the uses and limitations of the fetal biophysical profile
TRANSCRIPT
The Uses andLimitations of theFetal BiophysicalProfi le
Yinka Oyelese, MD, MRCOGa,b,*, Anthony M. Vintzileos, MDc,d
KEYWORDS
� Fetal biophysical profile � Antepartum fetal assessment� Real-time ultrasound � Non-stress test
In the second half of the twentieth century, true antepartum fetal assessment becamepossible, mainly due to the advent of real-time ultrasound. Initially, the most widelyused form of antepartum fetal assessment was electronic fetal heart rate (FHR)monitoring, through the nonstress test (NST) or the oxytocin-induced contractionstress test (CST). It was soon realized, however, that these forms of monitoring hadsignificant limitations. The NST or CST, when normal, is highly predictive of fetalwell-being. Both the NST and CST, however, have high false-positive rates (45%–75%),1,2 with the possibility of unnecessary and sometimes preterm delivery of a fetusactually in good health. The biophysical profile (BPP) allows a more thorough evalua-tion of fetal well-being and has the potential to significantly reduce the false-positiverate of the NST/CST.The BPP was initially described by Manning and colleagues3 in 1980 and aimed at
a more complete evaluation of fetal well-being. The fetal BPP, as these investigatorsdescribed it, consisted of 5 fetal activities: FHR assessment, fetal movement (FM),fetal tone (FT), fetal respiratory movements, and amniotic fluid (AF) volume(Table 1). Each of these components, when present (normal), is assigned a score of 2.
a The Perinatal Institute, Department of Obstetrics & Gynecology, Jersey Shore UniversityMedical Center, Suite 203, 1944 State Route 33, Neptune, NJ 07753, USAb Division of Maternal Fetal Medicine, Department of Obstetrics, Gynecology & ReproductiveSciences, UMDNJ-Robert Wood Johnson Medical School, 125 Paterson Street, New Brunswick,NJ 08901, USAc Department of Obstetrics & Gynecology, Winthrop University Hospital, 259 First Street,Mineola, NY 1150, USAd Department of Obstetrics, Gynecology & Reproductive Medicine, State University of NewYork, Stony Brook, NY 11794, USA* Corresponding author. Division of Maternal Fetal Medicine, Department of Obstetrics, Gyne-cology & Reproductive Sciences, UMDNJ-Robert Wood Johnson Medical School, 125 PatersonStreet, New Brunswick, NJ 08901.E-mail address: [email protected]
Clin Perinatol 38 (2011) 47–64doi:10.1016/j.clp.2010.12.008 perinatology.theclinics.com0095-5108/11/$ – see front matter � 2011 Elsevier Inc. All rights reserved.

Table 1Fetal biophysical profile scoring
Score 2 Score 0
Movements Three or more gross body movementsin a 30-minute period.Simultaneous trunk and limbmovements count as a singlemovement
Fewer than 3 gross body movementsin a 30-minute period
Tone At least one movement of a limb froma position of flexion to one ofextension, with a rapid return toflexion
Fetal limb in extension with no returnto flexion with movement
Breathing At least 30 seconds of sustained FBMsobserved over a 30-minute period
Fewer than 30 seconds of sustainedFBMs observed over a 30-minuteperiod
AF At least a single amniotic fluid pocketmeasuring 2 cm � 2 cm in 2perpendicular planes
No amniotic fluid pocket thatmeasures at least 2 cm � 2 cm in2 perpendicular planes
FHR At least 2 accelerations (of >15 bpm,lasting at least 15 seconds) in a40-minute period
Fewer than 2 accelerations in 40minutes
Data from Manning FA, Platt LD, Sipos L. Antepartum fetal evaluation: development of a fetalbiophysical profile. Am J Obstet Gynecol 1980;136:787–95.
Oyelese & Vintzileos48
Thus, the maximum score attainable is a 10. Because of their belief that fetuses thatshowed some biophysical activities that did not meet the criteria for a score of 2 arelikely different from those that show a total absence of the particular biophysicalactivity (both assigned a score of 0 according to Manning’s BPP), Vintzileos andcolleagues4 subsequently proposed an alternative BPP scoring system (Box 1). Inthis scoring system, intermediate scores of 1 were given when a fetus demonstratedsome activity that did not qualify for a score of 2 in an attempt to determine for eachcomponent the minimum requirements for “normalcy.” In addition, these investigatorsadded a sixth component of the BPP scoring system, placental grading (PL). In thisscoring system, the maximum score possible is 12.
OBJECTIVES OF THE BIOPHYSICAL PROFILE
The primary objectives of the BPP are to reduce stillbirth and to detect hypoxia earlyenough to allow delivery in time to avoid permanent fetal damage resulting from fetalasphyxia. Before going into a discussion about the BPP, however, it is important tounderstand that the efficacy of any fetal surveillance method to prevent fetal deathor damage depends on an understanding of the particular pathophysiologic processthat leads to neurologic damage or fetal death.5,6 Kontopoulos and Vintzileos5 havepreviously described the different pathophysiologic processes that result in fetal deathand asphyxia (Table 2) and proposed the concept of condition-specific antepartumfetal testing, with testing modalities selected based on the particular process that pla-ces a fetus at risk. It is crucial for obstetricians to realize that there is no ideal test forevery high-risk fetus/pregnancy.6 Some common clinical indications for antepartumfetal surveillance are shown in Box 2. Before deciding about the appropriate antepar-tum testing, however, clinicians should always take into consideration the specificpathophysiologic process or processes that accompany these clinical indications.
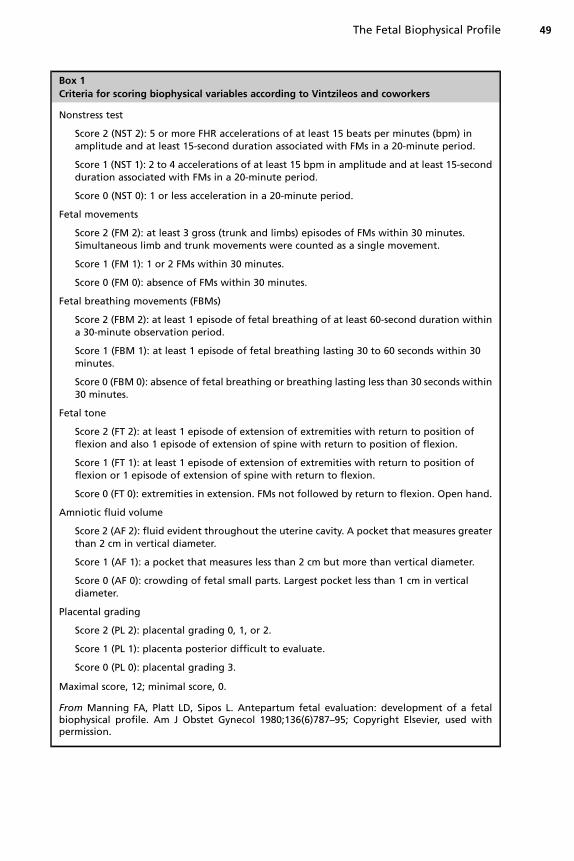
Box 1
Criteria for scoring biophysical variables according to Vintzileos and coworkers
Nonstress test
Score 2 (NST 2): 5 or more FHR accelerations of at least 15 beats per minutes (bpm) inamplitude and at least 15-second duration associated with FMs in a 20-minute period.
