ultrasound diagnosis of carotid plaques
TRANSCRIPT

581
DOI: 10.5797/jnet.ra.2018-0066
Introduction
Various imaging modalities including MRI plaque imaging are used for the evaluation of carotid artery plaques, but ultrasonography, which can be performed readily and non-invasively at the bedside, is convenient for follow-up examination and rapid diagnosis in emergency situations. Conventionally, ultrasound examination of carotid artery plaques has focused on narrowing the blood vessels due to
plaques and emphasized quantitative aspects such as the degree of stenosis. Indeed, much evidence that has been reported concerning the risk of cerebral infarction has been based on the evaluation of the degree of stenosis. Clini-cally, however, we often encounter refractory plaques that repeatedly cause ischemic events and resist treatment despite a relatively low degree of stenosis. With the use ofcarotid artery ultrasound for screening examinations of cerebrovascular disorders, opportunities to detect asymp-tomatic plaques and asymptomatic stenosis caused by them have increased, and the necessity of qualitative eval-uation of plaques in question to assess the risk of the future occurrence of stroke is considered to be increasing. This report, therefore, focuses on the qualitative ultrasound diagnosis of carotid artery plaques.
Quantitative Evaluation of the Degree of Stenosis
The degree of stenosis is evaluated by ultrasonography according to the area ratio and vascular diameter ratio (the
Special Issue: Carotid Artery Plaque Diagnosis
Ultrasound Diagnosis of Carotid Plaques
Kozue Saito1 and Hiroshi Yamagami2
Various methods including MRI plaque imaging have been used to evaluate carotid artery plaques, but ultrasonography, which can be performed readily and non-invasively at the bedside, is excellent for follow-up examination and rapid diagnosis in emergency situations. Conventionally, ultrasound examination of carotid artery plaques has focused on vascular stenosis due to plaques and emphasized quantitative aspects such as the degree of stenosis. Clinically, however, some plaques resist treatment and repeatedly cause ischemic events despite a relatively low degree of stenosis. In such cases, qualitative diagnosis based on the evaluation of plaque vulnerability is important. In addition to the items that have been conventionally evaluated, such as the plaque echogenicity, ulceration, and mobility, evaluation of diverse aspects of plaques has become possible due to the advent of new ultrasound techniques. Plaque neovascularization can be evaluated by contrast-enhanced ultrasound (CEUS), visualization of slow blood flows has become possible without the use of a contrast agent by superb micro-vascular imaging (SMI), and detailed morphology and volume can now be examined using a 3D probe. Moreover, because of the excellent portability of ultrasound devices, the evaluation of plaque properties is occasionally useful for the planning of the therapeutic strategy in the acute phase of cerebral infarction. Thus, ultrasonography can provide a wide range of diagnostic information.
Keywords▶ �carotid artery ultrasonography, plaque, vulnerable plaque, contrast agent, atherosclerosis
1Department of Neurology, Nara Medical University, Kashihara, Nara, Japan2Division of Stroke Care Unit, National Cerebral and Cardiovas-cular Center, Suita, Osaka, Japan
Received: April 18, 2018; Accepted: August 21, 2018Corresponding author: Kozue Saito. Department of Neurology, Nara Medical University, 840 Shijo-cho, Kashihara, Nara 634-8522, JapanEmail: [email protected]
This work is licensed under a Creative Commons Attribution-NonCommercial- NoDerivatives International License.
©2018 The Japanese Society for Neuroendovascular Therapy
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)
Journal of Neuroendovascular Therapy 2018; 12: 581–591
Online October 25, 2018

582
Saito K and Yamagami H
the degree of stenosis has progressed compared with the previous examination (Fig. 2).
