torfaen north neighbourhood care network action plan 2015-16 north ncn action plan... · on-going...
TRANSCRIPT

1
Torfaen North Neighbourhood Care Network Action Plan 2015-16

2
Torfaen North Draft Action Plan 2015-16
Strategic Aim 1: To understand the needs of the population served by the Network
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
Progress/RAG
1.1 Smoking
1.1.1 Smokers in the NCN
area quit smoking (SEE
APPENDIX 1 – ACTION
PLAN)
Retained as a local
priority 2015-16 –
agreed 16.07.15
Links to Communities First Healthy Lifestyles project
Links to ABUHB Service Change Plan No. 3 Links to MIND – ‘you in mind’ project for young people
• Build on 2014/15
• Review data on uptake of
services and quit rates at
NCN meetings including
with non-medical members
• Recovery plan if progress
• Increase number of
Smoking Champions
Number of smokers is
reduced in line with
target i.e. 5% of smokers
make quit attempt with
at least 40% CO
validation quit rate at 4
weeks
PH/SSW
NCN
Third Sector
Social
Services
31.3.16 Torfaen action plan
developed
ABUHB R&D poster
developed
Networks team working
with PHW to secure
current data – issues with
SSW data systems
redesign leading to delays
Management Team
Priority
Highest number of
smoking champions in Pan
NCN area
Highest referral rate to
SSW in Pan NCN area
1.2 Engagement
1.2.1 NEW: Identify a range
of methods to increase
awareness of the work
of the NCN & partners
Links to Torfaen SIP
Map options
Continue to up-date ABUHB
intranet page
To support development of
a public facing web-page
To support the work of the
ABUHB engagement team
in implementing the
engagement strategy
To attend at least two
‘listening events’ in 2015-
16
Feedback analysis leads
to evidence to inform
improved service delivery
with increased patient
satisfaction
NCN /
TVA /
Commun-
ities First /
Bron Afon
Housing
31.3.16 Identified as a shared
outcome in the Torfaen
SIP
Links made with ABUHB
Engagement Team to
identify Torfaen specific
events
Strategic Aim 2: To ensure the sustainability of core GP services and access arrangements that meet the reasonable needs of
local patients
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
Progress/RAG
2.1 Access
2.1.1 Identify and share good
practice across GP
• Map which strategies have
been adopted to reduce
Maximise use of
appointment slots to
NCN /
Practices /
31.3.16 Gwent wide access SCP for
2015-16

3
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
Progress/RAG
Practices to reduce DNA
rates
Adopted as a local
priority 2015-16 –
agreed 16.07.15
Links to ABUHB Service Change Plan No. 3
DNAs
• Use PDP reports (28.11.14
– embedded) as a baseline
• Engage non-clinical
members
reduce wasted time
within Practices
AMD / NCN
leads / LMC Cluster Level Report - Measure 44 - GP DNA Rates -October 2015.docx
2.1.2 NEW: Contracted
Services: To engage
with and utilise skills of
other Primary Care
services i.e.
