thesis 22st march 55961 - portsmouth research portal · web viewphysiotherapy treatment has been...
TRANSCRIPT

CHAPTER ONE – INTRODUCTION
1. 0. Introduction
This study aims to investigate the problems of adherence to physiotherapy for adults with cystic fibrosis (CF), and to develop an intervention in the form of a self-management physiotherapy programme (SMPP) to improve the ability to adhere to physiotherapy treatment and thereby postulate a new and improved model of physiotherapy clinical practice. Physiotherapy is an integral part of the daily treatment and management for CF (Association of Chartered Physiotherapists in Cystic Fibrosis (ACPCF)/CF Trust, 2011; Pryor et al., 2010) as it aims to keep the airways clear of secretions, encourages exercise/activity to keep as fit and as healthy possible, promotes good posture in order to reduce the impact of osteoporosis and the development of adverse respiratory mechanics in the chest wall (kypho-scoliosis) and reduces the risk of musculo-skeletal joint pain. Physiotherapy, which is one component of the complex and time consuming treatment regimens for CF, provides challenges in balancing the optimal treatment needed to maintain a good health status with the burden of regular daily treatment, which may affect a persons quality of life (QoL) and make adherence to treatment difficult (Christian, 2007; Daniels, 2010; Kettler, Sawyer, Winefield, & Greville, 2002). Of all of the treatment regimens carried out by people with CF, daily physiotherapy is the least liked (Daniels, 2010; Ireland, 2003; White, Stiller, & Haensal, 2007; Zindani, Streetman, Streetman, & Nasr, 2006) and has the lowest levels of adherence which can result an increased frequency of chest infections, pharmacological costs and hospitalisation in addition to a reduced quality of life (QoL). Physiotherapy treatment has been perceived by some people with CF as being ineffective, time consuming and its clinical benefits not always discernable (Llorente, Bousono, & Martin, 2008; Myers & Horn, 2006). Whilst highlighting adherence as a significant issue, the CF literature does not provide explanations or strategies to address this problem because studies into adherence to physiotherapy for adults with CF are in their infancy, as it is only in recent years that people with CF are living longer into adulthood.
1. 1 Cystic Fibrosis
CF is a complex multi-system life threatening disease with a poor prognosis and no cure. It is the most common recessively inherited genetic disease of Caucasian populations, with a carrier rate of 1 in 25 and an incidence of 1 in 2,500 live births
1

(CF Trust, 2011a). There are approximately 9,000 people with CF (CF Trust, 2011a) in the UK. Life expectancy is improving as there was a median predicted survival of only 16 years in the 1970’s, where as for a child born in the 1990’s the median survival was predicted to be greater than 40 years (Elborn, Shale, & Britton, 1991; Yankaskas, Marshall, Sufian, Simon, & Rodman, 2004) and for a child born now this life expectancy is likely to be into the fifth decade (CF Trust, 2011a; Dodge, Lewis, Stanton, & Wilsher, 2007). The overall figures for the increased number of people with CF surviving into and past their third and fourth decades masks wide variations in survival rates across and within countries, and that women are more likely to die at a younger age than men, for reasons that are unclear (CF Trust, 2011a; Patterson, Wall, Berge, & Milla, 2008)
Dorothy Anderson first accurately described the disease in 1938 and at that stage 70% of infants diagnosed with CF died in the first year of life (Andersen, 1938). By the 1980’s inhaled antibiotics helped to prolong life expectancy (Hodson, Panketh, & Batton, 1984), in 1984 Tsui discovered the CF gene (Tsui, 1985) paving the way for a future cure, in 1988 the first bilateral lung transplant for CF took place (Ramirez et al., 1992) and the first heart and lung transplant in 1985 (Yacoub et al., 1990). Current research is investigating gene therapy as a means of controlling the defective mechanism (CF Trust, 2011a).
1. 1. 1. Presentation
CF is a disease of exocrine gland function that involves multiple organ systems but chiefly results in chronic respiratory infections, pancreatic enzyme insufficiency and associated complications if untreated (CF Trust, 2001). The clinical presentation, age at diagnosis, severity of symptoms and rate of disease progression in the organs involved vary widely. Diagnosis is based on typical pulmonary and gastro-intestinal (GI) tract manifestations, a family history and positive sweat chloride test results and genotyping (CF Trust, 2011a; Walters & Mehta, 2007). Newborn screening for CF is universally offered in the UK (Price, 2006). The majority present in early childhood with respiratory tract infections which are slow to clear, or persistent, intestinal malabsorption and failure to thrive (Lee & Southern, 2007). Pulmonary involvement is progressive: beginning as bronchiolitis, bronchitis and then bronchiectasis which leads to corpulmonale, end-stage lung disease and death. Severity of pulmonary disease determines prognosis and ultimate outcome (Kolbe. 2007).
2

1. 1. 2. Patho-Physiology
CF is a lethal, autosomal recessive, multisystem disease primarily affecting the organs of epithelial origin (Coakley & Boucher, 2007) with the respiratory system being the major cause for morbity and mortality. It is the result of mutations affecting the gene which encodes for a chloride channel known as the cystic fibrosis transmembrane conductance regulator (CFTR) and is essential for the regulation of salt and water movements across cell membranes (CF Trust, 2001). The gene responsible for CF is localised to 7q31.2 in the long arm of chromosome 7. It encodes a membrane-associated protein called the cystic fibrosis transmembrane conductance regulator (CFTR) (Coakley & Boucher, 2007). To date 1500 mutations have been identified with the most common gene mutation, ΔF508, occurring in about 70% of the CF population (Castellani et al., 2008; Kolbe, 2007). Because the CFTR mutations have poor penetration the genotype does not predict the pattern or severity of disease.
The CFTR protein has different roles in different types of epithelial cells. Normally, this protein allows chloride ions to exit the mucus producing cells. CFTR is anchored to the outer membrane of epithelial cells in the sweat glands, lungs, pancreas and other affected organs. The protein spans the cell membrane and acts as a channel connecting the inner part of the cell (cytoplasm) to the surrounding fluid in order to facilitate the movement of chloride across the cell membrane (Walters & Mehta, 2007). When the CFTR protein does not work chloride is trapped inside and outside of the cell membrane (Kolbe, 2007). Because chloride is negatively charged it creates a difference in the electrical potential inside and outside the cell causing cations to cross into the cell. Sodium is the most common cation in the extracellular space and the combination of sodium and chloride creates salt which is lost in high amounts in the sweat of individuals with CF (Walters & Mehta, 2007). This lost salt forms the basis for the sweat test which is used to diagnose CF.
Because the chloride ions are blocked from exiting the mucus producing cells the mucus has increased viscosity and obstructs the various pathways (CF Trust, 2001). This obstructive process also prevents bacteria from being cleared from the cells and thereby increases the potential for infection. Nearly all exocrine glands are affected in varying distribution and degrees of severity depending on the extent of the CFTR mutation (Coakley & Boucher, 2007). The chief manifestations of CF are found primarily in the respiratory and gastro-intestinal systems and to a lesser extent in the musculo-skeletal and urinary tract systems.
3

1. 1. 3. Manifestations of Cystic Fibrosis
Although CF chiefly affects the respiratory and GI systems for the purposes of this study only a details of it manifestations in the respiratory system are outlined below:
Respiratory
The disease is characterised by abnormally viscid purulent secretions, chronic infection especially by Staphylococcus aureus and Pseudomonas aeruginosa, recurrent infective exacerbations, progressive damage to airways and parenchyma, and worsening airflow obstruction that eventually leads to respiratory failure and death (CF Trust, 2001; Wallis, 2007). Although the lungs are generally histologically normal at birth, most commonly pulmonary disease develops in infancy or early childhood. Mucus plugging and chronic bacterial infection, accompanied by a pronounced inflammatory response, damage the airways and ultimately lead to bronchiectasis and respiratory insufficiency (Gibson et al., 2003; Balfour-Lynn & Elborn, 2007). The respiratory manifestations of CF are characterised by episodic infections leading to progressive decline in pulmonary function. Pulmonary damage is initiated by diffuse obstruction in the small airways caused by abnormally thick mucus secretions (Kolbe, 2007). Bronchiolitis and mucopurulent plugging of the airways occur secondary to obstruction and infection. As the disease progresses the bronchial airways narrow due to inflammatory changes, making airway clearance an increasingly difficult daily procedure (Chimiel, Berger, & Konstan, 2002;Gibson et al., 2003). With increasing obstruction of the airways exhalation becomes more difficult resulting in the alveoli expanding and air trapping occurring (CF Trust, 2001). Much of the pulmonary damage may be caused by inflammation secondary to the release of proteases by neutrophils in the airways (Kolbe, 2007). This damaging inflammatory process results in the progressive development of chronic hypoxemia which leads to muscular hypertrophy of the pulmonary arteries, pulmonary hypertension, right ventricular hypertrophy which progresses to raised pulmonary arterial pressure, right sided heart failure and ultimately death.
1. 2. Treatment for Cystic Fibrosis
The aim of treatment is to improve nutritional status, prevent or slow down the decline in pulmonary function and to aim for as “normal” a life as possible with the best quality (Daniels, 2010). Due to its complex nature CF requires an aggressive multi-system approach to treatment.
4

Management of adults with CF should be comprehensive and multi-disciplinary with an individualised approach to each person’s needs. The aim of treatment is to minimise or delay the onset of inflammatory changes, delay the decline in organ function, maintain a good nutritional state, increase life expectancy, improve/ maintain exercise tolerance, improve QoL and reduce healthcare costs (Hodson, Geddes, & Bush, 2007).
Treatment of CF is preventative, complex, time consuming, expensive and in some cases is not without significant adverse effects. CF treatment can also have a major impact on a person’s QoL due to the accumulation of a variety of necessary and burdensome daily treatments particularly for those with advanced disease (Abbott, Havermas, & Hart, 2009; Kettler et al., 2002; Kolbe, 2007; Sawicki, Sellers, & Robinson, 2009). Currently the main focus of treatment are the respiratory and GI systems with antibiotics proving one of the mainstays of treatment.
The main cause of mortality for people with CF is respiratory failure, which is a consequence of progressive lung damage. The airways of people with CF are susceptible to initial colonisation and subsequent infection by organisms that are not adequately cleared (Balfour-Lynn & Elborn, 2007). The most common bacteria causing chronic infection in adults is Pseudomonas aeruginosa and, based on its purported role in airway inflammation and damage, anti-psuedomonal antibiotics are the treatment of choice. Antibiotic therapy is directed at preventing, eradicating, or controlling respiratory infections. The prompt use of effective antibiotics in these situations has been a major reason for the decreased respiratory morbidity and increased longevity seen over the last several decades (CF Trust, 2011a). As this study focuses on the impact which adhering to physiotherapy has on the respiratory system only a brief outline of the complex treatment regimen for the respiratory system for adults is outlined below:
Treatment of respiratory problems can involve the following:
Inhaled bronchodilators to dilate the airways facilitating airway clearance Antibiotics taken orally, inhaled or intravenously in cases of more severe
infections Steroids to reduce the impact of the inflammatory process whereby the airways
become swollen. Steroid nasal drops and sprays are used to treat nasal polyps Non-steriodal anti-inflammatory drugs (NSAIDs) e.g. ibuprofen Mucolytics, e. g. inhaled enzyme RhDNase, are used to reduce the viscosity of
respiratory secretions and facilitate chest clearance
5

Osmotics e.g. hypertonic sodium chloride 7% In advanced disease oxygen, delivered through a variety of devices and systems, is
given for hypoxemia Non-invasive ventilation to aid gaseous exchange and chest clearance. Physiotherapy - Airway clearance & exercise
Heart/Lung and Lung Transplantation
Transplantation is used in instances of end stage organ failure, with either a heart and lung transplant being undertaken or a single/double lung transplantation. In recent years there has been a move to bilateral sequential lung transplants. Five year survival rates for adult lung transplantation is 78 ± 5% (Ilhan et al., 2012) and increasing but availability of donors is problematical (Aurora, Gyi, & Carby, 2007).
Other Pharmacological Treatments
Treatment for the digestive system focuses on pancreatic enzymes which help to digest fats and proteins and increase absorption of vitamins. Nutritional supplements are also given to compensate for poor digestion and give additional energy and nutrients. Without treatment mal-absorption would result in poor nutrition and a low immunity precipitating an increased propensity for debilitating chest infections. For CF Bone Disease bisphosphonates are implemented in order to help maintain bone density and reduce the risk of fractures while vaccinations, particularly for flu, are important as people with CF as they are susceptible to complications resulting from infection.
1. 3. Physiotherapy for Cystic Fibrosis
Physiotherapy is the use of physical approaches to promote, maintain and restore physical, psychological and social well-being, taking account of variations in health status (Chartered Society of Physiotherapy (CSP), 2010). Physiotherapy is science-based and committed to extending, evaluating and reviewing the evidence that underpins and informs its clinical practice. The role of the physiotherapist in the treatment and management of CF is that of clinician, educator, manager and researcher. These factors are particularly relevant in CF where the specialist skills of a respiratory physiotherapist, in terms of the treatment and management of respiratory problems, the promotion of a healthy life style through exercise/activity and the encouragement of good posture, are needed to deliver high standards of care and
6

effective outcomes (ACPCF/CF Trust, 2011; International Physiotherapy Group for Cystic Fibrosis (IPGCF), 2009).
At the time of the study people with CF were recommended to do daily chest physiotherapy in some form to either clear their chests or check that their chests were clear and to undertake exercise to maintain and promote a healthy life style (ACPCF/CF Trust, 2002). In the past the delivery of chest physiotherapy was dependent upon the assistance of another person and the use of gravity dependent postural drainage positions to facilitate sputum clearance (van der Schans, Prasad, & Main, 2009). Recent UK guidance suggests that chest physiotherapy facilitates sputum clearance by various ACTs or by using mechanical devices, or both (ACPCF/CF Trust, 2011; Bott et al., 2009; Bradley & Moran, 2011; IPGCF, 2009
1. 3. 1. Context of Physiotherapy in the Overall Management of Adults with Cystic Fibrosis
In CF physiotherapy is one of a range of essential daily treatments for this complex, multi-system, life limiting disease. Due to the time consuming nature of the overall daily treatment regimens adherence is problematical. Pharmacological treatment primarily focuses on the respiratory and GI systems while physiotherapy treatment is focuses on the respiratory, musculo-skeletal and urinary tract systems. In this study physiotherapy treatment was confined to the respiratory system and the musculo-skeletal system where exercise enhances airway clearance and acts a means of keeping fit and healthy. As the major cause of death is pulmonary in origin physiotherapy treatment for airway clearance plays a key role in the treatment and management of CF.
Daily chest physiotherapy aims to keep the airways clear of secretions or check that they are already clear thereby minimising lung damage and preserving lung function(ACPCF/CF Trust 2011; Bott et al., 2009; IPGCF, 2009). Regular exercise also promotes a healthy lifestyle and can facilitating airway clearance (Bradley & Moran, 2011). Together the result should be better health outcomes and potentially a reduction in healthcare utilisation and heath care costs with a subsequent improvement in Qo,L although to date no studies have been undertaken to establish the nature of the relationship between these factors.
Physiotherapy treatment is primarily preventative and aims to:
7
Reduce
The decline in respiratory function by reducing the incidence and impact of chest infections
The impact of CF bone disease (osteoporosis) The impact of musculo-skeletal problems (joint pains and poor posture)
Optimise health outcomes by
Using airway clearance techniques (ACTs) and adjuncts to facilitate the removal of secretions from the respiratory tract and/or keep the chest clear of secretions
Optimising ventilation Encouraging exercise/activity to keep fit and healthy and to reduce the impact
of osteoporosis and the occurrence of musculoskeletal pain. Promoting good posture in order to minimise the development of adverse
respiratory mechanics in the chest wall (kypho-scoliosis) and musculoskeletal joint pain
Educate by
Improving knowledge and skills, enabling people with CF to optimise their healthcare outcomes by encouraging them to take responsibility/ ownership for their health care
Reduce Health care costs by
Reducing hospital utilisation Reducing the demand on CF healthcare staff by encouraging self-management Reducing pharmacological costs by reducing the frequency and impact of
repeated chest infections and reducing musculoskeletal pain through posture correction exercises and good physiotherapy management of joint pain
With increasing emphasis placed on evidence-based practice, physiotherapists have been required to scrutinise their practice carefully (Dodd & Prasad, 2005). High quality, scientifically proven justification of chest physiotherapy is needed in order to persuade people with CF and their carers of the value of a respiratory routine which may not offer immediate or obvious benefit. Proven justification would reassure physiotherapists of the efficacy of their practice.
8

1. 3. 2. Physiotherapy Treatment Regimens
Physiotherapy for CF encompasses a range of treatment approaches and techniques which are outlined below:
(a) Respiratory System
Described below are a range of ACTs and adjuncts to facilitate chest clearance that are advised by the Association of Chartered Physiotherapists in Cystic Fibrosis (ACPCF) in the ACPCF/CF Trust (2011) Standards of Care and Good Clinical Practice for the Management of CF, the Association of Chartered Physiotherapists in Respiratory Care (ACPRC)/British Thoracic Society (BTS) Guidelines for the Physiotherapy Management of the Adult, Medical, Spontaneously Breathing Patient. (Bott et al., 2009) and the IPGCF (2009) Clinical Guidelines for Physiotherapy Management of CF and Physiotherapy for People with C F.
Airway Clearance Techniques
Active Cycle of Breathing Technique (ACBT)
The ACBT comprises a cycle of breathing exercises involving breathing control (gentle relaxed breathing at tidal volume), thoracic expansion exercises (three/four deep breaths with emphasis on inspiration) and one or two forced expiration techniques (with an open glottis from mid to low lung volumes) to mobilise peripheral secretions. Once the secretions have been mobilised they can be cleared from the airways by coughing. The ACBT can be adapted to individual needs but with each component of the cycle clearly defined (Button & Holland, 2008). As it is not dependent on a device, it is an ACT that every patient should be taught. ACBT has been shown to be effective and efficient in the mobilisation and clearance of secretions and improvement in lung function (ACPCF/CF Trust, 2011). It does not increase hypoxaemia or airflow obstruction.
Autogenic Drainage Autogenic drainage (AD) is a three-phased breathing regime using high expiratory flow rates at varying lung volumes to facilitate mucus clearance (McIlwaine, Davidson, Wong, & Pirie, 1991; Miller, Hall, Clayton, & Nelson, 1995). The technique aims to maximise expiratory flow velocity to produce shearing forces and mobilise secretions. While expiratory flow should be high, it should not be forced and airway closure avoided. AD can be performed in any position.
9

Positive Expiratory Pressure (PEP) Applying a resistance during expiration provides a PEP which can be utilised to enhance the mobilisation of bronchopulmonary secretions. Periods of PEP breathing are combined with the forced expiration technique (FET) to facilitate airway clearance. PEP breathing induces a temporary increase in functional residual capacity (FRC) and an increased inter-dependence between alveoli (Groth et al., 1985). It facilitates collateral ventilatory flow and opens up closed airways. It is suggested that the PEP induces increases in gas volume and pressure behind airway secretions making expiratory manoeuvres more effective (Anderson, Qvist, & Kann, 1979). PEP may be applied via a mouthpiece or mask. Treatment is usually undertaken in the sitting position but may also be performed in other positions such as supine or side lying to increase ventilation in a particular area. Breathing through the device should be at tidal volume with only slightly active expiration (not prolonged or forced) interspersed with breathing control. In order to select the appropriate level of expiratory resistance a manometer should be inserted between the expiratory valve and the resistor to measure mid-expiratory pressure. The appropriate resistance is one which achieves a stable mid-expiratory pressure of 10-20cm H2O (ACPCF/CF Trust 2011).
Oscillatory Devices in cystic fibrosisOscillatory devices are designed to alter the expiratory airflow by using a device in either an intra or extra thoracic manner. Oscillations or interruptions during expiratory airflow have been postulated to mechanically reduce the visco-elasticity of sputum and enhance muco-ciliary clearance (Button & Holland, 2008; Pryor, Webber, & Hodson, 1990). Intra-thoracic oscillations are generated orally and created using variable resistances within the airways generating controlled oscillating positive pressure. When the oscillation frequency approximates the resonance frequency of the pulmonary system, endo-bronchial pressure oscillations are amplified and result in vibrations of the airways (ACPCF/CF Trust, 2011). The intermittent increases in endo-bronchial pressure reduce the collapsibility of the airways during exhalation and thereby facilitate the likelihood of mucus being cleared from the tracheo-bronchial tract. The airflow accelerations increase the velocity of the air being exhaled, facilitating the movement of mucus up the airways (ACPCF/CF Trust, 2011, 2002). Exhalation through these devices generates both oscillations of positive pressure in the airways and repeated accelerations of expiratory airflow that have been shown to result in improved sputum clearance. Extra-thoracic oscillatory devices, such as an inflatable vest attached to a machine, vibrate at variable frequencies and intensities as
10

set by the operator to ensure the individual's comfort and associated adherence. The devices frequently employed for this purpose are:
a. Flutter®A small plastic device containing a large ball bearing which repeatedly interrupts the outward flow of air (Pryor, 1999; Konstan, Stern, & Doershuk, 1994).
b. AcapellaA flow-operated oscillatory PEP device, which uses a counterweighted plug and magnet to generate the oscillatory resistance (Volsko, DiFiore, & Chatburn, 2003).
c. CornetA horn-shaped tube which houses a rubber inner tube. The degree of rotation of this inner tube reflects the resistance generated. As the individual exhales through the horn the inner tube unfurls generating a rhythmic bending and unbending of the inner tube within the horn throughout the expiration phase (Pryor, 1999).
d. Extra-thoracic Oscillations Extra-thoracic oscillations are generated by forces external to the respiratory system, for example high frequency chest wall oscillation (HFCWO) (Warwick & Hansen, 1991) such as an inflatable vest (ACPCF/CF Trust, 2011).
Intrapulmonary Percussive Ventilation (IPV)Intrapulmonary percussive ventilation uses a mechanical device that combines internal thoracic percussion and inspiratory pressure through rapid mini bursts of air superimposed on a spontaneous breathing pattern (ACPCF/CF Trust, 2011). Expiration against the percussive element of the device leads to the maintenance of positive pressure within the airways (Newhouse, White, Marks, & Homnick, 1998). The proposed methods of action include; the maintenance of small airway patency and prevention of airway closure and atelectasis, enhanced movement of secretions and an improved distribution of nebulised medications in some instances (ACPCF/CF Trust, 2011).
Intermittent Positive Pressure Breathing (IPPB)Intermittent positive pressure breathing provides intermittent positive pressure ventilation (on inspiration only) that augments tidal volume, and indirectly improves ventilation (ACPCF/CF Trust, 2011). It is a useful adjunct where there is increased work of breathing/fatigue due to impaired secretion clearance, or atelectasis due to
11

mucus plugging. In addition, nebulisation is also possible using IPPB which offers advantages in patients with suppurative lung disease. IPPB is administered via a mouth pieces of a face mask.
Inhalation Therapy Inhalation therapy offers the delivery of a wide range of medications using a variety of devices (Bott et al., 2009). Inhaled medication includes the use of bronchodilators to open up the airways, inhaled antibiotics and mucolytics/osmotics including saline, hypertonic saline and RhDNase, which facilitate the removal of secretions. Inhalation therapy is a significant component of the management of the respiratory sequelae associated with CF. ACTs may be enhanced with effective inhalation therapy and inhalation therapy may be enhanced by effective ACTs (Button & Holland, 2008). The main determinants of deposition pattern for nebulized medications are breathing pattern during inhalation, droplet size and age/condition of the lung (Boe, et al., 2001). Inhalation therapy techniques and equipment therefore have the potential to alter the amount of drug which is delivered to its desired destination.
Non-Invasive VentilationNon-invasive ventilation (NIV) is ventilatory support provided via a nose or face mask. NIV reduces the work on the respiratory muscles by providing positive pressure during inspiration and expiration which results in improved respiratory muscle performance, increased alveolar ventilation and improved gas exchange (Button & Holland, 2008), the effects of which are crucial to the clinical application of NIV in CF. This cyclical mode of ventilation increases gas volume and pressure behind airway secretions and facilitates expiratory airway clearance procedures. In adults and children NIV has been reported as reducing the work of breathing by between 20 – 60% (Serra, Polese, Braggion, & Rossi, 2002; Piper, Parker, Torzillo, Sullivan, & Bye, 1992; Hodson, Madden, Steven, Tsang, & Yacoub, 1991). This effect is associated with a 30% increase in minute ventilation and tidal volume and a 7% reduction in transcutaneous carbon dioxide (Piper et al., 1992). As in IPPB the FRC is increased by creating inter-dependence between alveoli, improved co-lateral ventilation and the recruitment of previously closed airways (Button & Holland, 2008). NIV is accepted as a management tool for hypercapnic respiratory failure, nocturnal hypoventilation or as a bridge to lung transplantation. It may also be used as an adjunct to airway clearance and to facilitate exercise (Button & Holland, 2008).
(b) Musculo-Skeletal System Exercise/Activity
12

The ideal exercise prescription for people with CF has not been established. Both aerobic training (endurance exercise) and anaerobic training (resistance training or high-intensity, short duration training) are beneficial (Bradley & Moran, 2008). Aerobic training results in improved maximum exercise capacity and muscle strength (Button & Holland, 2008). Anaerobic training has positive effects on lactate levels, peak power and fat-free mass. Both types of exercise may have positive effects on respiratory function (Schneiderman-Walker et al., 2000). Exercise programs have beneficial effects both during admission for acute exacerbations and in the stable out-patient (Bradley & Moran, 2008).
Exercise is a cornerstone of therapy for patients with CF. Aerobic fitness is an independent predictor of survival and those with better physical fitness have a better QoL (Nixon, Orenstein, Kelsey, & Doershuk, 1992). There is a growing body of evidence showing that people with CF are not only affected by decreased cardio-respiratory fitness (i.e. aerobic) but also decreased muscle power, strength and endurance (i.e. anaerobic) (ACPCF/CF Trust, 2011). Furthermore poor posture and flexibility are common features. The aim of encouraging exercise/activity is to increase minute ventilation leading to the mobilisation of pulmonary secretions and enhanced airway clearance (Button & Holland, 2008; Lannefors & Wollmer, 1992). Some people with mild lung disease and good lung function use exercise together with forced expiration (huffing), coughing and expectoration as stand-alone airway clearance therapy. Others with more extensive lung disease and larger volumes of sputum use exercise as an adjunct to a formal airway clearance therapy regimen. A transient increase in the lung function tests of the FEV1 (Forced Expiratory Volume in one second) and the peak expiratory flow rate (PEFR) following exercise has been demonstrated in CF (Bilton, Dodd, Abbot, & Webb, 1992), suggesting that exercise may result in increased flow transients and bronchodilation. This may facilitate the clearance of secretions and improve ventilation. Coughing induced by exercise also contributes to its effectiveness as an ACT (Button & Holland, 2008). There is some evidence that structured exercise programs for people with CF improve fitness and slow the rate of pulmonary decline (Bradley & Moran, 2008). For this reason it is recommended that all patients should be encouraged to exercise several times per week.
Clinically, physical exercise is used as an adjunct to ACTs to achieve the following (Button & Holland, 2008):
Mobilise mucus Open up collapsed or plugged airways by increasing ventilation
13
Increase expiratory flow which loosens mucus from the airway wall via shearing forces
Increase resting lung volumes Increase regional ventilation via gravitational effects by exercising in different positions such as upright, sitting, supine, side lying or prone lying
Patients with milder lung disease may prefer to carry out physical exercise before airway clearance therapy as it mobilises secretions and makes airway clearance therapy more effective, where as those with advanced bronchiectasis and large volumes of daily sputum need to do airway clearance therapy before being able to enjoy exercise. Suitable forms of exercise to promote mucociliary clearance include: walking, running, and bicycling (Button & Holland, 2008). Team sports such as hockey and football combine the physiological benefits of exercise while incorporating group and social activity, which in turn promotes regular participation in physical exercise. Forced expirations and expectoration should always be interspersed with physical exercise in order to optimise airway clearance therapy (button & Holland, 2008).
1. 3. 3. Definition of Physiotherapy Treatment for the Purpose of the Study
Physiotherapy treatment, for the purpose of this study, refers to chest physiotherapy in the form of ACTs and exercise which are common treatment modalities for all adults with CF. The study excludes physiotherapy treatment for urinary incontinence and musculo-skeletal problems as they are not universal problems in the adult CF population. The study does not seek to investigate the efficacy of physiotherapy treatments. All recommended treatments for the study participants were based on clinical judgement and the best evidence-based practice available at the time.
1. 4. Adherence
1. 4. 1. Adherence to Treatment in Cystic Fibrosis
Poor adherence to treatment in CF is prevalent and attempting to improve it is challenging. Poor adherence can potentially result in sub-optimal health outcomes, increased healthcare costs and hospitalisation in addition to a reduced QoL, although to-date there have been no studies undertaken that directly prove a between link these factors. Adherence is a complex area of study, from which there is as yet no consistent single reason or set of predictor variables to emerge, that explain why
14

people with CF engage in adherent, partially adherent or non-adherent behaviours. Koocher, McGrath and Gudas (1990) described three types of non-adherence behaviours from CF treatments: firstly those who have an inadequate knowledge or a lack of understanding of the information available, secondly those who present with psychosocial resistance and thirdly those who demonstrate educated non-adherence, i.e. by making an informed choice not to carry out treatment. Lask (1994) however proposed that adherence can be categorised as behavioural rather than cognitive. He classified those who were non-adherent as ‘refusers’ who make no effort to conceal their non-adherence; “procrastinators” who will admit to only occasional omissions and ‘deniers’ who will not admit to non-adherence. However, White, Stiller and Haensal (2007) in their study on adherence to physiotherapy in CF did not classify their study population in terms of ‘adherence’ but as having an ‘acceptable frequency of treatment’. There needs to be a definition of, and criteria for, adherence which accurately reflects behaviour, in order to facilitate the development of evidence-based practice for adherence to physiotherapy for adults with CF. Kettler et al. (2002) proposed that in future the merger of medication and health monitoring technologies could assist in behaviour change and give a more objective means of identifying and measuring any changes.
Previously adherence to treatment was seen from a professional ‘expert’ perspective, where recommendations were made and the patients were expected to carry them out. Invariably this would present a dilemma, because if patients perceived that the treatment was of no benefit to them, or was too complicated and time consuming, their ability to adhere to it would be compromised (Daniels, 2010; Myers & Horn, 2006). The words ‘compliance’ and ‘adherence’ have been used interchangeably in the medical literature with more recent studies favouring adherence. Meyers and Midence (1998) in their study on adherence to physiotherapy in CF, quoted Leventhal (1993) who proposed that the conceptual shift from compliance to adherence represents an important first step in moving away from roles emphasising obedience to instructions towards models emphasising independence and self-regulatory activity, i.e. a person with CF may make an ‘educated’ decision not to continue with treatment (Abbott & Gee, 1998; Lask, 1994). The expectation of total adherence is unrealistic, yet to date, an acceptable level of non-adherence for each treatment regimen has not been established.
Previously, adherence studies had focused on children and their family/carers but due to increasing longevity, studies into the problems which adults experience are emerging. Bucks et al. (2009) in their report quoted a number of studies highlighting possible factors that influence adherence to treatment in CF, including lack of
15

knowledge about the disease (Ievers et al., 1999), locus of control and health beliefs (Carr, Pryor, Smith & Partridge, 1996; Myers & Myers, 1999), self-efficacy (Czajkowski & Koocher, 1987), perceived disease severity (Abbot, Dodd, & Webb, 1995; Gudas, Koocher, & Wypij, 1991), degree of optimism (Gudas et al., 1991), coping style (Abbott, Dodd, Gee, & Webb, 2001), support (Abbott, Dodd, Bilton, & Webb, 1994), the burden of carrying out time consuming treatment that impacts on a persons QoL (Abbott et al., 1994; Conway et al., 1996; White et al., 2007) and the perceived effectiveness or otherwise of physiotherapy treatment (Myers & Horn, 2006). The impact of these factors on the ability of adults to adhere to treatment have yet to be fully investigated.
1. 4. 2. Adherence to Physiotherapy Treatment in Cystic Fibrosis
Non-adherence to physiotherapy treatment can reduce the benefits of good medical care (Dodd & Prasad, 2005) and potentially lead to more a rapid deterioration in clinical status, more frequent hospitalisation, increased healthcare costs and reduced QoL. Although physiotherapists recommend best practice it cannot be taken for granted that the patient will adhere to a recommended treatment if they perceive no clinical benefit from it. If adults with CF are not adhering to treatment they need to be identified so that scarce physiotherapy resources are efficiently and effectively utilised, and appropriate educational strategies put in place to potentially optimise adherence and thereby potentially bring about improved health outcomes and reduced health care utilisation. However, to date there is no conclusive evidence of a relationship between adherence to chest physiotherapy and long-term outcomes (van der Schans et al., 2009).
Adherence behaviours are not clearly understood. The factors influencing adherence to physiotherapy treatment in CF are multi-factorial and are outlined below:
No Cure – There is currently no cure for CF, therefore physiotherapy treatment is palliative with the aim of delaying for as long as possible the onset of debilitating chest infections and encouraging the promotion of health and well being through exercise. The consequences of there being no cure for CF can have a significant impact on peoples’ health beliefs as ultimately the disease will lead, in the majority of cases, to an early death.
Health Outcomes – Research has shown that adherence to treatment in CF is associated with improved pulmonary status and increased longevity (Abbott, Havermas, & Hart, 2009; Bucks et al., 2009), therefore promoting adherence
16

through the development of evidence-based patient education strategies is an essential part of the treatment of CF.
Health Beliefs – Adults with CF who have positive health beliefs and an external locus of control are more likely to adhere to treatment (Bucks et al., 2009; Carr, Pryor, Smith, & Partridge, 1996), as they would think that what they do has a positive impact on the course of their disease. If they have negative health beliefs, with an internal locus of control, they are more likely to think that whatever they did will make no difference as there is no cure for CF. This approach would compromise their ability to adhere to physiotherapy treatment.
CF – Although a life limiting disease, people with CF may not feel ill and this can impact on their ability to adhere to physiotherapy treatment from which they may feel no discernable clinical benefit nor an apparent need when they are feeling well (Huyard, 2008).
Quality of Life (QoL) – Adults with CF are living longer but only as a result of complex and time consuming treatment programmes which can impact on their QoL. Adults make decisions about which treatments they are going to undertake in order to lead as normal a life as possible (Abbott et al., 1994; Daniels, 2010).
Perceptions of Physiotherapy Treatment – Physiotherapy treatment has been perceived by some non-adherent adults with CF as being ineffective (Abbott et al., 2009; Daniels, 2010), and if people do not understand the benefits of treatment they are unlikely to do it. By their very nature ACTs are repetitive and have been perceived as “boring” (Carr et al., 1996; Myers & Horn, 2006). However recent guidelines (ACPCF/CF Trust, 2011; Bott et al., 2009; Flume et al., 2009) support the use of ACTs to improve sputum clearance, and the need for them to be carried out on a daily basis.
Lack of knowledge – if people with CF do not have sufficient knowledge or understanding of their condition and the benefits that treatments can bring their adherence can be compromised.
These factors mentioned above, combined with the time consuming nature of treatments for CF, can compromise adherence.
1. 5. Classification of Adherence for the Purpose of the Study
17

There is no universally accepted definition of the term ‘adherence’ and how it can be measured in relation to physiotherapy treatment for CF, therefore for the purposes of this study ‘adherence’ has been classified by the researcher/practitioner as:
Adherent - that which has been agreed between the researcher/ physiotherapist and the participant and the participant reports that they are implementing it.
Partial Adherent - that which has been agreed between the participant and the physiotherapist but the participant reports that they are only partially implementing it.
Non-Adherent - that which has been agreed between the physiotherapist and the participant but the participant reports that they are not implementing it, and participants who report that they do not do any physiotherapy.
This classification of adherence is subjective. The recording of adherence is dependent upon the physiotherapist’s judgement, the patient’s honesty, memory and how accurately they carried out the treatment. Treatment can be carried out but not competently, or the patient may believe they are doing it competently but the therapist would consider it of a poor standard.
As discussed, people with CF may not adhere to physiotherapy treatment for a variety of reasons (Christian, 2007) such as no obvious clinical benefit, they do not see the need to do physiotherapy, it is too time consuming to fit it into their life styles, it is repetitive and boring. These reasons do not form sub-divisions of the classification of non-adherence for the purposes of this study. The issues surrounding the problems of adhering to physiotherapy are explored as part of the study and therefore do not form part of the categorisation.
1. 6. Self-Management Programmes in Chronic Disease
In recent decades awareness of the need to address chronic illnesses through self-management and other approaches in order to minimise the distress and other costs they impose, has risen up the healthcare agendas of all ‘rich world’ nations (The Kings Fund, 2010). The focus on disease self-management is an important conceptual advance in the understanding of chronic illness and improving health outcomes (Holman & Lorig, 2004; Warsi, Wang, La Valley, Avorn, & Solomon, 2004). The characteristics of chronic disease are:
No cure
18

Managed over a period of time Undulating course Obscure prognosis Need for continual patient engagement in their health care Patient and the professional working in partnership Patients educated about their disease can apply their knowledge to guiding their
own disease management, with the healthcare professional acting as a teacher to facilitate learning (Holman & Lorig, 2004).
These concepts have been advocated in government initiatives such as the “Expert Patient” (DoH, 2007) where patients with a long term condition are given the necessary knowledge and skills to be empowered to become active co-partners with the professional in order to take increasing responsibility for their healthcare, so that adherence is optimised and health care outcomes improved.
Self-management has been defined as collaboratively helping patients and their families to acquire the knowledge, confidence and skills to manage their condition and is increasingly important given the rising burden of chronic illness and the resulting impact on heath services (Harris, Williams, Dennis, Zwar, & Powell- Davis, 2008).
The aim of self-management in chronic disease is to:
Increase adherence to treatment Change behaviour Improve knowledge and skills Empower to manage their condition Reduce unnecessary visits and admissions to hospital Improve healthcare delivery Optimise health care resources Optimise health outcomes Improve QoL
Disease-specific models of self-management have been delivered by health care providers for asthma, diabetes, arthritis, chronic lung and cardiac disease (Kralik, Koch, Price, & Howard, 2004; The Kings Fund, 2010; Warsi et al., 2004). They have proved to be well used and effective in improving disease-specific intermediate health outcome measures such as glucose control in diabetes and blood pressure in hypertension. In a study by Lorig, Sobel, Ritter, Laurent, & Hobbs (2001) the
19

effectiveness of a self-management programme for people with chronic disease was compared to those who did not have the ability to self-manage their condition. The study demonstrated that the group that did not have the ability to self-manage themselves showed limitations in exercise tolerance, cognitive symptom management, communication with physicians, self-reported general health, health distress, fatigue, disability, social/role activities and QoL. Those who self-managed their condition had reduced medication costs, reduced hospitalisation and an improved QoL, the results of which persisted for as long as three years (Lorig et al., 2001). During the 1990s Sobel, Lorig, & Hobbs (2002) developed a Chronic Disease Self-Management Program (CDSMP) to provide generic self-management courses. The development of the new programme involved participants of varied ages and with a range of primary and co-morbid conditions. The CDSMP was based on three underlying assumptions
patients with different chronic diseases have similar self-management problems and disease-related tasks
patients can learn to take responsibility for the day-today management of their disease(s)
confident, knowledgeable patients practising self-management will use fewer healthcare resources.
The strongest evidence for the impact of self-management education on hospital admissions and the use of the emergency departments comes from studies in the United States of America (USA) which have relatively less developed primary care gate keeping and therefore greater scope for self-management to affect hospital admission rates (The Kings Fund, 2010). In the UK the DoH has encouraged self-management through its Expert Patient Programme (2001b) and in its report ‘Self Care – A Real Choice’ (DoH, 2005) which argued that there is growing evidence that supporting self-care can help to improve health and QoL leading to an increase in patient satisfaction and a reduction in the use of services and health care costs. With the right support people can be empowered and learn to be active participants in improving existing symptoms, avoiding flare-ups, slowing deterioration, preventing the development of complications and helping them achieve a better QoL, whilst living with and taking care of their conditions (DoH, 2005).
In respiratory conditions the benefits of self-management for asthma is a well developed and recognised treatment modality. Gibson et al. (2002a; 2002b), in their work on two Cochrane Reviews ‘Self-management education and regular practitioner review for adults with asthma’ and ‘Limited information only patient education programmes for adults with asthma’, reported that training in asthma self-
20

management, which involves self-monitoring coupled with regular medical reviews and a written action plan, appeared to improve health outcomes and QoL more than having a limited information only education programmes.
Although self-management being taught in groups for conditions such as asthma, diabetes, chronic respiratory disease and heart disease has proved to be very effective, this management approach would contravene the CF Trust Guidelines on Cross Infection (2004a;2004b). People with CF are advised not to mix with each other due to the risk of cross infection with Pseudomonas Auringeosa and Cepacia (CF Trust, 2004a; 2004b). Self-management on an individual basis supported by literature, the internet and tele-healthcare for monitoring purposes would be the most effective means of delivering self-management programmes for people with CF.
Self-management programmes need to be personalised to meet the patient’s needs, to be achievable and to have key indicators of what to do when unwell (Holman & Lorig, 2004). For these outcomes to be realised the patient needs to be educated so that they have sufficient knowledge and skills to carry out their healthcare programmes.
1. 6. 1. Self-Management Programmes in Cystic Fibrosis
Self-management programmes have been developed for children with CF and their families but they are not applicable to adults who are independent in their own care. However self-management programmes for adults with CF are gaining prominence as an effective way of giving people the necessary knowledge and skills to empower them to be more responsible for their health care in order to improve their adherence to treatment. These self-management programmes were aimed at people whose disease had been diagnosed later in life and for whom non-adherence would have swiftly produced unpleasant signs and symptoms (The Kings Fund, 2010; Holman & Lorig, 2004; Warsi et al., 2004). This would not be the case with the current CF adult population because when they were diagnosed with CF it was considered to be a disease of childhood due to early mortality. Apart from a few who were diagnosed in late childhood or early adulthood, adults with CF would have grown up with a life limiting disease yet they may not have felt unwell. If people with CF do not carry out their physiotherapy treatment they may not feel any immediate detrimental effects and if they do their physiotherapy treatment they may not feel clinically better, which can make adherence to treatment more difficult if there is no detectable change in clinical status.
21

