tunel carpo po
TRANSCRIPT
8/8/2019 tunel carpo PO
http://slidepdf.com/reader/full/tunel-carpo-po 1/7
644 AJR:193, September 2009
Materials and Methods
Our institutional review board approved this
study, and oral inormed consent was obtained
rom all patients.
Patient Sample
We perormed a retrospective study o 47 wrists
o 47 patients (11 men, 36 women; mean age, 55
years; range, 27–81 years) consecutively reerred
or MRI by an orthopedic surgeon at our institu-
tion. Because they had upper extremity symptoms
ater open surgical release o the median nerve,
the 47 patients had been consecutively reerred to
and reexamined by the orthopedic surgeon or
electrophysiologic evidence o CTS. The previous
surgical release had been perormed by several or-
thopedic surgeons at other institutions. No patientreceived steroid injections or other treatments to
manage chronic pain syndromes beore the MRI
examination. During reexaminations, nerve con-
duction studies and needle EMG were used to de-
termine the presence or absence o recurrent CTS
ater surgery.
Thirty-ve patients had EMG evidence o recur-
rent CTS. The 12 patients without EMG evidence
o recurrent CTS were the control group. The con-
trol group was not a truly disease-ree group. The
MRI Assessment of Recurrent
Carpal Tunnel Syndrome AfterOpen Surgical Release of theMedian Nerve
Raphaël Campagna1
Eric Pessis1
Antoine Feydy1
Henri Guerini1
Dominique Le Viet2
Patrick Corlobé2
Jean-Luc Drapé1
Campagna R, Pessis E, Feydy A, et al.
1
Université Paris Descartes, Assistance Publique-Hôpitaux de Paris, Service de Radiologie B, Hôpital
Cochin, 27 rue du Faubourg Saint Jacques, 75679 Paris
Cedex 14, France. Address correspondence to
R. Campagna ([email protected]).
2Institut de la Main, Paris, France.
Musculoskeleta l Imaging • Orig ina l Research
AJR 2009; 193:644–650
0361–803X/09/1933–644
© American Roentgen Ray Society
The diagnosis o carpal tunnel syn-
drome (CTS) relies on clinical
eatures and electrophysiologic
data. Although imaging o the
median nerve in the carpal tunnel has received
attention in the literature, the technique has
limited value in the diagnosis o CTS in daily
practice [1, 2]. Surgical release o the median
nerve is requently needed when conservative
treatment has ailed. However, ater surgical
release, some patients continue to have symp-
toms. Because ailure o nerve decompression
has numerous causes [3–7], including teno-
synovitis o fexor tendons, nerve section, -
brosis, extrinsic nerve compression, nerve en-
trapment, and bone racture, these patients
pose a challenging clinical problem. In addi-tion, the occurrence o subjective pain ater
surgery is well known [8], and objective evi-
dence o nerve dysunction must be present
or urther surgical exploration. Imaging can
be helpul in the postoperative care o these
patients. We aimed to determine with MRI
the morphologic eatures o the median nerve
in patients with electrophysiologic (electro-
myographic [EMG]) evidence o recurrent
CTS ater surgical release.
Keywords: carpal tunnel, electromyography, MRI, wrist
DOI:10.2214/AJR.08.1433
Received June 24, 2008 ; accepted ater revision
February 3, 2009.
F O C U S O N :
OBJECTIVE. The purpose o this study was to retrospectively determine the accuracy o
MRI in identication o the morphologic eatures o median nerve dysunction ater surgical
release o the median nerve or carpal tunnel syndrome.
MATERIALS AND METHODS. Two blinded readers independently evaluated axial
1.5-T MR images or retinacular regrowth, morphologic characteristics o the median nerve,
and presence o mass eect, brosis, and carpal tunnel decompression. All 47 patients (11
men, 36 women; mean age, 55 years; range, 27–81 years) had undergone open surgical releaseo the median nerve or carpal tunnel syndrome. Thirty-ve patients had electromyographic
evidence o recurrent carpal tunnel syndrome. The other 12 patients did not have electrophys-
iologic evidence o recurrent carpal tunnel syndrome and were the control group.
RESULTS. A statistically signicant dierence between the recurrent carpal tunnel syn-
drome and control groups was ound or brosis ( p = 0.009), nerve enhancement ( p = 0.04),
and median nerve width ( p = 0.008) and ratio ( p = 0.01) at the pisiorm level.
CONCLUSION. MRI may be used in association with electromyography or accurate
postoperative evaluation o the carpal tunnel.
Campagna et al.MRI o Carpal Tunnel Syndrome
Musculoskeletal ImagingOriginal Research

8/8/2019 tunel carpo PO
http://slidepdf.com/reader/full/tunel-carpo-po 2/7
AJR:193, September 2009 645
MRI of Carpal Tunnel Syndrome
patients had undergone MRI because o clinical
and electrophysiologic suspicion o ulnar nerve en-
trapment in Guyon’s tunnel (n = 1), clinical suspi-
cion o tenosynovitis (n = 3), and discrepancy be-
tween normal EMG results and clinical examination
ndings (loss o grip strength, scar discomort) (n =
8). To eliminate alse-positive results, we excluded
patients who had undergone EMG or MRI within 6
months ater surgery [9].
