unlocking constraints for better private sector …
TRANSCRIPT

PARTNERSHIPS FOR A HEALTHIER INDONESIA
UNLOCKING CONSTRAINTS FOR BETTER PRIVATE SECTOR PARTICIPATION
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

PARTNERSHIPS FOR A HEALTHIER INDONESIA
UNLOCKING CONSTRAINTS FOR BETTER PRIVATE SECTOR PARTICIPATION

ACKNOWLEDGMENTS
This document has been prepared by Vikram Rajan (Senior Health Specialist, World Bank) and Massimiliano Calì (Senior Economist, World Bank), in collaboration with Dev Terway (Health Care Consultant, World Bank Group), and with the assistance of Pui Shen Yoong (Economist, World Bank). It is a joint product of the Health, Nutrition and Population (HNP) and the Macroeconomics, Trade and Investment (MTI) Global Practices of the World Bank Group. The team would like to thank Tomio Komatsu (Senior Investment Officer, International Finance Corporation [IFC]), Jeffrey Delmon (Senior Public-Private Partnership [PPP] Specialist, World Bank), Dhawal Jhamb (Investment Officer, PPP Advisory Services, IFC), Natasha Beschorner (Senior Digital Development Specialist, World Bank), Pandu Harimurti (Senior Health Specialist, World Bank), Reem Hafez (Senior Economist, Health, World Bank), Eko Pambudi (Health Specialist, World Bank), and the Health Policy Plus private sector team for useful comments, as well as Nabil Rizky Ryandiansyah (Consultant, World Bank) for excellent research assistance. The layout design was done by Indra Irnawan.
We would also like to thank all the stakeholders in the health sector (the government, private sector providers, investor groups, consulting firms, and other development partners) who shared their valuable insights with us. The team would also like to thank Rodrigo A. Chaves (Country Director, Indonesia) and Enis Baris (Practice Manager, East Asia and Pacific, HNP) for their overall guidance. The opinions and conclusions shared in this document are the sole responsibility of the authors

CONTENTS
EXECUTIVE SUMMARY 1
section oneIntroduction 5
section twoDemand for and supply of health services and the role of the private sector 9
Growing demand for health services 10
Supply of health services has increased, but the quality is uneven 12
Private sector can help close the gaps between demand and supply 14
Private sector involvement also poses risks that call for proper oversight 15
section threeThe markets for health care providers 17
Primary health care 18
Secondary/specialist health care providers 24
Diagnostics providers 29
section fourAddressing constraints to private sector participation in health 31
The government should articulate a clear private sector engagement strategy for health 33
Revenue and expenditure reforms should address BPJS-K financial deficits 34
BPJS-K should strengthen its strategic purchasing function to improve quality of services and fill supply-side-gaps 36
Reforms in health education and in recognition of qualifications are needed to expand the quantity and quality of HRH 39
The government should ease establishment rules for hospitals to facilitate private investments, including in primary care 46
MoH and BPJS-K should strengthen their capacity to plan, design, manage, and monitor high-impact PPPs 48
The government should strengthen hospital and primary accreditation capacity to facilitate empanelment by BPJS-K 54
MoH should clarify and ease e-health regulations to foster digital health innovations 56
APPENDIXES 63

Abbreviations & Acronyms
AI Artificial Intelligence
AP Availability Payments
AR Accounts Receivable
ASEAN Association of Southeast Asian Nations
ASSRI Asociasi Rumah Sakit Swasta Indonesia or Indonesian Private Hospitals Association
BKPM Badan Koordinasi Penanaman Modal or Investment Coordinating Board
BMC Bhubaneswar Municipal Corporation
BPJS Badan Penyelenggara Jaminan Sosial (BPJS) or National Social Insurance Agency
BPJS-K Badan Penyelenggara Jaminan Sosial - Kesehatan or National Social Insurance Agency - Health
Bappenas Badan Perencanaan dan Pembangunan Nasional or Ministry for National Development Planning
BUMD Badan Usaha Milik Daerah or Provincial/Municipal-Owned Enterprises
BUMN Badan Usaha Milik Negara or State-Owned Enterprises
COB Coordination of Benefits
CSR/KTJS Social Responsibility Partnership
CT Scan Computerized Tomography Scan
DAK Dana Alokasi Khusus or Special Allocation Fund
DinKes Dinas Kesahatan or District Health Office
DJSN Dewan Jaminan Sosial Nasional or National Social Security Council
DNI Daftar Negatif Investasi or Negative Investment List
DRG Diagnosis-related Group
EMR Electronic Medical Record
FBC Full Business Case
FHP Foreign Health Professional
GDP Gross Domestic Product
GNI Gross National Income
GoI Government of Indonesia
GP General Practitioner
HHG Hermina Hospital Group
HIS Hospital Information Systems
HNP Health, Nutrition and Population
HPV Human Papillomavirus Virus
HRH Human Resources for Health
ICT Information and Communication Technology
IDI Ikatan Dokter Indonesia or Indonesian Doctors Association
IDHS Indonesia Demographic and Health Survey
IFC International Finance Corporation
IFLS Indonesia Family Life Survey
IIGF Indonesia Infrastructure Guarantee Fund
INA-CBG Indonesia Case-mix Based Groups
ISQua International Society for Quality in Health Care
IT Information Technology
JKN Jaminan Kesehatan Nasional or National Health Insurance Scheme
KAFKTP Komisi Akreditasi Fasilitas Kesehatan Tingkat Primer or Primary Care Accreditation Commission
KARS Komisi Akreditasi Rumah Sakit or Hospital Accreditation Commission
KBK Kapitasi Berbasis Komitmen or Commitment-based Capitation
KKI Konsil Kedokteran Indonesia or Indonesian Doctors’ Council

KPBU Kerjasama Pemerintah Dengan Badan Usaha or Government Cooperation with Business Entities
KSO Kerjasama Operasi or Operational Cooperation Contract
LPDP Lembaga Pengelola Dana Pendidikan or Indonesia Endowment Fund for Education
MCU Medical Checkups
MMR Maternal Mortality Rate
MoF Ministry of Finance
MoH Departemen Kesehatan or Ministry of Health
MRA Mutual Recognition Arrangements
MRI Magnetic Resonance Imaging
MTI Macroeconomics, Trade and Investment
MTKI Majelis Tenaga Kesehatan Indonesia or Indonesian Health Practitioners Assembly
NCD Noncommunicable Disease
NTT Nusa Tenggara Timur or East Nusa Tenggara
NUS National University of Singapore
OBC Outline Business Case
OECD Organisation for Economic Co-operation and Development
OOP Out-of-pocket
OTC Over-the-counter
PBI Penerima Bantuan Iuran or Public Subsidy for Insuring the Poor
PDF Project Development Facility
PERSI Perhimpunan Rumah Sakit Seluruh Indonesia or Association of All Indonesian Hospitals
PERKENI Perkumpulan Endokrinologi Indonesia or Indonesian Society of Endocrinologists
PHC Primary Health Care
PMK Peraturan Menteri Kesehatan or Minister of Health Regulation
PPP Public-Private Partnership
R&D Research and Development
RPTKA Rencana Penempatan Tenaga Kerja Asing or Foreign Worker Utilization Plan
RSCM Rumah Sakit Cipto Mangkukusumo or the Jakarta National Hospital
SIP Surat Ijin Praktek or Practice License
SUPAS Survey Penduduk Antar Sensus
TB Tuberculosis
UHC Universal Health Coverage
UI University of Indonesia
VGF Viability Gap Funding
WHO World Health Organization
vi
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation

