tumor therapy with monoclonal antibodies gerhard moldenhauer
Post on 21-Dec-2015
230 views
TRANSCRIPT
Tumor Therapy with Monoclonal Antibodies
Gerhard Moldenhauer

Innate and Adaptive Immunity

Lymphocyte Activation

Effector Functions of Antibodies
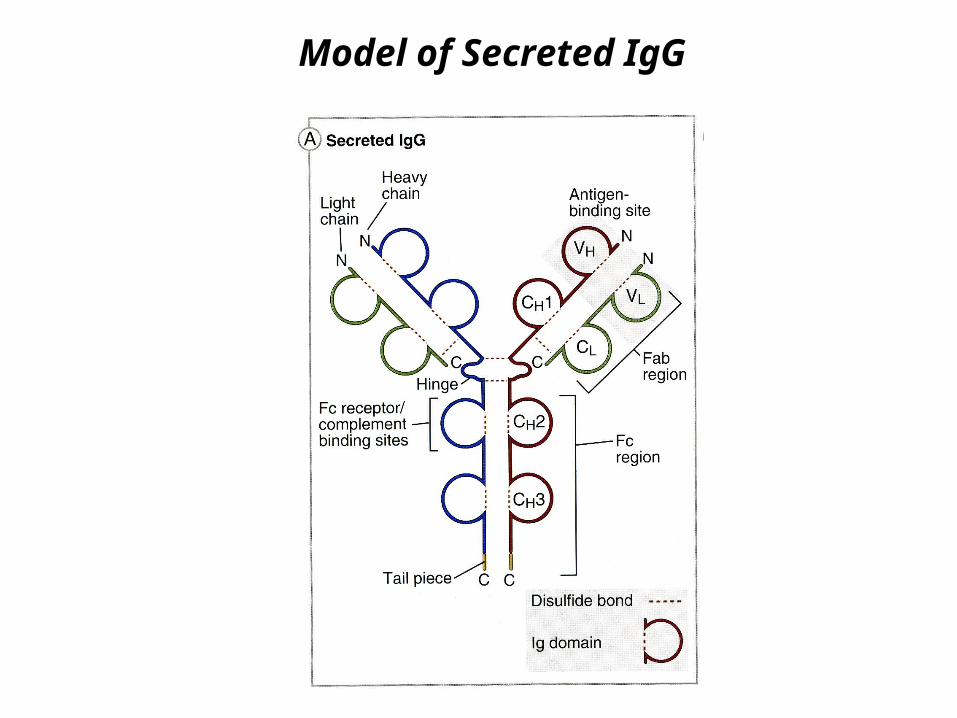
Model of Secreted IgG

Structure of an IgG Antibody
Original by Dr. Mike Clark

Generation ofMonoclonal Antibodies
G. Köhler and C. Milstein1975
Monoclonal antibodies are
♦ monospecific
=> recognize onl y one epitope (antigenic determinan)t
♦ homogenous
=> identica l immunoglobulin molecules=> display identica l binding strengths (affinity)
♦ produced in unlimited quantities
♦ usually deri vedfrom mouse
Characteristics of Monoclonal Antibodies
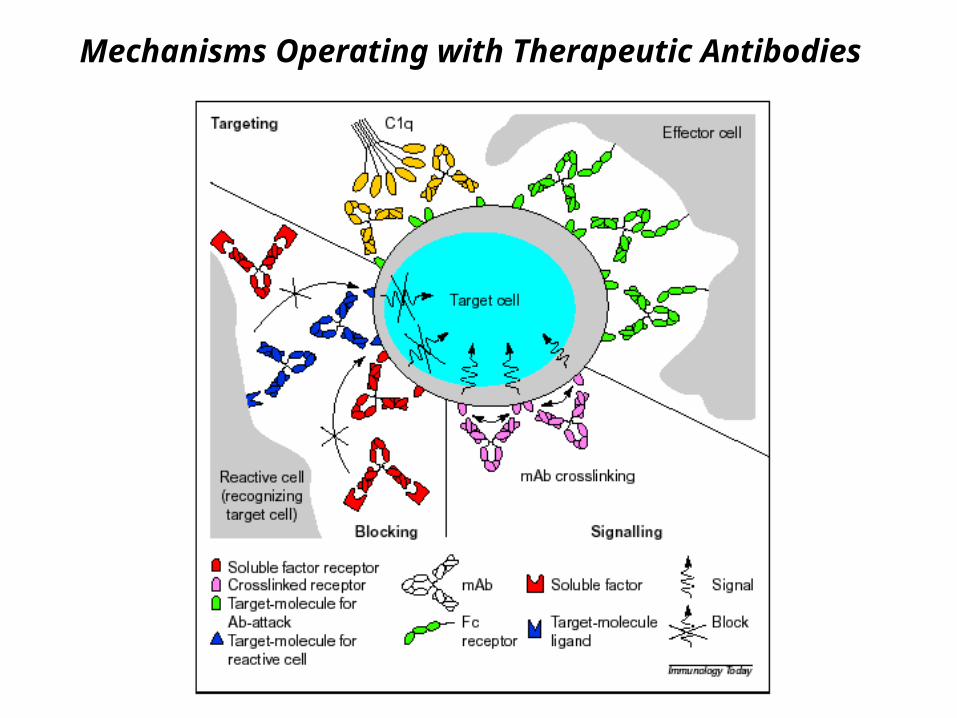
Mechanisms Operating with Therapeutic Antibodies