Imaging
MRI was perormed with a 1.5-T MRI unit
(Signa Excite, GE Healthcare) with a dedicated
quadrature wrist coil. All patients were placed in
the MR imager in the prone position with the el-
bow extended overhead and the pronated hand in
the center o the coil. The pulse sequences were an
axial spin-echo T1-weighted sequence (TR/TE,
400/14; section thickness, 4 mm; eld o view, 6
cm; acquisition time, 4 minutes 21 seconds; num-
ber o signals acquired, 4; matrix size, 256 × 160;
gap, 0.4 mm), an axial ast spin-echo STIR se-
quence (2,320/14; inversion time, 150 millisec-
onds; echo-train length, 9; section thickness, 4
mm; eld o view, 6 cm; acquisition time, 3 min-
utes 36 seconds; number o signals acquired, 4;
matrix size, 256 × 160; gap, 0.4 mm), and an axial
ast spin-echo T1-weighted sequence with at sup-
pression ater IV injection o 0.1 mmol/kg o body
weight o gadoterate dimeglumine (Dotarem,
Guerbet) (600/15; echo-train length, 3; section
thickness, 4 mm; eld o view, 6 cm; acquisition
time, 4 minutes 24 seconds; number o signals ac-
quired, 4; matrix, 256 × 160; gap, 0.4 mm). The
mean time between surgery and MRI was 28months (range, 6–193 months), and the mean time
between MRI and electrophysiologic testing was 3
months (range, 0–24 months).
Electrophysiologic Tests
Electrophysiologic studies included needle EMG
and routine motor and sensory nerve conduction
studies. All studies were perormed by the same
electrophysiologist beore MRI. The needle elec-
trode was connected to an EMG system (Viking,
Nicolet). The 12 patients in the control group had
normal results o EMG and nerve conduction stud-
ies with the ollowing data: no spontaneous muscu-
lar activity, distal motor latency less than 4.4 milli-seconds, sensitive conduction velocity greater than
44 m/s, and Kimura centimetric value less than 0.2
ms/cm. Patients with at least one abnormal EMG or
nerve conduction result were included in the recur-
rent CTS group (n = 35) according to previous de-
scriptions [10–13]. Results can vary over the time
owing to environmental and technical actors [14].
In our study, however, all tests were perormed by
the same electrophysiologist, and the temperature
o the room and the skin was monitored. All electro-
physiologic studies were perormed at least 6
months ater surgery.
Image Analysis
Two musculoskeletal radiologists (4 and 15
years o experience) blinded to electrophysiologic
results reviewed the images independently and
retrospectively at random using a PACS worksta-
tion (Carestream, Kodak). Discrepancies were re-
solved by consensus.
According to previous MRI descriptions o the
preoperative ndings o CTS and known operative
complications [3, 6, 15–19], the ollowing ndings
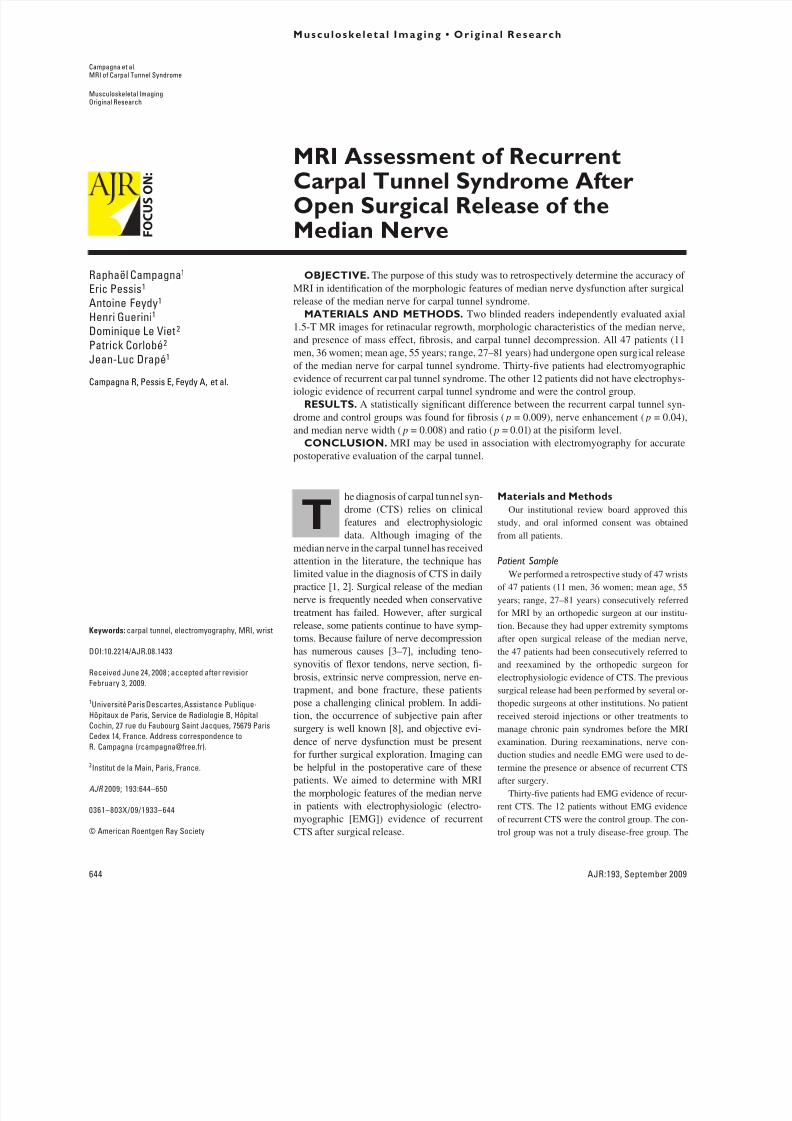
were reviewed. First, regrowth o the fexor reti-
naculum was dened as a continuous, linear area
o low signal intensity supercial to the nerve and
thickened in the area deep in relation to the subcu-
taneous scar (Figs. 1 and 2). Regrowth included
incomplete resection o the retinaculum, the pres-
ence o scar tissue that mimicked retinaculum,
and true regrowth o the retinaculum.
