thinking ahead: conversations across california report
TRANSCRIPT
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 1
Final Report

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 2
September 2015
Authors
Mark Starford
Charlene Jones
The Board Resource Center is the primary entity for facilitating focus groups,
collecting, reviewing, and reporting outcomes related to
Thinking Ahead: Conversations across California.
Since 1994, BRC activities have addressed education and training needs that
foster leadership, self-determination, and community inclusion. Our focus
areas include person-centered strategies and multi-media plain language
products that aim to increase informed decision-making and engagement in
public policy making.
BRC strives to make our products available to the public and accessible to a
variety of audiences. If you have any comments about this or any other BRC
project or report, email us at [email protected].
BRC’s products are available online: www.brcenter.org
Please direct comments to:
Board Resource Center
Thinking Ahead: Conversations across California
Post Office Box 601477
Sacramento, CA 95860
This report, videos and additional resources can be found online at:
http://you-determine.org
© 2015 Board Resource Center. Sacramento, CA 95860

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 3
Table of Contents
Summary ................................................................................ 4
Personal Story ........................................................................ 5
Purpose .................................................................................. 7
Background ........................................................................... 9
Method ................................................................................ 12
Findings ................................................................................ 15
Recommendations ............................................................. 19
Discoveries ........................................................................... 21
Next Steps ............................................................................ 22
Discussion ............................................................................. 25
Challenges .......................................................................... 27
Acknowledgements ........................................................... 28
End Notes ............................................................................. 29

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 4
Summary
Health literacy surveys reveal only 12 percent of adults have proficient
skills necessary to maintain health, prevent disease, and use the U.S.
health care system. Nearly 9 out of 10 adults may lack the ability to
manage their health and make informed decisions. Moreover,
information in health-care systems is often challenging, especially when faced
during stressful circumstances or at the end of life.
“Thinking Ahead - Conversations across California” is an undertaking to gain
insight into use of end-of-life advance planning user-centered information and
communication formats. BRC’s method of inquiry was a series of learning focus
groups comprised of representatives from five California cities. Representatives
from the palliative care and advocacy communities were also involved as
advisors to guide the project.
BRC identified, with the support of community organizations, participants for the
groups. These included assisted living residents and providers, users and
providers of in-home supports, hospice and health care services, family
members, and advocates within the disability and senior communities.
Participants provided insight about their understanding of end-of-life advance
planning, and made recommendations for user-friendly information and
communication approaches.
What became clear early on were prominent apprehensions; individuals were
worried about not having choices or being denied the basic right to decision
making at the end of their lives. There was also confusion about end-of-life
treatments, the authority of advance planning documents and the
responsibility of healthcare agents. Most important, participants expressed
concerns that their preferences not be ignored.
Findings from this inquiry illustrate a call for consumer-centered informational
tools and comprehensive strategies that include both accessible information
and new communication approaches.
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 5
A Personal Story
Paramedics rushed an 85 year-old woman to the hospital.
Years earlier in healthier days, she had completed an Advance
Directive, identifying her end-of-life treatment preferences and
healthcare agent. She did not want heroic efforts to prolong her life.
She did not want to be resuscitated. Most important, family and
friends knew her preferences.
Then it happened, the unforeseen.
After getting out of bed one night - to get a glass of water - she took a
tumble. She lay on the floor in a semi-conscious state until a family
member discovered her the next morning. After being admitted to an
Intensive Care Unit, doctors investigated her condition. A series of tests
revealed the problem. Doctors diagnosed sepsis, a life-threatening
condition that can lead to organ failure and death (killing more than
258,000 people each year).
A hospital physician recommended an endoscopy for further evaluation,
but the procedure carried risks and required the family to make decisions.
Members of the ICU care staff approached the patient’s health care
agent, her daughter, and asked that she complete a form authorizing the
surgery. The authorization included questions pertaining to treatment
choices, in the event the procedure resulted in unintended outcomes.
The patient, awake and lucid, was excluded from these conversations;
excluded from participating in decisions impacting her care and end-of-
life treatment.
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 6
Not ready to see her mother die, the health care agent ignored her
mother’s expressed end-of-life choices as identified in her Advance
Directive. She directed the hospital to employ every measure to keep her
mother alive. The patient was simply told by family members that
“everything will be okay.”
Immediately after the endoscopy, while still in the operating room, the
patient suffered a heart attack and multiple strokes. She was left
extremely weakened, blind and paralyzed on one side of her body. By
the time the patient returned to the ICU, she was intubated and
dependent on a respirator to breathe. The health care agent approved
subsequent medical interventions, and ignored the patient’s preference
for pain medications for relief.
For 16 long days, the patient’s life was sustained with only an occasional
and marginal reprieve from pain. Finally, after more than two weeks of
suffering, she succumbed.
End-of-life Care in California “You don’t always get what you want.
“Why Doctors Fail”
BBC Audio recording with Atul Gawande, MD 2014
“Despite having an advance directive,
things can go wrong.” Participant
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 7
Purpose
Over the past decade, the need to effectively address health literacy
increasingly points to accessible, functional health information.1 A recent
review of health literacy interventions, revealed people with limited literacy
have less health knowledge and comprehension of health information, have
higher rates of hospitalization and emergency care, and for seniors is
associated with poorer health status and quality of life.2
The purpose of “Thinking Ahead: Conversations across California” was to
engage representative partners across the community, both service
providers and consumers, to learn from them about self-determination at
the end of life. Most particularly, the project sought to gather information
about barriers to understanding life sustaining treatment options, and the
use of end-of-life planning tools for decision making, as well as
recommendations regarding development of related “user-friendly”
media to better serve patients and consumers.
Surveys reveal most Californians would choose a natural death at home.
However, few discuss these issues or document their preferences, leaving
their loved ones unsure. While 82 percent indicate that it is important to
put wishes in writing, less than one quarter have actually done so. Nearly 8
in 10 Californians say that if seriously ill, they would want to speak with their
doctor about end-of-life care, but fewer than 1 in 10 reports having done
so. In addition, more than half report they have not talked with a loved
one about the kind of care they want at the end of life.3
“I want to have a voice in deciding what the last few weeks of my life will
be like. And, I want my wishes to be honored.” Participant

