undamentals of obstetrics - ucsf medical · pdf fileginger may decrease nausea...
TRANSCRIPT

FUNDAMENTALS OF OBSTETRICS
Christine Pecci, MD Associate Clinical Professor UCSF Department of Family and Community Medicine March 2017
No disclosures
OBJECTIVES Describe the group prenatal care model Review criteria for ultrasound vs LMP dating Review management of women at risk for
preterm delivery Describe guidelines for diagnosis, treatment and
management of preeclampsia, gestational diabetes and thyroid disease in pregnancy
List infections in pregnancy and how to manage or prevent these from occurring
PRENATAL CARE MODELS: DO WE KNOW WHAT’S BEST? Traditional care-ACOG
Q 4 wk visits until 28 weeks Q 2 wk visits until 36 weeks Q 1 wk visits until delivery
Traditional care- ICSI 8-11 visits total 6-8 wks, 10-12 wks, 16-18 wks, 22 wks, 28 wks, 32
wks, 36 wks, 38-41 wks Group Prenatal Care
Group of 5-12 patients x 2 hours q 2-4 wks

GROUP OR TRADITIONAL PRENATAL CARE? Similar rates of PTD, NICU admission and
breastfeeding initiation rates African American women with significantly lower
PTD rate* but not among Latina Decreased rate of LBW overall**
No harm in doing group care and likely benefit in
certain groups
Carter et al OB GYN Sept 2016
Tanya is a 23 yo G1P0 who presents for early pregnancy care. EGA 10 1/7 wks by a sure LMP
She had a visit to ED for nausea and vomiting
Given 1 liter NS Electrolytes were normal TSH 0.1

NAUSEA AND VOMITING IN PREGNANCY Nausea in 50-80% Vomiting/retching 50% Hyperemesis gravidarum 0.3-3%
Persistent vomiting Weight loss Ketonuria Usually electrolyte, thyroid, liver abnormalities
Lower rate of miscarriage
ACOG Practice Bulletin April 2015
TREATMENT OF N/V IN PREGNANCY Multivitamin x 3 months before conception Ginger may decrease nausea Acupuncture/acupressure- no difference in RCTs First line treatment pyridoxine +/- doxylamine Metoclopromide, ondansetron second line
Limited safety data, but overall risk low Oral corticosteroids used as last resort– avoid 1st
trimester
ACOG Practice Bulletin April 2015

NORMAL THYROID FUNCTION AND PREGNANCY Hcg stimulates TSH receptor, increasing thyroid
production and decreasing TSH Total thyroid hormone levels increase due to
elevated thyroid-binding globulin (TBG) Free T4 unchanged (direct assays ok but many labs use
automated assays which can be inaccurate) TSH is a reliable indicator of maternal thyroid
status (American Thyroid Association) First trimester 0.1-2.5 mIU/L Second trimester 0.2-3.0 mIU/L Third trimester 0.3-3.0 mIU/L

HYPERTHYROIDISM IN PREGNANCY Avoid meds in 1st trimester If medication needed, use PTU
risk of liver failure Risk face and neck cysts
Consider changing methimazole after 16 wks (aplasia cutis) other congenital malformations
Smallest possible dose as medications cross placenta and can be more potent for fetal thyroid
Target: at or just above upper range of normal Moniter TSH/T4 every 4 wks if on medication

HYPOTHYROIDISM Case control trials showed hypothyroidism
associated with low IQ in the fetus RCTs do NOT confirm that treatment of
subclinical hypothyroidism improves neurocognitive outcomes Both initiated Rx after first trimester
Universal screening for thyroid disease in pregnancy is not indicated* Increased pregnancy loss with elevated TSH,
especially if TPO ab elevated Effectiveness of Rx not yet proven Maybe need to screen 4-7 wks?
*ACOG, Endocrine Society, American Association of Clinical Endocrinologists