Optometrists,
Pharmacists & Dentists
Links to ABUHB Service Change Plan No. 3
NCN funding to facilitate
recruitment
Contractors act as advisors
to NCNs with
communication plan
established
Increased communication
leads to improved
understanding of Primary
Care issues
AMD / NCN /
CDs / NCN
leads
31.3.16 Funding agreed to support
this
Scope of contribution to be
discussed/agreed
All Gwent NCN Independent Contractor Support.docx
All 3 posts appointed to
2.1.3 NEW: Social Prescribing
post to increase access
to information relating
to health conditions
through dedicated role
Links to Communities First Healthy Lifestyles project Links to ABUHB Service Change Plan No. 5
Appoint Social Prescriber to
signpost people to local
services
Develop and implement
referral mechanism into
community services;
To map range of services
promoting mental wellbeing
and good health across
Third and Public Sector -
facilitate web based
database;
Identify priorities for people
based on referral
information and individual
circumstances;
Feed-back progress to the
NCN;
Develop promotional
materials;
Implement effective
monitoring systems to
evaluate project progress
Evidence shows increased
access to information /
advice & support leads to
improved well-being
NCN /
Communities
First / Public
Health
31.3.16 Slippage funding agreed at
NCN to develop Social
Prescribing role
Public Health Wales co-
production lead
presentation at NCN
meeting
Linked to ‘Bridging The
Gap’:
Bridging The Gap - May 2011.pdf
Post appointed to with
project group established
4
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
Progress/RAG
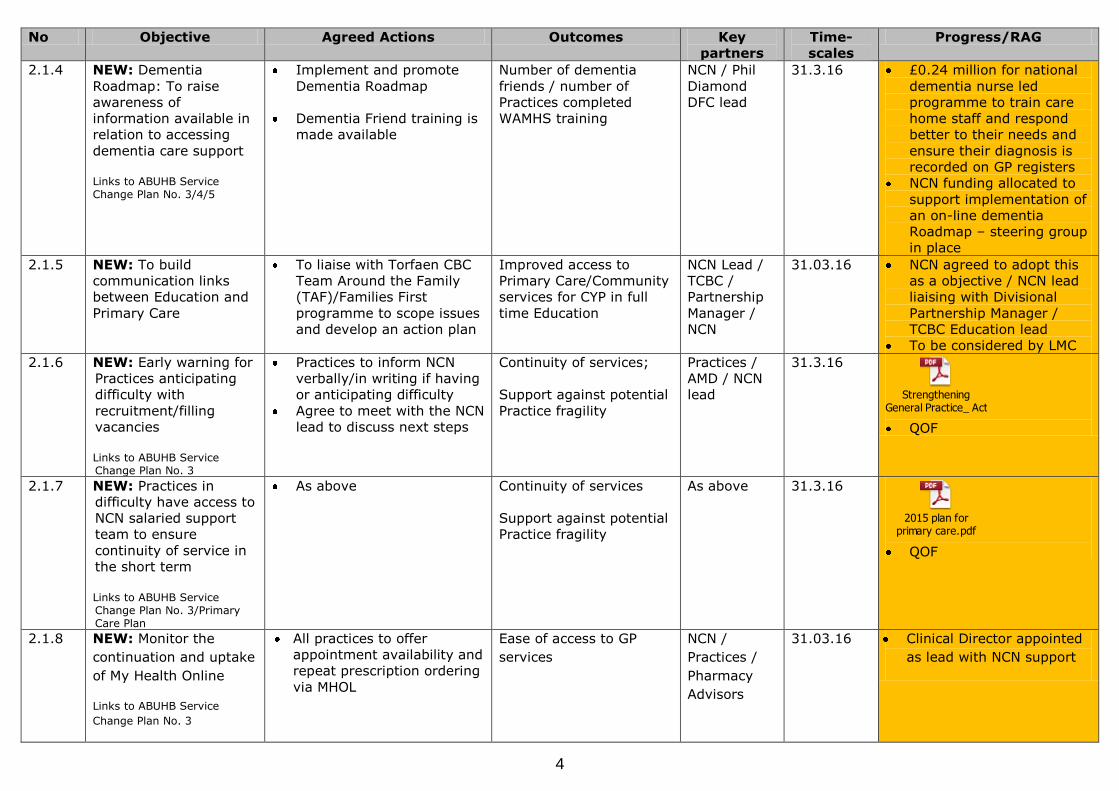
2.1.4 NEW: Dementia
Roadmap: To raise
awareness of
information available in
relation to accessing
dementia care support
Links to ABUHB Service Change Plan No. 3/4/5
Implement and promote
Dementia Roadmap
Dementia Friend training is
made available
Number of dementia
friends / number of
Practices completed
WAMHS training
NCN / Phil
Diamond
DFC lead
31.3.16 £0.24 million for national
dementia nurse led
programme to train care
home staff and respond
better to their needs and
ensure their diagnosis is
recorded on GP registers
NCN funding allocated to
support implementation of
an on-line dementia
Roadmap – steering group
in place
2.1.5 NEW: To build
communication links
between Education and
Primary Care
To liaise with Torfaen CBC
Team Around the Family
(TAF)/Families First
programme to scope issues
and develop an action plan
Improved access to
Primary Care/Community
services for CYP in full
time Education
NCN Lead /
TCBC /
Partnership
Manager /
NCN
31.03.16 NCN agreed to adopt this
as a objective / NCN lead
liaising with Divisional
Partnership Manager /
TCBC Education lead
To be considered by LMC
2.1.6 NEW: Early warning for
Practices anticipating
difficulty with
recruitment/filling
vacancies
Links to ABUHB Service Change Plan No. 3
Practices to inform NCN
verbally/in writing if having
or anticipating difficulty
Agree to meet with the NCN
lead to discuss next steps
Continuity of services;
Support against potential
Practice fragility
Practices /
AMD / NCN
lead
31.3.16
Strengthening General Practice_ Actions for a brighter future for patien .pdf
QOF
2.1.7 NEW: Practices in
difficulty have access to
NCN salaried support
team to ensure
continuity of service in
the short term
Links to ABUHB Service Change Plan No. 3/Primary Care Plan
As above Continuity of services
Support against potential
Practice fragility
