theprognosticimpactoftype2diabetesmellitusonearlycervical...
TRANSCRIPT

Gynecologic Oncology
The Prognostic Impact of Type 2 Diabetes Mellitus on Early Cervical
Cancer in AsiaHUNG-YANGKUOa ZHONG-ZHE LINbc RAYMONDKUOgWEN-YI SHAUh CHIU-LIN LAIg YEN-YUNYANGg YU-YUNSHAObe CHIUNHSUbe
WEN-FAN CHENGde ANN-LII CHENGbce JAMES CHIH-HSIN YANGbe MEI-SHU LAIfgiaDepartment of Internal Medicine National Taiwan University Hospital Hsin-Chu Branch Hsinchu Taiwan Republic of ChinaDepartments of bOncology cInternal Medicine and dObstetrics and Gynecology National Taiwan University Hospital Taipei TaiwanRepublicofChina eGraduate InstituteofOncologyCollegeofMedicine and fInstituteofEpidemiologyandPreventiveMedicineCollegeofPublic Health National Taiwan University Taipei Taiwan Republic of China gCenter for Comparative Effectiveness Research NationalCenterofExcellence forClinical Trial andResearchTaipeiTaiwanRepublicofChina hDivisionofHealthTechnologyAssessmentCenter forDrug Evaluation Taipei Taiwan Republic of China iTaiwan Cancer Registry Taipei Taiwan Republic of ChinaContributed equallyDisclosures of potential conflicts of interest may be found at the end of this article
Key Words Diabetes mellitus x Cervical cancer x Cancer registry x Cancer-specific survival x Prognosis
ABSTRACT
BackgroundMany studies have shown that type 2 diabetesmellitus (DM) increases the risk for several types of cancer butnot cervical cancer (CC) Although DM and insulin-like growthfactor 1 have preclinical and clinical implications for CC less isknown about the prognostic impact of DM on patients withearly stage CCPatients andMethodsWeusedthenationwideTaiwanCancerRegistry database to collect the characteristics of stage IndashIIAcervical cancer patients diagnosed between 2004 and 2008DM and other comorbidities were retrieved from the NationalHealth Insurance database Cervical cancer-specific survival(CSS) and overall survival (OS) times of patients according toDM statuswere estimated using the Kaplan-MeiermethodWeused a Cox proportional hazards model to calculate adjusted
hazardratios (HRs) fortheeffectsofDMandother risk factorsonmortalityResults A total of 2946 patients had primary stage IndashIIA CCand received curative treatments and 284 (96) hadDMThe5-year CSS and OS rates for patients with DM were significantlylower than thosewithoutDM(CSS 854vs 915OS 739vs 879) After adjusting for clinicopathologic variables andcomorbidities DM remained an independent unfavorableprognostic factor for CSS (adjusted HR 146) and OS (adjustedHR 155)Conclusion In Asian patients with early cervical cancer DMis an independent unfavorable prognostic factor influ-encing both OS and CSS even after curative treatmentsThe Oncologist 2015201051ndash1057
Implications for Practice Type 2 diabetesmellitus (DM) increases the incidence of several types of cancer but not cervical cancer(CC)however less isknownaboutthe impactofDMonpatientswhoalreadyhaveCCThis studysuggeststhatDMmay increase theriskof cancer recurrence anddeath forearly stageCCpatients evenafter curative treatments IncorporatingDMcontrol should beconsidered part of the continuum of care for early stage CC patients and close surveillance during routine follow-up in thispopulation is recommended
INTRODUCTION
Cervical cancer (CC) is a major health concern for women indeveloping countries and remains the fourth most commoncancer in women worldwide Although the incidence rate ofCC has decreased gradually 528000 new cases and 266000deaths were reported in 2012 with 85 of deaths occurring
in developing countries [1] Assisted by cytological and molec-ular screening increasing numbers of patients have beendiagnosed at an early stage Surgery and radiotherapy aretreatments of choice for early stage CC and provide high curerates however certain patients still die of disease recurrence
Correspondence James Chih-Hsin Yang MD PhD Graduate Institute of Oncology and Cancer Research Centre College ofMedicine NationalTaiwanUniversity 5FNo2XuzhouRoadZhongzhengDistrictTaipeiCity100TaiwanRepublicofChinaTelephone886-2-23123456ext67511E-Mail chihyangntuedutw orMei-Shu LaiMD PhD Institute of Epidemiology and PreventiveMedicine College of Public Health NationalTaiwan University Room 518 No 17 Xuzhou RoadTaipei City 100Taiwan Republic of ChinaTelephone 886-2-33668018 E-Mail mslaicphntuedutw Received March 18 2015 accepted for publication June 3 2015 published Online First on August 3 2015 copyAlphaMed Press1083-71592015$20000 httpdxdoiorg101634theoncologist2015-0111
TheOncologist 2015201051ndash1057 wwwTheOncologistcom copyAlphaMed Press 2015
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
Prognostic factors including pelvic lymph node metastasisstromal invasion lymphovascular space invasion and largetumor size affect the outcome of CC [2 3] The variability inrecurrence-free and overall survival (OS) among patients withsimilar clinical and pathological characteristics implies in-completeness among the current prognostic factors
In recentdecades numerous comprehensive cohort studiesand meta-analyses have reported the consistent associationbetweendiabetesmellitus (DM)andan increased riskof severaltypes of cancer including liver pancreas endometrium colonand breast cancer [4ndash7] The underlying mechanism affectingthe association between DM and cancer remains elusive andone of themost commonly adopted hypotheses involves insulin-like growth factor 1 (IGF-1) Hyperinsulinemia may increase theproduction of free IGF-1 which activates downstream pathwaysinvolved in proliferation invasion and metastasis after bindingto IGF-1 receptors (IGF-1Rs) [8 9]
Although researchers have reportedpreclinical and clinicalimplications of IGF-1 for early stage CC [10 11] studies havenot determined a significant correlation between the in-cidence of CC and DM [12 13] The impact of DM on OS andcancer-specific mortality of patients with early stage CC hasnever been addressed Based on a comprehensive literaturereview this population-based study is the first to investigatethe impact of DM on cancer-specific survival (CSS) in CC Weanalyzed patient information by using the Taiwan CancerRegistry (TCR) and National Health Insurance (NHI) databasesBoth databases included almost all patients covered by man-datory national health insurance in Taiwan hence this cohortstudy is highly representative
MATERIALS AND METHODS
Data SourcePatients with primary CCwhowere newly diagnosed between2004 and 2008 were selected from the TCR database for thisnationwide population-based cohort study The TCR database
was established and is maintained by the Health PromotionAdministration (HPA)Ministry ofHealth andWelfare in Taiwan[14 15]Major cancer care providers in Taiwanmust report thedataofnewlydiagnosedcancerpatientstotheTCRthustheTCRdatabase covers 976 of cancer patients in Taiwan [16] Thefollowing informationwasobtained for finalprognosticanalysispatient demographics clinicopathological status treatmentmodality and details regarding major treatment courses
Subsequently we linked the data to the Taiwan NHIdatabase to identify DM status and other comorbidities TheNHI program is a mandatory single-payer health insuranceprogram that coversmore than 99of the residents of Taiwan[17] This unified reimbursement system includes outpatientclinic and inpatient hospitalization services provided by boththeprivateandpublic sectorsAllmedical claimsaresubmittedand recorded electronically [18] For our study we linked thepatient records to the National Death Registry (NDR) toidentify mortality outcomes between 2004 and 2011
Identities of patients were encrypted and all data were an-alyzed anonymously to comply with personal electronic data pri-vacy regulationsThe studydatawere approved for release by thedata release review board of the HPA and the protocol was ap-proved by the research ethics committee of the College of PublicHealth National Taiwan University (protocol number 990205)
Study PopulationPatientsnewlydiagnosedwithCCbetween2004and2008wereidentified using the following inclusion criteria (a) an initialdiagnosisofCCasaprimarytumor (b)thepresenceofstage IndashIIAdisease according to the American Joint Cancer Committeeon Cancer system (sixth edition) [19] and InternationalFederation of Gynecology and Obstetrics staging system(1994) [20] and (c) age$40years Patientswith the followingcharacteristics were excluded (a) had other cancers in thepast (b) exhibited multiple primary cancers (c) exhibitedpathology other than squamous cell carcinoma or adenocar-cinoma (d) received treatment other than standard curativetreatment (surgery definitive radiotherapy and concurrentchemoradiation) such as neoadjuvant chemotherapy chemo-therapy alone or unknown therapy (missing data) and (e)exhibited a positive or unknown surgical margin
Study Variables and Endpoint DefinitionsTo determine whether the patients had DM we used theInternational Classification of Diseases Ninth Revision ClinicalModification (ICD-9-CM) codesderived fromtheNHI claimsdatato screen for comorbidities a revised version of the mappingalgorithm by Quan et al [21] was used All comorbidities in theDeyo-Charlson Comorbidity Index were examined [22] anddiagnosis codes from both the inpatient and outpatient clinicswere included A DM diagnosis was established only if it had beenreported more than two times in outpatient clinics in differentmonths or at least once during hospital admissionwithin 1 yearEach comorbidity was coded and analyzed as a dichotomizedvariable (ie yes or no) The following ICD-9-CM codes wereused type 2DM(ICD-9-CMcode 250x) congestive heart failure(ICD-9-CMcodes39891402014021140291404014040340411 40413 40491 40493 4254-4259 428x) cerebro-vascular disease (ICD-9-CM codes 36234 430x-438x) de-mentia (ICD-9-CM codes 290x 2941 3312) renal disease
Figure 1 Patient flow diagramAbbreviation DM diabetes mellitus
copyAlphaMed Press 2015TheOncologistreg
1052 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
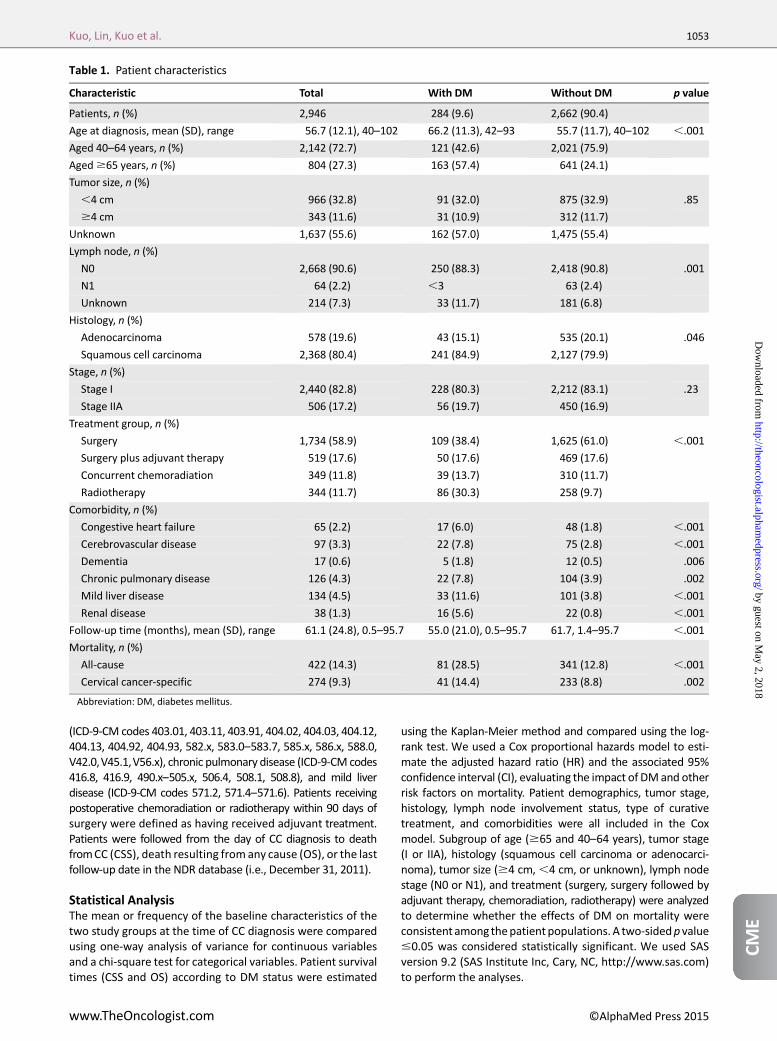
(ICD-9-CM codes 40301 40311 40391 40402 40403 4041240413 40492 40493 582x 5830ndash5837 585x 586x 5880V420V451V56x) chronic pulmonary disease (ICD-9-CM codes4168 4169 490xndash505x 5064 5081 5088) and mild liverdisease (ICD-9-CM codes 5712 5714ndash5716) Patients receivingpostoperative chemoradiation or radiotherapy within 90 days ofsurgery were defined as having received adjuvant treatmentPatients were followed from the day of CC diagnosis to deathfromCC (CSS) death resulting from any cause (OS) or the lastfollow-up date in the NDR database (ie December 31 2011)
Statistical AnalysisThe mean or frequency of the baseline characteristics of thetwo study groups at the time of CC diagnosis were comparedusing one-way analysis of variance for continuous variablesand a chi-square test for categorical variables Patient survivaltimes (CSS and OS) according to DM status were estimated
using the Kaplan-Meier method and compared using the log-rank test We used a Cox proportional hazards model to esti-mate the adjusted hazard ratio (HR) and the associated 95confidence interval (CI) evaluating the impact of DMand otherrisk factors on mortality Patient demographics tumor stagehistology lymph node involvement status type of curativetreatment and comorbidities were all included in the Coxmodel Subgroup of age ($65 and 40ndash64 years) tumor stage(I or IIA) histology (squamous cell carcinoma or adenocarci-noma) tumor size ($4 cm4 cm or unknown) lymph nodestage (N0 or N1) and treatment (surgery surgery followed byadjuvant therapy chemoradiation radiotherapy) were analyzedto determine whether the effects of DM on mortality wereconsistent among thepatient populations A two-sidedp value005 was considered statistically significant We used SASversion 92 (SAS Institute Inc Cary NC httpwwwsascom)to perform the analyses
Table 1 Patient characteristics
Characteristic Total With DM Without DM p value
Patients n () 2946 284 (96) 2662 (904)
Age at diagnosis mean (SD) range 567 (121) 40ndash102 662 (113) 42ndash93 557 (117) 40ndash102 001
Aged 40ndash64 years n () 2142 (727) 121 (426) 2021 (759)
Aged$65 years n () 804 (273) 163 (574) 641 (241)
Tumor size n ()
4 cm 966 (328) 91 (320) 875 (329) 85
$4 cm 343 (116) 31 (109) 312 (117)
Unknown 1637 (556) 162 (570) 1475 (554)
Lymph node n ()
N0 2668 (906) 250 (883) 2418 (908) 001
N1 64 (22) 3 63 (24)
Unknown 214 (73) 33 (117) 181 (68)
Histology n ()
Adenocarcinoma 578 (196) 43 (151) 535 (201) 046
Squamous cell carcinoma 2368 (804) 241 (849) 2127 (799)
Stage n ()
Stage I 2440 (828) 228 (803) 2212 (831) 23
Stage IIA 506 (172) 56 (197) 450 (169)
Treatment group n ()
Surgery 1734 (589) 109 (384) 1625 (610) 001
Surgery plus adjuvant therapy 519 (176) 50 (176) 469 (176)
Concurrent chemoradiation 349 (118) 39 (137) 310 (117)
Radiotherapy 344 (117) 86 (303) 258 (97)
Comorbidity n ()
Congestive heart failure 65 (22) 17 (60) 48 (18) 001
Cerebrovascular disease 97 (33) 22 (78) 75 (28) 001
Dementia 17 (06) 5 (18) 12 (05) 006
Chronic pulmonary disease 126 (43) 22 (78) 104 (39) 002
Mild liver disease 134 (45) 33 (116) 101 (38) 001
Renal disease 38 (13) 16 (56) 22 (08) 001
Follow-up time (months) mean (SD) range 611 (248) 05ndash957 550 (210) 05ndash957 617 14ndash957 001
Mortality n ()
All-cause 422 (143) 81 (285) 341 (128) 001
Cervical cancer-specific 274 (93) 41 (144) 233 (88) 002
Abbreviation DM diabetes mellitus
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1053
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
RESULTS
Patient CharacteristicsThe TCR registered 21352 patients with newly diagnosed CCbetween2004and2008 In total 2946patientswith stage IndashIIAprimary CC underwent curative treatment and satisfied theeligibility criteria of this study (Fig 1) A total of 284 patients(96) had DM and they were older compared with patientswithout DM (mean age 662 vs 557 years p 001)Patients with DM were more likely to have squamous cellcarcinoma (p5 046) (Table 1) unknownnodal stage (p5 001)and other comorbidities (congestive heart failure cerebro-vascular disease dementia chronic pulmonary disease mildliver disease and renal disease) DMpatients were alsomorelikely to receive definitive radiotherapy instead of curativesurgery (p 001) Tumor sizes and stages differed non-significantly between the two study groups
Survival AnalysisDuring the follow-up period (mean 611 months) 81 patients(285) in the DM group and 41 (144) in the non-DM groupdied Patients in theDMgroupexhibited shorterOS times thandid patients without DM and the difference was significant(p 0001) (Fig 2A)TheOSrates forpatientswithandwithoutDMwere 856 and 948 respectively at 2 years and 739and 879 respectively at 5 years Patients in the DM groupalso exhibited significantly shorter CSS times than did those inthenon-DMgroup(p5 0003) (Fig2B)TheCSSratesforpatientswith and without DM were 909 and 959 respectively at2 years and 854 and 915 respectively at 5 years