CF poses a challenge for self-management in view of the high level of daily treatment activity for adults regardless of age or disease severity. Sawicki, Sellings and Robinson (2009) identified in their Project on Adult Care in CF (PAC-CF), that the time spent on airway clearance rather than gender, age or pulmonary function, was associated with a higher perceived treatment burden which could compromise the efficacy of a self-management programme. Although a patient may have a good knowledge of CF and of the need to do physiotherapy it cannot be assumed that they will carry out their treatment (Abbott & Gee, 1998). Connversely, some patients may have a poor level of knowledge yet adhere conscientiously to treatment (Abbott & Gee, 1998) while Sawicki et al. (2009) noted that the adults were making decisions as to which treatment to do each day and there were acceptable reasons why they did so.
One of the key aspects of a successful self-management programme is to educate the patient to ensue that they have the necessary knowledge and skills to fully understand what is involved, why they are doing it and to make changes to their treatment within agreed limits. Sawicki et al. (2009) identified in their study on self-management in CF, that there was a lack of awareness of what self-management involved and that people with CF need to be empowered to be more involved in planning their own healthcare.
1. 6. 2. Patient Education in Self-Management Programmes
In a traditional model of patient education the professional was seen as the expert with the patient taking a more passive and compliant role. In recent years, particularly with the development of self-management programmes, the humanistic concepts of education, where the teacher acts as a facilitator by working in partnership with the learner, have been given increasing prominence (DoH, 2007; Knowles, 1989). The benefits of a humanistic approach are its motivational characteristics, the promotion of patient-centred learning, and the facilitation of the therapist and the patient working together to define problems, the development of solutions and implementation of jointly agreed goals (Dreeben, 2010). The humanistic theory of learning is dependent upon the patient being engaged and empowered to work in partnership with the professional so that they have greater ‘ownership’ of their health care, and will potentially be more adherent to treatment (DoH, 2007).
1. 6. 3. Empowerment in Self-Management Programmes
Empowerment reflects a shift of emphasis in the delivery of health care from patients being recipients of care to becoming empowered and liberated to play a central role in
22

decisions about their illness (Bradshaw & Bradshaw, 2004; DoH, 2010; Wensing, 2000). Empowerment has been defined by Rodwell (1996, p. 300) as
The process of enabling or imparting power transfer from one individual or group to another. It includes the elements of power, authority, choice and permission.
Empowerment is seen as a process of transferring power and includes the development of a positive self-esteem and the recognition of the worth of self and others (Mason, Backer, & Georges, 1991). Although the concept of the relationship between the professional and the patient is based on equality, in practice this cannot be the case in a health care setting (Hudson, 1999; Hugman, 1991; Webb & Tosell, 1991). The professional has skills, knowledge and access to facilities and equipment which the patient will need to avail themselves of, thus creating an unequal balance of ‘power’ with the patient in the dependent position. The concept of ‘user empowerment’ (Hudson, 1999) is at the heart of addressing the unequal power relations in the traditional medical model of care by attempting to redress this imbalance and putting the wishes of the user at the heart of the service. There is an implicit assumption that some choices are better than others and that healthy choices are rational choices but that may not be the case (Rogers, 2005). Patient choice is influenced by their health beliefs, i.e. how effective they perceive their treatment to be and the impact it has on their lives.
1. 6. 4. Health Belief Model in Self-Management Programmes
The Health Belief Model (HBM) has been a useful and enduring theoretical model associated with preventative health behaviours and has been used as a tool to predict adherence. Willis and Campbell (1992, p. 82) define the HBM as:
Behaviour is predicted based on the value one places on an outcome and on one’s expectation that a given behaviour will lead to that outcome.
The HBM has limitations as it does not account for diversity of motives and it lacks standardised measurement tools. Some studies have placed considerable emphasis on the HBM (Carr et al., 1996) while others (Abbott, et al., 1996; Myers & Myers, 1999) have focused on attempting to predict behaviour. By being aware of the patient’s health beliefs the health professional would be able to determine how a patient makes health care decisions and potentially be able to predict levels of adherence to treatment. Health professionals could also help to address negative health beliefs in order to promote better adherence to treatment.
23

One of the most salient features of the patient’s health beliefs is their ‘locus of control’. Moreau (2002, p. 13) defined locus of control as ‘a patient’s perception of his ability to bring about change’. A patient with a strong locus of control who feels they are able to influence events around them is considered to have an internal locus of control, while a patient who has a passive acceptance of a situation and believes that their circumstances are being controlled by other factors has an external locus of control. Studies into adherence to physiotherapy in CF found that health beliefs influenced the ability to adhere to treatment (Carr et al., 1996; Myers & Horn, 2006). These two different sets of loci of control and health beliefs require different educational approaches to facilitate learning in order to optimise the ability to adhere to treatment.
1. 6. 5. Self-Management Physiotherapy Programmes for Adults with Cystic Fibrosis
To date no defined self-management physiotherapy programmes (SMPP) have been developed for adults with CF. The purpose of this study was to develop a SMPP and to evaluate its effectiveness in optimising the ability to adhere to treatment.
1. 7. Practitioner-Based Research
Patient education is an essential component of a successful self-management programme. This unique exploratory study questioned the role of the physiotherapist in patient education in CF. It was by critically enquiring into the role of the physiotherapist in patient education that an opportunity for reflective practice arose. Reflective practice was first conceptualised by Schon (1987) in an educational context. He advocated that it was a retrospective process concerned with thinking about action. By conducting research into a situational work based problem the physiotherapist is developing a practitioner-based research approach to the professional role of the physiotherapist. This practitioner-based research model is seen (Holloway & Race, 1993) as a means of contributing to the theoretical basis of practice. By conducting an exploratory research study, theory can subsequently inform clinical practice. Holloway (1994) argues that the practitioner-based model avoids the separation of theory and practice and contributes to the development of the professional role. The CSP (2007) and the Health Professions Council’s Standards of Proficiency for Physiotherapists (2007) encourage EBP as it closes the gap between theory and practice and thereby achieves the government healthcare objectives (DoH, 2010) of improving quality of care.
24

In this study the role of the physiotherapist in CF patient education will be challenged by moving from the traditional medical model, where the professional is the expert and the patient takes a passive role, to a humanistic psycho-social model where the physiotherapist acts as a facilitator, empowering the patient to work in partnership with the professional in order to optimise the ability to adhere to physiotherapy treatment see Fig. 1.1. below.
Traditional Medical Model Role of the Physiotherapist(expert) Educational Role (passive) Model of the Learner (behavioural)
Psycho-Social Model Role of the Physiotherapist (facilitator)
Educational Role (empowerment) Model of the Learner (behavioural)
Fig. 1. 1. The role of the physiotherapist in cystic fibrosis
1. 8. Rationale for the Study
CF is a complex life threatening disease requiring daily burdensome time-consuming treatment of which physiotherapy is the least liked component (Abbott, Havermas & Hart, 2009; Daniels, 2010). Physiotherapy, which is an essential part of a CF treatment programme, aims to keep the chest clear of secretions, promote fitness and well being and thereby improve health outcomes and QoL in addition to potentially reducing healthcare costs. Poor adherence to physiotherapy in CF is a well recognised problem (Daniels, 2010; Ireland, 2003; White, Stiller & Haensal, 2007) the consequences of which can result in a faster rate of decline necessitating increased hospitalisation and health care costs and a reduced QoL and life expectancy.
The rationale for this study is to test a model for improving treatment adherence through the development and evaluation of a SMPP for adults with CF, which in concequence would potentially bring about improved health ooutcomes, reduced health care costs, a better QoL and additional life expectancy. No such research has been undertaken to date, so this study will contribute original knowledge to the evidence base for physiotherapy clinical practice.
25

1. 9. Professional Doctorate
This study has been undertaken as a part of the researcher’s Continuing Professional Development (CPD) programme. The CSP actively encourages research as part of developing professionalisation (CSP, 2010) which is the process whereby any new occupational group takes on the characteristics of a profession (Bithell, 1999). The emphasis of a professional doctorate (PD) is that learning is based on professional practice and work-based experience, requiring and enabling students to draw on their professional activity within their learning and to relate their learning back to their practice (CSP, 2010). A PD (University of Portsmouth, 2011) advocates the need for health care professionals to actively engage in the development of clinical practice through evidence-based research, appraisal, evaluation, leadership in the professional field, the development of expert practitioners, professional autonomy and reflective practice. The study enabled the learning outcomes of the course to be effectively utilised in the development of professional expertise and to have that expertise recognised within an academic context.
The development and design of this unique clinical work-based study fulfils the attributes of a PD by investigating a complex physiotherapy clinical problem that requires critical thinking, reflective practice and autonomous judgement to develop a new and improved model of clinical practice that contributes to improved health care outcomes. The development of the study will provide an original contribution to physiotherapy practice, the results of which will be disseminated to a variety of audiences.
1. 10. Study Aims
The study aims to improve adherence to physiotherapy in order to improve health care outcomes, reduce health care costs and ultimately improve QoL. This study sought to investigate the complex problems that adults with CF have in adhering to physiotherapy treatment by establishing, from their perspective, what these problems are and to develop an educational strategy in the form of a SMPP to potentially optimise their ability to adhere to physiotherapy treatment. The study was confined to chest physiotherapy and exercise and did not attempt to investigate the efficacy of current physiotherapy clinical practice. If the SMPP proves to be effective in improving adherence to physiotherapy then a new model of physiotherapy clinical practice can be postulated.
26

The Research Question
Will the newly developed SMPP optimise the ability of adults with CF to adhere to physiotherapy treatment?
Aims
1. To investigate the problems that people with CF have with adherence to physiotherapy treatment prior to the study.
2. To investigate the level of adherence to physiotherapy treatment prior to the study.
3. To develop and test the effectiveness a new SMPP.
4. To evaluate the impact of the new SMPP on adherence to physiotherapy treatment.
5. To postulate a new model of clinical practice for the future physiotherapy treatment and management for people with CF.
The purpose of this work based study was to contribute to improved health outcomes for adults with CF through the conduct and application of relevant high quality research. The intention was to improve the scope, relevance and quality of physiotherapy practice, to inform policy and clinical practice in CF health care, to contribute to the development of knowledge-based physiotherapy clinical practice and to ensure that the benefits of the research study are systematically and effectively translated into practice. These features fall within the scope of good professional practice, which is part of the government’s drive to develop clinical governance (DoH, 2010) and they contributed towards the requirement of a PD by enabling the researcher to be recognised as an expert practitioner.
27

CHAPTER TWO – LITERATURE REVIEW
2. 0. Introduction
The aim of this chapter is to review the literature on CF covering the following topics:- the efficacy of chest physiotherapy, adherence to physiotherapy and adherence to self-management programmes. This will be achieved by firstly explaining the search strategy, identifying the key terms used in the search and the inclusion and exclusion criteria, secondly discussing how the papers were appraised, and thirdly reviewing the papers.
2. 1. Search Strategy
The search strategy used the following techniques:
Bibliographical Database Search
A systematic search was conducted in order to find relevant and specific literature for the review. The databases and websites accessed in this search are listed in Fig. 2.1 and Fig. 2. 2 below.
DATABASES AHMED
CINAHL
Cochrane Database of Systematic Reviews (CDSR)
DARE (Database of Abstracts of Reviews of Effectiveness) produced by NHS Centre for Reviews and Dissemination (CRD)
DoH (Department of Health)
Embase
British Nursing Index (BNI)
Health STAR (Health Services, Technology, Administration and Research)
HMIC (Health Management Information Consortium)
Medline
NHS RD (Research & Development Programme)
NHS HTA (Health Technology Assessment) Programme
NIHR (National Institute for Health Research)
NICE (National Institute for Health & Clinical Excellence)
Physiotherapy Evidence Database (PEDro)
PsychINFO
Fig. 2. 1. Databases
28

WEBSITES ACPCF (Association of Chartered Physiotherapist in Cystic Fibrosis)
ACPRC (Association of Chartered Physiotherapists in Respiratory Care)
CSP (Chartered Society of Physiotherapy)
CF Trust (Cystic Fibrosis Trust)
British Thoracic Society (BTS)
Public Health Resource Unit
Fig. 2. 2. Websites
Search Terms
Searches were performed using thesaurus terms and key words designed to find articles investigating the issues surrounding adherence to physiotherapy in CF and self-management programmes. Specific terms were used as outlined in Fig. 2. 3. The thesaurus terms ensured case synonyms such as “physiotherapy” and “physical therapy” were not inadvertently omitted.
Thesaurus Terms Key Words
Cystic Fibrosis Physiotherapy Adherence Patient Education Self care Health Beliefs Patient Compliance Physical Therapy Attitude to Health
Health Beliefs Self-Management Empowerment Compliance Adherence/Adhere
Fig. 2. 3. Search Terms
Thesaurus terms and key words terms were combined with the Boolean operators ‘AND’, or ‘OR’ as outlined in Appendix A. Truncation was used on key words to expand the sensitivity of the word stem. The process for retrieving the literature is outlined in Appendix B. The search strategy (Appendix C) was re-run at six-monthly intervals to update the literature search.
Inclusion and Exclusion Criteria
Articles were included if they met the following criteria:
29

Time frame of up to 30 years as treatment of CF has developed and life expectancy increased. Earlier studies would not be relevant as there was only a small adult population and studies into adherence behaviours had not been undertaken
Only English language papers, as translation was not possible due limited funding
Studies involving children and adolescents were included if they were relevant Nursing and psychological literature databases were deliberately selected to
enable the study to have a comprehensive perspective by giving consideration to the point of view of people who have CF
Qualitative and quantitative evidence was not limited to specific study designs Hand Searching
In addition to the search of electronic databases, the University of Southampton Health Services Library, the University of Portsmouth Library, the University of Oxford Medical Library and St. Mary’s Hospital, Isle of Wight, Health Services Library resources were searched for relevant books, pamphlets, journals and periodicals and they provided full text copies of relevant papers.
2. 2. Methodology
2. 2. 1. Critical Appraisal Tools
In order to be objective in reviewing the retrieved literature several methodological appraisal tools were considered, such as the Scottish Intercollegiate Guidelines Network (SIGN), the Journal of the American Medical Association (JAMA) user guides and the Sheffield Evidence for Effectiveness and Knowledge (SEEK), with each having their own strengths and weakness. All of these methodological tools were unsuitable as critical appraisal tools (CATs) for this thesis. SIGN was more appropriate for the development of practice guidelines, while SEEK acts as a electronic gateway for information on evidence-based resources but does not provide a tool to evaluate effectiveness, and JAMA user guides were more appropriate for medical models of treatment. In view of these limitations the Critical Appraisal Skills Programme (CASP) (www.caspinternational.org/) was chosen as it provided a common methodological approach to each of the research frameworks. It was more suitable for a clinical decision making approach as it seeks to make sense of research evidence in order to put knowledge into practice.
30

CASP is based on the guidelines produced by the Evidence Based Medicine approach devised by clinicians at McMaster University and colleagues across North America. The tools were adapted from the work carried out by Oxman, Cook and Guyatt (1994) who developed a users guide to appraising medical literature. The aim of the CASP approach is to systematically examine research evidence with a view to assessing its validity, results and relevance before using it to inform a decision. Critical appraisal (Hill & Spittlehouse, 2001) is an essential part of evidenced-based clinical practice as it includes the process of systematically finding, appraising and acting on evidence of effectiveness. Critical appraisal allows sense to be made of research evidence with the aim of closing the gap between research and practice. It is the process of assessing and interpreting evidence by systematically considering its validity, results and relevance.
Although the CASP system is a strategic approach more limited than the protocols used for groups such as the Cochrane Collaboration (www.thecochranelibrary.com), it nevertheless fulfils the essential elements of a structured and systematic framework for evaluating research studies. The literature is identified according to an explicit search strategy, selected according to defined inclusion and exclusion criteria and is evaluated against consistent methodological standards. The research studies were divided into methodological groups so that the appropriate CASP appraisal tools could be used:-
Meta-analyses ● Case control
Systematic reviews ● Economic studies
Cohort studies ● Qualitative studies
The appraisal of a paper resulted in a level of evidence being given. The methodological assessment was based on a number of key questions that focused on those aspects of the study design that research had shown to have had a significant influence on the validity of the results reported and the conclusions drawn. These key questions differ between study types and a range of check lists was used to bring a degree of consistency to the assessment process.
An example of key preliminary questions for systematic reviews are outlined below:
Is the study valid? What are the results? Will the results help locally?
31

These key preliminary questions were then followed by more detailed questions which acted as check lists (Appendix D). These CASP check lists were subjected to evaluation and adaptation to meet the requirements for a balance between methodological rigour and practicality of use. How the hierarchy of evidence was graded is outlined below in Table 1.
2. 2. 2. Hierarchy of Evidence
The hierarchy of evidence used was based on the Scottish Intercollegiate Guidelines Network (SIGN, 2008), with each study having a level of evidence accompanying it.
Table 2. 1. Levels of Evidence Based on SIGN (2008)
Level Type of Evidence
I++ High quality meta-analysis, systematic reviews of randomised Controlled trails (RCTs) or RCTs with a very low risk of bias.
I+ Well conducted meta-analysis, systematic reviews, or RCTs with a low risk of bias.
I- Meta-analysis, systematic reviews, or RCTs with a high risk of bias
2++
High quality systematic reviews of case-control or cohort studies. High quality case-control or cohort studies with a very low risk of confounding or bias and a high probability that the relationship is casual
2+ Well-conducted case-control or cohort studies with a low risk of confounding orbias and a moderate probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a significant risk that the relationship is not causal
3 Non-analytical studies (e.g. case reports, case series )
4 Expert opinion
2. 3. Analysis of the Literature
The analysis of the literature was divided into 4 sections, each with an accompanying table of evidence presenting key studies:-
Physiotherapy Airway Clearance Techniques (ACTs) for adults with CF Adherence to treatment for adults with CF Exercise in the management of adults with CF Self-management for adults with CF
2. 3. 1. Physiotherapy ACTs for Adults with cystic fibrosis
Table 2. 2. Reviewing the key evidence for ACT’s is presented on p. 34
32

Although it was not the remit of this study to investigate the efficacy of chest physiotherapy using ACT, a review of the literature was undertaken in view of it being perceived as ineffective or unnecessary by some adults with CF (Abbott, et al, 1994; Daniels, 2010; Llorente, et al., 2008). Questioning the effectiveness of ACTs in CF can compromise the ability to adhere to physiotherapy. Of the six papers reviewed five were Cochrane Reviews each of which commented on the poor quality of the studies, the lack of universally agreed definitions and the variety of outcome measures, making meta-analysis difficult to undertake. Each of the reviews were rigorous and systematic in their approach to selecting studies which were valid and reliable enough to influence physiotherapy clinical practice. Although it is well recognised that the physiotherapy management of CF is burdensome, to date airway clearance studies have shown little interest in patient reported outcomes, which needs to be addressed if adherence to treatment is to be optimised (Daniels, 2010). The five Cochrane Reviews are discussed below:
Firstly, Robinson, McKoy, Saldanha, and Odelola (2010) assessed the efficacy of the active cycle of breathing technique (ACBT) compared to other ACTs. Of the initial 17 studies considered, only four, involving 98 participants met the inclusion criteria. The review concluded that the ACBT was comparable to other ACTs in outcome measures such as patient preference, lung function, sputum weight, oxygen saturation and the number of pulmonary exacerbations. The review was hampered by the lack of long term randomised controlled studies, insufficient data and the lack of consistency in outcome measures which made comparisons difficult.
The second review (Morrison & Agnew, 2009) investigated oscillating devices and reviewed 34 studies, involving 859 participants, which met the inclusion criteria. Oscillating devices prevent premature closure of the bronchi by loosening secretions in order to facilitate detaching mucus from the airway walls (IPG/CF, 2009). The duration of these 19 studies lasted from one week to one year.
The data was insufficient to perform a meta-analysis. The lung function test of the FEV1 was the most frequently used outcome measure. The review concluded that there was no clear evidence that oscillating devices were more or less effective than any other form of airway clearance. The measurement tools however may not have been sensitive enough to detect changes that could have distinguished between devices.
33

Table 2. 2. Physiotherapy airway clearance techniques
TITLE Author YEAR TYPE OF ARTICLE
SUMMARY OF THE EVIDENCE LEVEL
Cochrane Review: Conventional chest physiotherapy compared to other airway clearance techniques for cystic fibrosis
Cochrane Review: Positive expiratory pressure physiotherapy for airway clearance in people with cystic fibrosis
Cochrane Review: Chest physiotherapy compared to no chest physiotherapy for cystic fibrosis
Cochrane Review: Oscillating devices for airway clearance in people with cystic fibrosis
Cochrane Review: Active cycle of breathing technique for cystic fibrosis
Beyond postural drainage and percussion: Airway clearance in people with cystic fibrosis
Main, Prasad, & van der Schans
Elkins, Jones, & van der Schans
Van der Schans, Prasad & Main
Morrison & Agnew
Robinson, Mckoy Saldanha, & Odelola
Pryor, Tannenbaum, Scott, Burgess, Cramer, Gyi & Hodson
2009
2009
2009
2009
2010
2010
Systematic Review
Systematic Review
Systematic Review
Systematic Review
Systematic Review
Randomised Controlled Trial
83 publications identified;29 met the inclusion criteria (15 data sets); 475 participants . Outcome measure – standard lung function tests. Insufficient evidence to confirm or exclude any differences between CCPT and other airway dependant techniques in terms of respiratory function but this may have been reflected insufficient evidence rather than equivalence between methods.
40 studies identified,;25 met the inclusion criteria; 507 participants. No clear evidence that PEP was a more or less effective intervention than other forms of physiotherapy. Limited evidence
126 trials identified; 6 met the inclusion criteria; 66 participants. Airway clearance techniques have short-term effects in terms of increasing mucus transport. No evidence was found on which to draw conclusions concerning the long term effects.
78 references identified; 34 met the inclusion criteria; 859 participants. . Insufficient data to perform a meta-analysis. Fev1 most frequently used outcome measure. Conclusion – no clear evidence that oscillating devices wer any more effective than any other airway clearance device.
58 studies identified; 17 met the inclusion criteria; 364 participants. There is insufficient evidence to support or reject the use of ACBT over any other airway clearance technique. Longer term studies are needed to more adequately assess the effects of ACBT on outcomes important for patients such as quality of life and patient preference.
Prospective RCT (n = 75). There was no statistical difference between 5 airway clearance techniques. Patient preference was important
1++
1++
1++
1++
1++
1+
34

The third review (Main, Prasad, & van der Schans, 2009) compared conventional chest physiotherapy (CCPT) to other ACTs and identified 83 studies of which 29, involving 474 participants, were selected as they met the search criteria of being a randomised or quasi-randomised trial or a cross-over design. Studies that were undertaken during acute exacerbations demonstrated significant gains in respiratory function, measured by standard lung function tests, irrespective of the ACT used. The review was unable to determine any advantage of CCPT over any other ACT in terms of respiratory function. The studies reported individual participant preferences for technique, with self-administered techniques being the most preferred. The lack of consistency in outcome measures precluded a meta-analysis being undertaken.
The fourth review (Elkins, Jones, & van der Schans, 2009) investigated the efficacy of positive expiratory pressure (PEP). PEP is the use of positive pressure at the end of expiration to keep the small airways open to facilitate sputum clearance. This review identified 40 studies of which 25, involving 507 participants, met the inclusion criteria. The quality of the studies was poor which limited the usefulness of the conclusions and prevented a meta-analysis being undertaken. Only nine studies recorded participant preference. The review concluded that there was limited evidence that PEP was preferred by participants compared to other ACTs, but this finding was from studies of low quality.
The fifth review (van der Schans, Prasad, & Main, 2009) investigated chest physiotherapy compared to no chest physiotherapy. Of the 126 studies reviewed six cross-over trials, with 66 participants, were eligible for inclusion. The studies were all of short duration, being less than seven days. The review did not distinguish between studies involving children and adults, thereby reducing its validity as the anatomy and physiology of adults and children are dissimilar. Studies were difficult to compare due to the variety of outcome measures including cough, sputum and radioactive tracer clearance. The study was able to conclude that ACTs do have short term effects in increasing mucus transport, which was assessed using objective measures, and therefore supported current clinical practice.
The five reviews (Elkins et al., 2009; Main et al., 2009; Robinson et al., 2010; Morrison & Agnew, 2009; van der Schans et al., 2009) concluded that ACTs had the short term effect of increasing mucus transport and that there appeared to be no advantage of either conventional chest physiotherapy (CCPT) or oscillating devices over other any other ACT in the primary outcome measure of lung function. No distinction was made in the conclusions indicating whether the studies involved
35

children, although this would have implications for validity when applied to adults as children would have had physical assistance from their parents/carers with shaking/vibrations to aid sputum clearance, and their anatomy and physiology is different. The reviews concluded that there was little evidence to show the long term effects in chest clearance, QoL, or survival but this may well reflect the paucity of evidence available to date.
Pryor et al. (2010) investigated the efficacy between five different ACTs used by adults with CF over a period of a year. The randomised controlled trial involved 63 participants. The primary outcome measure in their study was the lung function measurement of the forced expiratory volume in one second (FEV1). Although the study was careful in ensuring that the participant’s ACT was as accurate as possible, studies in respiratory physiotherapy are reliant on the participants’ self-reporting and therefore dependent on honesty, accuracy of technique and memory, which may be unreliable over a long period of time. The efficacy of physiotherapy is difficult to establish over a long period of time as treatment strategies for other aspects of CF treatment would influence the course of the disease. Pryor et al. (2010) concluded that there was no statistically significant difference in effectiveness between the five ACTs investigated, which therefore supported current physiotherapy practice.
With the exception of the Pryor et al. (2010) study there is a paucity of rigorous trials into the effectiveness of ACTs for adults with CF, with the few studies that have been conducted being underpowered (Marks, 2007), lacking in clarity as to which outcome measures are most useful for comparing various ACTs, and none longer than three months duration. The presentation of pulmonary function tests provides a more convincing efficacy (Yankaskas, Marshall, Sufian, Simon, & Rodman, 2004) and was used in the Pryor et al. (2010) study as a primary outcome. To date, the five Cochrane Reviews involving short term studies and one long term study of one year (Pryor et al., 2010) concluded that for adults with CF, physiotherapy ACTs are effective in facilitating chest clearance but with no one ACT being any more effective than any other.
2. 3. 2. Adherence to Treatment for Adults with Cystic Fibrosis
Table 2.3. Reviewing the key evidence for adherence to CF treatment for adults with CF is presented on p. 38.
Difficulties of assessing adherence
36

Studies relating to adherence to treatment in CF are difficult to compare due to the different aspects of treatment involved (e.g. physiotherapy or medication), resulting in increasing complexity and duration of daily treatment as the disease progresses. Adherence rates for each treatment are influenced by the difficulty of administering it and its perceived benefits. Studies into adherence are difficult to compare as there is a variable interpretation of terms used and treatment for CF changes, consequently cross-sectional studies into adherence cannot compare like with like. Studies into the management of chronic diseases found that adherence can vary according to factors other than disease severity (Myers & Horn, 2006; Myers & Midence, 1998) and that treatment complexity, which is relatively common in chronic conditions, can compromise adherence (Badlan, 2006; Bernard & Cohen, 2004).
In a review by Abbott et al. (2009) of thirteen papers on adherence to treatment in CF, they noted that poor adherence was common and the principle cause of treatment failure, resulting in faster disease progression, reduced survival and compromised medication dosage in clinical trials. Non-adherence rates varied considerably with higher adherence for pill taking but lower for more burdensome treatments such as chest physiotherapy (DiMatteo, Giordani, Lepper, & Croghan, 2002; Quittner, Modi, Lemanek, Ievers-Landis, & Rapoff, 2008). The wide variation in adherence rates are probably exacerbated by inconsistent approaches, a lack of definition of adherence and different methods of measurement used, thus making comparisons difficult. It is difficult to assess the adequacy of samples used in studies, particularly when a proportion of the sample has specific treatments. Many studies used convenience samples from single centres with no sample size justified.
There are several factors that compromise a critical appraisal of the literature on adherence to treatment in CF:-
Firstly, there is no consensus on the definition of adherence. Kettler et al. (2002), in their review of the literature on adherence to treatment in CF, concluded that there was no consensus of opinion on the definition of adherence in general, making studies difficult to compare.
37

Table 2. 3. Adherence to treatment for adults with CF
TITLE AUTHOR YEAR TYPE OF ARTICLE
SUMMARY OF THE EVIDENCE LEVEL
Predicting medical compliance among adolescents with cystic fibrosis
Medical compliance and coping with Cystic Fibrosis
Typologies on non-adherence in cystic fibrosis developmental and behavioural paediatrics
Treatment compliance in adults with Cystic Fibrosis
Non-adherence to treatment in cystic fibrosis
Difference perceptions of disease severity and self care between patients with cystic fibrosis, their close companions and physicians
Czajkowski & Koocher
Czajkowski & Koocher
Koocher et al.
Abbott et al.
Lask
Abbot et al.
1986
1987
1990
1994
1994
1995
Case control
Descriptive
Descriptive
Descriptive study
Descriptive
Descriptive
The assessment technique used offers a new avenue of approach in the prediction of non-compliance which in turn may enable the use of interventions to reduce patient’s morbidity.
There was an identifiable behaviour difference in coping skills between compliant and non-compliant patients which may prove useful to clinicians treating children with cystic fibrosis.
The conceptual framework of inadequate knowledge, psychosocial resistance and educated non-adherence could be put to clinical use in order to enhance diagnostic and treatment efforts.
The reported degree of compliance and reasons for poor compliance were treatment specific. Demographic and disease severity variables were not associated with compliance. Those involved in the care of patients with cystic fibrosis were able to predict compliance.
The recognition and management of non-adherence is complex and an important aspect of cystic fibrosis care. Successful treatment is dependant upon a correct and complete understanding of the underlying issues.
From the physician’s viewpoint, patients and close companions under estimate the severity of cystic fibrosis and over estimate patient self care.
2++
2++
3
3
3
3
38
Compliance with treatment in adult patients with cystic fibrosis
Adherence to medical treatments in adolescents with cystic fibrosis: the development and evaluation of family-based interventions
Adherence to physiotherapy and quality of life for adults and adolescents with cystic fibrosis
Psychological interventions for cystic fibrosis
Increasing adherence to cystic fibrosis treatment: a systematic review of behavioural techniques
Adherence to treatment in children and adolescent patients with cystic fibrosis
Conway et al.
Quittner et al.
Ireland
Glasscoe & Quittner
Bernard & Cohen
Zindani et al.
1996
2000(b)
2003
2008
2004
2006
Survey
Descriptive study
Literature review
Systematicreview
Systematic review of the literature
Case control
91 participants - self-completed questionnaire. Non-compliance is universal and should be recognised as normal behaviour. There are no reliable criteria for predicting any patients’ level of compliance. Treatment protocols should be planned around individual patient’s requirements, modifying treatment ideals where necessary according to the exigency and pattern of that patient’s lifestyle.
Behavioural scientists have made substantial progress in developing and evaluating family-based interventions that hold promise for improving adherence behaviours and family functions.
Longitudinal studies on individually tailored evidence-based treatment, accommodating patients’ health beliefs need to be undertaken in order to improve adherence to physiotherapy treatment and potentially a patient’s quality of life.
There is some evidence that behavioural interventions can improve emotional outcomes in people with cystic fibrosis and their carers. Multi-centre approaches are required to increase the sample size of studies in the psychological field and to enhance the power and precision of the findings.
Behavioural techniques provide a practical way to increase adherence to cystic fibrosis treatment regimens. Gender related differences should be examined.
Parental supervision and disease severity are likely to play a major role in adherence to treatment. A partnership with parents and families about the treatment plan might be important in improving adherence rate. Adherence to treatment is influenced by treatment that patient view as beneficial and/or leads to a decrease of symptoms.
3
2
3
1++
1+
-2
39

Young people living withcystic fibrosis: an insight into their subjective experience
Gender differences in treatment adherence among youth with cystic fibrosis; development of a new questionnaire.
Adherence to treatment in adolescents with cystic fibrosis. The role of illness perceptions and treatment beliefs
Adherence to the medical regimen: clinical implication sof new findings
Badlan
Patterson, Wall,Berge & Milla
Bucks, Hawkins, Skinner, Horn, Seddon & Horne
Abbott, Havermas & Hart
2006
2008
2009
2009
Non-experimental descriptive study
Survey
Survey
Meta-Analysis
Priorities in the life of the patient are likely to differ from those of healthcare professionals consequently total adherence to medical care will be compromised. Healthcare professionals need to understand that a degree of non-adherence is normal, necessary and acceptable. Patients want to be in control of their lives and be ‘normal’ which will result in a ‘trade off’ between treatment and leading a normal life.
Living with CF appears to have a greater emotional impact on girls compared to boys which may account for poorer pulmonary function among girls with CF. Low response rate of 58%
Support for self-regulatory model. Treatment beliefs and beliefs about the chronicity of CF were significant predictors of adherence to physiotherapy. Small study population of 38 participants but considered by the authors that with a 73% response rate the results were generaliseable. Partial adherence was not accounted for
13 studies reviewed. High perceived treatment burden in CF. Tailored interventions and good communication are essential factors in improving adherence. Future studies need to be theoretical and longitudinal.
3
3
3
1-
40

The definitions that do exist demonstrate a lack of patient involvement in determining their health care programmes as they assume a passive acceptance of a health care recommendation by the patient e.g. “a person’s behaviour being consistent with health care recommendations” (Abbot et al., 2009, p. 597). The apparent lack of recognition of patient involvement by health professionals may in part account for low rates of adherence for physiotherapy. The chronic and variable nature of CF and its interdependent components of care, with lack of evidence for optimum levels of adherence for maximum clinical benefit for most aspects of the CF treatment, makes determination of a criteria for adherence an ongoing process of adjustment and balance (Kettler et al., 2002).
Secondly, measuring adherence to treatment is complex and is determined by what the professional recommended, what people do when they carry out a treatment, duration and frequency of treatment and the honesty, re-call and accuracy when recording treatment. To date measuring adherence has been dependent upon ad hoc questionnaires (Abbott et al., 2009). In particular, there are two questionnaires available that investigate adherence to treatment in CF, i.e. the Manchester Adult CF Questionnaire (Abbott et al, 1994) and the CF–Treatment and Management Questionnaire (CF-TMQ) (Cowland, Yorke, & Carr, 2009), which was developed using the Medical Compliance Incomplete Stories Test (MCIT) Koocher, McGrath, & Gudas (1990). Two measurement tools have been developed, the Disease Management Interview - CF (Quittner, Espelage, Ievers-Landis & Drotar, 2000a) and the Treatment Adherence Rating Scale (TARS) (Delambo, Ievers-Landis, Drotar, & Quittner, 2004) both of which have shown some good psychometric properties, but as they relate to children and their families they are not directly applicable to adults. Adherence rates, which vary over a period of time, are usually counted as a percentage and need to be treated with caution, as missing a treatment can produce large percentage changes in studies with small populations. Studies on adherence behaviour utilise self-report which is subject to bias, errors, or intentional manipulation which is likely to over estimate the extent of adherence (Daniels, 2010). Methods such as diary cards, with a duration of 24 hours to three months, and electronic monitoring of nebulisers have been used. Each method has its relative merits pertaining to reliability, validity, feasibility and cost with electronic monitoring (which would not be possible to do for chest physiotherapy treatment) viewed as the gold standard. Modi and Quittner (2006) concluded, in their multi-method assessment of treatment adherence in CF, that adherence varied with both the treatment and measurement method, with the self-reported questionnaire producing considerably higher result values, which should therefore be treated with caution.
41

Thirdly, although there are various degrees and types of adherence, the literature frequently reports (Kettler et al., 2002; Myers & Horn, 2006; White et al., 2007) adherence as a dichotomous construct of being adherent or non-adherent with no reference made to a degree of normal non-adherence nor to partial adherence.
Finally, studies into the influence of gender in adherence to treatment in CF are beginning to emerge, with gender ratios and differences in adherence levels between the sexes measured. Gender studies (Dodd & Webb, 2000; Patterson, Wall, Berge, & Milla, 2008; Willis, Miller, & Wynn, 2001) have noted that males who have a longer life expectancy (CF Trust, 2011a) were more adherent than females, while Patterson et al. (2008) hypothesised that the stresses and strains related to adherence behaviour may be sex-related, with women finding it more difficult to cope than men as well as having a shorter life expectancy. However Sawicki et al, (2009) in their survey of 304 participants concluded that gender was not associated with a perceived higher treatment burden.
Further examples of studies that investigate adherence behaviours in adults with CF are outlined below:
Table 2. 4. Examples of studies that appear to influence adherence behaviour
Influencing Factors Studies
Patient Education/Knowledge Czajkowski & Koocher, 1987; Ievers et al., 1999; Kettler et al., 2002
Health beliefs and locus of control Carr et al., 1996; Myers & Myers , 1999; Pryor et al., 2010
Perceived disease severity Abbott, Dodd, & Webb, 1995; Bucks et al., 2009; Gudas, Koocher, & Wypij, 1991; Kettler et al., 2002
Efficacy of physiotherapy Pryor et al., 2010; Abbott et al., 1994 Carr et al., 1996; Daniels, 2010; Elkins et al., 2009; Main et al., 2009; Robinson et al., 2001; van der Schans et al., 2009
Coping style Abbott et al., 2001
Burden of treatment (boring, timeconsuming, embarrassing)
Abbott et al., 2009; Carr et al., 1996; Christian, 2007; Daniels, 2010; Kettler et al., 2002; Myers & Horn, 2006;White et al., 2007
These studies highlighted the multi-factorial influences on adherence behaviours in CF, which will vary with disease progression, complexity of treatment, life style and life events. For those with severe disease, adherence to treatment is particularly difficult because of the lack of positive reinforcement from any obvious beneficial effect (Kettler et al., 2002).
42

