the slow agonizing death of the long spine board in · pdf fileagainst the long spine board in...
TRANSCRIPT

Mounting Evidence Against the Long Spine Board in EMS Ryan C Jacobsen MD EMT-P Johnson County EMS System Medical Director Assistant Professor of Emergency Medicine Truman Medical CenterChildrenrsquos Mercy Hospitals and Clinics
Disclosure
bull This presentation was compiled from many gracious EMS Medical Directors throughout the US and I take little credit for any of ithellipIt is merely a synopsiscompilation of many others hard work for which I am very grateful
Specific thanks to
Charles (Chuck) Cady MD
Bryan Bledsoe MD
Keith Wesley MD
David Cone MD
Michael Millin MD
Steve Andrews MD
Kevin Sirmons MD
John Lyng MD
Objectives
bull Understand current state of spinal care in EMS and associated dogma
bull Understand the historical perspectives on prehospital spinal care and immobilization in the US
bull Review of the evidenceliterature surrounding prehospital spinal immobilization
bull Benefits of reducing the use of the long spine board as an immobilization device
bull Examples of various protocols being used throughout US as well as internationally
bull Barriers to the implementation of protocols reducing long spine board use
Divorce LSB from C-collars
bull Wersquore NOT talking about cervical spine clearance There would be NO change in current c-spine clearance protocol
bull Wersquore NOT talking about limiting cervical collar use in the field
bull This may actually increase the use of C-collars in the field
bull penetrating trauma
Scope
bull Approximately 1 million spinal injuries in EDrsquos every year
bull 2-3 have actual spine injury (of those only handful unstable)
Dogma regarding Spinal Immobilization bull Trauma=unstable spine injury=spinal cord injury=permanent
neurological deficit=bad
bull Any additional movement of the neckback may cause an injury that was not present immediately following the initial traumahellipor it may worsen an injury that was there prior to any subsequent medical intervention
bull Further injury is avoided by immobilizing the spine
bull Immobilization of the spine is safe
bull Medicolegal issues prevent us from changing
History
History
bull Geisler et al 1966
bull Retrospective study of trauma patients with delayed paralysis
bull ldquofailure to recognize the injury and protect the patient from the consequences of his unstable spinerdquo hellipregarding an MVC patient with skull fracture in 1955 who had delayed onset of paraplegia T4
bull ldquothe importance of proper first-aid (by EMS providers in field) was deduced from the fact that 29 patients [in their review] developed further paralysis through faulty handlingrdquo
Geisler WO Wynne-Jones M Jousse AT Early management of patients with trauma to the spinal cord Med Serv J of Can 19664512-23
The Dogma beginshellip
bull Now the medical community believes that trauma patients should be immobilized on rigid devices to minimize the risk of delayed paralysis in the setting of occult spinal column injury
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Disclosure
bull This presentation was compiled from many gracious EMS Medical Directors throughout the US and I take little credit for any of ithellipIt is merely a synopsiscompilation of many others hard work for which I am very grateful
Specific thanks to
Charles (Chuck) Cady MD
Bryan Bledsoe MD
Keith Wesley MD
David Cone MD
Michael Millin MD
Steve Andrews MD
Kevin Sirmons MD
John Lyng MD
Objectives
bull Understand current state of spinal care in EMS and associated dogma
bull Understand the historical perspectives on prehospital spinal care and immobilization in the US
bull Review of the evidenceliterature surrounding prehospital spinal immobilization
bull Benefits of reducing the use of the long spine board as an immobilization device
bull Examples of various protocols being used throughout US as well as internationally
bull Barriers to the implementation of protocols reducing long spine board use
Divorce LSB from C-collars
bull Wersquore NOT talking about cervical spine clearance There would be NO change in current c-spine clearance protocol
bull Wersquore NOT talking about limiting cervical collar use in the field
bull This may actually increase the use of C-collars in the field
bull penetrating trauma
Scope
bull Approximately 1 million spinal injuries in EDrsquos every year
bull 2-3 have actual spine injury (of those only handful unstable)
Dogma regarding Spinal Immobilization bull Trauma=unstable spine injury=spinal cord injury=permanent
neurological deficit=bad
bull Any additional movement of the neckback may cause an injury that was not present immediately following the initial traumahellipor it may worsen an injury that was there prior to any subsequent medical intervention
bull Further injury is avoided by immobilizing the spine
bull Immobilization of the spine is safe
bull Medicolegal issues prevent us from changing
History
History
bull Geisler et al 1966
bull Retrospective study of trauma patients with delayed paralysis
bull ldquofailure to recognize the injury and protect the patient from the consequences of his unstable spinerdquo hellipregarding an MVC patient with skull fracture in 1955 who had delayed onset of paraplegia T4
bull ldquothe importance of proper first-aid (by EMS providers in field) was deduced from the fact that 29 patients [in their review] developed further paralysis through faulty handlingrdquo
Geisler WO Wynne-Jones M Jousse AT Early management of patients with trauma to the spinal cord Med Serv J of Can 19664512-23
The Dogma beginshellip
bull Now the medical community believes that trauma patients should be immobilized on rigid devices to minimize the risk of delayed paralysis in the setting of occult spinal column injury
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Objectives
bull Understand current state of spinal care in EMS and associated dogma
bull Understand the historical perspectives on prehospital spinal care and immobilization in the US
bull Review of the evidenceliterature surrounding prehospital spinal immobilization
bull Benefits of reducing the use of the long spine board as an immobilization device
bull Examples of various protocols being used throughout US as well as internationally
bull Barriers to the implementation of protocols reducing long spine board use
Divorce LSB from C-collars
bull Wersquore NOT talking about cervical spine clearance There would be NO change in current c-spine clearance protocol
bull Wersquore NOT talking about limiting cervical collar use in the field
bull This may actually increase the use of C-collars in the field
bull penetrating trauma
Scope
bull Approximately 1 million spinal injuries in EDrsquos every year
bull 2-3 have actual spine injury (of those only handful unstable)
Dogma regarding Spinal Immobilization bull Trauma=unstable spine injury=spinal cord injury=permanent
neurological deficit=bad
bull Any additional movement of the neckback may cause an injury that was not present immediately following the initial traumahellipor it may worsen an injury that was there prior to any subsequent medical intervention
bull Further injury is avoided by immobilizing the spine
bull Immobilization of the spine is safe
bull Medicolegal issues prevent us from changing
History
History
bull Geisler et al 1966
bull Retrospective study of trauma patients with delayed paralysis
bull ldquofailure to recognize the injury and protect the patient from the consequences of his unstable spinerdquo hellipregarding an MVC patient with skull fracture in 1955 who had delayed onset of paraplegia T4
bull ldquothe importance of proper first-aid (by EMS providers in field) was deduced from the fact that 29 patients [in their review] developed further paralysis through faulty handlingrdquo
Geisler WO Wynne-Jones M Jousse AT Early management of patients with trauma to the spinal cord Med Serv J of Can 19664512-23
The Dogma beginshellip
bull Now the medical community believes that trauma patients should be immobilized on rigid devices to minimize the risk of delayed paralysis in the setting of occult spinal column injury
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Divorce LSB from C-collars
bull Wersquore NOT talking about cervical spine clearance There would be NO change in current c-spine clearance protocol
bull Wersquore NOT talking about limiting cervical collar use in the field
bull This may actually increase the use of C-collars in the field
bull penetrating trauma
Scope
bull Approximately 1 million spinal injuries in EDrsquos every year
bull 2-3 have actual spine injury (of those only handful unstable)
Dogma regarding Spinal Immobilization bull Trauma=unstable spine injury=spinal cord injury=permanent
neurological deficit=bad
bull Any additional movement of the neckback may cause an injury that was not present immediately following the initial traumahellipor it may worsen an injury that was there prior to any subsequent medical intervention
bull Further injury is avoided by immobilizing the spine
bull Immobilization of the spine is safe
bull Medicolegal issues prevent us from changing
History
History
bull Geisler et al 1966
bull Retrospective study of trauma patients with delayed paralysis
bull ldquofailure to recognize the injury and protect the patient from the consequences of his unstable spinerdquo hellipregarding an MVC patient with skull fracture in 1955 who had delayed onset of paraplegia T4
bull ldquothe importance of proper first-aid (by EMS providers in field) was deduced from the fact that 29 patients [in their review] developed further paralysis through faulty handlingrdquo
Geisler WO Wynne-Jones M Jousse AT Early management of patients with trauma to the spinal cord Med Serv J of Can 19664512-23
The Dogma beginshellip
bull Now the medical community believes that trauma patients should be immobilized on rigid devices to minimize the risk of delayed paralysis in the setting of occult spinal column injury
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Scope
bull Approximately 1 million spinal injuries in EDrsquos every year
bull 2-3 have actual spine injury (of those only handful unstable)
Dogma regarding Spinal Immobilization bull Trauma=unstable spine injury=spinal cord injury=permanent
neurological deficit=bad
bull Any additional movement of the neckback may cause an injury that was not present immediately following the initial traumahellipor it may worsen an injury that was there prior to any subsequent medical intervention
bull Further injury is avoided by immobilizing the spine
bull Immobilization of the spine is safe
bull Medicolegal issues prevent us from changing
History
History
bull Geisler et al 1966
bull Retrospective study of trauma patients with delayed paralysis
bull ldquofailure to recognize the injury and protect the patient from the consequences of his unstable spinerdquo hellipregarding an MVC patient with skull fracture in 1955 who had delayed onset of paraplegia T4
bull ldquothe importance of proper first-aid (by EMS providers in field) was deduced from the fact that 29 patients [in their review] developed further paralysis through faulty handlingrdquo
Geisler WO Wynne-Jones M Jousse AT Early management of patients with trauma to the spinal cord Med Serv J of Can 19664512-23
The Dogma beginshellip
bull Now the medical community believes that trauma patients should be immobilized on rigid devices to minimize the risk of delayed paralysis in the setting of occult spinal column injury
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Dogma regarding Spinal Immobilization bull Trauma=unstable spine injury=spinal cord injury=permanent
neurological deficit=bad
bull Any additional movement of the neckback may cause an injury that was not present immediately following the initial traumahellipor it may worsen an injury that was there prior to any subsequent medical intervention
bull Further injury is avoided by immobilizing the spine
bull Immobilization of the spine is safe
bull Medicolegal issues prevent us from changing
History
History
bull Geisler et al 1966
bull Retrospective study of trauma patients with delayed paralysis
bull ldquofailure to recognize the injury and protect the patient from the consequences of his unstable spinerdquo hellipregarding an MVC patient with skull fracture in 1955 who had delayed onset of paraplegia T4
bull ldquothe importance of proper first-aid (by EMS providers in field) was deduced from the fact that 29 patients [in their review] developed further paralysis through faulty handlingrdquo
Geisler WO Wynne-Jones M Jousse AT Early management of patients with trauma to the spinal cord Med Serv J of Can 19664512-23
The Dogma beginshellip
bull Now the medical community believes that trauma patients should be immobilized on rigid devices to minimize the risk of delayed paralysis in the setting of occult spinal column injury
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

