university of groningen erythropoietin in cardiac …these findings imply also a possible...
TRANSCRIPT

University of Groningen
Erythropoietin in cardiac ischemiaLipsic, Erik
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2006
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Lipsic, E. (2006). Erythropoietin in cardiac ischemia. Groningen: [s.n.].
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 15-08-2020

Erythropoietin in cardiac ischemia
The cover illustration depicts the face of Janus, Roman god of gates and beginnings. Janus was frequently used to symbolize change and transition, one
face reflecting on the past while the other face looks forward into the future. In cells, erythropoietin activates JAK (Janus kinase), which contains two
domains critical for signal transduction. The two faces of Janus may also symbolize the “old” hematopoietic and “new” non-hematopoietic functions
of erythropoietin, as well as the two effects of erythropoietin in the heart: inhibition of apoptosis and stimulation of neovascularization.
Financial support by the Groningen University Institute of Drug Exploration (GUIDE) and Van Buchem Stichting for the publication of this thesis is gratefully acknowledged.
ISBN 90-367-2567-4
© Copyright Erik Lipšic, 2006All rights reserved. No part of this publication may be reproduced, or transmitted in any form or by any means, without permission of the author.
Layout: Helga de Graaf, Studio Eye Candy te Groningen. (www.proefschrift.info) Printed by: Ipskamp PrintPartners Enschede, The Netherlands.
RIJKSUNIVERSITEIT GRONINGEN
Erythropoietin in cardiac ischemia
Proefschrift
ter verkrijging van het doctoraat in de Medische Wetenschappen
aan de Rijksuniversiteit Groningenop gezag van de
Rector Magnificus, dr. F. Zwarts,in het openbaar te verdedigen op
maandag 8 mei 2006om 14.45 uur
door
Erik Lipšicgeboren op 8 juli 1973te Bratislava (Slowakije)

Promotores: Prof. Dr. W.H. van Gilst Prof. Dr. D.J. van Veldhuisen
Copromotores: Dr. R.G. Schoemaker Dr. A.A. Voors
Beoordelingscommissie: Prof. Dr. P. Ponikowski Prof. Dr. F. Zijlstra Prof. Dr. A.J. van Zonneveld

Paranimfen: Peter van der Meer Peter Ochodnický
Publication of this thesis was financially supported by: Amgen BV, Astellas Pharma BV, Bayer BV, Boehringer Ingelheim BV, Merck Sharp & Dohme BV, Pfizer BV, Roche Nederland BV, Sanofi-Aventis, Servier Nederland Farma BV, AstraZeneca BV, Janssen-Cilag BV, St. Jude Medical Nederland BV.


Per vivere tranquilli occorrono cinque cose:1. un bicchiere di scienza
2. una bottiglia di sapienza3. un barile di prudenza
4. una botte di coscienza5. un mare di pazienza
S.Alfonso
To the memory of Peter Kubica,exceptional person,
best friend,......we shall overcome.
Contents
Chapter 1 General introduction and aims of the thesis
Chapter 2 Erythropoietin improves left ventricular function and coronary flow in an experimental model of ischemia-reperfusion injury Eur J Heart Fail 2004;6(7):853-9
Chapter 3 Timing of erythropoietin treatment for cardioprotection in ischemia/reperfusion J Cardiovasc Pharmacol 2004;44(4):473-9
Chapter 4 Erythropoietin induces neovascularization and improves cardiac function in rats with heart failure after myocardial infarction J Am Coll Card 2005;46(1):125-33
Chapter 5 Erythropoietin attenuates heart failure in a hematocrit independent manner Submitted
Chapter 6 A single bolus of a long-acting erythropoietin analogue darbepoetin in patients with an acute myocardial infarction: a randomized feasibility and safety study. Cardiovasc Drugs Ther 2006; in press
Chapter 7 Hemoglobin levels and 30-day mortality in patients after myocardial infarction Int J Cardiol 2005;100(2):289-92
Chapter 8 Protective effects of erythropoietin in cardiac ischemia: from bench to bedside (review article) Submitted
Chapter 9 Summary and conclusions
Samenvatting en conclusies
Zhrnutie a záver
Dankwoord
Bibliography
11
21
35
51
69
85
99
109
127
135
141
147
153


Chapter 1
Introduction and aims of the thesis

Chapter 1
12
General introduction and aims of the thesis
Introduction
Myocardial infarction (MI) is the major cause of death in the Western world. Currently, the emphasis in the treatment of MI is on early reperfusion. Although timely reperfusion is a prerequisite for salvaging of myocardium, the restoration of blood flow to previously ischemic cells results in number of deleterious effects referred to as reperfusion injury (1). Additional interventions that preserve the viability during ischemia and reperfusion may further limit the extend of acute MI and improve the clinical outcome (2).Still, myocardial infarction and consequent loss of contractile myocardium is a frequent cause of chronic heart failure (CHF). Approximately half of patients with acute MI would develop heart failure, either during hospital admission or over longer time period (3;4). In the Framingham population, MI accounts for 34% cases of CHF in men and 13% in women (5). Paradoxically, the declining mortality after an acute MI together with improved post-MI therapy, may contribute to the increasing prevalence of CHF (6). Current pharmacological treatment of CHF is focused on suppressing the neurohormonal systems, chronic stimulation of which leads to deterioration of heart function. However, despite this “optimal” therapy, the patients diagnosed with heart failure have a poor prognosis (7). Half of the patients die within 4 years, and in patients with severe heart failure over 50% will die within 1 year (8). Importantly, conventional medical strategies for post-MI heart failure do not attempt to correct the underlying cause (i.e. damaged myocardium), raising a need for strategies aimed at myocardial regeneration and repair (9).
Erythropoietin
Erythropoietin (EPO) is a glycoprotein hormone produced primarily in the kidneys, traditionally known to stimulate hematopoiesis. Synthesis of EPO is upregulated by hypoxia and mediated by hypoxia-inducible factor-1 (HIF-1) (10). In bone marrow, EPO acts on a specific receptor (EPO-R), with subsequent activation of various signaling pathways (STAT5, MAPK, PI3/Akt)(11). Interestingly, rather than stimulating proliferation, activation of these pathways leads to inhibition of programmed cell death (apoptosis) (12). EPO thus acts primarily as a survival factors for erythroid progenitor cells, and in this manner increases the number of mature red blood cells in the circulation. Cloning of human EPO and production of recombinant human EPO (rhEPO) represented a breakthrough in the treatment of anemia caused by EPO deficiency due to chronic kidney disease (13). At present, rhEPO is approved also for treatment of anemia caused by other conditions, including anemia associated with chemotherapy, HIV antiviral treatment or to reduce the need for transfusion in perioperative surgical patients (14). Recently, a novel erythropoiesis stimulating factor (NESP, darbepoetin) has been synthesized (15), containing higher content of carbohydrates than rhEPO, rendering this molecule a longer plasma half-life with obvious advantages regarding administration frequency.
Introduction
13
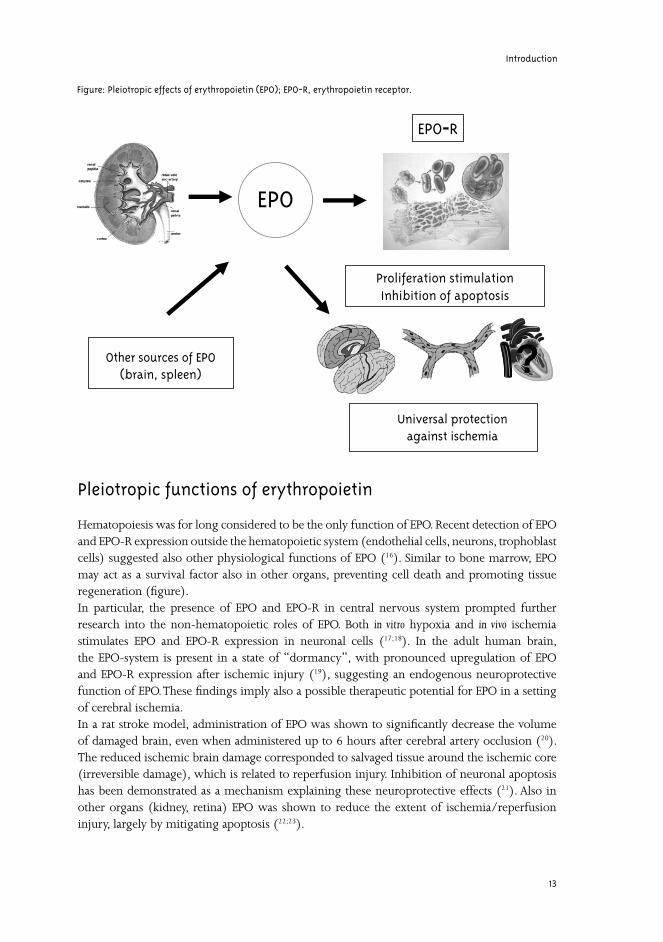
Pleiotropic functions of erythropoietin
Hematopoiesis was for long considered to be the only function of EPO. Recent detection of EPO and EPO-R expression outside the hematopoietic system (endothelial cells, neurons, trophoblast cells) suggested also other physiological functions of EPO (16). Similar to bone marrow, EPO may act as a survival factor also in other organs, preventing cell death and promoting tissue regeneration (figure). In particular, the presence of EPO and EPO-R in central nervous system prompted further research into the non-hematopoietic roles of EPO. Both in vitro hypoxia and in vivo ischemia stimulates EPO and EPO-R expression in neuronal cells (17;18). In the adult human brain, the EPO-system is present in a state of “dormancy”, with pronounced upregulation of EPO and EPO-R expression after ischemic injury (19), suggesting an endogenous neuroprotective function of EPO. These findings imply also a possible therapeutic potential for EPO in a setting of cerebral ischemia.In a rat stroke model, administration of EPO was shown to significantly decrease the volume of damaged brain, even when administered up to 6 hours after cerebral artery occlusion (20). The reduced ischemic brain damage corresponded to salvaged tissue around the ischemic core (irreversible damage), which is related to reperfusion injury. Inhibition of neuronal apoptosis has been demonstrated as a mechanism explaining these neuroprotective effects (21). Also in other organs (kidney, retina) EPO was shown to reduce the extent of ischemia/reperfusion injury, largely by mitigating apoptosis (22;23).
EPO
EPO-R
Proliferation stimulationInhibition of apoptosis
?Other sources of EPO(brain, spleen)
Universal protectionagainst ischemia
Figure: Pleiotropic effects of erythropoietin (EPO); EPO-R, erythropoietin receptor.

Chapter 1
14
Protection against ischemia and reperfusion injury in the heart
Infarct size is a major determinant of prognosis in patients after acute MI (24). Early reperfusion with percutaneous coronary stenting or thrombolytic therapy remains so far the best strategy to reduce infarct size (2) and is associated with improved short and long-term survival (25). However, reperfusion may be viewed as a “double edged sword”, as it may initiate additional myocardial injury beyond that generated by ischemia alone (26). This is referred to as “reperfusion injury” and is manifested by myocardial stunning, endothelial dysfunction and irreversible cellular damage (27). Animal models of sustained ischemia have shown exacerbation of myocardial injury during reperfusion, mediated largely by cytotoxic effects of free radical generation, complement activation, shifts in substrate use and inflammation (28). These changes occur both within the already irreversibly damaged myocardium, but reperfusion may also lead to conversion from reversible to irreversible injury in a population of severely impaired myocytes (29).Two forms of cell death are implicated during ischemia and reperfusion in the heart, namely necrosis and apoptosis (1). Although the exact contribution of these two forms of death is still under discussion, apoptosis progressively develops and accelerates during the reperfusion (30;31). Furthermore, apoptosis has been detected in the heart not only during acute MI, but may also contribute to progressive loss of surviving cells during subacute and chronic ischemic stages (32). Targeting anti-apoptotic mechanisms of cellular protection at the time of reperfusion may therefore offer a potential approach to attenuate reperfusion-induced cell death (33). In conclusion, although early reperfusion with primary coronary intervention and stenting in the management of acute MI salvages greater amount of myocardium than is irreversibly damaged by reperfusion injury, additional cell protection may provide even greater benefits in terms of infarct size reduction and improvements in clinical outcome.
Repair of the failing heart
Recently, a decades old dogma declaring an inability of myocardial regeneration has been revised. Experimental studies and early-phase clinical trials have made the futuristic dream of heart repair an achievable therapeutic goal (9). Several concepts for cardiac repair have been proposed, among which implantation of cells capable to replace cardiomyocytes and/or myocardial vasculature (9). The most promising results have been obtained with recruitment of bone marrow-derived stem cells into the area of infarction. Although transdifferentiation of these cells into cardiomyocytes has been suggested (34), it appears very limited in an in vivo situation and other mechanisms seem more plausible. Stem cells may release paracrine mediators that inhibit apoptosis or enhance endogenous repair mechanisms in the heart (35). Most likely, stem cells may stimulate neovascularization, leading to augmented oxygen tissue supply. Neovascularization may be mediated by physical incorporation of bone marrow-derived endothelial progenitor cells (EPCs) into new capillaries (36) or by angiogenic cytokines (VEGF) secreted from these cells that potentiate angiogenic activity of endogenous cells (37). EPCs stimulated neovascularization of the peri-infarct zone in the heart was shown to prevent ventricular remodeling and improve cardiac function (38;39).Although the mechanism of stem (progenitor) cells therapy is far from being understood, numerous clinical studies with bone marrow-derived cells have already been performed.

Introduction
15
Besides establishing safety and feasibility, preliminary efficacy data also suggest that stem cell therapy has the potential to improve myocardial perfusion and contractile function in patients after acute MI, coronary artery disease or heart failure (35). In the BOOST trial, intracoronary infusion of autologous bone marrow cells after myocardial infarction improved the global left ventricular ejection fraction 6 months after cell transfer (40). However, other trials have provided conflicting results with many open questions, and cautiousness in rapid translation of experimental results to clinical situation is warranted. If there exists also an opposite direction from bench to bedside, it should be probably (at least partly) applied in this field. Erythropoietin was also shown to mobilize EPCs from bone marrow and enhance ischemia-induced neovascularization (41). In addition, EPO may also promote new capillary formation from preexisting vessels into ischemic area (42). Capillary growth has been observed in rat aortic rings after incubation with EPO (43) and also in endothelial cells derived from myocardial tissue (44).
Aims of the thesis
This thesis focuses on the non-hematopoietic effects of EPO in the heart. The two main aims of the experimental part of this thesis were:
1. To establish the presence and functionality of EPO system in the heart and to further study the effect of EPO administration on cardiac ischemia/reperfusion injury.
2. To investigate the influence of EPO treatment on neovascularization in a postischemic heart failure.
Therefore we employed experimental models of ischemia/reperfusion injury (chapter 2,3) and post-MI heart failure (chapter 4,5). Furthermore, we aimed to elucidate the mechanisms associated with both acute and chronic effects of EPO in the heart. Importantly, we seeked to separate the hematopoietic and non-hematopoietic effects of EPO treatment on heart structure and function. In the clinical part of the thesis, we intended to translate the results of the experimental studies into first clinical, randomized study to assess the safety and feasibility of EPO administration in patients with acute MI (chapter 6).Because anemia is associated with worse prognosis in heart failure and stable coronary artery disease, in chapter 7 we studied the prognostic value of low hemoglobin levels on short-term mortality in patients with acute MI. Chapter 8 summarizes the “state-of-art” of EPO-mediated cardioprotection and presents future perspectives on this clinically relevant topic.

Chapter 1
16
Reference List1. Yellon DM, Baxter GF. Protecting the ischaemic and reperfused myocardium in acute myocardial infarction:
distant dream or near reality? Heart. 2000;83:381-387.
2. Kloner RA, Rezkalla SH. Cardiac protection during acute myocardial infarction: where do we stand in 2004? J Am Coll Cardiol. 2004;44:276-286.
3. Cleland JG, Torabi A, Khan NK. Epidemiology and management of heart failure and left ventricular systolic dysfunction in the aftermath of a myocardial infarction. Heart. 2005;91 Suppl 2:ii7-13.
4. Hellermann JP, Jacobsen SJ, Redfield MM et al. Heart failure after myocardial infarction: clinical presentation and survival. Eur J Heart Fail. 2005;7:119-125.
5. Kannel WB. Incidence and epidemiology of heart failure. Heart Fail Rev. 2000;5:167-173.
6. Guidry UC, Evans JC, Larson MG et al. Temporal trends in event rates after Q-wave myocardial infarction: the Framingham Heart Study. Circulation. 1999;100:2054-2059.
7. Weir R, McMurray JJ. Treatments that improve outcome in the patient with heart failure, left ventricular systolic dysfunction, or both after acute myocardial infarction. Heart. 2005;91 Suppl 2:ii17-ii20.
8. Swedberg K, Cleland J, Dargie H et al. Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26:1115-1140.
9. Dimmeler S, Zeiher AM, Schneider MD. Unchain my heart: the scientific foundations of cardiac repair. J Clin Invest. 2005;115:572-583.
10. Ebert BL, Bunn HF. Regulation of the erythropoietin gene. Blood. 1999;94:1864-1877.
11. Smith KJ, Bleyer AJ, Little WC et al. The cardiovascular effects of erythropoietin. Cardiovasc Res. 2003;59:538-548.
12. Wojchowski DM, Gregory RC, Miller CP et al. Signal transduction in the erythropoietin receptor system. Exp Cell Res. 1999;253:143-156.
13. Lin FK, Suggs S, Lin CH et al. Cloning and expression of the human erythropoietin gene. Proc Natl Acad Sci USA. 1985;82:7580-7584.
14. Henry DH, Bowers P, Romano MT et al. Epoetin alfa. Clinical evolution of a pleiotropic cytokine. Arch Intern Med. 2004;164:262-276.
15. Macdougall IC. Novel erythropoiesis stimulating protein. Semin Nephrol. 2000;20:375-381.
16. Ribatti D, Vacca A, Roccaro AM et al. Erythropoietin as an angiogenic factor. Eur J Clin Invest. 2003;33:891-896.
17. Bernaudin M, Marti HH, Roussel S et al. A potential role for erythropoietin in focal permanent cerebral ischemia in mice. J Cereb Blood Flow Metab. 1999;19:643-651.
18. Lewczuk P, Hasselblatt M, Kamrowski-Kruck H et al. Survival of hippocampal neurons in culture upon hypoxia: effect of erythropoietin. Neuroreport. 2000;11:3485-3488.

Introduction
17
19. Siren AL, Knerlich F, Poser W et al. Erythropoietin and erythropoietin receptor in human ischemic/hypoxic brain. Acta Neuropathol (Berl). 2001;101:271-276.
20. Brines ML, Ghezzi P, Keenan S et al. Erythropoietin crosses the blood-brain barrier to protect against experimental brain injury. Proc Natl Acad Sci U S A. 2000;97:10526-10531.
21. Siren AL, Fratelli M, Brines M et al. Erythropoietin prevents neuronal apoptosis after cerebral ischemia and metabolic stress. Proc Natl Acad Sci U S A. 2001;98:4044-4049.
22. Junk AK, Mammis A, Savitz SI et al. Erythropoietin administration protects retinal neurons from acute ischemia-reperfusion injury. Proc Natl Acad Sci U S A. 2002;99:10659-10664.
23. Sharples EJ, Patel N, Brown P et al. Erythropoietin protects the kidney against the injury and dysfunction caused by ischemia-reperfusion. J Am Soc Nephrol. 2004;15:2115-2124.
24. Perez-Gonzalez J, Botvinick EH, Dunn R et al. The late prognostic value of acute scintigraphic measurement of myocardial infarction size. Circulation. 1982;66:960-971.
25. Van Domburg RT, Sonnenschein K, Nieuwlaat R et al. Sustained benefit 20 years after reperfusion therapy in acute myocardial infarction. J Am Coll Cardiol. 2005;46:15-20.
26. Braunwald E, Kloner RA. Myocardial reperfusion: a double-edged sword? J Clin Invest. 1985;76:1713-1719.
27. Moens AL, Claeys MJ, Timmermans JP et al. Myocardial ischemia/reperfusion-injury, a clinical view on a complex pathophysiological process. Int J Cardiol. 2005;100:179-190.
28. Cannon RO, III. Mechanisms, management and future directions for reperfusion injury after acute myocardial infarction. Nat Clin Pract Cardiovasc Med. 2005;2:88-94.
29. Buja LM. Myocardial ischemia and reperfusion injury. Cardiovasc Pathol. 2005;14:170-175.
30. Zhao ZQ, Velez DA, Wang NP et al. Progressively developed myocardial apoptotic cell death during late phase of reperfusion. Apoptosis. 2001;6:279-290.
31. Scarabelli T, Stephanou A, Rayment N et al. Apoptosis of endothelial cells precedes myocyte cell apoptosis in ischemia/reperfusion injury. Circulation. 2001;104:253-256.
32. Takemura G, Fujiwara H. Role of apoptosis in remodeling after myocardial infarction. Pharmacol Ther. 2004; 104:1-16.
33. Hausenloy DJ, Yellon DM. New directions for protecting the heart against ischaemia-reperfusion injury: targeting the Reperfusion Injury Salvage Kinase (RISK)-pathway. Cardiovasc Res. 2004;61:448-460.
34. Orlic D, Kajstura J, Chimenti S et al. Bone marrow cells regenerate infarcted myocardium. Nature. 2001; 410:701-705.
35. Wollert KC, Drexler H. Clinical applications of stem cells for the heart. Circ Res. 2005;96:151-163.
36. Jackson KA, Majka SM, Wang H et al. Regeneration of ischemic cardiac muscle and vascular endothelium by adult stem cells. J Clin Invest. 2001;107:1395-1402.
37. Yoshioka T, Ageyama N, Shibata H et al. Repair of infarcted myocardium mediated by transplanted bone marrow-derived CD34+ stem cells in a nonhuman primate model. Stem Cells. 2005;23:355-364.
Chapter 1
18
38. Kawamoto A, Tkebuchava T, Yamaguchi J et al. Intramyocardial transplantation of autologous endothelial progenitor cells for therapeutic neovascularization of myocardial ischemia. Circulation. 2003;107:461-468.
39. Schuster MD, Kocher AA, Seki T et al. Myocardial neovascularization by bone marrow angioblasts results in cardiomyocyte regeneration. Am J Physiol Heart Circ Physiol. 2004;287:H525-H532.
40. Wollert KC, Meyer GP, Lotz J et al. Intracoronary autologous bone-marrow cell transfer after myocardial infarction: the BOOST randomised controlled clinical trial. Lancet. 2004;364:141-148.
41. Heeschen C, Aicher A, Lehmann R et al. Erythropoietin is a potent physiologic stimulus for endothelial progenitor cell mobilization. Blood. 2003;102:1340-1346.
42. Marti HH, Bernaudin M, Petit E et al. Neuroprotection and Angiogenesis: Dual Role of Erythropoietin in Brain Ischemia. News Physiol Sci. 2000;15:225-229.
43. Carlini RG, Reyes AA, Rothstein M. Recombinant human erythropoietin stimulates angiogenesis in vitro. Kidney Int. 1995;47:740-745.
44. Jaquet K, Krause K, Tawakol-Khodai M et al. Erythropoietin and VEGF exhibit equal angiogenic potential. Microvasc Res. 2002;64:326-333.


Chapter 2
Erythropoietin improves left ventricular function and coronary flow in an
experimental model of ischemia-reperfusion
injury
Peter van der Meer, Erik Lipšic, Robert H. Henning, Rudolf A. de Boer,
Albert J.H. Suurmijer, Dirk J. van Veldhuisen, Wiek H. van Gilst
European Journal of Heart Failure 2004;6:853-9

Chapter 2
22
Abstract
Background: Recent studies show that erythropoietin (EPO) plays a protective role in brain ischemia. In this condition, administration of EPO protects neurons from ischemic damage. Recently, it has been shown that in patients with chronic heart failure (CHF), EPO treatment improved cardiac function. In the present study we assessed the role of EPO and EPO-receptor (EPO-R) in the heart.Methods and Results: We studied the presence and functionality of the EPO-R in isolated rat hearts in the Langendorff set-up. Hearts were perfused for 20 minutes with 10 U/ml EPO or vehicle. Immunohistochemistry revealed the presence of the EPO-R on endothelial cells, fibroblasts and to a lesser extent cardiomyocytes. Furthermore, perfusion with EPO resulted in a 50% increase in the phosphorylated MAP kinases p42/p44. To evaluate the protective role of EPO in cardiac ischemia, we performed low-flow (0.6 ml/min) ischemia/reperfu-sion experiments in isolated rat hearts. Administration of EPO (10 U/ml) reduced the cel-lular damage by 56% (p<0.05) during reperfusion, diminished apoptosis by 15% (p<0.05) and resulted in a significantly improved recovery of left ventricular pressure (p=0.02) and coronary flow (p=0.01).Conclusion: The present data suggest that a functional EPO-R is present in rat adult cardiac tissue and that exogenous EPO administration improves cardiac function after ischemia/re-perfusion injury.
Introduction
In response to ischemia, mammalian cells express a variety of proteins, including erythro-poietin (EPO) and vascular endothelial growth factor (VEGF) (1). The regulation of these two proteins is mediated by hypoxia inducible factor 1 (HIF-1). Expression of HIF-1 increases exponentially, as cellular O
2 concentrations decrease (1;2). Erythropoietin (EPO) is a glyco-
protein hormone, primarily produced in the kidney. It mediates the physiological response to hypoxia by increasing red blood cell production. However, expanding evidence suggests that EPO also plays a major role in non-erythropoietic processes. Several reports showed its efficacy in brain and retinal diseases (3-5). A study in rats subjected to cerebral ischemia showed a significant reduction in brain infarct size (5;6). Specificity and biological relevance of these changes were demonstrated by the observation that neutraliza-tion of endogenous EPO with soluble EPO-R augments ischemic brain damage (7). During ischemia, the EPO-receptor (EPO-R) is locally upregulated in brain tissue (8). After binding with its receptor, EPO signals through various intracellular pathways, including the MAP p42/p44 and JAK2-STAT5 tyrosine kinases (9). It was recently shown that activation of these pathways by EPO resulted in anti-apoptotic effect in various tissues including brain, retinal cells and erythroid precursor cells (3;10;11). Little is known about the presence and protective role of EPO and its receptor in the heart. Juul et al, have described the presence of EPO and EPO-R in human fetal cardiac tissue (12). Experiments with knock-out mice, deficient for the genes expressing EPO and EPO-R, pro-vide more evidence for its role in cardiac tissue, as both EPO-/- and EPO-R-/- mice suffer from ventricular hypoplasia and abnormalities in the vascular network (13). Silverberg et al, have shown that EPO treatment, in patients with CHF, results in an increased left ventricular ejec-

Erythropoietin improves cardiac function
23
tion fraction, as compared with the placebo control group and there is a growing interest in this subject in the last few years (14;15). The present study was designed to examine the presence and functionality of the EPO-R in adult cardiac tissue. In addition, we evaluated the protective effects of exogenous EPO admin-istration in ischemia/reperfusion injury in the isolated rat heart.
Methods
Study designLangendorff experiments were performed in isolated rat hearts that were perfused with EPO (10 U/ml) or vehicle for 20 minutes. These hearts were used to determine the expression and localization of EPO-R, and common signaling pathways were explored. To determine the protective effects of EPO treatment on ischemia/reperfusion injury, we studied 2 experimen-tal groups (each consisting of 6 rats): ischemia/reperfusion without EPO and ischemia/re-perfusion with EPO.
Langendorff perfusionThis well established experimental set-up has been described earlier (11;16-19). In short, rats were anaesthetised with isoflurane in O
2/N
2 and 500 U of heparin were injected in the tail
vein. The heart was rapidly excised and the aorta was immediately perfused retrogradely by a modified Tyrode solution (glucose 10, NaCl 128.3, KCl 4.7, NaHCO
3 20.2, CaCl
2 1.35,
NaH2PO
4 0.42, MgCl
2 1.05; all mmol/liter) and was equilibrated with 95% O
2 and 5% CO
2.
Perfusion pressure was maintained at 60 mmHg. Coronary flow (CF) was measured by a microprocessor, which controlled the perfusion pressure by adjusting a peristaltic perfusion pump. CF and left ventricular pressure (LVP) were monitored continuously. After equilibrat-ing for 15 minutes, hearts were subjected to low flow ischemia (0.6 ml/min) for 40 min-utes, followed by a 2 hours reperfusion period at a constant 60 mmHg perfusion pressure. EPO (10 U/ml) or vehicle was administered from stabilization throughout the protocol. All the experiments conform with the Guide for the Care and Use of Laboratory Animals pub-lished by the US National Institutions of Health.
Analysis of coronary effluentDuring stabilization (t=5 minutes), ischemia (t=20, t=30 and t=54 minutes) and reperfu-sion (t=55, t=56, t=57, t=60, t=70, t=90, t=120 and t=150 minutes), coronary perfusate samples were collected. Purines, a sensitive indicator of myocardial ischemia, were deter-mined by high-performance liquid chromatography (HPLC) as previously described (20;21). The total amount of purines released during ischemia and reperfusion, corrected for coro-nary flow and left ventricular weight, was calculated (area under the curve).
RT-PCR Snap-frozen LV tissues were used to extract total RNA. Total RNA was isolated using the method of acid guanidium thiocyanate lysis (22). RNA was quantified using a GeneQuant II (Pharmacia Biotechnology). First strand cDNA was synthesized from 1 μg RNA using the RT-PCR Core kit (Perkin-Elmer). Reverse transcriptase (RT) PCR for EPO-R was performed using a forward (5’- AGGACACCTACCTGGTATTGGA-3’) and reverse primer (5’-CAGGCCCAGAGA-

Chapter 2
24
GGTTCTCA-3’), yielding a product of 73 bp. To determine the specificity of the PCR reaction the amplicon was digested with Nci I to obtain the expected 39 bp and 34 bp fragments.
Western blottingSnap frozen LV tissues were homogenized in Radio-Immuno-Precipitation-Assay (RIPA) buf-fer (1% NP40, 0.5% sodium deoxycholate, 0.1% sodium dodecyl sulfate (SDS), 10 mM -mercaptoethanol, 10 mg/ml PMSF, 5 μl/ml aprotinin, 100 mM sodium orthovanadate, 5 μl/ml benzamidine, 5 μl/ml pepstatine A, 5 μl/ml leupeptine in 1× PBS). Protein concen-trations were determined using the DC assay (Bio-Rad) with a bovine albumin standard. Protein levels of EPO-R, phosphorylated MAP kinases p42/p44 and phosphorylated STAT5 were determined by Western blot. Protein samples (50 μg) were separated by sodium do-decyl sulfate–polyacrylamide gel electrophoresis (SDS–PAGE) and transferred to nitrocel-lulose membranes, followed by staining with Ponceau S solution (Sigma). Membranes were incubated with primary antibody against phosphorylated MAP kinases p42/p44 (1:1000 dilution, New England Biolabs), phosphorylated STAT5 (1:1000 dilution, Upstate biotech) and EPO-R (1:250 dilution; C-20 and M-20, Santa Cruz Biotechnology). Horseradish per-oxidase-conjugated anti-mouse or anti-rabbit IgG (1:2000, Santa Cruz Biotechnology) was used as secondary antibody. Signals were detected by the ECL-detection method (Amersham) and quantified by densitometry.
ImmunohistochemistryFor immunohistochemistry, cryosections (4 μm) from a midpapillary slice of the left ven-tricle were fixed in acetone. Hereafter, sections were incubated with two different polyclonal anti-EPO-R antibodies (1:50) (M-20, C-20; Santa Cruz). A two-step indirect peroxidase de-tection system was employed to visualize the expression pattern of the EPO-R. Sections of placenta and breast carcinoma were used as a positive control (23;24). Slides omitting the primary antibody and preincubation with blocking peptide (10:1) were used as negative controls. For apoptosis detection, sections were incubated with an antibody that specifically recognizes the active form of caspase-3 (1:50; New England Biolabs), as previously reported (25). For quantitative analysis, active caspase-3 positive cells in thirty random fields per section (80-120 cells per field) were counted at high-power magnification. Tissue sections of colonic adenocarcinoma served as a positive control (26;27).
Statistical AnalysisValues shown are mean ± SEM. We used a linear regression model with repeated measures to compare the functional responses to EPO treatment. Data regarding the purine overflow and caspase-3 immunohistochemistry were analyzed by Student’s t-test. Statistical significance was defined as p<0.05.
Erythropoietin improves cardiac function
25
Results
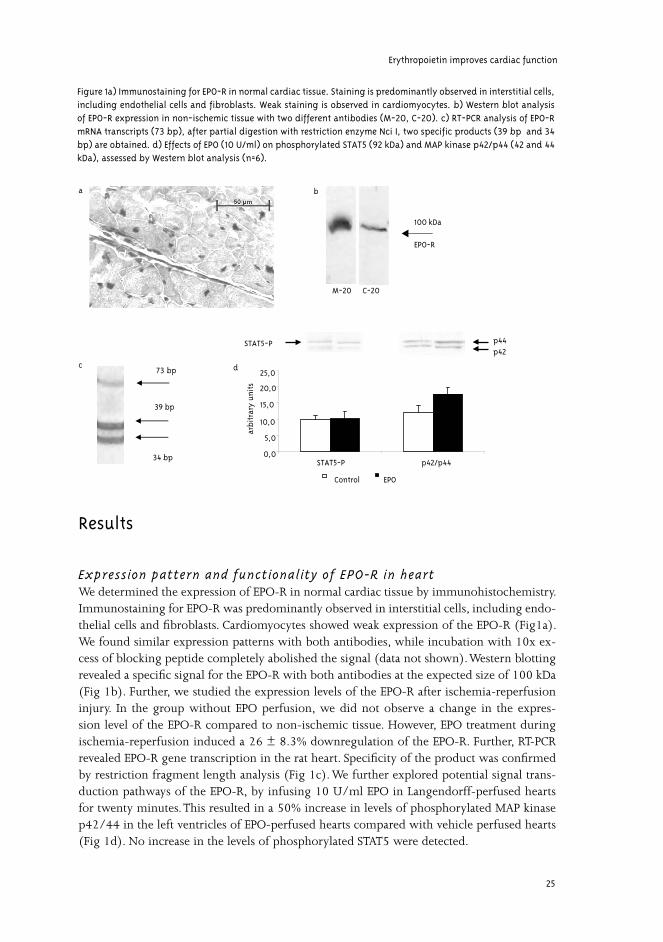
Expression pattern and functionality of EPO-R in heartWe determined the expression of EPO-R in normal cardiac tissue by immunohistochemistry. Immunostaining for EPO-R was predominantly observed in interstitial cells, including endo-thelial cells and fibroblasts. Cardiomyocytes showed weak expression of the EPO-R (Fig1a). We found similar expression patterns with both antibodies, while incubation with 10x ex-cess of blocking peptide completely abolished the signal (data not shown). Western blotting revealed a specific signal for the EPO-R with both antibodies at the expected size of 100 kDa (Fig 1b). Further, we studied the expression levels of the EPO-R after ischemia-reperfusion injury. In the group without EPO perfusion, we did not observe a change in the expres-sion level of the EPO-R compared to non-ischemic tissue. However, EPO treatment during ischemia-reperfusion induced a 26 ± 8.3% downregulation of the EPO-R. Further, RT-PCR revealed EPO-R gene transcription in the rat heart. Specificity of the product was confirmed by restriction fragment length analysis (Fig 1c). We further explored potential signal trans-duction pathways of the EPO-R, by infusing 10 U/ml EPO in Langendorff-perfused hearts for twenty minutes. This resulted in a 50% increase in levels of phosphorylated MAP kinase p42/44 in the left ventricles of EPO-perfused hearts compared with vehicle perfused hearts (Fig 1d). No increase in the levels of phosphorylated STAT5 were detected.
M-20 C-20
100 kDa
EPO-R
ba
p44p42
STAT5-P
0,0
5,0
10,0
15,0
20,0
25,0
STAT5-P p42/p44
arbi
trar
yun
its
EPOControl
d73 bp
39 bp
c
34 bp
Figure 1a) Immunostaining for EPO-R in normal cardiac tissue. Staining is predominantly observed in interstitial cells, including endothelial cells and fibroblasts. Weak staining is observed in cardiomyocytes. b) Western blot analysis of EPO-R expression in non-ischemic tissue with two different antibodies (M-20, C-20). c) RT-PCR analysis of EPO-R mRNA transcripts (73 bp), after partial digestion with restriction enzyme Nci I, two specific products (39 bp and 34 bp) are obtained. d) Effects of EPO (10 U/ml) on phosphorylated STAT5 (92 kDa) and MAP kinase p42/p44 (42 and 44 kDa), assessed by Western blot analysis (n=6).
Chapter 2
26
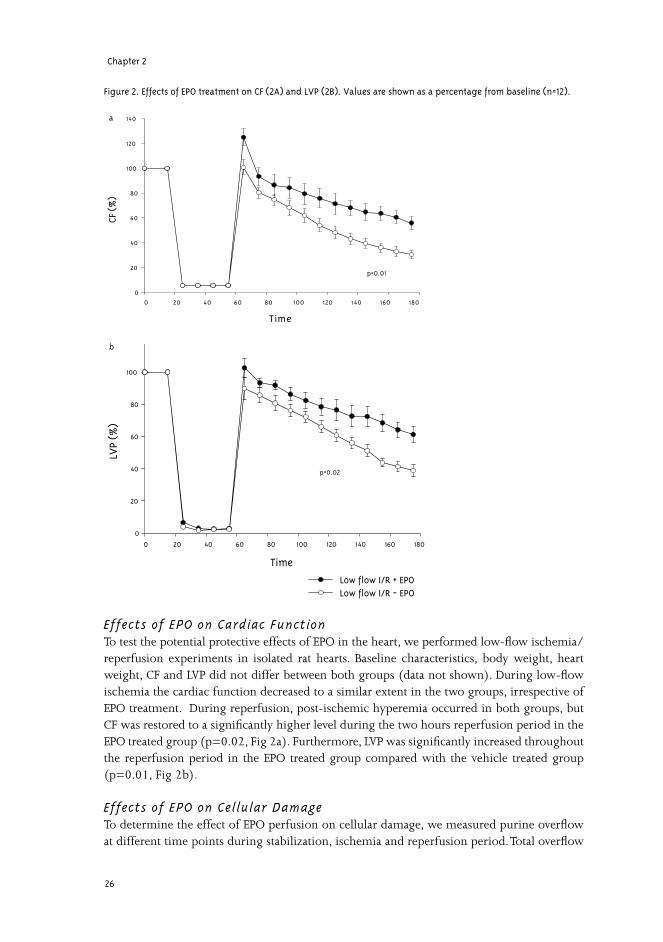
Effects of EPO on Cardiac FunctionTo test the potential protective effects of EPO in the heart, we performed low-flow ischemia/reperfusion experiments in isolated rat hearts. Baseline characteristics, body weight, heart weight, CF and LVP did not differ between both groups (data not shown). During low-flow ischemia the cardiac function decreased to a similar extent in the two groups, irrespective of EPO treatment. During reperfusion, post-ischemic hyperemia occurred in both groups, but CF was restored to a significantly higher level during the two hours reperfusion period in the EPO treated group (p=0.02, Fig 2a). Furthermore, LVP was significantly increased throughout the reperfusion period in the EPO treated group compared with the vehicle treated group (p=0.01, Fig 2b).
Effects of EPO on Cellular DamageTo determine the effect of EPO perfusion on cellular damage, we measured purine overflow at different time points during stabilization, ischemia and reperfusion period. Total overflow
Figure 2. Effects of EPO treatment on CF (2A) and LVP (2B). Values are shown as a percentage from baseline (n=12).
Time
0 20 40 60 80 100 120 140 160 180
LVP
(%)
0
20
40
60
80
100
120
Low flow I/R + EPOLow flow I/R - EPO
Time
0 20 40 60 80 100 120 140 160 180
CF (
%)
0
20
40
60
80
100
120
140
p=0.01
b
p=0.02
a

Erythropoietin improves cardiac function
27
of purines during reperfusion showed a 56% decrease (711 ± 183 nmol/g versus 1614 ± 317 nmol/g) (p<0.05) in the EPO treated group, compared with the vehicle treated hearts. A smaller difference was observed during the ischemic period between the EPO perfused hearts and the control group, 660 ± 53 nmol/g versus 898 ± 200 nmol/g, respectively (p=NS; Fig 3). No purines were detected at baseline. Furthermore, we studied the anti-apoptotic effects of EPO perfusion on the heart. Staining with anti-active caspase-3 was mostly restricted to endothelial cells and fibroblasts (Fig 4a). The hearts perfused with EPO demonstrated a 15% reduction in apoptotic cells (2.1% ± 0.12 versus 1.8% ± 0.09) (p<0.05, Fig 4b).
Discussion
In the present study, we demonstrated the presence of a functional EPO-R in adult cardiac tissue and we showed that EPO administration limited cardiac damage and preserved cardiac function after ischemia/reperfusion injury. However, the mechanism by which EPO pre-serves cardiac function is currently unknown. We found that EPO stimulation increases the levels of phosphorylated MAP kinases p42/p44 in normal rat heart. This pathway has already been implicated as a survival pathway in cardiac cells after ischemia/reperfusion injury, by inhibiting apoptosis (28-30). A study by Yue et al. pro-vided more evidence for the role of MAP kinases in ischemia/reperfusion injury by demon-strating that inhibition of the MAP kinases p42/p44 pathway exacerbated cardiac injury and showed a diminished functional recovery compared with control hearts (31). Thus, activation of this pathway seems to be important for survival of cardiac cells by protecting them from programmed cell death. With respect to STAT5, we did not observe difference in the amount of phosphorylated STAT5 after EPO perfusion for twenty minutes. This might be related to
Figure 3. Effect of EPO perfusion on total purine overflow during ischemia and reperfusion (area under the curve). Purines are a marker for ATP breakdown and therefore an indicator of reversible and irreversible damage to the myocardium (n=12).
I s c h e m i a R e p e r f u s i o n
Puri
ne o
verf
low
(ng
/ml)
0
2 0 0
4 0 0
6 0 0
8 0 0
1 0 0 0
1 2 0 0
1 4 0 0
1 6 0 0
1 8 0 0
2 0 0 0
+ E P O- E P O
p < 0.05

Chapter 2
28
different time-points of STAT5 phosphorylation after perfusion with EPO. Furthermore, this pathway could play a minor role in the cardiac EPO signaling, as shown in vascular smooth muscle cells by Ammarguellat et al (32). Future experiments will be needed to precisely ex-plore the EPO signaling pathways in the heart.Both ischemic and reperfused myocardium can undergo apoptosis, however, during reperfu-sion, accelerated apoptosis occurs in cardiac cells (33). We observed that EPO limits cardiac damage by 56% during reperfusion. A recent paper from Scarabelli et al. showed that in the early stages of reperfusion, apoptosis is first seen in endothelial cells and is spreading to sur-rounding cardiac myocytes, suggesting that reperfusion induces the release of pro-apoptotic mediators from endothelial cells (34). We found that the EPO-R was predominantly localized to endothelial cells and fibroblasts. Interestingly, we observed in these cells a reduction in apoptosis of 15%, when the hearts were perfused with EPO. By preventing apoptosis in these cells, it is tempting to speculate that EPO can preserve vascular flow and ultimately protect the
Apop
toti
c ce
lls (
%)
0,0
1,0
1,5
2,0
2,5
+ EPO- EPO
p < 0.05b
a
Figure 4a) Immunostaining for active caspase-3 in ischemic cardiac tissue without EPO treatment. b) Percentage of ac-tive caspase-3 positive cells at the end of reperfusion in isolated rat hearts perfused with or without EPO and subjected to 40 min. of low-flow ischemia and 2 hours of reperfusion (n=12).

