treating dyslipidemia: an evolving paradigm filetreating dyslipidemia: an evolving paradigm om p....
TRANSCRIPT
Treating Dyslipidemia: An Evolving Paradigm
Om P. Ganda MDDirector, Lipid ClinicJoslin Diabetes Center
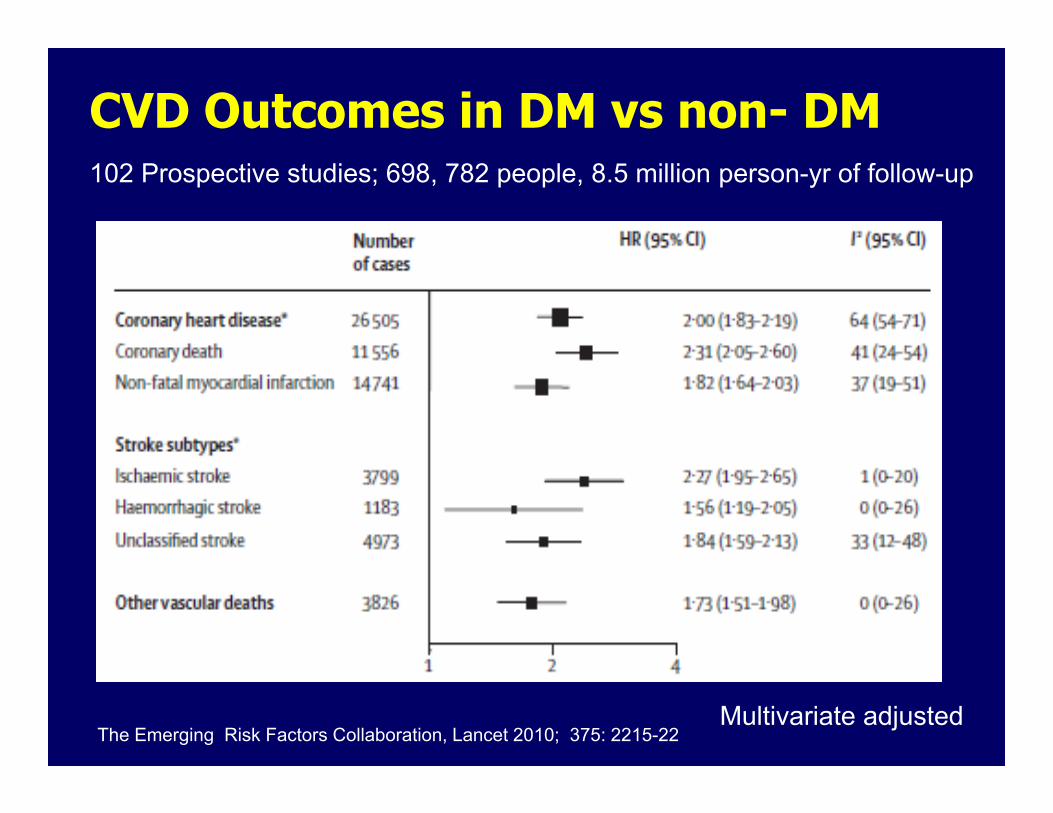
CVD Outcomes in DM vs non- DM102 Prospective studies; 698, 782 people, 8.5 million person-yr of follow-up
The Emerging Risk Factors Collaboration, Lancet 2010; 375: 2215-22Multivariate adjusted
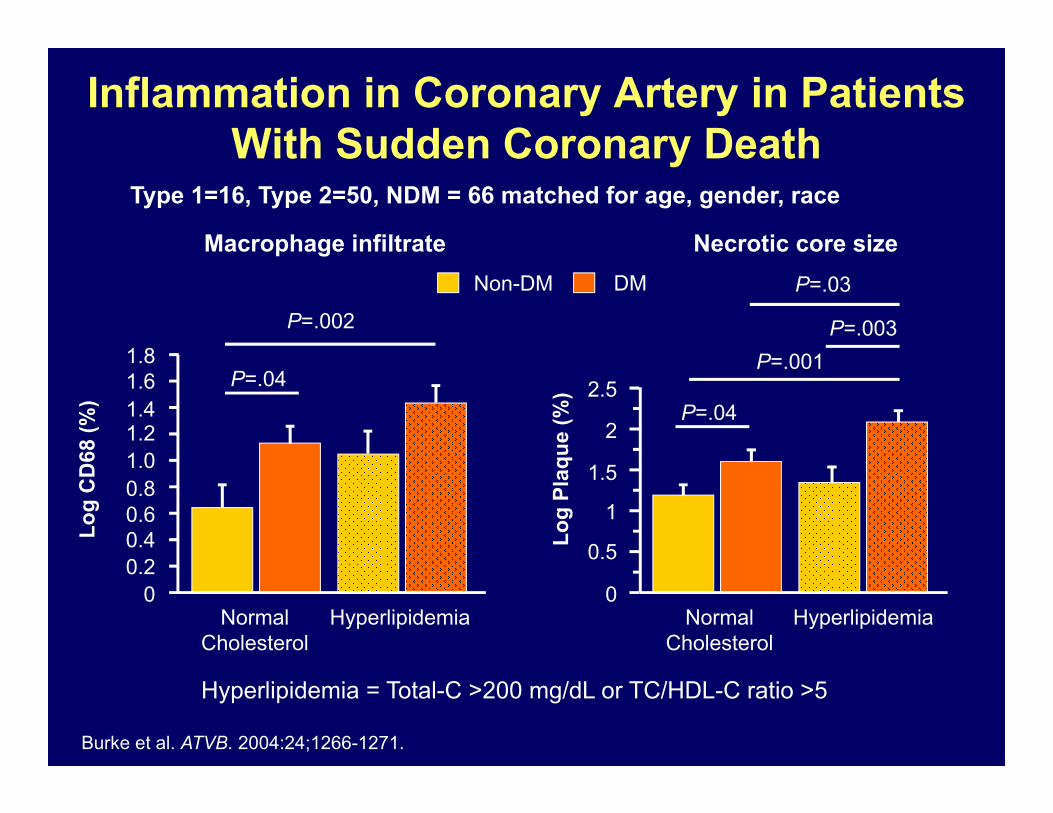
Inflammation in Coronary Artery in Patients With Sudden Coronary Death
Type 1=16, Type 2=50, NDM = 66 matched for age, gender, race
Hyperlipidemia = Total-C >200 mg/dL or TC/HDL-C ratio >5
Burke et al. ATVB. 2004:24;1266-1271.
