undescended testes
TRANSCRIPT


0Define the undescended testes.
0Differentiate between the undescended testes , retractile testes .
0 Etiology and complication of the undescended testes.
0Work up and management plan for the undescended testes .

Introduction
0Cryptorchidism is the most common congenital abnormality of the genitourinary tract . Most cryptorchid testes are undescended, but some are absent .
0Cryptorchidism by definition suggests a hidden testis: a testis that is not within the scrotum and does not descend spontaneously into the scrotum by four months of age .

Bilateral undescended
testicles

Cont…
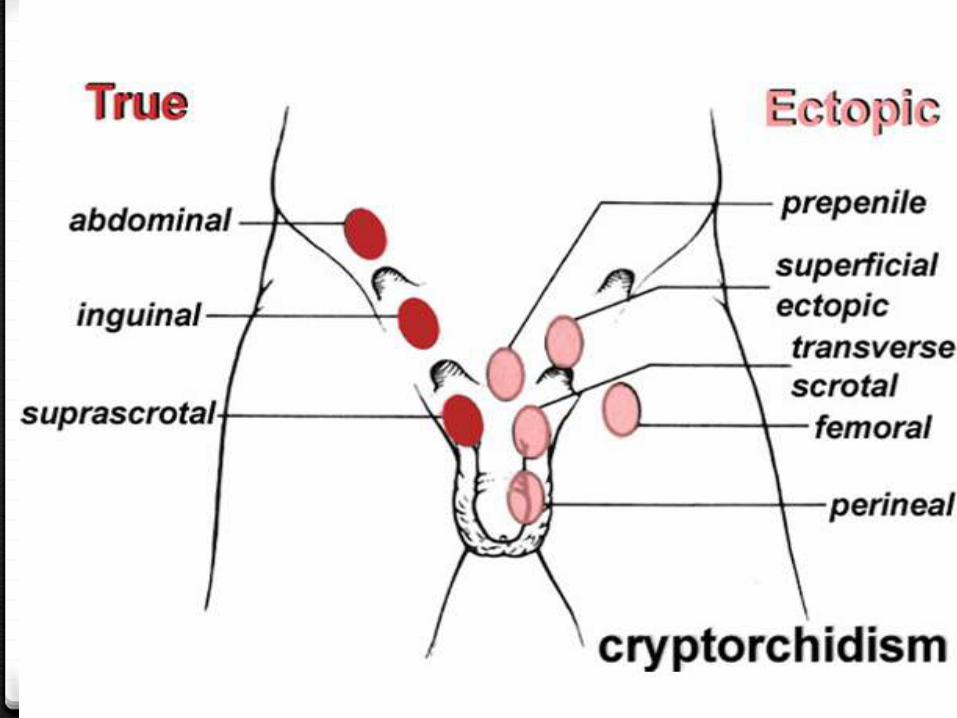
0Undescended testes – True undescended testes have stopped short along their normal path of descent into the scrotum .They may remain in the abdominal cavity (or they may be palpable in the inguinal canal (intracanalicular) or just outside the external ring (suprascrotal) .

Laparoscopic view of
intraabdominal testis

Bilateral suprascrotal
undescended testes

Cont..
0Retractile testes : Retractile testes are normal testes that have been pulled into a suprascrotalposition by the cremasteric reflex.
0 These testes can be brought into a dependent scrotal position and will remain there if the cremasteric reflex is overcome (eg , holding the testis in the scrotum for at least one minute ).