Predicting Adherence
Correlations have made between medical and paramedical staffs’ view of whether patients were adhering to treatment and the patients own self-reported adherence levels. Abbott et al. (1995) investigated whether it was possible to accurately predict adherence to treatment for people with CF, and carried out a study where a close carer/parent/friend was asked in-depth questions regarding the study participant’s adherence to treatment. The handing in of prescriptions was considered to be an objective and accurate outcome measure of the participant’s adherence to treatment which was then correlated with the clinician’s own judgement of their level of adherence and the carer/parent/friend’s opinion. The use of this method of measurement raises ethical issues because the handing in of a prescription is not indicative of the medication being used. Although a parallel may be sought, it is not conclusive proof that failure to collect medication is an indication of general non-adherence, because those who do collect their prescriptions may not always take it and adherence rates can vary between different treatments. This study concluded that those involved in the care of patients with CF were able to predict patient compliance (adherence). This finding was not supported by Conway et al. (1996) whose study, which used a self-report questionnaire issued to 91 adults with CF, with a response rate of 88%, concluded that clinicians were likely to overestimate adherence by up to 20%. This conclusion was support by Kettler et al. (2002) in their review of adherence as they concluded that physicians are likely to overestimate the level of adherence while Daniels et al. (2011) demonstrated that professional carers were poor judges of adherence. The study by Daniels et al., (2011) involved 78 adults with CF who were questioned about their adherence to prescribed nebulisers over the previous three months. Self-report and clinician report was compared to stored adherence data downloaded from the I-Neb nebulizer system. The study concluded firstly that self and clinician reporting of adherence did not provide accurate measurement of adherence when compared to electronic monitoring, and secondly that using inaccurate measures had implications for treatment burden, clinician prescribing practices and funding.
Health Beliefs and Perceptions of Having CF
A study by Abbott et al. (1996) (see Table 2. 3) attempted to ascertain whether health perceptions influence adherence to treatment in CF. The study involved selecting 60 adults attending consecutively a CF out-patient clinic. Each of the participants completed three questionnaires (Health Perception Scale; Health Locus of Control Scale; Manchester Cystic Fibrosis Compliance Questionnaire) under the guidance of a
43

psychologist. The study concluded that worrying about CF, and the perception of having little personal control over their disease progression encouraged adherence. Adherence was self-reported, and the study claimed that patients who admitted to not carrying out a treatment rarely lied. This finding corresponds with a similar finding from a later review on adherence by Abbott and Gee (1998). However this finding has been challenged by Bucks et al. (2009) in their cross-sectional study of 38 adolescents who completed three self-administered questionnaires (Revised Illness Questionnaire (IPQ-R); Beliefs about Medicines Questionnaire-Specific (BMQ-Specific); Cystic Fibrosis Treatment Questionnaire (CFTQ)), who concluded that patients do lie because they do not want to jeopardise their relationship with the members of their CF healthcare team. However it was unclear how the researcher were able to come to such a conclusion. It is also possible that inaccuracy in self-reporting adherence may occur through lack of understanding, or instances of non-adherence are forgotten. The study by Abbott et al., (1996) was vulnerable to bias as it could not record the views of the non-attenders who may be the patient group who has the most difficulty adhering to treatment, as they did not attend clinic. The study findings may also have been biased by the influence of the psychologist who guided them when they completed the questionnaires. Questionnaires rely on the honesty of the participants, their memory and an assumed commonality of understanding of the terms used.
Abbott et al. (2009) in their review on adherence to treatment in CF, critically evaluated 13 studies involving 747 participants and concluded that there was limited evidence to support the view that health beliefs and perceptions of illness were important predictors of adherence to treatment. The limited nature of these findings may reflect the poor quality of the studies and the lack of sensitivity of the measurement tools to record changes in behaviour, all of which are dependent upon honesty, recall and accuracy in understanding the task. Although the data collection methods covered a wide variety of approaches, they nevertheless indicated that health beliefs and illness perception did have some influence on adherence behaviours. These findings can be applied clinically, as understanding health beliefs can be used to potentially predict adherence.
Coping with Cystic Fibrosis
Studies have shown that adults with CF do have problems coping with the enormous treatment demands made on them, which can potentially influence their ability to adhere to treatment (Daniels, 2010; Dodd & Webb, 2000; Pfeffer, Pfeffer, & Hodson, 2003). The studies on adherence in CF are almost totally cross-sectional and attention needs to be given to the fact that adherence behaviours can vary over a period of time,
44
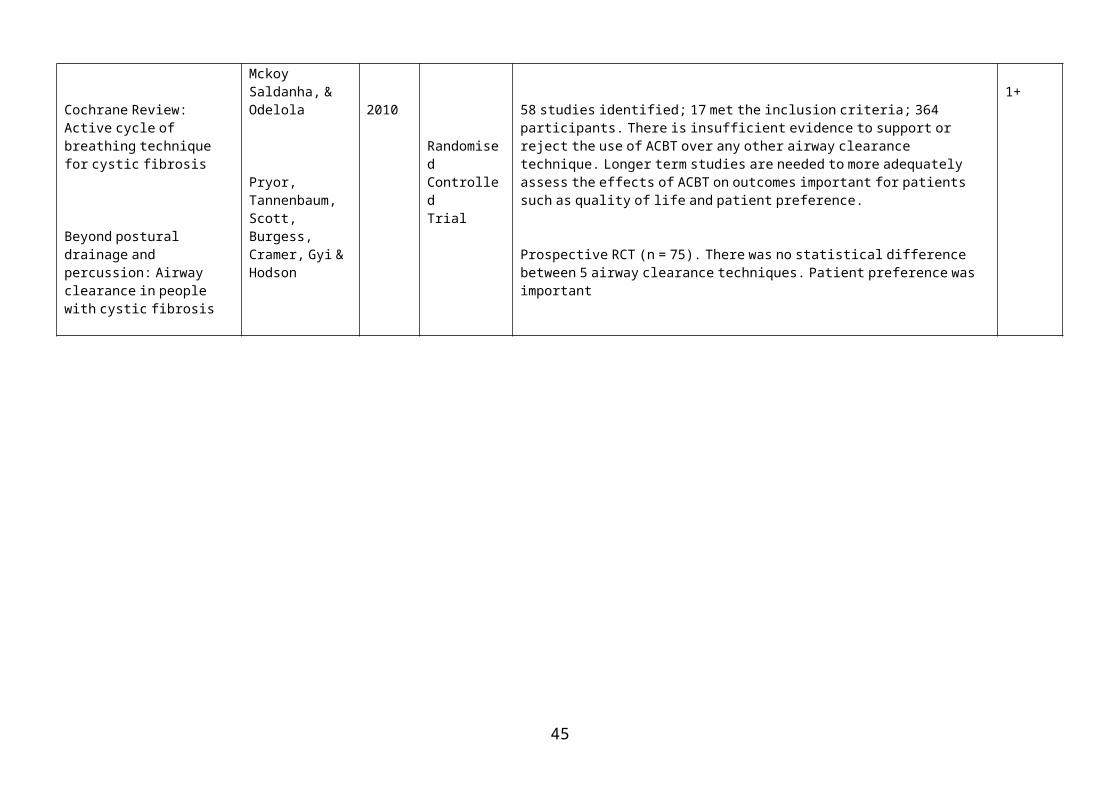
particularly during exacerbations which require high levels of adherence which are more difficult to achieve (Daniels et al., 2011). In a study by Abbott et al. (2001), a coping scale was developed and validated for the purpose of investigating the relationship between coping styles and treatment adherence. The study used a cross-sectional questionnaire and two sets of interviews. The aim of the study was to develop a patient-derived self-report measure to evaluate the ways in which people with CF cope with their disease. The study demonstrated that 65% of the optimistic/acceptance group were adherent to physiotherapy compared to 33% in the avoidance/coping group. A level of 65% of adherence to physiotherapy is high, and the validity questionable, as studies have demonstrated that self-reporting frequently results in over estimation and that percentages as an outcome measure need to be treated with caution (Daniels, 2010; Myers & Horn, 2006). The study concluded that adherence to treatment was influenced by a person’s coping style and that generally optimistic acceptance and hopefulness were associated with greater adherence to treatment. Gender differences have also been noted in the ability to cope with CF. Patterson et al. (2008) in their study of 103 adolescents (10 – 21 year olds), which used a self-report survey (Living with CF Questionnaire – LCFQ), identified that the females found having CF to be more stressful than the males, which may compromise their ability to adhere to physiotherapy treatment and so jeopardise their health outcomes
2. 3. 3. Adherence to Physiotherapy Treatment in Adults with Cystic Fibrosis
Table 2. 5, reviewing the key evidence for adherence to physiotherapy treatment by adults with CF is presented on p. 46-47.
There is a paucity of evidence into adherence to physiotherapy in adults with CF. To date studies have been chiefly confined to children and their families. The findings from these studies indicate possible factors that could influence adherence behaviours but they cannot be directly applied to adults, as children are reliant on their parents/carers to carry out their physiotherapy treatment and their anatomy and physiology it different. Self-administered ACTs have been developed for adults so they can be self-administered and would therefore be unsuitable for younger children.
45

Table 2. 5. Key papers relating to adherence to physiotherapy
TITLE AUTHOR YEAR TYPE OF ARTICLE
SUMMARY OF THE EVIDENCE LEVEL
Cystic fibrosis patients’ views and beliefs about chest clearance and exercise
Treatment of cystic fibrosis in adults
Clinical guidelines for the physiotherapy management of cystic fibrosis
Practical management of cystic fibrosis
Adherence to chest physiotherapy in adults with cystic fibrosis
Guidelines for the physiotherapy management of the adult, medical, spontaneously breathing patient
Carr et al.
Hodson
ACPCF/CF Trust
Dodd & Prasad
Myers & Horn
Bott et al.
1996
2000
2002
2005
2006
2009
Descriptive study
Descriptivestudy
Descriptive study
Descriptivestudy
Survey
Meta-analysis
Patients’ views about physiotherapy and exercise were extremely positive. Adherence can be facilitated by eliciting and understanding a patient’s views and beliefs when negotiating a treatment programme with them. Optimum airway clearance and exercise programmes need to be tailored to each individual’s needs and beliefs.
Specialised services need to be set up to deliver the best possible care. Reasons for improved survival are multi-factorial. There is considerable scientific evidence to support the use of postural drainage with an active cycle of breathing technique and for use of the pep mask.
Studies are hampered by lack of long-term projects and the inability to conduct randomised controlled trials. The effectiveness of airway clearance techniques are a significant feature in adherence to treatment.
The efficacy of routine chest physiotherapy for milder and ‘asymptomatic’ individuals continues to be debated and requires further research. Onerous daily programme of self care. Exercise is an established part of of the physiotherapy programme.
563 participants (39.8% response rate). Self-administered questionnaire. Adherent 29.5%; 63.2% partially adherent; 7.3% non-adherent. Conclusion – to carry out regular airway clearance in a way that suits their lifestyle.
83 publications; 15 data sets; 475 participants. Outcome measure – standard lung function tests. Insufficient evidence to confirm or exclude any differences between CCPT and other airway dependent techniques in terms of respiratory function, but this may have reflected insufficient evidence and lack of sensitivity in the outcome measures.
3
3
3
3
3a
1++
46

Adherence of adult cystic fibrosis patients with airway clearance and exercise regimens
Physiotherapy management strategies for the treatment of cystic fibrosis
Standards of Care and Good Practice for the Physiotherapy Management of Cystic Fibrosis
White et al.
Daniels
ACPCF/CF Trust
2007
2010
2011
Survey
Descriptive
Descriptive
Adherence 70.2% to daily physiotherapy – a higher rate than preciously reported. Time related factors most commonly reported reason for reduced adherence
With increased life expectancy treatment becomes more complex and time consuming. Physiotherapy is balances precariously between lifestyle and adhering to effective treatment The efficacy of treatment techniques needs further study. Patient preferences need to be taken into account when planning programmes.
Review of the evidence of the evidence with recommendations for practice. There are few valid and reliable studies for ACT making a meta-analysis difficult. Outcome measures require further study. Recommendations for practice based on best available evidence.
3
3
1+
47

Studies into adherence to physiotherapy in adults with CF have formed part of larger research projects (Abbott et al.,1994; Conway et al., 1996; Sawicki et al., 2009) investigating adherence to CF treatment in general, with physiotherapy being one of several treatment components. Physiotherapy was identified in these studies as being particularly difficult to adhere too. The studies used the survey method of self-administered questionnaires to collect data on a wide spectrum of treatment modalities for CF. The questions relating to physiotherapy gave only limited data as they were few in number and not sensitive enough to illicit detailed and reliable information.
Plummer, Costall and Torry (2008) in their qualitative study into adherence to treatment in adults with CF, interviewed 25 adults and 10 members of a multi-disciplinary team. Physiotherapy was one component of the treatments being investigated. The participants reported 50% adherence to physiotherapy, however partial adherence was not accounted for and a definition of adherence was lacking, making the study difficult to interpret.
Adherence behaviours investigated by Modi et al. (2006) involved 37 children and their primary care givers. The study used a multi-method approach of diaries, pharmacy re-fill history and electronic monitoring to record adherence, and concluded that accurate means of measurement is important in developing effective interventions to influence behaviour. Although electronic recording is accurate other methods rely on honesty and recall. The use of pharmacy re-fill history cannot assume that medications collected have been taken.
Quittner, Modi, Lemanek, Ievers-Landis and Rapoff (2008) in their systematic review on methods of accurately recording adherence behaviour to medical treatment in chronic disease by children, adolescents and their care givers, investigated empirical evidence of 18 measures utilising three types of recoding adherence - self-report and structured interviews, daily diary methods and electronic monitors. The study commented on the innovative methods used and the opportunities for triangulation by using two methods such as self-reporting and electronic monitoring to enhance reliability and validity. The study concluded that in order to enhance adherence behaviours further development of measurement methods is required so that health outcomes can be optimised. As in the previous studies the findings cannot be directly applied to adults but the conclusions are informative.
During the past 15 years there have only been three studies (White et al., 2007; Myers & Horn, 2006; Carr et al., 1996) which have specifically investigated adherence to
48

physiotherapy in adults with CF, with only two studies (Myers & Horn, 2006; Carr et al., 1996) being undertaken in the UK. The third study by White et al. (2007) was conducted in Australia. The studies by Carr et al. (1996) and White et al. (2007) included chest physiotherapy and exercise while the study by Myers and Horn (2006) focused on chest physiotherapy alone. All three studies used self-administered questionnaires to collect data, which have generally low response rates and consequent biases (Oppenheim, 1992). The study by Carr et al. (1996) investigated to what extent the efficacy of physiotherapy and health beliefs influenced the ability to adhere to physiotherapy treatment.
The use of questionnaires in investigating adherence to physiotherapy for adults with cystic fibrosis
The study by White et al. (2007) used an adapted Manchester Cystic Fibrosis Compliance Questionnaire (MCFCQ). It was piloted to two people with CF as a means of testing its clarity, ease of completion and content. This is an inadequate number for a pilot study as it originated in the UK and the study was under taken in Australia, so cultural differences may have occurred in the terms used. The robustness of the findings was weakened as it cannot be assumed that there is a commonality of understanding across cultures.
The self-administered questionnaire used by Myers and Horn (2006) was based on wording from two questionnaires used in studies on adherence and chronic disease (Cooke, Myers, & Deraksham, 2003; Griva, Myers, & Newman, 2000) which were not content specific for CF. This self-administered questionnaire, which collected quantitative and qualitative data, was not piloted which therefore compromised its validity and reliability as the participants may not have fully understood the questions. The study’s validity and reliability was further compromised by a failure to describe the tools used to specifically design their questionnaire which would make the study difficult to reproduce. The ability of a self-administered questionnaire to collect qualitative data is limited compared to an interview where the interviewer can elicit rich detail through sensitive questioning and prompts.
In the Carr et al. (1996) study a self-administered questionnaire, designed by the researchers, was issued to all the study participants, to elicit their views on the efficacy of physiotherapy treatment and the influence of their health beliefs on their ability to adhere to physiotherapy treatment. The study participants did not contribute to the design of the questionnaire, thereby compromising its validity and reliability as the questions designed by the researchers may not have elicited full responses. The
49

participants needed to be involved in the design of the research tools to ensure that they could describe their experiences in their own words, as the collection of quantitative data alone would not take into account their views on the effectiveness of physiotherapy and the impact that their health beliefs had on their ability to adhere to physiotherapy treatment. The validity and reliability of the study was further compromised because a pilot study was not undertaken to ensure that the participants correctly understood the questions in the questionnaire.
Self-administered questionnaires specifically investigating adherence to physiotherapy treatment in adults with CF, and studies investigating adherence to CF of which physiotherapy was one component, demonstrate wide ranges in response rates. Tables illustrating some examples are presented below.
Table 2. 6. Response rates to questionnaires specifically investigating adherence to physiotherapy in cystic fibrosis
Author Study Pop
Response Rate %
Questionnaire Design
Adherent Partially Adherent
Non –Adherent
Carr et al. (1996) 94 54% Self-Admin/Postal N/R N/R N/R
Myers & Horn (2006) 563 39.8% Self-Admin/Postal 29% N/R N/R
White et al. (2007) 57 67.9% Self-Admin/Researcher present
36.8% 33.4% 29.4%
*N/R – Not Recorded
Table 2. 7. Response rates to questionnaires on adherence to treatment in cystic fibrosis of which physiotherapy was one component
Author Study Pop.
Response Rate %
QuestionnaireDesign
Adherent PartiallyAdherent
Non-Adherent
Abbott et al. (1996) 60 89.5 Self-Admin. 47% 10.9% 26.8%
Sawicki et al. (2008) 204 69 Self-Admin. 47.4% 32.1% 20.5%
Llorente et al. (2008) 34 100 Self-AdminResearcher present
38% 17.6% 20.6%
Bucks et al. (2009) 38 100 Self-Admin Researcher present
N/R N/R N/R
The study by White et al. (2007), where the researcher personally approached each potential participant, had a 67.9% response rate (n = 84) while Carr et al. (1996), who sent their postal questionnaires to a randomly selected clinic population (n = 94), had a response rate of 54%. The questionnaire used in the Myers and Horn (2006) study was sent to everyone over the age of 18 on the UK CF Trust’s mailing list (n = 1407) which resulted in 563 (39.8%) usable replies. This study did not define what they considered chest physiotherapy or adherence to be, which compromised the accuracy
50
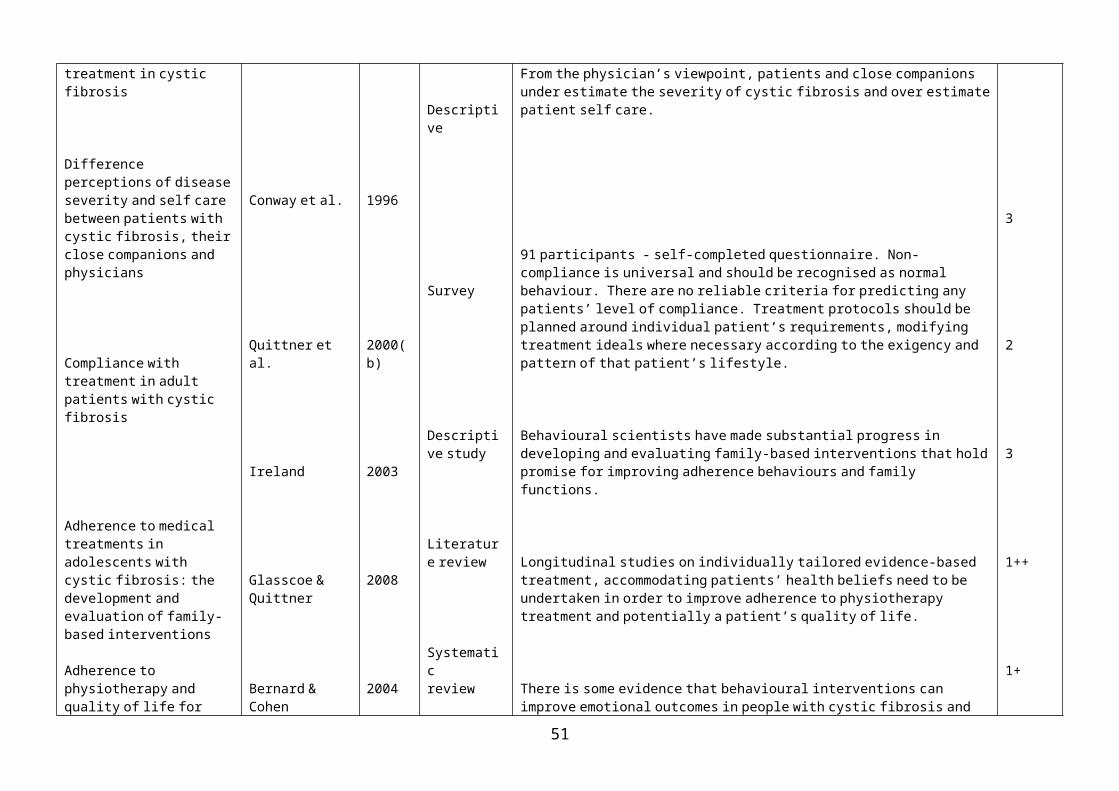
of the results. The Myers and Horn (2006) study concluded that some participants perceived physiotherapy to be ineffective and/or time consuming, and they only did it when they were unwell. The self-administered questionnaires used in these three studies, specifically investigating adherence to physiotherapy, may have been biased due to self-report being unreliable, and in the Myers and Horn (2006) study, which had a low response rate, the validity and reliability were challenged.
Personally approaching potential participants resulted in a higher response rate, giving greater reliability and validity to the White et al. (2007) study. In the studies by Llorente et al. (2008) and Bucks et al. (2009), which involved a researcher administering the questionnaire to the participants, a response rate of 100% was reported giving greater reliability and validity to their results. However, having a researcher present may have also biased the results, as the answers would no longer be anonymous and the participants may not have felt able to fully express their views. When response rates are low inevitable biases occur as the views of those who decide not to take part are unaccounted for.
Reported level of adherence to physiotherapy for adults with CF
In the three studies specifically investigating adherence behaviours in physiotherapy treatment, Myers and Horn (2006) reported an adherence rate of 29.8% but did not record the percentage of participants who were non-adherent or partially adherent; Carr et al. (1996), did not specifically record the level of adherence to physiotherapy treatment in their study as they were investigating whether health beliefs influence adherence behaviours; while White et al. (2007) reported rates of 36.8%, 33.4% and 29.8% for adherent, partially adherent and non-adherent behaviours respectively. Conway et al. (1996) reported, in their “snap shot” survey into adherence to treatment in CF, of which physiotherapy formed one component, that 33% of their patient group had good adherence 18% moderate and 27% poor which is similar to that found by White et al. (2007).
Interestingly the White et al. (2007) study recorded that 27% of patients preferred exercise to ACT and 13% of patients reported that chest physiotherapy made no difference. However this study classified participants not as “adherent” but as whether they had an “acceptable frequency of treatment,” and it did not accurately account for partial adherence, so when a study participant was partially adherent they were classified as adherent. Only 36.8% of study participants were fully adherent with 33.4% missing an occasional treatment. The figure of 36.8% adherence to chest physiotherapy is similar to that of Conway et al. (1996). The White et al. (2007) study
51

considered exercise to be a form of airway clearance, but was not a substitute for using ACTs. In their study population of 54/57 (91.2%) participants undertook regular exercise but as this study was conducted in Australia, climatic and cultural differences may have resulted in a high uptake of exercise.
The Carr et al. (1996) study, which investigated the participants’ perception of the effectiveness of physiotherapy alongside their health beliefs, and the impact that these two factors had on adherence behaviours, found that health beliefs did influence the ability to adhere to physiotherapy treatment as those participants with positive health beliefs were more adherent to treatment.
Studies into adherence to chest physiotherapy are difficult to compare due to the lack of consensus as to what constitutes chest physiotherapy and a failure to account for adherence varying over a period of time. Studies also lack rigor, validity, reliable outcome measures and frequently rely on percentages, which can have a disproportionate impact, making the results unreliable. The inconsistency in these studies into adherence indicate that further investigation needs to be carried out to define adherence, treatment frequency, duration and measurement tools, and to develop strategies to address them.
2. 3. 4. Exercise in the Management of Adults with Cystic Fibrosis
Table 2. 8, reviewing the key evidence for the role exercise plays in the management of adults with CF is presented on p. 53.
The studies selected focus on the role of exercise in CF in relation to its influence on airway clearance and as part of a healthy lifestyle. Initially research into physiotherapy treatment for CF focused on chest physiotherapy, but in the 1980/90’s studies began to emerge looking into the effects of exercise on facilitating airway clearance, and promoting a healthy lifestyle (ACPCF/CF Trust, 2002). All people with CF should participate in regular physical activity (ACPCF/CF Trust, 2011; CF Trust, 2011a) and it should be part of their routine physiotherapy programme. Exercise programmes for people with CF improve cardio-respiratory fitness, morale, lead to a higher degree of perceived competence, improve self-esteem and quality of life (Bradley & Moran, 2011). Exercise should complement chest physiotherapy but not be a substitute for it.
52

TITLE AUTHOR YEAR TYPE OF ARTICLE
SUMMARY OF THE EVIDENCE LEVEL
Effect of exercise and physiotherapy in aiding sputum expectoration in adults with CF
Salh et al. 1989 Cross over trial 2 groups; 31 participants; different combination of chest physiotherapy and exercise concluded that for exercise was complimentary to airway clearance.
2-
The benefits of exercise combined with physiotherapy in the treatment of CF
Bilton, Dodd, Abbott & Webb
1992 Cross over trial 18 participants in 4 different treatment of chest physiotherapy and exercise. Concluded that exercise enhanced airway clearance but was not a substitute for it.
2-
Effect of addition of exercise to chest physiotherapy on sputum expectoration and lung function in adults with CF
Baldwin et al. 1994 RCT Exercise itself leads to more sputum expectoration than occurs at rest and further increases sputum clearance afforded by physiotherapy. Neither physiotherapy nor exercise have significant effects on lung function.
1-
Individualised exercise training in adults with cystic fibrosis: a 1 year randomised controlled trial
Moorcroft, Dodd, Morris, & Webb
2004 RCT Three sessions per week of exercise based on individualised preferences (n = 30) or to a control group (n = 18). Pulmonary function improved. The primary outcome measure was improved fitness as assessed by change in blood lactate concentration. Secondary outcome measurements showed ↓ heart rate and pulmonary function. Conclusion - exercise programmes should be encouraged as an important component of care in cystic fibrosis.
2-
Efficacy of exercise in the management of CF
Shoemaker, Hunt & Arndt
2008 Systematic Review
12 studies; 374 participants; effects of exercise unclear but appears to have a preservation effect of pulmonary function; not possible to draw a conclusion regarding the impact of exercise on hospitalisation and QoL.
1-
Effects of exercise on respiratory flow and sputum properties
Dwyer, Alison, McKeough, Daviskas, & Bye
2010 Cross over trial 14 participants, ventilation and respiratory flow measured during 20 minuets of exercise. Ease of expectoration and sputum properties measured before and after. Conclusion – treadmill exercise appears to improve expectoration more than cycling. Further evaluation required before treadmill exercise promoted as an adequate ACT
2-
Physical training to improve exercise capacity for people with CF
Bradley & Moran 2011 Systematic Review
7 studies; 231 participants; short term studies; meta analysis not possible due to different study designs. Conclusion no evidence to discourage exercise for people with CF
1++
Table 2. 8. Exercise in the management of cystic fibrosis
53

In a comparative study by Salh et al. (1989), the role of exercise in aiding sputum expectoration in patients with CF and the comparative roles of exercise and physiotherapy in sputum expectoration were assessed. In the first arm of the study 19 adult participants undertook a two month programme of home exercise using a cycle ergonometer. Of the 12 patients completing the study, peak work capacity, maximum oxygen consumption, and maximum minute ventilation had increased significantly by the end of the exercise programme, although the increase in daily sputum weight was not significant. In the second arm of the study (n = 10) more sputum was expectorated during and after physiotherapy than during and after exercise. The study concluded that exercise may have a role in aiding sputum expectoration in patients with CF but should not be considered as a replacement for physiotherapy. Sputum volume was used as an outcome but this can be unreliable because of contamination with saliva. A cross over study by Bilton, Dodd, Abbott and Webb (1992) involving 18 participants in four different treatment combinations of chest physiotherapy and exercise came to a similar conclusion. The validity of this study was reduced as it was only of four days duration and it again used sputum weight as an outcome measure, which can be unreliable for the reason previously outlined. The use of the forced expiratory volume in one second (FEV1) for lung function measurement would have been a more reliable indication of improved airway flow. A cross over study involving 8 participants, by Baldwin, Hill, Peckham and Knox (1994), investigated the effects of exercise on sputum production and lung function by adding an exercise programme to the participants’ airway clearance programme on two consecutive days. The study concluded that exercise enhanced sputum clearance. The validity of this result is reduced as the study intervention period was of short duration, lasting only two days, and sputum weight was used, which is an unreliable outcome measure.
A systematic review by Shoemaker, Hurt and Arndt (2008), on the efficacy of exercise in the management of CF, included 12 studies with a total of 274 participants and concluded that there was strong support for the use of aerobic and resistance training to improve aerobic capacity and strength, but the effect on exercise training on pulmonary function and health related QoL, hospitalisation and healthcare utilisation was unclear. This systematic review was criticised by the Centre for Reviews and Dissemination for its lack of methodological rigor in view of the author reporting significant results when it was not always clear whether the authors were referring to statistically significant changes within groups, resulting in the conclusions being unreliable.
54

In a study by Dwyer, Alison, McKeough, Daviskas and Bye (2010) on the effects of exercise on respiratory flow and sputum properties in cystic fibrosis the methodology involved a three day cross-over study of 14 participants who used a treadmill and a cycle exercise to establish if exercise enhanced airway clearance. The study concluded that the improvement in expectoration may have been brought about by higher ventilation and respiratory flow during exercise and in particular the treadmill appeared to be more effective in facilitating airway clearance than cycling. The study, however, did not ascertain the hydration state of the participants nor of their airways. The study was of short study duration comprising of three days and the results may not be sustained over a longer period of time. The study was not postulating this outcome as indicative of exercise being and used as an airway clearance technique without further investigation.
A Cochrane Review by Bradley and Moran (2011) investigated the impact of physical training on people with CF and reviewed seven studies involving 231 participants. A meta-analysis was not possible due to the different study designs. The short term studies did not demonstrate differences between treatments and there were not enough studies in the review to compare aerobic training to anaerobic training or a mixture of these two. The review was limited by the small size of the study populations, the short duration of the studies and the outcome measures which needed refining, but concluded that there was no evidence to actively discourage exercise for people with CF, and it may improve QoL in the short term. Current guidelines on the physiotherapy management of CF from the ACPCF/CF Trust (2011) and the Association of Chartered Physiotherapists in Respiratory Care (ACPRC)/British Thoracic Society (BTS) (Bott et al., 2009) supports the use of exercise for people with CF for its benefits of general well being and the enhancement of airway clearance, but there was a low grade of evidence supporting this opinion.
Although there is a lack of rigor and poor methodology in the literature specific to CF, exercise is encouraged by the DoH (2010) for all members of the general population thereby making it an activity which people with CF can join in with their peers, which can contribute to optimising adherence (Moorcroft, Dodd, Morris, & Webb, 2004).
2. 3. 5. Self-Management for adults with cystic fibrosis
Due to increasing life expectancy, self-management studies on adults with CF is an emerging concept and to-date there is only one study that has been undertaken
55

(Sawicki et al., 2008). Self-management programmes have been developed for children and their families but they are not directly applicable to adults. Currently a Cochrane Review is being conducted into self-management programmes for children with CF and is due to report in 2012. This study may not be generalisable to adults, but its conclusions will be informative.
In the United States of America (USA) considerable work was carried out by Bartholomew et al. (1997; 1993; 1991; 1988) on self-management programmes for families with a child affected with CF. In the early 1990s Bartholomew et al. (1993) developed performance objectives for the self-management of CF. They recognised that the self-management of a chronic illness, such as CF, would require the patient to perform several cognitive and behavioural tasks, and patients could be empowered through a self-management programme to undertake behaviour such as self-monitoring, reporting, decision making and planning. They also highlighted the need for education in health care programmes to receive greater attention. Although giving indicators for the development and effectiveness of self-management programmes for children and their families the conclusions cannot be applied to adults, where chest physiotherapy is focused on independence and self-administrated techniques. Downs, Roberts, Blackmore, Le Souel and Jenkins (2006) conducted a multi-centred, randomised, controlled trial investigating the effectiveness of a self-management programme called “Airways” in 62 children (6 – 11 years) with CF and their caregivers, and found that adherence had increased following the programme but this had not been maintained when assessed at a 12 month follow up. The study was hampered by the limitations of objectively recording the treatment that had been carried out as it relied on self-reporting, honesty and the re-call of the parents/carers.
The study by Sawicki et al. (2008), investigating self-management for adults with CF, was developed as part of the Project on Adult Care CF (PAC_CF) to investigate the burden of all CF treatment, which is a challenge to self-management. The study used a self-administered questionnaire which was completed by 204/294 participants and formed the 6th survey wave of this longitudinal study. Self-reporting as a means of monitoring adherence is prone to inaccuracies which can compromise the validity and reliability of the outcomes, as discussed above. The study concluded that the high treatment burden for CF contributed to the day-to-day patient decision making process and the knowledge of how they made their decisions was a step towards understanding patient-based disease management.
Self-Management Physiotherapy Programmes for Adults with CF
56

To date no self-management physiotherapy programmes for adults with CF have been developed.
2. 3. 6. Summary of Background Literature Search
Physiotherapy is an integral part of the daily management of CF (ACPCF/CF Trust, 2011; Bott et al., 2009;). Although five Cochrane Reviews (Elkins et al., 2009; Main et al., 2009; Morrison & Agnew, 2009; Robinson et al., 2010; van der Schans et al., 2009) concluded that in the short term ACTs are effective in airway clearance, and a study by Pryor et al. (2010) demonstrated their long term benefits, the physiotherapy element of treatment remains one of the most difficult to adhere to and has one of the lowest rates of adherence (Abbott et al., 2009; Daniels, 2010; Dodd & Prasad, 2005). Studies into adherence to physiotherapy treatment (CF Trust, 2002; Main et al., 2009; van der Schans et al., 2009), are hampered by a lack of a universally accepted definition, the inability to conduct double blind RCTs, short time frames, the limitations of measurement techniques, the lack of a benchmark of what is an acceptable level of adherence for physiotherapy treatment and a limited interest in patient preferences.
It is essential that people with CF are educated to have sufficient knowledge and skills to successfully cope with self-management (Bucks et al., 2009; Sawicki et al., 2008). Self-management is an important means of ensuring that people with CF are empowered, informed and sufficiently knowledgeable to make autonomous decisions about their physiotherapy treatment. The influence of self-management programmes on the ability to adhere to physiotherapy treatment for adults with CF has yet to be explored. It is believed that this study is unique, as it seeks to increase physiotherapy knowledge about the problems of adhering to physiotherapy treatment for adults with CF and to develop an educational strategy in the form of a SMPP to potentially improve it. This exploratory study aims to answer the research question by means of postulating a new model of clinical practice through the development and evaluation of the effectiveness of a SMPP in optimising the ability to adhere to treatment.
57

CHAPTER 3 METHODOLOGY
3.0 Introduction
This chapter outlines the theoretical methodological approach that was selected to meet the research aims. How this theoretical model was applied to the to the research process is described in detail in Chapters 4 and 5.
Chapter three is divided into five sections:
3. 1 Action Research
Action Research Typology – Professionalising
3. 3 Ethics
3. 4 Population and Sampling
3. 5 Recruitment
3. 1. Action Research
Introduction
The study aims to identify the problems adults with CF have in adhering to physiotherapy and then sets out to address these problems by developing an educational intervention in the form of a new model of clinical practice by using a Self-Management Physiotherapy Programme (SMPP). The aim of the SMPP is to improve adherence to physiotherapy treatment for adults with CF. The study then proceeds to evaluate the usefulness of the SMPP.
In order to investigate the problems people with CF have in adhering to treatment, it was important to select a methodology that gave them a opportunity to express in their own words what problems they experience with adhering to physiotherapy, and to engage and empower them to be involved in the research process so that they contribute to finding a solution. By taking responsibility for identifying their problems and seeking a solution a successful outcome would be more likely to be achieved.
This research project sits within the social science paradigm. A variety of qualitative and quantitative research frameworks were considered in order to provide a flexible, reflective and responsive method to systematically investigate how to optimise the ability of adults with CF to adhere to physiotherapy treatment, with the aim of developing a new model of clinical practice. After careful consideration, an action research approach was initially adopted.
58

3. 1. 1. Action Research Approach
The Action Research approach uses a cyclical process which enables the findings from each stage to inform the development of the whole direction of the study. It is best described as a dynamic, democratic and problem-solving change intervention which provides a flexible methodology that enables the researcher to adopt a participatory approach by involving the participants in both the change and the research process (Hart & Bond, 1996; Lincoln, 2001; Reason & Bradbury, 2001; Waterman, Tillen, Dickson, & de Koning, 2001) It is particularly suited to being applied to NHS heath care settings (Meyer, 2000) as the action research process begins with identifying problems and sets out to develop potential solutions to improve practice. Action Research narrows the “theory-practice” gap and is gaining prominence as the NHS strives to achieve evidence-based health care that delivers patient focused high standards of clinical care in a cost effective and safe environment (DoH, 2008).
Action research was first conceptualised by Kurt Lewin (1947, 1946) in the USA as a cycle of interventions to bring about change, with particular emphasis on group dynamics and the participation of all stakeholders. The concept has been developed and adapted by educationalists such as Kemmis and McTaggart (1981) who viewed it from a social science perspective and Stenhouse (1985) who set it within the framework of an educational environment. Reflection, which has been defined by Schon (1983) as a process concerned with thinking about action, is an integral part of the dynamic action research approach as each part of the process informs the following stages. In its simplest form action research involves four parts; planning, action, evaluation and reflection with repeated cycles, as outlined by Lewin (1946). The four stages form a continuous change process which influences all stages of a project. (Fig. 3. 1.)
THE ACTION RESEARCH CYCLE
59

Fig. 3. 1. Lewin’s (1946) sequence of action steps comprising of four stages
Action research used in a health care setting enables a research enquiry to be undertaken with the aim of improving clinical practice through the partnership, co-operation, participation and empowerment of the participants whose problems are being investigated. The four stages of the action research cycle are outlined in greater detail below: The Action Research Cycle
The cyclical process of action research begins with the identification of the problem and typically has four parts:
Part 1. Plan (identifying the problem; developing the intervention; preparation for change)
Part 2. Action (implementation of change – implementing the intervention)
Part 3. Evaluation (impact of change process)
Part 4. Reflection (assessment of effectiveness and recommendations)
Each of the four parts is described in detail below.
Part 1 - Plan
The first part of the action research cycle is that of “Planning” which is concerned with ‘what to do’. Within the planning phase, there are three further sub-stages:-
(i) Identifying the problem
PLAN
ACTION
EVALUATION
REFLECTION
60

(ii) Development of an innovation
(iii) Preparation for change
(i) Stage I – Identification of the Problem
Introduction
The problem under investigation in this study needed to be identified by the participants so that they were engaged and empowered in the process of change and improvement. The researcher used reflective practice (Greenwood, 1984; Schon, 1983) from personal experience to contribute to the identification of the problem. In order to accurately identify the problems and contribute to the design of a new intervention to potentially resolve them, decisions were made about methodological approaches and appropriate data collection methods so that the data collected was accurate, reliable and valid. Because action research involves the participants and combines both inductive and deductive methodological approaches it was initially chosen for this study.
Inductive and Deductive Approaches
The Inductive Approach
An inductive approach starts with specific observations and measures which begin to form patterns and regularities from which it is possible to formulate some tentative hypotheses which are then explored with the result that the process ends up with the development of some general conclusions or theories (Newell & Burnard, 2011; Parahoo, 2006). Inductive reasoning (Cohen, Manion, & Morrison, 2011), by its very nature, is more open-ended and exploratory, especially at the beginning. An example of the inductive approach is qualitative research which is the examination, analysis and interpretation of observations for the purpose of discovering underlying meanings and patterns of relationships, including classifications of types of phenomena and entities, in a manner that does not involve mathematical models (Newell & Burnard, 2011; Polit & Beck, 2006). The best-known qualitative methods of inquiry include in-depth interviews, focus groups, and participant observation. Qualitative methods can also provide a dual function by seeking an in-depth understanding of human behaviour, as well as perceived reasons that govern that behaviour (Polit & Beck, 2006). In this study the semi-structured interview was chosen as it gave the participants an opportunity to express in their own words the problems they experience in adhering to physiotherapy, and to use that information to contribute to a
61

solution. How the semi-structured interview was applied to the study is outlined in Chapter 4.
The Deductive Approach
Deductive reasoning is more narrow in nature and is concerned with testing or confirming hypotheses. Deductive research works from the more general to the more specific. The deductive approach in this study used a cross-sectional survey, designed and issued in two parts before and after the intervention, to monitor any changes that may have occurred as a result of the a ‘top-down’ approach (Parahoo, 2006; Topping, 2006). It begins with thinking up a theory about a topic of interest, which then narrows down to a more specific hypothesis that can then be tested. This process is further narrowed down when observations are collected to address the hypotheses. This process ultimately leads to testing a hypothesis with specific data as a confirmation (or not) of the original theories. An example of a deductive approach is quantitative research which in the social sciences refers to the systematic empirical investigation of phenomena, and their relationships (Newell & Burnard, 2011). The objective of quantitative research is to develop and employ mathematical models, theories and or hypotheses pertaining to phenomena and has its roots in a positivist framework (Richardson, 1996). It can be a useful approach for giving precision measurements of when, how much and how often. In social sciences quantitative research is often contrasted with qualitative research.
Combining Qualitative and Quantitative Data
Combining qualitative and quantitative data can give a greater understanding of the findings and the issues involved. For example a person’s behaviour may be influenced by the impact of their disease severity. Disease severity is measured in quantitative terms, e.g. total lung capacity is measured in litres, while exploring a person’s behaviour requires a qualitative approach. A multiple approach to data collection can act as a form of triangulation (Topping, 2006). Triangulation provides completeness of data as the topic being investigated is being measured in different ways (Cohen et al., 2011). It enhances the validity and credibility of a study as it can give cross verification of the results and findings. In this study the problem was investigated using two approaches, i.e. semi-structured interviews (inductive) and a survey (deductive) in the form of a questionnaire. This dual approach enabled the outcomes from each data collection method to act as a form of validation, as the same problems were identified by different means.
62