Qualitative Evaluation of Plaques (Evaluation of Plaque Vulnerability)
Plaque echogenicityThe qualitative evaluation of plaques by ultrasound has long been made according to the echogenicity. Hypoechoic plaques are called soft plaques and have been pathologi-cally demonstrated to suggest intraplaque hemorrhage with a necrotic core (Fig. 3). Patients with hypoechoic plaques showing an echo level close to that of the vascular lumen are known to suffer ischemic events more frequently than those with isoechoic plaques.4) The echogenicity of plaques is evaluated by comparison with the echogenicity of the surrounding intima-media complex (IMC), but plaques with an echo level similar to that of the vascular lumen may be overlooked by B-mode ultrasonography, and cau-tion is needed. There are some plaques so hypoechoic that they can be recognized only as defects by color Doppler imaging (Fig. 3). Turbulent flows may occur at the bifurcation of the carotid artery and interfere with adequate
Fig. 1 Methods for evaluation of carotid artery stenosis. A case of severe stenosis at the origin of the internal carotid artery. (A) Area ratio; (B) Vascular diameter ratio (NASCET method, ECST method); (C) PSV of the blood flow by pulsed Doppler imaging. ECST: European Carotid Surgery Trial; NASCET: the North American Symptomatic Carotid Endarterectomy Trial; PSV: peak systolic velocity
ab
cd
e
Area(%)=a-ba 100= 92.9%
NASCET(%)
e-ce 100=76.4%
ECST(%)
d 100=89.1%d-c
PSV=440cm/s
A
B
C
North American Symptomatic Carotid Endarterectomy Trial [NASCET], European Carotid Surgery Trial [ECST]) and according to the maximum systolic blood flow velocity by Doppler ultrasonography (Fig. 1). Overseas, the evalu-ation of the blood flow velocity by the Doppler technique is the primary diagnostic method, and the area ratio is not used frequently. The vascular diameter ratio by the NASCET method is an index often used when surgical treatment is considered, and while it may be evaluated by ultrasonogra-phy, it may lack reliability as the accurate measurement of the diameter of the distal part of the internal carotid artery is often difficult. Particularly, when the common carotid artery is bifurcated at a high position, the evaluation of the segment distal to the plaque is difficult. For these reasons, the peak systolic velocity (PSV) measured by the Doppler technique and the vascular diameter ratio determined by the ECST method are mainly used as indices for the ultra-sound evaluation of the degree of stenosis. Severe stenosis is known to be associated with a high risk of cerebral isch-emic events.1) A PSV of ≥2 m/s suggests NASCET ≥70% stenosis.2) In addition, patients with progressive stenosis are known to more often have events than those with non-progressive stenosis,3) and caution is necessary when
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)

583
Ultrasound Diagnosis of Carotid Plaques
Fig. 2 A case of progressive asymptomatic stenosis that led to cerebral infarction. Asymptomatic stenosis at the origin of the internal carotid artery periodically followed up with medical treatment. (A) ECST was 75%, PSV was 152 cm/s, and the plaque was hypoechoic. (B) Since stenosis progressed to an ECST of 79% and a PSV of 272 cm/s during an 8-month follow-up period, the patient was examined in detail by hospitalization to evaluate treatment indications. Although surgical treatment was indicated, internal treatment was continued due to the patient’s wishes. (C) After half a year, the patient developed cerebral infarction with mild right-sided paralysis and dysar-thria (C) top, diffusion-weighted MRI of the head, and stenosis progressed further to an ECST of 91% and a PSV of 439 cm/s. The top panels in (A and B) are color Doppler short-axis views, middle panels in (A–C) are color Doppler long-axis views, and bottom panels in (A–C) are pulsed Doppler images). ECST: European Carotid Sur-gery Trial; PSV: peak systolic velocity
PSV 152cm/s 272cm/s
Area 82% Area 90%
439cm/s
ECST 75% ECST 79% ECST 91%
+ 8 mos + 6 mos
A B C
color representation and be mistaken for plaques, so care-ful examination is necessary. Particularly, a severe stenotic lesion is easy to recognize as a source of emboli, but whether mild stenosis is the responsible lesion or not is often difficult to judge. However, as there are mild stenotic lesions that cause repeated recurrence, careful examination not to overlook hypoechoic lesions, in particular, is neces-sary (Fig. 4). Also, whether the echogenicity of the plaque is homogeneous or not is another point of examination. The echogenicity of plaques may be heterogeneous and par-tially hypoechoic or contain discrete white areas (DWAs), which are not accompanied by an acoustic shadow and are recognized as white hyperechoic areas. There have been reports that the presence of DWAs was related to the risk of the occurrence of events,5) that inflammation and hemo-siderin deposits were demonstrated by pathological examination in DWAs, and that DWAs suggest plaque vul-nerability.6)
In clinical situations, the echogenicity is evaluated qualita-tively by comparison with IMC, but techniques to quantify the echogenicity including gray scale median (GSM) and integrated backscatter (IBS) have been developed. By GSM, B-mode images are input into a computer, and the echogenic-ity of the plaque is calculated by correction for the echogenic-ity of the intima/media and the vascular lumen, and this can be performed using commercial image processing software.7) In carotid artery stenting, the risk of ischemic events has been shown to be high when a hypoechoic plaque with a GSM value of ≤25 is noted.8) On the other hand, IBS is calculated by integrating the intensity of raw signals, and, use of raw signals characterizes the less differences of image quality among the devices.9) Using this index, quantitative evalua-tion by comparison with pathological findings of plaques10) and therapeutic effect of statin11) have been reported. These quantification methods may lead to more objective evalua-tion of echogenicity and a decrease in inter-rater variation.
