thyriod gland imaging part 1 (radiological anatomy differential diagnosis developmental disease) dr...
TRANSCRIPT

بسم هللا الرحمن الرحيم
Dr Ahmed Esawy

Dr. Ahmed Eisawy
MBBS M.Sc MD
Dr Ahmed Esawy

FULL STORY OF
THYRIOD IMAGING (US.CT.MRI.NUCLEAR)
GIOTRE HYPERTHYRIODISM
(HYPERTHYROXINEMIA) HYPOTHYRIODISM
Dr Ahmed Esawy
CONTENTS 1-Normal thyriod gland imaging 2-pathology 3-differential diagnosis 4-developmental thyriod gland disease 5-diffuse thyriod gland disease (hyperthyriodism/hypothyriodism) 6-benign mass /nodule 7-malignant mass /nodule 8-TIRAD 9-nuclear thyriod gland imaging
Dr Ahmed Esawy

1-Normal thyriod gland imaging
Dr Ahmed Esawy

THE THYROID GLAND
OVER TRACHEA
TWO LARGE LATERAL LOBES CONNECTED BY AN
ISTHMUS
15 to 20 g
FUNCTIONAL UNIT IS THE FOLLICLE: EPITHELIAL
CELLS AROUND A HOLLOW VESSICLE FILLED WITH
THYROGLOBULIN
Dr Ahmed Esawy


Transverse US scan of normal thyroid/neck
Dr Ahmed Esawy

SONOGRAPHICALLY DIVIDED INTO THREE SEGMENTS UPPER ,MIDDLE ,LOWER THIRDS
Dr Ahmed Esawy

NORMAL THYROID GLAND THE NORMAL THYROID HAS THIS “GROUND GLASS” APPEARANCE. IT IS
BORDERED ANTERIORLY BY THE STRAP MUSCLES (SM), LATERALLY BY THE
CAROTID ARTERY (C), INTERNAL JUGULAR VEIN (J), AND STERNOCLEIDOMASTOID
MUSCLE (SCM). THE LONGUS COLI MUSCLE (LC) LIES POSTERIORLY. THE
ESOPHAGUS (E) PROTRUDES ON THE LEFT.
RIGHT LEFT
SM SM
SCM
SCM
TRACHEA
E LC
LC
C
C
J
Dr Ahmed Esawy

Normal Anatomy
Dr Ahmed Esawy

Normal Anatomy
Dr Ahmed Esawy

Normal Thyroid
Adult Thyroid
40-60 mm long
13-18 mm AP
Isthmus 4-6 mm AP
Newborn: 18-20
mm long; 8-9 mm
AP
Age 1: 25 mm
long; 12-15 mm AP
Dr Ahmed Esawy

Longitudinal US scan of normal thyroid/neck
Dr Ahmed Esawy

Normal thyroid gland: US
Dr Ahmed Esawy

Normal echo-pattern
Dr Ahmed Esawy

Normal thyroid gland : US
Dr Ahmed Esawy

Normal thyroid gland and thyroid mass. A, Enhanced axial neck CT at the level of the thyroid gland. Note the normal right and left lobes of the thyroid gland (L) and the isthmus (arrows).
Dr Ahmed Esawy

Normal thyroid gland. Unenhanced CT images through the upper portion (A), midportion (B), and lower portion (C) of the thyroid gland demonstrate the two lobes of the gland (black arrowheads) as structures of relatively high attenuation value adjacent to the trachea (T). The thyroid isthmus (white arrowhead) connects the right and left lobes. C, common carotid artery; J, internal jugular vein; E, esophagus; arrows, longus colli muscles.
Dr Ahmed Esawy

Normal thyroid gland. Unenhanced CT images through the upper portion (A), midportion (B), and lower portion (C) of the thyroid gland demonstrate the two lobes of the gland (black arrowheads) as structures of relatively high attenuation value adjacent to the trachea (T). The thyroid isthmus (white arrowhead) connects the right and left lobes. C, common carotid artery; J, internal jugular vein; E, esophagus; arrows, longus colli muscles.
Dr Ahmed Esawy

