ub medicine summer 2015
DESCRIPTION
For friends of the University at Buffalo School of Medicine and Biomedical Sciences.TRANSCRIPT
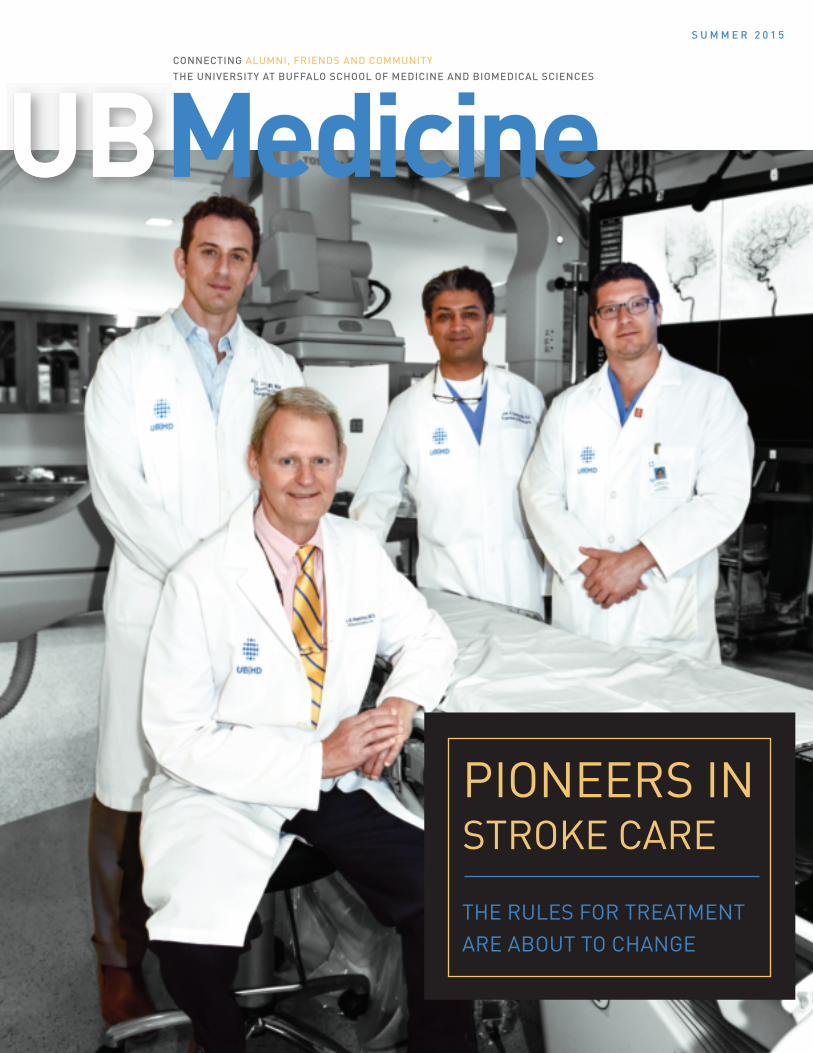
UB MedicineCONNECTING ALUMNI, FRIENDS AND COMMUNITY THE UNIVERSITY AT BUFFALO SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCES
S U M M E R 2 0 1 5
UB
PIONEERS IN STROKE CARE THE RULES FOR TREATMENT ARE ABOUT TO CHANGE
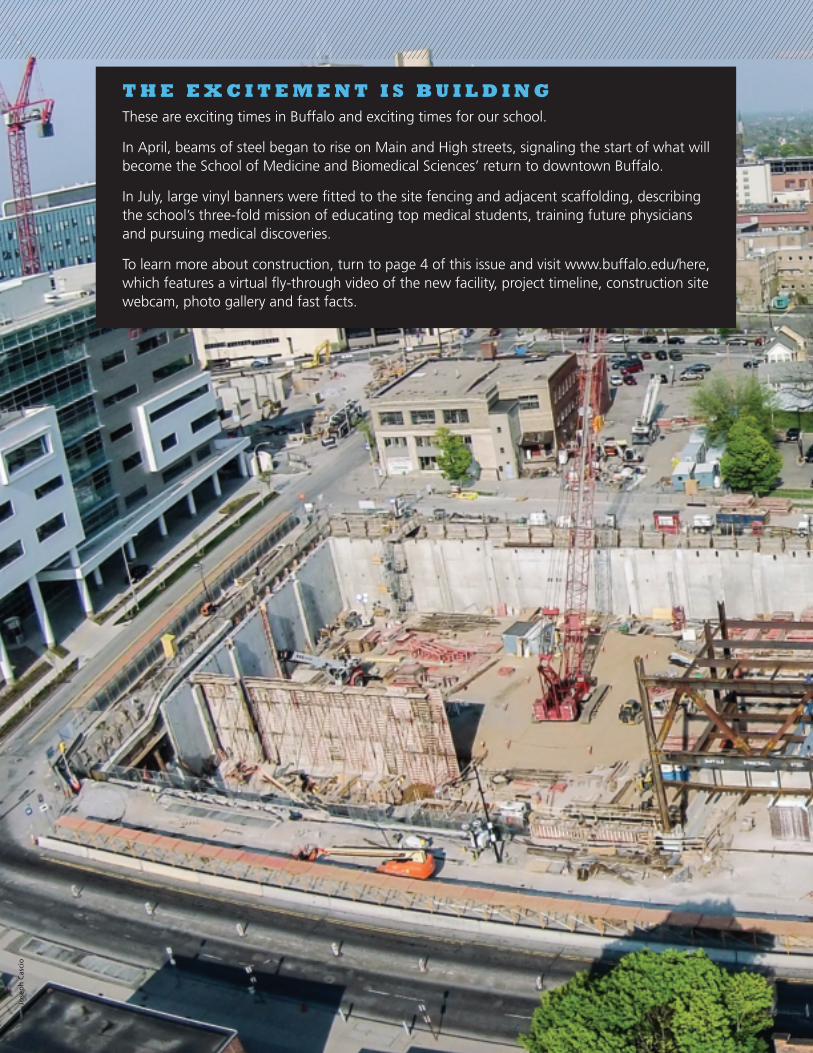
T H E E X C I T E M E N T I S B U I L D I N GThese are exciting times in Buffalo and exciting times for our school.
In April, beams of steel began to rise on Main and High streets, signaling the start of what will become the School of Medicine and Biomedical Sciences’ return to downtown Buffalo.
In July, large vinyl banners were fitted to the site fencing and adjacent scaffolding, describing the school’s three-fold mission of educating top medical students, training future physicians and pursuing medical discoveries.
To learn more about construction, turn to page 4 of this issue and visit www.buffalo.edu/here, which features a virtual fly-through video of the new facility, project timeline, construction site webcam, photo gallery and fast facts.
Jose
ph
Cas
cio

Pho
to b
y Jo
sep
h C
asci
o
Michael E. Cain, MD Vice President for Health Sciences and Dean, School of Medicine and Biomedical Sciences
EditorStephanie A. Unger
Contributing Writers Jill U Adams, Jim Bisco, Mary Cochrane, John DellaContrada, Lori Ferguson, Ellen Goldbaum, Colleen Karuza
CopyeditorTom Putnam
PhotographyJoseph Cascio, Philip J. Cavuoto, Sandra Kicman, Douglas Levere
Art Direction & DesignKaren Lichner
Editorial AdvisersJohn J. Bodkin II, MD ’76Elizabeth A. Repasky, PhD ’81
Major Affiliated Teaching HospitalsErie County Medical CenterRoswell Park Cancer InstituteVeterans Affairs Western New York Healthcare System
Kaleida Health Buffalo General Medical Center Gates Vascular Institute Women and Children’s Hospital of Buffalo Millard Fillmore Suburban Hospital
Catholic Health Mercy Hospital of Buffalo Sisters of Charity Hospital
Correspondence, including requests to be added to or removed from the mailing list, should be sent to: Editor, UB Medicine, 901 Kimball Tower, Buffalo, NY 14214; or email [email protected]
UB Medicine is published by the UB School of Medicine and Biomedical Sciences to inform alumni, friends and community about the school’s pivotal role in medical education, research and advanced patient care in Buffalo, Western New York and beyond.
Visit us: medicine.buffalo.edu/alumni
www.facebook.com/UBMedicalAlumniAssociation
15-DVC-004
UB MEDICINE MAGAZINE, Summer 2015, Vol. 3, No. 2
T A B L E O F C O N T E N T S
3 VITAL LINES
Progress notes
28 COLLABORATIONS
Partnerships at work
30 PATHWAYS
People in the news
32 Q & A
Conversations with experts
10 Prime Time for Stroke Care UB neurosurgeons have led efforts to explore minimally invasive approaches to stroke that are now being proven highly effective.
14 A LONG-TERM PLAN FOR PHYSICIAN SHORTAGESThe Western New York Medical Scholarship Fund, a community wide effort, aims to keep young physicians in our region.
18 THE RIGHT TEAM WITH THE RIGHT TOOLSUB is helping to reshape primary care through interprofessional education and improved electronic health records.
24 A STUDY IN SURVIVALThe clinical trials and extraordinary care that saved Baby Brown.
14
UBMEDICINE
COVER IMAGE: Clockwise: UB neurosurgeons L. Nelson “Nick” Hopkins III, MD, seated; Elad Levy, MD; Adnan Siddiqui, MD, PhD, and Kenneth Synder, MD.
Photo by Joseph Cascio
Do
ug
las
Leve
re
Alyssa Volmrich, Class of 2018, is one of the first recipients of the Western New York Medical Scholarship. Her scholarship is sponsored by HealthNow.

U B M E D V I T A L L I N E S
Stephanie T. Mucha, 97, who lives in the University Heights district of Buffalo, used to take evening walks in the neighborhood with her husband, the late Joseph J. Mucha. Their close proximity to theUB South Campus meant they often would meet and talk with UB students during these excursions. The Muchas so enjoyed speaking with these young people, they vowed to someday give money to create scholarships for UB students. After Joseph died, Stephanie carried out their plan, contribut-ing and pledging significant gifts to the university and several of its schools. Most recently, she made a gift of $1 million to UB’s new medical school, now being constructed on the Buffalo Niagara Medical Campus. In recognition of her gift, UB will name the dean’s suite in the new school the Stephanie T. Niciszewska Mucha and Joseph J. Mucha Dean’s Suite. Stephanie and Joseph had always been hard workers. Joseph emigrated to the U.S. from Poland as a teenager and worked as a machinist, and Stephanie worked as a licensed practical nurse. They also lived simply, driving only one car and converting their home into three apartments and renting out two of them. But Stephanie also had a knack for investing wisely in the stock market and would re-invest any profits rather than spend them. When she went to work at the Buffalo Veterans Administration Hospital, where she enjoyed a 44-year career, Stephanie witnessed a pivotal moment in the history of medicine that prompted her and Joseph to make an investment of a lifetime. What she saw was one of
AN INVESTMENT OF A LIFETIMEStephanie T. Mucha makes $1 million gift to new medical school
the hospital’s physicians, William Chardack, MD, and local inventor Wilson Greatbatch surgically insert the first implantable cardiac pace-maker into a dog, bringing it back to life. She went home and told Joseph about it, leading the couple to buy shares in Medtronic, the company licensed in 1961 to manufacture the device. That investment—50 shares for just over $250—and others increased exponentially over the course of five decades, leaving the Muchas with a healthy portfolio and a determination to give much of it to UB. Stephanie has fulfilled the pact she made with Joseph several times over, making significant gifts to support scholarships in UB’s schools of engineering, dental medicine and nursing, and in the College of Arts and Sciences. Her latest gift etches her and her husband’s names into the history of the UB School of Medicine and Biomedical Sciences and represents yet another investment of a lifetime. In a tribute to Stephanie’s self-taught investment knowledge, Barron’s news magazine—America’s premier financial publication—published an article about Stephanie in its September 2014 issue, calling her “The Oracle of Buffalo.” In 2015, UB named Stephanie the recipient of the highly coveted Walter P. Cooke Award, presented to non-alumni for notable and meritorious contributions influencing the growth and improvement of the university.
Stephanie Mucha and Dean Michael E. Cain, MD, with a rendering of the Stephanie T. Niciszewska Mucha and Joseph J. Mucha Dean’s Suite.
Pho
to b
y Je
nn
y Lu
k
3U B M E D I C I N ES U M M E R 2 0 1 5

