients with myxoidliposarcoma
• IHC for adipogenesis and • IHC for adipogenesis and proliferation-related proteins (RET, IGF1R, IGF2)
• >50% considered positive
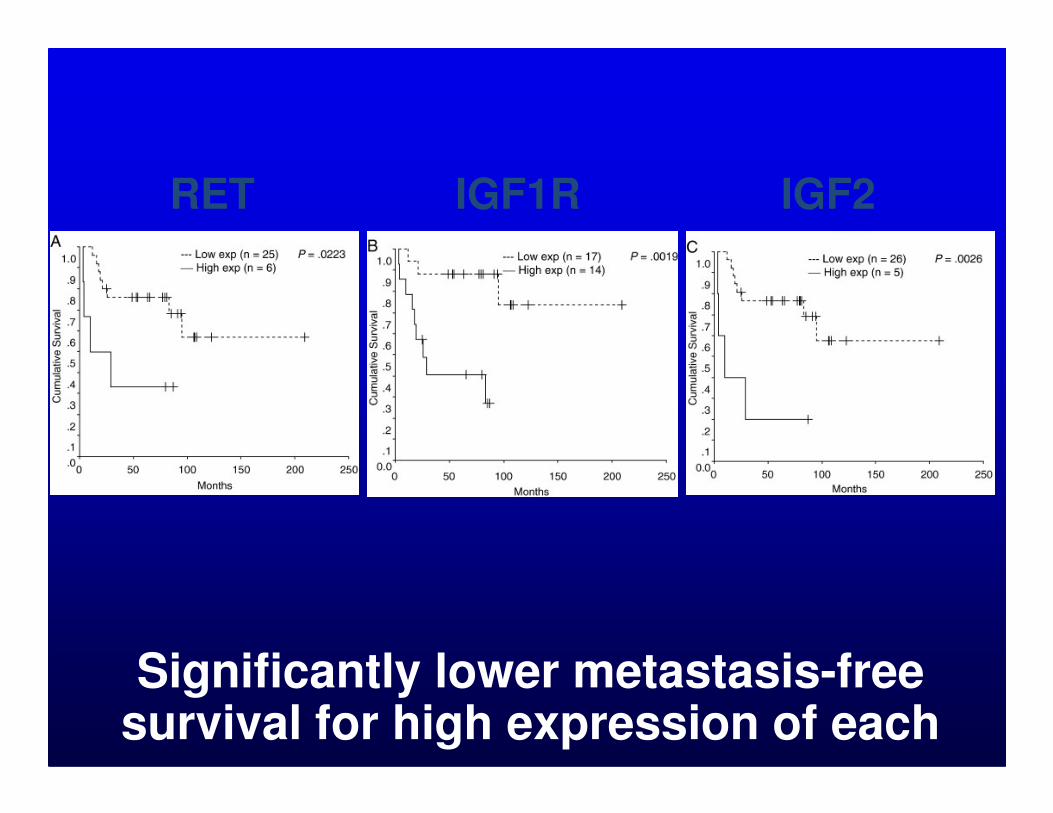
RET IGF1R IGF2
Significantly lower metastasis-free survival for high expression of each
Mod Pathol. 2009;22:1432-8.Tsiatis et al.