Normal thyroid gland. Unenhanced CT images through the upper portion (A), midportion (B), and lower portion (C) of the thyroid gland demonstrate the two lobes of the gland (black arrowheads) as structures of relatively high attenuation value adjacent to the trachea (T). The thyroid isthmus (white arrowhead) connects the right and left lobes. C, common carotid artery; J, internal jugular vein; E, esophagus; arrows, longus colli muscles.
Dr Ahmed Esawy
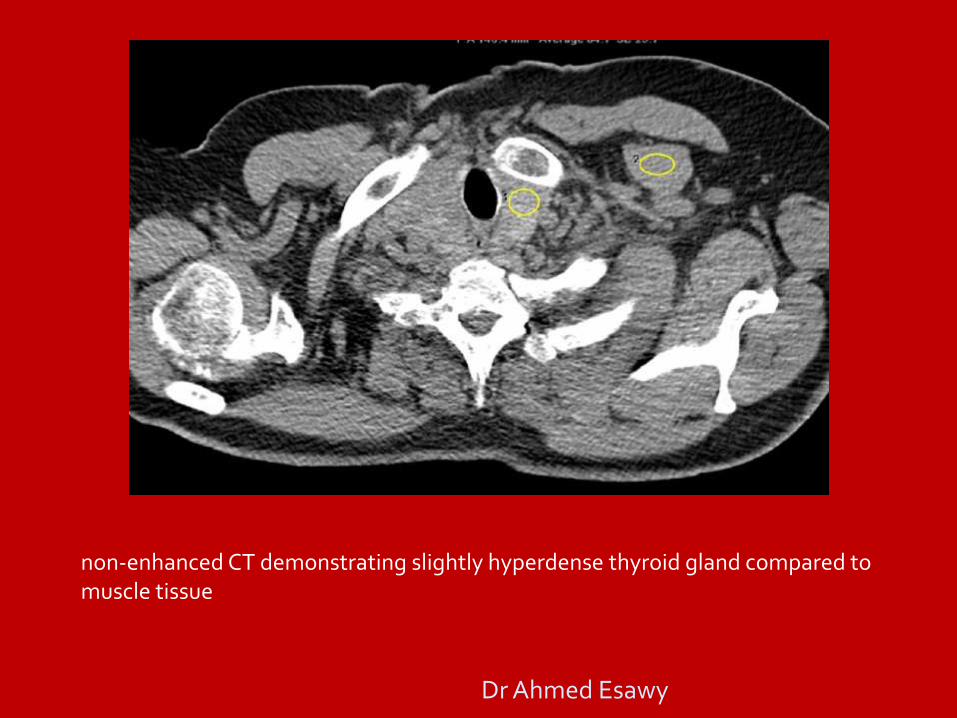
non-enhanced CT demonstrating slightly hyperdense thyroid gland compared to muscle tissue
Dr Ahmed Esawy

contrast enhanced CT demonstrating enhancement of thyroid tissue compared to muscle.
Dr Ahmed Esawy

T1w TSE image showing slight hyperintensity of thyroid gland compared to muscle tissue.
Dr Ahmed Esawy

T2w TSE image showing hyperintensity of thyroid gland compared to muscle tissue.
Dr Ahmed Esawy

Axial MR images of the neck. A, T1-weighted image shows mild hyperintensity in the thyroid gland. B, T2-weighted image shows a more pronounced hyperintensity, compared with muscle, in the thyroid gland.
Dr Ahmed Esawy

2-pathology
Dr Ahmed Esawy

Abnormalities of thyriod
functional Structural anatomical
Enlarged =goitre NOT ENLARGED FOCAL(mass / nodule)
hyperthyriodism hypothyriodism
euthyriod
NODULAR DIFFUSE Dr Ahmed Esawy

GOITRE =thyroid enlargment
(British English) or goiter (American English) (from the Latin gutteria, struma) is a swelling of the neck or larynx resulting from enlargement of the thyroid gland (thyromegaly), associated with a thyroid gland that is not functioning properly. Worldwide, over 90% cases of goitre are caused by iodine deficiency Goitrogens are substances (whether in drugs, chemicals, or foods) that disrupt the production of thyroid hormones by interfering with iodine uptake in the thyroid gland. This triggers the pituitary to release TSH, which then promotes the growth of thyroid tissue, eventually leading to goiter.
Dr Ahmed Esawy