RECOMMENDATIONS Treat if TSH >10 TSH>2.5 check TPO Ab status ?treat if TPO Ab+ and TSH >2.5 Don’t treat if TPO neg and TSH > upper nl <10
If treating
Target lower half of preg specific range or <2.5 Measure q4 wks in pregnancy then at least once near
30 wks
American Thyroid Association 2017

SUPPLEMENTATION AND PREGNANCY 50-85% need increase in thyroid replacement Preconception treat to <2.5 Should increase dose by 25-30% ASAP post
conception (can give two extra pills/wk)
Postpartum following delivery go back to pre-pregnancy dose and recheck in 6 wks
If Rx started in pregnancy with nl TSH reasonable to stop and recheck in 6 wks
LMP VS. US DATING Tanya also had an US done in the ED Crown-rump length = 9 2/7 weeks LMP 10 1/7 wks
6 days different than EDD based on LMP
Should you change her dating based on 1st trimester US?
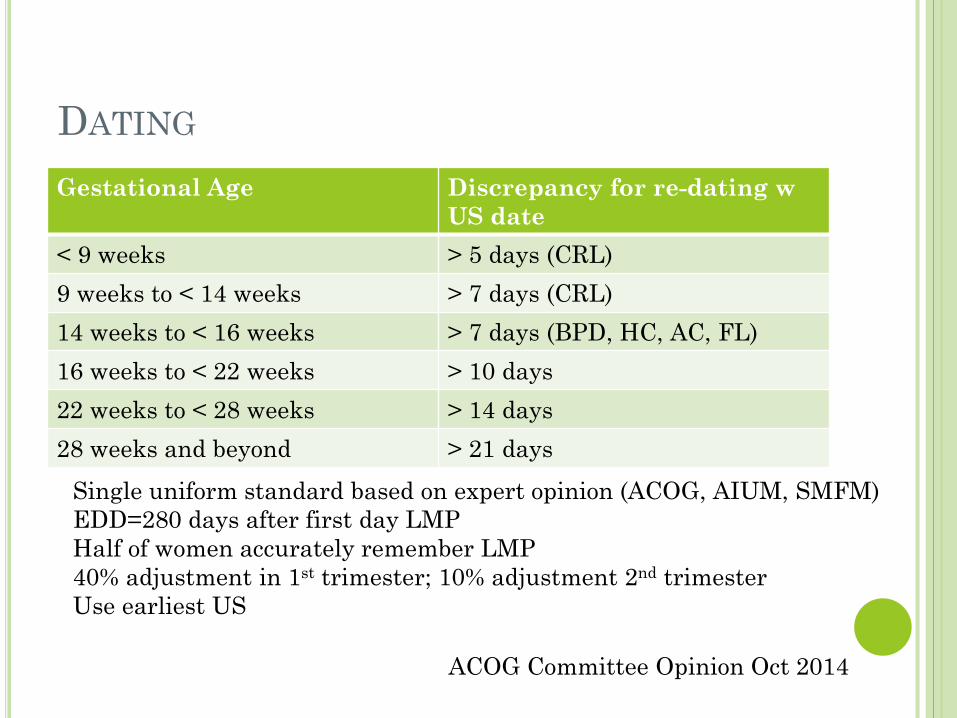
DATING Gestational Age Discrepancy for re-dating w
US date < 9 weeks > 5 days (CRL) 9 weeks to < 14 weeks > 7 days (CRL) 14 weeks to < 16 weeks > 7 days (BPD, HC, AC, FL) 16 weeks to < 22 weeks > 10 days 22 weeks to < 28 weeks > 14 days 28 weeks and beyond > 21 days
ACOG Committee Opinion Oct 2014
Single uniform standard based on expert opinion (ACOG, AIUM, SMFM) EDD=280 days after first day LMP Half of women accurately remember LMP 40% adjustment in 1st trimester; 10% adjustment 2nd trimester Use earliest US
WILL MY BABY BE NORMAL? She has been reading about a new test for
making sure the baby is normal. She wants to know if you can order this test. Will having a normal test guarantee that this baby will be okay?