(ii) Stage II - Development of an Intervention
Having identified the problem, which in this study is the problems adults experience in adhering to physiotherapy, a suitable intervention needs to be developed to potentially bring about a change in behaviour or a situation, with the aim being to contribute to the resolution of the problem. The participants whose problem was being investigated needed to be actively involved in the development of the innovation and its implementation so they were engaged and empowered in the change process. However in a healthcare setting, action research can have limited involvement for the participants due to it being process driven, and the professional having greater clinical knowledge (Meyer, 2006).
(iii) Stage III - Preparation for Change
The aim of an action research study is to facilitate a positive change in a situation or behaviour in order to bring about an improvement (Hart & Bond, 1996). In action research, preparation for change includes engagement of the participants and the preparation of the planning stages of the project. By actively involving the participants in the research process they become engaged in the development and design of the study. The participants are actively engaged in the identification of the ‘problem’ or ‘situation’ in which they are situated by means of effective communication methods such as focus groups or in-depth interviews. By consenting to participate in the research process it demonstrates a potential willingness to change and contributes to a greater understanding of the problem or situation being investigated (Cohen et al., 2011). This involvement also gives the participants ‘ownership’ of the research process, encourages commitment to it and prepares them for the change processes. Partnership between participant and researcher can empower the participant, thus facilitating change. Continual engagement by disseminating information to the participants throughout the different stages of the research process can also facilitate the change process, as the participants receive incremental feedback during their involvement.
Part of getting ready for change is the careful planning of the actions which will facilitate the change process, minimise potential disruptions and ensure a more successful outcome. Preparation for change can involve:
Obtaining funding Seeking of permission from an ethics committee to undertake a study
63

Creating a willingness to change – this is dependent on the participants perceiving the need to change by being empowered and engaged in the change process.
Once the problem has been identified and the intervention developed, the action research process moves on to the second part, the ‘Action’, which is the implementation of the intervention.
Part 2 - Action
The second part of the action research cycle is when the implementation of the change innovation or ‘action’ takes place, with the intention of bringing about a change for the better in behaviour or in a situation. The change intervention is participatory, dynamic and practical and in a health care setting is part of change management to bring about practice development (Meyer, 2006). It is important that the participants understand the need for change and are engaged and empowered to actively contribute to the change process. The change process requires them to make changes in their own behaviour in order for the ‘action’ to be successful. Change can also occur when the individual participant sees the need to change and actively seeks to bring it about. In this study the action was the SMPP, the aim of which was to optimise the ability to adhere to physiotherapy treatment and, in doing so improve healthcare outcomes, reduce healthcare costs and improve QoL.
Part 3 - Evaluation
The third part of the action research cycle is concerned with evaluating the impact of the change process (Waterman et al., 2001). The purpose of evaluation in action research is to establish the effectiveness of the change process by critically appraising the change process, the measurement tools and the outcomes. The definition and assessment of ‘change’ needs to be carefully considered so that the tools used to collect data are sensitive enough to register any changes which may have occurred. The occurrence of ‘change’ is not just dependent on the full implementation of an innovation. It is still valuable to collect data in circumstances where partial change has been achieved, or change which has taken place over a period of time, or indeed no change has occurred (Hart & Bond, 1996). Even if a partial change or no change has occurred this is still relevant as it can contribute to the critical analysis of the study, inform future cycles of intervention and add to the knowledge and understanding of the topic.
Although change may have occurred, it is the effectiveness of the ‘impact’ brought about by the innovation which is reviewed in the evaluation. ‘Impact’ has been
64

defined as the ‘lasting effect or influence’ (Waterman et al., 2001, p. 27) of an intervention and is part of a change management process. Change management (Gerrish, 2006; McKenna, Hasson, & Keeney al., 2006) is the process during which changes to a system are implemented in a controlled manner by following a pre-defined framework. How the ‘impact’ of the change is reliably measured is critical to the evaluation process because in action research it can be difficult to attribute outcomes and impacts to the action research process if the methodology and tools used to collect the data are not sensitive and valid enough to enable evaluation to take place.
Part 4 – Reflection
Reflection is an integral part of the cyclical nature of the action research process. It is a process whereby reflection on an experience (Kolb, 1984; Schon, 1991) can be used to improve action and professional practice, which in the case of this study is physiotherapy clinical practice. It is the last part in the action research cycle and is concerned with assessing the effectiveness of the research process, its implementation and the ‘action’, in order to make recommendations for improvement in professional practice (Hart & Bond, 1996). Reflection is concerned with identifying what differences the study made to clinical practice and what could be done differently when developing the next cycle of planning, intervention, implementation and evaluation.
Reflection requires the use of critical thinking skills in order to assess how effective the action research process has been. Critical thinking seeks to ‘think beneath the surface’ in a logical and fair way and in doing so, questions information, conclusions and points of view (Paul & Elder, 2006). Critical thinking involves determining the meaning and significance of what is observed, expressed, inferred or put forward as an argument, and then determines whether there is adequate justification to accept the conclusion as true. It requires the researcher to ‘step back’ and use their knowledge, experience and judgment of the evidence base to form a rational opinion which can be potentially incorporated into professional practice. In action research the production of research is not viewed as separate from developments in practice.
To accommodate the complex situation of the ‘real world’, action research typologies have been developed to give a range of flexible approaches to undertaking action research.
3. 2. Selecting the Action Research Typology - Professionalising
65

In order to accommodate a wide range of complex ‘real world’ situations, many different typologies have been developed within the action research framework, with each one reflecting a different approach to the action research process (Reason & Bradbury, 2001). Hart and Bond (1996) have attempted to formally classify approaches and activity by developing a typology which encompasses a whole range of approaches and practices each grounded in a different tradition. Their typology distinguishes four types of action research - Professionalising, Experimental, Organisational, and Empowering - each with seven distinguishing criteria (Appendix E). Their types are the ideal and not prescriptive of action research. All four types display the seven distinguishing characteristics: 1. an education focus; 2. problem orientated; 3. change intervention; 4. aims at improvement and involvement; 5. deals with individuals as members of a group; 6. involves cyclical processes; 7. founded on collaboration. Hart and Bond (1996) developed their typology in order to retain a distinct identity of action research while spanning the spectrum of research approaches. It attempts to clarify action research types by avoiding the problems associated with narrow definitions (Reason & Bradbury, 2001; Waterman et al., 2001).
The typology selected for this study was the ‘Professionalising’ typology (Fig. 3. 2., p.67) since its characteristics of being professionally and process led, involving the use of reflective practice, and seeking to improve professional practice on behalf of the users (Hart & Bond, 1995) was most suited to achieve the aims of this exploratory study.
Professionalising Typology
The professionalising typology is based on the assumption that the experts have greater experience, knowledge, and theoretical resources than the participants, who act at the level of providing ‘on the ground feedback’ within fixed parameters. The ‘Professionalising’ typology is used when there is a need to ‘test’ the effectiveness of a particular pre-defined intervention. The relationship between researcher and researched in action research gives emphasis to the concept (Heron, 1996; Reason & Bradbury, 2001) that research is carried out ‘with’ and ‘for’ the participants rather than ‘to’ them. In reality this concept is difficult to implement in a health care setting as there is an unequal balance of power in the researcher-participant relationship (Meyer, 2000). In the ‘Professionalising’ typology there is an assumption that the ‘experts’ have a greater knowledge and experience. This inequality of knowledge and experience means that the participants become involved in the study but not as equal partners with the professional. Even when egalitarian outcomes are sought, action
66

researchers still actively facilitate change in others. By utilising critical thinking skills, which are required in reflective practice, the researcher is able to take the “imbalance” between the patient and the professional into account when facilitating change. The key features of the Professionalising Typology are outlined in Fig. 3. 2.
Distinguishing Criteria
Educative Base
Reflective practice Enhancing professional control and the individual’s ability to
control the work situation Empowering professional groups; advocacy on behalf of
patients/clients Practitioner focused
Problem Focus Problem defined by a professional group; some negotiation
with users Contested professionally determined definitions of success
Change Intervention
Professionally led - Pre-defined - Process led
Improvement & Involvement
Towards improvements in practice defined by professionals and on behalf of the users
Fig. 3. 2. Professionalising typology - key features (Hart & Bond, 1995, p. 41)
The emphasis in the ‘Professionalising’ typology is with the professional seeking a change in their practice in order to bring about potential improvement for the benefit of the participants. The professional can use reflective practice to identify the problems in the first instance, however an improvement or change cannot be achieved without the willingness of all the participants to become involved (Meyer, 2000) and collaborate in the change process. In this study the ‘Professionalising’ typology incorporates reflective practice by the researcher to facilitate change management in order to improve professional practice for the benefit of the participants. How is was applied to the study is outlined in Chapter 4, p.83..
In action research it is through the use of reflective practice that the researcher is able to critically appraise and evaluate the usefulness of the methodologies, results and findings so that a balance of perspectives is achieved. It is also important for action researchers to recognise the vulnerability of the participants (Parahoo, 2006). Participants are encouraged to think of themselves as being equal partners with the professional, although they may not have the knowledge or skills to be truly equal. The researcher in this study was also the practitioner, and consequently uniquely placed to use reflective practice from her own clinical experiences to take the side of
67

the participants, help them understand their real situation and show ways of change and ‘liberation’ (Sarantakos, 1998, p. 113).
Summary for Action research
Lack of adherence to physiotherapy is a well recognised problem in CF. The aim of this study was to explore whether adherence to physiotherapy treatment in adults with CF was optimised using a new model of clinical practice in the form of a SMPP. The action research approach was chosen as it is a cyclical process which enabled the findings from each stage to inform the development and direction of the study, and involved the people affected by the problem being investigated to participate in finding a solution to their problems.
The action research approach used in this study was informed by the ‘Professionalising’ typology and follows the four parts of the action research cycle. This typology (Hart & Bond, 1995) was selected as it is concerned with the improvement of professional practice on behalf of the users and is carried out when there is a need to ‘test’ the effectiveness of a particular pre-defined intervention, which in this study was the SMPP.
How the action research process was applied to the study is outlined in Table 3. 1.
Table 3. 1. Key stages of the study
68

Stages of the Study Actioned By
Study Population Selected R
Inclusion and exclusion criteria applied Study population recruited R
PLAN
First Set Semi-Structured Interviews C P
Analysis of First Set of Semi-Structured Interviews R & C PSecond Set of Semi-Structured Interview
C PAnalysis of Second Set of Semi-Structured Interviews R & CP
Pre-Intervention Physiotherapy Questionnaire developed from the findings (themes) of both semi-structured interviews
R
Pre-Intervention Physiotherapy Questionnaire piloted
R
Pre-Intervention Physiotherapy Questionnaire issued R
Pre-Intervention Physiotherapy Questionnaire returned and analysed
INTERVENTION /ACTION
SMPP designed R
SMPP piloted - Sub-group R
Start of Intervention: SMPP issued R
3 month Follow-Up: SMPP reviewed and evaluated using Feedback Chart R
Finish: 6 month Follow Up: SMPP reviewed; Post-Intervention Physiotherapy Questionnaire issued RPost-Intervention Physiotherapy Questionnaire returned
EVALUATION
Pre & Post Intervention Physiotherapy Questionnaires Analysed and Feedback Chart evaluated
R
REFLECTION
Legend
69

Sub-groups were selected from total study population (n = 49) + Reasons for the study population reducing CP = Clinical Psychologist R = Researcher/Physiotherapist
Each stage is described in greater detail in Chapters 4 and 5 as the research process progresses. Outlined below are the ethical considerations and the Population, Sampling and Recruitment Strategy for the study.
3. 3. Ethics
Background
In the National Health Service (NHS) it is mandatory for research studies involving patients to be reviewed by an ethics committee, whose principles are based on the World Medical Association Helsinki Declaration (1964) (WMA, 2008). Although there are many safeguards, such as research ethics committees, National Research Ethics Services (NRES) and NHS clinical governance procedures (DoH, 2001a; 2006b; 2011; Dawson & Sausman, 2005), the protection of the participants’ interests in matters of research often rely on the professionalism and personal integrity of the researcher or the research team (Johnson & Long, 2006; Speziale & Carpenter, 2003). Ethical issues surrounding volunteering for research (CSP, 2001; Consumers for Ethics in Research (CERES), 1994; General Medical Council (GMC), 2002) were carefully considered. Potential participants needed to be fully informed, to understand what the study involved and what would be asked of them. A Patient Information Leaflet outlining the study was prepared for them to read (Appendix F). It contained information on the purpose and process of the study and was given to each potential participant who was approached to be in the study, so that they were able to make an informed decision as to whether they wished to participate or not. Contact numbers for the researcher were also included in the information so they could speak to the researcher at any time to request further clarification, or if any queries arose they could be answered. The medical consultant responsible for the Adult Specialist CF Clinic was given an information leaflet outlining the protocol of the study (Appendix G).
Submission to the Ethics Committee
70

The application for ethical approval was supported by the medical consultant responsible for the Adult CF Specialist Services and a standardised proposal (Appendix H) for the study was submitted to the local NHS research ethics committee. Following minor revisions (the inclusion of a telephone extension so the potential participant could contact the researcher/physiotherapist directly) approval was granted (Appendix I). Professional Indemnity for the study is outlined in Appendix J. The researcher ensured that procedures agreed by the ethical committee were strictly adhered to and that sensitivity was shown towards the participants as issues involving CF could be distressing, due to it being a life limiting disease. Ethical issues such as consent, being fully informed, betrayal, anonymity and data protection are discussed below.
Consent
The consent forms were developed from the standardised ones issued by the Local Research Ethics Committee (Appendix K). The consent forms were personalised for the study by using the title of the study and a contact telephone number for the researcher, should participants wish to discuss the study at any point. Two different consent forms to participate in the study were each signed by the researcher and the by the participant. A photocopy of each of the two consent forms was given to the participant to keep and the two originals were put in the participant’s medical notes. For the participants who agreed to take part in a semi-structured interview an additional consent form (Appendix L), adapted from that of the standardised Local Research Ethics Committee form, was used. The participant and the researcher each signed this consent form. The original was kept in the participant’s medical notes and a photocopy was given to the participant.
Betrayal
Betrayal involves a breach of trust. Cohen et al. (2011) consider that the research method most vulnerable to betrayal is that of action research, because of its participatory nature. As a result, particular attention was given to ethical issues as there was a blurring of roles between the researcher and the researched. Great care was taken by the researcher to ensure that there was a distinction between when she was functioning as a researcher and when she was in her role as a clinician, by explaining carefully to the participant what was required for research purposes and what was required for the purposes of their clinical treatment.
Data Collection, Recording and Protection
71

All the data was collected by the researcher/physiotherapist except for the semi-structured interviews which it was collected by the interviewer and it was analysed by a statistician. The participants were informed in the Patient Information leaflet (Appendix F) that the information collected in the questionnaires would be anonymised by each participant being given an identification code known only to the researcher, and all information would be treated as confidential. Data was safely stored in a locked filing cabinet with only the researcher having access, and at the end of the study all information was destroyed. The computer was restricted to use by the researcher only and password protected. The study complied with the Data Protection Act (Office of Public Sector Information (OPSI) (1998).
Qualitative studies challenge the anonymity of participants. The more information that is given by the participants as their stories unfold, the easier it may be for them to become identifiable to others (Speziale & Carpenter, 2003). Although anonymity could be accommodated in questionnaires, as the participants had identification numbers, it would not be possible for this to happen during the semi-structured interviews, as only confidentiality, not anonymity, could be offered. Care was taken to ensure that the information given would not result in the participant being identified in publications and in the literature.
Insurance
As there were no physical interventions carried out as part of the study the risks regarding insurance were considered to be low. Nevertheless the researcher made sure that all research actions were covered by insurance and indemnity both for the researcher, the participant and the hospital Trust, in order to comply with the governance requirements of the National Research Ethics Service (DoH, 2001a).
3. 4. Population and Sampling
Background
As this was an exploratory study, and the outcomes unknown, the study site was confined to one Adult Specialist CF Centre, it being considered too unwieldy and unmanageable to attempt a multi-centre study involving other Adult Specialist CF Centres. Whilst it is acknowledged that there are limitations to confining the study to one specialist clinic the decision taken was a pragmatic one. The study took place in an Adult CF Specialist Clinic in a university teaching hospital in a
72

provincial city on the south coast of England, serving a local population of 245,000 people. The clinic acted as a regional resource whereby district general hospitals in the adjacent areas could link up to its specialist services.
The Adult Specialist CF Centre population comprised of two patient groups; the ‘full care’ group (n = 61) who received all their care at the centre and the ‘shared care’ group (n = 90) who received their routine care at their local hospital and attended the Adult Specialist CF Centre for specialist services and their annual review. The decision was taken not to include the ‘shared care’ group as achievement of a successful outcome in an action research study requires the researcher to have an in-depth knowledge and understanding of the study population, in order to effectively facilitate a change in behaviour. By including the ‘shared care’ patients the researcher would not have a sufficiently detailed knowledge of them, as their day to day treatment would be carried out at other hospitals, and they would only attended the Adult Specialist CF Centre a few times a year. The ‘shared care’ group would have a variety of physiotherapists seeing them at their local hospitals which would lead to a lack of consistency in assessment and in the implementation and monitoring of the SMPP.
Sampling Frame
An investigation of a specific population was selected since statistical representativeness is not commonly sought in qualitative research, when the primary aim is to understand the participants’ experience/behaviour in order to bring about a change in it. In view of this a purposive sample was chosen.
Purposive Sample
A purposive sample is one that has been selected by the researcher as representative of the group that is being studied (Holloway & Wheeler, 2010). This type of sample includes a population with specific characteristics that have been identified in advance. The purposive sample chosen in this study were all the patients in the “full care” group (n = 61) registered in the Adult Specialist CF Centre, thereby ensuring a full range of disease severity, with all the males and females represented. At the time of the study there was only one physiotherapist working in this Adult Specialist CF Centre and this physiotherapist was also the researcher for the study. The characteristics of the purposive sample therefore comprised the total population of the “full care” group (n = 61), which included all the males and females, and they all saw the same physiotherapist.
73

This purposive sampling frame of “full care” patients functioned as a non-probability sample and as such was representative of the group. Acting as a complete sampling frame it ensured maximum representation and was unbiased in its selection. The disadvantage was that if there was a high number of non-participants the collected data would be incomplete and unrepresentative of the whole population, and potentially limit the validity of the results.
The following inclusion and exclusion criteria, within the available purposive sample, were used in the study:-
Inclusion Criteria
All the patients registered as “full care” in an Adult CF Specialist Clinic based in a university teaching hospital (aged 17 upwards)
Resident in the UK for the duration of the study Understands English – as a non-funded study it was not possible to provide
translation services Patients who had been seen at least once by the CF physiotherapist
Exclusion Criteria
Post heart-lung transplant - because after transplantation there is no need to do routine chest physiotherapy as the lungs are normal
Learning difficulties that might preclude participants from completing the self-completed questionnaires
Not resident in the UK for the duration of the study. One patient was registered as “full care” in the clinic but was not resident in the UK. They did not attend the clinic frequently enough for their progress during the study to be accurately monitored
3. 5. Recruitment Strategy
Background
There were a total of 61 “full care” patients registered in the Adult CF Specialist Centre available to be recruited to the study. When the selection criteria were applied the eligible number was reduced to 55. In order to ensure maximum recruitment it was intended that all the eligible participants would be approached during face-to-face contact over a four month period during an in-patient stay or an out-patient visit. Throughout the study participants were only approached when they were in a
74

medically stable state. If at the end of the four month recruitment period some potential participants had not been approached they would be contacted by telephone. The recruitment strategy is outlined in Fig. 3. 3, p. 76. .
A four month recruitment time frame was chosen as it was a slightly extended time beyond the interval of three monthly routine follow ups recommended in the Standards of Clinical Care (ACPCF/CF Trust, 2002) at the time of the study. It was not advisable to extend the recruitment time frame for too long a period as it was likely that, for some of the participants with severe disease, a significant deterioration could occur and result in non-participation or withdrawal from the study. As far as possible, routine visits were used as opportunities to recruit and collect data, to minimise disruption and unnecessary travelling for participants.
75

RECRUITMENT STRATEGY
Mixed Methodology
Fig. 3. 3. Recruitment Strategy
Face to Face
n = 61 - Full care patients in the Specialist CF Clinic
Criteria for Eligibility Applied – 6 excluded• 2 - learning difficulties that rendered taking part too difficult for the participant. • 1 - post heart lung transplant• 2 - unable to understand and speak English • 1 – not resident in the UK for the duration of the study (n = 55)
ApproachedFace to Face46 patients
6 patients declined No reason given for withdrawal
Approached by telephone 9 patients
Total recruited to
the study (n = 49)
Recruitment timeframe4 months
76

Of the 55 eligible patients 46 were approached face to face by the researcher during an in-patient stay or during an out-patient visit and given a full explanation of what participating in the study involved. A Patient Information Leaflet was given (Appendix F) for them to read. Since there were a number of phases, including multiple data collection, it was explained to them that they were being asked to take part in a study which involved them in using and testing a new self-management physiotherapy programme (SMPP) the purpose of which was to improve their adherence to physiotherapy. This would involve them in being asked to complete two questionnaires issued at the beginning and end of the study period to evaluate the effectiveness of the SMPP. In addition they may also be asked to participate in a semi-structured interview or in pilot studies for the self-completed questionnaire or the SMPP. Participating in the study would involve them being contacted several times over the study period. It was anticipated that participation in the research would not involve additional visits to the hospital. They were also informed that they could withdraw from the study at any point and not have to give a reason why. They were reassured that if they chose to withdraw their treatment would not be affected in any way. The researcher’s contact telephone numbers were given in case they needed to discuss taking part, or to obtain further details. It was stressed that the study was seeking their views, their comments would be valued and they would not be judged by their replies. There were no right or wrong answers and that their input was essential to ensure that any potential improvements to the delivery of physiotherapy treatment would be developed from their perspective. It was emphasised that the information they gave would be confidential and that the responses would have names removed, with each participant given a code number known only to the researcher. They were encouraged to take time to consider whether they wanted to participate or not and given an opportunity to ask questions. If they were prepared to continue, the patient was asked to sign two consent forms (Appendix K) which were witnessed by the researcher. A copy of each of the consent forms was given to the participant and the two originals were put in their medical notes. In the face to face recruitment phase, 46 patients were approached.
Telephone
When the four month face to face recruitment period passed there were nine eligible patients still remaining to be seen. When contacted by telephone, patients who showed an interest in the study were given preliminary information about it and sent the Patient Information Leaflet (Appendix F) and the Consent Forms (Appendix K). A stamped addressed envelope was enclosed for the return of the consent forms. Each patient was encouraged to contact the researcher for further information if they
77

wished and a contact telephone number was given to them in the Patient Information Leaflet (Appendix F). For patients who had not responded after three weeks, a one off follow up telephone call was made. If the patient expressed an interest but after a further three week period the consent forms had not been returned, a letter was sent as a one off reminder. If the consent forms had still not been returned no further action was taken since it was unethical to be coercive in recruiting participants. Of the 55 eligible patients 46 were approached face to face, nine were approached by telephone and in total 49 patients agreed to participate in the study.
Study Population
The total study population comprised 49 participants from which sub-groups were selected to take part in semi-structured interviews and pilot studies for the development of the self-completed questionnaire and the SMPP. The semi-structured interviews are outlined in Chapter 4 and the pilot studies are outlined in detail in Chapters 5 and 6.
3. 6. Outcome Measures
In order to evaluate the effectiveness, or other wise, of the SMPP to improve adherence to physiotherapy it was important to select outcomes measures that were sensitive enough to accurately measure changes that had occurred as a result of the implementation of the SMPP. Initially QoL was chosen but it was subsequently not used for reasons outlined below. The lung function test of the forced expiratory volume in one second (FEV1) and Body Mass Index (BMI) were used in addition to the participants self-reporting their level of adherence at the beginning and end of the study period by means of a self-completed questionnaire.
(a) QoL
The ethical submission for the study included the use of a CF health related QoL outcome measure that had been developed and validated by Gee, Abbott, Conway, Etherington and Webb (2000). It was initially postulated that if the SMPP improved adherence and thereby potentially brought about improved health outcomes the participant’s QoL would benefit. However prior to the start of the study the use of this QoL measure was re-evaluated and it was decided that the factors outlined below would compromise the validity and reliability of any QoL findings as the effectiveness or otherwise of the SMPP had yet to be determined. Without knowing
78

whether the SMPP improved or impeded the ability to adhere to physiotherapy treatment it would not be possible to evaluate any related changes the participants QoL for the following reasons:
QoL is used to evaluate well being and is a complex issue. QoL is a measure of how a person perceives their own well being to be and is not the absence of ill health. It needs to be distinguished from health status which is an objective measurement of the state of a persons’ health (World Health Organisation Quality of Life (HOQOL), 1995). In CF health status is frequently measured in physiological terms of lung function, using the FEV1, and the Body Mass Index (BMI) as an indicator of nutritional status. It has been identified in CF QoL studies (Abbott, Dodd, & Webb, 1995; Gee et al., 2000) that how a person with CF evaluates their own QoL is based significantly more on how they perceive their health to be rather than their actual health status. There are also gender differences in how QoL is perceived for people with CF, with women who have a similar health status to men reporting a poorer QoL (Gee et al., 2000; Patterson et al., 2008) for reasons that remain unclear.
Duration of the study
The study intervention period of six months was over the winter period which is when there is usually an increased prevalence of chest infections accompanied by a corresponding increase in chest physiotherapy treatment. Chest physiotherapy has been identified as burdensome in several studies (Daniels, 2010; White et al., 2007; Ireland, 2003) therefore it would be unlikely that during the winter months when there is often a need to increase chest physiotherapy, that the participants would perceive that their QoL had improved as the burden of increased treatment would probably compromise their QoL in the short term. In the longer term (i.e. a year or more) adherence to physiotherapy treatment would be expected to reduce the impact of deteriorating lung function brought about by repeated chest infections and thereby be more likely to bring about a measurable improvement in QoL but this could not be established during the short duration of this study.
Sample Size
At the time of the study the number of potential participants was low (n = 61). This number would be further reduced due to those who would decline to take part, the inclusion/exclusion criteria, drop out rate, life changes, serious illness and death. Because QoL is perceived differently by men and women, if the study population was divided by gender the number of participants in each group would be very small and
79

consequently compromise the validity and reliability of any QoL outcome measures as they may not then be applicable to the general CF population.
In view of the above factors it was decided not to use a QoL outcome measure until the effectiveness or otherwise of the SMPP had been established. If the SMPP proved to be effective in improving the ability to adhere to physiotherapy treatment then future long term studies of greater than a year would warrant the inclusion of a valid QoL measure, the purpose of which would be to assess the impact of increased adherence to physiotherapy bringing about improved health outcomes.
(b) FEV1
FEV1 was used as an outcome measure to monitor the participants level of disease severity before and after the trial period as part of the process of evaluating the effectiveness or otherwise of the SMPP. FEV1 is a lung function test that is a valid, reliable and objective method of measuring the respiratory state of the lungs. It is a simple standardised objective pulmonary function test that is a well established marker of disease severity and life expectancy (ATS, 1989; Aurora et al., 2000; Sharma, et al., 2001; Belkin, Henig, Singer, Chaparro, Rubenstein et al., 2006). It is measured as a percentage of predicted normal values and provides information about the nature of airway obstruction. FEV1 has been defined as the maximal volume of air exhaled in the first second of a forced expiration from a position of full inspiration, expressed in litres at BTPS (Body temperature (i.e. 37°C)) (Miller et al., 2005). Percentages are calculated based on predicted normal values for FEV1, age, sex, height, weight and ethnicity with levels of severity graded appropriately for each specific respiratory disease. Values of between 80% and 120% of the average value are considered normal.
It was important to determine the study participant’s FEV1 for two reasons: To establish the level of disease severity of the study population in relation to
the National CF Database (CF Trust, 2000) population at the time of the study in order to determine whether the results were generalisable or not
To determine whether the FEV1 deteriorated significantly during the six months study period. However, studies have shown that people with CF (Abbott et al., 1996; Kettler et al., 2002) increase their adherence to treatment if they are anxious about their deteriorating health, so in this study a finding of increased adherence to physiotherapy could be attributed to anxiety about deteriorating health rather than effectiveness of the SMPP to improve adherence. Therefore the study would need to
80

demonstrate that adherence had increased and the FEV1 had not fallen significantly in which case the increase in adherence could be attributed to the effectiveness of the SMPP. Without measuring the FEV1 it would impossible to evaluate the effectiveness or other wise of the SMPP.
(c) Body Mass Index
Body Mass Index (BMI) is used to indicate how well nourished a person is (Walters & Mehta, 2007). Mal-nourishment and accompanying weight loss occurs in CF as a result of pancreatic insufficiency, mal-absorption and the inability to digest fat. As body weight for the normal population has a significantly large range, the BMI is commonly used as an alternative indicator of how well nourished a person is. The BMI is calculated by dividing the weight in kilograms by the square of the height in metres (KG/M2); the normal range is 20-25 kilograms/M2. Indices below 20 are considered to be under weight, indices between 25 and 30 are classified as overweight, while values exceeding 30 are classified as obese. Having a BMI of less than 20 is indicative of mal-nourishment which results in depression of the immune system, and in CF an increased risk of infection and fatigue of the respiratory muscles (Pryor & Prasad, 2008). Fatigue is a significant problem for people with CF as it can reduce the ability to effectively carry out chest physiotherapy and exercise programmes.
It was important to determine the study participants’ BMI in order to establish their nutritional level in relation to that of the National CF Database (CF Trust, 2000) at the time of the study. The purpose of the National CF Database (CF Trust, 2000) was to register of all the adults and children in the UK with CF in order to establish their health and social characteristics so that standards for treatment could be developed, health care costs identified and trends for future care needs predicted. If the study population’s BMI was significantly higher than that of the National CF Database (CF Trust, 2000) then the study population would be likely to be fitter, healthier, tire less quickly and as a result be able to do their chest physiotherapy and exercises more effectively and potentially have fewer chest infections. The converse would also be true, that if the study population’s BMI was significantly worse it would result in a greater need for chest physiotherapy due to a poor immune system that would result on an increase in chest infections. This increased burden of treatment could compromise the ability to adhere to treatment. If there was no significant difference then the health of the study population would be comparable to that of the National CF Database (CF Trust, 2000) making the results generalisable.
81

Summary for Methodology
The purpose of the study was to discover why people with CF have difficulty adhering to physiotherapy and to use that information to develop an intervention in the form of a SMPP to potentially optimise the ability to adhere to treatment. The action research approach selected, the “Professionalising” typology chosen and the outcomes measures set. The study population was defined and the recruitment strategy implemented. How the action research process was initially applied to the study is described in Chapter 4.
82
CHAPTER FOUR – THE ACTION REASERCH CYCLE APPLIED TO THE STUDY
4. 0. Introduction
The aim of this chapter was to meet the first three study objectives:
1. To investigate the problems that people with CF have with adherence to physiotherapy prior to the study
2. To investigate the level of adherence to physiotherapy treatment prior to the study
3. To develop and test the effectiveness of the SMPP
The study set out to apply an action research approach to identify the problems adults have with adhering to physiotherapy from their perspective. The action research model has four parts comprising plan, action/intervention, evaluation and reflection which are incorporated into one cycle (Ch. 3 p. 60). Each stage of the action research cycle influenced the development of the next stage although in this process led and professionally determined action research “Professionalising” typology the process, but not the content, was pre-determined. Although many stages overlapped for reasons of clarity the process undertaken at each stage is fully described sequentially.
How the action research model was initially applied to the study is outlined below. Following the analysis and findings of the semi-structured interviews in Part I – Plan (Stage I – Identification of the Problem), it became apparent that action research, which requires the participants to be fully involved in the development, design, and evaluation of the research process, was not warranted and therefore the study no longer complied with the action research approach. How the research process was subsequently re-designed is outlined in p. 115.
4. 1. Initial Structure of the Study
How the four parts of the action research cycle were initially planned are outlined below:
83

Fig. 4. 1. The action research cycle
Part 1 - The Plan
Part 1 – Plan (What to Do) had three stages. Within each stage there were several phases as outlined above:
4. 2. Stage 1 - Identification of the Problem
4. 2. 0. Introduction
Stage 1 was concerned with identifying the problem by means of
THE ACTION RESEARCH PROCESS – FIRST CYCLE
1. Plan The Planning phase has 3 stages: Stage 1. Identification of the Problem Selection of methodological approaches and the development of the methodological tools
Phase I – First Set of Semi- Structured Interviews Phase II – Second Set of Semi- Structured Interviews Phase III- The Survey
Stage 2. Development of the Innovation Phase I – Developing the SMPP Phase III – Piloting the SMPP
Stage 3. Preparation for Change 2. ActionImplementation of the intervention (SMPP)
4. Reflection Discussion Conclusion Recommendations for
Clinical Practice Recommendations for
Future Research Limitations Reflections
3. Evaluation
Stage I Evaluation Tools Feedback Chart Post - Intervention Physiotherapy Questionnaire Stage 2. Analysis of the Pre and Post Intervention Physiotherapy Questionnaires Stage 3 Evaluation, Results and Discussion
84

(a) selecting the methodological approaches
(b) development of methodological tools
The research process was influenced by the need to comply with infection control guidelines issued by the CF Trust (2011a, 2008, 2004a, 2004b). In a health care setting infection control is a major issue for people with CF as they are not encouraged to mix socially with each other due to the risk of cross infection through exposure and resultant colonisation of the pathogens Pseudomonas and MRSA (Methicillin Resistant Staphylococcus Aureus). Both of these pathogens result in a marked deterioration in lung function and general health. The CF Trust (2011a; 2008a, 2004a, 2004b) advocates a policy of segregation for people with CF identified as having MRSA or Pseudomonas during in-patient admissions and out-patient clinics.
Although consideration was given to such research tools as focus groups, which encourage interactive discussion across a broad range of topics, it was dismissed because of the risk of cross infection between participants and also because some participants could find it an inhibiting environment and prevent them from disclosing rich detail. Observation would be impractical and case studies unsuitable due to the diversity in health and social characteristics in the study population. In view of these factors careful consideration was given to the selection of data collection methods which are outlined in section 4. 2. 2. (b) Development of Methodological Tools, p. 86.
4. 2. 1. (a) Selecting the Methodological Approaches
The information obtained during the extensive literature search (Chapter 2) helped in both the selection and development of the methodological approach. This action research study set out to apply the “Professionalising” typology (Hart & Bond, 1996) using a mixed methodology, involving the collection of qualitative and quantitative data in order to understand the complex problems of adhering to physiotherapy from the participants perspective.
Qualitative Data
Qualitative research seeks to describe, understand and explain a particular phenomenon in order to make visible the experiences and perceptions of the research participants (Parahoo, 2006; Topping, 2006). Qualitative research provides explanations of why something happens in a particular way and seeks typologies or classifications of grouping people (or situations) that tend to have common
85

characteristics, opinions and experiences (Marshall & Rossman, 2006). Qualitative data was needed to identify what problems the study participants encountered whilst doing their physiotherapy, their coping skills, health beliefs, their perceptions of having CF, and the impact CF and physiotherapy treatment had on their lives. This qualitative data informed the development of questions for the survey and the design of the SMPP. The collection of qualitative data was a proceeding step to ensure the relevance of the survey and the SMPP. In view of these considerations the qualitative data collection method chosen was the semi-structured interview and is described in section 4. 2. 2. (b) below - Development of Methodological Tools – Qualitative Approach below.
Quantitative Data
In the social sciences, quantitative research refers to the systematic empirical investigation of phenomena and their relationships. The objective of quantitative research is to develop and employ mathematical models, theories and/or hypotheses pertaining to phenomena (Parahoo, 2006; Topping, 2006). The process of measurement is central to quantitative research because it provides the fundamental connection between empirical observation and mathematical expression of quantitative relationships. The quantitative data method chosen for the study was a survey and is described in section 4. 2. 2. (b) Development of Methodological Tools – Quantitative Approach below. .
4. 2. 2. (b) Development of Methodological Tools
The methodological tools of the semi-structured interview and the survey were selected following careful consideration of the need to meet the research objectives and to comply with the CF Trust’s infection control guidelines (CF Trust 2004a; 2004b).
Qualitative Approach: Method – The Semi-Structured Interview
The semi-structured interview gives a one-to-one relationship between the participant and the interviewer enabling rich detail to be collected (Silverman, 2005). The semi-structured interview is conducted by grouping topics and questions that the interviewer can ask in different ways for different participants in a topic guide (Denzin & Lincoln, 2005; Topping, 2006). This freedom can help an interviewer tailor their questions to the interview situation and to the people they are interviewing, with the aim of providing in-depth qualitative information from the participant’s perspective about a ‘real world’ situation. A semi-structured interview, informed by a
86

topic guide, enables an experienced interviewer to probe the answers in detail but the order and content of the prompts can vary depending on the individual’s response (Tod, 2006).
The disadvantages of the interview method is that it is time-consuming, expensive if it is necessary to have help transcribing the interviews (McKenna, Hasson, & Keeney, 2006), and it can be prone to reflexivity on the part of the interviewer. Reflexivity occurs when there is a lack of objectivity in how a situation is being evaluated. The risks can be minimised by using critical thinking to reflect on the information being analysed and by asking a colleague to be involved in the analysis and evaluation to bring rigour and objectivity to the process.
Quantitative Approach: Method - The Survey
The purpose of a survey is to obtain information on a current situation or phenomena in order to describe what exists with respect to variables or conditions (McKenna et al., 2006; Silverman, 2005). In this study a survey in the form of a self-administered questionnaire was developed, as at the time of the study there was no validated questionnaire for collecting information from adults with CF that would meet the study objectives. The purpose of the survey was to collect data from a purposive sample of all the eligible participants in the study group which ensured that no sub-group was excluded and that the information collected was as representative as possible. The survey was issued in two stages, before and after the implementation of the SMPP, to monitor any changes which may have occurred. The questionnaire, developed and administered before the implementation of the SMPP was called the ‘Pre-Intervention Physiotherapy Questionnaire’. It was issued again at the end the study period as the Post-Intervention Physiotherapy Questionnaire when two additional questions were added to evaluate the effectiveness of the SMPP to improve their ability to adhere to physiotherapy.
4. 2. 3. Summary of Selecting Methodological Approach
By combining qualitative and quantitative methodological approaches and selecting valid and reliable methodological data collection tools (the semi-structured interviews and the survey) information giving an in-depth understanding of the complex issues surrounding adherence to physiotherapy could be better understood. How this information was collected is outlined in Phase I and II.
87

4. 3. Stage 1 Phase I – The First Set of Semi-Structured Interviews
4. 3. 1. The Development of the Semi-Structured Interview
The First Set of Semi-Structured Interviews were conducted so that the participants could describe, in their own words, the problems they were having with adhering to physiotherapy and their perceptions of having CF. The information from these semi-structured interviews was analysed and used to inform the development of the survey and the design of the SMPP.
The purpose of conducting the semi-structured interviews was to meet the following research aims:
1. To investigate the problems that people with CF have with adherence to physiotherapy prior to the study
2. To investigate the level of adherence to physiotherapy treatment prior to the study
3. To contribute to the development of the intervention – the SMPP
The same prompts were used for all the interview participants enabling comparisons to be made from the responses. This would not be possible in an unstructured interview, as the interviewee determines the course of the interview which could result in some important aspects not being addressed, the collection of large amounts of irrelevant information and the analysis being made more difficult.
4. 3. 2. Process
The First Set of Semi-Structured Interviews were carried out by a clinical psychologist who had experience of working with adults with CF but had not worked in the Adult Specialist CF Centre. The clinical psychologist was chosen because of their pervious experience of working with adults who had CF and there was an expectation that the participants could speak more freely to someone who was unknown to them. It was deemed inappropriate for the researcher/ physiotherapist to conduct the semi-structured interviews as it was considered that this would assert undue influence on the information being exchanged, because at the time of the study, the researcher was the only physiotherapist responsible for this group of patients and was well known to them.
The disadvantage however was that the clinical psychologist might not have an in depth knowledge of physiotherapy and therefore may not be able to set the
88

information given into context or explore the issues raised in sufficient depth. This problem was minimised by the researcher/physiotherapist discussing in detail with the clinical psychologist the physiotherapy treatment modalities for CF in order to ensure they had sufficient knowledge to enable exploration of these issues during the interview process. The interviews took place in one of the CF Centre offices which was a private area and a familiar setting for the participants. The interviewer used a topic guide to provide a framework and relied on the interviewee to direct the conversation.
The Semi-Structured Interview Topic Guide
The interview topic guide was developed following a review of the literature and discussions between the researcher/physiotherapist and the clinical psychologist. The topic guide was developed around the areas of discovering what problems the participant had with adhering to physiotherapy, what having CF meant to them and what health beliefs they had. Prompts were used to ensure that the topics raised were fully explored. Open-ended questions, based on topic areas, were pre-prepared but not prescriptive. This approach can give a richness and depth in the replies around the topic areas (Tod, 2006) whilst providing opportunities for both the interviewer and interviewee to clarify questions and responses. At the end, an open question was added to ensure that the participants had the opportunity to raise any issues they considered had not been addressed. The following topics were covered (Fig 4.2).
Topic Guide Experience of having CF The impact that physiotherapy had on their lives Establish what physiotherapy they were doing/not doing Establish their views on the effectiveness of their physiotherapy programme Establish what they considered the impact of not doing physiotherapy to be Establish what exercise/activity they were doing Enquire whether they had any further views about having CF and
physiotherapy that may not have been discussed in the interview
Fig. 4 . 2. Topic guide for the semi-structured interviews
Based on recommendations (Rubin & Rubin, 1995) of the importance of bringing the participants back to a positive frame of mind and leaving them feeling calm, the interviewer ended with summing up the main points of the interview and emphasised the valuable contribution of the interviewee towards meeting the study objectives.
89