Direct effects
♦ / Blockade of growth factors growth factor receptors
♦ Induction of apoptosis
♦ Inhibition of angiogenesis
Indirect effects
♦ - Complement dependent ( )cytotoxicity CDC
♦ - Antibody dependent cellular ( )cytotoxicity ADCC
♦ , Vehicel for toxins radionuclides and cytostatic drugs
♦ -Anti idiotype antibody formation
♦ Effector cell targeting using bispecific antibodies
Therapeutic Effects of Monoclonal Antibodies

in vivo:♦ mAb against differentia tionantigens (AD ,CC compleme ntfixation)♦ mAb with direc tanti-proliferative effects (grow threceptors, apoptosis)♦ mAb interfering w ithangiogenesis♦ mAb as carrier sfo r radioisotope s(radioimmunotherapy)♦ mAb as carrier sfo r toxins(immunotoxins)♦ Ant -i idiotype mAb♦ Bispecific mAb tofoc useffector cell ac tivity(effector cell targeting)
e xvivo:♦ Autologous / BM SC transplanta :tion pur ging of th eautograf twith mAb♦ Allogeneic /BM SC transplanta : tion prevention of GVHD by T ce ll depletion
Strategies for Therapeutic Application of Monoclonal Antibodies

Patient Suffering from NHL

Immunocytology of Bone Marrow Smear from a Patient with NHL
♦ Group of malignancies that affect primarily the lymphatic system.
♦ Prevalent forms derive from malignant B lymphocytes (80% of cases).
=> Incidence 6-17 cases per 100,00 habitants per year.
=> Increase world-wide at about 4% a year.
=> Mortality 9,000 patients in Western Europe (330 Million population).
♦ Early and intermediate stages of NHL can be cured by chemotherapy.
♦ The disease-free survival at advanced stage-NHL is 25% at 5 years and less
than 10% at 10 years.
Non-Hodgkin‘s lymphomas

Target Antigens on Malignant B-cellsTarget Antigens on Malignant B-cells
HLA-DR
TDT
CD19
CD10
CD20
CD22
CD21
CD38
Stem cell
Pro-B cell
Pre-B cells
ImmatureB cell
MatureB cell
ActivatedB cell
Plasmacell
Neoplasias: Leukemias from B-cell Precursors (B-ALL)
B-cell Lymphomas (NHL, CLL) Multiple Myeloma
Antigen independent Antigen dependent

First Report on Treatment of a Cancer Patientwith Monoclonal Antibody
♦ Tumor cell heterogeneity (escape)
♦ Antigen modulation (loss of surface antigens)
♦ Blocking effects of circulating antigens
♦ Insufficient penetration into the tumor
♦ Insufficient activation of human effector mechanisms
♦ Cross reactivity with normal tissue antigens
♦ Antibodies against mouse immunoglobulin (anti-isotype,
anti-allotype, anti-idiotype)
Monoclonal Antibody Therapy - Problems

Fab
Fv
Fc
Hinge
VL
VH
CL
CH
CH2
CH3
(a) Immunoglobulin G
VHVL
Domain Structure of Immunoglobulins
scFv IgG

Human
Murine Chimeric Humanized
Antibodies for Therapeutic Application
scFvFragment
Bispecific

Rituximab

Rituximab

in vivo:♦ mAb against differentia tionantigens (AD ,CC compleme ntfixation)♦ mAb with direc tanti-proliferative effects (grow threceptors, apoptosis)♦ mAb interfering w ithangiogenesis♦ mAb as carrier sfo r radioisotope s(radioimmunotherapy)♦ mAb as carrier sfo r toxins(immunotoxins)♦ Ant -i idiotype mAb♦ Bispecific mAb tofoc useffector cell ac tivity(effector cell targeting)
e xvivo:♦ Autologous / BM SC transplanta :tion pur ging of th eautograf twith mAb♦ Allogeneic /BM SC transplanta : tion prevention of GVHD by T ce ll depletion
Strategies for Therapeutic Application of Monoclonal Antibodies

Kinase Growth Factor Pathway
Cell membrane
Ligand binding
Activated receptor
Y Y
YYP
P
P
P
Proliferation Migration
Tumour growthand metastases
Survival
Signal transduction
Tyrosine kinase receptor
Tyrosine kinase domain
Original by Dr. Axel Ullrich