Macrophage infiltrate Necrotic core size
Log
CD
68 (%
)
Log
Plaq
ue (%
)
Normal Cholesterol
Hyperlipidemia
1.81.61.41.21.00.80.60.40.2
0
P=.04
P=.002
0.5
0
1
1.5
2
2.5P=.04
P=.001P=.003
P=.03
Normal Cholesterol
Hyperlipidemia
Non-DM DM

Supremacy of Statins in CVD Risk Reduction
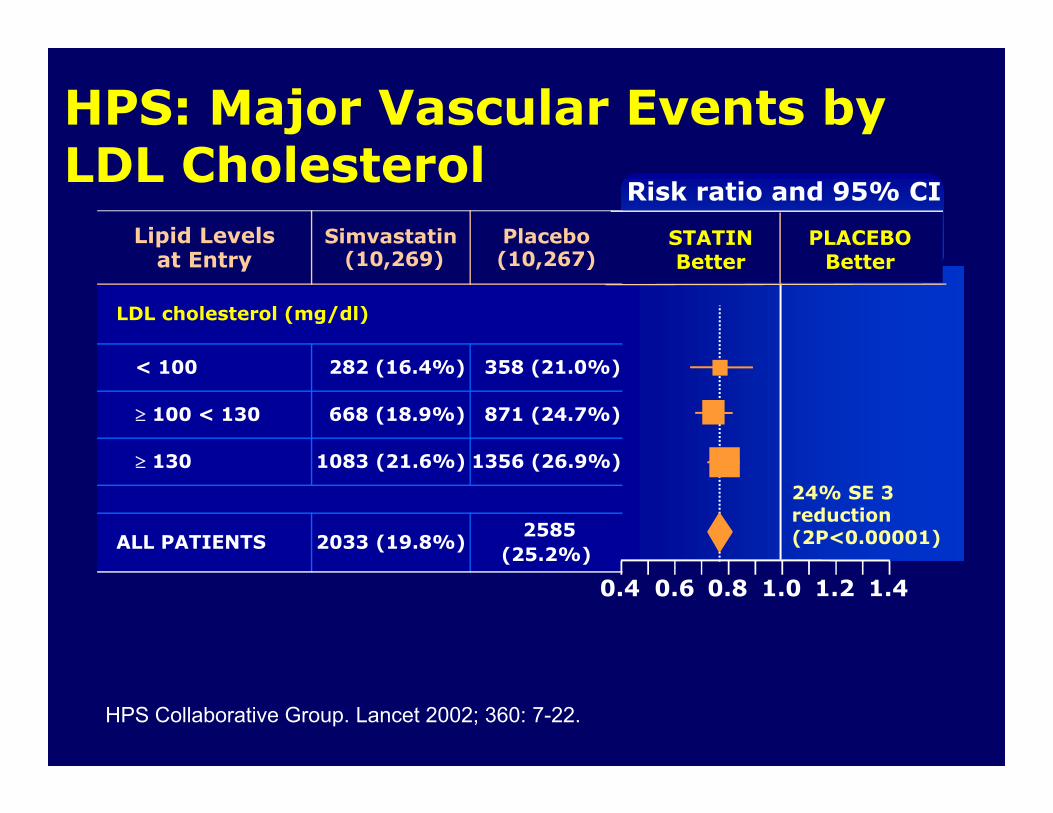
Lipid Levelsat Entry
Simvastatin(10,269)
Placebo (10,267)
LDL cholesterol (mg/dl)
< 100 282 (16.4%) 358 (21.0%)
100 < 130 668 (18.9%) 871 (24.7%)
130 1083 (21.6%) 1356 (26.9%)
ALL PATIENTS 2033 (19.8%)2585
(25.2%)
HPS: Major Vascular Events by LDL Cholesterol
Risk ratio and 95% CI
STATINBetter
PLACEBOBetter
24% SE 3reduction(2P<0.00001)
0.6 0.8 1.0 1.2 1.40.4
HPS Collaborative Group. Lancet 2002; 360: 7-22.
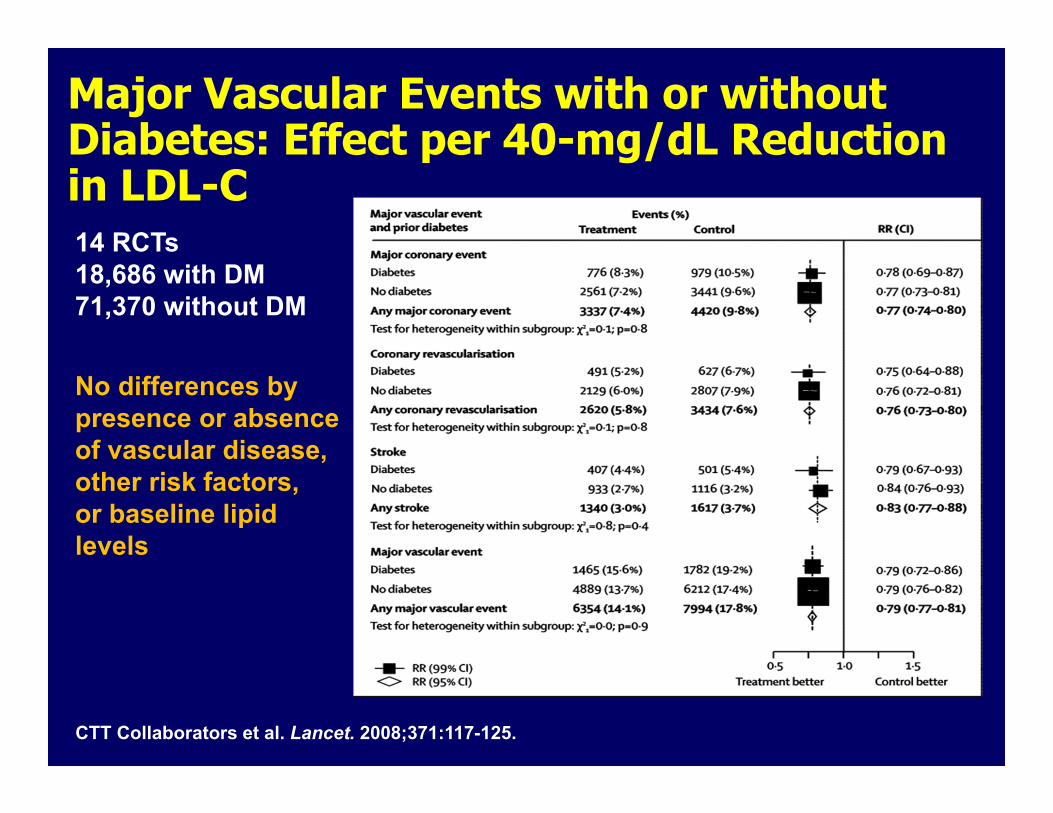
Major Vascular Events with or without Diabetes: Effect per 40-mg/dL Reduction in LDL-C14 RCTs18,686 with DM71,370 without DM
CTT Collaborators et al. Lancet. 2008;371:117-125.
No differences by presence or absence of vascular disease, other risk factors, or baseline lipid levels
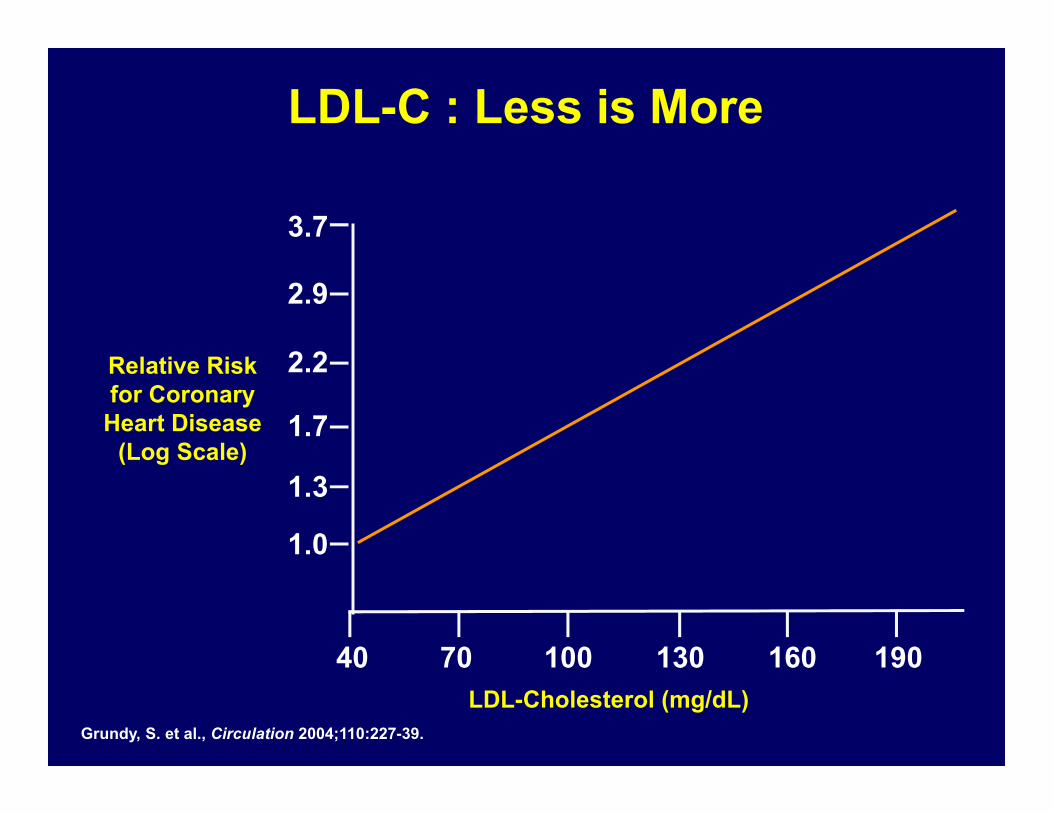
LDL-C : Less is More
3.7
2.9
2.2
1.7
1.3
1.0
40 70 100 130 160 190
Relative Risk for Coronary
Heart Disease (Log Scale)
LDL-Cholesterol (mg/dL)Grundy, S. et al., Circulation 2004;110:227-39.