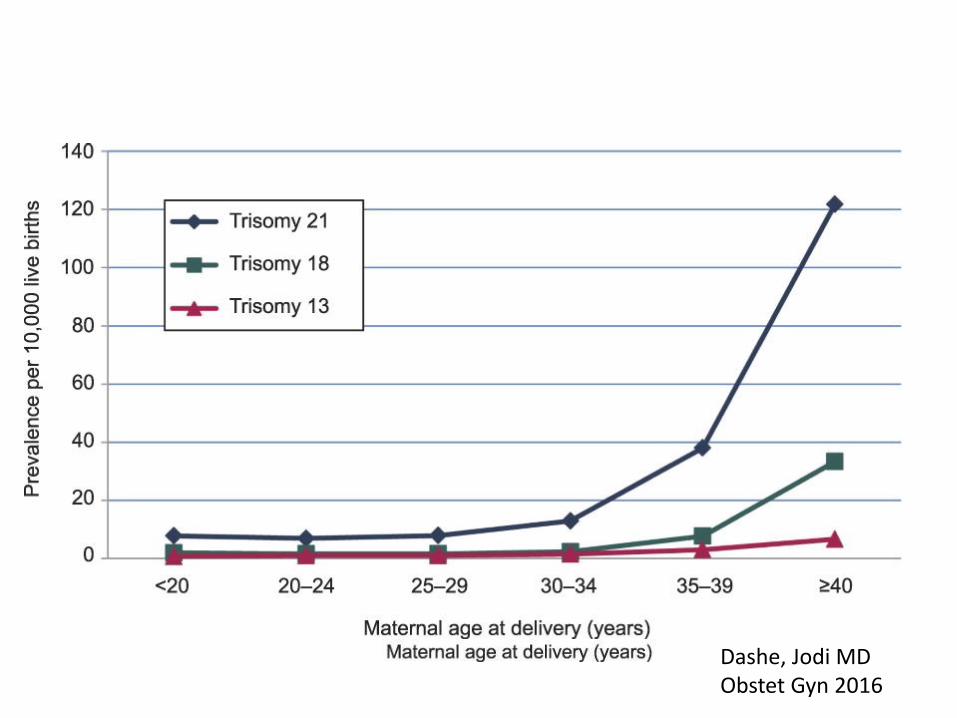
Characteristics of screening tests:T21
Dashe, Jodi MD Obstet Gyn 2016

Options for screening
First Trimester Second Trimester hcg + PAPP-A hcg + AFP + estradiol + inhibin 11-14 wks 15-22 wks Can be combined w NT Anatomy scan AFP in 2nd trimester for NTD Includes AFP
• 1st trimester screening gives the patient early results • 2nd trimester screening good for late entry to care • DON’T do both independently • CAN do combined (7 serum markers + NT)
COMBINED 1ST AND 2ND TRIMESTER SCREENING Sequential testing
Stepwise high risk offered diagnostic testing after 1st trimester Others get results after second trimester Contingent highest risk offered diagnostic testing after 1st tri lowest risk reassured- no further testing Others get results after 2nd trimester
Integrated testing

CELL-FREE DNA Circulating DNA fragments placental in origin
from apoptotic trophoblasts Can be done anytime after 9-10 wks gestation Available in 7-10 days Best for trisomy 21 and 18 but also screens for
trisomy 13 and sex chromosome aneuploidies Gender Can be used as primary or secondary screening
AJOG June 2016 SMFM Consult Series
Dashe, Jodi MD Obstet Gyn 2016
I’M SO NERVOUS… Tanya is worried specifically about preeclampsia
because her sister had it and needed to be induced a few weeks before her due date.
“Is there anything that you can give me so that I don’t get this disease too?”
PREECLAMPSIA: YOU WILL SEE IT! Incidence 2-8% Has increased by 25% in last two decades More likely in patients with hypertension Unrecognized has serious health consequences
for mom and baby Risk factor for future CV and metabolic disease
Task Force for Hypertension in Pregnancy, 2013
INITIATE ASA 12-28 WKS FOR HIGH RISK History of pre-eclampsia, esp if adverse outcome Multi-fetal gestation Chronic hypertension Diabetes type 1 or 2 Renal disease Autoimmune disease (SLE, APS)
Patient with history of preeclampsia <34 wks
Prevalence 40% NNT 1:20
Practice Advisory on Low-Dose Aspirin and Prevention of Preeclampsia: Updated Recommendations July 11 , 2016
CATEGORIES Preeclampsia-eclampsia
With or without severe features Chronic hypertension Gestational hypertension- hypertension without
proteinuria after 20 week Chronic hypertension with superimposed
preeclampsia
Task Force for Hypertension in Pregnancy, 2013