Afteradjustment forage tumorsize andstage nodal stagehistologymodalities ofcurative treatment andcomorbiditiesDM remained an independent predictor of a lower CSSprobability (adjusted HR 146 95 CI 103ndash208 p 5 032)(Table 2) and OS probability (adjusted HR 155 95 CI121ndash200 p5 0007) (Table 2)
Subgroup analyses demonstrated the consistent prognosticinfluence of DM among the various subgroups including agetumor size and stage node stages histology modalities ofcurative treatment and comorbidities No strong heteroge-neity between the HRs of the subgroups was foundThe rangesof the adjusted HRs were 089ndash314 for CC-specific mortalityand113ndash297 foroverallmortalityamongthesubgroups (Fig3)
DISCUSSION
In this comprehensive population-based study we demon-strated thatDMwasan independentadverseprognostic factorfor patients in Taiwan who received curative treatment forearly stage CC The prognostic impact of DM was significantaccording to multivariate analysis and it remained consistentamong various subgroups differentiated by age stage tumorsize histology and treatment modality Patients with DMexhibited significantly shorter CSS times than did thosewithout DM (p5 0003 CSS rates 854 vs 915 at 5 years)and DM remained an independent predictor of lower CSSprobability (adjusted HR 146 95 CI 103ndash208 p 5 032)according to multivariate analysis
Previous studies have reported DM as a poor prognosticfactor of early stage liver and breast cancers [23 24] because it
increases cancer-specific mortality Our study reveals a similarresult in early CC One of the common characteristics of thesecancers is a high level of IGF-1R overexpression [25ndash27] Theassociation between the IGF-1 level and CC has been reported[28] andhigh-gradeexpressionof IGF-1Rcanbeusedtopredictthe high risk of death and disease recurrence in early CC [29]Hyperglycemia and hyperinsulinemia in patients with DMmay reduce the hepatic production of IGF binding protein1 and increase the free IGF-1 level [30 31] An increasedIGF-1 level in DM patients and overexpression of IGF-1R inCC cells activates the IGF axis and possibly results in poorprognosis
Thesubgroupanalyses (Fig 3)demonstrated that the impactof DMwas consistent for OS and CSS among all subgroups Thenegative impact ofDMwasmore prominent in adenocarcinomacompared with squamous cell carcinoma Nearly all cancers(pancreas endometrium liver colon andbreast)with a positiveassociation with DM are adenocarcinoma in pathology Thedifferenceofthe IGF-1andIGF-1Raxisbetweenadenocarcinomaandsquamouscell carcinoma remainsunclear andmore studiesarewarranted to clarify the systemrsquos role in themetastasis of CCparticularly adenocarcinoma
Treatment modalities other than surgery alone were asso-ciated with less favorable OS and CSS Patients for whom sur-gery is contraindicated might exhibit unfavorable risk factorssuch as poor performance or inadequate control of DM which
Figure 2 Survival of stage IndashIIA cervical cancer patients bydiabetes mellitus diagnosis status (A) Overall survival (B)Cervical cancer-specific survival
Abbreviation DM diabetes mellitus
copyAlphaMed Press 2015TheOncologistreg
1054 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
could imply unfavorable prognosis A large retrospective studyperformed byMD Anderson Cancer Center revealed that obesecervical cancer patients were more likely to be treated withprimary radiotherapy rather than surgery and had poorersurvival comparedwithhealthy-weightpatients [32]They foundthat obesity is also an independent poor prognostic factorfor cervical cancer patients DM patients also tend to haveobesity and that potentially leads to inadequate treatmentdosein several respects that could impair outcomes Inaccuracy inradiation dose calculationmdashespecially for lateral or obliquetreatment fields [33] inadequate pelvis penetration even byhigh-energy radiation beams and deviation in daily setupdue to skin folds [34]mdashcontributes to difficulties in deliveringradiotherapy to obese patients In addition up to 40 ofobese patients still receive smaller doses of chemotherapythan expected by their actual body weight although interna-tional guidelines suggest giving full-weight-based cytotoxicchemotherapy doses for obese patients [35] Without surgerysubclinical metastatic lymph nodes could impair survival in
patients who receive underdosing of radiotherapy and che-motherapy Although we do not have body mass index datain this study because of limitations in our database morbidobesity is lesscommonlyseeninAsianpopulationsandmayplaya minor role in this study In addition only patients exhibitingunfavorable pathological factors receive adjuvant treatmenttherefore they have a higher risk of disease recurrenceand death
For this nationwide population-based study we used datafrom the Taiwan NHI database thereby reducing the patientselection bias commonly found in institute-based studieshowever the study was retrospective and several limitationswere present First nonsurgical patients were not issuedpathological reports documenting tumor size therefore inac-curacy in or lack of records of the clinical tumor size resulted inunknown tumor sizes Except for the unknown parts of thedata distribution of tumor size was similar between the twogroups Second we could not analyze several aforementionedcrucial prognostic factors that may affect the choice of
Table 2 Cox regression model for stage IndashIIA
Variable
Overall mortality Cancer-specific mortality
Adjusted HR (95 CI) p value Adjusted HR (95 CI) p value
DM
No Ref Ref
Yes 155 (121ndash200) 0007 146 (103ndash208) 0320
Age 104 (103ndash105) 0001 102 (101ndash103) 0005
Tumor size
4 cm Ref Ref
$4 cm 140 (106ndash186) 0183 159 (114ndash223) 0066
Unknown 085 (068ndash106) 1459 085 (064ndash112) 2500
Lymph node
N0 Ref Ref
N1 471 (311ndash713) 0001 497 (315ndash784) 0001
Unknown 099 (073ndash133) 9328 100 (067ndash149) 9939
Histology
Squamous cell carcinoma Ref Ref
Adenocarcinoma 177 (138ndash227) 0001 212 (158ndash283) 0001
Stage
Stage I Ref
Stage IIA 149 (120ndash185) 0001 175 (134ndash229) 0001
Treatment
Surgery Ref Ref
Surgery plus adjuvant therapy 175 (131ndash234) 0002 190 (135ndash266) 0002
Concurrent chemoradiation 216 (158ndash296) 0001 237 (162ndash347) 0001
Radiotherapy 252 (184ndash346) 0001 230 (152ndash347) 0001
Comorbidity
Congestive heart failure 130 (080ndash211) 2843 132 (067ndash262) 4281
Cerebrovascular disease 118 (079ndash176) 4154 134 (078ndash229) 2901
Dementia 168 (087ndash325) 1247 077 (019ndash319) 7218
Chronic pulmonary disease 116 (079ndash169) 4463 126 (077ndash206) 3592
Mild liver disease 138 (096ndash199) 0817 097 (056ndash168) 9145
Renal disease 188 (108ndash327) 0248 068 (022ndash215) 5103
Abbreviations CI confidence interval DM diabetes mellitus HR hazard ratio Ref reference
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1055
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
curative treatment modality Although there are many limi-tations DM remained an independent prognostic factorfor OS and CSS after adjusting confounding factors bymultivariate analysis
InconclusionwedemonstratedthatearlystageCCpatientswith DM exhibited less favorable OS and CSS after curativetreatment The prognostic impact of DM remained significantafter adjustment for patient demographics and other comor-bidities We should continue to search for more accurateprognostic factors and to determine which would justify morefrequent surveillance in high-risk groups for early detection ofcurable disease recurrence To confirm the role of the IGF axisfor cancer survival in humans more clinical trials of IGF-targeted agents for CC patientsmdashparticularly thosewith DMoradenocarcinomamdashare required
ACKNOWLEDGMENTS
We thank the Collaboration Center of Health InformationApplication (CCHIA) Department of Health Executive Yuan
Taiwan for providing the databaseThis studywas supported bythe Bureau of National Health Insurance Department of HealthTaiwan (DOH96-NH-1003) and the Science and TechnologyUnit Department of Health Taiwan (DOH99-TD-B-111ndash001DOH100-TD-B-111ndash001)
AUTHOR CONTRIBUTIONSConceptionDesign Hung-Yang Kuo Zhong-Zhe Lin Yu-Yun Shao Chiun HsuAnn-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
Provision of study material or patients Raymond KuoWen-Yi Shau Chiu-LinLai Yen-Yun Yang
Collection andor assembly of data Raymond KuoWen-Yi Shau Chiu-Lin LaiYen-Yun Yang
Data analysis and interpretation Hung-Yang Kuo Zhong-Zhe Lin RaymondKuo Chiu-Lin Lai Yen-Yun Yang
Manuscript writing Hung-Yang Kuo Zhong-Zhe LinFinal approval of manuscript Hung-Yang Kuo Zhong-Zhe Lin Raymond KuoWen-Yi Shau Chiu-Lin Lai Yen-Yun Yang Yu-Yun Shao Chiun HsuWen-FanCheng Ann-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
DISCLOSURES
The authors indicated no financial relationships
REFERENCES
1 Cervical cancer Estimated incidence mortalityand prevalence worldwide in 2012 Available athttpglobocaniarcfrPagesfact_sheets_canceraspxcancer5cervix Accessed March 10 2015
2 Peters WA III Liu PY Barrett RJ II et al
Concurrent chemotherapy and pelvic radiation
therapy compared with pelvic radiation therapy
alone as adjuvant therapy after radical surgery in
high-riskearly-stagecancerof thecervix JClinOncol
2000181606ndash1613
3 Rotman M Sedlis A Piedmonte MR et al A
phase III randomized trial of postoperative pelvic
irradiation in stage IB cervical carcinoma with poor
prognostic features Follow-up of a gynecologic
oncology group study Int J Radiat Oncol Biol Phys200665169ndash176
4Vigneri P Frasca F Sciacca L et al Diabetes andcancer Endocr Relat Cancer 2009161103ndash1123
5Yood MU Oliveria SA Campbell UB et alIncidence of cancer in a population-based cohortofpatientswith type2diabetesDiabMet SyndrClinRes Rev 2009312ndash16
6 Inoue M Iwasaki M Otani T et al Diabetesmellitus and the risk of cancer Results from a large-scale population-based cohort study in Japan ArchIntern Med 20061661871ndash1877
7 Atchison EA Gridley G Carreon JD et al Risk ofcancer in a large cohort of US veterans withdiabetes Int J Cancer 2011128635ndash643
8Weinstein D Simon M Yehezkel E et alInsulin analogues display IGF-I-like mito-genic and anti-apoptotic activities in culturedcancer cells Diabetes Metab Res Rev 20092541ndash49
9 Law JH Habibi G Hu K et al Phosphorylatedinsulin-like growth factor-iinsulin receptor ispresent in all breast cancer subtypes and isrelated to poor survival Cancer Res 20086810238ndash10246
10 Shen MR Hsu YM Hsu KF et al Insulin-likegrowth factor 1 is a potent stimulator of cervicalcancer cell invasiveness and proliferation that ismodulated by alphavbeta3 integrin signaling Car-cinogenesis 200627962ndash971
Figure 3 Subgroup analysis of adjusted hazard ratios of mortality for patients with and without diabetes mellitus using the Coxproportional hazards model
Abbreviations CCRT chemoradiotherapy CI confidence interval DM diabetes mellitus HR hazard ratio OP surgery RT radiotherapy
copyAlphaMed Press 2015TheOncologistreg
1056 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
11 Huang YF Shen MR Hsu KF et al Clinicalimplications of insulin-like growth factor 1 system inearly-stage cervical cancer Br J Cancer 2008991096ndash1102
12Wideroff L Gridley G Mellemkjaer L et alCancer incidence in a population-based cohort ofpatients hospitalized with diabetes mellitus inDenmark J Natl Cancer Inst 1997891360ndash1365
13 OrsquoMara BA Byers T Schoenfeld E Diabetesmellitus and cancer risk A multisite case-controlstudy J Chronic Dis 198538435ndash441
14 ChiangCJChenYCChenCJetalCancer trendsin Taiwan Jpn J Clin Oncol 201040897ndash904
15Taiwan Cancer Registry Available at httptcrcphntuedutwmainphpPage5N2 AccessedMarch 10 2015
16Taiwan Cancer Registry annual report2011 [in Chinese] Available at httpwwwhpagovtwBHPNetWebStatStatisticsShowaspxNo5201404160001 Accessed March 10 2015
17 Statistics and surveys Available at httpwwwnhigovtwEnglishwebdatawebdataaspmenu511ampmenu_id5296ampwebdata_id51942ampWD_ID5296 Accessed March 10 2015
18 Introduction to the National Health InsuranceResearch Database (NHIRD) Taiwan Available athttpw3nhriorgtwnhirddate_01html AccessedMatch 10 2015
19 Greene FL Page DL Fleming ID et al AJCCCancer Staging Handbook 6th edNew York NYSpringer 2002
20 Quinn MA Benedet JL Odicino F et al Carci-nomaof the cervixuteri FIGO26thAnnual Report on
the Results of Treatment in Gynecological CancerInt J Gynaecol Obstet 200695(suppl 1)S43ndashS103
21 Quan H Sundararajan V Halfon P et al Codingalgorithms for defining comorbidities in ICD-9-CMand ICD-10 administrative data Med Care 2005431130ndash1139
22 DeyoRA CherkinDC CiolMAAdaptinga clinicalcomorbidity index for use with ICD-9-CM administra-tive databases J Clin Epidemiol 199245613ndash619
23 ShauWYShaoYYYehYCetalDiabetesmellitusis associated with increased mortality in patientsreceiving curative therapy for hepatocellular carci-noma The Oncologist 201217856ndash862
24 Chen WW Shao YY Shau WY et al The impactof diabetes mellitus on prognosis of early breastcancer in Asia The Oncologist 201217485ndash491
25 Desbois-Mouthon C Baron A Blivet-VanEggelpoel MJ et al Insulin-like growth factor-1receptor inhibition induces a resistancemechanismvia theepidermalgrowth factor receptorHER3AKTsignaling pathway Rational basis for cotargetinginsulin-like growth factor-1 receptor and epidermalgrowth factor receptor in hepatocellular carcinomaClin Cancer Res 2009155445ndash5456
26 Steller MA Delgado CH Bartels CJ et al Over-expression of the insulin-like growth factor-1 recep-tor and autocrine stimulation in human cervicalcancer cells Cancer Res 1996561761ndash1765
27 Shimizu C Hasegawa TTani Y et al Expressionof insulin-like growth factor 1 receptor in primarybreast cancer Immunohistochemical analysis HumPathol 2004351537ndash1542
28 Lee SW Lee SY Lee SR et al Plasma levels ofinsulin-like growth factor-1 and insulin-like growth
factor binding protein-3 in women with cervicalneoplasia J Gynecol Oncol 201021174ndash180
29 Luo M Shen D Zhou X et al MicroRNA-497 isa potential prognostic marker in human cervicalcancer and functions as a tumor suppressor bytargeting the insulin-like growth factor 1 receptorSurgery 2013153836ndash847
30 Ooi GT Tseng LY Tran MQ et al Insulin rapidlydecreases insulin-like growth factor-binding protein-1gene transcription in streptozotocin-diabetic rats MolEndocrinol 199262219ndash2228
31 Powell DR Suwanichkul A Cubbage ML et alInsulin inhibits transcription of the human gene forinsulin-like growth factor-binding protein-1 J BiolChem 199126618868ndash18876
32 Frumovitz M Jhingran A Soliman PT et alMorbid obesity as an independent risk factor fordisease-specific mortality in women with cervicalcancer Obstet Gynecol 20141241098ndash1104
33 Fisher CM Fortenberry BR Jhingran A et alNovel technique for simulation and external beamtreatment planning for obese patients Pract RadiatOncol 20111152ndash155