• 28 patients with leiomyosarcomaof deep somatic soft tissue
• IHC for c-myc• IHC for c-myc
• >5% considered positive

LMS c-myc
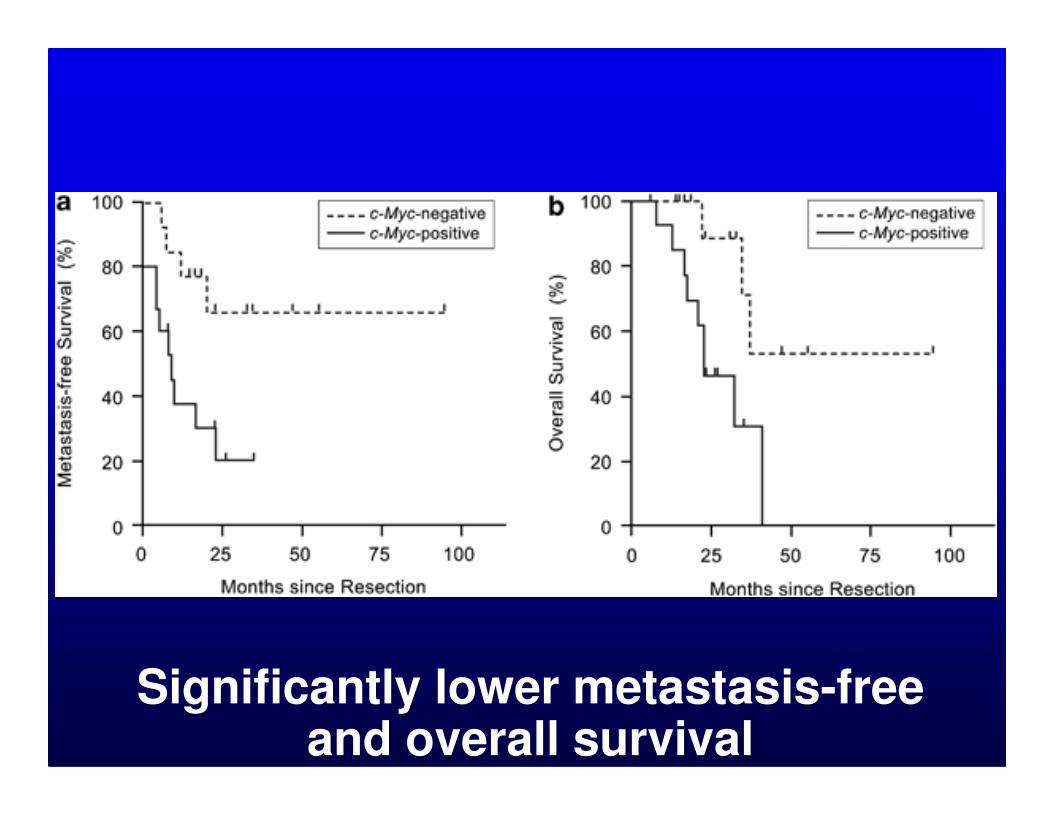
Significantly lower metastasis-free and overall survival
Am J Surg Pathol. 2008;32:1627-42.Schirosi et al.
• 88 patients with pleuropulmonarysolitary fibrous tumor
• IHC for p53, various kinases• IHC for p53, various kinases
• >5% considered positive
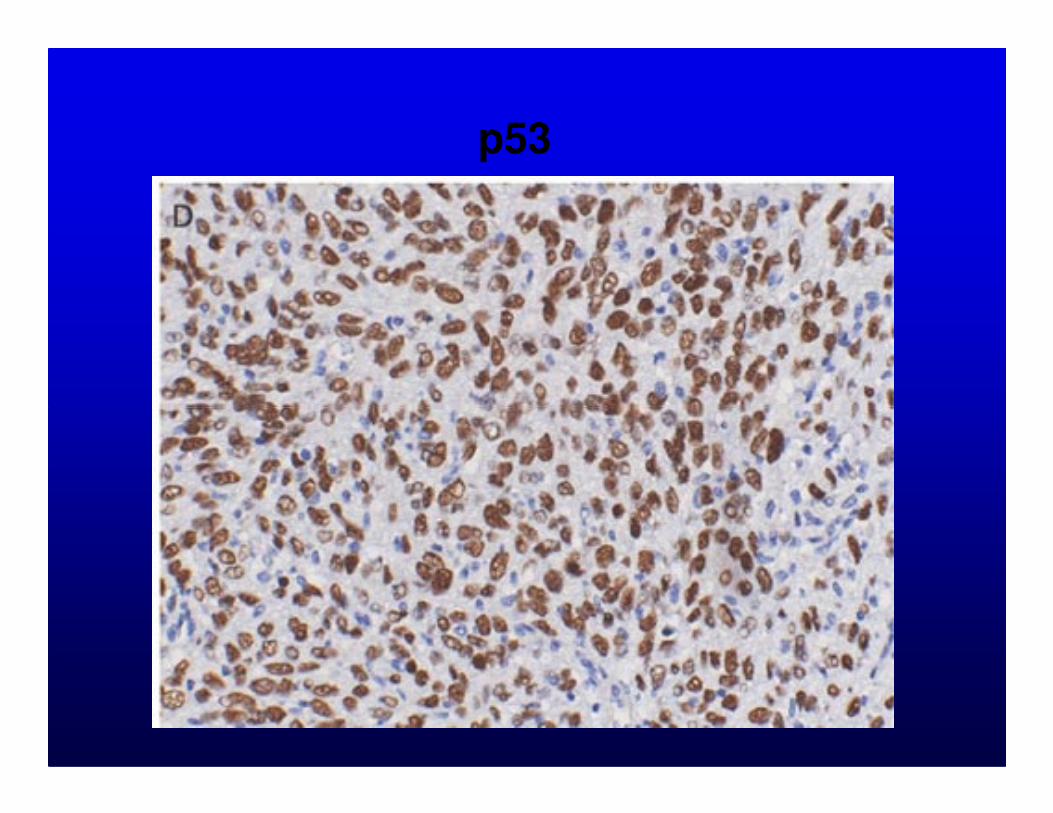
p53
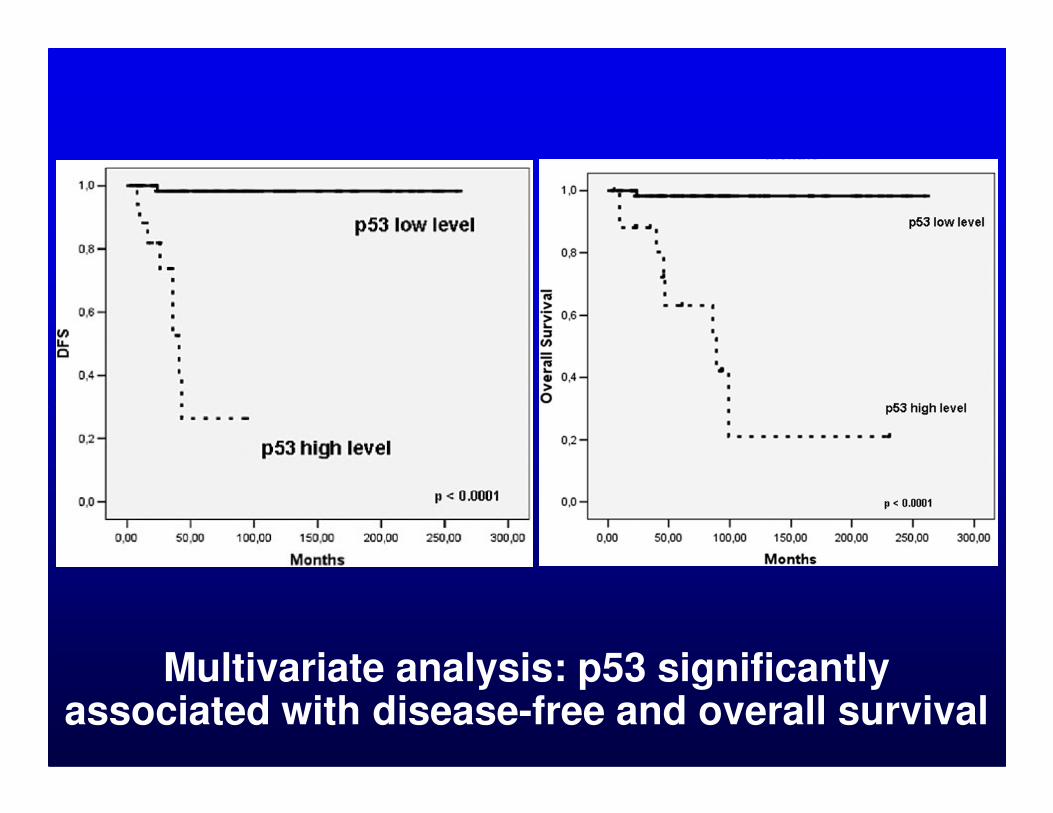
Multivariate analysis: p53 significantly associated with disease-free and overall survival
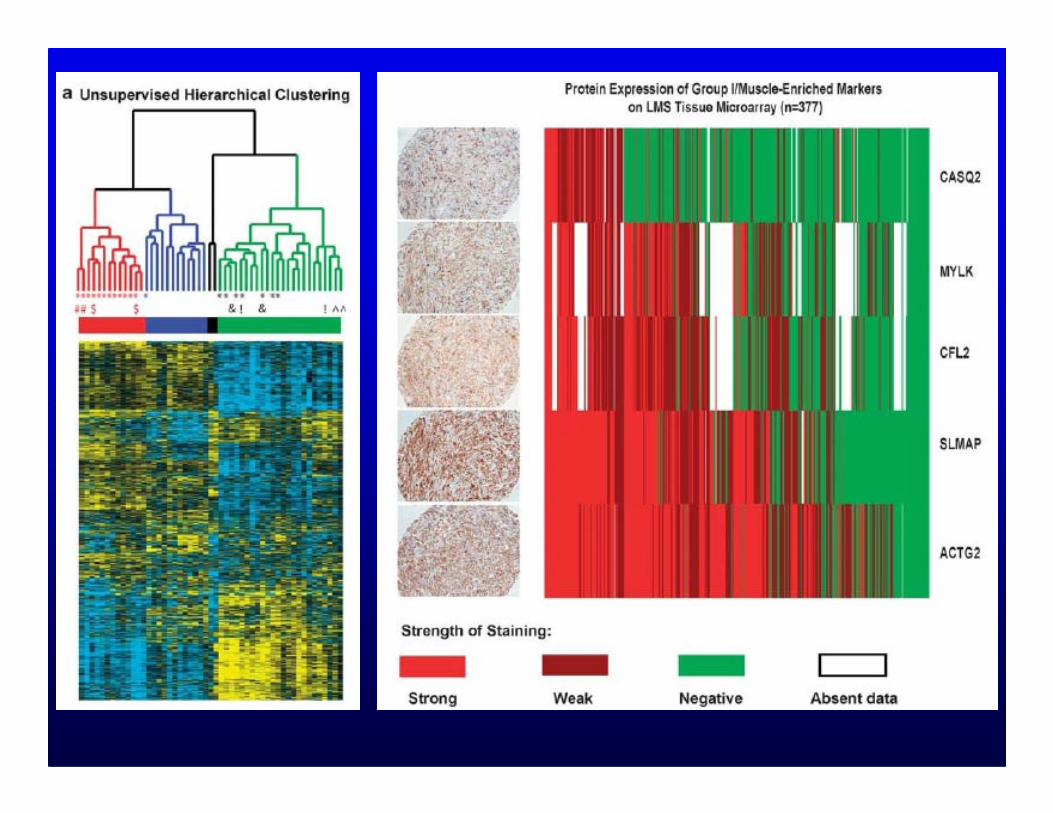
Oncogene 2009 Nov 9 [Epub]Beck et al.
• Gene expression profiling on 51 leiomyosarcomas
• Unsupervised clustering: 3 • Unsupervised clustering: 3 clusters (1 “muscle-enriched”)
• IHC on TMA for 5 markers with high mRNA in “muscle-enriched” cluster
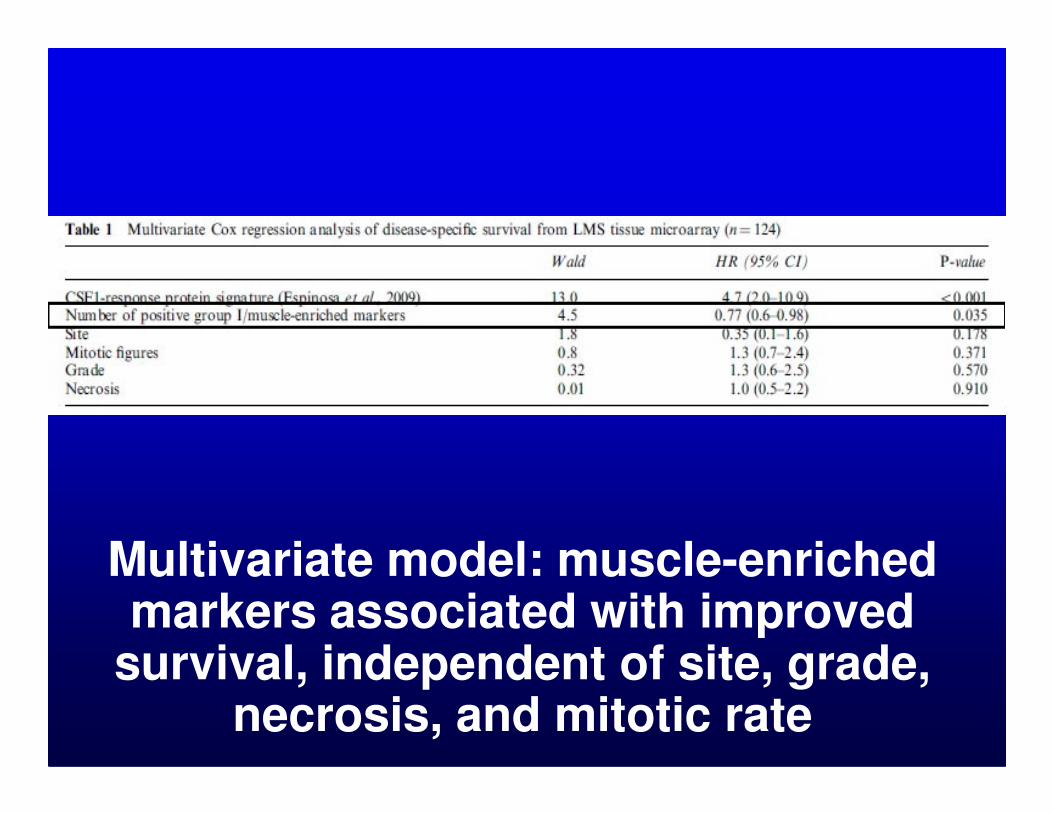
Multivariate model: muscle-enriched markers associated with improved
survival, independent of site, grade, necrosis, and mitotic rate
Final Comments IPrognostic Role of IHC in Sarcomas
