tipos infrecuentes de cáncer de mama
TRANSCRIPT

Annals of Oncology 20: 1763–1770, 2009
doi:10.1093/annonc/mdp245
Published online 14 July 2009review
Breast carcinoma—rare types: review of the literature
R. Yerushalmi1*, M. M. Hayes2 & K. A. Gelmon1
1Division of Medical Oncology and 2Department of Pathology, British Columbia Cancer Agency, Vancouver, British Columbia, Canada
Received 23 February 2009; accepted 26 March 2009
Invasive breast cancer is a heterogeneous disease in its presentation, pathological classification and clinical course.
However, there are more than a dozen variants which are less common but still very well defined by the World Health
Organization (WHO) classification. The rarity of many of these neoplasms does not allow large or randomized studies
to define the optimal treatment. Many of the descriptions of these cancers are from case reports and small series. Our
review brings updated information on 16 epithelial subtypes as classified by the WHO system with a very concise
histopathology description and parameters helpful in the clinic. The aim of our review is to provide a tool for breast
cancer caregivers which will enable a better understanding of the disease and its optimal approach to therapy. This
may also stand as a clinical framework for a future understanding of these rarer breast cancers when gene analysis
work is reported.
Key words: breast carcinoma, epithelial breast cancer, prognosis, treatment, triple negative, World Health
Organization classification
introduction
Invasive breast cancer is a heterogeneous disease in itspresentation, pathological classification and clinical course.Most tumors are derived from mammary ductal epithelium,principally the terminal duct-lobular unit, and up to 75% of thediagnosed infiltrating ductal carcinoma are defined as invasiveductal carcinoma, not otherwise specified (IDC-NOS). Thesecond most common epithelial type is invasive lobularcarcinoma which comprises of 5%–15% of the group.However, there are more than a dozen variants which are lesscommon but still very well defined by the World HealthOrganization (WHO) classification.Recently, there has been an increased emphasis on the
immunohistochemical and genetic profile of tumors and theseclassifications are evolving as a standard part of the diagnosticprocess. This novel approach pushes aside traditionaldescriptive definitions. An estrogen receptor (ER)-negativeductal (NOS) as well as adenoid cystic, acinic and metaplasticcarcinoma may all receive the title of triple-negative disease andthis may affect decision making for those less familiar with thenuances of the rare tumor types. Furthermore, the classificationusing gene expression profile was established using a cohort ofductal carcinoma NOS, without including cancers of specialtypes. We therefore indicate that it is extremely important tohighlight what is known about the different behavior of eachtumor and gather together the published data with the goal ofmarrying the rare tumor types with a current molecular
definition of breast cancer. The rarity of many of theseneoplasms does not allow large or randomized studies to definethe optimal treatment. Many of the descriptions of thesecancers are from case reports and small series.Our review brings updated information on 16 epithelial
subtypes as classified by the WHO system [1] with a veryconcise histopathology description and parameters helpful inthe clinic. The aim of our review is to provide a tool for breastcancer caregivers which will enable a better understanding ofthe disease and its optimal approach to therapy. This may alsostand as a clinical framework for a future understanding ofthese rarer breast cancers when gene analysis work is reported.Our review is based on Pubmed research updated to
December 2008.
good prognosis, ER positive
Findings are summarized in Table 1.
tubular carcinoma
definition and epidemiology. The definition of a tubularcarcinoma (TC) requires tumor purity with 90% tubulararchitecture. The characteristic finding histologically is opentubules composed of single layer of epithelial cells and cellulardesmoplastic stroma. Nuclear grade is low. TC comprises of0.7%–10.3% of the invasive epithelial breast cancer (IEC) and ismore likely to occur in postmenopausal women. A population-based study of nodal metastases with 171 TC patients has foundthe proportion of cases with axillary nodal involvement atpresentation to be lower in TC than in the grade 1 IDC group(12.9% and 23.9%, respectively) [2]. A smaller study (n = 33)
revie
w
*Correspondence to: Dr R. Yerushalmi, Division of Medical Oncology, British Columbia
Cancer Agency, 600 W 10th Avenue, Vancouver, British Columbia, Canada V5Z 4E6. Tel:
+1-604-877-6000-2594; Fax: +1-604-877-0585; E-mail: [email protected]
ª The Author 2009. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
All rights reserved. For permissions, please email: [email protected]

reported on 25% of the cases to involve axillary nodes, mostoften micrometastases [3].
diagnostic imaging. TC has a variety of presentations, but it ismostly seen on mammography as a small spiculated mass andon sonography as an irregular mass with posterior acousticshadowing [11].
immunohistology. Most of the cases are ER (>90%) andprogesterone receptor (PgR) positive with a low proliferationindex. HER-2 status (as determined by immunohistochemicalstaining or fluorescence in situ hybridization) and epidermalgrowth factor receptor are negative [12].
prognosis. Survival is not significantly different from that of thegeneral population [13], even with positive axillary lymph nodes[14]. Five-year disease-free survival (DFS) for node-positivepatients was 94% (n = 64). Interestingly, in this series, the 5-yearDFS of those who did not receive systemic treatment was 100%.
invasive cribriform carcinoma
definition and epidemiology. These grade 1 tumors arecharacterized by a cribriform pattern in the majority of theinvasive component. Tumors are divided into pure, classicaland mixed forms of invasive cribriform carcinoma (ICC). Inthe classical and the mixed forms, <50% of the tumor consistsof other histological types [4]. This tumor accounts up to 3.5%of the IEC, hence the data are based on case reports and smallseries. The mean age is 53–58 years. Page et al. reported 14.3%of the cases to involve axillary lymph nodes [4, 5].
diagnostic imaging. Stutz et al. reported on eight radiologicalcases. Only four were seen on mammography and theultrasound was not entirely typical of breast carcinoma [15].
immunohistology. ER is positive in 100% and PgR in 69% of thecases [5]; HER-2 is negative [16].
prognosis. In an older series, the 5-year survival was 100% forpure and ‡50% ICC, 88% for <50% ICC and 78.3% for the IDCcontrols [5]. Ten-year breast-specific survival for the pure caseswas 100% [4].
