the vasoplegic syndrome following …©2017 mfmer | slide-1 the vasoplegic syndrome following...
TRANSCRIPT

©2017 MFMER | slide-1
The Vasoplegic Syndrome Following Cardiopulmonary Bypass
Patrick Wieruszewski, PharmD PGY2 Critical Care Resident
Pharmacy Grand Rounds December 12, 2017

©2017 MFMER | slide-2
Objectives
• Review the pathology and consequences of the cardiac vasoplegic syndrome
• Determine the role of salvage therapies for catecholamine-refractory cardiac vasoplegia
• Develop a treatment strategy for a vasoplegic patient following cardiopulmonary bypass
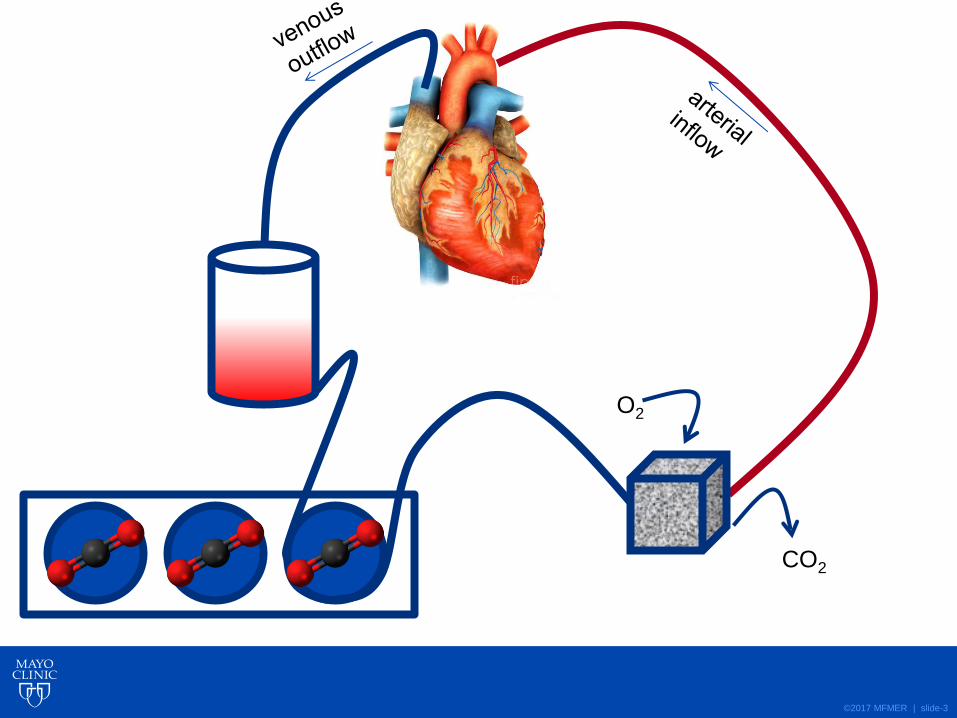
©2017 MFMER | slide-3
O2
CO2

©2017 MFMER | slide-4
↓SVR
↓BP
Protamine reversal
Exposure of blood to
CPB circuit
Blood transfusion
Complement
activation
CPB = cardiopulmonary bypass
SIRS = systemic inflammatory response syndrome
SVR = systemic vascular resistance
BP = blood pressure
Intraoperative
hypotension
↑ nitric oxide SIRS
+
↑ baroreceptor
stimulation
↑ nitric oxide
↓ vasopressin Aortic cross clamp
release
Reperfusion
syndrome
Smooth muscle
hyperpolarization
Omar et al. Am J Med Sci 2015;349:80-8.
Fischer et al. Semin Thoracic Surg 2010;22:140-4.

©2017 MFMER | slide-5
The Cardiac Vasoplegic Syndrome
• Incidence, ~5 to 45%
• Vasodilatory shock
• Good cardiac function
• Good circulatory volume
• Requires vasopressors
• Hypoperfusion
• Multi-organ failure
• Death
Omar et al. Am J Med Sci 2015;349:80-8.
Fischer et al. Semin Thoracic Surg 2010;22:140-4.

