tobacco treatment in people with schizophrenia · tobacco treatment in people with schizophrenia...
TRANSCRIPT

Tobacco Treatment in People with Schizophrenia Tony P. George, MD, FRCPC Chief, Addictions Division, CAMH Professor and Co-Director, Division of Brain and Therapeutics, Department of Psychiatry, University of Toronto
ECHO-TEACH Talk, MD Anderson Cancer Center, February 7, 2017

Learning Objectives:
Slide 2 3/30/2016
n Develop an evidence-based approach to assessment and treatment for tobacco use disorder in people with schizophrenia and other serious mental illness.
n Understand an approach to developing a tobacco-free mental health and addictions facility for the benefit of patients, staff and visitors
Medical Impact of Tobacco
Slide 3
n Tobacco use is the leading cause of preventable death in Western world (Giovino, GA, 2007)
n Over 470,000 deaths per year in USA and >50,000 annual deaths in Canada attributable to tobacco addiction (George, TP, 2015. Chapter 32, Cecil Textbook of Medicine, 25th Edition)
n Significant contributor to cardiovascular, pulmonary disease and to many cancers (e.g. lung, throat) (George, 2015)
n Reducing smoking leads to some health improvements (e.g. better breathing and exercise tolerance), but reductions in cardiac, pulmonary and oncological disease are only seen when quitting smoking (George, 2015)
Slide 4
Mental Health Impact of Tobacco n Higher rates of smoking in mentally ill (MI) populations makes them more
vulnerable to tobacco-related medical illness (Mackowick et al., 2012)
n People with MI spend up to 25% of their disability income on tobacco (Ziedonis et al., 2008)
n Tobacco addiction shortens the lives of people with MI by 12-13 years (Wiliams et al., 2011)
n Rates of quitting smoking for MI smokers are 1/3 to 1/2 rates in the general population (Morisano et al., 2009)
n Quitting smoking in MI populations leads to better psychiatric and substance use disorder outcomes, including reductions in depression and alcohol use, and less suicidal behaviours and aggression (Mackowick et al., 2012; Morozova et al., 2015)
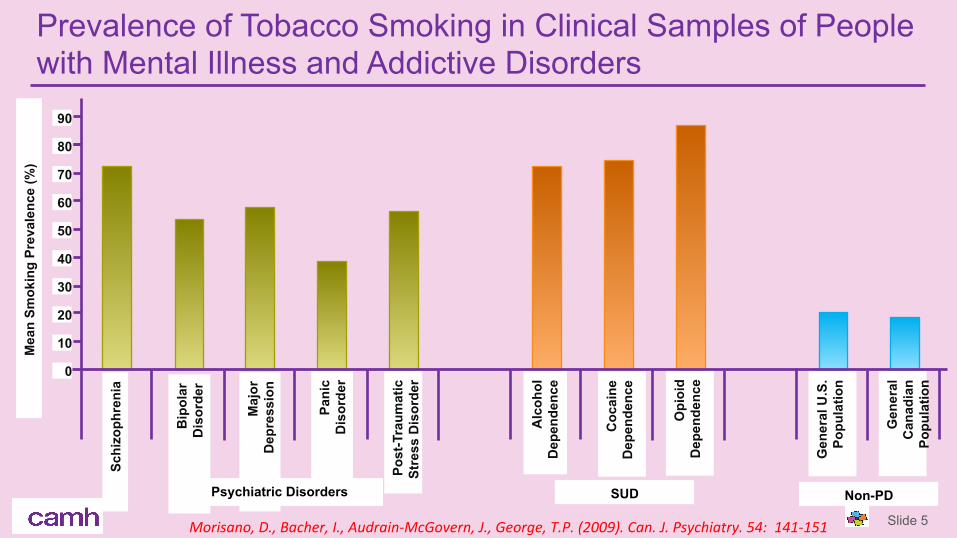
Prevalence of Tobacco Smoking in Clinical Samples of People with Mental Illness and Addictive Disorders
Schi
zoph
reni
a
Bip
olar
Dis
orde
r
Maj
or
Dep
ress
ion
Slide 5 Morisano,D.,Bacher,I.,Audrain-McGovern,J.,George,T.P.(2009).Can.J.Psychiatry.54:141-151
Mea
n Sm
okin
g Pr
eval
ence
(%)
Pani
c D
isor
der
Post
-Tra
umat
ic St
ress
Dis
orde
r
Alc
ohol
Dep
ende
nce
Coc
aine
D
epen
denc
e
Opi
oid
Dep
ende
nce
Gen
eral
U.S
. Po
pula
tion
Gen
eral
Can
adia
n Po
pula
tion
Psychiatric Disorders SUD Non-PD
0
10
20
30
40
50
60
70
80
90