Erythropoietin improves cardiac function
29
myocardium. Although a reduction of 15% in apoptotic cells seems modest, recent investiga-tions suggest that apoptosis after myocardial infarction is progressive, and therefore small amounts of apoptotic cells may result in more extensive cell loss (35). Recent data reported on the beneficial effects of preconditioning in the rodent heart in which exposure of wild-type mice to intermittent hypoxia resulted in protection from ischemia-reperfusion injury (36). Ischemic preconditioning was absent in mice heterozygous for a knockout in the HIF-1α gene. Further, in wild-type mice, EPO administration at 24 hours prior to ex vivo ischemia-re-perfusion resulted in a reduction in apoptosis and an increased cardiac recovery. While these findings are in accordance with our results the present study suggests that there is no need for an extended period of pretreatment with EPO to exert its protective effects.In addition to its anti-apoptotic effects, EPO may protect the myocardium through other mechanisms that have not been assessed in this work. Oxidative stress plays an important role in the reperfusion damage observed in the myocardium (37). Recent research suggests that EPO can also directly protect tissue against the effects of free radicals (38). Furthermore, it has been shown that EPO may increase the nitric oxide (NO) production when EPO-in-duced erythrocytosis occurs, reviewed by Smith et al.(39). Transgenic mice overexpressing human erythropoietin showed higher NO synthase levels and an increased NO-mediated endothelium derived relaxation (40). On the other hand, Noguchi et al showed that one-week of erythropoietin treatment in rabbits resulted in a decreased response to endothelium dependent vasodilators (41). EPO has also been shown to act as a cardioprotective agent, by modulating the cardiac Na+-K+-pump (42). EPO has been widely used in clinical practice for more than a decade. A recent study of Sil-verberg et al. showed the beneficial effects of rh-EPO therapy in CHF patients (14). They con-ducted a placebo controlled study in 32 mild anemic patients with severe CHF (NYHA ≥III) and treated them with rh-EPO. Over a mean of 8.2 +/- 2.6 months, left ventricular ejection fraction increased by 5.5% in the treatment group, compared to a decrease of 5.4% in the control group. These results strongly suggest an important role for rh-EPO in patients with CHF. Although correction of anemia has beneficial effects on cardiac function, non-erythro-poietic effects are also likely to play a role. More evidence for non-erythropoietic effects of EPO in human was provided by Ehrenreich et al. (43). They recently conducted a pilot double blind randomized clinical trial to investigate the acute effects of EPO treatment in patients with ischemic stroke. Administration of EPO within 8 hrs after stroke reduced brain infarct size and improved the clinical outcome. As there are many similarities between brain and heart ischemia, EPO administration may become an adjunctive therapy for the treatment of acute coronary syndromes. Further work is needed to determine the mechanisms by which EPO reduces cardiac damage and preserves cardiac function.In conclusion, this study suggests that EPO treatment is effective in reducing myocardial damage and preserving cardiac function after ischemia/reperfusion injury. This implies an organ protective role of EPO beyond erythropoiesis and warrants the search for organ spe-cific EPO analogues.
AcknowledgmentsThe authors thank Egbert Scholtens, Cécile Driessen, Kristien Boddeus and Jacko Duker for expert technical assistance. Peter van der Meer is supported by NWO ZonMW. Erik Lipšic is supported by GUIDE.
Chapter 2
30
Reference List1. Shweiki D, Itin A, Soffer D, Keshet E. Vascular endothelial growth factor induced by hypoxia may mediate
hypoxia-initiated angiogenesis. Nature 1992;359:843-5.
2. Wang GL, Jiang BH, Rue EA, Semenza GL. Hypoxia-inducible factor 1 is a basic-helix-loop-helix-PAS het erodimer regulated by cellular O2 tension. Proc Natl Acad Sci U S A 1995;92:5510-4.
3. Grimm C, Wenzel A, Groszer M et al. HIF-1-induced erythropoietin in the hypoxic retina protects against light-induced retinal degeneration. Nat Med 2002;8:718-24.
4. Chong ZZ, Kang JQ, Maiese K. Erythropoietin is a novel vascular protectant through activation of Akt1 and mitochondrial modulation of cysteine proteases. Circulation 2002;106:2973-9.
5. Siren AL, Fratelli M, Brines M et al. Erythropoietin prevents neuronal apoptosis after cerebral ischemia and metabolic stress. Proc Natl Acad Sci U S A 2001;98:4044-9.
6. Brines ML, Ghezzi P, Keenan S et al. Erythropoietin crosses the blood-brain barrier to protect against experimental brain injury. Proc Natl Acad Sci U S A 2000;97:10526-31.
7. Sakanaka M, Wen TC, Matsuda S et al. In vivo evidence that erythropoietin protects neurons from ischemic damage. Proc Natl Acad Sci U S A 1998;95:4635-40.
8. Siren AL, Knerlich F, Poser W, Gleiter CH, Bruck W, Ehrenreich H. Erythropoietin and erythropoietin receptor in human ischemic/hypoxic brain. Acta Neuropathol (Berl) 2001;101:271-6.
9. Haq R, Halupa A, Beattie BK, Mason JM, Zanke BW, Barber DL. Regulation of erythropoietin-induced STAT serine phosphorylation by distinct mitogen-activated protein kinases. J Biol Chem 2002;277:17359-66.
10. Chong ZZ, Kang JQ, Maiese K. Hematopoietic factor erythropoietin fosters neuroprotection through novel signal transduction cascades. Journal of Cerebral Blood Flow and Metabolism 2002;22:503-14.
11. Ratajczak J, Majka M, Kijowski J et al. Biological significance of MAPK, AKT and JAK-STAT protein ac-tivation by various erythropoietic factors in normal human early erythroid cells. Br. J. Haematol 2001; 115:195-204
12. Juul SE, Yachnis AT, Christensen RD. Tissue distribution of erythropoietin and erythropoietin receptor in the developing human fetus. Early Hum Dev 1998;52:235-49.
13. Wu H, Lee SH, Gao J, Liu X, Iruela-Arispe ML. Inactivation of erythropoietin leads to defects in cardiac morphogenesis. Development 1999;126:3597-605.
14. Silverberg DS, Wexler D, Sheps D et al. The effect of correction of mild anemia in severe, resistant con-gestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study. J Am Coll Cardiol 2001;37:1775-80.
15. Silverberg DS, Wexler D, Iaina A. The importance of anemia and its correction in the management of severe congestive heart failure. Eur J Heart Fail 2002;4:681-6.
16. Sato M, Engelman RM, Otani H et al. Myocardial protection by preconditioning of heart with losartan, an angiotensin II type 1-receptor blocker: implication of bradykinin- dependent and bradykinin-inde-pendent mechanisms. Circulation 2000;102:III346-III351.
17. Pinto YM, Bader M, Pesquero JB et al. Increased kallikrein expression protects against cardiac ischemia. FASEB J 2000;14:1861-3.

Erythropoietin improves cardiac function
31
18. Nawata T, Takahashi N, Ooie T, Kaneda K, Saikawa T, Sakata T. Cardioprotection by streptozotocin-induced diabetes and insulin against ischemia/reperfusion injury in rats. J Cardiovasc Pharmacol 2002;40:491-500.
19. De Jonge R, Out M, Maas WJ, De Jong JW. Preconditioning of rat hearts by adenosine A(1) or A(3) receptor activation. Eur J Pharmacol 2002;441:165-72.
20. Backstrom T, Goiny M, Lockowandt U, Liska J, Franco-Cereceda A. Cardiac outflow of amino acids and purines during myocardial ischemia and reperfusion. J Appl Physiol 2003;94:1122-8.
21. Van Gilst WH, De Graeff PA, Kingma JH, Wesseling H, De Langen CD. Captopril reduces purine loss and reperfusion arrhythmias in the rat heart after coronary artery occlusion. Eur J Pharmacol 1984;100:113-7.
22. Chomczynski P, Sacchi N. Single-step method of RNA isolation by acid guanidinium thiocyanate- phe-nol-chloroform extraction. Anal Biochem 1987;162:156-9.
23. Conrad KP, Benyo DF, Westerhausen-Larsen A, Miles TM. Expression of erythropoietin by the human placenta. FASEB J 1996;10:760-8.
24. Acs G, Zhang PJ, Rebbeck TR, Acs P, Verma A. Immunohistochemical expression of erythropoietin and erythropoietin receptor in breast carcinoma. Cancer 2002;95:969-81.
25. De Boer RA, van Veldhuisen DJ, van der WJ et al. Additional use of immunostaining for active caspase 3 and cleaved actin and PARP fragments to detect apoptosis in patients with chronic heart failure. J Card Fail 2000;6:330-7.
26. Jonges LE, Nagelkerke JF, Ensink NG et al. Caspase-3 activity as a prognostic factor in colorectal carci-noma. Lab Invest 2001;81:681-8.
27. Yang L, Cao ZH, Yan H, Wood WC. Coexistence of high levels of apoptotic signaling and inhibitor of apoptosis proteins in human tumor cells: Implication for cancer specific therapy. Cancer Research 2003;63:6815-24.
28. Schulman D, Latchman DS, Yellon DM. Urocortin protects the heart from reperfusion injury via upregu-lation of p42/p44 MAPK signaling pathway. Am J Physiol Heart Circ Physiol 2002;283:H1481-H1488.
29. Sheng Z, Knowlton K, Chen J, Hoshijima M, Brown JH, Chien KR. Cardiotrophin 1 (CT-1) inhibition of cardiac myocyte apoptosis via a mitogen-activated protein kinase-dependent pathway. Divergence from downstream CT-1 signals for myocardial cell hypertrophy. J Biol Chem 1997;272:5783-91.
30. Zu YL, Ai Y, Gilchrist A et al. High expression and activation of MAP kinase-activated protein kinase 2 in cardiac muscle cells. J Mol Cell Cardiol 1997;29:2159-68.
31. Yue TL, Wang C, Gu JL et al. Inhibition of extracellular signal-regulated kinase enhances Ischemia/Reoxy-genation-induced apoptosis in cultured cardiac myocytes and exaggerates reperfusion injury in isolated perfused heart. Circ Res 2000;86:692-9.
32. Ammarguellat F, Llovera M, Kelly PA, Goffin V. Low doses of EPO activate MAP kinases but not JAK2-STAT5 in rat vascular smooth muscle cells. Biochem Biophys Res Communtions 2001;284:1031-8.
33. Fliss H, Gattinger D. Apoptosis in ischemic and reperfused rat myocardium. Circ Res 1996;79:949-56.
34. Scarabelli T, Stephanou A, Rayment N et al. Apoptosis of endothelial cells precedes myocyte cell apoptosis in ischemia/reperfusion injury. Circulation 2001;104:253-6.
Chapter 2
32
35. Sam F, Sawyer DB, Chang DL et al. Progressive left ventricular remodeling and apoptosis late after myo-cardial infarction in mouse heart. Am J Physiol Heart Circ Physiol 2000;279:H422-H428.
36. Cai Z, Manalo DJ, Wei G et al. Hearts from rodents exposed to intermittent hypoxia or erythropoietin are protected against ischemia-reperfusion injury. Circulation 2003;107:107-13.
37. Dhalla NS, Elmoselhi AB, Hata T, Makino N. Status of myocardial antioxidants in ischemia-reperfusion injury. Cardiovasc Res 2000;47:446-56.
38. Chattopadhyay A, Choudhury TD, Bandyopadhyay D, Datta AG. Protective effect of erythropoietin on the oxidative damage of erythrocyte membrane by hydroxyl radical. Biochem Pharmacol 2000;59:419-25.
39. Smith KJ, Bleyer AJ, Little WC, Sane DC. The cardiovascular effects of erythropoietin. Cardiovasc Res 2003;59:538-48.
40. Ruschitzka FT, Wenger RH, Stallmach T et al. Nitric oxide prevents cardiovascular disease and determines survival in polyglobulic mice overexpressing erythropoietin. Proc Natl Acad Sc USA 2000;97:11609-13.
41. Noguchi K, Yamashiro S, Matsuzaki T et al. Effect of 1-week treatment with erythropoietin on the vascu-lar endothelial function in anaesthetized rabbits. British J Pharmacol 2001;133: 395-405.
42. Sterin-Borda L, Barcelo AC, Bozzini CE. Erythropoietin improves cardiac contractility in post-hypoxic mice. Br J Haematol 2003;121:180-6.
43. Ehrenreich H, Hasselblatt M, Dembowski C et al. Erythropoietin therapy for acute stroke is both safe and beneficial. Mol Med 2002;8:495-505.


Chapter 3
Timing of erythropoietin treatment for
cardioprotection in ischemia/reperfusion
Erik Lipšic, Peter van der Meer, Robert H. Henning, Albert J.H. Suurmeijer,
Kristien M. Boddeus, Dirk J. van Veldhuisen, Wiek H. van Gilst, Regien G. Schoemaker
Journal of Cardiovascular Pharmacology 2004;44(4):473-9
Chapter 3
36
Abstract
Erythropoietin (EPO) is a hormone known to stimulate hematopoiesis. However, recent research suggests additional properties of EPO, such as protection against ischemia/reperfusion (I/R) injury in various tissues. We studied the effect of timing of EPO administration on cardioprotection during I/R in the heart. Male Sprague-Dawley rats were subjected to 45 minutes of coronary occlusion, followed by 24-hours of reperfusion. Animals were randomized to receive saline or single dose of EPO (5.000 IU/kg) either 2 hours before I/R, at the start of ischemia or after the onset of reperfusion. The ratio of infarct area/area at risk (planimetry), left ventricular (LV) function (pressure development) and apoptosis (number of active caspase-3 positive cells) were determined after 24-hour reperfusion. Administration of EPO during different time points resulted in a 19-23 % (p<0.05) reduction in the infarct area/area at risk, which was accompanied by a trend towards better LV hemodynamic parameters. Apoptosis was significantly attenuated in groups treated with EPO at the start of ischemia (29% reduction) and after the onset of reperfusion (38%), and to a lesser extent (16%) in the group pre-treated with EPO. Thus, in vivo administration of EPO at different time points protects the myocardial structure and preserves cardiac function during I/R. Cardioprotective effect of EPO is associated with inhibition of apoptosis.
Introduction
Erythropoietin (EPO) is an endogenous hematopoietic hormone produced by the kidney in response to hypoxia. EPO targets erythroid progenitor cells in bone marrow to increase the number of mature red blood cells (1). Rather than directly stimulating the proliferation, EPO inhibits the apoptosis of erythroid precursor cells (2). Independent of its hematopoietic effect, EPO was recently shown to be protective in vascular disease (3). Furthermore, systemic administration of EPO to rats subjected to cerebral ischemia/reperfusion (I/R) resulted in a significant reduction in brain infarct size (4). Application of EPO was beneficial also in the setting of hypoxic retinal disease (5) and renal ischemic injury (6). Protection against apoptosis was implicated as a possible mechanism of the observed EPO effects (7;8), suggesting the extension of EPO anti-apoptotic property to other tissues. Both in vitro and in vivo, EPO has been shown to activate a number of signaling kinases (Akt, MAP-kinase, STAT-5) associated with the prevention of apoptosis (9;10). Accordingly, activation of these pathways during cardiac ischemia was reported to have cytoprotective effects (11).Recently, evidence is accumulating for a protective role of EPO during ischemia in the heart. In isolated cardiomyocytes, EPO was shown to protect against hypoxia-induced apoptosis, through an Akt-dependent pathway (9). Pre-treatment with EPO increased functional recovery and decreased apoptosis in isolated rat hearts subjected to I/R 24-hours later (12). In a study performed by our group, perfusion with EPO during ex vivo (Langendorff) ischemia/reperfusion improved left ventricular (LV) function and limited cellular damage (13). Repeated administration of EPO in a rat coronary I/R model reduced cardiomyocyte loss and normalized diastolic hemodynamic dysfunction within 1 week after reperfusion (14). Most recently, Parsa et al. (15) showed cardioprotective and anti-apoptotic effects of EPO administered to rabbits at the time of myocardial infarction. In-vitro, EPO also exhibits angiogenic potential in myocardial tissue, which could also

Timing of erythropoietin cardioprotection
37
account for its cardioprotective effect (16).However, the optimal timing of EPO administration during I/R in the heart remains unknown. The aim of our study was to provide a clinically relevant “window of opportunity” for EPO treatment. Applied into the clinical situation, EPO would be administered to patients presenting with chest pain- without irreversible ischemic damage (unstable angina), with already evolving myocardial infarction, or undergoing revascularization procedures. Accordingly, we investigated the effects of EPO treatment at 3 different time points during I/R procedure (before and at the onset of ischemia, and after the start of reperfusion).
Methods
Animal modelThe experiments were conducted in accordance with the international Guide for the Care and Use of Laboratory Animals. The experimental protocol was approved by the Animal Research Committee of the University of Groningen.Male Sprague-Dawley rats (270-320 g) were obtained from Harlan (Zeist, The Netherlands). At the time of operation anesthesia was induced and maintained with 2.0-2.5% isoflurane (Isofluraan, Rhodia Organique Fine Ltd., UK). The trachea was intubated and the rats were mechanically ventilated (Amsterdam Infant Ventilator, Hoek/Loos, Schiedam, The Netherlands) using room air enriched with 1.0 l/min oxygen. Left thoracotomy was performed and the heart exposed through the fifth intercostal space. The pericardium was incised and a 6-0 silk suture (Perma-Hand seide, Johnson& Johnson, Belgium) was placed around the proximal portion of the left coronary artery, beneath the left atrial appendage. The ligature ends were passed through a small length of plastic tube to form a snare. For coronary artery occlusion, the snare was pressed onto the surface of the heart directly above the coronary artery and hemostat was applied to the snare. Ischemia was confirmed by the blanching of the myocardium and dyskinesis of the ischemic region. After 45 min. of occlusion, the hemostat was removed and snare released for reperfusion, with the ligature left loose on the surface of the heart (17). Successful reperfusion was indicated by the restoration of normal rubor. The wounds were sutured and the thorax was closed under negative pressure. The rats were weaned from mechanical ventilation and returned to cages to recover. In sham-operated rats, the same procedure was executed, without tightening the snare. Body core temperature was monitored during the surgical procedure with a rectal thermometer and maintained between 370- 380C by heating pads.
Experimental protocolAnimals were randomly allocated to 5 groups. To determine the effect of timing on the cardioprotective effect of EPO during ischemia/reperfusion, 3 groups of rats received recombinant human EPO (5.000 IU/kg in 0.5 ml of saline, i.p.) at 3 different time points: 2 hours before I/R (EPO-pre group; n=25), at the start of ischemia (EPO-isch group; n=16) and 5 min. after the onset of reperfusion (EPO-rep group; n=20). Control (MI group; n=20) and sham-operated (SHAM group; n=6) groups received corresponding injections of saline (0.5 ml, i.p.; Fig. 1).

Chapter 3
38
Hemodynamic measurementsTwenty-four hours after the coronary reperfusion, rats were reanesthetized. Microtip pressure transducer (Millar Instr. Inc., Houston, TX) was inserted into the left ventricular cavity via the right carotid artery. Left ventricular systolic pressure (LVSP) and its first derivatives (dP/dt
max and dP/dt
min), left ventricular end-diastolic pressure (LVEDP), and heart rate were
measured. The catheter was retracted into the aortic arch and arterial systolic and diastolic blood pressures were recorded.
Measurement of Infarct SizeAt the end of hemodynamic measurements, the chest was reopened, the heart rapidly excised and retrogradely perfused with 5 ml saline to remove any blood. The coronary artery was reoccluded by tightening the ligature that had remained at the site of the previous occlusion, and the heart was injected through the aorta with trypan blue (0.4%, Sigma Chemical, St. Louis, MO), to stain the perfused myocardium blue, whereas the non-perfused area at risk (AR), remained unstained. The heart was trimmed of the right ventricle and both atria and sliced transversely into 2-mm thick sections, which were incubated for 10 min in 370C nitro blue tetrazolium (Sigma Chemical, St. Louis, MO; 1 mg/ml Sörensen buffer, pH 7.4) to delineate the viable area (stained) and the infarcted area (IA- unstained) inside the AR, as described before (17). The sections were weighed and different regions were then measured by computed planimetry. Total weight of AR was calculated and expressed as percentage of total LV weight, IA was expressed as percentage of AR. Afterwards the sections were fixed in 10% formalin and embedded in paraffin.
MI (control)
EPO-pre
EPO-isch
EPO-rep
SHAM
45 min2 hrs 24 hrs
45 min2 hrs 24 hrs
45 min2 hrs 24 hrs
45 min2 hrs 24 hrs
45 min2 hrs 24 hrs
coronaryocclusion
reperfusion
Figure 1. Experimental protocol. Coronary artery occlusion was maintained for 45 min., followed by 24-hour reperfusion. Solid arrows indicate the time of EPO (5.000 IU/kg, i.p.) administration. Open arrows indicate the time of corresponding saline injections.

Timing of erythropoietin cardioprotection
39
ImmunohistochemistryParaffin embedded sections were dewaxed in xylene and dehydrated through graded alcohols.For the assessment of apoptosis the antigen retrieval was carried out by microwave treatment in a citrate buffer (10mM, pH 6.0). The endogenous peroxidase activity was blocked by 3% H
20
2. The sections were then incubated for 1 hour at room temperature with rabbit
polyclonal active caspase-3 antibody (1:50; New England Biolabs, Beverly, MA) (18), followed by incubation with peroxidase conjugated goat anti-rabbit and rabbit anti-goat IgG for 30 minutes at room temperature. To determine the proliferative activity, sections were immersed overnight at 800C in Tris-HCl solution (0.1 M, pH 9.0) and incubated for 1 hour with monoclonal mouse anti-Ki67-antigen antibody (1:25; Immunotech Marseille, France) (19), followed by incubation with peroxidase conjugated rabbit anti-mouse and goat anti-rabbit IgG for 30 minutes at room temperature. In both stainings 3,3´ diaminobenzidine (DAB) was used as chromogen and the sections were counterstained with hematoxylin.Positively stained cells were counted in ten randomly selected fields in the AR at 400x amplification. Anti-Ki67 staining was considered positive only when localization was nuclear. Blinded for treatment, the results from each heart sample were quantified and expressed as a percentage of total number of cells/nuclei. Tissue sections of colonic adenocarcinoma served as a positive control for both stainings (20).
Serum EPO analysisSerum human EPO levels were measured 24 hours after the surgery using the IMMULITE® EPO assay (DPC, Los Angeles, CA), which has been described before (21).
MaterialsAll experiments were performed using recombinant human Erythropoietin (rhEPO) alfa (EPREX, Janssen-Cilag, Tilburg, The Netherlands; 10.000 IU/ml). The rhEPO contains the same amino acid sequence as natural human EPO and possesses the same biological activity. It is ~ 80% homologous to rodent EPO, and it has been shown to be biologically active in rodents (22).
Statistical analysisData are presented as mean ± SEM. Statistical analysis between groups was performed by one-way ANOVA followed by LSD post-hoc analysis. Pearson’s correlation coefficients were calculated to determine the relationship between infarct size and LV function. Differences were considered significant at p<0.05. Animals with risk area, which exceeded 2SD of the average of all animals were excluded from the further analysis (MI: n=1; EPO-pre: n=2; EPO-isch: n=1; EPO-rep: n=1).

Chapter 3
40
Results
MortalityOverall 24-hour mortality in rats subjected to I/R was 24.7%. There was no significant difference in mortality rate between the non-treated MI group and groups treated with EPO (data not shown).
Hemodynamic measurementsIn vivo cardiac function was measured 24 hours after reperfusion by Millar catheterization. The data are presented in Figure 2. I/R in all groups resulted in a significant reduction
LVSP LVEDP
mm
Hg
0
80
100
120
140
0
5
10
15
20
25
MIEPO-preEPO-ischEPO-repSHAM
dpdt+ dpdt-
mm
Hg/
s
0
6000
8000
10000
12000
14000 -12000
-10000
-8000
-6000
0
†*
†† †
†† † †
*
*
† † † † †
Figure 2. Left ventricle (LV) hemodynamic parameters, 24-hours after reperfusion. Results are expressed as mean± ± SEM. LVSP indicates left ventricular systolic pressure; LVEDP-left ventricular end-diastolic pressure; dP/dtmax and dP/dtmin - maximal rate of increase and decrease of ventricular pressure; * p<0.05 vs. MI (control), †p<0.05 vs. SHAM.
Timing of erythropoietin cardioprotection
41
of LVSP, dP/dtmax
, dP/dtmin
when compared to sham-operated animals. Between the groups subjected to I/R, there was no significant difference in LVSP and LV dP/dt
max, although a trend
towards better systolic hemodynamic parameters was present in all three groups treated with EPO. LVEDP was significantly lower in EPO-isch and EPO-rep groups when compared to MI group. LV dP/dt
min was significantly enhanced in EPO-rep group compared to MI group.
LV function (dP/dtmax
and dP/dtmin
) correlated with the infarct size (r=-0.35, p=0.02 and r=0.38, p=0.01, respectively). Mean arterial pressure was not significantly different between treated and non-treated groups subjected to I/R (data not shown).
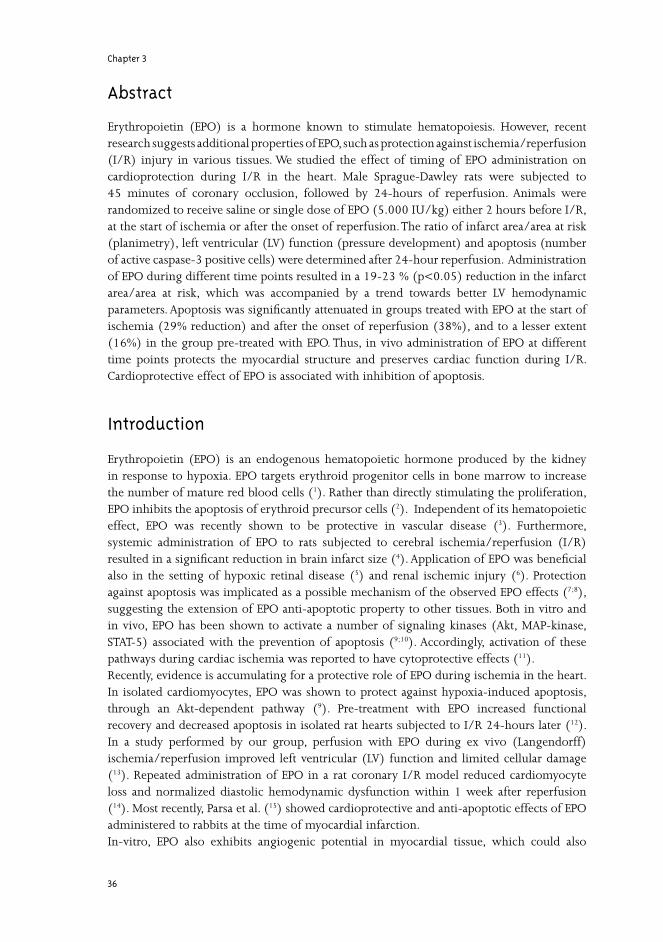
Infarct sizeInfarct sizes in the I/R groups are shown in Figure 3. There were no significant differences in the potential ischemic zone- area at risk (AR) between the control (MI) group and the three treatment groups. Similar areas of LV were thus exposed to I/R injury. In all groups treated with EPO, a significant reduction of the infarct area within AR was obtained compared with MI group (EPO-pre: 18.9%; EPO-isch: 22.8%; EPO-rep: 21.5% infarct size reduction), with no differences between the EPO treated groups.
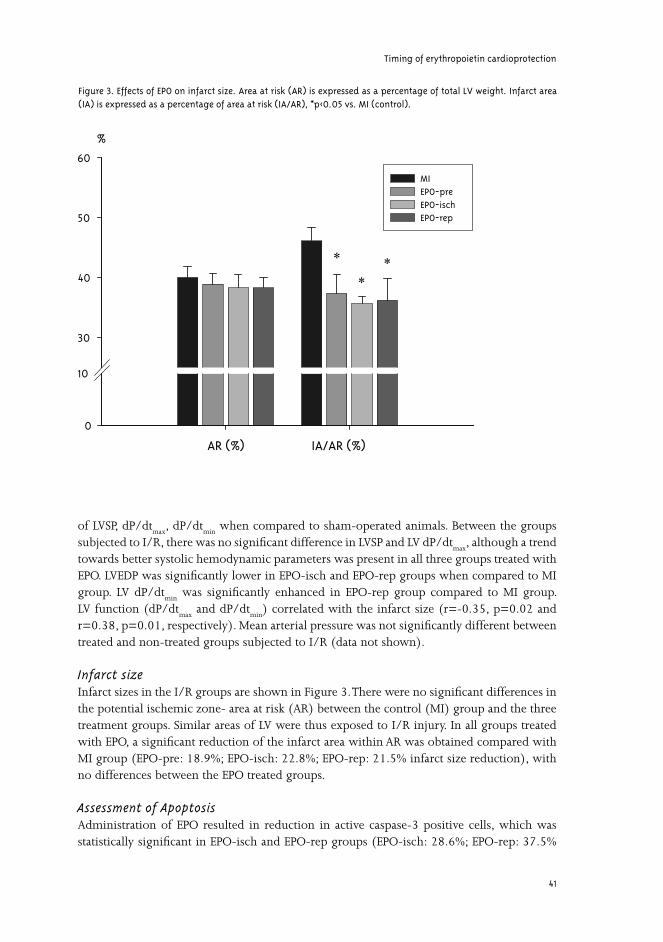
Assessment of ApoptosisAdministration of EPO resulted in reduction in active caspase-3 positive cells, which was statistically significant in EPO-isch and EPO-rep groups (EPO-isch: 28.6%; EPO-rep: 37.5%
AR (%) IA/AR (%)
%
0
10
30
40
50
60
MIEPO-preEPO-ischEPO-rep
*
**
Figure 3. Effects of EPO on infarct size. Area at risk (AR) is expressed as a percentage of total LV weight. Infarct area (IA) is expressed as a percentage of area at risk (IA/AR), *p<0.05 vs. MI (control).
Chapter 3
42
Figure 4. Effects of EPO on apoptosis. A) Graphic representation of active caspase-3 positive cells. Data are shown as a percentage of total number of cells, *p<0.05 vs. MI (control). B) Representative active caspase-3 stained LV section from a MI group (control). C) Representative active caspase-3 stained LV section from an EPO-rep group. Arrows indicate active caspase-3 positive cells.

Timing of erythropoietin cardioprotection
43
reduction compared to MI group; Fig. 4). A smaller difference, statistically non-significant, was observed in EPO-pre group (16.1% reduction).Active caspase-3 staining was mostly limited to the non-infarcted part of the area at risk, mainly to subendocardial and subepicardial regions. There were few active caspase-3 positive cells found outside the area at risk. No apoptotic cells were observed in the sham-operated group. Predominantly endothelial cells and fibroblasts were positive for active caspase-3 staining.
Determination of Proliferative ActivityOverall, the percentage of Ki67-antigen positive nuclei was very low (0.78% on average). We did not observe significant difference in proliferative activity as measured by the number of Ki67-antigen positive cells among the groups subjected to I/R (MI group: 0.75 ± 0.25%; EPO-pre: 0.99 ± 0.18%; EPO-isch: 0.72 ± 0.14%; EPO-rep: 0.68 ± 0.23% of total number of nuclei). In this respect mainly capillary wall cells appeared positive for the staining.
Serum EPO levelsIn rats, rhEPO is promptly absorbed after i.p. injection, with a plasma half-life of 7 hours (23). Twenty-four hours after reperfusion elevated levels of serum EPO were detected in the actively treated groups (EPO-pre: 4,236 ± 145 mIU/ml; EPO-isch: 5,213 ± 360 mIU/ml; EPO-rep: 5,597 ± 209 mIU/ml). Recombinant human EPO was undetectable in MI and sham-operated rats.
Discussion
In the present study, we show that a single dose of EPO at different time points during ischemia/reperfusion reduces the infarct size, which is accompanied by an improved LV function. To this point, these data confirm the previously reported cardioprotection by EPO in an I/R model (14;15). However, we take this concept one step further, by comparing the cardioprotective effects of EPO treatment over a relevant time frame. We demonstrate that the observed beneficial effects are independent of timing of EPO administration, from pre-ischemic until after the start of reperfusion.In our study, administration of EPO in all groups, including the group receiving EPO after the onset of reperfusion, markedly reduced the infarct size by limiting the area of irreversibly damaged tissue after ischemia/reperfusion injury and increasing the extent of viable myocardium. Since infarct size was significantly correlated with LV function (dP/dt
max
and dP/dtmin
), reducing the mass of infarcted tissue led also to improved LV hemodynamic parameters in groups treated with EPO (statistically significant LVEDP reduction in EPO-isch and EPO-rep groups and LV dP/dt
min in EPO-rep group).
Two forms of cell death are implicated during ischemia/reperfusion injury, namely apoptosis and necrosis (24). Although the exact contribution of these two forms of death is unclear, apoptosis progressively develops and accelerates during the reperfusion (18;25). Since EPO is known to have anti-apoptotic properties, we investigated the level of apoptosis by measuring the percentage of active caspase-3 positive cells. In all actively treated groups, EPO administration reduced the rate of apoptosis within the risk area. Surprisingly, apoptosis was most attenuated in the group treated with EPO after the start of reperfusion. The “window of
Chapter 3
44
protection” may thus be explained by the ability of the exogenous EPO to protect the cells in the risk area against the reperfusion-induced programmed cell death. Primarily protection against reperfusion damage confirms our previous results, in which the protective effects of EPO were mainly observed during the reperfusion of isolated rat hearts subjected to I/R (13). Scarabelli et al. (18) showed that in the early stages of reperfusion, apoptosis is firstly seen only in endothelial cells and is gradually spreading to surrounding cells. In our experiment we observed apoptosis specifically in endothelial and interstitial cells. We may hence hypothesize that EPO cardioprotection may be explained by preservation of the endothelial function and vascular flow in coronary vessels.Furthermore, early apoptosis after myocardial infarction is associated with later expansion of the infarct size and LV remodeling (26). This is supported by a study by Moon et al., where a single dose of EPO at the time of myocardial infarction in rats led to a 50% reduction in early apoptosis, with subsequent prevention of LV dysfunction over a period of 8 weeks (27). In addition to its anti-apoptotic effects, erythropoietin was recently shown to mobilize progenitor cells from the bone marrow (28) and stimulate neovascularization (16) , which was associated with the regeneration of the myocardium (29). Although we did not find any increase in proliferative activity in groups treated with EPO, this mechanism may play a role in a long-term EPO effect, positively shifting the balance between the cell death and regeneration in the infarcted myocardium (30).Since we assessed the short-term action of EPO, its effect on hemoglobin levels would be largely limited and can not explain the described results. Previously it has been shown that a single high-dose of EPO does not increase hemoglobin levels during the first 2-3 days (15;27).The molecular signals by which EPO provides its benefit in this study remain largely unresolved and their analysis goes beyond the scope of this article. In neuronal and hematopoietic cells EPO activates various protein kinase cascades (31;32). The primary kinase signaling pathway is the stress responsive Jak-2, activation of which leads to downstream phosphorylation of STAT-5, Akt-1 and MAPK. In the myocardium, the activation of these pro-survival kinase cascades during the first minutes of reperfusion has been shown to attenuate reperfusion-induced apoptosis (24). In previous experiments we found that EPO increases the levels of phosphorylated MAPK p42/p44 in isolated rat hearts (33). However, the level of STAT-5 and MAPK activation peaks at 5-30 minutes after EPO exposure, with returning to baseline values within 1 hour (34-36). Accordingly, in the present study we did not detect any difference in STAT-5 and MAPK phosphorylation between MI and EPO groups 24 hours after the reperfusion (data not shown). This may also explain the somewhat smaller anti-apoptotic effect found in the group pre-treated with EPO 2 hours before I/R, as it would result in insufficient activation of STAT-5/ MAPK pathways at the time of ischemia/reperfusion. However, further studies are needed to determine the precise mechanism of EPO induced cardioprotection.Additional mechanisms have been implicated in the protective role of EPO in vascular diseases. EPO was shown to modulate NO activity and thus could account for restored vascular homeostasis (37;38). Furthermore, antioxidative role of EPO could also play a role in cardioprotection during I/R (39).The clinical benefit of non-erythropoietic effects of EPO has been implicated by Ehrenreich et al. (40) in a pilot, double-blind, randomized clinical trial investigating the acute effects of EPO treatment in patients with ischemic stroke. There, administration of EPO within 8 hrs

Timing of erythropoietin cardioprotection
45
after stroke reduced brain infarct size and improved the clinical outcome. This short-term therapy with high-dose of EPO proved to be both safe and well tolerated. The serum EPO levels achieved in these patients (4.000-6.000 mIU/ml) were well comparable with those measured in our study. As there are many similarities between brain and heart ischemia, EPO administration may provide an adjunctive therapy for the treatment of acute coronary syndromes. So far the therapeutic strategies are more directed to shortening the time of ischemia (“open artery” theory) and to lesser extend to approaches salvaging the cardiac tissue during reperfusion. Prospective EPO therapy may thus protect the “area at risk” during ischemia and (particularly) reperfusion.
Conclusion
In our study, we have shown that in vivo administration of EPO at different time points protects the myocardial structure and preserves cardiac function during I/R. Cardioprotective effect of EPO extends beyond the start of reperfusion, providing a broad “window of opportunity” for the potential treatment of acute coronary syndromes.The present results and those of other groups, including the data on the safety of EPO administration in the clinical practice, warrant a pilot study with EPO treatment in patients with acute coronary syndromes.
Acknowledgments
The authors thank Bianca Meijeringh, Egbert Scholtens and Alex Kluppel for expert technical assistance. Erik Lipšic is supported by GUIDE. Peter van der Meer is supported by NWO ZonMW.
Chapter 3
46
Reference List1. Gabrilove J. Overview: erythropoiesis, anemia, and the impact of erythropoietin. Semin Hematol. 2000;37:1-3.
2. Fisher JW. Erythropoietin: physiology and pharmacology update. Exp Biol Med (Maywood ). 2003;228:1-14.
3. Chong ZZ, Kang JQ, Maiese K. Erythropoietin is a novel vascular protectant through activation of Akt1 and mitochondrial modulation of cysteine proteases. Circulation. 2002;106:2973-2979.
4. Brines ML, Ghezzi P, Keenan S et al. Erythropoietin crosses the blood-brain barrier to protect against experimental brain injury. Proc Natl Acad Sci U S A. 2000;97:10526-10531.
5. Grimm C, Wenzel A, Groszer M et al. HIF-1-induced erythropoietin in the hypoxic retina protects against light-induced retinal degeneration. Nat Med. 2002;8:718-724.
6. Vesey DA, Cheung C, Pat B et al. Erythropoietin protects against ischaemic acute renal injury. Nephrol Dial Transplant. 2004;19:348-355.
7. Siren AL, Fratelli M, Brines M et al. Erythropoietin prevents neuronal apoptosis after cerebral ischemia and metabolic stress. Proc Natl Acad Sci U S A. 2001;98:4044-4049.
8. Kumral A, Ozer E, Yilmaz O et al. Neuroprotective effect of erythropoietin on hypoxic-ischemic brain injury in neonatal rats. Biol Neonate. 2003;83:224-228.
9. Tramontano AF, Muniyappa R, Black AD et al. Erythropoietin protects cardiac myocytes from hypoxia-induced apoptosis through an Akt-dependent pathway. Biochem Biophys Res Commun. 2003;308:990-994.
10. Fuste B, Serradell M, Escolar G et al. Erythropoietin triggers a signaling pathway in endothelial cells and increases the thrombogenicity of their extracellular matrices in vitro. Thromb Haemost. 2002;88:678-685.
11. Negoro S, Kunisada K, Tone E et al. Activation of JAK/STAT pathway transduces cytoprotective signal in rat acute myocardial infarction. Cardiovasc Res. 2000;47:797-805.
12. Cai Z, Manalo DJ, Wei G et al. Hearts from rodents exposed to intermittent hypoxia or erythropoietin are protected against ischemia-reperfusion injury. Circulation. 2003;108:79-85.
13. Van der Meer P, Lipšic E, Henning RH et al. Erythropoietin improves left ventricular function and coronary flow in an experimental model of ischemia-reperfusion injury. Eur J Heart Fail. In press.
14. Calvillo L, Latini R, Kajstura J et al. Recombinant human erythropoietin protects the myocardium from ischemia-reperfusion injury and promotes beneficial remodeling. Proc Natl Acad Sci U S A. 2003;100:4802-4806.
15. Parsa CJ, Matsumoto A, Kim J et al. A novel protective effect of erythropoietin in the infarcted heart. J Clin Invest. 2003;112:999-1007.
16. Jaquet K, Krause K, Tawakol-Khodai M et al. Erythropoietin and VEGF exhibit equal angiogenic potential. Microvasc Res. 2002;64:326-333.
17. Van den Doel MA, Gho BC, Duval SY et al. Hypothermia extends the cardioprotection by ischaemic preconditioning to coronary artery occlusions of longer duration. Cardiovasc Res. 1998;37:76-81.
18. Scarabelli T, Stephanou A, Rayment N et al. Apoptosis of endothelial cells precedes myocyte cell apoptosis in ischemia/reperfusion injury. Circulation. 2001;104:253-256.
Timing of erythropoietin cardioprotection
47
19. Mehrabi MR, Serbecic N, Tamaddon F et al. Clinical and experimental evidence of prostaglandin E1-induced angiogenesis in the myocardium of patients with ischemic heart disease. Cardiovasc Res. 2002;56:214-224.
20. Yang L, Cao Z, Yan H et al. Coexistence of high levels of apoptotic signaling and inhibitor of apoptosis proteins in human tumor cells: implication for cancer specific therapy. Cancer Res. 2003;63:6815-6824.
21. Benson EW, Hardy R, Chaffin C et al. New automated chemiluminescent assay for erythropoietin. J Clin Lab Anal. 2000;14:271-273.
22. Egrie JC, Strickland TW, Lane J et al. Characterization and biological effects of recombinant human erythropoietin. Immunobiology. 1986;172:213-224.
23. Erbayraktar S, Grasso G, Sfacteria A et al. Asialoerythropoietin is a nonerythropoietic cytokine with broad neuroprotective activity in vivo. Proc Natl Acad Sci U S A. 2003;100:6741-6746.
24. Hausenloy DJ, Yellon DM. New directions for protecting the heart against ischaemia-reperfusion injury: targeting the Reperfusion Injury Salvage Kinase (RISK)-pathway. Cardiovasc Res. 2004;61:448-460.
25. Zhao ZQ, Velez DA, Wang NP et al. Progressively developed myocardial apoptotic cell death during late phase of reperfusion. Apoptosis. 2001;6:279-290.
26. Sam F, Sawyer DB, Chang DL et al. Progressive left ventricular remodeling and apoptosis late after myocardial infarction in mouse heart. Am J Physiol Heart Circ Physiol. 2000;279:H422-H428.
27. Moon C, Krawczyk M, Ahn D et al. Erythropoietin reduces myocardial infarction and left ventricular functional decline after coronary artery ligation in rats. Proc Natl Acad Sci U S A. 2003;100:11612-11617.
28. Heeschen C, Aicher A, Lehmann R et al. Erythropoietin is a potent physiologic stimulus for endothelial progenitor cell mobilization. Blood. 2003;102:1340-1346.
29. Orlic D, Kajstura J, Chimenti S et al. Mobilized bone marrow cells repair the infarcted heart, improving function and survival. Proc Natl Acad Sci U S A. 2001;98:10344-10349.
30. Van der Meer P, Voors AA, Lipšic E et al. Erythropoietin in cardiovascular diseases. Eur Heart J. 2004;25:285-291.
31. Bittorf T, Seiler J, Ludtke B et al. Activation of STAT5 during EPO-directed suppression of apoptosis. Cell Signal. 2000;12:23-30.
32. Digicaylioglu M, Lipton SA. Erythropoietin-mediated neuroprotection involves cross-talk between Jak2 and NF-kappaB signalling cascades. Nature. 2001;412:641-647.
33. Lipšic E, van der Meer P, Suurmeijer AJH et al. Erythropoietin protects against ischaemic damage in isolated rat heart. Eur Heart J. 2003;24:477 (abstract)
34. Ammarguellat F, Llovera M, Kelly PA et al. Low doses of EPO activate MAP kinases but not JAK2-STAT5 in rat vascular smooth muscle cells. Biochem Biophys Res Commun. 2001;284:1031-1038.
35. Fuste B, Serradell M, Escolar G et al. Erythropoietin triggers a signaling pathway in endothelial cells and increases the thrombogenicity of their extracellular matrices in vitro. Thromb Haemost. 2002;88:678-685.
36. Shi Y, Rafiee P, Su J et al. Acute cardioprotective effects of erythropoietin in infant rabbits are mediated by activation of protein kinases and potassium channels. Basic Res Cardiol. 2004;99:173-182.
37. Kanagy NL, Perrine MF, Cheung DK et al. Erythropoietin administration in vivo increases vascular nitric oxide synthase expression. J Cardiovasc Pharmacol. 2003;42:527-533.