U B M E D V I T A L L I N E S
Beams of steel began rising at the construction site at the corner of Main and High streets in downtown Buffalo in April, providing passersby with their first glimpse of the new School of Medicine and Biomedical Sciences, which will open in 2017. After a crawler crane was installed, steel erection began for floors 1 through 3. In July, a 280-foot tower crane will be erected to allow for construction of floors 4 through 8. Steel construction will take place for most of 2015, with installation of the exterior envelope of the building beginning in late 2015 and extending into 2016.
Building Mock-up Weathers the Test
Before the steel erection began, a 30-by-36-foot mockup of part of the building’s facade was constructed at the Construction Research Laboratory in Miami, where it then was subjected to simulations of powerful rain and windstorms to see how the building’s exterior will hold up against the elements. “The building mock-up passed with flying colors,” says Jennifer A. Kuhn, project manager for the new medical school building, who explains that the testing ran from mid-January to early March. The primary components tested were a glass curtain wall and its high-performance terra cotta rain screen. The glass walls and skylights will naturally illuminate the new medical school’s signa-ture feature, a light-filled, six-story glass atrium that will join the building’s two L-shaped structures.
THE EXCITEMENT IS BUILDING AS STEEL RISESInstallation of the exterior envelope begins in late 2015
“These are very rigorous, comprehensive tests that are typically done only on very large, custom projects,” says Michael Drozdowski, project manager with Gilbane/LiRo and the construction manager for the project.
Exterior Panels Manufactured Locally
It took 15 workers from LPCiminelli and their subcontractors about a month to construct the mock-up. They used the same glass and terra cotta panels that will comprise the building’s curtain wall, the exterior “skin” of modern, high-rise buildings that maximizes light-penetration, thermal-efficiency and water-diversion functions. Wind-pressure testing involved using an engine repurposed from an airplane.
U B M E D I C I N E4 S U M M E R 2 0 1 5

Pho
tos
by
Do
ug
las
Leve
re
“As its name suggests, High Street is one of the tallest points in the city of Buffalo, so it’s a fairly high wind pressure area,” notes David Schwartz, principal and senior project manager at HOK, the firm that designed the medical school. “For that reason, the building was tested to the maximum wind pressure that the site will realize: sustained winds of up to 50 or 60 miles per hour. We also modeled wind pressures to make sure that the building will be comfortable for pedestrians entering and leaving the facility.” How wind may affect the weight of snow drifts on the building’s rooftops during and after Buffalo’s snowstorms was studied earlier. The panels take advantage of local manufacturing expertise. They are being custom-made by Boston Valley Terra Cotta in Orchard Park, which, Schwartz points out, is one of the premier firms in the country that manufactures these panels. “Terra cotta was selected for a variety of reasons,” says
Schwartz. “It reflects and acknowledges the history of Buffalo’s architecture with colors emulating those on the Frank Lloyd Wright Darwin Martin House. The terra cotta panels also have an appealing, hand-made quality.” According to Schwartz, the rain screen is designed to allow rainwater to fall behind the terra cotta panels while reducing the pressure against the building so that if wind blows rain into the panels, the water will simply drain out at the bottom and away from the building. “We were trying to force it to leak,” Drozdowski adds, “trying to create the worst-case scenario so we can make any necessary modifications before beginning construction in Buffalo.” Even though off-site testing is complete, additional testing on the building will continue at the site. “All of this testing ensures that the quality control that occurred while we were at the testing lab will be the same quality control in Buffalo,” Drozdowski says.
5U B M E D I C I N ES U M M E R 2 0 1 5
U B M E D V I T A L L I N E S
The Margaret L. Wendt Foundation continued its commitment to improving the vitality of the Western New York region, making a $600,000 gift to support UB’s construction of a new medical school on the downtown Buffalo medical campus. The gift is in support of the Clinical Competency Center, a state-of-the-art facility that prepares medical students for national competency exams with real-world interactive scenarios featuring standardized patients. “The Wendt Foundation has been essential to fostering innovation at UB and throughout Western New York for many years, including pivotal gifts to develop the Buffalo Niagara Medical Campus,” says Michael E. Cain, MD, vice president for health sciences and dean, School of Medicine and Biomedical Sciences. “The foundation now continues its distinguished legacy of support
by investing in our new state-of-the-art facility,” Cain continues. “We appreciate this generous gift, which will help accelerate our collective efforts to promote excellence in biomedical education, research and patient care in our region.” The trustees of the foundation said they are giving to UB’s new medical school because of the vital role it will play in advancing health care treatment and research in the eight-county area. They stated: “The new UB medical school is now situated where it belongs—as an important physical presence and contributing partner among the comprehensive diagnostic, treatment, clinical and research institutions on the Buffalo Niagara Medical Campus. The Margaret L. Wendt Foundation, honoring the memory of its donor, is proud to support UB as it joins the campus in building a new era of medical education, treatment and discovery for our region.”
WENDT FOUNDATION SUPPORTS NEW ERA IN UB MEDICAL SCHOOL
Harold J. Levy, MD ’46, knows firsthand that UB’s new medical school building under construction is the second UB medical school to be located at Main and High streets. That’s because he graduated from the first. “Last fall, when I participated in the ground breaking for the new school, it brought back memories of the old school,” says Levy, who continues to hold the record as the youngest graduate of the medical school going back to its founding in 1846. A loyal supporter of the medical school, Levy is a founding member of the James Platt White Society and a longtime member of the Edmund Hayes Society. He has served as chair of each of his class’s five-year reunions since graduation; to date, the class has contributed more than any other (over $2 million). He has also made available to UB a fund of several hundred thousand dollars, through the Medical Student Aid Society, for interest-free loans to enable students to complete their education. He is a charter member of the President’s Associates Society and a longtime member of the Pillars of UB. A proponent of plans to return the medical school downtown, Levy recently made a gift of $150,000 to support construction of the new school. UB will recognize his generosity by naming the dean’s conference room in his honor. It is fitting that the Levy name be affixed to the UB medical school, as three generations of the family have graduated over the century. Levy’s father, Sidney H. Levy, MD ’19, practiced as one of the first radiologists in Buffalo. Harold’s son, Sanford H. Levy, MD ’86, is an internist and integrative holistic medicine specialist in Buffalo.
Harold Levy taught medical students and psychiatric residents as a volunteer faculty member for 60 years. After serving as the U.S. Army’s chief of psychiatry in Korea and Hawaii from 1948 to 1950, he returned to Buffalo, resumed teaching and completed a research fellowship at Erie County Medical Center. He then established a successful psychiatric practice. Today, at age 90, he continues to see patients.
HAROLD LEVY GIVES BACK TO SUPPORT THE FUTURE
Pho
to b
y D
ou
gla
s Le
vere
Harold J. Levy, MD ’46
U B M E D I C I N E6 S U M M E R 2 0 1 5

Women physicians and biomedical scientists affiliated with UB as faculty or alumnae recently gathered to participate in a conversation about ways to build and sustain a network that will empower female leaders in the field. If you are interested in attending a gathering for the group, contact Jennifer Britton, director of constituent and alumni engagement, at (716) 829-2586 or [email protected].
SCHWAITZBERG NAMED CHAIR OF SURGERY
Steven D. Schwaitzberg, MD, professor of surgery at Harvard Medical School and chief of surgery at the Cambridge Health Alliance, has been named chair of the Department of Surgery, effective June 1. He also will serve as medical director of surgical program development for Kaleida Health and Erie County Medical Center (ECMC). An internationally recognized expert in minimally invasive sur-gery, Schwaitzberg has been with Cambridge Health Alliance since 2005. That same year he became a visiting associate professor at Harvard Medical School and four years later was appointed a full-time faculty member. From 1986 until 2005, Schwaitzberg served as an assistant, then associate professor of surgery at Tufts University School of Medicine. He held several administrative posts at the New England Medical Center—now Tufts Medical Center—including medical director, director of surgical research, and vice chair and executive committee chair of its institutional review board. From 1990 to 1991, he served as surgical team chief and director of intensive care at the 365th Evacuation Hospital within the U.S. Military Complex in Seeb, Oman. Among Schwaitzberg’s most significant research accomplishments is demonstrating the feasibility of using microwaves to warm blood, facilitating transfusions. His work in this area led to the development and federal approval of a practical device. Schwaitzberg’s basic laboratory work on an anti-adhesion device in abdominal surgery progressed to a pivotal clinical trial supporting its use in patients. In addition to device development and preventing
Pho
to b
y Jo
sep
h C
asci
o
intra-abdominal adhesions, Schwaitzberg’s research focuses on skill acquisition in minimally invasive surgery, clinical evalua-tion of antibiotics and clinical outcomes. A past president of the Society of Ameri-can Gastrointestinal Endoscopic Surgeons, Schwaitzberg has authored more than 200 peer-reviewed manuscripts, articles, book chapters, editorials and clinical reviews. He is a fellow of the American College of Sur-geons and serves on its board of governors. He has won numerous awards, including the Laureate Achievement Award and many recognitions for teaching excellence. Schwaitzberg earned his undergraduate degree from Johns Hopkins University and his medical degree from Baylor College of Medicine. He completed surgical residency at the Baylor Affiliated Hospitals and a fellowship at the Pediatric Trauma Institute, Floating Hospital for Children. Schwaitzberg’s appointment brings to 15 the number of new chairs and chair-level appointees that Michael E. Cain, MD, has named since becoming medical school dean in 2006. The hires play a critical role in his strategic plan for the medical school, especially as the new medical school building—which will open in 2017—takes shape on the Buffalo Niagara Medical Campus.
Steven D. Schwaitzberg, MD
WOMEN IN MEDICINE AND SCIENCE NETWORKING RECEPTION
7U B M E D I C I N ES U M M E R 2 0 1 5

U B M E D V I T A L L I N E S
Robert G. Wilmers, chairman and chief executive officer of M&T Bank Corporation and co-chair of the Build the Vision campaign steering committee for the School of Medicine and Biomedical Sciences, was awarded the Chancellor Charles P. Norton Medal—UB’s highest honor—during the 169th annual University Commencement on May 17. The medal is presented annually in public recognition of a person who has, in Norton’s words, “performed some great thing which is identified with Buffalo. . . . a great civic or political act, a great book, a great work of art, a great scientific achievement or any other thing which, in itself, is truly great and ennobling, and which dignifies the performer and Buffalo in the eyes of the world.” As chairman and CEO of the Buffalo-based M&T Bank Corporation and its principal subsidiary, M&T Bank, since 1983, Wilmers has guided M&T from a financial institution with assets of $2 billion to its current holdings exceeding $98 billion.
WILMERS RECEIVES UB’S HIGHEST HONORRecognized for his dedication to the community
Widely regarded as a leader in the U.S. banking industry, he also is greatly admired within the Western New York community for his dedicated civic-mindedness. Deeply involved in the local community, Wilmers has had tremendous impact on numerous vital regional interests, among them the efficiency and effectiveness of health care, the quality of preK-12 education and neighborhood schools, and the viability of the Buffalo Philharmonic Orchestra, regional architectural treasures and the Buffalo Zoo.
Michael E. Cain, MD, vice president for health sciences and dean, School of Medicine and Biomedical Sciences, recently named three faculty to new leadership positions:
ALAN J. LESSE, MD,
associate professor of medicine, pharmacology and toxicology, and microbiology and immunology, has been appointed senior associate dean for medical curriculum. He will continue to serve as vice chair for education in the Department of Medicine and chief of the Infectious Disease Section at the Veterans
Affairs Western New York Healthcare System.
Lesse is a member of the Medical Curriculum Committee and teaches extensively in the school.
MARK R. O’BRIAN, PHD,
professor of biochemistry, has been appointed chair of the Department of Biochemistry, following a national search.
O’Brian is actively involved in the teaching mission of the Department of Biochemistry, and his primary research interest focuses on coordinated control of nutritional stress responses in bacteria. He is a recipient of the UB Exceptional Scholar Award for Sustained Achievement, and an American Society for Microbiology International Professorship.
DANIEL J. MORELLI, MD ’74,
professor of clinical family medicine, has been named chair of the Department of Family Medicine.
Morelli has taught medical students and residents since 1980. He also has served in numerous administrative roles, including vice chair of the department, chief medical officer
(CMO) for Millard Fillmore Hospital, interim CMO for Kaleida Health and CMO for Buffalo General Medical Center until 2011.
To learn more about each of these leaders, visit medicine.buffalo.edu/faculty.html.
THREE FACULTY NAMED TO LEADERSHIP POSITIONS
U B M E D I C I N E8 S U M M E R 2 0 1 5