Recruitment to the Semi-Structured Interview
Of the total clinic population of 61 ‘full care’ patients, 55 were deemed eligible, and of these 49 entered the study by consenting to participate in it. A purposive sample was chosen from this study population (n = 49). Three 3/49 (6.2%) participants were selected with each one representative of one of the three classifications of adherence to physiotherapy previously defined in Chapter 1, p. 17:
Adherent – that which has been agreed between the researcher/physiotherapist and the participant and the participant reports that they are implementing it.
Partial Adherent – that which has been agreed between the participant and the physiotherapist but the participant reports that they are only partially implementing it.
Non-Adherent – that which has been agreed between the physiotherapist and the participant but the participant reports that they are not implementing it, and participants who report that they do not do any physiotherapy.
The participants classification of adherence was determined by the participant self-reporting it and the clinical judgement of the researcher/physiotherapist. Although one participant from each level was a small number, the interviews at this stage were a preliminary information gathering exercise.
While they were in a stable state, either during an in-patient stay or an out-patient visit, the first participant to be approached in each of the three categories of adherence the researcher/physiotherapist agreed to be interviewed. The interviewees were identified as Interviewee 1 (adherent), 2 (partially-adherent) and 3 (non-adherent). An explanation was given as to the purpose of the interview, and how it would be conducted by using a topic guide covering areas that related to their values, feelings and behaviour regarding having CF, and any issues they may have in adhering to physiotherapy. Although the approach was made by the researcher/physiotherapist, thus potentially making it difficult for the participant to decline, every effort was made neither to influence nor coerce any of the participants to take part. Steps were taken to carefully explain the purpose of the interviews and answer any questions that potential interviewees had. They were also informed that they could refuse without having to give a reason, and it would not affect their treatment now or in the future. Written consent was obtained from each interviewee (Appendix L) and placed in the participant’s physiotherapy notes. It was considered that these three representative case studies would give a sufficient information about the problems of adhering to
90

physiotherapy, and the findings would provide valid and reliable information to inform the development of the survey and the design of the SMPP.
4. 3. 3. Three case studies selected for the first set of semi-structured interviews
The following three case studies were indicative of the three categories of adherence:
Interviewee 1 – Adherent
24 year old single female – full time student –living away from home Moderately severe CF disease – first admission to hospital at 14 years Rebelled as a teenager and avoided treatment – she felt that fewer hospital admissions would equate with her being well – he less attended the CF unit the better she thought she was Daily treatment - inhaled antibiotics and bronchodilators – 40 minutes twice a day plus vitamins and enzymes Has changed in her approach to CF over the years and now sees the CF Unit as being supportive This positive approach has resulted in improved and maintained good health CF does not interfere that much in her life – she adapts her life to accommodate its consequences She ‘normalises’ her life by comparing it to people who do not have CF – and is aiming to work from home She exercises twice a week and considers this “normal” activity to be part of her treatment She feels in control of her disease and that what she does has an impact on it Because she fells she can control her disease she is adherent to it
Fig. 4. 3. Interviewee 1 – Adherent
91

Interviewee 2 – Partially Adherent
24 year old single male who works full time in an office He considers that he copes well and just ‘gets on with life’ He has moderate/mild CF with liver and spleen complications Daily treatment ( antibiotics and bronchodilators – 40 minutes) and vitamins and enzymes He only does chest physiotherapy when he is unwell – being fit and active he considers is adequate He has an “educated” approach to doing chest physiotherapy. He considers that chest physiotherapy is beneficial when he is ill but there is no discernable clinical improvement in his chest when he is well, so he does not do any . Having CF does not stop him leading his life within normal parameters
Fig. 4 .4. Interviewee 2 – Partially Adherent
Interviewee 3 – Non-Adherent
24 year old single male – part time student – in a pop group Mild CF but moderate/severe asthma – weight and height below average Poor attendance at clinic- he feels well therefore does not see the need to attend Goes to the gym 3 or 4 times a week which he thinks is adequate Lives in a lively household with 4 other single men – busy social life goes clubbing at week-ends Daily treatment – nebulised bronchodilators and antibiotics – 40 minutes x 2 daily Does not do physiotherapy – knows what he ought to do. When an in-patient he is very adherent but does not continue with treatment on discharge Has a “happy go lucky” attitude that compromises his well being ● He considers that if he does not attend the CF Unit he must be well
Fig. 4. 5. Interviewee 3 – Non Adherent
Interview Process
Each interview was audio recorded and lasted approximately one hour. The three interviews were conducted over a period of three months by the clinical psychologist. The interviews took place on a day when the interviewee was attending clinic or was an in-patient or on a date and time that was convenient to them. After the interview each recording was fully transcribed by a medical secretary with experience in transcribing.
92

4 . 3. 4. Analysis of the First Set of Semi-Structured Interviews
There are a number of different ways of analysing qualitative data and after careful consideration thematic analysis approach was chosen. The analysis of qualitative research, which involves complex social phenomenon, necessitates a pragmatic, subjective and interpretive approach that allows for reflection on the findings as they emerge (Braun & Clarke, 2006). As the purpose of this exploratory study was descriptive, a theory building inductive approach was considered to be the most suitable, rather than a theory testing approach as evident in the deductive approach. When analysing qualitative research the researcher needs to have an awareness of reflexivity, as their own perspective on a situation can influence their interpretations of the phenomenon they are studying (Holloway & Wheeler, 2010). Although the researcher had extensive experience of CF, she was aware of the impact that this could potentially have when analysing the data and therefore had to be rigorous in maintaining an open perspective by using critical thinking as a form of reflection. Critical thinking (Castle, 2009; Paul & Elder, 2006) is the art of analysing and evaluating thinking, with a view to improving it. It is a self-directed, self-discipline which exercises clarity, accuracy and precision in thinking with the aim of eliminating bias and distorted thinking processes.
Thematic Analysis
Thematic analysis is a systematic approach to data analysis through a series of transparent steps that provides an audit trail (Holloway & Wheeler, 2010). Thematic analysis was chosen as it is a flexible approach that enables the researcher to make active choices about the particular form of analysis they are engaged in (Braun & Clarke, 2006). Thematic analysis is ideally suited to qualitative research and in particular exploratory studies, such as this one, where the participant’s views were unknown. Boyatizis (1998) characterises thematic analysis as a tool to use across different methods in order to identify, analyse and report patterns (themes) within data. It is the identification of themes within the interview data that informed the development of the survey and the design of the SMPP.
The underlying epistemology was based on an essentialist (realist) perspective where motivations, experience and meanings were interpreted in a straight forward way as it was assumed that there was a unidirectional relationship of meaning, experience and language. Braun and Clarke (2006) state that themes or patterns can be identified within the data through an inductive approach, which means that themes are strongly
93

linked to the data. This inductive data driven approach meant that the coding of the data did not fit into a pre-existing coding frame.
A theme (Braun & Clarke, 2006) captures something important about the data in relation to the research question and represents some level of patterned response or meaning within the data set. Themes were identified at a semantic (explicit/surface) level and no attempt was made to look for anything beyond what the participant said. The study was exploratory in nature and the area under researched, therefore it was considered that a “surface” level approach was appropriate at this stage.
The data was analysed according to the six phases of thematic analysis (Braun & Clarke, 2006):
Table 4. 1. The six phases of thematic analysis (Braun & Clarke 2006, p. 78)
Phases
Description
1. Familiarisation with the Data
Transcribing reading and re-reading the data
2. Generating initial Codes Coding interesting features of the data in a systematic fashion across the entire data set, collating data relevant to each initial code
3. Searching for Themes Collating initial codes into potential themes, gathering all data relevant to each potential theme
4. Reviewing the Themes Checking if the themes work in relation to the coded extracts (Level 1) and the entire data-set (level 2), generating a ‘thematic map’ of the analysis
5. Defining & naming themes
Ongoing analysis to refine the specifics of each theme and the overall story the analysis tells, generating clear definitions and names for each theme
6. Writing the Report Final opportunity for analysis. Selection of vivid, compelling extract examples, final analysis of selected extracts, relating back the analysis to the research question and literature, producing a scholarly report of the analysis.
The Application of Thematic Analysis to the First Set of Semi-Structured Interviews
Once the three semi-structured interviews had been conducted they were transcribed verbatim by a medical secretary and audited by the researcher/physiotherapist. Each transcript was carefully listened to, re-read, checked for accuracy and a preliminary thematic identification of both the taped and transcribed text was made (Miles & Huberman, 1994) using the thematic analysis approach outlined below.
94

Phase 1. Familiarisation
The researcher listened to the tape recordings and “actively” read and re-read the transcriptions so that she was fully immersed in the data, in order that the participants “life world” (Burnard, 1991, p. 161) could be appreciated and understood. The recalling of their experiences gave rich detail which contributed to the knowledge and understanding of the problems they experienced adhering to physiotherapy treatment.
Phase 2. Generating Initial Codes
When the transcripts were read through again core ideas and concepts began to emerge comprising of key words and phrases or frequently repeated terms and nouns (Rubin & Rubin, 1995). These words or phrases constituted “units of meaning” which were grouped together and generated initial codes as outlined below for each of the interviews (Fig. 4. 6). Each of the initial codes was used to describe a selection of the “units of meaning” assigned to them. The code numbers were a consecutive series of numbers selected as a convenient means of identifying initial codes. Examples of initial codes and their assigned number are illustrated below.
Number Initial Codes
1. Positive view of their ability to influence their health outcomes
2. Negative views on their ability to influence their health outcomes
3. Adherence to physiotherapy
4. Being in control
5. Optimistic
6. Effectiveness of physiotherapy
7. Problems of having CF
8. Having a life threatening disease
9. “Normalising” having CF
10. Denial of clinical state
Fig. 4. 6. Initial codes generated from the data set
95
How the “units of meaning” from each interview were initially coded is outlined below:
Interviewee – 1
Raw Data Extracted (Units of Meaning) Initial Code
Positive Approach 1 Interventions and treatment – enabling 3 Treatment is a good outcome 4; 5 Physiotherapy controls my disease 4; 6 Early interventions minimise impact of CF 5; 7 CF does not interfere with my life but is a big part of it 7; 8 I have to take CF into consideration 7; 8; 9 I’m worried about not doing physiotherapy 3 CF is not controlling me 4; 5; 8Physiotherapy has to be done. It does not often slip 3 CF is part of my normal life 7; 8; 9
Interviewee 2
Raw Data Extracted (Units of Meaning) Initial Codes
I am fit and active 1 Routine Physiotherapy has no benefit 6;3 When unwell I do physiotherapy 3; 6. I have mild disease therefore no need to do physiotherapy routinely 6; 7; 10Not disadvantaged by having CF 7; 9; 10I’m not too bad. I have mild CF; I’m lucky 7; 9; 10CF does not affect my life at all 7; 8; 10 Got to look after myself 1; 8; 10 I feel in control of my health 1; 4
Interviewee – 3
Raw Data Extracted (Units of Meaning) Initial Codes
I’m not in control of my life 4; 5 If I need treatment I must be unwell therefore if I do not have any treatment I must be well. It is a stupid way of looking at it but that’s it
1; 7; 10
I go to the gym – it is as good as chest Physio 6 I am happy to have Physio when in hospital but I give up when I go home
3; 6
I’m not too bad therefore there is no need for me to do it 6; 7; 10 CF gets me down but I do not dwell on it 7; 8 I know that physio is important but I cannot be bothered to do it 6; 2
96

Physio interferes with my life 7; 6
There is no one out there to remind me to do it 7; 8
Fig. 4. 7. Coding
Phase 3. Searching for Themes
The purpose of this stage was to identify potential themes that appeared from the initial coding of the data set, and to re-focus the analysis at the broader level of themes rather than at the initial coding. The aim was to combine, collapse and remove duplication. Initial codes were grouped into potential candidate themes which were set out in a table format. At this stage a relationship was being sought between the initial codes and the candidate themes, resulting in candidate themes being collapsed and merged into overarching themes. This process resulted in four overarching themes being identified (Table 4. 2., p.98).
Phase 4. Reviewing the Themes
The themes were reviewed and refined at two levels. Level one involved reviewing at the level of the data extracts that had been grouped into initial codes to check whether they had formed a coherent pattern that represented the analysed data. On being reviewed it appeared that the data extracts grouped into initial codes were correctly reflected in the candidate themes. The second stage involved the re-reading of the three transcripts in order the check that candidate themes and the four overarching themes accurately reflect the meanings evident in the data set as a whole, which they appeared to. A coherent pattern emerged of the overarching themes focusing on:
Health Beliefs Physiotherapy Perceptions of having CF Denial
These four overarching themes worked in relation to the data set and were collapsed into two final themes i.e. the overarching theme of “Denial” was submerged into the final theme of “Health Beliefs” while the theme of the ”Physiotherapy” was collapsed into the final theme of “Perceptions of Having CF”, because how a person perceives having CF can influence their ability to adhere to physiotherapy. These two final themes are further defined in Phase 5 which is outlined in Table 4. 4., p. 98.
97

Table 4. 2. The Themes
Quotes Initial Codes
Candidate Themes Overarching Themes
Final Themes
“you have to give it a go” ”I’m in control” “I put on a positive side and do anything
you want” “Should I bother really because I could
be dead in 2 years”
1 4 5
2
Positive views on their ability to influence health outcomes
Negative views on their ability to influence health outcomes Control Optimism
Health Beliefs
Health
Beliefs
“no need to do it unless I am unwell” “without it I would not be as well “It’s always horrible and negative”
N
10 6 2
Adherence Effectiveness of physiotherapy Physiotherapy
“my life is not any different to that of my friend”
”it hits you , I’m dying”
9
8
Problems of having CF Having a life threatening disease Normalising having CF
Perception of Having CF
Perception ofof Having CF
“I put it out of my mind” “I always forget about it” “Putting it on the back burner” “It is difficult to come to terms with”
10 310 7
Not acknowledging having CF Accessing the physiotherapy service but at
a sub-optimal Level
Denial
98

Phase 5. Defining and Naming the Final Themes
Phase five is the final defining and refinement of the themes which ensures that the final themes identify the essence of the candidate and over arching themes. The two final themes which emerged across the data set that appeared to influence the participant’s ability to adhere to physiotherapy treatment were:
Health Beliefs
The theme of “Health Beliefs” is significant because CF is a life limiting disease for which there is no cure. If a person with CF has positive health beliefs and thinks that what they are doing can have a positive impact on their health outcomes they are more likely to adhere to physiotherapy e.g. Interviewee 1, who was adherent, believed that “physiotherapy controls my disease”. The reverse is true with negative health beliefs e.g. Interviewee 3, who was non-adherent stated that “I know that physio is important but I cannot be bothered to do it”.
Perception of Having CF
The theme of “Perception of Having CF” is significant because if a person with CF accurately perceives their level of disease severity they are more likely to be able to effectively manage it by adhering to treatment and seek help promptly if they deteriorate, but if they fail to accurately perceive their disease severity then they are less likely to contact the CF Team in a timely fashion and less likely to adhere to treatment, e.g. Interviewee 3, who is non-adherent stated that “If I need treatment I must be unwell, therefore if I do not have any treatment I must be well. It is a stupid way of looking at it but that’s it”.
Having named and defined the overarching themes the report below sets them into the context of the study.
Phase 6. The Report
The purpose of the First Set of Semi-Structured Interviews was to provide background information to inform the development of the survey and the design of the SMPP so the report (conclusions) was brief and succinct. As this was just an exploratory information collecting process, it was not considered warranted to refer the transcripts and report back to the interviewees.
99

The report outlines the following conclusions:
1. The two final themes of ‘Health Beliefs’ and the ‘Perception of Having CF’ indicated that these factors influenced the interviewee’s approach to their disease, their management of it and how adherent they were to physiotherapy treatment. For purposes of clarity these two themes are presented with those from the Second Set of Semi-Structured Interviews in Discussion of the Findings (Themes) from the First and Second Set of Semi-Structured Interviews (p.98).
2. The analysis identified that for these three interviewees having CF was a significant burden which they attempted to rationalise and normalise so that they could cope more easily. For them physiotherapy was burdensome, time consuming and its effectiveness questioned by Interviewee 3. The participants in the First Set of Semi-Structured Interviews gave rich in-depth detail however following analysis of the transcripts and discussions with the interviewer it was decided that a second set of semi-structured interviews would be appropriate so that the issues raised in the first set could be explored in greater depth.
The process of the Second Set of Semi-Structured Interviews is outlined below in Phase II:
4. 4. Stage I - Phase II - The Second Set of Semi-Structured Interviews
4. 4. 0. Introduction
The aim of the Second Set of Semi-Structured Interviews was to explore issues raised in the First Set of Semi-Structured Interviews to add richness to the data. The final themes of ‘Health Beliefs’ and the ‘Perception of Having CF’ needed to be investigated in greater detail as they appeared to influence the ability of the interviewees to adhere to physiotherapy treatment. The knowledge obtained by the clinical psychologist from conducting the First Set of Semi-Structured Interviews enabled her to obtain greater depth when carrying out the Second Set of Semi-Structured Interviews.
4. 4. 1. Selection of Interviewees
Considerable thought was given to the selection of the interviewees to ensure that the sample was representative of the three categories of adherence, i.e. adherent, partially
100

adherent and non-adherent, as outlined in Chapter 1, p. 17. Ideally it would be appropriate to have representatives of all three levels of adherence as well as having a representative sample of males and females. The only way of achieving this was by purposive and opportunistic selection.
From the total study population (n = 49) a different set of participants from those chosen to be in the First Set of Semi-Structured Interviews was selected in order to ensure as wide a range of responses as possible. Of the first 8/49 (16.3%) study participants approached face-to-face while they were in a stable state, either during an in-patient stay or during an out-patient visit, 5/49 (10.3%) agreed to take part and signed the relevant consent form (Appendix L). The potential interviewees were informed of what the interview process involved and that they could refuse without it influencing their treatment now or in the future. The remaining 3/49 (6.1%) declined for a variety of reasons. The interviewees were identified as A, B, C, D, and E. Each tape-recorded interview took approximately one hour and was conducted in one of the offices in the Adult CF Specialist Centre. The topics were the same as those used in the First Set of Semi-Structured Interviews as they had proved to be effective in eliciting full answers.
The characteristics of the interviewees in the Second Set of Semi-Structured Interviews are outlined below.
Males Females
Approached 2 6
Declined 0 3
Adherent Partially Adherent
Non-Adherent
Males 1 1
Female 2 1 0
Fig. 4. 8. Categories of adherence and characteristics of the interviewees in the second set of interviews
4. 4. 2. Analysis of the Second Set of Semi-Structured Interviews
The Second Set of Semi-Structured Interviews was analysed using a different approach in order to have as wide a perspective as possible in understanding the
101

problems the participants had in adhering to physiotherapy to ensure that the design of the survey and the SMPP were valid and reliable research tools. The Burnard (1991) approach was chosen.
The Burnard Approach
The Burnard (1991) approach is a qualitative research approach ideally suited to the analysis and interpretation of interviews as it is seeks to understand the experiences of the interviewees from their perspective. The flexibility of the Burnard (1991) approach allows the researcher to undertake a systematic pathway to analysing the data without the need to develop an overarching theme. As CF is a complex life limiting disease varying in severity, the impact that it would have on the participants’ lives would be wide ranging, making it impossible to have one overarching theme. The Burnard (1991) approach is descriptive and a form of inductive content analysis, which is recommended when there are no previous studies dealing with the phenomenon or when knowledge is fragmented. The aim of the Burnard (1991, p. 461) method is to:
produce a detailed and systematic recording of the themes and issues addressed in the interviews and to link the themes and interviews together under a reasonably exhaustive category system
Burnard (1991, p. 461) describes his approach as “a method of thematic content analysis”. He acknowledges that his work has been adapted from that of Glaser and Strauss (1967) who developed the ’grounded theory’ approach from other works on content analysis (Babbie, 1979; Berg, 1989; Couchman & Dawson, 1990; Fox, 1982) and from the work of Bryman (1988) and Field and Morse (1985) who were concerned with the analysis of qualitative data. However, the Burnard (1991) approach does not go all the way to theory building as it only uses the initial systematic steps adapted from Glaser and Strauss (1967). How the Burnard (1991) approach (developed and adapted by Dewey, 2006) was used to analysis the data along with the actions and rationale for using each stage are set out in Table 4. 3, p. 104. .
As the purpose of the Second Set of Semi-Structured interviews was to provide background information for the development of the survey and the design of the SMPP the Burnard (1991) approach was adapted where the depth and rigor of thoroughly completing each stage was not required (Dewey, 2006).
Stage 1 – Initial notes made during data collection
102

Immediately following each interview verbal feed back was given by the clinical psychologist to the researcher and recorded in brief “field” notes, which acted as an “aide memoire” for data collection and data analysis. The notes focused on initial thoughts and feelings about the interview procedure, the content of the interview, including searching out developing patterns or themes, identifying possibly surprising phenomena, and being sensitive to the range of views expressed by the participants (Dewey, 2006). By making initial notes and discussing the interviews with the interviewer the preliminary development of a coding system emerged.
Stage 2 – Immersion in the data
The researcher read and re-read the final version of the transcripts so she was fully immersed in the data in order to make sense of it, to learn “what was going on” and to obtain a sense of the whole (Burnard, 1991; Field & Morse, 1985). This process enabled the researcher to have a greater awareness of the participant’s ’real world’as no-insights or theories can spring forth without the researcher being completely familiar with the data (Polit & Beck, 2006).
103

Table 4. 3. The Burnard (1991) approach developed and adapted by Dewey (2006)
Stage Action Rationale
1. Initial notes are made following the interview regarding topics discussed
These notes serve as a record and reminder to the researcher of emerging ideas and hypotheses
2. Interview transcripts are read through and annotated
“Immersing” the researcher in the data so they become familiar with the participants point of view. This stage helps the researcher to stay close to the data
3. Transcripts are read again and open coded
This stage allows more focused analysis since the researcher highlights significant units of meaning (Single word, sentence, phrase etc) as well as excluding “dross” or background information and data which are not related to the research question
4. The list of open codes are surveyed by the researcher and collapsed into higher order themes
Continuing on from Stage 3 above, the researcher continues to group related codes to together
5. The list of themes is reviewed and any repetitious or similar themes are removed
Careful checking of the initial themes identified avoids repetition and moves towards the final list of themes
6. Two independent colleagues are invited to open code the same data set
To enhance validity of the data analysis and to Safeguard against research bias
7. Transcripts are compared with the list of themes
Returning to the transcripts helps to establish the degree to which the data analysis has stayed close to the original meaning of the transcripts. Adjustments are made as necessary
8, 9. & 10.
Each transcript is worked through a final time using the agreed list of codes and themes to code significant units of meaning
Using the final list each part of the transcript is re-located to a code or theme and then grouped together either by cutting or pasting (by hand) or “highlighting techniques” using computer Software
11. A sub-group of the participants is asked to check the appropriateness of the themes
This stage known as “respondent validation,” acts as another method of measuring the presence of researcher bias
12. & Writing up – where all sections Methodical filing assists the researcher
104

13. are filled together with complete transcripts of interviews
during the write up process and provides an “audit trail” of decision making. Producing a report of the findings which includes relevant extracts and an analysis
14. Writing up Producing a report of the findings which includes relevant extracts and an analysis
Stage 3 – Open coding of the interview transcripts
After re-reading the transcripts again the process of systematically open coding the data commenced by recording, in the text and margins, notes and headings relevant to all the aspects of the content (Burnard,1991) and highlighting and assigning codes to words that had specific characteristics within the text as they emerged, e.g. Interviewee D’s “physiotherapy doesn’t make any difference if I do it” was coded as “perceptions of having CF”. Codes have been described as “tools to think with” as they allow the data to be thought about in a different way (Coffey & Atkinson, 1996) and they facilitate the process of analysis. Open coding, in the form of headings, focused the analysis so that words and phrases reflecting important “core ideas and concepts” (Rubin & Rubin, 1995) were identified. These “core ideas and concepts” made up a distinct unit of meaning. A unit of meaning contains words, sentences or paragraphs containing aspects related to each other through their content or context (Graneheim & Lundman, 2004).
The units of meaning that had a similar content were grouped into initial themes. A theme is a group of content that shares a commonality (Krippendorff, 1980) that is exhaustive, mutually exclusive and descriptive of the content. Themes are descriptive and act as a thread between the units of meaning and assist in organising the data (Dewey, 2006). Each initial theme was identified by the use of key words or phrases copied from the highlighted text in the units of meaning. Although not part of the Burnard (1991) approach a brief synopsis was made of each interview incorporating the initial themes in order to facilitate organising the data (Dewey, 2006) and to give an accurate understanding of the participant’s “life world” (Burnard, 1991). The themes were continually and systematically grouped and re-grouped, identifying similar content to reflect the text as a whole.
Synopsis : Interviewee C – Female Student
Initial Themes
Positive outlook.
Sees physiotherapy as part of a daily routine.
105

“Normalises” her physiotherapy treatment - no different from “normal” people who
want to stay healthy.
Uses physiotherapy as a means of controlling her disease. Balances treatment with the
need to lead a normal life.
Does not feel guilty if she takes time off work to give herself more time to get better.
Fig. 4. 9. Sample synopsis of interview themes
Stage 4 – Collapsing of themes
The number of themes was reduced by collapsing those that were similar or related into broader or higher order categories (Burnard, 1991; Dewey, 2006; Dey, 1993) for the purposes of clarity.
Memorising Memo
Themes Collapsed: ‘Diagnosis’ and ‘Living with CF’ into ‘Strain of having a
life threatening disease.
Being diagnosed at birth results in an emerging awareness of the impact of
having CF while being diagnosed as an adult is a more traumatic experience.
Categories collapsed but an awareness of the interviewees background is needed
to put their comments into context.
Fig. 4. 10. Memo providing an audit trail of the analysis
A memo was made of the ‘collapsing’ process so there was a clear audit trail of the analysis (Fig. 4. 10). The example above records the reasoning behind the meaning of two category headings ‘Diagnosis’ and ‘Living with CF’ being collapsed to provide a new overarching theme of ‘Strain of having a life threatening disease’.
Stage 5 – Producing a final list
The list of themes and sub-themes was revised several times during this stage to focus the analysis and reduce overlapping of themes.
Stage 6 – Validity of the themes
A nursing colleague, who was familiar with using the Burnard (1991) approach for analysing interviews, was involved at this stage. The colleague read through the transcripts and independently generated her own themes without seeing the
106

researcher’s list. The aim of this stage was to attempt to enhance the validity of the analysis and to guard against the researcher’s bias. The two sets of themes were similar, but not identical
Independent Assessor Researcher
Stay Alive Perception of having CF
Support (with the burden of coping with CF) Strain of having a life threatening disease
Knowledge of CF (need to make a balance of life/ perspective )
Physiotherapy Treatment – Life balance
Compliance with physiotherapy
Finding a suitable physiotherapy technique
Recognising the importance of physiotherapy treatment
Control
Concept of guilt
Fig. 4. 11. Comparison of themes identified by researcher and independent assessor
The interviews showed strong recurring themes that were evident to both the researcher and the independent assessor and highlighted the significant features of CF from the participant’s perspective. The themes from the two sets of analysis were indicative of how the interviewees coped with their disease and the factors that influenced their ability to adhere to physiotherapy treatment.
Stage 7 – Verifying the themes
Re-reading of the transcripts alongside the final agreed list of themes and sub-headings was carried out to ensure that the themes covered all aspects of the interviews. The purpose of this stage was to check that findings from the collected relevant data were not based on the researcher’s own attributions but representative of the participants views. Adjustments were made as necessary.
Stages 8, 9 and 10 – Finalising the list of themes
107

As the interviews were not an end point in their own right, and the six themes that emerged were similar to the four overarching themes that were evident in the First Set of Semi-Structured Interviews, further in-depth analysis was not considered to be warranted.
4 Overarching Themes from the First Set of
Set o Semi-Structured Interviews (n = 3)6 Themes from the Second Set of Semi-
Structured Interviews (n = 5)
Health Beliefs Control
Physiotherapy Recognising the importance of
physiotherapy treatment Balance between adhering to
physiotherapy treatment and leading a normal life
Experience of having CF Perception of having CF
Concept of guilt
Denial Strain of having a life threatening disease
Fig. 4. 12. Themes for the two sets of semi-structured interviews
In view of the flexibility of the Burnard (1991) approach it was decided not to condense the six themes in the Second Set of Semi-Structured Interviews any further as they were similar to those identified in the First Set of Semi-Structured Interviews but indicated greater depth. By condensing the six themes further valuable insights into the ‘life world’ (Burnard, 1991) for people with CF may have been missed.
Stage 11- Respondent validity
In the Burnard (1991) approach, the work is given to the participants so that the interpretative validity of the analysing process can be checked, but in this exploratory study this stage was omitted because the semi-structured interviews were conducted to inform the development of the research tools, i.e. the survey and the SMPP, and were not an end point in their own right. Due to time constraints, the infrequency of the participants’ visits to the CF clinic, the wide geographical distribution of the study
108

population and the time it would take to carry out this process, the transcripts and the list of themes were not returned to the participants, and this stage was omitted.
Stages 12, 13 & 14 - Writing up the Findings
Once the interview data had been analysed the process was stopped as sufficient information had been provided to inform the development of the survey and the design of the SMPP. The writing up of the interviews included verbatim quotes selected on the basis that they provided an example of the theme being described (Dewey, 2006) and helped the reader to judge how well the explanations were grounded in the data (Murphy, Digwall, Greatbatch, Parker, & Watson, 1998). Where appropriate the discussion of the findings was linked to the literature on the topic in order to make a comparison with findings from previous studies.
Because of the similarity of the themes in the First and Second Set of Semi-Structured Interviews, and for purposes of clarity and brevity, they are discussed together in the following section.
4. 4. 3. Discussion of the Findings (Themes) from the First and Second Set of Semi- Structured Interviews
The two themes that emerged from both sets of semi-structured interviews ‘Health Beliefs’ and ‘Perceptions of Having CF’ are presented below:
Health Beliefs
The influence of health beliefs in the management of CF has been identified in two other studies on adherence to physiotherapy in CF (Carr et al.,1996; Myers & Horn, 2006). Both studies considered that if people with CF had positive health beliefs they were more likely to adhere to treatment because they felt that they could influence their health outcomes for the better, with the converse being true for negative health beliefs e.g. Interview 1, who was adherent, stated that “physiotherapy controls my disease …it has to be done.” However in the management of chronic conditions health beliefs can change over a period of time with corresponding changes in levels of adherence. Positive health beliefs co-inside with a positive/optimistic attitude which enables a person with CF to cope better with their disease (Abbott et al., 2001) and therefore be more likely to adhere to treatment. Health beliefs and how people with CF perceive their disease are interlinked.
Perception of Having CF
109

One of the most influential factors in adherence to physiotherapy is the participant’s perception of what having CF means to them. Several studies (Bucks et al., 2009; Daniels et al., 2011) have shown that a discrepancy can exist between how a person with CF perceives their health to be and the objective measurements of their disease severity. The theme “Perception of Having CF” relates to the interviewees perspective of having CF and their physiotherapy treatment. Their perspectives varied from acceptance and being adherent to physiotherapy treatment to denial and being non-adherent. Perception (Collins, 2006, p. 83) “is the process of attaining awareness or understanding of information”. When applying this definition to the study it would mean the participant receiving, collecting and internalising information to formulate their own views of their disease, irrespective of the information given to them by the professional. Some people with CF have a tendency to be “over optimistic” about the severity of their disease (Abbott et al., 1995; Bernard & Cohen, 2004; Huyard, 2008) while others have a sense of hopelessness, i.e. Interview E who stated that “it’s always horrible and negative; should I bother really because I will be dead in two years.” Some participants demonstrated a desire to “normalise” their condition and to be positive in their approach to it. Interviewee A commented that she did not think that her life was “any different to that of my friend. I do what they do”. This “normalisation” gave her a positive approach to coping with CF. In some instances however, too positive a stance can be a form of denial. Interviewee 2, who was partially adherent with a moderate level of disease severity, commented that “CF does not affect my life at all”. He coped by only doing physiotherapy when he was unwell. A coping strategy of denial, in a mild form, can enable people with CF to get on with their lives and not always be troubled by it (Abbott et al., 2001). However, if taken too far it can result in denying the serious impact CF can have on their health outcomes by not promptly accessing medical and physiotherapy services. These factors are relevant as physiotherapy is one of the least liked and most poorly adhered to of all CF treatments (Abbott et al., 1996; Christian, 2007; Daniels, 2010; White et al., 2007; Zindani et al., 2006). It is not the degree of disease severity which can influence adherence to physiotherapy treatment but how accurately the level of disease severity is perceived.
Strain of Having a Life Threatening Disease
The strain of having a life limiting disease is divided into four sub-sections:
1. Diagnosis
110

All of the interviewees spoke about how distressing it was to have CF. Two Interviewees, E and D, were diagnosed late, when they were teenagers, and this had a profound affect upon their lives. For Interviewee D it meant that her whole life had been “turned upside down” and for Interviewee E it meant that “I could be dead in two years”. The impact of having a life limiting disease, for people who had previously considered themselves to be healthy, was a traumatic experience and it profoundly affected their approach to life and how they perceived having CF. People with CF want to lead a life style similar to their peers (Daniels, 2010) which is why patient preference is an important influence in adherence to daily physiotherapy treatment. People with CF have to fit in complex treatment programmes, so selecting an ACT that they prefer encourages adherence (Daniels, 2010).
2. Telling Others
Another difficulty identified was whether to tell other people about their condition. The literature suggests that it appeared that most people with CF tell their close friends and partners but saw no reason to share their diagnosis with other people (Abbott et al., 1994). Limiting the number of people who know about their condition gave them an opportunity to be treated as a peer in their work/social group.
3. Fertility
The strain for the women who want to have children or, in the case of Interviewee D who had two young children, is considerable. Interviewee D stated that “it hits you, I am dying… “It doesn’t make you feel any better to know that people have worse problems”. Interviewee D recalled reading that “mothers with CF who had children rarely make it past the first decade of their children’s lives”. Interestingly neither of the men spoke about their potential inability to have children but all of the women voiced their concerns about problems of sub-fertility. Interviewee E was undergoing In Vitro Fertilisation (IVF) treatment and was aware that this was a necessary procedure because having CF results in reduced fertility (Edenborough et al., 2008) She highlighted this by saying that she “had a period of transition for a few years; after that I was getting used to the fact that actually I have to be more vigilant. I have to pay more attention to my health”.
4. Everyday Activity
It is important that people with CF lead as normal a life as possible and an example of this is when people with CF take a positive approach to their health and well being by undertaking activities such as going to the gym (Bradley & Moran, 2011). This can be
111

embarrassing if exercising results in coughing in public. Interviewee E expresses her embarrassment about coughing by stating that “you think Oh God! People are looking at me”. In order to cope with this type of situation some people with CF say that they have asthma because asthma is not life threatening, it is better understood and avoids having to explain what CF is. Alternatively they go to the gym when they are well. In this context these avoidance/coping strategies are synonymous with positive health beliefs, as they demonstrate a recognition of the importance of exercise and activity in keeping fit and well, alongside a desire to lead a life similar to their peers.
Control
Another concern verbalised was the degree of control that the interviewees thought they had over the course of their disease. If the interviewees perceived that what they do can makes their lives better, e.g. adhering to physiotherapy treatment improves their health outcomes, it enabled them to establish a concept of having control over their disease and their life e.g. Interviewee C stated that “I’m in control…… rather than it’s controlling me” and Interviewee 1 stated that “physiotherapy controls my disease”. It is interesting to note that if people with CF make the connection between physiotherapy treatment and control then they can use their physiotherapy treatment as a control mechanism, which in turn can contribute to optimising their ability to adhere to their physiotherapy treatment.
Recognising the Importance of Physiotherapy Treatment
Although all the interviewees in the Second Set of Semi-Structured Interviews acknowledged the importance of doing physiotherapy, only two interviewees reported themselves as being adherent while in the First Set of Semi-Structure Interviews two of the participants, Interviewee 1 (adherent) and Interviewee 3 (non-adherent) considered physiotherapy to be important while Interviewee 2 (partially adherent) did not consider routine physiotherapy to be of benefit. Interviewees A and E in the Second Set of Semi-Structured Interviews perceived physiotherapy to be as a means of controlling their disease and improving their health outcomes. Interview B stated that he did physiotherapy “to clear my chest to help me feel better during the day…I think that without it I wouldn’t be so well”. Those who previously did not adhere to physiotherapy treatment such as Interviewee D (“I am trying to do it far more now….. It is easy not to give it enough time”), did recognise its importance but had difficulty doing it because it was ”time consuming” and “boring” as other research has indicated (Abbott et al., 2009; Carr et al.,1996). Interviewee 3 stated that “I know that physio is important but I cannot be bothered to do it”. There is a conundrum of trying to find a
112

balance in their lives, between doing physiotherapy treatment and making sure they have a good quality of life (Daniels, 2010).
The effectiveness of physiotherapy ACTs was an issue raised by several of the interviewees. If the ACT carried out was perceived by the interviewee to have no obvious benefit then they were less likely to continue with it. Interviewee E referred to the fact that she was using the PEP mask as treatment but considered that it was not as effective as exercise in clearing her chest. It is only in recent years that the short term benefits of ACTs have been established in five Cochrane Reviews (Elkins et al. 2009; Morrison & Agnew, 2009; Main et al., 2009; Robinson et al., 2010; van der Schans et al., 2009), the long term benefits in a study by Pryor et al. (2010), and also that patient preferences are important in influencing the ability to adhere to physiotherapy treatment (Daniels, 2010; Pryor et al., 2010).
Adhering to Physiotherapy Treatment – Life Balance
As people with CF are living longer and leading more normal lives, the pressures and burdens of physiotherapy treatment encroach upon their daily life (Daniels, 2010). This is particularly true in the case of Interviewee D who was a wife, a mother of two young children and, in addition to a part-time job, had to manage her disease as well. Her desire to be a “good mum and wife,” and ensure that her children had a normal life, meant that at times she was not able to do her physiotherapy as she could not fit it into her busy schedule. Her difficulty in adhering to physiotherapy treatment resulted in Interviewee D neglecting her health care. She questioned her ability to strike a balance between doing physiotherapy treatment and leading a normal life as a wife and mother e.g. “I wonder whether there really is a boundary…… I now have to physically say to myself stop, give yourself half an hour and put your feet up”. She acknowledged that if she does not look after herself then she will not be well enough to be the type of mother that she wants to be.
Another way of coping with the treatment/life balance was expressed by Interviewee C who stated that physiotherapy was “part of my routine”. Although single and working part-time she struck a balance in her life between doing physiotherapy treatment and having a “normal” life by making physiotherapy part of her normal daily routine e.g. “I just got better at balancing, living the life I wanted to lead and living the life I wanted to live with doing the treatment. I think it’s just as I got older the balance kind of levels off”. However, Interviewee 1 considered that “physiotherapy does not interfere with my life but is a big part of it ….. physiotherapy controls my disease”. For those who recognise the importance of physiotherapy and
113

use it to control their disease it can result in a good balance being achieved between having CF and leading a normal life (Daniels, 2010; Kettler et al., 2002; Pryor et al., 2010).
Concept of Guilt
It was evident that missing a treatment in some instances was associated with guilt. The interviewees recognised the importance of doing treatment and became concerned when they were not doing it to the level that they thought they should. Although feeling “guilty” if they missed a treatment, Interviewee C did not dwell on it and considered that the balance between daily living and physiotherapy treatment could not always be perfectly managed. Although the interviewees felt guilty about missing physiotherapy it did not lead to increased levels of adherence.
4. 5. How the Findings from the First and Second Set of Semi-Structured Interviews influenced the progression of the study
Once the analysis of the interviews was completed and themes apparent the next stage was to use the information to develop the survey and the design of the SMPP. The purpose of the survey was to collect information from the whole study population (n = 49) before and after the intervention (SMPP), so that any changes in adherence behaviour that may have occurred as a result of the intervention could be measured.
The study set out to use the Professionalising typology of an action research approach which required the participants to be actively engaged in the research process. In a health care setting it is challenging to implement pure action research as the participants cannot always be fully engaged in the process, because they do not have the knowledge and skills to work as equal partners with the professional (Hart & Bond, 1995) in this process led and pre-determined methodology. It became apparent following the analysis and findings from the two sets of semi-structured interviews that the experiences and insights of the participants would not lead to them having a significant enough influence on the development of the survey and the design of the SMPP as would be in keeping with an action research approach. Because the researcher had collected sufficient information from the semi-structured interviews and had an extensive knowledge and clinical experience of CF, the study populations’ further involvement in the design of the research tools was not warranted. Their involvement was confined to selected participants being part of two different representative samples in the pilot studies for the survey and the SMPP, participating
114

in two self-administered questionnaires in the survey and using the SMPP. It was felt that the research objectives of the study would be met by broadly following a Professionalising typology of the action research model (comprising Plan, Action/Intervention, Evaluation and Reflection), but without the participants being involved to the extent that would be required in a fully implemented action research approach. In view of this decision the research process was remodelled (Fig. 4. 13, p.115) but the key stages of the study remained unchanged and are outlined in Table 4. 4., p. 116.
Chapter 4. Plan – The Survey Designing the survey Piloting the survey Issuing the first part of the survey – Pre-Intervention Physiotherapy Questionnaire Results and analysis of the Pre-Intervention Physiotherapy Questionnaire
Chapter 5. Intervention/Action - The SMPP Designing the SMPP Piloting the SMPP Implementing the SMPP Issuing the Post-Intervention Physiotherapy Questionnaire
Chapter 6. Evaluation Analysis and results of the Pre and Post-Intervention Physiotherapy Questionnaires
Chapter 7. Reflection Discussion Conclusions Recommendations for clinical practice Recommendations for future research Limitations Reflection
Fig. 4. 13. The re-modelled research process
115