Score 1 (NST 1): 2 to 4 accelerations of at least 15 bpm in amplitude and at least 15-secondduration associated with FMs in a 20-minute period.
Score 0 (NST 0): 1 or less acceleration in a 20-minute period.
Fetal movements
Score 2 (FM 2): at least 3 gross (trunk and limbs) episodes of FMs within 30 minutes.Simultaneous limb and trunk movements were counted as a single movement.
Score 1 (FM 1): 1 or 2 FMs within 30 minutes.
Score 0 (FM 0): absence of FMs within 30 minutes.
Fetal breathing movements (FBMs)
Score 2 (FBM 2): at least 1 episode of fetal breathing of at least 60-second duration withina 30-minute observation period.
Score 1 (FBM 1): at least 1 episode of fetal breathing lasting 30 to 60 seconds within 30minutes.
Score 0 (FBM 0): absence of fetal breathing or breathing lasting less than 30 seconds within30 minutes.
Fetal tone
Score 2 (FT 2): at least 1 episode of extension of extremities with return to position offlexion and also 1 episode of extension of spine with return to position of flexion.
Score 1 (FT 1): at least 1 episode of extension of extremities with return to position offlexion or 1 episode of extension of spine with return to flexion.
Score 0 (FT 0): extremities in extension. FMs not followed by return to flexion. Open hand.
Amniotic fluid volume
Score 2 (AF 2): fluid evident throughout the uterine cavity. A pocket that measures greaterthan 2 cm in vertical diameter.
Score 1 (AF 1): a pocket that measures less than 2 cm but more than vertical diameter.
Score 0 (AF 0): crowding of fetal small parts. Largest pocket less than 1 cm in verticaldiameter.
Placental grading
Score 2 (PL 2): placental grading 0, 1, or 2.
Score 1 (PL 1): placenta posterior difficult to evaluate.
Score 0 (PL 0): placental grading 3.
Maximal score, 12; minimal score, 0.
From Manning FA, Platt LD, Sipos L. Antepartum fetal evaluation: development of a fetalbiophysical profile. Am J Obstet Gynecol 1980;136(6)787–95; Copyright Elsevier, used withpermission.
The Fetal Biophysical Profile 49

Table 2Antepartum maternal/fetal pathophysiologic processes that place the fetus at risk of in uterodeath or neurologic damage
Pathophysiologic Process Maternal/Fetal Condition
Decreased uteroplacentalblood flow
Chronic hypertensionPreeclampsiaCollagen/renal/vascular diseaseMost cases of fetal growth restriction (ie, <32–34 wk)
Decreased gas exchange Postdates pregnancy, some fetal growth restricted cases(ie, >32–34 wk)
Metabolic aberrations Fetal hyperglycemiaFetal hyperinsulinemia
Fetal sepsis PROMIntra-amniotic infectionMaternal fever, primary subclinical intra-amniotic
infection
Fetal anemia Fetomaternal hemorrhageErythroblastosis fetalisParvovirus B19 infection
Fetal heart failure Cardiac arrhythmiaNonimmune hydropsPlacental chorioangiomaAneurysm of the vein of Galen
Umbilical cord accident Umbilical cord entanglement (monoamniotic twins)Velamentous cord insertion/funic presentationNoncoiled umbilical cordOligohydramnios
Box 2
Some common clinical indications for antepartum fetal surveillance
1. Intrauterine growth restriction
2. Prior stillbirth
3. Diabetes
4. Hypertension
5. Preeclampsia
6. Postdates pregnancies
7. Preterm premature rupture of the membranes (PPROM)
8. Oligohydramnios
9. Decreased FMs
10. Prior stillbirth
11. Maternal lupus
12. Multifetal pregnancies, in particular those with growth disturbances or discordance
13. Cholestasis of pregnancy
Oyelese & Vintzileos50
The Fetal Biophysical Profile 51
TECHNIQUE
Two methods are used in the performance of the BPP. The first is the performance ofan NST. This is a continuous FHR tracing. The normal fetal baseline heart rate is 110to 160 bpm. The NST is considered reactive when there are 2 or more accelerations(a short increase in FHR of >15 bpm, lasting at least 15 seconds) in 20 minutes. Forgestations less than 32 weeks, the qualifying criteria for accelerations are greaterthan 10 bpm, lasting at least 10 seconds. A reactive NST is assigned 2 points inthe BPP.Real-time ultrasound is then performed. In this examination, fetal gross body move-
ments, tone, respiratory movements, and AF volume are assessed. A score of 2 pointsis assigned for each of these biophysical activities that is present. It is crucial thatproper technique be employed when performing a BPP. To obtain 2 points for eachbiophysical activity, the following should be present:
1. For FMs, there should be at least 3 rolling movements of the fetal trunk in 30minutes. Isolated limb movements do not qualify.
2. There should be continuous FBMs present for at least 30 seconds, with breath-breath intervals of less than 6 seconds.
3. To qualify for FT, there must be a rapid change from flexion to extension and thenback to flexion.
4. The AF volume measurement should be performed with the transducer perpendic-ular to the floor, and measurements should only include cord-free pockets.
The ultrasound portion of BPP is considered complete when all the biophysicalactivities have been observed, yielding a score of 8/8 (Manning scoring system) or12/12 (Vintzileos scoring system), or after 30 minutes of scanning. The BPP iscompleted in the first 4 minutes 90% of the time and the mean time taken to completethe BPP is under 8 minutes.7 Vibroacoustic stimulation using an artificial larynx mayshorten the time of testing as well as the number of nonreassuring tests.8,9
RATIONALE FOR THE BIOPHYSICAL PROFILE
The fetal BPP is based on the principle that the fetal biophysical activities arecontrolled by centers in the fetal brain that are sensitive to varying degrees of hypoxia.The presence of a particular biophysical activity is taken as evidence that the centerresponsible for that activity is intact and has not been subjected to hypoxia andacidosis. The absence of a particular biophysical activity does not necessarily meanthat the center is malfunctioning because of fetal compromise, however. The biophys-ical activities are subject to periodicity; the fetus undergoes sleep cycles, and theabsence of a biophysical activity may simply indicate that the testing was performedduring a sleep cycle. Furthermore, maternal depressant medications may also lead tosuppression of biophysical activities.The timingof theappearanceof thebiophysical activities hasbeenstudied.10 The first
of the biophysical activities to appear is FT, controlled by a center in the fetal cortex-subcortex, which appears at approximately 8 weeks of gestation. Shortly thereafter,theFMcenter in the fetal cortical nuclei becomesactive at approximately 9weeks. Fetalrespiratory movements, controlled by a center in the ventral surface of the fourthventricle, are first noted at approximately 21 weeks, and FHR reactivity, regulated inthe posterior hypothalamus and medulla, becomes established late in the secondtrimester or in the early third trimester. The proportion of NSTs that are reactiveincreases with gestational age up to 40 weeks.10,11 As pregnancies go past 40 weeks,

Oyelese & Vintzileos52
however, FBMs and AF volume become decreased.10 Baskett11 studied 5582 womenwith normal pregnancy outcomes who had a total of 11,012 BPPs performed. Theyfound that NSTs and breathing movements were more likely to be abnormal at 26 to33 weeks of gestation when compared with later gestational ages. They also foundincreased rates of abnormal NSTs and AF volumes as pregnancies went past 42weeksof gestation.11 Grade 3 placentas start to be seen at 32 weeks.10
The fetal BPP has been likened to examination of an adult’s vital signs and to theApgar score in a newborn. Thus, FHR, body movements, tone, and respiratory move-ments assess the well-being of a fetus.FHR reactivity, movement, tone, and respiratory movements are acute markers of
fetal well-being whereas AF volume and PL are chronic markers.The observation has been made that the last biophysical activities to appear in fetal
life are the first to disappear when a fetus becomes compromised by acidemia or infec-tion. This “gradual hypoxia concept”was first described by Vintzileos and coworkers.12
Themost sensitive centers to fetal hypoxia are the FHR reactivity andbreathing centers.These control the biophysical activities that appear last in gestation; they are also thefirst to become affected when a fetus is exposed to acidemia or infection. The authorspreviously showed that FHR reactivity and fetal breathing are abolishedwhen fetal pH isless than 7.20, whereas FM and tone are abolished at pH values less than 7.10.12 Asa fetus becomes progressively more hypoxic and acidemic, FMs and then tonedisappear.12 The absence of FT, the fetal biophysical activity that is that last to disap-pear when there is fetal compromise, is associated with a higher perinatal death rate(42.8%) than the absence of any other biophysical activities.4
THE BIOPHYSICAL SCORE IS INVERSELY RELATED TO FETAL ACIDOSIS
Vintzileos and colleagues12 carried out a prospective study on 124 consecutive preg-nant women undergoing cesarean deliveries prior to the onset of labor between 26and 43 weeks of gestation. These investigators performed BPPs on these patientswithin 6 hours of their cesarean deliveries. They then measured the umbilical cordpH (arterial and venous) immediately after delivery (Fig. 1). They divided the womeninto 3 groups based on their BPP scores (�4, 5–7, �8). They defined as fetal acidemiaan umbilical arterial cord pH less than 7.20. They reported sensitivity, specificity, and
Fig. 1. Relationship between the fetal biophysical score and umbilical cord arterial pH.(From Vintzileos AM, Gaffney SE, Salinger LM, et al. The relationship between the fetalbiophysical profile and cord pH in patients undergoing cesarean section before the onsetof labor. Obstet Gynecol 1987;70:196; with permission.)
