trina la pharmd. candidate university of georgia college of pharmacy
TRANSCRIPT

Trina LaPharmD. CandidateUniversity of GeorgiaCollege of pharmacy

OutlineIntroductionStudy 1: Glycemic control, complications, &
death in older diabetic patientsStudy 2: Combination of oral antibiabetic
agents with basal insulin versus premixed insulin ALONE in randomized elderly patients with Type 2 DM
Summary of oral antidiabetic agents and insulins
Conclusion

IntroductionDefinition
DM is a syndrome characterized by chronic hyperglycemia & disturbances of carbohydrate, fat & protein metabolism, associated with an absolute or relative deficiency in insulin secretion and/or insulin action
Associated problems affecting management in elderlyCerebral agingAtherosclerotic changesCompromised Cardio Respiratory ReserveCataractNeuropathyCerebral Vascular Disease

Diabetic Complications
4
Amputation
Microvascular Complications
Neuropathy
CerebrovascularDisease
Peripheral Vascular Disease
Macrovascular Complications
Retinopathy
Nephropathy
Heart Disease
Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329:977-986. Stratton IM et al. BMJ. 2000;321:405-412 with permission from the BMJ Publishing Group www.cdc.gov.
Amputation

ELBERT HUANG, JENNIFER LIU, HOWARD MOFFET, ET AL
Diabetes care 2011;34: 1329-1335
Funded by the institute of diabetes & digestive & kidney diseases

BackgroundPeople aged > 60 years comprise > 40% of the type
2 diabetic population in the U.S, yet identifying the optimal glucose control level for older patients with diabetes remains a significant challenge
Recommended glycemic targetsA1C <6.5% from American Association of Clinical
EndocrinologistsA1C <7.0% from the American Diabetes AssociationA1C < 8.0% from geriatric diabetes care guidelines for
older patients with limited life expectancyHowever, there has been limited evidence for any of
these targets of glycemic control for elderly patients

ObjectiveTo identify the range of glycemic levels
associated with the lowest rates of complications & mortality in older diabetic patients

OutcomesAcute metabolic events
Hospitalizations for diabetes with other comaDiabtes with hyperosmolarityDiabetes with ketoacidosisUncontrolled diabetes
Chronic microvascular eventEnd-stage renal diseaseAmputation Severe diabetic eye disease
Chronic cardiovascular eventsCoronary artery diseaseCongestive heart failureCerebralvascular diseasePeripheral vascular disease

Research Design & MethodsInclusion Criteria Exclusion Criteria
Type 2 diabetesAged ≥60 years Continuous Kaiser
membership & pharmacy benefits for at least 12 months before baseline
Type 1 diabetes or unknown diabetes
End-stage renal disease No A1C test result
during the year prior to baseline

Research Design & MethodsA restrospective cohort study (2004-2008) of
71,092 patients with type 2 diabetes, age ≥60 years, enrolled in Kaiser Permanente Northern California
Registry eligibility is based onPharmacy recordsLaboratory dataOutpatient Emergency roomHospitalization diagnose of diabetes

Research Design & MethodsA restrospective cohort study (2004-2008) of
71,092 patients with type 2 diabetes, age ≥60 years, enrolled in Kaiser Permanente Northern California
Registry eligibility is based onPharmacy recordsLaboratory dataOutpatient Emergency roomHospitalization diagnose of diabetes

A1C & Assessment of covariatesFor stratified analyses
A1CAssessment of covariates
DemographicsDuration of diabetesSystolic blood pressureLab findings within 1 year prior to baseline:
eGFR, urinary albumin excretion, BMI; prevalent complications & comorbidities ( hx of lower extremitiy amputation, photocoagulation)
Hospitalization for acute metabolic event, MI, stroke, CHF, ect
SmokingBaseline use of glucose-lowering medications

ResultsThe mean age of population: 71 yearsPopulation: ethnically diverseThe mean A1C: 7.0%The mean duration of diabtes: 8.3 yearsPatients with lower baseline A1C values tend to
beOlderMore likely to be non-Hispanic whiteMore likely to have a shorter duration of diabetesBetter cholesterol controlLower GFRLess evidence of other microvascular complicationMuch less likely to be treated with insulin