EXECUTIVE SUMMARY
1
EXECUTIVE SUMMARY

2
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
The supply of health care services in Indonesia has grown along with the demand for health services but public sector health services expansion remains strained. The demand for health services in Indonesia collects low fiscal revenues and allocates relatively little of its budgets to health services. As a result private providers have started to step up their investments and out-of-pocket (OOP) expenditures in health remain high. According to the Investment Coordinating Board (Badan Koordinasi Penanaman Modal or BKPM), private investment in the health and human services subsector reached US$148.7 million in 2018, growing some 130 percent per year, on average, since 2014. However, Indonesia’s annual inpatient admission rates, bed-to-population ratio, and doctor-to-population ratio remain among the lowest in the region and well below World Health Organization (WHO) recommendedstandards. The quality of health services offered in Indonesia also remains low, even for wealthier Indonesians who can afford better quality care.
The private sector involvement represents an opportunity to improve the availability and quality of health services by introducing better health products and medical technologies. Increased private investments that can bring better quality of services, improve access, and introduce efficient models of service delivery are key to ensure that supply meets demand. Besides providing needed scarce capital, greater private investment could promote local innovation, technology transfer, and low-cost solutions for health services and products such as medical devices and drugs.
However, increased private sector involvement is not a panacea and also poses challenges. Regulating private sector providers can be difficult to implement without effective regulatory levers and incentives. An expansion of the private sector could even worsen or create inequities in the distribution and quality of health services. Evidence does not necessarily support the assumption that private sector delivery by itself provides better quality care more efficiently. Similarly, for public-private partnerships (PPPs), results can be mixed and effectiveness depends on government commitment and capacity to
a large extent. Nonetheless, increasing private sector involvement in the health sector potentially offers more benefits than costs. The challenge is to manage trade-offs between equity and efficiency, growth and access to health, and private and public sector participation.
The private sector is already active at varying levels across all main health service sectors in Indonesia—primary, specialty, and diagnostics. Data on utilization rates suggest that it provides close to half of outpatient health services and 30–40 percent of inpatient services in Indonesia. The private sector’s presence in the primary care market is highly fragmented and is dominated by small providers with single doctor or multiple doctor clinics. The dominant form of private providers is general practitioner (GP) clinics, which are generally small and often consist of a single person business. Through providing online access to consultations, medications, and information, the emergence of digital health providers (such as HaloDoc, YesDoc, and Alodokter) can help address the limited access to primary health services particularly to underserved populations due to geographical location or socioeconomic status.
Private investment in the secondary/specialist health care subsector has grown rapidly, given the recent opening of the sector to foreign investments and the rapid development of the National Health Insurance Scheme (Jaminan Kesehatan Nasional, JKN). Unlike primary care, private investments in this segment are dominated by hospital groups (including Siloam, Hermina, Mitra Keluarga, and Awal Bros), which own many of the specialty hospitals. In spite of recent growth, they remain relatively small by international standards confirming the growth opportunities of the sector. The diagnostics sector has a similar structure, with a few specialized groups (including Prodia, BioMedika, and Paramita) dominating the private landscape and ample room existing for increased investments in light of rapidly rising demand.
The further development of private sector participation in the sector would require addressing a number of key regulatory/policy and nonregulatory constraints. The major constraints include (a) lack of a clearly articulated

EXECUTIVE SUMMARY
3
strategy for private sector engagement by the Government of Indonesia (GoI); (b) sustained and increasing financial deficit of the social health insurance agency or Badan Penyelenggara Jaminan Sosial - Kesehatan (BPJS-K)—the largest source of demand for many private providers—which constrain the ability of private providers to plan; (c) underutilization of the BPJS-K strategic purchasing function to drive improvements in service provision and quality; (d) inadequate availability of skilled health professionals; (e) restrictive establishment rules for private sector players—foreign in particular; and (f) lack of an enabling government environment to design, manage, and monitor PPPs. The other constraints are (g) poor capacity of the hospital and primary care accreditation systems; and (h) unclear and at times overly restrictive e-health regulations.
Possible options to address each of these constraints are described below
The government should articulate a clear private sector engagement strategy for health: (a) The Ministry of Health (Departemen Kesehatan, MoH), with BPJS-K, to prepare a database of private (and public) providers using multiple information sources and (b) the MoH, with BPJS-K, and the Ministry of National Development Planning (Badan Perencanaan dan Pembangunan Nasional, Bappenas to prepare a private sector engagement strategy, with differential strategies for various subsectors, to fulfill supply-side gaps by improving access, quality, and efficiency.
Revenue and expenditure reforms should address BPJS-K financial deficits: (a) Simplify the overall tobacco tax structure and increase tobacco excise taxes at the national level, with potential earmarking to BPJS-K; (b) update JKN premiums based on actuarial analysis; (c) subsidize premiums for the informal sector to address adverse selection by attracting and retaining a larger pool of healthy members; (d) address open-ended hospital payments where most spending occurs by introducing a budget and/or volume ceiling; and (e) introduce an explicit benefit package commensurate with available resources.
BPJS-K should strengthen its strategic purchasing function to improve quality of services and fill supply-side-gaps: (a) clarify roles of the MoH and BPJS-K to strengthen the purchasing role of BPJS-K; (b) BPJS-K, with the MoH, to strengthen performance-based capitation and hospital payments to incentivize broader health sector results; (c) the MoH, with BPJS-K, to target underserved areas and populations by introducing incentives; (d) the MoH, with BPJS-K, to develop an effective referral process regulation and modify/develop the necessary information systems to make this more patient centric, transparent, and supply evidence driven; (e) BPJS-K, with the MoH, to strengthen guidelines on quality of care by introducing clinical pathways, instituting clinical audits, strengthening monitoring of quality of care, and embedding quality-based criteria for reimbursement of providers.
Reforms in health education and in recognition of qualifications are needed to expand the quantity and quality of HRH: (a) Increase the domestic production of quality health professionals by expanding the capacity of the tertiary education sector; (b) relax restrictions to the hiring of foreign health professionals (FHPs), thus enabling the system to expand the stock of qualified human resources for health (HRH); and (c) reduce requirements to convert medical qualifications of Indonesian physicians who studied abroad.
The government should ease establishment rules for hospitals to facilitate private investments, including in primary care: (a) The MoH could remove the need for a recommendation letter from the local governments for the establishment of hospitals and have a transparent set of criteria for investment, endorsed by local governments, to replace it; (b) the MoH could remove the restriction on the scope of services for foreign hospitals; and (c) the President (through the decree on Negative Investment List [Daftar Negatif Investasi, DNI] could expand foreign equity limits to 100 percent across all health services sectors.
MoH and BPJS-K should strengthen their capacity to plan, design, manage, and monitor high-impact PPPs: (a) The Ministry of Finance
4
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
(MoF) and Bappenas, with MoH and BPJS-K, to establish a cross-government coordination mechanisms (also involving Indonesia Infrastructure Guarantee Fund [IIGF] and local governments) as well as public-private platforms to identify a pipeline of ‘high-impact PPPs’ that have private sector interest; (b) the MoH, with BPJS-K, to identify clear gaps which could be fulfilled by the private sector, including PPPs, based on demand patterns (population, disease burden, and utilization of services) as well as using available data on public and private sector provision; (c) the MoH and BPJS-K, with the MoF and Bappenas, to develop capacity as well as identify clear roles and responsibilities to design and manage the PPP transaction process, manage and monitor PPPs, and evaluate PPP results.
The government should strengthen hospital and primary accreditation capacity to facilitate empanelment by BPJS-K: The MoH and the Primary Care Accreditation Commission (Komisi Akreditasi Fasilitas Kesehatan Tingkat Primer, KAFKTP), to expand capacity (for facilitation and accreditation) and the latter to become fully independent of the MoH (both financially and institutionally) and (b) the Hospital Accreditation Commission (Komisi Akreditasi Rumah Sakit, KARS), to expand its capacity to cover the increased demand for hospital accreditation services.
MoH should clarify and ease e-health regulations to foster digital health innovations: (a) The MoH and BPJS-K should develop data privacy standards as well as pass the necessary legislation in consultation with stakeholders; (b) the MoH and BPJS-K should develop protocols for sharing data with privacy protections and consider using digital health providers for data analytics and service delivery; (c) the MoH, with BPJS-K, could develop legislation that focuses on e-prescriptions to improve access to prescribed medications, while maintaining necessary safeguards; (d) the MoH could lift restrictions on foreign telemedicine providers, specifically in pathology and radiology; and (e) the GoI to focus on the upgrading of mobile infrastructure in remote regions to improve access to 3G and the use of smartphones.
5section 1 .
Introduction

6
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Indonesians have become healthier in recent decades as confirmed by the progress on key health indicators. Over 1960–2016, average life expectancy increased from 45 to 69 years.1 Under-five mortality declined nearly tenfold to 25 per 1,000 live births, while infant mortality declined sixfold to 21 per 1,000 live births over the same period. The share of pregnant women receiving four or more antenatal care visits has also increased, from 55 percent in 1991 to 77 percent in 2017.2 Importantly, Indonesia has charted remarkable progress on its path towards universal health coverage (UHC). With the introduction of National Health Insurance Scheme (Jaminan Kesehatan Nasional, JKN) in 2014, health insurance coverage rates have increased significantly from 27 percent in 2004 to around 80 percent in 2018.3
Despite these advancements, significant challenges remain in improving maternal health and nutrition and in tackling persistent communicable diseases. Indonesia’s maternal mortality ratio remains high relative to its income level at 126 per 100,000 live births in 2015 (from 446 in 1990).4 This means that one Indonesian mother dies in childbirth every 1.4 hours on average. In addition, a third of children under five years or 9 million children suffer from stunting in 2018,5 the fifth highest prevalence in the world. Finally, Indonesia is now the second largest contributor to the global tuberculosis (TB) burden, with over 1 million cases reported in 2017 (WHO and MoH Indonesia 2018). New challenges such as multidrug-resistant TB have also emerged.
As the Indonesian population grows older, new challenges are emerging. Noncommunicable diseases (NCDs) already account for the largest share of the disease burden (66 percent),6 nearly doubling since 1990. NCDs are likely to rise further as the share of the population ages 65 years and above doubles to 10 percent between 2015 and 2030. Moreover, unhealthy lifestyle choices contribute to the prevalence of NCDs. Indonesia has one of the highest rates of cigarette consumption in the world: about half the adult population (about 85 million people) smoke, including 68 percent of adult males. Tobacco is an important risk factor in the top five leading causes of death in Indonesia, which are stroke, ischemic heart disease, diabetes, TB, and cirrhosis.7
Regional and income-related inequalities in health outcomes persist. National averages obscure wide disparities in health outcomes between urban and rural areas, the rich and poor, and East and West Indonesia. In 2012, the under-five mortality in the Eastern Indonesian provinces of East Nusa Tenggara (Nusa Tenggara Timur, NTT) and Maluku was close to 60 per 1,000 live births, much higher than the (then) national average of 40 per 1,000.8 In addition to large regional disparities, income-related inequalities9 remain across the country. Although the gap in health outcomes between the richest and poorest households has decreased over the last two decades, under-five and infant mortality rates are still more than double among poorer households.10
1 World Bank World Development Indicators; latest data available on April 1, 2019.2 Refers to the share of women ages 15–49 years who attended antenatal care visits once each in the first and second trimesters
and twice in the third trimester. Source: Indonesia Demographic and Health Survey (IDHS) 2017.3 Susenas household survey, various years, and estimation from online Badan Penyelenggara Jaminan Sosial - Kesehatan (BPJS-K)
database (health facilities).4 Based on World Health Organization (WHO)-United Nations Children’s Fund-World Bank estimates 2017. Census data indicate
that the maternal mortality rate (MMR) may be even higher; the official MMR used by the Government of Indonesia (GoI) is 305 per 100,000 live births, Survey Penduduk Antar Sensus (SUPAS) 2015.
5 MoH Riset Kesehatan Dasar (Riskesdas) survey, 2018.6 Institute of Health Metrics and Evaluation 2017.7 Ibid.8 IDHS 2012 is used to compare between regional and national estimates as this is not yet available for IDHS 2017. 9 The consumption Gini Index, a measure of income inequality, grew from 30 (2003) to 40 (2016).10 World Bank staff calculations from IDHS 2017.