©2017 MFMER | slide-6
Cardiac Vasoplegia
Hypotension (↓↓ SVR)
High or normal cardiac output
Adequate fluid
resuscitation

©2017 MFMER | slide-7
Based on the physiologic changes during cardiopulmonary bypass, what would be your first line therapy for cardiac vasoplegia?
A. Catecholamines (i.e. norepinephrine)
B. Vasopressin
C. Methylene blue
D. Hydroxocobalamin (vitamin B12)
E. Ascorbic acid (vitamin C)
©2017 MFMER | slide-8
1st Line: Vasopressors
• Catecholamines
• Vasopressin
• Vasopressor-refractory
• Incidence unknown
• Consequences of high vasopressor rates
• Strong predictor of mortality
• Salvage therapies
• Methylene blue
• Hydroxocobalamin
• Ascorbic acid

©2017 MFMER | slide-9
↑SVR
↑BP
Protamine reversal
Exposure of blood to
CPB circuit
Blood transfusion
Complement
activation
Intraoperative
hypotension
↑ nitric oxide SIRS
+
↑ baroreceptor
stimulation
↑ nitric oxide
↓ vasopressin Aortic cross clamp
release
Reperfusion
syndrome
Smooth muscle
hyperpolarization
Methylene Blue
Booth et al. Heart Surg Forum 2017;20:E234-8.
©2017 MFMER | slide-10
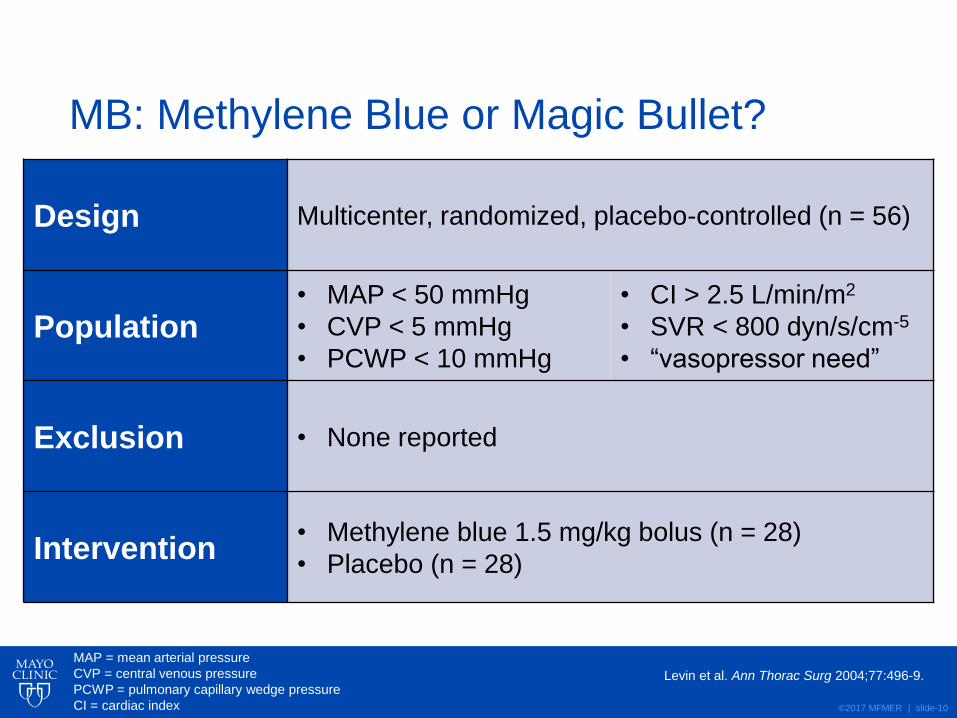
MB: Methylene Blue or Magic Bullet?
Design Multicenter, randomized, placebo-controlled (n = 56)
Population • MAP < 50 mmHg
• CVP < 5 mmHg
• PCWP < 10 mmHg
• CI > 2.5 L/min/m2
• SVR < 800 dyn/s/cm-5
• “vasopressor need”
Exclusion • None reported
Intervention • Methylene blue 1.5 mg/kg bolus (n = 28)
• Placebo (n = 28)
Levin et al. Ann Thorac Surg 2004;77:496-9.
MAP = mean arterial pressure
CVP = central venous pressure
PCWP = pulmonary capillary wedge pressure
CI = cardiac index
©2017 MFMER | slide-11
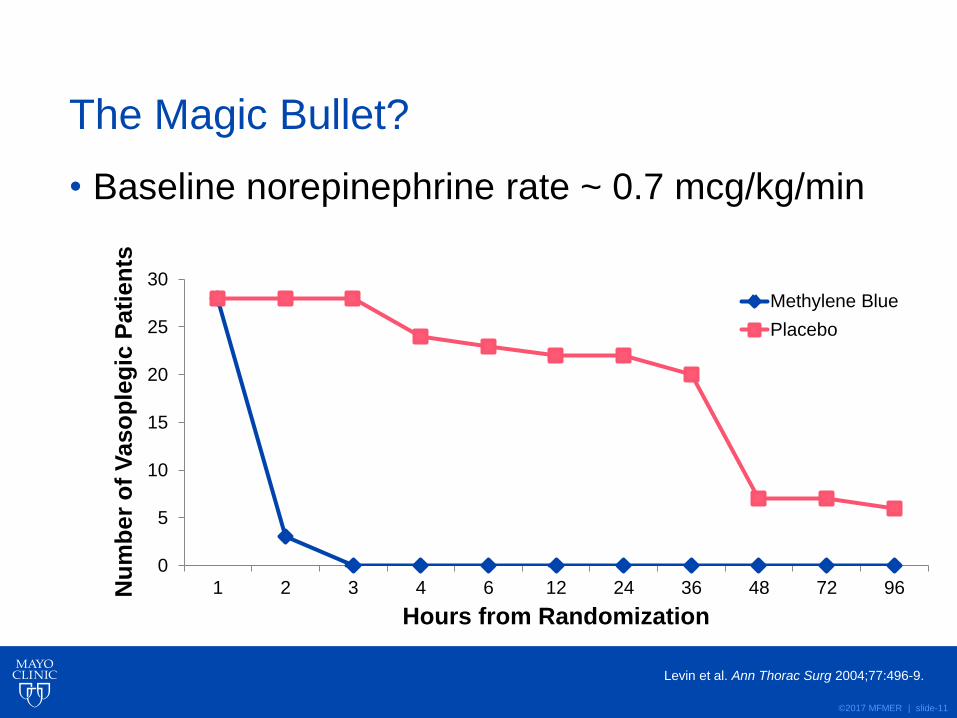
The Magic Bullet?
• Baseline norepinephrine rate ~ 0.7 mcg/kg/min
Levin et al. Ann Thorac Surg 2004;77:496-9.
0
5
10
15
20
25
30
1 2 3 4 6 12 24 36 48 72 96Nu
mb
er
of
Vaso
ple
gic
Pati
en
ts
Hours from Randomization
Methylene Blue
Placebo