Results: Baseline A1C, Complications, & mortality; Overall population results
Outcome Incidence Density (Events/1000 person-years)
Model A1C
<6.0 6.0-6.9 7-7.9 8.-8.9 9-9.9 10-10.9
≥11
Acute metabolic event
1.23 Adjusted HR95% CI
1 1.44.82-2.53
2.351.3-4.2
3.822.0-7.2
4.952.5-10
6.603-14.6
11.55.7-23.5
Chronic microvascular event
26.68 Adjusted HR95% CI
11
1.11.99-1.3
1.251.1-1.4
1.531.3-1.8
1.521.3-1.8
1.721.4-2.1
2.041.7-2.47
Chronic cardiovascular events
47.15 Adjusted HR95% CI
11
1.091.0-1.2
1.141.1-1.2
1.261.1-1.4
1.281.1-1.5
1.391.2-1.7
1.771.51-2.1
Mortality 40.42 Adjusted HR95% CI
11
0.840.8-0.9
0.830.7-0.9
0.900.8-1
1.020.9-1.2
1.211.0-1.45
1.311.09-1.6
Any complication 69.90 Adjusted HR95% CI
11
1.091.0-1.2
1.181.1-1.3
1.381.3-1.5
1.421.3-1.6
1.521.3-1.7
1.81.6-2.16
Any complication or Death
97.97 Adjusted HR95% CI
11
0.98.93-1.03
1.03.97-1.1
1.201.1-1.3
1.261.1-1.4
1.351.2-1.5
1.631.5-1.8
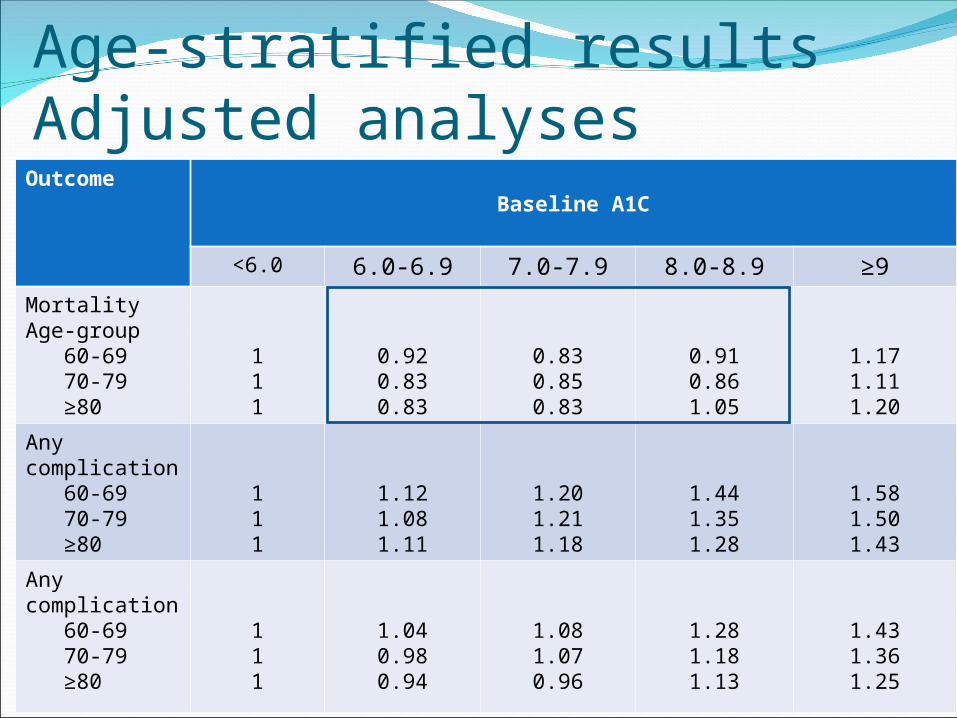
Age-stratified results Adjusted analyses
OutcomeBaseline A1C
<6.0 6.0-6.9 7.0-7.9 8.0-8.9 ≥9
Mortality Age-group 60-69 70-79 ≥80
111
0.920.830.83
0.830.850.83
0.910.861.05
1.171.111.20
Any complication 60-69 70-79 ≥80
111
1.121.081.11
1.201.211.18
1.441.351.28
1.581.501.43
Any complication 60-69 70-79 ≥80
111
1.040.980.94
1.081.070.96
1.281.181.13
1.431.361.25