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 8
While commendable in purpose, end-of-life planning materials may not
address the reading or utilization needs of individuals, their families and
support providers with health literacy limitations. Inclusive planning includes
tools useful to a wide range of patients to facilitate informed decision
making and minimize the need to decode their preferences.
BRC planned to learn from diverse patient or consumer audiences about
their experiences with end-of-life planning materials and media. It included
asking for specific recommendations about how tools may be improved to
assist wider engagement in end-of-life planning. Additional outcomes
included discovering what has worked for participants to gain greater self-
determination and recommendations to advance this area of health
literacy.
As a descriptive inquiry, BRC did not intend that findings be used to
generalize to larger groups but serve as a discussion and point to future
research, practice and policy. With this comes a challenge to many
stakeholders - governments, health management organizations, medical
professionals and care providers.4
“It’s Very Hard to Come to the Realization That You’re Dying.”

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 9
Background
Literacy
The National Adult Literacy Survey in 1993 and 20035 reported millions of
adults are functioning with less than basic skills. Defined simply as "not
having adequate reading skills for daily life”. On a practical level, they are
not able to:
Read stories to their children, a newspaper article or map
Read correspondence from a bank or government agency
Fill out job applications or compete effectively for work
Of significant consequence is health literacy, affecting not only a person’s
ability to understand diseases and disorders, and follow prescription
instructions, but to learn about insurance options, complete a coverage
application and make informed decisions about treatment choices.6