34Wong JR Gao Z Merrick S et al Potential forhigher treatment failure in obese patients Correla-tionofelevatedbodymass indexand increaseddailyprostate deviations from the radiation beam iso-centers in an analysis of 1465 computed tomographicimages Int J Radiat Oncol Biol Phys 20097549ndash55
35 Griggs JJ Mangu PB Anderson H et alAppropriate chemotherapy dosing for obese adultpatients with cancer American Society of ClinicalOncology clinical practice guideline J Clin Oncol2012301553ndash1561
CME This article is available for continuing medical education credit at CMETheOncologistcom
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1057
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from

Prognostic factors including pelvic lymph node metastasisstromal invasion lymphovascular space invasion and largetumor size affect the outcome of CC [2 3] The variability inrecurrence-free and overall survival (OS) among patients withsimilar clinical and pathological characteristics implies in-completeness among the current prognostic factors
In recentdecades numerous comprehensive cohort studiesand meta-analyses have reported the consistent associationbetweendiabetesmellitus (DM)andan increased riskof severaltypes of cancer including liver pancreas endometrium colonand breast cancer [4ndash7] The underlying mechanism affectingthe association between DM and cancer remains elusive andone of themost commonly adopted hypotheses involves insulin-like growth factor 1 (IGF-1) Hyperinsulinemia may increase theproduction of free IGF-1 which activates downstream pathwaysinvolved in proliferation invasion and metastasis after bindingto IGF-1 receptors (IGF-1Rs) [8 9]
Although researchers have reportedpreclinical and clinicalimplications of IGF-1 for early stage CC [10 11] studies havenot determined a significant correlation between the in-cidence of CC and DM [12 13] The impact of DM on OS andcancer-specific mortality of patients with early stage CC hasnever been addressed Based on a comprehensive literaturereview this population-based study is the first to investigatethe impact of DM on cancer-specific survival (CSS) in CC Weanalyzed patient information by using the Taiwan CancerRegistry (TCR) and National Health Insurance (NHI) databasesBoth databases included almost all patients covered by man-datory national health insurance in Taiwan hence this cohortstudy is highly representative
MATERIALS AND METHODS
Data SourcePatients with primary CCwhowere newly diagnosed between2004 and 2008 were selected from the TCR database for thisnationwide population-based cohort study The TCR database
was established and is maintained by the Health PromotionAdministration (HPA)Ministry ofHealth andWelfare in Taiwan[14 15]Major cancer care providers in Taiwanmust report thedataofnewlydiagnosedcancerpatientstotheTCRthustheTCRdatabase covers 976 of cancer patients in Taiwan [16] Thefollowing informationwasobtained for finalprognosticanalysispatient demographics clinicopathological status treatmentmodality and details regarding major treatment courses
Subsequently we linked the data to the Taiwan NHIdatabase to identify DM status and other comorbidities TheNHI program is a mandatory single-payer health insuranceprogram that coversmore than 99of the residents of Taiwan[17] This unified reimbursement system includes outpatientclinic and inpatient hospitalization services provided by boththeprivateandpublic sectorsAllmedical claimsaresubmittedand recorded electronically [18] For our study we linked thepatient records to the National Death Registry (NDR) toidentify mortality outcomes between 2004 and 2011
Identities of patients were encrypted and all data were an-alyzed anonymously to comply with personal electronic data pri-vacy regulationsThe studydatawere approved for release by thedata release review board of the HPA and the protocol was ap-proved by the research ethics committee of the College of PublicHealth National Taiwan University (protocol number 990205)
Study PopulationPatientsnewlydiagnosedwithCCbetween2004and2008wereidentified using the following inclusion criteria (a) an initialdiagnosisofCCasaprimarytumor (b)thepresenceofstage IndashIIAdisease according to the American Joint Cancer Committeeon Cancer system (sixth edition) [19] and InternationalFederation of Gynecology and Obstetrics staging system(1994) [20] and (c) age$40years Patientswith the followingcharacteristics were excluded (a) had other cancers in thepast (b) exhibited multiple primary cancers (c) exhibitedpathology other than squamous cell carcinoma or adenocar-cinoma (d) received treatment other than standard curativetreatment (surgery definitive radiotherapy and concurrentchemoradiation) such as neoadjuvant chemotherapy chemo-therapy alone or unknown therapy (missing data) and (e)exhibited a positive or unknown surgical margin
Study Variables and Endpoint DefinitionsTo determine whether the patients had DM we used theInternational Classification of Diseases Ninth Revision ClinicalModification (ICD-9-CM) codesderived fromtheNHI claimsdatato screen for comorbidities a revised version of the mappingalgorithm by Quan et al [21] was used All comorbidities in theDeyo-Charlson Comorbidity Index were examined [22] anddiagnosis codes from both the inpatient and outpatient clinicswere included A DM diagnosis was established only if it had beenreported more than two times in outpatient clinics in differentmonths or at least once during hospital admissionwithin 1 yearEach comorbidity was coded and analyzed as a dichotomizedvariable (ie yes or no) The following ICD-9-CM codes wereused type 2DM(ICD-9-CMcode 250x) congestive heart failure(ICD-9-CMcodes39891402014021140291404014040340411 40413 40491 40493 4254-4259 428x) cerebro-vascular disease (ICD-9-CM codes 36234 430x-438x) de-mentia (ICD-9-CM codes 290x 2941 3312) renal disease
Figure 1 Patient flow diagramAbbreviation DM diabetes mellitus
copyAlphaMed Press 2015TheOncologistreg
1052 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
(ICD-9-CM codes 40301 40311 40391 40402 40403 4041240413 40492 40493 582x 5830ndash5837 585x 586x 5880V420V451V56x) chronic pulmonary disease (ICD-9-CM codes4168 4169 490xndash505x 5064 5081 5088) and mild liverdisease (ICD-9-CM codes 5712 5714ndash5716) Patients receivingpostoperative chemoradiation or radiotherapy within 90 days ofsurgery were defined as having received adjuvant treatmentPatients were followed from the day of CC diagnosis to deathfromCC (CSS) death resulting from any cause (OS) or the lastfollow-up date in the NDR database (ie December 31 2011)
Statistical AnalysisThe mean or frequency of the baseline characteristics of thetwo study groups at the time of CC diagnosis were comparedusing one-way analysis of variance for continuous variablesand a chi-square test for categorical variables Patient survivaltimes (CSS and OS) according to DM status were estimated
using the Kaplan-Meier method and compared using the log-rank test We used a Cox proportional hazards model to esti-mate the adjusted hazard ratio (HR) and the associated 95confidence interval (CI) evaluating the impact of DMand otherrisk factors on mortality Patient demographics tumor stagehistology lymph node involvement status type of curativetreatment and comorbidities were all included in the Coxmodel Subgroup of age ($65 and 40ndash64 years) tumor stage(I or IIA) histology (squamous cell carcinoma or adenocarci-noma) tumor size ($4 cm4 cm or unknown) lymph nodestage (N0 or N1) and treatment (surgery surgery followed byadjuvant therapy chemoradiation radiotherapy) were analyzedto determine whether the effects of DM on mortality wereconsistent among thepatient populations A two-sidedp value005 was considered statistically significant We used SASversion 92 (SAS Institute Inc Cary NC httpwwwsascom)to perform the analyses
Table 1 Patient characteristics
Characteristic Total With DM Without DM p value
Patients n () 2946 284 (96) 2662 (904)
Age at diagnosis mean (SD) range 567 (121) 40ndash102 662 (113) 42ndash93 557 (117) 40ndash102 001
Aged 40ndash64 years n () 2142 (727) 121 (426) 2021 (759)
Aged$65 years n () 804 (273) 163 (574) 641 (241)
Tumor size n ()
4 cm 966 (328) 91 (320) 875 (329) 85
$4 cm 343 (116) 31 (109) 312 (117)
Unknown 1637 (556) 162 (570) 1475 (554)
Lymph node n ()
N0 2668 (906) 250 (883) 2418 (908) 001
N1 64 (22) 3 63 (24)
Unknown 214 (73) 33 (117) 181 (68)
Histology n ()
Adenocarcinoma 578 (196) 43 (151) 535 (201) 046
Squamous cell carcinoma 2368 (804) 241 (849) 2127 (799)
Stage n ()
Stage I 2440 (828) 228 (803) 2212 (831) 23
Stage IIA 506 (172) 56 (197) 450 (169)
Treatment group n ()
Surgery 1734 (589) 109 (384) 1625 (610) 001
Surgery plus adjuvant therapy 519 (176) 50 (176) 469 (176)
Concurrent chemoradiation 349 (118) 39 (137) 310 (117)
Radiotherapy 344 (117) 86 (303) 258 (97)
Comorbidity n ()
Congestive heart failure 65 (22) 17 (60) 48 (18) 001
Cerebrovascular disease 97 (33) 22 (78) 75 (28) 001
Dementia 17 (06) 5 (18) 12 (05) 006
Chronic pulmonary disease 126 (43) 22 (78) 104 (39) 002
Mild liver disease 134 (45) 33 (116) 101 (38) 001
Renal disease 38 (13) 16 (56) 22 (08) 001
Follow-up time (months) mean (SD) range 611 (248) 05ndash957 550 (210) 05ndash957 617 14ndash957 001
Mortality n ()
All-cause 422 (143) 81 (285) 341 (128) 001
Cervical cancer-specific 274 (93) 41 (144) 233 (88) 002
Abbreviation DM diabetes mellitus
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1053
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
RESULTS
Patient CharacteristicsThe TCR registered 21352 patients with newly diagnosed CCbetween2004and2008 In total 2946patientswith stage IndashIIAprimary CC underwent curative treatment and satisfied theeligibility criteria of this study (Fig 1) A total of 284 patients(96) had DM and they were older compared with patientswithout DM (mean age 662 vs 557 years p 001)Patients with DM were more likely to have squamous cellcarcinoma (p5 046) (Table 1) unknownnodal stage (p5 001)and other comorbidities (congestive heart failure cerebro-vascular disease dementia chronic pulmonary disease mildliver disease and renal disease) DMpatients were alsomorelikely to receive definitive radiotherapy instead of curativesurgery (p 001) Tumor sizes and stages differed non-significantly between the two study groups
Survival AnalysisDuring the follow-up period (mean 611 months) 81 patients(285) in the DM group and 41 (144) in the non-DM groupdied Patients in theDMgroupexhibited shorterOS times thandid patients without DM and the difference was significant(p 0001) (Fig 2A)TheOSrates forpatientswithandwithoutDMwere 856 and 948 respectively at 2 years and 739and 879 respectively at 5 years Patients in the DM groupalso exhibited significantly shorter CSS times than did those inthenon-DMgroup(p5 0003) (Fig2B)TheCSSratesforpatientswith and without DM were 909 and 959 respectively at2 years and 854 and 915 respectively at 5 years
Afteradjustment forage tumorsize andstage nodal stagehistologymodalities ofcurative treatment andcomorbiditiesDM remained an independent predictor of a lower CSSprobability (adjusted HR 146 95 CI 103ndash208 p 5 032)(Table 2) and OS probability (adjusted HR 155 95 CI121ndash200 p5 0007) (Table 2)
Subgroup analyses demonstrated the consistent prognosticinfluence of DM among the various subgroups including agetumor size and stage node stages histology modalities ofcurative treatment and comorbidities No strong heteroge-neity between the HRs of the subgroups was foundThe rangesof the adjusted HRs were 089ndash314 for CC-specific mortalityand113ndash297 foroverallmortalityamongthesubgroups (Fig3)
DISCUSSION
In this comprehensive population-based study we demon-strated thatDMwasan independentadverseprognostic factorfor patients in Taiwan who received curative treatment forearly stage CC The prognostic impact of DM was significantaccording to multivariate analysis and it remained consistentamong various subgroups differentiated by age stage tumorsize histology and treatment modality Patients with DMexhibited significantly shorter CSS times than did thosewithout DM (p5 0003 CSS rates 854 vs 915 at 5 years)and DM remained an independent predictor of lower CSSprobability (adjusted HR 146 95 CI 103ndash208 p 5 032)according to multivariate analysis
Previous studies have reported DM as a poor prognosticfactor of early stage liver and breast cancers [23 24] because it
increases cancer-specific mortality Our study reveals a similarresult in early CC One of the common characteristics of thesecancers is a high level of IGF-1R overexpression [25ndash27] Theassociation between the IGF-1 level and CC has been reported[28] andhigh-gradeexpressionof IGF-1Rcanbeusedtopredictthe high risk of death and disease recurrence in early CC [29]Hyperglycemia and hyperinsulinemia in patients with DMmay reduce the hepatic production of IGF binding protein1 and increase the free IGF-1 level [30 31] An increasedIGF-1 level in DM patients and overexpression of IGF-1R inCC cells activates the IGF axis and possibly results in poorprognosis
Thesubgroupanalyses (Fig 3)demonstrated that the impactof DMwas consistent for OS and CSS among all subgroups Thenegative impact ofDMwasmore prominent in adenocarcinomacompared with squamous cell carcinoma Nearly all cancers(pancreas endometrium liver colon andbreast)with a positiveassociation with DM are adenocarcinoma in pathology Thedifferenceofthe IGF-1andIGF-1Raxisbetweenadenocarcinomaandsquamouscell carcinoma remainsunclear andmore studiesarewarranted to clarify the systemrsquos role in themetastasis of CCparticularly adenocarcinoma
Treatment modalities other than surgery alone were asso-ciated with less favorable OS and CSS Patients for whom sur-gery is contraindicated might exhibit unfavorable risk factorssuch as poor performance or inadequate control of DM which
Figure 2 Survival of stage IndashIIA cervical cancer patients bydiabetes mellitus diagnosis status (A) Overall survival (B)Cervical cancer-specific survival
Abbreviation DM diabetes mellitus
copyAlphaMed Press 2015TheOncologistreg
1054 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
could imply unfavorable prognosis A large retrospective studyperformed byMD Anderson Cancer Center revealed that obesecervical cancer patients were more likely to be treated withprimary radiotherapy rather than surgery and had poorersurvival comparedwithhealthy-weightpatients [32]They foundthat obesity is also an independent poor prognostic factorfor cervical cancer patients DM patients also tend to haveobesity and that potentially leads to inadequate treatmentdosein several respects that could impair outcomes Inaccuracy inradiation dose calculationmdashespecially for lateral or obliquetreatment fields [33] inadequate pelvis penetration even byhigh-energy radiation beams and deviation in daily setupdue to skin folds [34]mdashcontributes to difficulties in deliveringradiotherapy to obese patients In addition up to 40 ofobese patients still receive smaller doses of chemotherapythan expected by their actual body weight although interna-tional guidelines suggest giving full-weight-based cytotoxicchemotherapy doses for obese patients [35] Without surgerysubclinical metastatic lymph nodes could impair survival in