ConclusionsObserved relationships between A1C &
combined end points support setting a target of A1C< 8.0% for older patients
A1C <6.0% were associated with increase mortality risk
Additional research is needed to evaluate the low A1C-mortality relationship
Ongoing research on care individualization in the elderly suggest that life expectancy, comorbid conditions, patient preferences are important consideration in glycemic control
Janka Hans, Plewe gerd, Busch klausJags 2007;55:182-188
Funded by a research grant from sanofi-aventis

BackgroundThe association between poor glycemic control &
the occurrence of micro-& macrovascular complications has been demonstrated in patients with type 1 & 2 DM
Tight glycemic control may be associated with greater frequency of hypoglycemic episodes; however it can have serious clinical consequences
Consensus opinion on how & when to initiate insulin tx in patients with type II DM is lacking
In older patients with type 2 DM, it is important that the insulin regimen be easy to apply, with optimal efficacy & safety.
Few studies have directly compared the leading methods of insulin initiation in this population

ObjectivesTo compare initiation of insulin therapy by
adding once-daily Lantus to oral antidiabetic agents(OAD) with premixed insulin alone

DesignA parallel-group, open-label, randomized,
multinational clinical trial with a 1 to 4 week screening phase & a 24-week treatment phase
A 1:1 randomization schedule stratified by center sequentially assigned treatment codes to eligible patients

Inclusion & Exclusion CriteriaInclusion Criteria Exclusion CriteriaAged 65 & olderType II DM for at least 1
yearTreated with a stable
dose of Sulfonylurea & Metformin for at least 1 month
BMI≤ 35 kg/m2
7.5 ≤A1C ≤10.5Fasting blood glucose(FBG)≥ 120mg/dL
Any additional use of other oral blood glucose-lowering agents
Prior use of insulin exceeding 3 days
A history of ketoacidosis

Study Protocol & TreatmentPrevious Sulfonylurea therapies were replaced
with 3 or 4 mg glimepiride during the screening phase
Metformin (≥850mg) administered during the study was provided & taken at the same dose as before study entry
The dose of Glimepiride & Metformin remained unchanged throughout the study
At the baseline visit, patients were randomly assigned to insulin Lantus given once daily in AM in combination with Glimepiride & Metformin or to human premixed insulin (70/30) BID

Study Protocol & TreatmentFor both groups, the FBG target was 100mg/dLFBG values & pre-dinner BG as well as
hypoglycemic episodes were recorded in a standardized diary
Hematological, clinical chemistry, & HbA1c values at baseline & 12, & 24 weeks were measured
The participating investigators noted any adverse events at every visit or telephone contact

Efficacy & Safety MeasurementsThe primary efficacy measure was change in A1C
level from baseline to endpointSecondary efficacy measurement:
Mean FBG levelsMean daytime BG levelsMean BG values from the 8-point profileThe proportion of patients with FBG levels of
100mg/dLThe proportion of patients with A1C levels of 7% or
less with no nocturial hypoglycemiaSafety measures were the proportion of patients
with hypoglycemia events & frequency of hypoglycemic events

Demographics & Baseline Characteristics of the Study Population
Characteristics Insulin Lantus+ OAD
Premixed Insulin
Patient, nMale/Female
Age, mean ± SDWeight, kg, mean ± SD
BMI, mean ± SDDuration of DM, years, mean
± SDDuration of OAD treatment,
years, mean ± SDC-peptide, ng/mL, mean ± SD
A1C, mean ± SDFasting blood glucose, mean
± SDmg/dL (range ≤100)mmol/L (range≤5.6)
6764/36
83.8±15.328.9±3.428.9±3.412.1± 6.78.9±5.9
3.5±2.08.84±1.06
165± 339.2±1.8
6348/52
69.6±4.180.5 ±13.028.9 ±3.311.1 ± 7.6
6.9±5.2
3.8±2.78.89±0.91
171±399.5 ± 2.2
ResultsGlycemic Control Blood glucose level Lantus + OAD
A1C decreased from 8.8% to 7.0%
Premixed insulin A1C decreased from 8.9% to
7.4% The mean adjusted decrease in
A1C was greater for Lantus +OAD than for premixed (P=0.03)
Overall, the proportion of patients that reached the target A1C level was significant higher in patients receiving Lantus+OAD (P=0.01)
Glargine +OADFBG decreased from
165 mg/dl to 111mg/dlPremixed insulin
FBF decreased from 171 mg/dl to 129 mg/dl
Decreases in mean adjusted FBG levels were significant greater with Lantus + OAD than premixed (P=0.02)