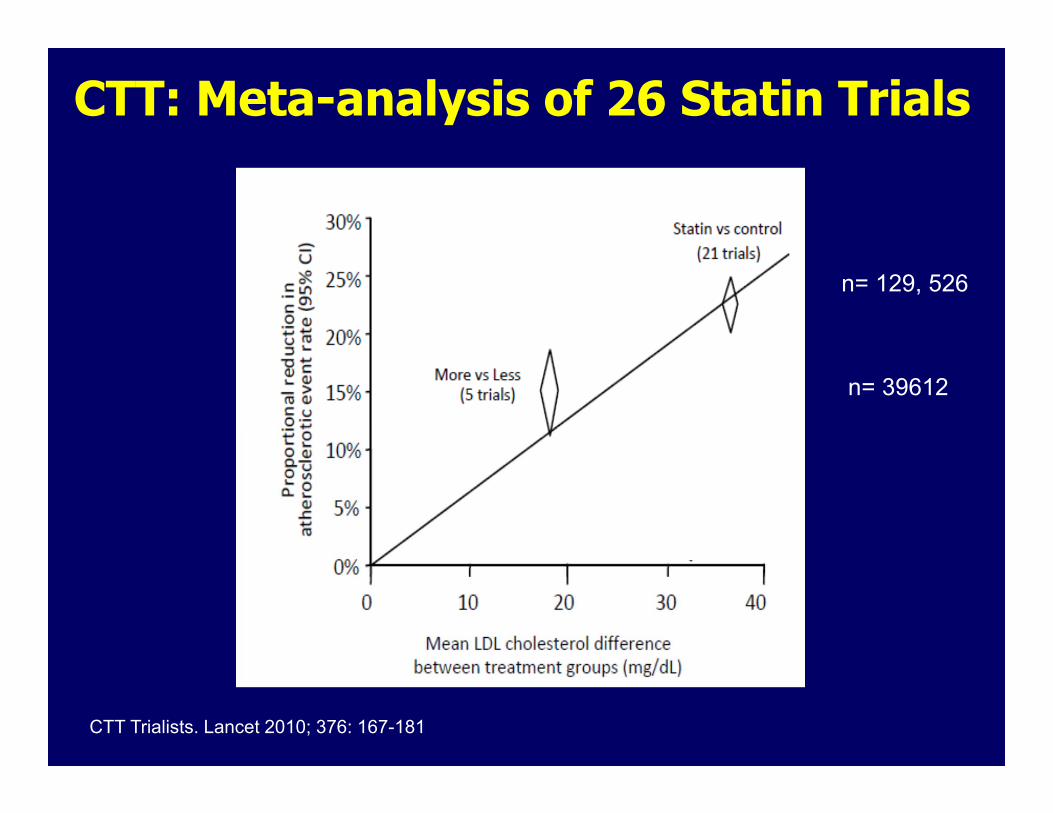
CTT: Meta-analysis of 26 Statin Trials
CTT Trialists. Lancet 2010; 376: 167-181
n= 129, 526
n= 39612
Is there a point of No-Return?
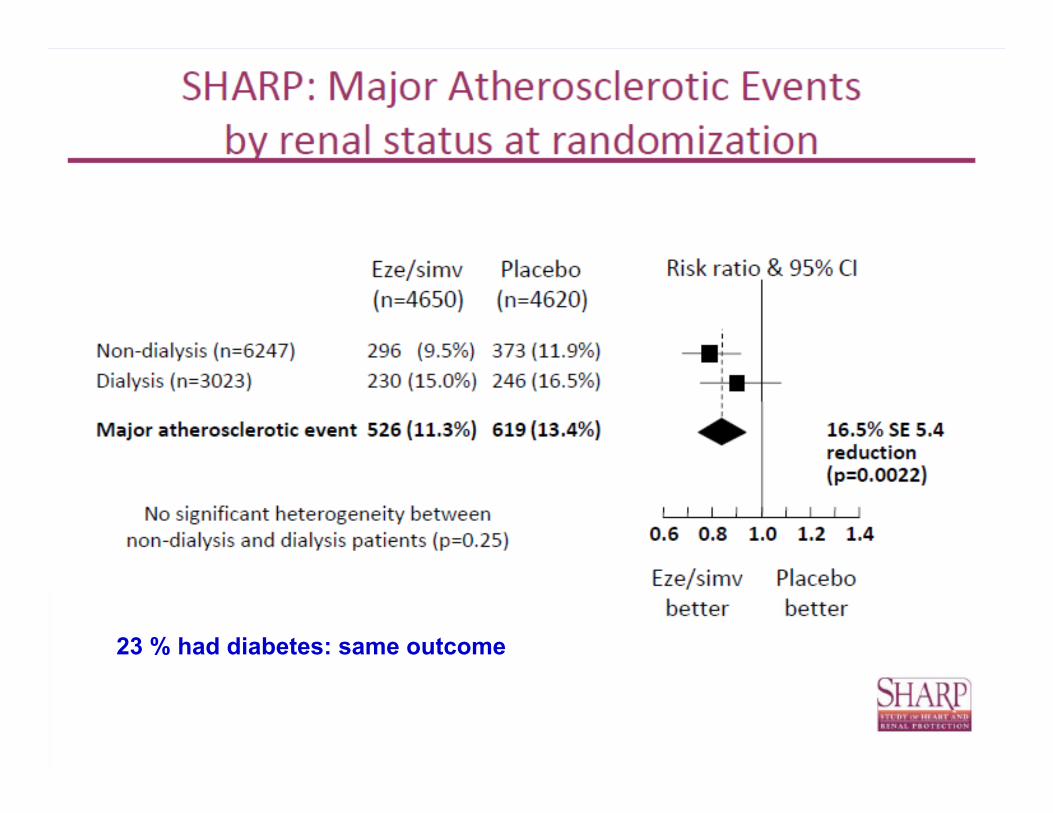
23 % had diabetes: same outcome
~ 10-15 % of patients have significant myalgia with statins, most with dose escalation
Underlying Mechanism(s)?

FDA Drug Safety Communication: New restrictions, contraindications, and dose limitations for simvastatin to reduce the risk of muscle injury
06-08-2011
Audience Response Question 1
Recent meta-analysis of clinical trials have shown an increased risk of diabetes. How high is the approximate risk?