• IHC for accurate diagnosis (critical for outcome prediction)
• Other than diagnosis, grade remains key • Other than diagnosis, grade remains key prognostic determinant
• Myogenic differentiation in pleomorphicsarcomas prognostic significance
• Other “biomarkers” not yet ready for prime time
Final Comments IIPrognostic Role of IHC in Sarcomas
• Studies of single tumor type (uniform histology, grade, etc.)
• Gene expression profiling identifying • Gene expression profiling identifying novel prognostic markers
• Goal will be to stratify patients into lower/higher risk groups – guide selection of therapy
Final Comments IIIPrognostic Role of IHC in Sarcomas
• How to establish threshold for “positive”?
• Need for uniform reporting
• Need for pooled analyses/systematic reviews
• How best to translate to clinical practice?

1
COMPANION MEETING OF THE INTERNATIONAL SOCIETY OF
BONE AND SOFT TISSUE PATHOLOGY
Washington, DC, March 21, 2010
PROGNOSTICATION IN TUMORS OF SOFT TISSUE AND BONE
THE PROGNOSTIC ROLE OF IMMUNOHISTOCHEMISTRY IN
SARCOMAS
Jason L. Hornick, M.D., Ph.D. Brigham and Women's Hospital and Harvard Medical School, Boston, MA, USA