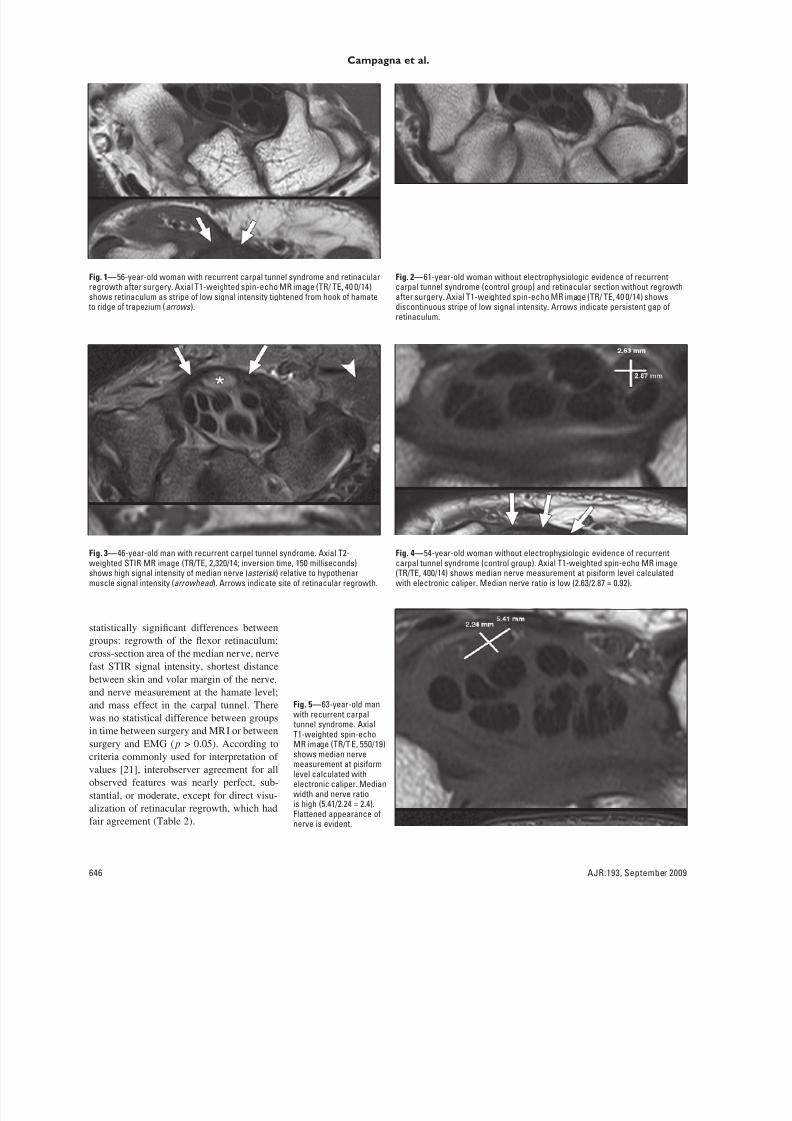
Second, median nerve analysis included the
presence o high signal intensity on ast STIR im-
ages in comparison with thenar muscle signal in-
tensity (Fig. 3). Median nerve measurements were
obtained with an electronic caliper at the proximal
(pisiorm) and distal (hook o the hamate) levels.
The cross-sectional area and ratio o width to
height (fattening ratio) were measured in milli-
meters at the two levels (Figs. 4 and 5). Nerve en-
hancement ater IV gadolinium injection was con-
sidered high i stronger than thenar muscle
enhancement (Fig. 6B). The shortest distance be-
tween the skin and the volar margin o the mediannerve was measured on axial images with an elec-
tronic caliper at the distal level (Fig. 7).
Third, analysis o mass eect in the carpal tun-
nel included the presence o bursitis (ocal fuid
collection > 1 cm in the carpal tunnel), a mass, ac-
cessory muscles or distal progression o the mus-
cle belly, bone racture or ragment, or fexor ten-
don tenosynovitis (excessive fuid within the
tendon sheath with gadolinium enhancement).