SPRING CLINICAL DAY AND REUNION WEEKEND 2015
Alumni came from around the country this spring to celebrate with classmates, friends, faculty and students. Over 500 people joined in the festivities, which included an alumni cocktail party, dinners, tours of the Buffalo Niagara Medical Campus, Spring Clinical Day and Medical Residents’ Scholarly Exchange, and presentation of the Distinguished Medical and Biomedical Alumnus awards and Volunteer of the Year Award (see pages 30 and 31). The weekend was sponsored by the UB Medical Alumni Association and the School of Medicine and Biomedical Sciences.
Herbert E. Joyce, MD ’45, left, pictured with Dean Michael E. Cain, MD, was honored for his role as a founding father of family medicine.
Members of the Class of 1990 celebrating 25 years in medicine, from left: Drs. Ngozi Osuagwu, Rohit Bakshi, Richard M. Craig Jr., M. Stella Pierre.
From left: Jack Coyne, MD ’85, Barbara Brar, MD ’85, Shirley V. Galucki, MD ’85, Maritza Alvarado, MD’ 85, Andrew M. Knoll, MD ‘84, JD.
Pho
tos
by
Jose
ph
Cas
cio
From left: Mrs.Sandra Lesser, Laurence Lesser, MD ’70, Julie Lippmann, Michael L. Lippmann, MD ’70, Donald Copley, MD ‘70.
9U B M E D I C I N ES U M M E R 2 0 1 5
BY ELLEN GOLDBAUM
PRIME TIME FOR
STROKE CARE
TECHNIQUE PIONEERED AT UB ISREVOLUTIONIZING TREATMENT
Elad Levy, MD, professor and chair of the Department of Neurosurgery and medical director of stroke services at Kaleida Health’s Gates Vascular Institute—a major UB teaching affiliate—was co-author of the study.
Pho
to b
y Sa
nd
ra K
icm
an
U B M E D I C I N E1 0 S U M M E R 2 0 1 5

Although brain surgeons are not known for mincing words, Levy, then a senior fellow in the UB Department of Neurosurgery, was surprised by the strong responses he received from the audience. “They ridiculed us. They called us cowboys,” recalls Levy, now professor and chair of the Department of Neurosurgery in the UB School of Medicine and Biomedical Sciences and medical director of stroke services at Kaleida Health’s Gates Vascular Institute, a major UB teaching affiliate. “Physicians in attendance got out of their seats to tell us how absurd it was to think that we could use stents for acute stroke. They called it unproven, untested and dangerous.” Levy returned to Buffalo dejected, but his mentor, L. Nelson “Nick” Hopkins III, MD, then chair of the Department of Neurosurgery, wasn’t concerned. “He told me, ‘If they’re not upset, then you’re not onto anything,’” recalls Levy.
THIS IS A GAME CHANGERToday those words resonate, as the standard of care for stroke treatment is about to undergo a revolution due, in large part, to the pioneering work done by the “cowboys” at UB. On April 16, the New England Journal of Medicine (NEJM) published a paper by UB neurosurgeons and colleagues, reporting that stroke patients have a much better chance of surviving and returning to normal function when they receive clot-busting drugs in conjunction with a wire mesh stent device, than when they receive the medications alone. Results from the international SWIFT PRIME trial (Solitaire With the Intention For Thrombectomy as PRIMary Endovascular Treatment), were first reported at the International Stroke Conference in Nashville in February. “This is a game changer,” says Levy, who co-authored the paper with Adnan Siddiqui, MD, PhD, professor and vice chair of neurosurgery at UB and site principal investigator for the trial at Gates Vascular Institute. Jeffrey Saver, MD, of the University of California at Los Angeles, and Mayank Goyal, MD, of the University of Calgary, were first authors. UB neurosurgeons—inspired by how effective stenting is in treating coronary heart disease—developed many of the techniques used in the trial, as well as in other similarly successful trials. In the late 1990s, Hopkins, now a SUNY Distinguished Professor of Neurosurgery, and his colleagues led efforts to
explore minimally invasive approaches to stroke treatments. Taking advantage of the body’s circulation system, they threaded micro-thin devices through an artery in the groin to reach blocked vessels in the brain that they treated with stents. Ischemic strokes, which occur as a result of an obstruction within a blood vessel supplying blood to the brain and which make up 87 percent of all stroke cases, are prime conditions for this type of treatment.
DAWN OF A NEW ERA IN STROKE TREATMENTThe SWIFT PRIME trial was conducted at 36 sites worldwide to determine if patients who experienced an ischemic stroke experienced better outcomes with the intravenous clot-busting drug tPA alone versus tPA in conjunction with the use of a wire mesh stent device called Solitaire, made by Covidien. The trial examined the use of the Solitaire™ FR (Flow Restoration) Revascularization Device within six hours of symptom onset. The device is inserted through a tiny incision in the groin and threaded through the femoral artery by catheter to the vessel in the brain that is blocked. When the mesh device is opened, it captures the clot and pulls it out as the catheter is removed. Normal flow to the brain is restored and damage to the brain due to lack of blood is mitigated. In SWIFT PRIME, tPA was administered to the patient prior to the Solitaire procedure. “The findings were definitive,” Siddiqui says. “When Solitaire is used along with tPA, patients have the best chance for survival and return to normal function.” Some patients treated with tPA plus the wire-mesh stent leave the hospital after just a few days, in stark contrast to what has been the standard of care, where patients spend several days in the intensive care unit, then additional time at a rehabilitation facility. “This restores blood flow to the brain far faster and provides the patient the absolute best chance for a positive outcome,” Levy explains. “In many cases, there’s no need for the ICU and no need for rehabilitation.” “We’re at the dawn of a new era in stroke treatment,” says Hopkins. Right now, that new era is coming only to select hospitals and stroke centers, like the Gates Vascular Institute, explains Levy. “It’s taken a decade of optimization to create here in Buffalo one of the best stroke centers with the best process in the world,” he adds.
Over a decade ago, Elad Levy, MD, spoke at a national meeting for neurosurgeons, describing a radically new procedure being developed at UB for treating strokes that involved the use of stents to physically remove clots from the brain, rather than relying solely on clot-busting drugs.
Pho
to b
y Sa
nd
ra K
icm
an
1 1U B M E D I C I N ES U M M E R 2 0 1 5

A REVOLUTION, START TO FINISHStreamlined workflow procedures in the emergency department have been identified as a key factor in successfully treating stroke patients. While Levy stresses that stroke treatment should not be viewed as just a race against time, he acknowledges that speed is a crucial component to successful outcomes. When emergency medical services in Buffalo respond to a suspected stroke call, they activate the stroke team from the field so its members are waiting in the emergency department when the patient arrives. “We want to be called while the
ambulance is en route to the hospital,” Levy says. “This is unique. We call our team together if it’s even the slightest possibility of a stroke.” Because of that immediate activation, the Gates Vascular Institute/UB team has overcome one of the most tragic reasons for disability and death in stroke. “Why do treatments for stroke fail?” Levy asks. “Because patients sit in the ER. So, here in Buffalo, we don’t let stroke patients sit anywhere. We keep them constantly moving through the ER. We even took MRI out of the equation for initial triage because it was less time efficient.” Siddiqui adds: “CT perfusion along with CT angiography allow us to make critical assessments for clinical decision-making, reserving MRI for patients who
do not need immediate intravenous tPA or mechanical thrombectomy.” The team continually reviews its procedures, searching for ways to further optimize them, identifying and eliminating any potential inefficiencies. SWIFT PRIME’s target was that it should take 70 minutes or less to go from qualifying image—where the occlusion is confirmed—to groin puncture. Of all the study centers in SWIFT PRIME, the Gates Vascular Institute/UB team achieved the fastest pace. The study’s organizers presented the team with a certificate for achieving the fastest groin to recanalization time of all 36 centers. In one case, the Buffalo team accomplished this in just 18 minutes. “Once we review the scan results, the patient is in a procedure lab within an hour,” explains Kenneth Snyder, MD, assistant professor of neurosurgery. “This is remarkably fast and is a direct result of the work-flow efficiency.”
RESEARCH BENEFITS THE COMMUNITYAnother advance the Gates Vascular Institute/UB team helped pioneer is the use of CT perfusion imaging, which allows physicians to visualize where the clot is located and what portion of the brain is not receiving blood. “About 10 or 15 years ago, people thought CT perfusion imaging was of no value and that time was the only major parameter in treating acute stroke,” Levy says. “Now we wouldn’t think of doing a stroke treatment without this kind of imaging.” Robert N. Sawyer Jr., MD, clinical associate professor
“By participating in such trials, we can provide patients with cutting-edge treatments.”—Robert N. Sawyer Jr., MD
Adnan Siddiqui, MD, PhD, professor and vice chair of neurosurgery at UB and principal investigator for the trial at Gates Vascular Institute, was a study co-author.
Pho
to b
y Jo
sep
h C
asci
o
U B M E D I C I N E1 2 S U M M E R 2 0 1 5

in the UB Department of Neurology and chief of stroke services for Kaleida Health, says participation in such landmark trials benefits the community in a major way. “By participating in such trials, we can provide patients with cutting-edge treatments,” he says. Of course, some stroke patients cannot be helped, Levy notes. “Sometimes people still die despite our best efforts. But more patients will die if they’re not treated with retrievable stents. We now have the evidence that proves it.” The next challenge, Levy says, is to work on identifying patients who are waking up from a stroke that may have occurred beyond the crucial six-hour window of time. That timeframe still governs stroke treatment today, but Levy believes that the next step is developing treatments that work even when clinicians can’t pinpoint exactly when the stroke occurred. “Our argument is that we know there are patients who will be able to be successfully treated even if the stroke occurs well beyond that time window. The question is, how to identify them.”
TRANSLATIONAL RESEARCHStent innovations are continuing to come in quick succession. Hopkins points out that the stent used in the SWIFT PRIME study already qualifies as a “Model T.” “We’ll see tremendous advances over the next decade, spurred by compelling data, showing that stenting strokes works,” he says. In fact, at the Jacobs Institute, just upstairs from the Gates Vascular Institute, adjacent to UB’s Clinical and Translational Research Center, startup companies are exploring these innovations.
In addition to vindicating the work that neurosurgeons at UB and Kaleida Health have done on stenting for stroke, these advances in care also demonstrate the value of the collaborative clinical translational research that takes place in the Gates Vascular Institute/UB Clinical and Translational Research Center building. Opened in 2012, the state-of-the art facility was designed to help researchers bridge the gap between basic biomedical discoveries and clinical treatments. The collaborative environment was expected to reduce barriers between academic disciplines and between institutions, resulting in exceptional clinical and translational advances in medicine. “The SWIFT PRIME trial is a big win for this building,” Levy notes. “It proves the value of having UB research upstairs and the operating rooms downstairs. You can take the elevator from research and translation to innovation to the clinical forum.” From his first days as a UB neurosurgery fellow, to his current post as department chair, Levy has seen how his own career has tracked closely the journey that stenting for stroke has taken—from maverick technique to the mainstream. He also has watched how Hopkins’ refusal to let go of an idea that at first few would believe in is now, finally, changing the standard of care. “Twenty-five years ago, my mentor, Dr. Hopkins, was the only one who knew this would work,” says Levy. “It took a quarter of a century to convince the world he was right.”
“It’s taken a decade of optimization to create here in Buffalo one of the best stroke centers with the best process in the world.”—Elad Levy, MD
Pho
to b
y Jo
sep
h C
asci
o
The Solitaire wire-mesh stent device is inserted through a tiny incision in the groin and threaded through the femoral artery by catheter to the vessel in the brain that is blocked.
1 3U B M E D I C I N ES U M M E R 2 0 1 5