History
History
bull Geisler et al 1966
bull Retrospective study of trauma patients with delayed paralysis
bull ldquofailure to recognize the injury and protect the patient from the consequences of his unstable spinerdquo hellipregarding an MVC patient with skull fracture in 1955 who had delayed onset of paraplegia T4
bull ldquothe importance of proper first-aid (by EMS providers in field) was deduced from the fact that 29 patients [in their review] developed further paralysis through faulty handlingrdquo
Geisler WO Wynne-Jones M Jousse AT Early management of patients with trauma to the spinal cord Med Serv J of Can 19664512-23
The Dogma beginshellip
bull Now the medical community believes that trauma patients should be immobilized on rigid devices to minimize the risk of delayed paralysis in the setting of occult spinal column injury
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
History
bull Geisler et al 1966
bull Retrospective study of trauma patients with delayed paralysis
bull ldquofailure to recognize the injury and protect the patient from the consequences of his unstable spinerdquo hellipregarding an MVC patient with skull fracture in 1955 who had delayed onset of paraplegia T4
bull ldquothe importance of proper first-aid (by EMS providers in field) was deduced from the fact that 29 patients [in their review] developed further paralysis through faulty handlingrdquo
Geisler WO Wynne-Jones M Jousse AT Early management of patients with trauma to the spinal cord Med Serv J of Can 19664512-23
The Dogma beginshellip
bull Now the medical community believes that trauma patients should be immobilized on rigid devices to minimize the risk of delayed paralysis in the setting of occult spinal column injury
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

The Dogma beginshellip
bull Now the medical community believes that trauma patients should be immobilized on rigid devices to minimize the risk of delayed paralysis in the setting of occult spinal column injury
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
History Continued
bull Farrington1968 bull Described the placement of a C-collar and a long or short backboard as
necessary to keep the head and neck from sagging during extrication bull The backboard was designed to assist in minimizing spinal movement
during complex extrication maneuvers by freeing the hands of rescuers from actively holding spinal precautions
bull The backboard was not initially envisioned to be a long-term device to actually immobilize someone onto after they were extricated
Farrington DJ Extrication of Victims Journal of Trauma 19688(493-512)
The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

The beginning of formal EMS
bull 1971 bull American Academy of
Orthopedic Surgeons (AAOS)published first guidelines for EMS Emergency Care and Transportation of the Sick and Injured
bull Advocated use of spinal immobilization using a backboard and C-collar for trauma patients with signs and symptoms of spinal injury
History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