7
The private sector can play an important role in driving better health outcomes for all Indonesians. In many developing countries where public resources are limited, the private sector could help ensure that the supply of health care services meets the demand. Indonesia is no exception, particularly at a time when growing incomes and demographic and epidemiological transitions increase the demand for health services and public sector providers are already strained. The private sector could also introduce efficiency and innovations through technology. Examples include digital health, telemedicine, low-margin high-volume specialty care, and innovations in diagnostics and radiology.
There has been increased utilization of outpatient and inpatient private sector health services by all Indonesians, including the poor (bottom 40 percent of the population in terms of wealth, Table 1). Also, with the introduction of JKN in 2014, utilization rates have almost doubled on average for inpatient care and for the poor, including in private sector facilities. While outpatient utilization rates have increased only marginally, even post JKN, private sector utilization constitutes between one-half and almost two-thirds of total outpatient utilization.

8
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Tabel 1 Inpatient and outpatient utilization rates for private and all facilities
Function 2011 2012 2013 2014 2015 2016 2017 2018
Outpatient utilization (all)
National 13.4 12.9 13.5 14.4 17.0 16.1 13.3 15.1
Bottom (40%) 12.2 11.8 12.3 13.2 16.0 15.1 12.2 14.3
Outpatient utilization (private)
National 8.4 8.5 9.1 9.8 10.8 10.1 8.5 9.1
Bottom (40%) 6.7 6.8 7.4 8.1 8.9 8.3 6.8 7.5
Inpatient utilization (all)
National 2.1 1.9 2.3 2.5 3.6 3.7 4.2 4.7
Bottom (40%) 1.4 1.3 1.6 1.7 2.6 2.7 3.1 3.6
Inpatient utilization (private)
National 1.0 0.8 1.1 1.2 1.7 1.7 2.0 2.2
Bottom (40%) 0.5 0.4 0.6 0.6 0.9 0.9 1.1 1.3
Source Susenas
Of course, increased private sector involvement is not a panacea. An expansion of the private sector could even worsen or create inequities in the distribution and quality of health services (Chanda 2002) by creaming off the top consumers and human resources in the system. In addition, a rapid expansion of the private sector in the health sector may generate the challenges of ensuring quality of care in a system with limited oversight capacity. The challenge is to manage trade-offs between equity and efficiency, growth and access to health, and private and public sector participation.
Considering these trade-offs, this report investigates the opportunities and constraints to more and better private sector participation in the Indonesian health services sector. It focuses on three key segments of the health care market—primary care (including digital health), secondary/specialist health, and diagnostics,11 drawing from interviews with existing private providers as well as recent secondary evidence to illustrate challenges faced on the ground. This report also benefits from discussions with policy makers from various government agencies on issues related to the report but not necessarily done only for the report. The report identifies some of these constraints and proposes possible recommendations to address them. While the list of factors and corresponding recommendations are not necessarily exhaustive, it does highlight key priority areas to be considered. The report concludes with some options for reforms that could help unleash the potential of the private sector to contribute towards a healthier, happier, and more productive Indonesia.
11 Given the large scope of private sector health delivery, the report focuses on three subsectors that were most service delivery oriented. Hence, this excludes other important subsectors such as pharmaceuticals and medical technology, which could be covered as part of additional analytical work.

9section 2 .
Demand for and supply of health services and the role of the private sector

10
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Out-of-pocket (OOP) expenditures on health are high in Indonesia compared to developed countries. In 2016, public health spending made up nearly half (45 percent) of total health spending in Indonesia but this was followed by private or OOP expenditures, which accounted for about 35 percent.12 Social health insurance accounted for about 17 percent and development aid accounted for the rest. The share of OOP spending has decreased in recent years and is on par with other lower-middle-income countries, but it remains nearly triple the average level in developed countries.13 The high OOP share is in part due to low public health expenditures and the fact that public facilities lack trained staff, diagnostic capacity, and medicines, driving patients to pay out of pocket for better quality services.
The demand for privately funded health services in Indonesia is likely to rise further as several trends persist.
Continued expansion of the middle class, especially in urban areas. The growth of the Indonesian economy, along with the increase in the share of the population living in urban areas, has facilitated the emergence of a large middle class14 that requires more and better health services. The middle class expanded at 10 percent per year between 2002 and 2016 and now represents a fifth of the population (World Bank, 2019). Growing affluence, along with limitations in public service delivery, is increasing the demand for private health services, especially in urban areas. In 2018, half of the households classified as middle class and 62 percent of the upper class used private hospitals for inpatient treatment,
compared with about one-fifth of Indonesians who are poor or vulnerable to poverty (Figure 1). Similarly, the middle and upper classes are more likely to go to a hospital for childbirth instead of the local health center or clinic and they are more likely to be attended by a doctor rather than a midwife or nurse. As economic growth and urbanization continue to boost the expansion of the middle class, demand for better quality health services—at least as perceived by the patient15 —will continue to grow.
Growing demand for health services
12 MoH National Health Accounts, 2016.13 According to WHO/World development Indicators data, OOP makes up only 13 percent of total current health expenditures in
high-income countries. The average for lower-middle-income countries excluding Indonesia is 40 percent. 14 Defined as those who have less than a 10 percent chance of being poor or vulnerable in the future, given their current consumption15 Patients may be able to perceive better services using proxies on how good the services are, but they may not be able to make a
judgment on whether they received the appropriate treatment or not.
Figure 1 Middle- and upper-class Indonesians are more likely to use private health services
(Choice of health care by consumption class, percent of households)
Source World Bank staff calculations using Susenas 2018..
Public hospital Puskesmas Private hospital Others
Vulnerable
24
Aspiringmiddle class
34
Middleclass
53
Upperclass
62
Poor
19

11
Demographic and epidemiological shifts. Demographic, epidemiological, and financing transitions will further increase the demand for health services. The rising burden of NCDs, in addition to existing communicable diseases and perinatal conditions, will increase the demand for health services, especially as the needs move toward continuous, chronic care rather than just acute, episodic care. Demand could also increase due to more frequent visits to facilities, longer treatment periods, and more specialized care at the primary and referral levels, as well as due to complications that arise from the lack of early diagnosis and effective treatment.
Expansion of health insurance. In 2014, Indonesia introduced JKN and committed to achieving UHC by 2019. As of April 1, 2019, nearly 220 million Indonesians or about 82 percent of the total population were covered by the scheme,16 making it the largest single payer social health insurance scheme in world. JKN provides a generous benefit package covering all medically necessary treatment with no caps or co-payments. It is separated into two categories: BPJS-K (for nonemployees, self-employed, or informal workers) and BPJS Ketenagakerjaan (for employees of public and
private companies, who are required to make contributions to BPJS-K). While the premium for the poor is completely covered through a public subsidy, Public Subsidy for Insuring the Poor (Penerima Bantuan Iuran, PBI), the remaining population pays for the premium through payroll or voluntary contributions (for informal sector nonpoor).
With the introduction of JKN, Indonesia’s private hospitals have seen a significant increase in the total number of patients seeking treatment. While most rural Indonesians only have access to a puskesmas (public primary health centers) as a means of primary care, populations in urban or semi-urban areas can also access several private sector providers for primary care, and if required, can be referred to specialist treatment by either public or private providers that are empaneled by BPJS-K. As a result, inpatient and to some extent outpatient utilization rates have increased since 2014, especially among the bottom 40 percent (Figure 2). Major hospital groups such as Siloam, Mitra Keluarga, and Hermina have long-term expansion plans for hospitals in second-tier cities, where increasing incomes and enrolment in private insurance have increased the demand for private providers.
16 Source: BPJS-K online dashboard. Accessed April 12, 2019. https://faskes.BPJS-K-kesehatan.go.id/aplicares/#/app/peta
Figure 2 Inpatient and outpatient utilization rates have increased after JKN introduction (2014)
Source World Bank staff calculations from Susenas.
0%
2%
4%
6%
8%
16%
National
Outpatient utilization (all)
2011 2013 2018
14%
12%
10%
Bottom (40%) National
Inpatient utilization (all)
Bottom (40%)