Cont..
0Ascending testes : Ascending testes are noted to be in a scrotal position in early childhood and then to "ascend" and become undescended (ie, acquired undescended testes) .
0 Ectopic testes : Ectopic testes descend normally through the external ring but then are diverted to an aberrant position. They may be palpable in the superficial inguinal pouch (most common), suprapubic region, femoral canal, perineum , or contralateral scrotal compartment (least common).
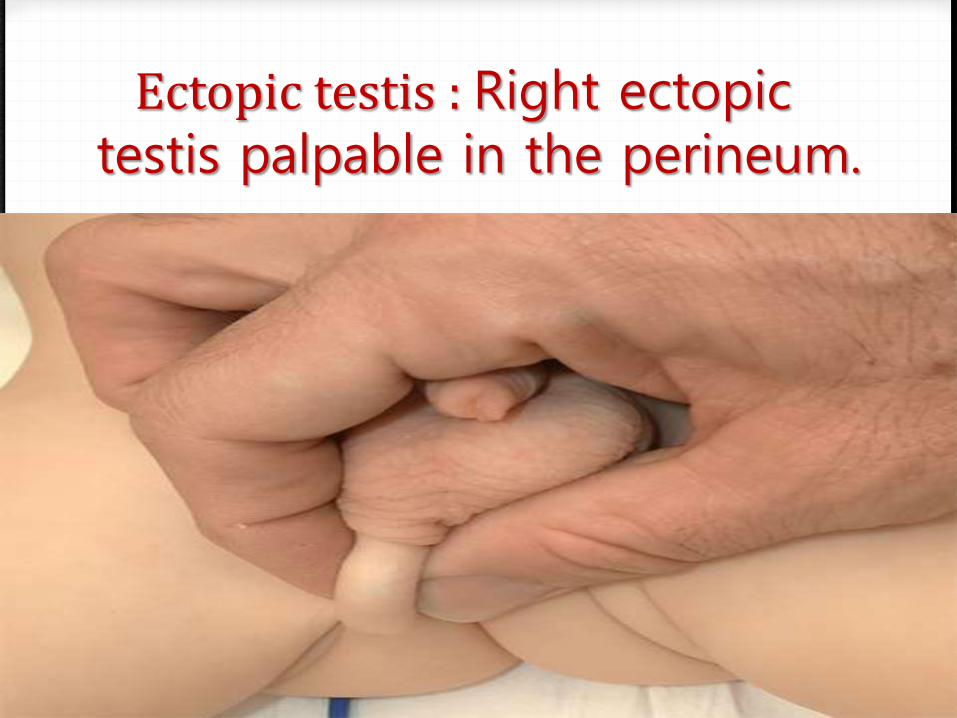
Ectopic testis : Right ectopic testis palpable in the perineum.

Embryology
(A) The testes appear on the urogenital ridge (second month).
(B) The coelomic cavity evaginates into the scrotal swelling where it forms
the processus vaginalis (middle of the third month).
(C) Testes begin descent into the scrotum guided by the gubernaculum
(seventh month).
(D) The processus vaginalis obliterates spontaneously (shortly after birth).
Cont..
0 The mechanisms responsible for normal testicular descent are not well understood.
0 The intraabdominal phase of descent is thought to be androgen-independent and mediated by descendin .
0Passage through the inguinal canal, which begins in the 28th week of gestation, is believed to result from interaction between mechanical, hormonal, and neurotransmitter effects.

Cont..
0Changes in abdominal pressure, patency of the processus vaginalis, gubernacular regression, androgens, gonadotropins, müllerian inhibiting substance (MIS), and calcitonin gene-related peptide are all thought to play a role.
PATHOGENESIS
0 The pathogenesis of undescended testes is less well understood than that of normal testicular descent .
0 Alterations in any of the factors that contribute to normal testicular descent may theoretically result in undescended testes.
0Gonadotropin deficiency in utero, decreased MIS, and increased expression of estradiol in the placenta have been proposed as contributing factors

EPIDEMIOLOGY
0 Between 2 and 5 percent of full-term and approximately 30 percent of premature male infants are born with an undescended testis.
0Most (approximately 70 percent) congenitally undescended testes descend spontaneously.

RISK FACTORS
0Risk factors for undescended testes includeprematurity, and birth weight <2.5 kg .
0Prenatal exposure to endocrine disruptors (eg, diethylstilbestrol, pesticides) also has been associated with cryptorchidism in some studies .
COMPLICATIONS
0 complications and sequelae of undescended testes include inguinal hernia, testicular torsion, testicular trauma, subfertility, and testicular cancer.
0 Surgical repositioning of the testis (orchiopexy) before puberty appears to decrease the risk of testicular cancer, but does not completely eliminate it.


