trauma system plan - contra costa countycchealth.org/ems/pdf/trauma_plan2001.pdf- a bi-county trauma...
TRANSCRIPT
Contra Costa Health Services Emergency Medical Services Agency
Trauma System Plan
Update for State Trauma Regulation Requirements
December 31, 2001


- i -
Table of Contents Trauma System Criteria (H&S §100254) ...............................................................7 Policy Development (H&S §100255) .......................................................................9 Plan Development (H&S §100256) ......................................1, 2, 5, 7, 17, 18, 23, 24 Data Collection (H&S §100257).............................................................................27 Section I Summary of Plan ......................................................................................... 1 Section II Organization Structure ............................................................................... 2 Section III Needs Assessment......................................................................................... 5 Section IV Trauma System Design................................................................................ 7 Section V Inter-County Trauma Center Agreements.............................................. 17 Section VI Objectives .....................................................................................................18 Section VII Implementation Schedule............................................................................23 Section VIII Fiscal Impact ................................................................................................24 Section IX Policy and Plan Development .....................................................................25 Section X Written Local Approval ..............................................................................26 Section XI Data Collection.............................................................................................27 Section XII Trauma System Evaluation.........................................................................28 List of Attachments..............................................................................................................30

- 1 -
Section I Summary of Plan
Contra Costa County’s Trauma System Plan was developed in 1985, approved by the Board of Supervisors on November 19, 1985, approved by the State Emergency Medical Services Authority (EMSA) on December 20, 1985 based upon the draft trauma regulations available at that time. The format and information contained in the plan was updated in October 1987 to conform to requirements of the adopted State trauma regulations and re-approved by EMSA on November 28, 1988. This current plan update was completed to comply with formatting and information requirements of the current State regulations, but does not represent any substantive change in the original trauma system play of 1985. Key elements of the trauma system plan include the following: - Designation of a single Level II trauma center to serve all of Contra Costa
County. - Trauma center designation to be made on the basis of an open competitive process
including use of an outside team of experts to evaluate trauma center applications. - Recognition of the Level II pediatric trauma center designated by Alameda
County as the appropriate facility to serve the needs of pediatric trauma patients. - Full integration of the trauma system into the existing EMS system - Field triage of all major trauma patients to a designated trauma center when
possible. - Use of air ambulance (helicopter) services to reduce trauma transport times when
appropriate. - Establishment of a trauma registry to track trauma system and trauma center
performance on a case-by-case basis. - A bi-county trauma audit (quality assurance and improvement) process to assure
outside expert review of the trauma center and the trauma system on an ongoing basis.

- 2 -
Section II Organization Structure
The Contra Costa County trauma system is an integral part of the County EMS system shown in Figure II-1. The Contra Costa Health Services Department is the designated Local EMS Agency (LEMSA) as designated by the Board of Supervisors. The regular LEMSA staff include the EMS Director, EMS Medical Director, the EMS Program Coordinator, the Health Services Emergency Preparedness Manager, two nursing positions, two prehospital care coordinators (nurse or paramedic), and two support staff.
John Muir Medical Center was designated in May 1986 following a request for proposal process as the County’s sole Level II Trauma Center serving the entire county. The current trauma center designation contract between John Muir and the County was entered into in May 1992 following a second request for proposal process in which all hospitals were given a second opportunity to seek trauma center designation. The term of the existing contract is continuous. While John Muir is the sole County-designated trauma center, the County recognizes Children’s Hospital Oakland as an Alameda County designated Level II Trauma Center with specialized capability to care for pediatric trauma and has established mechanisms to assure that most pediatric trauma is transported directly to Children’s.
Support Staff(2.0 FTE)
California EmergencyMedical Services Commission
HospitalsContra Costa
DoctorsJohn Muir
Kaiser-RichmondKaiser-Walnut Creek
Mt. DiabloSan RamonSutter Delta
Emergency Ambulance ServicesAmerican Medical Response
Moraga-Orinda FireSan Ramon Valley Fire
Trauma CentersJohn Muir
Children's (pediatric)
First RespondersBethel Island FireContra Costa FireEast Diablo FireEl Cerrito Fire
Moraga-Orinda FireOakley FirePinole Fire
Richmond FireSan Ramon Valley Fire
E M S P r o v i d e r s
Air AmbulanceCalSTARREACH
Rescue AircraftCalifornia Highway PatrolEast Bay Regional Parks
EMS Dispatch CentersContra Costa FireContra Costa SheriffRichmond PoliceSan Ramon Valley Fire
Figure II-1. Contra Costa County EMS SystemCalifornia EmergencyMedical Services Agency
Local EMS Agency
Contra CostaPre-TAC
Committee
Training ProgramsLos Medanos CollegeContra Costa College
Mt. Diablo Adult EducationSafety Compliance Management
Facilities & CriticalCare Committee
Emergency Medical Care Committee(EMCC)
RN/TraumaCoordinator
RN/ FirstResponderPrograms
PrehospitalCare Coord./Persn'l & MIS
PrehospitalCare Coord./Hosp. & QI
RN/FirstResponderQI Coord
(contract 15 hrs/wk)
EMS Program Coordinator
Medical AdvisoryCommittee
(MAC)
Alameda - Contra CostaTrauma Audit
Committee(TAC)
Quality Council
EMS Medical Director Health Services EmergencyPreparedness Manager
Special Projects
Emergency Medical ServicesDirector
Health Services Director/County Health Officer
Board ofSupervisors

- 3 -
The EMS Agency is responsible for overall trauma system monitoring and quality assurance and for administration of the trauma center designation contract. The trauma system quality assurance process established by Contra Costa County includes joint Alameda-Contra Costa County Trauma Audit Committee (TAC), a county-level Pre-TAC Committee, and a trauma registry maintained both by the Trauma Center and by the County EMS Agency. A County EMS nurse is assigned approximately half time as Trauma Coordinator. The Trauma Audit Committee meets bimonthly to review cases treated at any one of the four Contra Costa and Alameda County trauma centers. Cases referred to the Trauma Audit Committee have first been by a Pre-Trauma Audit Committee. Membership in the TAC and in the Contra Costa Pre-TAC is shown in Figures II-2 and II-3.
Figure II-2. Alameda-Contra Costa Trauma Audit Committee Membership EMS Medical Directors* (2) (Co-Chairs) Base Hospital Coordinator EMS Directors* (2) EMS Program Coordinator* EMS Trauma Coordinators* (2) Forensic Pathologist (2) Neurosurgeon (SF Neurological Society recommendation) Non-Trauma-Center Emergency Physician Pediatric Trauma Surgeon Trauma Center Anesthesiologist (rotating) Trauma Center Emergency Department Director or physician designee (4) Trauma Center Neurosurgeon (rotating) Trauma Center Trauma Chiefs (4) Trauma Center Trauma Coordinators (4) Trauma Surgeon (ACCMA recommendation) *Non-voting members.
Figure II-3. Contra Costa Pre-Trauma Audit Committee Membership Out-of-County Reviewing Surgeon (Chair) Base Hospital Liaison Physician EMS Medical Directors or designee EMS Program Coordinator* EMS Trauma Coordinator* Kaiser Surgeon Solano County Base Hospital Physician Trauma Center Emergency Department Director or physician designee Trauma Center Trauma Chief Trauma Center Trauma Coordinator