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 10
Health literacy
The American Medical Association defined health literacy as the
"constellation of skills, including the ability to perform basic reading and
numerical tasks required to manage a health care environment," and
included everyday functions such as the "ability to read and comprehend
prescription bottles and essential health related materials".7
Health literacy is complex. It is shaped by public health and socio-cultural
forces and reflects how well people understand information, can access
and utilize services in daily life. It is defined as “...the degree to which
individuals have the capacity to obtain, process, and understand basic
health information and services needed to make appropriate health
decisions.8
Health literacy surveys revealed only twelve percent of adults have
proficient skills, the level necessary to maintain health, prevent disease,
and use the U.S. health care system.
Nearly 9 out of 10 adults may lack skills needed to manage their health
and prevent disease. About twenty two percent had only basic literacy
and fourteen percent below basic health literacy. These adults were more
likely to report their health as poor9. The inability to properly care for
oneself and lack of planning and prevention can result in increased
emergency care, treatment and support services, with costs
overwhelming service systems.
"If we want health equity, we need to make health literacy a priority.”
Sylvia Mathews Burwell, Secretary of Health & Human Services
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 11
Plain Language and User-Friendly Design
Many factors such as education, language, age and cognitive ability,
can affect health literacy. The design, production and communication
can determine the impact and usability to the widest population.11
With emphasis on intended users and formative research, these and other
approaches provide insight necessary to the organization and content that
is essential for actionable information. Improving health literacy requires
comprehensive strategies; plain language, user-centered communication
that can be understood and used by targeted audiences.
It can be the poorly designed handout, booklet or website that contributes
to the inaccessibility of information, more so than the skill or experience of
the user.
Several features that make health information difficult:
• Language used in the health-care system is challenging and unfamiliar.
• Knowledge of health and illness is typically acquired from personal
experience, social conversations
• Understanding informational media, including the Internet is difficult
when a person is worried about their own condition.
• Health information is highly personal.
• Understanding and trusting the information is critical.10