Table 4. 4. Key stages of the Study
Stages of the Study Actioned By
Study Population Selected R
Inclusion and exclusion criteria applied Study population recruited R
PLANFirst Set Semi-Structured Interviews C P
Analysis of First Set of Semi-Structured Interviews R & C PSecond Set of Semi-Structured Interview
C PAnalysis of Second Set of Semi-Structured Interviews R & CP
Pre-Intervention Physiotherapy Questionnaire developed from the findings (themes) of both semi-structured interviews
R
Pre-Intervention Physiotherapy Questionnaire piloted
R
Pre-Intervention Physiotherapy Questionnaire issued R
Pre-Intervention Physiotherapy Questionnaire returned and analysed
INTERVENTION /ACTION
SMPP designed R
SMPP piloted - Sub-group R
Start of Intervention: SMPP issued R
3 month Follow-Up: SMPP reviewed and evaluated using Feedback Chart R
Finish: 6 month Follow Up: SMPP reviewed; Post-Intervention Physiotherapy Questionnaire issued R
116

Post-Intervention Physiotherapy Questionnaire returned
EVALUATION
Pre & Post Intervention Physiotherapy Questionnaires Analysed and Feedback Chart evaluated
R
REFLECTION
Legend CP = Clinical Psychologist R = Researcher/Physiotherapist
4. 6. Plan - The Survey
4. 6. 0. Designing the Survey
The design of the survey was part of the development of the research tools that would be required to accurately collect data in order to identify the problems adults with CF have with adhering to physiotherapy, and to inform the development of the SMPP. The research tools needed to be sensitive enough to record changes in behaviour that may have occurred as a result of using the SMPP. The information from the First and Second Set of Semi-Structured Interviews contributed to the development of the survey to ensure that its construction was content specific and relevant.
Surveys are a cross-sectional, inexpensive, descriptive data collection method used where the purpose is to describe how many people in a given population possess a particular attribute or opinion at a particular time, and aim to describe what exists (Robson, 2006). They investigate the relationship between variables but do not determine causation (Oppenheim, 1992). The survey used in this study was a self-completed questionnaire whose purpose was to provide a simple and straightforward approach to obtaining data on attitudes and values from the whole study population (n = 49) at a particular time period.
A survey gives anonymity to the respondent, allows for individual perceptions to be expressed via open questions, and can act as a confirmation tool in relation to other findings because there are set questions with responses that can be compared. The weaknesses are that it assumes literacy, relies on honesty, risks lack of clarity in the questions (but this can be reduced by conducting a pilot study to test it) and is weak on validity, because if the questions are not framed accurately the information collected will not enable the research questions to be answered (Cohen et al., 2011; McKenna et al., 2006). In considering the design tool, recognition was given to the
117

disadvantages of a survey, but they outweighed the advantages. The design of the survey involved the participants in a pilot study to enhance its validity and reliability.
The survey was cross sectional and issued at two points during the study in order to identify and describe any changes which may have occurred following the implementation of the SMPP.
Part (a) - the Pre-Intervention Physiotherapy Questionnaire which was issued at the beginning of the intervention period
Part (b) – the Post-Intervention Physiotherapy Questionnaire which was issued at the end of the intervention period
The Pre and Post-Intervention Physiotherapy Questionnaires both recorded the same information but the Post-Intervention Physiotherapy Questionnaire asked two additional questions on the effectiveness of the SMPP to optimise the ability to adhere to physiotherapy treatment. At the time of the study no questionnaire had been specifically designed involving adults with CF in investigating the problems they were experiencing with adhering to physiotherapy. The findings from the two sets of semi-structured interviews enhanced the validity and reliability of the survey and contributed to the design of the questions so that they were sensitive enough to identify the problems of adhering to physiotherapy from the participant’s perspective. Sensitivity was achieved by ensuring that the questions were relevant to the problems the participants had raised in the semi-structured interviews and that the language used to frame the questions was appropriate.
At the time of the study, apart from the Carr et al. (1996) paper, adherence to physiotherapy had been investigated in adults with CF (Abbott et al.; 2001; 1996; 1994; Conway et al., 1996; Dodd & Webb, 2000) as part of a larger study into adherence to treatment in CF. The questionnaires used in these studies were developed by the researchers without undertaking any preliminary measures that included people with CF, i.e. semi-structured interviews, that would provide the researcher with background information to help them in the development of their questionnaires. The Carr et al. (1996) study, however had developed a questionnaire (Appendix M) that was used as a foundation for the survey in this study, as it was the only questionnaire specifically designed to investigate adherence to physiotherapy in CF in the UK. As in the above mentioned studies the participants in this study had not contributed to the design of the questionnaire.
118

The Carr et al. (1996) questionnaire was not used as it stood because it failed to collect sufficiently detailed information on factors such as disease severity, the demographics of the study population and what problems the participants had in adhering to physiotherapy. It also failed to collect qualitative data seeking the thoughts, feelings and perceptions of the participants (Carr et al., 1996), which are important because if the problems of adhering to physiotherapy are not identified from the participants’ perspective then finding an effective solution would be compromised. The Carr et al. (1996) self-administered questionnaire had not been validated, therefore very careful consideration was given to the questionnaire design for this study, i.e. what questions needed to be asked, how they should be asked and why they should be asked, in order to illicit valid and reliable data. In view of the above factors a self-administered questionnaire was designed so that the participants could complete it in their own time and if necessary it could be posted to them.
Considerable attention was paid to the wording of the questions asked to ensure the accuracy of the information collected (Boynton & Greenhalgh, 2004; Oppenheim, 1992). In general two types of questions were asked; open questions seeking an opinion e.g. “to what extent do you consider that your attitude to CF influences the course of your disease” and closed questions in the form of multi-choice answers, e.g. “what is your marital status – single/separated/divorced/ with a partner/re-married”. The questions needed to be clear, succinct, and unambiguous in their wording. Leading questions were avoided as they would imply a certain answer which could prejudice the replies. The terminology of each question was carefully considered so that questions were phrased in a positive style to avoid causing any offence. Embarrassing questions such as those that related to coughing were avoided, but by using open questions about the impact of the disease it was anticipated that this would lead participants to freely share their embarrassing moments in their own words. Questions from the Carr et al. (1996) questionnaire designed to establish the social characteristics, physiotherapy regimens and medical treatment of their study population were used or adapted for the purposes of this study. Additional questions were added by the researcher/physiotherapist who, taking into account the findings from the two sets of semi-structured interviews, designed questions that sought to establish the study population’s perceptions of the efficacy of physiotherapy, the problems they encounter in doing physiotherapy and their health beliefs, e.g. Q. 46. “To what extent, if any, do you think you have control over the course of your disease?”
119

A range of approaches by which the questions could be answered were used, e.g. open and closed questions, multiple choice and Likert scales were used. An example of a multiple choice question is outlined below:
Q. 11 Over the past month how has your health been
1. [ ] very good
2. [ ] good
3. [ ] unwell
4. [ ] very unwell
Likert scales, which measure attitude with all items measuring the same dimension (Murphy-Black, 2006), were used as they are a psychometric scale to which respondents specify their level of agreement to a statement. As Likert scales are numbered, it facilitates the analysis of the replies. Multiple choice questions were also used to encourage a high response rate as they can be quickly answered. How the questionnaire in the survey was scored is described below.
4. 6. 1. Purpose of the Pre-Intervention Physiotherapy Questionnaire
A full description of each participant was sought through the collection of information regarding demographic data, physical health and the physiotherapy regimen each participant used. Each section is detailed below :-
1. Demographics - Base line quantitative and qualitative information on the social characteristics of the participants including age, sex, age at diagnosis and current employment status.
2. Qualitative information was collected using open questions which enabled the participants to express their beliefs, perceptions and feelings in their own words and were informed by the findings from both sets of semi-structured interviews e.g. Q. 21. What are your reasons for not doing chest physiotherapy?
3. Physiotherapy Treatment - The ACT and exercise undertaken by the participants was self-reported using multiple choice or open ended questions.
Questions were designed to identify how adherent to physiotherapy treatment the participants reported themselves to be, what difficulties they had in
120

adhering to physiotherapy treatment and their views on their physiotherapy treatment. Examples of such questions are outlined below:
Open questions - Q. 25. If you miss a physiotherapy session please state why……………….
Multiple choice - Q. 12. How much to you agree or disagree with the following statement? Doing chest physiotherapy is important to my feeling of well being. Please tick of one of the following boxes
1. Strongly agree ( )2. Agree ( )3. Neither agree or disagree ( )4. Disagree ( )5. Strongly disagree ( )
4. Medication Time Pre and Post-Physiotherapy – the amount of time taken to prepare inhaled medication prior to chest physiotherapy and the time taken to clean equipment post-nebulisation was elicited by self-reporting.
5. The major themes identified in the semi-structured interviews were explored
using open questions e.g. Q. 47. ‘To what extent, if any, do you think that
you have control over the course of your disease?’ in order to identify
whether the participants had positive or negative health beliefs towards their
disease, and to subsequently investigate whether there was a correlation
between their health beliefs and their adherence to physiotherapy treatment.
e.g. Q. 8. ‘Do you think you have CF very mildly/mildly/moderately/
moderately-severe/severe.’ In order to inform the theme “Perception of
Having CF,” and how the participants’ perception of their disease might
influence their ability to adhere to physiotherapy.
4. 6. 2. Piloting the Pre-Intervention Physiotherapy Questionnaire
Once the design of the Pre-Intervention Physiotherapy Questionnaire had been completed it was piloted to ensure that the questions were unambiguous and user-friendly in order to enhance its reliability and validity. A simple convenient sampling frame of 12/49 (24.4%) participants was chosen from the total study population (n = 49). Following discussions with the statistician it was considered that this would be a valid and reliable sub-sample representative of the whole study population, irrespective of their category of adherence. The first 12 participants in a stable condition were chosen randomly during an inpatient stay or during an out-patient visit on a first come first approached basis by the researcher/physiotherapist. All 12 agreed
121

to be in the pilot study. Of the 12 who agreed to be in the pilot study six were in-patients and six were out-patients; six were male and six were female. Their ages ranged from 17 – 39 (the age range of the whole study population was 16 – 53).
Being approached by the CF researcher/physiotherapist may have influenced the participants into volunteering for the pilot study but it was the only practical way to approach them. It was explained that they did not have to fill in the Pre-Intervention Physiotherapy Questionnaire but to read the questions and make sure that they understood what was being asked of them. The researcher/physiotherapist checked their understanding by asking questions to ensure that they knew what was being asked of them. They were also requested to make any comments or ask any further questions if they wished to do so. The information collected was used to develop the final version of the Pre-Intervention Physiotherapy Questionnaire and was not included in any of the findings or results.
Evaluation of the pilot study and recommendations for the Pre-Intervention Physiotherapy Questionnaire
Of the 12 participants involved in the pilot study, six gave recommendations for making some alterations e.g. the order of questions changed to a more logical sequence while six thought that the questionnaire was appropriate as it stood. The re-designed Pre-Intervention Physiotherapy Questionnaire was finalised for use in the study (Appendix N). The final version was considered to be a sufficiently valid and reliable tool to elicit the participants’ perception of physiotherapy, their perception of having CF, their health beliefs and the problems they encountered in adhering to physiotherapy.
4. 6. 3. Issuing the first part of the survey – the Pre-Intervention Physiotherapy Questionnaire
The eligible participants who had consented be in the study (n = 49) were approached by the researcher/physiotherapist during out-patient visits or during in-patient stays when they were in a stable state. These 49 participants also included the 12/49 (24.4%) participants who had taken part in the pilot study for the Pre-Intervention Physiotherapy Questionnaire as they were part of the study group and were required to fill in the finalised version of the Pre-intervention Physiotherapy Questionnaire so there was consistency of data for the purposes of analysis and evaluation.
The purpose of the self-administered Pre-Intervention Physiotherapy Questionnaire was explained to the study participants (n = 49), who were informed that they could
122

decide whether to complete it there and then or at a later date and return it in the stamped addressed envelope supplied. The study participants were informed that if they had any queries or difficulties completing the questionnaire then they were to contact the researcher using the telephone number on their Patient Information Leaflet (Appendix F). The use of the same self-administered questionnaire issued at the beginning and end of the study period enabled a continuous evaluation process to be put in place, as the same data was gathered at the beginning and end of the intervention period so that any changes following the implementation of the SMPP could be identified. To facilitate the evaluation of the SMPP two additional questions were inserted into the Post-Intervention Physiotherapy Questionnaire (Appendix O) which sought the participant’s views on the effectiveness of the SMPP to optimise their ability to adhere to physiotherapy. The Post-Intervention Physiotherapy Questionnaire is discussed in greater detail in Chapter 5, p. 144.
4. 6. 4. The Scoring System for Open and Multiple Choice Questions Used in the Survey
The open and multiple choice questions were identical in the Pre and Post-Intervention Physiotherapy Questionnaires. A scoring system (Appendix P), devised by the researcher/physiotherapist, was used so that the answers could be analysed and comparisons made between the replies before and after the implementation of the SMPP. Each of the multiple choice questions had a choice of up to six possible answers which were coded with a number from 1 - 6. The numbers were for the purposes of facilitating analysis and did not have any specific value attached to them. Where the answers to the open questions could be grouped together these groupings were also given a numerical code that did not have a specific value. Attitudes in the questionnaire were measured by means of Likert-style scales, ranking attitude choices.
4. 7. Analysis and Results of the Study Population
4. 7. 0. Introduction
The results are presented as follows:
The Study Population Analysis of the Pre-Intervention Physiotherapy Questionnaire
123

4. 7. 1. Study Population
Of the 49 eligible participants who consented to be in the study and were issued with the Pre-Intervention Physiotherapy Questionnaire 43/49 (87.7%) completed it. Of the 6/49 (12.3%) who failed to return the questionnaire 3/49 (6.12%) were male and 3/49 (6.12%) were female. :
Table 4. 5. The study population The Study Population
Numbers
%
Study population selected from ‘full care’ patients in the Adult CF Clinic 61 Application of inclusion and exclusion criteria Eligible to be in the study
55
Number who consented to be in the study and were issued with the Pre- Intervention Physiotherapy Questionnaire
49 100
Males entering the study 17 34.6 Females entering the study 26 53.1 Total Study Population The number who entered the study by completing the Pre-Intervention Physiotherapy Questionnaire
43
87.7
The Pre-Intervention Physiotherapy Questionnaire was analysed using the Statistical Package for the Social Sciences (SPSS) Windows 10 for descriptive statistics, bi-variate statistics and prediction of numerical outcomes i.e. linear regression. The values of each statistical test are presented with each result.
4. 7. 2. The study population compared to the National Cystic Fibrosis Database
The characteristics of the study group were compared to the CF National Database (CF, 2000) population that was current at the time of the study, for FEV1, BMI and age, so that the general health of the study group could be put into context. It was important to know whether the study population’s characteristics were comparable or not to the CF National Database (CF Trust, 2000) population and whether the results and findings could be generalisable.
124

The CF Trust established the National CF Database (CF Trust, 2000), which was the forerunner of the UK CF Registry, so that all the adults and children in the UK with CF were registered for the purpose of planning care, monitoring trends and raising standards of care. It was not possible to have assess to the raw data for the National CF Database population. Chi-squared tests were used to compare the frequency distributions of the study population to the National CF Database (CF Trust, 2000). Where small frequencies were present the Fisher-Freman-Halton exact test was used. The results and findings are described in the following sections.
FEV1
The Forced Expiratory Volume in 1 second (FEV1) is a very simple standardised objective pulmonary function test that is a well established marker of disease severity. The American Thoracic Society (1989) had graded disease severity in broad terms into three grades Mild >75%, moderate 40% - 60% and severe < 40%. For the purposes this study the FEV1 was sub-divided into the following five grades: less than 30% severe, 31%-40% moderate/severe, 41%-60% moderate, 61%-79% mild, with 80% and above graded as normal. This five level grading system was sensitive and equated with the subjective grading system used in this study in the Pre-Intervention Physiotherapy Questionnaire Q. 8 on how the participants perceive their health to be, thus enabling the relationship between perceived disease severity and FEV1 to be explored.
Fig. 4. 14. Distribution of FEV1 in the study group and the National CF Database
The mean and Standard Deviation (SD) of FEV1 in the study population was 48.5% and 20.2% respectively. The mean and SD of the study group males and
125

females was 45.1% (16.1%) and 51.9% (21.3%) respectively. The distribution of values, which ranged from 17% to 90%, is displayed in Fig. 4. 14.
In the study population 30/49 (61.2%) participants produced an FEV1 of 50% or less compared to 945/2394 (39%) in the National CF Database (CF Trust, 2000) population. This difference is statistically significant at the 5% level (Chi squared = 16.2, P < 0.001). All participants were clinically stable when their FEV1 were measured. It would appear that the study group were less well than the database group. The results were skewed by the fact that 5/49 (10.2%) of the study group had a FEV1 <30%. Relative to the National CF Database of 2,394 the study population of 49 was small and the impact of having 5/49 (10.2%) showing <30% would have a disproportional impact compared to the National CF Database (CF Trust, 2000) population with a population of 2,394.
Body Mass Index
Fig. 4. 15.
Distribution of BMI in the study group and the National CF Database
The distribution of BMI indices for the study population produced values marginally lower than those in the National CF Database (CF Trust, 2000) population (Fig. 4. 15), but not significantly so (Fisher’s Exact test, P = 0.1142) thereby enabling the results toe generalisable.
It was decided that the BMI would not be repeated at the end of the six month study period as the study period was too short to be able to use the BMI as a measure of the
126

affect of the BMI on the ability of the SMPP to improve adherence. Also the impact of the SMPP had yet to be established and the duration of the study period to evaluate any impact of BMI on adherence was to short.
Age
The mean (SD) of age in the study population was 25.3 (8.3) years with a range 17 – 53 years. The corresponding figures for males and females were 26.5 (9.3) with a range of 18 – 53 years and 24.4 (7.6) years with a range of 17 – 48 years.
Fig 4.
16 . Age
profile of the study group and the National CF Database
The distribution of age in the study group was not significantly different to that found in the National CF Database (CF Trust, 2000) population (Fisher Exact P = 0.1207).
Summary of the analysis of the study population and the National CF Database ion
There was no statistically significant difference between the study population and the National CF Database with regards to age and BMI. The study population did, however, contain significantly more individuals with an FEV1 below 50% compared
127

to the National CF Database population. As FEV1 is used as a predictor of life expectancy (Aurora et al., 2000) it could be said that the study group was less healthy than the database population. However in small studies (n = 49) large differences between sub-groups may be clinically significant but fail to achieve statistical significance, although trends can be identified.
Adherence Related to Gender
Only 36/49 (73.4%) participants answered both Q. 2 (Male or Female) and Q. 24 (How often do you miss a chest physiotherapy session in a week? 1/2/3/4/ if more please state) enabling the relationship between gender and adherence to be investigated. For the purposes of analysis, in this instance 36 was considered to be the total group.
Table 4. 6. Adherence related to gender
Level of adherence Gender
Total (%) Male (%) Female (%)
Non-adherent 7 (58.3%) 11 (45.8%) 18 (50.0%)
Partially adherent 2 (16.7%) 9(37.5%) 11 (31.6%)
Adherent 3 (25.0%) 4 (16.7%) 7 (19.4%)
Total 12 (100%) 24 (100%) 36 (100%)
The data provided no evidence of any significant association between gender and level of adherence (Fisher’s Exact test, p = 0.519).
128

0
2
4
6
8
10
12
14
16
18
20
1 2 3 4
Perceived disease severity (1-4)
Num
ber o
f par
ticip
ants
Complete
Partial
None
Adherence Related to Perceived Disease Severity
Only 36/49 (73.4%) participants answered Q. 8 (Do you think you have CF? very mildly/mildly/moderately/moderately-sever/severe) and Q. 24 (How often do you miss a chest physiotherapy session in a week? 1/2/3/4/ if more please state) enabling a relationship between adherence and perceived disease severity to be investigated. Therefore, for the purposes of analysis 36 was considered to be the total group. It would appear that those participants who perceived their condition to be moderate or severe were more inclined to adhere to treatment.
Fig. 4. 17. Adherence and its correlation to perceived disease severity
As can be seen in the graph above, there is a moderate association between level of adherence and perceived disease severity. (Spearman’s Rank Correlation = 0.471, p = 0.004).
129

130

0
2
4
6
8
10
12
1 2 3 4 5
Agreement adherence
Num
ber o
f par
ticip
ants
Complete
Partial
None
Adherence Related to its Perceived Importance
Of the 36/49 (73.4%) respondents who answered Q. 12 (How much do you agree or disagree with the following statement: “Doing chest physiotherapy is important to my feeling of well being,” 20/49 (56%) consider that chest physiotherapy was an important determinant of their well-being. Moreover, adherence increased with the level of perceived importance of physiotherapy (Spearman’s Rank Correlation = 0.48, p = 0.003). In this instance the total group is considered to be 36.
Fig. 4. 18. Adherence to physiotherapy and its perceived importance
131

Perceptions of Disease Severity in Relation to FEV1
In the study group there was a significant negative association between perceived disease severity and FEV1 (rs = 0.579, p < 0.001). (Fig. 4.19).
Perceived Disease Severity
5.04.03.02.01.00.0
FEV1
100
80
60
40
20
0
Fig. 4. 19. Perceptions of disease severity in relation to FEV1
The significant negative association between perceived disease severity and FEV1
(Fig. 4. 19.) demonstrates that the participants had a realistic view of their disease severity, with those having a lower FEV1 correctly perceiving their disease to be more severe. This result indicates that participants should be inclined to access appropriate treatment when needed. Interestingly, 5/49 (10.2%) participants whose FEV1’s fell in the severe category (< 30%) did not perceive their condition to be severe. Of these five participants four died before the study was completed.
132

4. 7. 3. Reasons given for adherence behaviours
Questions 21 - 25, 27 – 30, 33 – 7, and 45 – 47 focused on adherence to physiotherapy and its importance. The answers to these questions were scored for ease of analysis (Appendix P) using Likert scales, or coded if they were open questions. The data was analysed and the findings presented in the three categories of adherence, partial adherence and non- adherence as described in Section Chapter1, p. 17.
1. Reasons given forbeing adherent
23/49 (46%) took ownership/responsibility of their physiotherapy treatment as they considered it to be their personal responsibility to maintain or improve their well-being
32/49 (65.3%) considered physiotherapy to be effective in clearing their chest 30/49 (61.2%) participants considered that it was effective in maintaining a
clear chest 11/49 (22.4%) participants had help with their treatment which gave them
positive support
If physiotherapy is perceived as being effective then the participants will do it because it is of benefit to them.
2. Partial Adherence
As total adherence is unrealistic all participants at some time would be partially adherent. Reasons given for partial adherence were
A clear chest therefore physiotherapy was not needed Physiotherapy was not perceived as being effective in clearing their chests Treatment made no discernable difference.
It is a significant clinical finding that some participants felt no better at the end of their physiotherapy treatment as this perceived ineffectiveness would affect their ability to adhere to physiotherapy treatment.
3. Reasons for Non-Adherence/Missing Treatment
Lack of Time
20/49 (40.8%) participants reported that lack of time. This was particularly relevant to the case of participant 29 who had two young children to look
133

after. Two other mothers, participants 9 and 49, hardly did any physiotherapy due to the demands of caring for two young children each. Treatment time needs to be as short and as effective as possible in order to encourage adherence.
Clear Chest
29/49 (59%) missed a treatment or did not do it because they considered their chests to be clear.
For adults who have minimal respiratory symptoms the recommendation (ACPCF/CF Trust, 2002; 2011) is that they use their preferred ACT to check that their chest is clear, or if it has minimal secretions, in which case exercise or an activity is encouraged to keep as fit and as healthy as possible. Participant No. 3 stated that he did exercise as it kept his chest clear. Studies have shown (Bradley & Moran, 2011; Bilton, et al., 1992; Salh et al., 1989) that exercise contributes to keeping the chest clear but it is a contentious issue. Exercise/activity, which is encouraged by the government in the general population (DoH, 2006a), is a sociable activity and facilitates adherence to treatment.
Boring
4/49 (8.1%) participants found daily physiotherapy to be “boring” which therefore compromised their ability to adhere to treatment.
Carr et al. (1996) in their study recorded similar replies. The chest physiotherapy technique most frequently used was the active cycle of breathing technique (ACBT) 40/49 (80.16%), while 3/49 (6.1%) participants did Positive Expiratory Pressure (PEP). The ACBT had been taught to all participants in the group, with the option to learn another technique if they wanted to do so or if they did not consider ACBT to be effective for them. Airway clearance should be carried out at least once a day even if it is to check that their chests are clear. Physiotherapy is a repetitive procedure and it is understandable that the participants find it boring.
134

4. 8. Summary of the study group and findings from the Pre-Intervention Physiotherapy Questionnaire
The study group appeared to be less healthy than the National CF Database population, as the study population had lower FEV1s. This may be accounted for by the fact that 5/49 (10.2%) of the study group had FEV1 < 30% which demonstrated that in a small study population (n = 49) it was possible for a small number to have a disproportionate impact. There was no statistically significant difference in BMI or age between the study group and the National CF Database population.
There was a moderate association between increased adherence and poorer health. However, four participants in the more severe range (FEV1 <30%) did not perceive themselves to be severe. This is disconcerting as these participants may not contact the Adult CF Specialist Centre when unwell nor adhere to treatment, if they do not perceive the need to do so. Establishing the participant’s health beliefs is essential if the ability to adhere to physiotherapy treatment is to be optimised.
Lack of time was frequently given as a reason for not doing physiotherapy, therefore emphasis needs to be placed on personal preference for choice of ACT and for planning treatment so that it fits into a busy life style and with other CF treatment regimens. The efficacy of physiotherapy treatment needs to be proven. No statistically demonstrable association was found here between gender and adherence to chest physiotherapy.
The above factors were taken into account when developing the educational strategy (the SMPP) whose aim was to optimise the ability to adhere to physiotherapy treatment. The development of the innovation will be discussed in Chapter 5 – The Self-Management Physiotherapy Programme (SMPP).
135

CHAPTER 5 – INTERVENTION/ACTION – THE SMPP AND THE POST-INTERVETNION PHYSIOTHERAPY QUESTIONNAIRE
5. 0. Introduction
The development and implementation of the Self-Management Physiotherapy Programme (SMPP) fulfils the third aim of the study ‘to develop and test the effectiveness of the SMPP’. When implementing the SMPP the researcher/ physiotherapist functioned as facilitator, with a humanistic approach to patient education, in keeping with a psycho-social model of care, rather than in the traditional role of being the ‘expert’ with the participants passively accepting advice. By empowering the participant through partnership working it was intended that the participant would have greater ‘ownership’ of their healthcare and as a result potentially increase their ability to adhere to physiotherapy treatment.
It was decided that the intervention period would be limited to six months because it was important to evaluate the effectiveness of the SMPP in case it was having a detrimental effect on the ability to adhere to physiotherapy and because CF is a life threatening disease the participants’ health could deteriorate as an inevitable part of disease progression making it difficult to extrapolate whether deterioration was attributable to disease progression or the impact of the SMPP. A three month follow after the start of the SMPP was carried out so that the progress of the SMPP could be monitored and it coincided with the CF Trust recommended follow up at the time of the study, and as it coincided with the CF Trust’s guidelines (CF Trust, 2002) for routine follow up at the time of the study. Time frames of three months and six months were adhered too so that all the participants were using the SMPP for the same length of time.
The SMPP was designed as a simple framework of what the participants needed to do when they were in a stable state in order to maintain their health, e.g. their pre and post physiotherapy treatment medication, their ACT, posture correction, hamstring stretches and mobilising exercises for the spine and chest, in addition to exercise/activity.
How the SMPP and the Post-Intervention Physiotherapy Questionnaire were developed and implemented is outlined below.
136

5. 1. Designing the SMPP
The findings (themes) from the two sets of semi-structured interviews and the results from the Pre-Intervention Physiotherapy Questionnaire were used to inform the design of the SMPP, which was to be individually tailored for each study participant. Fig. 5. 1. shows the sections selected to be covered and the design of the form. The SMPP was simple in design and presentation, inexpensive and easily adapted for individual use so that it was as inconspicuous as possible in order to appear to be part of a routine clinic review. This approach was taken in preference to a more ostentatious design which could induce a Hawthorne effect (Mayo, 1949) where participants respond to an intervention because they know they are being observed and as a result compromise the validity of the results. The SMPP took the form of a signed mutually agreed contract to encourage greater commitment to adhering to physiotherapy treatment.
137

SELF-MANAGEMENT PHYSIOTHERAPY PROGRAMME
Name Date
WHAT TO DO WHEN WELL:
Technique: Frequency
Duration Postural Drainage Position
Medication Pre-Physiotherapy
1. 2
.
Medication Post-Physiotherapy
2. 2
EXERCISE/ACTIVITY/SPORT
POSTURE CORRECTION MOBILISING EXERCISES FOR YOUR SPINE
GOALS
1.
2.
3.
4.
WHAT TO DO WHEN FEELING UNWELL
If you have any of the following;
∙
↑ Sputum ↑Wheeze ↑Cough ↓Energy ∙↓Exercise Tolerance
Telephone 0000 000000 and let us know Increase/modify your physiotherapy by ……………………………………
Fig 5. 1. Physiotherapy Self-Management Programme (SMPP)
138

● Health Beliefs and the Importance of Physiotherapy Treatment
Prior too completing the SMPP it would be important to identify each participant’s health beliefs in order to improve their ability to adhere to physiotherapy treatment. If they had negative health beliefs they were less likely to adhere to physiotherapy treatment as they would not see it as being beneficial to them. The researcher/ physiotherapist identified each participants’health beliefs by means of sensitive questioning and prompts and then developed an individually tailored education programme to address them. The aim would be to increase the participant’s awareness of the effectiveness of ACT in maintaining a clear chest or in clearing airway secretions and also to make them aware of the benefits of exercise/activity in maintaining or improving fitness and also in enhancing airway clearance (Bott et al., 2009; Bradley & Moran, 2011).
What to do When Well
Having established each participant’s health beliefs and re-enforced the importance of doing chest physiotherapy and exercise the participants’ ACT of choice was checked to ensure that they were competent in its use and the frequency and duration of the ACT jointly agreed. If the participant took medication before and after physiotherapy their understanding of its use and their competency in administering was checked.
Coping with Having CF - Goals
In keeping with a busy lifestyle participant-centred goals were individually tailored to ensure that the SMPP was achievable, effective and capable of being maintained. Careful consideration was needed to be given to goal setting so that participants’ preferences were taken into account as they are influential in adherence behaviours (Abbott et al., 2009; Daniels et al., 2011).
Denial – How to manage a chest infection/exacerbation
In order to address the issue of denial, which occurs when there is an underestimation of disease severity with a resultant delay in seeking help, a section on what to do when unwell was included to act as a prompt to encouraging early intervention. The clinical signs and symptoms of a chest infection such as increased sputum and coughing, were identified in the SMPP so that the participant was encouraged to promptly contact the Adult Specialist CF Clinic team for treatment advice and for
139

advice regarding increasing/modifying their chest physiotherapy by a specified amount. It was important that participants contacted the clinic as soon as possible so that chest infections could be treated promptly to prevent further deterioration.
5. 2. Piloting the SMPP
In order to enhance the SMPPs validity, reliability and effectiveness a pilot study was undertaken to ensure that the SMPP was clearly understood, unambiguous and easy to use in a busy clinic setting. A pilot study would show that the proposed method was workable, acceptable to the study participants and manageable (Bond & Gerrish, 2006).
Population and Sample
The original study population (n = 49) was reduced to 37/49 (75.5%) for the reasons outlined in Table 5. 1.
Table 5. 1. Tracking the study population TRACKING THE STUDY POPULATION Implementation of the SMPP
Study Numbers
Study Population (n = 49) (100%)
6 failed to return Pre-Intervention Physiotherapy Questionnaire 43 (87.7%)
Population issued with their SMPP (2 participants moved away; 2 died; 1 declined to be involved in the SMPP; 1 not contactable)
37 (75.5%)
The SMPP was piloted using an opportunistic sample of 8/49 (16%) participants selected from the 37/49 (75.5%) remaining study participants. Following discussions with the statistician this number of participants was considered to be a representative sample for a pilot study with a small study population (n = 49). The participants were selected over a period of a week while they were in a stable state during an out-patient clinic visit or during an in-patient stay. The first eight participants approached agreed to take part. The purpose of the SMPP was explained to them. They were asked to read the SMPP and confirm that they understood the questions. Their understanding was then checked by the researcher/physiotherapist who questioned their responses to ensure they fully understood the content.
All the participants in the pilot study commented that the SMPP was clear and concise and following a few minor alterations the SMPP was finalised and implemented.
140

5. 3. Implementing the SMPP
Administration of the SMPP
Of the 37/49 (75.5%) participants who remained in the study 26/49 (53.0)%) were approached face to face by the researcher/physiotherapist when they were in a stable state and all agreed to use the SMPP except one participant who declined stating that she did not wish to be involved with the SMPP as she was doing her own self-management physiotherapy programme. It was explained to these 25/49 (51.0%) participants, who agreed to use the SMPP, that its aim was to improve their ability to adhere to physiotherapy treatment by working with the researcher/physiotherapist to design their own individually tailored SMPP. Their ACT preferences would be taken into account and their physiotherapy goals would be set jointly with the researcher/ physiotherapist so that they were effective, achievable and capable of being maintained. A section would focus on “what to do when unwell” by identifying the signs and symptoms of a chest infection at which point they could either modify their own physiotherapy programme and/or contact the CF Clinic for further advice and treatment.
The SMPP was a user-friendly intervention which was easily incorporated the routine three monthly clinic assessment. Its effectiveness was monitored using a Feedback Chart which recorded the participants comments on whether the SMPP improved their ability to adhere to physiotherapy. The SMPP focused on the participant’s physiotherapy needs. It did not incorporate the recording of clinical outcome measures such as FEV1 and sputum (volume, colour and viscosity) and exercise tolerance as they were recorded in the physiotherapy notes. Sputum results, chest x-ray scores, pathology results and pharmacological information were recorded in the medical notes and used as part of the physiotherapy assessment but only FEV1
readings at the start and finish of the intervention period were used as outcome measures.
The SMPP was tailored to meet the needs of each participant. During an in-patient stay, when they were in a stable state, or during and out-patient visit discussions took place between the participant and the researcher/physiotherapist to established the following factors which had been identified in the study as being influential in adherence behaviours:
141

Health beliefs – through careful questioning the participant’s health beliefs were identified so that any barriers to treatment were highlighted and addressed. This information was recorded in the physiotherapy notes.
Knowledge and understanding – through careful questioning the participant’s knowledge and understanding of CF and the need for physiotherapy was established. Any misconceptions were addressed through patient education. This information was recorded in the physiotherapy notes
Skills – each participant’s ACT was reviewed to ensure they were doing it correctly at the beginning of the study period and again if necessary at the three month and finally at the six month follow up.
Personal preferences for ACTs - at the time of the study the Adult CF Specialist Clinic was a new development with the majority of patients transferred from the hospital’s Paediatric Specialist CF Clinic. The ACBT was the most frequently used ACT as it was taught to all the participants while they were in the Paediatric CF Specialist Service. Each participant’s ability to carry out their ACT was checked to ensure that it was appropriate and their technique was effective. At the time of the study it was decided not to introduce a new ACT to a participant unless clinically warranted as it would be difficult to evaluate the effectiveness of the SMPP to improve adherence if the participant considered the new ACT was unsuitable.
The SMPP had to fit into the participant’s life style and both the researcher/ physiotherapist and the participant had to be confident that the programme could be maintained taking into account the other CF treatment regimens that also had to carry out, e.g. nebulisation of medication, nasgo-gastric feeding. For participants with mild CF (FEV1 > 75%) and minimal secretions an example of a SMPP would be a session of chest physiotherapy once a day using their preferred ACT for 15 minutes and a visit to the gym once a week in addition to general advice of keeping fit and active by walking when ever possible. For a participant with severe disease (i.e. an FEV1 < 30%) chest physiotherapy four times a day of 10 – 15 minutes could be recommended, with an exercise programme comprising of sit to stand five times in a row with a rest in between each sit to stand and after a further rest, one or two minutes of marching on the spot twice daily. For a participant with severe disease oxygen would be required during their physiotherapy programme.
After the three months 11/49 (22.4%) participants still remained to be seen and it was decided to write to them informing them of the planned implementation of their SMPP. An explanatory letter was sent with a blank copy of the SMPP outlining its
142
purpose. Introducing the concept of the SMPP in a letter enabled the participant to have time to think about it. From the researcher/physiotherapist’s perspective it was an efficient use of time because when the participant was seen at the Adult Specialist CF Centre the idea of having an SMPP would have already been introduced to them. By the time the 11/49 (22.4%) participants had received their letter 4/49 (81.6%) had already visited the clinic and agreed to use it.
All the remaining 7/49 (14.2%) participants who had been sent an explanatory letter with a blank SMPP were then contacted by telephone and all 7/49 (14.2%) agreed to use it. The telephone consultation with each participant was easily conducted as all the participants had previously received the relevant information by post. A personalised SMPP was designed for each of the 7/49 (14.2%) participants during the telephone contact and signed by the researcher/physiotherapist. A photocopy of the signed SMPP was sent to the participant for them to sign and return in a stamped addressed envelope (SAE) to the Adult Specialist CF Centre where it was placed in the participant’s physiotherapy notes and a photocopy of it returned to the participant. All of the participants were informed that if they wished to change their SMPP they were to contact the researcher/physiotherapist using the telephone number that had been given to them in their Patient Information Leaflet (Appendix F).
The study population issued with their SMPP is illustrated below:
Table 5. 2. Tracking the study population using the SMPP
Study population issued with their SMPP
Study Pop. Agreed to use the SMPP
Declined to use the SMPP
Total Study Population 49/49 (100%)
Participants remaining in the study 37/49 (75.5%)
Approached face to face (including 4 participants who had been sent a tletter) 29/49 (53%) 1/49 (2.04%)
Telephoned following no response from being sent a letter 7/49 (14.2%)
Population using the SMPP 36/49 (73.5%)
Three Monthly Follow Up
The participants were reviewed at three months because monitoring them at regular intervals would mean that they were more likely to adhere to their physiotherapy treatment (Abbot et al., 2009; Sawicki et al., 2008) in addition to complying with CF Trust Standards of Care (2001). The purpose of the three monthly follow up was to review the participants’ SMPP and make any necessary adjustments and also to
143

evaluating its effectiveness by recording the participants comments in the Feedback Chart.
By the three month follow up 1/49 (2.0%) participant was not contactable so the numbers remaining in the study were reduced from 36/49 (73.5%) to 35/49 (71.4%) (Table 5. 3, p. 146). Of these 35/49 (71.4%) participants 23(46.9%) were reviewed either as in or out-patients while in a stable state within the three month time period. The remaining 12/49 (24.9%) who had not been seen by the researcher/ physiotherapist for a variety of reasons were contacted by telephone. All 12/49 (24.9%) participants agreed to continue using the SMPP which was then reviewed and updated during the telephone contact. The participants views on its effectiveness were recorded on the Feedback Chart. A copy of their three month SMPP review was sent to the participant for them to sign and return to the researcher/ physiotherapist copies of which were placed in the physiotherapy and medial notes.
The Feedback Chart
The Feedback Chart used a simple layout to record the comments made by the participants on the effectiveness of the SMPP to optimise their ability to adhere to physiotherapy treatment. The researcher/physiotherapist made notes of the participants’ comments and recorded them at the three month follow up and again at the six month follow up which marked the end of the implementation period of the SMPP. By giving feedback on the effectiveness of the SMPP the participants were engaged and empowered to contribute to the evaluation of the study and thereby would potentially be more likely to remain in the study. It was important to review the participants ACT to ensure it was being carried out effectively and that they felt that it was effective for them because treatment preferences are influential in adherence behaviours (Abbott et al., 2009; Daniels, 2010; Pryor et al., 2010). It was also important to monitor the participants views on the SMPP at an early stage in case it was hindering their ability to adhere to physiotherapy treatment. If the SMPP had impeded adherence it would have been withdrawn and the study curtailed. Following the three month follow up the study population was reviewed again six months after the implementation of the SMPP.
Six Month (Final) Follow-Up
The six month follow up marked the end of the intervention period. The SMPP was reviewed and any necessary adjustments to treatment made. The participants’ comments on the effectiveness of the SMPP were recorded by the researcher/
144

physiotherapist on the Feedback Chart. The Post-Intervention Physiotherapy Questionnaire was issued at the same time as the participant’s SMPP was reviewed. How the Post-Intervention Physiotherapy Questionnaire was developed is outlined below. The number of study participants was reduced to 32/49 (65.3%) for a variety of reason outlined in Table 5. 3.(p. 146). Of the remaining 32/49 (65.3%) participants 24/49(48.9%) were reviewed either as an in-patient or as an out-patient when they were in a stable state while the remaining 8/49 (16.3%) participants were reviewed by telephone. Their comments of the SMPP were recorded on the Feedback Chart. In the course of the study all participants were followed up at least once in person at the three or six monthly follow up.
5. 4. Issuing the Post-Intervention Physiotherapy Questionnaire
Development of the Post-Intervention Physiotherapy Questionnaire
The purpose of the Post-Intervention Physiotherapy Questionnaire was to act as an evaluation tool to measure any changes which may have occurred following the implementation of the SMPP. To measure change it is necessary to have at least two cross-sectional surveys conducted on the same population (McKenna et al., 2006). The survey was issued in two stages with the Pre-Intervention Physiotherapy Questionnaire issued at the beginning of the intervention and the Post-Intervention Physiotherapy Questionnaire issued at the end of the study. The design of the Post-Intervention Physiotherapy Questionnaire was based on that of the Pre-Intervention Physiotherapy Questionnaire because in order to monitor any changes which may have occurred as a result of the implementation of the SMPP it was necessary to ask the same questions again. However, two additional questions were added in order to help assess the effectiveness of the SMPP to optimise the ability to adhere to physiotherapy treatment from the participants perspective.
Q. 49 How do you rate the Self-Management Physiotherapy Programme you have been using?
Q.50 How has the Self-Management Physiotherapy Programme helped you? Please give an example.
Although the researcher/physiotherapist recorded the participants’ comments on the effectiveness of the SMPP using the Feedback Chart, it was important to record the participants’ opinions using their own words by using a different tool, i.e. the Post-Intervention Physiotherapy Questionnaire, in order to enhance the reliability and
145

validity of the replies. By giving each participant a written and verbal opportunity to express their views on the effectiveness of the SMPP a comprehensive assessment was obtained.
Issuing the Post Intervention Physiotherapy Questionnaire
The Post-Intervention Physiotherapy Questionnaire was issued at the end of the study period to the remaining 32/49 (65.3%) participants at the same time as the review of their SMPP took place. Of the 32/49 (65.3%) participants remaining in the study 24/49 (48.9%) were reviewed as part of their routine out-patient clinic assessment where they were asked to complete the Post-Intervention Physiotherapy Questionnaire at a time convenient to them and return it in a stamped addressed envelop (SAE) while the remaining 8/49(16.3%) participants were followed up by telephone. The Post Intervention Physiotherapy Questionnaire was sent by post with a SAE for them to return it to the researcher/physiotherapist. The study population during the duration of the study is outlined below (Table 5. 3., p.146). Of the 32/49 (65.3%) remaining in the study 29/49 (59.1%) completed it by returning the Post-Intervention Physiotherapy Questionnaire.
146