©2017 MFMER | slide-12
Bolus Only
Leyh et al. J Thorac Cardiovasc Surg 2003;125:1426-31.
Mazzeffi et al. Ann Card Anaesth 2017;20:178-81.
• Retrospective cohort study (n = 54)
• Baseline norepinephrine ≥ 0.5 mcg/kg/min
• Bolus methylene blue 2 mg/kg
• ↓norepinephrine, ↑SVR at 1, 6, and 12 hours
• ↑ALT/AST
• In-hospital mortality, 6% (n = 3)
Leyh et al. 2003
• Retrospective cohort study (n = 88)
• Baseline N 12.5 mcg/min, V 0.09 units/min, E 7.4 mcg/min
• Bolus methylene blue 1-2 mg/kg
• ↓norepinephrine, ↑MAP
• ↑MAP, only variable associated with response
Mazzeffi et al. 2017
N = norepinephrine
E = epinephrine
V = vasopressin
ALT = alanine aminotransferase
AST = aspartate aminotransferase

©2017 MFMER | slide-13
Why Just One Dose?
• Retrospective cohort (n = 3608)
• Bolus 2 mg/kg then 0.5 mg/kg/h (n = 118)
Mehaffey et al. Ann Thorac Surg 2017;104:36-41.
0
1
2
3
4
5
6
7
8
9
10
4 8 12 16 20 24 28 32 36 40 44 48
Rate
(m
cg
/min
)
Hours from Administration
Norepinephrine
Epinephrine
58
60
62
64
66
68
70
72
74
4 8 12 16 20 24 28 32 36 40 44 48
MA
P (
mm
Hg
)
Hours from Administration

©2017 MFMER | slide-14
Have We Been Doing it Wrong?
Mehaffey et al. Ann Thorac Surg 2017;104:36-41.
Outcome OR (n = 48) ICU (n = 70) p-value
Adverse event 34 (71%) 53 (76%) 0.554
Transfusion 44 (92%) 58 (83%) 0.170
Length of stay (d) 12 (10, 19) 12 (6, 21) 0.447
Stroke 2 (4%) 4 (6%) 0.707
Renal failure 5 (10%) 20 (29%) 0.018
Reoperation 10 (21%) 21 (30%) 0.266
Sternal infection 1 (2%) 0 (0%) 0.219
Prolonged MV 11 (23%) 16 (23%) 0.994
30-day mortality 5 (10%) 20 (29%) 0.018

©2017 MFMER | slide-15
Limitations
• Low incidence of refractory vasoplegia
• No report of hemodynamic parameters
• Unknown amount of methylene blue received
• No description of vasopressor and hemodynamic behavior in early vs. late recipients
Mehaffey et al. Ann Thorac Surg 2017;104:36-41.

©2017 MFMER | slide-16
Methylene Blue
Fluid and tissue
discoloration
Hemolytic anemia
↓ Oximetry measurements
Serotonin Syndrome
Maximum dosage
Lavigne D. Semin Cardiothroac Vasc Anesth 2010;14:186-9.
Ramsay et al. Br J Pharmacol 2007;152:946-51.

©2017 MFMER | slide-17
↑SVR
↑BP
Protamine reversal
Exposure of blood to
CPB circuit
Blood transfusion
Complement
activation
Intraoperative
hypotension
↑ nitric oxide SIRS
+
↑ baroreceptor
stimulation
↑ nitric oxide
↓ vasopressin Aortic cross clamp
release
Reperfusion
syndrome
Smooth muscle
hyperpolarization
Hydroxocobalamin
Weinberg et al. Free Radic Biol Med 2009;46:1626-32.
©2017 MFMER | slide-18
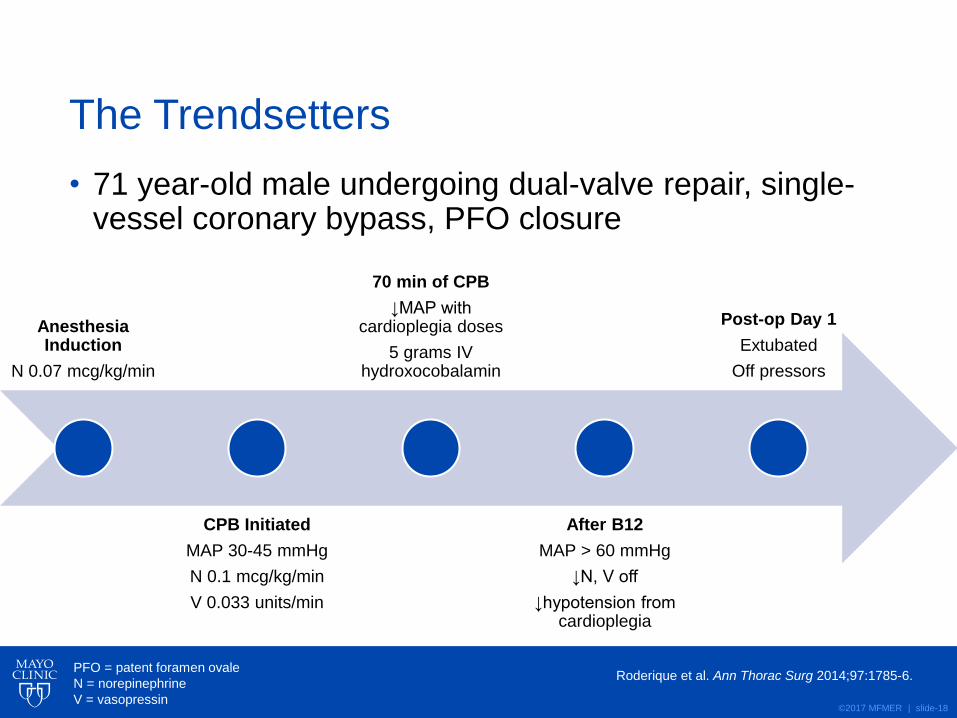
The Trendsetters
• 71 year-old male undergoing dual-valve repair, single-vessel coronary bypass, PFO closure
Roderique et al. Ann Thorac Surg 2014;97:1785-6.
Anesthesia Induction
N 0.07 mcg/kg/min
CPB Initiated
MAP 30-45 mmHg
N 0.1 mcg/kg/min
V 0.033 units/min
70 min of CPB
↓MAP with cardioplegia doses
5 grams IV hydroxocobalamin
After B12
MAP > 60 mmHg
↓N, V off
↓hypotension from cardioplegia
Post-op Day 1
Extubated
Off pressors
PFO = patent foramen ovale
N = norepinephrine
V = vasopressin