“It’s very important to consider your content from your user’s perspective.
Is it written so that your target audience will understand and relate to it?”
Content Strategy for the Web

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 12
Methods
Consumer engagement is essential for success with all models of care
delivery. Ensuring the presence of active end-user voices is especially
important for populations with specialized needs - such as individuals with
low literacy skills, seniors and people with disabilities.
The formative approach that BRC uses underpins its person-centered
focus and leads to outcomes shaped by needs and preferences of target
audiences. It is aimed to guide the development or adaptation of
programs and tools and help improve activities or outcomes.
BRC’s work also emphasizes a “plain language” practice that leads to
accessible and functional information that assists end users and
stakeholders to support and exercise informed decision making.12
Focus Learning Groups
Discussion is a mechanism for learning. A well-
facilitated discussion allows participants to explore
new ideas while supplying information or
perspectives.13
BRC, with the support of local organizations,
identified audiences of end users for “focused
learning” groups from five California cities -
Sacramento, Paradise (Chico), San Francisco,
Santa Barbara, and Clovis (Fresno).
These groups included assisted living providers and residents, users and
providers of in-home supports, users and providers of hospice and health
care services, family members, as well as disability and senior advocates.
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 13
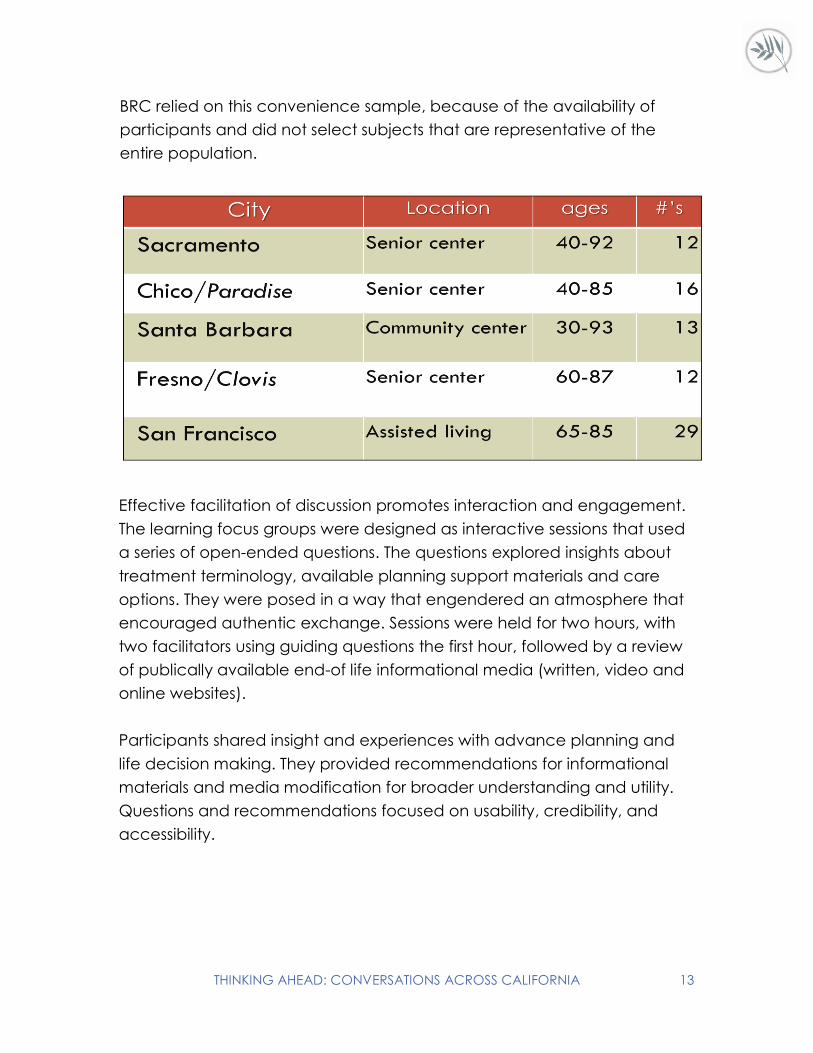
BRC relied on this convenience sample, because of the availability of
participants and did not select subjects that are representative of the
entire population.
Effective facilitation of discussion promotes interaction and engagement.
The learning focus groups were designed as interactive sessions that used
a series of open-ended questions. The questions explored insights about
treatment terminology, available planning support materials and care
options. They were posed in a way that engendered an atmosphere that
encouraged authentic exchange. Sessions were held for two hours, with
two facilitators using guiding questions the first hour, followed by a review
of publically available end-of life informational media (written, video and
online websites).
Participants shared insight and experiences with advance planning and
life decision making. They provided recommendations for informational
materials and media modification for broader understanding and utility.
Questions and recommendations focused on usability, credibility, and
accessibility.