- 5 -
Section III Needs Assessment
A. Trauma System Catchment Area The catchment area for the Contra Costa trauma system is the entire county and includes a population of 963,000 persons as of July 1, 2000.1 B. Major Trauma Patients Table III-1 shows the number of patients in Contra Costa meeting one or more of the County’s field trauma triage criteria broken down into those who were triaged in the field as major trauma patients and those triaged in the field as not having major trauma. The total number field triaged as having major trauma has run around one thousand or nearly one thousand patients each of the past five years. These include (1) those patients triaged as meeting criteria established by the EMS Agency for automatic trauma center transport and (2) those patients not meeting automatic trauma center transport when the base hospital has directed transport to a trauma center. Most of these patients (776 in 2000) are transported to the John Muir Trauma Center. The remaining patients are transport to Children’s Hospital as pediatric trauma cases, to other trauma centers when John Muir is on trauma bypass, or to non-trauma-center facilities due to unstable airway or, rarely, because John Muir is on trauma bypass and transport time to an out-of-county trauma center would be excessive.
Table III-2 shows over-triage and under-triage error rates for the five years 1996 – 2000. Typically, almost half of these patients triaged in the field as having major trauma (43.7 percent in 2000) turn out not to have major trauma following examination at the trauma center. Applying the overtriage rates to the number of patients transported to John Muir yields figures ranging from 339 to 430 as the number of retrospective major trauma patient transported to John Muir annually during the past five years by the EMS system. These retrospective major trauma patients are patients with an Injury Severity Score (ISS) of over 10 or patients with a lower ISS but who required a hospital stay of at least three days. Under-triage error rates representing patients mistakenly triaged as non-major-trauma have remained below 5 percent during the past five years and were only 1.1 percent in 2000.
Table III-3 shows the number of trauma patients treated and entered into the trauma registry at
the John Muir Trauma Center for Fiscal Year 2000-01. The number either admitted or who died in the emergency department – the number used for AB 430 reporting – was 1,169.
1 California Department of Finance.

- 6 -
Table III-1. On-scene Triage of Patients Within Contra Costa Meeting Field Trauma Criteria
1996 1997 1998 1999 2000
Total Patients Meeting One or More Field Trauma Triage Criteria 2,993 2,853 2,920 2,909 2,885
Triaged in field as major trauma 881 997 964 1,025 983
Transported to a trauma center 842 957 925 984 953
John Muir Medical Center 735 841 814 827 776
Children's Hospital, Oakland 87 88 99 129 129
Other trauma center 20 28 12 28 48
Transported to the closest receiving hospital 39 40 39 41 30
CPR/Unstable airway 38 39 38 41 29
Trauma center on bypass 1 1 1 0 1
Triaged in the field as not having major trauma 2,112 1,856 1,956 1,884 1,903
Table III-2. Undertriage and Overtriage Rates by Year (per 100 cases field triaged as major trauma)
Type of Triage Error 1996 1997 1998 1999 2000
Undertriage 2.4 3.8 2.9 1.3 1.1
Overtriage 46.5 50.3 45.0 52.0 43.7
Table III-3. John Muir Trauma Registry Patients, Fiscal Year 2000-2001
All trauma registry patients* 1,213
Treated and released from ED 60
Died in ED/transferred out 21
Admitted 1,132
Number admitted or died in ED (AB 430) 1,153
* Includes 150 trauma patients that were not admitted through the emergency department.

- 7 -
Section IV Trauma System Design
A. Inclusive Trauma system Design The Contra Costa County trauma system is an inclusive system involving all hospitals with basic emergency services and all EMS system providers. The roles of the various agencies are described below:
(1) John Muir Medical Center – Level II Trauma Center. John Muir is the designated Level II trauma center for Contra Costa County and is the sole trauma center designated by the County. By protocol, all major trauma patients are transported to John Muir except (a) pediatric trauma patients that can be transported to Children’s by ground ambulance or helicopter within reasonable time, (b) trauma patients with an unmanageable airway requiring transport to the nearest hospital basic emergency services, and (c) trauma patients transported to an out-of-county trauma center when John Muir is on trauma bypass. John Muir receives critical trauma patients as transfers when such patients have initially arrived at non-trauma-center facilities. As the trauma center, John Muir serves as the paramedic base hospital for all trauma cases and, since March 1, 2001, as the County’s sole paramedic base hospital. John Muir is responsible for conducting its own internal quality improvement program and for participating in the EMS system quality improvement program. John Muir is also responsible for providing trauma training opportunities for EMS field personnel and for providing injury prevention programs for the community.
(2) Children’s Hospital Oakland – Level II Trauma Center (Pediatric). Located in
the adjacent county of Alameda and designated as a Level II trauma center by Alameda County, Children’s Hospital Oakland specializes in the care of pediatric patients and maintains a pediatric intensive care unit. By protocol and by agreement with Children’s Hospital, all pediatric major trauma patients in Contra Costa County are transported to Children’s Hospital except where transport time would be excessive (transports exceeding 30 minutes require base hospital direction) or where the patient has an unmanageable airway. Children’s is responsible under its trauma center agreement with Alameda County, for conducting its own internal quality improvement program and for participating in the joint Alameda-Contra Costa County trauma system quality improvement program.
(3) Non-Trauma-Center Hospitals. Contra Costa has seven non-trauma-center
hospitals providing basic emergency services. These hospitals may receive major trauma patients by protocol when transport of a patient with an unmanageable airway to the nearest facility is required. Additionally, non-trauma-center hospitals may receive major trauma patients arriving by non-EMS transport or by EMS transport as a result of field triage error. John Muir, as the County’s Level II trauma center, is required to accept these patients as transfers when appropriate care is not available at the receiving facility and the patient can be safely transferred.

- 8 -
B. Coordination with Neighboring Agencies Contra Costa County’s trauma system cooperates with neighboring agencies in the following ways: 1. Pediatric trauma patients are generally transported to Children’s Hospital Level II
pediatric trauma center in Alameda County. 2. Adult trauma patients may be transported by ambulance to Alameda County trauma
centers (Highland, Eden) when John Muir is on trauma bypass. 3. John Muir trauma center accepts major trauma patients from adjacent counties.
Specifically, trauma patients are routinely air-transported from Solano and Marin Counties to John Muir.
4. Contra Costa utilizes air ambulances based out-of-county when units based in-county are
unavailable. 5. Air ambulances transport to out-of-county trauma centers in Alameda, Sacramento, and
Santa Clara when John Muir is on trauma bypass. 6. Since its inception, Contra Costa’s trauma system has included a joint Alameda-Contra
Costa Trauma Audit Committee overseeing the two counties’ trauma quality assurance programs. This two-county TAC is jointly chaired by the EMS medical directors and includes the trauma chiefs of each of the four trauma centers (John Muir, Highland, Eden, and Children’s), a neurosurgeon from each county, and other trauma center and non-trauma-center representatives. The TAC meets bi-monthly to review cases referred by local Pre-TAC (Z-TAC in Alameda County). The local Pre-TAC (or Z-TAC) includes representatives of a single trauma center whose cases are being reviewed, representatives of the local EMS agency, and a visiting trauma surgeon. The visiting trauma surgeon assignments are rotated so that, for example, John Muir will cases are reviewed at successive meetings by a trauma surgeon from Highland, Eden, and Children’s.
C. Rationale for Number and Location of Trauma Centers 1. Rationale for Number and Level of Trauma Centers
Contra Costa County’s Trauma System Plan was developed in 1985. At that time, the County’s estimated population was 705,000. The estimated annual number of major trauma patients based upon California Health Facilities Commission discharge data and County Coroner’s data for emergency room death was 449. The Trauma Care Review Committee charged with developing the County’s Trauma System Plan recommend that a single Level II trauma center be designated in an effort (1) to meet the American College of Surgeons recommendation that each trauma surgeon treat a minimum of 50 cases per year to maintain proficiency and (2) to achieve financial viability for a trauma center