New scholarship aims to keep young physicians in Western New York
By Ellen GoldbaumPhotos by Douglas Levere
Alarmed by the steady decline in the number of physicians practicing in
Western New York, local physicians and community leaders have created
a new organization designed to train and keep more doctors in the area.
A long-term plan forPhysician Shortages
The Western New York Medical Scholarship Fund is a new, independent, community organization that provides scholarships to Western New York students to attend the UB School of Medicine and Biomedical Sciences. Students accepted to the school must meet highly select criteria to be eligible for these scholarships. They must have graduated from a high school within the eight counties of Western New York, excel academically and have a demonstrated financial need. In order to accept the scholarship, they also must pledge to stay in Western New York to practice for at least five years after completing their training. Each awardee receives a minimum of $30,000 annually for medical school. Selected in February, the first three recipients are James Miller, a graduate of Frontier High School; Gina Sparacino, a Kenmore East High School graduate; and Alyssa Volmrich, a graduate of Holy Angels Academy.
“Our goal is to keep more locally trained doctors in Western New York,” says John J. Bodkin II, MD ’76, co-chair and founder of the Western New York Medical Scholarship Fund and an alumnus of the UB medical school. “The hospitals and insurers have backed it 100 percent,” he adds. “Everyone realizes this is an issue. For me, personally, it’s my chance to give back to the community.”
Building on Established Family TiesAs a family physician at Highgate Medical Group in Buffalo, Bodkin knows all too well how badly Western New York needs new doctors. “If I have patients who need to see a dermatologist, they may have to wait three to four months,” he says. “Their problem could be acute by then. If a family doctor like myself refers a diabetic patient to an endocrinologist, that’s because the patient is very sick. But it can take months before the
U B M E D I C I N E1 4 S U M M E R 2 0 1 5

endocrinologist can see them.” In 2013, the Healthcare Association of New York State (HANYS) reported that Western New York was experiencing one of the worst doctor shortages in the state. The nonprofit organization found that while the national average for the number of family medicine physicians is about 80 per 100,000 patients, Western New York had only 60 per 100,000. In general surgery, the national average is about eight per 100,000 and Western New York had only five. It’s well known, Bodkin says, that young physicians tend to remain in the same area where they have family and where they completed their medical education or training. “We felt that if we could offer scholarships to Western New York students who went to high school here and have established family ties here, and then offer incentives, such as mentoring by local doctors, we could influence them to stay and practice here after graduation and residency.” Organizations that have contributed a full scholarship
are Catholic Health System, Erie County Medical Center, HealthNow New York, Independent Health, Kaleida Health, Roswell Park Cancer Institute, the Patrick P. Lee Foundation, the John R. Oishei Foundation and West-Herr Automotive
Group, as well as the UB medical school and the UB Medical Alumni Association. Contributors to the fund’s endowment are Amherst Ear Nose and Throat, Great Lakes Medical Imaging, Highgate Medical Group, Nephrology Associates of WNY, Northtowns Cardiology, WNY Urology Associates, Windsong Radiology Group, David M. Zebro and Gerald Sufrin, MD. The fund’s goal is to sustain six to ten scholarships a year over the next decade. “We’re hoping the five-year commitment turns into a forever commitment,” Bodkin says. “Other areas of the country have done this with great success.” Michael E. Cain, MD, vice president for health sciences and dean of the UB medical school, says that the creation of the
“I was awestruck when I heard that I had won a scholarship. Coming from a family of seven children, I cannot begin to describe what this assistance means to me and how grateful I am.”—Gina Sparacino, Class of 2018
A long-term plan for
The first three recipients of the Western New York Medical Scholarship are, from left, Alyssa Volmrich, James Miller and Gina Sparacino. Their scholarships are sponsored by HealthNow, Erie County Medical Center and Kaleida Health, respectively.
Pho
to b
y D
ou
gla
s Le
vere
1 5U B M E D I C I N ES U M M E R 2 0 1 5

scholarship fund was extremely welcome news for health care in Western New York. “John Bodkin and his colleagues have demonstrated extraordinary creativity in responding to what is becoming a significant problem in our region,” he says. “The fund’s founders and the organizations that have stepped up to contribute to the scholarship fund are to be commended. In addition to helping address the region’s physician shortage, it provides some of our top students with an incentive to stay where many would prefer to practice—in the community where they grew up and have strong personal connections.” The UB medical school requires that to be considered for admission, applicants must be a U.S. citizen or a permanent resident of the U.S. The school will not consider or accept for admission applicants who are not U.S. citizens or permanent U.S. residents. Local leaders stress that addressing the physician shortage will require multiple approaches. Cain notes, for example, that the new UB medical school building, the largest such building under construction in the U.S., also will address the shortage because it will educate 40 more physicians each year, raising the class size to 180.
Right in Our Own BackyardRepresentatives from the Western New York Medical Scholarship Fund and the medical school conducted interviews and chose the
first three scholarship recipients, all of whom were in their first year of medical school at UB. Gina Sparacino, a Canisius College graduate, took a year off after graduation to work as a transcriptionist at Excelsior Orthopaedics in Buffalo, where she discovered an interest in medicine. “The doctors took note of my interest,” she says, “and generously allowed me to shadow them in the clinic.” When her grandfather was hospitalized at Roswell Park Cancer Institute, Sparacino’s interest in medicine matured into a calling. “Seeing firsthand what Western New York has to offer, I intuitively understood that high quality medical care exists right in our own backyard, and I wanted to be a part of it,” she says. “As young physicians with strong ties to our families and community, we have a responsibility to make sure that the tradition of excellence continues.” When Sparacino decided to pursue a career in medicine, she applied, with fingers crossed, to UB—her first choice in medical schools—but was wait-listed. Having been accepted to her “distant-second choice” in Pennsylvania, she half-heartedly left Buffalo. Six days into the program, she was offered a place in UB’s class of 2018 and lost no time in packing her bags. “I never looked back. UB was my dream school in my dream city,” she says. “I’m never leaving Buffalo. What’s not to like?
Other people my age may be tempted by wanderlust, but I get homesick very easily whenever I leave, even for a few days. I went to school here, I want to raise my family here and I intend to practice medicine here.” In the most important ways, she says, Buffalo reflects her family values: “a strong work ethic, respect for others, a sense of community and the obligation to give back.” And there would be more good news for Sparacino, who is considering specializing in orthopaedics. “I was awestruck when I heard that I had won a scholarship. Coming from a family of seven children, I cannot begin to describe what this assistance means to me and how grateful I am.” Jim Miller was equally astonished when he heard that he too had been chosen. “I thought it was really exciting,” he says. “I’ve heard of programs like this in other cities and I think it’s great to have something tailored for Western New York.” The son of a medical transcriptionist and a minister with a nursing license, Miller says “Medicine was probably a part of my DNA.” Born in Sacramento, Calif., and raised in Oregon, Miller explains that his family moved around “quite a bit” during his formative years, before permanently relocating to Western New York in 1995. “Buffalo has the same options as any big city,” he says, “but still maintains that special family-oriented, neighborly feel. For me, it has everything. I can’t imagine
“John Bodkin and his colleagues have demonstrated extraordinary creativity in responding to what is becoming a significant problem in our region.”—Dean Michael E. Cain, MD
U B M E D I C I N E1 6 S U M M E R 2 0 1 5

settling anywhere else.” Excelling in science and math in high school, Miller entered and completed the physician’s assistant program at St. John’s University in Pennsylvania. He then went on to work for eight years as a physician’s assistant at Erie County Medical Center with the late Zale Bernstein, MD. “I loved the work and the patient contact,” he says, “but in the back of my mind, I knew I wanted more.” Miller, who is married and has two children, ages one and three, calls his circuitous journey a rewarding one. “I love medical school, and feel like I’ve finally found my path.” He is considering a career in surgical oncology, but is keeping an open mind before committing. “I have a lot more to learn.” Born in Pittsburgh, Alyssa Volmrich moved to North Tonawanda with her mother—a native of Western New York—and younger brother after her parents divorced. Volmrich says she immediately liked the area,“especially the close-knit community feel it has.” A self-proclaimed “science nerd,” Volmrich began her undergraduate career at Duquesne University as a predental student, then switched to premed. Now, she’s interested in pursuing geriatrics, partly as a result
of her family demographics. “I only have one brother, and my mother is an only child, but my grandmother is one of seven children,” she says. “Growing up, I had a lot of contact with great aunts and uncles, so most of my closest relatives are now in their 80s. I feel like the elderly need the special care that they sometimes don’t get.” UB was also Volmrich’s first choice for medical school, and she has not been disappointed. “They delivered on every promise,” she says, “and with the scholarship, I don’t have to worry about school loans and I have greater opportunities.”
A Clear Priority in the CommunityBodkin got the idea to form the fund after discussing scholarships with members of the UB Medical Alumni Association. He then set to work with his co-chair, David M. Zebro, principal of Strategic Investments & Holdings, to generate
community interest and raise funds by reaching out to local physicians, business and health care industry leaders and concerned citizens. “It was clear that creating more scholarships for UB medical students is a priority,” says Bodkin, who explains that the idea especially caught on after the 2013 report from HANYS underscored the severity of the problem in Western New York. In addition to Bodkin and Zebro, members of the fund’s board are Michael O’Mara of O’Mara Financial and Edward J. Rutkowski, former county executive and Buffalo Bill. Two representatives from the UB medical school also serve on the board.
Colleen Karuza contributed to this article.
“Our goal is to keep more locally trained doctors in Western New York. The hospitals and insurers have backed it 100 percent. Everyone realizes this is an issue. —John J. Bodkin II, MD ’76
Members of the Western New York Medical Scholarship Fund board, from left: John J. Bodkin II, MD, David M. Zebro, Edward J. Rutkowski and Michael O’Mara.
Pho
to b
y D
ou
gla
s Le
vere
1 7U B M E D I C I N ES U M M E R 2 0 1 5
Many hands make light work. This ancient proverb goes to the heart of efforts underway to help address the shortage of primary care physicians in our country, a shortage that has been long in the making and, by all accounts, will take time, hard work and ingenuity to amend. A 2013 Health Workforce report by the U.S. Department of Health and Human Services concludes that if the system for delivering primary care were to remain fundamentally the same in 2020, there would be a shortage of about 20,400 primary care physicians nationwide. It goes on to say, however, that if mid-level primary care professionals such as nurse practitioners and physician assistants were fully integrated into health care delivery, the shortage could be alleviated. In particular, the report references the patient-centered medical home as a model of care that implements a team approach to providing care. The patient-centered medical home was first proposed in the late 1960s by the American Academy of Pediatrics and today is supported by the American Academy of Family Physicians and the American College of Physicians, as well as other organizations. “It’s a model that allows physicians to lead a team of health care professionals in providing highly coordinated care for a panel of patients rather than having an individual physician focus on volume of visits,” says John Fudyma, MD ’85, chief of the Division of Internal Medicine and a leading proponent of patient-centered medical homes in our region. “Instead of physicians being paid strictly on a fee-for-service basis, reimbursement in this model is increasingly
tied to quality outcomes data,” he continues. “And given this focus on outcomes data, technology—most especially the electronic health record—figures prominently as a means to help practices better manage their patient populations in terms of quality.” Patient-centered medical homes are most commonly accredited by the National Committee for Quality Assurance (NCQA), a private not-for-profit organization founded in 1990. An NCQA designation is awarded at three levels, with reimbursement from the govern-ment and other payers tied to these levels as well as outcomes data. The arduous work involved in establishing and maintaining viable patient-centered medical homes across our region is an ongoing community effort that involves collaboration between providers, payers, employers, patients and health sciences educators. The University at Buffalo is playing a key role in this and other related initiatives by developing interprofessional education programs that will graduate health care professionals well prepared to practice a team-based approach to care, and by researching ways to improve the functionality of electronic health records. In addition, among the university’s practice plans, collectively known as UBMD, the family medicine, internal medicine and pediatric practices have transitioned to patient-centered medical homes, a step that directly impacts the education and training of tomorrow’s primary care practitioners. First and foremost, the impetus behind the establishment of patient-centered medical homes is to improve the quality of care provided to patients.
The Right Team with the Right Tools
BY S.A. UNGER
PHOTOS BY
DOUGLAS LEVERE
ACADEMIC MEDICINE IS HELPING TO RESHAPE PRIMARY CARE
U B M E D I C I N E1 8 S U M M E R 2 0 1 5
The Right Team with the Right Tools
Paul Wietig, EdD, director of the UB Office of Interprofessional Education.
But evidence is mounting that along the way, improvements in quality of care are having a positive effect on the satisfaction primary care providers are deriving from their work, despite lingering frustrations tied to cumbersome data-gathering requirements and yet-to-be resolved reimbursement issues. It’s all a whole cloth, and it’s intriguing to see the pieces being woven together, often behind the scenes. Despite the formidable challenges they face, those devoted to this initiative across our community feel that progress is being made and that efforts in this direction are helping to gradually transform primary care as we know it today.
AHEAD OF AN LCME MANDATE
The surest indicator that team-based health care is here to stay is the fact that the Liaison Committee for Medical Education (LCME)—the accrediting body for medical schools in the U.S.—mandated in 2014 that four core competencies in interprofessional education be demonstrated as part of the LCME review process. These include (1) values and ethics for interprofessional practice, (2) roles and responsibilities, (3) interprofessional communication and (4) teams and teamwork. In anticipation of this mandate, Michael E. Cain, MD, vice president for health sciences and dean of the School of Medicine and Biomedical Sciences, established the Office of Interprofessional Education (IPE) at UB in February 2013 and named Paul Wietig, EdD, to head it. “Dr. Cain was very responsive and saw this coming,” says Wietig. “Even before the LCME declared its mandate, he said ‘We had better pay attention to this.’” All five of UB’s health sciences schools—medicine, dentistry, nursing, pharmacy and public health and health professions—along with the UB School of Social Work, are taking part in this initiative, which focuses on developing educational and training experiences that break down silos and encourage collaboration among health care professionals. Wietig says that preliminary data obtained from IPE programs nationwide indicate that the team-based approach to care improves patient satisfaction, health outcomes, patient safety and resource utilization and decreases staff turnover and health care costs. “This is early data,” he emphasizes. “But it’s a pretty impressive list.”
THIS IS THE WAY WE WANT TO LEARN
In the two and a half years that he has been in his new role, Wietig also has accumulated a pretty impressive list of accomplishments. He organized the first university-wide pilot class in IPE, whichculminated in a shared training exercise in UB’s state-of-the-art Behling Simulation Center. This center, which Wietig says is “the first simulation center in the country to be truly grounded in IPE,” was established in 2011 with the help of a $3 million gift from Ralph T. Behling, MD ’43. The facility, currently located on the South Campus, will be moving to the new medical school building downtown, where it will be one-third larger than it is today and where it will play a central role in IPE
training and continuing education for the entire Buffalo Niagara Medical Campus. In May 2013, Wietig invited faculty from the University of Toronto’s Centre for Interprofessional Education—acknowledged leaders in IPE—to come to Buffalo, where they provided an intensive orientation for select leaders in the academic, health care and business communities. In 2014, he took part in a medical school retreat led by the late Avery Ellis, MD ‘77, PhD ‘79, senior associate dean for medical curriculum, to explore ways to integrate the fundamental principles of IPE into the medical school’s curriculum. During the retreat, in addition to the four IPE core competencies mandated by the LCME, faculty decided to add a fifth: cultural diversity. Since that time, UB health sciences faculty have worked together to develop five 50-minute modules (four of which are required) that will
“DR. CAIN WAS VERY RESPONSIVE AND SAW THIS COMING. EVEN BEFORE THE LCME DECLARED ITS MANDATE, HE SAID ‘WE HAD BETTER PAY ATTENTION TO THIS.’”
1 9U B M E D I C I N ES U M M E R 2 0 1 5