A. 5%B. 10%C. 15 %D. 20%
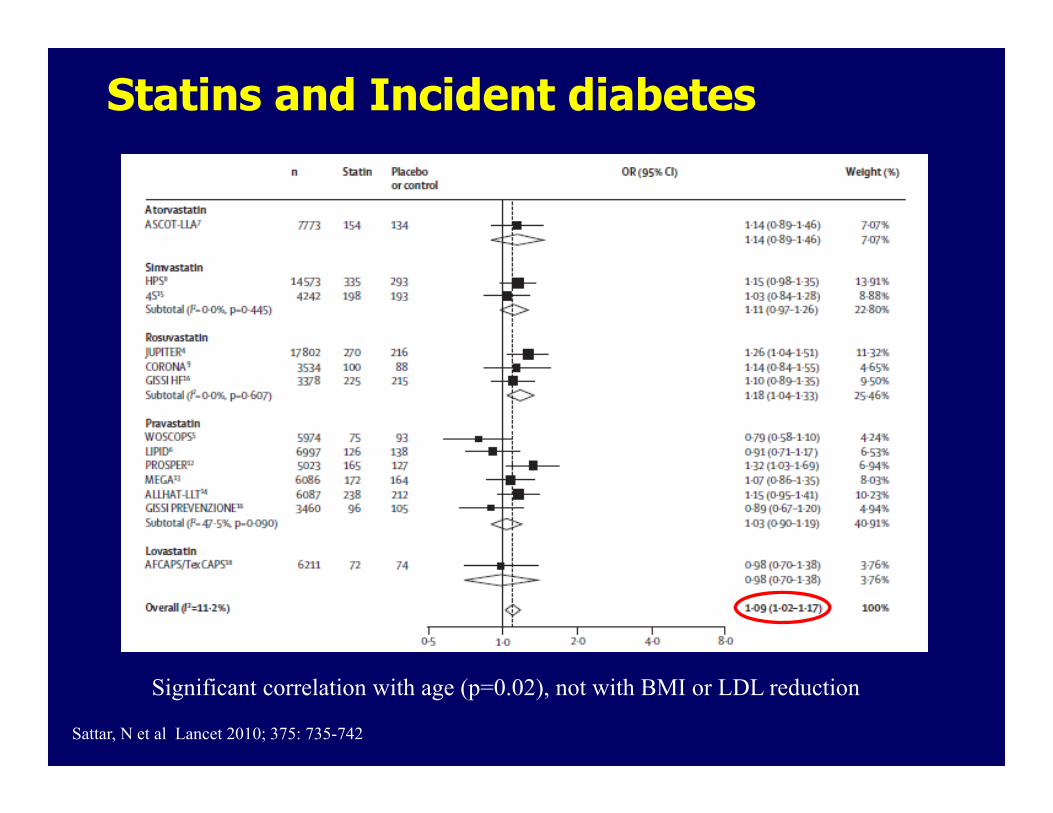
Statins and Incident diabetes
Significant correlation with age (p=0.02), not with BMI or LDL reduction
Sattar, N et al Lancet 2010; 375: 735-742
To put it in Perspective:
Incidence of Diabetes with statin therapy:
~1 new case per 200 persons treated over 5 years
Incidence of Major Cardiovascular Event~ 5 new events prevented per 200 persons treated over 5 years
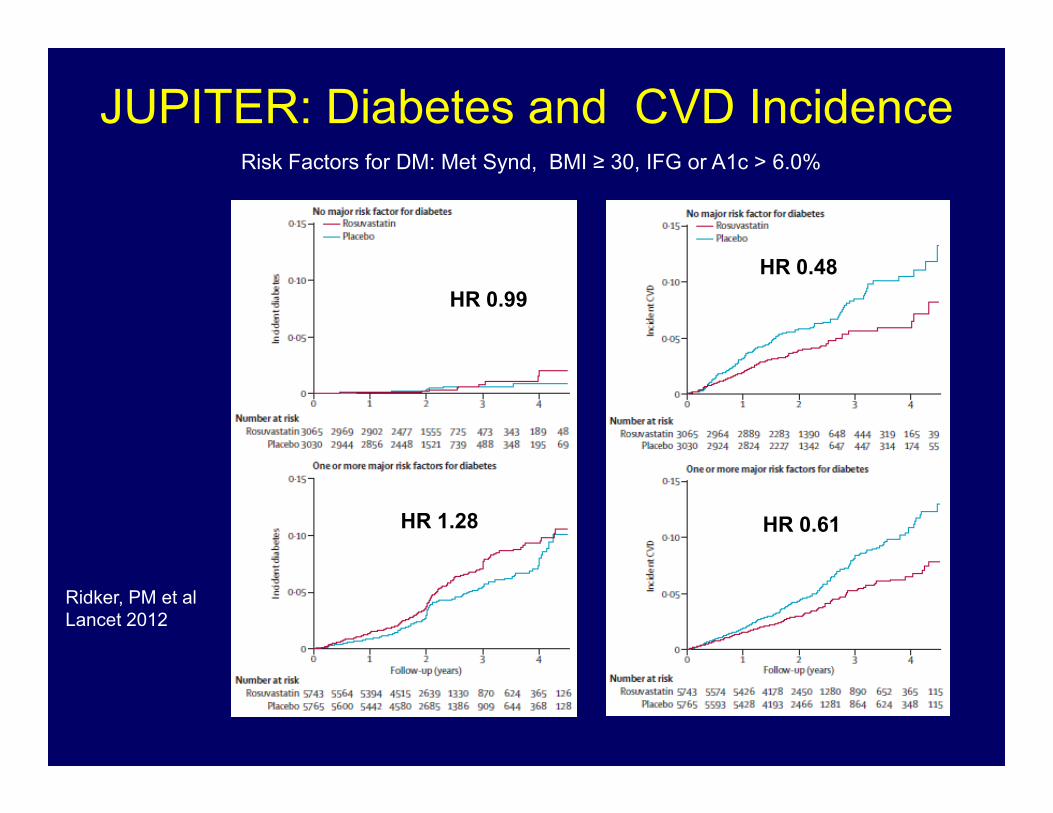
JUPITER: Diabetes and CVD IncidenceRisk Factors for DM: Met Synd, BMI ≥ 30, IFG or A1c > 6.0%
Ridker, PM et alLancet 2012
HR 0.99
HR 1.28
HR 0.48
HR 0.61
LDL-C-Lowering Drugs
Drugs reducing cholesterol synthesis • HMG CoA reductase inhibitors: statins (preferred)
– LDL-C reduction up to 60% – Latest addition: pitavastatin
Drugs reducing cholesterol absorption• Bile acid sequestrants (BAS)
– Colesevelam, cholestyramine, colestipol Bind to bile acids > increase excretion of cholesterol
LDL-C reduction 15-25%; TG may rise– Cholesterol transport inhibitor
Ezetimibe; binds to intestinal cholesterol transporterLDL-C reduction ~15-20%
Potential LDL Lowering Agents
Anti-sense apoB synthesis inhibitor: Mipomersen
~ 30% reduction in LDL-C in patients with FH
(Baseline LDL-C: >300 mg/dl)
MTP-1 Inhibitors: Lomitapide
Inhibits assembly of all Apo-B lipoporoteins