pure mucinous carcinoma
definition and epidemiology. The mucinous neoplasms arecharacterized by the production of abundant extracellular and/or intracellular mucin. The definition requires a mucinous
component >50% of the lesion. The pure type contains mucinin all of the IDC. The WHO classification divides this tumorinto three different subtypes: (i) mucinous carcinoma (ii)cystadenocarcinoma and columnar cell mucinous carcinomaand (iii) signet ring cell carcinoma [1]. Pure mucinouscarcinomas represent 1%–4% of all breast cancers, witha reputation of presenting at one of the oldest median ages(71 years). Despite often having a large tumor size, the axillarylymph nodes are rarely involved; in a recent large series, 111patients with mucinous breast cancer were identified. Ninety-six (86%) patients underwent nodal evaluation either bysentinel lymph node biopsy or by axillary dissection. Fourteenpatients (13%) were found to have lymph node metastasis.Node positivity was associated with larger tumor size (mean2.7 cm). None of the 31 patients with tumor size <1 cm hadknown lymph node metastasis (24 were node negative, andseven were not evaluated with sentinel lymph node biopsy oraxillary dissection) [17]. In contrast to this study, there arereports on small tumors <1 cm presenting with at least a 5%incidence of nodal involvement [6, 7].
imaging. Pure mucinous carcinomas present an imagingchallenge due to their isoechogenic appearance on ultrasound[18]. Typical magnetic resonance imaging (MRI) demonstratesa gradually enhancing contrast pattern and a very high signalintensity on T2 images [19, 20].
immunohistology. These are mostly well-differentiated lesionsfrequently associated with positive ERs (>90%) and PgRs (81.5%)and HER-2-negative disease. However, rare cases with HER-2-positive staining have been reported but these may need review.
prognosis. Mucinous tumors have a favorable prognosis with5-, 10-, 15- and 20-year survival rates of 94%, 89%, 85% and81%, respectively [7]. Node involvement was associated witha significant worse 5-year DFS or overall survival (OS) [13].Other traditional parameters such as age, T size, nuclear gradeand PgR status also significantly influence outcome [7].
invasive solid papillary carcinoma
definition and epidemiology. The literature is unclear whethersolid papillary carcinoma (SPC) is a form of in situ carcinomaor a true invasive malignancy and the WHO classificationdefines invasive SPC as a separate entity. SPC characteristicallyhas papillae with focal solid areas. Ductal carcinoma in situ(DCIS) is present in >75% of cases and lymphatic vesselinvasion in one-third of the cases. The tumor comprises <1% to2% of IEC and typically presents in postmenopausal womenwith only 15% of reported cases occurring under the age of 50.Otsuki et al. reported on 20 patients with pure SPC and noaxillary lymph node involvement [8].
immunohistology. In total, 100% of the tumors are ER positiveand HER-2 negative and 80%–100% are PgR positive. Almostall cases show positive staining for chromogranin and �40%are also positive for synaptophysin [8, 21].
imaging. The sonographic features are indistinguishablefrom papillomas. The only differential finding betweennoninvasive and invasive papillary cancers was circumscribedmargins [22].
Table 1. Good prognosis typically ER-positive tumors
Dominant HER-2
profile
Axillary lymph
node involvement %
Tubular Negative 13–25 [2, 3]
Invasive cribriform Negative 14.3 [4, 5]
Pure mucinous Negative £5 [6, 7]
Invasive solid papillary Negative 0 [8]
Apocrine 50% £4 [9]
Solid neuroendocrinea Negative £40 (n = 8) [10]
aDoes not differ from other carcinomas and depends very much on its
histological grade (see text).
ER, estrogen receptor.
review Annals of Oncology
1764 | Yerushalmi et al. Volume 20 |No. 11 | November 2009

prognosis. Of the 1603 breast cancers reviewed in the NationalSurgical Adjuvant Breast and Bowel Project (NSABP)-04 study,35 had papillary features and only three experienced treatmentfailure at 5 years [23]. Node-negative patients who had beenenrolled in the NSABP B-06 study revealed an improved survivalafter 10 years of follow-up compared with IDC-NOS [24].
apocrine carcinoma
definition and epidemiology. Microscopically, apocrinecarcinomas (ACs) demonstrate the same architectural growthpattern as invasive ductal carcinomas of no special type, differingonly in their cytological appearance. The cells are characterizedby typical apocrine features with abundant eosinophilic granularcytoplasm and prominent/multiple nucleoli. There is no agreeddefinition and some pathologists now confirm their diagnosisby staining for gross cystic disease fluid protein-15 [9, 25].Axillary lymph node incidence varies from <1% to 4% but thereis extremely sparse information in the literature.
immunohistology. These tumors are reported as ER positive in3.8%–60% of cases, PgR positive in 4.8%–40%, HER-2 positivein 50%, with a proliferation index of 6.9%–23.7% and p53alteration in 46%–50%. Androgen receptors are positive in56%–100% of AC [9].
prognosis. AC has a similar prognosis to IDC-NOS whenmatched for stage and grade [26].
neuroendocrine tumors
definition and epidemiology. Neuroendocrine (NE) was notrecognized as a single entity until the last WHO’s classification.This classification differentiates between four differentsubtypes: (i) small-cell carcinoma (SCC); (ii) large-cellcarcinoma; (iii) solid NE carcinoma; and (iv) atypical carcinoidtumor. Our experience shows that the NE differentiation hasno prognostic influence and on the whole they behave as pertheir Nottingham grade [27].For simplification, this section describes the solid
neuroendocrine subtype (SN) which represents a betterprognosis group. (The SCC subtype is described in the ‘poorprognosis, ER positive’ section.) The tumors consist of denselycellular, solid nests and trabeculae of cells separated by delicatefibrovascular stroma [1]. Prevalence is up to 0.5% of breastcancers. In a small series of eight patients, three presented withinvolved axillary lymph nodes.
immunohistology. As per the definition, there is synaptophysinor chromogranin immunohistochemical expression in >50% ofthe cells. Typically, these tumors present with ER- and PgR-positive and HER-2-negative status [10].
gene expression. Profile of endocrine carcinoma overlaps withthose of mucinous carcinomas [28].
imaging. There is no specific imaging presentation in thelimited number of SN tumors reported.
prognosis. The outcome of these cancers does not differ fromother carcinomas and depends very much on its histologicalgrade [27, 29]. The immunoprofile is reminiscent of theluminal A subtypes, and hence a good prognosis is expected,
although we are cautious of this claim with the small number ofcases reported.
good prognosis, ER negative
Findings are summarized in Table 2.
medullary carcinoma
definition and epidemiology. This carcinoma is composed ofpoorly differentiated cells with no glandular structures, scantstroma, circumscribed margins and a prominentlymphoplasmacytic infiltrate. If most but not all the features arepresent, the tumor is identified as ‘atypical medullarycarcinoma’ (AMC) [1]. Medullary carcinoma (MC) comprises1%–7% of IEC. In a large series of almost 1500 patients withMC, only 27% had involved nodes. Although MC is not anindication for BRCA gene screening, there are growing datathat indicate that MC may correlate with BRCA1 genemutation [30].