Dr Ahmed Esawy

Goiterogenesis
Iodine deficiency results in hypothyroidism
Increasing TSH causes hypertrophy of thyroid (diffuse
nontoxic goiter)
Follicles may become autonomous; certain follicles will
have greater intrinsic growth and functional capability
(mult inodular goiter)
Follicles continue to grow and function despite
decreasing TSH (toxic mul tinodular goiter)
Sporadic vs. endemic goiter
Dr Ahmed Esawy

Simple (Colloid) Goiter
Diffuse goiter
Usually euthyroid
Peaks in puberty
Endemic goiter
Compensatory TSH
Follicular cell hypertrophy and
hyperplasia
Goiterogens (eg, cassava)
Non endemic or sporadic less
common
Rare hereditary defects in thyroid
hormone synthesis
Note distension of follicles with colloid
and flattening of epithelial cells
Dr Ahmed Esawy

Multinodular Goiter
Most simple goiters become transformed into
multinodular goiters.
Nontoxic or toxic (induce thyrotoxicosis)
No ophthalmopathy or dermopathy
May cause cosmetic disfigurement and tracheal
compression
May induce the superior vena caval syndrome
Differentiation of a dominant nodule from a thyroid
tumour may be difficult.
Retrosternal extension
Dr Ahmed Esawy

3-Differential diagnosis
Dr Ahmed Esawy

GIOTRE
DIFFUSE FOCAL/NODULAR
MULTINODULAR UNINODULAR
NON-TOXIC TOXIC
Structural / Anatomy
Functional /biochemical
Dr Ahmed Esawy
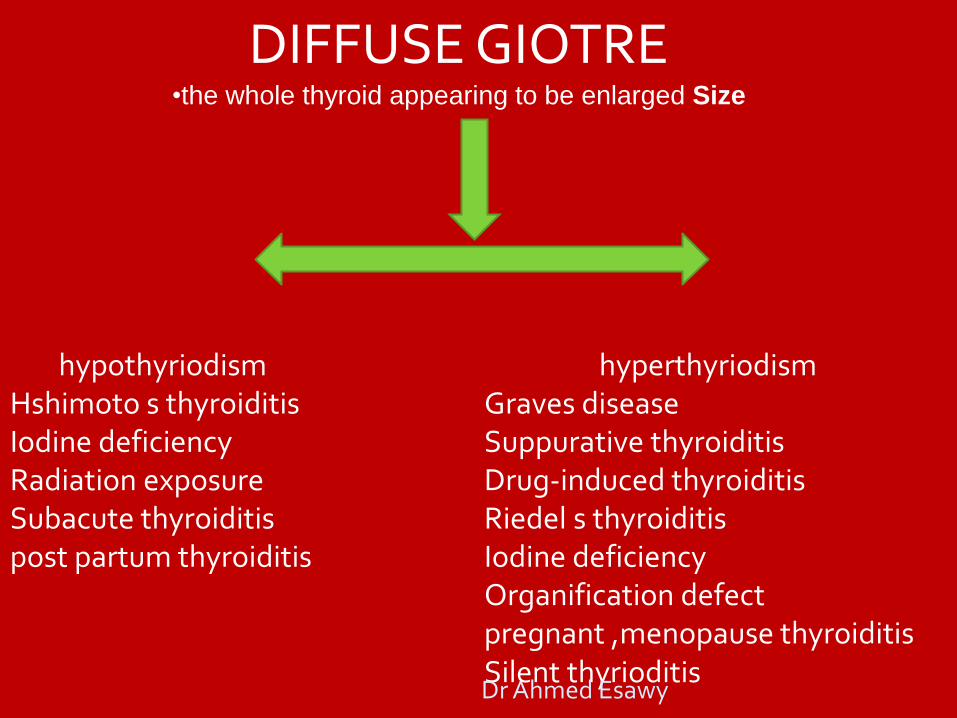
DIFFUSE GIOTRE •the whole thyroid appearing to be enlarged Size
hyperthyriodism Graves disease Suppurative thyroiditis Drug-induced thyroiditis Riedel s thyroiditis Iodine deficiency Organification defect pregnant ,menopause thyroiditis Silent thyrioditis
hypothyriodism Hshimoto s thyroiditis Iodine deficiency Radiation exposure Subacute thyroiditis post partum thyroiditis
Dr Ahmed Esawy