Over the past 25 years, immunohistochemistry (IHC) has played a central role in the
classification of mesenchymal tumors. The chief contribution of IHC to diagnosis is to
distinguish among histologically similar tumors, but IHC can also be applied (often for
reassurance) to support the diagnosis of rare tumor types or to support the diagnosis when a
tumor arises at an unusual location or in an unusual age group. The majority of the widely
available IHC markers for sarcomas suggest lines of differentiation, such as smooth muscle actin
and desmin for smooth muscle or myofibroblastic tumors, myogenin (myf-4) for skeletal muscle
neoplasms, and S-100 protein for nerve sheath (Schwann cell) tumors. Unfortunately, few of
these traditional markers are highly specific, and therefore a panel of markers is usually needed,
and the results must be interpreted carefully in the context of the histologic and clinical findings.
More recently, diagnostic IHC markers have been developed that can serve as surrogates for
specific molecular findings, such as ALK for inflammatory myofibroblastic tumor, MDM2 and
CDK4 for well-differentiated and dedifferentiated liposarcoma, TFE3 for alveolar soft part
sarcoma, INI1 for malignant rhabdoid tumor and epithelioid sarcoma, and TLE1 for synovial
sarcoma. However, IHC has no currently accepted clinical role in prognostication for sarcomas,
beyond its role in establishing a specific diagnosis (which, along with grade, is among the most
important prognostic factors).
Traditional prognostic markers for cancer in general, which provide critical information
to oncologists both for counseling patients on the likelihood of developing metastases and

2
selecting appropriate systemic therapies, include such factors as tumor size, stage, and grade, and
the presence of vascular invasion and lymph node metastases. In order for novel prognostic
markers to gain acceptance in clinical practice, several broad requirements should be met: (1) the
assessment must be reproducible and widely available with appropriate quality controls; (2) the
marker must have substantial added value beyond that of established prognostic markers; and (3)
the results of prognostic marker studies should be confirmed by additional independent studies.