©2017 MFMER | slide-19
And The Followers…
Case
Surgery
Pressor
Requirements
Other
Interventions
Outcome
1 AVR, MVR N ?
V 0.1 units/min
MB 1 mg/kg + 0.5
mg/kg
Pressors weaned
POD 2,
extubated POD 3
2 LVAD
implantation
N 0.25 mcg/kg/min
V 0.04 units/min MB 1 mg/kg x 2
Pressors weaned on
ICU arrival
3 Aortic aneurysm
repair
N 0.45 mcg/kg/min
V 0.04 units/min
MB 0.375 mg/kg +
0.75 mg/kg
Discharged ICU on
POD 17
4 TVR, PFO
closure N 0.2 mcg/kg/min None
Discharged ICU on
POD 12
5 AVR, MVR, TVR
N 0.2 mcg/kg/min
E 0.1 mcg/kg/min
V 0.06 units/min
MB 3.3 mg/kg total
ECMO
Pressors weaned
POD 4
Burnes et al. J Cardiothorac Vasc Anesth 2017;31:1012-4.
Cai et al. Ann Card Anaesth 2017;20:462-4.
Zundel et al. J Cardiothorac Vasc Anesth 2017;Ahead of Print.
Cheungpasitporn et al. Clin Kidney J 2017;10:357-62.
AVR = aortic valve replacement
MVR = mitral valve replacement
TVR = tricuspid valve replacement
LVAD = left ventricular assist device
ECMO = extra corporeal membrane
oxygenation
©2017 MFMER | slide-20
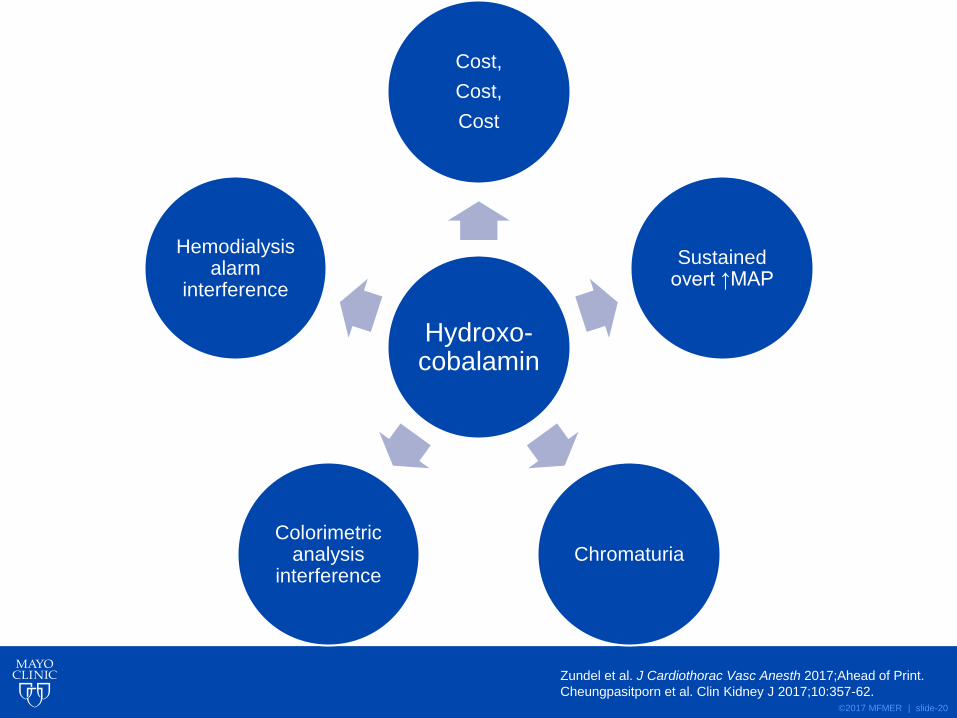
Hydroxo-cobalamin
Cost,
Cost,
Cost
Sustained overt ↑MAP
Chromaturia Colorimetric
analysis interference
Hemodialysis alarm
interference
Zundel et al. J Cardiothorac Vasc Anesth 2017;Ahead of Print.
Cheungpasitporn et al. Clin Kidney J 2017;10:357-62.