Chapter 3
48
38. Kumral A, Baskin H, Gokmen N et al. Selective Inhibition of Nitric Oxide in Hypoxic-Ischemic Brain Model in Newborn Rats: Is It an Explanation for the Protective Role of Erythropoietin? Biol Neonate. 2004;85:51-54.
39. Solaroglu I, Solaroglu A, Kaptanoglu E et al. Erythropoietin prevents ischemia-reperfusion from inducing oxidative damage in fetal rat brain. Childs Nerv Syst. 2003;19:19-22.
40. Ehrenreich H, Hasselblatt M, Dembowski C et al. Erythropoietin therapy for acute stroke is both safe and beneficial. Mol Med. 2002;8:495-505.

Chapter 4
Erythropoietin induces neovascularization
and improves cardiac function in rats with heart failure after myocardial infarction
Peter van der Meer, Erik Lipšic, Robert H. Henning, Kristien Boddeus,
Jolanda van der Velden, Adriaan A. Voors, Dirk J. van Veldhuisen, Wiek H. van Gilst,
Regien G. Schoemaker
Journal of the American College of Cardiology 2005;46:125-33

Chapter 4
52
Abstract
Objectives: We assessed the effects of erythropoietin (EPO) treatment in a rat model of post-myocardial infarction (MI) heart failure.Background: EPO, traditionally known as a hematopoietic hormone, has been linked to neovascularization. Whereas administration of EPO acutely after MI reduces infarct size and improves cardiac function, its role in the failing heart is unknown. Methods: Rats underwent coronary ligation or sham surgery. Rats with MI were randomly assigned to: untreated (MI), a single bolus of EPO immediately after MI induction (MI-EPO-early), EPO treatment immediately after MI and once every three weeks (MI-EPO-early+late) and EPO treatment starting three weeks after induction of MI, once every three weeks (MI-EPO-late). After nine weeks, hemodynamics, infarct size, myosin heavy chain (MHC) isoforms, myocyte hypertrophy and capillary density were measured. Results: EPO treatment started immediately after MI (MI-EPO-early and MI-EPO-early+late) resulted in a 23-30% reduction in infarct size (p<0.01), and accordingly hemodynamic im-provement. EPO treatment, started three weeks after MI (MI-EPO-late), did not affect infarct size, but resulted in an improved cardiac performance, reflected by a 34% reduction in left ventricular end-diastolic pressure (p<0.01), and 46% decrease in atrial natriuretic peptide levels (p<0.05). The improved cardiac function was accompanied by an increased capillary density (p<0.01), an increased capillary-to-myocyte ratio (p<0.05) and a partial reversal of β-MHC (p<0.05) in all treated groups. Conclusion: In addition to its effect on infarct size reduction, EPO treatment improves cardiac function in a rat model of post-MI heart failure. This observation may be explained by neovascularization, associated with an increased α-MHC expression.
Introduction
Erythropoietin (EPO) is best known as a hematopoietic growth factor, promoting prolifera-tion and differentiation of erythroid progenitor cells. However, the expression of the EPO-receptor outside the hematopoietic system, including endothelial cells, cardiomyocytes and neurons, may suggest additional effects of EPO beyond hematopoiesis (1-4). Because an insufficient amount of capillaries may lead to left ventricular (LV) dilation and heart failure after myocardial infarction (MI) (5), treatment directed towards increasing capil-lary density might be beneficial in heart failure. Expanding evidence shows that EPO is in-volved in angiogenesis. It has been shown that stimulation of cultured endothelial cells with EPO resulted in cell proliferation, chemotaxis and differentiation into vascular structures (6). Furthermore, Jaquet et al found that EPO and vascular endothelial growth factor (VEGF) were equally effective in stimulating angiogenesis in endothelial cells derived from the myocar-dium (7). Most recently, it has been shown that EPO treatment in a rat stroke model resulted in an increased capillary density around the ischemic lesion (8). In addition, EPO has been implicated to play a protective role during acute ischemia in brain (2;9;10) and heart (11-13). Pretreatment with exogenous EPO rescued hypoxic cultured cardio-myocytes from apoptosis (12). EPO perfusion during ex-vivo ischemia-reperfusion improved left ventricular function and reduced cellular damage(4;13;14). Acute, systemic treatment with EPO, in a rodent ischemia-reperfusion model, substantially reduced infarct size and decreased

Erythropoietin attenuates heart failure
53
myocardial apoptosis (12), even when EPO was administered after reperfusion(11;15). While the cardioprotective effects of EPO during acute MI are increasingly recognized, the role of EPO treatment in chronic heart failure (CHF) is unknown. Therefore, we assessed the effects of EPO treatment in a rat model of post-MI heart failure (16). In this model, induc-tion of MI leads to a time and infarct size related ventricular dilatation and heart failure (17). We hypothesized that EPO treatment initiated after heart failure development (three weeks after induction of MI) would improve cardiac performance, possibly by increasing capillary density. To distinguish the acute effects of EPO (i.e. infarct size reduction) from its effects in CHF, we studied two additional groups. In one group we administered only a single dose of EPO immediately after MI, and in a second group we administered EPO immediately after MI and continued EPO treatment during the experiment.
Methods
AnimalsWe used male Sprague Dawley rats weighing 270-330 g (Harlan, Zeist, The Netherlands). Animals were fed ad libitum, and housed in groups of four to five rats, according to institu-tional rules with 12:12 hours light-dark cycles. The experimental protocol was approved by the Animal Ethical Committee of the University of Groningen.
Design of the studyRats were either subjected to left coronary artery ligation (n=85) or sham surgery (n=8). Rats with MI were randomized to one of four groups; untreated (MI) or three different treat-ment strategies with EPO: a single bolus of EPO immediately after ligation (MI-EPO-early), EPO treatment directly after ligation and once every three weeks (MI-EPO-early+late) and EPO treatment starting three weeks after ligation, once every three weeks (MI-EPO-late). EPO (Darbepoetin-alpha; Aranesp, Amgen Inc., Thousands Oaks, CA, USA) was administered intraperitoneally at a dose of 40 μg/kg, which equals 8.000 U/kg recombinant human EPO (Amgen Inc.) and is in close range of known dosages for organ protection (11;12;18). Hematocrit was measured at baseline and at week one, three, four, six and nine after surgery. Persons blinded to the treatment groups performed the analysis of samples obtained from the experiments.
Myocardial infarction modelThis model has been described previously (16). Briefly, rats were anesthetized with 2% isoflu-rane in 1.0 L oxygen/minute. After intubation, the rats were put on a mechanical ventilator (frequency 90/min) and a left-side thoracotomy was performed. MI was induced by ligating the proximal portion of the left coronary artery, beneath the left atrial appendage. In sham operated rats, the same surgery was performed, without ligating the suture.
Hemodynamic measurementsAfter nine weeks rats were anaesthetized as described above. Microtip pressure transducer (Millar Instr. Inc., Houston, Texas) was inserted into the left ventricular cavity via the right carotid artery. After a 3-min period of stabilization, heart rate (HR), left ventricular systolic

Chapter 4
54
pressure (LVSP), left ventricular end-diastolic pressure (LVEDP), and developed left ventricu-lar pressure (dLVP=LVSP-LVEDP) were measured. As indices of contractility and relaxation, the maximal rates of increase and decrease in LVP (+dP/dt
max and -dP/dt
max) were determined.
The catheter was retracted into the aortic arch and arterial systolic and diastolic blood pres-sures (SBP, DBP) were recorded.
Plasma N-terminal ANP levels Arterial blood was collected after nine weeks, anti-coagulated with EDTA, and plasma was stored at –80˚C until assayed. Plasma N-terminal atrial natriuretic peptide (N-ANP) was mea-sured by a commercially available radioimmunoassay (Biotop, Oulu, Finland), as described previously (19).
Infarct size and left ventricular hypertrophyAfter hemodynamic measurements, hearts were rapidly excised and weighed. Mid-papillary slices were prepared for immunohistochemistry. Slices were fixed in 4% paraformaldehyde and paraffin-embedded. Infarct size was determined by planimetry at mid-ventricular levels in transverse slices on picrosirius red/fast green–stained sections. Infarct size was expressed as the percentage of scar length to total left ventricular circumference, as described previously(20;21). Deparaffinized 5-μm thick sections were stained with a Gomori’s silver staining, in order to visualize individual myocytes in the viable LV wall, the area with the
Table 1. Characteristics of the experimental groups
Sham MI MI-EPO-early MI-EPO-late MI-EPO-early+late
General
n 8 12 12 13 13
Infarct size (% of LV) … 43±3 30±2§ 41±3 33±2§
Hemodynamics
Heart rate (bpm) 313±8 324±6 332±7 326±7 328±8
SBP (mmHg) 127±3 111±4† 115±3† 120±3‡ 122±3‡
DBP (mmHg) 78±2 78±2 79±2 83±3 86±2
Body/organ weight
BW (g) 390±10 395±11 401±8 400±7 421±6
Lungweight/BW (mg/g) 3.9±0.1 6.4±1.0† 4.2±0.5§ 3.9±0.1§ 3.9±0.2§
Heartweight/BW (mg/g) 3.2±0.1 4.0±0.2† 3.8±0.1† 3.7±0.1* 3.7±0.1*
Hematocrit
baseline (%) 48±0.6 47±0.3 48±0.5 48±0.6 47±0.6
1 week (%) 48±0.6 47±1.1 58±0.9†,§ 46±0.7 59±0.7†,§
3 weeks (%) 50±1.1 49±0.7 53±0.5†,§ 49±0.7 53±0.7†,§
4 weeks (%) 50±0.5 51±0.8 50±0.4 62±0.5†,§ 64±1.8†,§
6 weeks (%) 50±0.4 50±0.7 49±0.6 60±0.7†,§ 61±0.7†,§
9 weeks (%) 44±0.5 44±1.5 44±0.7 54±1.3†,§ 56±1.7†,§
Data are presented as mean ± SEM. n indicates number of animals; LV, left ventricle; SBP, systolic blood pressure; DBP, diastolic blood pressure; BW, bodyweight. *p<0.05; †p<0.01 vs. Sham; ‡p<0.05,§ §p<0.01 vs. MI.

Erythropoietin attenuates heart failure
55
most pronounced underperfusion (22). Using image analysis (Zeiss KS 400, Jena, Germany), concentric myocyte hypertrophy in the viable LV wall, remote from the infarcted area, was measured as the cross-sectional area of transversally cut myocytes showing a nucleus. Myocyte density was calculated as the average number of myocytes per tissue area. In each stained section, measurements were averaged from three different counting fields (± 75 myocytes per heart).
Myosin Heavy Chain (MHC) Isoform AnalysisSamples of the left ventricle (not infarct area), were frozen in liquid nitrogen and stored at –80˚C. The freeze dried samples were dissolved in a buffer and gel electrophoresis was per-formed as described previously (23). Samples (0.5μg) were run at constant current (24 mA) for 5 hours. Silver staining of the gels and laser scanning densitometry was performed to identify differences in myosin isoform composition (i.e. α-MHC and β-MHC).
Capillary densityTo visualize capillaries in the myocardium in the same area as used for the measurements of the myocyte size, endothelial cells were stained with biotin-labeled Lectin GSL (1:100; Sigma-Aldrich, St. Louis, Missouri), as previously described (16). Since Lectins stain not only capillaries but also other vessels, a size criterion of 10 μm was used to exclude small arteri-oles and venules. Image analysis (Image Pro-plus version 4.5, Media Cybernetics Inc.,Silver Spring, Maryland) was used to measure capillary density, calculated as the number of capil-laries per tissue area. The measured total tissue area was corrected for the remaining inter-stitial space. Actual neovascularization was derived from an increased capillary-to-myocyte ratio, which has been calculated as capillary density divided by myocyte density (24).
Statistical analysisData are presented as mean ± SEM. Statistical analysis between groups was performed by 1-way ANOVA. When a statistically significant difference was detected, a Fisher’s protected LSD post-hoc analysis was performed. Correlation analysis was performed with Pearson’s correla-tion tests. Differences were considered significant at p<0.05.
Results
GeneralOverall mortality after MI was 41%. Mortality occurred only in the first 24 hours after in-duction of MI. There were no statistically significant differences in mortality between the four groups (MI:50%, MI-EPO-early: 40%, MI-EPO-late: 32% and MI-EPO-early+late: 41%; p=0.54). No mortality was observed in sham-operated rats. At baseline, no differences in body weight were observed (data not shown). General characteristics after nine weeks are shown in table 1. Body weight was comparable among the five groups. Among groups with MI, systolic blood pressure (SBP) was significantly lower only in MI and MI-EPO-early com-pared to sham; p<0.01. SBP was significantly higher in MI-EPO-late and MI-EPO-early+late, compared to MI group (p<0.05). No significant differences were observed in heart rate and diastolic blood pressure (DBP), although there was a trend towards higher DBP in the groups
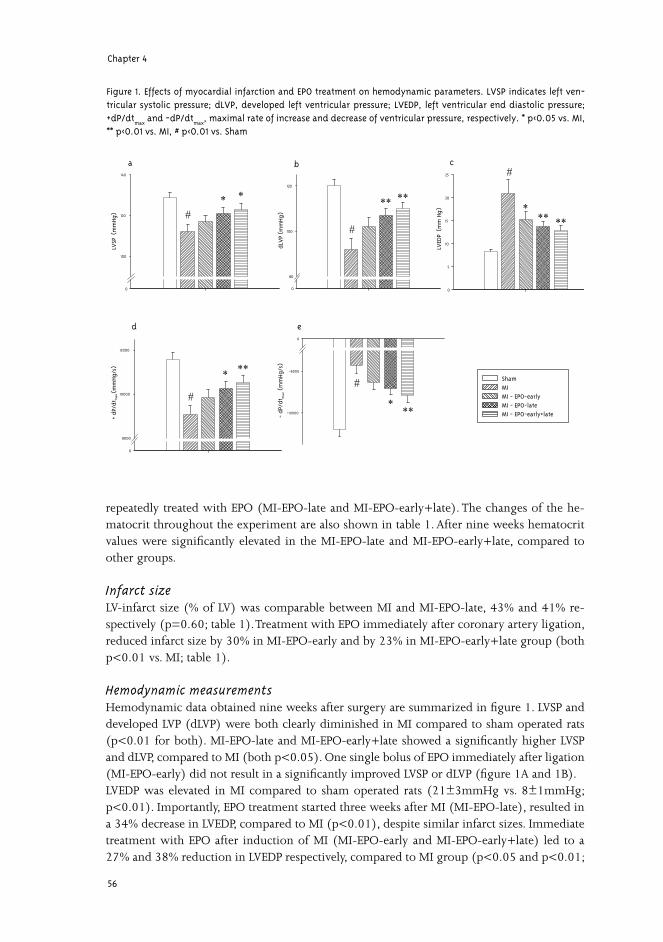
Chapter 4
56
repeatedly treated with EPO (MI-EPO-late and MI-EPO-early+late). The changes of the he-matocrit throughout the experiment are also shown in table 1. After nine weeks hematocrit values were significantly elevated in the MI-EPO-late and MI-EPO-early+late, compared to other groups.
Infarct size LV-infarct size (% of LV) was comparable between MI and MI-EPO-late, 43% and 41% re-spectively (p=0.60; table 1). Treatment with EPO immediately after coronary artery ligation, reduced infarct size by 30% in MI-EPO-early and by 23% in MI-EPO-early+late group (both p<0.01 vs. MI; table 1).
Hemodynamic measurementsHemodynamic data obtained nine weeks after surgery are summarized in figure 1. LVSP and developed LVP (dLVP) were both clearly diminished in MI compared to sham operated rats (p<0.01 for both). MI-EPO-late and MI-EPO-early+late showed a significantly higher LVSP and dLVP, compared to MI (both p<0.05). One single bolus of EPO immediately after ligation (MI-EPO-early) did not result in a significantly improved LVSP or dLVP (figure 1A and 1B).LVEDP was elevated in MI compared to sham operated rats (21±3mmHg vs. 8±1mmHg; p<0.01). Importantly, EPO treatment started three weeks after MI (MI-EPO-late), resulted in a 34% decrease in LVEDP, compared to MI (p<0.01), despite similar infarct sizes. Immediate treatment with EPO after induction of MI (MI-EPO-early and MI-EPO-early+late) led to a 27% and 38% reduction in LVEDP respectively, compared to MI group (p<0.05 and p<0.01;
Hem
atoc
rit (%
)
0
20
30
40
50
60
70
ShamMIMI - EPO-earlyMI - EPO-lateMI - EPO-early+late
LVED
P (
mm
Hg
)
0
5
10
15
20
25
dLV
P (m
mHg
)0
80
100
120
LVSP
(m
mHg
)
0
100
120
140
+ dP
/dt m
ax (
mm
Hg/s
)
0
8000
10000
12000
- dP
/dt m
ax (
mm
Hg/s
)
-10000
-8000
0
ca b
ed
* *
*
*
***
** **
**
**
**
#
#
#
##
Figure 1. Effects of myocardial infarction and EPO treatment on hemodynamic parameters. LVSP indicates left ven-tricular systolic pressure; dLVP, developed left ventricular pressure; LVEDP, left ventricular end diastolic pressure; +dP/dt
max and -dP/dt
max, maximal rate of increase and decrease of ventricular pressure, respectively. * p<0.05 vs. MI,
** p<0.01 vs. MI, # p<0.01 vs. Sham

Erythropoietin attenuates heart failure
57
figure 1C). Myocardial contractility (+dP/dt
max) and myocardial relaxation (-dP/dt
max) were both impaired
in MI compared to the sham group (both p<0.01). MI-EPO-late and MI-EPO-early+late showed an improved contractility and relaxation compared to MI (all p<0.05). In contrast, when only one single bolus of EPO was administered immediately after MI (MI-EPO-early), contractility and relaxation were not significantly improved compared to MI (figure 1D and 1E).
N-terminal ANP levelsFigure 2 shows that plasma N-ANP levels were three-fold increased in MI group (p<0.01 vs. sham-operated animals). Furthermore, N-ANP levels were significantly reduced in the MI-EPO-late and MI-EPO-early+late groups (both p<0.05 vs. MI), returning to sham values (both p=NS vs. sham). The MI-EPO-early group showed a trend towards lower N-ANP levels (p=0.07 vs. MI).
Organ weights and LV hypertrophyAs shown in table 1, the ratios of heart weight (HW) to body weight and that of lung weight to body weight were significantly increased in the MI compared to the sham-operated group (both p<0.01). Lung weight to body weight (an indirect expression of the LV-end diastolic pressure and thus severity of heart failure) was significantly reduced in all EPO treatment groups (all p<0.01 vs. MI). A trend towards lower HW to body weight compared to MI was observed in MI-EPO-late and MI-EPO-early+late groups. LV hypertrophy was further studied by histological analysis. Representative photomicrographs of Gomori stained sections of the viable LV free wall are shown in figure 3A. MI resulted in a 35% increase in myocyte cross-sectional area, compared to sham (p<0.05). All EPO treated groups showed a trend towards a smaller myocyte cross-sectional area, although this did not reach statistical significance (figure 3B).
N te
rmin
al-A
NP
(pm
ol/L
)
0
1
2
3
4
5
6ShamMI MI - EPO-earlyMI - EPO-lateMI - EPO-early+late
***
#
Figure 2. Plasma N-terminal ANP levels. * p<0.05 vs. MI, ** p<0.01 vs. MI, # p<0.01 vs. Sham.
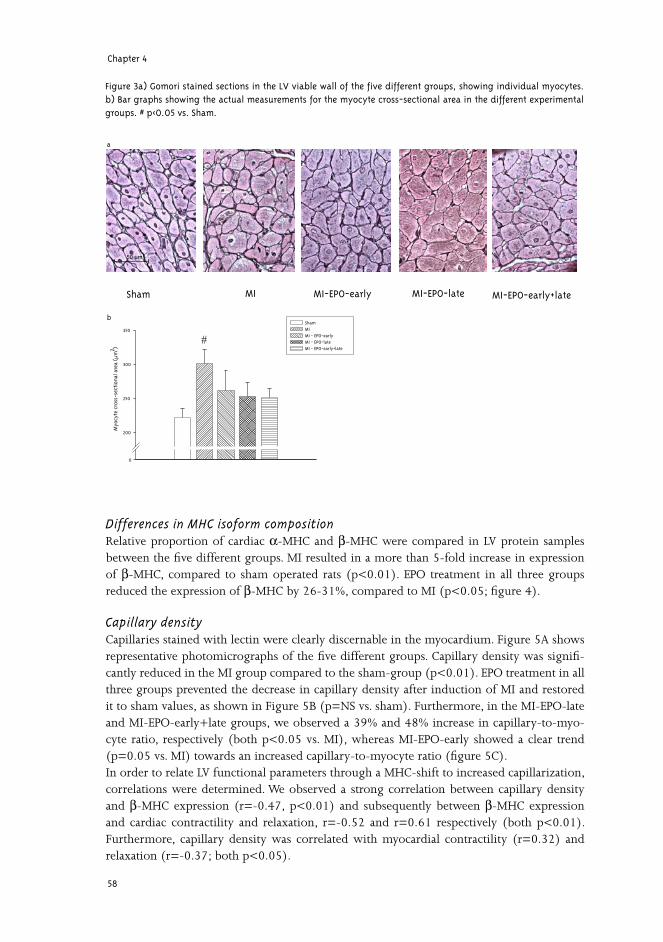
Chapter 4
58
Differences in MHC isoform compositionRelative proportion of cardiac α-MHC and β-MHC were compared in LV protein samples between the five different groups. MI resulted in a more than 5-fold increase in expression of β-MHC, compared to sham operated rats (p<0.01). EPO treatment in all three groups reduced the expression of β-MHC by 26-31%, compared to MI (p<0.05; figure 4).
Capillary densityCapillaries stained with lectin were clearly discernable in the myocardium. Figure 5A shows representative photomicrographs of the five different groups. Capillary density was signifi-cantly reduced in the MI group compared to the sham-group (p<0.01). EPO treatment in all three groups prevented the decrease in capillary density after induction of MI and restored it to sham values, as shown in Figure 5B (p=NS vs. sham). Furthermore, in the MI-EPO-late and MI-EPO-early+late groups, we observed a 39% and 48% increase in capillary-to-myo-cyte ratio, respectively (both p<0.05 vs. MI), whereas MI-EPO-early showed a clear trend (p=0.05 vs. MI) towards an increased capillary-to-myocyte ratio (figure 5C). In order to relate LV functional parameters through a MHC-shift to increased capillarization, correlations were determined. We observed a strong correlation between capillary density and β-MHC expression (r=-0.47, p<0.01) and subsequently between β-MHC expression and cardiac contractility and relaxation, r=-0.52 and r=0.61 respectively (both p<0.01). Furthermore, capillary density was correlated with myocardial contractility (r=0.32) and relaxation (r=-0.37; both p<0.05).
Myo
cyte
cro
ss-s
ecti
onal
are
a (µ
m2 )
0
200
250
300
350
ShamMIMI - EPO-earlyMI - EPO-lateMI - EPO-early+late
#
Sham MI MI-EPO-early MI-EPO-late MI-EPO-early+late
50 μm
a
b
Figure 3a) Gomori stained sections in the LV viable wall of the five different groups, showing individual myocytes. b) Bar graphs showing the actual measurements for the myocyte cross-sectional area in the different experimental groups. # p<0.05 vs. Sham.
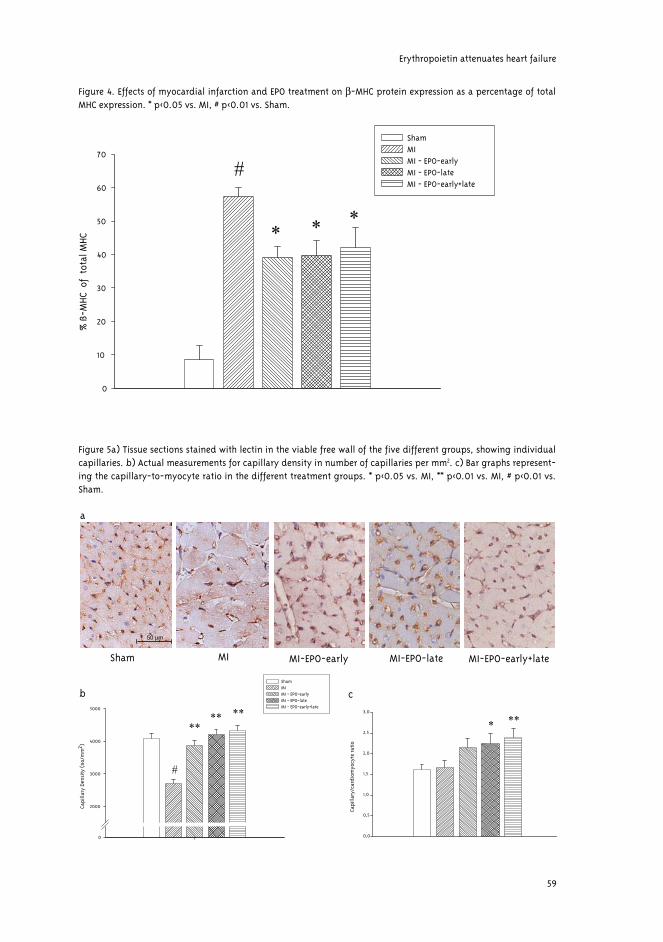
Erythropoietin attenuates heart failure
59
% ß
-MHC
of
tota
l MHC
0
10
20
30
40
50
60
70
ShamMIMI - EPO-earlyMI - EPO-lateMI - EPO-early+late
#
***
Figure 4. Effects of myocardial infarction and EPO treatment on β-MHC protein expression as a percentage of total MHC expression. * p<0.05 vs. MI, # p<0.01 vs. Sham.
Capi
llary
/car
diom
yocy
te ra
tio
0,0
0,5
1,0
1,5
2,0
2,5
3,0
Capi
llary
Den
sity
(no
/mm
2 )
0
2000
3000
4000
5000
ShamMI MI - EPO-earlyMI - EPO-lateMI - EPO-early+late
**** **
Sham MI MI-EPO-early MI-EPO-late MI-EPO-early+late
a
cb
50 μm
***
#
Figure 5a) Tissue sections stained with lectin in the viable free wall of the five different groups, showing individual capillaries. b) Actual measurements for capillary density in number of capillaries per mm2. c) Bar graphs represent-ing the capillary-to-myocyte ratio in the different treatment groups. * p<0.05 vs. MI, ** p<0.01 vs. MI, # p<0.01 vs. Sham.

Chapter 4
60
Discussion
In the present study, the effects of EPO treatment in a rat model of post-MI heart failure were examined. To our knowledge, this study shows for the first time that EPO treatment initiated three weeks after induction of MI results in an improved cardiac function, as shown by a 17% increase of dLVP at 34% reduction in LVEDP and a 46% decrease in N-ANP levels. Further-more, our data indicate that EPO restores capillary density to sham levels and increases the capillary-to-myocyte ratio, indicating neovascularization.
Myocardial structure and cardiac functionPrevious studies already revealed that EPO has ancillary properties besides hematopoiesis. One of the first studies on EPO in the heart showed that EPO injected intraperitoneally for seven days, reduced cardiomyocyte loss by 50% after ischemia-reperfusion injury (25). These observations have been confirmed by others. Parsa et al. showed a 25% reduction in infarct size after 4 days of permanent occlusion of the left circumflex coronary artery in rabbits(12). A single dose of EPO at the onset of MI reduced infarct size, which was accompanied by reductions in LV size and an improved LV ejection fraction, measured by echocardiography, during eight weeks follow-up (26). Our results are in line with these findings; one single dose of EPO administered immediately after induction of MI, reduces infarct size by 30% and im-proves hemodynamics. Mechanisms behind this acute protective effect of EPO may be related to its anti-apoptotic effect. We and others showed that in the acute phase of MI, EPO mark-edly prevents cardiac cells from undergoing programmed cell death (apoptosis)(11;12;15;26). After MI, apoptosis is first observed in endothelial cells of small coronary vessels, spreading to the surrounding cardiomyocytes (27). Since the EPO-receptor is predominantly expressed on endothelial cells, preventing apoptosis in these cells may rescue the underlying myocar-dium (13). Recently, it has been postulated that cardiac fibroblasts may also play a role in the cardioprotective effects of EPO (15). Although a single dose of EPO clearly improves cardiac performance, prolonged EPO treat-ment (MI-EPO-early+late) was associated with a further restoration of cardiac function. Mechanisms involved in this process are most likely distinct from its acute cardioprotective effect. This is clearly demonstrated by the finding that EPO treatment, initiated three weeks after MI, although not reducing infarct size, significantly improves cardiac function, reflected by a 17% increase of dLVP at 34% decrease in LVEDP, and restoring N-ANP levels to sham values. Since the effect of EPO treatment in this group could not be explained by infarct size reduction, other properties of EPO should be considered to elucidate the observed beneficial effects of EPO in heart failure.
NeovascularizationEPO has been shown to possess proangiogenic properties. As discussed above, the EPO-re-ceptor is expressed on endothelial cells and EPO has been shown to stimulate the prolifera-tion and migration of endothelial cells in vitro (6). Additional experiments in chick embryos demonstrated that EPO treatment results in angiogenesis similar to other well-known angio-genic cytokines (6). Furthermore, EPO induces vascular sprouting in a rat aortic ring model (28). In human cultured myocardial tissue, EPO stimulates capillary outgrowth comparable to VEGF (7). In a rodent model of hind-limb ischemia, EPO increases capillary density 1.6-fold (29). In a rat model of chronic renal failure, characterized by left ventricular hypertrophy

Erythropoietin attenuates heart failure
61
and capillary deficiency, EPO treatment results only in a small non-significant increase in cardiac capillary density (30). In a rat model of stroke, EPO treatment initiated 24 hours after infarction, enhances angiogenesis and improves neurological function, while it does not significantly influence infarct size. Our results suggest a similar effect of EPO in the heart. We find that EPO treatment restores capillary density to sham values and increases capillary- to-myocyte ratio, indicating actual capillary growth (24), which is more pronounced in the groups with prolonged EPO treatment. To study the functional consequences of increased capillarization, we examined the expres-sion of different MHC isoforms in heart tissue. Cardiomyocytes express both fast α-MHC and slow β-MHC isoforms, which differ on the basis of ATPase activity. Recently, it has been shown that expression of a small amount of α-MHC (~12%) in rat cardiomyocytes signifi-cantly increases power output, indicating that a small shift in MHC composition as we found in all EPO treated groups may improve contractility(31). Increased capillary density was sig-nificantly correlated with the percentage of β-MHC isoform as well as with myocardial func-tion (+dP/dt
max and -dP/dt
max), providing a link between neovascularization and functional
effects of EPO.The mechanism behind the effect of EPO on new blood vessel formation in the heart remains unknown. In general, stimulation of in situ endothelial cell proliferation or bone marrow- derived endothelial progenitor cells (EPCs) might play a role. Previous work showed that EPO effectively increases the amount of circulating EPCs (32), and significantly induces angio-genesis (29). Future experiments are needed to delineate the mechanism of EPO stimulated capillary growth.
Hematopoietic effectAnother important property of EPO that might be involved in the cardioprotective effect ob-served in our study, is its hematopoietic effect. Human recombinant erythropoietin increases the number of reticulocytes after administration to rats after 3-4 days with maximum after 8-11 days (33). In our study, we observed significant hematocrit elevation one week after a single dose of EPO. In the groups treated with multiple EPO doses, hematocrit remained significantly elevated throughout the experiment. The beneficial effects seen in these groups might thus, in part, be explained on the basis of increased oxygen-carrying capacity of blood. However, the effects of higher red blood cell mass on oxygen delivery is not straightforward, since el-evated hematocrit may downregulate nitric oxide synthesis and thus impair tissue blood flow (34). In the clinical setting, increasing the number of red blood cell mass by blood transfusion has been reported to improve outcome in elderly patients after acute MI (35). Nevertheless, this beneficial effect is only seen in patients with hematocrit <33%. On the other hand, re-duction in the infarct size observed in the early treated groups, could not be attributed to the hematopoietic effect of EPO, since cell death and MI expansion occur mainly during the first 3 days after ischemic insult (26) and thus before significant hematocrit elevation.Conversely, an increase in hematocrit may itself tend to deteriorate myocardial perfusion through adverse rheological effects. Elevated hematocrit levels (up to 80%) in polyglobulic mice, overexpressing EPO, enlarge cerebral infarct volumes and leukocyte infiltration after permanent occlusion of middle cerebral artery (36). Furthermore, EPO administration and consequent higher hematocrit has been associated with other adverse cardiovascular effects. Therapeutic levels of EPO may cause higher incidence of thrombosis (37) and could lead to blood pressure elevation (38). In the present study, rats repeatedly treated with EPO, had a

Chapter 4
62
higher systolic blood pressure. This increase might be related to the improved cardiac func-tion; however, the systolic blood pressure remained below the values observed in the sham operated group.
Clinical ImplicationsIn clinical settings, EPO treatment has already been used to correct anemia in patients with CHF. Anemia is frequently observed in patients with CHF and related to increased morbid-ity and mortality (39;40). Furthermore, not only anemia, but also elevated endogenous EPO levels are independently associated with an impaired outcome in CHF (41). Normalization of hemoglobin levels in mild anemic patients with CHF has a positive effect on LV ejection fraction (42) and peak VO
2 (43). In addition to correction of anemia, other non-hematopoietic
effects of EPO may play a role in the improvement observed in patients with CHF treated with EPO. Besides the treatment of anemia, EPO is currently under investigation for its neuroprotective properties. In the first clinical, randomized, proof-of concept trial, EPO was given to patients with ischemic stroke (44). EPO administration in high-doses (entire dose 100.000 IU/ given in three days) proved to be both safe and beneficial. Patients randomized to the EPO group showed significant improvement in clinical outcome parameters and a trend towards smaller infarct sizes. However, chronic therapy with EPO is also associated with adverse effects related to hemato-crit elevation, such as hypertension and tromboembolic complications. This could be over-come by using a lower dose of EPO, as shown by Bahlmann et al. (45). In this study, low-dose of darbepoetin (0.1 μg/kg/week) rendered tissue protection in the kidneys even without raising hematocrit levels. The recently discovered non-hematopoietic derivates of EPO, re-taining tissue protection, but without the undesired effects on hematopoiesis may become another possibility for chronic administration (46).
LimitationsSeveral limitations of the present study have to be acknowledged. Although a clear increase in capillary density and capillary-to-myocyte ratio was observed, the improvement of cardiac function might also be related to other effects of EPO treatment. Since we did not perform sequential measurements of cardiac function, further studies would be needed to specifically denote the time-dependent effect of EPO treatment on attenuation of heart failure develop-ment. We did not measure the direct myocardial perfusion, and therefore functional evidence of an improved perfusion remains unclear. However, we observed a clear correlation between capillary density and β-MHC expression and cardiac function. Furthermore, we used the Fisher’s LSD post-hoc statistical test for analyzing our data, which does not control for mul-tiple comparisons.
Erythropoietin attenuates heart failure
63
Conclusion
In summary, the present study demonstrates that EPO treatment in a rat model of heart fail-ure improves cardiac function beyond its effect on infarct size reduction. This improvement could be explained by the increased capillary density and capillary-to-myocyte ratio, indicat-ing formation of new blood vessels.
Acknowledgments
We thank Richard van Veghel for his expert technical assistance. We further thank dr. Frans Boomsma for N-ANP measurements.
Chapter 4
64
Reference List1. Anagnostou A, Liu Z, Steiner M et al. Erythropoietin receptor mRNA expression in human endothelial cells. Proc
Natl Acad Sci U S A 1994;91:3974-8.
2. Chong ZZ, Kang JQ, Maiese K. Erythropoietin is a novel vascular protectant through activation of Akt1 and mitochondrial modulation of cysteine proteases. Circulation 2002;106:2973-9.
3. Van der Meer P., Voors AA, Lipšic E, van Gilst WH, van Veldhuisen DJ. Erythropoietin in cardiovascular diseases. Eur Heart J 2004;25:285-91.
4. Wright GL, Hanlon P, Amin K, Steenbergen C, Murphy E, Arcasoy MO. Erythropoietin receptor expression in adult rat cardiomyocytes is associated with an acute cardioprotective effect for recombinant erythropoietin during ischemia-reperfusion injury. Faseb J 2004;18:1031-3.
5. De Boer RA, Pinto YM, van Veldhuisen DJ. The imbalance between oxygen demand and supply as a potential mechanism in the pathophysiology of heart failure: The role of microvascular growth and abnormalities. Mi-crocirculation 2003;10:113-26.
6. Ribatti D, Presta M, Vacca A et al. Human erythropoietin induces a pro-angiogenic phenotype in cultured en-dothelial cells and stimulates neovascularization in vivo. Blood 1999;93:2627-36.
7. Jaquet K, Krause K, Tawakol-Khodai M, Geidel S, Kuck K. Erythropoietin and VEGF exhibit equal angiogenic potential. Microvasc Res 2002;64:326-33.
8. Wang L, Zhang ZG, Wang Y, Zhang RL, Chopp M. Treatment of stroke with erythropoietin enhances neurogen-esis and angiogenesis and improves neurological function in rats. Stroke 2004;35:1732-7.
9. Sakanaka M, Wen TC, Matsuda S et al. In vivo evidence that erythropoietin protects neurons from ischemic damage. Proc Natl Acad Sci U S A 1998;95:4635-40.
10. Siren AL, Fratelli M, Brines M et al. Erythropoietin prevents neuronal apoptosis after cerebral ischemia and metabolic stress. Proc Natl Acad Sci U S A 2001;98:4044-9.
11. Lipšic E, van der Meer P, Henning RH et al. Timing of erythropoietin treatment for cardioprotection in isch-emia/reperfusion. J Cardiovasc Pharmacol 2004;44:473-9.
12. Parsa CJ, Matsumoto A, Kim J et al. A novel protective effect of erythropoietin in the infarcted heart. J Clin Invest 2003;112:999-1007.
13. Van der Meer P, Lipšic E, Henning RH et al. Erythropoietin improves left ventricular function and coronary flow in an experimental model of ischemia-reperfusion injury. Eur J Heart Fail 2004;6:853-9.
14. Cai ZQ, Semenza GL. Phosphatidylinositol-3-kinase signaling is required for erythropoietin-mediated acute protection against myocardial ischemia/reperfusion injury. Circulation 2004;109:2050-3.
15. Parsa CJ, Kim J, Riel RU et al. Cardioprotective effects of erythropoietin in the reperfused ischemic heart - A potential role for cardiac fibroblasts. J Biol Chem 2004;279:20655-62.
16. Van Kerckhoven R, van Veghel R, Saxena PR, Schoemaker RG. Pharmacological therapy can increase capillary density in post-infarction remodeled rat hearts. Cardiovasc Res 2004;61:620-9.
Erythropoietin attenuates heart failure
65
17. Pfeffer JM, Pfeffer MA, Fletcher PJ, Braunwald E. Progressive ventricular remodeling in rat with myocardial infarction. Am J Physiol 1991;260:H1406-H1414.
18. Wang Y, Zhang ZG, Wang L, Zhang RL, Chopp M. Erythropoietin enhances neurogenesis and angiogenesis in the brain and improves functional recovery after embolic stroke in the adult rat. Stroke 2004;35:239.
19. De Boer RA, Pinto YM, Suurmeijer AJ et al. Increased expression of cardiac angiotensin II type 1 (AT(1)) receptors decreases myocardial microvessel density after experimental myocardial infarction. Cardiovasc Res 2003;57:434-42.
20. Loot AE, Roks AJM, Henning RH et al. Angiotensin-(1-7) attenuates the development of heart failure after myocardial infarction in rats. Circulation 2002;105:1548-50.
21. Nelissen-Vrancken HJMG, Kuizinga MC, Daemen MJAP, Smits JFM. Early captopril treatment inhibits DNA synthesis in endothelial cells and normalization of maximal coronary flow in infarcted rat hearts. Cardiovasc Res 1998;40:156-64.
22. Kalkman EAJ, Bilgin YM, vanHaren P, van Suylen RJ, Saxena PR, Schoemaker RG. Determinants of coronary reserve in rats subjected to coronary artery ligation or aortic banding. Cardiovasc Res 1996;32:1088-95.
23. Van der Velden J, Moorman AFM, Stienen GJM. Age-dependent changes in myosin composition correlate with enhanced economy of contraction in guinea-pig hearts. J Physiol 1998;507:497-510.
24. Sladek T, Sladkova J, Kolar F et al. The effect of AT1 receptor antagonist on chronic cardiac response to coronary artery ligation in rats. Cardiovasc Res 1996;31:568-76.
25. Calvillo L, Latini R, Kajstura J et al. Recombinant human erythropoietin protects the myocardium from isch-emia- reperfusion injury and promotes beneficial remodeling. Proc Natl Acad Sci U S A 2003;100:4802-6.
26. Moon C, Krawczyk M, Ahn D et al. Erythropoietin reduces myocardial infarction and left ventricular functional decline after coronary artery ligation in rats. Proc Natl Acad Sci U S A 2003;100:11612-7.
27. Scarabelli T, Stephanou A, Rayment N et al. Apoptosis of endothelial cells precedes myocyte cell apoptosis in ischemia/reperfusion injury. Circulation 2001;104:253-6.
28. Carlini RG, Reyes AA, Rothstein M. Recombinant-Human-Erythropoietin Stimulates Angiogenesis In-Vitro. Kidney Int 1995;47:740-5.
29. Heeschen C, Aicher A, Lehmann R et al. Erythropoietin is a potent physiologic stimulus for endothelial pro-genitor cell mobilization. Blood 2003;102:1340-6.
30. Amann K, Buzello M, Simonaviciene A et al. Capillary/myocyte mismatch in the heart in renal failure - a role for erythropoietin? Nephrol Dial Transplant 2000;15:964-9.
31. Herron TJ, McDonald KS. Small amounts of alpha-myosin heavy chain isoform expression significantly increase power output of rat cardiac myocyte fragments. Circ Res 2002;90:1150-2.
32. Bahlmann FH, DeGroot K, Duckert T et al. Endothelial progenitor cell proliferation and differentiation is regu-lated by erythropoietin - Rapid communication. Kidney International 2003;64:1648-52.
33. Eder H, Rosslenbroich B, Failing K. A dose-dependent effect of recombinant erythropoietin on the reticulocyte population of rats. Blut 1989;59:184-7.

Chapter 4
66
34. Ruschitzka FT, Wenger RH, Stallmach T et al. Nitric oxide prevents cardiovascular disease and determines sur-vival in polyglobulic mice overexpressing erythropoietin. Proc Natl Acad Sci U S A 2000;97:11609-13.
35. Wu WC, Rathore SS, Wang Y, Radford MJ, Krumholz HM. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med 2001;345:1230-6.
36. Wiessner C, Allegrini PR, Ekatodramis D, Jewell UR, Stallmach T, Gassmann M. Increased cerebral infarct vol-umes in polyglobulic mice overexpressing erythropoietin. J Cereb Blood Flow Metab 2001;21:857-64.
37. Wolf RF, Gilmore LS, Friese P, Downs T, Burstein SA, Dale GL. Erythropoietin potentiates thrombus develop-ment in a canine arterio-venous shunt model. Thromb Haemost 1997;77:1020-4.
38. Roger SD, Baker LR, Raine AE. Autonomic dysfunction and the development of hypertension in patients treated with recombinant human erythropoietin (r-HuEPO). Clin Nephrol 1993;39:103-10.
39. McMurray JJ. What are the clinical consequences of anemia in patients with chronic heart failure? J Card Fail 2004;10:S10-S12.
40. Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, Borenstein J. Anemia is associated with worse symp-toms, greater impairment in functional capacity and a significant increase in mortality in patients with ad-vanced heart failure. J Am Coll Cardiol 2002;39:1780-6.
41. Van der Meer P, Voors AA, Lipšic E, Smilde TDJ, van Gilst WH, van Veldhuisen DJ. Prognostic value of plasma erythropoietin on mortality in patients with chronic heart failure. J Am Coll Cardiol 2004;44:63-7.
42. Silverberg DS, Wexler D, Sheps D et al. The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study. J Am Coll Cardiol 2001;37:1775-80.
43. Mancini DM, Katz SD, Lang CC, LaManca J, Hudaihed A, Androne AS. Effect of erythropoietin on exercise capac-ity in patients with moderate to severe chronic heart failure. Circulation 2003;107:294-9.
44. Ehrenreich H, Hasselblatt M, Dembowski C et al. Erythropoietin therapy for acute stroke is both safe and ben-eficial. Mol Med 2002;8:495-505.
45. Bahlmann FH, Song R, Boehm SM et al. Low-dose therapy with the long-acting erythropoietin analogue darbepoetin alpha persistently activates endothelial Akt and attenuates progressive organ failure. Circulation 2004;110:1006-12.
46. Fiordaliso F, Chimenti S, Staszewsky L et al. A nonerythropoietic derivative of erythropoietin protects the myocardium from ischemia-reperfusion injury. Proc Natl Acad Sci U S A 2005;102:2046-51.