Effects of Trastuzumab (Herceptin) on Breast Cancer Cells
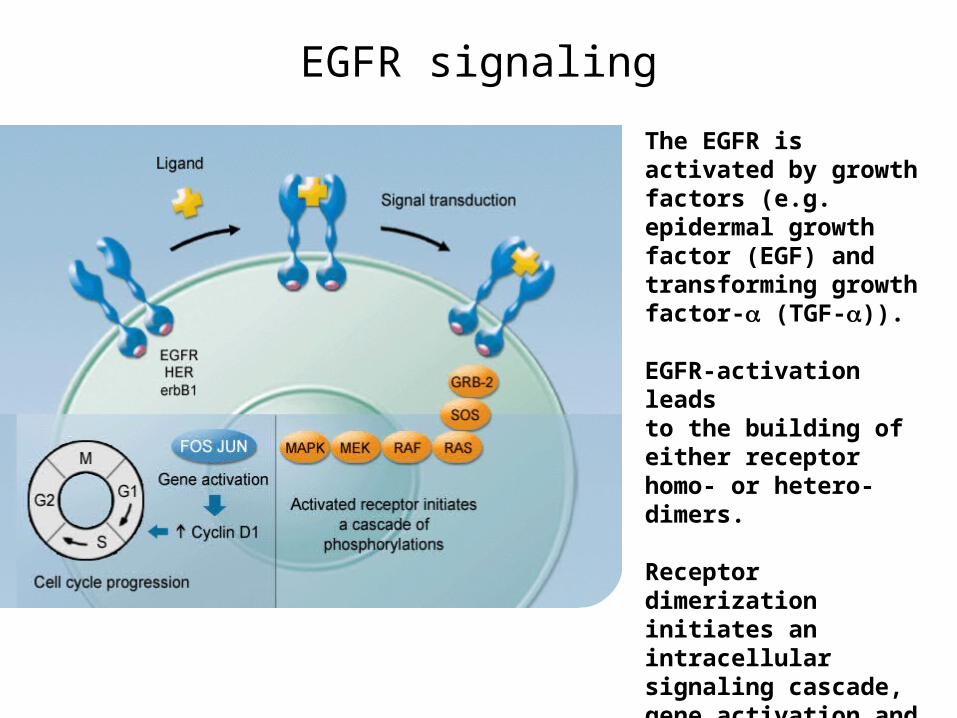
EGFR signaling
The EGFR is activated by growth factors (e.g. epidermal growth factor (EGF) and transforming growth factor- (TGF-)).
EGFR-activation leads to the building of either receptor homo- or hetero-dimers.
Receptor dimerization initiates an intracellular signaling cascade, gene activation and the stimulation of cell cycle progression.

The importance of EGFR as a target
“Evidence for a role for the EGFR in the inhibition and pathogenesis of various cancers has led to the rational design and development of agents that selectively target this receptor.”*
* Baselga 2002

Erbitux® (cetuximab)
• Erbitux® (cetuximab) is an IgG1 MAb targeting the EGFR
• Binding blocks EGFR signaling and inhibits proliferation, angio-genesis and metastasis, and stimulates apoptosis and differentiation
• The main toxicity is an acne-like rash that generally improves during treatment, and usually does not preclude continued treatment
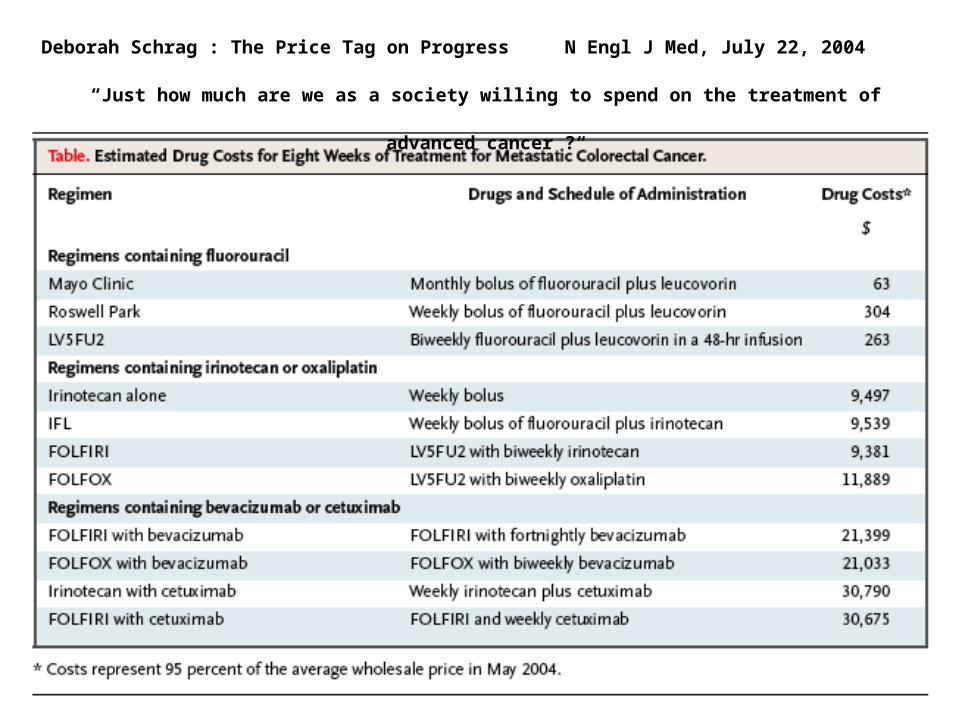
Deborah Schrag : The Price Tag on Progress N Engl J Med, July 22, 2004
“Just how much are we as a society willing to spend on the treatment of advanced
cancer ?“