The Fetal Biophysical Profile 53
positive and negative predictive values of an abnormal BPP score (defined as a scoreof <8) for fetal acidemia as 90%, 96%, 82%, and 98%, respectively.12 The 3 groupshad statistically different cord arterial pH values, and the pH after delivery correlatedwith the BPP. All 9 fetuses with BPP scores less than 4 were acidemic. The meanumbilical arterial pH value in this group was 6.99� 0.10 (mean� SD). Themean umbil-ical artery pH in those 102 fetuses with a BPP score of greater than or equal to 8 was7.28 � 0.04 (mean � SD). Two fetuses with a BPP score of greater than or equal to 8were acidemic. Nine out of 13 fetuses with a score of 5 to 7 were acidemic (mean cordpH 7.19� 0.06 [mean� SD]). The relationship between the biophysical score and cordvenous pH was similar. Thus, this study demonstrated worsening fetal acid-basestatus in association with lower BPP scores.Ribbert and coworkers13 performed BPPs prior to fetal blood sampling by cordo-
centesis in 14 severely growth restricted fetuses and reported that fetal BPP corre-lated with fetal blood PO2, pH, oxygen saturation, and oxygen content. Theseinvestigators found that FHR reactivity was compromised when the observed pH sub-tracted from the appropriate mean for gestation (Δ pH) fell below �2 SDs. When theΔ pH values fell below �3 SDs, FBMs were compromised. Fetal body movementsand tone were compromised when the Δ pH values fell below �4 SDs. Because cor-docentesis allows accurate assessment of fetal blood acid-base status without con-founding by labor or medications, these findings confirm that fetal BPP predicts thedegree of fetal acidemia. The findings support the gradual hypoxia concept. FHRreactivity and FBMs are the first biophysical activities to become compromised inresponse to hypoxia/acidemia, and as hypoxia and acidemia worsen, fetal grossbody movements and tone become compromised.
INDIVIDUAL FETAL BIOPHYSICAL ACTIVITIES HAVE DIFFERENT SENSITIVITIESTO FETAL HYPOXIA/ACIDEMIA
In a subsequent study, Vintzileos and colleagues14 prospectively studied 62 womenundergoing cesarean delivery prior to the onset of labor, performing BPPs within 3hours of their cesarean deliveries. They correlated the presence and absence of indi-vidual fetal biophysical activities with the umbilical cord arterial and venous pHvalues obtained immediately after delivery. Fetuses with absent breathing or nonre-active NSTs had lower umbilical arterial pH values than those where breathing waspresent or where the NST was reactive.14 Similarly, fetuses with absent movementsand tone had lower umbilical arterial pH values than those in whom movement ortone were present. Closer analysis revealed that the presence of individual biophys-ical activities was related to the degree of fetal acidemia.14 The NST became nonre-active and FBMs became absent at higher pH values than it took for FM and tone todisappear (Fig. 2A).14 A similar pattern was observed for all other blood gases (seeFig. 2B–D).14
In a study of 124 nonlaboring patients who had BPPs prior to cesarean delivery,in the 96 patients with reactive NSTs and/or fetal breathing, no fetus wasacidemic.12 Fetuses demonstrating a nonreactive NST and absent breathing butwith normal movements and tone had a mean umbilical arterial pH of 7.20. Fifty-nine percent of fetuses in this group were acidemic. In fetuses with absent fetalbreathing or nonreactive NSTs, and also with reduced FMs (1 or 2 instead of atleast 3 gross body movements in 30 minutes) or tone, the mean umbilical arterialpH was 7.16. When all biophysical activities were absent, the mean umbilical arte-rial pH was 6.95 and all the fetuses were acidemic at birth. Of the individualbiophysical components, FHR reactivity and fetal breathing had 100% sensitivities
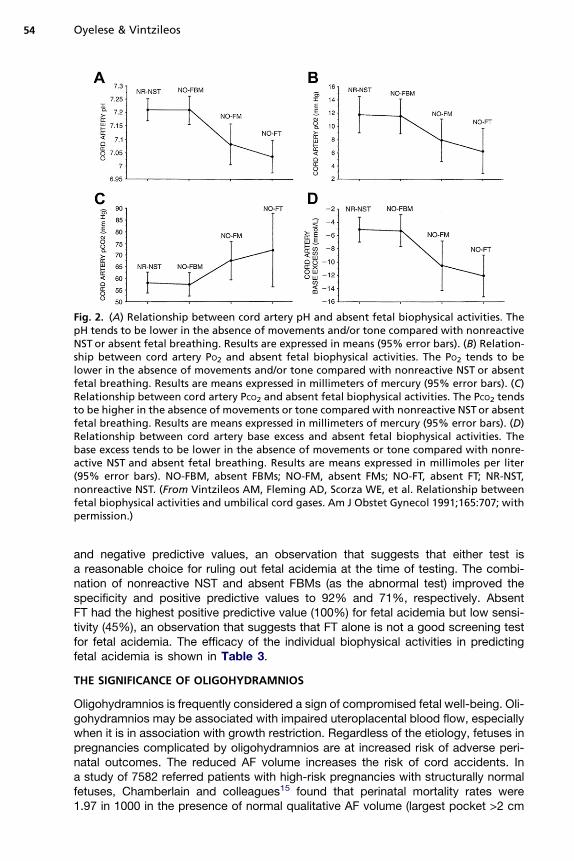
Fig. 2. (A) Relationship between cord artery pH and absent fetal biophysical activities. ThepH tends to be lower in the absence of movements and/or tone compared with nonreactiveNST or absent fetal breathing. Results are expressed in means (95% error bars). (B) Relation-ship between cord artery PO2 and absent fetal biophysical activities. The PO2 tends to belower in the absence of movements and/or tone compared with nonreactive NST or absentfetal breathing. Results are means expressed in millimeters of mercury (95% error bars). (C)Relationship between cord artery PCO2 and absent fetal biophysical activities. The PCO2 tendsto be higher in the absence of movements or tone compared with nonreactive NSTor absentfetal breathing. Results are means expressed in millimeters of mercury (95% error bars). (D)Relationship between cord artery base excess and absent fetal biophysical activities. Thebase excess tends to be lower in the absence of movements or tone compared with nonre-active NST and absent fetal breathing. Results are means expressed in millimoles per liter(95% error bars). NO-FBM, absent FBMs; NO-FM, absent FMs; NO-FT, absent FT; NR-NST,nonreactive NST. (From Vintzileos AM, Fleming AD, Scorza WE, et al. Relationship betweenfetal biophysical activities and umbilical cord gases. Am J Obstet Gynecol 1991;165:707; withpermission.)