GIOTRE
DIFFUSE FOCAL/NODULAR
MULTINODULAR
UNINODULAR
HYPERTHYRIODISM thyrotoxic giotre
HYPOTHYRIODISM Hypothyriod giotre
Euthyroid goiter: - Diffuse goiter – U/S - MNG – U/S, FNA for dominant nodule Dr Ahmed Esawy

NODULAR GIOTRE
BENIGN ADENOMA NEOPLASM COLLIOD
Cyst Complex cyst
Focal thyrioditis
MALIGNANT
As function: biochemical - hot (toxic) - cold (N :TSH) cold nodule in a toxic thyroid (as may occur in Grave’s disease) Dr Ahmed Esawy

Nontoxic Goiter
Simple, Colloid, or Multinodular Enlargement of entire gland without
producing nodularity and without evidence of functional disturbance (euthyroid)
Causes Lack of Iodine
Compensatory increase of TSH = follicular cell hypertrophy
Sporadic Goiter Diffuse, Uninodular, or multinodular
Ingestion of Substances, hereditary enzyme defects
Simple Goiters may evolve = Multinodular Goiters Calcification, Degeneration, Fibrosis,
and Hemorrhage
Dr Ahmed Esawy

BENIGN NODULAR GIOTRE Non toxic
NEOPLASM Benign thyroid cysts (degenerated nodules) Simple cyst Haemorrhagic Cystic nodule in solid tumour
COLLIOD Dominent colliod nodule in MNG uninodular
Adenoma
macrofollicular (simple colliod) microfollicular (fetal) embryonal (trabecular) hurthe cell adenoma atypical adenoma adenoma with papillae signet ring adenoma
Inflammatory disorder subacute thyrioditis lymphocystic thyrioditis granulomatous disease (sarciodosis/TB) abscess
developmental dermiod unilateral lobe agenesis
Dr Ahmed Esawy

MALIGNANT NODULAR GIOTRE
MALIGNANT Papillary carcinoma Follicular carcinoma
Hurthle cell tumor Medullary Thyroid Carcinoma Anaplastic Carcinoma Lymphoma of thyroid
Dr Ahmed Esawy

NODULAR GIOTRE
UNINODULAR
MULTINODULAR MNG
INACTIVE
COLD
TOXIC NODULE
TOXIC NODULE
TOXIC MULTINODULAR GIOTRE INACTIVE
COLD
MALIGNANT BENIGN Dr Ahmed Esawy

Cold Thyroid Nodule BENIGN TUMOR
Nonfunctioning adenoma Cyst (20%) Involutional nodule Parathyroid tumor
INFLAMMATORY MASS Focal thyroiditis Granuloma Abscess
MALIGNANT TUMOR Carcinoma Lymphoma Metastasis
Dr Ahmed Esawy

“Cold” nodule = focal defect
Dr Ahmed Esawy

Cold nodule, R lobe (99mTcO4)
Dr Ahmed Esawy

Cystic Areas in Thyroid 25% of all thyroid nodules!
Anechoic fluid + smooth regular wall: Colloid accumulation in goiter = colloid-filled dilated macrofollicle Simple cyst (extremely uncommon)
Solid particles + irregular outline: Hemorrhagic colloid nodule Hemorrhagic adenoma (30%) Necrotic papillary cancer (15%) Liquefaction necrosis in adenoma / goiter Abscess Cystic parathyroid tumor
bloody fluid = benign / malignant lesion
clear amber fluid = benign lesion
Cystic lesions often yield insufficient numbers of cells!
Dr Ahmed Esawy

HYPOTHYRIODISM
CONGENITAL Hypoplasia & mal-descent Agenesis ,hemiagenesis Ectopia thyriod (sublingual thyriod) Familial enzyme defects Iodine deficiency (endemic cretinism) Intake of goitrogens during pregnancy Pituitary defects Idiopathic
Iodine deficiency(diffuse giotre) Hashimoto´s thyroiditis (autoimmune thyroiditis) Subacute (De Quervein’s) thyroiditis
Thyroidectomy or RAI therapy TSH or TRH deficiency Medications (iodide & Cobalt,amiodarone)) Idiopathic Post partum amyliodosis
ACQUIRED
Dr Ahmed Esawy