- 9 -
program which would incur significant fixed costs related to meeting trauma center requirements, such as the requirement to maintain in-house trauma surgery capability. In the year 2000, Contra Costa’s population had grown to 947,000 and the number of major trauma patients treated at the John Muir Trauma Center was 776. While based upon population Contra Costa would qualify to designate two Level II trauma centers, the County believes that the goals of trauma team proficiency and trauma center financial viability continue to be best met with a single trauma center.
2. Level I Trauma Centers Contra Costa has no Level I trauma centers. 3. Level III and IV Trauma Centers Contra Costa has no Level III or IV trauma centers.
4. Resource Availability to Meet Staffing Requirements for Trauma Center The following requirements, which generally meet or exceed the trauma center
resource requirements set forth in California Code of Regulations §100259-100264, were established by the Trauma System Plan for Contra Costa County (Attachment C) adopted in January 1986 and remain in effect. In those instances where the State trauma regulations establish standards that differ from the 1986 County trauma plan, John Muir has agreed to meet the State standards. (See Attachment F – memorandum from John Muir Medical Center.)
VIII. {PRIVATE }TRAUMA CENTER STANDARDSTRAUMA CENTER STANDARDS{tc \l 1 "TRAUMA CENTER STANDARDS"}
The following standards have been adopted from the California State Trauma Regulations (draft, October, 1985).
The state regulations provide for three levels of trauma centers. It was determined that only a Level II Trauma Center was possible and appropriate in Contra Costa County. Additional local standards have been added to the state minimum standards. These additional local standards are noted with an asterisk. Those standards which are essential are marked with an "E", while those that are desirable but not essential are marked with a "D".
A. Organizational Requirements E 1. Trauma Service: A trauma service or multidisciplinary trauma committee shall be included in the hospital organization. This
service will provide for the implementation of the requirements specified in this section and provide for coordination with the Office of EMS. The trauma service shall have the following functions:
a. To provide and coordinate the care of patients with severe trauma through all phases of their care. b. To ensure the quality of care for patients with severe or multiple trauma. 2. Surgical Services: The hospital organization shall include at least the following department(s), services(s), or section(s) staffed by
qualified surgical specialists: E a. General E b. Cardiothoracic E c. Neurologic E d. Orthopedic E e. Ophthalmic E f. Oral, otorhinolaryngologic, maxillofacial and/or plastic E g. Urologic E 3. Emergency Services:

- 10 -
The emergency department, division, service, or section shall be staffed so that trauma patients receive immediate and appropriate initial care.
B. Medical Staff Availability All professional staff listed in Sections 1, 2, and 3 as Essential shall be Board Certified by the appropriate board
recognized by the American Board of Medical Specialties. Each shall be credentialed by the facility for the appropriate specialty.
E 1. Emergency Medicine: In-house and immediately available at all times. 2. Surgery: Qualified surgical specialist(s) available as follows: E a. General Surgery: Immediately available at all times (immediately available is defined to mean that the
surgeon is unencumbered by conflicting duties or responsibilities; responding without delay when notified; and being within the specified area of the trauma center when the patient is delivered). The on-call general surgeon while on first-call to the trauma center is to be dedicated exclusively to that facility.
b. The following surgical specialties shall be on call and promptly available from inside and outside the
hospital: E 1) Cardiothoracic E 2) Neurologic: The on-call neurosurgeon while on first-call to the trauma center is to be dedicated
exclusively to that facility. E 3) Orthopedic E 4) Ophthalmic E 5) Oral, otorhinolaryngologic, maxillofacial and/or plastic, depending on local circumstances E 6) Urologic E 7) General Surgery (second physician on call) E 8) Hand E 9) Obstetric/Gynecologic E 10) Vascular E 3. Anesthesia: Immediately available at all times. May be on-call provided that the anesthesiologist is in the
operating room when the patient arrives. The on-call anesthesiologist, while on first-call to the trauma center, is to be dedicated exclusively to that facility.
4. Non-surgical specialties: Available on-call by page or telephone from inside or outside the hospital and
promptly available as necessary for the welfare of the patient as determined by the physician in charge. E a. Cardiology D b. Gastroenterology E* c. Hematology D* d. Infectious Diseases E e. Internal Medicine/Family Practice E f. Nephrology D* g. Neurology E h. Pathology E i. Pediatrics D* j. Psychiatry E* k. Pulmonary Medicine E l. Radiology D* m. Rehabilitation and Physical Medicine C. Trauma Service 1. Personnel E a. Medical 1) Medical Director: Board Certified in General Surgery. This physician will be responsible for
coordinating the inhospital services and their relationship to the Emergency Department. E 2) Surgical Staff: Board Certified in General Surgery within three years of completion of residency or
fellowship, or within three years of joining a trauma team if more than three years have elapsed since completion of residency or fellowship. The on-duty trauma surgeon is responsible for the supervision of trauma patient care with appropriate sub-specialty back-up.
a) Must maintain current certification in ACLS b) Must maintain current certification in ATLS E b. Administrative 1) Trauma Care Coordinator: This person will be responsible for: a) Internal administration of data and reporting requirements b) Coordination and liaison between the service, the hospital and the EMS System. c) Program monitoring. d) Coordination of internal and EMS System training of personnel. e) Participation in trauma center administration meetings. f) Other duties as assigned by the trauma service.

- 11 -
This individual must have experience and/or training in systems management and data collection/reporting.
c. Nursing 1) Trauma Nursing Coordinator: This person will be responsible for trauma center functions as
related to nursing care of the trauma patient. The requirements for level of training for this nurse are as follows:
E* a) Must be a Registered Nurse licensed in the State of California. E b) Must maintain current ACLS certification. E* c) Must have CEN or CCRN. E* d) Must maintain certification in Emergency Nurses Association Trauma Nursing when
available (Tract 1 and Tract 2). Until available, appropriate orientation to all aspects of trauma nursing, including successful completion of a written examination and appropriate skills testing.
E* e) Ten hours of BRN approved continuing education in trauma nursing each year, or teaching BRN approved continuing education in trauma. Trauma or trauma nursing research may be substituted.
The Trauma Care Coordinator and the Trauma Nursing Coordinator roles may be performed by the same individual if all qualifications are met.
d. Facility E 1. Designated trauma resuscitation area, physically separated from other patient areas, of adequate
size to accommodate multi-system injured patients and equipment. E 2. Helicopter landing site with immediate access to trauma resuscitation room and operating suite. E e. Support Provision for immediate response from the blood bank, laboratory, pulmonary/respiratory therapy
department, and operating room. D. Special Facilities/Resources/Capabilities 1. Emergency Department: Must have special permit from the State of California to operate as a basic
emergency medical service. E a. Designated Medical Director E 1) Board Certified by the American Board of Emergency Physicians. E* 2) Full-time practice (at least 30 clinical hours per week) in emergency medicine at trauma center
hospital. E 3) Must maintain both current ACLS and ATLS certifications. b. Physician personnel E 1) Diplomate of the American Board of Emergency Medicine within three years of completing
residency. E 2) Must maintain both current ACLS and ATLS certifications. c. Nursing personnel E* 1) There shall be a Designated Clinical Liaison Nurse with the following qualifications: D* a) CEN. E* b) Must maintain current ACLS certification. E* c) Ten hours of BRN approved continuing education in trauma nursing each year, or teaching
BRN approved continuing education in trauma. Trauma or trauma nursing research may be substituted.
E* d) Must maintain certification in Emergency Nurses Association Trauma Nursing when available (Tract 1). Until available, appropriate orientation to all aspects of trauma nursing, including successful completion of a written examination and appropriate skills testing.
2) Staff Nurses shall have the following qualifications: D* a) CEN. E* b) Must maintain current ACLS certification. E* c) Ten hours of BRN approved continuing education in trauma nursing each year, or teaching
BRN approved continuing education in trauma. Trauma or trauma nursing research may be substituted.
D* d) Must maintain certification in Emergency Nurses Association Trauma Nursing when available (Tract 1). Until available, appropriate orientation to all aspects of trauma nursing, including successful completion of a written examination and appropriate skills testing.
d. Equipment and facilities Shall conform to the requirements of California Administrative Code, Title XXII, Section 70441, et seq. The equipment shall include, but not be limited to the following and shall be available in the ER at all
times: E 1) Airway control and ventilation equipment, including laryngoscopes and endotracheal tubes of all
sizes, bag-mask resuscitator, and a source of oxygen and mechanical ventilator available. E 2) Sterile surgical sets for procedures standard for the Emergency Department including laparotomies
and thoracotomies. E 3) Peritoneal lavage equipment. E 4) Drugs and supplies necessary for usual emergency medical care and the initial resuscitation of
major trauma patients. E 5) X-ray capability.