As above 31.3.16
2015 plan for primary care.pdf
QOF
2.1.8 NEW: Monitor the
continuation and uptake
of My Health Online
Links to ABUHB Service
Change Plan No. 3
All practices to offer
appointment availability and
repeat prescription ordering
via MHOL
Ease of access to GP
services
NCN /
Practices /
Pharmacy
Advisors
31.03.16
Clinical Director appointed
as lead with NCN support

5
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
Progress/RAG
2.2 Workforce
2.2.1 NEW: Training: Practice
staff can access timely,
relevant training
Links to ABUHB Service Change Plan No. 3
Establish a Divisional/NCN
Task & Finish group –
training plan developed
Develop a process for
Practice staff to access
training
Training providers and
costs are identified
Practices are informed of
training options and criteria
Quality of care / skilled
workforce – enables
sharing of ideas/skills
and good practice
NCN /
ABUHB /
Practices
31.3.16 Process in place via
proposal applications £1.1m allocated to NCNs:
Training options
considered from slippage
funds year on year – T&F
group established
2.2.2 NEW: Increase access
to primary care based
Phlebotomy service
Links to ABUHB Service
Change Plan No. 3
Implement local service
closer to home and in care
homes
Increase access to
phlebotomy service for
house bound population
(WAO report on district nursing
indicates that 30% of community
nursing time could be released, for
example to manage LTCs, if no longer
required to take blood)
Increased capacity
within/ access to District
Nursing service
NCN /
ABUHB
Divisions /
District
Nursing
service
31.3.16 £4.4m funding approved
for new Phlebotomy
service
2.2.3 NEW: Ensure local
support structure is fit
for purpose to meet
demands of strategic
NCN development
Implement a
NCN/Integrated
Management Team
Agree local framework /
membership to underpin
strategic NCN development
Terms of reference
developed and ensure all
members/partners have
equal standing in decision
making process
Improved guidance, co-
ordination and
development to meet the
needs of the local
population
NCN lead /
HoPN /
PC&ND /
ISPB / NCN
31.3.16 Workshop held with key
stakeholders to agree
membership of
Management Group, remit,
immediate action required
and next steps
Action Plan developed
Strategic Aim 3: Planned care - to ensure that patients’ needs are met through prudent care pathways, facilitating rapid, accurate
diagnosis and management and minimising waste and harm

6
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
Progress/RAG
3.1 Mental Health
3.1.1 To improve integration
at Practice level
between Primary Care
(PCMHSS)
Links to Torfaen SIP Links to Communities First Healthy Lifestyles project Links to ABUHB Service Change Plan No. 3
Links to MIND – ‘you in mind’ project for young people
NEW: To receive regular
performance reports to include
referral data specific to North
Torfaen, and to identify action
required across NCN & partners
Evidence shows services
collaborate to ensure
timely access to support
NCN
Practices
PCMHSS /
MH Division
31.3.16 Representation at
Management Team
meetings
On-going dialogue and
reporting via NCN meetings
GAVO Mental Health Service Directory for Gwent.pdf
Strategic Aim 4: To provide high quality, consistent care for patients presenting with urgent care needs and to support the
continuous development of services to improve patient experience, coordination of care and the effectiveness of risk
management
No Objective Agreed actions Outcomes Key
partners