INCREASE THYRIOD HORMONE
Thyrotoxicosis refers to the manifestation of excessive quantities of circulating thyroid hormone
Hyperthyroidism refers only to the subset of thyrotoxic diseases caused by the overproduction of the thyroid hormone by the gland itself.
Dr Ahmed Esawy

HYPERTHYROIDISM
ETIOLOGY
• Graves’ disease ( autoimmune ).
• Toxic multi-nodular goiter ( toxic MNG ).
• Toxic nodule (hot or warm nodule)
Dr Ahmed Esawy

COMMON CAUSES OF HYPERTHYROIDISM
autoimmune diseases Graves disease (the most common cause of hyperthyroidism Lymphocytic thyroiditis With hyperthyroidism (silent thyroiditis) Postpartum thyrotoxicosis (PPT)
functioning thyroid adenomas (Hyperfunctioning thyroid
nodules (toxic adenoma, toxic multinodular goiter, Plummer's disease)
Toxic multinodular goiter
Dr Ahmed Esawy

High blood levels of thyroid hormones (hyperthyroxinemia)
Inflammation of the thyroid (thyroiditis). (subacute thyrioditis) (DeQuervain's) and Hashimoto's thyroiditis (Hypothyroidism immune-
mediated), These may be initially associated with secretion of excess thyroid hormone, but
usually progress to gland dysfunction and, thus, to hormone deficiency and hypothyroidism.
Oral consumption of excess thyroid hormone tablets
Amiodarone, an antiarrhythmic drug,
Postpartum thyroiditis (PPT)
A struma ovarii is a rare form of monodermal teratoma that contains mostly thyroid tissue
Excess iodine consumption notably from algae such as kelp.
Hypersecretion of thyroid stimulating hormone (TSH), which in turn is almost always caused by a pituitary adenoma
Thyroid tumor. A noncancerous thyroid tumor may make and secrete increased amounts of thyroid hormones.
LESS COMMON CAUSES OF THYROTOXICOSIS HYPERTHYROIDISM
Dr Ahmed Esawy

Varieties of Thyrotoxicosis
Associated with thyroid hyperfunction:
Excess production of TSH(rare)
Abnormal thyroid stimulator-Eg:Graves’ disease
Intrinsic thyroid autonomy-Eg:Hyperfunctioning adenoma, Toxic multinodular goitre
Not associated with thyroid hyperfunction:
Disorders of hormone storage-Eg:Subacute thyroiditis, chronic thyroiditis
Extrathyroid source of hormone- Thyrotoxicosis factitia,ectopic thyroid tissue- struma ovarii, functioning follicular Ca.
Dr Ahmed Esawy

DEVELOPMENTAL ABNORMALITIES OF
THYROID GLAND
Dr Ahmed Esawy

developmental process of the thyroid gland during the embryonic period. Descent of the thyroid gland during embryological development can be visualized from the thyroglossal duct cyst or remnant/ectopic tissue to its ultimate position, in the pretracheal region Dr Ahmed Esawy

Hemiagenesis of the thyroid gland. Axial contrast-enhanced CT scan demonstrates absence of the left lobe, which is a typical finding in hemiagenesis.
Dr Ahmed Esawy

Right lobe is enlarged, with mixed echogenic mass (arrows). Fine-needle aspiration was consistent with adenoma.
Thyroid Hemiagenesis with Adenoma
Dr Ahmed Esawy

CT scan obtained 9 months before sonogram shows absent left thryoid lobe and enlarged right thryoid lobe with small low-attenuation lesion (arrows).
Dr Ahmed Esawy

A 44-yearold woman with midline thyroid remnant tissue. Contrast-
enhanced CT image (a) shows a small, strongly enhanced mass between the strap muscles at the anterior aperture of the thyroid cartilage (arrows). The thyroid gland has a normal appearance in the lower neck (b).
Dr Ahmed Esawy

a–d. A 39-year-old woman with midline thyroid remnant tissue. T1- (a) and T2-weighted (b) MR images show a superficial lesion with intermediate signal intensity in the right paramedian region, at the anterior aperture of the thyroid cartilage (arrows). Contrast-enhanced T1-weighted MR images (c, d) show strong homogeneous enhancement of the mass (c, arrows). This lesion has the same signal intensity and enhancement pattern as the thyroid gland in all sequences. Dr Ahmed Esawy