patients who receive underdosing of radiotherapy and che-motherapy Although we do not have body mass index datain this study because of limitations in our database morbidobesity is lesscommonlyseeninAsianpopulationsandmayplaya minor role in this study In addition only patients exhibitingunfavorable pathological factors receive adjuvant treatmenttherefore they have a higher risk of disease recurrenceand death
For this nationwide population-based study we used datafrom the Taiwan NHI database thereby reducing the patientselection bias commonly found in institute-based studieshowever the study was retrospective and several limitationswere present First nonsurgical patients were not issuedpathological reports documenting tumor size therefore inac-curacy in or lack of records of the clinical tumor size resulted inunknown tumor sizes Except for the unknown parts of thedata distribution of tumor size was similar between the twogroups Second we could not analyze several aforementionedcrucial prognostic factors that may affect the choice of
Table 2 Cox regression model for stage IndashIIA
Variable
Overall mortality Cancer-specific mortality
Adjusted HR (95 CI) p value Adjusted HR (95 CI) p value
DM
No Ref Ref
Yes 155 (121ndash200) 0007 146 (103ndash208) 0320
Age 104 (103ndash105) 0001 102 (101ndash103) 0005
Tumor size
4 cm Ref Ref
$4 cm 140 (106ndash186) 0183 159 (114ndash223) 0066
Unknown 085 (068ndash106) 1459 085 (064ndash112) 2500
Lymph node
N0 Ref Ref
N1 471 (311ndash713) 0001 497 (315ndash784) 0001
Unknown 099 (073ndash133) 9328 100 (067ndash149) 9939
Histology
Squamous cell carcinoma Ref Ref
Adenocarcinoma 177 (138ndash227) 0001 212 (158ndash283) 0001
Stage
Stage I Ref
Stage IIA 149 (120ndash185) 0001 175 (134ndash229) 0001
Treatment
Surgery Ref Ref
Surgery plus adjuvant therapy 175 (131ndash234) 0002 190 (135ndash266) 0002
Concurrent chemoradiation 216 (158ndash296) 0001 237 (162ndash347) 0001
Radiotherapy 252 (184ndash346) 0001 230 (152ndash347) 0001
Comorbidity
Congestive heart failure 130 (080ndash211) 2843 132 (067ndash262) 4281
Cerebrovascular disease 118 (079ndash176) 4154 134 (078ndash229) 2901
Dementia 168 (087ndash325) 1247 077 (019ndash319) 7218
Chronic pulmonary disease 116 (079ndash169) 4463 126 (077ndash206) 3592
Mild liver disease 138 (096ndash199) 0817 097 (056ndash168) 9145
Renal disease 188 (108ndash327) 0248 068 (022ndash215) 5103
Abbreviations CI confidence interval DM diabetes mellitus HR hazard ratio Ref reference
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1055
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
curative treatment modality Although there are many limi-tations DM remained an independent prognostic factorfor OS and CSS after adjusting confounding factors bymultivariate analysis
InconclusionwedemonstratedthatearlystageCCpatientswith DM exhibited less favorable OS and CSS after curativetreatment The prognostic impact of DM remained significantafter adjustment for patient demographics and other comor-bidities We should continue to search for more accurateprognostic factors and to determine which would justify morefrequent surveillance in high-risk groups for early detection ofcurable disease recurrence To confirm the role of the IGF axisfor cancer survival in humans more clinical trials of IGF-targeted agents for CC patientsmdashparticularly thosewith DMoradenocarcinomamdashare required
ACKNOWLEDGMENTS
We thank the Collaboration Center of Health InformationApplication (CCHIA) Department of Health Executive Yuan
Taiwan for providing the databaseThis studywas supported bythe Bureau of National Health Insurance Department of HealthTaiwan (DOH96-NH-1003) and the Science and TechnologyUnit Department of Health Taiwan (DOH99-TD-B-111ndash001DOH100-TD-B-111ndash001)
AUTHOR CONTRIBUTIONSConceptionDesign Hung-Yang Kuo Zhong-Zhe Lin Yu-Yun Shao Chiun HsuAnn-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
Provision of study material or patients Raymond KuoWen-Yi Shau Chiu-LinLai Yen-Yun Yang
Collection andor assembly of data Raymond KuoWen-Yi Shau Chiu-Lin LaiYen-Yun Yang
Data analysis and interpretation Hung-Yang Kuo Zhong-Zhe Lin RaymondKuo Chiu-Lin Lai Yen-Yun Yang
Manuscript writing Hung-Yang Kuo Zhong-Zhe LinFinal approval of manuscript Hung-Yang Kuo Zhong-Zhe Lin Raymond KuoWen-Yi Shau Chiu-Lin Lai Yen-Yun Yang Yu-Yun Shao Chiun HsuWen-FanCheng Ann-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
DISCLOSURES
The authors indicated no financial relationships
REFERENCES
1 Cervical cancer Estimated incidence mortalityand prevalence worldwide in 2012 Available athttpglobocaniarcfrPagesfact_sheets_canceraspxcancer5cervix Accessed March 10 2015
2 Peters WA III Liu PY Barrett RJ II et al
Concurrent chemotherapy and pelvic radiation
therapy compared with pelvic radiation therapy
alone as adjuvant therapy after radical surgery in
high-riskearly-stagecancerof thecervix JClinOncol
2000181606ndash1613
3 Rotman M Sedlis A Piedmonte MR et al A
phase III randomized trial of postoperative pelvic
irradiation in stage IB cervical carcinoma with poor
prognostic features Follow-up of a gynecologic
oncology group study Int J Radiat Oncol Biol Phys200665169ndash176
4Vigneri P Frasca F Sciacca L et al Diabetes andcancer Endocr Relat Cancer 2009161103ndash1123
5Yood MU Oliveria SA Campbell UB et alIncidence of cancer in a population-based cohortofpatientswith type2diabetesDiabMet SyndrClinRes Rev 2009312ndash16
6 Inoue M Iwasaki M Otani T et al Diabetesmellitus and the risk of cancer Results from a large-scale population-based cohort study in Japan ArchIntern Med 20061661871ndash1877
7 Atchison EA Gridley G Carreon JD et al Risk ofcancer in a large cohort of US veterans withdiabetes Int J Cancer 2011128635ndash643
8Weinstein D Simon M Yehezkel E et alInsulin analogues display IGF-I-like mito-genic and anti-apoptotic activities in culturedcancer cells Diabetes Metab Res Rev 20092541ndash49
9 Law JH Habibi G Hu K et al Phosphorylatedinsulin-like growth factor-iinsulin receptor ispresent in all breast cancer subtypes and isrelated to poor survival Cancer Res 20086810238ndash10246
10 Shen MR Hsu YM Hsu KF et al Insulin-likegrowth factor 1 is a potent stimulator of cervicalcancer cell invasiveness and proliferation that ismodulated by alphavbeta3 integrin signaling Car-cinogenesis 200627962ndash971
Figure 3 Subgroup analysis of adjusted hazard ratios of mortality for patients with and without diabetes mellitus using the Coxproportional hazards model
Abbreviations CCRT chemoradiotherapy CI confidence interval DM diabetes mellitus HR hazard ratio OP surgery RT radiotherapy
copyAlphaMed Press 2015TheOncologistreg
1056 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
11 Huang YF Shen MR Hsu KF et al Clinicalimplications of insulin-like growth factor 1 system inearly-stage cervical cancer Br J Cancer 2008991096ndash1102
12Wideroff L Gridley G Mellemkjaer L et alCancer incidence in a population-based cohort ofpatients hospitalized with diabetes mellitus inDenmark J Natl Cancer Inst 1997891360ndash1365
13 OrsquoMara BA Byers T Schoenfeld E Diabetesmellitus and cancer risk A multisite case-controlstudy J Chronic Dis 198538435ndash441
14 ChiangCJChenYCChenCJetalCancer trendsin Taiwan Jpn J Clin Oncol 201040897ndash904
15Taiwan Cancer Registry Available at httptcrcphntuedutwmainphpPage5N2 AccessedMarch 10 2015
16Taiwan Cancer Registry annual report2011 [in Chinese] Available at httpwwwhpagovtwBHPNetWebStatStatisticsShowaspxNo5201404160001 Accessed March 10 2015
17 Statistics and surveys Available at httpwwwnhigovtwEnglishwebdatawebdataaspmenu511ampmenu_id5296ampwebdata_id51942ampWD_ID5296 Accessed March 10 2015
18 Introduction to the National Health InsuranceResearch Database (NHIRD) Taiwan Available athttpw3nhriorgtwnhirddate_01html AccessedMatch 10 2015
19 Greene FL Page DL Fleming ID et al AJCCCancer Staging Handbook 6th edNew York NYSpringer 2002
20 Quinn MA Benedet JL Odicino F et al Carci-nomaof the cervixuteri FIGO26thAnnual Report on
the Results of Treatment in Gynecological CancerInt J Gynaecol Obstet 200695(suppl 1)S43ndashS103
21 Quan H Sundararajan V Halfon P et al Codingalgorithms for defining comorbidities in ICD-9-CMand ICD-10 administrative data Med Care 2005431130ndash1139
22 DeyoRA CherkinDC CiolMAAdaptinga clinicalcomorbidity index for use with ICD-9-CM administra-tive databases J Clin Epidemiol 199245613ndash619
23 ShauWYShaoYYYehYCetalDiabetesmellitusis associated with increased mortality in patientsreceiving curative therapy for hepatocellular carci-noma The Oncologist 201217856ndash862
24 Chen WW Shao YY Shau WY et al The impactof diabetes mellitus on prognosis of early breastcancer in Asia The Oncologist 201217485ndash491
25 Desbois-Mouthon C Baron A Blivet-VanEggelpoel MJ et al Insulin-like growth factor-1receptor inhibition induces a resistancemechanismvia theepidermalgrowth factor receptorHER3AKTsignaling pathway Rational basis for cotargetinginsulin-like growth factor-1 receptor and epidermalgrowth factor receptor in hepatocellular carcinomaClin Cancer Res 2009155445ndash5456
26 Steller MA Delgado CH Bartels CJ et al Over-expression of the insulin-like growth factor-1 recep-tor and autocrine stimulation in human cervicalcancer cells Cancer Res 1996561761ndash1765
27 Shimizu C Hasegawa TTani Y et al Expressionof insulin-like growth factor 1 receptor in primarybreast cancer Immunohistochemical analysis HumPathol 2004351537ndash1542
28 Lee SW Lee SY Lee SR et al Plasma levels ofinsulin-like growth factor-1 and insulin-like growth
factor binding protein-3 in women with cervicalneoplasia J Gynecol Oncol 201021174ndash180
29 Luo M Shen D Zhou X et al MicroRNA-497 isa potential prognostic marker in human cervicalcancer and functions as a tumor suppressor bytargeting the insulin-like growth factor 1 receptorSurgery 2013153836ndash847
30 Ooi GT Tseng LY Tran MQ et al Insulin rapidlydecreases insulin-like growth factor-binding protein-1gene transcription in streptozotocin-diabetic rats MolEndocrinol 199262219ndash2228
31 Powell DR Suwanichkul A Cubbage ML et alInsulin inhibits transcription of the human gene forinsulin-like growth factor-binding protein-1 J BiolChem 199126618868ndash18876
32 Frumovitz M Jhingran A Soliman PT et alMorbid obesity as an independent risk factor fordisease-specific mortality in women with cervicalcancer Obstet Gynecol 20141241098ndash1104
33 Fisher CM Fortenberry BR Jhingran A et alNovel technique for simulation and external beamtreatment planning for obese patients Pract RadiatOncol 20111152ndash155
34Wong JR Gao Z Merrick S et al Potential forhigher treatment failure in obese patients Correla-tionofelevatedbodymass indexand increaseddailyprostate deviations from the radiation beam iso-centers in an analysis of 1465 computed tomographicimages Int J Radiat Oncol Biol Phys 20097549ndash55
35 Griggs JJ Mangu PB Anderson H et alAppropriate chemotherapy dosing for obese adultpatients with cancer American Society of ClinicalOncology clinical practice guideline J Clin Oncol2012301553ndash1561
CME This article is available for continuing medical education credit at CMETheOncologistcom
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1057
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
(ICD-9-CM codes 40301 40311 40391 40402 40403 4041240413 40492 40493 582x 5830ndash5837 585x 586x 5880V420V451V56x) chronic pulmonary disease (ICD-9-CM codes4168 4169 490xndash505x 5064 5081 5088) and mild liverdisease (ICD-9-CM codes 5712 5714ndash5716) Patients receivingpostoperative chemoradiation or radiotherapy within 90 days ofsurgery were defined as having received adjuvant treatmentPatients were followed from the day of CC diagnosis to deathfromCC (CSS) death resulting from any cause (OS) or the lastfollow-up date in the NDR database (ie December 31 2011)
Statistical AnalysisThe mean or frequency of the baseline characteristics of thetwo study groups at the time of CC diagnosis were comparedusing one-way analysis of variance for continuous variablesand a chi-square test for categorical variables Patient survivaltimes (CSS and OS) according to DM status were estimated
using the Kaplan-Meier method and compared using the log-rank test We used a Cox proportional hazards model to esti-mate the adjusted hazard ratio (HR) and the associated 95confidence interval (CI) evaluating the impact of DMand otherrisk factors on mortality Patient demographics tumor stagehistology lymph node involvement status type of curativetreatment and comorbidities were all included in the Coxmodel Subgroup of age ($65 and 40ndash64 years) tumor stage(I or IIA) histology (squamous cell carcinoma or adenocarci-noma) tumor size ($4 cm4 cm or unknown) lymph nodestage (N0 or N1) and treatment (surgery surgery followed byadjuvant therapy chemoradiation radiotherapy) were analyzedto determine whether the effects of DM on mortality wereconsistent among thepatient populations A two-sidedp value005 was considered statistically significant We used SASversion 92 (SAS Institute Inc Cary NC httpwwwsascom)to perform the analyses
Table 1 Patient characteristics
Characteristic Total With DM Without DM p value
Patients n () 2946 284 (96) 2662 (904)
Age at diagnosis mean (SD) range 567 (121) 40ndash102 662 (113) 42ndash93 557 (117) 40ndash102 001
Aged 40ndash64 years n () 2142 (727) 121 (426) 2021 (759)
Aged$65 years n () 804 (273) 163 (574) 641 (241)
Tumor size n ()
4 cm 966 (328) 91 (320) 875 (329) 85
$4 cm 343 (116) 31 (109) 312 (117)
Unknown 1637 (556) 162 (570) 1475 (554)
Lymph node n ()
N0 2668 (906) 250 (883) 2418 (908) 001
N1 64 (22) 3 63 (24)
Unknown 214 (73) 33 (117) 181 (68)
Histology n ()
Adenocarcinoma 578 (196) 43 (151) 535 (201) 046
Squamous cell carcinoma 2368 (804) 241 (849) 2127 (799)
Stage n ()
Stage I 2440 (828) 228 (803) 2212 (831) 23
Stage IIA 506 (172) 56 (197) 450 (169)
Treatment group n ()
Surgery 1734 (589) 109 (384) 1625 (610) 001
Surgery plus adjuvant therapy 519 (176) 50 (176) 469 (176)
Concurrent chemoradiation 349 (118) 39 (137) 310 (117)
Radiotherapy 344 (117) 86 (303) 258 (97)
Comorbidity n ()
Congestive heart failure 65 (22) 17 (60) 48 (18) 001
Cerebrovascular disease 97 (33) 22 (78) 75 (28) 001
Dementia 17 (06) 5 (18) 12 (05) 006
Chronic pulmonary disease 126 (43) 22 (78) 104 (39) 002
Mild liver disease 134 (45) 33 (116) 101 (38) 001
Renal disease 38 (13) 16 (56) 22 (08) 001
Follow-up time (months) mean (SD) range 611 (248) 05ndash957 550 (210) 05ndash957 617 14ndash957 001
Mortality n ()
All-cause 422 (143) 81 (285) 341 (128) 001
Cervical cancer-specific 274 (93) 41 (144) 233 (88) 002
Abbreviation DM diabetes mellitus
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1053