Chapter 5
Erythropoietin attenuates heart failure in a
hematocrit independent manner
Erik Lipšic, Peter van der Meer, Pim van der Harst, B. Daan Westenbrink,
Johan Koster, Gideon J. du Marchie Sarvaas, Adriaan A. Voors, Dirk J. van Veldhuisen, Regien G. Schoemaker, Wiek H. van Gilst
Submitted

Chapter 5
70
Abstract
Objective: The hematopoietic hormone erythropoietin (EPO) induces postnatal neovasculariza-tion and stimulates endothelial progenitor cells (EPCs). We hypothesized that EPO mobilizes EPCs, increases capillarization and preserves cardiac function in post-myocardial infarction (MI) heart failure, independent of erythropoietic effects.Methods and Results: Rats underwent coronary ligation and were left untreated (MI group) or long-acting EPO analogue darbepoetin treatment was started 3 weeks after MI in a low-dose (0.4 μg/kg/3 weeks, MI-EPO-low) or high-dose (40 μg/kg/3 weeks, MI-EPO-high). Hematocrit increased in the MI-EPO-high, but not in MI-EPO-low group (p<0.01). In both EPO-treated groups, serial echocardiography demonstrated preservation of left ventricular systolic function, and hemodynamic measurements revealed improved cardiac contractility (dP/dt
max) and relaxation (dP/dt
min) at 9-weeks, compared to MI group (all p<0.05). In addi-
tion, in EPO-treated groups the number of EPCs was significantly increased (MI-EPO-high: 82 [66-147] and MI-EPO-low: 67 [55-107] vs. MI: 23 [19-33] cells/high-power field; both p<0.01). This was associated with a 42% increase in capillary-to-myocyte ratio in MI-EPO-high (p<0.01) and 28% in MI-EPO-low (p<0.05), compared to MI group.Conclusions: EPO treatment preserves cardiac function in post-MI heart failure, even in non-erythropoietic doses. This is associated with EPCs mobilization and induction of neovascu-larization.
Introduction
The classical role of erythropoietin (EPO) is related to its hematopoietic effects. EPO is pro-duced in kidneys and acts as a major regulator of erythropoiesis, by increasing survival and promoting proliferation of erythroid precursor cells. Recently, several non-erythropoietic effects of EPO have been reported. EPO was shown to render vascular protection in various experimental models of ischemia, including stroke and myocardial infarction (1). During ex-vivo ischemia-reperfusion in isolated rat hearts, EPO perfusion improved cardiac function and increased coronary flow (2,3). Acute, systemic treat-ment with EPO, in a rodent ischemia-reperfusion model, substantially reduced infarct size and decreased myocardial apoptosis (4), even when EPO was administered after reperfu-sion(5). In addition, EPO was shown to promote postnatal neovascularization, at least in part by en-hancing endothelial progenitor cells (EPCs) mobilization from the bone marrow (6). EPCs-mediated neovascularization of the peri-infarct zone prevents ventricular remodeling and improves cardiac function (7). Interestingly, the level of EPCs predicts cardiovascular out-comes in patients with coronary artery disease (8). Recently, we assessed the effects of EPO treatment in a rat model of post-myocardial infarc-tion (MI) heart failure. In this study, prolonged high-dose EPO treatment was associated with improved cardiac function and neovascularization (9). However, because high-dose EPO treatment is also associated with increased hematocrit val-ues, the observed beneficial effects may, at least to some extend, be related to the increased oxygen-carrying capacity of blood. In the clinical situation, repeated therapy with high-dose EPO could lead to unwanted elevation of hematocrit, coupled with higher risk for thrombo-

Hematocrit independent effects of erythropoietin
71
sis and hypertension. In addition, the existence of different receptors that mediate the effects of EPO in distinct tissues (10), may suggest also different dose-response relationships for the various protective effects.Therefore, we studied the effects of high- and low-dose EPO treatment on cardiac function over time, EPCs mobilization and neovascularization in a post-MI heart failure.
Methods
AnimalsWe used male Sprague Dawley rats weighing 270-330 g (Harlan, Zeist, The Netherlands). Animals were fed ad libitum, and housed in groups of four to five rats, according to institu-tional rules with 12:12 hours light-dark cycles. The experimental protocol was approved by the Animal Ethical Committee of the University of Groningen.
Design of the studyRats were either subjected to left coronary artery ligation (n=63) or sham surgery (n=11). Rats with MI were allocated to 3 groups: control (MI) and two EPO treatment groups with different dosages of long-acting EPO analogue darbepoetin: 40 μg/kg (MI-EPO-high) and 0.4 μg/kg (MI-EPO-low). Darbepoetin-alpha (Aranesp, Amgen Inc., Thousands Oaks, CA, USA) was administered intraperitoneally, once every three weeks, starting three weeks after the coronary artery ligation, hence after the healing phase of MI. Control (MI) and SHAM rats received corresponding injections of saline. The allocation of MI rats to different groups was based on echocardiography performed at week 3 (before the start of the therapy), groups were matched based on left ventricular (LV) end-diastolic diameter and LV fractional shortening.The high dose of darbepoetin was based on our previous study (9), demonstrating increased neovascularization in this model, together with significant elevation of hematocrit levels. To avoid the effect of EPO treatment on hematocrit we included a low-dose EPO group, with 100-times lower darbepoetin dosage (0.4 μg/kg/3 weeks), which in our pilot experiment did not cause elevation of hematocrit (data not shown). Hematocrit was measured at base-line and at week 3, 4, 6 and 9 after surgery.
Myocardial infarction modelThis model has been described previously (11). Briefly, rats were anesthetized with 2.5% isoflurane and placed on a heating pad (370C). Animals were intubated and mechanically ventilated (Amsterdam Infant Ventilator, Hoek/Loos, Schiedam, The Netherlands; frequency 90/min) using room air enriched with 1.0 l/min oxygen. After left-side thoracotomy, MI was induced by ligating the proximal portion of the left coronary artery, beneath the left atrial appendage. In sham operated rats, the same surgery was performed, without ligating the suture.
Echocardiographic measurementsCardiac function was assessed by echocardiography (Vivid 7, GE Healthcare, Chalfont St. Giles, United Kingdom; equipped with a 10-Mhz phase array linear transducer) at baseline

Chapter 5
72
(before coronary artery ligation), at week 3 (before start of the therapy), 6 and 8. The echo-cardiographic measurements were performed under general anesthesia with 2.5% isoflurane, by two researchers blinded for the treatment allocation. The transducer was applied paraster-nally and maneuvered to obtain both 2-dimensional (2D) images in parasternal long-axis and short-axis view and 2-D guided M-mode tracing. Long axis views were obtained, ensuring that the mitral and aortic valves and the apex were visualized. Short axis views were recorded at the level of mid-papillary muscles. LV end-systolic diameter (LVESD) and LV end-diastolic diameter (LVEDD) were measured from the M-mode and calculated as an average from short- and long-axis view. LV fractional shortening (FS %) was calculated as FS= (LVEDD-LVESD)/LVEDD x 100. LV ejection fraction (EF %) was calculated using the Teichholz method of esti-mated LV volumes (12).
Hemodynamic measurementsAfter nine weeks rats were anesthetized as described above. Microtip pressure transducer (Millar Instr. Inc., Houston, Texas, USA) was inserted into the left ventricular cavity via the right carotid artery. After a 3-min period of stabilization, heart rate (HR), left ventricular systolic pressure (LVSP), left ventricular end-diastolic pressure (LVEDP), and developed left ventricular pressure (dLVP=LVSP-LVEDP) were measured. As indices of contractility and relaxation, the maximal rates of increase and decrease in LVP (dP/dt
max and dP/dt
min) were determined. The
catheter was retracted into the aortic arch and arterial systolic and diastolic blood pressures (SBP, DBP) were recorded.
Infarct size and myocyte hypertrophyAfter hemodynamic measurements, hearts were rapidly excised and weighed. Mid-papil-lary slices were fixed in 4% paraformaldehyde and paraffin-embedded. Infarct size was de-termined by planimeter in transverse slices on picrosirius red/fast green–stained sections. Infarct size was expressed as the percentage of scar length to total left ventricular circum-ference, as described previously (13). Deparaffinized 5-μm thick sections were stained with a Gomori’s silver staining. Using image analysis (Zeiss KS 400, Jena, Germany), concentric myocyte hypertrophy in the viable LV wall, remote from the infarcted area, was measured as the cross-sectional area of transversally cut myocytes showing a nucleus (11). Myocyte density was calculated as the average number of myocytes per tissue area (mm2). In each stained sec-tion, measurements were averaged from three different counting fields (± 75 myocytes per heart).
Blood derived endothelial progenitor cellsFull blood was collected in heparine tubes (17 IU/ml). Mononuclear cells were isolated us-ing Histopaque-1083 (Sigma Chemical, St. Louis, MO, USA) according to the instructions as supplied by the manufacturer and counted on microcellcounter (Sysmex F-800, Toa Medical Electronics, Kobe, Japan). Isolated mononuclear cells (1×106) were seeded into fibronectin-precoated 24-well plates (BD BioCoat, Bedford, MA, USA) in EndoCult medium (StemCell Technologies, London, UK) supplemented with Penicillin (100 U/mL) and Streptomycin (100 μg/mL). After 6 days, adherent cells were washed with medium, incubated with 1,1’-dioctadecyl-3,3,3’,3’-tetramethylindocarbocyanine-labeled acetylated LDL (10 μg/mL DiT AcLDL; Molecular Probes, Invitrogen, Carlsbad, CA, USA) for 12 hours, fixed with 1% para-formaldehyde for 10 minutes, and counterstained with fluorescein isothyiocyanate-labeled
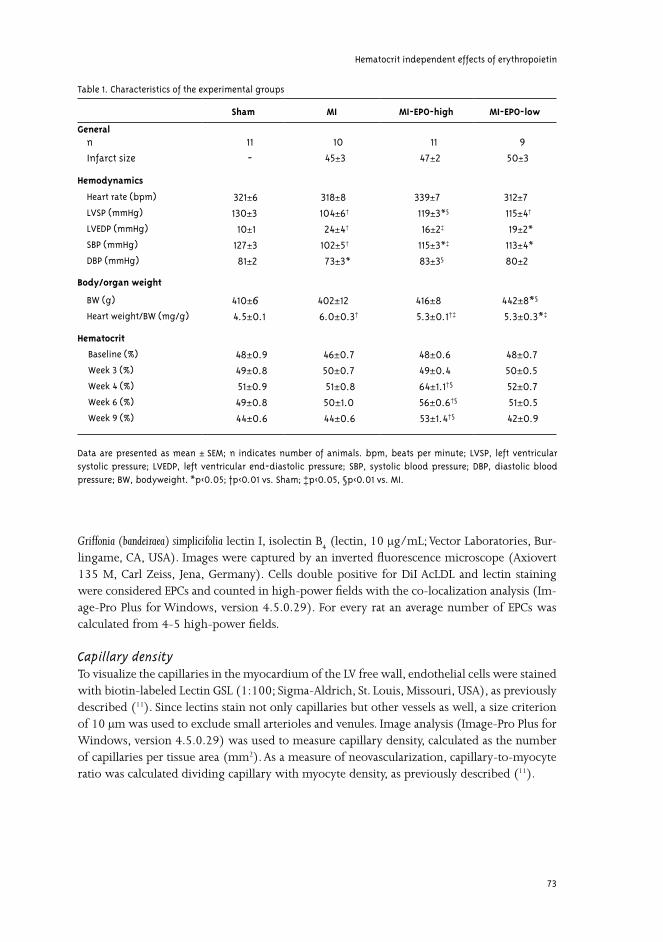
Hematocrit independent effects of erythropoietin
73
Griffonia (bandeiraea) simplicifolia lectin I, isolectin B4 (lectin, 10 μg/mL; Vector Laboratories, Bur-
lingame, CA, USA). Images were captured by an inverted fluorescence microscope (Axiovert 135 M, Carl Zeiss, Jena, Germany). Cells double positive for DiI AcLDL and lectin staining were considered EPCs and counted in high-power fields with the co-localization analysis (Im-age-Pro Plus for Windows, version 4.5.0.29). For every rat an average number of EPCs was calculated from 4-5 high-power fields.
Capillary densityTo visualize the capillaries in the myocardium of the LV free wall, endothelial cells were stained with biotin-labeled Lectin GSL (1:100; Sigma-Aldrich, St. Louis, Missouri, USA), as previously described (11). Since lectins stain not only capillaries but other vessels as well, a size criterion of 10 μm was used to exclude small arterioles and venules. Image analysis (Image-Pro Plus for Windows, version 4.5.0.29) was used to measure capillary density, calculated as the number of capillaries per tissue area (mm2). As a measure of neovascularization, capillary-to-myocyte ratio was calculated dividing capillary with myocyte density, as previously described (11).
Table 1. Characteristics of the experimental groups
Sham MI MI-EPO-high MI-EPO-low
Generaln
Infarct size
11
-
10
45±±3
11
47±2
9
50±3
Hemodynamics
Heart rate (bpm)
LVSP (mmHg)
LVEDP (mmHg)
SBP (mmHg)
DBP (mmHg)
321±6
130±3
10±1
127±3
81±2
318±8
104±6†
24±4†
102±5†
73±3*
339±7
119±3*§
16±2‡
115±3*‡
83±3§
312±7
115±4†
19±2*
113±4*
80±2
Body/organ weight
BW (g)
Heart weight/BW (mg/g)
410±6 4.5±0.1
402±12
6.0±0.3†
416±8
5.3±0.1†‡
442±8*§
5.3±0.3*‡
Hematocrit
Baseline (%)
Week 3 (%)
Week 4 (%)
Week 6 (%)
Week 9 (%)
48±0.9
49±0.8
51±0.9
49±0.8
44±0.6
46±0.7
50±0.7
51±0.8
50±1.0
44±0.6
48±0.6
49±0.4
64±1.1†§
56±0.6†§
53±1.4†§
48±0.7
50±0.5
52±0.7
51±0.5
42±0.9
Data are presented as mean ± SEM; n indicates number of animals. bpm, beats per minute; LVSP, left ventricular systolic pressure; LVEDP, left ventricular end-diastolic pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; BW, bodyweight. *p<0.05; †p<0.01 vs. Sham; ‡p<0.05, §p<0.01 vs. MI.
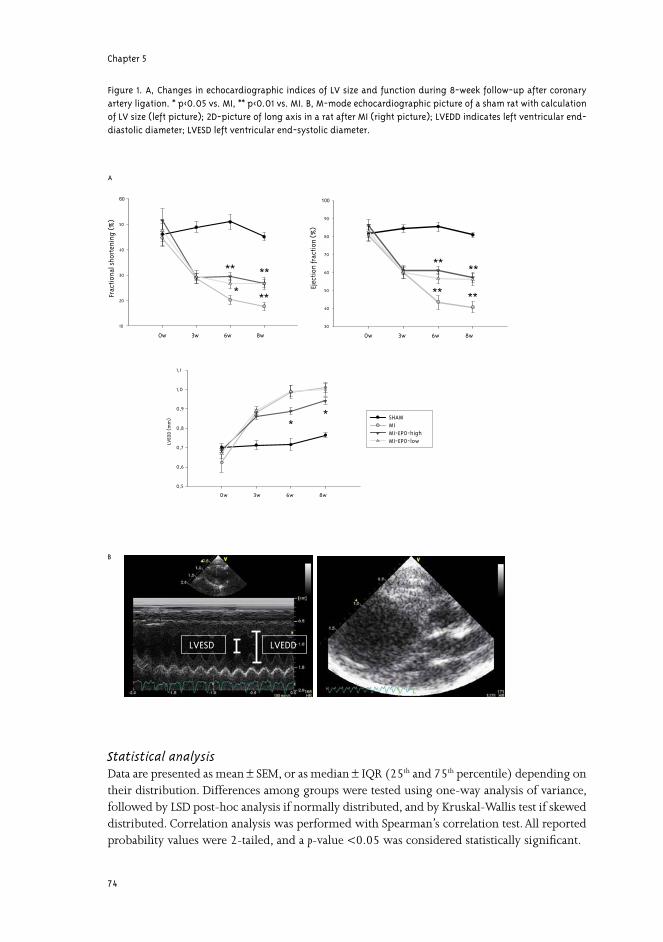
Chapter 5
74
Statistical analysisData are presented as mean ± SEM, or as median ± IQR (25th and 75th percentile) depending on their distribution. Differences among groups were tested using one-way analysis of variance, followed by LSD post-hoc analysis if normally distributed, and by Kruskal-Wallis test if skewed distributed. Correlation analysis was performed with Spearman’s correlation test. All reported probability values were 2-tailed, and a p-value <0.05 was considered statistically significant.
0w 3w 6w 8w
LVED
D(m
m)
0,5
0,6
0,7
0,8
0,9
1,0
1,1
SHAMMIMI-EPO-highMI-EPO-low
**
0w 3w 6w 8w
Frac
tion
alsh
orte
ning
(%)
10
20
30
40
50
60
*
** **
**
0w 3w 6w 8w
Ejec
tion
frac
tion
(%
)
30
40
50
60
70
80
90
100
**
**
**
**
LVEDDLVESD
A
B
Figure 1. A, Changes in echocardiographic indices of LV size and function during 8-week follow-up after coronary artery ligation. * p<0.05 vs. MI, ** p<0.01 vs. MI. B, M-mode echocardiographic picture of a sham rat with calculation of LV size (left picture); 2D-picture of long axis in a rat after MI (right picture); LVEDD indicates left ventricular end-diastolic diameter; LVESD left ventricular end-systolic diameter.
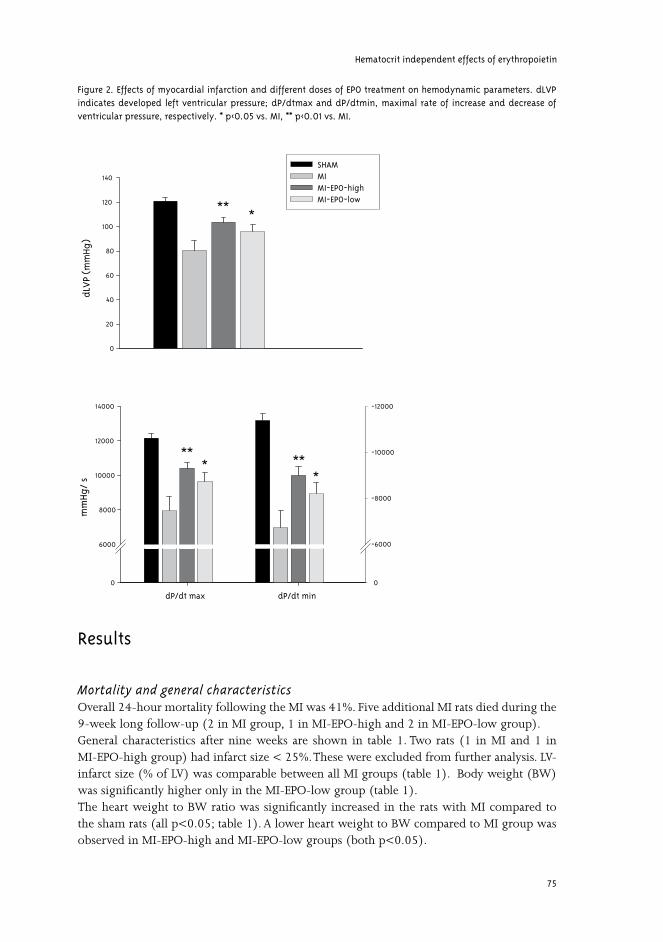
Hematocrit independent effects of erythropoietin
75
Results
Mortality and general characteristicsOverall 24-hour mortality following the MI was 41%. Five additional MI rats died during the 9-week long follow-up (2 in MI group, 1 in MI-EPO-high and 2 in MI-EPO-low group).General characteristics after nine weeks are shown in table 1. Two rats (1 in MI and 1 in MI-EPO-high group) had infarct size < 25%. These were excluded from further analysis. LV-infarct size (% of LV) was comparable between all MI groups (table 1). Body weight (BW) was significantly higher only in the MI-EPO-low group (table 1). The heart weight to BW ratio was significantly increased in the rats with MI compared to the sham rats (all p<0.05; table 1). A lower heart weight to BW compared to MI group was observed in MI-EPO-high and MI-EPO-low groups (both p<0.05).
dLV
P(m
mHg
)
0
20
40
60
80
100
120
140
SHAMMIMI-EPO-highMI-EPO-low
dP/dt max dP/dt min
mm
Hg/
s
0
6000
8000
10000
12000
14000 -12000
-10000
-8000
-6000
0
** *
*** **
*
Figure 2. Effects of myocardial infarction and different doses of EPO treatment on hemodynamic parameters. dLVP indicates developed left ventricular pressure; dP/dtmax and dP/dtmin, maximal rate of increase and decrease of ventricular pressure, respectively. * p<0.05 vs. MI, ** p<0.01 vs. MI.
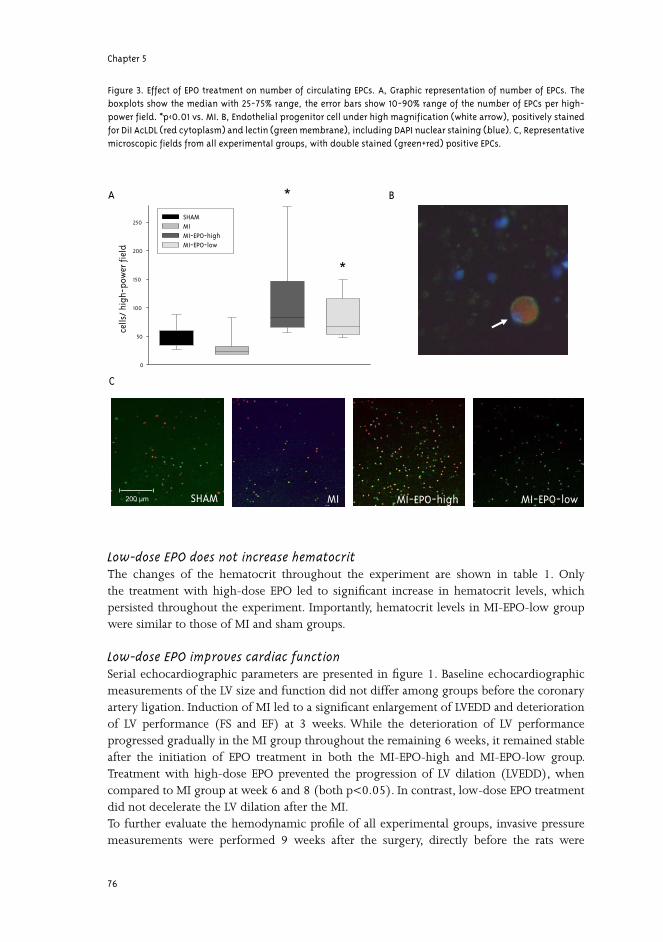
Chapter 5
76
Low-dose EPO does not increase hematocritThe changes of the hematocrit throughout the experiment are shown in table 1. Only the treatment with high-dose EPO led to significant increase in hematocrit levels, which persisted throughout the experiment. Importantly, hematocrit levels in MI-EPO-low group were similar to those of MI and sham groups.
Low-dose EPO improves cardiac functionSerial echocardiographic parameters are presented in figure 1. Baseline echocardiographic measurements of the LV size and function did not differ among groups before the coronary artery ligation. Induction of MI led to a significant enlargement of LVEDD and deterioration of LV performance (FS and EF) at 3 weeks. While the deterioration of LV performance progressed gradually in the MI group throughout the remaining 6 weeks, it remained stable after the initiation of EPO treatment in both the MI-EPO-high and MI-EPO-low group. Treatment with high-dose EPO prevented the progression of LV dilation (LVEDD), when compared to MI group at week 6 and 8 (both p<0.05). In contrast, low-dose EPO treatment did not decelerate the LV dilation after the MI. To further evaluate the hemodynamic profile of all experimental groups, invasive pressure measurements were performed 9 weeks after the surgery, directly before the rats were
cells
/ hi
gh-p
ower
fiel
d
0
50
100
150
200
250SHAMMIMI-EPO-highMI-EPO-low
SHAM MI MI-EPO-high MI-EPO-low
A
C
*
*
B
200 μm
Figure 3. Effect of EPO treatment on number of circulating EPCs. A, Graphic representation of number of EPCs. The boxplots show the median with 25-75% range, the error bars show 10-90% range of the number of EPCs per high-power field. *p<0.01 vs. MI. B, Endothelial progenitor cell under high magnification (white arrow), positively stained for DiI AcLDL (red cytoplasm) and lectin (green membrane), including DAPI nuclear staining (blue). C, Representative microscopic fields from all experimental groups, with double stained (green+red) positive EPCs.
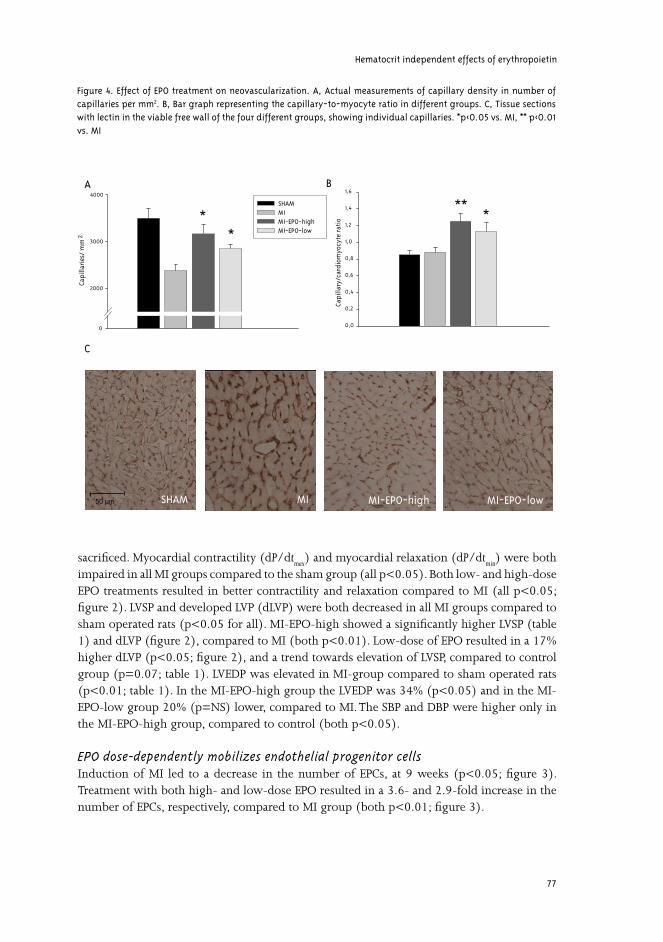
Hematocrit independent effects of erythropoietin
77
sacrificed. Myocardial contractility (dP/dtmax
) and myocardial relaxation (dP/dtmin
) were both impaired in all MI groups compared to the sham group (all p<0.05). Both low- and high-dose EPO treatments resulted in better contractility and relaxation compared to MI (all p<0.05; figure 2). LVSP and developed LVP (dLVP) were both decreased in all MI groups compared to sham operated rats (p<0.05 for all). MI-EPO-high showed a significantly higher LVSP (table 1) and dLVP (figure 2), compared to MI (both p<0.01). Low-dose of EPO resulted in a 17% higher dLVP (p<0.05; figure 2), and a trend towards elevation of LVSP, compared to control group (p=0.07; table 1). LVEDP was elevated in MI-group compared to sham operated rats (p<0.01; table 1). In the MI-EPO-high group the LVEDP was 34% (p<0.05) and in the MI-EPO-low group 20% (p=NS) lower, compared to MI. The SBP and DBP were higher only in the MI-EPO-high group, compared to control (both p<0.05).
EPO dose-dependently mobilizes endothelial progenitor cells Induction of MI led to a decrease in the number of EPCs, at 9 weeks (p<0.05; figure 3). Treatment with both high- and low-dose EPO resulted in a 3.6- and 2.9-fold increase in the number of EPCs, respectively, compared to MI group (both p<0.01; figure 3).
Capi
llari
es/
mm
2
0
2000
3000
4000
SHAMMIMI-EPO-highMI-EPO-low
*
A
C
*
MI MI-EPO-high MI-EPO-lowSHAM50 μm
Capi
llary
/car
diom
yocy
tera
tio
0,0
0,2
0,4
0,6
0,8
1,0
1,2
1,4
1,6B
** *
Figure 4. Effect of EPO treatment on neovascularization. A, Actual measurements of capillary density in number of capillaries per mm2. B, Bar graph representing the capillary-to-myocyte ratio in different groups. C, Tissue sections with lectin in the viable free wall of the four different groups, showing individual capillaries. *p<0.05 vs. MI, ** p<0.01 vs. MI

Chapter 5
78
Low- and high-dose EPO treatment induces neovascularizationFigure 4C shows representative photomicrographs of the four different groups. Capillary density was significantly reduced in MI compared to sham-group (p<0.01). High-dose EPO treatment prevented the decrease in capillary density after induction of MI and restored it to sham values, as shown in Figure 4A (p=NS vs. sham). In this group (MI-EPO-high) we observed a 33% increase in capillary density compared to MI group (p<0.01). Treatment with low-dose EPO resulted in a 20% higher capillary density (p<0.05). The cross-sectional area of cardiomyocytes increased in MI compared to sham group (290±16 vs. 204±10 μm2; p<0.01). EPO treatment had no effect on attenuation of myocyte hypertrophy (MI-EPO-high: 286±15 and MI-EPO-low: 323±27 μm2). However, the capillary-to-myocyte ratio increased by 42% in MI-EPO-high (p<0.01) and by 28% in MI-EPO-low (p<0.05), compared to MI group (figure 4B). The differences between MI-EPO-high and MI-EPO-low group were not statistically significant.In order to relate mobilization of EPCs to increased capillary-to-myocyte ratio, correlations were determined. We observed a positive correlation between the capillary-to-myocyte ratio and the number of peripheral EPCs (r=0.48, p<0.01), which was even stronger in the rats subjected to coronary artery ligation (r=0.60, p<0.01).
Discussion
In the present study, we demonstrate beneficial effects of EPO on cardiac function in a post-MI heart failure model, without affecting hematocrit. Furthermore, this is associated with mobilization of EPCs and increased capillary-to-myocyte ratio, indicating new vascular growth.Recently, several experimental studies have demonstrated important ancillary functions of EPO, such as protection against ischemic injury in various tissues. In the first in vivo study on the EPO effects in the heart, Calvillo et al. (14), employed a rat model of coronary ischemia-reperfusion. Administration of EPO (5.000 IU/kg/day) for seven consecutive days after reperfusion reduced the loss of cardiomyocytes by 50%, an extent sufficient to normalize hemodynamic function. However, the hematocrit increased by 20-30% by the end of the study, and to some degree, such a change could lead to improved cardiac function merely by improving the delivery of oxygen. In the clinical setting, current therapy in patients after MI is focused on prevention of ventricular remodeling and development of heart failure. Myocardial regeneration may offer possibilities that could improve cardiac function in these patients (15). Although cardiomyocytes proliferation after ischemic injury seems limited, the formation of new vessels in the non-infarcted part of the ventricle could lead to an improvement of function and attenuation of ventricular remodeling (16,17). EPO was recently shown to mobilize EPCs from the bone marrow, which was associated with neovascularization (vasculogenesis) of ischemic tissue (6). EPO has also been shown to stimulate proliferation of endothelial cells in situ (angiogenesis) (18). The effect of EPO on the formation of new vessels has been observed in an experimental model of stroke. EPO treatment, initiated 24 hours after induction of stroke, enhanced neovascularization and improved neurological function, whereas it did not significantly influence infarct size(19). In this study, high-dose EPO treatment increased the density of microvessels at the stroke
Hematocrit independent effects of erythropoietin
79
boundary (ischemic penumbra), but it also resulted in a 44% increase in hematocrit level.We addressed this issue in the heart, evaluating the effect of EPO treatment on new vascular formation in an experimental heart failure model (9). Rats were subjected to coronary artery ligation and therapy with high-dose EPO analogue darbepoetin was initiated 3-weeks post-MI. Although not reducing infarct size, EPO treatment significantly improved cardiac function. This improvement was coupled to increased capillary density and capillary-to-myocyte ratio, indicating neovascularization. Furthermore, these beneficial effects were also associated with increased percentage of alpha-MHC (myosine-heavy chain) isoforms, a molecular marker of enhanced myocardial contractility.However, the dosages used in the previous studies, when applied to clinical situation, could cause EPO overdose which may lead to hypertension, seizures, vascular thrombosis and death, possibly related to abruptly increased hematocrit values (20). This could be of potential concern in patients with already elevated cardiovascular risk.In the present study, we investigated effects of a non-erythropoietic EPO dose to avoid elevation of hematocrit, and consequently the changes in rheology and oxygen-binding capacity of the blood, which could both influence our results. We compared these effects to those of a high EPO dose (MI-EPO-high), leading to marked hematocrit elevation, which effects on cardiac function in post-MI heart failure were already established (9). The low-dose of EPO was two orders of magnitude lower compared to high-dose. We did not observe any differences in hematocrit levels between the MI-EPO-low and both saline treated groups (MI and sham), while in MI-EPO-high the hematocrit remained significantly elevated during the treatment follow-up.Treatment with low-dose EPO prevented the deterioration of LV function over time, as assessed by LV ejection fraction and fractional shortening, serially evaluated by echocardiography. However, low-dose EPO, as opposed to high-dose, did not avoid the progression of LV dilation. While this could mean a dose-dependent effect of EPO, bigger infarct size in MI-EPO-low group, although not significantly different from other groups, could have averted the beneficial effects of EPO on LV geometry. Low-dose EPO treatment thus, in spite of advanced LV dilation, improves contractile properties of the non-infarcted part of the myocardium. Importantly, this effect was also confirmed by invasive hemodynamic measurements at the end of the study. Although the treatment with high-dose resulted in noticeable improved cardiac function, low-dose treatment also caused a significant enhancement of developed LVP, together with contractility and relaxation indices of the LV. We confirmed the findings of our previous experiments, that high-dose EPO treatment increases capillary-to-myocyte ratio, which is indicative of neovascularization. In addition, low-dose EPO, although to a lesser extent, raised the capillary-to-myocyte ratio by 28%. Both high- and low-dose EPO treatment increased the number of EPCs. This is line with findings of Bahlmann et al.(21), who found that darbepoetin stimulates bone marrow-derived EPCs at doses that do not increase the hematocrit. Low-dose of EPO thus differentially stimulates the bone marrow precursor cells (i.e. erythroid vs. endothelial). Moreover, the increased number of EPCs was significantly correlated with capillary-to-myocyte ratio, providing an interesting link between EPCs mobilization and increased vascular growth in the heart. Application of lower doses of EPO was also shown to confer vascular and tissue protection in the kidney (22). Low-dose darbepoetin treatment in a rat remnant kidney model improved the survival, ameliorated endothelial damage and preserved renal function, without increase in hematocrit levels. Another option to avoid the negative effects of chronic EPO therapy on

Chapter 5
80
hematocrit values, could be the use of recently discovered non-erythropoietic derivates of EPO, retaining the tissue protecting property, without undesired effect on erythropoiesis (23). The possibility to separate the erythropoietic and tissue-protective effect could be explained through interaction of EPO with different receptors in bone marrow and in “peripheral” tissues (24). However, the role of these receptors in EPCs stimulation is unknown, and thus the regenerative capacity of the novel EPO derivates may be limited by reduced mobilization of EPCs.In summary, EPO treatment preserves cardiac function in post-MI heart failure, even in doses not increasing hematocrit. This is associated with stimulation of EPCs mobilization and induced neovascularization. Although time-limited treatment with high-dose EPO may be beneficial and safe during acute ischemic injury, if prolonged therapy is required (heart failure), drug regimens using low-dose EPO may be more suitable to avoid the adverse effects of the treatment.
Acknowledgments
We thank Azuwerus van Buiten, Maaike Goris, Liza Wong and Richard van Veghel for expert technical assistance.
Hematocrit independent effects of erythropoietin
81
Reference List 1. Van der Meer P., Voors AA, Lipšic E, van Gilst WH, van Veldhuisen DJ. Erythropoietin in cardiovascular diseases.
Eur Heart J 2004;25:285-291.
2. Cai Z, Semenza GL. Phosphatidylinositol-3-kinase signaling is required for erythropoietin-mediated acute protection against myocardial ischemia/reperfusion injury. Circulation 2004;109:2050-2053.
3. Van der Meer P, Lipšic E, Henning RH, De Boer RA, Suurmeijer AJ, Van Veldhuisen DJ, Van Gilst WH. Erythropoietin improves left ventricular function and coronary flow in an experimental model of ischemia-reperfusion injury. Eur J Heart Fail 2004;6:853-859.
4. Parsa CJ, Matsumoto A, Kim J, Riel RU, Pascal LS, Walton GB, Thompson RB, Petrofski JA, Annex BH, Stamler JS, Koch WJ. A novel protective effect of erythropoietin in the infarcted heart. J Clin Invest 2003;112:999-1007.
5. Lipšic E, van der Meer P, Henning RH, Suurmeijer AJ, Boddeus KM, Van Veldhuisen DJ, Van Gilst WH, Schoemaker RG. Timing of erythropoietin treatment for cardioprotection in ischemia/reperfusion. J Cardiovasc Pharmacol 2004;44:473-479.
6. Heeschen C, Aicher A, Lehmann R, Fichtlscherer S, Vasa M, Urbich C, Mildner-Rihm C, Martin H, Zeiher AM, Dimmeler S. Erythropoietin is a potent physiologic stimulus for endothelial progenitor cell mobilization. Blood 2003;102:1340-1346.
7. Kawamoto A, Tkebuchava T, Yamaguchi J, Nishimura H, Yoon YS, Milliken C, Uchida S, Masuo O, Iwaguro H, Ma H, Hanley A, Silver M, Kearney M, Losordo DW, Isner JM, Asahara T. Intramyocardial transplantation of autologous endothelial progenitor cells for therapeutic neovascularization of myocardial ischemia. Circulation 2003;107:461-468.
8. Werner N, Kosiol S, Schiegl T, Ahlers P, Walenta K, Link A, Bohm M, Nickenig G. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med 2005;353:999-1007.
9. Van der Meer P, Lipšic E, Henning RH, Boddeus K, van der Velden J, Voors AA, Van Veldhuisen DJ, Van Gilst WH, Schoemaker RG. Erythropoietin induces neovascularization and improves cardiac function in rats with heart failure after myocardial infarction. J Am Coll Cardiol 2005;46:125-133.
10. Brines M, Grasso G, Fiordaliso F, Sfacteria A, Ghezzi P, Fratelli M, Latini R, Xie QW, Smart J, Su-Rick CJ, Pobre E, Diaz D, Gomez D, Hand C, Coleman T, Cerami A. Erythropoietin mediates tissue protection through an erythropoietin and common beta-subunit heteroreceptor. Proc Natl Acad Sci U S A 2004;101:14907-14912.
11. Van Kerckhoven R, van Veghel R, Saxena PR, Schoemaker RG. Pharmacological therapy can increase capillary density in post-infarction remodeled rat hearts. Cardiovasc Res 2004;61:620-629.
12. Teichholz LE, Kreulen T, Herman MV, Gorlin R. Problems in echocardiographic volume determinations: echocardiographic-angiographic correlations in the presence of absence of asynergy. Am J Cardiol 1976;37:7-11.
13. Westendorp B, Schoemaker RG, Buikema H, Boomsma F, van Veldhuisen DJ, van Gilst WH. Progressive left ventricular hypertrophy after withdrawal of long-term ACE inhibition following experimental myocardial infarction. Eur J Heart Fail 2005.
14. Calvillo L, Latini R, Kajstura J, Leri A, Anversa P, Ghezzi P, Salio M, Cerami A, Brines M. Recombinant human erythropoietin protects the myocardium from ischemia-reperfusion injury and promotes beneficial remodeling. Proc Natl Acad Sci U S A 2003;100:4802-4806.
Chapter 5
82
15. Lee MS, Makkar RR. Stem-cell transplantation in myocardial infarction: a status report. Ann Intern Med 2004;140:729-737.
16. Dimmeler S, Zeiher AM, Schneider MD. Unchain my heart: the scientific foundations of cardiac repair. J Clin Invest 2005;115:572-583.
17. Murry CE, Soonpaa MH, Reinecke H, Nakajima H, Nakajima HO, Rubart M, Pasumarthi KB, Virag JI, Bartelmez SH, Poppa V, Bradford G, Dowell JD, Williams DA, Field LJ. Haematopoietic stem cells do not transdifferentiate into cardiac myocytes in myocardial infarcts. Nature 2004;428:664-668.
18. Ribatti D, Presta M, Vacca A, Ria R, Giuliani R, Dell’Era P, Nico B, Roncali L, Dammacco F. Human erythropoietin induces a pro-angiogenic phenotype in cultured endothelial cells and stimulates neovascularization in vivo. Blood 1999;93:2627-2636.
19. Wang Y, Zhang ZG, Wang L, Zhang RL, Chopp M. Erythropoietin enhances neurogenesis and angiogenesis in the brain and improves functional recovery after embolic stroke in the adult rat. Stroke 2004;35:239.
20. Besarab A, Bolton WK, Browne JK, Egrie JC, Nissenson AR, Okamoto DM, Schwab SJ, Goodkin DA. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med 1998;339:584-590.
21. Bahlmann FH, De Groot K, Spandau JM, Landry AL, Hertel B, Duckert T, Boehm SM, Menne J, Haller H, Fliser D. Erythropoietin regulates endothelial progenitor cells. Blood 2004;103:921-926.
22. Bahlmann FH, Song R, Boehm SM, Mengel M, von Wasielewski R, Lindschau C, Kirsch T, de Groot K, Laudeley R, Niemczyk E, Guler F, Menne J, Haller H, Fliser D. Low-dose therapy with the long-acting erythropoietin analogue darbepoetin alpha persistently activates endothelial Akt and attenuates progressive organ failure. Circulation 2004;110:1006-1012.
23. Fiordaliso F, Chimenti S, Staszewsky L, Bai A, Carlo E, Cuccovillo I, Doni M, Mengozzi M, Tonelli R, Ghezzi P, Coleman T, Brines M, Cerami A, Latini R. A nonerythropoietic derivative of erythropoietin protects the myocardium from ischemia-reperfusion injury. Proc Natl Acad Sci U S A 2005;102:2046-2051.
24. Leist M, Ghezzi P, Grasso G, Bianchi R, Villa P, Fratelli M, Savino C, Bianchi M, Nielsen J, Gerwien J, Kallunki P, Larsen AK, Helboe L, Christensen S, Pedersen LO, Nielsen M, Torup L, Sager T, Sfacteria A, Erbayraktar S, Erbayraktar Z, Gokmen N, Yilmaz O, Cerami-Hand C, Xie QW, Coleman T, Cerami A, Brines M. Derivatives of erythropoietin that are tissue protective but not erythropoietic. Science 2004;305:239-242.