diagnostic imaging. MC commonly manifests as well-circumscribed masses. Magnetic resonance mammographyappearance is nonspecific and often indicative of a benignlesion [35, 36].
immunohistology. MC shares common characteristics with thebasal type breast cancer.Most of the tumors are hormone receptorand HER-2 negative and CKT 5/6 positive (94%) [30, 37].MC but not AMC lacks Bcl-2 and there are data that show
they differ in expression of human leukocyte antigen-DR, b2-microglobulin, E cadherin and beta-catenin compared withother tumors [38].
prognosis. Paradoxical to its histology features, MC usually hasa good prognosis. In one series, 10-year distant relapse-freesurvival reached 95% [30]. In another study, 10-year OS was 85%for MC as compared with 68% in the IDC-NOS patients [39].Studies are hampered by lack of reproducibility of the
pathological diagnosis, small numbers of patients and poorstatistical power.
secretory breast carcinoma
definition and epidemiology. Secretory breast carcinoma (SBC)is also known as juvenile carcinoma. This is an extremely raretumor with limited data available.Two distinctive pathological characteristics of SBC are
intracellular/extracellular secretion and granular eosinophiliccytoplasm of the neoplastic cells. Although secretory carcinomamay occur in adults, the median and mean age are 33 and
Table 2. Good prognosis typically ER-negative tumors
Dominant HER-2
profile
Axillary lymph
node involvement %
Medullary Negative 27 [30]
Secretory Negative 15 [31]
Adenoid cystic Negative 0–4.6 [32, 33]
Acinic cell Negative 17 [34]
ER, estrogen receptor.
Annals of Oncology review
Volume 20 |No. 11 | November 2009 doi:10.1093/annonc/mdp245 | 1765

40 years, respectively. The literature mentions nodalinvolvement in 15% of the patients at presentation [31].
imaging. SBC frequently appears as a small benign/intraductallesion on sonography [40].
immunohistochemistry. This subtype has the triple-negativephenotype (ER, PgR, and HER-2 negative). It has beendemonstrated that SCs of the breast consistently harbor thet(12;15)ETV6-NTRK3 translocation [41].
prognosis. SBC has a favorable prognosis in children andadolescents but seems slightly more aggressive in older patients.Metastatic cases have been reported [1].
adenoid cystic carcinoma
definition and epidemiology. Adenoid cystic carcinomas (ACCs)are characterized by a mixture of proliferating glands,myoepithelial cells and stromal/basement elements. Data in theliterature are based on �200 cases. The tumor represents 0.1%of breast carcinoma and is diagnosed predominantly inpostmenopausal women. Pain is a prominent symptom due toneural involvement [42]. Most of the reports document a lowrate of axillary involvement of 0%–4.6%; however, there aresome small series that report on up to 27% lymph nodemetastases [32, 33].
immunohistochemistry. The tumor displays triple-negativephenotype [43, 44]. However, a study with 28 patients found46% of the cases to be ER positive and 36% to be PgR positive[45]. In another study, all (n = 18) cases were c-kit (CD-117)positive. MIB-1 antibody (monoclonal antibody that isimmunoreactive with Ki-67) stains demonstrate lowproliferative fraction [46].
prognosis. The 5-, 10- and 15-year OS rates were 85%–88%, 75%and 60%, respectively, for ACC. Millar et al. reported anincidence of 26% (n = 5) for second malignancies at 15 years.Themajority of the second cancers were not within the treated orcontralateral breast [33]. Metastases are rare and have beenreported to spread many years from diagnosis and without priornodal disease [45, 47]. The most frequent site of metastases islung. Patients may live many years with metastases.
acinic cell carcinoma
definition and epidemiology. Acinic cell carcinoma is consideredas one of the types of salivary gland-like tumors of the breastthat show serous differentiation. Eighteen cases have beenreported in the literature. Ages range from 35 to 80 years. Threecases with positive lymph nodes are recorded [34].
imaging. A well-defined mass creates a differential diagnosiswithMC, intracystic carcinoma andmetaplastic carcinoma [48].
immunohistochemistry. This neoplasm is characterized by thelack of ER, PgR and HER-2. Expression of markers such asamylase, lysozyme and chymotrypsin is usually seen as in aciniccells of the salivary glands. Stains positive for epithelialmembrane antigen and S100 protein are frequently found.
prognosis. The literature categorizes this tumor as a favorableone; however, even within a short follow-up period, systemic
and local recurrences were recorded. Larger series are requiredfor definite conclusions [49].
poor prognosis, ER positive
Findings are summarized in Table 3.
high-grade small-cell NE carcinoma
The literature describes <40 cases of breast small cell NEcarcinoma (SCC) but this may be underreporting. Thisneoplasm is similar to NE tumors presenting in the lung orwith extrapulmonary areas and share the same tumor markers.Diagnosis requires ruling out a nonmammary origin [53].
The presence of in situ component may be helpful but is notessential [50, 54]. Most patients are in the sixth or seventhdecades of life and �59% present with involved lymph nodes.
immunohistology. As per the definition, it expresses NEmarkers, neurone-specific enolase, protein gene product 9.5,chromogranin and synaptophysin, in >50% of the cellpopulation [1]. Most of the cases are positive for cytokeratinCAM5.2, AE1/3 and cytokeratin 7 as well. Surprisingly, thetumor often expresses ERs and PgRs and this correlates with thedegree of differentiation; well-differentiated tumors are themore likely to express hormone receptors with a variedfrequency of 0%–50%. Her-2 status is typically negative [55, 56].
imaging. Radiological findings are not specific but meet thecriteria for a suspicious mass [57].
prognosis. SCC tumor is considered an aggressive tumor witha poor prognosis. However, there are some reports about long-term survival when the diagnosis is made early [58]. NEdifferentiation using synaptophysin, chromogranin A, andneuron-specific enolase had no prognostic influence [27].
invasive micropapillary carcinoma
definition and epidemiology. Hollow aggregates of malignantcells and lymphatic invasion is a common feature of this tumor,ranging from 72.3% to 91% of cases [51]. The pure variant isextremely rare. Mean age is 52.5 years (range 33–78). Asopposed to the pure SPC, �70% of the patients present withinvolved axillary lymph nodes [51, 52].