History Continued bull Bohlman 1979
bull Linked delayed paraplegia in 100 of 300 hospitalized cervical spine fracture patients with concern that these injuries were being ldquounder-appreciatedrdquo
bull Blamed EMS=inevitable knee jerk response
bull Began applying spinal immobilization using backboards and C-collars based on mechanism of injury alone
bull Bohlman HH Acute fractures and dislocations of the cervical spine J Bone amp Joint Surg 197961A1119-42
bull Riggins RS Kraus JF The risk of neurologic damage with fractures of the vertebrae J Trauma 197717126-133
bull Soderstrom CA Brumback RJ Early care of the patient with cervical spine injury Orthopedic Clinics of North America 1986173-13
bull Burney RE Waggoner R Maynard FM Stabilization of spinal injury for early transfer J Trauma 1989291497-1499
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Evidence
NO randomized controlled studies ever done
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Evidence that Long Spine Boards cause HARM bull Respiratory compromise (reduces FVC FEV1 in healthy
patients strapped to a board)
bull Effect on injured patients Ptx pulm contusions rib fx etc
bull Bauer D Kowalski R Effect of spinal immobilization devices on pulmonary function in the healthy nonsmoking man Ann Emerg Med 198817915-8
bull Walsh M Grant T Mickey S Lung function compromised by spinal immobilization Correspondence Ann Emerg Med 199019615-6
Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Evidence for HARM
bull Pressure sorestissue hypoxia bull Good evidence that even short time periods on
board cause tissue hypoxia on contact points as well as pressure woundshelliphellipbecomes worse with elderly and severely injured folks who canrsquot readjust on board (aka spinal cord injured patient)
bull Linares HA Mawson AR Suarez E Biundo JJ Association between pressure sores and immobilization in the immediate post-injury
period Orthopedics 198710571-3 bull Sheerin F de Frein R The occipital and sacral pressures experienced by healthy volunteers under spinal immobilization a trial of
three surfaces J Emerg Nurs 200733447-50 bull Cordell WH Hollingsworth JC Olinger ML Stroman SJ Nelson DR Pain and tissue-interface pressures during spine-board
immobilization Ann Emerg Med 19952631-36 bull Berg G Nyberg S Harrison P Baumchen J Gurss E Hennes E Near-infrared spectroscopy measurement of sacral tissue oxygen
saturation in healthy volunteers immobilized on rigid spine boards Prehosp Emerg Care 201014419-24
Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Evidence for HARM
bull Increased pain
Healthy subjects placed on boards developed numerous complaints when on boards for short times (headaches back neck pain dizziness nausea)
bull Barney RN Cordell WH Miller E Pain associated with immobilization on rigid spine boards Ann Emerg Med 198918918
bull Lerner EB Billittier AJ Moscati RM The effects of neutral positioning with and without padding on spinal immobilization of healthy subjects Prehosp Emerg Care 19982112-6
bull Chan D Goldberg R Tascone A Harmon S Chan L The effect of spinal immobilization on healthy volunteers Ann Emerg Med 19942348-51
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Evidence for HARM
bull Increase in unnecessary radiologic imaging in ED (this is both a cost and radiation risk issue)
bull March J Ausband S Brown L Changes in physical examination caused by use of spinal immobilization Prehosp Emerg Care
20026421-4
bull Berrington de Gonzaacutelez A Mahesh M Kim K Bhargavan M Lewis R Mettler F Land C Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007 Arch Intern Med 20091692071-77
bull Hall E Brenner D Cancer risks from diagnostic radiology Br J Radiol 2008 May81362-78
bull Forley F Pham J Kirsch T Use of advanced radiology during visits to US emergency departments for injury-related conditions 1998-2007 JAMA 20103041465-71
Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Evidence for Harm
bull Hauswald et al 1998
bull Compared neurologic outcomes of spinal injury patients in New Mexico where every EMS patient received full spinal immobilization to those of spinal injury patients in Malaysia where none of the EMS patients received spinal immobilization
bull Hauswald M Ong G Tandberg D Omar Z Out-of-hospital spinal immobilization its effect on neurologic injury
Acad Emerg Med 19985214-19
Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Malaysia vs New Mexico
Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Malaysia versus New Mexico
RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