PCSK-9 Inhibitors: REGN 727
Prevent degradation of LDL receptors
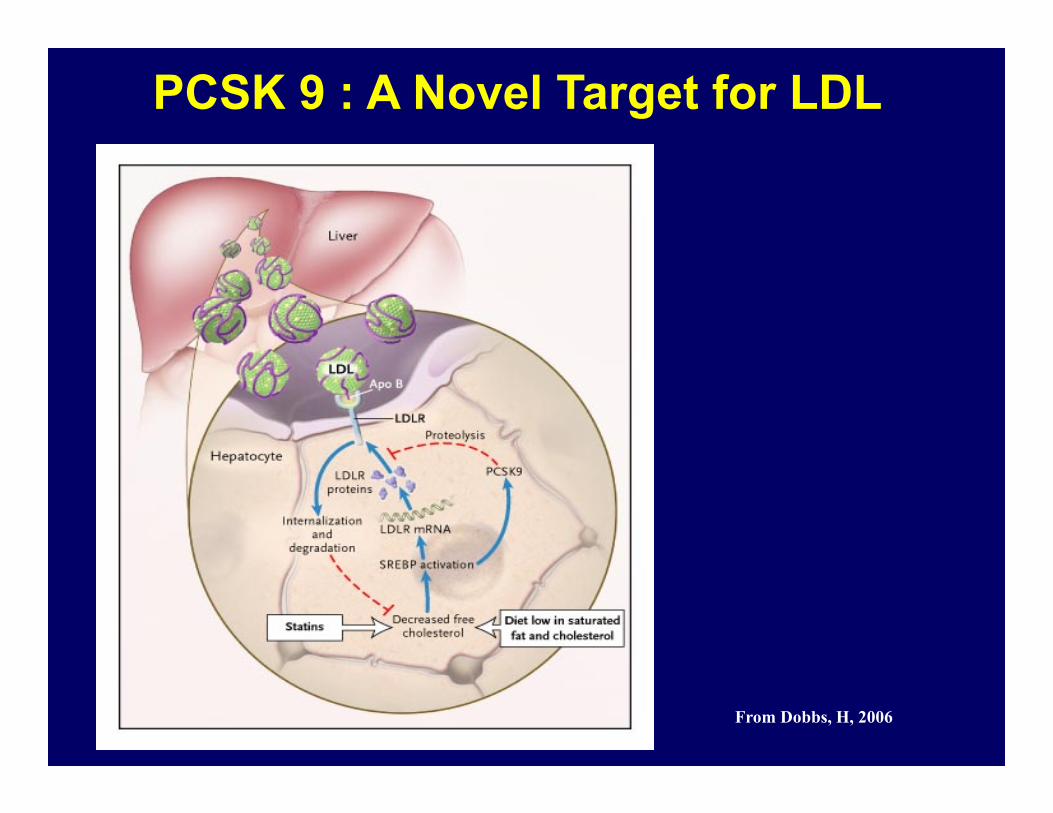
PCSK 9 : A Novel Target for LDL
From Dobbs, H, 2006
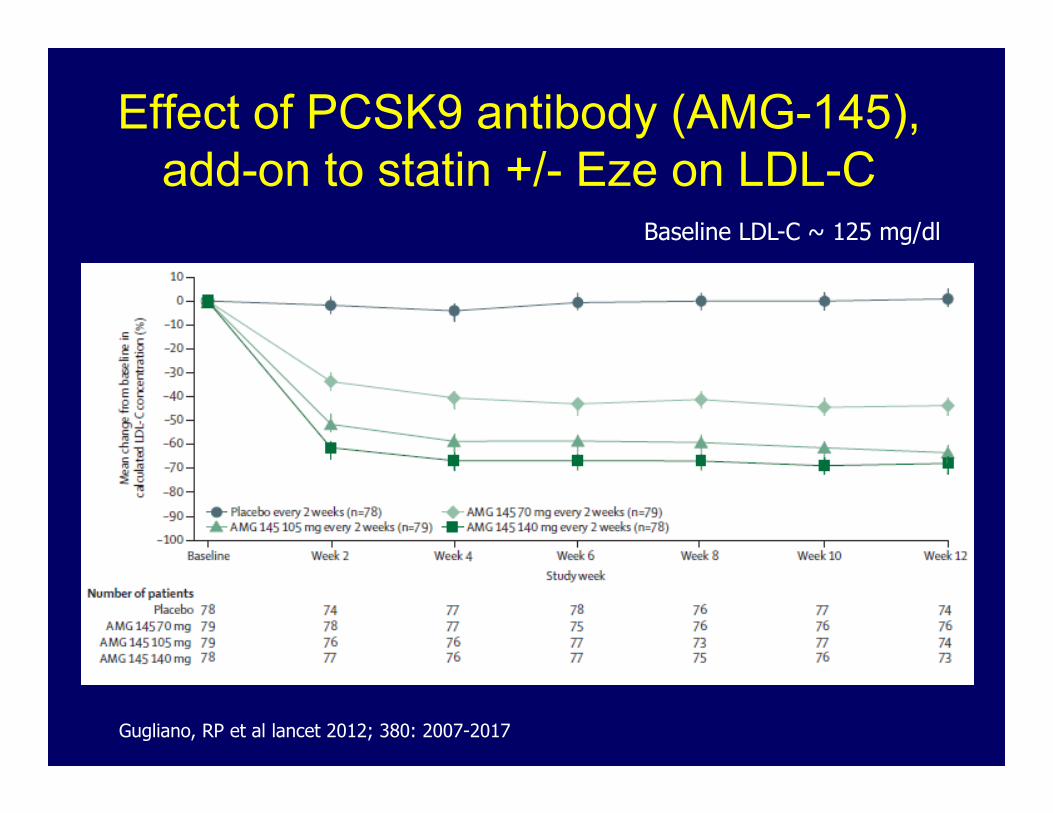
Effect of PCSK9 antibody (AMG-145), add-on to statin +/- Eze on LDL-C
Baseline LDL-C ~ 125 mg/dl
Gugliano, RP et al lancet 2012; 380: 2007-2017
How to deal with the Residual Risk of CVD after achieving
LDL-C Goal?
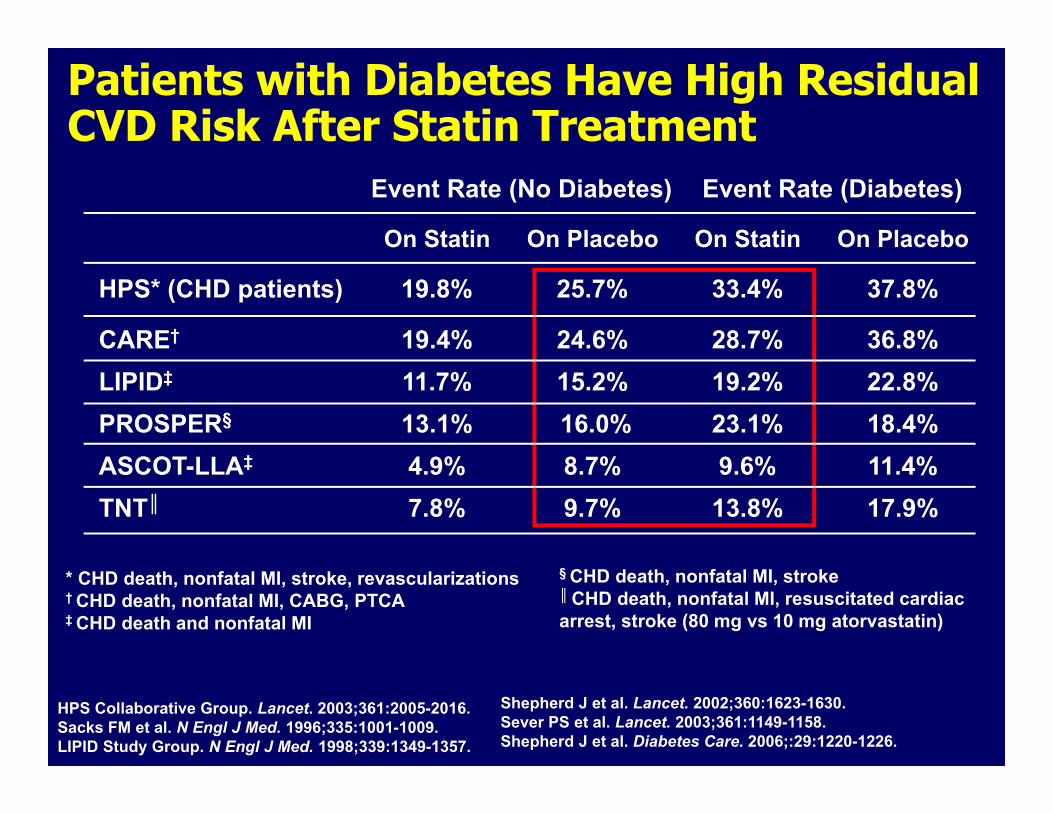
Patients with Diabetes Have High Residual CVD Risk After Statin Treatment
Event Rate (No Diabetes) Event Rate (Diabetes)
On Statin On Placebo On Statin On Placebo
HPS* (CHD patients) 19.8% 25.7% 33.4% 37.8%
CARE† 19.4% 24.6% 28.7% 36.8%LIPID‡ 11.7% 15.2% 19.2% 22.8%PROSPER§ 13.1% 16.0% 23.1% 18.4%ASCOT-LLA‡ 4.9% 8.7% 9.6% 11.4%TNT║ 7.8% 9.7% 13.8% 17.9%
* CHD death, nonfatal MI, stroke, revascularizations† CHD death, nonfatal MI, CABG, PTCA‡ CHD death and nonfatal MI
HPS Collaborative Group. Lancet. 2003;361:2005-2016. Sacks FM et al. N Engl J Med. 1996;335:1001-1009. LIPID Study Group. N Engl J Med. 1998;339:1349-1357.
§ CHD death, nonfatal MI, stroke║ CHD death, nonfatal MI, resuscitated cardiac arrest, stroke (80 mg vs 10 mg atorvastatin)
Shepherd J et al. Lancet. 2002;360:1623-1630. Sever PS et al. Lancet. 2003;361:1149-1158.Shepherd J et al. Diabetes Care. 2006;:29:1220-1226.