12
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
17 Indonesia spends US$49 per capita on health, well below the recommended US$110 per capita needed to deliver an essential package of UHC (according to the Disease Control Priorities initiative, DCP3). In share of GDP terms, total current health spending in Indonesia is among the lowest in the world at 3.3 percent of GDP.
As the demand for health services has risen, so has the overall supply of health care services, but public services are underfunded. Total per capita spending on health care has steadily increased in Indonesia, growing by 14 percent per year between 2000 and 2015.17 Nonetheless, public expenditure on health only amounts to 1.4 percent of gross domestic product (GDP)—almost half of what other lower-middle-income countries spend. This is in part due to the fact that Indonesia
Supply of health services has increased, but the quality is uneven
does not collect sufficient revenues for a country of its size and income level, constraining the overall envelope available for public spending (at 14.7 percent of GDP in 2017, Indonesia has one of the lowest revenue-to-GDP ratios in the world). However, this is also due to a relatively low allocation of public expenditures to health. Even the Dominican Republic, with a similar revenue-to-GDP ratio and GDP per capita, spent twice the amount on health as a share of GDP (Figure 3).
Figure 3 Indonesia spends less on health compared to countries with similar per capita income
(Y-axis: General Government health expenditures as a share of GDP, X-axis: log GDP per capita in 2011 purchasing power parity terms)
Source World Bank staff calculations from World Development Indicators.Note Data on GDP per capita for 2017; data on general government health expenditure from 2015.
Dominican Republic
Indonesia
Malaysia
Thailand
Vietnam
-2
0
2
4
6
8
10
6 7 8 9 10 11 12

13
As the expansion in public services is unable to meet the demand for health care, private providers have started to step up their investments. According to the Investment Coordinating Board (BKPM), private investment in the health and human services subsector reached US$148.7 million in 2018, growing some 130 percent per year on average since 2014 (Figure 4). Most of the increase is due to growth in domestic investment, which still accounts for the bulk of private investment in the health sector, but foreign investment has also charted remarkable growth, increasing by 73 percent per year over the same period to US$43 million in 2018. There is clearly still scope for increased private sector participation, as domestic and foreign investments in health accounted for only 0.45 and 0.15 percent, respectively, of total investments.
Notwithstanding the increase in the public and private supply of health care services, pockets of the Indonesian population remain underserved. Indonesia’s annual inpatient admission rate remains one of the lowest in the region and despite recent increases the bed-to-population ratio remains low at 1.16 per 1,000 people—more than half the WHO-recommended standard of 2.5 beds per 1,000 people. Furthermore, the national average
masks the maldistribution of beds across the country, as the ratio ranges from 0.68 in West Nusa Tenggara to 2.24 in Jakarta.18 Many Indonesians, especially in eastern provinces, still face significant physical and time barriers in accessing health care (World Bank 2016), resulting in high morbidity and mortality rates and the inefficient use of potentially productive time by patients as well as of accompanying family members and friends (Schoeps et al. 2011).
The perceived quality of health services offered in Indonesia also leaves much to be desired, especially for wealthier Indonesians who can afford better quality care. In 2015, it was estimated that 600,000 Indonesians sought medical tests and treatment abroad, spending US$1.4 billion,19 mostly in Malaysia, followed by Singapore and Thailand. When indirect spending is included, it is estimated that Indonesia is losing some US$4 billion a year due to outbound medical tourism (Lim et al. 2018). However, while Indonesian patients with the financial means can seek medical treatment abroad, the domestic market—particularly for those that fall just below the affordability line of foreign medical treatment—remains the prime targets for the top domestic hospitals.
Figure 4 Investment in health has increased significantly, especially since reducing some restrictions in 2016
Source BKPM, World Bank staff calculations.
18 MoH Profil Kesehatan 2017.19 https://www.liputan6.com/bisnis/read/2455394/berobat-ke-luar-negeri-orang-ri-habiskan-rp-182-triliun
0,0
20,0
40,0
60,0
80,0
100,0
120,0
2012 2013 2014 2015 2016 2017 2018
Domestic investment in health in USD mn Foreign investment in health, USD mn
14
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
The unmet demand for health services in Indonesia represents an opportunity for the private sector. Globally, the private sector plays an important role in health financing and health service delivery. This is especially the case in lower-middle-income countries such as Indonesia where limited fiscal space and competing development priorities constrain the amount of public resources that can be channeled toward addressing public health needs. Private providers can also help improve access to health care services by lower-income populations, especially if they are linked to social health insurance schemes. Indeed, analysis by World Bank (2010) shows that the rise in private physicians in Indonesia has been associated with greater utilization of health services by the poor, through a reduction in the congestion in clinics.
Private sector can help close the gaps between demand and supply
The private sector also plays a critical role in improving the availability and quality of health products and the development of medical technologies. The private sector plays a critical role in research and development (R&D) and manufacturing of medicines, commodities, and medical devices, spending over US$135 billion a year on pharmaceutical R&D. In emerging markets such as Indonesia, greater private investment could promote local innovation, technology transfer, and low-cost solutions to improve the availability of medical devices and drugs. Again, the private sector also has a role to play in diminishing inequities: in Tanzania, for example, AirTel Tanzania sends free text messages about infant care to mothers and pregnant women, helping reduce infant mortality by 64 percent and maternal mortality by 55 percent (West 2015). Advancements in telemedicine can also help develop the quality of human resources for health (HRH), for example, through remote diagnosis and training.

15
This is not to say that greater involvement of the private sector automatically improves the overall quality of care or efficiency. Evidence does not necessarily support the assumption that private sector delivery by itself provides better quality care more efficiently. While the private sector performs better on drug supply, timeliness, and patient hospitality, some reviews point to poor quality of care and worse patient outcomes and efficiency than in the public sector—partly because of the perverse incentives for unnecessary testing and treatment that are provided by fee-for-service systems (Basu et al. 2012; Berendes et al. 2011; Herrera et al. 2014; Patouillard et al. 2007). This may also be reflective of the enormous heterogeneity of providers in the private sector.
In Indonesia, a study on primary health care (PHC) supply-side readiness indicated that publicly funded puskesmas were in fact more prepared to provide both general and specific PHC services compared to private general practitioner (GP) clinics. The general service readiness—an index20 of tracer indicators that measures supply-side readiness as a key prerequisite for improved quality of care21 —for public primary health facilities was 78 percent while private health facilities was 61 percent (Rajan et al. 2018). Put differently, to assess the facilities’ readiness for provision of general health care services, this report analyzed the availability of about 34 components—including basic amenities, equipment, diagnostics, and essential medicines.
Private sector involvement also poses risks that call for proper oversight
On average, the puskesmas had 26 components available compared to private GP clinics that had only 20 components. There are significant gaps in the readiness of private sector clinics to serve patients: for example, only 35 percent of all private primary health facilities had facilities for basic diagnostics compared to 66 percent of puskesmas.22 Among private sector facilities, those empaneled for BPJS-K tend to be more supply-side ready than those that were not. For all the specific clinical and outreach services, such as for child health, immunization, and communicable diseases, the puskesmas were better prepared than the private clinics to offer services.
Without the necessary regulation, private sector health care expansion may lead to distortions in service provision, including the distribution, quality, and price of health services. These distortions arise from the failures usually associated with health care markets due to the underlying information and power asymmetry between providers and patients associated with many health care interventions (Doherty and McIntyre 2013). Hence, normal market mechanisms that provide incentives for profit making can threaten broader health policy objectives such as the achievement of equitable, efficient, and sustainable health systems (Afifi, Busse, and Harding 2003). In the context of an expanding private health sector, it is important that regulatory frameworks are established to ensure that these potential market failures are
20 Service readiness is measured by a set of tracer indicators across five domains: basic amenities, basic equipment, standard precautions for infection prevention, diagnostic capacity, and essential medicines.
21 The results of this study should not, therefore, be interpreted as a study on quality of care outcomes at the public and private sector PHC facilities in Indonesia but as a measure of supply-side readiness as a necessary, but not sufficient, prerequisite to improve quality of care.
22 Part of the reason for the low level of capital equipment of private primary care clinics is their low profitability which typically does not suffice for capital investments beyond the basic level.