PROTEINURIA >300 mg in 24 hrs Spot urine:creatinine ratio > 0.3 Dipstick 1+
Proteinuria is classically part of the syndrome But NOT required to make diagnosis of
preeclampsia

DIAGNOSIS Elevated BP
>140/90 on two occasions 4 hours apart Proteinuria or “severe features”
>160/110 Plts <100K LFTs twice normal Persistent RUQ pain or epigastric pain Creatinine >1.1 or double Pulmonary edema New onset cerebral or visual disturbance

WHEN TO DELIVER? Chronic hypertension
Deliver after 38 0/7 wks Gestational hypertension:
Deliver at 37 0/7 weeks weekly dip for proteinuria + BP check (can be at
home) NST q week
WHEN TO DELIVER? Preeclampsia without severe features:
Deliver at 37 0/7 weeks 2x week BP, once a week labs 2x week NST
Preeclampsia with severe features Deliver at 34 0/7 weeks Monitor in hospital
Severe uncontrolled htn, eclampsia, pulm edema, abruption, DIC, NRFHR, IUFD Immediate delivery after initial stabilization
INTRAPARTUM INTERVENTIONS Mg with severe preeclampsia only Anti hypertensive meds only for > 160/110 Administer steroids prior to delivery
POSTPARTUM FOLLOW-UP Check BP 72 hours post delivery and 7-10 days
postpartum Treat for >150/100 on two occasions 4-6 hrs apart Preconception- glycemic control, weight loss
ALL patients should receive education on warning signs


ROUTINE US 18-22 WKS Confirms dating if not already done Anatomy scan ? Cervical length
Universal screening not indicated
SCREEN FOR GDM AT 24-28 WKS
Overall incidence of DM in pregnancy 6%
90% of these are GDM Early screening- if
prior GDM, known impaired fasting glucose, BMI >30