Current Smoking among Adults Aged 18 or Older
Based on Serious Psychological Distress Status of Previous Month (NHIS, 1997 to 2011)
Slide 6
*DifferencebetweenesKmateandesKmatefor2011isstrategicallysignificantatthe0.5level
Perc
ent %
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 0
10
20
30
40
50

Slide 7
Tobacco Bans in Hospital Settings
Mossetal.,Am.J.Addict.2010
Disadvantages
n Inpatients generally not interested in quitting, as this is low on their “hierarchy of needs”
n Staff are often reluctant as it can be perceived as a distraction to treatment plans, and is a critical “positive” reinforcer
n Lack of training of unit staff or other qualified people to conduct smoking cessation counseling
n Unmotivated inpatients pose a barrier to success of those few patients wanting to quit
LawnandPols,2005;Mossetal.,2010
Advantages
n Great opportunity to provide motivational interventions for those not initially willing to try to quit (a “teachable moment”)
n Reduction in episodes of seclusion and restraint, decreased PRN* use and Length Of Stay (LOS)
n The goals of a smoke-free work environment are promoted and are consistent with wellness interventions that are being implemented in most inpatient settings
*PRN–KnownasmedicaKonsthataretaken“asneeded”

Key Elements of Tobacco Free CAMH
Slide 8
1. No Smoking (or Vaping) at any campus site (2 main campuses + outpatient satellites)
2. No Possession of Tobacco Products on the Premises
3. Presence of Community “Ambassadors”, Patients and Staff who promote tobacco-free CAMH though a Wellness and Recovery Culture using a positive reinforcement approach and act as “Champions” for the Initiative

Pre-Launch N=454
Post-Launch N=356
Pre-Launch N=123
Post-Launch N=106
Staff and Patient Attitudinal Survey Results
Slide 9
Patient
Staff 10 % n Increase in staff confidence in having appropriate access to team / management support or
training required to comply with the tobacco-free policy (12% to 22%)
7 %
n Increase in awareness of how to help / where to refer a client if they want to quit (13% to 20%)
19 % n Increase in the support of the creation of a tobacco-free policy at CAMH (48% to 67%)
17 % n Increase in the belief that lowering tobacco use on CAMH property is important (51% to 68%)
16 % n Increase in contributing to the success of the policy by not smoking at CAMH (56% to 72%)
Riad-Allen et al., 2016. Am. J. Addict., in press

Effects of CAMH Tobacco Free on Aggression (Code Whites)
Slide 10
Riad-Allen, L. et al. (2017). Am. J. Addict., in press
*p<0.05

An approach to tobacco cessation in smokers with schizophrenia
Slide 11
Quitting smoking is easy – I’ve done it several hundred times …
- Mark Twain

Case #1 n 40 year old black male with schizophrenia, never married, lives in a shelter in
a major city.
n Smokes 3 packs per day (illegal cigarettes), first cigarette is within 2 minutes of awakening. He also started smoking e-cigarettes (“Vapes”).
n Multiple quit attempt failures since started smoking at age 14. Has tried all NRTs (gum, patch, inhaler)
n Psychosis is well-managed with depot antipsychotic (Risperidone Consta), at 50 mg qmonth. Takes some oral risperidone for breakthru symptoms
n Family Hx+ for CAD, Lung CA. He himself had anterior wall MI 6 months ago, after months of chest pain, took himself to local general hospital.
n He doesn’t really want to quit, but does not want to die from (another) MI …

Question
n What can we do for this man?
17-02-08 14

Vulnerabilitymarkersfortobaccoaddic4oninschizophrenia
Wing, VC et al. (2012). Ann. NY Acad. Sci. 1249: 89-106

Reduced Smoking – A Viable Target or Not?
n Many smokers are simply unable to quit smoking.
n Should sustained reductions in smoking been considered a goal of tobacco treatment or should reduction be a transitional goal towards eventual smoking abstinence (Hughes, 2002; George and Vessicchio, 2002; McChargue et al., 2002)?
n A recent study suggests that sustained smoking reductions (50% reduction) do not reduce cancer or cardiac disease risk (Tverdall and Bjartveit, 2006).

