thyroid surgery - johanniter.de · waldkrankenhaus waldstraße 73 53177 bonn phone: 0228 383 - 0...
TRANSCRIPT

Thyroid SurgeryPatient information

2
Dear patient,
your doctor has advised you to undergo thyroid surgery. With this brochure we want to give you an overview about the necessity for thyroid surgery, about a modern minimal-invasive surgical method and the course of the upcoming treatment. The unpleasant prospect of under-going neck surgery arouses needless fears in affected patients. The information in this brochure shall help you overcome these problems, as thyroid surgery is little in-crimatory due to modern operation techniques and po-stoperative treatment concepts.
In our department, the surgical treatment of all benign and malignant thyroid diseases takes place in close col-laboration with general practitioners and other depart-ments. Thyroid surgery is one of our specialties. Depen-ding on the degree of thyroid alteration, we also perform the innovative minimal-invasive surgical method (MIVAT) with excellent cosmetical results. For this we provide modern devices such as ultrasonic scissors, HDTV video assistance and neuromonitoring for the safe exploration of the vocal cord nerve (Recurrent laryngeal nerve).We hope to provide prime information with this brochure and are pleased to speak to you personally.
Best regards,
Dr. Stefan Klozoris
Preface

3
Characteristical features of illnesses of the thyroid gland are palpable or visible enlargement of the neck with nodule formation or changes of the metabolism, such as hypo- or hyperthyroidism. Usually the test for thyroid hormones in the blood (T3, T4, TSH) and sonography of the gland is the first step of diagnostics, followed by nuclear medical examinations (scintigraphy) characteri-zing the activity of particular parts of the thyroid.
Based on these results your doctor (general practitioner, specialist for nuclear medicine) will give you a treatment suggestion within the range of conservative (i.e. watch-ful waiting, surveillance etc. including sonography, me-dication, fine-needle aspiration biopsy or radiation the-rapy) to surgical treatment.
If surgery is the choice of treatment, a specialist for ear, nose and throat should perform a preoperative laryngos-copy to check the function of the vocal cord nerve. It can also be performed in our clinic by the ENT-department prior to surgery.
Preliminary examination and treatment methods
4
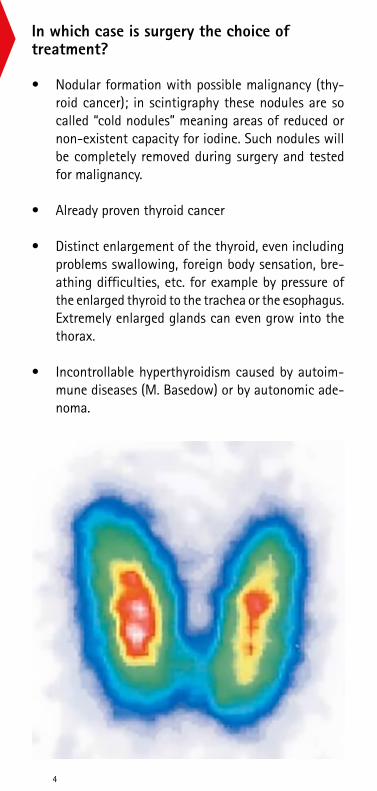
• Nodular formation with possible malignancy (thy-roid cancer); in scintigraphy these nodules are so called “cold nodules” meaning areas of reduced or non-existent capacity for iodine. Such nodules will be completely removed during surgery and tested for malignancy.
• Already proven thyroid cancer
• Distinct enlargement of the thyroid, even including problems swallowing, foreign body sensation, bre-athing difficulties, etc. for example by pressure of the enlarged thyroid to the trachea or the esophagus. Extremely enlarged glands can even grow into the thorax.
• Incontrollable hyperthyroidism caused by autoim-mune diseases (M. Basedow) or by autonomic ade-noma.
In which case is surgery the choice of treatment?

5
For this procedure the surgeon conducts a slightly arch-shaped transversal section along the Langer lines of skin tension (to avoid “thick” scars) to dissect the thyroid gland. By this section any thyroid disease up to very large goiters can be treated. We are always anxious to make the section as small as possible to accomplish an optimal cosmetical result. If there are malign altera-tions it can be necessary to remove nearby lymph nodes as well. This can also be done with the section described above with the same good cosmetical result, as the scar-ring can be minimized.
Surgical procedures

6
Conventional thyroid surgeryFor this procedure the surgeon conducts a slightly arch-shaped transversal section along the Langer lines of skin tension (to avoid “thick” scars) to dissect the thyroid gland. By this section any thyroid disease up to very large goiters can be treated. We are always anxious to make the section as small as possible to accomplish an optimal cosmetical result. If there are malign altera-tions it can be necessary to remove nearby lymph nodes as well. This can also be done with the section described above with the same good cosmetical result, as the scar-ring can be minimized.
Minimal-invasive video assisted thyroidectomy: MIVATThe MIVAT-technique (Minimal-invasive video assisted thyroidectomy) combines the conventional and the en-doscopic surgical method. The section is also conducted at the front of the neck but is much shorter (approx. 2 cm). The operating field is carefully kept open by retrac-tors. The dissection happens under sight through a 5 mm rigid tube which is inserted into the operating field. By this a much shorter section is needed.
This method is also suitable for men. However, the extend of the thyroid alteration is a limitating factor to perform this method (alterations up to 35 ml of thyroid volume or up to 2,5 cm diameter of the nodule). If the thyroid is larger the length of the section depends on the extent of the alterations.
We would like to explain to you the up- and downsides of the methods in a personal conversation to recommend the method which fits your individual condition.

