trauma arrests - gathering of eagles
TRANSCRIPT

10/5/2012
1
Most Important Non-EMS Articles
Corey M. Slovis, M.D.Vanderbilt University Medical Center
Metro Nashville Fire DepartmentNashville International Airport
Nashville, TN
2011-2012
EAGLES
Trauma Arrests
J Trauma 2011;71:1997-1002
• 294 trauma Arrests over 8 years
• Mount Sinai, Chicago
• Evaluated Survival
• Evaluated Costs
• Should we adhere to TOR protocols?
• Withhold Care in Blunt Trauma if:
Traumatic Cardiac ArrestsNAEMSP/ACS-COT Guidelines
– Apneic, Pulseless, Asystolic or PEA
• Withhold Care in Penetrating: if apneic, pulseless, asystolic, and no signs of life
• Do not transport if > 15 min of unsuccessfulCPR
• Transport penetrating trauma if: organized ECG activity (PEA > 40) +/or signs of life, including pupils
J Trauma 2011;71:1997-1002
• 294 patients met TOR criteria, but were transported
• 35% arrived with signs of life
• 12.6% got ROSC in ED
Results
ED and ROSC
35%
12.6%
37
103
J Trauma 2011;71:1997-1002

10/5/2012
2
Short Term Survival
55%
25.2%
74
164
J Trauma 2011;71:1997-1002
4.8%
142.7%
8
• 8 patients to ICU s/p OR
Overall Survival of 294 Patients
• 4 declared brain dead
• 2 died within 24 hrs
• 1 had care withdrawn
• No organ donors
1/294 Survival (0.3%)GCS of 6 to long-term care
• $8,424 – pronounced in ED
• $43,080 - if admitted to OR or ICU
Charges for Trying to Save Victims Who Qualify for TOR
• Asystole
NFD Trauma ArrestsBegin Ventilation
- Contact Medical Control for Termination
• PEA- Blunt
- Contact Medical Control
- Penetrating- If rate under 40 contact Medical Control
• VF- Treat Like Medical Arrest
• VF
• Penetrating EMD-PEA Arrests
Transport Trauma ArrestsONLY IF
if rate > 40
Tourniquets

10/5/2012
3
• 499 patients
• 862 tourniquets on 651 limbs
• 635/651 appropriately applied or used
• Evaluated survival benefits
J Emerg Med 2011;41:590-597
• Survival was 87%
• 1.6% rate for nerve palsies
• 1.7% first 6 months, 1.5% next 6 months
• 0.4% major limb shortening
J Emerg Med 2011;41:590-597
Effectiveness of Tourniquets
Tourniquet Take Homes
should be on all EMS units!Tourniquets
TXA
Lancet 2010;376-23-32
• Does TXA work in severe hemorrhage?
• 20,211 patients with major trauma
• 10,046 patients got TXA within 8 hours
• Hospitals in Africa, Asia, Eastern Europe
0
5
10
15
20
Dea
th (
%)
30d All Cause Mortality Crash-2
16% 14.5%
Lancet 2010;376:23-32
p=0.0035
Placebo TXA

10/5/2012
4
• Reanalyzes prior CRASH-2 data
• 20,211 trauma patients
• Randomized to TXA or placebo
• Administered up to 8 hours post trauma
Does time to TXA matter?
Lancet 2011;377:1096-1101
RR
0.68
0.79
1.44
Bleeding Death with TXA vs PlaceboLancet 2011;377:1096-1101
<1 hr 1-3 hr 3 hr
• Crash-2 showed early TXA reducedmortality from traumatic bleeding
• Could it really affect worldwidemortality?
• Should TXA only be used in thirdworld countries?
BMC Emerg Med 2012;12: 1-7
TXA Potential Benefits(if given within 3 hours)
BMC Emerg Med 2012;12: 1-7
Crash- 2
TXA reduces trauma mortality
if given within 3 hours
from bleeding by about 1/3
• At the present time both the US and British
Current TXA Use
• UK National Health Service recommends
Armies include TXA in trauma protocol
TXA for all major trauma victims
• TXA is now a WHO “ Essential Medication”