GESTATIONAL DIABETES HAPO trials show continuous relationship-
neonatal hypoglycemia, macrosomia Increased hyperbilirubinemia, operative delivery,
shoulder dystocia 2010 International Association of Diabetes and
Pregnancy Study Group (endorsed by ADA) (92, 180, 153) No data regarding therapeutic intervention
ACOG Practice Bulletin Aug 2013
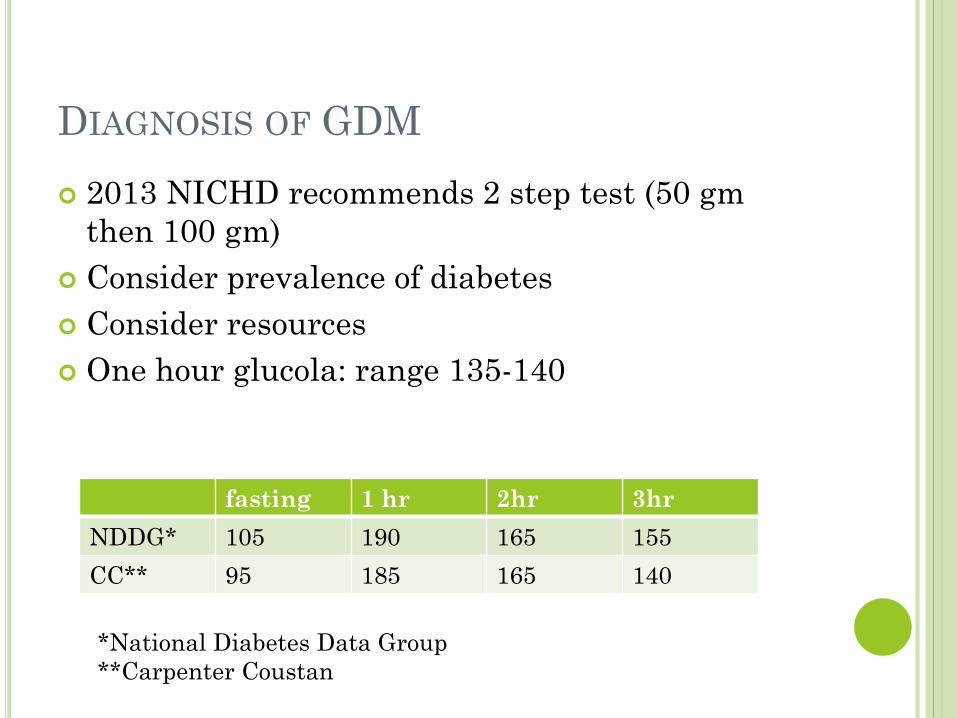
DIAGNOSIS OF GDM 2013 NICHD recommends 2 step test (50 gm
then 100 gm) Consider prevalence of diabetes Consider resources One hour glucola: range 135-140
fasting 1 hr 2hr 3hr NDDG* 105 190 165 155 CC** 95 185 165 140
*National Diabetes Data Group **Carpenter Coustan
MANAGEMENT AND TREATMENT QID fingersticks Goal <140 on 1 hr and < 120 2 hr Carbs 33-40% of diet; Protein 20%; fat 40% Moderate exercise If fasting consistently >95, consider insulin Insulin does not cross the placenta Glyburide and metformin
not approved but being used Glyburide crosses placenta but no measurable levels
in cord blood
WHEN TO DELIVER? Induce at 39 weeks if pre-gestational or
gestational DM on meds For well controlled GDM without meds, unclear
whether induction is indicated.
MODE OF DELIVERY WITH DIABETES Prevention of a single permanent brachial plexus
palsy Cesarean delivery for 4500 gm NNT 588 Cesarean delivery for 4000 gm NNT 962
POSTPARTUM FOLLOW-UP 15-50% with GDM develop DM 20+ years later
Varies by ethnicity (60% Latina within 5 years) Fasting or 2 hr GTT 4-12 wk postpartum
IGT picked up by 2 hr Repeat testing q 3 years if normal