immunohistochemistry. About two-thirds of the cases are ERpositive and up to 68% are PgR positive, one-third to one-halfof the patients present with HER-2-positive status and 66%with Bcl-2 positive. p53 overexpression was identified in 48% ofthe cases [51, 59]. No basal-like immunostaining pattern wasdetected [60].
imaging. Mammography is able to diagnose >80% of the cases.Masses appear with high density. The margins are commonly
Table 3. Poor prognosis typically ER-positive tumors
Dominant HER-2
profile
Axillary lymph
node involvement %
Small cell Negative 59 [50]
Invasive micropapillary £50% 70 [51, 52]
ER, estrogen receptor.
review Annals of Oncology
1766 | Yerushalmi et al. Volume 20 |No. 11 | November 2009
speculated; however, in approximately one-third of thepatients, indistinct or microlobulated margins were seen.Microcalcifications were present in 43.8% of patients. Onsonography, masses are typically hypoechoic, with only 60% ofthe masses showing posterior acoustic shadowing [61].
prognosis. Carcinoma with micropapillary features harborsa poor survival. The amount of IMC component correlatesstrongly with the number of involved axillary lymph nodes.In the 5-year follow-up (range 4–199 months) of 98
patients, 10-year OS was 48% and breast-specific survivalwas 63.3%. The outcome of the patients did not differsignificantly from infiltrating ductal carcinomas of similarnode status [62, 63].
poor prognosis, ERs negative
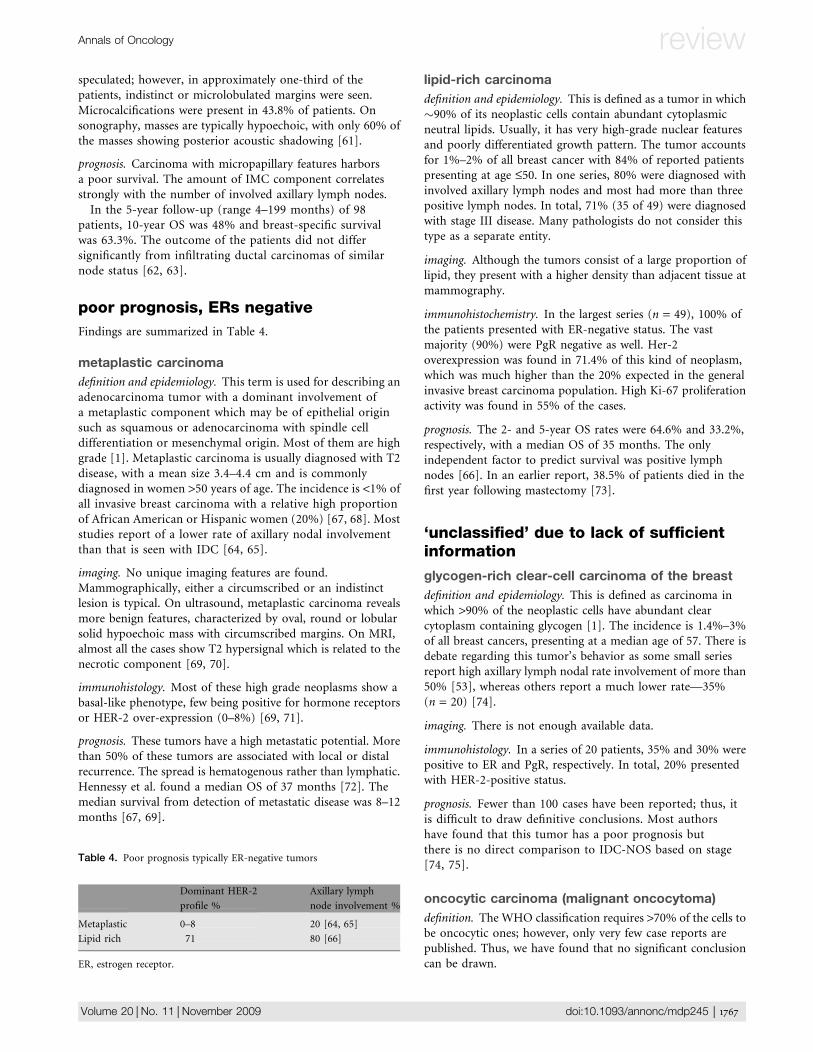
Findings are summarized in Table 4.
metaplastic carcinoma
definition and epidemiology. This term is used for describing anadenocarcinoma tumor with a dominant involvement ofa metaplastic component which may be of epithelial originsuch as squamous or adenocarcinoma with spindle celldifferentiation or mesenchymal origin. Most of them are highgrade [1]. Metaplastic carcinoma is usually diagnosed with T2disease, with a mean size 3.4–4.4 cm and is commonlydiagnosed in women >50 years of age. The incidence is <1% ofall invasive breast carcinoma with a relative high proportionof African American or Hispanic women (20%) [67, 68]. Moststudies report of a lower rate of axillary nodal involvementthan that is seen with IDC [64, 65].
imaging. No unique imaging features are found.Mammographically, either a circumscribed or an indistinctlesion is typical. On ultrasound, metaplastic carcinoma revealsmore benign features, characterized by oval, round or lobularsolid hypoechoic mass with circumscribed margins. On MRI,almost all the cases show T2 hypersignal which is related to thenecrotic component [69, 70].
immunohistology. Most of these high grade neoplasms show abasal-like phenotype, few being positive for hormone receptorsor HER-2 over-expression (0–8%) [69, 71].
prognosis. These tumors have a high metastatic potential. Morethan 50% of these tumors are associated with local or distalrecurrence. The spread is hematogenous rather than lymphatic.Hennessy et al. found a median OS of 37 months [72]. Themedian survival from detection of metastatic disease was 8–12months [67, 69].
lipid-rich carcinoma
definition and epidemiology. This is defined as a tumor in which�90% of its neoplastic cells contain abundant cytoplasmicneutral lipids. Usually, it has very high-grade nuclear featuresand poorly differentiated growth pattern. The tumor accountsfor 1%–2% of all breast cancer with 84% of reported patientspresenting at age £50. In one series, 80% were diagnosed withinvolved axillary lymph nodes and most had more than threepositive lymph nodes. In total, 71% (35 of 49) were diagnosedwith stage III disease. Many pathologists do not consider thistype as a separate entity.
imaging. Although the tumors consist of a large proportion oflipid, they present with a higher density than adjacent tissue atmammography.
immunohistochemistry. In the largest series (n = 49), 100% ofthe patients presented with ER-negative status. The vastmajority (90%) were PgR negative as well. Her-2overexpression was found in 71.4% of this kind of neoplasm,which was much higher than the 20% expected in the generalinvasive breast carcinoma population. High Ki-67 proliferationactivity was found in 55% of the cases.
prognosis. The 2- and 5-year OS rates were 64.6% and 33.2%,respectively, with a median OS of 35 months. The onlyindependent factor to predict survival was positive lymphnodes [66]. In an earlier report, 38.5% of patients died in thefirst year following mastectomy [73].