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 14
Learning Focus Group Participants
Advisory Team
BRC established an advisory team with healthcare service delivery
professionals, end-of-life treatment planning and training consultants, and
persons with disabilities. Under their guidance, BRC collected end-of-life
planning data and tools in current use, reviewed literature, and identified
learning focus group participants.
With assistance from the advisory team project findings and
recommendations will be shared with consumers, service providers and
stakeholder organizations.
Thinking Ahead: My Way, My Life, My Choice at the End, 2007, developed by BRC for CA Department of Developmental Services and Coalition for Compassionate Care of California.
Plain language, graphic design and videos assist persons with disabilities to complete advance directives.
CDC
Information and tools to improve health literacy and communication with
people about health. National Institutes of Health
Health Literacy
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 15
Findings
BRC gathered data and specific recommendations about approach,
design and content of information that facilitates health literacy, as well as
the emotional dimensions of self-determination at end of life. Findings
describe information collected and do not lead to conclusions regarding
relationships or larger groups. Themes to significant concerns expressed by
group participants were organized. Answers to the question series were
summarized and recommendations regarding improved communication
approaches and informational media were listed.
Of significant interest from all participants was the need for more
information and opportunities to have conversations about end-of-life and
personal choices. As important, they emphasized the value of being heard
as they speak for themselves about medical care at the end-of-life.
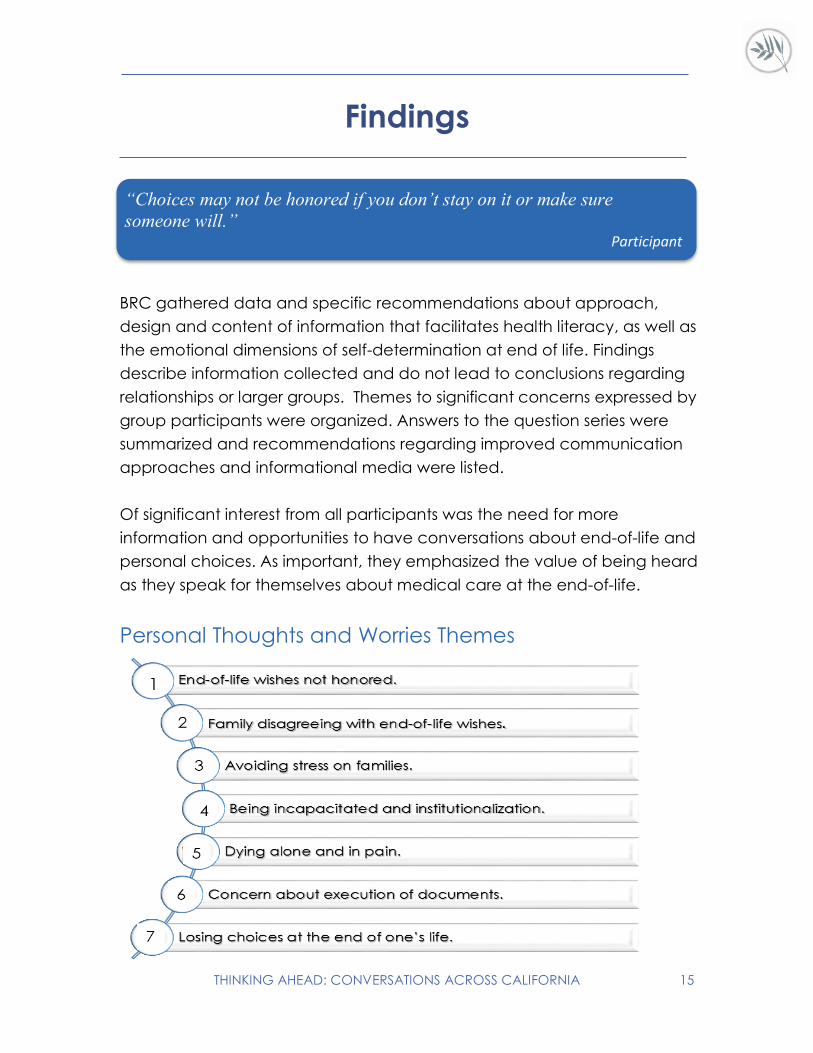
Personal Thoughts and Worries Themes
“Choices may not be honored if you don’t stay on it or make sure
someone will.” Participant