INFECTIONS IN PREGNANCY
HSV Genital herpes affects 20% women in US? Incidence of new infection in preg 2% Women with recurrent HSV-75% can expect
episode during preg, 14% at delivery 80% of infected infants born to women with no
reported history 20% neonatal survivors have long-term
neurosequealae
HSV-GIVE PROPHYLAXIS AT TERM Primary infection transmission - 30-60% at delivery Recurrent infection transmission 3% at delivery; no
lesions 2/10,000 Acyclovir, famcyclovir, valcyclovir all class B, most
data on acyclovir Routine screening not recommended Genital Sx or lesions- c/s decreases transmission from
7.2% to 1.2% even after ROM
Acyclovir 400 mg TID @ 36 weeks til delivery
HIV Opt out screening for ALL women Low threshold for repeating in third trimester; offer
testing on L&D Early viral suppression is of upmost importance Elective cesarean if VL >1000 near delivery Intrapartum AZT unless consistent VL <1000 Neonatal AZT prophylaxis required for 4-6 weeks
add if NVP high risk Consider offering presumptive treatment (AZT+NVP+3TC)
No breastfeeding (developed countries) Clinician Consultation Center Perinatal hotline 24/7
http://nccc.ucsf.edu/
GBS Screen all women at 35-37 wks, unless
Previous child with early onset GBS disease GBS bacteruria in index pregnancy
Treat with intrapartum IV penicillin first line Ask for sensitivities if has pcn anaphylaxis to see if
can give Clinda/erythro Cefazolin if no anaphylaxis reaction to penicillin Vanco reserved for those with anaphylaxis or those
without sensitivities Adequate treatment >4 hours pcn or cefazolin
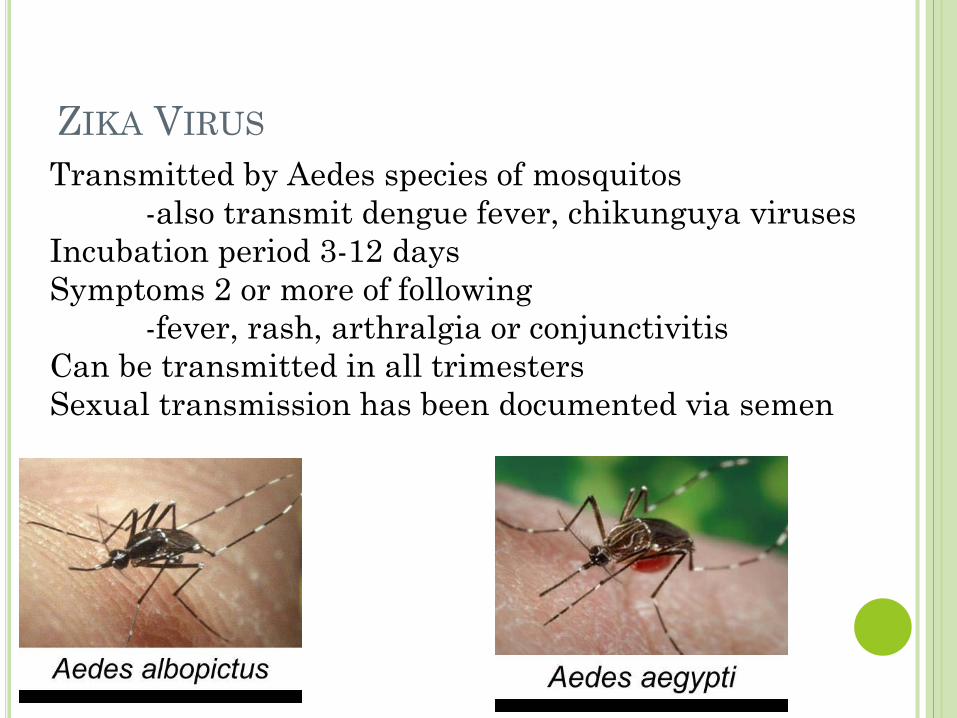
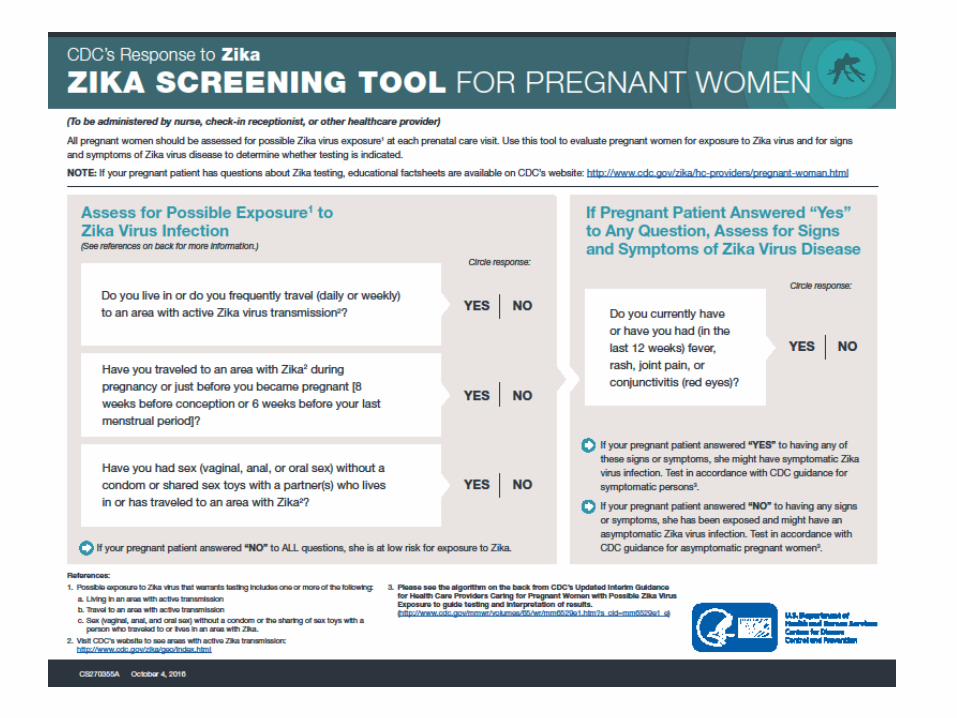
ZIKA VIRUS Transmitted by Aedes species of mosquitos -also transmit dengue fever, chikunguya viruses Incubation period 3-12 days Symptoms 2 or more of following -fever, rash, arthralgia or conjunctivitis Can be transmitted in all trimesters Sexual transmission has been documented via semen