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
RESULTS
Patient CharacteristicsThe TCR registered 21352 patients with newly diagnosed CCbetween2004and2008 In total 2946patientswith stage IndashIIAprimary CC underwent curative treatment and satisfied theeligibility criteria of this study (Fig 1) A total of 284 patients(96) had DM and they were older compared with patientswithout DM (mean age 662 vs 557 years p 001)Patients with DM were more likely to have squamous cellcarcinoma (p5 046) (Table 1) unknownnodal stage (p5 001)and other comorbidities (congestive heart failure cerebro-vascular disease dementia chronic pulmonary disease mildliver disease and renal disease) DMpatients were alsomorelikely to receive definitive radiotherapy instead of curativesurgery (p 001) Tumor sizes and stages differed non-significantly between the two study groups
Survival AnalysisDuring the follow-up period (mean 611 months) 81 patients(285) in the DM group and 41 (144) in the non-DM groupdied Patients in theDMgroupexhibited shorterOS times thandid patients without DM and the difference was significant(p 0001) (Fig 2A)TheOSrates forpatientswithandwithoutDMwere 856 and 948 respectively at 2 years and 739and 879 respectively at 5 years Patients in the DM groupalso exhibited significantly shorter CSS times than did those inthenon-DMgroup(p5 0003) (Fig2B)TheCSSratesforpatientswith and without DM were 909 and 959 respectively at2 years and 854 and 915 respectively at 5 years
Afteradjustment forage tumorsize andstage nodal stagehistologymodalities ofcurative treatment andcomorbiditiesDM remained an independent predictor of a lower CSSprobability (adjusted HR 146 95 CI 103ndash208 p 5 032)(Table 2) and OS probability (adjusted HR 155 95 CI121ndash200 p5 0007) (Table 2)
Subgroup analyses demonstrated the consistent prognosticinfluence of DM among the various subgroups including agetumor size and stage node stages histology modalities ofcurative treatment and comorbidities No strong heteroge-neity between the HRs of the subgroups was foundThe rangesof the adjusted HRs were 089ndash314 for CC-specific mortalityand113ndash297 foroverallmortalityamongthesubgroups (Fig3)
DISCUSSION
In this comprehensive population-based study we demon-strated thatDMwasan independentadverseprognostic factorfor patients in Taiwan who received curative treatment forearly stage CC The prognostic impact of DM was significantaccording to multivariate analysis and it remained consistentamong various subgroups differentiated by age stage tumorsize histology and treatment modality Patients with DMexhibited significantly shorter CSS times than did thosewithout DM (p5 0003 CSS rates 854 vs 915 at 5 years)and DM remained an independent predictor of lower CSSprobability (adjusted HR 146 95 CI 103ndash208 p 5 032)according to multivariate analysis
Previous studies have reported DM as a poor prognosticfactor of early stage liver and breast cancers [23 24] because it
increases cancer-specific mortality Our study reveals a similarresult in early CC One of the common characteristics of thesecancers is a high level of IGF-1R overexpression [25ndash27] Theassociation between the IGF-1 level and CC has been reported[28] andhigh-gradeexpressionof IGF-1Rcanbeusedtopredictthe high risk of death and disease recurrence in early CC [29]Hyperglycemia and hyperinsulinemia in patients with DMmay reduce the hepatic production of IGF binding protein1 and increase the free IGF-1 level [30 31] An increasedIGF-1 level in DM patients and overexpression of IGF-1R inCC cells activates the IGF axis and possibly results in poorprognosis
Thesubgroupanalyses (Fig 3)demonstrated that the impactof DMwas consistent for OS and CSS among all subgroups Thenegative impact ofDMwasmore prominent in adenocarcinomacompared with squamous cell carcinoma Nearly all cancers(pancreas endometrium liver colon andbreast)with a positiveassociation with DM are adenocarcinoma in pathology Thedifferenceofthe IGF-1andIGF-1Raxisbetweenadenocarcinomaandsquamouscell carcinoma remainsunclear andmore studiesarewarranted to clarify the systemrsquos role in themetastasis of CCparticularly adenocarcinoma
Treatment modalities other than surgery alone were asso-ciated with less favorable OS and CSS Patients for whom sur-gery is contraindicated might exhibit unfavorable risk factorssuch as poor performance or inadequate control of DM which
Figure 2 Survival of stage IndashIIA cervical cancer patients bydiabetes mellitus diagnosis status (A) Overall survival (B)Cervical cancer-specific survival
Abbreviation DM diabetes mellitus
copyAlphaMed Press 2015TheOncologistreg
1054 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
could imply unfavorable prognosis A large retrospective studyperformed byMD Anderson Cancer Center revealed that obesecervical cancer patients were more likely to be treated withprimary radiotherapy rather than surgery and had poorersurvival comparedwithhealthy-weightpatients [32]They foundthat obesity is also an independent poor prognostic factorfor cervical cancer patients DM patients also tend to haveobesity and that potentially leads to inadequate treatmentdosein several respects that could impair outcomes Inaccuracy inradiation dose calculationmdashespecially for lateral or obliquetreatment fields [33] inadequate pelvis penetration even byhigh-energy radiation beams and deviation in daily setupdue to skin folds [34]mdashcontributes to difficulties in deliveringradiotherapy to obese patients In addition up to 40 ofobese patients still receive smaller doses of chemotherapythan expected by their actual body weight although interna-tional guidelines suggest giving full-weight-based cytotoxicchemotherapy doses for obese patients [35] Without surgerysubclinical metastatic lymph nodes could impair survival in
patients who receive underdosing of radiotherapy and che-motherapy Although we do not have body mass index datain this study because of limitations in our database morbidobesity is lesscommonlyseeninAsianpopulationsandmayplaya minor role in this study In addition only patients exhibitingunfavorable pathological factors receive adjuvant treatmenttherefore they have a higher risk of disease recurrenceand death
For this nationwide population-based study we used datafrom the Taiwan NHI database thereby reducing the patientselection bias commonly found in institute-based studieshowever the study was retrospective and several limitationswere present First nonsurgical patients were not issuedpathological reports documenting tumor size therefore inac-curacy in or lack of records of the clinical tumor size resulted inunknown tumor sizes Except for the unknown parts of thedata distribution of tumor size was similar between the twogroups Second we could not analyze several aforementionedcrucial prognostic factors that may affect the choice of
Table 2 Cox regression model for stage IndashIIA
Variable
Overall mortality Cancer-specific mortality
Adjusted HR (95 CI) p value Adjusted HR (95 CI) p value
DM
No Ref Ref
Yes 155 (121ndash200) 0007 146 (103ndash208) 0320
Age 104 (103ndash105) 0001 102 (101ndash103) 0005
Tumor size
4 cm Ref Ref
$4 cm 140 (106ndash186) 0183 159 (114ndash223) 0066
Unknown 085 (068ndash106) 1459 085 (064ndash112) 2500
Lymph node
N0 Ref Ref
N1 471 (311ndash713) 0001 497 (315ndash784) 0001
Unknown 099 (073ndash133) 9328 100 (067ndash149) 9939
Histology
Squamous cell carcinoma Ref Ref
Adenocarcinoma 177 (138ndash227) 0001 212 (158ndash283) 0001
Stage
Stage I Ref
Stage IIA 149 (120ndash185) 0001 175 (134ndash229) 0001
Treatment
Surgery Ref Ref
Surgery plus adjuvant therapy 175 (131ndash234) 0002 190 (135ndash266) 0002
Concurrent chemoradiation 216 (158ndash296) 0001 237 (162ndash347) 0001
Radiotherapy 252 (184ndash346) 0001 230 (152ndash347) 0001
Comorbidity
Congestive heart failure 130 (080ndash211) 2843 132 (067ndash262) 4281
Cerebrovascular disease 118 (079ndash176) 4154 134 (078ndash229) 2901
Dementia 168 (087ndash325) 1247 077 (019ndash319) 7218
Chronic pulmonary disease 116 (079ndash169) 4463 126 (077ndash206) 3592
Mild liver disease 138 (096ndash199) 0817 097 (056ndash168) 9145
Renal disease 188 (108ndash327) 0248 068 (022ndash215) 5103
Abbreviations CI confidence interval DM diabetes mellitus HR hazard ratio Ref reference
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1055
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
curative treatment modality Although there are many limi-tations DM remained an independent prognostic factorfor OS and CSS after adjusting confounding factors bymultivariate analysis
InconclusionwedemonstratedthatearlystageCCpatientswith DM exhibited less favorable OS and CSS after curativetreatment The prognostic impact of DM remained significantafter adjustment for patient demographics and other comor-bidities We should continue to search for more accurateprognostic factors and to determine which would justify morefrequent surveillance in high-risk groups for early detection ofcurable disease recurrence To confirm the role of the IGF axisfor cancer survival in humans more clinical trials of IGF-targeted agents for CC patientsmdashparticularly thosewith DMoradenocarcinomamdashare required
ACKNOWLEDGMENTS
We thank the Collaboration Center of Health InformationApplication (CCHIA) Department of Health Executive Yuan
Taiwan for providing the databaseThis studywas supported bythe Bureau of National Health Insurance Department of HealthTaiwan (DOH96-NH-1003) and the Science and TechnologyUnit Department of Health Taiwan (DOH99-TD-B-111ndash001DOH100-TD-B-111ndash001)
AUTHOR CONTRIBUTIONSConceptionDesign Hung-Yang Kuo Zhong-Zhe Lin Yu-Yun Shao Chiun HsuAnn-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
Provision of study material or patients Raymond KuoWen-Yi Shau Chiu-LinLai Yen-Yun Yang
Collection andor assembly of data Raymond KuoWen-Yi Shau Chiu-Lin LaiYen-Yun Yang
Data analysis and interpretation Hung-Yang Kuo Zhong-Zhe Lin RaymondKuo Chiu-Lin Lai Yen-Yun Yang
Manuscript writing Hung-Yang Kuo Zhong-Zhe LinFinal approval of manuscript Hung-Yang Kuo Zhong-Zhe Lin Raymond KuoWen-Yi Shau Chiu-Lin Lai Yen-Yun Yang Yu-Yun Shao Chiun HsuWen-FanCheng Ann-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
DISCLOSURES
The authors indicated no financial relationships
REFERENCES
1 Cervical cancer Estimated incidence mortalityand prevalence worldwide in 2012 Available athttpglobocaniarcfrPagesfact_sheets_canceraspxcancer5cervix Accessed March 10 2015
2 Peters WA III Liu PY Barrett RJ II et al
Concurrent chemotherapy and pelvic radiation
therapy compared with pelvic radiation therapy
alone as adjuvant therapy after radical surgery in
high-riskearly-stagecancerof thecervix JClinOncol
2000181606ndash1613
3 Rotman M Sedlis A Piedmonte MR et al A
phase III randomized trial of postoperative pelvic
irradiation in stage IB cervical carcinoma with poor
prognostic features Follow-up of a gynecologic
oncology group study Int J Radiat Oncol Biol Phys200665169ndash176
4Vigneri P Frasca F Sciacca L et al Diabetes andcancer Endocr Relat Cancer 2009161103ndash1123
5Yood MU Oliveria SA Campbell UB et alIncidence of cancer in a population-based cohortofpatientswith type2diabetesDiabMet SyndrClinRes Rev 2009312ndash16
6 Inoue M Iwasaki M Otani T et al Diabetesmellitus and the risk of cancer Results from a large-scale population-based cohort study in Japan ArchIntern Med 20061661871ndash1877
7 Atchison EA Gridley G Carreon JD et al Risk ofcancer in a large cohort of US veterans withdiabetes Int J Cancer 2011128635ndash643
8Weinstein D Simon M Yehezkel E et alInsulin analogues display IGF-I-like mito-genic and anti-apoptotic activities in culturedcancer cells Diabetes Metab Res Rev 20092541ndash49
9 Law JH Habibi G Hu K et al Phosphorylatedinsulin-like growth factor-iinsulin receptor ispresent in all breast cancer subtypes and isrelated to poor survival Cancer Res 20086810238ndash10246
10 Shen MR Hsu YM Hsu KF et al Insulin-likegrowth factor 1 is a potent stimulator of cervicalcancer cell invasiveness and proliferation that ismodulated by alphavbeta3 integrin signaling Car-cinogenesis 200627962ndash971
Figure 3 Subgroup analysis of adjusted hazard ratios of mortality for patients with and without diabetes mellitus using the Coxproportional hazards model
Abbreviations CCRT chemoradiotherapy CI confidence interval DM diabetes mellitus HR hazard ratio OP surgery RT radiotherapy
copyAlphaMed Press 2015TheOncologistreg
1056 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
11 Huang YF Shen MR Hsu KF et al Clinicalimplications of insulin-like growth factor 1 system inearly-stage cervical cancer Br J Cancer 2008991096ndash1102
12Wideroff L Gridley G Mellemkjaer L et alCancer incidence in a population-based cohort ofpatients hospitalized with diabetes mellitus inDenmark J Natl Cancer Inst 1997891360ndash1365
13 OrsquoMara BA Byers T Schoenfeld E Diabetesmellitus and cancer risk A multisite case-controlstudy J Chronic Dis 198538435ndash441
14 ChiangCJChenYCChenCJetalCancer trendsin Taiwan Jpn J Clin Oncol 201040897ndash904
15Taiwan Cancer Registry Available at httptcrcphntuedutwmainphpPage5N2 AccessedMarch 10 2015
16Taiwan Cancer Registry annual report2011 [in Chinese] Available at httpwwwhpagovtwBHPNetWebStatStatisticsShowaspxNo5201404160001 Accessed March 10 2015
17 Statistics and surveys Available at httpwwwnhigovtwEnglishwebdatawebdataaspmenu511ampmenu_id5296ampwebdata_id51942ampWD_ID5296 Accessed March 10 2015
18 Introduction to the National Health InsuranceResearch Database (NHIRD) Taiwan Available athttpw3nhriorgtwnhirddate_01html AccessedMatch 10 2015
19 Greene FL Page DL Fleming ID et al AJCCCancer Staging Handbook 6th edNew York NYSpringer 2002
20 Quinn MA Benedet JL Odicino F et al Carci-nomaof the cervixuteri FIGO26thAnnual Report on
the Results of Treatment in Gynecological CancerInt J Gynaecol Obstet 200695(suppl 1)S43ndashS103
21 Quan H Sundararajan V Halfon P et al Codingalgorithms for defining comorbidities in ICD-9-CMand ICD-10 administrative data Med Care 2005431130ndash1139
22 DeyoRA CherkinDC CiolMAAdaptinga clinicalcomorbidity index for use with ICD-9-CM administra-tive databases J Clin Epidemiol 199245613ndash619
23 ShauWYShaoYYYehYCetalDiabetesmellitusis associated with increased mortality in patientsreceiving curative therapy for hepatocellular carci-noma The Oncologist 201217856ndash862
24 Chen WW Shao YY Shau WY et al The impactof diabetes mellitus on prognosis of early breastcancer in Asia The Oncologist 201217485ndash491
25 Desbois-Mouthon C Baron A Blivet-VanEggelpoel MJ et al Insulin-like growth factor-1receptor inhibition induces a resistancemechanismvia theepidermalgrowth factor receptorHER3AKTsignaling pathway Rational basis for cotargetinginsulin-like growth factor-1 receptor and epidermalgrowth factor receptor in hepatocellular carcinomaClin Cancer Res 2009155445ndash5456