Nancy Nielsen, PhD, MD ’76, senior associate dean for health policy at UB and a former president of the American Medical Association.
“YOU HAVE TO REMEMBER THAT AS RECENTLY AS 2011, ALMOST NO MEDICARE PHYSICIAN PAYMENTS WERE QUALITY BASED; EVERYTHING WAS VOLUME BASED...”
be posted online and embedded in specific courses. In the medical school, Andrew Symons, MD ’02, has led efforts to integrate these modules into the Clinical Practice of Medicine course (year one), which he directs. “The other health sciences schools are integrating similar modules in courses that are aligned with the topics,” Wietig explains. Currently, Wietig is focusing his efforts on the next step, which he calls “the hard part”—scheduling times when faculty, students and residents from all the health science professions can come together to work and learn in a clinical setting. “When you put all of this content into practice, that’s when the rubber hits the road,” he says. Finding a common time for this to take place, however, is proving so difficult that schools everywhere are exploring ways to change scheduling platforms and are looking for new opportunities to introduce IPE into learning, including restructuring grand rounds to make them more team based.
“It took the University of Toronto ten years to find one day in the year that could be designated as a time for their health sciences faculty to come together to learn and practice,” Wietig explains. Despite these challenges, every indication is that IPE is here to stay and that it is what the students want and expect. “We’re hearing from the students,” Wietig says, “and they are telling us, ‘This is the way we want to learn.’ It makes sense to them. “However, there’s no doubt that IPE represents a change in culture,” he cautions, “and it’s not going to happen overnight. That’s why I emphasize the maxim, ‘Change is a process and not an event.’”
ELECTRONIC HEALTH RECORDS ARE STILL CATCHING UP WITH MANDATES
Not surprisingly, the team-based approach to providing quality care—an endeavor that is highly reliant on the sharing of information—is dependent on the electronic health record (EHR) for its success. This trend continues to gain momentum, as reimburse-ment for the delivery of health care services in our country is increasingly tied to outcomes data that measure quality. In January, U.S. Health and Human Services Secretary Sylvia M. Burwell sent shock waves through the health care industry by announcing that by the end of next year, 30 percent of all traditional Medicare payments to providers will be tied to value or quality payment models, a number that will rise to 50 percent by 2018. “You have to remember that as recently as 2011, almost no Medicare physician payments were quality based; every-thing was volume based, fee for service,” explains Nancy Nielsen, PhD, MD ’76, senior associate dean for health policy at UB and a former president of the American Medical Association (AMA). “What’s really stunning about this announcement,” Nielsen adds, “is that it’s more for hospitals. By the end of 2016, it will be 85 percent value-based payments for them, and by 2019, 90 percent. And just as important as the announcement itself was who stood there on the stage with Secretary Burwell: heads of insurance plans, who have been advocating for this for a long time, and representatives of employer groups, who want to pay for quality, not quantity.” This spring, Congress passed and President Obama signed a bill that repealed Medicare’s sustainable growth rate physician payment system. “This will further accelerate the move away from the fee-for-service payment system by rewarding physicians who’ve moved to alternative payment models,” says Nielsen, who notes that the bill was strongly supported by medical organizations. Yet with this shift, physicians are caught in a dilemma. On the one hand, they understand better than most why capturing data in an EHR is essential to providing quality, population-based health care. On the other hand, they
U B M E D I C I N E2 0 S U M M E R 2 0 1 5

Peter Winkelstein, MD ’90, MBA ’10, executive director of the UB Institute for Healthcare Informatics, chief medical informatics officer for UBMD, and chief medical informatics officer for Kaleida Health, a major UB teaching affiliate.
“WHEN YOU LOOK AT MODELS SUCH AS THE PATIENT-CENTERED MEDICAL HOME, YOU’RE TALKING ABOUT COORDINATION OF TEAM-BASED CARE, AND THAT REALLY IS ALL ABOUT INFORMATION.”
know from experience that the technology behind EHRs is still catching up to the tasks that are being mandated by both government and private payers. Nielsen reports that in 2014 the AMA contracted with the Rand Corp. to survey physicians across the country to get a snapshot of things that frustrated them the most and the things that gave them the most joy in their work. “The results weren’t a big surprise,” she says. “The vast majority said that their number one problem was the electronic health record, and it didn’t matter what system they had. Despite this widespread frustration, however, the study also revealed that physicians don’t want to go back to paper records. They know that the electronic health record has potential value, but it’s very time consuming and there are enormous problems with operability.”
TWO BIG FRONTIERS IN HEALTH DATA
Peter Winkelstein, MD ’90, MBA ’10, is a pediatrician and medical informatics expert who is exploring solutions to the EHR dilemma in collaboration with his peers across our region. Winkelstein wears many hats. He is executive director of the UB Institute for Healthcare Informatics, chief medical informatics officer for UBMD, and chief medical informatics officer for Kaleida Health, UB’s major teaching affiliate. “When you look at models such as the patient-centered medical home, you’re talking about coordination of team-based care, and that really is all about information,” says Winkelstein. “It’s the old adage: ‘You can’t manage what you can’t measure.’ “EHRs are a hard problem. Information doesn’t flow well at all on paper, so we need to collect it digitally,” he explains. “Unfortunately, it doesn’t yet flow as smoothly as we would like electronically. It’s one thing to check a box on an online form, but how does a system process dictated notes or handwritten pieces of paper? This is an imperfect field, but we’re working hard to make it better, and we’re better off than we were a few years ago.” Winkelstein explains that there are “two big frontiers in the EHR world” today: The first is interoperability: How do we get the records to talk to each other so that we can exchange data more readily? And the second is data analytics: How do we use the data that is in the EHRs to improve health? For a couple of reasons, EHRs are now positioned to evolve more rapidly than they have in the past, according to Winkelstein. That’s because the focus for the last five years has been on getting EHRs implemented in practices and hospitals as well as sorting out regulatory guidelines connected to their use. Moving forward, the focus will be on operability. “The implementations are largely done, so we’re past that now,” he explains. “New regulations are still coming down the pipeline, but that is slowing down a bit, so there’s going to be some bandwidth on the development side for vendors to start doing innovative work to improve the products and address
the operability concerns of users.” Data security is another issue that Winkelstein focuses on. “I probably spend more time talking about security—privacy and confidentiality—than any other single issue,” he says. “All of us working on this issue in our community are very conscious of it. The way we look at it is that we are holding this data in trust for the community and for individuals, so it’s incumbent on us to do the best we can to protect it from malicious use. While it’s impossible to be 100 percent secure, we are working very hard to minimize that risk, even though it will never be zero—and that’s true of all data, whether cell phone, financial or other.” The challenge, Winkelstein concludes, it to balance risk with benefit. If EHRs evolve as Winkelstein anticipates they will, then physicians—and the health-care teams they lead—will have a better tool to help them provide the best hands-on care.
2 1U B M E D I C I N ES U M M E R 2 0 1 5

Pamela Reed, MD ’89, brings a lifetime of experience to primary care
When Pamela Reed, MD ’89, describes her path to medicine, she speaks unreservedly of the many blessings in her life.
A PRIVILEGE TO SERVE THE COMMUNITY
By S. A. Un g e r
A mainstay figure in the field of primary care in Buffalo for over two decades, Reed has been a leader in the UBMD internal medicine practice and a highly regarded early advocate of the electronic health record (EHR) as a means to optimally manage entire populations of patients. In 2014, Reed was recruited to serve as chief medical officer (CMO) for the Community Health Center of Buffalo. While she had reservations about leaving academic medicine after 20 years, she saw this new opportunity as a chance to bring a lifetime of skills to bear upon her service to the community.
It Takes a VillageThe desire to serve others, Reed says, is a value instilled by her parents, who raised her and her younger sister in the Village of Greenport on Long Island. Both parents worked at the small hospital in the village—her mother as a nurses aide and her father as an orderly. “My parents dedicated their lives to helping others,” Reed says. “It was a small town, and it’s what people did. They would call on my father to do anything, and it was the same with my mother. We always had a house full of other people’s children.” The village helped Reed, too. When she was in high school, several teachers noticed her talent for science and encouraged her to apply for a summer internship at the Plum Island Animal Disease Center. She was accepted and spent several months working with scientists from a variety of fields, a number of whom were on the faculty at Cornell University. “They said to me, ‘You must go to Cornell,’” recalls Reed. “‘It would be the right place for you. You’re great at science, and you love doing it.’” She took her mentors’ advice, applied to Cornell and was admitted, setting in motion her journey toward medicine. “I loved Cornell,” says Reed, explaining that she lived in a dormitory called Ujamaa “with lots of bright, young African-American students who were very diverse in what they wanted to do and were striving to achieve.”
It was there that Reed met her future husband, Timothy McDaniel, MD ’88, a native of Brooklyn, who was majoring in neurobiology. Over the years the couple forged friendships that would endure. “We had a core group of students who attended classes and studied together, tutoring one another,” Reed recalls. “It was our network and our social support.” Reed worked the entire time she was at Cornell, including summers. When she went home for winter breaks, her village found ways to support her education. “Greenport is a really small town, so any accomplishment made its way into the newspaper. And when I went home, people would stop me and congratulate me, and they made sure I had small jobs to do over the break.” Reed thrived as a biology major and was soon drawn to medicine. “I’m a huge people person,” she says with a laugh. “Medicine was the best of both worlds for me, combining science and my love of people.” During Reed’s senior year at Cornell, she and McDaniel—then a first-year student in the School of Medicine and Biomedical Sciences—became engaged. Reed was accepted to UB medical school the following year, when the couple married.
A Leader in the Migration to EHRsAfter graduation, Reed and McDaniel completed residencies in internal medicine and pursued careers in primary care, deciding to stay in Buffalo and call it home. Reed joined the Department of Medicine and went into practice with John Fudyma, MD ’85, now chief of the Division of Internal Medicine. The university’s practice plans, collectively known as UBMD, had not yet been established, so the model was that of a private practice, Reed explains. She also taught at Erie County Medical Center, where she directed the internal medicine residency outpatient clinic. Later, when the clinic moved to the Dent Tower, Reed was tapped to direct the primary care portion of the practice and lead its migration from the paper record to the EHR.
U B M E D I C I N E2 2 S U M M E R 2 0 1 5

