unipolar depression. sad & helpless every day for weeks loss of interests, energy, appetite feel...
TRANSCRIPT
Unipolar Depression
Unipolar Depression
• Sad & helpless every day for weeks
• Loss of interests, energy, appetite
• Feel worthless
• Contemplate suicide
• Difficulty in concentrating
• Restless agitation
• Little or no pleasure from eating or sex

Unipolar Depression• 2 X as often in women as in men
• ~ 5% of adults in US have “clinically significant” depression
• The lifetime risk for Major depressive disorder in community samples has varied from 10% to 25% for women and from 5% to 12% for men.
• Approximately 50%-60% of individuals with major
depressive disorder, single episode, can be expected to
have a second episode. Individuals who have had two
episodes have a 70% chance of having a third, and
individuals who have had three episodes have a 90%
chance of having a fourth.

Unipolar Depression• Relative Risk of MDD is 2-5x greater in relatives of
depressed patients than controls
• A genetic component
– 60% concordance for monozygotic twins
– 20% for dizygotic twins
– Especially for early-onset & among female relatives
– Not a single-gene defect
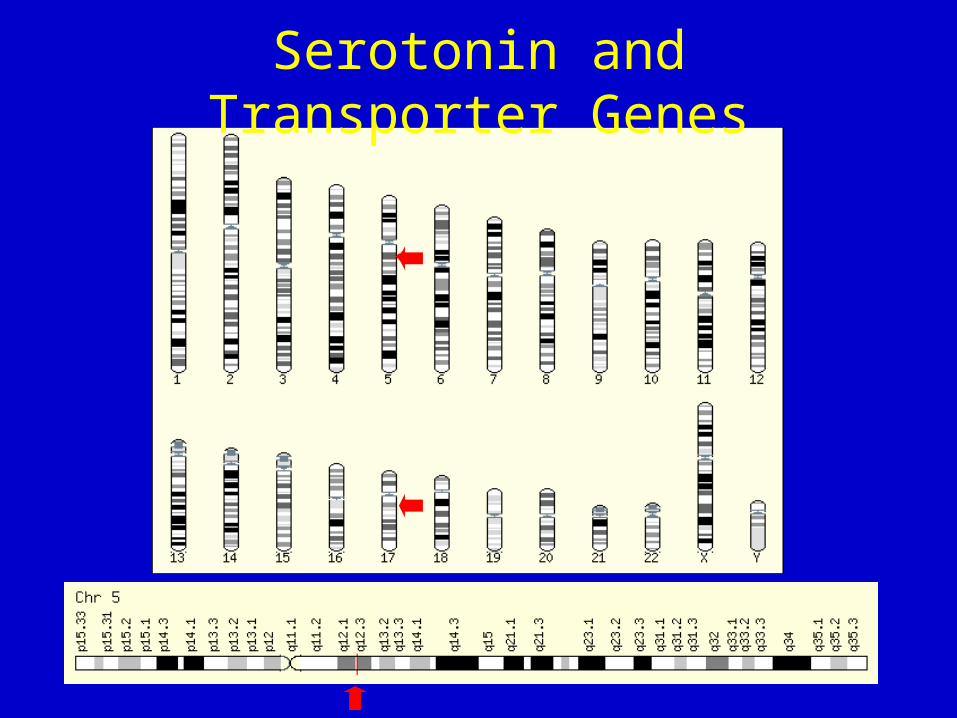

Influence of Life Stress on Depression: Moderation by a Polymorphism in the 5-HTT Gene Caspi et al. Science Vol 301, Issue 5631, 386-389, 2003

DEPRESSION
NORMAL MOOD
RECOVERY OR REMISSION
EPISODE OF DEPRESSIONEPISODE OF DEPRESSION
TIME6 - 24 months

acute 6 - 12 weeks
continuation4-9 months
maintenance1 or more years
REMISSION
RECOVERY
DEPRESSION
NORMAL MOOD
100%
TIME

5-4 Stahl S M, Essential Psychopharmacology (2000)
acute 6 - 12 weeks
continuation4-9 months
maintenance1 or more years
TIME
DEPRESSION
NORMAL MOOD RELAPSE RECURRENCE