0 Important aspects of the history in a patient with cryptorchidism include :
Whether or not the testes were in a scrotal location in the neonatal period .
Previous inguinal surgery (may be associated with iatrogenic cryptorchidism related to mechanical tethering of the testis or cord in scar tissue).
Evidence of endocrine abnormalities during pregnancy (eg, maternal androgen exposure, which may result in significant virilization of a female fetus).
Family history of unexplained neonatal deaths or genital anomalies, abnormal pubertal development, or infertility.
0 The testicular examination in the infant and young child requires two hands. The hands may be lubricated with surgical lubricant or warm, soapy water if necessary. One hand is placed near the anterior superior iliac spine and the other on the scrotum.
0 The first hand is swept from the anterior iliac spine along the inguinal canal to gently express any retained testicular tissue into the scrotum. A true undescended or ectopic inguinal testis may slide or "pop" under the examiner's fingers during this maneuver.
0 A low ectopic or retractile testis may be felt by the second hand as the testis is milked into the scrotum by the first hand.

Cont…
0 The ectopic testicle will immediately spring out of the scrotum when it is released. The retractile testicle will remain momentarily in the scrotum until further stimulation causes a cremastericreflex.
Cont..
0Differentiation of a retractile testis from a true undescended testis is sometimes difficult; consultation with a urologist may be valuable. Position, consistency and size of the undescended testicle in relation to the opposite testis are noted.
0 If a testis cannot be palpated in the inguinal canal or the scrotum, or in ectopic sites such as the femoral region or perineum, evaluation for a nonpalpable testis must be initiated.
Cont..
0 Sometimes tissue in the scrotum may feel like an atrophic testicle. Occasionally this tissue represents gubernaculum or dissociated epididymis and vas deferens, and may coexist with an intra-abdominal testis. Unless the presence of a testicle is clear, examination by a urologist is indicated.
Cont..
0 In addition to examination of the testes, examination of the genitalia should include assessment of the phallus, position of the urethral meatus, scrotum, and inguinal canal.
Phallus – A small phallus may be a clue to a disorder of sexual development or hypopituitarism.
Urethral meatus – Hypospadias, particularly if the meatus is scrotal or perineal, is associated with disorders of sexual development.

Cont..
0 Scrotum – A hypoplastic or poorly rugated scrotum may indicate decreased likelihood of spontaneous descent , a bifid scrotum may be a clue to a disorder of sexual development.
0 Inguinal canal – The inguinal area should be examined for fullness. Inguinal fullness may be associated with an intracanalicular testis, inguinal hernia, or inguinal lymphadenopathy.
0 Almost 90 percent of undescended testes have an associated patent processus vaginalis .Occult inguinal hernia in boys with untreated undescended testis can present at any time with the typical symptoms or complications, including incarceration.


Imaging
0 Imaging is not routinely warranted to locate nonpalpable testes. Imaging studies lack the sensitivity and the specificity to alter the need for exploratory surgery .
0Ultrasound examination may be advisable in the infant with bilateral nonpalpable testes to look for gonads and to exclude the presence of a uterus, which would suggest a state of intersexuality.
0Ultrasound examination may also be helpful in the overweight child to detect inguinal testicles that are difficult to palpate.

(eg, mixed gonadal dysgenesis)

Mixed gonadal dysgenesis
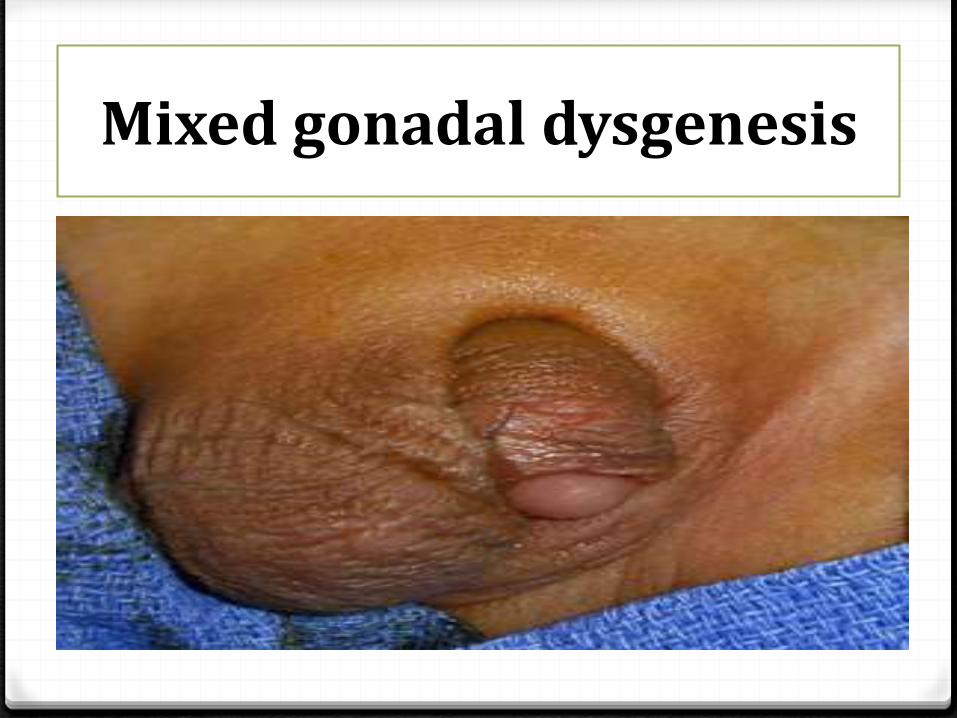
Mixed gonadal dysgenesis
Hormonal therapy
0 Treatment for cryptorchidism can be hormonal, surgical or a combination of the two. Because the process of testicular descent is hormonally mediated, it can sometimes be induced with hormone administration.
0 In the United States, the only hormone labeled for the treatment of cryptorchidism is hCG, which is administered intramuscularly.
0 A high undescended testis is unlikely to descend completely; if it does, it will probably ascend after the hormone stimulation is withdrawn.