in vivo:♦ mAb against differentia tionantigens (AD ,CC compleme ntfixation)♦ mAb with direc tanti-proliferative effects (grow threceptors, apoptosis)♦ mAb interfering w ithangiogenesis♦ mAb as carrier sfo r radioisotope s(radioimmunotherapy)♦ mAb as carrier sfo r toxins(immunotoxins)♦ Ant -i idiotype mAb♦ Bispecific mAb tofoc useffector cell ac tivity(effector cell targeting)
e xvivo:♦ Autologous / BM SC transplanta :tion pur ging of th eautograf twith mAb♦ Allogeneic /BM SC transplanta : tion prevention of GVHD by T ce ll depletion
Strategies for Therapeutic Application of Monoclonal Antibodies

Inhibition of Angiogenesis






in vivo:♦ mAb against differentia tionantigens (AD ,CC compleme ntfixation)♦ mAb with direc tanti-proliferative effects (grow threceptors, apoptosis)♦ mAb interfering w ithangiogenesis♦ mAb as carrier sfo r radioisotope s(radioimmunotherapy)♦ mAb as carrier sfo r toxins(immunotoxins)♦ Ant -i idiotype mAb♦ Bispecific mAb tofoc useffector cell ac tivity(effector cell targeting)
e xvivo:♦ Autologous / BM SC transplanta :tion pur ging of th eautograf twith mAb♦ Allogeneic /BM SC transplanta : tion prevention of GVHD by T ce ll depletion
Strategies for Therapeutic Application of Monoclonal Antibodies
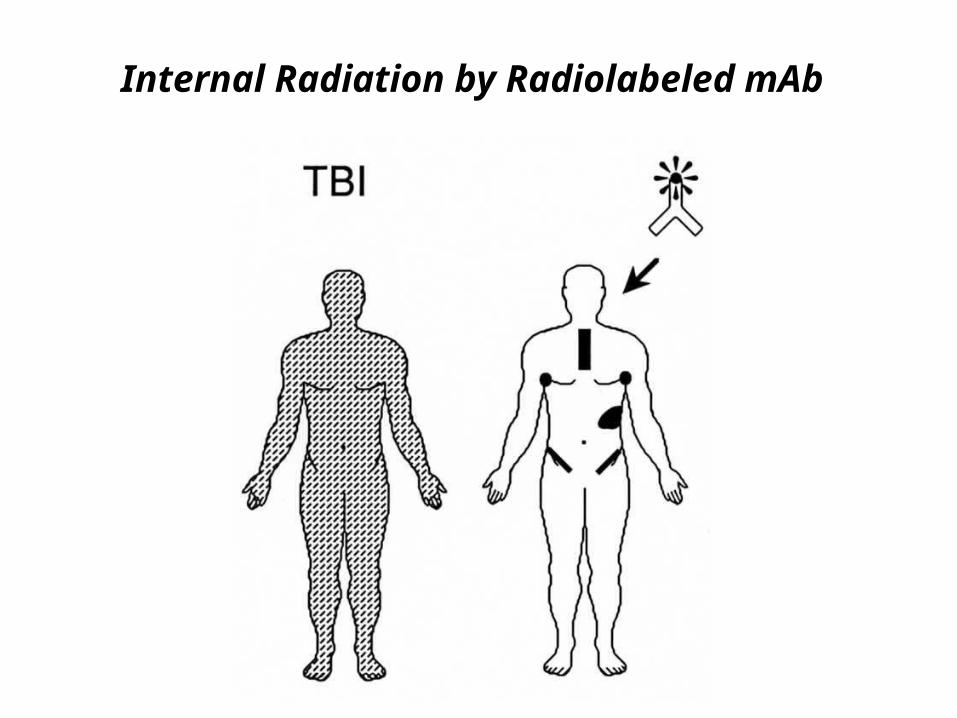
Internal Radiation by Radiolabeled mAb
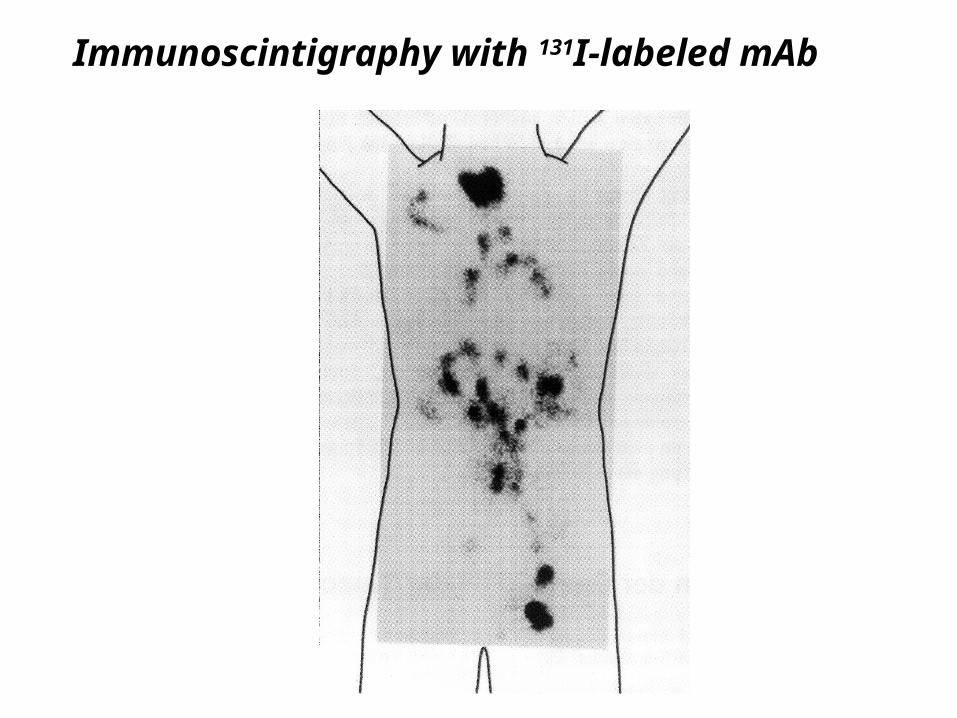
Immunoscintigraphy with 131I-labeled mAb
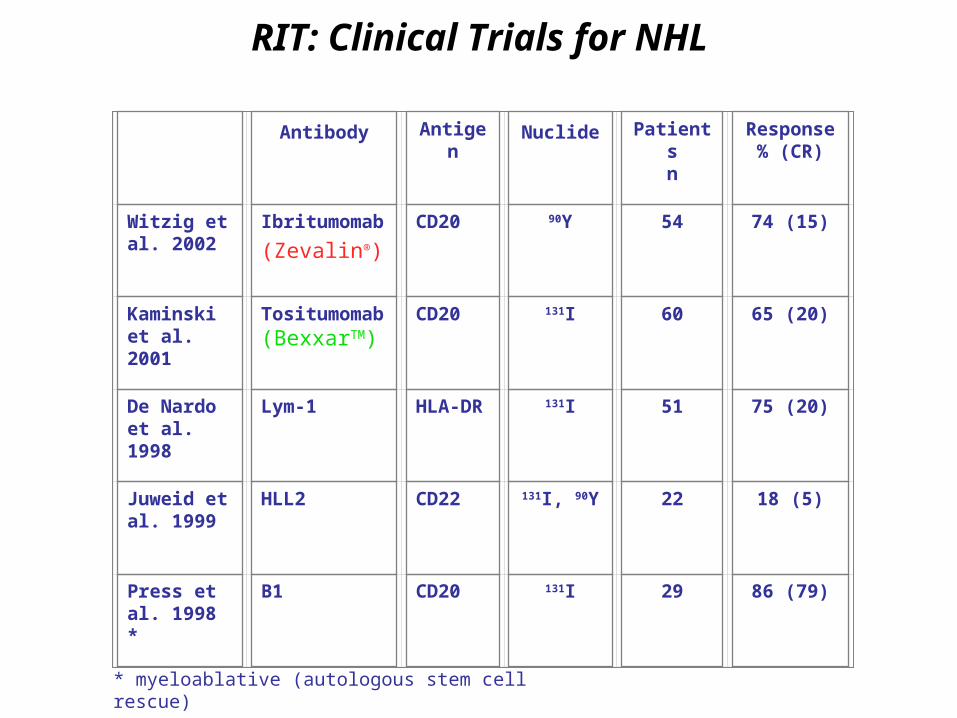
RIT: Clinical Trials for NHL
* myeloablative (autologous stem cell rescue)
Antibody Antigen Nuclide Patientsn
Response% (CR)
Witzig et al. 2002
Ibritumomab
(Zevalin®)
CD20 90Y 54 74 (15)
Kaminski et al. 2001
Tositumomab(BexxarTM)
CD20 131I 60 65 (20)
De Nardo et al. 1998
Lym-1 HLA-DR 131I 51 75 (20)
Juweid et al. 1999
HLL2 CD22 131I, 90Y 22 18 (5)
Press et al. 1998 *
B1 CD20 131I 29 86 (79)