5-5 Stahl S M, Essential Psychopharmacology (2000)
DEPRESSION
NORMAL MOOD
MANIA
HYPOMANIA
MIXED EPISODE
5-9 Stahl S M, Essential Psychopharmacology (2000)
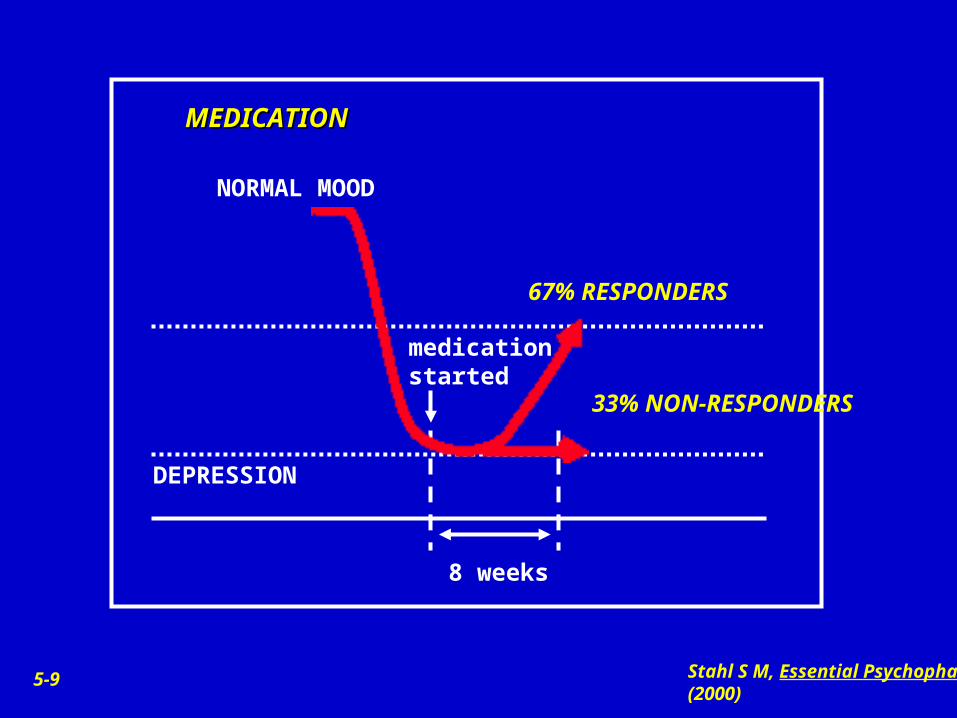
8 weeks
DEPRESSION
NORMAL MOOD
67% RESPONDERS
MEDICATIONMEDICATION
medication started
33% NON-RESPONDERS

5-10 Stahl S M, Essential Psychopharmacology (2000)
8 weeks
DEPRESSION
NORMAL MOOD
33% RESPONDERS
PLACEBOPLACEBO
placebo started
67% NON-RESPONDERS

5-11 Stahl S M, Essential Psychopharmacology (2000)
DEPRESSION
NORMAL MOOD
50% continue response
PLACEBO PLACEBO SUBSTITUTIONSUBSTITUTION
antidepressant treatment
placebo
50% relapse

5-12 Stahl S M, Essential Psychopharmacology (2000)
DEPRESSION
NORMAL MOOD
90% continue response
DRUG DRUG CONTINUATIONCONTINUATION
antidepressant treatment
10% relapse


Monoaminergic Theory of Depression
• Reserpine-(antihypertensive drug) caused depression, depleted monoamine stores in rodent studies
• Iproniazid- (antituburcular drug) elevated mood, blocked degradation of monoamines
• Imipramine-antidepressant effects, blocked reuptake of norepinephrine (and serotonin)
These findings supported the hypothesis that norepinephrine is decreased in depression and elevated with mania and in effective treatments of depression.