a–c. A 35-year-old man with midline ectopic thyroid tissue. Contrastenhanced CT image (a) shows round, enhanced ectopic thyroid tissue at the anterior aperture of the thyroid cartilage (arrows). The thyroid gland is located in the normal location; however, agenesis of the isthmus with hypoplastic thyroid lobes exists (b, asterisk). An image of the I-131 scan (c) illustrates a well-defined area of uptake nearly at the hyoid bone, located at the midline (arrows).
Dr Ahmed Esawy

a, b. A 42-year-old man with lateral ectopic thyroid tissue. Contrast-enhanced CT images (a, b) show ectopic thyroid tissue in the submandibular and parapharyngeal regions at the hyoid bone level. The left submandibular gland is pushed anterolaterally by the ectopic tissue (a, arrows). The right thyroid lobe is visualized in the normal location and incidentally detected as a hypodense nodule in the right lobe. Agenesis of the isthmus and left thyroid lobe is noted (b).
Dr Ahmed Esawy
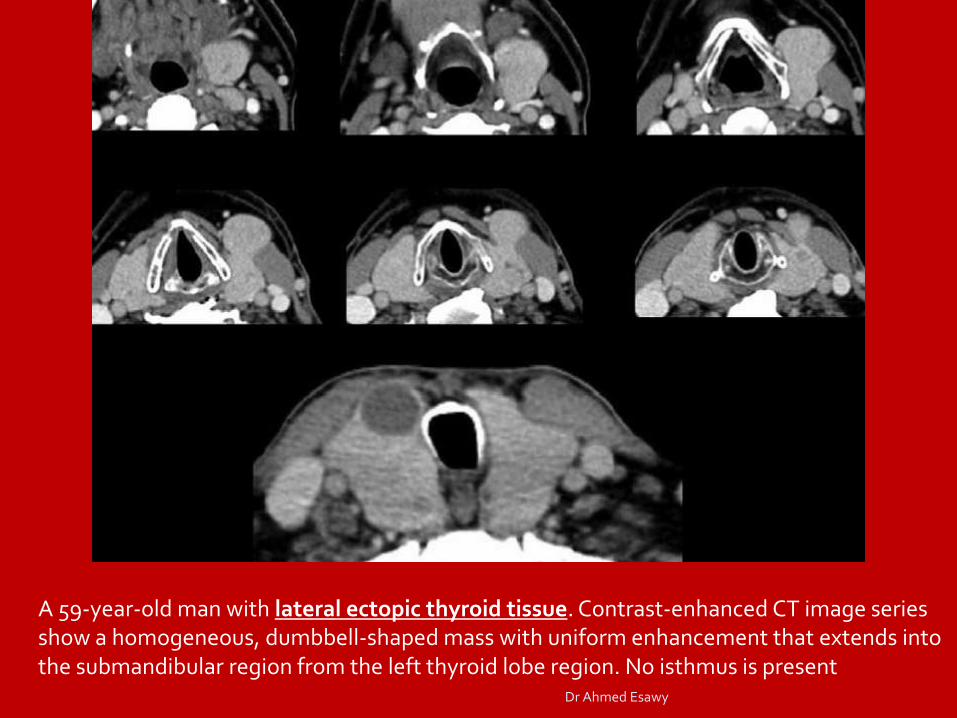
A 59-year-old man with lateral ectopic thyroid tissue. Contrast-enhanced CT image series show a homogeneous, dumbbell-shaped mass with uniform enhancement that extends into the submandibular region from the left thyroid lobe region. No isthmus is present
Dr Ahmed Esawy