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)

584
Saito K and Yamagami H
However, internal properties of calcified plaques cannot be evaluated sufficiently by ultrasound due to acoustic shad-ows. Usually, the event risk of calcified lesions is not con-sidered high, but studies using CT and MRI have suggested that some plaques surrounded by a wide calcified area may exhibit signals suggestive of intraplaque hemorrhage and that such plaques need attention as they may have a high risk of ischemic events.12,13)
UlcerationUlceration is the state in which plaque has ruptured, and the atheroma inside is exposed in the vascular lumen. It may cause thrombus attachment and increases the risk of embolism if it, along with the exposed atheroma, scatters into the intracranial arteries. In addition, recurrence is known to be more frequent in patients with symptomatic stenotic lesions accompanied by ulcerated lesions,14) so ulceration is an important item to be evaluated. By ultrasound, ulcerated lesions are characterized as blood flow signals inside the plaque. Formerly, depressions 2 mm or greater in depth were
diagnosed as ulcers, but, with improvements in ultrasound devices, those with clear unevenness on the plaque surface are currently diagnosed as ulcers regardless of the depth. Since some lesions are misdiagnosed as ulcers by B-mode ultrasonography due to apparent unevenness of the plaque surface, which is caused by the similarity of the echo level of hypoechoic components to that of the vascular lumen, the blood flow inside the lesion must be checked simultaneously by color Doppler imaging. However, the identification of ulcers is often difficult if color signals are not obtained insuf-ficiently due to turbulence or attachment of thrombus inside the plaques. Moreover, ulcers have been reported to be often overlooked if the stenosis is severe.15) With improvements in the resolution of the ultrasound device, it has also been reported that the clarity of the image of the plaque surface has increased and that rupture of structures corresponding to relatively hyperechoic fibrous cap on the surface has become observable, permitting the diagnosis of rupture of the fibrous cap.16) In addition, as discussed below, the ability to visualize ulcers has been improved with technological
Fig. 3 A case of symptomatic stenosis that had the onset with transient amaurosis and recurrence with a transient isch-emic attack. On carotid artery ultrasonography, the plaque at the origin of the internal carotid artery was hypoechoic and was visualized by color Doppler imaging as a defect of color signal (A) B-mode long-axis view, (B) color Doppler long-axis view. Angiography also showed marked stenosis due to a plaque at the same site (C) lateral view (arrow). On MR plaque imaging (D) MPRAGE image, the plaque was hyperintenese, suggesting intraplaque hemorrhage. The histopathological sample obtained by endarterectomy (E) Masson trichrome stain showed a wide area of hemorrhage inside the plaque (asterisk). ECA: external carotid artery; ICA: internal carotid artery; MPRAGE: magnetization-prepared rapid acquisition with gradient echo; MR: magnetic resonance
ECA
ICA
A B
EC D
2 mm
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)

585
Ultrasound Diagnosis of Carotid Plaques
sign, and this sign is known to be a risk factor for events since it suggests rupture of the fibrous cap and is fre-quently associated with recurrence.19) While evaluation of individual patients is necessary, surgical treatment is an option when the lesion is considered a source of emboli, particularly, if it is symptomatic and recurrent. As men-tioned above, ultrasonography is advantageous for serial evaluations, and follow-up at short intervals should be considered, particularly, when the plaque is symptomatic and is accompanied by a mobile lesion, as its morphology may change within a few days.