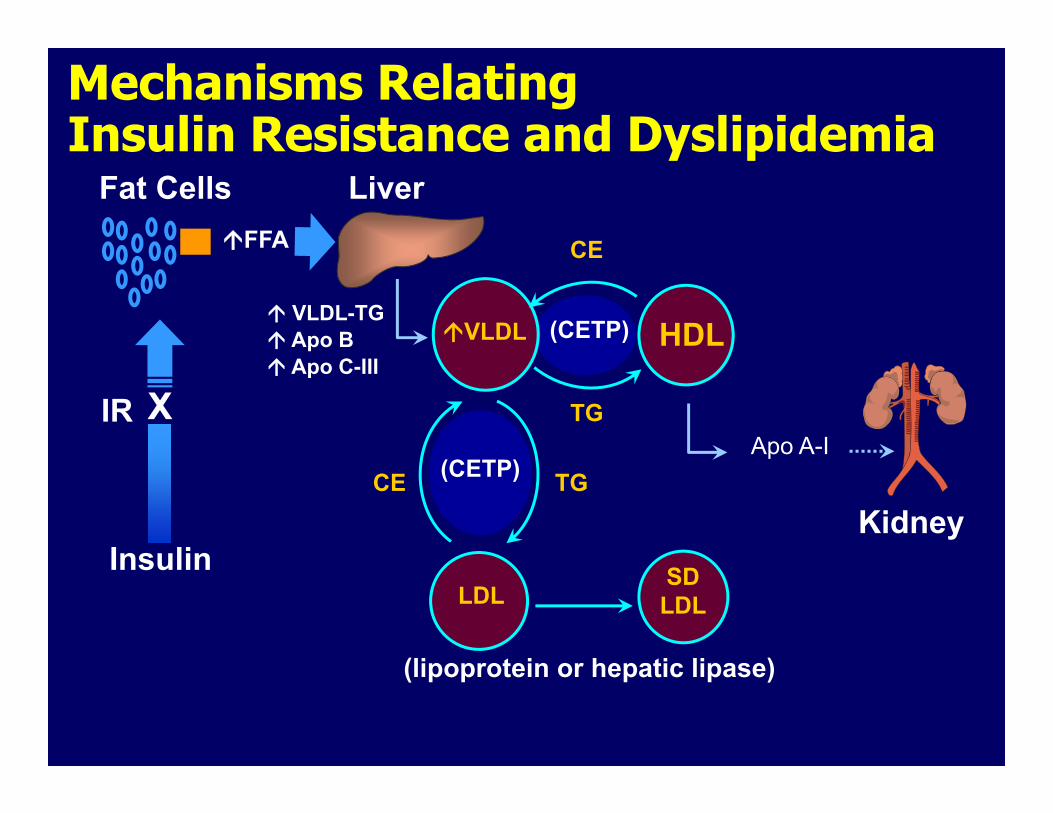
Mechanisms Relating Insulin Resistance and Dyslipidemia
Fat Cells Liver
KidneyInsulin
IR X
(CETP)
CE
VLDL-TG Apo B Apo C-III
(CETP)
VLDL HDL
(lipoprotein or hepatic lipase)
SDLDLLDL
TGApo A-I
TGCE
FFA
ATPIII: Recommendations for Non-HDL-C
Grundy, SM et al Circulation 2004; 110:227-239
If Triglyceride 200 ‐499 mg/dL:
Non‐HDL‐C (total C minus HDL) is a secondary target of therapy with a goal of 30 mg/dL higher than the LDL goal.
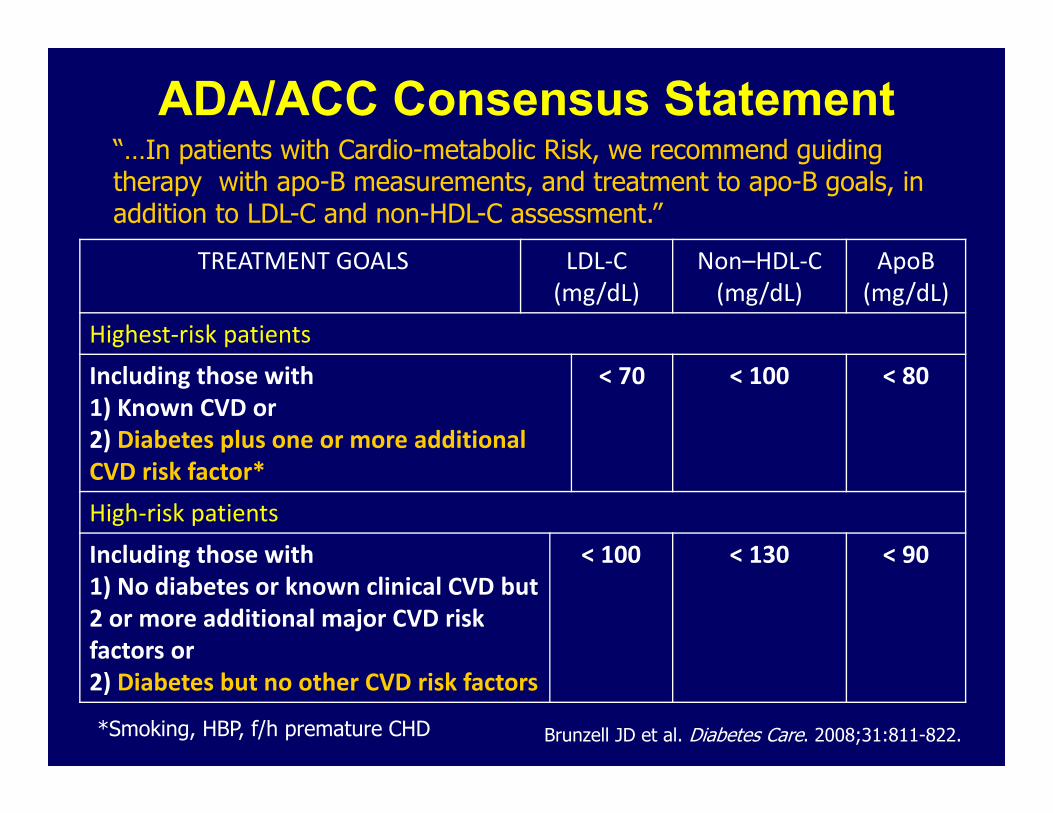
ADA/ACC Consensus Statement
TREATMENT GOALS LDL‐C (mg/dL)
Non–HDL‐C (mg/dL)
ApoB (mg/dL)
Highest‐risk patientsIncluding those with 1) Known CVD or 2) Diabetes plus one or more additional CVD risk factor*
< 70 < 100 < 80
High‐risk patientsIncluding those with 1) No diabetes or known clinical CVD but 2 or more additional major CVD risk factors or 2) Diabetes but no other CVD risk factors
< 100 < 130 < 90
“…In patients with Cardio-metabolic Risk, we recommend guiding therapy with apo-B measurements, and treatment to apo-B goals, in addition to LDL-C and non-HDL-C assessment.”
*Smoking, HBP, f/h premature CHD Brunzell JD et al. Diabetes Care. 2008;31:811-822.