Rates of Confirmed Hypoglycemic Events per Patient-YearType of Hypoglycemia
Lantus+ Oral Antidiabetic Agents
Premixed Insulin
P-Value
All episodes of hypoglycemia (confirmed + unconfirmed)
5.59 11.39 0.01
All episodes of confirmed hypoglycemia
3.68 9.09 0.008
Confirmed symptomatic hypoglycemia
2.22 5.01 0.06
Confirmed nocturnal hypoglycemia
0.39 0.71 0.26
Severe hypoglycemia 0.00 0.09 0.21

Weight gain & Adverse EventsMean weight gain
Glargine + OAD: 1.3 ± 3 kgPremixed insulin: 2.2 ± 3.9 kgP value = 0.17
Adverse EventsSimilar between two groupsMost common AE
Respiratory, nervous system & GI disordersWithdraw from the study due AE
Lantus+ OAD: 1 patient Premixed insulin:2 patient

DiscussionThe results presented
Patients aged 65 & older with type II DM poorly controlled on oral therapy, adding a single injection of Lantusto glimepiride & Metformin can provide more effective glycemic control than stop OAD & starting BID 70/30
Lantus + OAD regimen enabled 55% of patients to reach A1C of 7% or less without experiencing nocturnal hypoglycemia

Some considerationsRisk of comorbidities in elderly patientsThe possibility that patients developed
contraindications to OADs over timeIndividual assessment with tailored therapy
is still importantMust consider the compromise between
achieving tight glycemic control & limiting the risk of hypoglycemia in this patient populations

ConclusionThis study demonstrated that, for elderly
patients with type II DM who are inadequately controlled with Metformin + a sulfonylurea, adding a Once daily injection of Lantus is a simple method that is more effective in improving glycemic control & less likely to cause hypoglycemia than starting BID injection of premixed insulin without oral agents

Oral Antidiabetic MedicationsDrugs Drugs Mechanism of
ActionComments
Glyburide Glipizide Glimipiride
Sulfonylureas
Increase insulin secretion
-Start low dose in elderly, renal adjustmnent- Most SE: hypoglycemia, N/V & skin reactions
PrandinStarlix
Meglitinides Stimulate insulin secretion
Rapid absorption, short duration of action, dose with meals
Precose Glyset
Alpha-glucosidase Inhibitors
Delay glucose absorption, decrease rate of carbohydrate digestion
No renal adjustmentContraindication: -Cirrhosis (Precose)-Colon ulceration-IBS/ bowel obstruction

Oral Antidiabetic MedicationsDrugs Drug class Mechanism of
ActionComments
Metformin Biguanides - Increase insulin sensitivity;-Decrease insulin resistance- Decrease glucogenesis
-Weight reduction- Lipid improvement (↑ TG & ↓LDL)-Contraindication: SCr(males) ≥1.5 & (female)≥ 1.4
Actos Avandia
Thiazolidinediones (TZD)
Insulin sensitizers -Good for fasting sugar & no renal adjustment- SE: Increase LFT, edema, weight gain-Actos: Risk for bladder cancer
JanuviaOnglyzaTradjenta
DPP4 Inhibitors -Increase insulin synthesis & secretion-Decrease glucagon-Delay gastric emptying , promotes b-cell proliferation
-Safe SE profile- Onglyza: drug interaction with CYP3A4

Insulin Type of Insulin
Onset Role in blood glucose management
HumalogNovologApidra
Rapid acting 15 to 30 minutes
-Cover insulin needs before or immediately after meals- Used with long acting insulin
Novolin RHumulin R
Short acting 30 minutes to 1 hour
- Given 30 to 60 minutes before meals
LantusLevemir
Long acting 30 minutes to 3 hours
-Cover insulin needs for one full day
Humalog mix Novolog mix
Pre-mixed 30 minutes -A combination of specific proportions of intermediate-acting & short acting insulin-Give twice daily before meals

GLP-1 Effects in HumanDrug class: Glucagon-Like Peptide Receptor
AgonistTherapeutic benefits:
Enhance glucose dependent insulin secretionPromote satiety & reduces appetiteDecreases post meal glucagon secretionDelays gastric emptying
Available:Byetta ®Victoza®

SummaryManagement of diabetes is a life-long
commitmentManagement of diabetes includes diet,
exercise and drugs Regular physicianConsiderations when developing or
recommending drug therapy planEfficacy therapySafety of therapyImpact on compliance Financial burden