26 Steller MA Delgado CH Bartels CJ et al Over-expression of the insulin-like growth factor-1 recep-tor and autocrine stimulation in human cervicalcancer cells Cancer Res 1996561761ndash1765
27 Shimizu C Hasegawa TTani Y et al Expressionof insulin-like growth factor 1 receptor in primarybreast cancer Immunohistochemical analysis HumPathol 2004351537ndash1542
28 Lee SW Lee SY Lee SR et al Plasma levels ofinsulin-like growth factor-1 and insulin-like growth
factor binding protein-3 in women with cervicalneoplasia J Gynecol Oncol 201021174ndash180
29 Luo M Shen D Zhou X et al MicroRNA-497 isa potential prognostic marker in human cervicalcancer and functions as a tumor suppressor bytargeting the insulin-like growth factor 1 receptorSurgery 2013153836ndash847
30 Ooi GT Tseng LY Tran MQ et al Insulin rapidlydecreases insulin-like growth factor-binding protein-1gene transcription in streptozotocin-diabetic rats MolEndocrinol 199262219ndash2228
31 Powell DR Suwanichkul A Cubbage ML et alInsulin inhibits transcription of the human gene forinsulin-like growth factor-binding protein-1 J BiolChem 199126618868ndash18876
32 Frumovitz M Jhingran A Soliman PT et alMorbid obesity as an independent risk factor fordisease-specific mortality in women with cervicalcancer Obstet Gynecol 20141241098ndash1104
33 Fisher CM Fortenberry BR Jhingran A et alNovel technique for simulation and external beamtreatment planning for obese patients Pract RadiatOncol 20111152ndash155
34Wong JR Gao Z Merrick S et al Potential forhigher treatment failure in obese patients Correla-tionofelevatedbodymass indexand increaseddailyprostate deviations from the radiation beam iso-centers in an analysis of 1465 computed tomographicimages Int J Radiat Oncol Biol Phys 20097549ndash55
35 Griggs JJ Mangu PB Anderson H et alAppropriate chemotherapy dosing for obese adultpatients with cancer American Society of ClinicalOncology clinical practice guideline J Clin Oncol2012301553ndash1561
CME This article is available for continuing medical education credit at CMETheOncologistcom
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1057
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from

RESULTS
Patient CharacteristicsThe TCR registered 21352 patients with newly diagnosed CCbetween2004and2008 In total 2946patientswith stage IndashIIAprimary CC underwent curative treatment and satisfied theeligibility criteria of this study (Fig 1) A total of 284 patients(96) had DM and they were older compared with patientswithout DM (mean age 662 vs 557 years p 001)Patients with DM were more likely to have squamous cellcarcinoma (p5 046) (Table 1) unknownnodal stage (p5 001)and other comorbidities (congestive heart failure cerebro-vascular disease dementia chronic pulmonary disease mildliver disease and renal disease) DMpatients were alsomorelikely to receive definitive radiotherapy instead of curativesurgery (p 001) Tumor sizes and stages differed non-significantly between the two study groups
Survival AnalysisDuring the follow-up period (mean 611 months) 81 patients(285) in the DM group and 41 (144) in the non-DM groupdied Patients in theDMgroupexhibited shorterOS times thandid patients without DM and the difference was significant(p 0001) (Fig 2A)TheOSrates forpatientswithandwithoutDMwere 856 and 948 respectively at 2 years and 739and 879 respectively at 5 years Patients in the DM groupalso exhibited significantly shorter CSS times than did those inthenon-DMgroup(p5 0003) (Fig2B)TheCSSratesforpatientswith and without DM were 909 and 959 respectively at2 years and 854 and 915 respectively at 5 years
Afteradjustment forage tumorsize andstage nodal stagehistologymodalities ofcurative treatment andcomorbiditiesDM remained an independent predictor of a lower CSSprobability (adjusted HR 146 95 CI 103ndash208 p 5 032)(Table 2) and OS probability (adjusted HR 155 95 CI121ndash200 p5 0007) (Table 2)
Subgroup analyses demonstrated the consistent prognosticinfluence of DM among the various subgroups including agetumor size and stage node stages histology modalities ofcurative treatment and comorbidities No strong heteroge-neity between the HRs of the subgroups was foundThe rangesof the adjusted HRs were 089ndash314 for CC-specific mortalityand113ndash297 foroverallmortalityamongthesubgroups (Fig3)
DISCUSSION
In this comprehensive population-based study we demon-strated thatDMwasan independentadverseprognostic factorfor patients in Taiwan who received curative treatment forearly stage CC The prognostic impact of DM was significantaccording to multivariate analysis and it remained consistentamong various subgroups differentiated by age stage tumorsize histology and treatment modality Patients with DMexhibited significantly shorter CSS times than did thosewithout DM (p5 0003 CSS rates 854 vs 915 at 5 years)and DM remained an independent predictor of lower CSSprobability (adjusted HR 146 95 CI 103ndash208 p 5 032)according to multivariate analysis
Previous studies have reported DM as a poor prognosticfactor of early stage liver and breast cancers [23 24] because it
increases cancer-specific mortality Our study reveals a similarresult in early CC One of the common characteristics of thesecancers is a high level of IGF-1R overexpression [25ndash27] Theassociation between the IGF-1 level and CC has been reported[28] andhigh-gradeexpressionof IGF-1Rcanbeusedtopredictthe high risk of death and disease recurrence in early CC [29]Hyperglycemia and hyperinsulinemia in patients with DMmay reduce the hepatic production of IGF binding protein1 and increase the free IGF-1 level [30 31] An increasedIGF-1 level in DM patients and overexpression of IGF-1R inCC cells activates the IGF axis and possibly results in poorprognosis
Thesubgroupanalyses (Fig 3)demonstrated that the impactof DMwas consistent for OS and CSS among all subgroups Thenegative impact ofDMwasmore prominent in adenocarcinomacompared with squamous cell carcinoma Nearly all cancers(pancreas endometrium liver colon andbreast)with a positiveassociation with DM are adenocarcinoma in pathology Thedifferenceofthe IGF-1andIGF-1Raxisbetweenadenocarcinomaandsquamouscell carcinoma remainsunclear andmore studiesarewarranted to clarify the systemrsquos role in themetastasis of CCparticularly adenocarcinoma
Treatment modalities other than surgery alone were asso-ciated with less favorable OS and CSS Patients for whom sur-gery is contraindicated might exhibit unfavorable risk factorssuch as poor performance or inadequate control of DM which
Figure 2 Survival of stage IndashIIA cervical cancer patients bydiabetes mellitus diagnosis status (A) Overall survival (B)Cervical cancer-specific survival
Abbreviation DM diabetes mellitus
copyAlphaMed Press 2015TheOncologistreg
1054 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
could imply unfavorable prognosis A large retrospective studyperformed byMD Anderson Cancer Center revealed that obesecervical cancer patients were more likely to be treated withprimary radiotherapy rather than surgery and had poorersurvival comparedwithhealthy-weightpatients [32]They foundthat obesity is also an independent poor prognostic factorfor cervical cancer patients DM patients also tend to haveobesity and that potentially leads to inadequate treatmentdosein several respects that could impair outcomes Inaccuracy inradiation dose calculationmdashespecially for lateral or obliquetreatment fields [33] inadequate pelvis penetration even byhigh-energy radiation beams and deviation in daily setupdue to skin folds [34]mdashcontributes to difficulties in deliveringradiotherapy to obese patients In addition up to 40 ofobese patients still receive smaller doses of chemotherapythan expected by their actual body weight although interna-tional guidelines suggest giving full-weight-based cytotoxicchemotherapy doses for obese patients [35] Without surgerysubclinical metastatic lymph nodes could impair survival in
patients who receive underdosing of radiotherapy and che-motherapy Although we do not have body mass index datain this study because of limitations in our database morbidobesity is lesscommonlyseeninAsianpopulationsandmayplaya minor role in this study In addition only patients exhibitingunfavorable pathological factors receive adjuvant treatmenttherefore they have a higher risk of disease recurrenceand death
For this nationwide population-based study we used datafrom the Taiwan NHI database thereby reducing the patientselection bias commonly found in institute-based studieshowever the study was retrospective and several limitationswere present First nonsurgical patients were not issuedpathological reports documenting tumor size therefore inac-curacy in or lack of records of the clinical tumor size resulted inunknown tumor sizes Except for the unknown parts of thedata distribution of tumor size was similar between the twogroups Second we could not analyze several aforementionedcrucial prognostic factors that may affect the choice of
Table 2 Cox regression model for stage IndashIIA
Variable
Overall mortality Cancer-specific mortality
Adjusted HR (95 CI) p value Adjusted HR (95 CI) p value
DM
No Ref Ref
Yes 155 (121ndash200) 0007 146 (103ndash208) 0320
Age 104 (103ndash105) 0001 102 (101ndash103) 0005
Tumor size
4 cm Ref Ref
$4 cm 140 (106ndash186) 0183 159 (114ndash223) 0066
Unknown 085 (068ndash106) 1459 085 (064ndash112) 2500
Lymph node
N0 Ref Ref
N1 471 (311ndash713) 0001 497 (315ndash784) 0001
Unknown 099 (073ndash133) 9328 100 (067ndash149) 9939
Histology
Squamous cell carcinoma Ref Ref
Adenocarcinoma 177 (138ndash227) 0001 212 (158ndash283) 0001
Stage
Stage I Ref
Stage IIA 149 (120ndash185) 0001 175 (134ndash229) 0001
Treatment
Surgery Ref Ref
Surgery plus adjuvant therapy 175 (131ndash234) 0002 190 (135ndash266) 0002
Concurrent chemoradiation 216 (158ndash296) 0001 237 (162ndash347) 0001
Radiotherapy 252 (184ndash346) 0001 230 (152ndash347) 0001
Comorbidity
Congestive heart failure 130 (080ndash211) 2843 132 (067ndash262) 4281
Cerebrovascular disease 118 (079ndash176) 4154 134 (078ndash229) 2901
Dementia 168 (087ndash325) 1247 077 (019ndash319) 7218
Chronic pulmonary disease 116 (079ndash169) 4463 126 (077ndash206) 3592
Mild liver disease 138 (096ndash199) 0817 097 (056ndash168) 9145
Renal disease 188 (108ndash327) 0248 068 (022ndash215) 5103
Abbreviations CI confidence interval DM diabetes mellitus HR hazard ratio Ref reference
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1055
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
curative treatment modality Although there are many limi-tations DM remained an independent prognostic factorfor OS and CSS after adjusting confounding factors bymultivariate analysis
InconclusionwedemonstratedthatearlystageCCpatientswith DM exhibited less favorable OS and CSS after curativetreatment The prognostic impact of DM remained significantafter adjustment for patient demographics and other comor-bidities We should continue to search for more accurateprognostic factors and to determine which would justify morefrequent surveillance in high-risk groups for early detection ofcurable disease recurrence To confirm the role of the IGF axisfor cancer survival in humans more clinical trials of IGF-targeted agents for CC patientsmdashparticularly thosewith DMoradenocarcinomamdashare required
ACKNOWLEDGMENTS
We thank the Collaboration Center of Health InformationApplication (CCHIA) Department of Health Executive Yuan
Taiwan for providing the databaseThis studywas supported bythe Bureau of National Health Insurance Department of HealthTaiwan (DOH96-NH-1003) and the Science and TechnologyUnit Department of Health Taiwan (DOH99-TD-B-111ndash001DOH100-TD-B-111ndash001)
AUTHOR CONTRIBUTIONSConceptionDesign Hung-Yang Kuo Zhong-Zhe Lin Yu-Yun Shao Chiun HsuAnn-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
Provision of study material or patients Raymond KuoWen-Yi Shau Chiu-LinLai Yen-Yun Yang
Collection andor assembly of data Raymond KuoWen-Yi Shau Chiu-Lin LaiYen-Yun Yang
Data analysis and interpretation Hung-Yang Kuo Zhong-Zhe Lin RaymondKuo Chiu-Lin Lai Yen-Yun Yang
Manuscript writing Hung-Yang Kuo Zhong-Zhe LinFinal approval of manuscript Hung-Yang Kuo Zhong-Zhe Lin Raymond KuoWen-Yi Shau Chiu-Lin Lai Yen-Yun Yang Yu-Yun Shao Chiun HsuWen-FanCheng Ann-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
DISCLOSURES
The authors indicated no financial relationships
REFERENCES
1 Cervical cancer Estimated incidence mortalityand prevalence worldwide in 2012 Available athttpglobocaniarcfrPagesfact_sheets_canceraspxcancer5cervix Accessed March 10 2015
2 Peters WA III Liu PY Barrett RJ II et al
Concurrent chemotherapy and pelvic radiation
therapy compared with pelvic radiation therapy
alone as adjuvant therapy after radical surgery in
high-riskearly-stagecancerof thecervix JClinOncol
2000181606ndash1613
3 Rotman M Sedlis A Piedmonte MR et al A
phase III randomized trial of postoperative pelvic
irradiation in stage IB cervical carcinoma with poor
prognostic features Follow-up of a gynecologic
oncology group study Int J Radiat Oncol Biol Phys200665169ndash176
4Vigneri P Frasca F Sciacca L et al Diabetes andcancer Endocr Relat Cancer 2009161103ndash1123
5Yood MU Oliveria SA Campbell UB et alIncidence of cancer in a population-based cohortofpatientswith type2diabetesDiabMet SyndrClinRes Rev 2009312ndash16
6 Inoue M Iwasaki M Otani T et al Diabetesmellitus and the risk of cancer Results from a large-scale population-based cohort study in Japan ArchIntern Med 20061661871ndash1877
7 Atchison EA Gridley G Carreon JD et al Risk ofcancer in a large cohort of US veterans withdiabetes Int J Cancer 2011128635ndash643
8Weinstein D Simon M Yehezkel E et alInsulin analogues display IGF-I-like mito-genic and anti-apoptotic activities in culturedcancer cells Diabetes Metab Res Rev 20092541ndash49
9 Law JH Habibi G Hu K et al Phosphorylatedinsulin-like growth factor-iinsulin receptor ispresent in all breast cancer subtypes and isrelated to poor survival Cancer Res 20086810238ndash10246
10 Shen MR Hsu YM Hsu KF et al Insulin-likegrowth factor 1 is a potent stimulator of cervicalcancer cell invasiveness and proliferation that ismodulated by alphavbeta3 integrin signaling Car-cinogenesis 200627962ndash971
Figure 3 Subgroup analysis of adjusted hazard ratios of mortality for patients with and without diabetes mellitus using the Coxproportional hazards model
Abbreviations CCRT chemoradiotherapy CI confidence interval DM diabetes mellitus HR hazard ratio OP surgery RT radiotherapy
copyAlphaMed Press 2015TheOncologistreg
1056 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
11 Huang YF Shen MR Hsu KF et al Clinicalimplications of insulin-like growth factor 1 system inearly-stage cervical cancer Br J Cancer 2008991096ndash1102
12Wideroff L Gridley G Mellemkjaer L et alCancer incidence in a population-based cohort ofpatients hospitalized with diabetes mellitus inDenmark J Natl Cancer Inst 1997891360ndash1365