Prognostic marker studies can be classified into three general groups: phase I exploratory
(hypothesis generating) studies that seek associations between potential markers and disease
characteristics that have known prognostic importance, such as stage or grade; phase II
exploratory studies that evaluate the ability of prognostic markers to discriminate between
patients at high and low risk of disease progression or death; and phase III confirmatory studies
that seek to validate the results of phase II studies using independent (preferably large and
collaborative) data sets. These latter studies would ideally be prospective and protocol-driven,
although systematic reviews or meta-analyses of phase II studies using pooled data are
reasonable alternatives. Unfortunately, nearly all prognostic studies of IHC markers are phase
II-type studies, without confirmatory follow-up studies using independent data sets. Indeed, it is
uncommon for more than one study to evaluate a specific potential prognostic IHC marker.
In addition to the lack of critical confirmatory studies and systematic reviews, there are
many other important issues that must be addressed for prognostic marker studies to yield
clinically meaningful and applicable results. For example, how should continuous markers be
dichotomized into "high" (or positive) and "low" (or negative) results? This question is
particularly relevant to IHC studies, where the evaluated markers often show a range of staining
in terms of both extent and intensity. Publication bias is also a significant issue for IHC-based
prognostic studies, since such studies that yield negative results are rarely published, and,
similarly problematic, published studies sometime omit the results of markers that failed to reach
significance. Furthermore, multivariable regression models that include all known prognostic
factors must be employed to determine whether the evaluated markers have independent
prognostic significance. There are also additional problems that pertain to prognostic marker
studies particularly relevant to sarcomas. Since sarcomas are very rare diseases, sample size is
always an issue, and prospective studies are nearly impossible to perform. In addition, there can
3
be variability in both diagnosis and treatment of sarcomas among different cancer centers,
pathologists and oncologists.
Many potential prognostic "biomarkers" have been evaluated in sarcomas, most in single
or small numbers of retrospective studies. These range from "traditional" markers such as Ki-67
and p53, which have been studied for more than 20 years, to newer markers that are being
identified through gene expression profiling. Ki-67 (or MIB-1) recognizes a nuclear antigen
expressed in proliferating cells, preferentially in late G1, S, G2, and M phases of the cell cycle,
but not in quiescent cells (G0). Ki-67 is widely used in pathology as a marker of proliferation,
and, in some organ systems, as a criterion for malignancy or grading. The p53 gene encodes a
protein that plays a key role in the cell cycle and apoptosis. p53 acts as a tumor suppressor gene;
a wide variety of human cancers harbor loss-of-function p53 mutations. Since the wild-type p53
protein is rapidly degraded, IHC for p53 shows negative or weak staining in normal cells,
whereas mutant p53 proteins usually have an extended half-life, and therefore tumor cells
harboring p53 mutations usually show strong positive staining by IHC.
The "first generation" of prognostic IHC marker studies of sarcomas included all types
(and grades) of tumors. These studies often reported conflicting results with regard to the
prognostic significance of positive staining for p53 and/or a high Ki-67 index, and most failed to
demonstrate independent prognostic significance of these markers in multivariate analysis. In
contrast, more recent individual tumor type-specific prognostic IHC marker studies of sarcomas,
including synovial sarcoma and myxoid liposarcoma, have demonstrated independent prognostic
significance for expression of p53 and other IHC markers. Similarly, recent studies using gene
expression profiling have identified groups of markers whose expression is associated with
prognosis. These results have yet to be confirmed by other groups on independent data sets, and
it is not yet clear how these findings can be translated to clinical practice.