RESULTS
bull The Odds Ratio for disability was higher for patients in the United States (all with spinal immobilization) after adjustment for the effect of all other independent variables (203 95 CI 103-399 p = 004)
bull The estimated probability of finding data as extreme as this if immobilization has an overall beneficial effect is only 2 Thus there is a 98 probability that immobilization is harmful or of no value
bull They repeated analysis using only the subset of patients with isolated cervical level deficits They again failed to show a protective effect of spinal immobilization (OR 152 95 CI 064-362 p = 034)
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
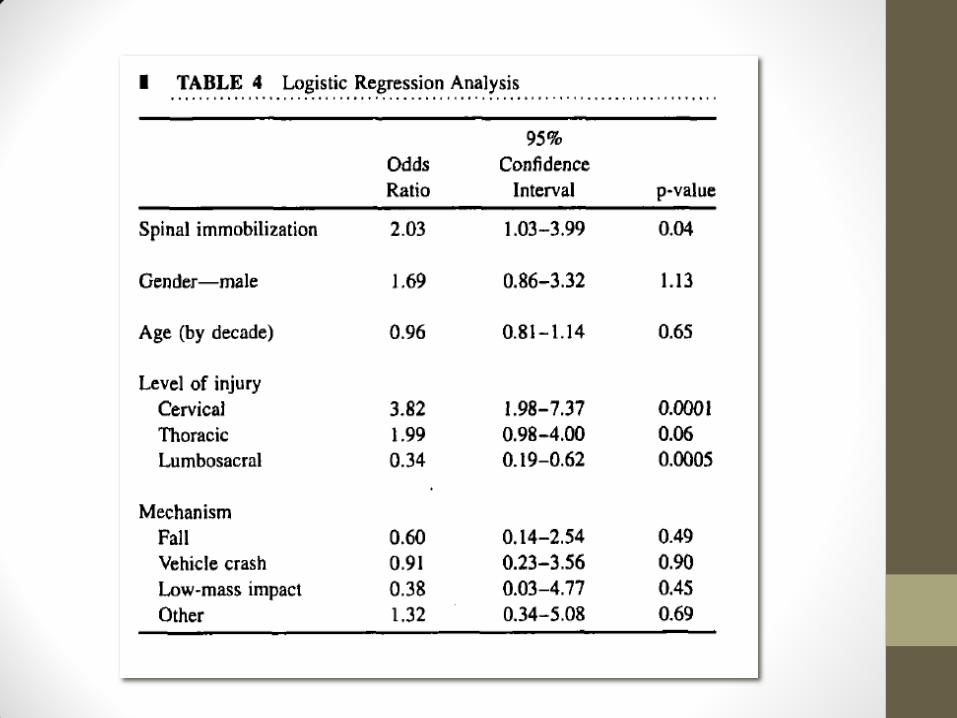
Evidence for Harm
bull Leonard et al 2012
bull Pediatric trauma patients (prospective cohort)
bull spinal immobilization was associated with increased pain and radiographic usage and increased admission to the hospital
pain score (3 versus 2)
cervical radiography (566 versus 134)
Admitted (416 versus 143)
Leonard J Mao J Jaffe D Potential adverse effects of spinal immobilization in children Prehosp Emerg Care 201216513-518
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Penetrating trauma and Spine Immobilization bull We should NOT be immobilizing penetrating trauma
bull Increases mortality and clear support from all parties involved (AANS ACS-COT NAEMSP NAEMT ATLSPHTLS etc)
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Evidence for Harm in Penetrating Trauma bull Cornwell EE et al 2001
bull BACKGROUND bull Previous studies have suggested that patients transported by emergency medical services (EMS) following major trauma had a longer
injury-to-treatment interval and a higher mortality rate than their non-EMS-transported counterparts bull HYPOTHESIS bull There is little actual benefit of thoracolumbar immobilization for patients with torso gunshot wounds (GSW) bull DESIGN bull Retrospective analysis of prospectively gathered data from the Maryland Institute for Emergency Medical Service Systems State Trauma
Registry from July 1 1995 through June 30 1998 bull SETTINGS bull All designated trauma centers in Maryland bull PATIENTS bull All patients with torso GSW bull MAIN OUTCOME MEASURES bull (1) A patient was considered to have benefited from immobilization if he or she had less than complete neurologic deficits in the
presence of an unstable vertebral column as shown by the need for operative stabilization of the vertebral column (2) mortality bull RESULTS bull There were 1000 patients with torso GSW Among them 141 patients (141) had vertebral column andor spinal cord injuries Two
patients (02) (95 confidence interval -0077 to 048) required operative vertebral column stabilization while 6 others required other spinal operations for decompression andor foreign body removal The presence of vertebral column injury was actually associated with lower mortality (71 vs 148 Plt02)
bull CONCLUSIONS bull This study suggests that thoracolumbar immobilization is almost never beneficial in patients with torso GSW and that a higher
mortality rate existed among those GSW patients without vertebral column injury vs those with such injuries The role of formal thoracolumbar immobilization for patients with torso GSW should be reexamined
Arch Surg 2001 Mar136(3)324-7 Thoracolumbar immobilization for trauma patients with torso gunshot wounds is it necessary Cornwell EE 3rd
Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Evidence for Harm in Penetrating Trauma bull Haut ER 2010
bull BACKGROUND bull Previous studies have suggested that prehospital spine immobilization provides minimal benefit to penetrating
trauma patients but takes valuable time potentially delaying definitive trauma care We hypothesized that penetrating trauma patients who are spine immobilized before transport have higher mortality than nonimmobilized patients
bull METHODS bull We performed a retrospective analysis of penetrating trauma patients in the National Trauma Data Bank (version
62) Multiple logistic regression was used with mortality as the primary outcome measure We compared patients with versus without prehospital spine immobilization using patient demographics mechanism (stab vs gunshot) physiologic and anatomic injury severity and other prehospital procedures as covariates Subset analysis was performed based on Injury Severity Score category mechanism and blood pressure We calculated a number needed to treat and number needed to harm for spine immobilization
bull RESULTS bull In total 45284 penetrating trauma patients were studied 43 of whom underwent spine immobilization Overall
mortality was 81 Unadjusted mortality was twice as high in spine-immobilized patients (147 vs 72 p lt 0001) The odds ratio of death for spine-immobilized patients was 206 (95 CI 135-313) compared with nonimmobilized patients Subset analysis showed consistent trends in all populations Only 30 (001) patients had incomplete spinal cord injury and underwent operative spine fixation The number needed to treat with spine immobilization to potentially benefit one patient was 1032 The number needed to harm with spine immobilization to potentially contribute to one death was 66
bull CONCLUSIONS bull Prehospital spine immobilization is associated with higher mortality in penetrating trauma and should not be
routinely used in every patient with penetrating trauma
Haut ER Kalish BT Efron DT et al Spine immobilization in penetrating trauma more harm than good J Trauma 201068115-20 discussion 120-1
Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Evidence for Harm in Penetrating Trauma bull Rhee P et al 2006
bull 57523 trauma patients
bull Evaluated by
bull Blunt assault
bull Stab wounds
bull Gunshot wounds
Rhee P et al Cervical spine injury is highly dependent on the mechanism of injury following blunt and penetrating
assault J Trauma 2006611166-1170
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Evidence for Harm in Penetrating Trauma bull Rates for C-spine Fx
bull GSW (135)
bull Blunt Assault (041)
bull Stab Wound (012)
bull Rates of Spine Cord Inj
bull GSW (094)
bull Blunt Assault (014)
bull Stab Wound(011) bull Rhee P et al Cervical spine injury is
highly dependent on the mechanism of injury following blunt and penetrating assault J Trauma 2006611166-1170
bull Surgical stabilization
bull GSW (26158 [155])
bull Blunt Aslt(619 [316])
bull Stab Wnd (311 [278])
bull No patient with penetrating SCI regained significant neurologic recovery
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Authorrsquos Conclusions
bull Donrsquot get shot in the spinal cordhelliphellip
bull Neurologic deficits from penetrating assault were established and final at the time of presentation
bull Concern for protecting the neck should not hinder the evaluation process or life saving procedures
bull Donrsquot waste time on scene ldquopackagingrdquohellipjust go
Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Evidence for Harm in Penetrating Trauma
Vanderlan WB et al 2009
bull NOLA retrospective chart review bull 847 charts bull 188 studied patients
bull 35 (229) died bull 27 immobilized bull 8 not immobilized bull GSW (94) bull Stab wound (6)
bull Vanderlan WB Tew BE McSwain NE
Increased risk of death with cervical spine immobilization in penetrating cervical trauma Injury 200940880-883
bull C-spine immobilization in this study was associated with an increased risk of death (p = 0016 odds ratio 277 95 CI 118- 649)
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Evidence for Harm in Penetrating Trauma
Kaups KL et al 1998
bull Fresno study
bull 215 patients with GSW to head bull DOA and c-spine injuries
excluded
bull Cervical spine clearance was determined in 202 (93)
Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine immobilization and evaluation J Trauma 199844865-867
bull No patients had indirect c-spine injury
bull 3 patients had direct c-spine injury that was readily apparent
Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Authorrsquos Conclusions
bull More intubation attempts occurred in patients with cervical collars
bull 49 attempts in 34 patients with c-collars
bull 5 attempts in 4 patients without c-collars (p=0008)
bull Indirect spinal injury does not occur with GSWs to head
bull Kaups KL Davis JW Patients with gunshot wounds to the head do not require cervical spine
immobilization and evaluation J Trauma 199844865-867
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
GSWs rarely cause spine injuries bull DuBose et al 2009
bull 4204 patients with GSWrsquos to the head neck or
bull torso
bull 327 (78) had spinal column injuries
bull 173327 had spinal cord injuries
bull 2 (06) patients required surgery
bull None had unstable spinal injuries
DuBose et al The role of routine spinal imaging and immobilization in asymptomatic patients after gunshot wounds Injury 200940860-863
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
American Academy of Neurological Surgeons (AANS) Position bull Theodore N et al 2013 Neurosurgery
bull ldquoSpinal immobilization in patients with penetrating trauma is not recommended because of increased mortality from delayed resuscitationrdquo
PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

PHTLS Position
bull There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso
bull There are no data to support routine spinal mobilization in patients with isolated penetrating trauma to the cranium
bull Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma
bull Stuke LE Pons PT Guy JS Chapleau WP Butler FK McSwain NE Prehospital
spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee J Trauma 201171763-9 discussion 769-70
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Cochrane Review
bull ldquoUnwarranted spinal immobilization can expose patients to the risks of iatrogenic pain skin ulceration aspiration and respiratory compromise which in turn can lead to multiple radiographs resulting in unnecessary radiation exposure longer hospital stay and increased costs The potential risks of aspiration and respiratory compromise are of concern because death from asphyxiation is one of the major causes of preventable death in trauma patientsrdquo
bull Kwan I Bunn F Roberts I Spinal immobilization for trauma patients Cochrane Database of Systematic Reviews 200911-15
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
US Consortium of Metropolitan Medical Directors Position Statement aka The Eagles ldquoCurrent best practices reflect that there are no randomized controlled trials to evaluate the benefits of spinal immobilization in out-of-hospital trauma patients As a result current EMS protocols are based principally on historical precedent dogma and medico-legal concerns and not on scientific evidence This situation is further complicated by the reality that such studies will not likely be performed in the future primarily as a result of perceived legal and ethical concerns There is however a growing body of literature that points to the potential deleterious effects of spinal immobilization whether or not this modality is applied in an appropriate fashionrdquo
The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

The Eagles
bull Taking it one step furtherhellip(they apparently donrsquot like c-collars that much either)
bull ldquoWe might therefore consider discontinuing the use of the cervical collar in alert cooperative trauma patients even with a suspected C-spine fracture unless consciousness deteriorates or if the application of a collar might provide the patient with a degree more comfort It is certainly also time for EMS systems to remove collars from their protocols for the management of patients with penetrating traumardquo
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Evidence for Benefit
bull
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
We have assumption that LSBrsquos actually immobilize the spinehellip
3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