13 OrsquoMara BA Byers T Schoenfeld E Diabetesmellitus and cancer risk A multisite case-controlstudy J Chronic Dis 198538435ndash441
14 ChiangCJChenYCChenCJetalCancer trendsin Taiwan Jpn J Clin Oncol 201040897ndash904
15Taiwan Cancer Registry Available at httptcrcphntuedutwmainphpPage5N2 AccessedMarch 10 2015
16Taiwan Cancer Registry annual report2011 [in Chinese] Available at httpwwwhpagovtwBHPNetWebStatStatisticsShowaspxNo5201404160001 Accessed March 10 2015
17 Statistics and surveys Available at httpwwwnhigovtwEnglishwebdatawebdataaspmenu511ampmenu_id5296ampwebdata_id51942ampWD_ID5296 Accessed March 10 2015
18 Introduction to the National Health InsuranceResearch Database (NHIRD) Taiwan Available athttpw3nhriorgtwnhirddate_01html AccessedMatch 10 2015
19 Greene FL Page DL Fleming ID et al AJCCCancer Staging Handbook 6th edNew York NYSpringer 2002
20 Quinn MA Benedet JL Odicino F et al Carci-nomaof the cervixuteri FIGO26thAnnual Report on
the Results of Treatment in Gynecological CancerInt J Gynaecol Obstet 200695(suppl 1)S43ndashS103
21 Quan H Sundararajan V Halfon P et al Codingalgorithms for defining comorbidities in ICD-9-CMand ICD-10 administrative data Med Care 2005431130ndash1139
22 DeyoRA CherkinDC CiolMAAdaptinga clinicalcomorbidity index for use with ICD-9-CM administra-tive databases J Clin Epidemiol 199245613ndash619
23 ShauWYShaoYYYehYCetalDiabetesmellitusis associated with increased mortality in patientsreceiving curative therapy for hepatocellular carci-noma The Oncologist 201217856ndash862
24 Chen WW Shao YY Shau WY et al The impactof diabetes mellitus on prognosis of early breastcancer in Asia The Oncologist 201217485ndash491
25 Desbois-Mouthon C Baron A Blivet-VanEggelpoel MJ et al Insulin-like growth factor-1receptor inhibition induces a resistancemechanismvia theepidermalgrowth factor receptorHER3AKTsignaling pathway Rational basis for cotargetinginsulin-like growth factor-1 receptor and epidermalgrowth factor receptor in hepatocellular carcinomaClin Cancer Res 2009155445ndash5456
26 Steller MA Delgado CH Bartels CJ et al Over-expression of the insulin-like growth factor-1 recep-tor and autocrine stimulation in human cervicalcancer cells Cancer Res 1996561761ndash1765
27 Shimizu C Hasegawa TTani Y et al Expressionof insulin-like growth factor 1 receptor in primarybreast cancer Immunohistochemical analysis HumPathol 2004351537ndash1542
28 Lee SW Lee SY Lee SR et al Plasma levels ofinsulin-like growth factor-1 and insulin-like growth
factor binding protein-3 in women with cervicalneoplasia J Gynecol Oncol 201021174ndash180
29 Luo M Shen D Zhou X et al MicroRNA-497 isa potential prognostic marker in human cervicalcancer and functions as a tumor suppressor bytargeting the insulin-like growth factor 1 receptorSurgery 2013153836ndash847
30 Ooi GT Tseng LY Tran MQ et al Insulin rapidlydecreases insulin-like growth factor-binding protein-1gene transcription in streptozotocin-diabetic rats MolEndocrinol 199262219ndash2228
31 Powell DR Suwanichkul A Cubbage ML et alInsulin inhibits transcription of the human gene forinsulin-like growth factor-binding protein-1 J BiolChem 199126618868ndash18876
32 Frumovitz M Jhingran A Soliman PT et alMorbid obesity as an independent risk factor fordisease-specific mortality in women with cervicalcancer Obstet Gynecol 20141241098ndash1104
33 Fisher CM Fortenberry BR Jhingran A et alNovel technique for simulation and external beamtreatment planning for obese patients Pract RadiatOncol 20111152ndash155
34Wong JR Gao Z Merrick S et al Potential forhigher treatment failure in obese patients Correla-tionofelevatedbodymass indexand increaseddailyprostate deviations from the radiation beam iso-centers in an analysis of 1465 computed tomographicimages Int J Radiat Oncol Biol Phys 20097549ndash55
35 Griggs JJ Mangu PB Anderson H et alAppropriate chemotherapy dosing for obese adultpatients with cancer American Society of ClinicalOncology clinical practice guideline J Clin Oncol2012301553ndash1561
CME This article is available for continuing medical education credit at CMETheOncologistcom
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1057
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from

could imply unfavorable prognosis A large retrospective studyperformed byMD Anderson Cancer Center revealed that obesecervical cancer patients were more likely to be treated withprimary radiotherapy rather than surgery and had poorersurvival comparedwithhealthy-weightpatients [32]They foundthat obesity is also an independent poor prognostic factorfor cervical cancer patients DM patients also tend to haveobesity and that potentially leads to inadequate treatmentdosein several respects that could impair outcomes Inaccuracy inradiation dose calculationmdashespecially for lateral or obliquetreatment fields [33] inadequate pelvis penetration even byhigh-energy radiation beams and deviation in daily setupdue to skin folds [34]mdashcontributes to difficulties in deliveringradiotherapy to obese patients In addition up to 40 ofobese patients still receive smaller doses of chemotherapythan expected by their actual body weight although interna-tional guidelines suggest giving full-weight-based cytotoxicchemotherapy doses for obese patients [35] Without surgerysubclinical metastatic lymph nodes could impair survival in
patients who receive underdosing of radiotherapy and che-motherapy Although we do not have body mass index datain this study because of limitations in our database morbidobesity is lesscommonlyseeninAsianpopulationsandmayplaya minor role in this study In addition only patients exhibitingunfavorable pathological factors receive adjuvant treatmenttherefore they have a higher risk of disease recurrenceand death
For this nationwide population-based study we used datafrom the Taiwan NHI database thereby reducing the patientselection bias commonly found in institute-based studieshowever the study was retrospective and several limitationswere present First nonsurgical patients were not issuedpathological reports documenting tumor size therefore inac-curacy in or lack of records of the clinical tumor size resulted inunknown tumor sizes Except for the unknown parts of thedata distribution of tumor size was similar between the twogroups Second we could not analyze several aforementionedcrucial prognostic factors that may affect the choice of
Table 2 Cox regression model for stage IndashIIA
Variable
Overall mortality Cancer-specific mortality
Adjusted HR (95 CI) p value Adjusted HR (95 CI) p value
DM
No Ref Ref
Yes 155 (121ndash200) 0007 146 (103ndash208) 0320
Age 104 (103ndash105) 0001 102 (101ndash103) 0005
Tumor size
4 cm Ref Ref
$4 cm 140 (106ndash186) 0183 159 (114ndash223) 0066
Unknown 085 (068ndash106) 1459 085 (064ndash112) 2500
Lymph node
N0 Ref Ref
N1 471 (311ndash713) 0001 497 (315ndash784) 0001
Unknown 099 (073ndash133) 9328 100 (067ndash149) 9939
Histology
Squamous cell carcinoma Ref Ref
Adenocarcinoma 177 (138ndash227) 0001 212 (158ndash283) 0001
Stage
Stage I Ref
Stage IIA 149 (120ndash185) 0001 175 (134ndash229) 0001
Treatment
Surgery Ref Ref
Surgery plus adjuvant therapy 175 (131ndash234) 0002 190 (135ndash266) 0002
Concurrent chemoradiation 216 (158ndash296) 0001 237 (162ndash347) 0001
Radiotherapy 252 (184ndash346) 0001 230 (152ndash347) 0001
Comorbidity
Congestive heart failure 130 (080ndash211) 2843 132 (067ndash262) 4281
Cerebrovascular disease 118 (079ndash176) 4154 134 (078ndash229) 2901
Dementia 168 (087ndash325) 1247 077 (019ndash319) 7218
Chronic pulmonary disease 116 (079ndash169) 4463 126 (077ndash206) 3592
Mild liver disease 138 (096ndash199) 0817 097 (056ndash168) 9145
Renal disease 188 (108ndash327) 0248 068 (022ndash215) 5103
Abbreviations CI confidence interval DM diabetes mellitus HR hazard ratio Ref reference
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1055
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
curative treatment modality Although there are many limi-tations DM remained an independent prognostic factorfor OS and CSS after adjusting confounding factors bymultivariate analysis
InconclusionwedemonstratedthatearlystageCCpatientswith DM exhibited less favorable OS and CSS after curativetreatment The prognostic impact of DM remained significantafter adjustment for patient demographics and other comor-bidities We should continue to search for more accurateprognostic factors and to determine which would justify morefrequent surveillance in high-risk groups for early detection ofcurable disease recurrence To confirm the role of the IGF axisfor cancer survival in humans more clinical trials of IGF-targeted agents for CC patientsmdashparticularly thosewith DMoradenocarcinomamdashare required
ACKNOWLEDGMENTS
We thank the Collaboration Center of Health InformationApplication (CCHIA) Department of Health Executive Yuan
Taiwan for providing the databaseThis studywas supported bythe Bureau of National Health Insurance Department of HealthTaiwan (DOH96-NH-1003) and the Science and TechnologyUnit Department of Health Taiwan (DOH99-TD-B-111ndash001DOH100-TD-B-111ndash001)
AUTHOR CONTRIBUTIONSConceptionDesign Hung-Yang Kuo Zhong-Zhe Lin Yu-Yun Shao Chiun HsuAnn-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
Provision of study material or patients Raymond KuoWen-Yi Shau Chiu-LinLai Yen-Yun Yang
Collection andor assembly of data Raymond KuoWen-Yi Shau Chiu-Lin LaiYen-Yun Yang
Data analysis and interpretation Hung-Yang Kuo Zhong-Zhe Lin RaymondKuo Chiu-Lin Lai Yen-Yun Yang
Manuscript writing Hung-Yang Kuo Zhong-Zhe LinFinal approval of manuscript Hung-Yang Kuo Zhong-Zhe Lin Raymond KuoWen-Yi Shau Chiu-Lin Lai Yen-Yun Yang Yu-Yun Shao Chiun HsuWen-FanCheng Ann-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
DISCLOSURES
The authors indicated no financial relationships
REFERENCES
1 Cervical cancer Estimated incidence mortalityand prevalence worldwide in 2012 Available athttpglobocaniarcfrPagesfact_sheets_canceraspxcancer5cervix Accessed March 10 2015
2 Peters WA III Liu PY Barrett RJ II et al
Concurrent chemotherapy and pelvic radiation
therapy compared with pelvic radiation therapy
alone as adjuvant therapy after radical surgery in
high-riskearly-stagecancerof thecervix JClinOncol
2000181606ndash1613
3 Rotman M Sedlis A Piedmonte MR et al A
phase III randomized trial of postoperative pelvic
irradiation in stage IB cervical carcinoma with poor
prognostic features Follow-up of a gynecologic
oncology group study Int J Radiat Oncol Biol Phys200665169ndash176
4Vigneri P Frasca F Sciacca L et al Diabetes andcancer Endocr Relat Cancer 2009161103ndash1123
5Yood MU Oliveria SA Campbell UB et alIncidence of cancer in a population-based cohortofpatientswith type2diabetesDiabMet SyndrClinRes Rev 2009312ndash16
6 Inoue M Iwasaki M Otani T et al Diabetesmellitus and the risk of cancer Results from a large-scale population-based cohort study in Japan ArchIntern Med 20061661871ndash1877
7 Atchison EA Gridley G Carreon JD et al Risk ofcancer in a large cohort of US veterans withdiabetes Int J Cancer 2011128635ndash643
8Weinstein D Simon M Yehezkel E et alInsulin analogues display IGF-I-like mito-genic and anti-apoptotic activities in culturedcancer cells Diabetes Metab Res Rev 20092541ndash49
9 Law JH Habibi G Hu K et al Phosphorylatedinsulin-like growth factor-iinsulin receptor ispresent in all breast cancer subtypes and isrelated to poor survival Cancer Res 20086810238ndash10246
10 Shen MR Hsu YM Hsu KF et al Insulin-likegrowth factor 1 is a potent stimulator of cervicalcancer cell invasiveness and proliferation that ismodulated by alphavbeta3 integrin signaling Car-cinogenesis 200627962ndash971
Figure 3 Subgroup analysis of adjusted hazard ratios of mortality for patients with and without diabetes mellitus using the Coxproportional hazards model
Abbreviations CCRT chemoradiotherapy CI confidence interval DM diabetes mellitus HR hazard ratio OP surgery RT radiotherapy
copyAlphaMed Press 2015TheOncologistreg
1056 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
11 Huang YF Shen MR Hsu KF et al Clinicalimplications of insulin-like growth factor 1 system inearly-stage cervical cancer Br J Cancer 2008991096ndash1102
12Wideroff L Gridley G Mellemkjaer L et alCancer incidence in a population-based cohort ofpatients hospitalized with diabetes mellitus inDenmark J Natl Cancer Inst 1997891360ndash1365
13 OrsquoMara BA Byers T Schoenfeld E Diabetesmellitus and cancer risk A multisite case-controlstudy J Chronic Dis 198538435ndash441
14 ChiangCJChenYCChenCJetalCancer trendsin Taiwan Jpn J Clin Oncol 201040897ndash904
15Taiwan Cancer Registry Available at httptcrcphntuedutwmainphpPage5N2 AccessedMarch 10 2015
16Taiwan Cancer Registry annual report2011 [in Chinese] Available at httpwwwhpagovtwBHPNetWebStatStatisticsShowaspxNo5201404160001 Accessed March 10 2015
17 Statistics and surveys Available at httpwwwnhigovtwEnglishwebdatawebdataaspmenu511ampmenu_id5296ampwebdata_id51942ampWD_ID5296 Accessed March 10 2015
18 Introduction to the National Health InsuranceResearch Database (NHIRD) Taiwan Available athttpw3nhriorgtwnhirddate_01html AccessedMatch 10 2015
19 Greene FL Page DL Fleming ID et al AJCCCancer Staging Handbook 6th edNew York NYSpringer 2002
20 Quinn MA Benedet JL Odicino F et al Carci-nomaof the cervixuteri FIGO26thAnnual Report on
the Results of Treatment in Gynecological CancerInt J Gynaecol Obstet 200695(suppl 1)S43ndashS103
21 Quan H Sundararajan V Halfon P et al Codingalgorithms for defining comorbidities in ICD-9-CMand ICD-10 administrative data Med Care 2005431130ndash1139
22 DeyoRA CherkinDC CiolMAAdaptinga clinicalcomorbidity index for use with ICD-9-CM administra-tive databases J Clin Epidemiol 199245613ndash619
23 ShauWYShaoYYYehYCetalDiabetesmellitusis associated with increased mortality in patientsreceiving curative therapy for hepatocellular carci-noma The Oncologist 201217856ndash862
24 Chen WW Shao YY Shau WY et al The impactof diabetes mellitus on prognosis of early breastcancer in Asia The Oncologist 201217485ndash491
25 Desbois-Mouthon C Baron A Blivet-VanEggelpoel MJ et al Insulin-like growth factor-1receptor inhibition induces a resistancemechanismvia theepidermalgrowth factor receptorHER3AKTsignaling pathway Rational basis for cotargetinginsulin-like growth factor-1 receptor and epidermalgrowth factor receptor in hepatocellular carcinomaClin Cancer Res 2009155445ndash5456
26 Steller MA Delgado CH Bartels CJ et al Over-expression of the insulin-like growth factor-1 recep-tor and autocrine stimulation in human cervicalcancer cells Cancer Res 1996561761ndash1765
27 Shimizu C Hasegawa TTani Y et al Expressionof insulin-like growth factor 1 receptor in primarybreast cancer Immunohistochemical analysis HumPathol 2004351537ndash1542
28 Lee SW Lee SY Lee SR et al Plasma levels ofinsulin-like growth factor-1 and insulin-like growth
factor binding protein-3 in women with cervicalneoplasia J Gynecol Oncol 201021174ndash180