7
The preoperative preparations usually begin with an ap-pointment in our thyroid clinic (daily on appointment). Here we talk about the surgery itself and their risks and schedule the date of the inpatient residence. The admis-sion can take place the day before the surgery or the day of the surgery. We want to make your hospital stay as short as possible. After the surgery you will be taken care of at one of our surgical wards (ward 6 or 11). Normally a drainage will be inserted into the wound for around two days to relieve wound secretion. Typically the hos-pital stay lasts for three to four days. The stitching ma-terial doesn’t need to be removed as it is adsorbed by the body. Usually patients don’t have significant pain after surgery. Analgesia can be achieved with light and well tolerated pain killers.
Stationärer Aufenthalt
8
There are general surgical complications such as bleeding, secondary bleeding, prolonged wound healing or infec-tion of the wound. Due to the accurate and minimal-in-vasive surgical techniques these complications are rare. Typical, but also very rare is the injury of the vocal cord nerve (Recurrent laryngeal nerve) or the removal of the parathyroid.
Both vocal cord nerves are located behind the thyroid lobes near the trachea. In a low percentage of thyroid surgeries it can occur, that this nerve is injured or irritated resulting in a temporary or definite paralysis of the ner-ve. Unilateral damage can lead to a slightly throaty voice with impaired sound. In some patients these alteration are not noticeable and only the ENT-examination shows the effect on the vocal cord. In the most cases the da-mage of the nerve is caused by pressure, pull, edema or hematoma rather than complete transection which leads to full recovery in three-fourths of the cases. Only if the nerve doesn’t recover after one year a permanent im-pairment must be considered. If so the function of the vocal cord can be regained by logopedic treatment.
Risks of the surgery

9
To avoid injuries of the nerve we regularly perform neu-romonitoring of the Recurrent laryngeal nerve. The func-tion of the nerve is monitored during the surgery to fa-cilitate nerve-sparing dissection.
The parathyroid glands are two pairs of glands behind both thyroid lobes, which in some cases are closely con-nected to the thyroid.
Its function is the regulation of calcium in the blood by releasing the parathyroid hormone. Usually these glands can be identified and spared.
Nevertheless, sometimes circulatory disorder or acciden-tal removement of the glands can occur. The result is a decrease of the calcium in the blood. The calcium in the blood can be increased by oral substitution of calcium or Vitamin D. In most cases the decrease is reversible, which means the substitution is temporary.
Voruntersuchungen und Behandlungsmethoden

10
After discharge you should rest for some days.
The food intake is possible without difficulty, so there is no necessity for a special diet.
Activities of the everyday life are possible after a few days.
Three days after surgery it is allowed to take a shower. You should avoid heavy lifting for two weeks. In this period you should not perform serious sport, but you should be able to go for a walk after being discharged. Likewise you should start riding the bicycle after one week at the earliest.
The length of the inability to work differs from patient to patient and depends on the workload. Please clarify this question in on of the preliminary consultations.
Behaviour after discharge

11
Contact:Dr. med. Stefan KlozorisChefarzt der Abteilung fürAllgemein- und ViszeralchirurgieJohanniter GmbHWaldkrankenhausWaldstraße 7353177 Bonn
Terminvereinbarung:Phone: 0228 383 -258Fax: 0228 383 -257E-Mail: [email protected]

So finden Sie uns
Anfahrt aus Richtung Meckenheim/Wachtberg:Von der L 158 kommend biegen Sie links in die »Quellenstraße« und folgen deren Verlauf. Dann links in die »Venner Straße« und bis zum Ende folgen.
Anfahrt aus Richtung Bad Godesberg über die B 9:Von der B 9 (»Bonner Straße«) kommend biegen Sie rechts in die L 158 (»Burgstraße«) ein. An der dritten Ampel rechts in die »Winterstraße« und dieser 3 km folgen.
Mit öffentlichen Verkehrsmitteln:Ab Bad Godesberg Bahnhof fährt die Buslinie 615 (Rich-tung Stadtwald) bis zur Endhaltestelle Waldkrankenhaus.
Johanniter GmbHWaldkrankenhausWaldstraße 7353177 Bonn
Phone: 0228 383 - 0Fax: 0228 383 - 99
Aus Richtung Bad Godesberg
Waldkrankenhaus
Aus Richtung Meckenheim/Wachtberg
Waldstraße
Quellenstraße
L 158
Winterstraße
Venn
er St
r.
Horion
str.
www.bn.johanniter-kliniken.de