Indoleamine Hypothesis of Depression
• Serotonin is functionally deficient in depression– Decreased brain 5-HT and CSF 5-HIAA in
many depressed patients– Antidepressants tend to increase central
serotonin transmission– Depressed patients show reduction in 5-HT
reuptake sites– Blunted neuroendocrine challenges

Neurotransmitter Hypothesis of Mood Disorders
• Led to catecholamine hypothesis– NE ↓ in depression and in mania– 5-HT ↓ production or reuptake in depression
• Flaws: depression or mania not reliably produced and clinical response exceeds mechanism of action of drug
Neurobiology of Mood Disorders
• Neuroendocrine abnormalities: reflect central neurotransmitter dysfunction– hyperactivity of HPA: increased cortisol,
nonsuppression of cortisol in DST– blunting of TSH release following TRH infusion– blunting of GH release with alpha-2 adrenergic
agonism and serotonin-mediated increases in prolactin

Kindling-Sensitization Hypothesis of Mood Disorders
• Suggests that repeated exposure to stress and/or neurochemical changes during depressed episode sensitize brain regions responsible for affect
• Repeated episodes may permanently alter systems within the CNS
• Leads to shorter well periods, increased frequency and severity of illness


MAO enzyme destroying neurotransmitter
monoamine neurotransmitter
NORMAL STATE -- no depression
MONOAMINE HYPOTHESIS
DEPRESSION -- caused by neurotransmitter deficiency

Increase in neurotransmitters causes return to normal state
MAO inhibitor blocks the enzyme from destroying monoamine neurotransmitter
reuptake pump blocked by antidepressant

Norepinephrine Synthesis and Metabolism
Tyrosine L-Dopa Dopamine Norepinephrine
Tyrosine Hydroxylase
Metabolites (MHPG)
Epinephrine
COMT Monoamine oxidase
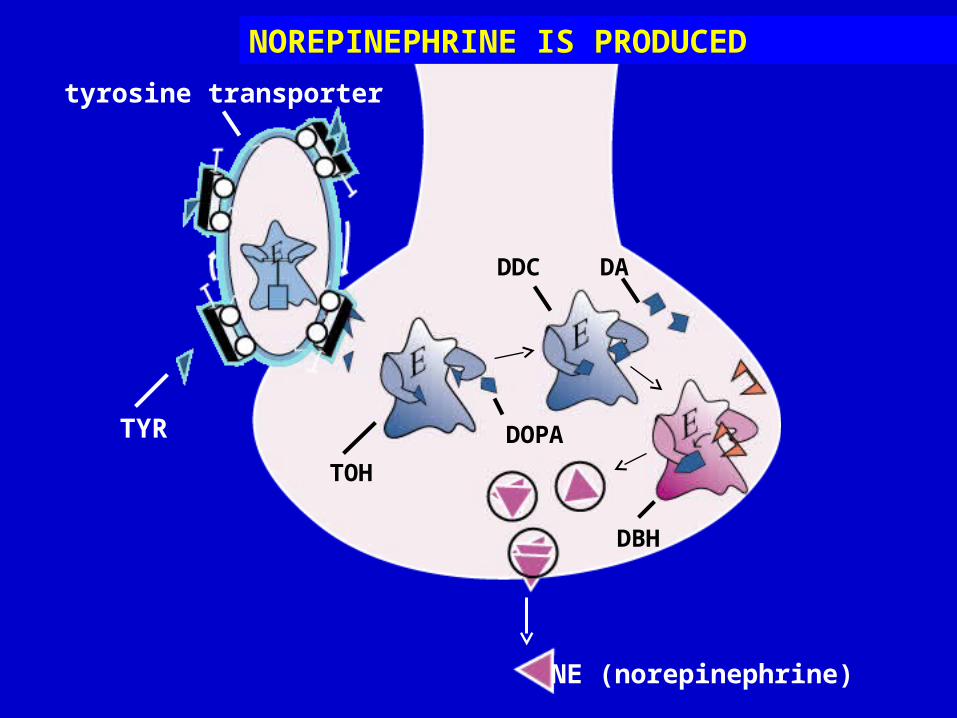
NE (norepinephrine)
tyrosine transporter
TYR
TOH
DOPA
DDC DA
DBH
NOREPINEPHRINE IS PRODUCED

NOREPINEPHRINE IS DESTROYED
COMT destroys NEnorepinephrine
transporter
MAO
Noradrenergic Receptors
• receptors are both presynaptic and postsynaptic; often elevated in depressed patients in platelets and brains of suicide patients
• ß receptors are postsynaptic; often decreased in brains of suicide patients

There can be noradrengeric changes with depressive and anxious disorders
We don’t know if these are the cause of depression or a result of
depression.