in vivo: ♦ mAb against differentiation antigens ( ,ADCC complement fixatio )n ♦ mAb with direct anti-proliferative effects (growth ,receptors apop )tosis ♦ mAb interfering with angiogenesis ♦ mAb as carriers for radioisotopes (radioimmunotherap )y ♦ mAb as ca rriers for toxins (immunotox )ins ♦ Anti-idiotype mAb ♦ Bispecific mAb to focus effector cell activity (effector cell targeti )ng
ex vivo: ♦ Autologous BM/SC transplantation: purging of the autograft with mAb ♦ Allogeneic BM/SC transplantation: preventio n o f GVHDby T cell depletion
Strategies for Therapeutic Application of Monoclonal Antibodies
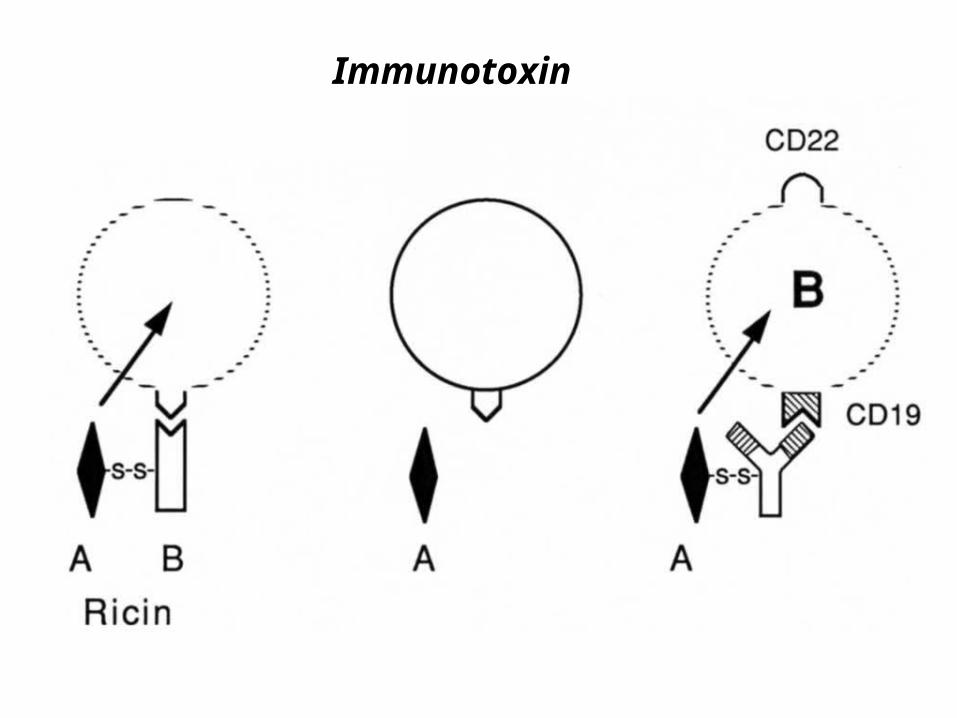
Immunotoxin
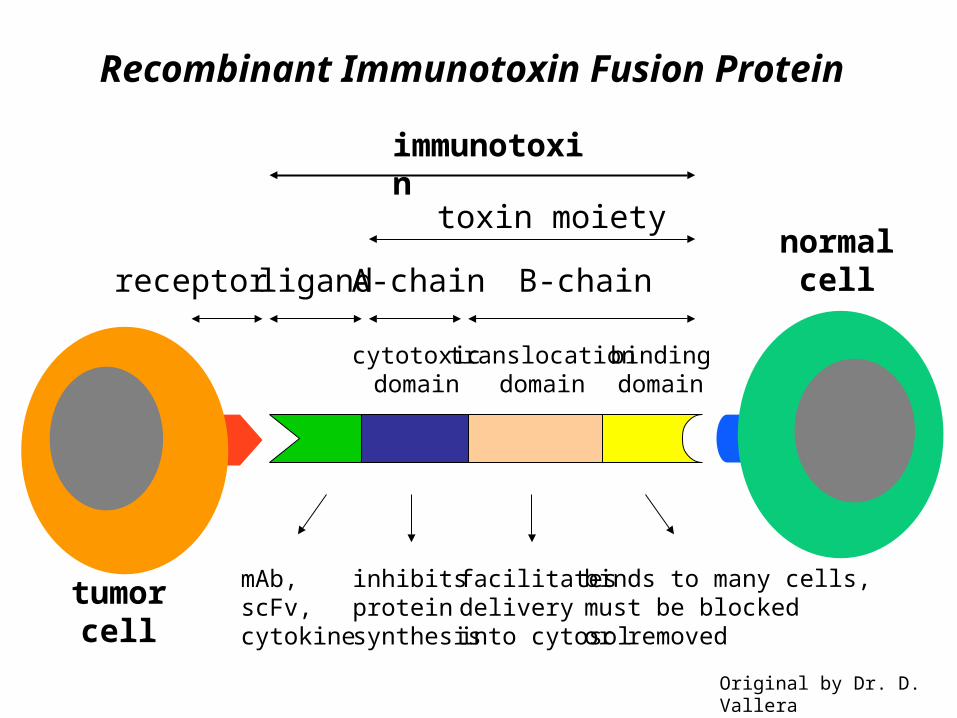
tumorcell
normalcellligand A-chain B-chain
immunotoxin
facilitatesdeliveryinto cytosol
binds to many cells,must be blockedor removed
inhibitsproteinsynthesis
mAb,scFv,cytokine
receptor
cytotoxicdomain
translocationdomain
bindingdomain
toxin moiety
Recombinant Immunotoxin Fusion Protein
Original by Dr. D. Vallera