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 16
Level of Understanding Advance Planning Terminology
Physician Orders for Life Sustaining Treatment (POLST)
Less than thirty percent in each group indicated they had heard of
POLST. Only two participants in total shared a more complete
explanation of its purpose, most knew nothing or were unsure. Less
than ten participants reported that they had spoken with their
doctors about POLST. Primarily, there was uncertainty about when POLST comes
into play and which document supersedes others.
Advance Directive
More than seventy percent in all but one group indicated they had
completed some form of an Advance Directive. Fewer reported
sharing their wishes with loved ones, and less than ten in total had
conversations with their doctors.
More than half understood an Advance Directive’s health care agent as
legally required to follow expressed choices.
Others shared, from experience, that health care agents may not always follow
choices because other factors may interfere or prevail (i.e., hospitals, family
members, or agent making decisions different from those written).
Hospice
All participants indicated basic knowledge of hospice as end-of-life
comfort care and support. More than twenty percent had questions
that reflected myths about hospice such as, time limits on services,
and medications. More than fifty percent did not know under what
circumstances and where it may be provided and who covers the cost.
About half indicated being familiar with the term “palliative care” as treating a
patient’s pain but questioned how it differs from hospice.

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 17
Do Not Resusitate (DNR)
Nearly all participants were familiar with the term “do not resuscitate”
but more than fifty percent were unclear about the circumstances
for use and/or who would follow the orders.
Primary concern was how to inform EMTs or others about a DNR and whether
one can change a DNR at another time.
Cardiopulmonary Resuscitation (CPR)
All participants were familiar with the term but several had questions
about different methods used and under what circumstances it is
used (i.e., in hospitals, on the street, if there is a DNR in place).
More than half in each group were concerned about the physical method and
had heard there might be a danger, but did not know more.
Experience with End-of-Life Planning Tools and Care
The majority of participants indicated they had completed an advance
directive. As mentioned above, very few reported sharing their wishes with
loved ones, other than the identified health care agent.
As group conversations progressed, some participants expressed deep
concerns about their health care agent following prescribed end-of-life
wishes. All felt they needed to communicate their preferences, not only to
their agent, but to friends and family members to better assure choices
would be honored.
Many participants in each group reported that they had assisted a family
member or friend with end of their life decision making, while expressing
they had limited understanding, themselves.
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 18
Noteworthy comments and concerns
• Disagreeing with family members or doctors is very challenging.
• There is reluctance addressing the subject with family.
• Advance directives can be ignored if hospitals do not prioritize
reviewing directives before treatments.
• Doctors may not check the medical chart for advance directives.
• Assisting someone with end-of-life choices and care is an honor and
privilege.
“University of California” Prepare for Your Care
“University of Tennessee” Hello, May I Help You Plan Your Final Months?
“Video Caregiving” Advance Directives Planning Ahead-Advance Medical Directives
“Conversation Project”
“Improving Quality and Honoring Individual Preferences Near the End of Life”
Institute of Medicine
“There are two overriding goals for advance care planning: establishing a
surrogate decision-maker, which is a legal activity and expressing your
values, treatment goals and wishes, a communications task.”
Charles Sabatino, Director Commission on Law and Aging American Bar Association
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 19
Recommendations
Beginning the Conversation
Start the conversation with family early, don’t wait.
Provide consumers with tips about how to start
conversations with families.
Create opportunities to talk with personal physician.
Ensure physicians use everyday language.
Come prepared with questions and ask for clarification (as many times
as needed).
Health care providers and social service organizations need to arrange
opportunities for peer to peer end-of-life care discussions.
Written Materials
Simple design invites a reader.
Large font with a lot of white space
Graphics that help explain the text.
Photos of everyday people
Single subject short booklets.
Information presented in short segments, limit text.
Provide clear directions or action steps.
Simple headings, with bullet points.
Plain concise language, authoritative but everyday language.
Specific topics requested:
Health care agent’s responsibility.
Purpose of each document and when to use.
Explanation of treatment options.
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 20
Videos/Websites
• Invites the user, not somber.
Provide tips for conversations.
Questions to ask medical providers.
• Introduces topics and presents everyday examples.
Provides short stories, help to see selves in situations.
Uses clear understandable language with short messages.
Emphasizes importance of planning, choosing a trusted health care agent.
All decisions are personal, personal preferences are to be honored.
Has easy access to web resources, for self and to show family members.
Consider younger audiences, what will attract them.
Best Way to Learn
• In a comfortable support group with peers.
• With people close to you.
• Meetings with doctors or healthcare social worker.
• Brochures produced in plain language.
• Through the Internet.
• Small groups at senior centers, residences, or service groups.
With family, but after learning about the topic.

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 21
Discoveries
Confusion about differing authorities of POLST, Advance Directives,
powers of attorney.
Advance Directives may not be followed, if doctor and/or family is
unaware of document, or health care agent is unavailable to
advocate.
Choosing a health care agent requires very careful consideration.
Advance planning requires careful consideration and time to learn
about options and what they mean.
Assure family, friends, health care agent understand importance of
honoring preferences.
Advance Directives need regular review to see that health care agent
is available and personal choices are clear or changed if necessary.
Preparation can relieve the burden on everyone: family, friends, and
providers.
People want to be involved in all elements of producing end-of-life
planning materials, videos and websites.
“Information needs to be in attractive and easy to understand, with real
life examples that people can relate to.” Participant
“A Guide about how to deliver actionable and engaging health
information” www.health.gov/healthliteracyonline
“A one-stop source for government web designers to learn how to
make websites more usable, useful, and accessible”
www.usability.gov
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 22
Next Steps
Practice
Research has not yet provided explanations as to how advance planning
can facilitate informed decision-making and adherence to end-of-life
treatment preferences. This small descriptive inquiry also revealed themes
that speak to the need for further research, particularly regarding models
of communication and tools that facilitate conversations and planning.
This exploration does not seek to apply findings to the general population.
It does encourage a respectful approach to end-of-life conversations in
which consumers are supported to exercise their right to adequate
information and personal decision making.
Because medical treatment options can be difficult to understand or
imagine, increasing the opportunity to learn is key. Planning tools, most
commonly Advance Directives, Powers of Attorney for Health Care,
POLST, and DNR orders are perplexing in how or when they direct care.
Most importantly, designated health care agents play a central role in
patient advocacy, but how does one assure that a person is up to the
task? He or she may not be effective in supporting the patient’s wishes.15
With efforts to improve health literacy and self-determination at the end of
life, stakeholders must address concerns expressed by looking to improved
models of learning and application.
“Present your planning or wishes for end-of-life care as a “gift” to
family and friends, after decisions are made.” Participant