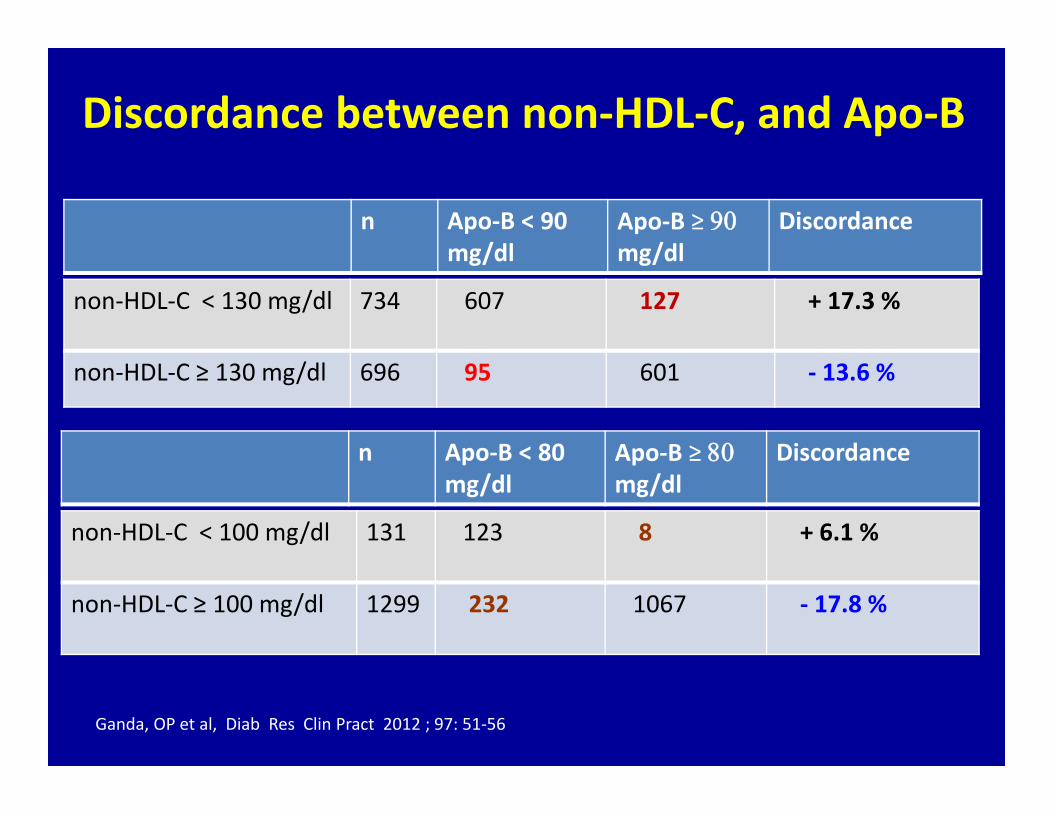
Discordance between non‐HDL‐C, and Apo‐B
n Apo‐B < 90mg/dl
Apo‐B ≥ mg/dl
Discordance
non‐HDL‐C < 130 mg/dl 734 607 127 + 17.3 %
non‐HDL‐C ≥ 130 mg/dl 696 95 601 ‐ 13.6 %
Ganda, OP et al, Diab Res Clin Pract 2012 ; 97: 51‐56
n Apo‐B < 80mg/dl
Apo‐B ≥ mg/dl
Discordance
non‐HDL‐C < 100 mg/dl 131 123 8 + 6.1 %
non‐HDL‐C ≥ 100 mg/dl 1299 232 1067 ‐ 17.8 %
Effect of Lowering Triglycerides (with Fibrates) in Reducing Residual Risk?
ACCORD Study Group. N Engl J Med. 2010;362:1563-1574.
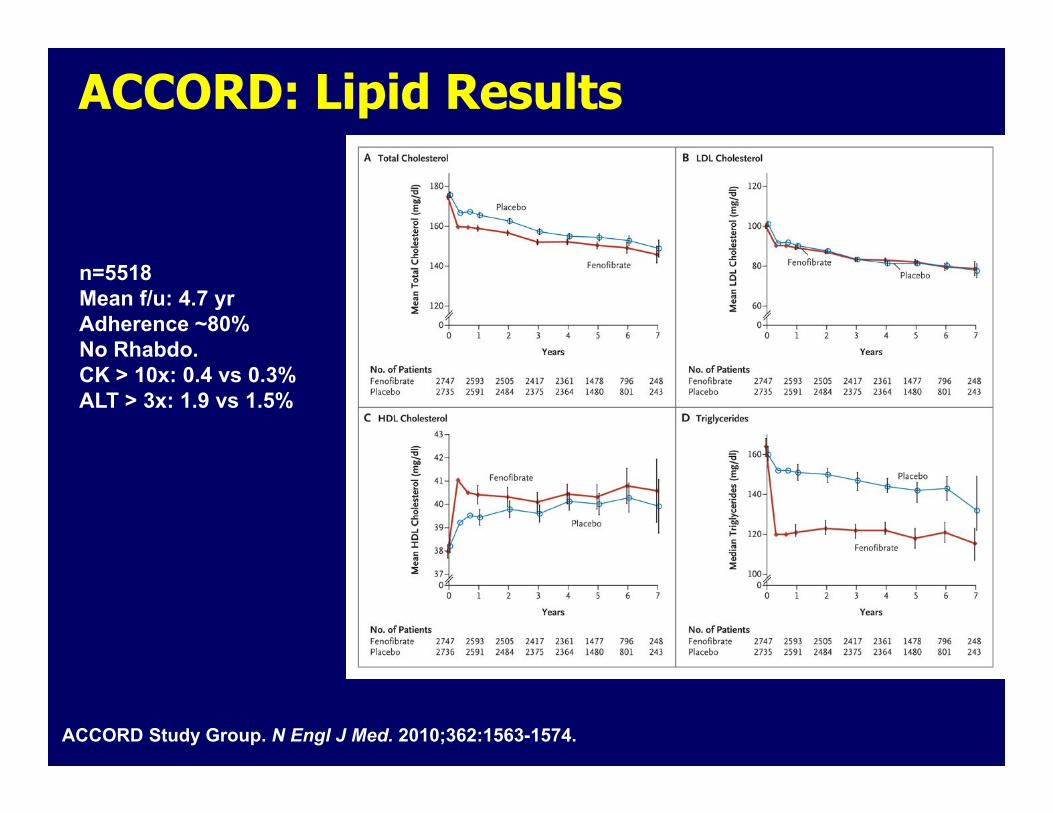
n=5518Mean f/u: 4.7 yrAdherence ~80%No Rhabdo.CK > 10x: 0.4 vs 0.3%ALT > 3x: 1.9 vs 1.5%
ACCORD: Lipid Results

ACCORD Study Group. N Engl J Med. 2010;362:1563-1574.
ACCORD Lipid: Primary Outcome in Pre-specified Subgroups
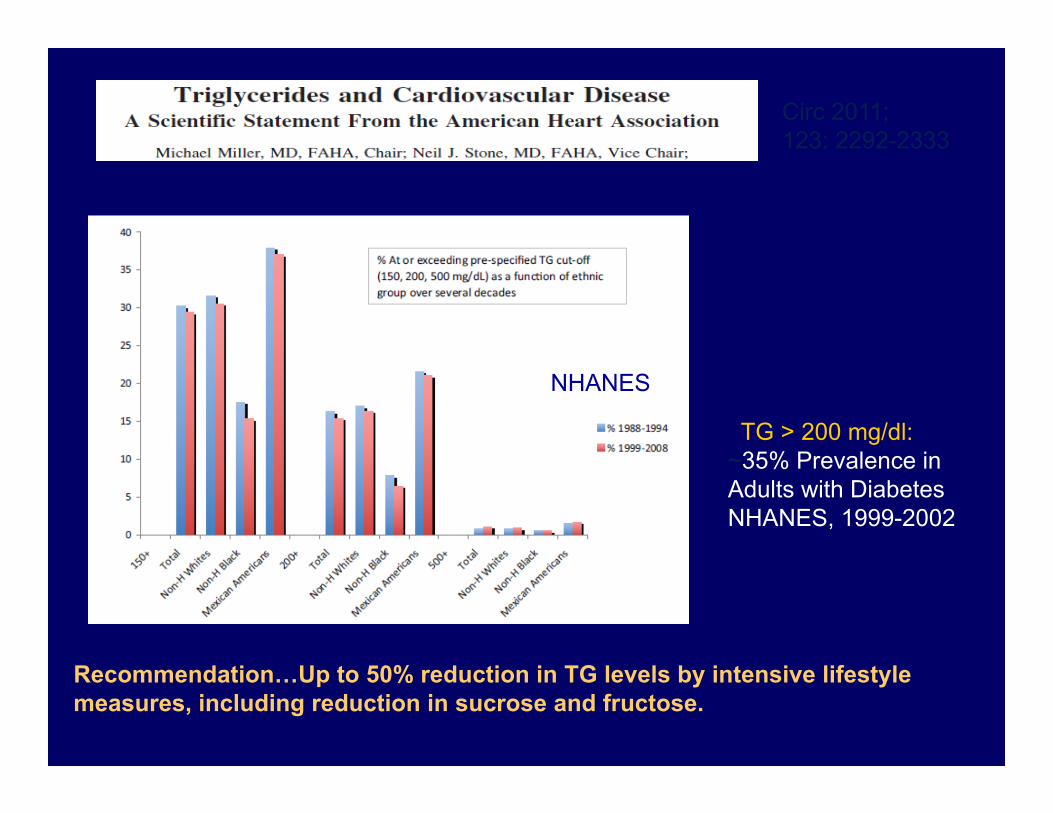
NHANES
Circ 2011; 123: 2292-2333
TG > 200 mg/dl:~35% Prevalence in Adults with DiabetesNHANES, 1999-2002
Recommendation…Up to 50% reduction in TG levels by intensive lifestyle measures, including reduction in sucrose and fructose.