- 12 -
E* 6) Two-way radio linked with emergency transport vehicles in accordance with the policies and procedures of the EMS System.
E* 7) MAST suit (also needed as supply replacement for EMS vehicles). E 8) Skeletal tongs. E* 9) Backboards and spinal immobilization boards. E* 10) Blood warmer. E 11) Autotransfuser. 2. Intensive Care Unit (ICU) For trauma patients, the ICU may be a separate specialty unit. It shall conform to requirements of California
Administrative Code, Title XXII, Section 70491, et seq. E* a. There shall be a designated Medical Director. E* b. There shall be a physician on duty in the ICU 24 hours per day or immediately available at all times. c. Nursing personnel E* 1) Designated Clinical Liaison Nurse with trauma nursing experience. E* a) Must maintain current ACLS certification. D* b) CCRN. E* c) Ten hours of BRN approved continuing education in trauma nursing each year. E* d) Must attend orientation to all aspects of trauma nursing, including successful completion of a
written examination and appropriate skills testing. 2) Staff Nurses D* a) CCRN. E* b) Must maintain current ACLS certification. E* c) Ten hours of BRN approved continuing education in trauma nursing each year. E* d) Must attend orientation to all aspects of trauma nursing, including successful completion of a
written examination and appropriate skills testing. d. Equipment shall include, but not be limited to, the following: E* 1) Pulmonary Artery monitoring (Swan-Ganz) E 2) Cardio output monitor E 3) Electronic pressure monitor E* 4) Mechanical ventilator-respirator E 5) Patient weighing devices E 6) Pulmonary function measuring devices E 7) Thermal control device E 8) ICP monitoring E e. Immediate access to clinical laboratory services. E 3. Post-anesthetic Recovery Room (PAR) (Surgical intensive care unit is acceptable). Shall meet the requirements of California Administrative Code,
Title XXII, Section 70231, et seq. E* a. RN's and other essential personnel shall be available 24 hours per day. E* b. There shall be appropriate monitoring and resuscitation equipment. D* c. Nursing staff must maintain current ACLS certification. E* d. Nursing staff must attend orientation to all aspects of trauma nursing, including successful completion of
a written examination and appropriate skills testing. 4. Operating Suite Special Requirements Shall meet the requirements of California Administrative Code, Title XXII, Section 70221, et seq. and shall
include, but not be limited to: E a. An operating (trauma) room adequately staffed in-house and immediately available at all times. E* b. Nursing staff must attend orientation to all aspects of trauma nursing, including successful completion of
a written examination and appropriate skills testing. D* c. Nursing staff must maintain current ACLS certification. d. Thermal control equipment E 1) For patient E 2) For blood E* e. X-ray capability. E* f. C-Arm fluoroscopy with appropriate table. D* g. Cardiopulmonary bypass pump oxygenator. D* h. Operating microscope. E* i. Fracture table. E* j. Image intensifier. E k. Endoscopes (bronchoscopes, gastroscopes, and esophagoscopes) available to the operating room. E l. Craniotome. E* m. Mechanical Ventilator Respirator. E* n. Auto Transfuser. E o. Patient monitoring equipment. E 5. Hemodialysis Capability (or transfer agreement) E 6. Burn Unit a. Physician-directed Burn Center/Unit staffed by nursing personnel trained in burn care and equipped to
properly care for the extensively burned patient;

- 13 -
or b. Transfer agreement with nearby burn centers or hospital with a burn unit. E 7. Acute Spinal Cord Injury management capability or a signed transfer agreement with a regional spinal cord
injury rehabilitation center. 8. Radiological Service - available 24 hours per day E a. Certified radiological technician in-house at all times for general radiological procedures. E b. Angiography of all types. E c. Sonography. E d. Computerized tomography, head and body with a technician who is promptly available at all times. 9. Rehabilitation Program Shall meet the requirements of California Administrative Code, Title XXII, Section 70595, et seq. E a. To commence in the Trauma Center as soon as it is medically feasible. E b. Signed transfer agreements with recognized Rehabilitation Centers in the area. E c. Follow-up at community hospital and/or Rehabilitation Centers. E* 10. Pharmacy: The pharmacy shall be in-house with 24 hour per day on-call availability of a pharmacist. 11. Clinical Laboratory Services E Shall meet the requirements of California Administrative code, Title XXII, Section 70241, et seq., and shall
include, but not be limited to the following: E a. Comprehensive blood bank or access to a community central blood bank and adequate hospital storage
facilities. Have the capability of collecting blood and storing blood for emergency care. E b. Be able to do blood gases and pH determinations. E c. Drug and alcohol screening capability. E d. Capability to determine serum and urine osmolality. E e. Coagulation studies. E f. Have laboratory and pulmonary technician available 24 hours per day. 12. Human Support Service E Shall meet the requirements of California Administrative Code, Title XXII, applicable Section noted: E a. Physical Therapy (Section 70555, et seq.) E b. Occupational Therapy (Section 70515, et seq.) E c. Social Service (Section 70629, et seq.) E d. Nutrition Services E. Quality Assurance E 1. Medical and Nursing Care Evaluation, including: E a. Detailed audit for trauma deaths, major complications, and transfers. E b. Trauma conference, multi-disciplinary (morbidity and mortality conference), that includes all members
of the trauma team held at least monthly. E* c. Medical records review, utilization review, tissue review of trauma cases. E* d. Clinical trauma nursing audit. E* 2. Disaster Planning and Rehearsal. E* 3. Participation in Trauma Audit Committee (bi-county). E* 4. Regional Trauma Committee, if required by EMS Office. E* 5. Regional Trauma System Evaluation, if required by EMS Office. E* 6. Special Audit of triage appropriateness, if required by EMS Office. E* 7. Special audit of the cost of trauma by diagnosis, if required by the EMS Office. E 8. Participation in the trauma system data management system. F. Education 1. Formal continuing education programs in trauma care for: E a. Staff Physicians E b. Staff Nurses E c. Staff allied health personnel d. Local EMS personnel including: E 1) First Responders E 2) EMT-IA's E 3) Paramedics E e. Community Physicians and other health care personnel. E* 2. Public Education programs including: a. Injury prevention in the home and industry, and on the highways and athletic fields. b. Problems confronting public, medical profession, and hospitals regarding optimal care for the injured.