NOREPINEPHRINE RECEPTORS
presynaptic alpha 2 autoreceptor
postsynaptic alpha 2
receptorpostsynaptic beta 1 receptor
alpha 1 receptor

terminal alpha 2 autoreceptor
somatodendritic alpha 2
autoreceptor

NE occupying somatodendritic autoreceptor causes a decrease in firing and a decrease of NE release
NE

NE occupying terminal alpha 2 receptor halts release of NE
NE

Norepinephrine Pathways
Locus Coeruleus
beta 1 receptor
DepressionFrontal 1

alpha 2 receptor
Frontal 2 Attention

Limbic
EmotionsAgitationEnergy Level

Dopamine
• Some studies show lower levels of DOPAC and HVA in urinary and CSF samples in depressed patients.
• In contrast, elevated levels of mesolimbic dopamine found in some patients with delusional depression.
• Changes in the HPA axis may lead to changes in dopaminergic system

tyrosine transporter
TOH
TYR
DOPA
DDC
DA (Dopamine)
DOPAMINE IS PRODUCED
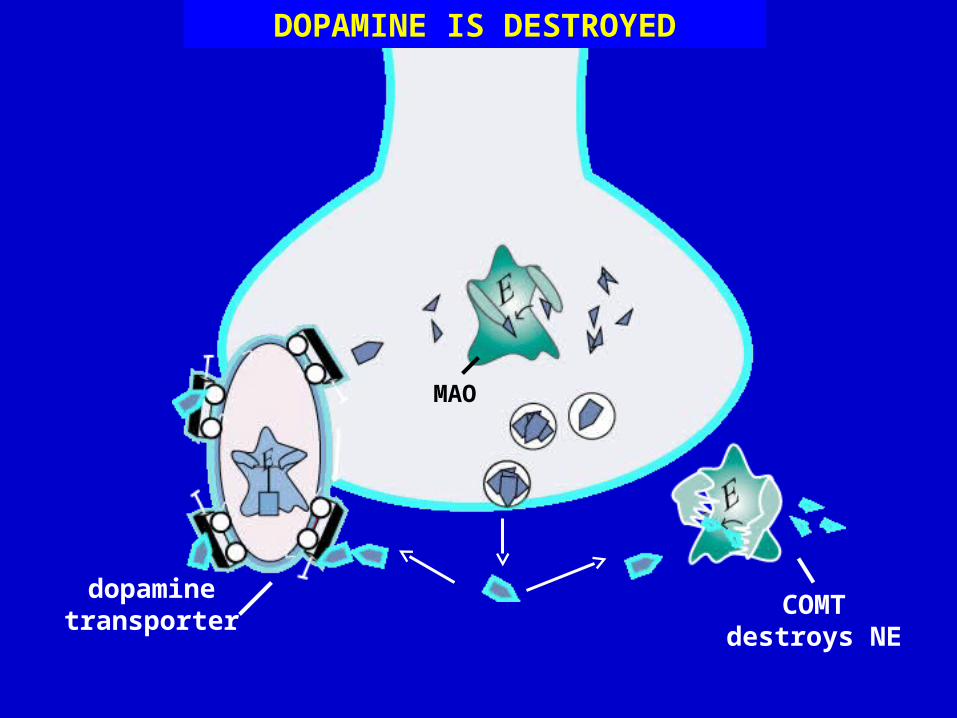
COMT destroys NE
dopamine transporter
MAO
DOPAMINE IS DESTROYED