Progresses in Ultrasound Plaque Imaging
The ability of ultrasonography for qualitative diagnosis of plaques has improved as previously unknown techniques
development. At any rate, careful examination including the morphology of the plaque surface is important.
Evaluation of plaque mobilityBy MRI and CT, the morphology of plaques can be evalu-ated if they are protruded, but their mobility is usually dif-ficult to evaluate. Ultrasonography, on the other hand, is excellent in real-time evaluation of the plaque mobility. Mobile plaques have been reported pathologically to often contain a necrotic core with thrombus.17) Mobile lesions have a high risk of embolism, and, as symptomatic mobile lesions are related to the risk of recurrence, close fol-low-up is needed.18) Video recording is recommended if they are detected. Also, if the plaque is not clearly pro-truded, jellyfish sign, or wobbling of part of the plaque with pulses like a jellyfish, is occasionally observed. Intraplaque hemorrhage is observed at the site of jellyfish
Fig. 4 A case of recurrent cerebral infarction despite mild stenosis at the origin of the internal carotid artery. The patient had the onset with right hemiplegia and was found to have a focus of infarction in the left MCA territory (A) diffusion- weighted MRI. Carotid artery ultrasonography showed a hypoechoic plaque from the bifurcation to the origin of the carotid artery (D). At this site, stenosis was mild on carotid artery MRA with a NASCET of 22% (C), but the signal intensity was high on MR images (MPRAGE) (B). On CEUS images, many linear traces of microbubbles into the plaque were observed (E), suggesting neovascularization. Since the grade of stenosis was mild, the patient was observed with internal treatment but had recurrence of cerebral infarction of the left MCA territory with mild right-sided paralysis after 1 year (F). Although the lesion was also a hypoechoic plaque on color-Doppler imaging (G), CEUS demonstrated ulcers that could not be identified by color Doppler imaging (H). CEUS: contrast-enhanced ultrasound; MCA: middle cerebral artery; MPRAGE: magnetization-prepared rapid acquisition with gradient echo; NASCET: the North American Symptomatic Carotid Endarterectomy Trial
B
CD
E
G
A F
H
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)

586
Saito K and Yamagami H
of insoluble gas with shells. In addition, as a contrast- enhancing effect can be obtained at a fixed low acoustic pressure without destroying the bubbles, movements of bubbles along the blood flow can be observed continu-ously. This has made visualization of not only vascular lumens with a slow minute blood flow but also newly formed vessels inside the plaque possible. Neovessels in the plaque, which are vulnerable and likely to rupture, may cause intraplaque hemorrhage and are a factor of plaque vulnerability. A correlation between contrast-enhancement and plaque neovascularization has been pathologically demonstrated, and they are also reported to be related to symptoms.20) (Figs. 4E and 5).
Small ulcers that emit no blood flow signals in non- contrast imaging are also visualized clearly by the use of an ultrasound contrast agent21) (Fig. 4H). Since contrast- enhanced ultrasonography is advantageous for visualization of slow blood flows, it clearly delineates even pseudo- occlusion that appears to be occluded on non-contrast
have become available in B-mode, color Doppler, and Dop-pler imaging on the daily practice level with improvements in the ultrasound device. In B-mode ultrasonography, eval-uation of small mobile lesions and the properties of the plaque surface suggestive of rupture of the fibrous cap, which was mentioned above, has become possible with improvement in resolution. Non-contrasted imaging of slow blood flow in ulcer and neovessels of plaques has also become possible, and further improvements are expected for the future. In Doppler blood flow imaging, the continu-ous-wave Doppler method using a linear probe has become available, and the evaluation of faster blood flows and more accurate blood flow evaluation have been made possible. Further improvements are also expected in this field.