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 23
According to the Centers for Disease Control and Prevention, 16 two
decades of research indicate that health information is presented in ways
that are not understandable by most Americans.
If health professionals want to reach people, they must ensure
information, products, and services are accessible and understandable.
Information must be:
1. Accurate: Not “dumbed-down” but presented in ways people can
understand.
2. Accessible: Easy to scan, large font, sub-heads, bullets, images and
graphics that match content with captions across media platforms.
3. Actionable: Gives suggestions so information is useful to doing
something.
Healthcare Partners must:
1. Engage patients or consumers with all content - make it personal, less
formidable.
2. Motivate with suggestions, tips on taking first steps to difficult
conversations, and planning in advance so personal choices are
understood by others.
3. Help access and adapt informational content using multi-media tools,
especially the Internet, for wider utility by stakeholders.
4. Emphasize plain language design, including personal stories.
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 24
Policy
Research points to collective evidence that health organizations and
support service providers must consider programmatic and financial
factors that can improve health literacy. Most significantly, twenty percent
of the U.S. population will be 65 or older by 2050.17
As so many approach the end of their years and decision making related
to treatment and care, the following issues will need to be considered:
Health information is not understandable by most Americans.
Adjust the “more is always better” treatment approach and focus on
the values of the patient.
• Create programs specific to needs of cultures and communities.
• Ensure programs are acceptable and feasible before launching
Recognizing the enormous communication challenges facing today’s
public service and health professionals, research on media design that is
truly user-friendly has to be the guiding force to development of
functional information tools.14
As specified by the Center for Plain Language, to be successful, the
intended audience must be able to find what it needs, understand, and
utilize. Materials produced in clear and open styles, with simple navigation
of information can satisfy most users.
However, much more needs to be done, not only with thoughtful
consumer-centered products but approaches to health literacy that
facilitate learning and application.

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 25
Discussion
Board Resource Center initially approached this inquiry prepared with
facts and implications about low literacy, particularly as it relates to health
and informed decision making. The project was intended to expand upon
BRC’s earlier work “Thinking Ahead, My Way, My Choice at the End,” a
plain language planning tool and advance directive. It was targeted at
the needs of persons with cognitive limitations and their service providers.
“Thinking Ahead across California” sought to learn from a broader
audience about informational formats that could be modified or created
for a wider range of users for end-of-life planning and decision making.
More prominent concerns, however, emerged from focus groups with
individuals who had experience with end-of-life decision making for
themselves and others. While suggestions for modifying written materials
and website content were collected, the need for facilitated
conversations to address several end-of-life topics was heard in all groups.
These centered round the need for fuller understanding of end-of-life
treatment options and situations in which these are used. Even more
significant, were worries about health care agents and personal choices
not being honored. In addition, firsthand experience with Advance
Directives did not ameliorate confusion about the authority of end-of-life
planning tools (i.e., Advance Directive, POLST, and Power of Attorney for
HealthCare) and which would prevail under what circumstances.
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 26
What became clear is the injurious consequence to self-determination
when there is confusion about end-of-life treatments, advance planning
documents and healthcare agent obligations. Expressions of preferences
were or could be misunderstood or ignored by family members, health
care agents and especially medical providers. Participants worried
deeply about “not having choices,” or being denied the basic human
right to decision making, even at the end.
These discoveries shift sights not only to the need for more research into
efficacy of tools and communication approaches but to the need for
advocacy. Calls for vigorous public health education regarding end-of life
conversations, care, treatment and decision-making are key.
If self-determination at the end of life is to be planned and promised, patients
and consumers must have opportunities to exercise basic rights to actionable
information and decision making.
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 27
Challenges
There were no project-related adverse events. The biggest
limitation was in identifying interested agency hosts. We
experienced a lack of interest from community organizations.
The general attitude was that they preferred not to arrange
meetings to discuss end-of-life planning. Once locations and
host organizations were secured, representatives and staff were eager to
use resources to promote the learning groups.
Specific barriers included:
Community service agencies appeared to reflect generally held views
that end-of-life conversations are difficult and avoided the topic.
Length of time with groups did not allow for as much exploration as
hoped for.
Groups that were smaller provided greater opportunities for discussion
and recommendations.
More questions, both open and close ended, in written form would
have provided greater detail to augment findings.
Hosts (three out of five) had limited ability to advertise meetings.
A few hosts had limited or no access to the internet.
BRC pursued a descriptive approach to the inquiry. Drawbacks to
using small sample include:
Results that may have systemic bias
Limitations in generalizing about larger populations.
Readers are advised not to draw causal inferences based on the
results presented.