Several retrospective studies have evaluated the prognostic significance of myogenic
differentiation in pleomorphic sarcomas. In the first such study by Fletcher and colleagues in
2001, 100 extremity and trunk wall tumors formerly diagnosed as "malignant fibrous
histiocytoma" were re-classified applying strict diagnostic criteria, in conjunction with IHC and
4
electron microscopy (in select cases). Upon re-review, the most common sarcoma types were
high grade leiomyosarcoma and myxofibrosarcoma. In total, 30 of the tumors were classified as
some form of high grade myogenic sarcoma. When the localized myogenic sarcomas were
compared to non-myogenic tumors, the myogenic tumors showed a higher rate of metastasis. In
a follow-up study by Deyrup and colleagues, 92 pleomorphic sarcomas of the extremities were
immunostained for the myogenic markers smooth muscle actin, muscle-specific actin, desmin,
and myoglobin; 42 tumors were positive for at least one marker. Similar to the prior study,
myogenic differentiation was found to be an independent adverse prognostic indicator.
Furthermore, there was an inverse relationship between the number of positive myogenic
markers and survival. A subsequent study by Massi and colleagues re-evaluated 65 pleomorphic
sarcomas of the extremities. Similar to the study by Fletcher, the most common diagnoses on re-
review were leiomyosarcoma and myxofibrosarcoma; 31 tumors in all were some form of
myogenic sarcoma. Upon multivariate analysis, myogenic differentiation was the only
independent predictor of overall survival. These studies confirm the prognostic value of
subclassifying pleomorphic sarcomas, for which IHC plays an important role, as well as
demonstrate that pleomorphic sarcomas with myogenic differentiation (not only pleomorphic
leiomyosarcoma and rhabdomyosarcoma, which are known to pursue an aggressive clinical
course) have a higher metastatic potential. Such prognostic information can be helpful to select
patients for clinical trials of novel chemotherapeutic agents.
Previous studies have shown that alveolar rhabdomyosarcoma typically displays diffuse
staining for the skeletal muscle transcription factor myf4 (myogenin), whereas embryonal
rhabdomyosarcoma (which has a better clinical outcome) usually expresses myf4 in only
scattered cells. A recent study by Heerema-McKenney and colleagues evaluated the prognostic
significance of the extent of myf4 staining in 71 pediatric rhabdomyosarcomas (>80% nuclear
staining was defined as "diffuse"). Interestingly, the authors found that diffuse staining for myf4
was an independent predictor of overall survival, after adjusting for histologic subtype, anatomic
site, stage, and age.
At present, IHC plays a limited role in prognostication for sarcomas, beyond supporting
accurate diagnosis (which is a critical determinant of outcome). IHC is helpful to identify
5
pleomorphic sarcomas with myogenic differentiation, which have a higher metastatic risk than
those without such differentiation. Other potential "biomarkers" are not yet ready for routine
clinical application. Before the introduction of new IHC prognostic markers, thresholds for
"positive" results will need to be examined, both in terms of biological relevance and so that the
results can be reliably (and reproducibly) reported. Along these lines, there is a need for more
uniform reporting of the results of these sorts of studies, to allow for systematic reviews
including pooled analyses of data, so that novel prognostic markers can be validated and become
a routine part of evaluation by surgical pathologists.
Key words: immunohistochemistry, soft tissue sarcomas, biomarkers, p53, Ki-67

6
Selected references:
Antonescu CR, Leung DH, Dudas M, Ladanyi M, Brennan M, Woodruff JM, Cordon-Cardo C.
Alterations of cell cycle regulators in localized synovial sarcoma: A multifactorial study with
prognostic implications. Am J Pathol. 2000;156:977-83.
Antonescu CR, Tschernyavsky SJ, Decuseara R, Leung DH, Woodruff JM, Brennan MF, Bridge
JA, Neff JR, Goldblum JR, Ladanyi M. Prognostic impact of P53 status, TLS-CHOP fusion
transcript structure, and histological grade in myxoid liposarcoma: a molecular and
clinicopathologic study of 82 cases. Clin Cancer Res. 2001;7:3977-87.
Beck AH, Lee CH, Witten DM, Gleason BC, Edris B, Espinosa I, Zhu S, Li R, Montgomery KD,
Marinelli RJ, Tibshirani R, Hastie T, Jablons DM, Rubin BP, Fletcher CD, West RB, van de Rijn
M. Discovery of molecular subtypes in leiomyosarcoma through integrative molecular profiling.
Oncogene. 2009 Nov 9. [Epub ahead of print] PMID: 19901961.
Cheng H, Dodge J, Mehl E, Liu S, Poulin N, van de Rijn M, Nielsen TO. Validation of immature
adipogenic status and identification of prognostic biomarkers in myxoid liposarcoma using tissue
microarrays. Hum Pathol. 2009;40:1244-51.