Oyelese & Vintzileos54
and negative predictive values, an observation that suggests that either test isa reasonable choice for ruling out fetal acidemia at the time of testing. The combi-nation of nonreactive NST and absent FBMs (as the abnormal test) improved thespecificity and positive predictive values to 92% and 71%, respectively. AbsentFT had the highest positive predictive value (100%) for fetal acidemia but low sensi-tivity (45%), an observation that suggests that FT alone is not a good screening testfor fetal acidemia. The efficacy of the individual biophysical activities in predictingfetal acidemia is shown in Table 3.
THE SIGNIFICANCE OF OLIGOHYDRAMNIOS
Oligohydramnios is frequently considered a sign of compromised fetal well-being. Oli-gohydramnios may be associated with impaired uteroplacental blood flow, especiallywhen it is in association with growth restriction. Regardless of the etiology, fetuses inpregnancies complicated by oligohydramnios are at increased risk of adverse peri-natal outcomes. The reduced AF volume increases the risk of cord accidents. Ina study of 7582 referred patients with high-risk pregnancies with structurally normalfetuses, Chamberlain and colleagues15 found that perinatal mortality rates were1.97 in 1000 in the presence of normal qualitative AF volume (largest pocket >2 cm
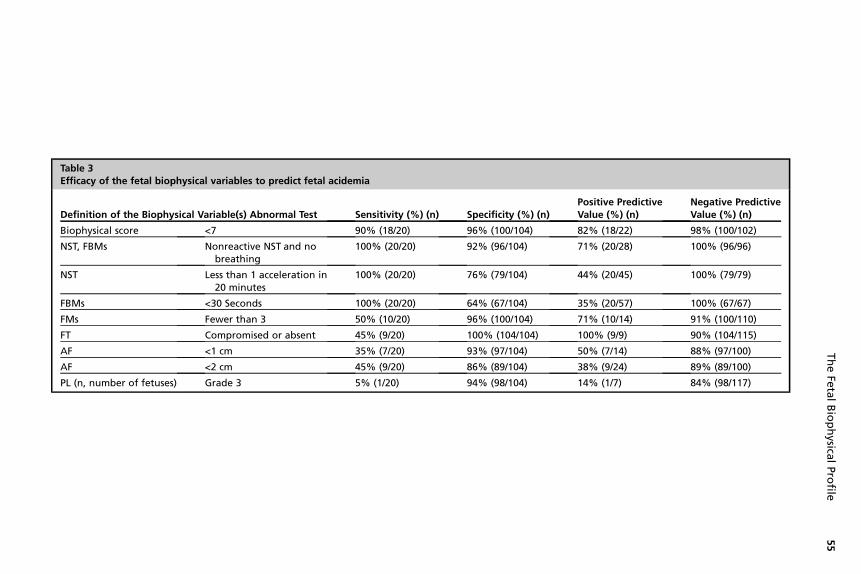
Table 3Efficacy of the fetal biophysical variables to predict fetal acidemia
Definition of the Biophysical Variable(s) Abnormal Test Sensitivity (%) (n) Specificity (%) (n)Positive PredictiveValue (%) (n)
Negative PredictiveValue (%) (n)
Biophysical score <7 90% (18/20) 96% (100/104) 82% (18/22) 98% (100/102)
NST, FBMs Nonreactive NST and nobreathing
100% (20/20) 92% (96/104) 71% (20/28) 100% (96/96)
NST Less than 1 acceleration in20 minutes
100% (20/20) 76% (79/104) 44% (20/45) 100% (79/79)
FBMs <30 Seconds 100% (20/20) 64% (67/104) 35% (20/57) 100% (67/67)
FMs Fewer than 3 50% (10/20) 96% (100/104) 71% (10/14) 91% (100/110)
FT Compromised or absent 45% (9/20) 100% (104/104) 100% (9/9) 90% (104/115)
AF <1 cm 35% (7/20) 93% (97/104) 50% (7/14) 88% (97/100)
AF <2 cm 45% (9/20) 86% (89/104) 38% (9/24) 89% (89/100)
PL (n, number of fetuses) Grade 3 5% (1/20) 94% (98/104) 14% (1/7) 84% (98/117)
TheFe
talBiophysica
lProfile
55
Oyelese & Vintzileos56
and <8 cm) compared with 37.7 in 1000 and 109.4 in 1000, respectively, in fetuses withmarginal (largest pocket 1–2 cm) and decreased AF (largest pocket <1 cm). In a studyof 6423 pregnancies greater than 34 weeks, Casey and colleagues16 found that 147pregnancies (2.3%) were complicated by oligohydramnios.16 They found that thesepregnancies had an increased risk of labor induction, nonreassuring FHR patterns,cesarean delivery, neonatal intensive care unit admission, meconium aspiration, still-birth, and neonatal death.
PLACENTAL GRADING
PL as a component of the BPP has not found widespread acceptance. Vintzileos andcolleagues4 found an increased rate of placental abruption and labor complicationsamong patients with grade 3 placentas. A recent study has demonstrated an up to6-fold increase in adverse perinatal outcomes (including placental abruption, low birthweight, low Apgar score, and perinatal death) among pregnancies where a grade 3placenta was identified prior to 32 weeks of gestation.17 Thus, even though PL isnot commonly used in the BPP, the recognition of a grade 3 placenta prior to 32 weeksshould lead to a high index of suspicion for fetal jeopardy.