10/5/2012
5
Authors Conclude
TXA has the potential to save between
112,000-128,000 lives per year worldwide
BMC Emerg Med 2012;12: 1-7
if given within 1-3 hours of trauma
Arch Surg 2012;147:113-114
• TXA vs. no-TXA
• US Troops in Afghanistan
• All pts required >1 unit blood
• Subgroup got > 10 units PRBC
• Retrospective study, 896 pts
5
10
15
20
25
30
Mortality %
TXA in US Military
23.9%17.4%
ISS25.2
ISS22.5
p =0.03
Arch Surg 2012;147:113-114
No TXA
N=603
TXA
N=293
5
10
15
20
25
30
Mortality %
TXA in Massive Transfusion
28.1%
14.4%
p =0.004
Arch Surg 2012;147:113-114
No TXA
N=196
TXA
N=125
• TXA dramatically decreased mortality
• Benefits greatest in those requiring
Conclusions
• TXA decreased coagulopathy
TXA in the Military
massive transfusion
• TXA increased survival by factor of 7.228 for those requiring massive transfusion
• Seems to decrease bleeding deaths acutely
• Need to give within 3 hours of event
TXA 2012-2013 Take Homes
• Role in Level 1 Trauma unclear
• Has potential to save 100,000 + lives

10/5/2012
6
TXA Take Homes
• No controlled US or English study yet done
• Evidence is very much in favor
• Complications not shown to be significant
• Cost is very low
on TXA in rapid transport trauma system.
Response Times
Circ J 2011;75:580-588
Is under 8 minutes for ALS really important
to decrease mortality?
• Used only Delta & Echo call who
• Evaluated In-hospital mortality
Circ J 2011;75:580-588
• 24% > 8 minutes from 911 answer till
were admitted to the hospital
• 7760 EMS responses, Alberta Canada
EMS arrival
Response TimesPrehosp Emerg Care 2012;16:142-151
Response Times and Mortality Prehosp Emerg Care 2012;16:142-151
• OR of 1.19 if less or greater than8 minutes is only variable
• Author concludes that ≥ 8 minutes for EMS does not significantly affect mortality
• Rapid responses may make a significantdifference in only a small number of cases

10/5/2012
7
Response Times and Mortality
• Large sums of money spent on EMSto get times under 8 minutes
may not be justified!
• Until more studies show where time is
Prehosp Emerg Care 2012;16:142-151
crucial we may be judged on a false “standard”
Pain Control
Is Ketamine plus Morphine superior to Morphine only in Prehospital Pain Relief ?
Ann Emerg Med 2012; 59:497-503 • 135 EMS patients, Melbourne, Australia
• Pain score > 5 after 5 mg Morphine
• Measured pain score s/p M + K vs M alone
• Evaluated complications including
Ann Emerg Med 2012; 59:497-503
nausea, sedation, BP
Injury Types
M% K+M%
Extremity 26 (37%) 29 (45%)
Soft Tissue Injury 17 (24) 15 (23)
Fracture, Other 14 (20) 13 (20)
Dislocation 11(16) 7 (11)
Burn 2(3) 1 (1)
Ann Emerg Med 2012; 59:497-503-5.6
-3.2
Ketamine + Morphine
Morphine Only
Pain Scale Change

10/5/2012
8
• No significant VS change differences• 2x Nausea with Morphine (9.2% vs
4.3%)• 3 patients had LOC with Ketamine
vs 1 with Morphine• 4 emergence reactions with Ketamine
vs 0 with Morphine
Ann Emerg Med 2012; 59:497-503
Complications
M K+M%
Extremity 6 (9.2%) 3 (4.3%)
Soft Tissue Injury 0 1
Fracture, Other 1 3
Dislocation 0 8 (11.4%)
Burn 0 4 (5.7%)
Take Home PointsKetamine + Morphine in EMS
• Ketamine does improve pain relief
• Is associated with increase in the usual “Ketamine Complications”
• Most complications mild
• Consider Ketamine + Morphine for longer transports and selected urban services
TASERS
• All completed intense exercise
• Then a prolonged TASER discharge
• Pre and Post ECGs evaluated
J Emerg Med 2011;41:466-472
• Medical Questionnaire
• 30 seconds of rapid pushups
• Then treadmill at 8 mph at 8 elevation
• When exhausted; PH 7.22
• Then TASER for 15 seconds lying down
J Emerg Med 2011;41:466-472
Methods
o