DOPAMINE RECEPTORS
presynaptic autorecptor
D1 D2 D3 D4 D5
dopamine transporter


Serotonin
Tryptophan
Tryptophan hydroxylase
5-Hydroxytryptophan Serotonin
5-HIAA
Monoamine oxidase
A number of studies find low CSF 5-HIAA levels in depression.
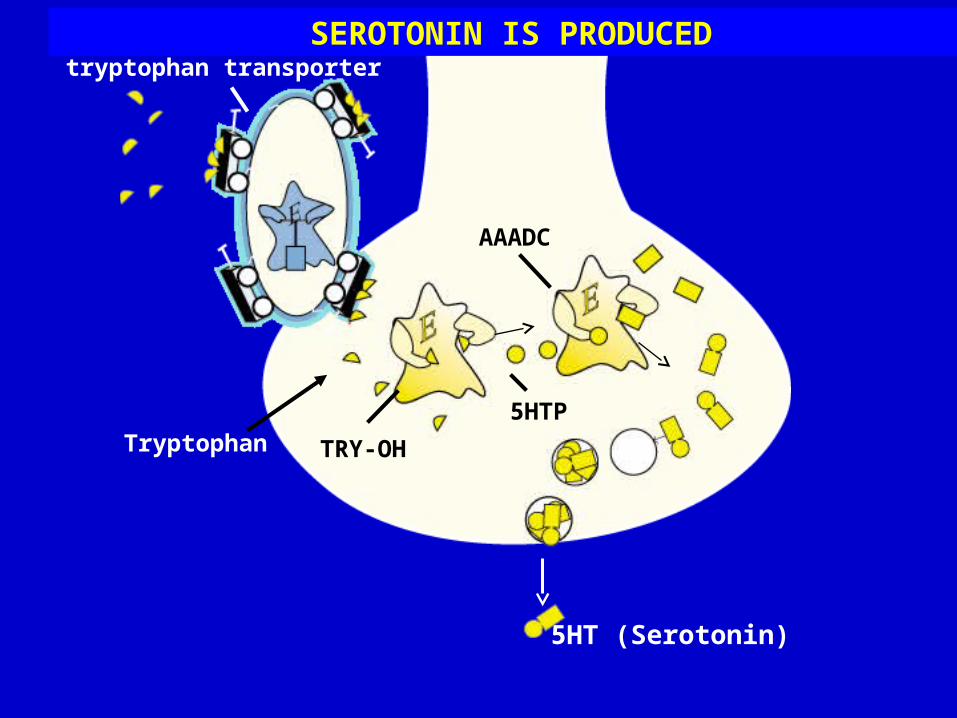
5HT (Serotonin)
SEROTONIN IS PRODUCEDtryptophan transporter
TRY-OH
5HTP
AAADC
Tryptophan
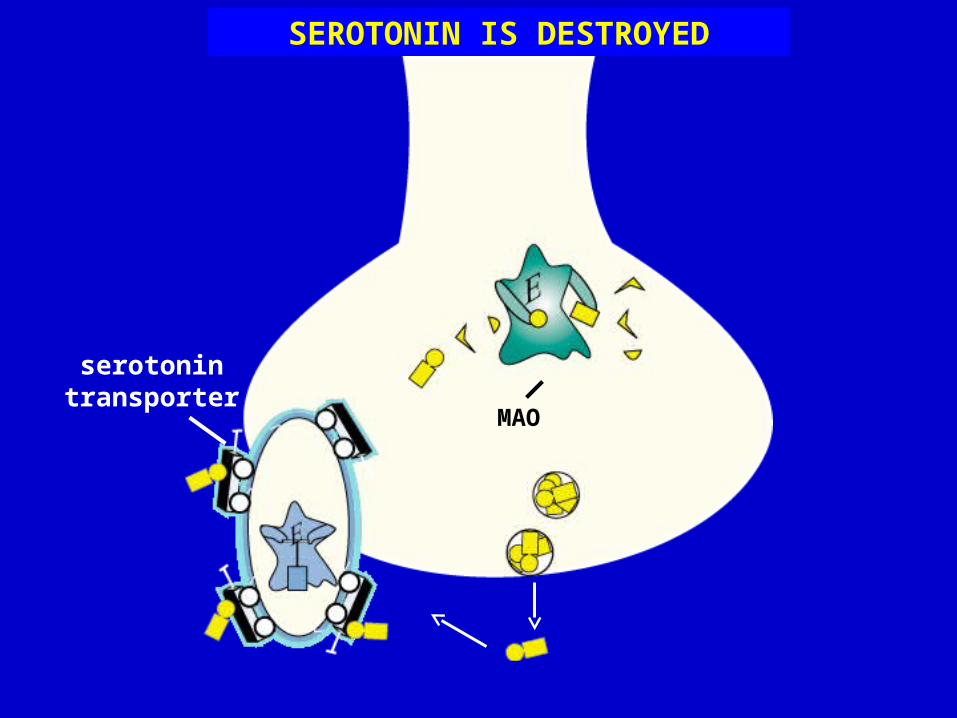
serotonin transporter
MAO
SEROTONIN IS DESTROYED