Diagnosis of plaque vulnerability by contrast- enhanced ultrasonographyUltrasound contrast agents, such as Sonazoid, produce con-sistent contrast-enhancing effects using microbubbles made
Fig. 5 A case of symptomatic internal carotid artery pseudo-occlusion. Poor color Doppler image showed pseudo-oc-clusion in the area distal to the lesion due to severe stenosis (B) color Doppler long-axis view. On CEUS images, the site of stenosis was clearly delineated, and the internal carotid artery distal to the lesion was also visualized. Moreover, many neovessels were delineated in the plaque (A) long-axis view, (C) short-axis view (arrows). In the histopathological sample, severe stenosis accompanied by intraplaque hemorrhage and many neovessels corresponding to the images of CEUS were identified in the plaque (D) Masson trichrome stain, (E) immunological staining for von Willbrand factor in the square in (D); the tubular structures stained brown are neovessels. CEUS: contrast-enhanced ultrasound
D
A
B
C
E
2 mm
20 mµ
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)

587
Ultrasound Diagnosis of Carotid Plaques
Fig. 6 A case of symptomatic stenosis at the origin of the internal carotid artery in which CEUS suggested a thrombus attaching to the plaque. The plaque morphology could not be clearly visualized by non-contrast carotid artery ultra-sonography (A) color Doppler long-axis view partly due to turbulence caused by severe stenosis, but CEUS (B) clearly visualized the plaque as a filling defect and suggested the presence of a thrombus at the distal end (B: arrow). At the same site, carotid artery CTA showed similar morphology and also suggested a thrombus at the distal end of the plaque (C: arrow). CEUS: contrast-enhanced ultrasound
CA
B
imaging due to marked stenosis and the consequent lack of blood flow signals on the distal side (Fig. 5). Moreover, by contrast-enhanced ultrasonography, the morphology of plaques which cannot be evaluated by color Doppler imag-ing due to turbulence caused by their complex shape can also be visualized, and thrombi that attach to the plaque can be clearly delineated as filling defects (Fig. 6). Thus, contrast-enhanced ultrasonography may provide necessary and important detailed information on the routine clinical level. Since ultrasound contrast agents have few adverse effects and do not affect the renal function, they can also be used safely in patients who do not tolerate iodine-based contrast media. However, as their use is presently restricted to the liver and breast lesions, and their application to the brain and carotid arteries is not covered by insurance in Japan, their clinical availability is limited.
Superb micro-vascular imagingNon-contrast imaging techniques that permit detection of even slower blood flows than those detectable by conventional color Doppler or power Doppler methods at a
high frame rate by suppression of motion artifact have begun to be provided. Using superb micro-vascular imag-ing (SMI), lesions that are used to be impossible to identify by conventional color Doppler imaging such as pseudo- occlusions and minute ulcers (Fig. 7) and, occasionally, intraplaque new vessels (Fig. 8) have become identifiable. Using such techniques, images similar to those by contrast- enhanced imaging may become available without using a contrast agent for the future. They may be useful in situations where a contrast agent is not usable, and further develop-ment of the technology is awaited.
Plaque evaluation by 3D ultrasonographyThe evaluation of the morphology of ulcerated lesions and protruding plaques is facilitated by 3D rather than 2D obser-vation. The evaluation of the shape of ulcers and plaques has become possible by collecting 3D data of the carotid artery simply using a linear type 3D probe and reconstruct-ing the data (Fig. 9). There is also the technique to create 3D images by collecting ultrasound images simultaneously with positional information using a 2D probe to which a
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)

588
Saito K and Yamagami H
leading to reports that the plaque volume was correlated with cardiovascular events22) and that changes in plaque volume were used for the evaluation of the effectiveness of medical treatment.23) If the measurement of the plaque volume is facilitated further, the application range of this technique is expected to be expanded.