- 14 -
5. Transport Times
6. Service Areas The Contra Costa County trauma system includes a single service area, which is the entire area of the county. In January 1986, following approval of the County’s Trauma System Plan, a request for proposal was submitted to all hospitals licensed for Basic Emergency Services. Only one hospital, John Muir Medical Center located in Walnut Creek, chose to submit a trauma center proposal. Six years later in 1992, the County Board of Supervisors reopened trauma center designation to all hospitals. John Muir Medical Center remained the only hospital interested in trauma center designation.
Table IV-1. Average Code 3 Transport Time to John Muir Medical Center, 2000
Community Average
Transport Time (minutes)
Number of Code 3 Transports
Alamo NA 4 Antioch 23.7 32 Bay Point 18.0 8 Clayton 11.3 9 Concord 11.4 151 Crockett 24.5 2 Danville NA 3 El Cerrito 31.5 4 El Sobrante 25.5 4 Hercules 21.5 2 Lafayette 10.8 33 Martinez 18.1 29 Moraga 17.7 6 Oakley 27.2 6 Orinda 12.0 6 Pacheco 9.8 4 Pinole 26.3 6 Pittsburg 18.6 35 Pleasant 9.3 41 Richmond 28.7 46 Rodeo 8.0 1 San Pablo 33.2 10 San Ramon NA 12 Walnut Creek 7.6 193 Total 13.3 647

- 15 -
7. Coordination with Neighboring Trauma Systems (See Section IV-B, above.) 8. Prehospital Services Prehospital services are provided by fire service first responders, by contract
ambulance services in exclusive operating areas (EOA’s), and by designated helicopter air ambulance services.
Contra Costa has not used air transport to geographically expand the primary
service area of the Contra Costa trauma system. However, the John Muir trauma center does cooperate with other counties and other trauma systems to accept out-of-county trauma patients when appropriate; i.e., when John Muir is the nearest available trauma center with a heliport for any patient for whom helicopter transport to a trauma center has been deemed appropriate.
Contra Costa’s Trauma System Plan as approved by the Board of Supervisors in
1985 requires that the County-designated trauma center have a “helicopter landing site with immediate access to trauma resuscitation room and operating suite.”
All prehospital personnel were trained in the County’s trauma treatment and triage
protocols prior to the implementation of the trauma system in 1985. Following that time, these protocols are included as a part of the accreditation required of all new paramedics. Additionally, all paramedics are required to by PHTLS or BTLS certified.
All ambulances are required by County ordinance to equipped with two-way
radios operating on the County MEDARS system, which provides for ambulance-to-hospital communication. In addition, all contracted ambulances services used for 9-1-1 response are required to equip paramedic ambulance units with cellular telephones.
County trauma protocols require early notification of trauma centers of the
impending arrival of a trauma patient. 9. Hospital Service Delivery (A) Critical Care See Section IV-C-4 “Resource Availability to Meet Staffing Requirements for
Trauma Center,” pp. 9-13, above. (B) Medical Organization and Management See Section IV-C-4 “Resource Availability to Meet Staffing Requirements for
Trauma Center,” pp. 9-13, above.

- 16 -
(C) Quality Improvement See Section IV-C-4 “Resource Availability to Meet Staffing Requirements for
Trauma Center,” pp. 9-13, above, and Section XII “Trauma System Evaluation,” pp. 28-29, below.

- 17 -
Section V Intercounty Trauma Center Agreements
A. Trauma Bypass
Contra Costa permits John Muir Trauma Center to go on “trauma bypass” under specified conditions when the resources of the trauma center are temporarily unavailable to care for additional trauma patients. Each episode of trauma bypass, including the conditions justifying bypass, is reported to the EMS agency for review. Attachment D is an agreement with Alameda County for transport of Contra Costa trauma patients to Alameda County trauma centers when John Muir is on trauma bypass.
B. Pediatric Trauma Center
Pediatric trauma patients meeting trauma center transport criteria are transported to the Children’s Hospital Level II pediatric trauma center in Alameda County. Attachment E is a copy of the agreement with Children’s Hospital.

- 18 -
Section VI Objectives
Seven objectives were identified in the Contra Costa County Trauma System Plan (1/86). During the past two years, each of these objectives has been addressed in detail. A brief description of how each objective has been met is given below. 1. Establish Standards for Trauma System Preparation and Response.
As part of initial trauma system planning, standards were identified for both the prehospital and the trauma center response to trauma system activation. In addition, training and educational standards were developed for those individuals in the field and in the trauma center who provide care to the acutely injured patient.
The set of standards for the Contra Costa County designated trauma center includes:
a. Organizational requirements b. Medical staff availability c. Trauma service requirements d. Special facilities, resources and capabilities e. Quality Assurance requirements f. Education requirements g. Written policy of non-discrimination h. Written transfer agreements with regional trauma centers. i. Written by-pass agreements and protocols with other designated trauma centers in
the region.
These standards meet or exceed those required in current State Trauma Care System Regulations for a Level II trauma center. The initial trauma center designation review and all subsequent reviews have demonstrated that John Muir Trauma Center, including its medical, nursing, and ancillary staffs, has met and maintained set standards.
Criteria for the triage and treatment of trauma patients in the prehospital setting have been established and policies reflecting these standards have been implemented. Evaluation of triage data over the last 20 months indicates that these triage standards have been effective.
Mechanisms for trauma system orientation have been established for EMT-Is, EMT-Ps, first responders and base hospital and receiving hospital personnel. Trauma system orientation programs were provided extensively for all groups prior to trauma system implementation. A video taped trauma system orientation program has been used since that time by ambulance provider agencies and base hospitals to assure new employees are well prepared to participate in the trauma care system. Extensive review of all trauma calls by the base hospitals and EMS staff has shown this method of orientation to be quite effective.
The trauma training standard established for prehospital personnel was defined in the Trauma System Plan as a training program which would meet or exceed that established by the American College of Surgeons as outlined in the Prehospital Life Support Curricula. Basic Trauma Life Support (BTLS), sponsored by the American College of Emergency Physicians has also been identified as an appropriate program to meet this standard. A number of paramedics, MICNs and emergency physicians have recently become BTLS instructors or providers and a series of BTLS courses is planned. Most prehospital personnel have not yet been trained to this standard, however.

- 19 -
Finally, standards for prehospital and trauma center response to trauma system activation have set the standard of care expected for Contra Costa County trauma patients. As such, these standards serve as a screening tool for the County and the internal trauma center quality assurance programs. All trauma cases, as identified through the trauma system are evaluated to these standards. This ongoing evaluation has clearly demonstrated an effective response to the needs of critically injured patients.
2. Establish Mechanisms to Ensure Continuing Compliance With Trauma System Standards
A number of mechanisms have been developed to ensure continuing compliance with trauma system standards. These mechanisms are detailed in Trauma System Policy 16.0. Over the last 20 months, findings generated through these mechanisms have been consistent and offer assurance that the mechanisms are effective and that set standards continue to be met.
3. Integrate and Coordinate Trauma Care with the Existing Emergency Medical System
Emphasis was placed on this objective during the planning and pre-implementation phases of trauma system development.
A multidisciplinary trauma care review committee was appointed to evaluate available emergency medical and trauma care resources and to make recommendations on appropriate standards for all phases of a trauma care system for Contra Costa County.