Time-
scales
Progress/RAG
4.1 Urgent Access
4.1.1
REVISED: To maximise
utilisation of alternative
avenues for advice
adopting prudent
healthcare principles
To identify other sources
for advice e.g. email /
telephone (inc mobile
access & new 111
service for urgent
advice)
To record secondary care
email advice incidents
CPD session on reducing
referrals for inappropriate
diagnostic tests
Data shows reduction in
reliance upon multi-
agency services;
Contributes to reduced
waiting times for
secondary care services
PC&ND,
ABUHB
Radiology
and USC
Divisions
31.3.16 Improving referral quality
and maximising utilisation
of alternative avenues for
advice:
Rheumatology/Cardiology
telephone and email
advice routes;
Impact of Teledermatology
service with reduction in
secondary care waiting
times;
SEPSIS 6 guidelines
adopted;
Review of GP urgent
referral letters
Strategic Aim 5: Improving the delivery of end of life care [EOLC] (National Priority – to be discussed locally)
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
RAG
5.1.1 Review delivery of EOLC
using Individual Case
NCN to support Practices
to review audit of patients
Audit outcome leads to
improved care during End
NCN Leads /
Practices /
31.3.16 Year-end report expected

7
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
RAG
Review Audit
Links to ABUHB Service Change Plan No. 4
who have died to be
reflected upon/inform
future care delivery
of Life phase NCN Support
5.1.2 Summarise case review
data, and any arising
issues and actions
identified, for sharing
with the network and
the wider health board
Links to ABUHB Service Change Plan No. 4
Highlight best practice for
improvement to be
highlighted and shared in
a multi-professional
discussion
Learning through shared
experience will inform
improvements for
patients on the EOL
pathway
NCN Leads /
St Davids /
Practices /
NCN Support
31.3.16 Year-end report expected
5.1.3 Establish a review cycle,
to monitor progress (or
maintenance of high
quality), report to NCN
and wider health board
as appropriate
Links to ABUHB Service Change Plan No. 4
Agreement of ‘best
practice’ in EOLC.
Identification and
monitoring of areas for
improvement so that
appropriate education and
support can be delivered
Improved consistency in
standard of care
delivered
NCN Leads /
Practices /
NCN Support
31.3.16 Year-end report expected
August 2015: Audit
outcomes reported to GP
Macmillan co-ordinator with
learning points included in
the Palliative care Delivery
Plan.
5.1.4 NEW: Themes identified
by audits lead to agreed
action
Links to ABUHB Service Change Plan No. 4
NCN to discuss +/- use of
EOLC template for all
patients who enter
terminal stage of illness,
not just those with
cancer;
NCN to discuss READ Code
training for Practice staff
to improve recording of
diagnostic symptoms;
Develop patient recording
protocols for Care Homes,
by using the Integrated
Care Pathway framework,
to ensure patient record
consistency;
Practices identify carers
and record when patients
are first diagnosed /
placed on the register
Improved consistency in
standard of care
delivered.
Practices
NCN Lead
HoPN
31.3.16 Year-end report expected

8
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
RAG
Ensure Carer’s Packs are
available at all GP
Practices;
To map/ensure access to
interpreter services for
patients whose first
language is not English;
Improve communication
with OOH Services re
‘Special Notes’ and use of
Adastra to provide up to-
date patient records.