Chapter 6
A single bolus of a long-acting erythropoietin analogue darbepoetin alfa
in patients with acute myocardial infarction:
a randomized feasibility and safety study
Erik Lipšic, Peter van der Meer, Adriaan A. Voors, B. Daan Westenbrink, Ad F.M. van den Heuvel,
Hetty C. de Boer, Anton J. van Zonneveld, Regien G. Schoemaker, Wiek H. van Gilst,
Felix Zijlstra, Dirk J. van Veldhuisen
Cardiovascular Drugs and Therapy 2006; in press

Chapter 6
86
Abstract
Aims: Besides stimulating hematopoiesis, erythropoietin (EPO) protects against experimental ischemic injury in the heart. The present study evaluated the safety and tolerability of EPO treatment in non-anemic patients with acute myocardial infarction (MI).Methods and Results: In this single-center, investigator-initiated, prospective study, patients with a first acute MI were randomized to one bolus of 300 μg darbepoetin alfa or no additional medication before primary coronary intervention. Twenty-two patients (mean age 59±2 years) were included. In the darbepoetin group, serum EPO-levels increased to 130-270 times that of controls, within the first 24-hours. After darbepoetin administration, only small and non-significant changes in hematocrit levels were observed, while endothelial progeni-tor cells (EPCs, CD34+/CD45-) were increased at 72-hours (2.8 vs. 1.0 cells/μl in control group; p<0.01). No adverse events were recorded during the 30-day follow-up. After 4 months, left ventricular ejection fraction was similar in the two groups (52±3% in darbepo-etin vs. 48±5% in control group, p=NS). Conclusions: Intravenous single high-dose darbepoetin alfa in acute MI is both safe and well tolerated. Darbepoetin treatment after MI stimulates EPCs mobilization. The results of this first pilot study support a larger scale clinical trial to establish efficacy of EPO administration in patients after acute MI.
Introduction
Erythropoietin (EPO) is a glycoprotein produced primarily by the kidney in response to hypoxia and subsequently targets erythroid progenitor cells in bone marrow to increase the number of erythrocytes (1). Independent of its hematopoietic effect, EPO was recently shown to be protective against ischemic injury in various organs, including the heart. A functional EPO receptor was found in rat myocardium, expressed mainly on endothelial cells (2). These results were recently expanded by a finding of EPO receptor expression in human heart tissue. Both ventricular myocytes and endothelial cells in the adult human heart were positive for the EPO receptor (3). In several experimental studies, administration of EPO both during cardiac ischemia-reperfusion or after permanent coronary artery occlusion, led to infarct size reduction and improvement in left ventricular (LV) function (4,5). Clinically important, our group showed the extension of the EPO cardioprotective effect when applied after the onset of ischemia and even after the start of reperfusion (6). Protection against apoptosis was implicated as a possible mechanism of the observed EPO effects (5,7).In addition to its anti-apoptotic effects, EPO was shown to stimulate the mobilization of endothelial progenitor cells (EPCs) in bone marrow (8). Mobilization and activation of these progenitor cells was associated with neovascularization of ischemic myocardium, a process that may play a beneficial role in the later phase of post-myocardial infarction (MI) LV re-modeling (9).Epoetin alfa is the recombinant (rhEPO) form of the endogenous cytokine, with equal bio-logical activity (10). RhEPO has been used in clinical settings for more than a decade, initially for the management of anemia caused by end stage renal disease (11). The indication for EPO treatment has broadened in the last few years also to include other forms of anemia
Erythropoietin in acute myocardial infarction
87
where EPO deficiency is not causative (myelodysplastic syndromes, cancer patients treated with chemotherapy, prophylactic treatment to reduce the need for transfusions before major surgery) (12). Considering an established safety profile of EPO in clinical practice, together with the results of experimental studies in cardiac ischemia, we designed a pilot clinical study with EPO treatment in acute MI patients. The primary objective of this single center, investigator-initiated, randomized study was to evaluate the safety and tolerability of long-acting EPO analogue darbepoetin alfa treatment in non-anemic patients with acute ST-elevation myocardial infarction (STEMI) treated with primary coronary angioplasty (PCI).
Methods
Patient populationMale patients, aged 18 to 76, with first acute STEMI and referred for PCI were considered for enrollment in the study. The inclusion and exclusion criteria are summarized in Table 1. Written informed consent was obtained from all patients before the study, and the institutional review board of the University Hospital of Groningen approved the study protocol. The study was consistent with the principles outlined in the Declaration of Helsinki. Randomization was performed by Trial Coordination Center of the Academic Hospital Groningen, based on a computer-generated randomization list. Patients were randomized to either darbepoetin alfa infusion or no infusion on a 1:1 basis. The planned number of patients to be enrolled in each group was 10.
Table 1. Inclusion and exclusion criteria
Inclusion criteriaMale between 18-76Acute myocardial infarction diagnosed by:
- chestpain suggestive for acute myocardial infarction- symptom onset < 6 hours- ECG with ST-T elevation > 1 mV in 2 or more leads
Indication for primary angioplastyKillip class I
Exclusion criteriaHemoglobin levels > 16.0 g/dLAcute myocardial infarction pre-treated with thrombolysisPrevious myocardial infarctionSystolic bloodpressure > 150 mmHgDiastolic bloodpressure > 95 mmHgSerum creatinine > 140 μmol/lPrevious treatment with rh-EPOBlood transfusion < 12 weeks prior to randomizationIndication for blood transfusionPolycythemia veraConcomitant inflammatory or malignant diseaseRecent trauma or major surgeryPrevious thrombo-embolic complication
Chapter 6
88
Study designAll patients with a first STEMI and indication for PCI were screened for participation in the study. Before inclusion, medical history, physical examination and ECG were obtained. Intravenous injection of long-acting EPO analogue darbepoetin alfa (300 μg, Aranesp, Amgen Inc., Thousand Oaks, CA, USA) was administered directly before PCI. In the control arm of the study no additional medication was administered. The dose of darbepoetin was chosen on the basis of the safety and efficacy study of EPO in acute stroke (13). In this study, 100.000 IU of short-acting recombinant human EPO was used, with an elimination half-life of 12 hours. To achieve similar plasma EPO levels with a long-acting EPO analogue darbepoetin alfa (elimination half-life of 21 hours), we chose a 40% lower dose: 300 μg (≈ 60.000 IU). The patients were otherwise treated according to the guidelines of the European Society of Cardiology for the treatment of STEMI (14). After PCI, all patients were monitored on the coronary care unit of our institution for at least 24-hours, with ECG monitoring and frequent controls of blood pressure. Following the discharge from the hospital, patients underwent clinical and laboratory controls at day 10 and 30 after the MI, at the out-patient clinic of our department.
Safety parametersPatients were closely monitored for adverse events. Besides frequent hemodynamic monitoring, each patient had complete blood cell count, blood urea nitrogen, creatinemia, electrolytes, glucose and liver enzymes evaluated at baseline (before PCI). The complete blood cell count was further closely followed and determined at time points: 24-hours, 72-hours, 10- and 30-days after PCI.
Clinical parameters Cumulative ST-elevation was calculated as a sum of ST-elevations in 12 ECG leads, before PCI. A standard CK and CK-MB monitoring was completed in all patients. Serum EPO levels were measured at baseline, after 4, 24 and 72-hours and 10 and 30-days after PCI, using IMMULITE EPO assay (DPC, Los Angeles, California), as described before (15,16). Quantification of circulating blood CD34+/CD45- cells was performed 72-hours after MI, with double labeling, with FITC-anti-CD45 and phycoerythrin-anti-CD34 monoclonal antibodies (Becton Dickinson, NJ, USA) on FACSCalibur (Becton Dickinson, NJ, USA) according to standardized procedures (17,18). Four months after the admission for MI, LV function was determined by radionuclide ventriculography, using standard method. Scans were assessed by a physician blinded for treatment allocation.
Statistical analysisData are given as mean ± SEM, or as median ± IQR (range from the 25th to the 75th percentile) if adequate, and as frequencies for categorical variables. For the continuous variables, differences between the groups were tested using one-way analysis of variance if normally distributed, and by Mann-Whitney ranksum test if skewed distributed. For the categorical variables, the two groups were compared using a chi-square test. Correlation analysis was performed with Spearman’s correlation test. We used a general linear model with repeated measures to compare the levels of serum EPO within the control group during the follow-up. All reported probability values were 2-tailed, and a p-value <0.05 was considered statistically significant. For all statistical analysis SPSS version 11.0 was used.
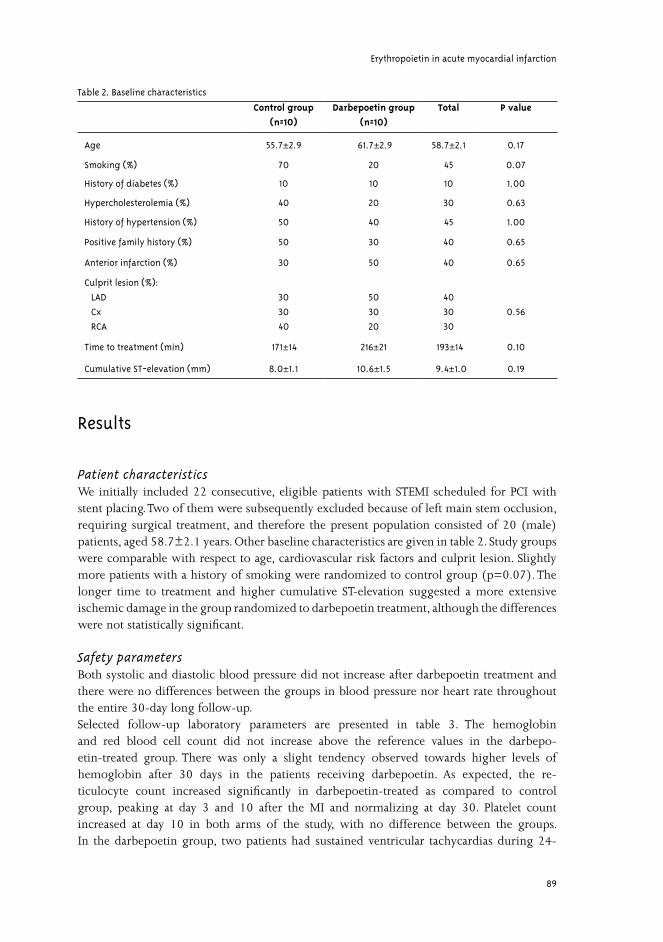
Erythropoietin in acute myocardial infarction
89
Results
Patient characteristicsWe initially included 22 consecutive, eligible patients with STEMI scheduled for PCI with stent placing. Two of them were subsequently excluded because of left main stem occlusion, requiring surgical treatment, and therefore the present population consisted of 20 (male) patients, aged 58.7±2.1 years. Other baseline characteristics are given in table 2. Study groups were comparable with respect to age, cardiovascular risk factors and culprit lesion. Slightly more patients with a history of smoking were randomized to control group (p=0.07). The longer time to treatment and higher cumulative ST-elevation suggested a more extensive ischemic damage in the group randomized to darbepoetin treatment, although the differences were not statistically significant.
Safety parametersBoth systolic and diastolic blood pressure did not increase after darbepoetin treatment and there were no differences between the groups in blood pressure nor heart rate throughout the entire 30-day long follow-up.Selected follow-up laboratory parameters are presented in table 3. The hemoglobin and red blood cell count did not increase above the reference values in the darbepo-etin-treated group. There was only a slight tendency observed towards higher levels of hemoglobin after 30 days in the patients receiving darbepoetin. As expected, the re-ticulocyte count increased significantly in darbepoetin-treated as compared to control group, peaking at day 3 and 10 after the MI and normalizing at day 30. Platelet count increased at day 10 in both arms of the study, with no difference between the groups. In the darbepoetin group, two patients had sustained ventricular tachycardias during 24-
Table 2. Baseline characteristics
Control group(n=10)
Darbepoetin group(n=10)
Total P value
Age 55.7±±2.9 61.7±±2.9 58.7±±2.1 0.17
Smoking (%) 70 20 45 0.07
History of diabetes (%) 10 10 10 1.00
Hypercholesterolemia (%) 40 20 30 0.63
History of hypertension (%) 50 40 45 1.00
Positive family history (%) 50 30 40 0.65
Anterior infarction (%) 30 50 40 0.65
Culprit lesion (%):
LAD
Cx
RCA
30
30
40
50
30
20
40
30
30
0.56
Time to treatment (min) 171±±14 216±±21 193±±14 0.10
Cumulative ST-elevation (mm) 8.0±±1.1 10.6±±1.5 9.4±±1.0 0.19
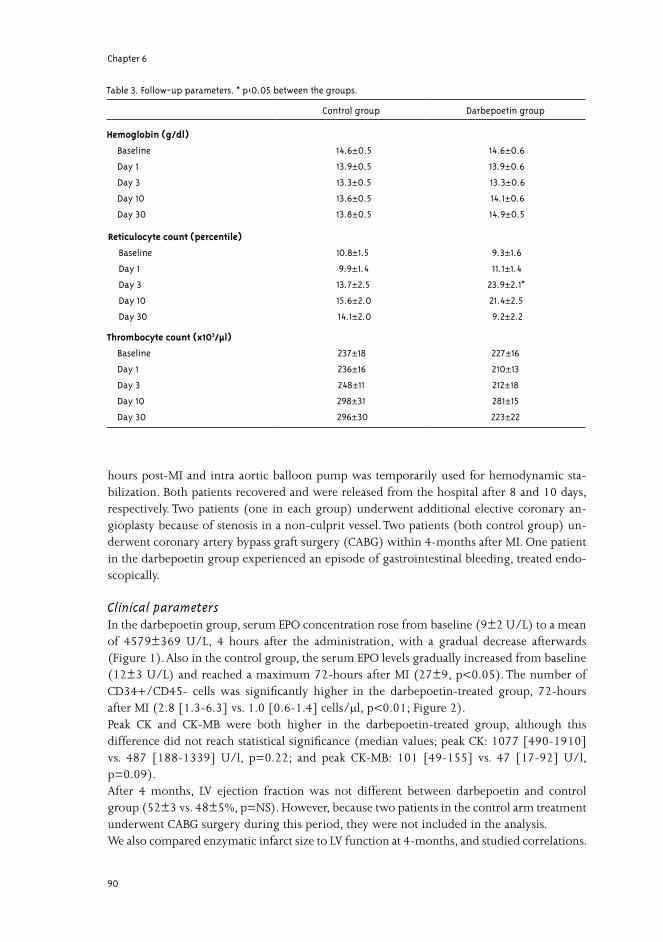
Chapter 6
90
hours post-MI and intra aortic balloon pump was temporarily used for hemodynamic sta-bilization. Both patients recovered and were released from the hospital after 8 and 10 days, respectively. Two patients (one in each group) underwent additional elective coronary an-gioplasty because of stenosis in a non-culprit vessel. Two patients (both control group) un-derwent coronary artery bypass graft surgery (CABG) within 4-months after MI. One patient in the darbepoetin group experienced an episode of gastrointestinal bleeding, treated endo-scopically.
Clinical parametersIn the darbepoetin group, serum EPO concentration rose from baseline (9±2 U/L) to a mean of 4579±369 U/L, 4 hours after the administration, with a gradual decrease afterwards (Figure 1). Also in the control group, the serum EPO levels gradually increased from baseline (12±3 U/L) and reached a maximum 72-hours after MI (27±9, p<0.05). The number of CD34+/CD45- cells was significantly higher in the darbepoetin-treated group, 72-hours after MI (2.8 [1.3-6.3] vs. 1.0 [0.6-1.4] cells/μl, p<0.01; Figure 2).Peak CK and CK-MB were both higher in the darbepoetin-treated group, although this difference did not reach statistical significance (median values; peak CK: 1077 [490-1910] vs. 487 [188-1339] U/l, p=0.22; and peak CK-MB: 101 [49-155] vs. 47 [17-92] U/l, p=0.09).After 4 months, LV ejection fraction was not different between darbepoetin and control group (52±3 vs. 48±5%, p=NS). However, because two patients in the control arm treatment underwent CABG surgery during this period, they were not included in the analysis.We also compared enzymatic infarct size to LV function at 4-months, and studied correlations.
Table 3. Follow-up parameters. * p<0.05 between the groups.
Control group Darbepoetin group
Hemoglobin (g/dl)
Baseline
Day 1
Day 3
Day 10
Day 30
14.6±±0.5
13.9±±0.5
13.3±±0.5
13.6±±0.5
13.8±±0.5
14.6±±0.6
13.9± ±0.6
13.3±±0.6
14.1±±0.6
14.9±±0.5
Reticulocyte count (percentile)
Baseline
Day 1
Day 3
Day 10
Day 30
10.8±±1.5
9.9±±1.4
13.7±±2.5
15.6±±2.0
14.1±2.0
9.3±±1.6
11.1±±1.4
23.9±±2.1*
21.4±±2.5
9.2±±2.2
Thrombocyte count (x103/μl)
Baseline
Day 1
Day 3
Day 10
Day 30
237±±18
236±±16
248±±11
298±±31
296±±30
227±±16
210±±13
212±±18
281±±15
223±±22
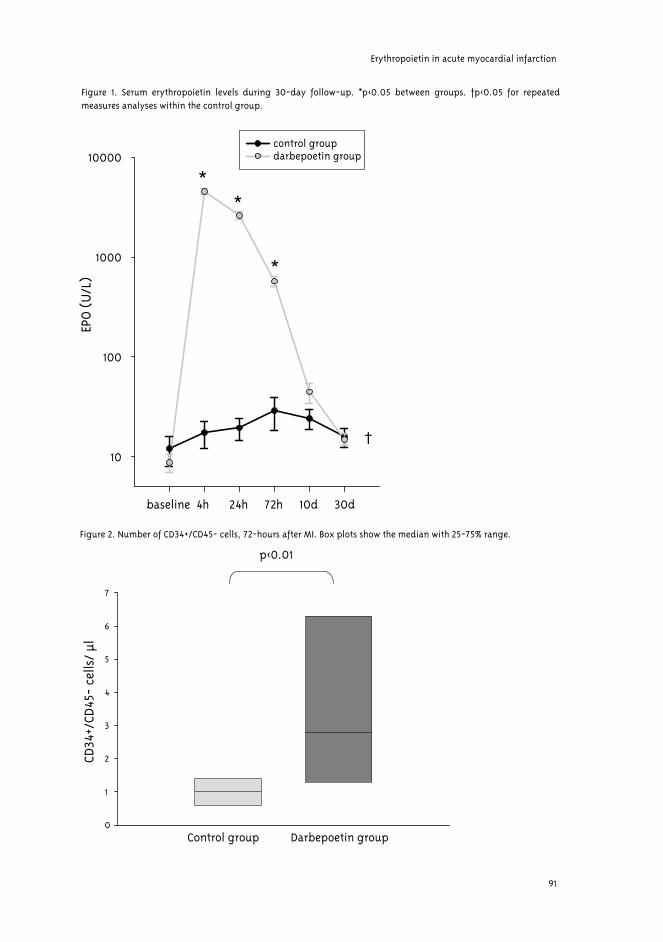
Erythropoietin in acute myocardial infarction
91
baseline 4h 24h 72h 10d 30d
EPO
(U
/L)
10
100
1000
10000control groupdarbepoetin group
**
*
†
Figure 1. Serum erythropoietin levels during 30-day follow-up. *p<0.05 between groups. †p<0.05 for repeated measures analyses within the control group.
CD34
+/CD
45-
cells
/µl
0
1
2
3
4
5
6
7
p<0.01
Control group Darbepoetin group
Figure 2. Number of CD34+/CD45- cells, 72-hours after MI. Box plots show the median with 25-75% range.
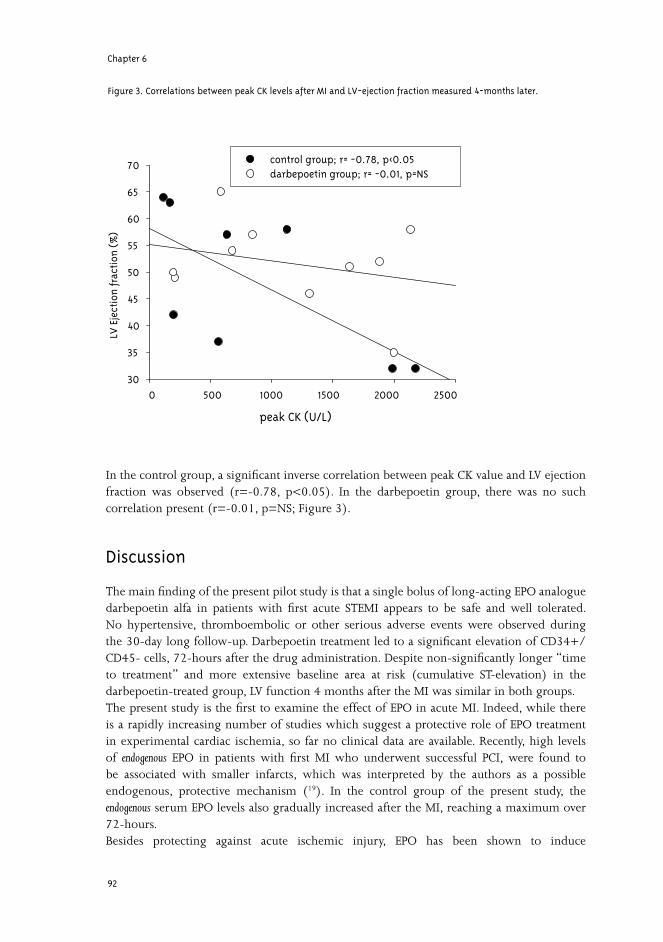
Chapter 6
92
In the control group, a significant inverse correlation between peak CK value and LV ejection fraction was observed (r=-0.78, p<0.05). In the darbepoetin group, there was no such correlation present (r=-0.01, p=NS; Figure 3).
Discussion
The main finding of the present pilot study is that a single bolus of long-acting EPO analogue darbepoetin alfa in patients with first acute STEMI appears to be safe and well tolerated. No hypertensive, thromboembolic or other serious adverse events were observed during the 30-day long follow-up. Darbepoetin treatment led to a significant elevation of CD34+/CD45- cells, 72-hours after the drug administration. Despite non-significantly longer “time to treatment” and more extensive baseline area at risk (cumulative ST-elevation) in the darbepoetin-treated group, LV function 4 months after the MI was similar in both groups.The present study is the first to examine the effect of EPO in acute MI. Indeed, while there is a rapidly increasing number of studies which suggest a protective role of EPO treatment in experimental cardiac ischemia, so far no clinical data are available. Recently, high levels of endogenous EPO in patients with first MI who underwent successful PCI, were found to be associated with smaller infarcts, which was interpreted by the authors as a possible endogenous, protective mechanism (19). In the control group of the present study, the endogenous serum EPO levels also gradually increased after the MI, reaching a maximum over 72-hours.Besides protecting against acute ischemic injury, EPO has been shown to induce
peak CK (U/L)
0 500 1000 1500 2000 2500
LVEj
ecti
onfr
acti
on(%
)
30
35
40
45
50
55
60
65
70 control group; r= -0.78, p<0.05darbepoetin group; r= -0.01, p=NS
Figure 3. Correlations between peak CK levels after MI and LV-ejection fraction measured 4-months later.

Erythropoietin in acute myocardial infarction
93
neovascularization over a longer time period (20). We have evaluated this issue in a rat model of post-MI heart failure (21). EPO treatment improved cardiac function, which was associated with increased capillary density and capillary-to-myocyte ratio, indicating formation of new blood vessels.The mechanism behind the effect of EPO on neovascularization remains largely unknown. Both stimulation of in situ endothelial cells proliferation or mobilization of EPCs derived from the bone marrow may play a role. Recently, increased levels of circulating EPCs were associated with reduced risk of death from cardiovascular causes in patients with confirmed coronary artery disease (22). EPO was shown to stimulate the mobilization and functional activity of EPCs (23). In the BOOST trial, intracoronary infusion of autologous CD34+ bone marrow cells after myocardial infarction improved the global LV ejection fraction 6 months after cell transfer (24). Administration of darbepoetin in the present pilot study led to almost a 3-fold increase in the number of circulating CD34+/CD45- cells, measured 72-hours after MI. We observed non-significantly higher peak CK and CK-MB levels in patients randomized for darbepoetin treatment. The most probable explanation for this finding is the longer “time to treatment” in the darbepoetin-treated group, as shown in the study by Liem et al. (25), in which comparable time delay (ca. 40 minutes) led to a significantly larger enzymatic infarct size and lower LV ejection fraction at 6 months. However, despite higher peak CK in patients treated with darbepoetin, the LV ejection fraction 4 months after the MI was similar in both groups. In numerous studies, enzymatic infarct size significantly correlates with LV function assessed at various time points after the MI(26 -28). Because a linear relationship exists between peak CK levels after acute MI and LV ejection fraction during the follow-up (26), we calculated the correlations in both groups of patients. While we observed a strong inverse correlation between peak CK value and LV ejection fraction in the control group, with comparable linear regression equations as previously described (28), no such correlation was detected in darbepoetin group. This may suggest a positive effect of darbepoetin treatment on longer-term infarct healing and/or cardiac remodeling. While the present study was conducted in patients with normal hemoglobin levels, recent studies showed that cardiovascular mortality in patients with acute coronary syndromes increases as hemoglobin levels become lower (29,30). Specific therapeutic strategies, including EPO treatment, in such anemic patients with MI should also be further considered.To date the only clinical study evaluating the non-hematopoietic effects of EPO was performed in stroke patients (13). In this first clinical, randomized, double-blind trial, EPO was given to patients with ischemic stroke presenting within 8 hours after the onset of symptoms. In spite of the relatively small number of patients in this study (n=40), EPO administration in high-doses (entire dose 100.000 IU/ given in three days) proved to be both safe and beneficial. Patients randomized to the EPO group showed significant improvement in clinical outcome parameters and a trend toward smaller infarct sizes, assessed by MRI. Furthermore, the serum levels of brain infarct damage marker (S100β) were significantly attenuated in EPO-treated group. Currently, a larger, multicenter “EPO stroke study” is being carried out in Germany (31). The dose of darbepoetin used in our study was based on the results of experimental studies, as well as on the basis of the above-mentioned EPO study in acute stroke (13). However, be-cause of a longer elimination half-life of darbepoetin alfa we chose a single high-dose darbe-poetin infusion instead of multiple EPO administrations used in stroke patients. Importantly,

Chapter 6
94
the measured serum EPO levels (4000-6000 U/L) were similar in both studies.In cardiology, EPO has been used to correct anemia in patients with chronic heart failure (CHF). In a number of small studies, normalization of hemoglobin levels in these patients was associated with improved LV ejection fraction (32) and enhanced exercise capacity (33). While this amelioration could be partly attributed to hemoglobin elevation and thus in-creased oxygen-binding capacity of blood, the non-hematopoietic effects of EPO must also be considered. Although treatment with EPO is generally well tolerated and safe, it may be associated with adverse effects (34). Rapid increases in hematocrit may cause hypertension (12), which de-velops in 20-30% of renal patients treated with EPO (35). Postulated mechanisms for EPO-induced hypertension include increased viscosity or vasoconstrictive responses due to the correction of anemia (34). Furthermore, EPO could also have direct vasopressor effect at the level of small resistance vessels (36). In our study, both systolic and diastolic blood pressure was lower during the whole follow-up in the group of patients treated with darbepoetin, as compared to controls. An other potential side effect is the increase in the number of thrombotic events (37), and EPO was also shown to increase the platelet count by 10-20% (38). However, most, if not all, of the above-mentioned complications are associated with an increase in hematocrit levels, which occurs mainly during chronic EPO therapy. With respect to the present study, administration of a single dose darbepoetin will generally not lead to a significant increase in hematocrit, but merely support the restoration of hematocrit levels after MI. In addition, we did not observe any thrombotic complications or elevation of plate-let count in the group treated with darbepoetin. Thus, by avoiding adverse effects of chronic therapy, EPO administration remains attractive in a setting of acute MI.In conclusion, high-dose darbepoetin treatment in acute MI is both safe and well tolerated. Darbepoetin treatment after MI stimulates EPCs mobilization. A larger scale clinical trial is warranted to assess the possible beneficial effect of EPO treatment in patients presenting with acute cardiac ischemia.
Acknowledgments
Dr. Lipšic is being supported by GUIDE, Dr. van der Meer is being supported by Zon-MW. Dr. van Veldhuisen is an Established Investigator of the Netherlands Heart Foundation (grant D97-017). Dr. de Boer is supported in part by Netherlands Heart Foundation (grant NHS 2002B157). Although previous experimental studies were supported by an unrestricted educational grant from Amgen Inc. (Thousand Oaks, CA, USA), no industrial funding was provided for the present study.
Erythropoietin in acute myocardial infarction
95
Reference List 1. Jelkmann W, Hellwig-Burgel T. Biology of erythropoietin. Adv Exp Med Biol 2001;502:169-187.
2. Van der Meer P, Lipšic E, Henning RH, De Boer RA, Suurmeijer AJ, Van Veldhuisen DJ, Van Gilst WH. Erythropoietin improves left ventricular function and coronary flow in an experimental model of ischemia-reperfusion injury. Eur J Heart Fail 2004;6:853-859.
3. Depping R, Kawakami K, Ocker H, Wagner JM, Heringlake M, Noetzold A, Sievers HH, Wagner KF. Expression of the erythropoietin receptor in human heart. J Thorac Cardiovasc Surg 2005;130:877-2.
4. Moon C, Krawczyk M, Ahn D, Ahmet I, Paik D, Lakatta EG, Talan MI. Erythropoietin reduces myocardial infarction and left ventricular functional decline after coronary artery ligation in rats. Proc Natl Acad Sci U S A 2003;100:11612-11617.
5. Parsa CJ, Matsumoto A, Kim J, Riel RU, Pascal LS, Walton GB, Thompson RB, Petrofski JA, Annex BH, Stamler JS, Koch WJ. A novel protective effect of erythropoietin in the infarcted heart. J Clin Invest 2003;112:999-1007.
6. Lipšic E, van der Meer P, Henning RH, Suurmeijer AJ, Boddeus KM, Van Veldhuisen DJ, Van Gilst WH, Schoemaker RG. Timing of erythropoietin treatment for cardioprotection in ischemia/reperfusion. J Cardiovasc Pharmacol 2004;44:473-479.
7. Tramontano AF, Muniyappa R, Black AD, Blendea MC, Cohen I, Deng L, Sowers JR, Cutaia MV, El Sherif N. Erythropoietin protects cardiac myocytes from hypoxia-induced apoptosis through an Akt-dependent pathway. Biochem Biophys Res Commun 2003;308:990-994.
8. Heeschen C, Aicher A, Lehmann R, Fichtlscherer S, Vasa M, Urbich C, Mildner-Rihm C, Martin H, Zeiher AM, Dimmeler S. Erythropoietin is a potent physiologic stimulus for endothelial progenitor cell mobilization. Blood 2003;102:1340-1346.
9. Dzau VJ, Gnecchi M, Pachori AS, Morello F, Melo LG. Therapeutic potential of endothelial progenitor cells in cardiovascular diseases. Hypertension 2005;46:7-18.
10. Egrie JC. Characterization and biological effects of recombinant human erythropoietin. Immunobiology 1986;172:213-224.
11. Winearls CG. Effect of human erythropoietin derived from recombinant DNA on the anaemia of patients maintained by chronic haemodialysis. The lancet 1986;2:1175-1178.
12. Henry DH, Bowers P, Romano MT, Provenzano R. Epoetin alfa. Clinical evolution of a pleiotropic cytokine. Arch Intern Med 2004;164:262-276.
13. Ehrenreich H, Hasselblatt M, Dembowski C, Cepek L, Lewczuk P, Stiefel M, Rustenbeck HH, Breiter N, Jacob S, Knerlich F, Bohn M, Poser W, Ruther E, Kochen M, Gefeller O, Gleiter C, Wessel TC, De Ryck M, Itri L, Prange H, Cerami A, Brines M, Siren AL. Erythropoietin therapy for acute stroke is both safe and beneficial. Mol Med 2002;8:495-505.
14. Van de Werf F, Ardissino D, Betriu A, Cokkinos DV, Falk E, Fox KA, Julian D, Lengyel M, Neumann FJ, Ruzyllo W, Thygesen C, Underwood SR, Vahanian A, Verheugt FW, Wijns W. Management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J 2003;24:28-66.
15. Benson EW, Hardy R, Chaffin C, Robinson CA, Konrad RJ. New automated chemiluminescent assay for erythropoietin. J Clin Lab Anal 2000;14:271-273.
Chapter 6
96
16. Van der Meer P, Voors AA, Lipšic E, Smilde TD, Van Gilst WH, Van Veldhuisen DJ. Prognostic value of plasma erythropoietin on mortality in patients with chronic heart failure. J Am Coll Cardiol 2004;44:63-67.
17. Barnett D, Granger V, Kraan J, Whitby L, Reilly JT, Papa S, Gratama JW. Reduction of intra- and interlaboratory variation in CD34+ stem cell enumeration using stable test material, standard protocols and targeted training. DK34 Task Force of the European Working Group of Clinical Cell Analysis (EWGCCA). Br J Haematol 2000;108:784-792.
18. Rabelink TJ, de Boer HC, de Koning EJ, van Zonneveld AJ. Endothelial progenitor cells: more than an inflammatory response? Arterioscler Thromb Vasc Biol 2004;24:834-838.
19. Namiuchi S, Kagaya Y, Ohta J, Shiba N, Sugi M, Oikawa M, Kunii H, Yamao H, Komatsu N, Yui M, Tada H, Sakuma M, Watanabe J, Ichihara T, Shirato K. High serum erythropoietin level is associated with smaller infarct size in patients with acute myocardial infarction who undergo successful primary percutaneous coronary intervention. J Am Coll Cardiol 2005;45:1406-1412.
20. Wang L, Zhang Z, Wang Y, Zhang R, Chopp M. Treatment of stroke with erythropoietin enhances neurogenesis and angiogenesis and improves neurological function in rats. Stroke 2004;35:1732-1737.
21. Van der Meer P, Lipšic E, Henning RH, Boddeus K, van der Velden J, Voors AA, Van Veldhuisen DJ, Van Gilst WH, Schoemaker RG. Erythropoietin induces neovascularization and improves cardiac function in rats with heart failure after myocardial infarction. J Am Coll Cardiol 2005;46:125-133.
22. Werner N, Kosiol S, Schiegl T, Ahlers P, Walenta K, Link A, Bohm M, Nickenig G. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med 2005;353:999-1007.
23. Bahlmann FH, De Groot K, Spandau JM, Landry AL, Hertel B, Duckert T, Boehm SM, Menne J, Haller H, Fliser D. Erythropoietin regulates endothelial progenitor cells. Blood 2004;103:921-926.
24. Wollert KC, Meyer GP, Lotz J, Ringes-Lichtenberg S, Lippolt P, Breidenbach C, Fichtner S, Korte T, Hornig B, Messinger D, Arseniev L, Hertenstein B, Ganser A, Drexler H. Intracoronary autologous bone-marrow cell transfer after myocardial infarction: the BOOST randomised controlled clinical trial. Lancet 2004;364:141-148.
25. Liem AL, ‘t Hof AW, Hoorntje JC, de Boer MJ, Suryapranata H, Zijlstra F. Influence of treatment delay on infarct size and clinical outcome in patients with acute myocardial infarction treated with primary angioplasty. J Am Coll Cardiol 1998;32:629-633.
26. Freimark D, Matetzky S, Hod H, Chouragui P, Kaplinsky E, Rabinowitz B. High early peak creatine kinase after thrombolysis in patients with acute anterior infarction predicts poor left ventricular function. Cardiology 1995;86:411-416.
27. Panteghini M, Cuccia C, Bonetti G, Giubbini R, Pagani F, Bonini E. Single-point cardiac troponin T at coronary care unit discharge after myocardial infarction correlates with infarct size and ejection fraction. Clin Chem 2002;48:1432-1436.
28. Van der Laarse A, Kerkhof PL, Vermeer F, Serruys PW, Hermens WT, Verheugt FW, Bar FW, Krauss XH, van der Wall EE, Simoons ML. Relation between infarct size and left ventricular performance assessed in patients with first acute myocardial infarction randomized to intracoronary thrombolytic therapy or to conventional treatment. Am J Cardiol 1988;61:1-7.
29. Lipšic E, van der Horst IC, Voors AA, van der Meer P, Nijsten MW, van Gilst WH, van Veldhuisen DJ, Zijlstra F. Hemoglobin levels and 30-day mortality in patients after myocardial infarction. Int J Cardiol 2005;100:289-292.

Erythropoietin in acute myocardial infarction
97
30. Sabatine MS, Morrow DA, Giugliano RP, Burton PB, Murphy SA, McCabe CH, Gibson CM, Braunwald E. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation 2005;111:2042-2049.
31. Ehrenreich H, Timner W, Siren AL. A novel role for an established player: anemia drug erythropoietin for the treatment of cerebral hypoxia/ischemia. Transfus Apheresis Sci 2004;31:39-44.
32. Silverberg DS, Wexler D, Sheps D, Blum M, Keren G, Baruch R, Schwartz D, Yachnin T, Steinbruch S, Shapira I, Laniado S, Iaina A. The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study. J Am Coll Cardiol 2001;37:1775-1780.
33. Mancini DM, Katz SD, Lang CC, LaManca J, Hudaihed A, Androne AS. Effect of erythropoietin on exercise capacity in patients with moderate to severe chronic heart failure. Circulation 2003;107:294-299.
34. Smith KJ, Bleyer AJ, Little WC, Sane DC. The cardiovascular effects of erythropoietin. Cardiovasc Res 2003;59:538-548.
35. Maschio G. Erythropoietin and systemic hypertension. Nephrol Dial Transplant 1995;10 Suppl 2:74-79.
36. Heidenreich S, Rahn KH, Zidek W. Direct vasopressor effect of recombinant human erythropoietin on renal resistance vessels. Kidney Int 1991;39:259-265.
37. Besarab A, Bolton WK, Browne JK, Egrie JC, Nissenson AR, Okamoto DM, Schwab SJ, Goodkin DA. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med 1998;339:584-590.
38. Stohlawetz PJ, Dzirlo L, Hergovich N, Lackner E, Mensik C, Eichler HG, Kabrna E, Geissler K, Jilma B. Effects of erythropoietin on platelet reactivity and thrombopoiesis in humans. Blood 2000;95:2983-2989.