BiobehaviouralVulnerabilityFactorstoTobaccoAddic4oninSchizophrenian Biochemical(reducednAChRlevels,higherbaselinenico8nelevelsinSzversusControls)
n Gene8c(α7nAChR,α3nAChR,COMT,DISC1,Reelin)
n Behavioral(deficitsinreinforcement/reward)
n Neurocogni8ve(neurophysiological/neuropsychological)
Wing, VC et al., 2012. Ann. NY Acad. Sci. 1248-89-106
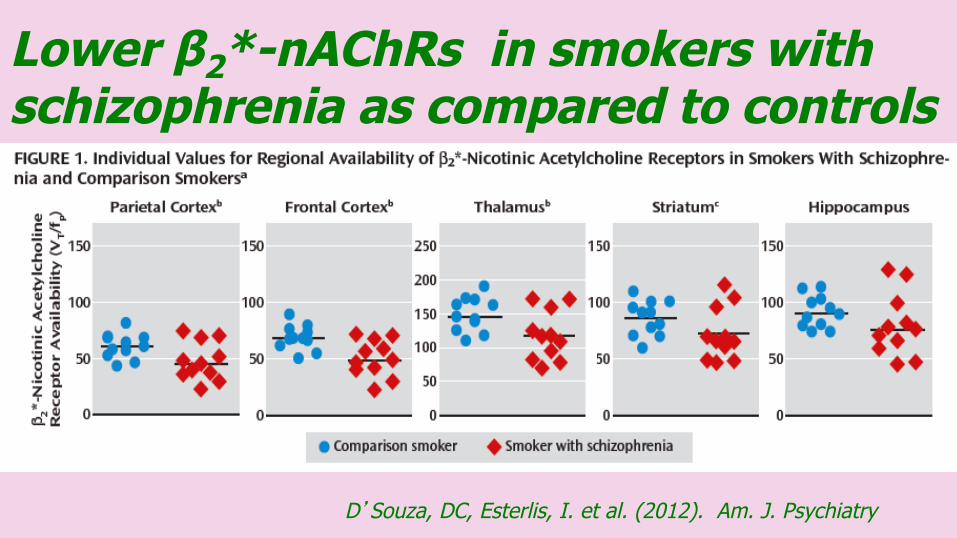
Lower β2*-nAChRs in smokers with schizophrenia as compared to controls
D’Souza, DC, Esterlis, I. et al. (2012). Am. J. Psychiatry

BehavioralFactors–MecamylamineEffectsonReinforcement,Consump4onandRelapseTopography – Puff Volume
McKee et al (2009). Schizophrenia Res.
Smoking Cue-Reactivity
* *p<0.05 vs. PLO
*p<0.05 vs 10 mg/day
Fonder et al. (2005). Biol. Psychiatry
Consumption (Cigarettes/Session)
Weinberger et al (2007). Schizophrenia Res.
*p<0.05 vs. PLO
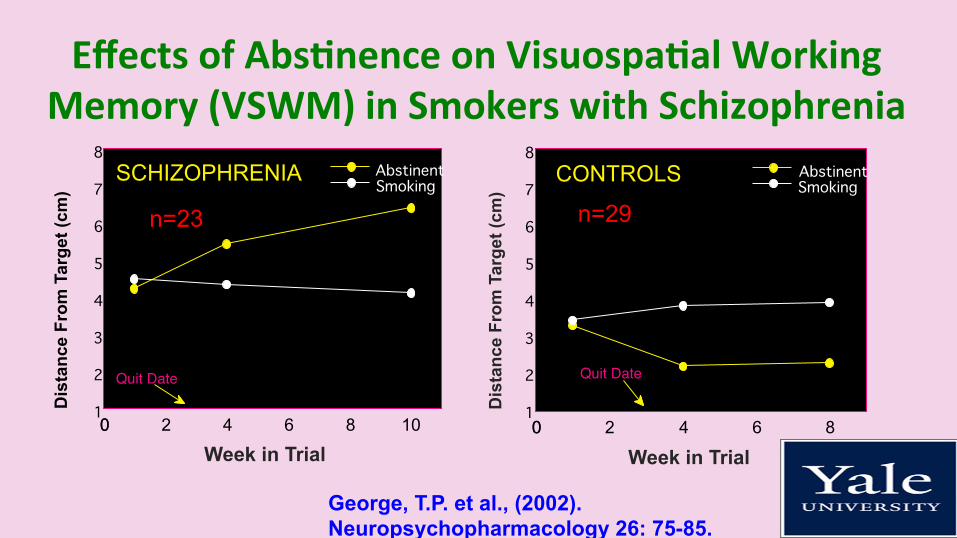
EffectsofAbs4nenceonVisuospa4alWorkingMemory(VSWM)inSmokerswithSchizophrenia
10 8 6 4 2 0 0 1 2 3 4 5 6 7 8
Abstinent Smoking
Week in Trial
Dis
tanc
e Fr
om T
arge
t (cm
)
Quit Date
SCHIZOPHRENIA
8 6 4 2 0 0
Abstinent Smoking
Week in Trial D
ista
nce
From
Tar
get (
cm)
Quit Date
CONTROLS
n=23 n=29
George, T.P. et al., (2002). Neuropsychopharmacology 26: 75-85.
1 2 3 4 5 6 7 8