Cont..
0 Some side effects of hCG administration can be disturbing for parents. These include enlargement of the penis, pubic hair growth, increased testicular size and aggressive behavior during administration.
0GnRH is not currently labeled for use in the treatment of cryptorchidism in the United States.
0 Testosterone minimally effective . (why )

SURGERY FOR THE UNDESCENDED TESTIS
o Palpable testes :
0Orchiopexy is a well-established surgical procedure for repositioning undescended testes that are palpable . The testis is manipulated into the scrotum and sutured in place.
0
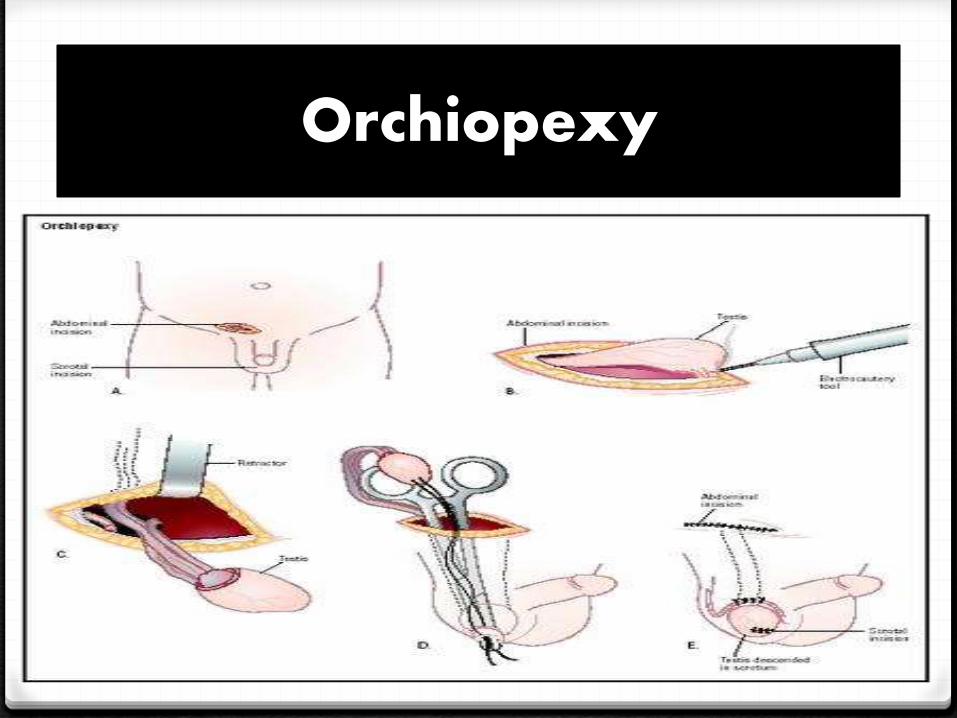
Orchiopexy
Cont..
oNonpalpable testes :0 Exploratory surgery for the nonpalpable testis is
diagnostic and potentially therapeutic. The first surgical objective is to determine whether or not the testis is present; viable testes are positioned and fixed within the scrotum.
0 nonviable testicular remnants are removed. At the time of surgery, approximately 10 percent of boys with nonpalpable testes are found to have blind-ending testicular vessels, indicating an absent testicle .
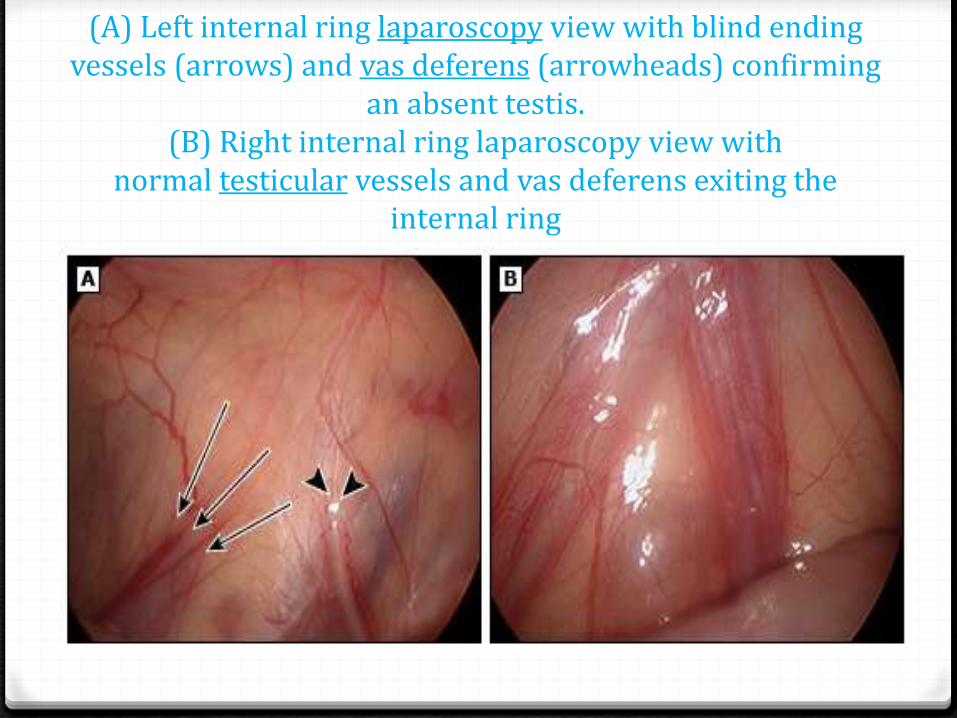
(A) Left internal ring laparoscopy view with blind ending vessels (arrows) and vas deferens (arrowheads) confirming
an absent testis.(B) Right internal ring laparoscopy view with
normal testicular vessels and vas deferens exiting the internal ring

Two surgical approaches are used in the management of boys with nonpalpable testes: the open inguinal approach and the laparoscopic approach.