Strategic Aim 6: Targeting the prevention and early detection of cancers (National Priority)
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
RAG
6.1.1 Review care of all
patients newly diagnosed
between 1 January 2015
to 31 December 2015
with lung,
gastrointestinal & ovarian
cancer
Links to ABUHB Service Change Plan No. 4
Audit tool Patient referral
information reviewed and
Outpatient appointments
/ results followed up
NCN / NCN
Leads /
Practices
31.3.16 Year-end report expected
NICE issued: Suspected
Cancer recognition and
Referral – NG12 (June
2015)
GI Consultant attended NCN
to discuss learning points
and solutions – impact of
new NICE = WLIs /
Weekend & evening clinics
6.1.2 Learning and actions to
be shared with NCN
and the wider health
board as appropriate
Links to ABUHB Service Change Plan No. 4
Practices complete audit
and discuss findings
Audit tool ensures
continuous review,
reflection & improvement
in processes/ care
pathways for cancer
patients
NCN / NCN
Leads /
Practices
31.3.16 Year-end report expected
6.1.3 Identify and include
relevant actions to be
addressed in Practice
Development Plans
Links to ABUHB Service Change Plan No. 4
Practice by practice NCN
USC cancer data will be
collated to provide better
informed demographic
data relating to cancers on
a regular basis
Improved patient
information/ Patient
choice & preferred place
of death
NCN / NCN
Leads /
Practices
31.3.16 Year-end report expected
9
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
RAG
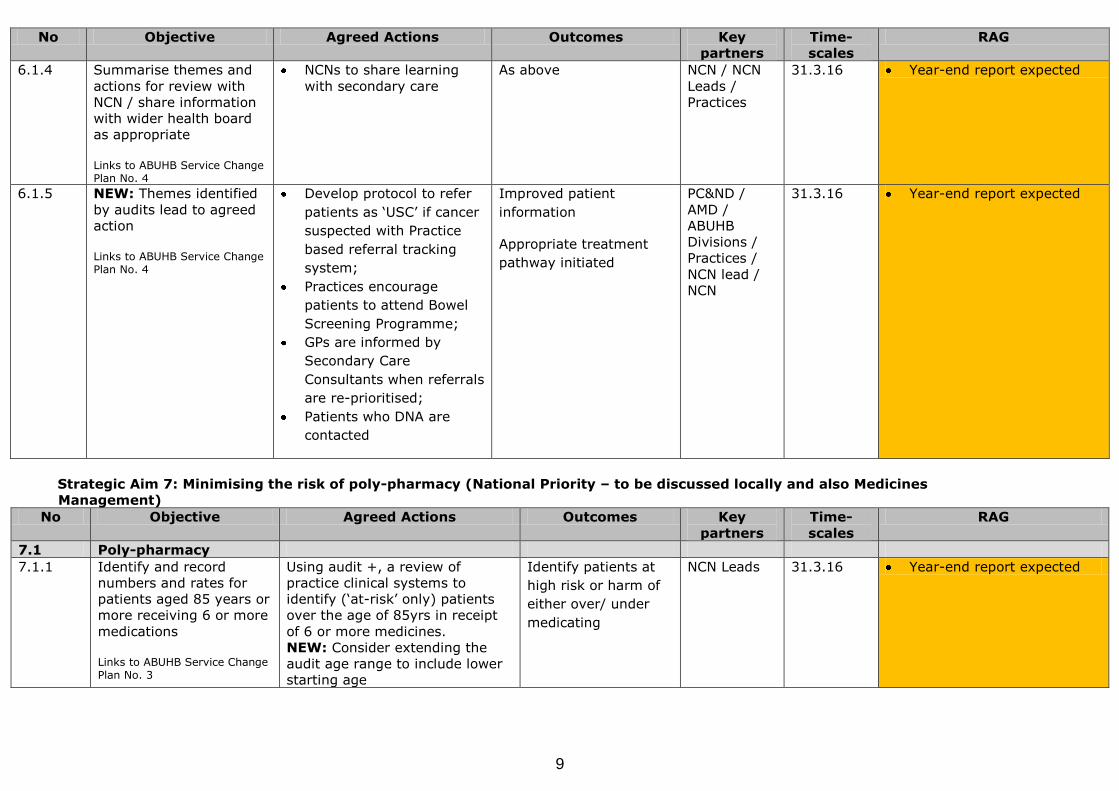
6.1.4 Summarise themes and
actions for review with
NCN / share information
with wider health board
as appropriate
Links to ABUHB Service Change Plan No. 4
NCNs to share learning
with secondary care
As above NCN / NCN
Leads /
Practices
31.3.16 Year-end report expected
6.1.5 NEW: Themes identified
by audits lead to agreed
action
Links to ABUHB Service Change Plan No. 4
Develop protocol to refer
patients as ‘USC’ if cancer
suspected with Practice
based referral tracking
system;
Practices encourage
patients to attend Bowel
Screening Programme;
GPs are informed by
Secondary Care
Consultants when referrals
are re-prioritised;
Patients who DNA are
contacted
Improved patient
information
Appropriate treatment
pathway initiated
PC&ND /
AMD /
ABUHB
Divisions /
Practices /
NCN lead /
NCN
31.3.16 Year-end report expected
Strategic Aim 7: Minimising the risk of poly-pharmacy (National Priority – to be discussed locally and also Medicines
Management)
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
RAG
7.1 Poly-pharmacy
7.1.1 Identify and record
numbers and rates for
patients aged 85 years or
more receiving 6 or more
medications
Links to ABUHB Service Change Plan No. 3
Using audit +, a review of
practice clinical systems to
identify (‘at-risk’ only) patients
over the age of 85yrs in receipt
of 6 or more medicines.
NEW: Consider extending the
audit age range to include lower
starting age
Identify patients at