3 points of contact for LSB
bull Occiput
bull T-spine
bull Sacrum
We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

We painted a studenthellip
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Then carefully laid them on a LSB
Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Then lifted the student offhellip
occiput
T-spine
sacrum
HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

HOW WELL DO BOARDS IMMOBILIZE
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
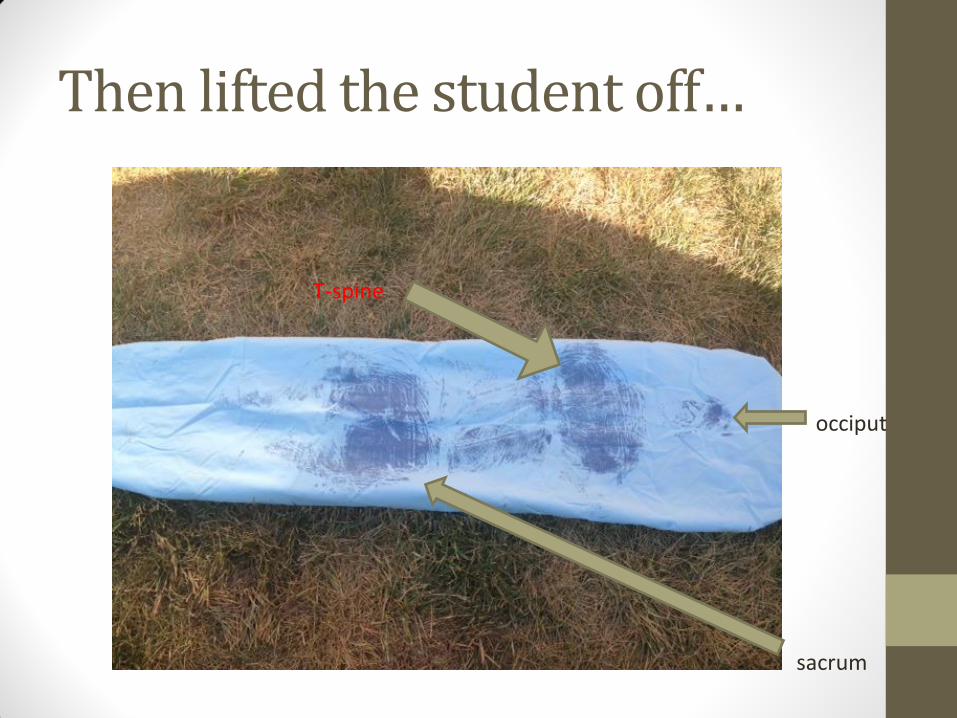
Spine boards as immobilization devices bull Mazolewski et al 1994
bull Study of different strapping techniques demonstrated that healthy cooperative volunteers are still able to move when strapped to a backboard
bull Mazolewski P Manix T The effectiveness of strapping techniques in spinal immobilization Ann Emerg Med 1994231290-5
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
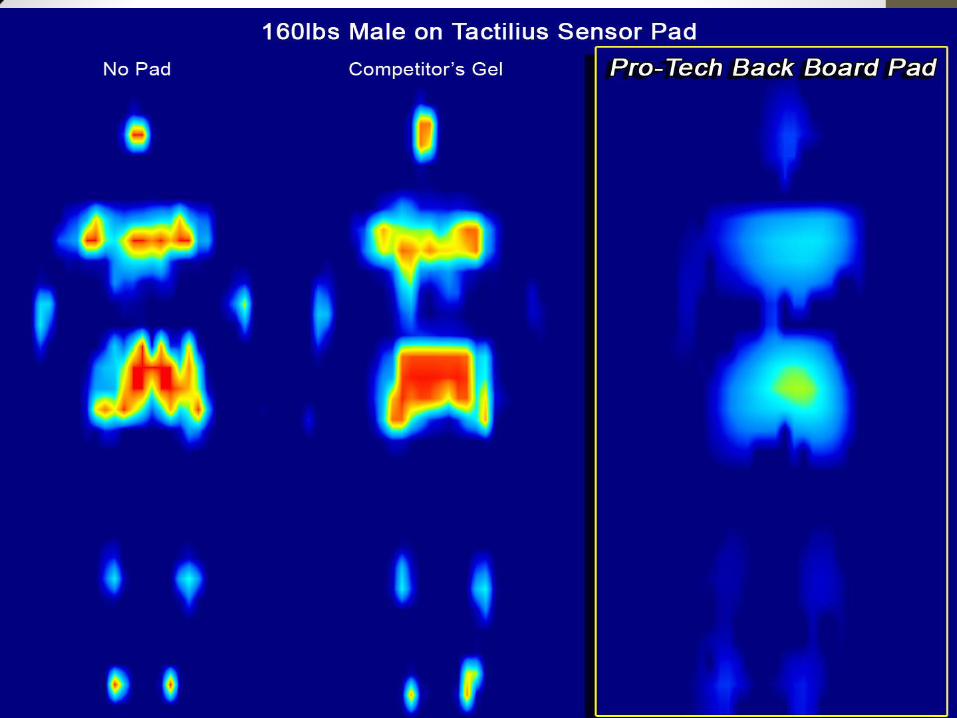
Spine boards as immobilization device bull Silbergleit R et al 1991
bull During transport once on a backboard patients still subject to significant head to toe and side to side forces
bull (remember boards are slippery and we fix their head to them and allow body to move)
bull Silbergleit R Dedrick DK Pape J Burney RE Forces acting during air and ground transport on patients stabilized by standard
immobilization techniques Ann Emerg Med 199120875-877
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Spine boards as immobilization devices bull Peery et al 2007
bull A prospective observational study showed 70 of study patients had at least one backboard strap with 4 or more cm of slack and 12 of study patients had 4 or more backboard straps with 4 or more cm of slack
bull Peery CA Brice J White WD Prehospital spinal immobilization and the backboard quality assessment study
Prehosp Emerg Care 200711293-7
Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Combative Patients
bull We pin them down onto a board while they squirm and are held down at head Likely increasing energyforces transmitted to spine
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Uncooperative Patient
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Combative patients
bull We claim that we are forcefully pinning their head down and forcing them supine on a hard board in order toe ldquoprotect their spinerdquo from themselves as they violently squirm under the straps
bull This technique likely increases forcesenergy transmitted to the spine
bull Allowing them to have collar on and get into position of comfort likely less energy to spine
Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Forced Immobilizationhellipworse than no immobilization bull Hauswald M 2012
bull Tightening the straps may restrict movement but not the forces generated by the patient on the spine in resistance to restraining efforts Attempting to enforce immobilization of
the uncooperative patient may result in more force transmission to the spine than
before the struggle commenced
bull Hauswald M A re-conceptualisation of acute spinal care Emerg Med J 2012001ndash4
Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Spine board as immobilization device bull The clinical significance of strap tightness and patient
movement while ldquoimmobilizedrdquo has not been established but such movement cannot qualify as immobilization the very purpose for which backboards continue to be used during transport
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Spine Boards as Immobilization Devices bull If patients are still able to move despite being strapped to a
backboard spinal immobilization is more a function of their cooperation than the due to the ability of the backboard and straps to assure spinal immobilization
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Limitations of Studies on Long Spine Boards bull Studies on the effectiveness of backboards as an
immobilization device have only included cooperative patients healthy volunteers and cadaver models no study has been done evaluating patient resistance and its effect on the spine
What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