Table 5. 3. Tracking the study population
Stages of the Study Nos.
involved at each stage
Actioned by
Select study population: Specialist Adult CF Clinic – full care group - total eligible population
61 R
Inclusion and exclusion criteria applied 55
Recruited to study +(6 declined)
49 (100%) R
PLAN First Set Semi-Structured Interviews – Sub-group (n = 3) * C P
Analysis of First Set of Semi-Structured Interviews R & C P
Second Set of Semi-Structured Interview - Sub group (n = 5)* (Interviewees did not comprise of the same participants who were in the first set of semi-structured interviews )
C P
Analysis of Second Set of Semi-Structured Interviews R & CP
Pre-Intervention Physiotherapy Questionnaire developed from the findings (themes) of both semi-structured interviews
R
Pre-Intervention Physiotherapy Questionnaire pilotedSub-group (n = 12)*
R
Pre-Intervention Physiotherapy Questionnaire issued to study population
49 (100%) R
Pre-Intervention Physiotherapy Questionnaire returned 43 (87.7%)Pre-Intervention Physiotherapy Questionnaire analysed R
INTERVENTION/ACTIONSMPP designed RSMPP piloted - Sub-group (n = 12)* RStart of Intervention: SMPP issued +(2 moved away; 2 died; 1 declined to use the SMPP; 2 not contactable)
36 (73.4%) R
3 month Follow-Up SMPP reviewed and evaluated using Feedback Chart+(1 not contactable)
34 (69.3%) R
Finish: 6 month Follow Up: SMPP reviewed; Post-Intervention Physiotherapy Questionnaire issued +(1 went travelling; 2 died)
32 (65.3%) R
Post-Intervention Physiotherapy Questionnaire returned
29 (59.1%)
EVALUATION Pre & Post Intervention Physiotherapy Questionnaires Analysed and Feedback Chart evaluated
R
REFLECTION
Legend* Sub-groups were selected from total study population (n = 49)+ Reasons for the study population reducing
CP = Clinical Psychologist R = Researcher/Physiotherapist
147

The issuing of the Post-Intervention Physiotherapy Questionnaire marked the end of the intervention period. The analysis of the Post-Intervention Physiotherapy Questionnaire and the findings from the Feedback Chart are presented in Chapter 6, P. 148.
148

CHAPTER 6 – EVALUATION
The results and analysis are presented below:
6. 0. Introduction
The aim of this chapter was to meet the fourth aim of the study ‘to evaluate the impact of the new SMPP on adherence to physiotherapy’. The analysis and results of the Pre-Intervention Physiotherapy Questionnaire compared with the Post-Intervention Physiotherapy Questionnaire and the findings from the Feedback Chart are presented below:
6. 1. Results and Findings on Adherence from the Comparison of the Pre and Post Intervention Physiotherapy Questionnaires
The Post-Intervention Physiotherapy Questionnaire was analysed using Windows SPPS 10. The data was analysed for each participant and the results compared with those of the Pre-intervention Physiotherapy Questionnaire so that any changes which may have occurred as a result of the implementation of the SMPP could be presented. The statistical tests and p values used in the analysis are described in each example.
Adherence was classified as outlined in Chapter 1 p. 17. Although 29/49 (59.1%) participants completed the study, for the purposes of analysis some statistical tests were not able to be performed on the full 29/49 (59.1%) participants as in some instances insufficient participants answered the required questions to enable an analysis to be carried out.
Analysis of the Pre and Post-Intervention Physiotherapy Questionnaires revealed an increased trend in adherence following the introduction of the SMPP.
Adherence was measured using the following evaluation:
Measurement of Adherence
Adherence was measured at the beginning and end of the study period to monitor any changes in adherence behaviour which may have occurred as a result of the SMPP. Questions 22, 24, 33 and 34 were used in the Pre and Post Intervention Physiotherapy questionnaires to assess the participant’s level of adherence at the beginning and end of the study so that any changes could be recorded.
149

By the participant answering Q. 22, 24, 33 and 34 with a range of possible answers of 0 – 4 or more times a day it was possible to establish if they were adherent, partially adherent or non–adherent. Adherence is a complex issue and there is no universally accepted definition for the purpose of physiotherapy, nor any treatment specific objective outcome measures in CF to monitor adherence behaviour. The researcher/ physiotherapist developed their own definition of adherence for the purpose of the study (Ch. 1, p. 17). As 100% compliance is unrealistic adjustments were made when categorising the participant’s level of adherence when responding to the above questions:
Adherent – treatment which has been agreed between the researcher/ physiotherapist and the participant and the participant reports that they are implementing it (with an allowance for missing three or less physiotherapy sessions a week).
Partial Adherent – treatment which has been agreed between the participant and the researcher/physiotherapist but the participant reports that they are only partially implementing it (with an allowance for missing four or more physiotherapy sessions a week)or did it intermittently and when they were unwell.
Non-Adherent – treatment which has been agreed between the researcher/ physiotherapist and the participant but the participant reports that they are not implementing it and participants who are not in agreement with the physiotherapist over the need for physiotherapy and report that they do not do any.
Only 21 participants had answered both questions in the Pre and Post Intervention Physiotherapy Questionnaire enabling the impact of the SMPP on their ability to adhere to physiotherapy treatment to be evaluated. When making recommendations for chest physiotherapy the researcher/physiotherapist would have recommended the frequency and duration of daily treatment following assessment of the participant’s clinical needs and having discussed their programme with them so that the recommendations were jointly set.
The results are presented in three ways Table 6. 1. shows the overall changes in adherence before and after the
implementation of the SMPP Fig 6. 1. presents these changes in a bar graph format Table 6. 2. presents the same results by means of identifying each participant’s
change in level of adherence.
150

0
2
4
6
8
10
12
14
Num
ber o
f Ppa
rtici
pant
s
Adherent Partially Non
Adherence to physiotherapy
Before
After
Table 6. 1. Change in adherence attributable to the implementation of the SMPP
Before After
Total Adherent Partially Non
Adherent 9 3 0 12
Partially 3 3 0 6
Non 2 1 0 3
Tota 14 7 0 21
Based upon the data presented above the observed change in level of adherence was not statistically significant (McNemar’s test, p = 0.505). However, the numbers were small and although it would not be possible to draw a statistically significant conclusion it is evident that overall adherence to physiotherapy treatment in the study group increased. The trend in increased adherence is also reflected in the positive comments made by the participants in the Feedback Chart and in the Post-Intervention Physiotherapy Questionnaire. The results are further illustrated in the bar graph in Fig 6. 1.
Fig. 6. 1. Change in adherence before and after the implementation of the SMPP
The results show the changes in behaviour before and after the implementation of the SMPP. The following changes took place:
151

Increase in adherence: for 3/49 (6.1%) participants their level of adherence increased from being partially adherent to being fully adherent;. for 2/49 (4.08%) participants their level of adherence increased from being non- adherent to being fully adherent and 1/49 (2.04%) non-adherent participant became partially adherent
No change in adherence: 9 participants remained adherent before and after the implementation of the SMPP while 3 remained partially adherent
Reduced adherence: for 3/49 participants their level of adherence dropped from being adherent before to being partially adherent
Overall for six participants (12.29%) the trend was for adherence to increase, for 12/49 (24.48%) participants it remained unchanged and for 3/49 participants it reduced.
These results are presented again in Table 6. 2., p. 152 which demonstrates the change in each participant’s level of adherence following the implementation of the SMPP.
152

Individual participant’s level of adherence before and after the implementation of the SMPP
Table 6. 2. Adherence measured before and after using the SMPP
Participant ACT* Level of AdherenceStart**
Level of AdherenceEnd**
Outcome
1 ACBT P/A No A2 ACBT A P/A Down3 ACBT No A No A4 ACBT - A5 ACBT/PEP P/A -6 ACBT N/A P/A Up7 X X X8 ACBT A A =9 NONE No A -10 ACBT A P/A Down11 ACBT A A =12 ACBT A -13 NONE - -14 FLUTTER P/A -15 ACBT P/A P/A =16 ACBT No A P/A17 ACBT A -18 NONE N/A -19 FLUTTER A A =20 ACBT A -21 ACBT A -22 PEP P/A P/A =23 ACBT P/A A Up24 ACBT A A =25 ACBT A A =26 NONE No A No A27 ACBT/PEP A A =28 ACBT A P/A Down29 PEP/FLUTTER P/A P/A =30 DB&C N/A A Up31 ACBT P/A -32 X X X33 ACBT P/A .34 ACBT P/A A Up35 DB&C No A -36 X X X37 AD No -N/A -38 DB&C No A A39 NONE No A No A40 PEP A A =41 DB&C N/A A Up42 NONE No A N/A43 DB&C N/A -44 X X X45 X X X46 ACBT A A =47 AD A A =48 X X X49 PEP P/A A Up
153

Legend
*Airway Clearance Technique (self-reported) in the total study population
22/49 (44.9%) ACBT (Active Cycle of Breathing Technique) 3/49 (6.12%) PEP (Positive Expiratory Pressure) 2/49 (4.08%) AD (Autogenic Drainage) 2/49 (4.08%) F (Flutter) 5/49 ( 10.2%) D B & C (Deep Breathing & Coughing) 2/49 (4.08%) ACBT/PEP 1/49 (2.0%) PEP/F
6/49 (12.2%) NONE -Did not do any physiotherapy 6/49 (12.2%) X – Consented to be in the study but did not complete the Pre-
Intervention Physiotherapy Questionnaire
** Level of Adherence A – Adherent (agreed to do physiotherapy and either complied fully or missed
3 or less sessions a week)
PA – Partially Adherent (agreed t odo physiotherapy but missed 4 or more physiotherapy sessions in a week or did physiotherapy on an irregular basis or when unwell)
NA – Non Adherent (either agreed to do physiotherapy and did no td oit or did not do any physiotherapy at all)
***Replies X – Consented to take part but did not return the questionnaires No A– All the relevant questions were not answered - Did not return questionnaire.
.
6. 1. 1. Adherence attributable to use of ACT
154
The study group predominantly used the ACBT. At the time of the study the adult clinic had recently started up with the majority of participants progressing from the Paediatric Specialist CF Clinic where the ACT most frequently taught was the ACBT. Because of the small numbers of participants who used an ACT other than the ACBT it was not possible to investigate relationships between each of these different ACTs and adherence behaviour.
Table 6. 3. ACT used by the participants who completed the study
ACT
Numbers
ACBT 12/21 (57.1%)
PEP 3/2 (14.2%)
AD 1.21(4.7%)
Flutter 1.21(4.7%)
DB & C 2/21 (9.5%)
ACBT/PEP 1/21(4.7%)
PEP/FLUTTER 1/21(4.75)
6. 2. Disease Severity Before and After the Implementation of the SMPP
155

The FEV1 is a universally accepted objective means of measuring lung function which gives and indication of disease severity (Miller et al., 2005). The table below records the change in FEV1 for the 29/49 (59.1%) participants who completed the study.
Table 6 . 4. Summary of statistics for FEV1
Fev1 Before After Change
Mean (SD) 47.7 (16.5) 43.9 (15.5) 3.8 (10.9)
The observed fall in FEV1 of 3.8% is not statistically significant (t = 1.9, p = 0.066) although it might be considered a borderline result but a fall of 3.8% is of clinical concern. However, the study was carried out over the winter months and people with CF are more prone to chest infections in winter which could account for the fall. In a small study population a few participants with chest infections would have a disproportionate impact on the percentage calculation but this would statistically not be of significance.
It was important to establish if the FEV1 of the participants had fallen as studies (Abbott et al., 1996; Kettler et al., 2002) have shown that adherence can increase as a result of anxiety about progressive deterioration. If adherence to chest physiotherapy had increased it would not be possible to attribute it to the effectiveness of the SMPP if the FEV1 of the group had fallen significantly (i.e. > 3%) as the increase may have been due to anxiety. If the SMPP had remained the same or had fallen slightly but within expected parameters for a six month time frame then an increased level of adherence could possibly be attributed to the SMPP. The fall of 3.8% in this study is slightly greater than a 2.5% fall which would be in keeping with the expected fall for adults in this age group at the time that the study was undertaken (Que, Cullin, & Geddes, 2006). If the result of the study demonstrated that adherence had increased and the FEV1 had not fallen significantly then it would be possible to attribute the increase in adherence to the effectiveness of the SMPP. Without measuring the FEV1
it would impossible to evaluate the effectiveness or other wise of the SMPP to improve adherence to physiotherapy treatment.
CF is a life limiting disease and a deterioration of -3.8 in the course of a year would be expected in this age cohort (Que, Cullinan, & Geddes, 2006). Therefore a fall of 3.8% in this study was not too significant considering the this time of year. It can be considered that for those who completed the study they were in a relatively stable state. This result could also be interpreted that the deterioration could be due to the
156

intervention of the SMPP however, as CF is a multi-system life limiting disease involving complex treatment, such an opinion would preclude this as the sole interpretation.
Health care professionals have to understand that people make choices and the decision not to adhere to treatment for what ever reason has to be accepted providing it is not based on inaccurate information or a false perceptions (Nunes et al., 2009).
6. 3. Change in FEV1 in Relation to Levels of Adherence
157

Table 6. 5. Changes in FEV1 by levels of adherence
Change in FEV1
Level of Adherence
Adherent ( n = 12)
Partially Adherent (n = 7)
Non Adherent ( n = 3)
Mean (SD) 6.3 (12.9) -3.6 (7.5) 7.3 (13.4)
As discussed in 6.1 in order for the level of adherence to be classified the participants had to answer both Q. 22 and Q. 34 of the Pre and Post-Intervention Physiotherapy Questionnaires. Of the 29/49 (59.1%) participants who completed both sets of questionnaires only 21/49 (42.8%) answered both these questions leaving 8/49 (16.3%) participants whose level of adherence could not be classified and the impact of the SMPP on their ability to adhere to physiotherapy treatment unaccounted for.
There was no evidence of any statistically significant difference with regard to change in FEV1 between the participants in the three groups (analysis of variance, p = 0.214), suggesting that the study group had remained statistically stable in relation to their level of disease severity. Relating this to the levels of adherence the results indicate that during the study period the level of disease severity did not influence the participant’s level of adherence. The statistical analysis does not take into account the four participants who died.
Adherence Related to Perceived Disease Severity
158

The participants’ perceived level of disease severity was self-reported by answering the multiple choice question Q. 11 “Over the past month how has your health been? 1. Very Good; 2. Good; 3. unwell; 4. very unwell?”
Statistical analysis using the Spearman’s Rank Correlation showed a value of r = 0.135 (p = 0.528) indicating no association between these two variables. This result demonstrates that adherence was not related to anxiety regarding the participants’ perception of their disease severity.
159
6. 5. The Findings from the Feedback Chart and the Post-Intervention Physiotherapy Questionnaire on the Effectiveness of the SMPP
Feedback Chart
The effectiveness of the SMPP to optimise the ability to adhere to physiotherapy treatment was reviewed at the three and six monthly follow ups using the Feedback Chart to monitor the participants’ comments. The 29/49 (59.1%) participants who completed the study made the following comments
Table 6. 6. Comments on the effectiveness of the SMPP.
Feedback Chart Comments Numbers
Excellent 2/49 (4.1%)
Very good 18/49 (36.7%)
Good 5/49 (10.2%)
No comment 1/49 (2.0%)
Negative comment 3/49 (6.0%)
Of the total study population (n = 49) 25/49(50.1%) made positive comments on the effectiveness of the SMPP. Examples of the comments are outlined below in Table 6. 6.
Table 6 . 7. Comments on the effectiveness of the SMPP
Negative Positive
● It did not make any difference I was doing it anyway.● I don’t really do physio unless I am ill so it didn’t alter my approach.
● It helps to jointly set goals.
● It was helpful to have it written down.
Although there was a significant difference in the verbal responses from the participants regarding the effectiveness of the SMPP it was predominately perceived as being a contributing factor in optimising the ability to adhere to physiotherapy treatment.
160

Post-Intervention Physiotherapy Questionnaire – Comments on the SMPP
The participants positive comments on the effectiveness of the SMPP as recorded in the Feedback Chart were augmented by the replies given in response to Q. 50 (How has the self-management programme helped you?) in the Post-Intervention Physiotherapy Questionnaire. Of the 29/49 (59.1%) who completed the study by returning their Post-Intervention Physiotherapy Questionnaire 20/49 (40.8%) commented positively about the SMPP while 5/49 (17.2%) participants did not comment, 3/49 (10.3%) gave unequivocal answers and 1/49 (2.04%) considered that they were unable to use the SMPP due to ill health.. Examples of the comments are presented in Fig. 6. 2.
Positive Comments on the SMPP
It inspired me to do more You feel that you are helping yourself I felt more committed It was a boost to see it written down and to know
that the physio was checking
Fig 6. 2. Positive comments on the SMPP
These subjective comments gave valuable insights into how effective the participants considered the SMPP to be. It could be argued that these participants thought positively about the intervention and therefore they completed the study when they could have dropped out.
Summary
The group of 29/49 participants who completed the study represents 59.1% of the total study population (n = 49) and therefore gave valid insights into the effectiveness of the SMPP. The positive comments received from the participants in the Post-Intervention Physiotherapy Questionnaire acted as a form of triangulation when compared with the positive comments from the Feedback Chart.
The discussion and implications of how the SMPP appeared to help improve adherence to physiotherapy and how effectively the research aims were met is presented in Chapter 7.
161

CHAPTER 7 – REFLECTION
The reflection on the research process and its outcomes are presented as follows;
Discussion Conclusions Recommendations for Clinical Practice Recommendations for Future Research Limitations Reflection
7. 0. Discussion
The impact of the SMPP is discussed as follows:
7. 1. The Impact of the SMPP
This is a unique clinically-based exploratory study that used a mixed methodology to investigate the many complex issues in the specialist field of adherence to physiotherapy in CF. To date no studies have been undertaken to investigate the effectiveness of an SMPP to improve the ability to adhere to physiotherapy treatment for adults with CF. The purpose of the study was to investigate the problems adults with CF have in adhering to physiotherapy treatment by establishing, from their perspective, what these problems are and developing an educational strategy in the form of a SMPP to potentially improve their ability to adhere to physiotherapy treatment.
The study demonstrated a trend in increased adherence to physiotherapy treatment which can potentially lead to improved health outcomes such as reducing the rate of respiratory decline, the need for hospitalisation and the frequency and duration of physiotherapy treatment time. These improved outcomes can also contribute to a reduction in healthcare and pharmalogical costs in addition to a reduced dependency on social benefits as people with CF become healthier and consequently more employable. All of these factors can potentially contribute to an increased life expectancy and a better QoL.
162

7. 1. 1. Increased Trend in Adherence to Physiotherapy Treatment
The study demonstrated that following the implementation of the SMPP there was an increased trend in adherence to physiotherapy treatment. For the 21/49 (42.8%) participants who completed the study and answered the relevant questions (Q. 22, Q. 24, Q. 33, and Q. 34 ) enabling their level of adherence to be measured, adherence had increased for six as 3/49 (6.15%) partially adherent participants became adherent and non-adherence had reduced from 3/49 (6.15%) participants to nil. This trend, although not statistically significant, indicates that the SMPP was likely to have been effective in optimising the participants’ ability to adhere to physiotherapy treatment and in doing so answered the research question “Will the newly developed SMPP optimise the ability of adults with CF to adhere to physiotherapy treatment?” This outcome was supported by the participants’ positive comments about the SMPP in the Feedback Chart and in the Post-Intervention Physiotherapy Questionnaire.
Analysis of the Post-Intervention Physiotherapy Questionnaire indicated that this trend in increased adherence was not related to disease severity (Table 6. 3. p. 154) as there was no association between the participants’ perception of their disease severity and their level of adherence to physiotherapy (Ch. 6. 5, p.157). This outcome suggests that anxiety about their disease severity was not the cause of an increase in adherence. Also, over the six month study period, which was conducted during the winter months when there is an increased prevalence of chest infections, the participants’ lung function had remained stable with a fall of only 3.8%, indicating that anxiety about their condition was unlikely to have induced the increase in adherence. Other studies (Abbott et al., 1996; Kettler et al., 2002) show conflicting findings. Abbott et al. (1996) in their study on health perceptions and adherence to treatment concluded that anxiety regarding disease severity did increase adherence, while Llorente et al. (2008) found in their study that an increase in disease severity corresponded with a reduction in adherence to treatment.
A reduction in adherence may be accounted for by the fact that if the level of disease severity becomes too great for some individuals to cope with they may avoid perceptions and behaviours which compel them to acknowledge the seriousness of the situation (Abbott et al., 1996). A reduction in adherence to physiotherapy treatment can also occur with disease severity when no clinical benefit is detectable following treatment (Kettler et al., 2002). In this study the trend in increased adherence did not appear to be due to the participants worrying that their condition had deteriorated and correspondingly increasing their level of adherence, but was more probably due to the SMPP optimising their ability to adhere to physiotherapy treatment.
163

To date there have been no studies conducted into adherence to physiotherapy in CF using a SMPP so it is not possible to compare the results with other similar studies, as to date there have been no studies conducted into adherence to physiotherapy in CF using a SMPP. However self-management programmes have been successfully developed for use in other chronic respiratory diseases such as chronic obstructive pulmonary disease (COPD) (Effing et al., 2007) and asthma (Powell & Gibson, 2003) where they have proved to be effective.
An SMPP is an effective means of addressing barriers to adherence as a persons health beliefs, knowledge and skills need to be identified prior to using a SMPP and an individually tailored education programme put in place to address them. For those with negative health beliefs and the perception that physiotherapy was ineffective, educating them about the benefits of physiotherapy and how it can be used as a means of controlling their disease can contribute to removing barriers to adherence.
A successful self-management programme requires regular reviews (Sawyer & Aroni, 2005) and good communication in order to improve the necessary knowledge and skills to bring about positive behavioural changes (Nunes et al., 2009). Over the six month study period the participants were followed up at three months and again finally at six months in order to re-enforce the implementation of the negotiated agreed goals.
7. 1 2. Health Beliefs, Perceptions of Having CF and Perceptions of Disease Severity
The importance of health beliefs in adherence to physiotherapy were first identified by Carr et al. (1996) who stated that to facilitate adherence to physiotherapy treatment health beliefs and perceptions of the effectiveness of physiotherapy need to be identified and a treatment programme designed to address them. This finding has also been noted in other studies (Abbott et al., 2009; 2001; 1996; Bucks et al, 2009; Daneils, 2010; Kettler et al., 2002; Myers & Horn, 2006; White et al., 2007). It is possible that as the disease gradually progresses and QoL deteriorates (Badlan, 2006), accommodation is made so that the true level of disease severity is not accurately perceived and therefore appropriate treatment is not adhered too.
In this study there was a significant negative association between perceived disease severity and FEV1 (Fig. 4. 19, P. 131) demonstrating that the participants had a realistic view of the level of their disease severity and therefore should access appropriate treatment when needed. Other studies have shown this not to be the case
164

(Abbott et al, 1996; Dodd & Webb, 2000) and have commented that people with CF are more inclined to underestimate the significance of their disease severity thus making it potentially less likely that they would seek medical help or implement the necessary treatment.
The outcome of no association between perceived level of disease severity and the level of adherence following analysis of the Post-Intervention Physiotherapy Questionnaire (Ch. 6. 4, p. 158) is different to that indicated following analysis of the Pre-Intervention Physiotherapy Questionnaire (Fig. 4. 19, p. 131) where it appeared that those participants who perceived their condition to be moderate or severe were more inclined to adhere to treatment. However, four severely ill participants died during the course of the study period and the difference in the outcomes between the beginning and end of the study period could indicate that at the end of the intervention period, the remaining group of participants were in a better state of health and potentially less worried about their disease. This result could also be said to support the view that the trend in increased adherence was due to the effectiveness of the SMPP and not due to the participants being anxious about their condition and consequentially increasing their adherence to physiotherapy treatment. Abbott et, al. (1996) and Myers and Horn (2006) demonstrated that a positive attitude and an optimistic yet realistic view of having CF resulted in greater adherence to treatment because treatment was perceived to be important and beneficial in reducing the impact of having CF.
In this study positive health beliefs together with a strong internal locus of control, developed through a humanistic approach to patient education, empowered the participants to work in partnership with the professional to design their SMPP. This psycho-social approach to the management of chronic disease challenges the traditional model of a medically dominated care pathway where the patient is in a passive/dependent position.
7. 1. 3. The efficacy of physiotherapy and adherence to treatment
The effectiveness of chest physiotherapy was questioned by several participants indicating that the participants either needed to feel clinically better following a treatment or they need to believe that chest physiotherapy was important even if they did not feel clinically better following treatment. Studies have demonstrated (Abbott et al., 2009; Nunes et al., 2009) that if a treatment is perceived as being of benefit then it is more likely to be adhered too. However, health care professionals have to understand that people make choices and the decision not to adhere to treatment for
165

what ever reason has to be accepted, providing it is not based on inaccurate information or a false perceptions (Nunes et al., 2009). For example one non-adherent participant (No. 43) strongly agreed that physiotherapy was important but failed to comply with the two sessions a day recommended by the CF researcher/ physiotherapist and only carried out physiotherapy twice a week. It is relevant to point out that this female participant had two young children and found adhering to treatment problematical. The effect of the responsibility of having children on a participant’s ability to adhere to physiotherapy has yet to be explored as few people with CF have children. The direct relationship between increased adherence and the perceived importance of physiotherapy (Fig 4. 18, p. 130) is significant as these participants would have presumably thought that physiotherapy is beneficial to their well being. The participants who disagreed with the concept of physiotherapy being important to their well being were in the partial and non-adherent groups and may have considered physiotherapy to be ineffective or unnecessary.
There was a significant range in the reasons for non-adherence of physiotherapy ACTs with some study participants perceiving physiotherapy to be “boring” and “time consuming” and its clinical benefits unclear (“it doesn’t make any difference”) while others considered that “without it I would not be so well”. Studies (Abbott et al., 2009; Daniels, 2010; Kettler et al., 2002) suggest that participants may not adhere to physiotherapy treatment if they do not feel clinically better for doing it, or experience no detrimental effects for failing to do a treatment, or are unaware of the consequences of non-adherence. These findings can be interpreted as a perception that chest physiotherapy is only effective if sputum is produced, therefore if little or no sputum is produced then either it is not needed or it is not effective (Huyard, 2008). At the time of the study the CF Trust’s guidelines for physiotherapy clinical practice (ACPCF/CF Trust, 2002) had been published, supporting the use of ACTs for chest physiotherapy but acknowledging that the evidence was poor. A Cochrane Review (van der Schans, Prasad & Main, 2000) investigated chest physiotherapy compared to no chest physiotherapy and came to the conclusion that ACTs had a short term effect in facilitating mucus transport but the supporting evidence lacked reliability and validity. Although these findings were incorporated into the clinical practice of the researcher/physiotherapist, the evidence base to support ACTs was limited which may have influenced the participants’ level of adherence. If there was inconclusive evidence to support the use of ACTs they may have been perceived as not being necessary/effective which would be a barrier to adherence. Physiotherapy can be time consuming and when complex treatment programmes involving several components need to be carried out people with CF make decisions as to which is the most
166

beneficial in the time they have available for treatment. Health care professionals should be aware that a degree of non-adherence is acceptable if people living with CF are to maintain a sense of normality in their lives (Badlan, 2006; Daniels et al., 2011; Daniels, 2010; Nunes et al., 2009).
Studies into the efficacy of physiotherapy are difficult to evaluate due to the inability to conduct randomised controlled trials because the withdrawal of treatment would be unethical and placebo treatment impossible to implement. To have a control group with one arm not having physiotherapy treatment would require careful ethical consideration as physiotherapy is a recommended treatment modality for CF (Bott et al., 2009; ACPCF/CF Trust, 2011). Frequently physiotherapy studies on ACTs are short term and do not account for changes in adherence over a period of time. As there is no objective outcome measure for physiotherapy treatment, studies rely on the honesty and recall of the participants, which can be unreliable and the accuracy with which the physiotherapy treatment is uncertain.
In recent years substantial work, including five Cochrane Reviews (Elkins et al., 2009; Main et al., 2009; Morrison & Agnew, 2009; Robinson et al., 2010; van der Schans et al., 2009) and one long term study (Pryor et al., 2010) have contributed significantly to the knowledge regarding the efficacy of ACTs. These studies give greater credence to recommending ACTs which is reassuring for people with CF and can contribute to improving adherence to physiotherapy. People with CF need to be informed of the evidence that supports clinical practice and the positive benefits that good airway clearance can bring to their health outcomes such as reduced hospitalisation and improved QoL. Whether this improved efficacy would have contributed to an increase in adherence to physiotherapy treatment in this study is a debatable point.
7. 1. 4. Gender and Adherence
The study demonstrated that there was a trend for the female participants to be less adherent than the males (Table 4. 6., p.128) but this was not statistically significant due to the small number involved as only 12/49 (20.4%) males and 24/49 (48.9%) females answered both Q. 2, which established their gender and Q. 22, 24, 33 and 34 which self-reported their level of adherence to physiotherapy treatment. This result is a similar to another study by Willis et al. (2001) who demonstrated that young women were less adherent to physiotherapy than young men. Their study however was based upon a much younger population of 16 – 20 year olds. It would be advantageous to
167
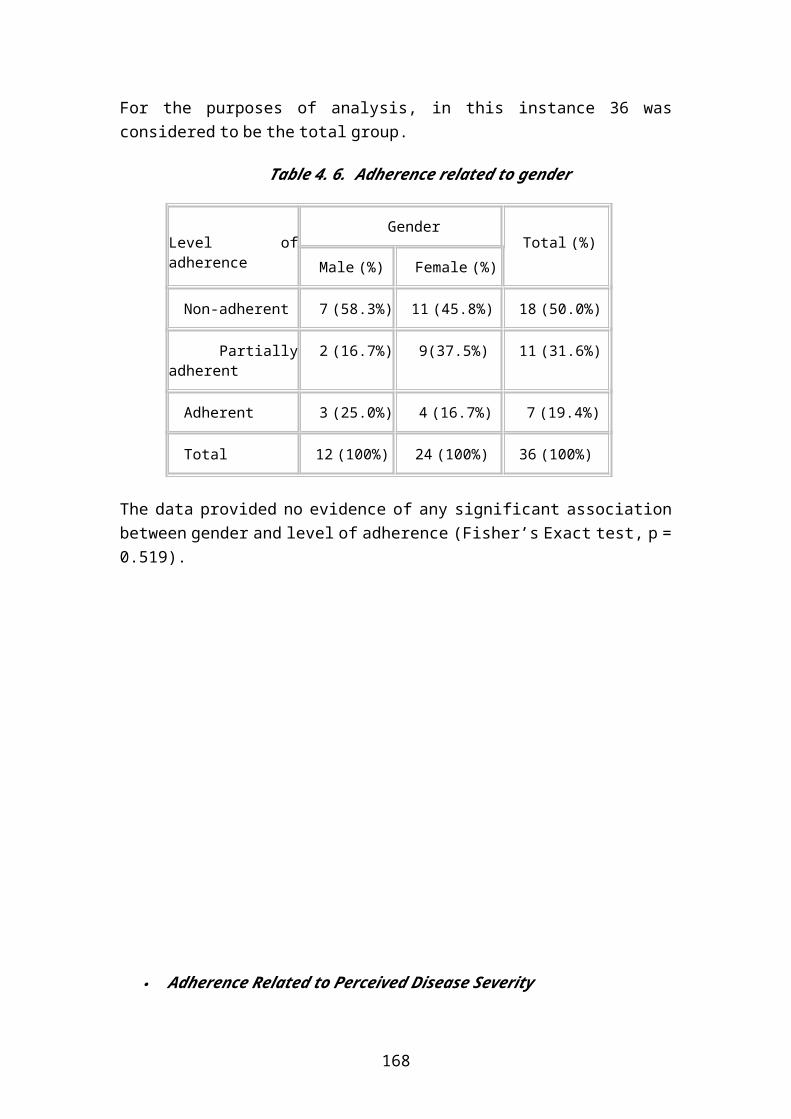
follow the cohort in the Willis et al. (2001) study to establish whether their level of adherence to physiotherapy changed as they grew older.
There are gender differences in CF, with females having a poorer prognosis than males (CF Trust, 2011b; Myers & Horn, 2006; Sawyer et al., 1995). Studies (Myers & Horn, 2006; White et al., 2007) into adherence to physiotherapy identify the ratio of males to females in the study population but do not extrapolate any differentials in adherence rates between the two groups. In this study the FEV1 of the study group remained fairly stable for the population who completed the study (Table 6. 4, p. 155). There was also no statistical difference in the level of adherence (Fisher’s Exact test p = 0.0519, Table 4. 6. p. 126) between the males and the females, consequently the greater adherence to treatment by females may be due to gender rather than anxiety about the severity of their disease. Gender differences identified in this study warrant further investigation as to date there is little research carried out into this aspect of adherence to physiotherapy treatment. An appropriately powered study may show a significant effect.
7. 1. 5. Exercise and Airway Clearance
In this study exercise was one of the components of the SMPP, with every participant having an exercise goal e.g. to go to the gym once a week and carry out their exercise programme. Exercise provides a means of “peer identification” as exercise is not just a treatment modality for CF, it is an activity that is encouraged by the DoH (2010) to improve the nations health and well being. Exercise contributes to a positive self concept which enhances confidence and self respect (Bucks et al., 2009). Studies (Abbott et al., 2009; Daniels, 2010) have highlighted that having a normal life style and not appearing different from their peers was important for people with CF. However some participants found it embarrassing to cough when exercising in a gym and therefore only attended the gym when well. Some participants reported doing exercise instead of chest physiotherapy. Although it is considered that exercise can enhance airway clearance it is not a substitute for chest physiotherapy (Bott et al., 2010; Bradley & Moran, 2011).
7. 1. 6. Patient Education, Empowerment and Adherence
An SMPP is an effective means of addressing barriers to adherence as a persons health beliefs, knowledge and skills need to be identified. For those with negative health beliefs and the perception that physiotherapy was ineffective, educating them about the benefits of physiotherapy and how it can be used as a means of controlling
168

their disease can remove barriers to adherence. Patient education is an important factor in the health care management for people with CF because they need to be aware of the benefits of chest physiotherapy in optimising their health outcomes even though they may not feel any clinical benefit following treatment. Recent Cochrane Reviews (Elkins et al., 2009; Main at al., 2009; Morrison & Agnew, 2009; Robinson et al., 2010; van der Schans et al., 2009) and a study by Pryor et al., (2010) have demonstrated the effectiveness of ACT and support current clinical practice and there by contribute to encouraging adherence behaviours.
In this study involving the participants appeared to improve their sense of ‘ownership’ of their treatment programme and encouraged greater adherence. In working with the professional the participant was viewed as being an ‘expert’ of their own condition while the professional was viewed as an ‘expert’ in their clinical practice. This joint working as equal partners gave ‘permission’ for the participant to be more assertive and pro-active, as their views were requested and taken into account in designing their own SMPP. The participants would not have as extensive a knowledge and understanding of the range of ACTs and the evidence-base that supports these treatment regimens as the professional. This inequality was ‘corrected’ by the researcher/professional being aware of the imbalance and actively contributing the necessary professional input when designing a participant’s SMPP by seeking the participants’ involvement and respecting their opinions. Empowering the participant by increasing their knowledge and skills enabled them to be an “expert patient” which is in keeping with the government’s policy of making people more responsible for their health care (DoH, 2007). It also gave them the confidence to use their SMPP effectively.
Patient education can be used to encourage hard to reach populations who are partially or non-adherent to make informed decisions about their physiotherapy treatment choices. Physiotherapists need to have an understanding of how adults learn and the humanistic educational principles (DoH, 2007; Knowles, 1989; Rogers, 1983) which underpin this approach i.e. self-directed learning, with the teacher acting as a facilitator. The principals of adult education can be incorporated into the development of self-management programmes so they are effective in empowering people to take responsibility for their healthcare and potentially optimise their ability to adhere to treatment. Over the six month study period the participants were followed up at three months and again finally at six months in order to re-enforce the implementation of the negotiated agreed goals.
169