Lingual thyroid
Dr Ahmed Esawy
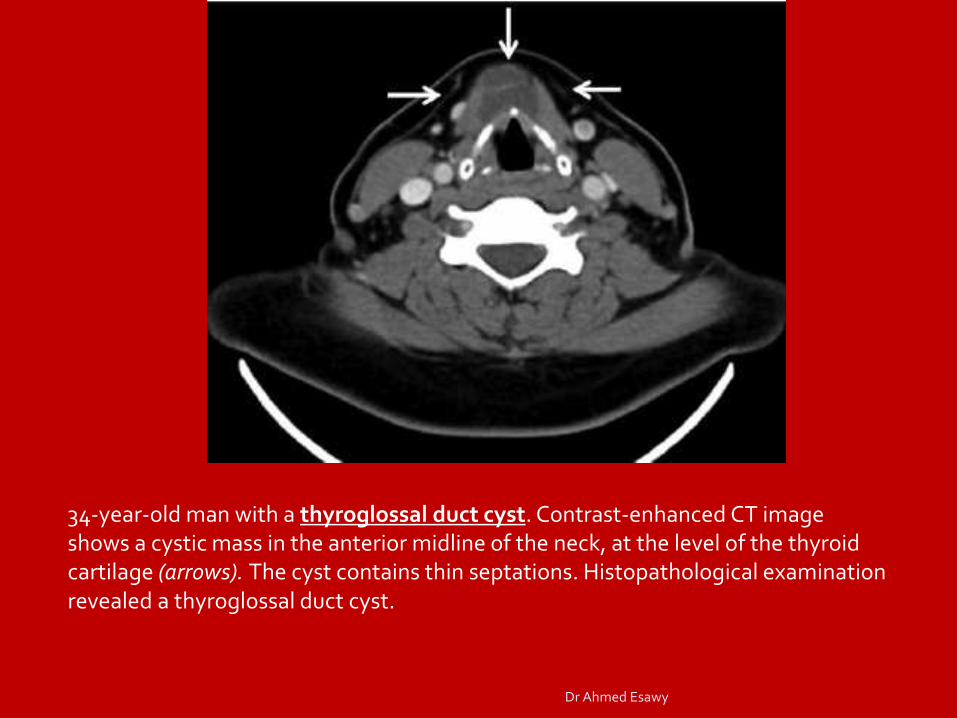
34-year-old man with a thyroglossal duct cyst. Contrast-enhanced CT image shows a cystic mass in the anterior midline of the neck, at the level of the thyroid cartilage (arrows). The cyst contains thin septations. Histopathological examination revealed a thyroglossal duct cyst.
Dr Ahmed Esawy

Thyroglossal duct cyst. A cystic left mass (asterisk) embedded within the paralaryngeal strap muscles on T1-weighted MR image. The fluid is mildly hyperintense; the subcutaneous fat is normal.
Dr Ahmed Esawy

Thyroglossal duct cyst. Enhanced CT (A) shows a hypodense left neck lesion (asterisk) located within the paralaryngeal strap muscles (m). This appearance resembles a "snake swallowing an egg" (B). Thyroglossal duct cyst (asterisk), strap muscles (m). Dr Ahmed Esawy

Thyroglossal duct cyst. Enhanced CT at level of hyoid bone (A) shows a lateral cystic lesion (asterisk) notching the inner surface of the hyoid (arrow). Inferiorly at the level of the pyriform sinuses (B), the lesion (asterisk) is embedded in the paralaryngeal strap muscles (m).
Dr Ahmed Esawy

Thyroglossal duct cyst. Enhanced CT at level of hyoid bone shows a lateral cystic lesion (asterisk) notching the inner surface of the hyoid (arrow). Inferiorly at the level of the pyriform sinuses (B), the lesion (asterisk) is embedded in the paralaryngeal strap muscles (m).
Dr Ahmed Esawy

Thyroglossal duct cyst. T1-weighted MR image demonstrating a mildly hyperintense midline lesion (arrow) notching the dorsal surface of the hyoid bone (arrowheads).
Dr Ahmed Esawy

a–d. A 48-year-old woman with a giant thyroglossal duct cyst. Axial T1-weighted MR image (a) shows a well-defined cystic mass in the floor of the mouth at the tongue base, the classic location for a thyroglossal duct cyst. The increased signal intensity of the cyst is due to either proteinaceous content or a prior hemorrhage (a, arrows). Coronal T2-weighted MR image (b) reveals high hyperintensity of the cyst, with mural thickening (arrows).
The axial (c) and sagittal (d) contrast-enhanced T1-weighted MR images with fat suppression show mild rim enhancement of the cyst with strong enhancement of the thickened wall due to residual thyroid tissue (arrows).
Dr Ahmed Esawy

Pyramidal lobe. Axial contrast-enhanced CT scan shows persistence of the distal portion of the thyroglossal duct. This condition is present in 50% of the population. P = pyramidal lobe.
Dr Ahmed Esawy