Selec4veEnhancementofVSWMbyCigareJeSmokinginSchizophrenia:BlockadebyMecamylamine
* * p = 0.001 vs. 5 mg/day * p < 0.001 vs. 10 mg/day p < 0.001 vs. CON Diagnosis x Dose: F=10.65, df=2,128, p<0.01
Sacco, K.A., Termine, A. et al. (2005). Arch. Gen. Psychiatry. 62: 649-659.

DeficitsinFrontal-Execu4vePerformancePredictSmokingCessa4onFailureinSchizophrenia
Schizophrenia
p=0.052
Dolan, S.L., Sacco, K.A. et al., (2004). Schizophrenia Res. 70: 263-275.
Trail Making Test - Part B
020406080
100120140160
Quit Not Quit
Quit Status at Trial Endpoint
Numb
er of
Seco
nds.
Digit Span Backward
012345678
Quit Not Quit
Quit Status at Trial Endpoint
Numb
er of
Digits.
p<0.05
Moss, T.G. et al. (2009). Drug Alcohol Depend. 104: 94-99.
p<0.05

Cor4calDopamineFunc4onandSpa4alWorkingMemory
George, T.P. et al., 2003, APPI
14 12 10 8 6 4 2 0 0 0
25
50
75
100
125
CORTICAL DOPAMINE ACTIVITY SPAT
IAL
WO
RK
ING
MEM
ORY
(%)
NORMAL
SCHIZOPHRENIA STRESS
Smoking Smoking

Atypical Versus Typical Antipsychotic Drugs and Nicotine Patch for Smoking Cessation in Schizophrenia (N=45)
George, T.P. et al. (2000). Am. J. Psychiatry. 157: 1835-1842.
*p<0.05 vs. Typical
Endpoint Last Four Weeks 6-Month F/U 0
25
50
75 Atypical Typical
Smok
ing
Abs
tinen
ce R
ate
(%)
*
*
*

Combina4onofTransdermalNico4neandBupropionSRisSuperiortoPlacebo+PatchforSmokingCessa4oninSchizophrenia(N=58)
34.5
10.3
27.6
3.4
16
00
5
10
15
20
25
30
35
% S
mok
ing A
bstin
ence
..
EndpointAbstinence
ContinuousAbstinence
Six MonthAbstinence
BUPPlacebo*
*
Fisher’s Exact Test + p = 0.056 * p < 0.05 # p=0.11
George, T.P., Vessicchio, J.C. et al. (2008). Biol. Psychiatry. 63: 1092-1096.
#

Varenicline (Champix®) n An α4β2-selective nAChR partial agonist
n Approved by the FDA in May, 2006 and by Health Canada in April, 2007.
n In Phase III clinical trials, demonstrated superiority to both bupropion SR and placebo in continuous abstinence outcomes (Gonzalez et al., 2006, Jorenby et al., 2006)
n Prevents smoking-relapse with treatment up to 24 weeks (Tonstad et al., 2006).
n Dosing regimen is 0.5 mg qd x 3 days, then 0.5 mg bid x 4 days, then up to 1.0 mg bid for 12 weeks, with a label to extend treatment to 24 weeks as necessary.

Varenicline– Side Effects n Main side effects are nicotine-like: Nausea (~30%), insomnia, headache and
abnormal dreams.
n Black Box warnings issued by FDA, Health Canada and EMEA regarding anecdotal reports of treatment-emergent suicidality, homocidality, aggression, psychosis and mania – needs further study.

Cigarette Smoking, Cytochrome P450 and Psychotropic Drug Plasma Levels
n Metabolized by CYP 1A2/3A4
n Clozapine
n Olanzapine
n Haloperidol
n Chlorpromazine
n Caffeine
n Not Metabolized
n Risperidone
n Ziprasidone
n Aripiprazole
n Quetiapine
n Bupropion
n SSRI’s DeLeon, J. (2004). Psychiatric Serv. 55: 491-493.
VareniclineandPsychiatricPopula4onsn Severalcasereportsbothpublished(Freedman,2007;KohenandKremen,2007)andunpublished(FDAMedwatch)implica8ngvareniclineinneuropsychiatrictreatment-emergentadverseevents(TEAEs),includingsuicidality,homicidality,psychosisandmania(O’Malley,2010).
n However,clinicalstudiescomparingPsychiatricHx+toHx-smokersinvareniclinetreatmentsuggestthattreatmentoutcomesandadverseeventsarecomparable(e.g.Stapletonetal.,2008;McClureetal.,2010).
n Recentcontrolledstudiessupportitssafetyandefficacyinschizophrenia,,includinginabs8nence-ini8a8on(Williamsetal.,2012.J.Clin.Psychiatry;Anthenelli,RMetal.2016Lancet)andrelapse-preven8on(Evinsetal.,2014.JAMA)studies.
n Fourstudiessuggestsitssafetyandefficacyinsmokerswithbipolardisorder(Weinbergeretal.,2008;Wuetal.,2012;Fryeetal.,2013;Chengappaetal.,2014)