16
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
mitigated and private health markets contribute to achievement of health policy goals. Regulatory frameworks clarify policy objectives, establish instruments for regulation (such as legislation or voluntary incentives), set up regulatory structures, ensure dialogue between the members of regulatory networks, and monitor the effectiveness of regulation (Afifi, Busse, and Harding 2003).
Regulating private sector providers can be more difficult and expensive than public sector providers (Wadge et al. 2017). It is important to note that the impact of private sector participation in health can also differ by subsector, depending on the barriers to entry. There is a strong case for private sector involvement in outpatient services, for instance, because it is easier to establish criteria for licensing and regulating service provision, making them more contractible and open to
competition. Pharmacies and laboratory services are also easy to regulate, so they also see high levels of private provision. On the other hand, it is more difficult to monitor services provided by informal health providers or unauthorized drug retailers operating in more remote areas. It is estimated that in many low-income and lower-middle-income countries about 28.5 percent of medicines can be counterfeit or substandard (Almuzaini, Choonara, and Sammons 2013).
The private sector does offer some advantages over the public sector and can be a policy option, if the distortions arising due to the health market failures are mitigated (Doherty and McIntyre 2013). Hence, increasing private sector involvement in the health sector needs carefully designed and well-implemented policies and regulations to ensure that the potential benefits outweigh the costs.
Tabel 2 Potential benefits and costs of increased private sector participation in the health sector
POTENTIAL BENEFITS POTENTIAL COSTS
Reduce the patients’ burden of public sector structures Reduce the quality of and accessibility to health services for the poor
Expand the range and quality of health services Internal brain drain (poaching of the private sector from the public sector)
Help retaining health professionals Reduce support for quality public health services
Facilitate positive spillovers to public sector (for example, via exchanges of ideas, knowledge, imitation effects)
Deteriorate quality of training due to private sector-led expansion
Use of private sector to reach public sector objectives (for example, public-private partnership [PPP])
Upgrade and expand the health services infrastructures
Expand health training facilities
Facilitate expansion of health insurance
Source Cali and Stern 2009

17section 3 .
The Markets for Health Care Providers

18
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
The primary care market is highly fragmented in Indonesia, consisting mostly of puskesmas or publicly funded community health care centers and private GP clinics. There are roughly 9,909 puskesmas across the archipelago.23 Although there are no reliable statistics on the number of private primary care providers, there are at least an estimated 10,000 private GP clinics that have been approved by BPJS-K. Since the introduction of BPJS-K, the number of GPs has seen a significant increase in their patient numbers, and they have been instrumental in relieving some of the demand from puskesmas and public hospitals.
Each puskesmas covers a large catchment area, and their growth has not kept pace with demand growth, thus opening further opportunities for private sector participation. Each puskesmas meets the needs of close to 30,000 people, mostly catering for outpatient services although about a third of them also provides inpatient care. The supply of public PHC facilities grew at 0.4 percent per year from 2013 to 2017, suggesting that the government’s focus has been to expand secondary and tertiary care facilities rather than primary care facilities. This creates further investment opportunities for the private sector whose growth presents challenges as well.
While health care groups have developed some chains of primary clinics, the private sector remains dominated by single-practice GP clinics. Some hospital groups have invested in primary care clinic chains, such as Mayapada Clinics, Siloam Clinics, and Brawijaya Clinics. These clinics are located mostly in Jakarta and Bali and serve as outpatient service providers or
Primary Health Care
as referral centers to their hospitals for patients covered by private insurance and OOP payers. However, the absence of clear economies of scale and the importance of patients’ relation with the GP—as opposed to the brand of the clinic—have largely kept the private sector highly dispersed. GP clinics represent the highest number of private primary care facilities across the country, with many being individual or group GP clinics that provide outpatient services.
While there are no specific data on the cost structures of these private primary care clinics, the fact that supply-side readiness in these clinics is lower than that of puskesmas may indicate that this is a lower-margin business that may need specific investments and incentives from the public sector to improve quality and performance. In terms of broader health system efficiency, this would be beneficial as early diagnosis and treatment at the primary care level (primary and secondary prevention) would be much less expensive than treating complications of undiagnosed and untreated diseases at the hospital level,24 justifying public financing. In addition, most OOP expenditures to purchase services at the private clinics are inefficient by themselves.
The Ministry of Health (Departemen Kesehatan, MoH) and the Indonesian Doctors Association (Ikatan Doktor Indonesia, IDI) allow for the issuance of three practice licenses (Surat Ijin Praktek, SIPs) to both GPs and specialist doctors. The implementation of this is strict for GPs where they can utilize their SIPs at a private or public hospital, a clinic, and a private practice. GPs are
23 As of end-2017. Source: MoH, Profil Kesehatan 2017.24 Diagnosis and treatment of hypertension to control blood pressure versus treatment of complications like cardiovascular disease
or stroke.

19not required to utilize all three licenses. However, many doctors work at one hospital in the morning hours, one in the afternoon/evening hours, and at a private practice (usually at their home). The regulations require that a doctor obtain an SIP from the local district Department of Health (Dinas Kesehatan, DinKes) where they practice.
The market is dominated by domestic investors, as foreign investors are essentially not allowed to invest in the PHC sector under current regulations. The latest Negative Investment List (Daftar Negatif Investasi, DNI) (Presidential Regulation No. 44/2016) reserves virtually all of the PHC services to domestic investors.25 Foreign investors are instead allowed to invest in outpatient polyclinics but are required to provide specialist doctor outpatient services (such as dental clinics and rehabilitation services). However, specialist doctors in Indonesia typically prefer to work at hospitals where they can provide higher-value inpatient services, or at their own private practice for outpatient services; hence, foreign specialized outpatient polyclinics are rare.
The role of JKN in (re-)shaping PHC
The JKN scheme is increasingly responsible for the growing demand for PHC, with BPJS-K now covering all public clinics and around half of the private ones. BPJS-K patients can receive treatment under BPJS-K coverage across the country in all of the 9,909 puskesmas and in approximately half of the 10,000 private clinics and pratama clinics (primary care outpatient clinics). There are also an estimated 2,100 private hospitals, 1,200 dentists, and 1,050 opticians that cater to BPJS-K patients.26 On the other hand, private hospitals and clinics are not authorized to receive BPJS-K patients for GPs, so a majority of patients that receive primary care at hospitals come from private insurance, employee benefits, and OOP payers. GPs that are certified to receive BPJS-K patients at their private practice now benefit from increased patient flow, particularly in areas that are underserved by hospitals and clinics.
25 These restrictions apply to Indonesia Standard Industrial Classification or Klasifikasi Baku Lapangan Usaha Indonesia (KBLI) 86103, 86104, and 86109.
26 https://www.thejakartapost.com/academia/2018/04/06/qa-BPJS-K-kesehatan-health-for-all-indonesians.html.

20
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
BPJS-K pays PHC clinics through a capitation scheme based on registered patients, which should incentivize prevention. The base rates were calculated using the capitation structure applicable under the Jaminan Kesehatan Masyarakat (Jamkesmas)—the social health insurance scheme for the poor and near-poor that was wrapped into JKN in 2014 (Britton, Koseki, and Dutta 2018). The capitation rates for private facilities were then adjusted to account for higher cost structures in the private sector. The maximum capitation amount for private sector facilities is IDR 10,000 per member per month versus IDR 6,000 per member per month for a puskesmas. Primary clinics are paid a set amount per month per member assigned to their clinics, regardless of whether they have provided any service to that member. Thus, in theory, this payment arrangement should incentivize providers to focus on preventive care. Some disease-specific services such as family planning are reimbursed separately (non-kapitasi).
The JKN has helped consolidate the role of primary care clinics as the first point of call for all nonemergency illnesses thus enhancing the use of their services. Unless they are in emergencies or labor and delivery, BPJS-K patients are required to access primary clinics which become the gatekeepers of the health system. While puskesmas typically have basic diagnostic equipment (blood glucose, cholesterol, and uric acid tests), that is not always the case in private facilities. The latter often cannot afford the capital costs associated with such equipment and cannot ensure the volumes needed to make these investments profitable. If specialist care is necessary, the primary care clinic must refer the patient to either Class C or D hospitals. These hospitals then become the gatekeepers for further specialized care, where the providers from these hospitals must refer the patient up to Class A or B hospitals should the patient want or need care at that highly specialized level.
BPJS-K empanelment appears to greatly enhance the patients’ flow to private health care centers in areas interviewed. Interviews conducted for this study in Bali suggest that a number of GPs have opened BPJS-K-empaneled certified clinics and have seen a significant increase in the number of patients they treat (up to 50 percent) since they were BPJS-K empaneled. However, this varies across the country and a majority of the population is still enrolled by puskesmas to receive capitation compared to the population enrolled by private sector clinics. This increased demand for basic health services is also encouraging GPs to establish home-based clinics to treat additional patients outside of working hours, an option that requires the use of multiple SIPs (up to three) that doctors can avail in Indonesia. At the same time, private insurance and OOP expenditures are still an important source of demand for many private GP clinics, particularly in more affluent urban areas, where the need to empanel with BPJS-K is less stringent among private facilities.
The availability of health centers is disparate across regions reflecting different population densities and relative market size. In particular, primary health centers are concentrated in areas with higher population and incomes, including Java-Bali. However, given the high populations in these areas, the number of centers per 1,000 is lower than in more sparsely populated regions in eastern Indonesia (Figure 5). At the same time, the sparse population implies that there are many villages in more remote regions without any health centers (Figure 6).
27 According to the WHO, ‘digital health’ or e-Health is defined as the cost-effective and secure use of information and communication technologies (ICTs) for health- and health-related fields. It also includes mobile health (m-Health), which involves the provision of health services and information through mobile technologies.