10/5/2012
9
• 24/25 ECGs WNL at start
• 1 with PVC’s
J Emerg Med 2011;41:466-472
Results
Post TASER all ECG’s were WNL
Circulation 2012;125:2417-2422
• Are Tasers really safe?
• Reviews 8 cases of Loss of Consciousness
• Attempts to determine cause and effect
Circulation 2012;125:2417-2422
Immediate LOC then Arrest Taser Cases
• Ages: seven were 16-33 yo; one 48
• ΔT to ECG: usually 5-10 minutes
• Rhythm: VT/VF in 7; one AS
• Drug Screen: Two negative, others with
Circulation 2012;125:2417-2422
ETOH* or THC
• Autopsy: 7/8 died, 1 WNL, othersvariable findings(2 at > 300 mg%)
• X26 can cause capture in pigs and sheep
• Tasers can induce VF in pigs
• Epinephrine increase likelihood of capture
• Capture is usually at 200-240 BPM
• ↑ HR + ↓ BP presumed to cause
EP Data with Tasers
VT/VF arrests
Circulation 2012;125:2417-2422
ConclusionsThe animal and clinical data support the conclusion that ECD shocks from a TASER model X26 delivered via probes to the chest can cause cardiac electrical capture. Furthermore, if the capture rate increases sufficiently or if R on T occurs, the development of VF, either directly or via a transition through VT, occurs in animals and, in my opinion, in humans as well.
Douglas P. Zipes, MD
10/5/2012
10
There is no reliable data that shows
TASERs to be dangerous in normal patients,
even if performed after high levels
of physical activity.
TASER Take Homes Taser Take Homes
• Safe in normals
• Associated with deaths
• May induce VF
• Repeat taser is drugs bad
• We are still unsure
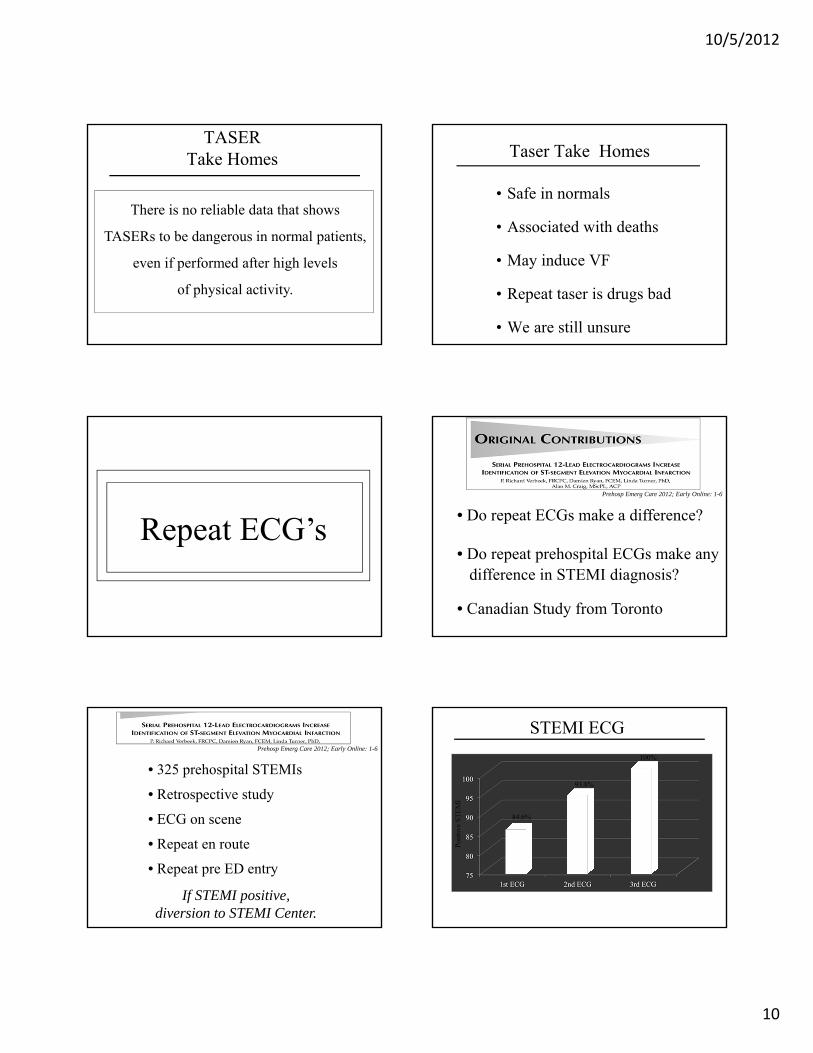
Repeat ECG’s• Do repeat ECGs make a difference?
Prehosp Emerg Care 2012; Early Online: 1-6
difference in STEMI diagnosis?• Do repeat prehospital ECGs make any
• Canadian Study from Toronto
• 325 prehospital STEMIs
• Retrospective study
• ECG on scene
• Repeat en route
• Repeat pre ED entry
Prehosp Emerg Care 2012; Early Online: 1-6
If STEMI positive, diversion to STEMI Center.
Pos
itiv
e S
TE
MI
84.6%
93.8%
100%
STEMI ECG