- 20 -
The Committee recommendations were incorporated into the Contra Costa County Trauma System Plan. To a large extent, trauma system components meshed well with the existing EMS system components, although several potential problems were immediately apparent. The solutions developed to allow full integration of the trauma system, have proved to be major EMS system enhancements as well. Communications - Field hospital communications capabilities had been identified as a major weakness of the EMS system. There was concern that the additional trauma communication demands could over stress field communications capabilities. Procedures for dispatch and field personnel were implemented to make efficient and effective use of available radio communications resources. Back-up procedures were implemented specific for trauma patient destination determination in the event that hospital communication was unavailable. Although this carefully monitored communications system appeared to work effectively with the integration of the trauma system, the subsequent integration of the cellular telephones into the EMS communications system was a clear enhancement. As a result of the 1986 emergency ambulance request for proposal process, all paramedic units are equipped with cellular telephones in addition to required County radio communications equipment. Transportation - As it had been determined that only one level 2 trauma center was needed to serve all of Contra Costa County, patient transport mechanisms were developed to assure county—wide access to the trauma system. Although no ALS helicopters were stationed in CCC, four private ALS helicopter provider agencies stationed in surrounding counties were in a position to provide adequate scene response times to areas remote from the trauma center, if contacted by first response units. Helicopter access procedures were developed in conjunction with ALS helicopter provider agencies. First responder and EMS dispatch agencies received orientation to these procedures. This transport resource is utilized on an average of 8 times per month. Comprehensive protocols for ALS and BLS ambulances were developed which included time-distance parameters and base contact for medical control points. Monthly review of all transported trauma cases by the EMS Agency and the base hospital indicates that patients needing trauma center level care are being transported to the trauma center. Those patients with longer transport times (30 minutes - 1 hour), have not been diverted to closer basic ED facilities with few exceptions, and do not appear to have suffered any ill effect from the extended transport. It is felt that any extended transport time is more than made up in the immediate availability of trauma center care.
ALS Field Management of Trauma Patients
Prior to trauma system implementation, the EMS Agency had been struggling in its efforts to introduce intubation as a paramedic skill. It was clear that implementation of this skill was mandatory for the safe transport of a number of these critically injured patients. The major stumbling block for this program had been the unavailability of OR experience as part of initial and on-going training. With the local hospital interest in and support for the trauma system, the EMS Agency was able to encourage hospitals to provide the necessary clinical training. Currently CCC paramedics are able to perform this skill if necessary.

- 21 -
4. Ensure for Definitive Trauma Care Regardless of Ability to Pay
The CCC trauma center is required by contract to accept all CCC trauma victims triaged and transported to the trauma center and provide appropriate medical treatment for said victims without regard to the patient’s ability to pay. In addition, the trauma center is required to provide inpatient medical care continuously and, where indicated and currently available at the hospital, out patient care for follow-up or rehabilitative services until the patient is discharged completely from medical care, except that certain patients may be transferred as follows:
(i) Patients who are members of recognized Health Maintenance Organizations may be promptly transferred to a hospital of that organization when such transfer is deemed prudent and medically indicated by the trauma physician in charge of the major trauma patient’s medical care in consultation with a physician representing the Health Maintenance Organization;
(ii) Patients who are covered by Medi-Cal may be transferred to a Medi-Cal contract hospital if the Trauma Center is not a Medi-Cal contract hospital when such transfer is deemed prudent and medically indicated by the physician in charge of the patient’s medical care in consultation with a physician representing a Medi-Cal contract hospital; and
(iii) Patients who are uninsured or otherwise unable to pay as determined by Hospital may be promptly transferred to a County hospital or other hospital designated by County when such transfer is deemed prudent and medically indicated by the trauma physician in charge of the major trauma patient’s medical care and when such transfer is accepted by County on medical grounds and in accordance with 24-hour per day, seven-day per week procedures presently established by the County Health Officer. A patient’s inability to pay shall not be a consideration in the medical treatment of the patient. County agrees to accept patients transferred pursuant to this provision when such patients are residents of Contra Costa County.
(iv) Regardless of the above, Hospital reserves the right to transfer any patient when it is determined that such transfer is necessary to provide such patient with treatment or medical care not available at Hospital.
This process appears to be working well, based on feed—back from the quality assurance processes. In addition, CCC recently adopted “Patient Transfer Guidelines” which include the establishment of a Transfer Review Panel. This panel will review all patient transfers between acute care facilities including transfers of trauma patients. This process will provide an additional mechanism for assuring that this objective is being met.
5. Coordinate Trauma Services with Service in Adjacent Counties
Potential weak links in a trauma system with only one trauma center are in the areas of quality assurance, specialized pediatric trauma care and back—up trauma resources. Fortunately, the Alameda County trauma system became operational shortly after implementation in CCC. From the beginning, the two EMS Agencies have worked together to develop mechanisms to enhance both systems.
The development of the bi-county Trauma Audit Committee, have provided CCC with trauma expertise in reviewing local trauma center care in an ongoing basis. (See Trauma Policy
- 22 -
#16 in Appendix B.)
Policies and procedures have been developed that include the consideration of Children’s Hospital, Oakland, the Alameda County designated pediatric trauma center, as the direct field destination for critically injured children. (See Trauma policy #8 in Appendix B.) The local adult trauma center is encouraged to transfer pediatric trauma when stable for transfer.
Trauma Center by-pass arrangements have been adopted by CCC and Alameda Counties so that trauma center level care is available during those times that the local trauma center is on by-pass. (See Trauma Policy #10 in Appendix B.)
The CCC EMS Agency continues to act as a resource to surrounding counties as they address the trauma care issue, and is committed to the regionalization of trauma care.
6. Ensure Accountability and Objective Evaluation Throughout the Trauma System
The quality assurance and system evaluation mechanisms described in Trauma Policy #16, Appendix B, have been tested and have proved to be effective tools in ensuring that this objective has been met.
7. Promote Public Awareness and Information Regarding Trauma Services
The Emergency Medical Care Committee’s Public Information and Education Sub-Committee has developed an information packet and a trauma system speakers bureau consisting of knowledgeable individuals who are available to give presentations to community groups.
John Muir Trauma Center has developed a trauma system brochure that has been made available. Trauma center personnel are also responsive to community requests for speakers on the CCC trauma system.
- 23 -
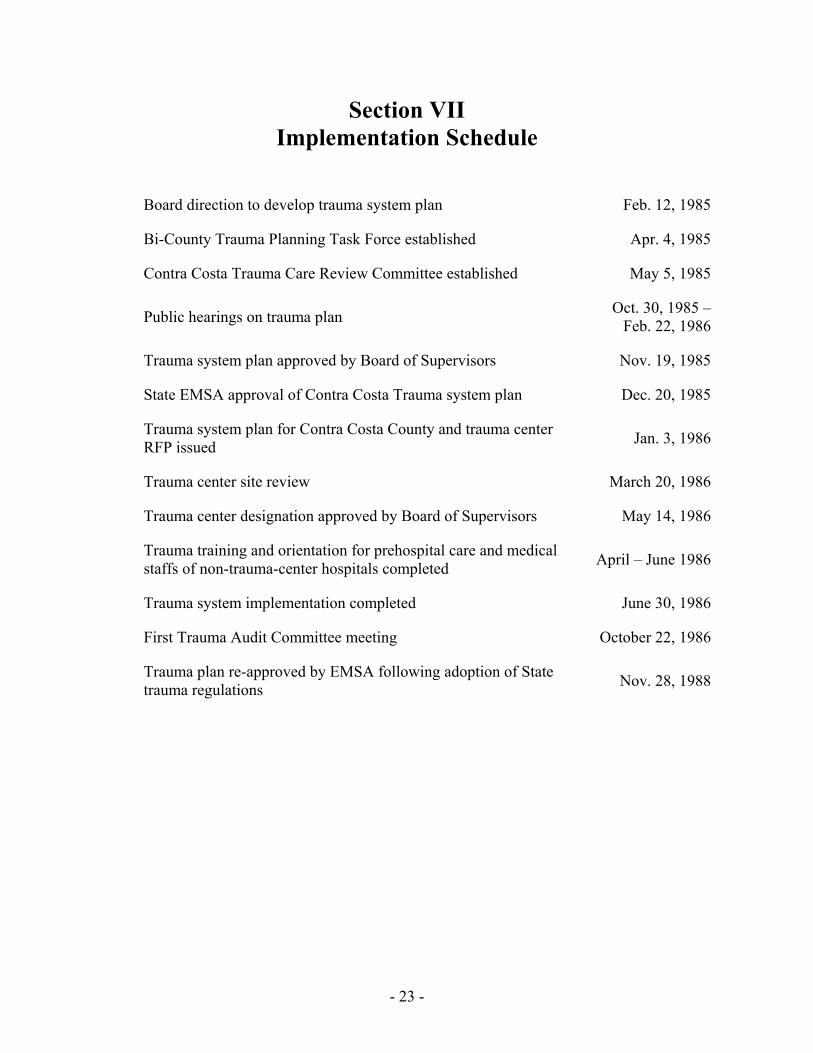
Section VII Implementation Schedule
Board direction to develop trauma system plan Feb. 12, 1985
Bi-County Trauma Planning Task Force established Apr. 4, 1985
Contra Costa Trauma Care Review Committee established May 5, 1985
Public hearings on trauma plan Oct. 30, 1985 – Feb. 22, 1986
Trauma system plan approved by Board of Supervisors Nov. 19, 1985
State EMSA approval of Contra Costa Trauma system plan Dec. 20, 1985
Trauma system plan for Contra Costa County and trauma center RFP issued Jan. 3, 1986
Trauma center site review March 20, 1986
Trauma center designation approved by Board of Supervisors May 14, 1986
Trauma training and orientation for prehospital care and medical staffs of non-trauma-center hospitals completed April – June 1986
Trauma system implementation completed June 30, 1986
First Trauma Audit Committee meeting October 22, 1986
Trauma plan re-approved by EMSA following adoption of State trauma regulations Nov. 28, 1988