‘unclassified’ due to lack of sufficientinformation
glycogen-rich clear-cell carcinoma of the breast
definition and epidemiology. This is defined as carcinoma inwhich >90% of the neoplastic cells have abundant clearcytoplasm containing glycogen [1]. The incidence is 1.4%–3%of all breast cancers, presenting at a median age of 57. There isdebate regarding this tumor’s behavior as some small seriesreport high axillary lymph nodal rate involvement of more than50% [53], whereas others report a much lower rate—35%(n = 20) [74].
imaging. There is not enough available data.
immunohistology. In a series of 20 patients, 35% and 30% werepositive to ER and PgR, respectively. In total, 20% presentedwith HER-2-positive status.
prognosis. Fewer than 100 cases have been reported; thus, itis difficult to draw definitive conclusions. Most authorshave found that this tumor has a poor prognosis butthere is no direct comparison to IDC-NOS based on stage[74, 75].
oncocytic carcinoma (malignant oncocytoma)
definition. The WHO classification requires >70% of the cells tobe oncocytic ones; however, only very few case reports arepublished. Thus, we have found that no significant conclusioncan be drawn.
Table 4. Poor prognosis typically ER-negative tumors
Dominant HER-2
profile %
Axillary lymph
node involvement %
Metaplastic 0–8 20 [64, 65]
Lipid rich 71 80 [66]
ER, estrogen receptor.
Annals of Oncology review
Volume 20 |No. 11 | November 2009 doi:10.1093/annonc/mdp245 | 1767

sebaceous carcinoma
definition and epidemiology. This carcinoma is characterized bya lobular or nested growth pattern of tumor cells variablyadmixed with those displaying sebaceous differentiation. Toour knowledge, only seven cases have been reported in theliterature with ages ranging from 43 to 83 years. Sebaceoustumor may precede internal malignancies and a geneticconsultation to rule out Muir–Torre Syndrome should beconsidered. A case with involved lymph node at presentationwas reported [76].
immunohistochemistry. The hormone receptor status istypically positive; however, two cases were reported to benegative. No HER-2 overexpression was detected. In threeanalyzed cases, the percentage of Ki-67-positive tumor cells wasrelatively high and ranged from 16% to 38% [77].
prognosis. Sebaceous carcinoma (SC) is generally felt to havea worse prognosis than other cutaneous carcinomas. Due tothe only scant published data, it is difficult to compare it withthe breast IDC-NOS. SC that had metastasized to the bone andskin was reported .The case may imply on its aggressivepotential [77, 78].
treatment data from the literature
These epithelial tumors are far too rare to have been studiedwith specific randomized clinical trials to determine theoptimal surgical, radiation, chemotherapeutic or endocrinetreatment. Although occasionally these rare tumor types havebeen included in large trials, the numbers are too small to drawany conclusions regarding their response to treatment. In mostsituations, they have been treated with standard therapy asthere are no data to indicate special protocols.Surgery is the first step of treatment of most of the early
breast cancers. The standard of care is lumpectomy/mastectomy with sentinel node biopsy (SNB). Many of thespecial types such as tubular, cribriform, medullary andmucinous have a low risk for regional involved lymph nodesbut without more data, it is not clear whether SNB can be safelyomitted.Adjuvant radiation therapy has shown its benefit in breast
cancer not only as a local control procedure but also asa treatment to prolong survival. ‘Favorable tumors’ tend tohave lower rate of local and distant recurrences. Whencomparing IDC-NOS to medullary, tubular and mucinoustypes, no statistically significant differences were found in thelocal–regional failure rate among the four groups. In total, 31%of TCs and up to 37.5% of ACCs that had been treated withexcision only developed local recurrence [33, 47, 79].The significant parameters were still the traditional ones:
age, margins, lymphovascular invasion and extensive DCIS[13, 39, 80].Baker has stated that pure TC <1 cm in size could be treated
by excision only [81]. However, the NSABP B-20 trial that hadrandomly assigned patients with small IDC tumors to yes/noadjuvant radiation could not find any subgroup which did notbenefit from radiation therapy [82]. The secretory type which istypically diagnosed in young girls represents a possibleexception since there is a strong effort to preserve the breast
bud without jeopardizing local control and to avoid rib, lungand other tissue damage. Thus, radiation may be omittedaccording to some experts but again, there is only scanty data.As we cannot create systemic treatment algorithms using
randomized trials with level one evidence due to the rarity of allthese tumors, can we use small case reports? Diab et al. foundthat axillary node involvement was a poor prognostic feature inmucinous carcinomas but not in TCs. Their conclusion wasthat systemic adjuvant therapy and node dissection may beavoided in many patients with TC [13]. This conclusion is inaccordance with the recent knowledge regarding the lack ofsensitivity of luminal A breast cancers to chemotherapy and therole of endocrine treatments [83, 84]. However, further dataare required before completely changing our guidelines forthese tumors.ACC as a histological definition appears to have both
prognostic and predictive significance by some authors as thereare concerns regarding the sensitivity of this subtype tochemotherapy based mainly on the documented low responserate in the head and neck adenoid cystic literature. There aredata that this tumor has some response to chemotherapy drugssuch as anthracyclines and 5-fluorouracil as well as moremodern agents such as paclitaxel [85, 86]. Large series,however, are not available.Recently, there has been interest in the platinum agents and
they have been incorporated into the arsenal of treatment of thetriple-negative or basal subtypes. Several studies had shownactivity of these agents in the metastatic and neoadjuvanttreatment but larger studies are still pending. Knowing thatphase III trial results for these rare types will not beforthcoming, can we make a leap and recommend platinumagent in the adjuvant setting for certain rare triple-negativesubtypes such as metaplastic or the aggressive small-celltumors? There is certainly rationale in administering adjuvantcisplatin regimen in SCC breast cancer. This tumor has anaggressive course and there are data showing a high rate ofresponse in small-cell lung and extrapulmonary metastaticdisease. If NE breast cancers are just another extrapulmonarysite of small-cell tumors, they may be treated in a similarfashion but we do need to remember that for the adjuvantbreast cancer setting, this is not an evidence-basedrecommendation. For other types of these tumors, furtherstudies are necessary before treatment algorithms canbe created.