VareniclineforSmokingCessa4oninPeoplewithSchizophrenia(N=127)
Williams, J.M., Anthenelli, R.M., Morris, C., Tredow, J., Thompson, J.R., Yunis, C., George, T.P. (2012). J. Clin. Psychiatry. 73: 654-660.

VareniclineEffectsonPosi4veandNega4veSymptomsinSmokerswithSchizophrenia
Williams, J.M. et al. (2012). J. Clin. Psychiatry.73: 654-660.

Evins,AEetal.,JAMA.311:145-154.

17-02-08 33
EAGLES Study – Randomized Comparison of Varenicline, Bupropion SR, Nicotine Patch and Placebo for Smoking Cessation in Mentally Ill versus
Non-Mentally Ill Smokers (N=8144)
Anthenelli, R.M. et al. (2016). Lancet. 387: 2507-2520.
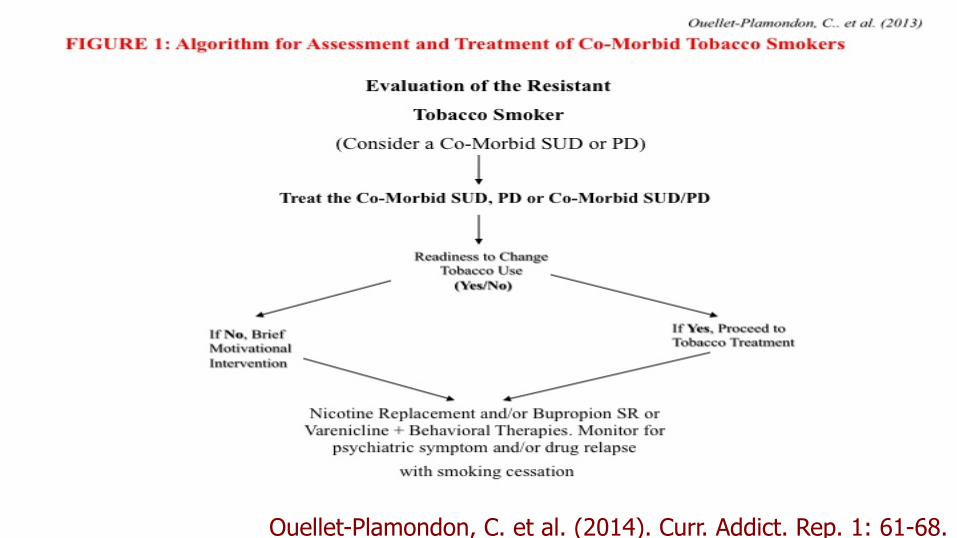
Ouellet-Plamondon, C. et al. (2014). Curr. Addict. Rep. 1: 61-68.

n Stimulates the cortex by trains of magnetic pulses.
n Frequencies of 1 to 50Hz
n rTMS has recently been used to treat neuropsychiatric disorders (e.g. depression, schizophrenia, parkinson’s disease)
epetitive ranscranial agnetic timulation
r T M S
Caroline Wass, Ph.D.

Factor 1
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Factor 2
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Desire to Smoke
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Anticipation of positive effects of smoking
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Anticipation of relief from withdrawal after smoking
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Intention to Smoke
3
3.5
4
4.5
5
5.5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Factor 1
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Factor 2
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Desire to Smoke
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Anticipation of positive effects of smoking
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Anticipation of relief from withdrawal after smoking
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Factor 1
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Factor 2
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Desire to Smoke
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Anticipation of positive effects of smoking
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Anticipation of relief from withdrawal after smoking
2.5
3
3.5
4
4.5
5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
Intention to Smoke
3
3.5
4
4.5
5
5.5
Pre-rTMS Post-rTMS
TQSU
score
Active rTMS (n=4)
Sham rTMS (n=6)
rTMS reduces tobacco cravings in patients with schizophrenia
Wing, VC et al, (2012) Schizophr. Res. 139: 264-266.