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 28
Acknowledgments
We extend our appreciation to the many individuals who contributed time
and expertise to this project. Special thanks to the SCILS Group for
providing the funding to conduct the focus groups and video report. We
acknowledge the following people for their assistance:
Advisors
Amy Tucci, CEO
Hospice Foundation of America
LeAnn Kingsbury, MPA
Judy Thomas, JD
Coalition for Compassionate Care of California
Brian Marsh, MBA, MPH
Sutter Health
Molly Kennedy, MPA
Disability Advisor
Host Agencies
E.M. Hart Senior Center
Education and Activity Center
Sacramento, CA
Clovis Senior Activity Center
Education and Activity Center
Clovis, CA
Paradise Ridge Senior Center
Senior Community Center
Paradise, CA
Santa Barbara Village
Senior Community Center
Santa Barbara, CA
Martin Luther Tower
Senior Care Services
San Francisco, CA
THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 29
End Notes
1 S.A. Somers and R. Mahadevan (2010) “Health Literacy Implications of the
Affordable Care Act.” Center for Health Care Strategies, Inc.
2 N. D. Berkman, S.L. Sheridan, K.E. Donahue, D.J. Halpern, A. Viera, K. Crotty, A.
Holland, M. Brasure, K.N. Lohr, E. Harden, E. Tant, I. Wallace, M. Viswanathan M.
(2011). “Health Literacy Interventions and Outcomes: An Updated Systematic
Review.”
3 California Health Care Foundation (2012). Final Chapter: Californians' Attitudes
and Experiences with Death and Dying.
4 L. Nielsen-Bohlman, A.M. Panzer, D.A. Kindig, eds.(2004). Health Literacy: A
Prescription to End Confusion.
5 U.S. Dept. of Education National Center for Education Statistics. (1993, 2003).
National Assessment of Adult Literacy. A First Look at the Literacy of America’s
Adults in the 21st Century
6 I.S. Kirsch, A. Jungeblut, L. Jenkins, A. Kolstad (1993). Adult Literacy in America:
A First Look at the Results of the National Adult Literacy Survey. U.S. Department
of Education National Center for Education Statistics.
7 American Medical Association (1999). “Health literacy: Report of the Council
on Scientific Affairs.” Journal of the American Medical Association, 281(6),
552– 557.
8 S.C. Ratzan, R.M. Parker (2000). “Introduction.” In National Library of Medicine
Current Bibliographies in Medicine: Health Literacy. Pub. No. CBM 2000-1.
9 U.S. Department of Education National Center for Education Statistics (2006).
The Health Literacy of America's Adults: Results from the 2003 National
Assessment of Adult Literacy. (1993, 2003). National Assessment of Adult
Literacy.
10 CommunicateHealth (2013). Green Paper When It Comes to Health
Information Plain Language Is Not Enough.

THINKING AHEAD: CONVERSATIONS ACROSS CALIFORNIA 30
11 J.Kimble (2002). “The Elements of Plain Language.” Michigan Bar Journal,
81:44-45. U.S. Dept. of Education National Center for Education Statistics.
12 Plain Language Commission (2010). Tips on Writing Plain English.
13 Brown University, the Sheridan Center for Teaching & Learning Tips.
Facilitating Effective Group Discussions:
14 Schriver, K. (1997). Dynamics in Document Design Creating Texts for Readers.
New York: Wiley Computer Publishing.
15 J. M. Teno, M.Stevens, S. Spernak, J. Lynne (1998). “Role of Written Advance
Directives in Decision Making Insights from Qualitative and Quantitative Data.”
Journal of General Internal Medicine, 13(7): 439–446.
16 U.S. Department of Health and Human Services Office of Disease Prevention
and Health Promotion. Quick Guide to Health Literacy Strategies.
17 U.S. Census Bureau, (May 2010) The Next Four Decade The Older Population in
the United States: 2010-2050. U.S. Department of Commerce Economics and
Statistics Administration.