What about Scoop Stretchers
bull Del Rossi et al 2010
bull Scoop Stretchers and the ldquolift and sliderdquo technique were able to restrict motion of the spine as well as the log-roll technique with long board
bull Del Rossi et al Are Scoop Stretchers Suitable for
use on spine-injured patients American Journal of Emergency Medicine 2010
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
What Extrication Technique Causes Least Spine Movement bull Shafer et al 2009 West J Emerg Med 2009 May 10(2) 74ndash78
bull Cervical Spine Motion During Extrication A Pilot Study
bull They used motion capture video to look at motion of spine during different techniques of extrication from car
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Extrication techniques and Spine Motion
4 Different Techniques were compared
1 The patient was allowed to exit the vehicle on their own and lie on a backboard
2 The patient was allowed to exit the vehicle on their own with a C-Collar in place and lie on a backboard
3 The patient was extricated head first via standard technique by two paramedics with a C-Collar alone (Standard technique involves turning the driver so that the legs are in the passengerrsquos seat allowing the driver to lie back and raising the right hip so a long board can be placed under the hip A second paramedic who enters the front seat passengerrsquos door helps slide the patient up on to the board)
4 The patient was extricated head first via standard technique by the two paramedics with a C-Collar and a KED
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Author Conclusions
bull ldquoUltimately we documented the least movement of the cervical spine in subjects who had a cervical collar applied and were allowed to simply get out of the car and lie down on a stretcherrdquo
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Extrication techniques on Spine Movement
Emerg Med J 2013 Jun 28 Dixon M OHalloran J Cummins NM METHODS A crew of two paramedics and four fire-fighter first responders extricated a
simulated patient from a prepared motor vehicle using nine different extrication techniques The patient was marked with biomechanical sensors and relative movement between the sensors was captured via high speed infrared motion analysis cameras A 3D mathematical model was developed from the recorded movement
RESULTS Control measurements were taken from the patient during self-extrication and
movement was recorded of 4194deg left of midline (LOM) to 2408deg right of midline (ROM) resulting in a total movement of 6602deg The least deviation recorded during equipment aided extrication was movement of 3365deg LOM and 8352deg ROM resulting in a total movement of 11717deg The most deviation recorded during equipment aided extrication was movement of 1588deg LOM and 24498deg ROM resulting in a total movement of 26086deg
CONCLUSIONS Conventional extrication techniques record up to four times more cervical
spine movement during extrication than controlled self-extrication This proof of concept study demonstrates the need for further evaluation of current rescue techniques and the requirement to investigate the clinical and operational significance of such movement
Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Ambulance Cots are essentially Padded Long Spine Boards bull Once the patient is secured to the ambulance cot the
backboard becomes redundant as the standard transport cot provides a flat surface to which the patient can be secured
bull Like the hospital bed the ambulance cot and straps can provide spinal protection reducing spinal flexion rotation and lateral motion
bull In addition the cot mattress can conform to the anatomic shape of the spine and the non-slick surface minimizes patient movement on the cot
bull Transport on a mattress is largely without the downside risks of the backboard
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
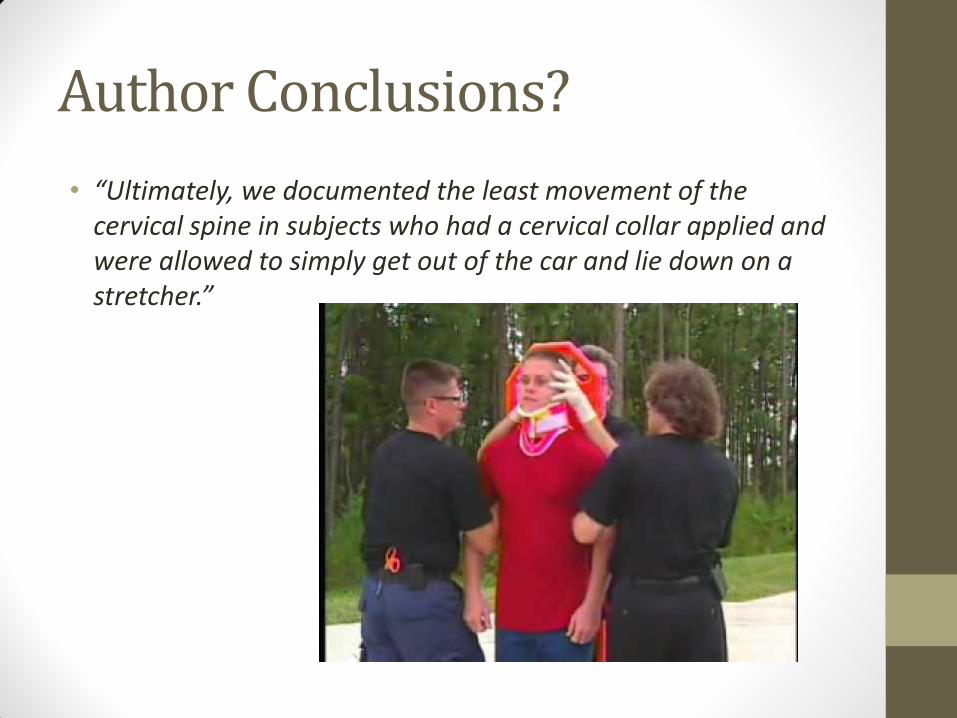
Our EMS Cot
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
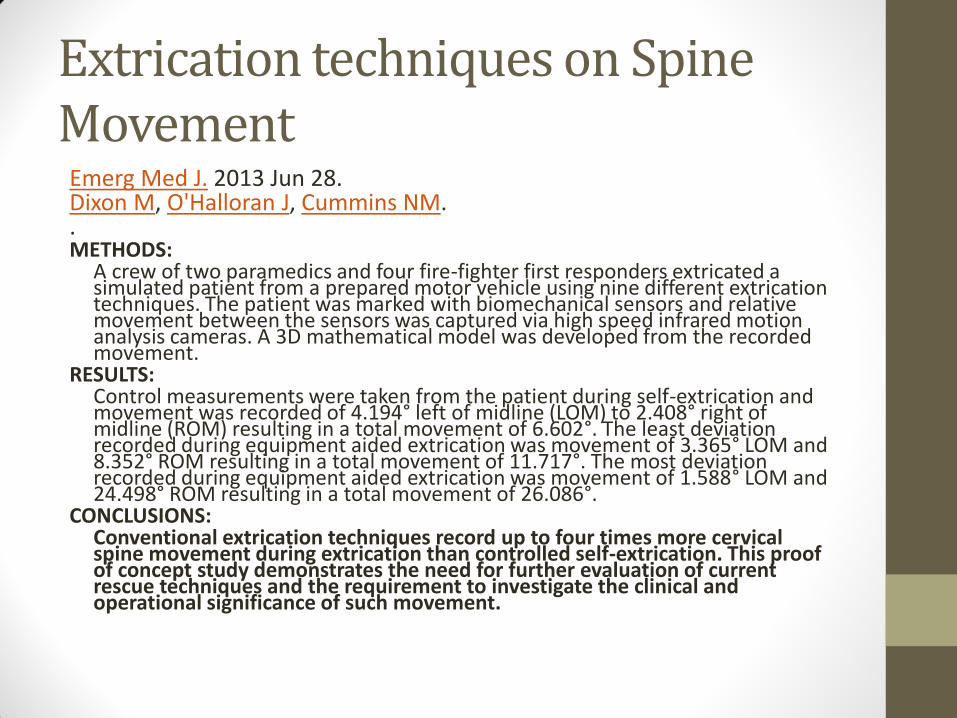
We re-painted our studenthellipand laid him on our cot mattress
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Comparison of points of contact showed likely increased points of contact and more comfortable than LSB
Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Using Logic as an argument to reduce LSB use in the field
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Wersquove all met these elderlykyphotic patients
bull Riskgtgtgtgtbenefit
Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Faulty Assumptions
The time that the patient hits the ED door
DOES NOT mean that their evaluation andor care
begins at that point in time
Patients who arrive immobilized may stay that
way for significant periods of time until they are
seen and removed from the board by someone
authorized to do so
Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Should I go to the hospital
bull Wersquove always instinctively known that these patients donrsquot need a Long Spine Board
bull Minor falls
bull Ambulatory patients
bull Minor MVCrsquos
bull What does the ED do with walk-ins
New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