Chapter 7
Hemoglobin levels and 30-day mortality in patients
after myocardial infarction
Erik Lipšic, Iwan C.C. van der Horst, Adriaan A. Voors, Peter van der Meer,
Maarten W.N. Nijsten, Wiek H. van Gilst, Dirk J. van Veldhuisen, Felix Zijlstra
International Journal of Cardiology 2005;100(2):289-92

Chapter 7
100
Abstract
Background: Anemia is an independent risk factor for cardiovascular (CV) outcomes in patients with coronary artery disease and heart failure. However, the effect of hemoglobin levels on short-term CV mortality in patients with acute myocardial infarction (MI) remains unclear. Methods: In a retrospective study we analyzed 1841 consecutive patients admitted with the diagnosis of acute MI. The primary end-point of the study was 30-day mortality. Patients were categorized according to the hemoglobin level on admission (10 g/dl or less, or greater than 10 g/dl). Results: The overall 30-day mortality was 10.3%. The mortality was 21.6% in patients with hemoglobin levels on admission ≤10 g/dl and 9.3% in patients with hemoglobin levels >10 g/dl (p<0.001). Multivariate logistic regression analysis showed, that lower hemoglo-bin concentration is an independent predictor of 30-day mortality, when adjusted for other risk factors (HR 1.76, CI 1.08-2.85; p=0.02). Conclusions: Lower levels of hemoglobin are associated with higher short-term mortality in patients with acute MI. Specific therapeutic strategies in anemic patients with MI should be further considered.
Introduction
Anemia is common in patients admitted to the cardiac intensive care unit (1). Although critically-ill patients are able to tolerate low levels of hemoglobin (2), presence of cardiovascular (CV) disease significantly increases the risk of anemia (3). Two large observational studies in patients with CV disease showed that lower preoperative hemoglobin levels were associated with an impaired survival following general surgery (4) and coronary artery bypass surgery (5). In both studies patients with preoperative hemoglobin levels lower than 10 g/dl had a significantly greater risk of in-hospital mortality. Recently, two studies addressed the effect of anemia on longer-term survival in patients with established coronary artery disease (CAD). Reinecke et al. (6) showed that anemia is associated with reduced survival in patients with CAD after elective percutaneous coronary intervention. Al Falluji et al. (7) evaluated the effect of anemia on 1-year mortality in patients after myocardial infarction (MI) and concluded that anemia has no direct significant effect on survival. However, exact hemoglobin levels, as well as renal function of the patients were not analyzed in this study. Anemia is independently associated with increased risk of death during follow-up after MI in patients with renal insufficiency (8). In a large retrospective study, blood transfusion in elderly patients with myocardial infarction and hematocrit value below 30% was associated with reduced 30-day mortality (9). Anemia is also an independent predictor of poor outcome in patients with chronic heart failure (10;11).However, there are limited data on the short-term prognostic importance of anemia in patients who present with an acute MI. The aim of our study was to establish the relation between hemoglobin levels and 30-day mortality in patients with acute MI.
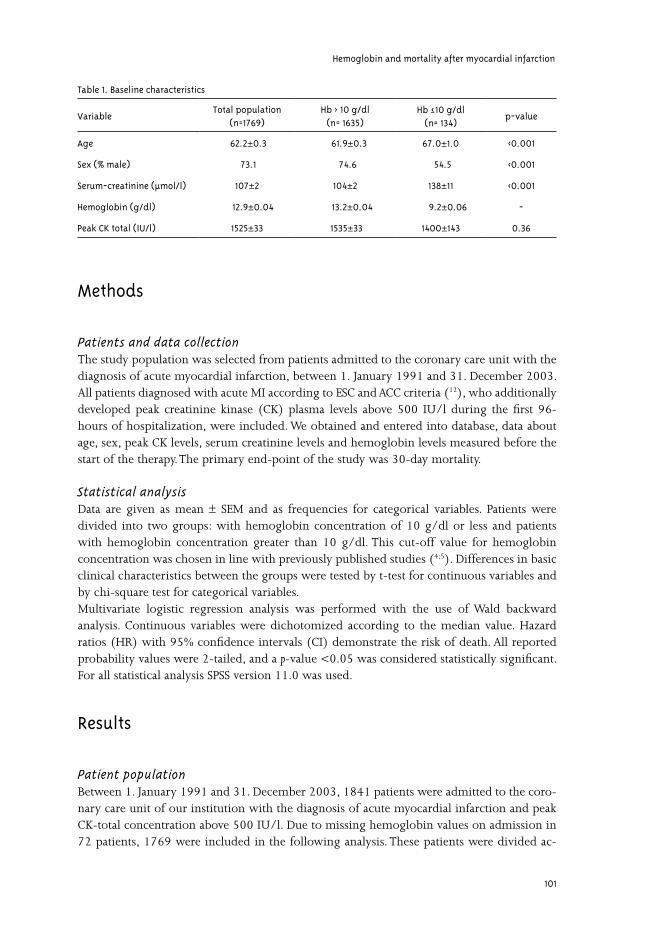
Hemoglobin and mortality after myocardial infarction
101
Methods
Patients and data collectionThe study population was selected from patients admitted to the coronary care unit with the diagnosis of acute myocardial infarction, between 1. January 1991 and 31. December 2003. All patients diagnosed with acute MI according to ESC and ACC criteria (12), who additionally developed peak creatinine kinase (CK) plasma levels above 500 IU/l during the first 96-hours of hospitalization, were included. We obtained and entered into database, data about age, sex, peak CK levels, serum creatinine levels and hemoglobin levels measured before the start of the therapy. The primary end-point of the study was 30-day mortality.
Statistical analysisData are given as mean ± SEM and as frequencies for categorical variables. Patients were divided into two groups: with hemoglobin concentration of 10 g/dl or less and patients with hemoglobin concentration greater than 10 g/dl. This cut-off value for hemoglobin concentration was chosen in line with previously published studies (4;5). Differences in basic clinical characteristics between the groups were tested by t-test for continuous variables and by chi-square test for categorical variables. Multivariate logistic regression analysis was performed with the use of Wald backward analysis. Continuous variables were dichotomized according to the median value. Hazard ratios (HR) with 95% confidence intervals (CI) demonstrate the risk of death. All reported probability values were 2-tailed, and a p-value <0.05 was considered statistically significant. For all statistical analysis SPSS version 11.0 was used.
Results
Patient populationBetween 1. January 1991 and 31. December 2003, 1841 patients were admitted to the coro-nary care unit of our institution with the diagnosis of acute myocardial infarction and peak CK-total concentration above 500 IU/l. Due to missing hemoglobin values on admission in 72 patients, 1769 were included in the following analysis. These patients were divided ac-
Table 1. Baseline characteristics
VariableTotal population
(n=1769)Hb > 10 g/dl
(n= 1635)Hb ≤ 10 g/dl
(n= 134)p-value
Age 62.2±±0.3 61.9±0.3 67.0±±1.0 <0.001
Sex (% male) 73.1 74.6 54.5 <0.001
Serum-creatinine (μmol/l) 107±±2 104±±2 138±±11 <0.001
Hemoglobin (g/dl) 12.9±±0.04 13.2±±0.04 9.2±±0.06 -
Peak CK total (IU/l) 1525±±33 1535±±33 1400±±143 0.36

Chapter 7
102
cording to the level of hemoglobin into 2 groups: with hemoglobin concentration of 10 g/dl or less (n=134) and patients with hemoglobin concentration greater than 10 g/dl (n=1635). Baseline characteristics of both groups are given in table 1. Significant differences were found between the groups regarding age, sex and serum creatinine concentration.
Predictors of mortalityThe overall 30-day mortality was 10.3%. The crude mortality rate was more than two times higher among patients with hemoglobin values of 10 g/dl or less (29 patients, 21.6%) than among those with higher hemoglobin concentration (153 patients, 9.3%; p<0.001). In a multivariate logistic regression analysis, low levels of hemoglobin remained an independent predictor of 30-day mortality, even after adjusted for gender, age and serum creatinine concentration (hazard ratio 1.76, 95% confidence interval 1.08-2.85; p=0.02; table 2). When the patients were divided in 4 subgroups with regard to hemoglobin concentration (<8 g/dl, 8-10 g/dl, 10-12 g/dl and >12 g/dl) a continuous trend towards lower mortality was present with increasing hemoglobin values (Fig.1).
Discussion
In our study, lower hemoglobin concentrations are associated with higher mortality in pa-tients with acute myocardial infarction. We found a statistically significant increase in 30-day mortality in patients presenting with hemoglobin concentrations lower than 10 g/dl. Since other covariates in our analysis (age, sex, renal function) were stronger predictors of sur-vival, hemoglobin levels to a certain degree reflect also other co-morbidities or disease states. Nevertheless, even after adjustment for these variables low hemoglobin levels remained sig-nificantly related to 30-day mortality.Our data support the study by Zindrou et al. (5) who showed higher in-hospital mortality in anemic patients after coronary bypass surgery. In contrast, Reinecke et al. (6) did not observe an effect of hemoglobin concentration on in-hospital mortality in patients after elective percutaneous coronary intervention. This could be explained by greater extent of ischemia and worse hemodynamic status in patients with acute MI/ or undergoing bypass surgery.There are several potential mechanisms by which anemia may worsen the prognosis of patients with acute MI. Although the resting human heart can withstand acute severe isovolemic anemia as low as 5.0 g/dl (13), CV disease significantly impairs the heart’s ability to tolerate low levels of hemoglobin (4).
Table 2. Multivariate predictors of 30-day mortality
HR CI P
Hb (≤ 10 g/dl) 1.76 1.08-2.85 0.02
Age (> 63.5) 4.63 3.02-7.10 <0.001
Sex (female) 2.00 1.41-2.84 <0.001
Serum creatinine level (>92 μmol/l) 3.34 2.27-4.93 <0.001

Hemoglobin and mortality after myocardial infarction
103
Anemia causes hypoxia-induced vasodilatation leading to increased sympathetic activity and cardiac output. This mechanism decreases coronary reserve (14), which is already limited in patients with CAD because of high extraction rate of oxygen in the cardiac circulation (1). Manifestation of myocardial ischemia may thus occur with only mild anemia (hematocrit 20-30%) (15). Elevated sympathetic activity was also repeatedly associated with worse outcome after acute MI (16). In the long-term, these alterations lead to gradual development of cardiac enlargement and LV hypertrophy (17), causing higher oxygen consumption and aggravating ischemia. Conversely, markedly elevated hemoglobin levels also have been associated with worse CV prognosis. High blood viscosity and increased thrombus formation (18) have been implicated as causative factors. Some studies have also suggested protective role of iron depletion and thus iron deficiency anemia in CAD development (19). Lower levels of redox-active iron may decrease the oxidative stress and thus attenuate endothelial dysfunction (20). Studies in the general population (21) and recently also in patients with CAD (6) suggested J/U shaped relationship between levels of hemoglobin and CV morbidity and mortality. Association of high hematocrit and CV disease may however reflect presence of chronic obstructive lung disease causing both polycythemia and poorer CV survival (22). We have not detected any U-shape relationship between the hemoglobin level and short-term survival, although our study may have been underpowered to detect it.Experimental data and recent studies suggest that cardiac patients are less tolerant to anemia (23). Consequently, hemoglobin level thresholds for the treatment of anemia in these patients should be higher, particularly in a setting of acute cardiac ischemia (4;9;24). In other words, hemoglobin levels that have been considered as not yet significantly lowered may in fact already be too low in patients with heart disease. In addition to blood transfusion, with its possible adverse reactions and volume overload, therapy with recombinant human erythropoietin should also be considered (25). Moreover, erythropoietin has been found to have also direct
35
30
25
20
15
10
5
0
12
122
385
1250
Hemoglobin concentration, g/dl
30-d
ay m
orta
lity,
%
<8.0 8.0-10.0 10.1-12.0 >12
Figure.1. Crude 30-day mortality (in %) in patients after acute MI. Both groups (Hb higher than 10 g/dl and lower than 10 g/dl) were subdivided into 2 subgroups. At the top of each column, the number of patients in the subgroup is noted.

Chapter 7
104
cardioprotective effects, not associated with hematopoiesis (26). Further studies are needed to assess the benefit of anemia treatment in patients with acute coronary events. There are some limitations to our analysis. First, although the effect of hemoglobin levels on 30-day mortality was corrected for the most important covariates, we were unable to control for CV risk factors outside the scope of the data abstraction. Second, because of retrospective data collection and limited amount of available data, no conclusions can be drawn on possible mechanisms relating anemia to short-term mortality.
Conclusion
The present study clearly shows a relation between low hemoglobin concentration and 30-day mortality in patients with acute MI. However, low hemoglobin levels are also an important marker of other concomitant diseases that affect the mortality after MI. In the future, possible treatment options for anemic patients presenting with acute MI should be considered.
Hemoglobin and mortality after myocardial infarction
105
Reference List1. Freudenberger RS, Carson JL. Is there an optimal hemoglobin value in the cardiac intensive care unit? Curr Opin
Crit Care. 2003;9:356-361.
2. Alvarez G, Hebert PC, Szick S. Debate: transfusing to normal haemoglobin levels will not improve outcome. Crit Care. 2001;5:56-63.
3. Hebert PC, Wells G, Tweeddale M et al. Does transfusion practice affect mortality in critically ill patients? Transfusion Requirements in Critical Care (TRICC) Investigators and the Canadian Critical Care Trials Group. Am J Respir Crit Care Med. 1997;155:1618-1623.
4. Carson JL, Duff A, Poses RM et al. Effect of anaemia and cardiovascular disease on surgical mortality and morbidity. Lancet. 1996;348:1055-1060.
5. Zindrou D, Taylor KM, Bagger JP. Preoperative haemoglobin concentration and mortality rate after coronary artery bypass surgery. Lancet. 2002;359:1747-1748.
6. Reinecke H, Trey T, Wellmann J et al. Haemoglobin-related mortality in patients undergoing percutaneous coronary interventions. Eur Heart J. 2003;24:2142-2150.
7. Al Falluji N, Lawrence-Nelson J, Kostis JB et al. Effect of anemia on 1-year mortality in patients with acute myocardial infarction. Am Heart J. 2002;144:636-641.
8. Langston RD, Presley R, Flanders WD et al. Renal insufficiency and anemia are independent risk factors for death among patients with acute myocardial infarction. Kidney Int. 2003;64:1398-1405.
9. Wu WC, Rathore SS, Wang Y et al. Blood transfusion in elderly patients with acute myocardial infarction. N Engl J Med. 2001;345:1230-1236.
10. Szachniewicz J, Petruk-Kowalczyk J, Majda J et al. Anaemia is an independent predictor of poor outcome in patients with chronic heart failure. Int J Cardiol. 2003;90:303-308.
11. Tanner H, Moschovitis G, Kuster GM et al. The prevalence of anemia in chronic heart failure. Int J Cardiol. 2002;86:115-121.
12. Alpert JS, Thygesen K, Antman E et al. Myocardial infarction redefined--a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36:959-969.
13. Weiskopf RB, Viele MK, Feiner J et al. Human cardiovascular and metabolic response to acute, severe isovolemic anemia. JAMA. 1998;279:217-221.
14. Levy PS, Kim SJ, Eckel PK et al. Limit to cardiac compensation during acute isovolemic hemodilution: influence of coronary stenosis. Am J Physiol. 1993;265:H340-H349.
15. Most AS, Ruocco NA, Jr., Gewirtz H. Effect of a reduction in blood viscosity on maximal myocardial oxygen delivery distal to a moderate coronary stenosis. Circulation. 1986;74:1085-1092.
16. Graham LN, Smith PA, Stoker JB et al. Time course of sympathetic neural hyperactivity after uncomplicated acute myocardial infarction. Circulation. 2002;106:793-797.
17. Metivier F, Marchais SJ, Guerin AP et al. Pathophysiology of anaemia: focus on the heart and blood vessels. Nephrol Dial Transplant. 2000;15 Suppl 3:14-18.
Chapter 7
106
18. Carson JL, Duff A, Berlin JA et al. Perioperative blood transfusion and postoperative mortality. JAMA. 1998;279:199-205.
19. Sullivan JL. Iron and the sex difference in heart disease risk. Lancet. 1981;1:1293-1294.
20. Cooper CE. Nitric oxide and iron proteins. Biochim Biophys Acta. 1999;1411:290-309.
21. Gagnon DR, Zhang TJ, Brand FN et al. Hematocrit and the risk of cardiovascular disease--the Framingham study: a 34-year follow-up. Am Heart J. 1994;127:674-682.
22. Brown DW, Giles WH, Croft JB. Hematocrit and the risk of coronary heart disease mortality. Am Heart J. 2001;142:657-663.
23. Kalra PR, Bolger AP, Francis DP et al. Effect of anemia on exercise tolerance in chronic heart failure in men. Am J Cardiol. 2003;91:888-891.
24. Hebert PC, Wells G, Blajchman MA et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med. 1999;340:409-417.
25. Corwin HL, Gettinger A, Pearl RG et al. Efficacy of recombinant human erythropoietin in critically ill patients: a randomized controlled trial. JAMA. 2002;288:2827-2835.
26. Van der Meer P, Voors AA, Lipšic E et al. Erythropoietin in cardiovascular diseases. Eur Heart J. 2004;25:285-291.


Chapter 8
Protective effects of erythropoietin in
cardiac ischemia: from bench to bedside
Erik Lipšic, Regien G. Schoemaker, Peter van der Meer, Adriaan A. Voors,
Dirk J. van Veldhuisen,Wiek H. van Gilst
Submitted

Chapter 8
110
Abstract
Erythropoietin (EPO) is a hypoxia-induced hormone produced in kidneys that stimulates hematopoiesis in the bone marrow by inhibiting the apoptosis of erythroid precursors. However, recent studies demonstrated also important non-hematopoietic effects of EPO. Administration of EPO confers neuroprotection against stroke and other neurological disorders. An active EPO receptor is found also in the cardiovascular system, including endothelial cells and cardiomyocytes. In animal studies, treatment with EPO during ischemia/ reperfusion in the heart has been shown to limit the infarct size and the extent of apoptosis. In the longer term, EPO may promote ischemia-induced neovascularization, either by stimulating endothelial cells in situ or by mobilizing endothelial progenitor cells from bone marrow. The effects of EPO in the ischemic heart support the concept of EPO as a pleiotropic, tissue-protective agent for other organs expressing the EPO receptor. We recently performed a first randomized clinical study showing safety and feasibility of EPO administration in patients with acute myocardial infarction. Future clinical studies are warranted to translate the beneficial effects of EPO from basic experiments to cardiac patients.
Erythropoietin
Erythropoietin (EPO) is a hematopoietic hormone produced primarily in kidneys in response to hypoxia (1). Hematopoietic effects of EPO in the bone marrow are mediated by binding to a specific transmembrane receptor (EPO-R) which is expressed primarily by erythroid progenitor cells (2). The signaling by the EPO-R is initiated when it is dimerized by binding EPO (3), leading to activation of numerous intracellular pathways (PI3K/Akt, MAPK, STAT-5) associated with cell survival (4). Rather than directly stimulating the proliferation, EPO inhibits the apoptosis of erythroid precursor cells (5). By reducing the apoptosis of erythroid cells in bone marrow, EPO upregulates the number of mature red blood cells in circulation. Although only present in plasma at picomolar concentrations, EPO regulates the production of approximately 2.3 million cells per second (6). Epoetin alfa is the recombinant (rhEPO) form of the endogenous cytokine, with equal bio-logical activity (7). RhEPO was originally used only in management of anemia caused by chronic kidney disease (8). The indication for EPO treatment has broadened in the last few years also to include other forms of anemia where EPO deficiency is not causative. It is now widely used in anemic patients with myelodysplastic syndromes (9), cancer patients treated with chemotherapy (10), and as prophylactic treatment to reduce the need for transfusions before major surgery (11). In addition to the effects related to hematopoiesis, numerous experimental studies have recently demonstrated important non-hematopoietic functions of EPO, such as protection against ischemic injury in various tissues. This effect was observed independently of hema-topoiesis stimulation, indicating EPO may play a role as a pleiotropic survival and growth factor (6). This review summarizes the newly established non-hematopoietic properties of EPO, focus-ing on protection against ischemic injury in the heart and its possible future implications for treatment of acute coronary syndromes and post-myocardial infarction (MI) heart failure.
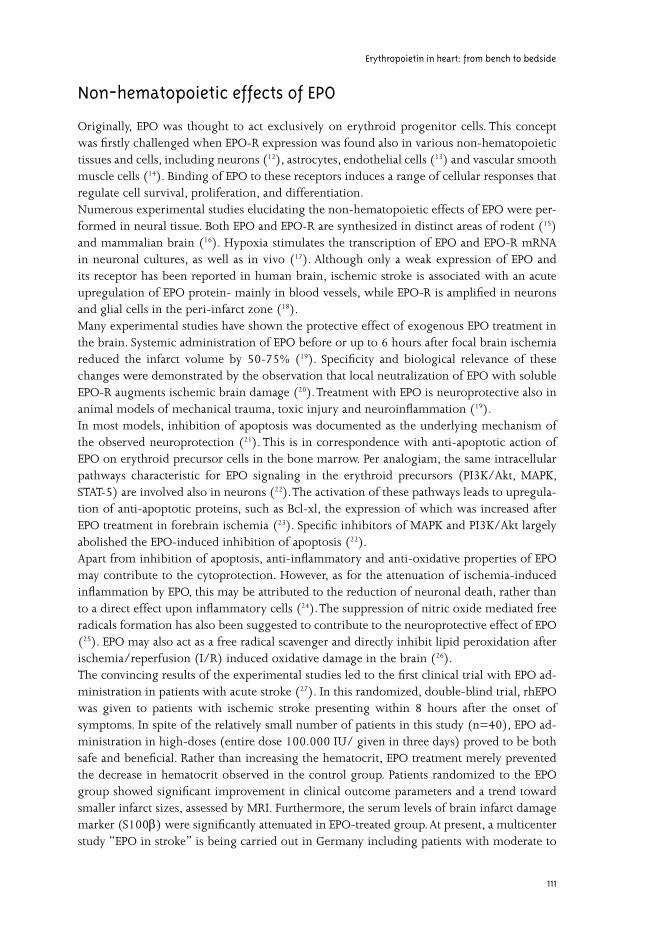
Erythropoietin in heart: from bench to bedside
111
Non-hematopoietic effects of EPO
Originally, EPO was thought to act exclusively on erythroid progenitor cells. This concept was firstly challenged when EPO-R expression was found also in various non-hematopoietic tissues and cells, including neurons (12), astrocytes, endothelial cells (13) and vascular smooth muscle cells (14). Binding of EPO to these receptors induces a range of cellular responses that regulate cell survival, proliferation, and differentiation. Numerous experimental studies elucidating the non-hematopoietic effects of EPO were per-formed in neural tissue. Both EPO and EPO-R are synthesized in distinct areas of rodent (15) and mammalian brain (16). Hypoxia stimulates the transcription of EPO and EPO-R mRNA in neuronal cultures, as well as in vivo (17). Although only a weak expression of EPO and its receptor has been reported in human brain, ischemic stroke is associated with an acute upregulation of EPO protein- mainly in blood vessels, while EPO-R is amplified in neurons and glial cells in the peri-infarct zone (18). Many experimental studies have shown the protective effect of exogenous EPO treatment in the brain. Systemic administration of EPO before or up to 6 hours after focal brain ischemia reduced the infarct volume by 50-75% (19). Specificity and biological relevance of these changes were demonstrated by the observation that local neutralization of EPO with soluble EPO-R augments ischemic brain damage (20). Treatment with EPO is neuroprotective also in animal models of mechanical trauma, toxic injury and neuroinflammation (19).In most models, inhibition of apoptosis was documented as the underlying mechanism of the observed neuroprotection (21). This is in correspondence with anti-apoptotic action of EPO on erythroid precursor cells in the bone marrow. Per analogiam, the same intracellular pathways characteristic for EPO signaling in the erythroid precursors (PI3K/Akt, MAPK, STAT-5) are involved also in neurons (22). The activation of these pathways leads to upregula-tion of anti-apoptotic proteins, such as Bcl-xl, the expression of which was increased after EPO treatment in forebrain ischemia (23). Specific inhibitors of MAPK and PI3K/Akt largely abolished the EPO-induced inhibition of apoptosis (22). Apart from inhibition of apoptosis, anti-inflammatory and anti-oxidative properties of EPO may contribute to the cytoprotection. However, as for the attenuation of ischemia-induced inflammation by EPO, this may be attributed to the reduction of neuronal death, rather than to a direct effect upon inflammatory cells (24). The suppression of nitric oxide mediated free radicals formation has also been suggested to contribute to the neuroprotective effect of EPO (25). EPO may also act as a free radical scavenger and directly inhibit lipid peroxidation after ischemia/reperfusion (I/R) induced oxidative damage in the brain (26).The convincing results of the experimental studies led to the first clinical trial with EPO ad-ministration in patients with acute stroke (27). In this randomized, double-blind trial, rhEPO was given to patients with ischemic stroke presenting within 8 hours after the onset of symptoms. In spite of the relatively small number of patients in this study (n=40), EPO ad-ministration in high-doses (entire dose 100.000 IU/ given in three days) proved to be both safe and beneficial. Rather than increasing the hematocrit, EPO treatment merely prevented the decrease in hematocrit observed in the control group. Patients randomized to the EPO group showed significant improvement in clinical outcome parameters and a trend toward smaller infarct sizes, assessed by MRI. Furthermore, the serum levels of brain infarct damage marker (S100β) were significantly attenuated in EPO-treated group. At present, a multicenter study “EPO in stroke” is being carried out in Germany including patients with moderate to

Chapter 8
112
severe infarcts and a 1-year follow-up (28).EPO’s protective properties were established also in other tissues. In the kidney, treatment with recombinant EPO significantly reduced the renal injury and dysfunction associated with I/R in rodents (29). This effect was related to the prevention of apoptosis by inhibiting the activation of caspase-3, a crucial step in the cascade of programmed cell death (30). Other reports documented benefit of EPO therapy in the setting of hypoxic retinal disease (31), gastrointestinal ischemia (32), as well as in the cardiovascular system (33-36).
EPO and EPO-R in cardiovascular system
The expression of EPO-R was found in a variety of cell lines originated from cardiovascular system. EPO-R is synthesized and present on the surface of human vascular endothelial cells(13). Short-term anoxia of bovine endothelial cells induces up to a two-fold increase in protein levels of EPO-R and exogenous EPO inhibits apoptosis of these cells when administered
casp
ase-
3ac
tivi
ty(%
ofco
ntro
l)
0
200
400
600
800
1000
1200
control24/6-EPO24/6+EPO, t=-2424/6+EPO, t=024/6+EPO, t=24
A B
C
control 60-min anoxia
*** * p<0.01
Figure 1. A, B) Expression of EPO receptor on bovine arterial endothelial cells (BAEC) during normoxia and after 60-min anoxia. C) BAEC were subjected to 24-hour anoxia, followed by 6-hour reoxygenation (24/6). EPO (10 IU/ml) was administered 24 hours before anoxia (t=-24), at the start of anoxia (t=0) and at the start of reoxygenation (t=24) (unpublished data). *p<0.01 vs. control.

Erythropoietin in heart: from bench to bedside
113
at various time points during hypoxia/reoxygenation (unpublished data; figure 1). In-vitro, EPO administration prevented apoptosis of endothelial cells subjected to hypoxia, through direct modulation of PI3K/Akt phosphorylation (37). In these cells, EPO was also shown to trigger the phosphorylation of STAT-5 and MAPK (38). Since apoptosis after myocardial infarction begins in endothelial cells and spreads to surrounding myocytes (39), protecting the endothelium may play a crucial role in preserving the myocardial structure.The expression of EPO-R was demonstrated also in neonatal (40) and adult rat cardiac myocytes (41). Similar to endothelial cells, EPO prevented the apoptosis of cardiomyocytes, by means of activating PI3/Akt pathway. In-vivo, EPO-R is expressed in normal rat cardiac tissue. Immunostaining for EPO-R is predominantly observed in interstitial cells, including endothelial cells and fibroblasts, with weak expression in cardiomyocytes (42). Perfusion of isolated rat hearts with EPO results in increased MAPK phosphorylation (42), which has been implicated as a survival pathway in cardiac cells during I/R injury, by inhibiting apoptosis (43). Recently, EPO-R expression was confirmed also in human heart tissue. Both ventricular myocytes and endothelial cells in the adult human heart were positive for the EPO-R (44).Expression of EPO itself in the heart, either under normal or hypoxic conditions, has not been reliably established (33).An entirely new concept of EPO-mediated protection was introduced by Leist et al. (45), through generating mutants of EPO, which do not bind to the classical dimeric EPO-R and lack hematopoietic activity, but nevertheless retain their protective properties in various models of tissue and organ ischemia. This could suggest existence of different types of receptors needed for hematopoietic and non-hematopoietic effects of EPO. Recently, a distinct receptor configuration mediating the tissue-protective EPO effects was identified, consisting of the EPO-receptor and beta-common receptor, which is present also in the myocardium (46).
Acute cardioprotective effects of EPO
In hematopoietic and non-hematopoietic tissues alike, EPO was shown to activate pathways leading to inhibition of apoptosis. Apoptosis, one of the major forms of cell death, has been implicated in different cardiovascular diseases. In myocardial infarction (MI) apoptosis might be a determinant of the final infarct size and its extent depends on the presence of post-isch-emic reperfusion (47). Recently, numerous ex vivo (in isolated rodent hearts) and in vivo studies have shown protective role of EPO during ischemic and ischemia/reperfusion (I/R) injury in the heart (Table 1).Pre-treatment of adult rats with EPO (5.000 IU/kg) 24-hours preceding I/R increased the functional recovery of isolated hearts during reperfusion (33). This was accompanied by pro-tection against apoptosis, as measured by the number of TUNEL positive cells and activity of pro-apoptotic marker caspase-3. The mechanism of EPO mediated protection was revealed by blockade of these effects with a specific inhibitor of PI3K/Akt pathway (48). The involve-ment of signal transducing pathways was further elucidated by Shi et al. in a rabbit isolated heart model, where the cardioprotective effects of EPO were abolished by inhibitors of two different MAPK (p38 and p42/44) (49). In the same study, potassium channels inhibitors also blocked the EPO effects, indicating a possible role of potassium channels in EPO-medi-ated preservation of heart function, possible due to reduction of calcium overload. In a study
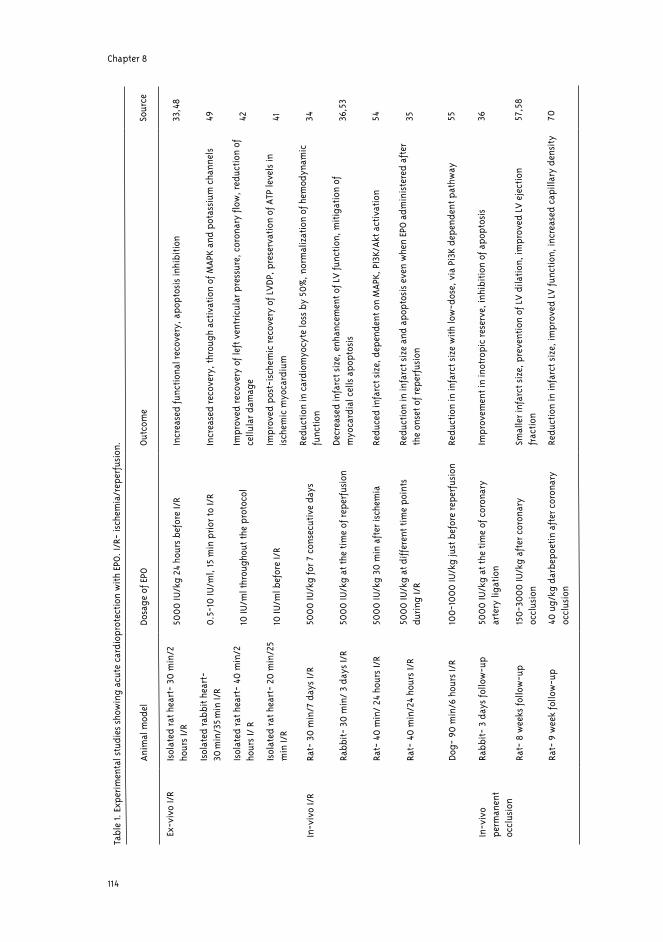
Chapter 8
114
Tabl
e 1.
Exp
erim
enta
l stu
dies
sho
win
g ac
ute
card
iopr
otec
tion
wit
h EP
O. I
/R-
isch
emia
/rep
erfu
sion
.
Anim
al m
odel
Dosa
ge o
f EPO
Out
com
eSo
urce
Isol
ated
rat h
eart
- 30
min
/2
hour
s I/
R50
00
IU/k
g 24
hou
rs b
efor
e I/
RIn
crea
sed
func
tion
al re
cove
ry, a
popt
osis
inhi
biti
on33
,48
Isol
ated
rabb
it h
eart
- 30
min
/35
min
I/R
0.5
-10
IU/m
l, 15
min
pri
or to
I/R
Incr
ease
d re
cove
ry, t
hrou
gh a
ctiv
atio
n of
MAP
K an
d po
tass
ium
cha
nnel
s49
Isol
ated
rat h
eart
- 40
min
/2
hour
s I/
R10
IU/m
l thr
ough
out t
he p
roto
col
Impr
oved
reco
very
of l
eft v
entr
icul
ar p
ress
ure,
cor
onar
y flo
w, r
educ
tion
of
cellu
lar d
amag
e42
Isol
ated
rat h
eart
- 20
min
/25
min
I/R
10 IU
/ml b
efor
e I/
RIm
prov
ed p
ost-
isch
emic
reco
very
of L
VDP
, pre
serv
atio
n of
ATP
leve
ls in
is
chem
ic m
yoca
rdiu
m41
In-v
ivo
I/R
Rat-
30
min
/7 d
ays
I/R
500
0 IU
/kg
for 7
con
secu
tive
day
sRe
duct
ion
in c
ardi
omyo
cyte
loss
by
≈50%
, nor
mal
izat
ion
of h
emod
ynam
ic
func
tion
34
Rabb
it-
30 m
in/
3 da
ys I/
R50
00
IU/k
g at
the
tim
e of
repe
rfus
ion
Decr
ease
d in
farc
t siz
e, e
nhan
cem
ent o
f LV
func
tion
, mit
igat
ion
of
myo
card
ial c
ells
apo
ptos
is36
,53
Rat-
40
min
/ 24
hou
rs I/
R50
00
IU/k
g 30
min
aft
er is
chem
iaRe
duce
d in
farc
t siz
e, d
epen
dent
on
MAP
K, P
I3K/
Akt a
ctiv
atio
n54
Rat-
40
min
/24
hour
s I/
R50
00
IU/k
g at
diff
eren
t tim
e po
ints
du
ring
I/R
Redu
ctio
n in
infa
rct s
ize
and
apop
tosi
s ev
en w
hen
EPO
adm
inis
tere
d af
ter
the
onse
t of r
eper
fusi
on35
Dog-
90
min
/6 h
ours
I/R
100
-10
00
IU/k
g ju
st b
efor
e re
perf
usio
nRe
duct
ion
in in
farc
t siz
e w
ith
low
-dos
e, v
ia P
i3K
depe
nden
t pat
hway
55
In-v
ivo
perm
anen
t oc
clus
ion
Rabb
it-
3 da
ys fo
llow
-up
500
0 IU
/kg
at th
e ti
me
of c
oron
ary
arte
ry li
gati
onIm
prov
emen
t in
inot
ropi
c re
serv
e, in
hibi
tion
of a
popt
osis
36
Rat-
8 w
eeks
follo
w-u
p15
0-3
00
0 IU
/kg
afte
r cor
onar
y oc
clus
ion
Smal
ler i
nfar
ct s
ize,
pre
vent
ion
of L
V d
ilati
on, i
mpr
oved
LV
eje
ctio
n fr
acti
on57
,58
Rat-
9 w
eek
follo
w-u
p40
ug/
kg d
arbe
poet
in a
fter
cor
onar
y oc
clus
ion
Redu
ctio
n in
infa
rct s
ize,
impr
oved
LV
func
tion
, inc
reas
ed c
apill
ary
dens
ity
70
Ex-v
ivo
I/R

Erythropoietin in heart: from bench to bedside
115
performed by our group, perfusion of isolated rat hearts with EPO during I/R attenuated the deterioration of left ventricular (LV) pressure and coronary flow during the reperfusion (42). EPO in this setting reduced also cellular damage (purine outflow) and number of cells en-tering apoptosis (active caspase-3 positive). This rapid cardioprotective effect of EPO during I/R injury is also associated with preservation of ATP levels in the ischemic myocardium (41), linking the anti-apoptotic function to metabolic normalization and consequently functional improvement.Although inhibition of apoptosis is widely accepted as a mechanism for EPO-mediated protection against acute ischemic injury, other possibilities should also be considered. Pretreatment with EPO was shown to inhibit the I/R induced myocardial inflammatory response (50), by preventing the “switching” of myocytes to proinflammatory phenotype, possibly also through upregulation of NO production. EPO can improve the cardiac function also by directly modulating the cardiac Na+/K+ pump (51) or stimulating the production of atrial natriuretic peptide in cardiac atrium (52).In the first in vivo study, Calvillo et al. (34), employed a rat model of coronary I/R. Administration of EPO (5.000 IU/kg/day) for seven consecutive days after reperfusion reduced the loss of cardiomyocytes by 50%, an extent sufficient to normalize hemodynamic function. However, the hematocrit increased by 20-30% by the end of the study and such a change alone may lead to improved cardiac function merely by improving the delivery of oxygen.In a rabbit model of MI, treatment with EPO at the time of permanent coronary ligation resulted in a trend towards reduced infarct size and improvement of cardiac contractility and relaxation when measured 3 days later. Moreover, the cardiac inotropic reserve, studied in response to beta-adrenergic receptor agonist, was significantly enhanced in the EPO-treated group (36). In addition, EPO administration in an in-vivo I/R was also found to be beneficial, resulting in a significant reduction of infarct size, expressed as a percentage of total ischemic area at risk (53). This protection was associated with the mitigation of myocardial cell apoptosis. Importantly, no significant differences in hematocrit levels were noted until day 3 after the infarction, discerning the hematopoietic from direct cardioprotective effects of EPO. Furthermore, in line with the results from ex vivo experiments, reduction of infarct size in vivo is dependent on the activation of pro-survival pathways PI3K/Akt and MAPK (54).The results of these studies raised two clinically important issues: that of the timing and the dosage of EPO administration. In a study performed by our group (35), EPO reduced infarct size and inhibited apoptosis when administered before the actual ischemic episode to until after the onset of reperfusion, providing a broad “window of opportunity” for the potential treatment of acute coronary syndromes. Since most of the previous experimental studies used high doses of EPO, parallel to those demonstrating neuroprotection (1.000-5.000 IU/kg), Hirata et al. (55) approached the issue of minimal EPO dose still rendering cardioprotection. EPO treatment in a canine model of I/R reduced infarct size in a dose-dependent manner, establishing the lowest effective dose of 100 IU/kg. The role of endogenous EPO/EPO-R system was revealed in a study with transgene mutant mice, which express EPO-R exclusively in the hematopoietic lineage (56). The infarct size after I/R injury in these mice was larger than in the wild type, subsequently accelerating the development of left ventricular remodeling.Importantly, the effects of EPO administration persist over a longer period after the ischemic insult. Moon et al. (57) found that a single dose of EPO (3.000 IU/kg) immediately after coronary artery ligation in rats reduced the infarct size to 15-25% that of untreated animals,

Chapter 8
116
examined 8 weeks later. This reduction in myocardial damage was accompanied by preven-tion of LV dilation and improved LV ejection fraction, as measured by repeated echocardiog-raphy. Importantly, the single EPO dose did not significantly increase hematocrit. This study was further elaborated by establishing the lowest effective dose (150 IU/kg) and extension of the therapeutic effect with higher doses up to 12 hours after MI (58). It seems that EPO may protect the myocardium also against more severe insults, such as permanent coronary occlu-sion and this effect becomes even more pronounced with time. Interestingly, for any given infarct size, EPO treatment has been shown to increase LV ejection fraction over a longer time frame (59), suggesting benefit on the infarct healing and post-MI remodeling.
Long-term effect of EPO in the heart
Current therapy in patients after MI is focused on prevention of ventricular remodeling and development of heart failure. Myocardial regeneration may offer possibilities that could im-prove cardiac function in these patients (60). Although regeneration of cardiomyocytes by proliferation or transdifferentiation seems lim-ited (61), the formation of new vessels in non-infarcted part may indirectly save cardiomyo-cytes and lead to improvement of ventricular function.Two processes contribute to postnatal formation of blood vessels. Angiogenesis is the sprout-ing of new vessels from existing ones, while vasculogenesis refers to formation of blood ves-sels from endothelial progenitor cells (EPCs)(62). These cells are undifferentiated bone mar-row cells, possessing the ability to mature into the cells lining the lumen of a blood vessel.Cytokine-induced mobilization of bone marrow cells after experimental MI leads to smaller infarct size and progressive improvement of ejection fraction, associated with forming of new vascular structures (63). After induction of MI, bone marrow-derived EPCs were found in foci of neovascularization at the border of the infarct (64).EPCs are mobilized also in patients during acute cardiac ischemic event (65). Recently, in-creased levels of circulating EPCs were associated with reduced risk of death from cardiovas-cular causes in patients with confirmed coronary artery disease (66). In the BOOST trial, in-tracoronary infusion of autologous bone marrow cells (CD34+) after myocardial infarction resulted in improved global LV ejection fraction 6 months after cell transfer (67). EPO was found to be a potent stimulus for EPCs mobilization, which was associated with neovascularization of ischemic tissue (68). The effect of EPO on the formation of new vessels has also been observed in an experimental model of stroke. EPO treatment, initiated 24 hours after induction of stroke, enhanced neovascularization and improved neurological function, while it did not significantly influence infarct size (69). In this study, high-dose EPO treatment for seven consecutive days (5.000-10.000 IU/kg/day), increased the density of microves-sels at the stroke boundary (ischemic penumbra), but it also resulted in a 44% increase in hematocrit level.We addressed this issue in the heart, evaluating the effect of EPO treatment on new vascular formation in an experimental heart failure model (70). Rats were subjected to coronary artery ligation and therapy with high-dose EPO analogue darbepoetin (40 μg/kg/3 weeks) was initiated 3-weeks post-MI. Although not reducing infarct size, EPO treatment significantly improved cardiac function. This improvement was coupled to increased capillary density and capillary-to-myocyte ratio, indicating neovascularization. Furthermore, these beneficial

Erythropoietin in heart: from bench to bedside
117
effects were also associated with increased percentage of alpha-MHC (myosine-heavy chain) isoforms, a molecular marker of enhanced myocardial contractility. In the clinical setting, treatment with rhEPO causes a significant mobilization and functional activation of EPCs in patients with renal anemia, as well as healthy subjects (71). EPO treatment in heart failure patients, while not influencing the number, significantly increased the adhesive and proliferative properties of EPCs (72). Interestingly, serum levels of EPO were significantly correlated with the number of circulating EPCs also in patients with established coronary artery disease (68).Besides stimulating and mobilizing EPCs, directly enhancing angiogenesis by EPO could also lead to neovascularization. EPO stimulates proliferation of endothelial cells in situ and their differentiation into vascular structures (73;74). In human cultured myocardial tissue, EPO stimulated capillary outgrowth comparable to VEGF (75). Treatment with EPO ameliorated healing of an ischemic skin wound, an effect attributable to increased microvessel density and higher level of VEGF expression (76;77).However, the doses used in the previous studies, when applied to clinical situation, could cause EPO overdose that may lead to hypertension, seizures, vascular thrombosis and death, possibly related to abruptly increased hematocrit values (78). This would be even of a greater concern in patients with already elevated cardiovascular risk.This considerable clinical problem was addressed by Bahlmann et al. (79). In their model of progressive renal disease, treatment with a low-dose EPO analogue darbepoetin conferred tissue protection and preserved capillary network in the kidney, but did not raise hematocrit. Also in patients with renal anemia, standard therapeutic dose of darbepoetin, markedly enhanced the proliferation (i.e. by about 300%) and differentiation of EPCs, compared with one order of magnitude lower increase in the number of red blood cells (i.e. about 30%) (80). In a recent study performed by our group we studied the effects of low (non-erythropoietic) dose darbepoetin in a rat model of post-MI heart failure. We showed that darbepoetin treatment preserves cardiac function, even in doses not affecting hematocrit level. This is associated with raised number of circulating EPCs and an increased capillary-to-myocyte ratio (submitted). Stimulation of EPCs, without increasing the number of red blood cells, implies specific EPO dose-effect relationships in different bone marrow cells.While time-limited treatment with high-dose EPO may be beneficial and safe during acute ischemic injury, if prolonged therapy is required (heart failure), drug regimens using low-dose EPO may be more suitable in avoiding the adverse effects of the treatment. In this regard the non-hematopoietic EPO derivates could also prove valuable, however their effect on vasculo- and/or angiogenesis is not yet established.
Clinical implications
Erythropoietin has been successfully used in clinical practice for more than two decades, for the most part to treat anemia in patients with chronic kidney disease (CKD), caused by diminished production of endogenous EPO. In these patients, anemia is an established risk factor for cardiovascular (CV) disease outcomes (81;82). Numerous smaller studies in pre-dialysis and dialysis patients have demonstrated a beneficial effect of anemia treatment with EPO on various surrogate CV endpoints (83;84). However, no conclusive data from randomized controlled trials exist establishing the impact of anemia treatment on cardiovascular and total

Chapter 8
118
mortality in patients with CKD (85). A recently started TREAT study will determine the effect of darbepoetin treatment on cardiovascular events in CKD patients (85).Anemia is also commonly observed in patients with chronic heart failure (CHF) and is related to the severity of the disease (86). Although the cause of anemia in these patients is multifactorial, inadequate EPO production and blunted response to EPO in the bone marrow play a major role (87). Consequently, elevated EPO levels are associated with the severity of CHF and are a prognostic marker for impaired survival, independent of hemoglobin levels (88;89). It seems that, although increased in absolute terms, EPO levels in anemic CHF patients are still relatively low to adequately stimulate the hematopoiesis in bone marrow. Higher levels of hematopoiesis inhibitors, such as Ac-SDKP, could also counterbalance the effects of EPO (90). In a number of small studies, normalization of hemoglobin levels with EPO in CHF patients was associated with improved LV ejection fraction (91) and enhanced exercise capacity (92). While this amelioration could be partly attributed to hemoglobin elevation and thus increased oxygen-binding capacity of blood, the non-hematopoietic effects of EPO must also be considered. Recently, two larger placebo-controlled phase II studies with EPO treatment in anemic CHF patients were conducted which also suggested a potential beneficial effects both in terms of quality of life, and clinical endpoints. For this reason a larger trial aimed at assessing its effect on morbidity and mortality is now being initiated.The non-hematopoietic tissue-protective properties of EPO may also be beneficial in treatment of patients with acute coronary syndromes. Currently, the emphasis in the treatment of myocardial infarction (MI) is on early reperfusion and hence limiting the damage of cardiac ischemia. However, development of post-MI heart failure remains a major challenge despite “optimal” therapy. EPO could on one hand acutely protect myocardial cells against ischemia/reperfusion induced injury and on the other hand attenuate the cardiac remodeling by stimulating the EPCs. Interestingly, high levels of endogenous EPO in patients with first MI who underwent successful primary coronary intervention (PCI), were found to be associated with smaller infarcts, which was interpreted by the authors as a possible endogenous, protective mechanism (93).We recently performed a first safety and feasibility study with darbepoetin treatment in patients with an acute MI (94). In this single-center, investigator-initiated, prospective study we randomized 22 non-anemic patients with a first acute MI to one bolus of 300 μg darbepoetin alfa or no additional medication before PCI. Administration of darbepoetin was both safe and well tolerated. In the darbepoetin group, serum EPO-levels increased to 130-270 times that of controls, within the first 24-hours. Darbepoetin administration led to only small and non-significant changes in hematocrit levels, while endothelial progenitor cells (CD34+/CD45-) were significantly increased at 72-hours. Despite a non-significantly longer “time to treatment” and more extensive baseline area at risk (cumulative ST-elevation) in the darbepoetin-treated group, left ventricular ejection fraction after 4 months was similar in the two groups (52±3% in darbepoetin vs. 48±5% in control group, p=NS). Recent studies showed that cardiovascular mortality in patients with acute coronary syndromes further increases as hemoglobin levels become lower (95;96). Specific therapeutic strategies, including EPO treatment, in such anemic patients with MI should also be further considered.
Erythropoietin in heart: from bench to bedside
119
Conclusions
A traditionally hematopoietic hormone erythropoietin is increasingly recognized as a pleiotropic cytokine, with effects reaching much further that stimulating red blood cells production (97). Although already used in cardiology to correct anemia in CHF patients, the non-hematopoietic effects of EPO may be beneficial also in non-anemic cardiovascular patients. From the experimental studies, EPO appears to influence two crucial processes during cardiac ischemic injury, first by acutely reducing the infarct size and inhibiting the apoptosis, and second by promoting new vessels formation over a longer time frame (figure 2). In clinics, randomized trials should translate the results of experimental studies and investigate the effectiveness of EPO treatment in various patient populations (acute MI, CHF).Although treatment with EPO is generally well tolerated and safe, it may be associated with adverse effects, such as hypertension and thromboembolism (98). These side effects are related mainly to high-dose chronic EPO treatment, associated with increased hematocrit. Using variants of EPO without hematopoietic effect, but retaining tissue protective activity could be useful in a clinical situation, where multiple EPO administrations would be warranted.Future studies should determine a place for EPO in the treatment of acute and chronic cardiac ischemia, which may have widespread implications for managing heart patients.
Figure 2. Biological functions of EPO. “Classical” hematopoietic effect and two mechanisms by which EPO renders cardioprotection in experiment.