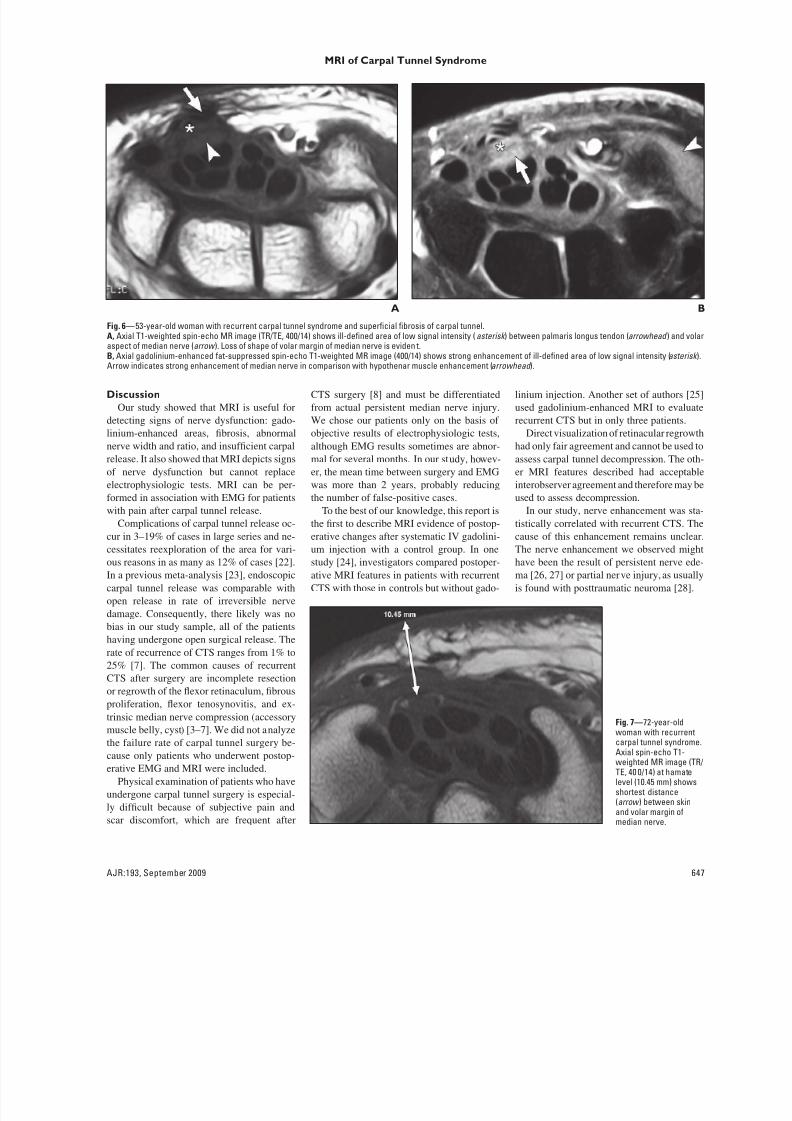
Fourth, the presence o brosis was dened by an
extensive area o low signal intensity with an ill-
dened nerve margin on T1-weighted images
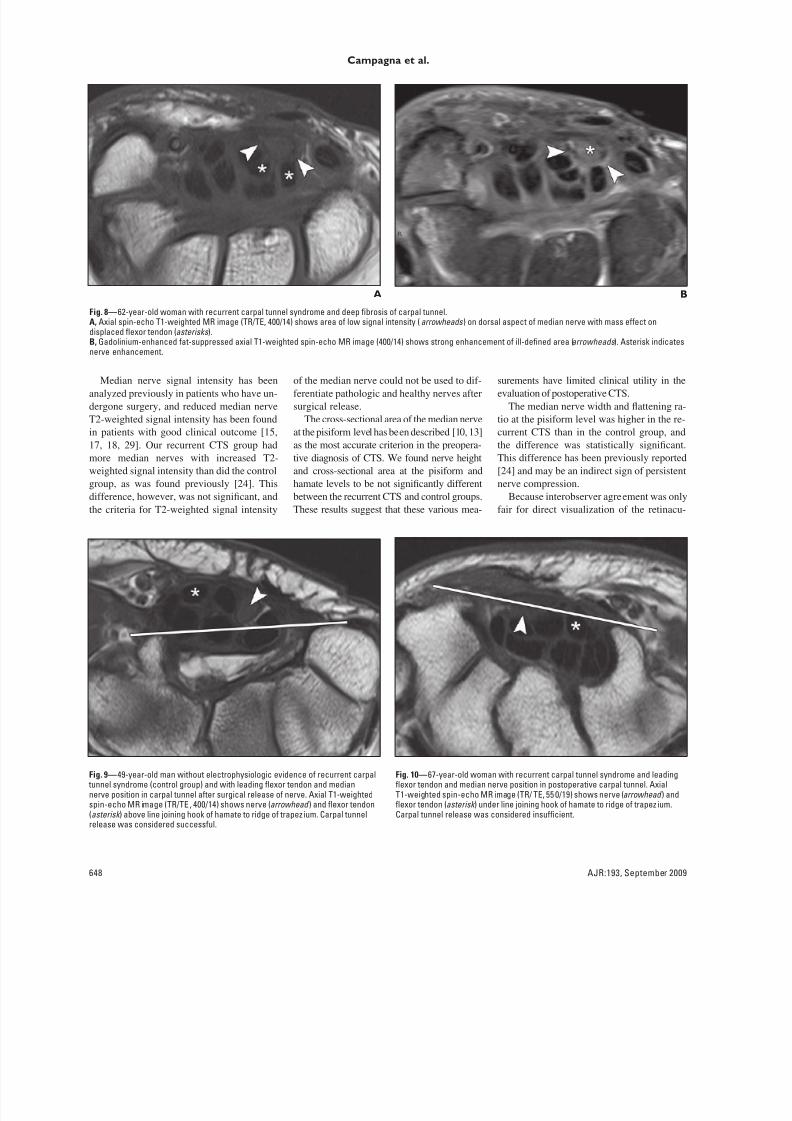
(Figs. 6 and 8). Fith, to assess the quality o car-
pal tunnel decompression, we determined the po-
sition o the median nerve and leading fexor ten-
don. This position was compared with the line
joining the hook o the hamate to the ridge o the
trapezium, according to previous ndings [20].