summary
Rare epithelial breast cancers are a heterogeneous group ofmalignancies with different behaviors and prognoses. Althoughhistopathology has been our standard, there is now thequestion of whether it is time to apply new technologies such asmicroarrays and deep gene analysis to further understand theserare tumors. Are they all really unique subtypes or not? Canthey be classified according to their molecular or geneticfeatures? Are the older histological subtypes of value inunderstanding the behavior of these rare tumors and are theyreally classifying specific tumors or not?We have tried to classify these tumors with the data we have
currently on ER status and outcome. These broad groups of
review Annals of Oncology
1768 | Yerushalmi et al. Volume 20 |No. 11 | November 2009

estrogen-positive good outcome or poor outcome or similarestrogen-negative groups may be helpful in terms ofconceptualizing where we are going but need furtherassessment. As well, the poor prognosis of some of thesesubtypes reflects the need for a better adjuvant treatment andan understanding of these specific groups based on both theirhistological appearance and their molecular staining.We are proposing and organizing a consortium of
investigators from around the world to gather a sizable numberof these rare tumor types, assess the tumors centrally bymodern array technology and try to group these with outcomeand treatment data. This has been established for the commontumors and we have many leads as to their subclassificationbut a further analysis of these rare tumors is also needed. Thisexercise may provide the necessary information to begin tofurther understand the behavior of these tumors and to beginto classify them according to their relevant features.Subsequently, there may be a role for trials usinga contemporary classification to look at uniform treatmentmodalities and begin to establish treatment algorithms andguidelines. Until such time, we believe broad classifications intothe good and bad prognostic groups may be helpful for theclinician faced with a patient with one of these tumors and onlyanecdotal case histories for reference.
acknowledgement
The authors declare no conflict of interests.
references
1. Tavassoli FA, Devilee P. World Health Organization Classification of Tumors,
Tumors of the Breast and Female Genital Organs, 2nd edition. Lyon, France:
IARC Press 2003.
2. Kader HA, Jackson J, Mates D et al. Tubular carcinoma of the breast:
a population-based study of nodal metastases at presentation and of patterns of
relapse. Breast J 2001; 7(1): 8–13.
3. Leikola J, Heikkila P, von Smitten K et al. The prevalence of axillary lymph-node
metastases in patients with pure tubular carcinoma of the breast and sentinel
node biopsy. Eur J Surg Oncol 2006; 32(5): 488–491.
4. Page DL, Dixon JM, Anderson TJ et al. Invasive cribriform carcinoma of the
breast. Histopathology 1983; 7(4): 525–536.
5. Venable JG, Schwartz AM, Silverberg SG. Infiltrating cribriform carcinoma of the
breast: a distinctive clinicopathologic entity. Hum Pathol 1990; 21(3): 333–338.
6. Li CI, Uribe DJ, Daling JR. Clinical characteristics of different histologic types of
breast cancer. Br J Cancer 2005; 93(9): 1046–1052.
7. Di Saverio S, Gutierrez J, Avisar E. A retrospective review with long term follow
up of 11,400 cases of pure mucinous breast carcinoma. Breast Cancer Res
Treat 2008; 111(3): 541–547.
8. Otsuki Y, Yamada M, Shimizu S et al. Solid-papillary carcinoma of the breast:
clinicopathological study of 20 cases. Pathol Int 2007; 57(7): 421–429.
9. O’Malley FP, Bane A. An update on apocrine lesions of the breast.
Histopathology 2008; 52(1): 3–10.
10. Lopez-Bonet E, Alonso-Ruano M, Barraza G et al. Solid neuroendocrine breast
carcinomas: incidence, clinico-pathological features and immunohistochemical
profiling. Oncol Rep 2008; 20(6): 1369–1374.
11. Gunhan-Bilgen I, Oktay A. Mammographic features of local recurrence after
conservative surgery and radiation therapy: comparison with that of the primary
tumor. Acta Radiol 2007; 48(4): 390–397.
12. Oakley GJ III, Tubbs RR, Crowe J et al. HER-2 amplification in tubular carcinoma
of the breast. Am J Clin Pathol 2006; 126(1): 55–58.
13. Diab SG, Clark GM, Osborne CK et al. Tumor characteristics and clinical outcome
of tubular and mucinous breast carcinomas. J Clin Oncol 1999; 17(5):
1442–1448.
14. Cabral AH, Recine M, Paramo JC et al. Tubular carcinoma of the breast: an
institutional experience and review of the literature. Breast J 2003; 9(4):
298–301.
15. Stutz JA, Evans AJ, Pinder S et al. The radiological appearances of invasive
cribriform carcinoma of the breast. Nottingham Breast Team. Clin Radiol 1994;
49(10): 693–695.
16. Soomro S, Shousha S, Taylor P et al. c-erbB-2 expression in different histological
types of invasive breast carcinoma. J Clin Pathol 1991; 44(3): 211–214.
17. Barkley CR, Ligibel JA, Wong JS et al. Mucinous breast carcinoma: a large
contemporary series. Am J Surg 2008; 196(4): 549–551.
18. Memis A, Ozdemir N, Parildar M et al. Mucinous (colloid) breast cancer:
mammographic and US features with histologic correlation. Eur J Radiol 2000;
35(1): 39–43.
19. Kawashima M, Tamaki Y, Nonaka T et al. MR imaging of mucinous carcinoma of
the breast. AJR Am J Roentgenol 2002; 179(1): 179–183.
20. Okafuji T, Yabuuchi H, Sakai S et al. MR imaging features of pure mucinous
carcinoma of the breast. Eur J Radiol 2006; 60(3): 405–413.
21. Reiner A, Reiner G, Spona J et al. Histopathologic characterization of human
breast cancer in correlation with estrogen receptor status. A comparison of
immunocytochemical and biochemical analysis. Cancer 1988; 61(6):
1149–1154.
22. Kim TH, Kang DK, Kim SY et al. Sonographic differentiation of benign and
malignant papillary lesions of the breast. J Ultrasound Med 2008; 27(1): 75–82.
23. Fisher ER, Palekar AS, Redmond C et al. Pathologic findings from the national
surgical adjuvant breast project (protocol no. 4). VI. Invasive papillary cancer. Am
J Clin Pathol 1980; 73(3): 313–322.