SEROTONIN RECEPTORS
alpha 2 hetero receptor
5HT1D autoreceptor
5HT1A
serotonin transporter
5HT2A5HT2C
5HT3 5HT45HTX
5HTY
5HTZ


5HT1D

norepinephrine
serotonin
alpha 2 hetero receptor
serotonin neuron

alpha 2 hetero receptor
serotonin neuron

norepinephrine
serotonin
alpha 1 receptor
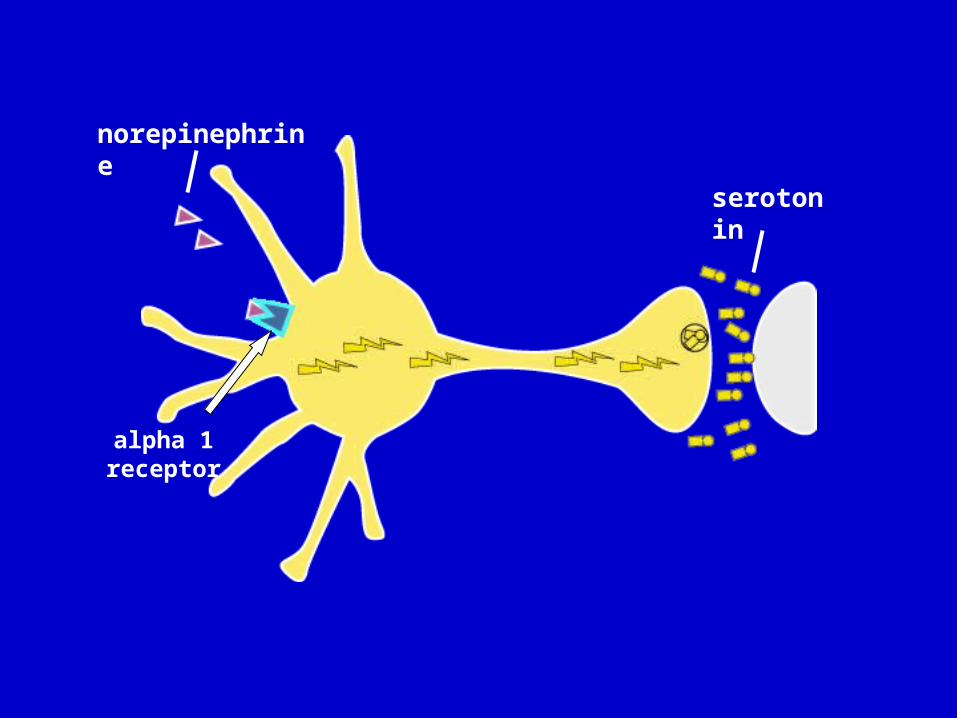
norepinephrine
serotonin
alpha 1 receptor

brake
accelerator
Locus Coeruleus
NE-5HT Interactions

Serotonin Receptors
• 5HT1a receptors are presynaptic and control the release of serotonin from the presynaptic terminal, but there are also post-synaptic 5HT1a receptors.
• Many studies find increased 5HT1a receptors in postmortem brains of depressed suicide patients
• Recent studies show 5HT1a receptor knock-out mice have increased anxious behavior, and “knocking in” the 5HT1a receptor with a cortex-specific promoter ameliorates the anxious behavior.

Serotonin Receptors
• 5HT2a receptors
– Post-synaptic receptor
– Binding to 5HT2a receptors in platelets is increased, particularly related to suicidal tendencies
– Increased number of 5HT2a receptors in post-mortem brain tissue in only some studies

Serotonin Transporter
• Pumps serotonin back into the presynaptic cell
• Decreased SERT activity in platelets of depressed patients, although brain studies less conclusive
• Higher incidence of depression in individuals with short forms of SERT

SSRIs are the most effective antidepressant medications currently
available.
However, screening for effectiveness of SSRIs often does not accurately
predict clinical response.

Serotonin Pathways
Raphe Nucleus
Frontal Cortex Mood

Basal Ganglia OCDAkathisia/Agitation

Limbic Anxiety

Hypothalamus Appetite/bulimia

Sleep Centers Insomnia
Spinal Cord Sexual Dysfunction