- 24 -
Section VIII Fiscal Impact
Specific data on the initial fiscal impact of the trauma system was not collected. At this time the Contra Costa County trauma system has been in continuous operation for over 15 years. During this period, there have been no significant changes in the operation of the trauma system which would have a fiscal impact on the trauma center, other hospitals, prehospital providers, or the local EMS agency.

- 25 -
Section IX Policy and Plan Development
The county’s trauma policies are contained in full in the February 1988 Addendum to the
Trauma System Plan for Contra Costa County (Appendix B), which was submitted to and approved by the Emergency Medical Services Authority in 1988. These policies include:
Trauma Policy 01.1 Trauma Care System – Multidisciplinary Approach Trauma Policy 02.0 Trauma Care System – Public Information and Education Trauma Policy 03.0 Trauma Care System – Marketing and Advertising Trauma Policy 04.0 Trauma Care System – Establishment of Service Area for the
Trauma Center Trauma Policy 05.0 Trauma Care System – EMS Dispatching Trauma Policy 06.0 Trauma Care System – Communication System Trauma Policy 07.0 Trauma Care System – Transportation
Attachment #1 – Operational Procedures for Helicopter Trauma Rendezvous at Brookside Helipad and General Operational Procedures for Patient Transport by ALS Helicopter
Attachment #2 – Transfer of Critical or Potential Critical Trauma Patients to the Trauma Center
Attachment #3 – Trauma Center By-pass Alert Trauma Policy 08.0 Trauma Care System – Pediatrics
Attachment #1 – Trauma – Pediatric – Field Treatment and Destination Determination
Trauma Policy 09.0 Trauma Care System – Training of Prehospital EMS Personnel Trauma Policy 10.0 Trauma Care System – EMS/Trauma Care Coordination and
Mutual Aid between Neighboring Counties Trauma Policy 11.0 Trauma Care System – Coordination and Integration of Trauma
Care with Non-Medical and Non-Trauma Center Emergency Services
Trauma Policy 12.0 Trauma Care System – Fees Trauma Policy 13.0 Trauma Care System – Medical Control and Accountability
Attachment #1 – Trauma Patient Identification and Triage Attachment #2 – Trauma – Adult – Field Treatment and Destination Determination Attachment #3 – Trauma Transport Guidelines for Field Personnel
Trauma Policy 14.0 Trauma Care System – Organization and Management Trauma Policy 15.0 Trauma Care System – Data Collection and Management
Attachment #1 – Bay Area Trauma Registry (Note: This has been superceded by the joint adoption by Contra Costa and Alameda Counties in ____ of the Lancet Trauma One registry.)
Trauma Policy 16.0 Trauma Care System – Quality Control and System Evaluation Trauma Policy 17.0 Trauma Care System – Availability of Trauma Personnel Trauma Policy 18.0 Trauma Care System – Trauma Center Designation Process

- 26 -
Section X Written Local Approval
In 1985, following extensive media publicity around delayed care and the subsequent death of a trauma patient initially transported to one of the county’s hospitals licensed to provide Basic Emergency Services, the Board of Supervisors directed the Department of Health Services to develop a countywide trauma system plan. An initial step was the formation of a Joint Contra Costa-Alameda Trauma Planning Task Force to help educate key personnel in both counties about trauma systems and trauma system planning. Subsequently, Contra Costa established a Trauma Care Review Committee to develop and recommend at trauma system plan for Contra Costa County. This plan was approved by the Board of Supervisor in November 19, 1985 and issued in January 1986. A copy of the Contra Costa Board of Supervisors action approving the plan is contained in Attachment G.

- 27 -
Section XI Data Collection
(1) Contra Costa County has adopted the Lancet Trauma One trauma registry for its
standardized data collection and data management system for trauma care. The Trauma One registry includes prehospital, emergency department, and hospital data for all trauma patients treated or admitted to the John Muir Medical Center. Trauma One registry data is also available to Contra Costa from Alameda County on those Contra Costa patients transported to an Alameda County trauma center. The trauma registry data is supplemented by prehospital care reports and hospital disposition data for those patients transported to a non-trauma-center hospital.
(2) Prehospital data included in the Trauma One registry as implemented in Contra Costa County
include all data elements required by §100176 of the EMT-P regulations. These are listed in Attachment H. (Contra Costa County does not have an EMT-II program.)
(3) Hospital data included in the Trauma One registry as implemented in Contra Costa County
include all data as outlined in §100257(c) of the trauma regulations. Specific elements are listed in Attachment H.
.
- 28 -
Section XII Trauma System Evaluation
(1) Ongoing evaluation of the trauma center is carried out through the bi-county Trauma
Audit Committee (TAC) and Pre-TAC process. The TAC provides medical quality assurance by reviewing the medical management of all trauma cases identified either by the Pre-TAC of by EMS staff and may include:
- trauma deaths occurring in the prehospital setting, in non-trauma-center hospitals,
or in a trauma center; - cases with aspects that vary from established standards; and - cases having teaching value or that demonstrate unusual or extraordinary
management skills. TAC membership includes: - the trauma director from each of the four trauma centers in Contra Costa and
Alameda Counties; - the emergency department director of physician designee from each trauma
center; - the trauma nurse coordinator for each trauma center; - an emergency physician from a non-trauma-center hospital in each county; - a trauma surgeon recommended by the Alameda-Contra Costa Medical
Association; - a trauma center neurosurgeon from the hosting trauma center (rotating); - an anesthesiologist from the hosting trauma center (rotation); - a pediatric trauma surgeon; - a forensic pathologist from each county; - a base hospital coordinator from each county; - the EMS medical director from each county (non-voting); - the EMS trauma coordinator from each county (non-voting); and - the EMS director or program coordinator from each county (non-voting).
Assisting the TAC is the Contra Costa Pre-TAC. The purpose of Pre-TAC is to screen major trauma cases and recommend those for review by TAC. Potential cases are reviewed for appropriateness and timeliness of care within trauma center as well as in the field setting. Pre-TAC membership includes:
- the Contra Costa trauma center medical director; - a visiting trauma center medical director (rotating); - the trauma center emergency department director or physician designee; - a base hospital liaison physician from Contra Costa County; - a base hospital liaison physician from Solono County; - the trauma center nurse coordinator; - a surgeon from the Kaiser Permenente Medical Group;

- 29 -
- the EMS medical director; and - the EMS trauma coordinator.
(2) Contra Costa County has established a process to receive information regarding the trauma plan, triage criteria, activation of the trauma team, and notification of specialists through the trauma registry.
(3) Periodic performance evaluation of the trauma system is provided on an annual basis
through the EMS Agency annual reporting system, which includes the County’s Emergency Medical Care Committee and the Alameda-Contra Costa Medical Association. Additionally, especially during the early years of the trauma system, the EMS Agency has used outside teams to provide periodic reviews.
(4) The Level II trauma center, which is the only facility designated by Contra Costa County to receive trauma patients, is required to have an internal quality improvement process as well as to participate in the TAC process described above.