THE BIOPHYSICAL PROFILE: EARLY STUDIES
In the first prospective study using the BPP for management of 1184 high-riskpatients, Manning and colleagues18 found a perinatal mortality rate of 5.06/1000,considerably lower than the rate of 63/1000 in historical controls (a similar high-riskpopulation from the same region the previous year). Baskett and colleagues19 in1984 published the results of a study where they used the BPP in managing 2400high-risk pregnancies with 2485 fetuses. They found a perinatal mortality rate ofonly 1/1000 in those 1980 fetuses with a normal BPP score within 7 days of delivery,compared with an overall perinatal mortality rate of 9.2/1000.Subsequently, Manning and colleagues carried out the first randomized trial using
the BPP and published the results in 1984. They compared the BPP in 375 patientswith the NST in 360 patients and found that the BPP was more predictive of low Apgarscores.20 Although the BPP’s sensitivity, specificity, positive predictive value andaccuracy were higher than those of the NST, these differences between the BPPand the NST did not achieve statistical significance.20 After this, the same investiga-tors studied 29 fetuses with an Apgar score of 0. They found that 14/29 of these peri-nates, almost half, died. Eleven were stillborn. In these, death occurred as soon as 30minutes and as late as 11 days after the last test.21
THE BIOPHYSICAL PROFILE: IMPACT ON PERINATAL MORTALITY
Several studies have demonstrated the efficacy of the BPP in reducing perinatalmortality. In a study of 12620 high-risk patients who had 26357 biophysical scores,Manning and colleagues22 found that there were 93 perinatal deaths. Twenty-four ofthese occurred in structurally normal, nonisoimmunized fetuses (corrected perinatalmortality rate 1.9/1000). Eight of these fetuses died within 7 days of a normal BPPtest (corrected false-negative rate of 0.634/1000). The uncorrected stillbirth rate was3.64/1000 and the uncorrected neonatal death rate was 3.72/1000.22 These investiga-tors found that the overall perinatal mortality ranged from 0.652/1000 births in patientswith a BPP score of greater than or equal to 8 to 187/1000 births in pregnancies witha BPP score of 0, confirming that lower BPP scores are associated with higher peri-natal mortality rates.22 The overwhelming majority of the BPPs (97.5%) were normal
The Fetal Biophysical Profile 57
and only 0.76% had a BPP score of less than or equal to 4. The same investigatorsreported their experience with 44,828 BPPs performed in 19,921 high-risk pregnan-cies. The intrauterine death rate among fetuses without anomalies after a normalBPP was 0.726/1000 (14 deaths). Of these, approximately one-third resulted fromcord prolapse. It is reasonable to assume these may not have been predicted byBPP assessment. If these deaths due to cord prolapse were excluded, the deathrate could have been as low as 0.518/1000. Almost half the antepartum deathsoccurred 5 to 7 days after a normal BPP result. It is as a result of this finding thatBPPs are often performed twice a week in an attempt to further reduce perinatalmortality.In a study of 4148 fetuses, Baskett and coworkers23 found an overall perinatal
mortality rate of 7.6/1000. Fetuses with a normal BPP (score 8–10) had a perinatal mor-tality rate of 1/1000, whereas fetuses with an equivocal score of 6 had a perinatalmortality of 31.3/1000. Even more importantly, fetuses with a BPP score of 0 to 4had an extremely high perinatal mortality rate of 200/1000.These studies confirm that patients with normal biophysical testing have reduced
perinatal mortality rates and that, conversely, perinatal outcomes worsen as BPPscores get lower.
THE MODIFIED BIOPHYSICAL PROFILE SCORE (AF AND NST)
Because of the excellent sensitivity of fetal NST for fetal acidemia, it has beenproposed that this acute marker alone may be used for fetal assessment in combina-tion with the AF volume assessment, a chronic marker. This combination, also knownas the modified BPP, has been shown to have excellent false-negative rates thatcompare with that of the complete BPP.24,25
THE BIOPHYSICAL PROFILE AND PRETERM PREMATURE RUPTURE OF THE MEMBRANES
The fetal BPP has been used in the assessment and management of pregnanciescomplicated by PPROM. Vintzileos and colleagues compared BPPs in women withpremature rupture of membranes (PROM) with women with intact membranes atgestational ages ranging from 25 to 44 weeks.10,26 They found no differences in totalBPP scores between the 2 groups. They did find a higher frequency of reduced AFvolume, reactive NSTs, and absent FBMs, however, in those patients with PROM.10
These same investigators subsequently performed BPPs every 24 to 48 hours on 73women with PPROM who were not in labor and found that PPROM did not affect theBPP score.27 They compared the last BPP score with the infection outcome of thepregnancy (clinical chorioamnionitis, possible neonatal sepsis, and neonatal sepsis).They found that an abnormal BPP score (<8) was associated with an overall infectionrate of 93.7%, whereas the overall infection rate in those pregnancies with a normalBPP score (8) was only 2.7%.27 They concluded that abnormal BPP scores werehighly predictive of infection outcome. They only found this relationship betweenabnormal BPP testing and infectious morbidity when the interval between testingand delivery was 24 hours or less. In fetuses with severe infection as evidenced byneonatal sepsis (defined as infection confirmed by positive blood, urine, or cerebro-spinal fluid culture), FMs and tone were compromised, whereas fetuses with possibleneonatal sepsis (evidence of infection but negative cultures) had absent breathingmovements and nonreactive NSTs. Because there was no difference in umbilicalcord arterial pH values between infected and noninfected cases, the compromisedbiophysical activities were thought to be due to fetal infection rather than to acidemia.Correlations have also been found between both degree of oligohydramnios26 and
Oyelese & Vintzileos58
nonreactive NSTs in PPROM and risk of intra-amniotic infection. Patients with PPROMand severe oligohydramnios (largest AF pocket <l cm) had the highest frequency ofclinical chorioamnionitis (47.3%), possible neonatal sepsis (26.3%), and neonatalsepsis (31.5%), compared with 9.2%, 3.7%, and 1.8%, respectively, in patientswith a largest AF pocket greater than 2 cm.26 In a retrospective analysis of 127consecutive patients with PROM who had NSTs performed every 24 to 48 hours aspart of the fetal BPP, those who initially had a reactive NST that subsequently con-verted to a nonreactive NST developed clinical intra-amniotic infection in almost90% of cases.28 FBMs have also been shown to predict the absence of infection inpatients with PPROM.29 Based on its ability to predict infection in PPROM, even indirect comparison to amniocentesis, Vintzileos and colleagues30 have suggestedthat daily BPPs could replace amniocentesis for prediction of infection in patientswith PPROM. Several other studies have examined the relationship between BPPscores in PPROM and perinatal infection.31–37 At least two-thirds of these studieshave demonstrated a correlation between the two. In those studies that did finda correlation, daily BPP testing was performed. Intra-amniotic infection with Myco-plasma hominis is not necessarily associated with an abnormal BPP.31
THE BIOPHYSICAL PROFILE SCORE AND LONG-TERM OUTCOMES
There may be some relationship between abnormal BPP scores and long-term neuro-developmental outcomes. Manning and colleagues,38 using 2 linked databases,attempted to determine if there was any relationship between the last BPP score inwomen having serial BPPs and the development of cerebral palsy at age 3 years.Of 22,336 high-risk pregnancies, 27 babies later developed cerebral palsy. Theseinvestigators found a relationship between last abnormal BPP scores and subsequentdevelopment of cerebral palsy. In a study of 84,947 live births, Manning andcolleagues38 found that the rate of cerebral palsy among those 26,290 high-risk preg-nancies that underwent BPP testing was 1.33 per 1000 live births, compared with 4.74per 1000 live births in those 58,657 low-risk/mixed pregnancies that were not tested.They found an inverse, exponential, and highly significant relationship between the lastBPP score and the development of cerebral palsy.38
MEDICATIONS AND THE BIOPHYSICAL PROFILE
Several medications used in pregnancy may affect the BPP. These include steroids,b-adrenergic agents, and magnesium sulfate.Rotmensch and colleagues39 studied 31 women between 27 and 32 weeks of
gestation who were receiving 2 doses of betamethasone. They found an approxi-mately 80% to 90% reduction in FBMs over 48 hours as well as a 50% reduction infetal body movements. FT and AF volume remained stable. Half of all fetuses hada BPP score of 6/8 or 4/8; within 96 hours, however, all BPP scores had returned tonormal. Similar reductions in fetal body and breathing movements after betametha-sone administration were observed by Jackson and colleagues.40 These investigatorsalso found, however, a reduction in AF volume in most patients, a finding they attrib-uted to a reduction in FBMs. Deren and coworkers41 also found a reduction in fetalbody movements and respiration after steroid administration. They also found morenonreactive NSTs after steroids. In all these studies, there was a reduction in BPPscores among some of the fetuses that received steroids. It is important to recognizethis effect of steroids on the BPP in order to avoid unnecessary interventions.Magnesium sulfate is one of the most commonly used tocolytics in the United
States. In a study of 31 fetuses (25 pregnancies), Gray and colleagues42 observed

The Fetal Biophysical Profile 59
that intravenous magnesium sulfate did not significantly affect the BPP. In a study of16 women with 22 fetuses at gestational ages of 26 to 34 weeks in spontaneouspreterm labor, Peaceman and colleagues43 found that approximately half of thefetuses developed nonreactive NSTs and most fetuses had reduced FBMs after intra-venous magnesium sulfate administration. Carlan and colleagues44 also founda reduction in FBMs, but no other changes in the BPP, in pregnancies when magne-sium sulfate was administered for tocolysis. Hallak and colleagues45 found that bothterbutaline and indomethacin, two other tocolytic agents in common use, increasedFBMs, but had no other effects on the BPP.