©2017 MFMER | slide-21
Making The Case: Ascorbic Acid
L-tyrosine L-DOPA Dopamine
Norepinephrine Epinephrine
Carr et al. Crit Care 2015;19:418.
Rodemeister et al. Nutrition 2014;30:673-8.
Berger et al. Curr Opin Clin Nutr Metab Care 2015;18:193-201.

©2017 MFMER | slide-22
Ascorbic Acid in Cardiac Surgery
Case
Age/
Sex
Surgery
CPB
time (m)
Pressors at Vitamin
C initiation
Shock co-therapies
1 22/
M
Septal
myectomy 55
N 0.1 mcg/kg/min
E 0.02 mcg/kg/min
V 0.04 units/min
None
2 18/
M
LVAD
exchange 85
N 0.12 mcg/kg/min
E 0.08 mcg/kg/min
V 0.04 units/min
Hydrocortisone
3 67/
M
AVR, MVR,
TVR 196
N 0.3 mcg/kg/min
E 0.08 mcg/kg/min
V 0.04 units/min
Hydrocortisone,
methylene blue, VA
ECMO
Wieruszewski et al. Unpublished data, under peer review.

©2017 MFMER | slide-23
0
0.1
0.2
0.3
0.4
0.5
0.6
0 12 24 36 48 60 72
Tota
l V
asopre
ssors
* Case 1
Case 2
Case 3
0
0.1
0.2
0.3
0.4
0 12 24 36 48 60 72
Nore
pin
ephrine
Time From Vitamin C Initiation (h)
Va
so
pre
ss
or
Re
qu
ire
me
nts
(m
cg
/kg
/min
)
*Norepinephrine equivalents
N 0.1 mcg/kg/min = E 0.1 mcg/kg/min = V 0.04 units/min
Wieruszewski et al. Unpublished data, under peer review.
©2017 MFMER | slide-24
Limitations to Current Vasoplegia Data
• Inconsistent definitions of vasoplegia including the “vasopressor-refractory” cases
• Heterogeneous outcome variables
• Ideal dosing schema not truly known
• No comparison of salvage therapies
• Salvage therapy vs. first line?
• Scant reporting of adverse events

©2017 MFMER | slide-25
In The Meantime…
• Standardized vasoplegia definition
• Particularly concerning need for vasopressors
• Proposal: vasopressin then when norepinephrine > 0.1 mcg/kg/min
• Consider methylene blue or ascorbic acid
• Hydroxocobalamin as last resort
• Consider methylene blue administration in the operating theatre when coming off pump