position sensor is attached and reconstructing the data. The use of this technique makes it possible not only to clarify 3D morphology but also to calculate the volume of the plaque. Since the plaque mass can be evaluated more accurately than by calculation using 2D data, changes in the plaque volume with time can be captured more sensitively,
Fig. 8 Neovessels observed in the plaque. In the areas that could not be identified by color Doppler imaging (A) short-axis view but were visualized as linear images by SMI (B) short-axis view; arrows, linear influx of microbubbles were also observed on CEUS (C) short-axis view (arrows), suggesting neovascularization. CEUS: contrast-enhanced ultrasound; SMI: superb micro-vascular imaging
CA B
Fig. 7 Ulcerated lesion of the origin of the internal carotid artery. SMI (B) long-axis view, (C) short-axis view; arrows showed an ulcer which could not be detected with color Doppler imaging (A) color Doppler image, long-axis view. SMI: superb micro-vascular imaging
C
A B
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)

589
Ultrasound Diagnosis of Carotid Plaques
stenosis, and the properties of the interior of the plaque such as the presence of a calcified area can also be evaluated (Fig. 10). While the definitive diagnosis is impossible by ultrasonography alone, if such information can be obtained readily in an early stage of examination, we can plan the ther-apeutic strategy for revascularization quickly.
Limitations of Plaque Diagnosis by Ultrasonography
Ultrasonography is highly portable and can be performed readily at the bedside, but the accuracy of the diagnosis depends on the skill of the examiner, and the possibility of inadequate diagnosis and poor reproducibility is undeni-able. In addition, in lesions accompanied by marked calci-fication, examination of the interior is impossible due to the acoustic shadows derived from the characteristics of ultrasound. Also, in patients with the bifurcation of the internal carotid artery at a high position, which is observed frequently in Japanese, the plaque of the internal carotid
Emergency Outpatient Diagnosis of Carotid Artery Plaques
In the treatment for acute cerebral infarction, the role of revascularization by endovascular treatment has been increasing recently. Ultrasonography is portable, can be performed readily in emergency outpatient care, and carotid artery ultrasonography, in particular, permits easy examination of the common carotid to internal carotid arteries from the body surface. The diagnosis of occlusion of major arteries, such as the common carotid artery and trunk of the middle cerebral artery, is possible by blood flow waveform analysis, and it is useful for emergency therapeutic planning. Detail evaluation of the origin of carotid arteries sometimes enables us to determine the etiology of occlusions, such as cardiac thrombus or atherosclerotic plaques. If it is caused by cardiac thrombus, a crab claw-like filling defect is observed, and it may oscillate back and forth. If it is caused by an athero-sclerotic plaque, progressive changes, such as the thickened intima and plaque, can be observed from before the site of
Fig. 9 Ulcerated lesion of the common carotid artery. The depth and shape of ulcer became easier to perceive by 3D recon-struction of 2D images of an ulcerated lesion (A) B-mode long-axis view (arrows) using a 3D linear probe (B). (D) is a schema of (C).
Ulcer
C
A B
D
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)
590
Saito K and Yamagami H
Disclosure Statement
The first author and coauthor have no conflicts of interest.
References 1) Nicolaides AN, Kakkos SK, Griffin M, et al: Severity of
asymptomatic carotid stenosis and risk of ipsilateral hemi-spheric ischaemic events: results from the ACSRS study. Eur J Vasc Endovasc Surg 2005; 30: 275–284.
2) Koga M, Kimura K, Minematsu K, et al: Diagnosis of inter-nal carotid artery stenosis greater than 70% with power Doppler duplex sonography. AJNR Am J Neuroradiol 2001; 22: 413–417.
3) Hirt LS: Progression rate and ipsilateral neurological events in asymptomatic carotid stenosis. Stroke 2014; 45: 702–706.
4) Gupta A, Kesavabhotla K, Baradaran H, et al: Plaque echo-lucency and stroke risk in asymptomatic carotid stenosis: a systematic review and meta-analysis. Stroke 2015; 46: 91–97.
5) Nicolaides AN, Kakkos SK, Kyriacou E, et al: Asymptom-atic internal carotid artery stenosis and cerebrovascular risk stratification. J Vasc Surg 2010; 52: 1486–1496.e1-5.
6) Mitchell CC, Stein JH, Cook TD, et al: Histopathologic val-idation of grayscale carotid plaque characteristics related to plaque vulnerability. Ultrasound Med Biol 2017; 43: 129–137.