in vivo:♦ mAb against leukocyte differentiation antige ns(ADCC, complement fixation)♦ mAb with direc tanti-proliferative effects (grow threceptors, apoptosis)♦ mAb as carrier sfo r radioisotope s(radioimmunotherapy)♦ mAb as carrier sfo r toxins(immunotoxins)♦ Ant -i idiotype mAb♦ Bispecific mAb tofoc useffector cell ac tivity(effector cell targeting)
e xvivo:♦ Autologous / BM SC transplanta :tion pur ging of th eautograf twith mAb♦ Allogeneic /BM SC transplanta : tion prevention of GVHD by T ce ll depletion
Strategies for Therapeutic Application of Monoclonal Antibodies

Monoclonal anti-Idiotype Antibodies

in vivo:♦ mAb against differentia tionantigens (AD ,CC compleme ntfixation)♦ mAb with direc tanti-proliferative effects (grow threceptors, apoptosis)♦ mAb interfering w ithangiogenesis♦ mAb as carrier sfo r radioisotope s(radioimmunotherapy)♦ mAb as carrier sfo r toxins(immunotoxins)♦ Ant -i idiotype mAb♦ Bispecific mAb tofoc useffector cell ac tivity(effector cell targeting)
e xvivo:♦ Autologous / BM SC transplanta :tion pur ging of th eautograf twith mAb♦ Allogeneic /BM SC transplanta : tion prevention of GVHD by T ce ll depletion
Strategies for Therapeutic Application of Monoclonal Antibodies
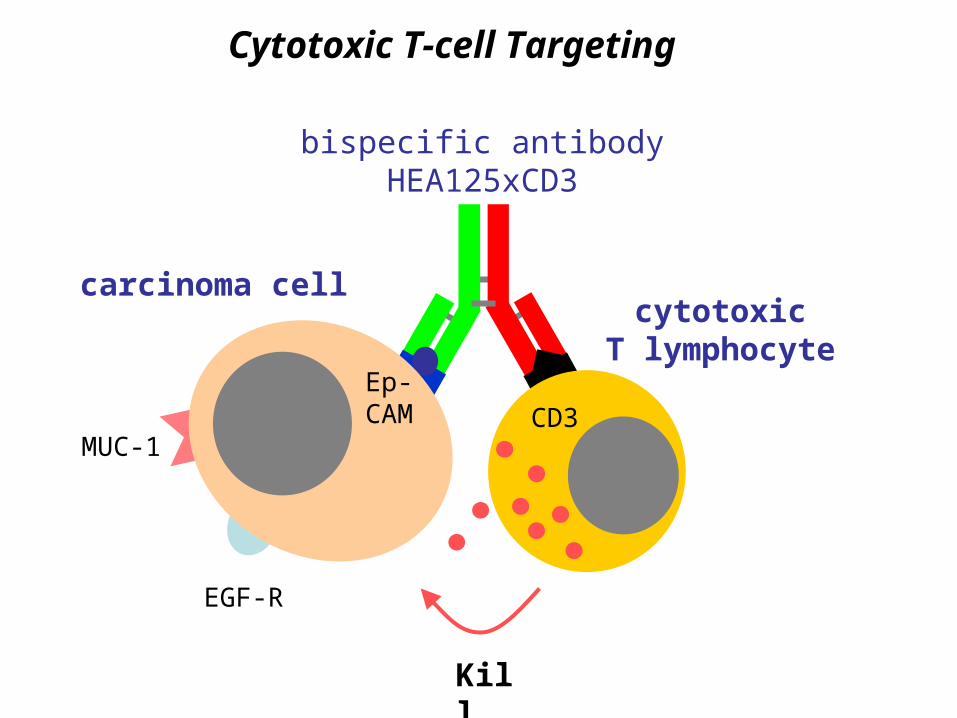
Kill
EGF-R
MUC-1
cytotoxicT lymphocyte
carcinoma cell
CD3Ep-CAM
bispecific antibodyHEA125xCD3
Cytotoxic T-cell Targeting