New Thoughts
bull Hauswald A Re-conceptualisation of Acute Spinal Care
bull Injury caused by ENERGY (MVC Fall GSW) not motion
bull Energy at time of injury great
bull Energy during EMS careextrication is minimal
bull Motion at uninjured segments different than injured segments and force may not equate to visible motion
bull Longboard low friction surface energy to anchor points (headneck)hellipisnrsquot that worse
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Questioning long held beliefs that movement by field providers causes harm bull Hauswald 2012 bull The spine requires little energy to move within its normal ROM and offers little
resistance to motion within this range bull Since the spinal components fail at similar force spinal injuries are either minor with
no threat to the spinal cord or are catastrophic with multiple irreversible failures that may irreparably damage the spinal cord so severely that they will be unaffected by prehospital emergency spinal care
bull If the force experienced to create the unstable fracture was not enough to injure the cord at that time then forces experienced during patient movement by EMS are unlikely to injure the cord
bull If the force results in injury but not gross instability additional forces applied by prudent rescuers during extrication and transport will be spread throughout the spine (as long as not outside normal ROM)
bull Most spinal injuries are ldquostablerdquo in the short term and those that are truly ldquounstablerdquo
and offer no resistance to motion are irrevocably damaged at the time of the event
Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Questioning Long Held Beliefs
bull Spinal column itself is very strong requiring up to 2000-6000 Newtons to fracture the cervical spine (approx 500-1500 pounds of force)
bull A 4kg head hanging off of the bed only generates about 40N of force
bull Spinal motion during extrication by careful rescuers creates forces at most on the
order of magnitude created by gravity and are spread throughout the spinal column unless the column itself ndash cord included ndash had lost all structural integrity at that level Thus motions induced by rescuers do not achieve the forces needed to threaten spinal column integrity
bull High friction comfortably firm surface (aka the cot or bed) is the ideal surface bull Traditional low friction hardslipper surfaces that are uncomfortable (ie can cause
tissue hypoxia) are bad
bull Maiman D Sances A Myklebust J Larson S Houterman C Chilbert M El-Ghatit A Compression injuries of the cervical spine a biomechanical analysis Neurosurgery 198313254ndash60
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Evidence for Benefit of Long Spine Board bull
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Potential Benefits to NOT using LSB bull Reduce amount of on-scene personnel
bull Reduce amount of patients lifted from ground on LSB who are already ambulatory
bull Reduce amount of awkward positions providers place themselves in to extricate otherwise well patients from vehicles
bull Reduce scene times by eliminating time spent immobilizing to board (cot straps are quickLSB strapping is NOT quick)
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Increases Ability for Providers to Expose Patients While Enroute to Hospital
Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Virtually Impossible to Gain Access to patient when strapped to Long Spine Board
bull If you do unstrap enroute yoursquoll only have head secured as fixed point (thatrsquos bad)
Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Benefits to reducing LSB use
bull Decreased awkward extrication of stable patients who could self-extricate
bull Less resourcesmanpower needed (two folks and a cot for most minor MVCrsquos with neck pain)
bull Less scene time when using cot straps and not securing head
bull More exposureaccess to patient enroute
bull More comfort for patient
bull Saves patient from ED doc who leaves on board in hospital
bull Decrease radiological studies
bull Decreases cost
bull Decrease in resistance to placing a c-collar in elderly or borderline patient when not mandated to use LSB
Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Wersquore not alone in our efforts to minimize LSB use
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
AgenciesEMS Systems Minimizing LSB use
North Memorial Ambulance amp Aircare
Minneapolis MN
HealthEast Medical Transportation
St Paul MN
Xenia Fire Department
Xenia OH
Rio Rancho Fire Department
New Mexico
Albuquerque-Bernalillo County Medical Control Board
New Mexico
Bernalillo County Fire Department
New Mexico
SERTAC (Southeast Regional Trauma Advisory Council in WI)
State of Connecticut (Department of Health)
State of Maryland
CentraCare Health
Monticello MN
Kenosha Fire Department
Kenosha WI
MedicWest Ambulance
Nevada
Norwalk Hospital
Connecticut
Eagle County Ambulance District
Colorado
Milwaukee EMS
WI
bull Outside of US
bull Queensland Ambulance Service Trauma clinical practice procedures Use of an extrication board 2012 httpwwwambulanceqldgovaumedicalpdf09_cpp_trauma_030912pdf
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Example Protocol Wording in Wisconsin bull SERTAC (Southeast Regional Trauma Advisory Committee)
bull Spinal immobilization consists of keeping the head neck and spine inline The neck can be immobilized with a well fitted cervical collar head blocks blanket rolls or other immobilization techniques Patients who are already walking or standing should be laid directly on the ambulance stretcher and secured to the stretcher with seatbelts Back boards and scoop stretchers are designed and should only be used to extricate patients
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries should only be immobilized if a focal neurologic deficit is noted on physical examination (although there is little evidence of benefit even in these cases)
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
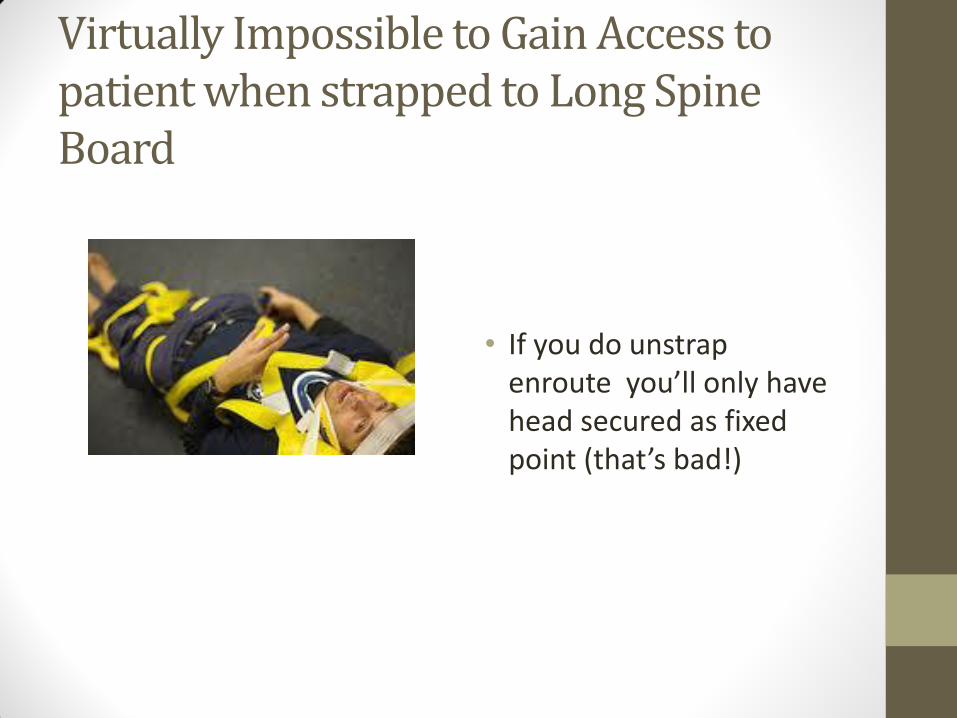
Example Protocol Wording
bull YaleNew Haven Sponsor Hospital EMS System
bull ldquoEffective immediately long backboards will no longer be utilized for spinal immobilization of ambulatory patients Patient who are ambulatory at the scene but who require cervical immobilization based on our selective spinal immobilization protocol will be placed in the position of comfort limiting movement of the neck during the process This change in procedure is the first step toward eventually using long boards only when needed to facilitate extrication and not during transportrdquo
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Queensland Ambulance
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Queensland Ambulance
Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Protocol Wording
bull If Spinal Immobilization is indicated an appropriately sized cervical collar should be placed
bull Patients who are already ambulatory or standing should NOT be placed on a long spine board but rather be laid directly on the ambulance cot and secured to the cot with seatbelts in a position of comfort
bull Back boards and scoop stretchers are designed for extrication and patient movement and should not be used for spinal immobilization
bull There is no role for the KED board in EMS
bull Once extricated patients should be taken off the back board or scoop stretcher and be placed directly on the ambulance stretcher
bull Patients with penetrating traumatic injuries (including head neck and
torso) should only be immobilized if a focal neurologic deficit is noted on physical examination
bull Decisional patientrsquos have the right to refuse any aspect of spinal immobilization
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Queensland
bull Notice they do NOT allow transport on a LSB
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Parting Thoughts
bull Despite the long-standing history and culture of spinal immobilization with a backboard and cervical collar using the best evidence available many abroad and in the US believe the risk-benefit analysis shows that the proven harm is much worse than the theoretical but unproven benefit of the backboard
People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