7) Grønholdt ML, Nordestgaard BG, Schroeder TV, et al: Ultrasonic echolucent carotid plaques predict future strokes. Circulation 2001; 104: 68–73.
8) Biasi GM, Froio A, Diethrich EB, et al: Carotid plaque echolucency increases the risk of stroke in carotid stent-ing: the Imaging in Carotid Angioplasty and Risk of Stroke (ICAROS) study. Circulation 2004; 110: 756–762.
9) Waki H, Masuyama T, Mori H, et al: Ultrasonic tissue char-acterization of the atherosclerotic carotid artery: histologi-cal correlates or carotid integrated backscatter. Circ J 2003; 67: 1013–1016.
10) Nagano K, Yamagami H, Tsukamoto Y, et al: Quantitative evaluation of carotid plaque echogenicity by integrated back-scatter analysis: correlation with symptomatic history and histologic findings. Cerebrovasc Dis 2008; 26: 578–583.
11) Yamagami H, Sakaguchi M, Furukado S, et al: Statin therapy increases carotid plaque echogenicity in hyper-cholesterolemic patients. Ultrasound Med Biol 2008; 34: 1353–1359.
12) Pini R, Faggioli G, Fittipaldi S, et al: Relationship between calcification and vulnerability of the carotid plaques. Ann Vasc Surg 2017; 44: 336–342.
13) van den Bouwhuijsen QJ, Bos D, Ikram MA, et al: Coexis-tence of calcification, intraplaque hemorrhage and lipid core
artery is located at a high position, and its detailed evalua-tion may be prevented by the mandible.
The primary theme of this paper is the qualitative diag-nosis of carotid artery plaques. With the development of technology, indices that can be evaluated by ultrasonography have increased recently, and ultrasonography is expected to contribute more to the evaluation of indications of treatments including endovascular treatment and examinations before and after the treatment.
Acknowledgments
The authors extend their sincere gratitude to Dr. Hatsue Ueda, Department of Pathology, National Cerebral and Cardiovascular Center, who provided histopathological images, and Dr. Tenyu Hino, Department of Neurosurgery, Tsukuba University Hospital and Dr. Akihiro Watanabe, Neurovascular Medicine, National Hospital Organization Osaka Minami Medical Center, who provided ultrasono-grams, for their help in the preparation of this paper.
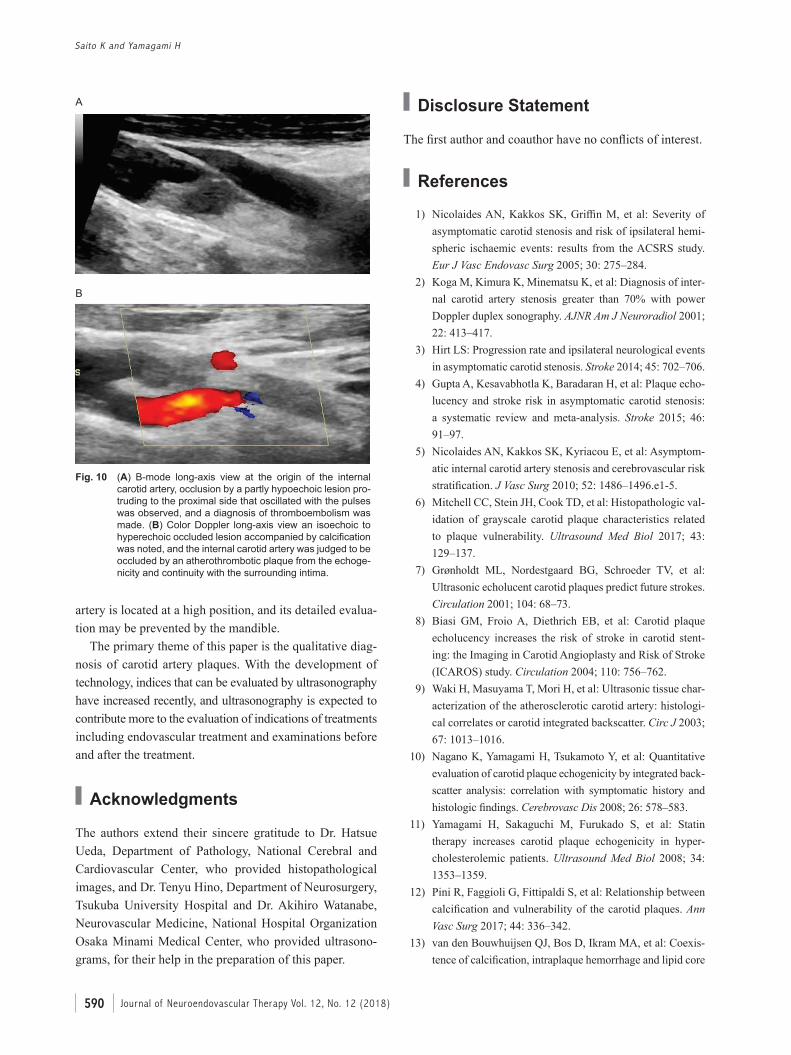
