treating late-life anxiety in primary care: current status and future directions melinda stanley,...
TRANSCRIPT

Treating Late-life Anxiety in Primary Care: Current Status and Future Directions
Melinda Stanley, Ph.D.
Menninger Department of Psychiatry and Behavioral Sciences, Baylor College of Medicine
Houston Center for Quality of Care and Utilization Studies, MEDVAMC



Community Prevalence of Anxiety Disorders in Later Life
Overall 6-month rates: 3.5 - 10.2% Most prevalent: GAD (1.9 – 7.3%)
More common than depression
Higher rates among institutionalized elderly
Prevalence of clinically significant anxiety symptoms even higher (20%)

Prevalence of Late-Life Anxiety in Primary Care
Anxiety Disorders
GAD Anxiety Symptoms
General medical samples
11 -15% 3-11% 20%
Patients with chronic
illness20% - 38% Up to
19%16% - 40%

Impact of Anxiety in Later Life
Physical activity & disability
Functional status Over and above
physical health status
Self-perceptions of health
Quality of life and satisfaction Loneliness
Increased mortality
Service utilization and health care costs

Treatment of Late-life Anxiety Most patients seen in primary care
Many remain unrecognized and without treatment
Medication most common modality Benzodiazepines:
• 10-20% (up to 43%)• Efficacy data• Risk-benefit profile limits utility
Antidepressants • Efficacious, but still drawbacks

Cognitive Behavior Therapy (CBT) for Late-Life Anxiety
Acceptance and preference data
Approach is Time-limited Directive Collaborative
Efficacy data Treatment of choice for anxiety in younger adults Older adults with depression

Goals of our Late-Life Anxiety Research Program:
Evaluate efficacy of CBT for late-life GAD Two academic clinical trials (1996, 2003)
Modify and test treatments in primary care Pilot work Ongoing trial Next efforts
Move from efficacy to effectiveness Increasing emphasis on translational value and
sustainability in primary care

Efficacy: Academic Clinical trials of CBT for Late-life GAD CBT includes
Education/awareness Relaxation Cognitive Therapy Exposure
12-15 weeks Control groups:
WL (d = .71) Supportive treatment (d =
.20 - .29)
Response rates Group treatment:
• Post: 28-45%• FU: 50-63%
Individual treatment:• Post: 40-75%• FU: 57-75%
Stanley MA, et al. J Consult Clin Psychol. 2003; Stanley MA, et al. Behav Ther. 1996; Wetherell JL, et al. J Consult Clin Psychol. 2003; Mohlman J, et al. Am J Geriatr Psychiatry. 2003; Mohlman et al., Behav Res Ther 2005.

Limitations of the Data Homogeneous and
non-representative samples Young old (mean age
mid-60’s) Medically healthy Cognitively intact Caucasian (80% – 90%) Well educated (mean
14 years)
Treatment not designed for older adults
Outcomes not optimal
All data from academic clinical settings

First steps toward effectiveness Develop collaborative relationship with primary care
Kelsey-Seybold Clinic Baylor Family Medicine MEDVAMC
Modify intervention model to: Improve outcomes Identify and meet the needs of more representative patient groups
Move toward collaborative care models Younger adult anxiety (Rollman, Craske) Older adult depression (Unutzer, Bartels) Effect sizes = .23 to .57

New Version of CBT for Late-Life GAD in Primary Care
8 – 10 sessions Increased attention to
learning & memory More flexible
treatment: Individual care Vary # and timing of
meetings Home visits Differential emphasis of
coping skills
Wider range of treatment components: Education/awareness Relaxation Changing thoughts Exposure Problem-solving Sleep management
skills

Pilot Work (Stanley et al., 2003, Am J Geriatr Psychiatry)
Open clinical trial, n = 8 Test feasibility Modify treatment based on therapist and patient input
Small clinical trial, n = 12 CBT vs. usual care (UC) Benefits in worry & GAD severity, depression

Ongoing trial: STOP Worry Project(NIMH renewal)
Goal: n = 150 older primary care patients with GAD
Settings Kelsey-Seybold Clinic Baylor Family Medicine
Inclusion criteria GAD MMSE > 24 English-speaking