In the open inguinal approach, the groin is explored. If cord structures or testicular remnants are found, they are removed, and the procedure is terminated. If the groin exploration is negative, the incision is extended, and the peritoneum is entered in a search for an intra-abdominal testis.
Cont..
The diagnostic laparoscopy is a safe procedure in experienced hands . The laparoscope, placed via the umbilicus, is used to examine the inguinal rings, determine the patency of the processusvaginalis, and examine testicular vessels.

Cont..
0 The finding of blind-ending spermatic, confirming the absent testis, permits termination of the procedure without a groin incision. Groin exploration is carried out if testicular vessels and vas deferens are visualized exiting the internal ring.
0 The laparoscopic identification of an intraabdominal testis permits planning for the definitive procedure (eg, open versus laparoscopic).

Summary
0 Most testes that are undescended at birth complete their descent within the first three to four months of life.
0 omplications and sequelae of undescended testes include inguinal hernia, testicular torsion, testicular trauma, subfertility, and testicular cancer.
0 the goal of management is to place and fix viable undescended testes in a normal scrotal position or to remove nonviable testicular remnants.
0 Surgical treatment of congenitally undescended testes is recommended as soon as possible after six months of age and definitely should be completed before the child is two years old. In children with testicular ascent later in childhood, surgery generally should be performed within six months of identification.
Reference