10/5/2012
11
90% of STEMIs requiring
more than 1 ECG are diagnosed
within 25 minutes of first ECG.
• Encourage more than 1 ECG
Repeat Prehospital ECGsTake Home
in high risk patients
• Repeat ECG in ED per AHA recommendations
• Repeat prehospital ECGs seem reasonableat 10-20 minutes
• Repeat sooner if patient has a significantchange in BP, pulse or chest pain.
• Encourage more than 1 ECG
Repeat Prehospital ECGsTake Home
in high risk patients
• Repeat ECG in ED per
• Repeat prehospital ECGs seemreasonable at 10-20 minutes
• Repeat sooner if patient has a significant change in BP,
AHA recommendations
pulse or chest pain
One ECG Begets Another
GIK • Can it decrease ACS → AMI
• Can we affect AMI survival ?
EMS Glucose-Insulin-Potassium
• Does EMS GIK work ?

10/5/2012
12
• Meta-analysis of 9 trials
• 1,932 patients randomized
• GIK reduced hospital mortality
Circulation 1997;76;1152-1156
• Authors recommend large randomized trial
• 28% reduction (p=0.004)
(16.1% vs. 21% ; p=0.004)
• Large multicenter GIK in STEMI Trial
• 470 centers, 20,201 pts
• Patients treated within 12 hrs
JAMA 2005;293:437-446
• GIK should work, does in lab
• IMMEDIATE is randomized blinded trial
• 13 cities, 36 EMS Agencies
• 871 patients, D5W vs. GIK
• Primary Outcome: ACS → AMI
JAMA 2012; 307;1925-1933 • D30% W ( 300 g/ Liter)
GIK Solutions
• 50 units/Liter Insulin
• 80 mcg KCL/ Liter
• Run at 1.5 ml/kg/hr
• Run at 100 ml/hr in 70 kg pi
1015
2025
3035
4045
50
5560
Progression of MIJAMA 2012;307: 1925-1933
52.6%
48.7%
D5W GIK
p=ns
30d Mortality and Cardiac Arrest
0
1
2
3
4
5
6
7
8
9
D5W GIK
6.1%
8.7%
p = ns
4.4%4.4%
JAMA 2012;307: 1925-1933
p = 0.01
Mortality Mortality or Cardiac Arrest
D5W GIK

10/5/2012
13
• Large multicenter GIK in STEMI Trial
• 470 centers, 20,201 pts
• Patients treated within 12 hrs
JAMA 2005;293:437-446
No differences at 30d in mortality, arrests, cardiogenic shockHF or re-infarction
• EMS GIK may be coming
• May be a cheap and effective ACS Rx
• Safe, cheap, easy to give
• Move to come in next 1-2 years
Glucose, Insulin, and PotassiumGIK Take Homes
Seizure Management• IM Midazolam vs. IV Lorazepam
• 893 prehospital seizing children and adults
• Is either more effective?
• Also evaluated complications
• Double Blind, Randomized, Non-inferiority
NEJM 2012;366:591-600
20
30
40
50
60
70
IV Ativan IV Versed
Seizures Stopped by ED Arrival
63.4%
73.4%
329448
282485
NEJM 2012;366:591-600
p < 0.001for non inferiority
0
1
2
3
4
5
6
7
AT Ver AT Ver
Min
utes
4.8
1.2
Time to Treat and Stop SeizureNEJM 2012;366:591-600
Time to Treat Time to Stop
1.2(6.0)
3.3(4.5)