7. 2. Conclusions
Although the study was hampered by a small study population, the lack of a control group, limited measurement techniques and the lack of an internationally agreed criteria for adherence, it nevertheless added to the understanding and knowledge of the complex issues surrounding adherence to physiotherapy treatment in CF. In addition it met the research aims and developed a SMPP that demonstrated a trend of improving the ability to adhere to chest physiotherapy treatment. The aim of chest physiotherapy is to keep the chest as clear as possible of secretions in order to reduce the frequency of chest infections and slow down the decline of lung damage (ACPCF/CF Trust, 2002; 2011) all of which can potentially bring about improved health outcomes, a reduction in health care utilisation, greater longevity and a better QoL.
The following conclusions can be drawn:
7. 2. 1. Overall health improvements and better disease management that the SMPP is likely to deliver as a result of the SMPP improving the ability to adhere to treatment
(a) Health Improvements
Outcomes
1. Facilitating chest clearance or maintaining a clear chest2. Reducing the rate of decline in respiratory function3. Reducing hospitalisation4. Reducing the need for additional out-patient visits5. Reducing physiotherapy treatment time due to better health 6. Increasing life expectancy with quality to added years
Improved QoL resulting in
1. Less disruption in employment, family and social life 2. Reduced dependency on psychological support 3. More able to lead a life in keeping with peers
Improved/maintained exercise tolerance potentially resulting in
1. Improved fitness and general well being2. Improved posture3. A reduction in the impact of osteoporosis and the development of
adverse
170

4. respiratory mechanics in the chest wall5. A reduction in the risk of musculo-skeletal joint pains
(b) Improved Disease Management
Reduced hospitalisation By giving people with CF the knowledge and skills to self-manage by incorporating a diary for detailed clinical monitoring (FEV1, sputum characteristics) in their SMPP it may reduce the need for additional out-patient visits, hospital admissions and the length of stay while an in-patient.
Reduced staff time
An effectively managed SMPP can reduce the demand on physiotherapy staff time as people with CF should be able to modify their own physiotherapy treatment.
Clinical monitoring
Detailed monitoring of clinical status, managed using a diary format and/or tele-monitoring, can form part of a SMPP. Sharing clinical information can act as feedback encouraging adherence to treatment and provide accurate information to enable people with CF to make decisions about modifying their physiotherapy treatment. Clinical monitoring can result in a more prompt approach to treatment for chest infections as individually tailored indicators of when to contact the CF physiotherapist/Adult CF Specialist Clinic can be incorporated into it e.g. if the FEV1
falls below a certain level then the CF physiotherapist needs to be contacted. Prompt treatment of a chest infection can mitigate the consequences of deteriorating respiratory function and therefore be less costly in terms of avoiding hospital admission and the prolonged use of expensive antibiotics.
Admission Avoidance and Early Discharge
An SMPP can be used to facilitate care at home and if required a physiotherapist an make home visits to ensure that optimal care is being delivered and potentially avoid admission and facilitate early discharge.
More Employable
171

By adhering to physiotherapy treatment people with CF can potentially be healthier and therefore more employable and take less time off work for sickness. Being employed can bring about an improved QoL and a better sense of well being. Employment reduces the dependency on social benefits and contributes to the national economy by paying taxes. As previously stated a SMPP, used in conjunction with clinical monitoring, can keep people at work during episodes of exacerbations treated with IV antibiotics and thereby reduce the risk of unemployment through high sickness levels.
Lower pharmacological costs
Improved adherence to physiotherapy treatment can potentially result in fewer chest infections and a reduced incidence of painful musculo-skeletal complications resulting in lower pharmacological costs, less time taking medication, and thereby reducing the burden of care.
Increased life expectancy and a better QoL
The trend of improved adherence to physiotherapy treatment can potentially bring about better health, an improved life expectancy and a better QoL. Such improvement can result in people with CF leading a life more in keeping with their peer, being better able to achieve milestones in life such as employment, marriage and having a family, thereby reducing the need for psychological support.
7. 2. 2. Adherence and Self-Management Programmes
This exploratory study demonstrated a trend for the SMPP to improve the ability to adhere to physiotherapy treatment for adults with CF and can consequently be postulated as a new model of clinical practice. The trend of improved adherence, although not statistically significant, was supported by the positive comments made in the qualitative information given by the participants in Feedback Chart and the Post-Intervention Physiotherapy Questionnaire. The SMPP is simple to administer, inexpensive and user friendly. Empowering people through increased knowledge and skills encouraged them to work in partnership with the researcher/physiotherapist to develop their own individually tailored SMPP.
7. 2. 3. Adherence and Health Beliefs
Health beliefs are important factors in influencing the ability to adhere to physiotherapy. If a person perceives that they are able to influence the course of their disease, in spite of there being no cure, they are more likely to adhere to treatment. If
172

people with CF consider that no matter what they do it will make no difference to the course of their disease then they are less likely to adhere to physiotherapy treatment. The study suggested that participants who saw physiotherapy as a means of controlling their disease were more adherent to physiotherapy, while the non-adherent participants had negative health beliefs that acted as a barrier to adherence. Health beliefs need to be identified and appropriate patient education strategies put in place to improve knowledge and understanding so that people with CF develop a positive attitude towards their physiotherapy treatment in order to optimise their ability to adhere to physiotherapy treatment.
Adherence and Gender
The relationship between gender and adherence behaviours is poorly understood. The female participants demonstrated a trend to be more adherent to physiotherapy treatment than the males for reasons that are unclear. This inequality needs to be investigated as there are significant differences in life expectancy with males living longer that females (CF Trust, 2011b), and improving adherence to physiotherapy for females could potentially reduce this.
Adherence, Patient Education and Empowerment
In order to improve adherence to physiotherapy for adults with CF, physiotherapists need further training on patient education strategies to improve knowledge and skills so that people with CF can use self-management programmes to best effect. The CF physiotherapist needs to take a humanistic approach to patient education by acting as a facilitator to encourage self-directed learning. Patient preferences for ACT need to be taken into account as physiotherapy treatment has to be fitted into the patient’s life style, so it is important that they can choose their preferred treatment (Daniels, 2010; Pryor et al., 2010). Good communication and close monitoring by means of a daily/weekly diary incorporated into the SMPP can give feedback that can contribute to improving adherence to physiotherapy treatment.
7. 2. 6. Summary
The trend of an increased adherence to physiotherapy, following the implementation of the SMPP, is a significant outcome because physiotherapy is one of the least liked of CF treatments and has the lowest levels of adherence (Abbott & Gee, 1998; Abbott et al., 2009; Daniels, 2010; White et al., 2007). If the SMPP, which is inexpensive and easy to issue in a busy clinic setting, is perceived by the participants as being effective
173

in improving their ability to adhere to physiotherapy treatment then a new model of physiotherapy clinical practice can be postulated.
The study has contributed to the development of evidence-based physiotherapy practice and consequently provided justification for a change in physiotherapy clinical practice, that will bring about a more effective and efficient use of scarce physiotherapy resources. The development of a new model of clinical practice that could potentially bring about improved health outcomes and better disease management complies with the CSP’s policy of clinical excellence (CSP, 2005) and the government’s policy (DoH, 2006b) of clinical governance, which encourages high standards of evidence-based practice to improve health outcomes for patients and improve service delivery.
174

7. 3. Recommendations for Future Research
7. 3. 0. Introduction
The findings from this exploratory study have contributed to physiotherapy knowledge of CF, provided useful insights and potential explanations into the complex behaviours and problems which surround poor adherence to physiotherapy treatment. There has been little published work in this area and as a result this study has raised issues which warrant further investigation.
7. 3. 1. Adherence to Physiotherapy
Studies into adherence to treatment in CF focus on why people do not adhere to treatment. A study into why adults with CF do adhere to physiotherapy would give insights into these behaviours, that may potentially be used to develop educational strategies to improve adherence to physiotherapy treatment for adults who have non-adherent behaviours. The measurement of adherence to physiotherapy is dependent on self-reporting which can be unreliable. The use of telemedicine to record FEV1 or physiotherapy treatment would result in closer monitoring of the study participants, which could act as feed back to encourage adherence behaviour (Daniels et al., 2011; Kettler et al., 2002; Quittner et al., 2000a; 2000b).
7. 3. 2. Health Beliefs
Greater recognition needs to be given to the importance of health beliefs and locus of control and the influence they have on the ability to adhere to physiotherapy treatment in CF. Assessment and monitoring tools such as interviewing or a questionnaire need to be developed to identify them. These assessment tools could be administered at the first attendance in an adult CF clinic and then regularly reviewed thereafter so that any changes in health beliefs can be monitored and the SMPP adapted accordingly.
7. 3. 3. Efficacy of ACTs
The efficacy of ACT needs further investigation using more rigorous research methods over a longer time period (i.e. a year) so that the justification for a particular physiotherapy treatment is supported by high quality evidence-based research. With advances in the medical treatment of CF resulting in a healthier population on going studies need to be conducted so that the evidence base for recommended physiotherapy treatments are relevant and up to date. To date a long term study of one year by Pryor et al. (2010), five Cochrane Reviews (Elkins et al., 2009; Main at al.,
175
2009; Morrison & Agnew, 2009; Robinson et al., 2010; van der Schans et al., 2009), the Association of Chartered Physiotherapists in Respiratory Care (ACPRC)/BTS Guidelines (Bott et al., 2009) and the ACPCF/CF Trust (2011) guidelines for the physiotherapy treatment for people with CF concluded that there was no evidence to support the view that one ACT was more effective than any other, but this conclusion was based on, in some instances poor quality studies. There are also wide ranges of disease severity and future research needs to investigate the effectiveness of ACTs in relation to disease severity. CF treatment can be complex and time consuming, making it difficult to fit into a busy life style, therefore physiotherapy treatment preferences are an important element in encouraging treatment adherence.
Physical exercise, which is an effective adjunct to ACTs as it enhances respiratory function (Button & Holland, 2008), warrants further research to investigate the most effective means of achieving enhanced airway clearance and identifying what is required to maintain/improve general health and well being. Such an approach would also be in keeping with the government’s drive to improve the health of the general population (DoH, 2010). Recommendations for exercise need to be evidence-based using rigorously designed studies that favour having people with CF as the participants so that the outcomes are as valid and as reliable as possible.
7. 3. 4. Mixed Methodology
Combining qualitative and quantitative research approaches gave a deeper understanding of the problems people with CF have in adhering to physiotherapy treatment and contributed to the development of an intervention to resolve them. Knowing why people do not adhere to treatment may allow greater accuracy in predicting poor adherence and the deployment of scarce physiotherapy resources.
The use of qualitative research needs to be encouraged within the physiotherapy profession as patient preferences are an important influence in adherence behaviour (Abbott et al., 2009; Daniels, 2010; Pryor et al., 2010). The use of semi-structured interviews, virtual focus groups and workshops can elicit rich detail of a participants “life world”, giving insights into their health beliefs and their perceptions of having CF, which are influencing factors in adherence behaviour. Although the randomised controlled trial is the “gold standard” of evidence based research it would raise ethical issues if physiotherapy was withdrawn in order to have a control group because physiotherapy is an established part of the treatment of CF, and it would be impossible to have “placebo” physiotherapy treatment.
176

Coping Skills
The study provided unique insights into having CF from the participant’s perspective. Although the life expectancy for people with CF is continuing to improve it nevertheless requires a considerable range of coping skills to be able to manage this life limiting disease in a positive manner. Further studies need to be undertaken to investigate strategies to develop a person’s ability to cope with CF. By encouraging a positive approach to physiotherapy treatment through education about its benefits, leading to a perception of physiotherapy as a means of controlling their disease process, adherence can be encouraged.
7. 3. 6. Infection Control
The need to comply with infection control issues (CF Trust, 2008; 2004a; 2004b) has implications for future research methodology as people with CF are not encouraged to mix socially with each other due to the risk of contacting MRSA or Pseudomonas, therefore focus groups or workshops are precluded. The development of the internet as a substitute social forum would be an alternative method of conducting focus groups and workshops but ethical issues involving anonymity would need to be addressed.
7. 3. 7. Patient Education
The benefits of exercise specifically for people with CF need to be investigated and the impact exercise has in enhancing airway clearance ACTs warrants further investigation, as to date it has yet to be proven (Bradley & Moran, 2011). Studies also need to be undertaken into the social benefits of exercise, as it enables people with CF to identify more closely with their peers which can have a positive impact on adherence behaviours.
To date no studies have been carried out into adult education in CF as it is only in recent years that people with CF have been living longer. Studies into how patient education can be made more responsive to the needs of people with CF will ensure that the necessary knowledge and skills are learnt, so that people with CF are able to use a SMPP to the best effect, and potentially optimise their ability to adhere to physiotherapy treatment.
177

7. 3. 8. Gender
Gender differences in adherence behaviours need to be investigated so that educational strategies can be developed to accommodate them. This is important when developing strategies to optimise the ability to adhere to physiotherapy.
Studies (Masterson, Wildman, Newberry, & Omlor, 2011; Patterson et al., 2008) have identified that adolescent girls find the impact of having CF more emotionally difficult to cope than adolescent boys and this may be directly linked to the fact that females also have a shorter life expectancy than males for reasons that remain unclear (Patterson et al., 2008). In view of these findings further research is warranted so that physiotherapy management can be specifically tailored to address these issues. Further qualitative research need to be undertaken to gain a greater understanding of why gender impacts on adherence behaviour so that patient education strategies can be developed to address it. If females become more adherent their health would potentially improve along with their life expectancy and QoL.
7. 3. 9. Telemedicine
The use of telemedicine to monitor clinical changes and give feedback can act as a means of encouraging adherence to physiotherapy treatment. Telemedicine can also be used as a treatment diary and to monitor health status e.g. recording FEV1 so that the information is available to the CF physiotherapist in order to modify the patient’s SMPP if necessary. Research needs to be carried out on how to use such electronic systems for optimal patient benefit and to improve disease management.
178

7. 4. Recommendations for Future Clinical Practice
Recommendations for future clinical practice are presented below:
7. 4. 1. Postulation of a New Model of Clinical Practice
As the SMPP demonstrated a trend to improve the ability to adhere to physiotherapy treatment adults with CF should be given the option to have their physiotherapy treatment managed using an SMPP. The SMPP empowered the participants and encouraged them to work in partnership with the researcher/ physiotherapist to jointly agree a treatment programme. The formalisation of the SMPP, by both the participant and the physiotherapist signing it, contributed to the “ownership” of the programme and improved the ability to adhere to physiotherapy treatment. The SMPP is inexpensive, easy to administer, user friendly, and adaptable to all levels of disease severity.
Each SMPP would need to be evaluated to ensure that it was effective. This could be achieved by means of a survey, in the form of a self-administered questionnaire, which could be issued to a clinic population at regular intervals to record the impact the SMPP was having on their ability to adhere to physiotherapy treatment.
7. 4. 2. Health Beliefs
Health beliefs need to be identified as they are a framework for understanding and explaining adherence behaviour. What beliefs a person with CF holds about their disease and their perception of the effectiveness or otherwise of their physiotherapy treatment needs to be identified on admission to an adult CF clinic and yearly thereafter as health beliefs can change over time. To date there has been no standardised format specifically designed to record health beliefs for adults with CF, therefore a validated questionnaire needs to be developed to identify and measure them. The key factors that need to be indentified are what having CF means to them, their views on the effectiveness of their physiotherapy treatment and any barriers that impede adherence to physiotherapy treatment. Inaccurate assumptions, which can act as barriers to treatment, need to be addressed by means of patient education. An individually tailored SMPP can then be designed to meet their needs in order to improve their ability to adhere to physiotherapy treatment.
179

7. 4. 3. Patient Education
It cannot be assumed that in spite of years of contact with a CF Clinic people with CF have an accurate and realistic understanding of their condition, the benefits of physiotherapy treatment and the consequences of not carrying out their treatment. Patient education is an important factor in the health care management for people with CF because they need to be aware of the benefits of chest physiotherapy in optimising their health outcomes even though they may not feel any clinical benefit following treatment. Recent Cochrane Reviews (Elkins et al., 2009; Main at al., 2009; Morrison & Agnew, 2009; Robinson et al., 2010; van der Schans et al., 2009) and a study by Pryor et al. (2010) have demonstrated the effectiveness of ACTs and support current clinical practice.
On admission to an adult CF clinic an assessment of a person’s knowledge, skills, understanding of their disease and their physiotherapy treatment needs to be undertaken so that any lack of knowledge or misunderstandings that could act as a barrier to treatment can be identified and addressed. This is particularly relevant as the effectiveness of physiotherapy has frequently been questioned. Information needs to be given of the benefits of physiotherapy (Elkins et al., 2009; Main at al., 2009; Morrison & Agnew, 2009; Pryor et al. 2010; Robinson et al., 2010; van der Schans et al., 2009), even if they are not clinically discernable, and the consequences of not adhering to treatment need to be clearly explained. Those with clear chest and normal lung function would still need to check daily that their chests are clear and if that is the case then treatment needs to focus on exercise/activity to improve/maintain their fitness and well being.
In order to effectively use an SMPP a patient’s knowledge and skills need to be regularly updated. Patient education can be managed through individual teaching sessions, videos, literature and the internet. The CF Trust and the ACPRC have an excellent range of teaching material. Patient education needs to be based on humanistic principals (Knowles, 1989) where the teacher acts as a facilitator of learning.
ACTs and Personal Treatment Preferences
Studies have shown that no one ACT is any more effective than any other (Daniels, 2010; Pryor et al., 2010) therefore personal preferences need to be taken into account when planning a SMPP. People with CF want to lead lives comparable with their peers therefore physiotherapy treatment needs to be as effective, efficient and
180
incorporated in to a persons life style as much as possible e.g. going to the gym which is a popular means of keeping fit used by the general population. People with CF are healthier, living longer, leading busy lives and therefore ‘what works for them’ is important as they are more likely to adhere to it. Where there are complex time consuming treatments personal preferences are important as a means of encouraging adherence behaviour.
Empowerment
People with CF need to be empowered to take more ownership for their condition as a means of encouraging adherence. Empowering people with long term conditions to become self-managing is part of the government’s drive for improved health outcomes and is embodied in the ‘Expert Patient Programme’ (DoH, 2001b; 2005). The concept of self-management is also part of the government’s initiative to deliver health services in the community (DoH, 2010a; 2010b) and reduce the need for hospitalisation e.g. Nunes (2009) acknowledges that choices must be respected whilst empowerment gives people the confidence to manage their own condition. This approach requires the patient to have the necessary knowledge and skills to actively participate in the decision making process required in a self-management programme. Self-management can be achieved through a humanistic approach (Knowles, 1989) to learning where the professional acts as a facilitator encouraging the patient to have the necessary knowledge, skills and confidence to undertake a self-management programme. A humanistic approach also encourages empowerment by means of the patient working in partnership with the professional to design their own self-management programme and thereby take more responsibility for their healthcare and reduce the demand on physiotherapy time. Although the Expert Patient Programme (DoH, 2001) is delivered in a group setting, which would not be possible for people with CF due to it contravening Infection Control Guidelines (CF Trust, 2004a; 2004b), the principles of it can be embodied in a one-two-one approach. When people with CF join an adult clinic the concept of them being empowered to take responsibility for their healthcare needs to be explained to them so they understand what is being asked of them.
Clinical Monitoring
Having demonstrated an increased trend in adherence the SMPP could be improved by incorporating a self-monitoring diary recording clinical details such as cough (dry, chesty, day or night, trigger factors), sputum (graded by colour chart, volume, viscosity) and FEV1 along with individually tailored indicators of when to contact the CF Clinic such as increased coughing, haemoptysis or reduced exercise tolerance.
181

Close monitoring can encourage prompt management of developing respiratory problems and thereby help to mitigate the damaging consequences on respiratory function. A diary can be used for tele-monitoring e.g. daily/weekly FEV1 recordings which can be sent to the CF clinic in situations where recovery from a chest infection is being managed by using intravenous (IV) antibiotics at home. Treatment can be closely monitored and advise such as changing/adapting an ACT or increasing exercise/activity can be given. Being treated at home can reduce heath care costs, the risk of hospital acquired infections, facilitate early discharge and for those in work it is less disruptive. Parameters can be set such as if the FEV1 falls below a certain level medical and physiotherapy intervention needs to be sought. Over a period of time diary recordings can demonstrate trends such as an increase in chest infections during the winter months warranting prompt treatment. Treating people at home may necessitate physiotherapists undertaking community visits to assess, treat and possibly prevent a hospital admission or an additional clinic visit.
IT and Telemedicine
IT and Telemedicine can also be used to record whether treatment such as inhaled antibiotics to treat chest infections is being taken, prescribed medicines have been collected and whether emails or texts giving information or treatment reminders have been opened.
Using electronic patient records can facilitate treatment by having them available to all members of a CF team for immediate information sharing, the documentation is legible, they can facilitate auditing of information to identify trends and facilitate prompt treatment by negating the need to wait for the patient notes. Using texting or the telephone to re-enforce an SMPP can encourage adherence proving the patient does not think it to be intrusive.
Video conferencing can be used between professionals to discuss difficult cases or using a patients television as a video link to the CF team for consultation can potentially avoid an additional out-patient visit, facilitate discharge or prevent hospital admission.
Infection Control Issues
The SMPP needs to be used in a one-to-one capacity as a peer group method of delivery would not be possible due to infection control guidelines which recommend segregation of people with CF to prevent colonisation of Pseudomonas and MRSA infections
182

7. 5. Limitations
The study had a number of limitations which are outlined below:
7. 5. 1. Definition of Adherence
Definition of AdherenceMeasurement of adherence was limited as there is no universally accepted definition of adherence to physiotherapy treatment. For the purposes of this study the researcher/ physiotherapist developed a definition of adherence based on a broad understanding of being adherent, partial adherent and non- adherent for the purposes of this study. The definition also accounted for the fact that 100% adherence is unrealistic and missing up to three treatments in a week for someone who was doing physiotherapy twice a day was still considered as being adherent. Having such a specific definition would limit the opportunity for meta-analysis as it was unique to this study. A universally accepted definition, accommodating for the fact that sustaining 100% adherence is unrealistic, needs to be developed so that peer review and meta-analysis studies can be undertaken for the purpose of improving clinical practice.
7. 5. 2 Measurement of Adherence
Studies into adherence to physiotherapy rely on self-reporting which can be inaccurate due to reliance on poor recall, honesty and a belief that what is being carried out is correct but the technique and/or duration is inadequate (Abbott,et al., 2009; Daniels, 2010). To date there is no valid and reliable outcome measure for physiotherapy. It is not possible to rely on the rate of adherence to other treatment modalities in CF being indicative of the rates of adherence to physiotherapy as there is considerable variation between treatment modalities (Abbott et al., 2009; Daniels et al., 2010). The study was limited in measuring adherence as it was only recorded on three occasions by asking the participants to self-report their level of adherence; firstly at the start of the study, at the three month follow up and a further three months later which marked the end of the six month study period. The evaluation of adherence was also based on the judgement of the researcher/physiotherapist which as studies have shown (Abbott et al., 2009; Daniels et al., 2010) self-reporting can be unreliable and inaccurate. A self-reported daily diary, which would have aided re-call and improved accuracy of reporting, was not incorporated into the SMPP. This detailed form of data collection would have potentially produced more accurate results and acted as a prompt to encourage greater adherence.
183

Rates of adherence in this study were recorded in terms of percentages to give an indication of the impact that the SMPP had on optimising the ability to adhere to physiotherapy treatment, but in a small study population (n = 49) such as this, percentages can give a disproportional impression.
7. 5. 3. Length of Study
This study was of limited duration with the implementation of the SMPP being conducted for six months over the winter period. This “snapshot” cannot account for the variations in the level of adherence to physiotherapy treatment which can occur over a longer period of time. Longitudinal studies of a year or more need to be undertaken to reflect a potentially variable pattern of adherence, as people with CF have longer periods of good health. Seasonal variations such as during the winter months when there is an increased tendency for developing chest infections requiring a corresponding increase in the frequency of chest physiotherapy, need to be accounted for. Ongoing longitudinal studies are a useful tool in giving feedback to the participants as they can re-enforce adherence behaviours by building on success (Quittner et al, 2000a; 2000b). Studies of one year need to be undertaken to identify if an intervention has significantly improved adherence and if so has the improvement been maintained.
7. 5. 4. Small Sample Size
Small Sample Size This exploratory study was limited to the full care group of patients in one Adult CF Specialist Centre. The study investigated potential behaviour changes in response to the intervention (SMPP) and warranted a more-in depth approach which only small numbers could provide. In this predominately qualitative study, to have increased the study population by including the ‘shared care’ group or having a multi-centre trial would have been problematical as the researcher/physiotherapist would have had insufficient knowledge of the additional participants, and there would be a lack of consistency in the clinical assessment of the participants and in the implementation of the SMPP if other researchers were involved. However, the small study population (n = 49) had a disproportionate impact on statistical analysis due to the attrition rate, through incomplete responses and the death of four of the participants. In some instances a result may not have been of statistical significance but was clinically important e.g. adherence rates by gender. None the less, 29/49 (59.1%) completed the study and because of the small numbers it was possible to collect rich detail of the issues surrounding adherence to physiotherapy for people with CF. Having
184

established that the SMPP appears to improve adherence to physiotherapy a future study could include the involvement of the ‘shared care’ patients. A multi-centre trial would have enabled a broader range of behaviours to have been investigated.
7. 5. 5. Definition of Physiotherapy Used
As this was an exploratory study physiotherapy was confined to the use of ACTs and exercise in relation to general activity and the possible enhancement of sputum clearance. Other treatment interventions such as non invasive ventilation (NIV), the use of nebulised medication and treatment for urinary incontinence, which come within the broader remit of physiotherapy, were excluded as not all people with CF require these treatments whereas all adults with CF should carry out ACTs and have an exercise programme. Including interventions such as NIV, nebulised medication and treatment for urinary incontinence would have introduced too many variables and been too unwieldy in this predominately qualitative study.
7. 5. 6. Reflexivity
The researcher was also responsible for the physiotherapy service to the study population which could have resulted in the recruitment and analysis of the results being biased. Measures were put in place to reduce the possibility of bias by ensuring that the potential participants were given time to reflect on whether they wished to participate, a psychologist conducted the two sets of semi-structure interviews giving the interviewees an opportunity to freely express their views, a colleague was involved in the analysis of the semi-structured interviews and the researcher/ physiotherapist used critical thinking to ensure her analysis and interpretation of the results and findings were as objective as possible. Reflexivity is discussed further in ‘Reflections on the Study Methodology Used’ (Chapter 7. 6, p.189)
7. 5. 7. The Survey
The cross-sectional survey comprising the Pre and Post-Intervention Physiotherapy Questionnaires was developed but not validated. It was not the remit of this unique study to validate a questionnaire, only to design one that met the research aims of investigating the problem of adhering to physiotherapy and to use the data collected in the Pre-Intervention Physiotherapy Questionnaire to contribute to the design of the SMPP. Collecting data on the total study population provided background information on its characteristics, and by issuing the questionnaire before and after the implementation of the SMPP, any changes that may have occurred could be monitored. The survey was based on the non-validated one designed by Carr et al.
185

(1996) as it was the only one that had been developed in the UK to investigate adherence to physiotherapy in adults with CF at the time of the study. Although this questionnaire had not been validated it was considered to be a valid and reliable data collecting tool for the purpose of this exploratory study.
Summary
As the adult population with CF is growing, is in better health and living longer measurement tools such as longitudinal surveys investigating adherence behaviours need to be developed and validated. Understanding adherence behaviours to physiotherapy, over the range of disease severity and age groups, would enable strategies to be developed to address the issues raised with the aim of bringing about improved adherence to treatment.
Clinical monitoring
The SMPP only recorded the participants’ physiotherapy programme. Incorporating a clinical diary, so that information which was recorded in the physiotherapy and medical notes was shared with the participants, could have acted as feedback to encourage adherence e.g. recording FEV1, sputum (colour, volume, viscosity), cough and exercise tolerance. This approach would have resulted in the participants being better informed of their condition, enabling them to make decisions about modifying their physiotherapy treatment if given parameters e.g. if the FEV1 falls below a certain level to contact the physiotherapist and the CF Team. Potentially it could encourage a more prompt response to clinical deterioration and help address issues such as denial which can result in delayed treatment.
Although available in the physiotherapy and medical notes outcome measurements such as hospital admissions, additional attendance at out-patient clinics and pharmacological changes were not used in the study. Recording these outcome measures for each participant, would have given a more detailed understanding of the impact of the SMPP on adherence behaviours.
The study was limited by the lack of follow up after implementing the SMPP. Contacting each participant by telephone after starting the SMPP and at the three and six month reviews, rather than advising them to contact the researcher/physiotherapist if they had problems, could have acted as a means of re-enforcing adherence behaviour which may have resulted in a more significant improvement in adherence to physiotherapy treatment. A study by Daniels (2010) have commented that
186

telephone contact can promote adherence providing it is not viewed by the participant as intrusive.
QoL
Several QoL measures have ben used (Gee et al., 2000; Henry, 2003; Quittner et al. 2005) in CF but were ‘stand alone’ surveys and were not used as an evaluation tool to measure the impact of an investigation.
The purpose of adhering to physiotherapy is to improve health and well being and as a consequence improve QoL. A QoL measurement was not used as the impact of the SMPP on the ability to improve adherence behaviour had yet to be established and was therefore an unknown variable. The small sample size (n = 49), which would reduce even further by the end of the study, the fact men and women with CF view QoL differently (Congleton, Hodson, & Duncan-Skingle, 1996) and as the disease progresses perceptions of QoL can vary would have resulted in such small numbers in each group that the reliability and validity of the outcomes would have been significantly compromised. The short duration of the study, being six months over the winter period when potentially chest infections are most prevalent, could have meant that an increase in burdensome chest physiotherapy that would reduce the participant’s QoL in the short term thereby making it difficult to extrapolate an overall change in QoL.
187
7. 6. Reflection
7. 6. 1. Reflections on the Study Methodology
The study demonstrated that the use of a mixed methodology of qualitative and quantitative research approaches provided an in-depth understanding of why people with CF vary in their levels of adherence to physiotherapy and the reasons that govern that behaviour. Initially the study used a democratising process-led “Professionalising” action research typology as it sought to involve the study participants in both the change and research processes (Hart & Bond, 1996; Reason & Bradbury, 2001; Waterman et al., 2001) with the aim of bringing about a service improvement. This approach was abandoned in the first part of the action research cycle (Plan) - because the participants could not be involved in the research process to the extent that would be fully compliant with an action research approach. Thereafter the study broadly followed an action research cycle of plan, action/intervention, evaluation and reflection but with the participants having a limited involvement.
Determining rigor and reliability in qualitative research has been a contested area. Broad agreement suggests four major considerations of trustworthiness, reliability, validity and generalisability to be important criteria for establishing the quality of the findings (Holloway & Wheeler, 2010; Pope & Mays, 1995).
Trustworthiness
It has been argued that “trustworthiness” of the quantitative research findings is difficult to achieve since it involves interpretative judgement (Lincoln & Guba, 1985) however it can be enhanced by using mixed research methods (Dewey, 2006). Qualitative research requires flexibility and open mindedness with a systematic and well organised approach to analysis in order to establish its validity. A mixed methodology, using qualitative and quantitative approaches, enabled the study to investigate how a person’s behaviour (qualitative approach) may be influenced by such factors as disease severity measured by their FEV1 (quantitative approach) and the implementation of the SMPP. With the use of different research tools i.e. semi-structured interviews, and a survey with different approaches to analysing the semi-structured interviews (Burnard, 1991) approach and thematic analysis (Braun & Clarke, 2006) the ‘trustworthiness’ of the findings were enhanced through cross verification. Using a mixed methodology provided greater flexibility to the analytical approach and functioned as a means of triangulation as the same phenomenon were examined in different ways and from different perspectives (Holloway & Wheeler,
188

2010). The use of a quantitative research tools (SPSS Windows 10) provided a rigorous structured approach to analysing the data which when used in conjunction with the findings from the qualitative research gave a deeper understanding of the complex issues involved in this area of study. By combining multiple approaches intrinsic biases and problems that come from a single method can be avoided (Dewey, 2006).
Generalisability
Generalisability is difficult to achieve in qualitative research as it focuses on specific instances or cases that are not necessarily representative of other cases or populations (Holloway & Wheeler, 2010). Research findings may only be generalisable once a valid and reliable analysis has been conducted, with a demonstrable audit trail. In this study a clear audit trail in the analysis of the semi-structured interviews was conducted with explanations given where the process was adapted for the purposes of the study. The researcher attempted to achieve some generalisability in order that the findings and conclusions may be applied in similar CF settings and populations. Every Adult CF Specialist Clinic will have a population with its own specific characteristics such as age, disease severity, social circumstances and variations in clinical practice meaning that the results and findings from one study in one clinic may not be replicated in another. However, all Adult CF Specialist Clinics follow the clinical guidelines as recommended by the CF Trust (2001), so the findings and results from this study may be applicable in other CF clinic populations.
Reliability
Reliability is concerned with the degree to which further implementation of a study would yield the same results (Jolley, 2010). To be reliable a measure needs to be repeatable and reproducible. In this predominately qualitative study, with a small study population, it can be said that the study was reliable as it aimed to accurately reflect the views of the participants. This was achieved by using semi-structured interviews where the participants had the opportunity to express in their own words their ‘life world’, their views on physiotherapy, what having CF meant to them, the survey eliciting how effective they considered the SMPP was in optimising their ability to adhere to physiotherapy treatment. The survey, in the form of the Pre and Post-Intervention Physiotherapy Questionnaire, was issued to the total study population thereby giving each participant an equal opportunity to express their views in their own words when answering the open ended questions. The participants were also actively involved in evaluating the SMPP by having their views of its
189

effectiveness being recorded in the Feedback Chart. By using a variety of data collection tools the reliability of the study was enhanced.
Reflexivity
Reflexivity refers to the ability of the researcher to suspend pre-conceived ideas and be open to the data as it is being collected and analysed (Jolley, 2010). In qualitative research this is through critical reflection on what has been thought and undertaken (Holloway & Wheeler, 2010). The dual role of the researcher, who was also the physiotherapist responsible for the physiotherapy service provision to the CF clinic could have potentially resulted in the outcomes being bias, however this was mitigated by the use of critical thinking skills which enabled the researcher/ physiotherapist to detach herself from the data. Critical thinking is a high level intellectual activity that goes beyond the acquisition of knowledge, and is seen as a key skill for all health professionals to master in an age where they are expected to be reflective practitioners and base their practice on sound evidence (Castle, 2009).
The researcher, using these principles was aware of the potential of the patients to feel unduly pressurised into participating in the study. However every effort was made to ensure that this did not happen by giving the potential participant time to consider if they wished to participate or not and assurances that if they declined then it would not affect their care. When collecting information on the Feedback Chart regarding the effectiveness of the SMPP the researcher/physiotherapist remained non-judgemental in order to reduce the risk of biasing the results. In this study, a colleague with research experience and a knowledge of CF, was used to independently review and refine the coding for the analysis of the second set of semi-structured interviews. It gave “fresh” insight into the data and enabled the researcher to distance herself from her pre-conceived ideas, be more objective in her analysis of the findings and be better able to put them into context (Dewey, 2006). The study was evaluated by demonstrating an ability to assess the strengths and weakness of evidence and recognise differences and similarities in data objectively (Castle, 2009) to ensure the validity and reliability of the outcomes.
Validity
A variety of measurement tools were used in the study (semi-structured interviews, a survey in the form of the Pre and Post-Intervention Physiotherapy Questionnaires, FEV1and BMI) to give valid data that was sensitive enough to record any changes that were made as a result of the SMPP and to record the participants’ views in their own
190

words. It was also important to collect valid and reliable data to develop the intervention (the SMPP) and to monitor and evaluate its effectiveness. A survey in the form of the Pre and Post-Intervention Physiotherapy Questionnaires ensured that the total study populations’ characteristics and opinions were sought in order to contribute to the design of the SMPP and to monitor its effectiveness, while the Feedback Chart gave the study participants a further opportunity to evaluate the SMPP.
Meeting the Research Aims
The research questions and study aims are outlined below:
Research Question
Will the SMPP optimise the ability to adhere to physiotherapy treatment in adults with CF?
Research Aims
1. To investigate the problems that people with CF have in adhering to physiotherapy treatment prior to the study
2. To investigate the level of adherence to physiotherapy treatment prior to the study
3. To develop and test the effectiveness of a new SMPP to optimise the ability of adults with CF to adhere to physiotherapy treatment.
4. To evaluate the impact of the new SMPP on adherence to physiotherapy treatment
5. To postulate a new model of clinical practice for the future
physiotherapy treatment for people with CF
In principal the study met the research aims, with limitations and areas for further research identified. The study established the level of adherence to physiotherapy treatment prior to the start of the study as measured by the criteria set by the researcher/physiotherapist, it set about critically evaluating the results and findings regarding the problems encountered by people with CF in adhering to physiotherapy treatment, developed and tested an educational strategy i.e. the SMPP, evaluated its effectiveness, contributed to new knowledge of physiotherapy treatment and developed a new model of clinical practice for the future physiotherapy treatment for people with CF. The study met the research aims of establishing whether the SMPP optimised the ability to adhere to physiotherapy treatment as the results demonstrated
191

a trend towards increased adherence, which was supported by the predominantly positive comments of the participants in the Feedback Chart and the Post-Intervention Physiotherapy Questionnaire. The trend was not statistically significant but was of clinical importance.
7. 6. 2. Reflections on the Professional Doctorate
Reflection is a learning process designed to gain insight into one’s own practice with the intention of improving it (Parahoo, 2006). The purpose of reflection in this study was to use the experiences and knowledge gained in the research process to improve physiotherapy professional practice.
This exploratory study formed part of my Continuing Professional Development (CPD) programme and provided an opportunity for reflection which enabled me to set about improving and developing my clinical practice. The study provided a direct link between theory and clinical practice and is an example of the work of Benner (1984), where the accumulation of experience and knowledge contributes to the development of the novice being able to progress to being an expert. It was through my clinical experience of treating people with CF that the problems involved in adhering physiotherapy treatment were observed and used as the basis for this research study. This unique study provided a stimulating workplace environment and is an example of the researcher/practitioner in action. The study formed part of the developing process of professionalisation, fulfilled the principles of the Professional Doctorate (PD) and provided an opportunity to critically appraise my own professional role in CF.
Conducting research into my physiotherapy clinical practice provided valuable insights into how people with CF perceive their disease, and the difficulties they experienced in adhering to physiotherapy treatment, as well as contributing new knowledge to physiotherapy practice. These insights contributed to the development of a new model of clinical practice, improved my professional judgement and expertise and enabled me to be recognised as an expert practitioner.
I initially considered a career as a consultant physiotherapist in CF but because of the financial constraints in the NHS such posts did not materialise. My career has consequently focused on being a senior manager. Currently the NHS is developing and encouraging service line management where senior clinicians also work as senior managers. A PD would be an ideal qualification for a career in this form of senior management.
192

I was very pleased to be awarded four national scholarships
British Thoracic Society British Lung Foundation Chartered Society of Physiotherapy – Educational Award Chartered Society of Physiotherapy – Research Scholarship
I have been very encouraged to have been awarded these national scholarships for my research work, particularly as it appeared that it was the first time the British Lung Foundation had given such an award to a physiotherapist. These scholarships were supplemented by sponsorship from pharmaceutical companies which contributed to my fees.
7. 6. 3. Evaluation of Learning
Evaluation seeks to assess the value or worth of something (Robson, 2006) which in this instance is the effectiveness and appropriateness of the PD course. A PD provided an ideal opportunity to improve my clinical practice by undertaking a substantial research project which incorporated critical reflection. Critical reflection is an integral part of a health professional’s CPD. It is a window (Taylor & White, 2000) through which to view and systematically track changes in practice issues in order to arrive at new insights to improve and change practice.
By undertaking a PD it has been possible to develop the study by completing the assignments in Part 1 of the course. Each assignment enabled the study to be progressed in a logical manner and to be robustly evaluated. The work for the assignments was based on my clinical practice and formed part of the research project. The first assignment was Professional Development which enabled me to set learning objectives for my course. In the second assignment Publication and Dissemination Unit my work had already been evaluated by peer review as the literature review for this research project had already been published in the Physiotherapy Journal. The third assignment, Advanced Research Techniques, enabled the skills and knowledge I had acquired to be utilised by contributing to the development of the research methodology and data collection methods. Passing the assignments, by means of systematic evaluation, enabled the study to be developed. in a robust and rigorous manner.
The undertaking of this small, unique clinically-based exploratory study enabled the problems of adhering to physiotherapy to be identified, an intervention to be developed to resolve them, the effectiveness of that intervention to be evaluated and a
193

new and improved model of clinical practice to be postulated. The study also contributed new knowledge about the problems people with CF experience with adherence to physiotherapy and closed the gap between theory and clinical practice.
7. 6. 4. Legacy & Professional Role
This new model of clinical practice will enhance the knowledge base of physiotherapy and encourage further research into the potential of SMPPs. By optimising adherence to physiotherapy treatment scarce physiotherapy resources can be utilised more effectively, if people with CF who have non-adherent and partially adherent behaviours can be identified then educational strategies developed to address them.
The development of a new model of clinical practice complies with the CSP (2010) vision of clinical excellence and the government’s policy on clinical governance (DoH, 2006a) both of which encourage high standards of evidence-based clinical practice to improve health care outcomes and service delivery. The CSP actively encourages research as part of the developing process of professionlisation (CSP, 2010) and it also validates the clinical practice of its members. This is a worked based clinical study, involving complex issues in a specialist field where research directly informed clinical practice.
194