Figure 5 Number of health centers per 1,000 people
Source Podes Survey 2018.
Figure 6 Share of villages without health centers
Source Podes Survey 2018.
< 0,1
0,1 - 0,18
0,18 - 0,27
0,27 - 0,41
> 0,41
< 20%
20 - 40%
40 - 60%
60 - 80%
> 80%
21

22
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Digital health providers
The scarce availability of primary health infrastructure makes it difficult for individuals to access the health systems, particularly in the less-affluent parts of the country; the emergence of digital health providers may eventually help relieve that constraint.27 A number of companies are starting to provide digital health services in Indonesia acting as a first point of contact with health professionals. For example, HaloDoc provides online consultations, helps set up doctors’ appointment, and provides last-mile delivery of over-the-counter (OTC) medicines from pharmacies or hospitals to the patient. The latter service could also help alleviate logistical difficulties that pharmaceutical companies and retail pharmacies face with inventory management, expiration of medications, and distribution costs of medicines to remote regions. Similarly, AloDokter is an online platform which provides medical-related content in Indonesia encouraging preventive care and helping people gauge the need for a medical checkup (MCU).
Besides the promise for the people with limited physical access, the digital health sector is currently growing on the back of technology-savvy urban populations in Indonesia. The great penetration and use of mobile broadband devices in Indonesia—even relative to countries at similar level of income (Figure 7)—has helped create a large base of customers for digital services, including health services. This base is particularly concentrated in urban areas where a more tech-savvy population is reducing transaction costs by exploiting the benefits of digital connectivity.28 Most of the emerging digital health services are provided through mobile platforms, which make them particularly suitable to Indonesia’s pattern of online usage, although the relatively slow download speed in the country can make it challenging to use video-based services (for
example, video call with health professionals and educational videos).
HaloDoc and AloDokter are the two key domestic players in the Indonesian digital health market, providing online access to consultations, medicine, and information. HaloDoc was incorporated in 2016 with the aim to ease the end-to-end experience for patients, by providing online appointments, consultations, diagnostic referrals, and medicine delivery through the ride hailing app GoJek, delivering medicine as quickly as within one hour from the order. HaloDoc has also partnered with private insurance groups to provide services to those covered by employee benefits.29 AloDokter is Indonesia’s leading health content portal (similar to WebMD in the United States) providing good-quality, relevant health information for patients in Bahasa Indonesia. The platform has eventually started to also provide direct chat facilities with doctors, as well as artificial intelligence (AI) bot-assisted question and answer sessions where patients can inquire about specific conditions and treatment options. According to AloDokter, they have over 20 million unique monthly users and 1 million patients using the chat platform to interact with doctors on the platform.
While the uptake of appointments, medicine delivery, and online content consultation has seen growth, mobile consultations with doctors have remained slow, as this requires patient behavioral change. Younger patients typically call a doctor through a platform for a general illness but will opt to see a specialist in person. This pattern is consistent with that on many global digital health platforms. An exception has been pediatric consultations, which have experienced significant growth through the HaloDoc platform, as many first-time parents prefer the peace of mind of speaking to a doctor when their child is ill. Dermatologists also have seen an increase in mobile consultations, as many of the diagnoses can be made over the phone and often require only OTC medicines.
27 According to the WHO, ‘digital health’ or e-Health is defined as the cost-effective and secure use of information and communication technologies (ICTs) for health- and health-related fields. It also includes mobile health (m-Health), which involves the provision of health services and information through mobile technologies.
28 Data collected by the leading digital health providers in Indonesia suggest that users under 30 years of age are increasingly using their mobile phones to find health information online.
29 The potential prospects of this business model in Indonesia have been confirmed by two significant rounds of funding, which have secured HaloDoc a total of US$76 million in 2017–2019.

23Other digital providers are also emerging providing appointment and telemedicine services. YesDok is a digital health service launched in 2017 that focuses on providing mobile consultations 24 hours a day. Other providers such as DokterSehat and KlikDokter are health content providers that also have chat and appointment services for physicians and diagnostics. Foreign providers such as Practo (India) and RingMD (Singapore) are seeking to provide telemedicine services direct to Indonesian patients with doctors abroad. Lifetrack Medical Systems provides tele-radiology for hospitals and diagnostic chains. The shortage of radiologists in Indonesia means that hospital groups or diagnostic providers could potentially utilize excess radiology capacity in markets such as India and the Philippines to increase the efficiency of operations in the Indonesian market.
While, to date, the ability of a patient to receive digital health services is limited to written or verbal interactions, the rapid technological advances may enable the sector to vastly expand its services. In particular, the increase
in wearables and other mobile medical devices could eventually improve a doctor’s ability to remotely monitor patients’ overall health and to provide tailored guidance for both medication and overall wellness. In addition, the progress in AI may enable digital companies to provide tailored advice to individuals on the basis of information such as symptoms and patients’ history. Besides health care provision, opportunities exist for digital health providers to create technology solutions for accessibility, coordination of benefits, and integration of hospital information systems (HISs) to mobile devices.
Digital platforms could also be utilized by BPJS-K to provide preventive health information. A key focus for future cost savings of BPJS-K is on preventive health and providing access to health care information to the public. Given the development of a wide range of health-related content, digital platforms are well positioned to provide the infrastructure for BPJS-K to provide targeted information campaigns to both health care workers and the general public.
Figure 7 Indonesia has a relatively high penetration of mobile broadband
Source ITU 2017 and World Development Indicators
Indonesia
Low Income
High IncomeMiddle Income
50
100
150
200
6 7 8 9 10 11 12
Log GNI per capita (current US$)
World
OECD
ASEAN
Indonesia

24
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Market landscape
Private investment in the secondary/specialist health care subsector has grown rapidly. The number of private hospitals has grown by 9.2 percent per year over 2014–2017—a much faster rate compared to the growth in the number of public hospitals, which increased by 1.3 percent per year over the same period.30 As of end-2017, about 60 percent of all 2,198 hospitals in the country were privately owned.31 By contrast, the number of hospitals owned by the MoH and state-owned enterprises (Badan Usaha Milik Negara, BUMN) has decreased substantially over the past two decades.
Secondary/specialist Health Care Providers
About a fifth of Indonesia’s hospitals are specialist hospitals. The specialist hospital market in Indonesia mostly consists of stand-alone hospitals that are either family-owned or have a few small investors that make up the ownership structure. The larger, conglomerate-owned hospital groups such as Siloam Hospitals (Lippo Group) or Mitra Keluarga (Kalbe Farma) maintain majority ownership, with foreign or domestic investors in the minority. Hermina Hospital Group (HHG) is the largest mid-market private chain that provides practicing doctors with ‘sweat equity’32 in the hospital where they operate, allowing for rapid expansion in second- and third-tier cities. These three hospital groups—Siloam, Hermina and Mitra Keluarga—are the
30 World Bank staff calculations using data from the MoH (Profil Kesehatan 2017). Latest data available as of April 12, 2019.31 MoH, Profil Kesehatan 2017.32 Sweat equity shares means equity shares that are issued by a company to its directors or employees at a discount or for
consideration, other than cash, for providing their know-how or services. The consensus among practicing doctors is that the equity model can be attractive in recruiting high-profile specialists in second- and third-tier cities.
2000 2017
Subnationalgovernment
357
Private550
Army/police111
State-owned enterprise/other department
68
Ministry of Health59
Ministry of Health14
Subnationalgovernment
672
Army/police164
State-owned enterprise/other department
14
Private1334
Figure 8 Total number of hospitals by ownership
Source MoH, World Bank staff calculations.