10/5/2012
14
• Similar times to stop seizures
NEJM 2012;366:591-600
Results
(Ativan: 6 min vs. Versed: 5 min; p = NS)
• Need for intubation the same
• Recurrent seizures the same
• Less hospital admissions with IM Versed(57.6% vs. 65.6%; p = 0.01)
Pediatric Care
• 45 EMS Crews; Simulated Peds Care
• 6 month old: AMS, SZ, Resp Arrest
• Crews used own equipment
• Two observers rated video observation
• Root cause analysis → 5 error themes
Acad Emerg Med 2012;19:37-47
• Don’t use peds equipment often
• Bags often sealed & tagged; not checked
• If stored with adult equip, not found
• If separate, often lacking equipment
Pediatric Error Themes Equipment Organization & Use
Acad Emerg Med 2012;19:37-47
Pediatric Error ThemesGlucose Measurement
Acad Emerg Med 2012;19:37-47
• Crews often forget to check glucose• Sepsis, AMS, OD:
all may be hypoglycemic
• Incorrect weight estimates
• Incorrect Broselow use
• Drug Calculation Errors
• 64% did not cross check dosages
Pediatric Error Themes Drug Administration
Acad Emerg Med 2012;19:37-47
they were often confused• If IV, IM, IN doses all different,

10/5/2012
15
Pediatric Error ThemesInappropriate CPR
Acad Emerg Med 2012;19:37-47
• Compressions with pulse present (<100 BPM)
• No pulse check per CPR
• Did not bring O2 to patients
• Could not find peds equipment
• Failed to use OPA in infants
• Poor ventilatory technique
Pediatric Error Themes O2 Delivery
Acad Emerg Med 2012;19:37-47
Expert Pediatric Emergency CareTake Homes
• We need to pay attention to paramedics
• Simulations great for diagnosing training
• Simulations great for teaching
• Pediatric EMS is rarely practiced
pediatric skills and skill retention
(1-2% for many services)
needs Anaphylaxis
• Online survey, 3357 NREMTs
• 98.9 recognized classic case
• Evaluated Epi use
• Evaluated routes of admin
Prehosp Emerg Care 2012 in press
Epinephrine in Anaphylaxis
Only 46.2% said Epi was initial drug in a classic case of a hypotensive, wheezing, tachycardia patient with tingling in his throat & hands, and hives on his chest.
Prehosp Emerg Care 2012 in press

10/5/2012
16
Epinephrine in Anaphylaxis
• An almost equal number (40%) started
• More gave Epi SQ (58.4%) than
• 1.7% gave Epi IV!
Prehosp Emerg Care 2012 in press
with Benadryl as started with Epi (46.2%)
IM (38.9%)
• One of the most important EMS
• Half of our paramedics may not give
Anaphylaxis Care
• Too many in EMS (and Medicine) think
Take Home Points
Epi when they should • More than half of our paramedics give
Epi SQ rather than IM
Benadryl is the first line drug for
emergencies
anaphylaxis
J Emerg Med 2012 in press
without increasing morbidity
• Excellent literature review
• 407 articles screened; 15 evaluated
• TPA is safe and effective
• Use 3-4.5 hrs post stroke improves outcome
In Summary
Atropine No, Epi Early
2 inches at 100-120 BPM
20 seconds or less for perishock pause
Mechanical CPR benefits still unproven
SGA’s may decrease cerebral flow and survivalFollow closely
Decrease transports of pulseless patients
Tasers still controversial
Repeat ECG’s
IM Versed for seizures
Anaphylaxis and Peds needs more teaching

10/5/2012
17
VanderbiltEM.com