- 30 -
List of Attachments
Attachment A Trauma System Plan for Contra Costa County, January 1986. Attachment B Trauma System Plan for Contra Costa County, Addendum – February 1988. Attachment C Hospital Agreement (Trauma Center Designation) contract between John Muir Medical
Center and Contra Costa County, May 22, 1992. Attachment D Memorandum from Alameda EMS to Contra Costa EMS dated May 15, 1987. Attachment E Letter from Children’s Hospital Oakland to Contra Costa EMS dated July 1, 1986. Attachment F Memorandum from John Muir Medical Center to Contra Costa EMS dated February 2, 2001. Attachment G Contra Costa Board of Supervisors action approving the Trauma System Plan for Contra
Costa County, November 19, 1985. Attachment H Trauma Registry Data Elements Collected by Contra Costa County.

Attachment A
Trauma System Plan for Contra Costa County, January 1986

Attachment B
Trauma System Plan for Contra Costa County, Addendum –
February 1988

Attachment C
Hospital Agreement (Trauma Center Designation) contract between John Muir Medical Center and Contra Costa County,
May 22, 1992

Attachment D
Memorandum from Alameda EMS to Contra Costa EMS dated May 15, 1987

Attachment E
Letter from Children’s Hospital Oakland to Contra Costa EMS dated July 1, 1986

Attachment F
Memorandum from John Muir Medical Center to Contra Costa EMS dated February 2, 2001

Attachment G
Contra Costa Board of Supervisors action approving the Trauma System Plan for Contra Costa County, November 19, 1985

Attachment H
Trauma Registry Data Elements Collected by Contra Costa County

Trauma Registry Data Fields Entered by John Muir Medical Center, Contra Costa County. Main/personal: 1. Account number 2. Medical record number 3. Admission date 4. Emergency record number 5. First trauma phase 6. Admission time 7. Last name 8. First name 9. Last name (AKA) 10. Sex 11. Age 12. Birth date 13. Race 14. Zip 15. Injury date 16. Prehospital form y/n 17. Trauma criteria 18. Next trauma phase 19. Length of stay (days) 20. Injury severity score 21. Financial 22. Total hospital charges Field Injury Details: 1. Patient severity 2. EMS provider(s) 3. Extrication performed 4. Street 5. City 6. State 7. County 8. Fall height 9. Injury class 10. Vehicular speed 11. Where was patient 12. What caused the injury 13. ICD-9 E-code 14. Protection 15. Motivation

Field VS/Treatments: 1. Pulse 2. Respirations 3. Systolic, diastolic, mean BPs 4. Circulation, respiratory rate, abdomen/thorax, motor, speech (CRAMS) 5. Eye opening, verbal, motor response, GCS 6. Raw revised Trauma score, Revised Trauma score. 7. Treatment, quantity Field Referring Facility: 1. Transferring facility date of arrival, 2. Transferring facility date of exit 3. Transferring facility time of arrival, 4. Transferring facility time of exit 5. Transferring facility prior trauma phase 6. Transferring facility next trauma phase Transport Details: 1. Referring facility 2. Transport date called, 3. Transport time called 4. Base contact time 5. Run sheet number 6. Transport agency 7. Transport mode 8. Rendezvous time 9. Time dispatched 10. Time at scene 11. Time departed scene 12. Transport unit id 13. ETA Trauma Receiving Area: 1. Major trauma y/n 2. Arrival date 3. Arrival time 4. Exit date 5. Exit time 6. Prior trauma phase 7. Next trauma phase 8. Time entered resus 9. Time left resus 10. TRA subcategory

11. Length of stay (hours) 12. Left via Trauma Team Details 1. Code date 2. Activation time 3. Specialty 4. Member id 5. Time called 6. Time arrived TRA Vitals: 1. Date 2. Time 3. Resp rate 4. Assisted resp rate 5. Systolic, diastolic mean BPs 6. Eye opening 7. Verbal response 8. Motor response 9. GCS 10. Pulse rate 11. Pulse oximetry 12. Raw revised trauma score 13. Revised trauma score 14. Circulation, respiration, abdomen/thorax, motor, speech (CRAMS) 15. Alcohol level mg% 16. Urine output ml/hr 17. Nasogastric output ml/hr 18. Chest tube output Trauma treatments: 1. Treatment 2. Quantity Trauma Surgical Procedures 1. ICD-9 2. Type 3. Primary surgeon Trauma Radiology: 1. Order time 2. Study 3. Body part

Trauma Consultations: 1. Physician 2. Specialty Emergency Department Receiving: 1. Major trauma y/n 2. Arrival date 3. Arrival time 4. Exit date 5. Exit time 6. Prior trauma phase 7. Next trauma phase 8. Time entered resus 9. Time left resus 10. ED subcategory 11. Length of stay (hours) 12. Left via Emergency Department Team Details: 1. Code date 2. Activation time 3. Specialty 4. Member id 5. Called 6. Arrived Emergency Department Vital Signs: (See TRA Vitals; same for this phase) Emergency Department Treatments: 1. Treatment 2. Quantity Emergency Department Radiology: 1. Order time 2. Study 3. Body part Emergency Department Consultations: 1. Physician 2. Specialty

Emergency Department Surgical Procedures: 1. ICD-9 2. Type 3. Primary surgeon Surgical Procedures, OR 1. Arrival date 2. Arrival time 3. Transfer date 4. Transfer time 5. Prior trauma phase 6. Unplanned return 7. OR subcategory 8. Length of stay (hours) 9. Next trauma phase Surgery details: 1. Date 2. Start time 3. End time 4. ICD-9 5. Type 6. Primary surgeon (SubOR 1,2,3 the same fields) Recovery Room: 1. Arrival date 2. Arrival time 3. Transfer date 4. Transfer time 5. Prior trauma phase 6. Next trauma phase 7. O.R.R. subcategory 8. Length of stay (hours) ICU: 1. Arrival date 2. Transfer date 3. Prior trauma phase 4. Next trauma phase 5. ICU subcategory 6. Unplanned return 7. Length of stay (days)

Surgical Procedure, ICU: 1. Date 2. ICD-9 3. Type 4. Primary Surgeon Post Hospital Details: 1. Date of hospital exit 2. Time of hospital exit 3. Prior trauma phase 4. Discharge to 5. Basis for choice 6. Final outcome 7. Destination facility Deaths: 1. Extent of autopsy 2. Organ donation requested y/n 3. Autopsy id number 4. Donated organs Readmission/Follow-up: 1. Arrival date 2. Next trauma phase 3. Transfer date 4. Prior trauma phase 5. Unplanned return Diagnoses: 1. Class 2. ICD-9 3. AIS value 4. Body part