25Figure 9 Breakdown of Indonesian private hospitals, by class (2011–2017)
Source Britton, Koseki, and Dutta (2018).
major players in the industry, with Siloam leading in terms of number of hospitals and revenues (around US$50 million), but the other two groups are in close proximity.
Many private hospitals have been built (or have been planned) following the implementation of JKN, with the intent to capture the increased demand for specialist services.33 Two of Indonesia’s leading private hospital groups—Siloam and Hermina—have opened 20 branded hospitals since 2016, with another 20 hospitals in the pipeline by the end of 2020.34 Most of Siloam’s hospitals have been acquisitions or management buy-outs of existing hospitals, whereas Hermina has mostly built greenfield hospitals, focusing on Type ‘C’ hospitals to receive BPJS-K referrals. Indeed, most general hospitals in Indonesia are of Type C or D, which only offer basic services.35 Foreign operators from Malaysia, India, and Singapore have also invested in private hospital
groups. Malaysia’s Creador, for example, has a minority stake in Hermina.
The number of lower-level hospitals, which are gatekeepers to higher-level specialist care, has grown faster than the higher-level ones, a possible result of the BPJS-K referral system. As mentioned previously, BPJS-K requires patients to access services first through the primary care level and be referred up to Class C and D hospitals should the need arise. If further specialist care is required, these hospitals will further refer up to Class A and B hospitals. Stakeholders note that since Class C hospitals are at a higher level than Class D and get higher reimbursement rates, but can still accept referrals directly from primary care, more facilities are upgrading to Class C hospitals. As such, the proportion of Class C and Class D hospitals has grown quite rapidly in the last years (Figure 9).
33 Britton, Koseki, and Dutta 2018.34 This is based on information collected through interviews with the companies.35 MoH Regulation No. 340/2010 classifies all general hospitals according to the services provided, with A being the most
advanced and D being the most basic. Type A provides, at a minimum, four basic specialist services, five medical support specialist services, twelve other specialist services, and thirteen subspecialist services. Type B provides, at a minimum, four basic specialist services, four medical support specialist services, eight other specialist services, and two subspecialist services. Type C provides, at a minimum, four basic specialist services and four medical support specialist services. Type D provides, at a minimum, two basic specialist services.
44%46% 46% 47% 51% 52% 53%
0
20
40
60
80
100
81%67%
2011 2012 2013 2014 2015 2016 2017
A B C D

26
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Key players
Since many large (200-bed plus) private hospital groups are owned by conglomerates, the need for foreign capital has remained limited to minority foreign equity stakes (as detailed below). A majority of foreign investment has flowed into hospitals, specialized health care groups, or start-up health care technology ventures. The large domestic players such as Lippo Group (Siloam Hospitals) and Kalbe Farma (Mitra Keluarga) have been rapidly expanding their hospitals as complementary businesses to their dominant real estate and pharmaceutical business, respectively. HHG and Awal Bros Hospitals are involved only in health care services and have taken on foreign and domestic private equity funding, respectively.
Siloam Hospitals is majority owned by the Lippo Group, with a 15 percent minority stake held by CVC Capital Partners. Siloam maintains the
largest hospital and clinic network in Indonesia, with 34 hospitals and approximately 6,000 beds.36 Eleven of its hospitals are located in the Greater Jakarta area, with the remainder across Java-Bali, Sumatra, Kalimantan, Sulawesi, and Nusa Tenggara. Siloam’s current focus is on acquiring existing hospitals in smaller cities and bringing them under Siloam management. It plans to have up to 40 hospitals and 30 outpatient clinics by 2020, primarily focused on the middle- and upper-middle-class segment. Siloam accepts BPJS-K patients at 24 out of its 34 hospitals. Moreover, hospitals in smaller cities accept BPJS-K referrals from provincial public hospitals.
HHG has traditionally focused on the middle-income segment and has an operating model where doctors are shareholders in their operating hospital. Hermina currently operates 30 hospitals with approximately 3,000 beds and has the largest coverage of hospitals across Indonesia of any private group. This doctor-owner model has allowed Hermina to rapidly expand in second-tier
36 Siloam Prospectus, 2019.
Tabel 3 Major hospital groups in Indonesia, 2018
Company Hospital name Number of hospitals
Number of hospitals serving BPJS-K
New hospitals planned in 2019
Siloam International Hospitals Siloam 34 24 7
HHG Hermina 30 30 4
Mitra Keluarga Karyasehat Mitra Keluarga 20 12 2
Awal Bros Awal Bros 12 n.a. n.a.
Source Company websites and press clippings. Information valid as at end-2018.
Tabel 4 Financial performance of market-listed hospital groups, end-2018
Assets Liabilities Equity Sales P/E ratio D/E ratio ROA ROE NPM
Mitra Keluarga 4,976 718 4,258 2,033 35.31 0.17 13.89 16.23 34.01
Hermina 3,950 1,566 2,384 2,288 51.78 0.66 5.47 9.06 9.44
Siloam 7,701 1,390 6,312 4,396 1,463.03 0.22 0.17 0.2 0.29
Source Indonesia Stock Exchange, Statistics 2018.Note P/E = Price to earnings; D/E = Debt to equity; ROA = Return on assets; ROE = Return on equity; NPM = Net profit margin.

27
cities with specialist practitioners as shareholders. All Hermina hospitals accept BPJS-K patients, with some of the hospitals having up to 50 percent of patients coming through BPJS-K referrals. Hermina plans to open 40 hospitals by 2020 and has started entering into hospital management agreements as it has done in Provita Jayapura Hospital (Papua). Hermina’s focus is to expand Class C hospitals through greenfield or managed service agreements. As a pure health care operator, Hermina is in a good position to develop PPPs in the form of joint ventures, particularly for the diagnostics sector and Centers of Excellence due to its doctor shareholder model, which allows for greater incentives to specialist doctors.
Mitra Keluarga has 13 hospitals mostly in the Greater Jakarta area, with approximately 2,200 beds. Its greatest advantage is the fact that it is part of Kalbe Farma (the parent company) and
its distribution and logistics platform, which allows for efficient distribution of pharmacies and consumables throughout Mitra Keluarga’s hospital chain. This has allowed the group to become the hospital of choice for private middle-income customers in the Greater Jakarta area. Kalbe Farma’s vast doctor network has also become a convenient recruiting ground for doctors across Indonesia. The group is now planning an acquisition and greenfield expansion of hospitals in second- and third-tier cities focused on BPJS-K customers. Backed by Kalbe Farma, Mitra Keluarga has the capital and human resources to develop PPPs, particularly in the area of diagnostics and specialty centers. As one of the largest pharmaceutical producers (both branded and generic), Kalbe Farma has a strong relationship with the government as a major pharmaceutical provider to BPJS-K.

28
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
The role of JKN and private hospitals
The initial uptake of BPJS-K patients by private hospitals was limited upon its rollout in 2014, as many providers initially feared that basic services would be overrun by BPJS-K patients. Private hospital groups were reluctant to take on a government body such as BPJS-K as a client. Those that did take on clients did view this cooperation between BPJS-K and private hospitals as a PPP. One medical director said there was a moral obligation on part of private health care providers to offset the sudden increase in demand of medical services that was overburdening the public health care system. In addition, the national socialization program for the public was not well coordinated, and there was a lack of understanding on the types of services covered by BPJS-K.
However, the uptake of BPJS-K services increased significantly in 2015–2016, particularly with lower-income patients, once the BPJS-K outreach program informed the public that their health care costs were now covered if patients go through the referral system. With incremental growth in private health insurance coverage, as well as an increase in health insurance provided through employee benefits, many of the hospitals serving the middle-income segment are seeing an overall increase in the number of patients utilizing BPJS-K where possible, and then topping
off with their employee benefits where required. Siloam and Hermina indicated that it was in their interest to accommodate BPJS-K patients and provide patients with the same level of service to their privately insured or OOP patients, as they would be paying customers in the future. One leading hospital group indicated that for four of its hospitals in the Greater Jakarta area, some 40–50 percent of the patients were using BPJS-K.
Today, private hospitals are required to have BPJS-K patients referred for specialist services at their facilities either through puskesmas or government hospitals. The determination of which hospital receives which patient for specialized care is determined by BPJS-K based on geography and the availability of the specialized services at the respective private hospitals. Private hospital groups that have a broader geographic footprint are in a better position to take advantage of BPJS-K patients, many of whom access health care in second- or third-tier cities. Since the coordination of health insurance benefits of BPJS-K and private insurance remains complicated at the hospital level (and reimbursement for the patient), many patients have opted to pay OOP once they reach the threshold of their BPJS-K coverage.

29
Market landscape
The diagnostics market in Indonesia works on a referral model, primarily due to the capital-intensive business model that requires high volumes of tests to break even. In Indonesia, most diagnostics providers work on the Operational Cooperation Contract (Kerjasama Operasi, KSO) model, where a provider leases diagnostic equipment and negotiates an annual fee (paid monthly) based on the total number of tests it conducts. This model is popular with pathology providers, as it provides time for a provider to build patient footfall into their laboratories. A few key players in the markets dominate with over 80 percent of pathology tests between them, with the leading diagnostics providers being Prodia, BioMedika, and Paramita. Almost all operate hub-and-spoke models where they utilize sample collection centers within an urban area and a central lab where all samples are delivered to be tested.
Diagnostics providers
Hospitals can achieve high patient volumes and can compete with diagnostic centers that generally service hospitals without full diagnostics, primary clinics, and doctors that are allowed to refer higher-parameter tests to centers that can provide it. The pathology model in Indonesia has also encouraged doctors to refer tests to specialist diagnostic centers in exchange for a flat fee to the referring doctor, a percentage of the value of the referred lab test, or a flat fee for a certain number of referrals within a given period. Hospitals have had little control over their doctor’s referring tests outside of the hospital diagnostic facilities, as, in the past, they could not compete on pricing with stand-alone diagnostic centers because they lacked the volume of tests. Hospitals had generally accepted this practice, so as not to upset a supplemental line of income for doctors. However, in many cases, hospitals were unable to provide the required pathology tests in- house because they could not justify the investment to compete with the likes of Prodia.