©2017 MFMER | slide-26
Who May Benefit From OR Administration
• Left ventricular assist device
• Heart failure, especially known reduced ejection fraction
• Multiple comorbidities (including pre-existing dialysis dependence)
• Previous sternotomy and bypass exposure
• Extended durations of CPB and aortic cross clamp timing
• Not isolated vessel bypass cases
©2017 MFMER | slide-27
Future Directions for Vasoplegia Research
• Identification of patients at highest risk of vasopressor-refractory vasoplegia
• Elucidation of optimal administration timing
• Perioperative or intensive care unit
• Taking advantage of all mechanisms of CPB resulting vasoplegia
• Identification of novel agents
©2017 MFMER | slide-28
The cardiopulmonary bypass circuit does which of the following?
A. Invokes a SIRS-like immune response
B. Results in vasopressin deficiency
C. Increases nitric oxide synthesis
D. All of the above

©2017 MFMER | slide-29
Ascorbic acid is proposed to
A. Inhibit nitric oxide synthesis
B. Increase endogenous catecholamine synthesis
C. Agonize the angiotensin-renin system
D. All of the above
©2017 MFMER | slide-30
Conclusion
• The cardiac vasoplegia syndrome is a significant contributor of morbidity and mortality in cardiac surgical patients
• Salvage therapies are necessary in some vasoplegia cases, though data supporting their use is sparse
• Future research should focus on optimal timing of initiation of salvage therapies

©2017 MFMER | slide-31
“The ultimate objective of my work in this field has been to be able to operate inside the heart
under direct vision.” John H. Gibbon, Jr., M.D., 1954

©2017 MFMER | slide-32
The Vasoplegic Syndrome Following Cardiopulmonary Bypass
Patrick Wieruszewski, PharmD [email protected]
Pharmacy Grand Rounds December 12, 2017

©2017 MFMER | slide-33
Procurement Costs
MAYO CLINIC CONFIDENTIAL DATA
Example Treatment Procurement Cost
Methylene blue 1 mg/kg, then 1mg/kg x
6h, 80kg patient ~$43
Hydroxocobalamin 5 grams once ~$770
Ascorbic acid 1.5 gm q6h x 4 days ~$82

©2017 MFMER | slide-34
Risk of Serotonin Toxicity
Citalopram Milnacipran Clomipramine Cocaine Ondansetron Fentanyl
Escitalopram Venlafaxine Desipramine Ecstasy Palonosetron Buspirone
Fluoxetine Bupropion Doxepin LSD Metoclopraminde Sumatriptan
Fuvoxamine Vilazodone Imipramine Tramadol Dexfenfluramine Rizatriptan
Paroxetine Trazodone Maprotiline Meperidine Carbamazepine Naratriptan
Sertraline Nefazodone Nortriptyline St. John’s Wort Sibutramine Almotriptan
Desvenlafaxine Amitriptyline Protriptyline Dolasetron Dextromethorphan Zolmitraptan
Duloxetine Amoxapine Trimipramine Granisetron Cyclobenzaprine Pentazocine
Procarbazine Fenfluramine Phentermine Valproate Dextroamphetamine Methamphetamine
Levodopa Cardidopa Lithium Phenelzine Tranylcypromine Isocarboxazid
Moclobemide Safinamide Selegiline Rasagiline Linezolid Tedizolid
©2017 MFMER | slide-35
VANCS Trial 2017
• Vasopressin 0.01 to 0.06 units/min vs. norepinephrine 10 to 60 mcg/min to maintain MAP ≥ 65 mmHg
• V ↓ primary endpoint (mortality + severe complications)
• Driven by renal failure (36% v. 10%, p <0.0001)
• V ↓ time on pressors, ICU, and hospital stay
• V ↓ atrial arrhythmias (82% v. 64%, p = 0.0004)
• No differences in adverse events
Hajjar et al. Anesthesiology 2017;126:85-93.