STOP Worry Project Team
Investigators
Mark Kunik, M.D. Diane Novy, Ph.D. Nancy Wilson, M.A.,
L.M.S.W. Howard Rhoades,
Ph.D. Anthony Greisinger,
Ph.D.
Current Study Staff
Paula Wagener, B.A. Cynthia Kraus, Ph.D. Christopher Griffith,
B.A. Jessica Calleo, M.A. Brandon Weiss
Design Elements
Efficacy Random
assignment Comprehensive
outcome battery Expert clinicians
and independent evaluators
Treatment integrity raters
“Clean” treatment
Effectiveness Recruit & treat in
primary care Less restrictive
inclusion criteria Telephone-based
assessments Control condition =
UC More flexible
treatment
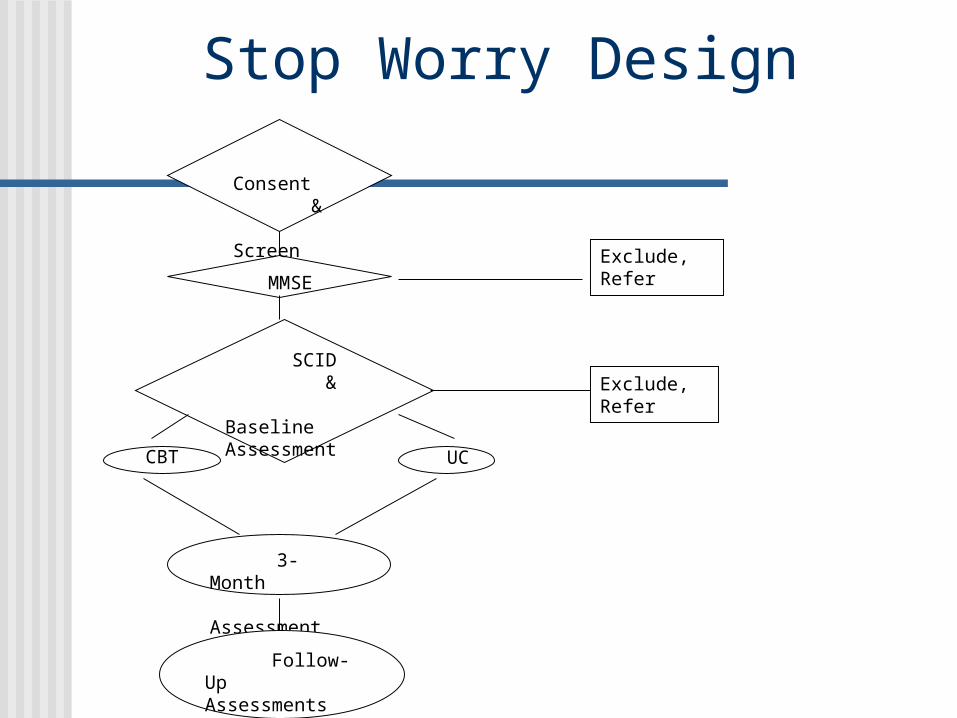
Stop Worry Design
MMSE
Consent & Screen
Exclude, Refer
Exclude, Refer
3-Month Assessment
Follow-Up Assessments (1 year)
UCCBT
SCID & BaselineAssessment
STOP Worry Design (cont’d)
CBT Conducted in the primary care clinic (or patient’s home) Master’s level clinicians Treatment integrity ratings - excellent
UC Biweekly telephone contact
Assessments (3 mo. & 1-year FU) Telephone-based Independent evaluators

Outcome Measures
Worry GAD Severity (GADSS) Penn State Worry
Questionnaire (PSWQ)
Anxiety Beck Anxiety
Inventory (BAI) SIGH-A (Hamilton)
Depression Beck Depression
Inventory (BDI)
Quality of Life Quality of Life
Inventory (QOLI) SF – 12
Health Service Use

Recruitment Strategies Timeline: 3/04 to 8/06
2 2-month interruptions Total 26 months
Self-referral Brochures: Waiting rooms, newsletters, Information
Center Letters to patients
Provider referral Presentations, meetings E-mail reminders

Recruitment Summary 968 patients referred
381 signed consent, 313 assessed
165 excluded No GAD, cognitive impairment 11 non-study clinical training cases
148 included (99% of target!) Approx. 6 per month 95% self-referred

Sample Characteristics (n = 148)
Demographics 78% women Mean age = 67 years (SD = 5.8) Mean education = 16 years (SD = 3.0) 17% African American; 9% Hispanic 50% using psychotropic medication
Coexistent psychiatric diagnosis 69% at least 1 45% Depression (MDD, Dysthymia, NOS) 26% Specific Phobia 14% Social Phobia