Chapter 8
120
Reference List 1. Henry DH. Epoetin alfa. Clinical evolution of a pleiotropic cytokine. Archives of internal medicine. 2004;164:262-
276.
2. Jelkmann W, Wagner K. Beneficial and ominous aspects of the pleiotropic action of erythropoietin. Ann Hematol. 2004;83:673-686.
3. Philo JS, Aoki KH, Arakawa T et al. Dimerization of the extracellular domain of the erythropoietin (EPO) receptor by EPO: one high-affinity and one low-affinity interaction. Biochemistry. 1996;35:1681-1691.
4. Ratajczak J, Majka M, Kijowski J et al. Biological significance of MAPK, AKT and JAK-STAT protein activation by various erythropoietic factors in normal human early erythroid cells. Br J Haematol. 2001;115:195-204.
5. Fisher JW. Erythropoietin: physiology and pharmacology update. Exp Biol Med (Maywood ). 2003;228:1-14.
6. Lappin TR. EPO’s alter ego: erythropoietin has multiple actions. Stem cells. 2002;20:485-492.
7. Egrie JC. Characterization and biological effects of recombinant human erythropoietin. Immunobiology. 1986;172:213-224.
8. Winearls CG. Effect of human erythropoietin derived from recombinant DNA on the anaemia of patients maintained by chronic haemodialysis. The lancet. 1986;2:1175-1178.
9. Stein RS. The role of erythropoietin in the anemia of myelodysplastic syndrome. Clin Lymphoma. 2003;4 Suppl 1:S36-S40.
10. Littlewood TJ. Effects of epoetin alfa on hematologic parameters and quality of life in cancer patients receiving nonplatinum chemotherapy: results of a randomized, double-blind, placebo-controlled trial. Journal of clinical oncology. 2001;19:2865-2874.
11. Feagan BG. Erythropoietin with iron supplementation to prevent allogeneic blood transfusion in total hip joint arthroplasty. A randomized, controlled trial. Annals of internal medicine. 2000;133:845-854.
12. Juul SE. Erythropoietin and erythropoietin receptor in the developing human central nervous system. Pediatric research. 1998;43:40-49.
13. Anagnostou A. Erythropoietin receptor mRNA expression in human endothelial cells. Proceedings of the National Academy of Sciences of the United States of America. 1994;91:3974-3978.
14. Ammarguellat F, Llovera M, Kelly PA et al. Low doses of EPO activate MAP kinases but not JAK2-STAT5 in rat vascular smooth muscle cells. Biochem Biophys Res Commun. 2001;284:1031-1038.
15. Digicaylioglu M, Bichet S, Marti HH et al. Localization of specific erythropoietin binding sites in defined areas of the mouse brain. Proc Natl Acad Sci U S A. 1995;92:3717-3720.
16. Marti HH, Wenger RH, Rivas LA et al. Erythropoietin gene expression in human, monkey and murine brain. Eur J Neurosci. 1996;8:666-676.
17. Lewczuk P, Hasselblatt M, Kamrowski-Kruck H et al. Survival of hippocampal neurons in culture upon hypoxia: effect of erythropoietin. Neuroreport. 2000;11:3485-3488.
18. Siren AL, Knerlich F, Poser W et al. Erythropoietin and erythropoietin receptor in human ischemic/hypoxic brain. Acta Neuropathol (Berl). 2001;101:271-276.
Erythropoietin in heart: from bench to bedside
121
19. Brines ML, Ghezzi P, Keenan S et al. Erythropoietin crosses the blood-brain barrier to protect against experimental brain injury. Proc Natl Acad Sci U S A. 2000;97:10526-10531.
20. Sakanaka M, Wen TC, Matsuda S et al. In vivo evidence that erythropoietin protects neurons from ischemic damage. Proc Natl Acad Sci U S A. 1998;95:4635-4640.
21. Cerami A, Brines M, Ghezzi P et al. Neuroprotective properties of epoetin alfa. Nephrol Dial Transplant. 2002;17 Suppl 1:8-12.
22. Siren AL, Fratelli M, Brines M et al. Erythropoietin prevents neuronal apoptosis after cerebral ischemia and metabolic stress. Proc Natl Acad Sci U S A. 2001;98:4044-4049.
23. Wen TC, Sadamoto Y, Tanaka J et al. Erythropoietin protects neurons against chemical hypoxia and cerebral ischemic injury by up-regulating Bcl-xL expression. J Neurosci Res. 2002;67:795-803.
24. Villa P, Bigini P, Mennini T et al. Erythropoietin selectively attenuates cytokine production and inflammation in cerebral ischemia by targeting neuronal apoptosis. J Exp Med. 2003;198:971-975.
25. Calapai G, Marciano MC, Corica F et al. Erythropoietin protects against brain ischemic injury by inhibition of nitric oxide formation. Eur J Pharmacol. 2000;401:349-356.
26. Solaroglu I, Solaroglu A, Kaptanoglu E et al. Erythropoietin prevents ischemia-reperfusion from inducing oxidative damage in fetal rat brain. Childs Nerv Syst. 2003;19:19-22.
27. Ehrenreich H, Hasselblatt M, Dembowski C et al. Erythropoietin therapy for acute stroke is both safe and beneficial. Mol Med. 2002;8:495-505.
28. Ehrenreich H, Timner W, Siren AL. A novel role for an established player: anemia drug erythropoietin for the treatment of cerebral hypoxia/ischemia. Transfus Apheresis Sci. 2004;31:39-44.
29. Patel NS, Sharples EJ, Cuzzocrea S et al. Pretreatment with EPO reduces the injury and dysfunction caused by ischemia/reperfusion in the mouse kidney in vivo. Kidney Int. 2004;66:983-989.
30. Sharples EJ, Patel N, Brown P et al. Erythropoietin protects the kidney against the injury and dysfunction caused by ischemia-reperfusion. J Am Soc Nephrol. 2004;15:2115-2124.
31. Grimm C, Wenzel A, Groszer M et al. HIF-1-induced erythropoietin in the hypoxic retina protects against light-induced retinal degeneration. Nat Med. 2002;8:718-724.
32. Squadrito F, Altavilla D, Squadrito G et al. Recombinant human erythropoietin inhibits iNOS activity and reverts vascular dysfunction in splanchnic artery occlusion shock. Br J Pharmacol. 1999;127:482-488.
33. Cai Z, Manalo DJ, Wei G et al. Hearts from rodents exposed to intermittent hypoxia or erythropoietin are protected against ischemia-reperfusion injury. Circulation. 2003;108:79-85.
34. Calvillo L, Latini R, Kajstura J et al. Recombinant human erythropoietin protects the myocardium from ischemia-reperfusion injury and promotes beneficial remodeling. Proc Natl Acad Sci U S A. 2003;100:4802-4806.
35. Lipšic E, van der Meer P, Henning RH et al. Timing of erythropoietin treatment for cardioprotection in ischemia/reperfusion. J Cardiovasc Pharmacol. 2004;44:473-479.
36. Parsa CJ, Matsumoto A, Kim J et al. A novel protective effect of erythropoietin in the infarcted heart. J Clin Invest. 2003;112:999-1007.
Chapter 8
122
37. Chong ZZ, Kang JQ, Maiese K. Erythropoietin is a novel vascular protectant through activation of Akt1 and mitochondrial modulation of cysteine proteases. Circulation. 2002;106:2973-2979.
38. Fuste B, Serradell M, Escolar G et al. Erythropoietin triggers a signaling pathway in endothelial cells and increases the thrombogenicity of their extracellular matrices in vitro. Thromb Haemost. 2002;88:678-685.
39. Scarabelli T, Stephanou A, Rayment N et al. Apoptosis of endothelial cells precedes myocyte cell apoptosis in ischemia/reperfusion injury. Circulation. 2001;104:253-256.
40. Tramontano AF, Muniyappa R, Black AD et al. Erythropoietin protects cardiac myocytes from hypoxia-induced apoptosis through an Akt-dependent pathway. Biochem Biophys Res Commun. 2003;308:990-994.
41. Wright GL, Hanlon P, Amin K et al. Erythropoietin receptor expression in adult rat cardiomyocytes is associated with an acute cardioprotective effect for recombinant erythropoietin during ischemia-reperfusion injury. FASEB J. 2004;18:1031-1033.
42. Van der Meer P, Lipšic E, Henning RH et al. Erythropoietin improves left ventricular function and coronary flow in an experimental model of ischemia-reperfusion injury. Eur J Heart Fail. 2004;6:853-859.
43. Ravingerova T, Barancik M, Strniskova M. Mitogen-activated protein kinases: a new therapeutic target in cardiac pathology. Mol Cell Biochem. 2003;247:127-138.
44. Depping R, Kawakami K, Ocker H et al. Expression of the erythropoietin receptor in human heart. J Thorac Cardiovasc Surg. 2005;130:877-2.
45. Leist M, Ghezzi P, Grasso G et al. Derivatives of erythropoietin that are tissue protective but not erythropoietic. Science. 2004;305:239-242.
46. Brines M, Grasso G, Fiordaliso F et al. Erythropoietin mediates tissue protection through an erythropoietin and common beta-subunit heteroreceptor. Proc Natl Acad Sci U S A. 2004;101:14907-14912.
47. Rodriguez M, Lucchesi BR, Schaper J. Apoptosis in myocardial infarction. Ann Med. 2002;34:470-479.
48. Cai Z, Semenza GL. Phosphatidylinositol-3-kinase signaling is required for erythropoietin-mediated acute protection against myocardial ischemia/reperfusion injury. Circulation. 2004;109:2050-2053.
49. Shi Y, Rafiee P, Su J et al. Acute cardioprotective effects of erythropoietin in infant rabbits are mediated by activation of protein kinases and potassium channels. Basic Res Cardiol. 2004;99:173-182.
50. Rui T, Feng Q, Lei M et al. Erythropoietin prevents the acute myocardial inflammatory response induced by ischemia/reperfusion via induction of AP-1. Cardiovasc Res. 2005;65:719-727.
51. Wald M, Gutnisky A, Borda E et al. Erythropoietin modified the cardiac action of ouabain in chronically anaemic-uraemic rats. Nephron. 1995;71:190-196.
52. Porat O, Neumann D, Zamir O et al. Erythropoietin stimulates atrial natriuretic peptide secretion from adult rat cardiac atrium. J Pharmacol Exp Ther. 1996;276:1162-1168.
53. Parsa CJ, Kim J, Riel RU et al. Cardioprotective effects of erythropoietin in the reperfused ischemic heart: a potential role for cardiac fibroblasts. J Biol Chem. 2004;279:20655-20662.
54. Bullard AJ, Govewalla P, Yellon DM. Erythropoietin protects the myocardium against reperfusion injury in vitro and in vivo. Basic Res Cardiol. 2005;100:397-403.
Erythropoietin in heart: from bench to bedside
123
55. Hirata A, Minamino T, Asanuma H et al. Erythropoietin just before reperfusion reduces both lethal arrhythmias and infarct size via the phosphatidylinositol-3 kinase-dependent pathway in canine hearts. Cardiovasc Drugs Ther. 2005;19:33-40.
56. Tada H, Ohta J, Takeda M et al. Deficiency of erythropoietin receptor gene in nonhematopoietic lineage deteriorates left ventricular remodeling after myocardial ischemia and reperfusion. Circulation. 2004;110:27 (abstract)
57. Moon C, Krawczyk M, Ahn D et al. Erythropoietin reduces myocardial infarction and left ventricular functional decline after coronary artery ligation in rats. Proc Natl Acad Sci U S A. 2003;100:11612-11617.
58. Moon C, Krawczyk M, Paik D et al. Cardioprotection by Recombinant Human Erythropoietin Following Acute Experimental Myocardial Infarction: Dose Response and Therapeutic Window. Cardiovasc Drugs Ther. 2005.
59. Hale SL, Sesti C, Kloner RA. Administration of erythropoietin fails to improve long-term healing or cardiac function after myocardial infarction in the rat. J Cardiovasc Pharmacol. 2005;46:211-215.
60. Lee MS, Makkar RR. Stem-cell transplantation in myocardial infarction: a status report. Ann Intern Med. 2004;140:729-737.
61. Murry CE, Soonpaa MH, Reinecke H et al. Haematopoietic stem cells do not transdifferentiate into cardiac myocytes in myocardial infarcts. Nature. 2004;428:664-668.
62. Szmitko PE, Fedak PW, Weisel RD et al. Endothelial progenitor cells: new hope for a broken heart. Circulation. 2003;107:3093-3100.
63. Orlic D, Kajstura J, Chimenti S et al. Mobilized bone marrow cells repair the infarcted heart, improving function and survival. Proc Natl Acad Sci U S A. 2001;98:10344-10349.
64. Asahara T, Masuda H, Takahashi T et al. Bone marrow origin of endothelial progenitor cells responsible for postnatal vasculogenesis in physiological and pathological neovascularization. Circ Res. 1999;85:221-228.
65. Shintani S, Murohara T, Ikeda H et al. Mobilization of endothelial progenitor cells in patients with acute myocardial infarction. Circulation. 2001;103:2776-2779.
66. Werner N, Kosiol S, Schiegl T et al. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med. 2005;353:999-1007.
67. Wollert KC, Meyer GP, Lotz J et al. Intracoronary autologous bone-marrow cell transfer after myocardial infarction: the BOOST randomised controlled clinical trial. Lancet. 2004;364:141-148.
68. Heeschen C, Aicher A, Lehmann R et al. Erythropoietin is a potent physiologic stimulus for endothelial progenitor cell mobilization. Blood. 2003;102:1340-1346.
69. Wang Y, Zhang ZG, Wang L et al. Erythropoietin enhances neurogenesis and angiogenesis in the brain and improves functional recovery after embolic stroke in the adult rat. Stroke. 2004;35:239.
70. Van der Meer P, Lipšic E, Henning RH et al. Erythropoietin induces neovascularization and improves cardiac function in rats with heart failure after myocardial infarction. J Am Coll Cardiol. 2005;46:125-133.
71. Bahlmann FH, De Groot K, Spandau JM et al. Erythropoietin regulates endothelial progenitor cells. Blood. 2004;103:921-926.
72. George J, Goldstein E, Abashidze A et al. Erythropoietin promotes endothelial progenitor cell proliferative and adhesive properties in a PI 3-kinase-dependent manner. Cardiovasc Res. 2005.
Chapter 8
124
73. Ribatti D, Presta M, Vacca A et al. Human erythropoietin induces a pro-angiogenic phenotype in cultured endothelial cells and stimulates neovascularization in vivo. Blood. 1999;93:2627-2636.
74. Carlini RG, Reyes AA, Rothstein M. Recombinant-Human-Erythropoietin Stimulates Angiogenesis In-Vitro. Kidney Int. 1995;47:740-745.
75. Jaquet K, Krause K, Tawakol-Khodai M et al. Erythropoietin and VEGF exhibit equal angiogenic potential. Microvasc Res. 2002;64:326-333.
76. Buemi M, Galeano M, Sturiale A et al. Recombinant human erythropoietin stimulates angiogenesis and healing of ischemic skin wounds. Shock. 2004;22:169-173.
77. Galeano M, Altavilla D, Cucinotta D et al. Recombinant human erythropoietin stimulates angiogenesis and wound healing in the genetically diabetic mouse. Diabetes. 2004;53:2509-2517.
78. Besarab A, Bolton WK, Browne JK et al. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med. 1998;339:584-590.
79. Bahlmann FH, Song R, Boehm SM et al. Low-dose therapy with the long-acting erythropoietin analogue darbepoetin alpha persistently activates endothelial Akt and attenuates progressive organ failure. Circulation. 2004;110:1006-1012.
80. Bahlmann FH, DeGroot K, Duckert T et al. Endothelial progenitor cell proliferation and differentiation is regulated by erythropoietin. Kidney Int. 2003;64:1648-1652.
81. Pereira AA, Sarnak MJ. Anemia as a risk factor for cardiovascular disease. Kidney Int Suppl. 2003;S32-S39.
82. Foley RN, Parfrey PS, Harnett JD et al. The impact of anemia on cardiomyopathy, morbidity, and and mortality in end-stage renal disease. Am J Kidney Dis. 1996;28:53-61.
83. Ayus JC, Go AS, Valderrabano F et al. Effects of erythropoietin on left ventricular hypertrophy in adults with severe chronic renal failure and hemoglobin <10 g/dL. Kidney Int. 2005;68:788-795.
84. McMahon LP, Mason K, Skinner SL et al. Effects of haemoglobin normalization on quality of life and cardiovascular parameters in end-stage renal failure. Nephrol Dial Transplant. 2000;15:1425-1430.
85. Mix TC, Brenner RM, Cooper ME et al. Rationale--Trial to Reduce Cardiovascular Events with Aranesp Therapy (TREAT): evolving the management of cardiovascular risk in patients with chronic kidney disease. Am Heart J. 2005;149:408-413.
86. Van der Meer P, Voors AA, Lipšic E et al. Erythropoietin in cardiovascular diseases. Eur Heart J. 2004;25:285-291.
87. Opasich C, Cazzola M, Scelsi L et al. Blunted erythropoietin production and defective iron supply for erythropoiesis as major causes of anaemia in patients with chronic heart failure. Eur Heart J. 2005;26:2232-2237.
88. Van der Meer P, Voors AA, Lipšic E et al. Prognostic value of plasma erythropoietin on mortality in patients with chronic heart failure. J Am Coll Cardiol. 2004;44:63-67.
89. George J, Patal S, Wexler D et al. Circulating erythropoietin levels and prognosis in patients with congestive heart failure: comparison with neurohormonal and inflammatory markers. Arch Intern Med. 2005;165:1304-1309.
Erythropoietin in heart: from bench to bedside
125
90. Van der Meer P, Lipšic E, Westenbrink BD et al. Levels of hematopoiesis inhibitor N-acetyl-seryl-aspartyl-lysyl-proline partially explain the occurrence of anemia in heart failure. Circulation. 2005;112:1743-1747.
91. Silverberg DS, Wexler D, Sheps D et al. The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study. J Am Coll Cardiol. 2001;37:1775-1780.
92. Mancini DM, Katz SD, Lang CC et al. Effect of erythropoietin on exercise capacity in patients with moderate to severe chronic heart failure. Circulation. 2003;107:294-299.
93. Namiuchi S, Kagaya Y, Ohta J et al. High serum erythropoietin level is associated with smaller infarct size in patients with acute myocardial infarction who undergo successful primary percutaneous coronary intervention. J Am Coll Cardiol. 2005;45:1406-1412.
94. Lipšic E, van der Meer P, Voors AA et al. A single bolus of long-acting erythropoietin analogue darbepoetin in patients with an acute myocardial infarction: randomized feasibility and safety study. Circulation. 2005;112:II-423 (abstract)
95. Lipšic E, van der Horst IC, Voors AA et al. Hemoglobin levels and 30-day mortality in patients after myocardial infarction. Int J Cardiol. 2005;100:289-292.
96. Sabatine MS, Morrow DA, Giugliano RP et al. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation. 2005;111:2042-2049.
97. Van der Meer P, Lipšic E, Van Gilst WH et al. Erythropoietin: from hematopoiesis to cardioprotection. Cardiovasc Drugs Ther. 2005;19:7-8.
98. Smith KJ, Bleyer AJ, Little WC et al. The cardiovascular effects of erythropoietin. Cardiovasc Res. 2003;59:538-548.


Chapter 9
Summary and conclusions

Chapter 9
128
Summary
Therapeutic strategies in the treatment of myocardial infarction (MI) are currently directed to shortening the time of ischemia by restoration of coronary blood flow (“open artery theory”). Although early reperfusion therapy of MI limits the extent of myocardial necrosis and improves the clinical outcome, morbidity and mortality after MI remains significant. Additional protection of myocardial cells during ischemia and reperfusion is needed to further limit cardiomyocyte death, with positive effect on cardiac function and prognosis of patients with acute MI (1).Furthermore, most patients will at some time after MI develop heart failure, or left ventricular (LV) systolic dysfunction (2). As the five-years mortality of patients with a diagnosis of heart failure remains above 50% (3), strategies aimed at regeneration of failing myocardium may be required.Traditionally viewed as a hormone stimulating hematopoiesis, erythropoietin (EPO) is recently considered to influence a broad array of cellular processes, that include protection against ischemic injury, angiogenesis and stem cell development (4).In recent years, expression of functional EPO-R has been demonstrated in non-hematopoietic cells and organs including brain, kidney and cardiovascular tissue. These findings suggest that besides stimulating hematopoiesis, EPO may play a role as a pleiotropic survival and growth factor (5).
Acute cardioprotectionMany experimental studies have shown the protective effect of EPO in the brain. Systemic administration of EPO before or up to 6 hours after focal brain ischemia reduced the infarct volume by 50-75% (6). In chapter 2 we examined the presence and functionality of EPO receptor in cardiac tissue and evaluated the effect of exogenous EPO administration on cardiac performance during ischemia/reperfusion (I/R). In the first part of the experiment we demonstrated the expression of EPO receptor in the rat heart, which is mainly present on endothelial cells and fibroblasts, and to a lesser extent on cardiomyocytes. Furthermore, the perfusion of isolated rat hearts (Langendorff set-up) with high concentration of EPO led to activation of important signaling pathway- MAPK, which was implicated in cell survival after reperfusion injury in the heart (7). In the second part of the study, administration of exogenous EPO during I/R resulted in improved recovery of left ventricular pressure and coronary flow. Moreover, this was associated with a 56% reduction of cellular damage during reperfusion and diminished apoptosis.In the last few years, different groups demonstrated that administration of EPO during in vivo cardiac I/R and permanent coronary ligation led to infarct size reduction associated with mitigation of apoptosis (8;9). Early reduction in infarct size and apoptosis inhibition was also associated with subsequent prevention of LV dysfunction (10). However, the clinically relevant question of therapeutic window for EPO-mediated cardioprotection during I/R in the heart remained to be answered. We addressed this issue in chapter 3, administrating EPO 2 hours before I/R, at the start of ischemia and after the onset of reperfusion. A single dose of EPO at different time points resulted in 19-23% reduction in infarct size, which was accompanied by an improved LV function. Furthermore, EPO reduced the number of cells entering apoptosis but had no effect on proliferative activity in myocardium. Thus rather than stimulating cell proliferation, EPO inhibits the programmed cell death associated

Summary
129
with acute I/R injury. Importantly, this effect could not be ascribed to hematocrit increase, since this would occur not before 2-3 days after the EPO administration. The extension of cardioprotective effects of EPO beyond the start of reperfusion provides a broad “window of opportunity” for potential treatment of acute coronary syndromes.
Post-MI Neovascularization and RegenerationBesides its acute cardioprotective effects, through inhibition of apoptosis, EPO may also in-fluence formation of new vessels (neovascularization) after ischemic injury. In a rat model of stroke, EPO treatment initiated 24 hours after the occlusion of cerebral artery improved neu-rological function and increased the density of cerebral microvessels in the stroke boundary (11). In the heart, neovascularization in the non-infarcted hypertrophied part of the myocar-dium, may improve cardiac function and attenuate post-MI LV remodeling (12). In chapter 4 we assessed the impact of EPO treatment on new vessels formation in a post-MI heart failure. We confirmed previous findings, that administration of EPO immediately after the induction of MI reduces the infarct size, which was associated with improved hemodynamics. More interestingly, EPO treatment started three weeks after MI, despite not affecting the infarct size, resulted in improved cardiac performance, as shown by a 17% increase in LV developed pres-sure and 46% decrease in N-ANP levels. This improvement was associated with restoration of capillary density to sham levels and significant increase in capillary-to-myocyte ratio, indicat-ing neovascularization. Furthermore, these beneficial effects were also related to increased percentage of alpha-MHC (myosine-heavy chain) isoforms, a molecular marker of enhanced myocardial contractility. Although our study showed apparent effect of EPO on formation of new blood vessels after MI, several questions remained unanswered. Hematocrit increased by 27% in the EPO treated rats, and although less likely, the elevated oxygen-carrying capacity of blood may have con-tributed to improved cardiac performance. In addition, when applied to clinical situation, chronic high-dose EPO treatment may cause hypertension, seizures, vascular thrombosis and death (13). This would be even of greater concern in patients with already elevated cardiovas-cular risk. Moreover, the mechanism behind the effect of EPO on neovascularization remains largely unknown. Both stimulation of in situ endothelial cells proliferation or mobilization of endothelial progenitor cells (EPCs) derived from the bone marrow may play a role. Recently, increased levels of circulating EPCs were associated with reduced risk of death from cardio-vascular causes in patients with confirmed coronary artery disease (14). Importantly, EPO was shown to stimulate the mobilization and functional activity of EPCs (15). To discern the hematopoietic from non-hematopoietic effects of EPO and study the possible mechanisms involved, we compared low- vs. high-dose EPO treatment in a post-MI heart failure rat model (chapter 5). We assessed cardiac function over time, EPCs mobilization and neovascularization. Hematocrit increased with high- but not with low-dose treatment. In both EPO-treated groups, serial echocardiography demonstrated preservation of left ventricular systolic function during 9-weeks long follow-up, and hemodynamic measurements revealed improved cardiac contractility and relaxation at the end of the study. In addition, in EPO-treated groups the number of circulating EPCs was significantly increased, which was associated with a 42% increase in capillary-to-myocyte ratio in high-dose and 28% in low-dose group. This is in line with a study performed in a rat model of progressive renal disease, where treatment with a low-dose EPO conferred tissue protection and preserved capillary network in the kidney, but did not raise hematocrit (16).

Chapter 9
130
Thus in situations where prolonged treatment is warranted (heart failure), low-dose EPO may maintain to be beneficial, and at the same time avoid the occurrence of adverse effect associated with hematocrit increase.
Clinical ImplicationsEPO has been used in clinical medicine for more than two decades, initially to treat anemia caused by reduced EPO production related to chronic kidney disease. The indications for EPO treatment have extended in the last years to include also anemia in patients with myelodysplastic syndromes, cancer patients treated with chemotherapy, and prophylactic treatment to reduce the need for transfusions before major surgery (17). In cardiology, EPO treatment in chronic heart failure patients with anemia has been shown to improve LV ejection fraction (18) and enhance exercise capacity (19). However, although the range of indications for EPO treatment is becoming broader, so far the main objective of the therapy is to increase hematocrit in anemic patients. Nevertheless, non-hematopoietic effects of EPO may also be beneficial in non-anemic patients experiencing acute ischemic event. Indeed, a first randomized, clinical trial in stroke patients showed that beyond being safe and well tolerated, EPO treatment also improves clinical outcome and ameliorates the ischemic brain damage (20).In heart, while there is a rapidly increasing number of studies which suggest a protective role of EPO treatment in experimental ischemia, so far no clinical data are available. Interestingly, higher levels of endogenous EPO were shown to be independently associated with smaller infarct size in patients with acute MI (21). In chapter 6 we performed a pilot clinical study with EPO treatment in acute MI patients. The primary objective of this single center, investigator-initiated, randomized study was to evaluate the safety and tolerability of long-acting EPO analogue darbepoetin alfa treatment in non-anemic patients with acute ST-elevation MI treated with primary coronary angioplasty (PCI). Twenty-two patients were randomized to receive one bolus of 300 μg long-acting EPO analogue darbepoetin alfa or no additional medication before PCI. Administration of darbepoetin alfa in patients was both safe and well tolerated. We did not encounter any adverse events associated with darbepoetin treatment. Rather than increasing the hematocrit above reference values, one bolus of darbepoetin merely prevented the decrease in hematocrit observed in the control group. Importantly, darbepoetin treatment led to a significant elevation of EPCs, 72-hours after the drug administration. Despite non-significantly longer “time to treatment” and more extensive baseline area at risk (cumulative ST-elevation) in the darbepoetin-treated group, LV function 4 months after the MI was similar in both groups. The results of this first pilot study support a larger scale clinical trial to establish efficacy of EPO administration in patients with acute MI. Already for a long time, anemia is recognized as a risk factor for cardiovascular (CV) outcomes in patients with chronic kidney disease and heart failure. Recently, anemia was associated also with reduced survival in patients with established and stable coronary artery disease (22). In chapter 7, we examined the effect of hemoglobin levels on short-term CV mortality in patients with acute MI. In a retrospective study, we analyzed 1841 consecutive patients admitted with the diagnosis of acute MI. We found a statistically significant increase in 30-day mortality in patients presenting with hemoglobin lower than 10 g/dl. Although other risk factors (age, renal function) were more strongly associated with the survival, and could in part explain the effect of anemia, low hemoglobin levels remained independent predictor of 30-day mortality even after adjustment for these variables. Specific therapeutic strategies, including EPO treatment, in such anemic MI patients should also be further considered.

Summary
131
Conclusions
A traditionally hematopoietic hormone erythropoietin is increasingly recognized as a pleiotropic cytokine, with effects reaching further that stimulating red blood cells production (discussed in chapter 8). The detection of EPO receptor expression outside the hematopoietic system implicated the possibility of various non-hematopoietic functions of EPO. In brain, EPO was shown to confer neuroprotection against stroke and other neurological disorders. Beneficial effects of EPO during ischemic injury were documented also in various other organs and tissues.Recombinant form of EPO has been used in clinical setting for almost two decades to treat different forms of anemia. Although treatment with EPO is generally well tolerated and safe, it may be associated with adverse effects, mainly related to hematocrit increase (13). The recently synthetized non-hematopoietic variants of EPO, which retain tissue protective activity, may prove to be both effective and safe alternative for non-anemic patients with organ ischemia (23).In heart, EPO appears to influence two crucial processes during experimental cardiac ischemia/reperfusion injury, first by acutely inhibiting the apoptosis and reducing the infarct size, and second by promoting neovascularization and preserving the myocardial structure and function over longer time frame. If these effects could be extrapolated to heart patients, EPO treatment of acute coronary syndromes may be able to “kill two birds with one stone”.
Chapter 9
132
Reference List1. Kloner RA, Rezkalla SH. Cardiac protection during acute myocardial infarction: where do we stand in 2004? J
Am Coll Cardiol. 2004;44:276-286.
2. Cleland JG, Torabi A, Khan NK. Epidemiology and management of heart failure and left ventricular systolic dysfunction in the aftermath of a myocardial infarction. Heart. 2005;91 Suppl 2:ii7-13.
3. Swedberg K, Cleland J, Dargie H et al. Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26:1115-1140.
4. Maiese K, Li F, Chong ZZ. New avenues of exploration for erythropoietin. JAMA. 2005;293:90-95.
5. Van der Meer P., Voors AA, Lipšic E et al. Erythropoietin in cardiovascular diseases. Eur Heart J. 2004;25:285-291.
6. Brines ML, Ghezzi P, Keenan S et al. Erythropoietin crosses the blood-brain barrier to protect against experimental brain injury. Proc Natl Acad Sci U S A. 2000;97:10526-10531.
7. Ravingerova T, Barancik M, Strniskova M. Mitogen-activated protein kinases: a new therapeutic target in cardiac pathology. Mol Cell Biochem. 2003;247:127-138.
8. Parsa CJ, Matsumoto A, Kim J et al. A novel protective effect of erythropoietin in the infarcted heart. J Clin Invest. 2003;112:999-1007.
9. Shi Y, Rafiee P, Su J et al. Acute cardioprotective effects of erythropoietin in infant rabbits are mediated by activation of protein kinases and potassium channels. Basic Res Cardiol. 2004;99:173-182.
10. Moon C, Krawczyk M, Ahn D et al. Erythropoietin reduces myocardial infarction and left ventricular functional decline after coronary artery ligation in rats. Proc Natl Acad Sci U S A. 2003;100:11612-11617.
11. Wang L, Zhang Z, Wang Y et al. Treatment of stroke with erythropoietin enhances neurogenesis and angiogenesis and improves neurological function in rats. Stroke. 2004;35:1732-1737.
12. Dzau VJ, Gnecchi M, Pachori AS et al. Therapeutic potential of endothelial progenitor cells in cardiovascular diseases. Hypertension. 2005;46:7-18.
13. Smith KJ, Bleyer AJ, Little WC et al. The cardiovascular effects of erythropoietin. Cardiovasc Res. 2003;59:538-548.
14. Werner N, Kosiol S, Schiegl T et al. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med. 2005;353:999-1007.
15. Bahlmann FH, De Groot K, Spandau JM et al. Erythropoietin regulates endothelial progenitor cells. Blood. 2004;103:921-926.
16. Bahlmann FH, Song R, Boehm SM et al. Low-dose therapy with the long-acting erythropoietin analogue darbepoetin alpha persistently activates endothelial Akt and attenuates progressive organ failure. Circulation. 2004;110:1006-1012.
17. Henry DH, Bowers P, Romano MT et al. Epoetin alfa. Clinical evolution of a pleiotropic cytokine. Arch Intern Med. 2004;164:262-276.
Summary
133
18. Silverberg DS, Wexler D, Sheps D et al. The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study. J Am Coll Cardiol. 2001;37:1775-1780.
19. Mancini DM, Katz SD, Lang CC et al. Effect of erythropoietin on exercise capacity in patients with moderate to severe chronic heart failure. Circulation. 2003;107:294-299.
20. Ehrenreich H, Hasselblatt M, Dembowski C et al. Erythropoietin therapy for acute stroke is both safe and beneficial. Mol Med. 2002;8:495-505.
21. Namiuchi S, Kagaya Y, Ohta J et al. High serum erythropoietin level is associated with smaller infarct size in patients with acute myocardial infarction who undergo successful primary percutaneous coronary intervention. J Am Coll Cardiol. 2005;45:1406-1412.
22. Reinecke H, Trey T, Wellmann J et al. Haemoglobin-related mortality in patients undergoing percutaneous coronary interventions. Eur Heart J. 2003;24:2142-2150.
23. Fiordaliso F, Chimenti S, Staszewsky L et al. A nonerythropoietic derivative of erythropoietin protects the myocardium from ischemia-reperfusion injury. Proc Natl Acad Sci U S A. 2005;102:2046-2051.


Samenvatting en conclusies

Samenvatting
136
Samenvatting
De behandeling van het myocard infarct (MI) is tegenwoordig gericht op verkorting van is-chemie-tijd door herstel van de coronair flow (“open arterie theorie”). Hoewel vroegtijdige reperfusietherapie van het MI de omvang van de myocardiale necrose beperkt, blijft de mor-biditeit en mortaliteit na het MI hoog. Additionele bescherming van de myocardcellen tijdens ischemie en reperfusie is nodig om afsterven van de cardiomyocyten verder te reduceren, zodat de hartfunctie en de prognose van patiënten met een acuut MI verbetert.Een MI leidt bij een groot deel van de patiënten op de langere termijn tot hartfalen, of linker ventrikel dysfunctie. Aangezien de vijf-jaars mortaliteit van patiënten met hartfalen hoger dan 50% blijft, zijn strategieën gericht op regeneratie van het falende hart noodzakelijk.Traditioneel werd erytropoëtine (EPO) gezien als een hematopoëtisch hormoon. Recent on-derzoek heeft echter laten zien dat EPO als een cytokine moet worden beschouwd dat ver-schillende cellulaire processen kan beïnvloeden, zoals bescherming tijdens ischemie, maar ook angiogenese of stimulatie van stamcellen.De afgelopen jaren hebben verscheidene onderzoeken aangetoond dat er een functionele EPO receptor aanwezig is in niet-hematopoëtische organen, zoals de hersenen, de nieren en ook in cardiovasculair weefsel. Deze bevindingen suggereren dat EPO naast de stimulatie van de hematopoëse ook een rol zou kunnen spelen als overlevings- en groeifactor.
Acute cardioprotectie
Verschillende experimentele studies hebben een beschermend effect van EPO tijdens hersenischemie laten zien. Systemische toediening van EPO voor of tot 6 uur na een herseninfarct leidt tot een 50-75% reductie van het infarctvolume. In hoofdstuk 2 hebben wij gekeken naar de aanwezigheid en functionaliteit van de EPO receptor in het hart en naar de effecten van exogene EPO toediening op de hartfunctie tijdens ischemie/reperfusie (I/R). In het eerste deel van het experiment lieten wij zien dat de EPO receptor tot expressie wordt gebracht in het hart, voornamelijk op endotheelcellen en fibroblasten, en in mindere mate ook op cardiomyocyten. Perfusie van de geïsoleerde rattenharten (Langendorff opstelling) met EPO leidde bovendien tot activatie van het belangrijke signaalpad MAPK, dat betrokken is bij de overleving van hartcellen na reperfusie. In het tweede deel van de studie werd aangetoond dat EPO behandeling tijdens I/R leidde tot herstel van linkerventrikel druk en coronaire flow. Deze effecten gingen gepaard met een reductie aan celschade van 56% gedurende reperfusie en met een verminderde apoptose.Recentelijk hebben verschillende groepen aangetoond dat EPO behandeling tijdens I/R van het hart in vivo, maar ook tijdens permanente coronaire occlusie, leidt tot reductie van de infarctgrootte, hetgeen geassocieerd is met remming van de apoptotische celdood. Vroeg-tijdige reductie van infarctgrootte en apoptose was tevens geassocieerd met een afname in linker ventrikel (LV) dysfunctie. Desondanks bleef het onduidelijk wanneer EPO toediening tijdens I/R nog cardiale protectie gaf. Dit onderwerp hebben wij in hoofdstuk 3 bestudeerd. EPO behandeling werd gegeven of 2 uur voor de I/R, aan het begin van de ischemie of na aanvang van de reperfusie. Een éénmalige toediening van EPO op de verschillende tijdspun-ten resulteerde in een reductie in infarctgrootte van 19-23%, die geassocieerd was met een verbeterde LV functie. Bovendien reduceerde EPO het aantal cellen dat apoptose onderging, zonder een effect op de proliferatieve activiteit van het myocard te hebben. Deze effecten kunnen niet toegeschreven worden aan een stijging van het hematocriet, aangezien deze
Samenvatting
137
zich pas 2 tot 3 dagen na toediening van EPO voordoet. De bevinding dat EPO toediening na de reperfusie ook cardioprotectief is, levert een grote therapeutische window op voor de potentiële behandeling van het acute coronaire syndroom.
Post-MI Neovascularisatie en RegeneratieNaast de acute cardioprotectieve effecten door apoptose remming, beïnvloedt EPO ook de neovascularisatie na een ischemisch letsel. In een CVA-rattenmodel leidde EPO toediening, 24-uur na occlusie van de cerebrale arterie, tot een verbetering in neurologische functie en zorgde het voor een toename in de dichtheid van de cerebrale capillairen. In het hart zou neovascularisatie van het niet-geïnfarceerde hypertrofische myocard de cardiale functie kun-nen verbeteren en de post-MI LV remodeling positief kunnen beïnvloeden. In hoofdstuk 4 hebben wij de invloed van EPO op de capillarisatie van het hart onderzocht. Wij hebben eerdere resultaten bevestigd, waarin werd gezien dat EPO toediening direct na het optreden van het MI leidde tot infarctgrootte reductie, hetgeen gepaard ging met een verbeterde he-modynamische functie. Hoewel EPO behandeling vanaf 3 weken na het infarct niet leidde tot een afname van de infarctgrootte, resulteerde het wel in een verbetering van cardiale functie, aangetoond aan de hand van een toename in de drukopbouw door de linker ventrikel en een afname in de N-ANP spiegels. Deze verbeterde hartfunctie was geassocieerd met herstel van de capillaire dichtheid naar ‘sham’ niveau en met een toename van het aantal capillairen per cardiomyocyt, hetgeen neovascularisatie aantoont. Daarnaast waren deze effecten gerelateerd aan hogere percentages van de alfa-MHC (myosin-heavy chain) isovormen, een moleculaire marker voor verbeterde myocardiale contractiliteit. Alhoewel onze studie een significant effect van EPO op de capillarisatie na het MI liet zien, zijn er veel vragen overgebleven. Het hematocriet steeg met 27% bij de EPO-behandelde ratten. En, hoewel dit minder waarschijnlijk lijkt, zou de verhoogde zuurstoftransportcapaciteit van het bloed hebben kunnen bijdragen aan de verbeterde hartfunctie. Ook van belang is dat de chronisch hoge dosering van EPO in de klinische situatie zou kunnen leiden tot hypertensie, beroertes en trombose in patiënten met een al verhoogd cardiovasculair risicoprofiel. Verder blijft het mechanisme achter de neovascularisatie onbekend. Stimulatie van endotheelcellen in situ of van de proliferatie en mobilisatie van endotheelvoorlopercellen (EPCs) vanuit het beenmerg zouden beiden een rol kunnen spelen. Recentelijk werd aangetoond dat verhoogde EPC-spiegels geassocieerd zijn met een lager risico op cardiovasculaire dood bij patiënten met coronairlijden. EPO toediening bij hartpatiënten stimuleert de mobilisatie en de functionele activiteit van EPCs.Om de hematopoëtische effecten van EPO te kunnen onderscheiden van de niet-hematopoëtische effecten en het hierbij behorende mechanisme te bestuderen, hebben wij een lage en een hoge dosering van EPO met elkaar vergeleken in een post-MI hartfalen model in de rat (hoofdstuk 5). Wij hebben gekeken naar het verloop van de hartfunctie in de tijd, naar mobilisatie van EPC’s en naar neovascularisatie. Het hematocriet steeg in de groep met de hoge dosering, maar niet in die met de lage dosering. In beide EPO-behandelde groepen liet sequentiële echocardiografie een consolidatie van de hartfunctie zien tijdens de 9-weken durende follow-up, terwijl de niet-behandelde groep een duidelijke afname van de hartfunctie liet zien. Bovendien nam de hoeveelheid EPCs in beide EPO-behandelde groepen significant toe, hetgeen geassocieerd was met een toename van 42% in het aantal capillairen per cardiomyocyt in de hoge-dosering groep en van 28% in de lage-dosering groep. Deze bevindingen komen overeen met die in een studie uitgevoerd in een rattenmodel voor

Samenvatting
138
progressief nierfalen, waarin behandeling met een lage dosering EPO de nieren beschermde en het capillaire netwerk handhaafde, zonder de hematocriet te verhogen.Samenvattend: in klinische situaties waarin chronische behandeling is geïndiceerd, zoals bij hartfalen, zou gebruik van EPO in een lage dosering gunstig kunnen werken, terwijl de bijwerkingen geassocieerd met een hematocriet stijging kunnen worden vermeden.
Klinische implicatiesEPO wordt al twee decennia lang gebruikt binnen de geneeskunde. Aanvankelijk was dit met name voor de behandeling van anemie veroorzaakt door EPO-tekort bij chronisch nierfalen. De indicaties voor EPO behandeling zijn de laatste jaren echter uitgebreid en omvatten nu ook anemie bij patiënten met myelodysplastisch syndroom, bij kankerpatiënten na chemo-therapie en profylaxe om de transfusiebehoefte bij grote chirurgische ingrepen te reduceren. In de cardiologie is aangetoond dat EPO toediening bij anemische patiënten met chronisch hartfalen leidt tot een toename van de LV ejectiefractie en tot een verbetering van het in-spanningsvermogen. Alhoewel de indicaties voor EPO gebruik steeds ruimer worden, blijft het doel van de behandeling toch het ophogen van het hematocriet bij anemische patiën-ten. Echter ook de niet-hematopoëtische effecten van EPO zouden gunstig kunnen zijn bij niet-anemische patiënten met een acute ischemische episode. De eerste gerandomiseerde klinische studie in patiënten met een herseninfarct liet zien dat EPO toediening goed werd verdragen en weinig bijwerkingen bleek te hebben. Daarnaast werd aangetoond dat EPO behandeling leidde tot een kleiner infarct en uiteindelijk zorgde voor een betere cognitieve functie. Hoewel er recent een groot aantal experimentele studies zijn uitgevoerd waarin het beschermende effect van EPO in het myocard infarct wordt aangetoond, zijn er tot op he-den geen klinische data beschikbaar. Wel werd aangetoond dat hoge endogene EPO spiegels onafhankelijk gecorreleerd waren met een kleiner infarct bij patiënten met een acuut MI. In hoofdstuk 6 hebben wij een klinische pilotstudie met EPO bij MI patiënten uitgevoerd. In deze single-center onderzoekergeïnitieerde gerandomiseerde studie hebben wij de veilig-heid van de langwerkende EPO analoog darbepoëtine bestudeerd bij niet-anemische patiën-ten met een acuut ST-elevatie MI. Tweeëntwintig patiënten werden voor percutane coronaire angioplatiek gerandomiseerd naar een bolus van 300 μg darbepoëtine of geen aanvullende medicatie. Toediening van darbepoëtine was veilig en werd goed verdragen. Er werden geen “adverse events” gezien tijdens de 30 dagen durende follow-up. In plaats van dat het hemato-criet tot boven de referentiewaarden werd verhoogd, voorkwam een bolus van darbepoëtine slechts de daling van het hematocriet die in de controle groep werd gezien. Daarnaast werd 72 uur na het MI een significante stijging van het aantal EPCs gezien in de groep behandeld met darbepoëtine. Ondanks de niet-significant langere tijd tot de start van de behandeling en de grotere “area at risk” (cumulatieve ST-elevaties) in de darbepoëtine groep, was de LV functie 4 maanden na het MI in beide groepen gelijk. De resultaten van deze eerste pilot studie pleiten voor een grotere klinische studie om de effectiviteit van EPO bij patiënten met een acuut MI verder te onderzoeken.Anemie is al langere tijd bekend als risicofactor voor cardiovaculaire morbiditeit en mortaliteit bij patiënten met chronische nierinsufficiëntie en hartfalen. Onlangs bleek anemie geassocieerd met een slechtere prognose van patiënten met stabiel coronairlijden. In hoofdstuk 7 hebben wij de effecten van hemoglobine spiegels op de korte-termijn mortaliteit bij patienten met een acuut MI bestudeerd. Wij vonden een significant verhoogde 30-daagse mortaliteit in patiënten met hemoglobine spiegels onder de 6.2 mmol/l (10 g/dl). Hoewel

Samenvatting
139
andere risicofactoren (leeftijd, nierfunctie) sterker geassocieerd zijn met overleving en dus gedeeltelijk de effecten van anemie verklaren, bleef een lagere hemoglobinespiegel een onafhankelijke voorspeller van de 30-daagse mortaliteit na correctie voor deze variabelen. Specifieke therapeutische strategieën gericht op het hemoglobine-niveau, waaronder EPO behandeling, zouden verder overwogen moeten worden.
Conclusie
Alhoewel EPO traditioneel wordt beschouwd als een hematopoëtisch hormoon, wordt het ook meer en meer gezien als een pleiotroop cytokine, met andere effecten dan alleen de stimulatie van de proliferatie van rode bloedcellen (bediscussieerd in hoofdstuk 8).De detectie van de EPO receptor buiten het hematopoietisch systeem suggereerde de mogelijkheid dat er verschillende niet-hematopoëtische effecten van EPO bestaan. EPO biedt neuroprotectie tegen een beroerte en bij andere neurologische aandoeningen. Gunstige effecten van EPO tijdens ischemie werden ook in andere organen en weefsels beschreven.De recombinante vorm van EPO wordt al bijna twee decennia lang in de kliniek gebruikt om verschillende vormen van anemie te behandelen. Hoewel het gebruik van EPO in het algemeen veilig is en goed verdragen wordt, zijn er bijwerkingen bekend gerelateerd aan de verhoging van het hematocriet.Recentelijk gesynthetiseerde niet-hematopoëtische varianten van EPO, die de weefsel-beschermende activiteit behouden, zouden een effectieve en veilige optie kunnen zijn voor niet-anemische patiënten met orgaan-ischemie.EPO blijkt twee cruciale processen tijdens ischemie/reperfusie in het hart te beïnvloeden. Ten eerste door tijdens het acute stadium de apoptose te remmen en de infarctgrootte te reduceren, en ten tweede door op de langere termijn de neovascularisatie te bevorderen en de myocardiale structuur en functie te bewaren. Als deze effecten naar hartpatiënten worden geëxtrapoleerd, zou EPO bij het acute coronaire syndroom “twee vliegen in één klap” kunnen slaan.