She went to Chicago to receive training and became “the physician champion” for implementing EHRs for the entire UBMD internal medicine practice when all the faculty, including subspecialists, moved to one location and began a concerted effort to increase interreferrals. Reed also led efforts to transition the UBMD internal medicine practice to a National Committee for Quality Assurance (NCQA)-certified patient-centered medical home model. When UBMD launched an initiative to bring all of its practices onto EHRs, Reed served on the committee formed to choose a system, later helping UBMD’s internal medicine practice to become the first to adopt it. In addition to these administrative tasks, Reed derived great satisfaction from teaching and mentoring students and residents in her practice. She says that being a mother of two girls—Maya, 19, a math major at the University of Pittsburgh, and Morgan, 17, a senior at City Honors—has made her especially sensitive to the needs of young minority women. While she sees that her own daughters “have this phenomenal confidence,” she also knows that this is something that needs to be fostered. “So few girls get that,” she observes, “even the very capable.”
Better with Every Passing YearToday, Reed is acclimating to her new role as CMO of the Community Health Center, partnering with its CEO and executive director, LaVonne Ansari, PhD, and the staff to ensure that all patients have affordable access to quality care.
She continues to be a strong proponent of population health management and emphasizes that “data is key to our being able to that.” She also knows it’s imperative to take into account the social determinants of health: “How can I counsel my patients to eat vegetables if they have limited transportation options and there is not a single grocery store within a five-mile radius of their home?” she asks. Reed is excited to report that the health center recently received a grant to house a farmers market at its new site in Niagara Falls to help address what she calls “a total food desert” in the area. Tackling complex problems clearly energizes Reed, who emphasizes again and again that it is a privilege, and blessing, to work as a primary care physician—a job that for her gets better with every passing year. “It’s so wonderful to be here in this position at this time in my career, when I can put the skills I have accumulated into service for the community,” she says. “It’s good for my heart.”
“I’m a huge people person. Medicine was the best of both worlds for me, combining science and my love of people.”
—Pamela Reed, MD ’89
A PRIVILEGE TO SERVE THE COMMUNITY
Pho
to b
y D
ou
gla
s Le
vere
Pamela Reed, MD ’89, a leader in primary care in Buffalo.
2 3U B M E D I C I N ES U M M E R 2 0 1 5
Wasting no time, she headed to her obstetrician, Shalom Press, MD, who confirmed she was leaking amniotic fluid and admitted her to Kaleida Health’s Women and Children’s Hospital of Buffalo, a UB teaching affiliate. “Everything was happening so quickly, and I was in a state of panic,” recalls Ann, who was not at risk for a preterm baby. Four years earlier, she and her husband, Walter, a physical therapist, had welcomed into the world their daughter, Sarah, who had been born full-term and free of complications. “The goal was to keep the baby inside me as long as possible,” explains Ann, who was told that once the amniotic fluid—vital to a baby’s lung growth and development—was depleted, it would be time to schedule a C-section. Complicating the situation was the fact that her husband and daughter were several states away, en route to South Carolina to visit family. “I knew that I might have to make some important decisions on my own,” she says. And so began the Brown family’s immersion in the intricately complex world of perinatal-neonatal care. Walter likes to say, in retrospect, that the “stars were aligned” for their then-unborn child, and indeed those constellations strategically fell into place on Day One of Ann’s hospitalization, beginning with the urgent mobilization of a critical mass of experts, including obstetrician Press and his practice partners, Kenneth Kahn, MD, and Murray Yost Jr., MD ’66. “Team Baby Brown”—with Corinne Leach, MD, PhD, as
attending physician—would do its best to anticipate, treat or prevent every conceivable health challenge that Ann and Walter’s baby might face. Owing largely to “the accelerated opportunities, pioneering discoveries and intellectual rigor of the academic health center behind his care,” Baby Brown would be in good hands, says Leach, a UB associate professor of pediatrics, who today directs the Quality Assurance Neonatal Intensive Care Unit (NICU) at Women and Children’s Hospital of Buffalo.
LIFESAVING SURFACTANT THERAPY DEVELOPED AT UBChief among Baby Brown’s health hurdles would be respiratory distress syndrome (RDS), which causes breathing difficulties due to an absence of surfactant, a naturally occurring material produced in the lungs primarily during the last month of gestation. At the time of his birth, a groundbreaking clinical trial was underway at Women and Children’s Hospital of Buffalo to study synthetic and natural forms of surfactant, given after birth, for their ability to restore the insufficient amount produced by the immature lungs of preterm babies. “From the get-go, I was asked to participate in a randomized clinical trial that compared two forms of surfactant,” says Ann. With her husband on the road, Ann, who had never heard of surfactant, sought trusted guidance from her family pediatrician, William Hartrich, MD. “He told me pointblank:
The clinical trials and extraordinary care that saved Baby Brown
A STUDY IN SURVIVAL
une 5, 1991. It was business as usual for Ann Brown, who, as on most
workdays, could be found behind her desk in the Communications Office at Erie
Community College. A tiny trickle of water, almost impalpable, ran down her
leg. Call it prescience or maternal instinct, but Ann, 25 weeks pregnant with her
second child, knew something was wrong.
JBy Co l l e e n KA r U z A
Ph o t o S B y Do U g l A S le v e r e
U B M E D I C I N E2 4 S U M M E R 2 0 1 5