Carpal release was considered successul i the
tendon or nerve was located above the line and i
no tendon or nerve was entirely located under this
line (Fig. 9). In the other cases, carpal tunnel re-
lease was considered insucient (Fig. 10).
Statistical Analysis
Quantitative variables were reported with the
mean and range (minimum to maximum). Cate-
goric variables were reported as count (percent-
age). Statistical analysis was perormed with a
nonparametric test (Mann-Whitney) or quantita-
tive variables and Fisher’s test or categoric vari-
ables. All tests were two sided. A value o p < 0.05
was considered signicant. Interrater agreement
was calculated or MRI ndings (kappa). All anal-
yses were perormed with statistical sotware
(MedCalc version 8.0, MedCalc Sotware).
Results
The sensitivity, specicity, and positive
and negative predictive values o MRI signs
are summarized in Table 1. The comparisons
o MRI signs or both groups are summa-rized in Tables 2 and 3. The ndings in the
recurrent CTS and control groups diered
statistically only or presence o brosis,
nerve enhancement, volar migration o nerve
and tendon (carpal decompression), and me-
dian nerve width and ratio at the pisiorm
level. For the ollowing items, there were no
TABLE 1: Sensitivity, Specificity, and Predictive Values of MRI Signs inDiagnosis of Recurrent Carpal Tunnel Syndrome
SignSensitivity
(%)Specicity
(%)Positive Predictive
Value (%)Negative Predictive
Value (%)
Retinacular regrowth 43 50 71 23Carpal tunnel mass eect 26 58 64 21
Fibrosis 60 83 92 42
Median nerve enhancement 40 92 94 34
Median nerve high signal intensity 74 33 77 31
Carpal tunnel decompression
Good 20 50 54 18
Insucient 80 50 82 46
8/8/2019 tunel carpo PO
http://slidepdf.com/reader/full/tunel-carpo-po 3/7
646 AJR:193, September 2009
Campagna et al.
statistically signicant dierences between
groups: regrowth o the fexor retinaculum;
cross-section area o the median nerve, nerve
ast STIR signal intensity, shortest distance
between skin and volar margin o the nerve,
and nerve measurement at the hamate level;
and mass eect in the carpal tunnel. Therewas no statistical dierence between groups
in time between surgery and MRI or between
surgery and EMG ( p > 0.05). According to
criteria commonly used or interpretation o
values [21], interobserver agreement or all
observed eatures was nearly perect, sub-
stantial, or moderate, except or direct visu-
alization o retinacular regrowth, which had
air agreement (Table 2).
Fig. 1—56-year-old woman with recurrent carpal tunnel syndrome and retinacularregrowth ater surgery. Axial T1-weighted spin-echo MR image (TR/ TE, 40 0/14)shows retinaculum as stripe o low signal intensity tightened rom hook o hamate
to ridge o trapezium (arrows ).
Fig. 2—61-year-old woman without electrophysiologic evidence o recurrentcarpal tunnel syndrome (control group) and retinacular section without regrowthater surgery. Axial T1-weighted spin-echo MR image (TR/ TE, 40 0/14) showsdiscontinuous stripe o low signal intensity. Arrows indicate persistent gap oretinaculum.
Fig. 3—46-year-old man with recurrent carpel tunnel syndrome. Axial T2-weighted STIR MR image (TR/TE, 2,320/14; inversion time, 150 milliseconds)shows high signal intensity o median nerve (asterisk ) relative to hypothenarmuscle signal intensity (arrowhead ). Arrows indicate site o retinacular regrowth.