Ovarian Carcinoma Stained for Ep-CAM Expression
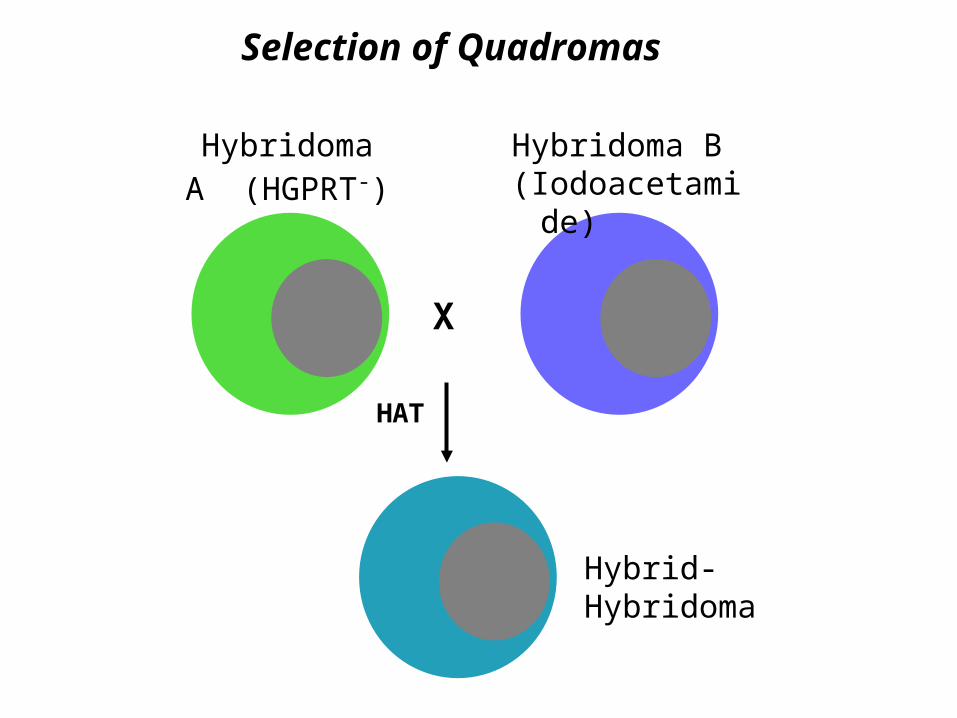
Selection of Quadromas
X
Hybridoma A (HGPRT-)
Hybridoma B (Iodoacetamide)
HAT
Hybrid-Hybridoma

Zur Anzeige wird der QuickTime™ Dekompressor „TIFF (Unkomprimiert)“ benötigt.
Antibody Mixture Produced by Hybrid-Hybridomas
♦ Leading cause of death among gynecological malignancies
♦ Therapy consists of cytoreductive surgery and combination chemotherapy
♦ Prognosis of advanced disease is very poor (5 year survival at stages III and IV
less than 20%)
=> Early spread of carcinoma cells from ovaries into the peritoneal cavity
giving rise to multiple metastases
=> Formation of malignant ascites leading to severe symptoms (anorexia,
dyspnea, obstruction of the gastrointestinal tract)
Ovarian Cancer

Patient inclusion criteria
- Histologically confirmed ovarian carcinoma
- Recurrent ascites
- Resistance to second- or third line chemotherapy
- Life expectancy > 6 month
- Written informed consent
S tud y p ro toc ol
- Removal of malignant ascites by ultrasound-guided puncture
- Weekly intraperitoneal application of 1 mg bsAb in 500 ml saline
- Evaluation after 4 courses of therapy
- In case of ascites regression continuation of therapy until progression
Obje ctives
- Toxicity (cytokine syndrome?)
- Reduction of ascites volume
- Cytokine profile in ascites
Clinical Trial of Intraperitoneal BsAb Therapyin Patients with Advanced Ovarian Cancer

Ascites production lowest value
during therapyPatient
1 1,020 263
2 135 03 218 04 190 05 533 06 290 07 571 3508 1,000 09 200 010 320 0
Ascites production before therapy
Ascites volume in ml/day
asc
ites
vo
lum
e
Changes in Ascites Volume during bsAb Therapy
Patient 2
0
100
200
300
400
500
600
700
800
0
500
1000
1500
2000
2500
3000
3500
4000
CA
125
ser
um
lev
el
ascites ml/d
CA125 U/ml
HEA125xOKT3 applications
8 month of follow up
All patients
Collaboration with the Department of Obstetrics and Gynecology at the University of Heidelberg(Dr. A. Marmé, Prof. G. Bastert)

Eighteen Therapeutic Antibodies
Approved by the FDA
Paul Ehrlich(1854-1915)
Finally, the dreams of Paul Ehrlichwho considered antibodiesas magic bullets have become reality.
Monoclonal antibodies haveestablished themselves as the mostimportant and rapidly expandingclass of drugs in oncology.