‘Surfactant will save your child’s life.’ He said that it didn’t matter which form we received; surfactant would give my child a fighting chance.” Prior to the introduction of surfactant replacement therapy, about 70 percent of preterm babies with RDS died. Today, that percentage is less than 5 percent. “We call research that seamlessly transitions from laboratory bench to bedside ‘translational,’ and surfactant replacement therapy is an outstanding example of what that means and how it benefits patients,” says Teresa Quattrin, MD, A. Conger Goodyear Professor and chair of pediatrics at UB, and pediatrician-in-chief at Women and Children’s Hospital of Buffalo. “The ‘era of surfactant’ was ushered in by an international medical research effort led by extraordinary visionaries, with UB faculty at the forefront,” says Quattrin. In the 1960s and 1970s, Swedish physiologist and obstetrician Goran Enhorning, MD, PhD, conducted pioneering studies that overturned conventional wisdom and helped convince doctors worldwide that surfactant-replacement therapy was a valid treatment for premature
infants with RDS. In 1986, Enhorning came to UB, where he joined pediatrics professors Edmund “Ted” Egan II, MD, and Bruce Holm, PhD, in an international race to develop an exogenous surfactant therapy. Their research resulted in two patents and led to the launch and eventual commercialization of Infasurf, which significantly helped decrease the mortality rate for preterm babies. The value of surfactant therapy—and UB’s historical role in its development and advancement—cannot be overstated, contends
Leach, who was recruited by Egan to the faculty of Women and Children’s Hospital of Buffalo in 1988. “I had just left Children’s Hospital of Philadelphia, one of the top university-affiliated pediatric hospitals in the world. I was astounded to find that very premature babies born with RDS, who were dying just a six-hour drive away, were surviving and thriving here in Buffalo. That’s how dramatic a difference this research made.” In 1991, when Baby Brown was born, surfactant was not available anywhere outside the Women and Children’s Hospital of Buffalo clinical trials, Leach says.
“He told me pointblank: ‘Surfactant will save your child’s life.’ He said that it didn’t matter which form we received; surfactant would give my child a fighting chance.”—Ann Brown
The Brown Family, from left: Ann, Ben, Sarah and Walter.
Pho
to b
y D
ou
gla
s Le
vere
2 5U B M E D I C I N ES U M M E R 2 0 1 5
CLINICAL TRIAL TO STUDY POTENTIAL BLINDNESSBaby Brown was also at risk for retinopathy of prematurity (ROP), a potentially blinding eye disorder. About half of babies with a birth weight of under 2¾ pounds will develop ROP, with about 90 percent having the mildest form, which leaves no permanent damage, accord-ing to pediatric ophthalmologist James D. Reynolds, MD, professor and chair of ophthalmology at UB and director of its Ross Eye Institute. At its most severe and left untreated, ROP will cause blindness in approximately 400-600 infants a year. Even after 23 years, Ann still recalls the day Reynolds came to see her in the hospital about a pilot study designed to determine the effect of ambient light reduction on ROP incidence. “Beginning in the late 1980s, there was a lot of debate
about the amount of lighting in nurseries,” says Reynolds, who was the study’s principal investigator. “I had hoped to put to rest some of these concerns.” The Browns agreed to the study. “It just seemed logical,” says Ann. “At the time, most nurses and parents believed that the bright lights in the NICU could damage a baby’s eyes. We felt that the alternative to not participating would be to needlessly risk our child’s eyesight.” Participation meant that babies would wear goggles, specially designed by Reynolds, to filter out 100 percent of UV light and 97 percent of visual light.
BABY STEPS ON THE LONG ROADEnrolled in two clinical studies even before he was born, Baby Brown made his entrance into the world on June 15—one and one-half weeks after Ann was admitted to Women
Pho
to b
y D
ou
gla
s Le
vere
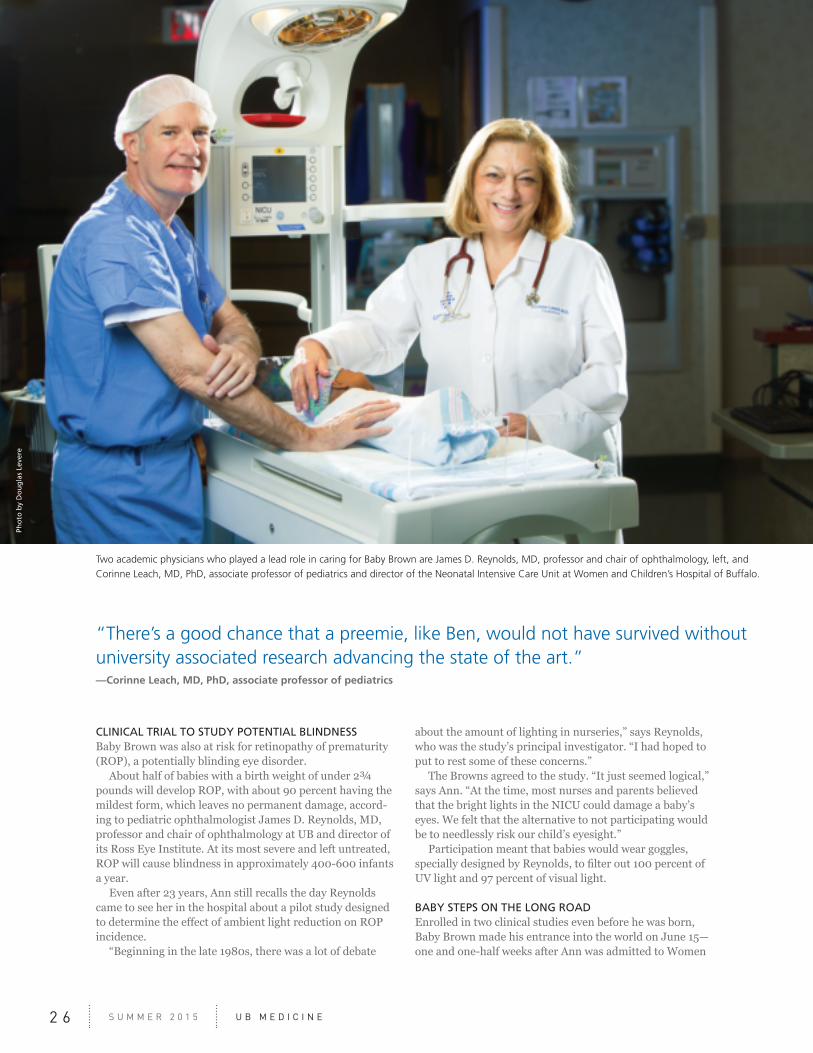
“There’s a good chance that a preemie, like Ben, would not have survived without university associated research advancing the state of the art.”—Corinne Leach, MD, PhD, associate professor of pediatrics
Two academic physicians who played a lead role in caring for Baby Brown are James D. Reynolds, MD, professor and chair of ophthalmology, left, and Corinne Leach, MD, PhD, associate professor of pediatrics and director of the Neonatal Intensive Care Unit at Women and Children’s Hospital of Buffalo.
U B M E D I C I N E2 6 S U M M E R 2 0 1 5
and Children’s Hospital of Buffalo and 12 weeks before her actual due date. Ann and Walter named their son Benjamin. He weighed 2.6 pounds. “When the nurse handed Ben to me for the first time,” says Walter, “she said that his first challenge would most likely be urological. Seconds later, he peed. I had to smile because even the smallest victories bring a parent relief.” Ben was transferred to the NICU, which today is a 64-bed unit that admits more than 740 babies annually. It has an average daily census of 52 and a baby-to-nurse ratio of 2:1. Ben was assigned to Karen Middler, RN, who stayed at his side from birth through discharge. For the Browns, Middler was a godsend. “It was important for us to have one person there to act as our advocate, liaison, support and go-to resource for information,” says Ann. Continuing his surfactant therapy in the NICU, Ben was also fitted with tiny blue goggles held together by Velcro, and, later, an investigational mouth guard to thwart the malformation of his palate due to intubation. “There were tests, and more tests,” says Walter. “It became an arduous waiting game.”
RETURN TO NEAR NORMALCYBen, attached to a heart monitor, was released from Women and Children’s Hospital of Buffalo on September 4, two days before Ann’s original due date. “It was a red-letter day for us, but it would be awhile before Ben was out of the woods,” says Ann. “We basically took him home and plugged him in.” Before leaving the hospital, the Browns were given CPR training, a virtual tome of special instructions and a list of essential emergency contacts. Ann was determined to make life as near normal as possible for Ben. “We had a block party that week and I placed him in his stroller, hid the wires and introduced him to our neighbors.” For the first two years of his life, Ben was under the watchful care of specialists at the Robert Warner, MD Center for Children with Special Needs, part of UB’s Division of Developmental Pediatrics and Rehabilitation, which provides comprehensive diagnostic, evaluative and therapeutic services to children in Western New York. Still, uncertainty and concern shadowed the family for years. “For me, the anxiety subsided when Ben was about 8,” says Walter. “As a physical therapist, I knew the road ahead would not be easy. When we brought Ben home, he
occasionally had full-body rigidity and spasms. Because we had a sense that there could be neurological problems and delays in the development of his motor skills, we got him involved in karate and competitive swimming to give him every advantage.” Today, the Browns breathe a collective sigh of gratitude and relief. Grown up, Ben is a robust 23-year-old college student and an avid outdoorsman who loves to read and has a passion for human ecology and urban planning. “There has not been a single residual effect from his early care,” says Ann, who joined the staff at UB five years ago as senior director of donor and alumni communications.
ACADEMIC MEDICINE MAKE A DIFFERENCEReynolds says it all boils down to the people behind the care. “UB populates its affiliated hospitals with faculty who value excellence and innovation and who help instill into patient care a commitment to quality.
“The clinical studies that academic medicine generates can make the difference between leading a normal or near-normal life, or leading a life of impairment,” he adds. “Future cures and break-throughs depend on carefully controlled randomized clinical trials, which, unfortunately, many patients decline.” Not the Browns. “We saw them as precious opportunities for our child to survive and thrive,” maintains Walter.
“There is a good chance that a preemie, like Ben, would not have survived without university associated research advancing the state of the art,” says Leach, whose own research in liquid ventilation further improved lung function in preterm babies.
ONE OF THEIR OWNOn Ben’s twelfth birthday, Ann took her son back to the NICU. “It was about 8 p.m., but the staff could not have been more warm or welcoming. As Ben looked through the glass at tiny babies in incubators, one resident kept gently punching his arm, saying, ‘That was you in 1991, Ben, and look at you now!’ “Ben was one of theirs, one of their many success stories,” says Ann. “But more than that, even after all that time, they were still there for us.”
Goggles worn by Baby Brown in the clinical trial.
“The ‘era of surfactant’ was ushered in by an international medical research effort led by extraordinary visionaries, with UB faculty at the forefront.” —Teresa Quattrin, MD, A. Conger Goodyear Professor and chair of pediatrics
2 7U B M E D I C I N ES U M M E R 2 0 1 5
U B M E D C O L L A B O R A T I O N S
A new support fund is helping a UB professor to further her research on severe, life-threatening muscle disorders that can be triggered by statin use, among other things. The Paul J. Rich Jr. and Doris Miller Rich Research Fund was established by Judith Rich Lauder to honor the memory of her parents, both University at Buffalo alumni (class of 1933). It supports pioneering research being conducted by longtime UB faculty member Georgirene Vladutiu, PhD, director of the Robert Guthrie Biochemical and Molecular Genetics Laboratory and professor of pediatrics, neurology, and pathology and anatomical sciences.
A Problem that Looms LargeWhile statins are one of several potential triggers of severe myopathies with rhabdomyolysis, the potential impact of statin-induced problems looms large because 40 million Americans take the cholesterol-lowering drugs. Ninety percent of statin users are unaffected, according to Vladutiu, but the remaining 10 percent experience muscle pain or muscle weakness (or both), which usually can be managed by lowering the dose, switching to another statin, or taking a drug holiday. The most at-risk group—approximately 0.5 percent of statin users, or up to 200,000 people in the U.S.—have a suspected genetic predisposition to develop
a very severe illness in response to taking the medication. “In severe statin-induced myopathy, patients have incapacitating muscle pain or muscle weakness or both,” Vladutiu says. “And the symptoms can be persistent. If you take the patient off the drug, many don’t get better.” Statins at higher doses are particularly troublesome. A patient might tolerate low doses (10-20 mg/day) just fine, but if their cholesterol level is still high, their doctor is likely to raise the dose. “At 40 mg/day, a patient may get all the muscle symptoms,” Vladutiu says. “They take a six-week drug holiday, then start back on a lower dose of the drug. Now, many can no longer tolerate the 10 or 20 mg/day dose.” The U.S. Food and Drug Administration has issued warnings about using the high-est doses of certain statins.
Expanding to a National-Level ServiceVladutiu has pursued the problem of triggered myopathies for 30 years. In 1984, she became director of the Guthrie
Laboratory, which was then housed at Women and Children’s Hospital of Buffalo and focused on inborn errors of metabolism. (The laboratory, which performs more than 5,000 specialized diagnostic tests every year, is now housed in Buffalo General Medical Center.) Soon after becoming director of the laboratory, Vladutiu was asked by UB professor of pathology and anatomical sciences Reid Heffner, MD, to expand the laboratory’s offerings to include mitochondrial problems and muscle diseases. She subsequently researched and established new protocols in the lab and began advertising the new services beyond Buffalo. “We started to get samples from around the country, and we became a national-level service,” Vladutiu says. “For many years, we were the largest clinical laboratory in the country dealing with metabolic muscle diseases.” Today, there are competitors vying for the title of largest; yet, UB has held on to its prominence, notes Teresa Quattrin, MD, A. Conger Goodyear Professor and chair of the Department of Pediatrics. “The Guthrie Laboratory is nationally recognized, not only for its specialization in inborn errors of metabolism, but also for its work with metabolic myopathies,” she says.
Identifying Genetic Profiles for PredispositionTriggerable muscle disease has been a concern for many, including the U.S. Armed Services. Known triggers include exertion, dehydration, sleep deprivation, viral infections and certain drugs. The predisposition to these myopathies is inherited, but it requires a trigger to emerge. In the late 1990s, the lab started getting many muscle biopsies from patients in the 40- to 60-year-old age group. “We were
GENETIC RESEARCH WITH PUBLIC HEALTH IMPLICATIONSBuffalo family supports investigations into statin-induced muscle disorder
By Ji l l U AD A m S
“Dr. Vladutiu has always understood the clinical component and has worked in tandem with clinicians.”— Teresa Quattrin, MD, A. Conger Goodyear Professor
and chair of pediatrics
U B M E D I C I N E2 8 S U M M E R 2 0 1 5

Pho
to b
y D
ou
gla
s Le
vere
seeing more and more muscle disease, but we weren’t sure of the trigger,” Vladutiu says. “While the disorders are relatively rare,” she adds, “an advantage of running a national lab is that we can pull out a rare occurrence.” Since then, Vladutiu and her collaborators, notably Paul Isackson, PhD, research associate professor of pediatrics, have been doing the painstaking work of trying to identify genetic profiles for the predisposition to triggerable myopathies. A five-year $2 million grant from the National Institutes of Health helped Vladutiu and Isackson study a broad range of genetic variations, from rare pathogenic variants to common variants, and determine how closely linked these signatures are to statin-induced myopathy. Using high-tech microarray chip technology, they investigated 12 muscle disease genes with 350 potentially pathogenic variants. It turned out that 17 percent of people with severe statin-induced muscle disease
had a pathogenic variant in at least one of the genes studied. Only 4 percent of control subjects had similar genetic profiles. The findings were a great start, but they also demonstrated the need for more research. “We knew we had to expand this—to look at more genes,” Vladutiu says. The researchers moved on to whole exome sequencing: the entire coding regions of people’s genomes were analyzed, rather than only a subset of suspect genes. “The cost of sequencing is relatively inexpensive today, but the data analysis afterwards? That’s a monster,” says Vladutiu, who collaborates with biostatisticians.
New Fund Supports Work to Validate TargetsVladutiu and Isackson have categorized their gene variants into five classes. Class 1 variants are so common that they’re not useful in discriminating susceptibility. Class 4 and 5 variants are the ones that matter.
Georgirene Vladutiu, PhD
Class 5 variants have some other evidence to implicate them in myopathies—either in clinical or animal studies. The class of variants that Vladutiu’s team is pursuing is class 4, which includes “probably pathogenic” and possibly never described before. “Paul Isackson has characterized patterns of variants in over 50 muscle disease genes in detail,” Vladutiu says. “Now we must validate those targets, and we’re grateful to have the Rich Fund for that work.” Nobody doubts Vladutiu’s smarts or resolve. “She never quits thinking of ways to creatively approach clinical and basic science,” Quattrin says. “Further, Dr. Vladutiu has always understood the clinical component and has worked in tandem with clinicians.” The long-term goal is to develop a screening test for susceptibility to statin-induced myopathy. “The statins are so widely distributed,” Quattrin says, “that Dr. Vladutiu’s contri-bution is really at the public health level.”
2 9U B M E D I C I N ES U M M E R 2 0 1 5