Fig. 4—54-year-old woman without electrophysiologic evidence o recurrentcarpal tunnel syndrome (control group). Axial T1-weighted spin-echo MR image(TR/TE, 400/14) shows median nerve measurement at pisiorm level calculatedwith electronic caliper. Median nerve ratio is low (2.63/2.87 = 0.92).
Fig. 5—63-year-old manwith recurrent carpal
tunnel syndrome. AxialT1-weighted spin-echoMR image (TR/T E, 550/19)shows median nervemeasurement at pisiormlevel calculated withelectronic caliper. Medianwidth and nerve ratiois high (5.41/2.24 = 2.4).Flattened appearance onerve is evident.
8/8/2019 tunel carpo PO
http://slidepdf.com/reader/full/tunel-carpo-po 4/7
AJR:193, September 2009 647
MRI of Carpal Tunnel Syndrome
Discussion
Our study showed that MRI is useul or
detecting signs o nerve dysunction: gado-
linium-enhanced areas, brosis, abnormal
nerve width and ratio, and insucient carpal
release. It also showed that MRI depicts signs
o nerve dysunction but cannot replace
electrophysiologic tests. MRI can be per-
ormed in association with EMG or patients
with pain ater carpal tunnel release.
Complications o carpal tunnel release oc-
cur in 3–19% o cases in large series and ne-
cessitates reexploration o the area or vari-
ous reasons in as many as 12% o cases [22].
In a previous meta-analysis [23], endoscopic
carpal tunnel release was comparable with
open release in rate o irreversible nerve
damage. Consequently, there likely was no
bias in our study sample, all o the patients
having undergone open surgical release. The
rate o recurrence o CTS ranges rom 1% to
25% [7]. The common causes o recurrent
CTS ater surgery are incomplete resection
or regrowth o the fexor retinaculum, brous
prolieration, fexor tenosynovitis, and ex-trinsic median nerve compression (accessory
muscle belly, cyst) [3–7]. We did not analyze
the ailure rate o carpal tunnel surgery be-
cause only patients who underwent postop-
erative EMG and MRI were included.
Physical examination o patients who have
undergone carpal tunnel surgery is especial-
ly dicult because o subjective pain and
scar discomort, which are requent ater
CTS surgery [8] and must be dierentiated
rom actual persistent median nerve injury.
We chose our patients only on the basis o
objective results o electrophysiologic tests,
although EMG results sometimes are abnor-
mal or several months. In our study, howev-
er, the mean time between surgery and EMG
was more than 2 years, probably reducing
the number o alse-positive cases.
To the best o our knowledge, this report is
the rst to describe MRI evidence o postop-
erative changes ater systematic IV gadolini-
um injection with a control group. In one
study [24], investigators compared postoper-
ative MRI eatures in patients with recurrent
CTS with those in controls but without gado-
linium injection. Another set o authors [25]
used gadolinium-enhanced MRI to evaluate
recurrent CTS but in only three patients.
Direct visualization o retinacular regrowth
had only air agreement and cannot be used to
assess carpal tunnel decompression. The oth-
er MRI eatures described had acceptable
interobserver agreement and thereore may be
used to assess decompression.
In our study, nerve enhancement was sta-
tistically correlated with recurrent CTS. The
cause o this enhancement remains unclear.
The nerve enhancement we observed might
have been the result o persistent nerve ede-
ma [26, 27] or partial nerve injury, as usually
is ound with posttraumatic neuroma [28].
A
Fig. 6—53-year-old woman with recurrent carpal tunnel syndrome and supercial brosis o carpal tunnel.A, Axial T1-weighted spin-echo MR image (TR/TE, 400/14) shows ill-dened area o low signal intensity ( asterisk ) between palmaris longus tendon (arrowhead ) and volaraspect o median nerve (arrow ). Loss o shape o volar margin o median nerve is eviden t.
B, Axial gadolinium-enhanced at-suppressed spin-echo T1-weighted MR image (400/14) shows strong enhancement o ill-dened area o low signal intensity (asterisk ).Arrow indicates strong enhancement o median nerve in comparison with hypothenar muscle enhancement (arrowhead ).
B
Fig. 7—72-year-oldwoman with recurrentcarpal tunnel syndrome.Axial spin-echo T1-weighted MR image (TR/TE, 40 0/14) at hamatelevel (10.45 mm) showsshortest distance(arrow ) between skinand volar margin omedian nerve.
8/8/2019 tunel carpo PO
http://slidepdf.com/reader/full/tunel-carpo-po 5/7
648 AJR:193, September 2009
Campagna et al.
Median nerve signal intensity has been
analyzed previously in patients who have un-
dergone surgery, and reduced median nerve
T2-weighted signal intensity has been ound
in patients with good clinical outcome [15,
17, 18, 29]. Our recurrent CTS group had
more median nerves with increased T2-
weighted signal intensity than did the control
group, as was ound previously [24]. This
dierence, however, was not signicant, and
the criteria or T2-weighted signal intensity
o the median nerve could not be used to di-
erentiate pathologic and healthy nerves ater
surgical release.
The cross-sectional area o the median nerve
at the pisiorm level has been described [10, 13]
as the most accurate criterion in the preopera-
tive diagnosis o CTS. We ound nerve height
and cross-sectional area at the pisiorm and
hamate levels to be not signicantly dierent
between the recurrent CTS and control groups.