Fig. 10 (A) B-mode long-axis view at the origin of the internal carotid artery, occlusion by a partly hypoechoic lesion pro-truding to the proximal side that oscillated with the pulses was observed, and a diagnosis of thromboembolism was made. (B) Color Doppler long-axis view an isoechoic to hyperechoic occluded lesion accompanied by calcification was noted, and the internal carotid artery was judged to be occluded by an atherothrombotic plaque from the echoge-nicity and continuity with the surrounding intima.
A
B
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)

591
Ultrasound Diagnosis of Carotid Plaques
19) Kume S, Hama S, Yamane K, et al: Vulnerable carotid arterial plaque causing repeated ischemic stroke can be detected with B-mode ultrasonography as a mobile compo-nent: Jellyfish sign. Neurosurg Rev 2010; 33: 419–430.
20) Saito K, Nagatsuka K, Ishibashi-Ueda H, et al: Contrast- enhanced ultrasound for the evaluation of neovasculariza-tion in atherosclerotic carotid artery plaques. Stroke 2014; 45: 3073–3075.
21) Hamada O, Sakata N, Ogata T, et al: Contrast-enhanced ultrasonography for detecting histological carotid plaque rupture: quantitative analysis of ulcer. Int J Stroke 2016; 11: 791–798.
22) van Engelen A, Wannarong T, Parraga G, et al: Three- dimensional carotid ultrasound plaque texture predicts vas-cular events. Stroke 2014; 45: 2695–2701.
23) Yamaguchi M, Sasaki M, Ohba H, et al: Quantitative assessment of changes in carotid plaques during cilostazol administration using three-dimensional ultrasonography and non-gated magnetic resonance plaque imaging. Neu-roradiology 2012; 54: 939–945.
within the asymptomatic atherosclerotic carotid plaque: the Rotterdam study. Cerebrovasc Dis 2015; 39: 319–324.
14) Redgrave JN, Lovett JK, Gallagher PJ, et al: Histological assessment of 526 symptomatic carotid plaques in relation to the nature and timing of ischemic symptoms: the Oxford plaque study. Circulation 2006; 113: 2320–2328.
15) Comerota AJ, Katz ML, White JV, et al: The preoperative diagnosis of the ulcerated carotid atheroma. J Vasc Surg 1990; 11: 505–510.
16) Devuyst G, Karapanayiotides T, Ruchat P, et al: Ultrasound measurement of the fibrous cap in symptomatic and asymp-tomatic atheromatous carotid plaques. Circulation 2005; 111: 2776–2782.
17) Funaki T, Iihara K, Miyamoto S, et al: Histologic character-
ization of mobile and nonmobile carotid plaques detected
with ultrasound imaging. J Vasc Surg 2011; 53: 977–983. 18) Ogata T, Yasaka M, Wakugawa Y, et al: Morphological
classification of mobile plaques and their association with early recurrence of stroke. Cerebrovasc Dis 2010; 30: 606–611.
Journal of Neuroendovascular Therapy Vol. 12, No. 12 (2018)