29 Luo M Shen D Zhou X et al MicroRNA-497 isa potential prognostic marker in human cervicalcancer and functions as a tumor suppressor bytargeting the insulin-like growth factor 1 receptorSurgery 2013153836ndash847
30 Ooi GT Tseng LY Tran MQ et al Insulin rapidlydecreases insulin-like growth factor-binding protein-1gene transcription in streptozotocin-diabetic rats MolEndocrinol 199262219ndash2228
31 Powell DR Suwanichkul A Cubbage ML et alInsulin inhibits transcription of the human gene forinsulin-like growth factor-binding protein-1 J BiolChem 199126618868ndash18876
32 Frumovitz M Jhingran A Soliman PT et alMorbid obesity as an independent risk factor fordisease-specific mortality in women with cervicalcancer Obstet Gynecol 20141241098ndash1104
33 Fisher CM Fortenberry BR Jhingran A et alNovel technique for simulation and external beamtreatment planning for obese patients Pract RadiatOncol 20111152ndash155
34Wong JR Gao Z Merrick S et al Potential forhigher treatment failure in obese patients Correla-tionofelevatedbodymass indexand increaseddailyprostate deviations from the radiation beam iso-centers in an analysis of 1465 computed tomographicimages Int J Radiat Oncol Biol Phys 20097549ndash55
35 Griggs JJ Mangu PB Anderson H et alAppropriate chemotherapy dosing for obese adultpatients with cancer American Society of ClinicalOncology clinical practice guideline J Clin Oncol2012301553ndash1561
CME This article is available for continuing medical education credit at CMETheOncologistcom
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1057
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from

curative treatment modality Although there are many limi-tations DM remained an independent prognostic factorfor OS and CSS after adjusting confounding factors bymultivariate analysis
InconclusionwedemonstratedthatearlystageCCpatientswith DM exhibited less favorable OS and CSS after curativetreatment The prognostic impact of DM remained significantafter adjustment for patient demographics and other comor-bidities We should continue to search for more accurateprognostic factors and to determine which would justify morefrequent surveillance in high-risk groups for early detection ofcurable disease recurrence To confirm the role of the IGF axisfor cancer survival in humans more clinical trials of IGF-targeted agents for CC patientsmdashparticularly thosewith DMoradenocarcinomamdashare required
ACKNOWLEDGMENTS
We thank the Collaboration Center of Health InformationApplication (CCHIA) Department of Health Executive Yuan
Taiwan for providing the databaseThis studywas supported bythe Bureau of National Health Insurance Department of HealthTaiwan (DOH96-NH-1003) and the Science and TechnologyUnit Department of Health Taiwan (DOH99-TD-B-111ndash001DOH100-TD-B-111ndash001)
AUTHOR CONTRIBUTIONSConceptionDesign Hung-Yang Kuo Zhong-Zhe Lin Yu-Yun Shao Chiun HsuAnn-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
Provision of study material or patients Raymond KuoWen-Yi Shau Chiu-LinLai Yen-Yun Yang
Collection andor assembly of data Raymond KuoWen-Yi Shau Chiu-Lin LaiYen-Yun Yang
Data analysis and interpretation Hung-Yang Kuo Zhong-Zhe Lin RaymondKuo Chiu-Lin Lai Yen-Yun Yang
Manuscript writing Hung-Yang Kuo Zhong-Zhe LinFinal approval of manuscript Hung-Yang Kuo Zhong-Zhe Lin Raymond KuoWen-Yi Shau Chiu-Lin Lai Yen-Yun Yang Yu-Yun Shao Chiun HsuWen-FanCheng Ann-Lii Cheng James Chih-Hsin Yang Mei-Shu Lai
DISCLOSURES
The authors indicated no financial relationships
REFERENCES
1 Cervical cancer Estimated incidence mortalityand prevalence worldwide in 2012 Available athttpglobocaniarcfrPagesfact_sheets_canceraspxcancer5cervix Accessed March 10 2015
2 Peters WA III Liu PY Barrett RJ II et al
Concurrent chemotherapy and pelvic radiation
therapy compared with pelvic radiation therapy
alone as adjuvant therapy after radical surgery in
high-riskearly-stagecancerof thecervix JClinOncol
2000181606ndash1613
3 Rotman M Sedlis A Piedmonte MR et al A
phase III randomized trial of postoperative pelvic
irradiation in stage IB cervical carcinoma with poor
prognostic features Follow-up of a gynecologic
oncology group study Int J Radiat Oncol Biol Phys200665169ndash176
4Vigneri P Frasca F Sciacca L et al Diabetes andcancer Endocr Relat Cancer 2009161103ndash1123
5Yood MU Oliveria SA Campbell UB et alIncidence of cancer in a population-based cohortofpatientswith type2diabetesDiabMet SyndrClinRes Rev 2009312ndash16
6 Inoue M Iwasaki M Otani T et al Diabetesmellitus and the risk of cancer Results from a large-scale population-based cohort study in Japan ArchIntern Med 20061661871ndash1877
7 Atchison EA Gridley G Carreon JD et al Risk ofcancer in a large cohort of US veterans withdiabetes Int J Cancer 2011128635ndash643
8Weinstein D Simon M Yehezkel E et alInsulin analogues display IGF-I-like mito-genic and anti-apoptotic activities in culturedcancer cells Diabetes Metab Res Rev 20092541ndash49
9 Law JH Habibi G Hu K et al Phosphorylatedinsulin-like growth factor-iinsulin receptor ispresent in all breast cancer subtypes and isrelated to poor survival Cancer Res 20086810238ndash10246
10 Shen MR Hsu YM Hsu KF et al Insulin-likegrowth factor 1 is a potent stimulator of cervicalcancer cell invasiveness and proliferation that ismodulated by alphavbeta3 integrin signaling Car-cinogenesis 200627962ndash971
Figure 3 Subgroup analysis of adjusted hazard ratios of mortality for patients with and without diabetes mellitus using the Coxproportional hazards model
Abbreviations CCRT chemoradiotherapy CI confidence interval DM diabetes mellitus HR hazard ratio OP surgery RT radiotherapy
copyAlphaMed Press 2015TheOncologistreg
1056 Diabetes Mellitus and Prognosis of Cervical Cancer
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from
11 Huang YF Shen MR Hsu KF et al Clinicalimplications of insulin-like growth factor 1 system inearly-stage cervical cancer Br J Cancer 2008991096ndash1102
12Wideroff L Gridley G Mellemkjaer L et alCancer incidence in a population-based cohort ofpatients hospitalized with diabetes mellitus inDenmark J Natl Cancer Inst 1997891360ndash1365
13 OrsquoMara BA Byers T Schoenfeld E Diabetesmellitus and cancer risk A multisite case-controlstudy J Chronic Dis 198538435ndash441
14 ChiangCJChenYCChenCJetalCancer trendsin Taiwan Jpn J Clin Oncol 201040897ndash904
15Taiwan Cancer Registry Available at httptcrcphntuedutwmainphpPage5N2 AccessedMarch 10 2015
16Taiwan Cancer Registry annual report2011 [in Chinese] Available at httpwwwhpagovtwBHPNetWebStatStatisticsShowaspxNo5201404160001 Accessed March 10 2015
17 Statistics and surveys Available at httpwwwnhigovtwEnglishwebdatawebdataaspmenu511ampmenu_id5296ampwebdata_id51942ampWD_ID5296 Accessed March 10 2015
18 Introduction to the National Health InsuranceResearch Database (NHIRD) Taiwan Available athttpw3nhriorgtwnhirddate_01html AccessedMatch 10 2015
19 Greene FL Page DL Fleming ID et al AJCCCancer Staging Handbook 6th edNew York NYSpringer 2002
20 Quinn MA Benedet JL Odicino F et al Carci-nomaof the cervixuteri FIGO26thAnnual Report on
the Results of Treatment in Gynecological CancerInt J Gynaecol Obstet 200695(suppl 1)S43ndashS103
21 Quan H Sundararajan V Halfon P et al Codingalgorithms for defining comorbidities in ICD-9-CMand ICD-10 administrative data Med Care 2005431130ndash1139
22 DeyoRA CherkinDC CiolMAAdaptinga clinicalcomorbidity index for use with ICD-9-CM administra-tive databases J Clin Epidemiol 199245613ndash619
23 ShauWYShaoYYYehYCetalDiabetesmellitusis associated with increased mortality in patientsreceiving curative therapy for hepatocellular carci-noma The Oncologist 201217856ndash862
24 Chen WW Shao YY Shau WY et al The impactof diabetes mellitus on prognosis of early breastcancer in Asia The Oncologist 201217485ndash491
25 Desbois-Mouthon C Baron A Blivet-VanEggelpoel MJ et al Insulin-like growth factor-1receptor inhibition induces a resistancemechanismvia theepidermalgrowth factor receptorHER3AKTsignaling pathway Rational basis for cotargetinginsulin-like growth factor-1 receptor and epidermalgrowth factor receptor in hepatocellular carcinomaClin Cancer Res 2009155445ndash5456
26 Steller MA Delgado CH Bartels CJ et al Over-expression of the insulin-like growth factor-1 recep-tor and autocrine stimulation in human cervicalcancer cells Cancer Res 1996561761ndash1765
27 Shimizu C Hasegawa TTani Y et al Expressionof insulin-like growth factor 1 receptor in primarybreast cancer Immunohistochemical analysis HumPathol 2004351537ndash1542
28 Lee SW Lee SY Lee SR et al Plasma levels ofinsulin-like growth factor-1 and insulin-like growth
factor binding protein-3 in women with cervicalneoplasia J Gynecol Oncol 201021174ndash180
29 Luo M Shen D Zhou X et al MicroRNA-497 isa potential prognostic marker in human cervicalcancer and functions as a tumor suppressor bytargeting the insulin-like growth factor 1 receptorSurgery 2013153836ndash847
30 Ooi GT Tseng LY Tran MQ et al Insulin rapidlydecreases insulin-like growth factor-binding protein-1gene transcription in streptozotocin-diabetic rats MolEndocrinol 199262219ndash2228
31 Powell DR Suwanichkul A Cubbage ML et alInsulin inhibits transcription of the human gene forinsulin-like growth factor-binding protein-1 J BiolChem 199126618868ndash18876
32 Frumovitz M Jhingran A Soliman PT et alMorbid obesity as an independent risk factor fordisease-specific mortality in women with cervicalcancer Obstet Gynecol 20141241098ndash1104
33 Fisher CM Fortenberry BR Jhingran A et alNovel technique for simulation and external beamtreatment planning for obese patients Pract RadiatOncol 20111152ndash155
34Wong JR Gao Z Merrick S et al Potential forhigher treatment failure in obese patients Correla-tionofelevatedbodymass indexand increaseddailyprostate deviations from the radiation beam iso-centers in an analysis of 1465 computed tomographicimages Int J Radiat Oncol Biol Phys 20097549ndash55
35 Griggs JJ Mangu PB Anderson H et alAppropriate chemotherapy dosing for obese adultpatients with cancer American Society of ClinicalOncology clinical practice guideline J Clin Oncol2012301553ndash1561
CME This article is available for continuing medical education credit at CMETheOncologistcom
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1057
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from

11 Huang YF Shen MR Hsu KF et al Clinicalimplications of insulin-like growth factor 1 system inearly-stage cervical cancer Br J Cancer 2008991096ndash1102
12Wideroff L Gridley G Mellemkjaer L et alCancer incidence in a population-based cohort ofpatients hospitalized with diabetes mellitus inDenmark J Natl Cancer Inst 1997891360ndash1365
13 OrsquoMara BA Byers T Schoenfeld E Diabetesmellitus and cancer risk A multisite case-controlstudy J Chronic Dis 198538435ndash441
14 ChiangCJChenYCChenCJetalCancer trendsin Taiwan Jpn J Clin Oncol 201040897ndash904
15Taiwan Cancer Registry Available at httptcrcphntuedutwmainphpPage5N2 AccessedMarch 10 2015
16Taiwan Cancer Registry annual report2011 [in Chinese] Available at httpwwwhpagovtwBHPNetWebStatStatisticsShowaspxNo5201404160001 Accessed March 10 2015
17 Statistics and surveys Available at httpwwwnhigovtwEnglishwebdatawebdataaspmenu511ampmenu_id5296ampwebdata_id51942ampWD_ID5296 Accessed March 10 2015
18 Introduction to the National Health InsuranceResearch Database (NHIRD) Taiwan Available athttpw3nhriorgtwnhirddate_01html AccessedMatch 10 2015
19 Greene FL Page DL Fleming ID et al AJCCCancer Staging Handbook 6th edNew York NYSpringer 2002
20 Quinn MA Benedet JL Odicino F et al Carci-nomaof the cervixuteri FIGO26thAnnual Report on
the Results of Treatment in Gynecological CancerInt J Gynaecol Obstet 200695(suppl 1)S43ndashS103
21 Quan H Sundararajan V Halfon P et al Codingalgorithms for defining comorbidities in ICD-9-CMand ICD-10 administrative data Med Care 2005431130ndash1139
22 DeyoRA CherkinDC CiolMAAdaptinga clinicalcomorbidity index for use with ICD-9-CM administra-tive databases J Clin Epidemiol 199245613ndash619
23 ShauWYShaoYYYehYCetalDiabetesmellitusis associated with increased mortality in patientsreceiving curative therapy for hepatocellular carci-noma The Oncologist 201217856ndash862
24 Chen WW Shao YY Shau WY et al The impactof diabetes mellitus on prognosis of early breastcancer in Asia The Oncologist 201217485ndash491
25 Desbois-Mouthon C Baron A Blivet-VanEggelpoel MJ et al Insulin-like growth factor-1receptor inhibition induces a resistancemechanismvia theepidermalgrowth factor receptorHER3AKTsignaling pathway Rational basis for cotargetinginsulin-like growth factor-1 receptor and epidermalgrowth factor receptor in hepatocellular carcinomaClin Cancer Res 2009155445ndash5456
26 Steller MA Delgado CH Bartels CJ et al Over-expression of the insulin-like growth factor-1 recep-tor and autocrine stimulation in human cervicalcancer cells Cancer Res 1996561761ndash1765
27 Shimizu C Hasegawa TTani Y et al Expressionof insulin-like growth factor 1 receptor in primarybreast cancer Immunohistochemical analysis HumPathol 2004351537ndash1542
28 Lee SW Lee SY Lee SR et al Plasma levels ofinsulin-like growth factor-1 and insulin-like growth
factor binding protein-3 in women with cervicalneoplasia J Gynecol Oncol 201021174ndash180
29 Luo M Shen D Zhou X et al MicroRNA-497 isa potential prognostic marker in human cervicalcancer and functions as a tumor suppressor bytargeting the insulin-like growth factor 1 receptorSurgery 2013153836ndash847
30 Ooi GT Tseng LY Tran MQ et al Insulin rapidlydecreases insulin-like growth factor-binding protein-1gene transcription in streptozotocin-diabetic rats MolEndocrinol 199262219ndash2228
31 Powell DR Suwanichkul A Cubbage ML et alInsulin inhibits transcription of the human gene forinsulin-like growth factor-binding protein-1 J BiolChem 199126618868ndash18876
32 Frumovitz M Jhingran A Soliman PT et alMorbid obesity as an independent risk factor fordisease-specific mortality in women with cervicalcancer Obstet Gynecol 20141241098ndash1104
33 Fisher CM Fortenberry BR Jhingran A et alNovel technique for simulation and external beamtreatment planning for obese patients Pract RadiatOncol 20111152ndash155
34Wong JR Gao Z Merrick S et al Potential forhigher treatment failure in obese patients Correla-tionofelevatedbodymass indexand increaseddailyprostate deviations from the radiation beam iso-centers in an analysis of 1465 computed tomographicimages Int J Radiat Oncol Biol Phys 20097549ndash55
35 Griggs JJ Mangu PB Anderson H et alAppropriate chemotherapy dosing for obese adultpatients with cancer American Society of ClinicalOncology clinical practice guideline J Clin Oncol2012301553ndash1561
CME This article is available for continuing medical education credit at CMETheOncologistcom
wwwTheOncologistcom copyAlphaMed Press 2015
Kuo Lin Kuo et al 1057
CME
by guest on May 2 2018
httptheoncologistalphamedpressorg
Dow
nloaded from