Prior to beginning his career in industry, Mertz was a postdoctoral fellow at the National Institutes of Health, where he conducted research on cell signal transduction and cell membrane receptor cloning, sequencing and expression.
D I S T I N G U I S H E D M E D I C A L A N D B I O M E D I C A L A L U M N U S A W A R D S
Dean Michael E. Cain, MD, and Lawrence Mertz, PhD ’89
PH
OT
OS
BY
JO
SE
PH
CA
SC
IO
Jeffrey S. Ross, MD ’75, and Lawrence Mertz, PhD ’89, are recipients of the 2015
Distinguished Medical and Biomedical Alumnus Awards for the School of Medicine
and Biomedical Sciences. They were honored at a dinner held on May 29 at Asbury
Hall in downtown Buffalo.
The event, sponsored by the UB Medical Alumni Association in conjunction with
the school, was attended by family and friends of the awardees, as well as alumni,
faculty and students.
DISTINGUISHED MEDICAL ALUMNUS
Jeffrey S. Ross, MD ’75, is the Cyrus Strong Merrill Professor and Chair of Pathology and Laboratory Medicine at Albany Medical Center and pathologist-in-chief at the Albany Medical Center Hospital, positions he has held since 1989.
Prior to that, Ross served as professor and assistant dean at the University of Massachusetts Medical School and research assistant professor at Harvard Medical School and the Massachusetts General Hospital.
An expert in genetic profiling, especially as it pertains to cancer, Ross has received numerous academic awards, holds four patents in molecular diagnostics and is the author of more than 810 peer-reviewed scientific articles and abstracts, four textbooks and numerous book chapters.
He has been a member of the NIH Clinical Oncology Study Section and serves on the editorial boards for numerous scientific journals. In 2004, Ross co-founded SYFR Inc., a specimen management and autostainer company.
DISTINGUISHED BIOMEDICAL ALUMNUS
Lawrence Mertz, PhD ’89 (biochemistry), is vice president of research and development for molecular diagnostics at Becton Dickinson, a Fortune 500 company. In this role, he supervises a staff of more than 130 scientists in facilities at Hunt Valley, Md., Raleigh, N.C., and Quebec City, Quebec, Canada.
Mertz is responsible for molecular in vitro diagnostic assay development for all molecular, oncologic and women’s health platforms. These assays include testing for infectious organisms and viruses that cause hospital-acquired infection, such as MRSA, as well as HPV, sexually transmitted, respiratory and enteric-based infections. He has a diverse range of experience, having been classically trained in biochemistry and molecular biology and has successfully developed products for the research life science, pharmaceutical/genomics and diagnostics markets for more than 25 years.
Jeffrey S. Ross, MD ’75, and Thomas J. Guttuso Sr., MD ‘60, president of the Medical Alumni Association.
U B M E D P A T H W A Y S
U B M E D I C I N E3 0 S U M M E R 2 0 1 5
CHARLES D. BAUER, MD ’46, —Cardiologist, internist and philanthropist
Charles D. Bauer, MD ’46, a cardiologist and internist who cared for patients in Kenmore and Amherst for more than 40 years, while providing physical and financial support to the next generations of physicians through his contributions to the School of Medicine and Biomedical Sciences, died on March 4 in Spring Hill, Fla. He was 91.
Bauer believed in the traditional role of the physician while also adapting to the changing dynamics of health care. He was the first medical director of Community Blue, holding the post from 1985-90, and he made his first donation to the UB Medical School in 1953, a gift of $45.
The UB Alumni Association presented Bauer its prestigious Samuel P. Capen Award in 2014 in recognition of his commitment to the university, where he and his wife, Mary, helped endow faculty positions, scholarships and other programs in the School of Medicine and Biomedical Sciences.
The Bauers established the Charles D. and Mary A. Bauer Foundation in
1998 and immediately began distributing aid to other local charities as well as the university.
Most recently, the foundation provided a $1 million gift to fund a clinical research nurse manager position at the new UB Clinical Research Center.
Bauer was born in Buffalo and was a lifelong resident, attending St. James Catholic Elementary School, Kensington High School and UB, where he received his medical degree in 1946.
He was on the boards of the Erie County Medical Society and the Western New York Society of Internal Medicine, serving as president of both groups, and was a delegate to the New York State Society of Internal Medicine. He was a member of the UB Dean’s Advisory Council from 1998 to 2006 and was a fellow of the American College of Physicians.
Bauer is survived by his wife of 66 years, Mary; two daughters, Christine Bakewell and Sandra Moe; three sons, C. Donald, Robert J. and Gregory M.; one brother, Alvin; and 15 grandchildren.
I N M E M O R I A M
VOLUNTEER OF THE YEAR
John J. Bodkin II, MD ’76, a family physician with Highgate Medical Group and chair of the Western New York Medical Scholarship Fund, is the recipient of the School of Medicine and Biomedical Sciences’ inaugural Volunteer of the Year Award.
A past president of the Medical Alumni Association, Bodkin was instrumental in galvanizing efforts to establish the Western New York Medical Scholarship Fund in collaboration with a network of community partners. Earlier this year, three UB medical students from Western New York were named the first recipients of the scholarship, the goal of which is to keep young physicians in our region for at least five years after they complete their medical education and training at UB (see related article on page 14).
Over the course of his career, Bodkin has served the medical school in a wide range of capacities: as a member of the Dean’s Advisory Council, chair of the Buffalo Physician editorial board, editorial advisor for UB Medicine magazine, and member of the board of directors of the Medical Alumni Association.
CALKINS RECEIVES NATIONAL AWARD, FEATURED IN FILM
Bethany Calkins, MS, MD ’07, a staff physician with The Center for Hospice and Palliative Care, has been named an inspirational leader in hospice and palliative medicine under the age of 40 by the American Academy of Hospice and Palliative Medicine (AAHPM).
AAHPM asked its 5,000 members to nominate individuals who are the young leaders in the field. Calkins is one of these physicians recognized by her peers for innovation in and dedication to the medical specialty of Hospice and Palliative Medicine and AAHPM.
In addition, Consumer Reports magazine featured Calkins in a video titled “A Beautiful Death—Paul’s Choice,” which it produced in con-junction with its December 2014 print edition. The video was a 2015 National Magazine Award finalist in the multimedia category, which honors digital storytelling and the integration of magazine media.
To view the 18-minute video, go to http://web.consumerreports.org/endoflife.htm.
Calkins earned a medical degree from UB in 2007 and has worked with The Center for Hospice and Palliative Care since 2012.
3 1U B M E D I C I N ES U M M E R 2 0 1 5
U B M E D Q & A
Gale R. Burstein, MD ’90, MPH, has been Erie County Commissioner of Health since 2012. She also serves as clinical professor of pediatrics in the School of Medicine and Biomedical Sciences and research professor in the School of Public Health and Health Professions. Her clinical and research interests focus on adolescent sexual health care services. UB Medicine asked Burstein about her efforts to improve the health of our county’s population, especially in regard to access to primary care.
Q: What is your top priority as county health commissioner?A: Our priority has been to expand, rebuild and open up access to primary care and family planning services throughout the county.
Q: What new access to primary care have you developed? A: We have worked with community partners to reopen our clinic at 1500 Broadway, now called the Erie County Health Mall. Catholic Health System offers primary care and ob/gyn services, including prenatal care. That area of the city had one the highest proportions of pregnant women who did not receive prenatal care. We’ve also worked with the UB School of Dental Medicine to establish a dental clinic there. And we have two mental health care clinics at that location: Lakeshore Behavioral Health for adults, and Mid-Erie Counseling and Treatment Services for children and adolescents.
Q: What measures have been taken to expand family planning services?A: With New York State Department of Health funds to expand family planning services in Erie County, our health department opened a family planning clinic in the Jesse Nash Health Center, and we’ve provided funding for similar services at the Community Health Center of Buffalo (see related article on page 22) and at two Neighborhood Health Center clinics. We are also helping Planned Parenthood expand its adolescent patient services. We have excellent partners in our community.
Q: How have you worked to increase access to sexual health services for adolescents?A: When I was on staff at Women and Children’s Hospital of Buffalo, I researched ways to routinely integrate sexual health care services into primary care in the community, and I helped providers plan ways to change their systems to make it easier for them to offer these services confidentially. I’m still working on that project, as well as looking for ways to bring these services to areas where they are needed but do not exist.
Q: What are some of your most pressing current challenges and initiatives?A: While we have made progress, we continue to have high rates of sexually transmitted infection and teen pregnancy. This year we’re improving the screening rates for chlamydia, the number one
cause of preventable infertility in sexually active women under the age of 25. We also have a huge problem with opioid abuse. This year, we’ve begun to train first responders and community residents to recognize opioid overdose and to deliver naloxone, an opioid antidote. We know we’ve been saving lives this way. We are also working with women’s health and pediatric offices to assist their patients in successful breast feeding through certified lactation counselors. Breast feeding is healthy for the baby and also for the mom. Working together with our community partners, we can strengthen the programs and complement each other.
—Jim Bisco
“That area of the city had one of the highest proportions of pregnant women who did not receive prenatal care.”—Gale R. Burstein, MD ’90, MPH
Building a completely new medical school is a once-in-a-lifetime opportunity. Seize this chanceto revolutionize medical education, health care and research in Western New York.
Become a partner at this pivotal moment in UB’s history. There are many ways to support your new medical school today or in the future. Opportunities include:
Medical School Building Fund t Circle of Leaders t Circle of Visionaries
Please contact Kim Venti for more information. 716-829-2773 | [email protected] | www.giving.buffalo.edu/ubmedicine
THE NEW UB SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCES ON THE BUFFALO NIAGARA MEDICAL CAMPUS
Count us in.
21st-century education, treatment and discovery
Thank you Class of 1960, the first UB medical school class to name a space—student study suites—in the new medical school.
Members of the Class of 1960 who gathered for their 55th class reunion. *Not pictured Joseph A. Chazan, MD.
IMPROVING ACCESS TO PRIMARY CARE THROUGH COMMUNITY PARTNERSHIPS
Burstein
U B M E D I C I N E3 2 S U M M E R 2 0 1 5
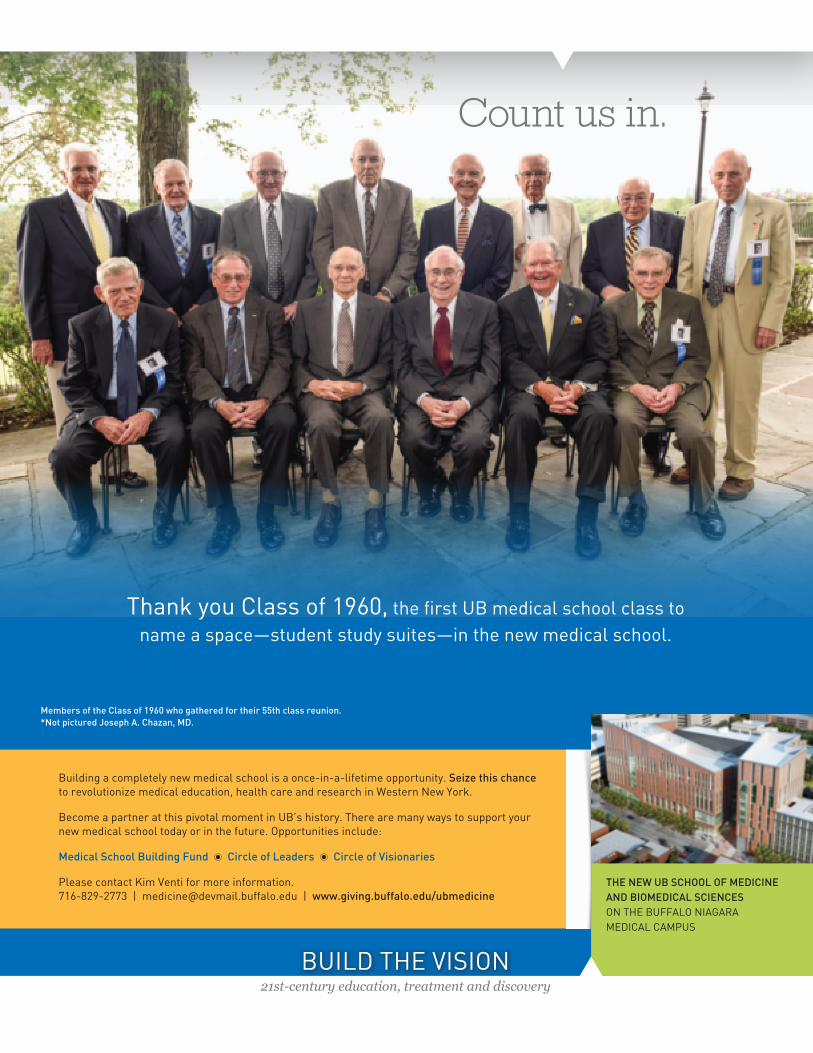
Building a completely new medical school is a once-in-a-lifetime opportunity. Seize this chance to revolutionize medical education, health care and research in Western New York.
Become a partner at this pivotal moment in UB’s history. There are many ways to support your new medical school today or in the future. Opportunities include:
Medical School Building Fund t Circle of Leaders t Circle of Visionaries
Please contact Kim Venti for more information. 716-829-2773 | [email protected] | www.giving.buffalo.edu/ubmedicine
THE NEW UB SCHOOL OF MEDICINE AND BIOMEDICAL SCIENCES ON THE BUFFALO NIAGARA MEDICAL CAMPUS
Count us in.
21st-century education, treatment and discovery
Thank you Class of 1960, the first UB medical school class to name a space—student study suites—in the new medical school.
Members of the Class of 1960 who gathered for their 55th class reunion. *Not pictured Joseph A. Chazan, MD.

UB Medicine University at Buffalo901 Kimball TowerBuffalo, NY 14214-8028
RETURN SERVICE REQUESTED
Nonprofit Org.
U.S. Postage
PAID
Buffalo, NY
Permit No. 311
I’m thankful.
The best public universities have the strongest private support.
www.giving.buffalo.edu or toll free at 855-GIVE-2-UB
Sara Zagroba says competing as a
pole vaulter and rower in college helped ready
her for the rigors of medical school. “There was
no free time and it prepared me for the pace
that I have in medical school,” says Sara, whose
UB scholarship helped pay for travel to Yantaló,
Peru, with classmates to be clinic volunteers.
Sara, who spent summers as a clinic volunteer
in New York, says wherever her work as a
physician takes her, she’ll give part of her time
to a clinic for the disadvantaged in society.
“The scholarship I received allows me to better
succeed in medical school and be better able to
give back to the community.”