LIMITATIONS OF THE BIOPHYSICAL PROFILE
The fetal BPP is a powerful tool in the assessment of fetal health. Yet, it is often misun-derstood and misused.46 Perhaps the most important reason that BPP is misusedrelates to failure to consider the entire clinical scenario.46 For instance, a fetus atterm with severe growth restriction should be delivered, despite the presence ofa reassuring BPP score.Among the most common problems is using the total score without any consider-
ation of the individual components.46 For instance, a score of 6/8 where 2 pointsare taken off for severe oligohydramnios is different from 6/8 where 2 points are takenoff for lack of movement, but where fetal breathing is present.Another example is where a fetus with a reactive NST and normal AF but without
obvious tone or movements during the examination is assigned a score of 4. In thiscase, however, both a reactive NST (the most sensitive acute marker) and normalAF volume (a chronic marker) are present, suggesting that the fetus is not compro-mised but that the absence of the other biophysical activities is due to periodicity.Unfortunately, such patients are often considered to have failed their BPP, and notinfrequently, delivery is undertaken, often by cesarean, and possibly prematurely.It is inappropriate to use the same interval of testing for all cases. Although a BPP
score is generally considered reliable for 1 week, certain high-risk conditions,including type 1 diabetes mellitus, growth restriction, or postdate pregnancies mayrequire more frequent testing. Manning and colleagues22 observed, in a study ofBPPs in 12,620 pregnancies, that half of the fetal deaths after reassuring BPP resultsoccurred between 5 and 7 days after testing. They, therefore, suggested that twice-weekly testing may reduce mortality. The interval between testing should be individu-alized based on the circumstances of each particular case.It is widely recommended that when a test is nonreassuring, it should be repeated in
24 hours. This approach, however, is likely to lead to further compromise or evendeath in a fetus in jeopardy. The authors recommend that rather than repeatingtesting, extend the period of testing beyond 30 minutes. This helps differentiatebetween a compromised fetus and one where biophysical activities are absent dueto periodicity.The BPP is often performed without an NST and considered adequate. This has the
potential to miss fetuses at risk of death from cord accidents, however, even in thepresence of a reassuring BPP score. FHR variable decelerations may be the onlywarning that a fetus is at risk for a cord accident. False reassurance may be providedif an NST is not performed.It is important, when the BPP is persistently nonreassuring, not to delay delivery due
to concerns, such as an unfavorable cervix or preterm gestation. This may increasethe risk of an adverse perinatal outcome.

Oyelese & Vintzileos60
It is important that the BPP be performed correctly. Often, operator inexperienceand faulty technique may lead to incorrect assessment of biophysical activities andinappropriate management decisions. Thus, AF measurements should be performedwith the transducer perpendicular to the ground, and measurements should be madein cord-free pockets of AF. FBMs should be continuous and last at least 30 seconds. Itis important to distinguish FBMs from fetal gasping movements. FMs should only beconsidered present if at least 3 rolling trunk movements are present in 30 minutes.
SUGGESTED ALGORITHM FOR BIOPHYSICAL PROFILE TESTING
One of the common questions asked about the BPP is when to start testing and withwhat frequency. The management of a pregnancy where the BPP score is not perfectis also a matter of controversy. Before going further, it is again crucial to emphasizethat these cases need to be managed on an individual case-by-case basis. Thus, toanswer the first question, the plan of antepartum testing must be appropriate for theindividual pregnancy circumstances and the underlying pathophysiologic process. Itis also important to appreciate the relationship between the individual biophysicalactivities and gestational age. So, starting biophysical testing at earlier gestationalages results in some activities not being present. If a physician does understandthis limitation, however, BPP testing may be utilized. For instance, at 26 weeks,some fetuses have not yet developed FHR reactivity, and BPP interpretation musttake this into consideration. BPP may have to be combined with other modalities oftesting, including Doppler studies, depending on the particular pathophysiologicprocess. Generally, in fetuses with a high-risk condition where fetal growth is normal,BPP testing is started at approximately 32 weeks. The reason for this is that at 32weeks, biophysical activities are all present in more than 95% of normal fetuses.BPP testing may be started earlier, however, in growth-restricted fetuses and in preg-nancies complicated by PROM, bleeding, and a host of other conditions where thefetus is at more immediate risk, as long as the aforementioned limitations imposedby gestational age are recognized. The frequency of BPP testing also depends onthe particular high-risk situation. A fetus with severe growth restriction may requireBPPs daily or twice a day, whereas one undergoing surveillance for a history of hyper-tension may have a BPP twice weekly. Manning and colleagues reported that a fewdeaths occurred within 4 days of a normal BPP; therefore, it has been proposedthat twice weekly testing may reduce the risk of stillbirth.Based on the fact that the combination of the nonreactive NST and absence of
FBMs has excellent sensitivity for predicting the acidemic fetus, consistent with thegradual hypoxia concept, Vintzileos and coworkers recommended a modified fetalevaluation scheme for patients with intact membranes (Fig. 3). This scheme is basedon the individual biophysical components rather than the score (see Fig. 3)4,46
Manning and coworkers47 have also observed that the NST, AF volume, and breathingmovements are the most powerful predictors of fetal compromise.The authors’ suggested protocol includes assessment of an acute marker (NST or