Treatment Progress (1/07)
CBT UC
Randomized 70 64
ITT 61 57
Completed 42 37
Overall attrition = 27%[9% before randomization; 12% before post-treatment;
6% during follow-up]Higher attrition in UC (26%) vs. CBT (13%)

ITT Analysis: PSWQ change scores
0
1
2
3
4
5
6
7
8
9
3-months 6-months
CBT
UC
3-month d = .64 (.001); 6-month d = .73 (.001)

ITT Analysis: SIGH-A change scores
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
3-months 6-months
CBT
UC
3-month d = .28 (ns); 6-month d = .46 (.02)

ITT Analysis: GADSS change scores
0
0.5
1
1.5
2
2.5
3-months 6-months
CBT
UC
3-month d = .35 (.06); 6-month d = .35 (.06)

Summary & Limitations
CBT is moderately effective relative to UC Effect sizes equivalent to other collaborative care
studies (.28 - .73 vs. .23 - .57) Increasing effects over time
Low attrition in CBT (13%) Translational value limited
Homogeneous, non-representative sample Limited generalizability of treatment to real-world care
(expert providers, long sessions, no attention to patient preference)

Future Directions: Peaceful Living Project
Increase emphasis on effectiveness and collaborative care models Examine effectiveness of CBT delivered by
non-expert providers Enhance communication and collaboration
with primary care via use of EMR Modify CBT to increase flexibility and enhance
translational value/sustainability Implement intervention in more diverse
medical setting (BCM, MEDVAMC)

Peaceful Living Team
Academic investigators
Mark Kunik, M.D. Nancy Wilson, M.A.,
L.M.S.W. Jeff Cully, Ph.D. Louise Quijano, Ph.D.,
L.C.S.W. Michael Kallen, Ph.D.,
M.P.H.
Primary care investigators
Michael Crouch, M.D. (BCM)
Victor Narcisse, M.D. (BCM)
Stinson Tillerson, M.D. (MEDVAMC)

Peaceful Living: CBT Modifications
Modular treatment Integrate telephone-based service
delivery Incorporate patient preference Briefer sessions and simplified procedures BA module to target coexistent
depression Extended duration of treatment, with
intensive telephone booster phase

Treatment Components
Core modules Education &
awareness Motivational
exercise Breathing Coping self-
statements
Elective modules Relaxation Cognitive therapy Sleep skills Problem-solving Behavioral
activation Exposure

Treatment Process
First 3 months Sessions 1-3: Core modules Sessions 6-9: Elective modules
• Patient preference: Content, mode Session 10: Review 26% telephone sessions
Second 3 months Intensive telephone follow-up

Peaceful Living: Open Trial Study sites
BCM Family Medicine MEDVAMC
New recruitment procedures Identify potential patients through EMR PCP sends letter of invitation
Recruitment success More physician-referred patients (44% vs. 5% in STOP Worry) Greater diversity (53% women; 67% Caucasian) Higher baseline severity (GADSS, SIGH-A)

Peaceful Living: Open Trial
Treatment process Group assignment:
• Anxiety Clinic Specialists (MA-level or above) • Counselor (BA-level or below)
Adherence/competence equivalent in 2 groups
Treatment progress 16 patients included CBT-ACS (n = 9); CBT-Counselor (n = 7) Completers: 3-months (n = 10); 6-months (n = 8) Within-subject d = .43 to 1.39

SIGH-A: STOP Worry vs. PLWithin CBT effect sizes
0
0.2
0.4
0.6
0.8
1
1.2
1.4
3-months 6-months
STOP WorryPeaceful Living

GADSS: STOP Worry vs. PLWithin CBT effect sizes
0
0.2
0.4
0.6
0.8
1
1.2
3-months 6-months
STOP WorryPeaceful Living

PSWQ: STOP Worry vs. PLWithin CBT effect sizes
0
0.2
0.4
0.6
0.8
1
1.2
1.4
3-months 6-months
STOP WorryPeaceful Living

Peaceful Living: Summary Effects generally are comparable to or
greater than STOP Worry Exception: PSWQ at 6-months
Patients are more diverse and have more severe symptoms
Intervention model is more sustainable
NIMH should give us 5 more years!