Deyrup AT, Haydon RC, Huo D, Ishikawa A, Peabody TD, He TC, Montag AG. Myoid
differentiation and prognosis in adult pleomorphic sarcomas of the extremity: an analysis of 92
cases. Cancer. 2003;98:805-13.
Drobnjak M, Latres E, Pollack D, Karpeh M, Dudas M, Woodruff JM, Brennan MF, Cordon-
Cardo C. Prognostic implications of p53 nuclear overexpression and high proliferation index of
Ki-67 in adult soft-tissue sarcomas. J Natl Cancer Inst. 1994;86:549-54.
Fletcher CD, Gustafson P, Rydholm A, Willén H, Akerman M. Clinicopathologic re-evaluation
of 100 malignant fibrous histiocytomas: prognostic relevance of subclassification. J Clin Oncol.
2001;19:3045-50.
Heerema-McKenney A, Wijnaendts LC, Pulliam JF, Lopez-Terrada D, McKenney JK, Zhu S,
Montgomery K, Mitchell J, Marinelli RJ, Hart AA, van de Rijn M, Linn SC. Diffuse myogenin
expression by immunohistochemistry is an independent marker of poor survival in pediatric
rhabdomyosarcoma: a tissue microarray study of 71 primary tumors including correlation with
molecular phenotype. Am J Surg Pathol. 2008;32:1513-22.
Heslin MJ, Cordon-Cardo C, Lewis JJ, Woodruff JM, Brennan MF. Ki-67 detected by MIB-1
predicts distant metastasis and tumor mortality in primary, high grade extremity soft tissue
sarcoma. Cancer. 1998;83:490-7.
Jensen V, Sørensen FB, Bentzen SM, Ladekarl M, Nielsen OS, Keller J, Jensen OM.
Proliferative activity (MIB-1 index) is an independent prognostic parameter in patients with
high-grade soft tissue sarcomas of subtypes other than malignant fibrous histiocytomas: a
7
retrospective immunohistological study including 216 soft tissue sarcomas. Histopathology.
1998;32:536-46.
Levine EA, Holzmayer T, Bacus S, Mechetner E, Mera R, Bolliger C, Roninson IB, Das Gupta
TK. Evaluation of newer prognostic markers for adult soft tissue sarcomas. J Clin Oncol.
1997;15:3249-57.
Massi D, Beltrami G, Capanna R, Franchi A. Histopathological re-classification of extremity
pleomorphic soft tissue sarcoma has clinical relevance. Eur J Surg Oncol. 2004;30:1131-6.
O'Reilly PE, Raab SS, Niemann TH, Rodgers JR, Robinson RA. p53, proliferating cell nuclear
antigen, and Ki-67 expression in extrauterine leiomyosarcomas. Mod Pathol. 1997;10:91-7.
Riley RD, Sauerbrei W, Altman DG. Prognostic markers in cancer: the evolution of evidence
from single studies to meta-analysis, and beyond. Br J Cancer. 2009;100:1219-29.
Schirosi L, Lantuejoul S, Cavazza A, Murer B, Yves Brichon P, Migaldi M, Sartori G, Sgambato
A, Rossi G. Pleuro-pulmonary solitary fibrous tumors: a clinicopathologic,
immunohistochemical, and molecular study of 88 cases confirming the prognostic value of de
Perrot staging system and p53 expression, and evaluating the role of c-kit, BRAF, PDGFRs
(alpha/beta), c-met, and EGFR. Am J Surg Pathol. 2008;32:1627-42.
Skytting BT, Bauer HC, Perfekt R, Nilsson G, Larsson O. Ki-67 is strongly prognostic in
synovial sarcoma: analysis based on 86 patients from the Scandinavian Sarcoma group register.
Br J Cancer. 1999;80:1809-14.
Tsiatis AC, Herceg ME, Keedy VL, Halpern JL, Holt GE, Schwartz HS, Cates JM. Prognostic
significance of c-Myc expression in soft tissue leiomyosarcoma. Mod Pathol. 2009;22:1432-8.
Würl P, Meye A, Schmidt H, Lautenschläger C, Kalthoff H, Rath FW, Taubert H. High
prognostic significance of Mdm2/p53 co-overexpression in soft tissue sarcomas of the
extremities. Oncogene. 1998;16:1183-5.