Effect of Raising HDL-C in Reducing Residual Risk?
Audience Response Question 2
Is HDL-C an important determinant of CVD events in patients with LDL-C < 70 mg/dL
A. YesB. NoC. Maybe
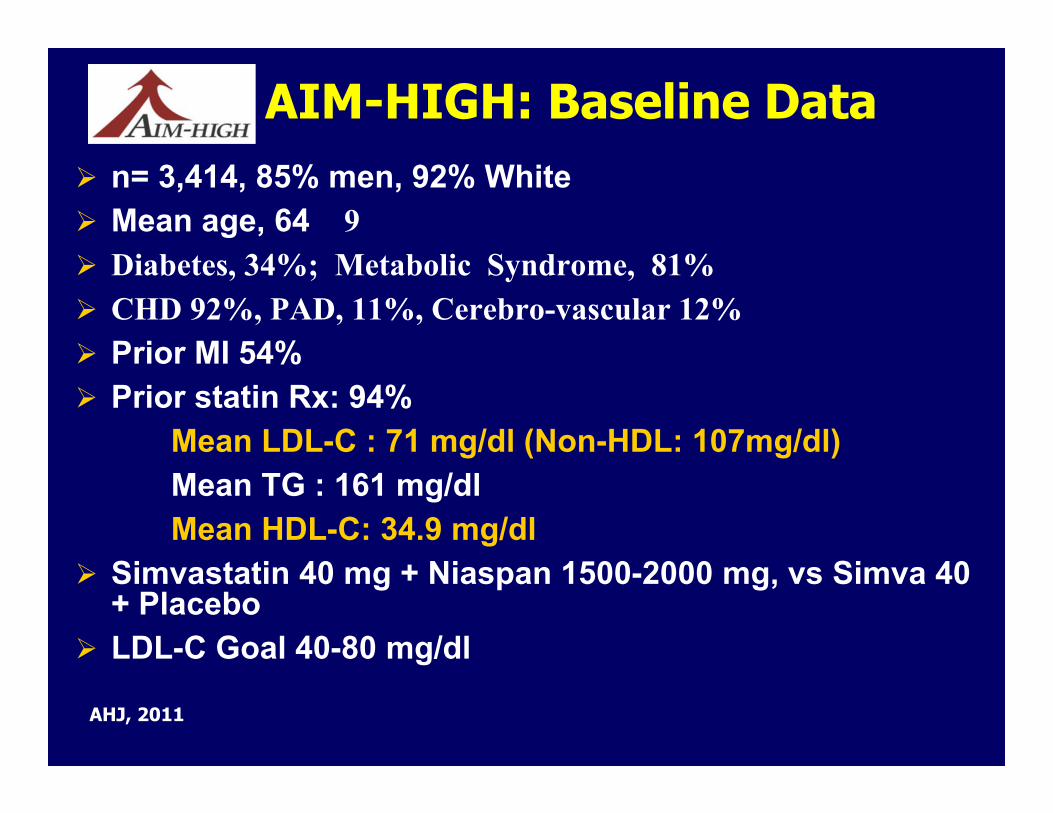
AIM-HIGH: Baseline Data n= 3,414, 85% men, 92% White Mean age, 64 9 Diabetes, 34%; Metabolic Syndrome, 81% CHD 92%, PAD, 11%, Cerebro-vascular 12% Prior MI 54% Prior statin Rx: 94%
Mean LDL-C : 71 mg/dl (Non-HDL: 107mg/dl)Mean TG : 161 mg/dlMean HDL-C: 34.9 mg/dl
Simvastatin 40 mg + Niaspan 1500-2000 mg, vs Simva 40 + Placebo
LDL-C Goal 40-80 mg/dl
AHJ, 2011

AIM-HIGH: Primary Endpoints
Boden,W et al NEJM 2011; Nov 15:on- line
25,673 high-risk patients with occlusive arterial disease from China, Scandinavia and UK
Randomized comparison: ER niacin/laropiprant (ERN/LRPT) 2g daily versus placebo
Primary end point: Major vascular events after median follow-up of 4 years
Pre-specified safety analyses: Median follow-up of 3.4 years (to January 2012)
Background LDL-lowering therapy with: Simvastatin 40mg (+/- ezetimibe 10mg) daily
ACC, 2013
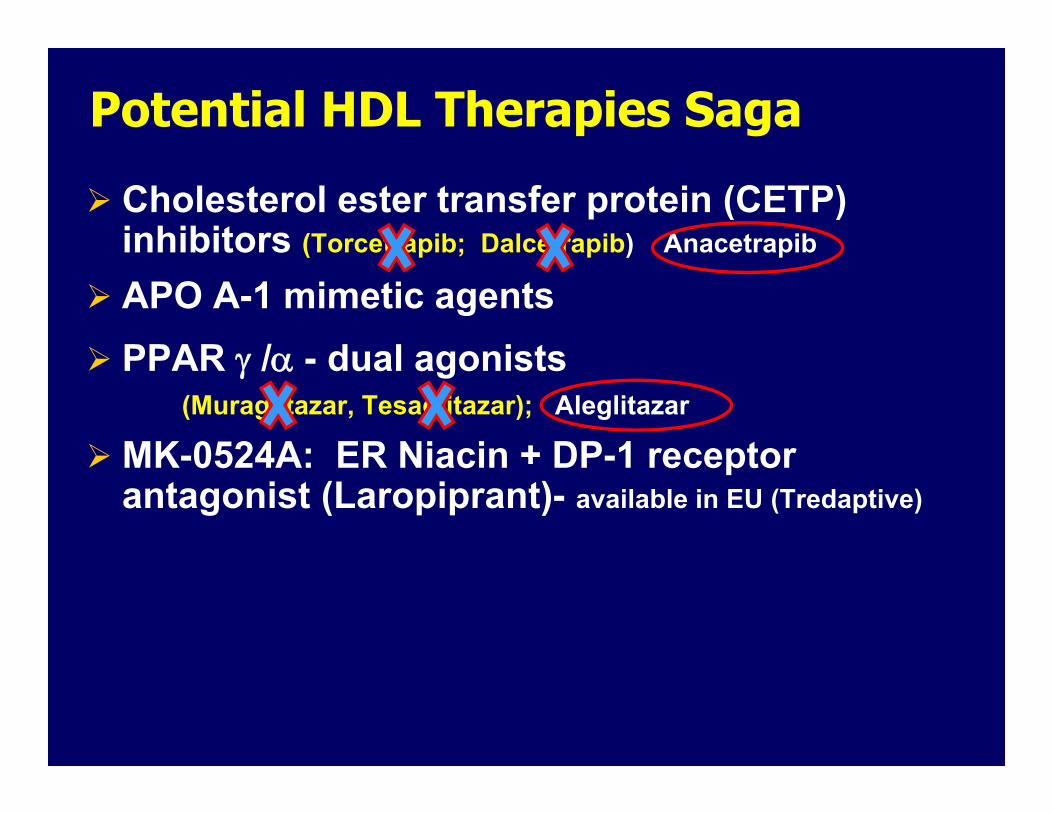
Potential HDL Therapies Saga
Cholesterol ester transfer protein (CETP) inhibitors (Torcetrapib; Dalcetrapib) Anacetrapib
APO A-1 mimetic agents PPAR /- dual agonists
(Muraglitazar, Tesaglitazar); Aleglitazar
MK-0524A: ER Niacin + DP-1 receptor antagonist (Laropiprant)- available in EU (Tredaptive)