People donrsquot like to changehellip
Note the conclusion in this article
If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

If Spine Boards were a Medication bull If a medication had the same riskbenefit as the LSB use of
the drug would be stopped immediately by the FDA
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
Barriers to Implementation
bull Overcoming DogmaInstitutional CultureLong Standing Traditions bull Buy-In from HospitalHelicopter AgenciesCritical Care Transport
Agencies bull Physicians bull Nursing bull Flight Crews
bull Buy-in from EMS Providers bull Risk ManagementLiability Issues bull Ensuring proper documentationQA bull EMS Provider educational roll-out bull Equipment Issues (differences between agencies budgetary issues) bull Logistics (actual procedures to be performed in field ensuring they are
quicksafeeffective) bull Appropriate wording of Protocol to ensure common
understandingintent by field providers bull Overcoming differences with StateNational Curriculums and Standards
Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Johnson County EMS Proposed Language (see bolded print) bull Spinal Immobilization bull Indications bull Blunt trauma patients that meet Step 1 2 or 3 (See appendix B) or experience axial load fall of gt3 feet rollover
ATV cycle or pedestrianvehicle accidents will be immobilized bull Patients with penetrating traumatic injuries should NOT be immobilized unless a focal neurologic deficit is
noted on physical examination bull Spinal immobilization is indicated in trauma patients who sustain a mechanism of injury sufficient to cause a neck
or back injury and who display at least one of the following criteria Use caution for occult fracture in age gt65 or lt4 years old or history of osteoporosis bone or vertebral disease bull Unreliable physical exam such as GCS lt 15 inability to fully cooperate evidence of intoxication or acute stress reaction bull Pain deformity or tenderness to the neck or back bull A distracting painful injury bull Neurologic deficit bull Pain produced on unassisted rotation of the head 45 degrees in each direction
bull Techniques bull Stabilize head and neck in neutral position unless movement causes pain deformity or resistance If so
immobilize the head and neck in the position found bull If the patient is ambulatory place an appropriately sized cervical collar and position the patient directly on the
ambulance cot in the position of comfort limiting movement of the spine during the process bull Patients that are stable alert and without neurological deficits may be allowed to self-extricate to the
ambulance cot after placement of a cervical collar Limit movement of the spine during the process bull If a Long Spine Board or Scoop Stretcher are used for extrication or patient movement the patient should be
taken off the long spine board or scoop stretcher and placed directly on the ambulance cot using an appropriate technique that minimizes movement of the spine
Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Issues to deal withhellip
bull What to do with multiple boarded patients when wersquod typically put one on the bench seat in full package
bull Vomiting patient that is not on board
bull Gravid patient not on board (how to roll them off their IVC)
bull Football players with helmets on
bull Swimming pools already packaged by lifeguards on arrival of EMS
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER
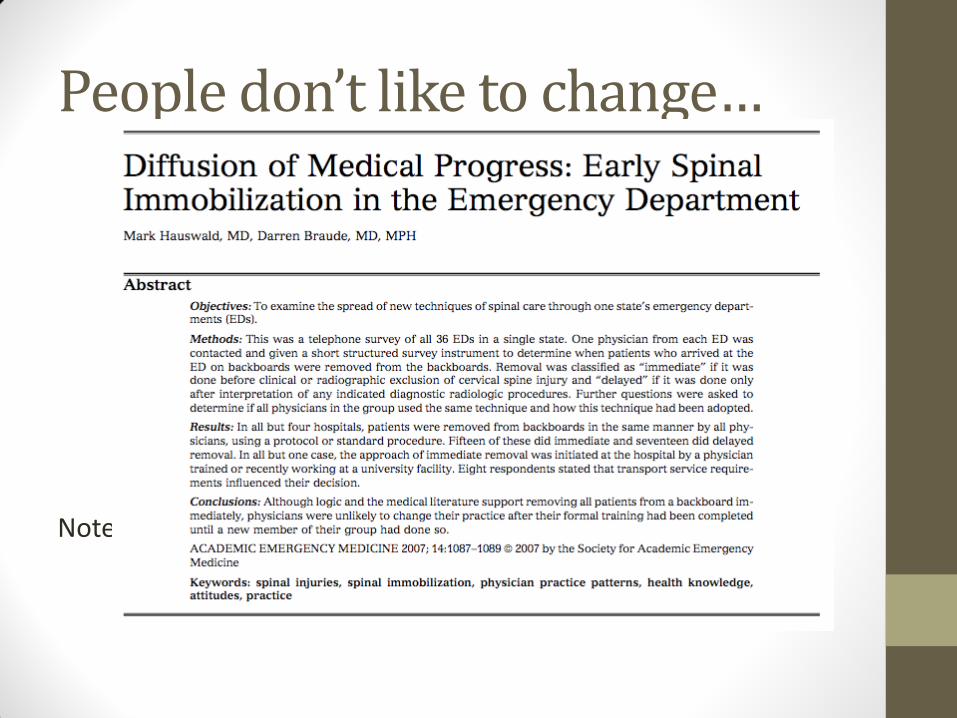
Pregnant patients vomiters
Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Seemed like a good idea at the timehelliphelliphellipbut
Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Spine Boards as Modern Art
bull Maybe their best use
Best Picture EVER

Best Picture EVER