high risk or harm of
either over/ under
medicating
NCN Leads
31.3.16 Year-end report expected

10
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
RAG
7.1.2 Undertake face to face
medication reviews,
using e.g. ‘No Tears’
approach
Links to ABUHB Service Change Plan No. 3
Using data from the review audit
book appointments for
medication reviews of patients
over the age of 85yrs receiving 6
or more medicines
Reduced avoidable
admissions;
Identification of
untreated
condition(s); Number
of MUR Consultations
NCN Leads /
Practices /
NCN Support
31.3.16 Year-end report expected
7.1.3 Identify any actions to be
addressed in Practice
Development Plans
Links to ABUHB Service Change Plan No. 3
Poly-pharmacy at NCN meetings
As above NCN /
Prescribing
advisors /
Practices /
NCN Support
31.3.16 Year-end report expected
Quarterly information to NCN on
utilisation of notional budget
7.2 Medicines
Management
7.2.1 NEW: Recruit Primary
Care based Pharmacist
from NCN funding to
integrate with GP
Practices, NCN and
partners
Links to ABUHB Service Change Plan No. 3
Initiate recruitment process –
Summer 2015
Induct Pharmacists into GP
Practices
Integration and outcomes
measured/ monitored via
NCN meetings
NCN Pharmacists
project team
developing a suite of
priorities &
outcomes;
Patients and
professionals have
access to a named
Pharmacist in
Primary Care
NCN
leads/NCN/P
C&ND
31.3.16 Year-end report expected
Post appointed to
July/August 2015
Integration and outcomes
measured/ monitored via
NCN meetings
Identify opportunities for
Pharmacists to further
develop appropriate skills
Funding allocated from NCN
budget
7.2.2 To monitor the NCN
prescribing budget and
delivery of the Medicines
Management plan
Links to ABUHB Service Change Plan No. 3
To receive regular prescribing
information (at NCN meetings)
Budget performance and
delivery of the savings plan
National Indicators / Clinical
Effectiveness Prescribing
Programme
Pharmacy and NCN Leads to
meet and decide on priorities
for NCNs to achieve in terms
of service improvement, costs
and quality
Efficient use of
resources leads to
re-investment &
more appropriate
care
NCN Lead /
Prescribing
lead /
Practices
31.3.16 Year-end report expected

11
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
RAG
7.2.3 To review the variation in
prescribing compared to
national guidance in
relation to Diabetes and
Respiratory and deliver
the NCN savings target
for these work-streams
within the three year plan
Links to ABUHB Service Change Plan No. 3
NCNs to work with Primary Care
and Networks Division Pharmacy
staff to:
Arrange scheduled visits by
the NCN Lead to discuss
Dashboards and Practice
performance;
Monitor performance change
through actual prescribing
spend on high dose
corticosteroids and diabetes
drugs;
Identify prescribing leads rep
and identify progress
against the SCEP;
Prescribing guidance to be
developed by Pharmacy Team
Minimise avoidable
harm from adverse
effects of inhaled
steroids;
Undertake minimum