fetal breathing) and a chronic marker (AF volume). A reactive NST or fetal breathinglasting greater than 30 seconds (even in the presence of a nonreactive NST) makesfetal acidemia at the time of testing highly unlikely. In patients with uncontrolled dia-betes, hyperglycemia may cause fetuses to exhibit FBMs even in the presence of(lactic) acidemia. For this reason, the authors recommend that the blood glucoseshould be checked in diabetic women at the time of the BPP assessment.When the NST is nonreactive, it becomes crucial to differentiate between fetal sleep
and fetal acidemia. The presence of fetal breathing lasting greater than 30 seconds
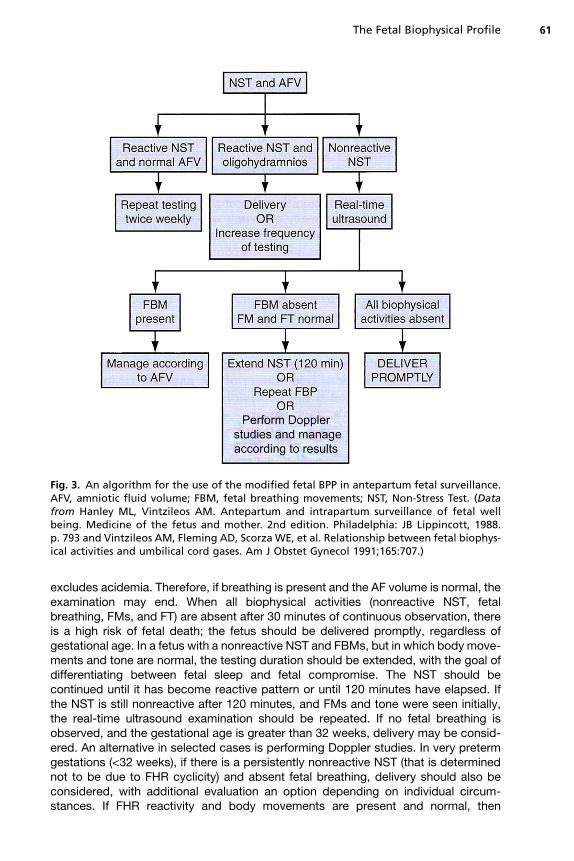
Fig. 3. An algorithm for the use of the modified fetal BPP in antepartum fetal surveillance.AFV, amniotic fluid volume; FBM, fetal breathing movements; NST, Non-Stress Test. (Datafrom Hanley ML, Vintzileos AM. Antepartum and intrapartum surveillance of fetal wellbeing. Medicine of the fetus and mother. 2nd edition. Philadelphia: JB Lippincott, 1988.p. 793 and Vintzileos AM, Fleming AD, Scorza WE, et al. Relationship between fetal biophys-ical activities and umbilical cord gases. Am J Obstet Gynecol 1991;165:707.)
The Fetal Biophysical Profile 61
excludes acidemia. Therefore, if breathing is present and the AF volume is normal, theexamination may end. When all biophysical activities (nonreactive NST, fetalbreathing, FMs, and FT) are absent after 30 minutes of continuous observation, thereis a high risk of fetal death; the fetus should be delivered promptly, regardless ofgestational age. In a fetus with a nonreactive NST and FBMs, but in which body move-ments and tone are normal, the testing duration should be extended, with the goal ofdifferentiating between fetal sleep and fetal compromise. The NST should becontinued until it has become reactive pattern or until 120 minutes have elapsed. Ifthe NST is still nonreactive after 120 minutes, and FMs and tone were seen initially,the real-time ultrasound examination should be repeated. If no fetal breathing isobserved, and the gestational age is greater than 32 weeks, delivery may be consid-ered. An alternative in selected cases is performing Doppler studies. In very pretermgestations (<32 weeks), if there is a persistently nonreactive NST (that is determinednot to be due to FHR cyclicity) and absent fetal breathing, delivery should also beconsidered, with additional evaluation an option depending on individual circum-stances. If FHR reactivity and body movements are present and normal, then
Oyelese & Vintzileos62
expectant management is indicated. Oligohydramnios (defined as a largest AF pocket<2 cm or AF index <5 cm) and/or significant variable FHR decelerations suggest thatthat a fetus is at risk for cord accidents. If these are found, the authors recommenddelivery if the pregnancy is at term or near term. Even in preterm gestations, thesefindings should always be considered concerning and may indicate a need for deliveryin viable, structurally normal fetuses with intact membranes, regardless of gestationalage. In very preterm gestations (<32 weeks) these pregnancies should be managed ona case-by-case basis, taking into consideration the results of Doppler velocimetry (ifthe underlying pathophysiology is reduced uteroplacental blood flow). Regardless, itis crucial to recognize that fetuses with growth restriction and oligohydramnios or vari-able decelerations are at increased risk of stillbirth, and that although prolonginggestation to improve maturity at birth, these fetuses may die while managed conser-vatively. In the presence of early severe fetal growth restriction, if delivery is not under-taken, the authors recommend frequent testing (every 24 hours) with Doppler studiesto assist in deciding management.
REFERENCES
1. Evertson LR, Gauthier RJ, Schifrin BS, et al. Antepartum fetal heart rate testing. I.Evolution of the nonstress test. Am J Obstet Gynecol 1979;133(1):29–33.
2. Gauthier RJ, Evertson LR, Paul RH. Antepartum fetal heart rate testing. II. Intra-partum fetal heart rate observation and newborn outcome following a positivecontraction stress test. Am J Obstet Gynecol 1979;133(1):34–9.
3. Manning FA, Platt LD, Sipos L. Antepartum fetal evaluation: development of a fetalbiophysical profile. Am J Obstet Gynecol 1980;136(6):787–95.
4. Vintzileos AM, Campbell WA, Ingardia CJ, et al. The fetal biophysical profile andits predictive value. Obstet Gynecol 1983;62(3):271–8.
5. Kontopoulos EV, Vintzileos AM. Condition-specific antepartum fetal testing. AmJ Obstet Gynecol 2004;191(5):1546–51.
6. Vintzileos AM. Antepartum fetal surveillance today: the case for condition-specificfetal testing. The Female Patient 2011;1(36):13–4.
7. Manning FA. Fetal biophysical profile. Obstet Gynecol Clin North Am 1999;26(4):557–77, v.
8. Pinette MG, Blackstone J, Wax JR, et al. Using fetal acoustic stimulation toshorten the biophysical profile. J Clin Ultrasound 2005;33(5):223–5.
9. Papadopoulos VG, Decavalas GO, Kondakis XG, et al. Vibroacoustic stimulationin abnormal biophysical profile: verification of facilitation of fetal well-being. EarlyHum Dev 2007;83(3):191–7.
10. VintzileosAM, Feinstein SJ, Lodeiro JG, et al. Fetal biophysical profile and the effectof premature rupture of the membranes. Obstet Gynecol 1986;67(6):818–23.
11. Baskett TF. Gestational age and fetal biophysical assessment. Am J ObstetGynecol 1988;158(2):332–4.
12. Vintzileos AM, Gaffney SE, Salinger LM, et al. The relationship between fetalbiophysical profile and cord pH in patients undergoing cesarean section beforethe onset of labor. Obstet Gynecol 1987;70(2):196–201.
13. Ribbert LS, Snijders RJ, Nicolaides KH, et al. Relationship of fetal biophysicalprofile and blood gas values at cordocentesis in severely growth-retardedfetuses. Am J Obstet Gynecol 1990;163(2):569–71.
14. Vintzileos AM, Fleming AD, Scorza WE, et al. Relationship between fetal biophys-ical activities and umbilical cord blood gas values. Am J Obstet Gynecol 1991;165(3):707–13.