24. Fisher ER, Anderson S, Redmond C et al. Pathologic findings from the national
surgical adjuvant breast project protocol B-06. 10-year pathologic and clinical
prognostic discriminants. Cancer 1993; 71(8): 2507–2514.
25. Miller WR, Shivas AA, Franchimont P et al. Breast gross cystic disease protein 15
in human breast cancer in culture. Eur J Cancer Clin Oncol 1988; 24(2):
223–228.
26. Japaze H, Emina J, Diaz C et al. ‘Pure’ invasive apocrine carcinoma of the
breast: a new clinicopathological entity? Breast 2005; 14(1): 3–10.
27. Makretsov N, Gilks CB, Coldman AJ et al. Tissue microarray analysis of
neuroendocrine differentiation and its prognostic significance in breast cancer.
Hum Pathol 2003; 34(10): 1001–1008.
28. Weigelt B, Horlings HM, Kreike B et al. Refinement of breast cancer classification
by molecular characterization of histological special types. J Pathol 2008;
216(2): 141–150.
29. Sapino A, Papotti M, Righi L et al. Clinical significance of neuroendocrine
carcinoma of the breast. Ann Oncol 2001; 12 (Suppl 2): S115–S117.
30. Vu-Nishino H, Tavassoli FA, Ahrens WA, Haffty BG. Clinicopathologic features
and long-term outcome of patients with medullary breast carcinoma managed
with breast-conserving therapy (BCT). Int J Radiat Oncol Biol Phys 2005; 62(4):
1040–1047.
31. Vieni S, Cabibi D, Cipolla C et al. Secretory breast carcinoma with metastatic
sentinel lymph node. World J Surg Oncol 2006; 4: 88.
32. Page DL. Adenoid cystic carcinoma of breast, a special histopathologic type with
excellent prognosis. Breast Cancer Res Treat 2005; 93(3): 189–190.
33. Millar BA, Kerba M, Youngson B et al. The potential role of breast conservation
surgery and adjuvant breast radiation for adenoid cystic carcinoma of the breast.
Breast Cancer Res Treat 2004; 87(3): 225–232.
34. Reis-Filho JS, Natrajan R, Vatcheva R et al. Is acinic cell carcinoma a variant of
secretory carcinoma? A FISH study using ETV6#split apart’ probes.Histopathology 2008; 52(7): 840–846.
35. Linda A, Londero V, Mazzarella F et al. Rare breast neoplasms: is there any
peculiar feature on magnetic resonance mammography? Radiol Med (Torino)
2007; 112(6): 850–862.
36. Majid AS, de Paredes ES, Doherty RD et al. Missed breast carcinoma: pitfalls and
pearls. Radiographics 2003; 23(4): 881–895.
Annals of Oncology review
Volume 20 |No. 11 | November 2009 doi:10.1093/annonc/mdp245 | 1769
37. Vincent-Salomon A, Gruel N, Lucchesi C et al. Identification of typical medullary
breast carcinoma as a genomic sub-group of basal-like carcinomas,
a heterogeneous new molecular entity. Breast Cancer Res 2007; 9(2): R24.
38. Xu R, Feiner H, Li P et al. Differential amplification and overexpression of HER-2/
neu, p53, MIB1, and estrogen receptor/progesterone receptor among
medullary carcinoma, atypical medullary carcinoma, and high-grade invasive
ductal carcinoma of breast. Arch Pathol Lab Med 2003; 127(11):
1458–1464.
39. Thurman SA, Schnitt SJ, Connolly JL et al. Outcome after breast-conserving
therapy for patients with stage I or II mucinous, medullary, or tubular breast
carcinoma. Int J Radiat Oncol Biol Phys 2004; 59(1): 152–159.
40. Mun SH, Ko EY, Han BK et al. Secretory carcinoma of the breast: sonographic
features. J Ultrasound Med 2008; 27(6): 947–954.
41. Tognon C, Knezevich SR, Huntsman D et al. Expression of the ETV6-NTRK3 gene
fusion as a primary event in human secretory breast carcinoma. Cancer Cell
2002; 2(5): 367–376.
42. McClenathan JH, de la Roza G. Adenoid cystic breast cancer. Am J Surg 2002;
183(6): 646–649.
43. Azoulay S, Lae M, Freneaux P et al. KIT is highly expressed in adenoid cystic
carcinoma of the breast, a basal-like carcinoma associated with a favorable
outcome. Mod Pathol 2005; 18(12): 1623–1631.
44. Trendell-Smith NJ, Peston D, Shousha S. Adenoid cystic carcinoma of the
breast: a tumour commonly devoid of oestrogen receptors and related proteins.
Histopathology 1999; 35(3): 241–248.
45. Arpino G, Clark GM, Mohsin S et al. Adenoid cystic carcinoma of the breast:
molecular markers, treatment, and clinical outcome. Cancer 2002; 94(8):
2119–2127.
46. Kleer CG, Oberman HA. Adenoid cystic carcinoma of the breast: value of
histologic grading and proliferative activity. Am J Surg Pathol 1998; 22(5):
569–575.
47. Leeming R, Jenkins M, Mendelsohn G. Adenoid cystic carcinoma of the breast.
Arch Surg 1992; 127(2): 233–235.
48. Tanahashi C, Yabuki S, Akamine N et al. Pure acinic cell carcinoma of the breast
in an 80-year-old Japanese woman. Pathol Int 2007; 57(1): 43–46.
49. Peintinger F, Leibl S, Reitsamer R et al. Primary acinic cell carcinoma of the
breast: a case report with long-term follow-up and review of the literature.
Histopathology 2004; 45(6): 645–648.
50. Sadanaga N, Okada S, Shiotani S et al. Clinical characteristics of small cell
carcinoma of the breast. Oncol Rep 2008; 19(4): 981–985.
51. Zekioglu O, Erhan Y, Ciris M et al. Invasive micropapillary carcinoma of the
breast: high incidence of lymph node metastasis with extranodal extension and
its immunohistochemical profile compared with invasive ductal carcinoma.
Histopathology 2004; 44(1): 18–23.
52. Walsh MM, Bleiweiss IJ. Invasive micropapillary carcinoma of the breast: eighty
cases of an underrecognized entity. Hum Pathol 2001; 32(6): 583–589.
53. Rosen PP. Rosen’s Breast Pathology, 2nd edition. Philadelphia, PA: Lippincott
Williams &Wilkins 2001.
54. Bigotti G, Coli A, Butti A et al. Primary small cell neuroendocrine carcinoma of
the breast. J Exp Clin Cancer Res 2004; 23(4): 691–696.