These results suggest that these various mea-
surements have limited clinical utility in the
evaluation o postoperative CTS.
The median nerve width and fattening ra-
tio at the pisiorm level was higher in the re-
current CTS than in the control group, and
the dierence was statistically signicant.
This dierence has been previously reported
[24] and may be an indirect sign o persistent
nerve compression.
Because interobserver agreement was only
air or direct visualization o the retinacu-
A
Fig. 8—62-year-old woman with recurrent carpal tunnel syndrome and deep brosis o carpal tunnel.A, Axial spin-echo T1-weighted MR image (TR/TE, 400/14) shows area o low signal intensity ( arrowheads ) on dorsal aspect o median nerve with mass eect ondisplaced fexor tendon (asterisks ).B, Gadolinium-enhanced at-suppressed axial T1-weighted spin-echo MR image (400/14) shows strong enhancement o ill-dened area (arrowheads ). Asterisk indicates
nerve enhancement.
B
Fig. 9—49-year-old man without electrophysiologic evidence o recurrent carpal tunnel syndrome (control group) and with leading fexor tendon and mediannerve position in carpal tunnel ater surgical release o nerve. Axial T1-weightedspin-echo MR image (TR/TE , 400/14) shows nerve (arrowhead ) and fexor tendon(asterisk ) above line joining hook o hamate to ridge o trapez ium. Carpal tunnelrelease was considered successul.
Fig. 10—67-year-old woman with recurrent carpal tunnel syndrome and leadingfexor tendon and median nerve position in postoperative carpal tunnel. AxialT1-weighted spin-echo MR image (TR/ TE, 55 0/19) shows nerve (arrowhead ) andfexor tendon (asterisk ) under line joining hook o hamate to ridge o trapez ium.Carpal tunnel release was considered insucient.
8/8/2019 tunel carpo PO
http://slidepdf.com/reader/full/tunel-carpo-po 6/7
AJR:193, September 2009 649
MRI of Carpal Tunnel Syndrome
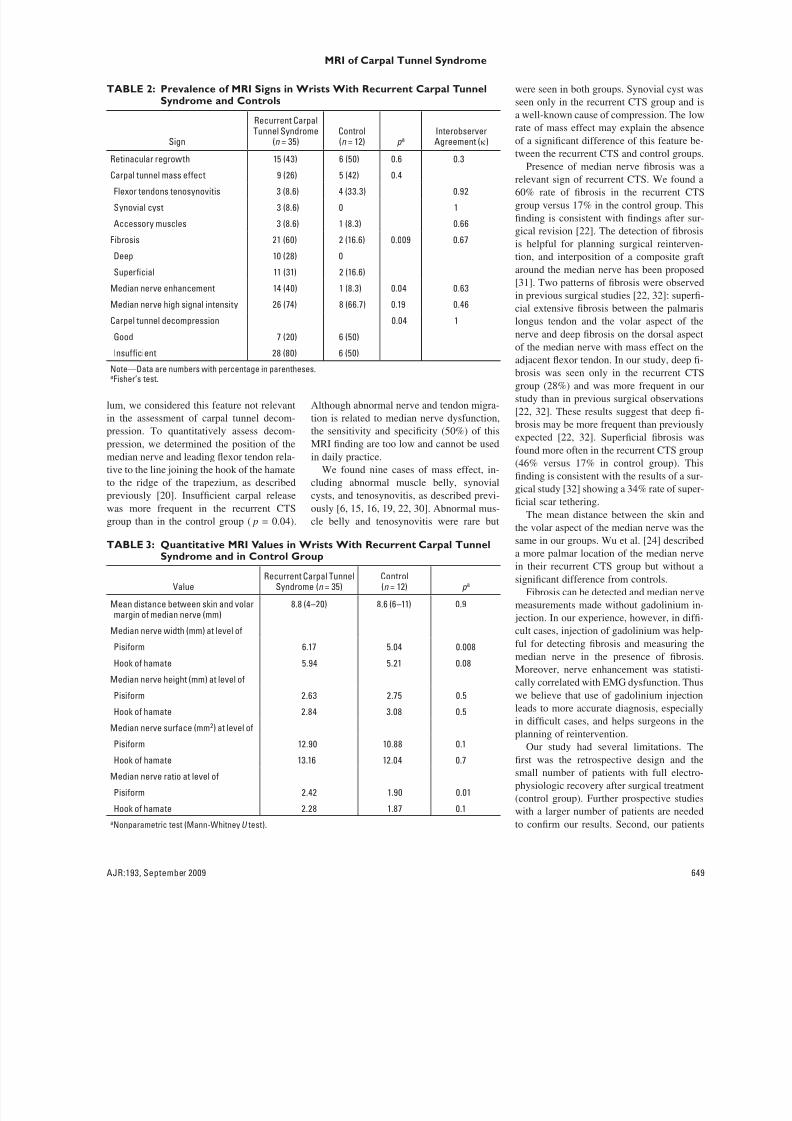
lum, we considered this eature not relevant
in the assessment o carpal tunnel decom-
pression. To quantitatively assess decom-
pression, we determined the position o the
median nerve and leading fexor tendon rela-
tive to the line joining the hook o the hamate
to the ridge o the trapezium, as described
previously [20]. Insucient carpal release
was more requent in the recurrent CTS
group than in the control group ( p = 0.04).