Zhrnutie a záver
Zhrnutie
142
Zhrnutie
Súčasná liečba infarktu myokardu (IM) je zameraná na skrátenie času ischémie skorou obnovou koronárnej perfúzie (teória „otvorenej artérie“). Napriek reperfúznej terapii limitujúcej rozsah nekrózy myokardu a zlepšujúcej klinické prežívanie, morbidita a mortalita po IM stále zostáva vysoká. Aditívna ochrana buniek myokardu počas ischémie a reperfúzie môže viesť k zlepšeniu prežívania myocytov, s následným kladným účinkom na srdcovú funkciu a prognózu pacientov s akútnym IM.U veľkej časti pacientov s IM sa okrem toho rozvíja srdcové zlyhanie alebo ľavokomorová (ĽK) dysfunkcia. Päťročné prežívanie pacientov s diagnózou srdcového zlyhania je nižšie ako 50% a jednoznačne si vyžaduje stratégie zamerané na regeneráciu zlyhavajúceho myokardu.Erytropoetín (EPO) je hormón produkovaný v parenchýme obličiek, stimulujúci hemopoézu v kostnej dreni. Nedávny objav funkčného EPO receptora v ne-hemopoetických bunkách (obličiek, nervového a kardiovaskulárneho systému) naznačil možné pleiotropné účinky erytropoetínu. EPO zrejme ovplyvňuje aj širokú škálu iných procesov v organizme a medzi nimi aj ochranu proti ischemickému poškodeniu, stimuláciu angiogenézy a proliferáciu kmeňových buniek.
Akútna ochrana myokarduViaceré experimentálne štúdie preukázali protektívny účinok erytropoetínu v centrálnom nervovom systéme. Systémové liečba erytropoetínom pred alebo do šiestich hodín po indukcií fokálnej mozgovej ischémie u potkanov znižuje rozsah infarktu o 50-75%. V kapitole 2. sme skúmali prítomnosť a funkčnosť EPO-receptora v srdcovom tkanive a vyhodnotili účinok aplikácie exogenného erytropoietínu na srdcovú činnosť počas ischemicko/reperfúzneho (I/R) poškodenia. V prvej časti štúdie sme preukázali expresiu EPO-receptora v srdci potkana, kde je prítomný hlavne v endotelových bunkách a fibroblastoch a v menšej miere aj v kardiomyocytoch. Perfúzia izolovaných potkaních sŕdc (Langendorffov model) vysokými koncentráciami erytropoetínu aktivuje navyše MAP kinázu - dôležitú signálnu dráhu pre prežívanie srdcových buniek pri reperfúznom poškodení. V druhej časti štúdie – aplikácia exogénneho erytropoetínu počas I/R poškodenia preukazatelne zvýšila ľavokomorový tlak a koronárny prietok. Tento účinok bol spojený s 56% redukciou bunkového poškodenia počas reperfúzie a tiež zníženou apoptózou.Viaceré štúdie v posledných rokoch preukázali, že podávanie erytropoetínu in vivo počas kardiálneho I/R poškodenia alebo trvalej koronárnej oklúzie vedie k zmenšeniu veľkosti infarktu, čo je spojené s inhibíciou apoptózy. Akútna redukcia veľkosti infarktu a apoptózy vedie následne k prevencii dysfunkcie ĽK. Napriek týmto výsledkom, klinicky relevantná otázka šírky „terapeutického okna“ pre EPO-mediovanú ochranu myokardu počas I/R poškodenia zostala nezodpovedaná. V kapitole 3. sme sa venovali možnosti využitia „terapeutického okna“. Erytropoetín bol podávaný 2 hodiny pred začiatkom ischémie, po indukcii ischémie alebo po začatí reperfúzie. Jedna dávka EPO vo vyššie uvedných rôznych časových intervaloch viedla k 19-23% redukcii veľkosti infarktu, spojenej so zlepšenou ĽK funkciou. EPO na jednej strane významne znížil počet buniek vstupujúcich do apoptózy, na strane druhej neovplyvnil proliferačnú aktivitu myokardu. Z toho vyplýva, že účinok EPO je skôr v inhibícii programovanej bunkovej smrti spojenej s I/R poškodením ako v stimulácii proliferácie. Dôležitým faktom je, že
Zhrnutie
143
tento účinok nie je možné pričítať vzostupu hematokritu, pretože k tomu dochádza až 2-3 dni po aplikácii erytropoetínu. Predĺženie kardioprotektívneho účinku erytropoetínu až za začiatok reperfúzie poskytuje široké “terapeutické okno“ pre potenciálnu liečbu akútnych koronárnych syndrómov.
Neovaskularizácia a regenerácia myokardu po IMOkrem akútneho kardioprotektívneho účinku pomocou inhibície apoptózy, erytropoetín ovplyvňuje rast nových ciev (neovaskularizáciu) po ischemickom poškodení. Liečba erytropoetínom 24-hodín po mozgovej ischémii u potkana zlepšuje neurologickú funkciu a zvyšuje počet cerebrálnych kapilár na okraji infarktu. Neovaskularizácia neinfarktovej, hypertrofovanej časti myokardu vedie k zlepšeniu kardiálnej funkcie a zamedzeniu postinfarktovej remodelácie ĽK.V kapitole 4. sme hodnotili efekt liečby erytropoetínom na rast nových ciev pri srdcovom zlyhaní po IM. Potvrdili sme doterajšie pozorovania o redukcii veľkosti infarktu v prípade podania erytropoetínu priamo po indukcii IM, čo bolo spojené so zlepšenou hemodynamic-kou funkciou srdca. Okrem toho, liečba s EPO zahájená tri týždne po začiatku IM, napriek tomu že neovplyvnila veľkosť infarktu, viedla k zlepšeniu srdcovej činnosti, čo potvrdzuje 17% zvýšenie rozdielu ľavokomorového systolického a diastolického tlaku a 46% redukcia hladiny N-ANP. Zlepšenie bolo spojené s obnovením hustoty kapilár na normálne (predinfarktové) hodnoty a významným zvýšením indikátora neovaskularizácie- kapiláro-myocytového pomeru. Tieto pozitívne účinky boli naviac spojené s vyšším percentom obsahu izoforiem alfa-MHC (myo-sine-heavy chain), molekulového markera zvýšenej kontraktility myokardu. Aj keď spomínaná štúdia ukázala jednoznačný efekt erytropoetínu na vznik nových kapilár po IM, viacero otázok zostalo nezodpovedaných. U potkanov liečených erytropoetínom stúpol hematokrit o 27% a aj keď je to menej pravdepodobné, zvýšená transportná kapacita krvi pre kyslík mohla teoreticky prispieť k zlepšenej kardiálnej činnosti. Na druhej strane v klinickej situácii môže chronická liečba vysokými dávkami erytropoetínu spôsobovať hypertenziu, cievnu príhodu, trombózu a následnú smrť. Tieto komplikácie sú prídatným rizikom hlavne u pacientov s kardiovaskulárnym ochorením. Inou otázkou je doteraz neznámy mechanizmus erytropoetínom indukovanej neovaskularizácie. Stimulácia in situ proliferácie endotelových buniek, ako i mobilizácia endotelových progenitorových buniek (EPB) v kostnej dreni by mohli vysveliť efekt erytropoetínu. Zvýšené hodnoty cirkulujúcich EPB boli v nedávnej štúdii spojené so zníženým rizikom z kardiovaskulárnej smrti u pacientov s dokázanou ko-ronárnou chorobou. V kapitole 5. sme za účelom rozlíšenia hemopoetických a ne-hemopoetických účinkov ery-tropoetínu a odkrytia možného mechanizmu jeho pôsobenia porovnali liečbu srdcového zlyhania nízkymi a vysokými dávkami erytropoetínu u potkanov s IM. Počas štúdie sme sek-venčne merali srdcovú funkciu, mobilizáciu EPB a neovaskularizáciu. Hematokrit sa význam-ne zvýšil v skupine s vysokým dávkovaním a zostal nezmenený v skupine s nízkym dávko-vaním EPO. V oboch erytropoetínom liečených skupinách sme pomocou echokardiografie preukázali zachovanie systolickej funkcie ĽK počas 9-týždňového sledovania a invazívne hemodynamické merania potvrdili zlepšenú kontrakčnú a relaxačnú činnosť srdca na konci štúdie. Liečba erytropoetínom navyše zvýšila počet cirkulujúcich EPB, čo bolo spojené s 42% nárastom kapiláro-myocytového pomeru u EPO vysoko- a 28% u nízko-dávkovanej skupiny. Naše výsledky sú v súlade so štúdiou uskutočnenou v modeli progresívneho obličkového

Zhrnutie
144
zlyhania u potkana, kde liečba nízkymi dávkami EPO mala napriek nezvýšeniu hematokritu nefroprotektívny účinok a zachovala kapilárnu sieť v obličkách.V situáciach kde je indikovaná chronická liečba (srdcové zlyhanie), použitie nízkych dávok erytropoetínu môže byť efektívne a zároveň nespôsobovať nežiadúce účinky spojené so zvýšením hematokritu.
Klinické využitieErytropoetín je používaný v klinickej medicíne po dve desaťročia, spočiatku hlavne na liečbu anémie spôsobenej zníženou produkciou erytropoetínu pri chronickom obličkovom zlyhaní. Indikácie na liečbu erytropoetínom sa v posledných rokoch rozšírili a sú zamerané na liečbu anémie u pacientov s myelodysplastickým syndrómom, aplastickou anémiou, onkologických pacientov s anémiou po chemoterapii, ako profylaktická liečba za účelom redukcie počtu transfúzii pred rozsiahlym operačným zákrokom a v iných indikáciách.Liečba erytropoetínom v kardiológii zvyšuje ejekčnú frakciu ĽK a zlepšuje záťažovú kapacitu u anemických pacientov s chronickým srdcovým zlyhaním. Napriek rozšíreniu indikácie erytropoetínu, zostáva doteraz hlavným účelom liečby zvýšenie hematokritu u anemických pacientov. Na druhej strane práve ne-hemopoetické účinky erytropoetínu môžu byť prospešné aj u pacientov s akútnou ischemickou príhodou bez anémie. Prvá randomizovaná klinická štúdia u pacientov s náhlou cievnou mozgovou príhodou preukázala, že okrem bezpečnosti a dobrej tolerancie, liečba erytropoetínom zlepšuje klinické parametre a znižuje ischemické poškodenie mozgu.Aj keď neustále narastá počet štúdií poukazujúcich na ochrannú úlohu erytropoetínu pri experimentálnej ischémii, doteraz nie sú k dispozícií žiadne klinické výsledky. Je pozoru-hodné, že vysoké hladiny endogénneho erytropoetínu boli spojené s menšími veľkosťami infarktov u pacientov s akútnym IM. V kapitole 6. sme uskutočnili prvú pilotnú klinickú štúdiu s aplikáciou erytropoetínu u pacientov s akútnym IM. Hlavným cieľom našej randomizovanej, nezaslepenej štúdie bolo vyhodnotenie bezpečnosti a tolerancie dlhoúčinkujúceho analógu erytropoetínu-darbopo-etínu-alfa u pacientov s akútnym ST IM liečeným primárnou koronárnou angioplastikou. Dvadsaťdva pacientov bolo randomizovaných na aplikáciu 300 μg darbopoetínu alebo žiad-nu aditívnu liečbu. Podávanie darbopoetínu-alfa u pacientov bolo bezpečné a dobre tole-rované. Počas 30-dňového klinického pozorovania sme nezaznamenali žiadne nežiadúce účinky. Jeden bolus darbopoetínu nespôsobil nárast hematokritu nad referenčné hodnoty ale predišiel poklesu hematokritu pozorovanom v kontrolnej skupine. Dôležítým pozorovaním bolo významné zvýšenie počtu EPB 72-hodín po aplikácii darbopoetínu. Napriek dlhšiemu „času k liečbe“ a rozsiahlejšej ohrozenej oblasti myokardu (kumulatívna ST-elevácia) bola ĽK funkcia štyri mesiace po IM rovnaká v oboch skupinách. Výsledky tejto klinickej štúdie podporujú začatie rozsahovo väčšej štúdie za účelom zistenia efektivity podávania erytropo-etínu u pacientov s akútnym IM.U pacientov s chronickou renálnou insuficienciou a srdcovým zlyhaním je anémia známym rizikovým faktorom zvýšenej kardiovaskulárnej morbidity a mortality. V posledných prácach bol výskyt anémie spojený s horším prežívaním aj u pacientov s dokázanou ischemickou chorobou srdca.V kapitole 7. sme skúmali účinok hladiny hemoglobínu na krátkodobú mortalitu u pacientov s akútnym IM. V tejto retrospektívnej štúdii sme analyzovali 1841 po sebe nasledujúcich pacientov prijatých s diagnózou akútneho IM. Významne zvýšenú 30-dňovú mortalitu sme zaznamenali u pacientov s hodnotou hemoglobínu pod 100 g/l. Aj

Zhrnutie
145
keď ostatné rizikové faktory (vek, obličková funkcia) boli výraznejšie spojené s prežívaním pacientov a čiastočne tak môžu vysvetlovať negativny efekt anémie, nízka hladina hemog-lobínu zostala nezávislým prediktorom 30-dňovej mortality aj po korekcii pre spomínané rizikové faktory. Špecifické liečebné postupy, vrátane liečby erytropoetínom, by mohli byť v budúcnosti zvažované u anemických pacientov s akútnym IM.
Záver
Tradične vnímaný ako hemopoetický (erytropoetický) hormón, erytropoetín je stále viac pokladaný za pleiotropný cytokín, s účinkami ďaleko prekračujúcimi len stimuláciu produk-cie červených krviniek (diskutované v kapitole 8).Detekcia EPO-receptora mimo hemopoetického systému implikovala možnosť rôznych ne-hemopoetických funkcií erytropoetínu. Aplikácia erytropoetínu v centrálnom nervovom systéme poskytuje ochranu neurónov pri ischemickej príhode a iných neurologických ochoreniach. Prospešné účinky erytropoetínu počas ischemického poškodenia boli dokázané aj v rôznych iných orgánoch a tkanivách.Rekombinantná forma erytropoetínu je používana na liečbu rôznych foriem anémie v klinickej medicíne už skoro dve desaťročia. Aj keď liečba erytropoetínom je vo všeobecnosti dobre tolerovaná a bezpečná, môže byť spojená aj s nežiadúcimi účinkami spojenými hlavne so vzostupom hematokritu. V poslednom čase syntetizované ne-hemopoetické varianty erytropoetínu, ktoré si zachovávajú ochranný účinok na tkanivá, môžu byť zároveň efektívnou a bezpečnou alternatívou u neanemických pacientov s orgánovou ischémiou.V srdci ovplyvňuje erytropoetín dva kľúčové procesy počas experimentálneho IM; akútne inhibíciou apoptózy a redukciou veľkosti infarktu, a z dlhodobého hľadiska stimuláciou neovaskularizácie a uchovaním štruktúry a funkcie myokardu. Pokiaľ bude možné dané účinky extrapolovať aj na pacientov so srdcovým ochorením, liečba akútnych koronárnych syndrómov erytropoetínom by mohla „ zabiť dve muchy jednou ranou“.


147
Dankwoord
Dit wordt een lang dankwoord…Vanaf het begin van mijn tocht als mens, arts en onderzoeker ben ik heel veel mensen tegengekomen die van grote invloed zijn geweest op mij. Bij degenen die betrokken zijn geweest bij het tot stand komen van dit proefschrift wil ik een moment stilstaan.
In “order of appearance”. Ergens in april 2001 ben ik naar Groningen gekomen met een voetbalploeg van het Academisch Ziekenhuis in Bratislava. Omdat ik al toen wist dat een carrière als profvoetballer er niet in zou zitten, heb ik contact opgenomen met de internationaliseringsafdeling van de Faculteit Medische Wetenschappen om te vragen of er mogelijkheden bestonden om cardiologisch onderzoek in Groningen te doen. De allereerste die ik tegenkwam was Dr. Caesar Hulstaert. Beste Caesar, ik wil je niet alleen bedanken voor je primeur, maar ook voor je altijd persoonlijke inzet en hulp.
De tweede met wie ik in contact kwam in Groningen was prof. dr. D.J. van Veldhuisen, mijn tweede promotor. Beste Dirk-Jan, sinds onze eerste ontmoeting wist jij misschien beter dan ikzelf dat ik voor een langere tijd in Groningen zou vastzitten. Bedankt voor deze “visie”, het besmettelijke enthousiasme en de dagelijkse betrokkenheid, met name in de laatste maanden van mijn promotietraject. Ik waardeer je praktische manier van werken en je vermogen om beslissingen te nemen. Tevens wil ik je bedanken voor de mogelijkheid om me te kunnen specialiseren tot cardioloog.
“Not last but surely not least”- mijn eerste promotor- prof. dr. W.H. van Gilst. Beste Wiek, toen ik naar Groningen kwam had ik er geen idee van dat ik in het lab van de Klinische Farmacologie zou belanden. Ik herinner me de koude dag in januari 2002 toen jij me onder je hoede kreeg- een onderzoeker-rookie. En toch had jij het vertrouwen om mij op een heel nieuw project in te zetten. Al heel vroeg had ik één ding door: hoewel jij misschien niet zo vaak en nadrukkelijk aan het woord bent, is het verstandig om nauwkeurig naar je te luisteren wanneer dat wel zo is. Ik heb veel waardering voor je brede wetenschappelijke kennis, je kritische blik, en de capaciteit om de verschillende onderwerpen in perspectief te zetten. Ik beschouw je als een onderzoeker met een grote “O”.
Hoewel ik al twee co-promotors heb, hadden het er eigenlijk drie moeten zijn. Mijn directe begeleider in de beginfase was dr. Rob Henning, die mij ook het aanbod heeft gedaan om de hele promotie in Groningen af te ronden. Beste Rob, hoewel jij de tweede helft van de wedstrijd meer op de bank hebt gezeten met af en toe een goede suggestie hoe wij verder moesten, maakte jouw inzet in de eerste helft het verschil tussen overwinning en nederlaag. Bedankt daarvoor en ook voor de gezellige discussies in de “Onderwerelt” van Lunteren.
De tweede helft was onder de regie van dr. R.G. Schoemaker, mijn eerste co-promotor. Beste Regien, jij kwam precies op tijd toen wij “nieuw bloed” nodig hadden. Ik vraag me ook af of het onderwerp van de eerste studie over de timing van de EPO-effecten slechts toeval heeft kunnen zijn. Je expertise op dierexperimenteel gebied bracht een gunstige wind in onze zeilen. Bedankt voor je steun, vanaf het opzetten van de studies tot het schrijven van de manuscripten.

148
Mijn tweede co-promotor is dr. A.A.Voors. Beste Adriaan, ik ben blij dat jij ook betrokken bent geweest bij het EPO-onderzoek. Ik vond in het bijzonder onze samenwerking tussen “bench and bedside” en de snelle toepassing van experimentele resultaten in de kliniek prettig. Tevens bedankt voor je bereidheid om er altijd voor mij te zijn, betreffende het onderzoek of voor meer persoonlijke zaken.
De leden van de beoordelingscommissie, prof. dr. F. Zijlstra en prof. dr. A.J. van Zonneveld, wil ik bedanken voor de bereidheid om mijn proefschrift kritisch te beoordelen. My special thanks go to prof. dr. P. Ponikowski for his readiness to accept the membership in the reading committee and his presence during the defence of the thesis.
Samenwerking was het belangrijkste woord waarom het in “ons EPO-project” draaide. Wij hebben daadwerkelijk grenzen overschreden- van cellen naar patiënten, van experiment naar kliniek, van Klinische Farmacologie naar Cardiologie… and much more. Bij het in vivo lab van de Klinische Farmacologie hebben Alex Kluppel, Azuwerus van Buiten, Bianca Meijeringh, Lisa Wong en Maaike Goris altijd voor me klaargestaan, bedankt. Een apart woord van dank gaat naar Egbert Scholtens. Beste Egbert, jij was de eerste die met mij in het Nederlands praatte. Ik herinner me de gezelligheid van het samen experimenten doen, en van het supporten van het Slowaakse hockey-team …. misschien worden het de volgende Olympische spelen. Tevens wil ik Marry Duin, Cécile Deelman-Driessen en Kristien Boddeus bedanken voor het aanleren van en het helpen met “de blots en de PCRs”, destijds voor mij een geheel onbekende wereld. Dr. Albert Suurmeijer heeft me veel belangrijke suggesties gegeven voor de apoptose-bepalingen.
Zeker de secretaresses zijn belangrijk in deze rij. Ik ben Ardy Kuperus, Alexandra Douglas en Ellen la Bastide van de Klinische Farmacologie, en Olga Klompstra en Alma Guikema van de Cardiologie zeer dankbaar.
Hoewel EPO in de nieren wordt geproduceerd, had ik wetenschappelijk weinig met de nefrologie te maken, en daarmee ook niet met de “tweede poot” van onze afdeling onder leiding van prof. dr. Dick de Zeeuw. Beste Dick, ik zou je desalniettemin willen bedanken voor de scherpe kritiek en gezellige discussies op de refereeravonden bij jou thuis. Tevens wil ik andere mensen bij de KF bedanken voor belangrijke suggesties en leuke samenwerking: Hendrik Buikema, Leo Deelman en Richard van Dokkum. Jan van den Akker en Wessel Sloof hebben voor mij heel wat logistieke problemen opgelost. Adriaan, het squashverhaal is nog niet voorbij.
Nu de lotgenoten- de andere AIO’s en PhD studenten: Simone G., Annemarieke, Bart, Bas, Els, Maria, Bernadet, Menno, Mirjam, Willemijn, Simone V., Cheng, Ying, Rik, Jacoba, Larissa, Willeke, Peter M., Hiddo en Hisko. Jullie hebben het allemaal behoorlijk makkelijker voor me gemaakt; bedankt daarvoor. Annemarieke, jij was de senior AIO toen ik naar KF kwam en de eerste met wie ik de lange avonden op donderdag doorbracht; één van de stellingen is daaraan gekoppeld. Beste Bart, we hebben een uitdrukking in het Slowaaks- beter laat dan nooit, en dat geldt ook voor onze vriendschap, waarvan ik weet dat wij haar ondanks de afstand in stand kunnen houden. Zet hem op in Canada!! Beste Maria, ik ben er zeker van dat jouw professionele dromen vervuld zullen worden, al zal de wereld een toegewijd
149
onderzoeker verliezen; veel succes samen met Orest. Onze co-assistente Willemijn wil ik veel plezier wensen bij het kennismaken met de echte patiënten. Lieve Mirjam, wat het leven boeiend maakt is de mogelijkheid een droom te verwezenlijken, bedankt voor de lange gesprekken en grote steun die jij voor mij bent geweest, tijdens goede en slechte tijden. Sommige dingen kan je niet verwoorden, toch zou ik je veel succes met jouw legende willen wensen, om die waar te maken heb jij naar mijn inziens alles in huis.
Anton Roks was geen AIO, maar toch hoorde hij er meestal een beetje bij. Beste Anton, dank voor je openheid en bereidheid om de intregratie voor elke “allochtoon” te veraangenamen. Ook wil ik Jurjen Zandstra en Jan Verbeek bedanken, de twee studenten die met veel enthousiasme betrokken waren bij het EPO onderzoek. Jurjen, we zouden toch een keer slivovitz in Slowakije moeten proberen.
In het tweede deel van mijn promotieonderzoek ontsnapte ik steeds vaker van de KF…. naar de cardiologie en de greenhouse. Tom, Pim, Wim, Rudolf, Folkert, Martin, Michiel, Patrick, Jessica, Marcella, Meint, Tone, Christiane, Jochem, Ruud, Pieter en Kevin, allen bedankt voor de gezelligheid. Toch een kleine suggestie: misschien zou de Senseo vervangen moeten worden door een ander apparaat. Daan, jij hebt de fakkel overgenomen, veel succes ermee! De cardiologen van de UMCG ben ik dankbaar dat ik tijdens mijn onderzoek het contact met de kliniek niet helemaal heb verloren. Bovendien waren de interventiecardiologen “conditio sine qua non” bij het uitvoeren van onze klinische pilotstudie bij patiënten met een acuut myocardinfarct. Tevens wil ik de mensen bij de cardio-research bedanken voor hun inzet en hulp, met name Peter, Anja en Greetje, en ook Zaza, Trinke en Margriet. Met Gideon, Johan en het echoapparaat hebben wij vele lange avonden doorgebracht, bedankt.
Bij een promotie zijn er altijd twee mensen die in noodgeval voor de promovendus zouden mogen invallen: de twee paranimfen- Peter van der Meer en Peter Ochodnický. Het is niet alleen symbolisch dat het twee Peters zijn; een Nederlander en een Slowaak. Deze twee mensen waren voor mij in de afgelopen vier jaren de belangrijkste collega’s, vrienden, “brothers in arm”. Ik heb een tweeling broer, maar jullie twee zijn letterlijk mijn andere twee tweelingbroers geworden. Eerst Peter van der Meer, mijn EPO tweeling. Beste Peter, bedankt voor de leuke samenwerking, ontspannen sfeer, jouw suggesties en hulp, of het nu in Groningen of in Deventer was. Ik had me geen beter maatje kunnen wensen. Ik waardeer jouw kwaliteiten en inzet als arts, onderzoeker, maar met name als mens, in de volle betekenis van het woord. Milý Peter, keď som prišiel do Groningenu, myslel som si že budem na širokom okolí jediným Slovákom. Teba som stretol hneď na druhý deň a štyri roky sme zdielali jednu pracovňu na fakulte. Okrem kolegu v práci si sa stal aj mojim spolubývajúcim, ale hlavne blízkym priateľom, s ktorým som mal veľa spoločného- názorov, záujmov, športov. Veľmi si vážim Tvoju bezprostrednosť, neúnavnú schopnosť rozdávať úsmev, trefný humor, ale aj Tvoju ochotu vždy nezištne pomáhať. Som šťastný že som v Groningene našiel takého priateľa ako si Ty, prajem Tebe aj Janke veľa šťastia, ale hlavne zdravia, lebo keď je to zdravie..... to ostatné už príde samo.
Slowaken in Groningen. Napriek tomu že by to nikto neočakával, vytvorili sme docela silnú (charakterom) komunitu aj v tomto neznámom severoholandskom meste. Martin W., Tibor, Rado, Erik, Silvia, Martin G., Miki, Jarka a veľa iných, ďakujem za pohodu a ten dôležitý
150
kúsok domova, bez ktorého by to bolo oveľa ťažšie. Mirka, všetko dobré v ceste za Tvojimi snami. Rodina Černáková vniesla po rokoch potrebné oživenie do našej malej komunity, ale aj môjho každodenného života. Mirkine večere a makový koláč a sobotný tenis s Vladom sú pre mňa už teraz sentimenálnou spomienkou.
I was utmost fortunate for being able to find a lot of international friends in Groningen. Kacper, Koen, Saravanan and others, good luck with your future career and take care.
Er is nog een speciaal persoon die ik niet mag vergeten: Rineke Klijnsma, het hoofd van de internationaliseringsafdeling van het UMCG. Beste Rineke, de wereld is klein, en wij hebben elkaar na jaren weer in Groningen ontmoet. Bedankt voor de gezelligheid in jouw tuintje, de leuke gesprekken en bereidheid er altijd voor mij te zijn.
Tevens wil ik bedanken alle assistenten en specialisten in Deventer Ziekenhuis voor de manier waarop ze mij hebben ontvangen, ik verheug me op de volgende jaren en onze samenwer-king. En nu even mijn familie en vrienden in Slowakije. Vyzerá to neuveriteľne dlho, tie štyri roky čo som strávil v Holandsku, výsledkom ktorých sú predchádzajúce stránky. To všetko by ale nebolo možné bez podpory rodiny a priateľov doma na Slovensku, častých návštev, posedení prí víne, na lyžovačkách, filozovaní pri grile, v pohode a kľude. To všetko mi dodávalo nevyhnutnú energiu ísť ďalej. V prvom rade patrí moje ďakujem Petrovi Kubicovi. Milý Kubo, po mojich rodičoch si bol prvý s ktorým som sa stretol vždy po príchode na Slovensko, nikto nám už nikdy nezoberie všetko čo sme spolu zažili. Ďakujem, v mojich myšlienkach zostaneš stále prvý... Milá Aďka, všetko už bolo povedané, zostávajú nám však spomienky a priateľstvo. Veľmi obdivujem Tvoju statočnosť a silu ísť ďalej a aj keď tomu občas neveríme, nakoniec určite prídu aj kľudné a šťastnejšie chvíle. Katka a Jožko, vás dvoch ešte čoskoro oslávime, prajem vám už dopredu veľa šťastia, obaja máte všetko potrebné na to aby to bol zaručený úspech. Ďakujem, že ste si našli čas prísť do Groningenu a teším sa, že to spoločne ešte dlho spolu “potiahneme”. Danka a Mirko, moja promócia sa časovo skoro kryje s kolaudáciou vášho nového domu- prajem vám dobrý vietor do nových plachiet. A ja tajne dúfam, Danka, že nám ešte zostáva pár narodeninových osláv v Lieskovom. Jožko K., Tibor, Tomáš D., Peter K.,Tomáš S., Michal, Martin- ďakujem za spoločné strávené chvíle, mali by sme v tom pokračovať nezávisle od geografických súradníc v ktorých sa práve nachádzame. Maroš, ďakujem za pohostinnosť vo Worcestri a na všetkých AHA a ACC kongresoch, možno nastal čas aby si už aj Ty začal chodiť na európske kongresy. Rovnako ďakujem všetkým ostatným, u ktorých som mohol čerpať veľa energie počas uplynulých rokov, veselých aj ťažkých chvíľ zároveň.
Rád by som sa poďakoval aj tým ktorí stáli na začiatku moje lekárskej kariéry, za podporu a pomoc, menovite prof. Balažovjechovi, doc. Dukátovi a prof. Traubnerovi.
A na záver tí najdôležitejší. Moja najbližšia rodina- moji rodičia. Mami & otec - Edita & Tomáš, obaja ste mi dali viac ako si ktorékoľvek dieťa môže želať, obaja a každý inak, ste boli a zostávate pre mňa vzormi ktoré chcem nasledovať. Za to čo som v mojom živote dosiahol patrí z veľkej časti vďaka vám dvom. Slovíčko ďakujem nemôže ani zďaleka vyjadriť moje

151
pocity čo k vám obom cítim, dúfam že vám to aspoň čiastočne budem vedieť vrátiť. Milý Dano, som veľmi šťastný, že mám takého brata ako Ty- už skoro tridsaťtri rokov... Obdivujem čo si vo svojom veku dosiahol, som na Teba (právom) hrdý a aj keď nie vždy s Tebou budem súhlasiť, vždy Ťa budem podporovať v tom čo robíš a pokladáš za správne.
And that is the end. It was not possible to thank everyone, and yet the contribution of those not named was not less important. Through my life I keep asking myself, why I keep meeting all those special persons at all the places, and I ended up with only two feasible explanations. Either I am the lucky one that always comes across the right people at the right time, or there is an abundance of exceptional people walking around the face of the Earth, in which case it really is a „a wonderful world“…...or both are true…


153
Bibliography
Articles1. Lipšic E, Balažovjech I, Kosmálová V, Makaiová I, Dekrét J, Zanou DF. Epinephrine produ-
cing pheochromocytoma. Is the secretory pattern decisive for the clinical manifestation? J Endocrinol Invest 2004;27:691-4.
2. Van der Meer P, Voors AA, Lipšic E, van Gilst WH, van Veldhuisen DJ. Erythropoietin in cardiovascular diseases. Eur Heart J 2004;25(4):285-91.
3. Van der Meer P, Voors AA, Lipšic E, Smilde TDJ, van Gilst WH, van Veldhuisen DJ. Prog-nostic Value of Plasma Erythropoietin on mortality in Patients with Chronic Heart Fail-ure. J Am Coll Card 2004;44(1):63-7.
4. Lipšic E, van der Meer P, Henning RH, Suurmeijer AJH, Boddeus KM, van Veldhuisen DJ, van Gilst WH, Schoemaker RG. Timing of Erythropoietin Treatment for Cardioprotection in Ischemia/ Reperfusion. J Cardiovasc Pharmacol 2004;44(4):473-9.
5. Van der Meer P, Lipšic E, Henning RH, de Boer RA, Suurmeijer AJH, van Veldhuisen DJ, van Gilst WH. Erythropoietin improves left ventricular function and coronary flow in an experimental model of ischemia-reperfusion injury. Eur J Heart Fail 2004;6(7):853-9.
6. Lipšic E, van der Horst ICC, Voors AA, van der Meer P, Nijsten MWN, van Veldhuisen DJ, van Gilst WH, Zijlstra F. Hemoglobin levels and 30-day mortality in patients after myo-cardial infarction. Int J Cardiol 2005;100(2):289-92.
7. Van der Meer P, Lipšic E, van Gilst WH, van Veldhuisen DJ. Erythropoietin: From hema-topoiesis to cardioprotection. Cardiovasc Drugs Ther. 2005;19(1):7-8.
8. Van der Meer P, Lipšic E, Henning RH, Boddeus K, Voors AA, van Veldhuisen DJ, van Gilst WH, Schoemaker RG. Erythropoietin induces neovascularization and improves cardiac function in rats with heart failure after myocardial infarction. J Am Coll Card 2005;46(1):125-33.
9. Lipšic E, Asselbergs FW, van der Meer P, Tio RA, Voors AA, van Veldhuisen DJ, van Gilst WH, Zijlstra F. Anemia predicts cardiovascular events in patients with coronary artery disease. Neth Heart J 2005;13:208-12.
10. Van der Meer P, Lipšic E, Westenbrink BD, Voors AA, Schoemaker RG, Vellenga E, van Veld-huisen DJ, van Gilst WH. Serum of anemic heart failure patients inhibits proliferation of hematopoietic stem cells. Circulation 2005; 112:1743-7.
11. Lipšic E, Voors AA, van Veldhuisen DJ. Serum erythropoietin levels and infarct size. [let-ter]. J Am Coll Card 2006; 47(2):468-9.
12. Lipšic E, van der Meer P, Voors AA, Westenbrink BD, van den Heuvel AFM, de Boer HC, van Zonneveld AJ, Schoemaker RG, van Gilst WH, Zijlstra F, van Veldhuisen DJ. A sin-gle bolus of long-acting erythropoietin analogue darbepoetin in patients with an acute myocardial infarction: a randomized feasibility and safety study. Cardiovasc Drugs Ther. 2006; In press.

154
13. Van der Meer P, Lipšic E. Erythropoietin: repair of the failing heart. J Am Coll Card 2006; In press.
14. Langeveld B, Lipšic E, Roks AJM, van Gilst WH, Zijlstra F. Long-acting erythropoietin improves endothelial function after stent implantation without influencing neointima formation. Submitted.
15. Xu Y, Henning RH, Lipšic E, van Buiten A, van Gilst WH, Buikema H. Increased mesen-teric myogenic constriction inversely relates to EDHF-mediated dilation in rats with experimental chronic heart failure. Submitted.
16. Lipšic E, van der Meer P, van der Harst P, Westenbrink BD, Koster J, du Marchie Sarvaas GJ, Voors AA, van Veldhuisen DJ, Schoemaker RG, van Gilst WH. Erythropoietin
attenuates heart failure in a hematocrit independent manner. Submitted.
17. Lipšic E, Schoemaker RG, van der Meer P, Voors AA, van Veldhuisen DJ, van Gilst WH. Protective effects of erythropoietin in cardiac ischemia: from bench to bedside. Submit-ted.
Abstracts1. Lipšic E, Kosmálová V, Makaiová I, Zanou DF, Dekrét J, Balažovjech I. Epinephrine pro-
ducing pheochromocytoma. Am J of Hypert 2001;14(4/2):251A.
2. Hirnerova E, Štvrtinová V, Ambrózy E, Lipšic E, Kosmálová V, Balažovjech I. Association between hypertension and carotid atherosclerosis. J of Hypert 2001;19(Suppl 2):S268.
3. Van der Meer P, Lipšic E, de Boer RA, Henning RH, van Veldhuisen DJ, van Gilst WH. A Functional Erythropoietin Receptor in a Rat Heart is Linked to Anti- Apoptotic Effects. J Am Coll Card 2003;41(6-abstr suppl A):330A.
4. Lipšic E, van der Meer P, Suurmeijer AJH, Schoemaker RG, van Veldhuisen DJ, van Gilst WH, Henning RH. Erythropoietin protects against ischaemic damage in isolated rat he-art. Eur Heart J 2003, 24(abstr suppl):477.
5. Van der Meer P, Lipšic E, Henning RH, de Boer RA, Suurmeijer AJ, van Veldhuisen DJ, van Gilst WH. Erythropoietin protects the heart against ischemia-reperfusion injury. Circula-tion 2003;108(17,abstr suppl):888.
6. Van der Meer P, Voors AA, Lipšic E, Smilde TD, van Gilst WH, van Veldhuisen DJ. Prognos-tic value of plasma erythropoietin on mortality in patients with chronic heart failure.J Am Coll Card 2004;43(5,abstr suppl A):221A-222A.
7. Lipšic E, van der Meer P, de Boer RA, Suurmeijer AJH, van Gilst WH, van Veldhuisen DJ, Henning RH. Erythropoietin activates map kinase in isolated rat hearts. N-S Arch Pharmacol 2004;369(Suppl 1):26.
8. Lipšic E, van der Meer P, Henning RH, Suurmeijer AJH, Voors AA, van Veldhuisen DJ, van Gilst WH, Schoemaker RG. Therapeutic window for cardioprotective effect of erythro-poietin during ischemia/reperfusion inury. Eur Heart J 2004, 25(abstr suppl):233.
155
9. Asselbergs FW, van der Meer P, Tio Ra, Lipšic E, van Veldhuisen DJ, van Gilst WH, Zijlstra F. Anemia predicts cardiovascular events in patients with coronary artery disease. Eur Heart J 2004, 25(abstr suppl):498.
10. Van der Meer P, Asselbergs FW, Lipšic E, Tio RA, Voors AA, van Veldhuisen DJ, Zijlstra F, van Gilst WH. Statin use is associated with lower EPO levels in patients with coronary artery disease. Eur Heart J 2004, 25(abstr suppl):603.
11. Van der Meer P, Lipšic E, Henning RH, Boddeus K, Suurmeijer AJH, Boomsma F, Voors AA, van Veldhuisen DJ, van Gilst WH, Schoemaker RG. Erythropoietin improves car-diac function in rats with heart failure after myocardial infarction. N-S Arch Pharmacol 2005;371(Suppl 1):R7.
12. Lipšic E, van der Meer P, Henning RH, Suurmeijer AJH, van Gilst WH, van Veldhuisen DJ, Schoemaker RG. Protective effect of erythropoietin on in-vivo ischemia/reperfusion injury in the heart. N-S Arch Pharmacol 2005;371(Suppl 1):R6.
13. Van der Meer P, Lipšic E, Henning RH, Boddeus K, Voors AA, van Veldhuisen DJ, van Gilst WH, Schoemaker RG. Erythropoietin increases capillary density and improves cardiac function in rats with heart failure after myocardial infarction. J Am Coll Card 2005;45(3,ab-str suppl A):183A.
14. Van der Meer P, de la Porte PWB, Lipšic E, Lok DJ, Voors AA, van Veldhuisen DJ. Anemia in chronic heart failure: an inadequate erythropoietic response? J Am Coll Card 2005;45(3,ab-str suppl A):178A.
15. Van der Meer P, Lipšic E, Henning RH, Boddeus KM, Voors AA, van Veldhuisen DJ, van Gilst WH, Schoemaker RG. Erythropoietin attenuates the development of heart failure and stimulates neovascularisation in a rat model of post MI-heart failure. Eur Heart J 2005, 26(Suppl 1):70.
16. Van der Meer P, Lipšic E, Westenbrink BD, Vellenga E, Schoemaker RG, van Veldhuisen DJ, Voors AA, van Gilst WH. Serum of anaemic heart failure patients inhibits haematopoiesis. Eur Heart J 2005, 26(Suppl 1):276.
17. Lipšic E, van der Meer P, Henning RH, Voors AA, van Veldhuisen DJ, van Gilst WH, Scho-emaker RG. Darbepoetin treatment reduces infarct size and stimulates vascular growth after myocardial infarction. Eur Heart J 2005, 26(Suppl 1):650.
18. Lipšic E, van der Meer P, Voors AA, Westenbrink BD, van Gilst WH, Zijlstra F, van Veldhu-isen DJ. A single bolus of long-acting erythropoietin analogue darbepoetin in patients with an acute myocardial infarction: A randomized feasibility and safety study. Circulation 2005; 112 (17):483.