55. Sapino A, Righi L, Cassoni P et al. Expression of the neuroendocrine phenotype
in carcinomas of the breast. Semin Diagn Pathol 2000; 17(2): 127–137.
56. Shin SJ, DeLellis RA, Ying L et al. Small cell carcinoma of the breast:
a clinicopathologic and immunohistochemical study of nine patients. Am J Surg
Pathol 2000; 24(9): 1231–1238.
57. Mariscal A, Balliu E, Diaz R et al. Primary oat cell carcinoma of the breast:
imaging features. AJR Am J Roentgenol 2004; 183(4): 1169–1171.
58. Kitakata H, Yasumoto K, Sudo Y et al. A case of primary small cell carcinoma of
the breast. Breast Cancer 2007; 14(4): 414–419.
59. Luna-More S, Casquero S, Perez-Mellado A et al. Importance of estrogen
receptors for the behavior of invasive micropapillary carcinoma of the breast.
Review of 68 cases with follow-up of 54. Pathol Res Pract 2000; 196(1):
35–39.
60. Kim MJ, Gong G, Joo HJ et al. Immunohistochemical and clinicopathologic
characteristics of invasive ductal carcinoma of breast with micropapillary
carcinoma component. Arch Pathol Lab Med 2005; 129(10): 1277–1282.
61. Gunhan-Bilgen I, Zekioglu O, Ustun EE et al. Invasive micropapillary carcinoma of
the breast: clinical, mammographic, and sonographic findings with
histopathologic correlation. AJR Am J Roentgenol 2002; 179(4): 927–931.
62. Nassar H, Qureshi H, Volkanadsay N et al. Clinicopathologic analysis of solid
papillary carcinoma of the breast and associated invasive carcinomas. Am J Surg
Pathol 2006; 30(4): 501–507.
63. Chen L, Fan Y, Lang RG et al. Breast carcinoma with micropapillary features:
clinicopathologic study and long-term follow-up of 100 cases. Int J Surg Pathol
2008; 16(2): 155–163.
64. Pezzi CM, Patel-Parekh L, Cole K et al. Characteristics and treatment of
metaplastic breast cancer: analysis of 892 cases from the National Cancer Data
Base. Ann Surg Oncol 2007; 14(1): 166–173.
65. Wargotz ES, Deos PH, Norris HJ. Metaplastic carcinomas of the breast. II.
Spindle cell carcinoma. Hum Pathol 1989; 20(8): 732–740.
66. Shi P, Wang M, Zhang Q, Sun J. Lipid-rich carcinoma of the breast. A
clinicopathological study of 49 cases. Tumori 2008; 94(3): 342–346.
67. Luini A, Aguilar M, Gatti G et al. Metaplastic carcinoma of the breast, an unusual
disease with worse prognosis: the experience of the European Institute Of Oncology
and review of the literature. Breast Cancer Res Treat 2007; 101(3): 349–353.
68. Tavassoli FA. Classification of metaplastic carcinomas of the breast. Pathol Annu
1992; 27(Pt 2): 89–119.
69. Tse GM, Tan PH, Putti TC et al. Metaplastic carcinoma of the breast:
a clinicopathological review. J Clin Pathol 2006; 59(10): 1079–1083.
70. Velasco M, Santamaria G, Ganau S et al. MRI of metaplastic carcinoma of the
breast. AJR Am J Roentgenol 2005; 184(4): 1274–1278.
71. Reis-Filho JS, Milanezi F, Steele D et al. Metaplastic breast carcinomas are
basal-like tumours. Histopathology 2006; 49(1): 10–21.
72. Hennessy BT, Krishnamurthy S, Giordano S et al. Squamous cell carcinoma of
the breast. J Clin Oncol 2005; 23(31): 7827–7835.
73. Ramos CV, Taylor HB. Lipid-rich carcinoma of the breast. A clinicopathologic
analysis of 13 examples. Cancer 1974; 33(3): 812–819.
74. Kuroda H, Sakamoto G, Ohnisi K et al. Clinical and pathological features of
glycogen-rich clear cell carcinoma of the breast. Breast Cancer 2005; 12(3):
189–195.
75. Hayes MM, Seidman JD, Ashton MA. Glycogen-rich clear cell carcinoma of the
breast. A clinicopathologic study of 21 cases. Am J Surg Pathol 1995; 19(8):
904–911.
76. Alzaraa A, Ghafoor I, Yates A et al. Sebaceous carcinoma of the skin of the
breast: a case report. J Med Case Reports 2008; 2: 276.
77. Hisaoka M, Takamatsu Y, Hirano Y et al. Sebaceous carcinoma of the breast:
case report and review of the literature. Virchows Arch 2006; 449(4): 484–488.
78. Cibull TL, Thomas AB, Badve S et al. Sebaceous carcinoma of the nipple. J
Cutan Pathol 2008; 35(6): 608–610.
79. Holland DW, Boucher LD, Mortimer JE. Tubular breast cancer experience at
Washington University: a review of the literature. Clin Breast Cancer 2001; 2(3):
210–214.
80. Vo T, Xing Y, Meric-Bernstam F et al. Long-term outcomes in patients with
mucinous, medullary, tubular, and invasive ductal carcinomas after lumpectomy.
Am J Surg 2007; 194(4): 527–531.
81. Baker RR. Unusual lesions and their management. Surg Clin North Am 1990;
70(4): 963–975.
82. Fisher B, Jeong JH, Dignam J et al. Findings from recent national surgical
adjuvant breast and bowel project adjuvant studies in stage I breast cancer. J
Natl Cancer Inst Monogr 2001; 30: 62–66.
83. Goldstein NS, Decker D, Severson D et al. Molecular classification system
identifies invasive breast carcinoma patients who are most likely and those who
are least likely to achieve a complete pathologic response after neoadjuvant
chemotherapy. Cancer 2007; 110(8): 1687–1696.
84. Penault-Llorca F, Cayre A, Bouchet Mishellany F et al. Induction chemotherapy
for breast carcinoma: predictive markers and relation with outcome. Int J Oncol
2003; 22(6): 1319–1325.
85. Laurie SA, Licitra L. Systemic therapy in the palliative management of advanced
salivary gland cancers. J Clin Oncol 2006; 24(17): 2673–2678.
86. Till BG, Martins RG. Response to paclitaxel in adenoid cystic carcinoma of the
salivary glands. Head Neck 2008; 30(6): 810–814.
review Annals of Oncology
1770 | Yerushalmi et al. Volume 20 |No. 11 | November 2009