appropriate
intervention to
ensure prudent
prescribing aligned
with NICE Guidance
NCN Lead
31.3.16 Year-end report expected
Strategic Aim 8: Delivery consistent, effective systems of Clinical Governance
No Objective Agreed actions Outcomes Key
partners
Time-
scales
RAG
8 Clinical Governance
8.1 To fully implement the
Clinical Governance
Toolkit
To ensure practices are
supported in completing the
CGSAT
Sessions to be established to
support GP practices in
completing the CGSAT
Target support for areas of
the CGSAT which are
identified as showing low
levels of achievement
Access arrangements - core
access arrangements; aids to
access user experience; the
impact of My Health On Line.
How practices respond to
urgent requests and same day
requests from care homes,
Welsh Ambulance Services
and Hospital emergency
departments.
Consistency and
safety in Practice and
NCN wide primary
care services
Practices /
PC&ND /
NCN
31.3.16
Year-end report expected

12
No Objective Agreed actions Outcomes Key
partners
Time-
scales
RAG
Actions to foster greater
integration of health and
social care.
Consideration of how
community resources can be
maximised to meet local
needs.
Consideration of how Third
Sector support may be
maximised
Map local GP services to
highlight where services are
delivered across practices (for
example, contraceptive
services, minor surgery)
How new approaches to the
delivery of primary care might
aid service delivery and
ensure sustainability of local
services
Consideration of the impact of
local care pathway work
relating to previous QOF work
Strategic Aim 9: Other Locality issues
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
Progress/RAG
9.1 See 2.1 NEW:
Access/DNA rates
9.2 NEW: Diabetes
9.2.1 Tackling the effects of
Diabetes (including
obesity)
Adopted as a local
priority 2015-16 –
agreed 16.07.15
Links to Communities First Healthy Lifestyles project Links to ABUHB Service Change
• To use PH observatory data
as a baseline for
improvement
Intervene more regularly,
with right information in the
right way – brief advice /
intervention
Map Level 2 services for
weight management and
refer/recommend –
Foodwise, commercial clubs,
NERS, led walks
Access to advice
from multi-
disciplinary team &
implementation of
new diabetes work
plan leads to
improved outcomes
for patients
NCN / Public
Health /
ABUHB
Divisions /
Diabetes
Nurse
31.3.16 Presentation given to NCN
at meeting
Agreed that diabetes
Practice Nurse will be a
member of the NCN
Primary Care diabetes
specialist nurses arranging
Practice visits
Diabetes Consultants
aligned to NCNs
Consultant email advice

13
No Objective Agreed Actions Outcomes Key
partners
Time-
scales
Progress/RAG
Plan No. 3/4/5
Refer routinely to Adult
Weight Management Service
Consider increasing AWMS
capacity for specific
populations (e.g. Pre-
diabetes, pregnant women)
e.g. BG West/Mon North
Engage with non medical
members
line open
Consultant/DSN telephone
advice
Further action agreed