Although abnormal nerve and tendon migra-
tion is related to median nerve dysunction,
the sensitivity and specicity (50%) o this
MRI nding are too low and cannot be used
in daily practice.
We ound nine cases o mass eect, in-
cluding abnormal muscle belly, synovial
cysts, and tenosynovitis, as described previ-
ously [6, 15, 16, 19, 22, 30]. Abnormal mus-
cle belly and tenosynovitis were rare but
were seen in both groups. Synovial cyst was
seen only in the recurrent CTS group and is
a well-known cause o compression. The low
rate o mass eect may explain the absence
o a signicant dierence o this eature be-
tween the recurrent CTS and control groups.
Presence o median nerve brosis was a
relevant sign o recurrent CTS. We ound a60% rate o brosis in the recurrent CTS
group versus 17% in the control group. This
nding is consistent with ndings ater sur-
gical revision [22]. The detection o brosis
is helpul or planning surgical reinterven-
tion, and interposition o a composite grat
around the median nerve has been proposed
[31]. Two patterns o brosis were observed
in previous surgical studies [22, 32]: super-
cial extensive brosis between the palmaris
longus tendon and the volar aspect o the
nerve and deep brosis on the dorsal aspect
o the median nerve with mass eect on the
adjacent fexor tendon. In our study, deep -
brosis was seen only in the recurrent CTS
group (28%) and was more requent in our
study than in previous surgical observations
[22, 32]. These results suggest that deep -
brosis may be more requent than previously
expected [22, 32]. Supercial brosis was
ound more oten in the recurrent CTS group
(46% versus 17% in control group). This
nding is consistent with the results o a sur-
gical study [32] showing a 34% rate o super-
cial scar tethering.
The mean distance between the skin and
the volar aspect o the median nerve was thesame in our groups. Wu et al. [24] described
a more palmar location o the median nerve
in their recurrent CTS group but without a
signicant dierence rom controls.
Fibrosis can be detected and median nerve
measurements made without gadolinium in-
jection. In our experience, however, in di-
cult cases, injection o gadolinium was help-
ul or detecting brosis and measuring the
median nerve in the presence o brosis.
Moreover, nerve enhancement was statisti-
cally correlated with EMG dysunction. Thus
we believe that use o gadolinium injection
leads to more accurate diagnosis, especiallyin dicult cases, and helps surgeons in the
planning o reintervention.
Our study had several limitations. The
rst was the retrospective design and the
small number o patients with ull electro-
physiologic recovery ater surgical treatment
(control group). Further prospective studies
with a larger number o patients are needed
to conrm our results. Second, our patients
TABLE 3: Quantitative MRI Values in Wrists With Recurrent Carpal TunnelSyndrome and in Control Group
ValueRecurrent Carpal Tunnel
Syndrome (n = 35)Control(n = 12) p a
Mean distance between skin and volarmargin o median nerve (mm)
8.8 (4–20) 8.6 (6–11) 0.9
Median nerve width (mm) at level o
Pisiorm 6.17 5.04 0.008
Hook o hamate 5.94 5.21 0.08
Median nerve height (mm) at level o
Pisiorm 2.63 2.75 0.5
Hook o hamate 2.84 3.08 0.5
Median nerve surace (mm2) at level o
Pisiorm 12.90 10.88 0.1
Hook o hamate 13.16 12.04 0.7
Median nerve ratio at level o
Pisiorm 2.42 1.90 0.01
Hook o hamate 2.28 1.87 0.1
aNonparametric test (Mann-WhitneyU test).
TABLE 2: Prevalence of MRI Signs in Wrists With Recurrent Carpal TunnelSyndrome and Controls
Sign
Recurrent CarpalTunnel Syndrome
(n = 35)Control(n = 12) p a
InterobserverAgreement (κ)
Retinacular regrowth 15 (43) 6 (50) 0.6 0.3
Carpal tunnel mass eect 9 (26) 5 (42) 0.4Flexor tendons tenosynovitis 3 (8.6) 4 (33.3) 0.92
Synovial cyst 3 (8.6) 0 1
Accessory muscles 3 (8.6) 1 (8.3) 0.66
Fibrosis 21 (60) 2 (16.6) 0.009 0.67
Deep 10 (28) 0
Supercial 11 (31) 2 (16.6)
Median nerve enhancement 14 (40) 1 (8.3) 0.04 0.63
Median nerve high signal intensity 26 (74) 8 (66.7) 0.19 0.46
Carpel tunnel decompression 0.04 1
Good 7 (20) 6 (50)
Insucient 28 (80) 6 (50)
Note—Data are numbers with percentage in parentheses.aFisher’s test.

8/8/2019 tunel carpo PO
http://slidepdf.com/reader/full/tunel-carpo-po 7/7