The Fetal Biophysical Profile 63
15. Chamberlain PF, Manning FA, Morrison I, et al. Ultrasound evaluation of amnioticfluid volume. I. The relationship of marginal and decreased amniotic fluid volumesto perinatal outcome. Am J Obstet Gynecol 1984;150(3):245–9.
16. Casey BM, McIntire DD, Bloom SL, et al. Pregnancy outcomes after antepartumdiagnosis of oligohydramnios at or beyond 34 weeks’ gestation. Am J ObstetGynecol 2000;182(4):909–12.
17. Chen KH, Chen LR, Lee YH. Exploring the relationship between pretermplacental calcification and adverse maternal and fetal outcome. UltrasoundObstet Gynecol 2010. [Epub ahead of print].
18. Manning FA, Baskett TF, Morrison I, et al. Fetal biophysical profile scoring:a prospective study in 1,184 high-risk patients. Am J Obstet Gynecol 1981;140(3):289–94.
19. Baskett TF, Gray JH, Prewett SJ, et al. Antepartum fetal assessment using a fetalbiophysical profile score. Am J Obstet Gynecol 1984;148(5):630–3.
20. Manning FA, Lange IR, Morrison I, et al. Fetal biophysical profile score and thenonstress test: a comparative trial. Obstet Gynecol 1984;64(3):326–31.
21. Manning FA, Harman CR, Morrison I, et al. Fetal assessment based on fetalbiophysical profile scoring. III. Positive predictive accuracy of the veryabnormal test (biophysical profile score 5 0). Am J Obstet Gynecol 1990;162(2):398–402.
22. Manning FA, Morrison I, Lange IR, et al. Fetal assessment based on fetalbiophysical profile scoring: experience in 12,620 referred high-risk pregnancies.I. Perinatal mortality by frequency and etiology. Am J Obstet Gynecol 1985;151(3):343–50.
23. Baskett TF, Allen AC, Gray JH, et al. Fetal biophysical profile and perinatal death.Obstet Gynecol 1987;70(3 Pt 1):357–60.
24. Miller DA, Rabello YA, Paul RH. The modified biophysical profile: antepartumtesting in the 1990s. Am J Obstet Gynecol 1996;174(3):812–7.
25. Nageotte MP, Towers CV, Asrat T, et al. Perinatal outcome with the modifiedbiophysical profile. Am J Obstet Gynecol 1994;170(6):1672–6.
26. Vintzileos AM, Campbell WA, Nochimson DJ, et al. Degree of oligohydramniosand pregnancy outcome in patients with premature rupture of the membranes.Obstet Gynecol 1985;66(2):162–7.
27. Vintzileos AM, Campbell WA, Nochimson DJ, et al. The fetal biophysical profile inpatients with premature rupture of the membranes—an early predictor of fetalinfection. Am J Obstet Gynecol 1985;152(5):510–6.
28. Vintzileos AM, Campbell WA, Nochimson DJ, et al. The use of the nonstress testin patients with premature rupture of the membranes. Am J Obstet Gynecol 1986;155(1):149–53.
29. Vintzileos AM, Campbell WA, Nochimson DJ, et al. Fetal breathing as a predictorof infection in premature rupture of the membranes. Obstet Gynecol 1986;67(6):813–7.
30. Vintzileos AM, Campbell WA, Nochimson DJ, et al. Fetal biophysical profileversus amniocentesis in predicting infection in preterm premature rupture ofthe membranes. Obstet Gynecol 1986;68(4):488–94.
31. Carroll SG, Papaioannou S, Nicolaides KH. Assessment of fetal activity and amni-otic fluid volume in the prediction of intrauterine infection in preterm prelabor am-niorrhexis. Am J Obstet Gynecol 1995;172(5):1427–35.
32. Ghidini A, Salafia CM, Kirn V, et al. Biophysical profile in predicting acuteascending infection in preterm rupture of membranes before 32 weeks. ObstetGynecol 2000;96(2):201–6.
Oyelese & Vintzileos64
33. Yucel N, Yucel O, Yekeler H. The relationship between umbilical artery Dopplerfindings, fetal biophysical score and placental inflammation in cases of prema-ture rupture of membranes. Acta Obstet Gynecol Scand 1997;76(6):532–5.
34. Gauthier DW, Meyer WJ, Bieniarz A. Biophysical profile as a predictor of amnioticfluid culture results. Obstet Gynecol 1992;80(1):102–5.
35. Roussis P, Rosemond RL, Glass C, et al. Preterm premature rupture ofmembranes: detection of infection. Am J Obstet Gynecol 1991;165(4 Pt 1):1099–104.
36. Miller JM Jr, Kho MS, Brown HL, et al. Clinical chorioamnionitis is not predicted byan ultrasonic biophysical profile in patients with premature rupture ofmembranes. Obstet Gynecol 1990;76(6):1051–4.
37. Vintzileos AM, Bors-Koefoed R, Pelegano JF, et al. The use of fetal biophysicalprofile improves pregnancy outcome in premature rupture of the membranes.Am J Obstet Gynecol 1987;157(2):236–40.
38. Manning FA, Bondaji N, Harman CR, et al. Fetal assessment based on fetalbiophysical profile scoring. VIII. The incidence of cerebral palsy in tested anduntested perinates. Am J Obstet Gynecol 1998;178(4):696–706.
39. Rotmensch S, Liberati M, Celentano C, et al. The effect of betamethasone on fetalbiophysical activities and Doppler velocimetry of umbilical and middle cerebralarteries. Acta Obstet Gynecol Scand 1999;78(9):768–73.
40. Jackson JR, Kleeman S, Doerzbacher M, et al. The effect of glucocorticosteroidadministration on fetal movements and biophysical profile scores in normal preg-nancies. J Matern Fetal Neonatal Med 2003;13(1):50–3.
41. Deren O, Karaer C, Onderoglu L, et al. The effect of steroids on the biophysicalprofile and Doppler indices of umbilical and middle cerebral arteries in healthypreterm fetuses. Eur J Obstet Gynecol Reprod Biol 2001;99(1):72–6.
42. Gray SE, Rodis JF, Lettieri L, et al. Effect of intravenous magnesium sulfate on thebiophysical profile of the healthy preterm fetus. Am J Obstet Gynecol 1994;170(4):1131–5.
43. Peaceman AM, Meyer BA, Thorp JA, et al. The effect of magnesium sulfate tocol-ysis on the fetal biophysical profile. Am J Obstet Gynecol 1989;161(3):771–4.
44. Carlan SJ, O’Brien WF. The effect of magnesium sulfate on the biophysical profileof normal term fetuses. Obstet Gynecol 1991;77(5):681–4.
45. Hallak M, Moise K Jr, Lira N, et al. The effect of tocolytic agents (indomethacinand terbutaline) on fetal breathing and body movements: a prospective, random-ized, double-blind, placebo-controlled clinical trial. Am J Obstet Gynecol 1992;167(4 Pt 1):1059–63.
46. Vintzileos AM, Campbell WA, Nochimson DJ, et al. The use and misuse of thefetal biophysical profile. Am J Obstet Gynecol 1987;156(3):527–33.
47. Manning FA, Morrison I, Harman CR, et al. The abnormal fetal biophysical profilescore. V. Predictive accuracy according to score composition. Am J ObstetGynecol 1990;162(4):918–24 [discussion: 924–7].