Laboratory-confirmed Zika virus disease cases reported to ArboNET by state or territory (as of February 1, 2017)
ZIKA VIRUS IN PRE/POST CONCEPTION Pre-conception
women: wait 8 wks after sx start or last exposure Men: wait 6 months
If pregnant: Avoid travel to active Zika virus areas or take measures to avoid mosquito bites
Use condom if partner is travelling to Zika areas For those living or travelling frequently to Zika
areas, do testing Ask about travel to endemic countries Protected from future infections
ZIKA TESTING Test those with clinical illnesses (2 or more sx)
during or within 2 weeks of travel RNA NAT and Zika Ig M
Offer RNA NAT to pregnant women 2-12 weeks after travel if they are Zika IgM
Testing done by CDC and state health depts
ZIKA AND FETAL CONCERNS Microcephaly (at birth or postnatally) Congenital Zika Syndrome
Severe microcephaly where skull partially collapsed Specific pattern of brain damage and decreased brain
tissue Damage to back of eye Joints with limited ROM (club foot) Hypertonia

ZIKA AND FETAL MONITORING Get ultrasound 3-4 weeks within exposure Serial scans q 3-4 wks Offer amnio in documented infection
unknown how long positive or ability of test to determine fetal injury
Send fetal tissue/placenta Ok to breastfeed

ZIKA RESOURCES https://www.cdc.gov/zika/hc-providers/pregnant-
woman.html Call 770-488-7100 and ask for the Zika
Pregnancy Hotline or email [email protected]
56

RUBELLA Do not give during pregnancy and avoid pregnancy x
28 days Not an indication for termination If lab evidence of immunity, no need to repeat If neg or equivocal titer after 1-2 doses, give third dose
and stop checking titers Ok for children of pregnant women to get May give with Rhogam, check titer in 3 months
MMWR June 2013

VARICELLA Lab evidence of immunity or
disease Birth in US before 1980 is not
sufficient for pregnant women Diagnosis or verification of
history of varicella or zoster by health care provider Should have link to a typical
case or lab confirmation if testing done during acute infection
Tanya declined the Tdap and flu shot pregnancy because she was afraid of it hurting the baby.
Postpartum she is willing to accept these two immunizations if you still recommend them. She got the flu shot last season and got a Tdap after her last pregnancy in 2011.
Which immunizations would you give her?

TDAP IN EACH PREGNANCY Tdap is indicated in EVERY pregnancy 27-36
wks EGA for transmission of antibodies to fetus Once baby is out, indication for Tdap is based on
maternal indications; she is up to date
Flu shot is indicated
SUMMARY Establish accurate dating Provide primary care
Immunizations, healthy lifestyles Preconception (thyroid adjustment, zika travel)
Watch for pregnancy related diseases Translates to risk of these diseases later in life Some interventions indicated early in pregnancy
We have interventions to prevent perinatal transmission of disease