30
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Key players
Prodia has 150 diagnostic and sample collection centers across Indonesia, making it the dominant player in the pathology market (estimated to control two-thirds of the private market). It also employs the largest number of pathologists and conducts the largest number of high-parameter pathology tests in Indonesia. It has cooperated with BPJS-K to provide free Human Papillomavirus (HPV) tests for qualified patients and is one of the few labs to do so in Indonesia. It is in the strongest position to develop PPPs with its geographic reach, referral partner hospitals, and total number of tests conducted annually.
BioMedika has 15 clinics across Jakarta and Bali and a referral network in the Greater Jakarta area for both pathology and radiology services. It has stated that it would be interested in looking at PPPs along with private investors. The group has experienced growth in preventive lab tests as more middle- and upper-income patients take greater control over their health care decisions.
Paramita is one of the market leaders in MCU for employee benefits alongside Prodia. It provides routine tests for employee benefits, BUMN employees, private patients, and insured patients. Its network is in areas with high numbers of industrial or agricultural employees. It is efficient at operating at high volumes and low margins per test. This places it in a favorable position to work with BPJS-K patients.
While the private diagnostic market is currently not so well developed, compared, for instance, to India and Malaysia, it is one of the most interesting perspective investments for the private sector. Health care groups in India, the Philippines, and Malaysia, and two private equity funds contacted for this report, have expressed interest in developing joint ventures with Indonesian providers to address capacity issues, with a starting point in diagnostics. Currently, a digital diagnosis performed by a foreign doctor abroad is not valid for a diagnosis and will have to be signed off by an Indonesian doctor for treatment. Since diagnostics achieve efficiency with higher volumes, foreign investors
have indicated interest in partnering with groups that are BPJS-K partners. A joint venture, as described by a foreign private equity director, would potentially involve developing greenfield diagnostic centers that could serve both privately insured and BPJS-K patients. Another method would be to inject capital for upgrading pathology and radiology services in existing centers to ensure the ability to provide higher-value tests referred by BPJS-K. At present, only routine laboratory tests and x-rays/magnetic resonance imagings (MRIs) are covered by BPJS-K at public hospitals and clinics, and if additional higher-value tests are required, the coverage is on a case-by-case basis, with many patients required to pay out of pocket.
Radiology and advanced pathology equipment are expensive, and many single private hospital operators remain reluctant to invest in expensive MRIs. However, some hospitals that experience higher volumes and demand—including BPJS-K patients—have begun to see the benefits of investing in higher-value equipment with higher utility rates of the equipment. Private equity investors have also expressed confidence that once there is a coordination of benefits (COB) mechanism between BPJS-K and private insurance, it will allow for patients to be covered for higher-value tests through employee benefits or private insurance.

31section 4 .
Addressing Constraints to Private Sector Participation in Health

32
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
While the private sector is already an integral part of health service provision, a number of factors still constrain greater and better private participation in each of the three segments of the sector considered. This section identifies some of these factors on the basis of field interviews gathered for this report as well as recent secondary evidence. For each of these constraints it then proposes possible recommendations to address them. While the list of factors and corresponding recommendations is not necessarily exhaustive, it does highlight key priority areas which should be considered.
The list of constraints includes (a) lack of a clearly articulated strategy for private sector engagement by the GoI; (b) sustained and increasing financial deficit of the public insurance scheme BPJS-K—the largest source of demand for many private providers—which constrain the ability of private providers to plan; (c) underutilization of the BPJS-K strategic purchasing function to drive improvements in service quality; (d) inadequate availability of skilled health professionals; (e) restrictive establishment rules for private sector players—foreign in particular; (f) lack of an enabling government environment to design, manage, and monitor PPPs; (g) poor capacity of the hospital and primary care accreditation systems; and (h) unclear and at times overly restrictive e-health regulations.
Addressing these constraints would require the GoI to engage the private sector effectively while also ensuring that its regulatory role is not captured. The private sector should be an important partner in designing and delivering the reforms addressing the constraints. This partnership can be facilitated through the various organizations through which the private sector is organized, such as IDI, the Association of All Indonesian Hospitals (Perhimpunan Rumah Sakit Seluruh Indonesia, PERSI), and the Indonesian Private Hospitals Association (Asosiasi Rumah Sakit Swasta Indonesia, ASSRI). These associations can be valuable sources of inputs and cooperation for the GoI (see Annex 2 for more details on these associations). At the same time, they also represent the providers of health services, so their needs have to be always set in the context of the benefits for the users of the health system

33
There has been increased utilization of outpatient and inpatient private sector health services by all Indonesians, including by the poor, which has increased even further (for inpatient services) after the introduction of JKN in 2014. The BPJS-K, which already contracts with about 10,000 private primary care facilities and 1,500 private hospitals and specialized clinics, is the key lever through which the government engages with the private health sector for UHC. In addition, the MoH and the local governments are responsible for the licensing of health facilities. The GoI had introduced hospital-level accreditation for both the public and private sectors in 1995 and the Hospital Accreditation Commission (Komisi Akreditasi Rumah Sakit, KARS) has been independent since 2011. Based on the two decades of experience in hospital accreditation, a Primary Care Accreditation Commission (Komisi Akreditasi Fasilitas Kesehatan Tingkat Primer, KAFKTP)was established in 2016 with a vision to expand capacity, become fully independent, cover both the public and private sectors, and eventually get accredited by ISQua.37
However, despite increased private sector utilization, and different levers of engagement already being implemented, there is a lack of a clearly articulated strategy for private sector engagement in health, led by the MoH. To begin with, there are no available data to the extent of private sector provision, the services they provide, and their supply-side readiness, despite having some of these data with BPJS-K, licensing authorities, and the KARS. Such data could help with identifying key gaps on the supply side in terms of quality and access, which could then be used by the MoH and BPJS-K to plan for
The government should articulate a clear private sector engagement strategy for health
incentives to fulfill such gaps through differential reimbursement rates by BPJS-K or by planning a pipeline of high-impact PPPs. For example, the current health PPP pipelines are limited to the expansion of infrastructure in a few hospitals. For the private sector, this could be available as a public good to plan expansion of their services and match it to clearly identified needs.
Recommendations1. The MoH, with BPJS-K, should prepare a
database of private (and public) providers using multiple information sources, including supply-side readiness of these facilities in terms of services provided, human resources, infrastructure, and equipment.
2. The MoH, with BPJS-K, and the Ministry of National Development Planning, (Badan Perencanaan dan Pembangunan Nasional, Bappenas), should prepare a private sector engagement strategy to fulfill supply-side gaps by improving access, quality, and efficiency, including putting in place a cross-government coordination platform to identify and resolve various private sector constraints in health. While preparing this strategy, it would be necessary to have differentiated options for each subsector, given the differences in their market structures.
37 International Society for Quality in Health Care—an accreditor of accreditation agencies
34
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
BPJS-K has been facing an increasing financial deficit since its inception, which is expected to grow further, if unaddressed. In 2017, BPJS-K recorded a deficit of IDR 8.6 trillion that has increased to IDR 19.3 trillion in 2018. Out of that, only 10.3 trillion is covered by the government, leaving BPJS-K with IDR 9.1 trillion of unresolved deficit. Throughout the first four months of this year, BPJS-K’s deficit has continued unabated, reaching IDR 3.7 trillion.
A number of structural design features of the JKN contribute to BPJS-K’s financial deficit. To start with, JKN’s generous open-ended benefits package includes only a few exceptions as part of a negative list (Tandon et. al. 2016), and some actuarial estimates (Hidayat, et al. 2015) indicate that the program is under resourced for the generous benefits package it offers. In addition, short activation periods for new or returning members and poor contribution compliance, especially with the informal sector nonpoor, further encourages adverse selection. Members from this segment are incentivized to only sign up when sick and stop paying once treatment has been received. Currently, it also has no co-payments or global caps on hospital expenditures, which is where the bulk of the expenditures (around 80 percent) occur. Finally, the incentives to strengthen primary care are still weak, leading to ineffective ‘gate-keeping’ and referral. In 2016, the GoI implemented Commitment-based Capitation (Kapitasi Berbasis Komitmen, KBK)—a capitation payment to primary health facilities that is linked to agreed performance indicators.38
Revenue and expenditure reforms should address BPJS-K financial deficits
At the same time, 95 percent of puskesmas meet all targets and receive the full capitation amount, which raises questions on the effectiveness of the KBK scheme to incentivize performance.
While some hospital providers may benefit in the short run, any medium-term planning to deepen services, expand geographical reach, improve quality, or introduce innovations is affected due to the uncertainty caused due to the fiscal deficit. Three out of the four largest hospital groups and two of Indonesia’s leading diagnostic chains reported this as a key issue that affects their investment plan. Hence, addressing BPJS-K deficit sustainably is not only necessary for Indonesia to achieve UHC, but it would also provide a more stable ecosystem to crowd in private sector investment.
Recommendations
The GoI (the Ministry of Finance [MoF], Bappenas, National Social Security Council [Dewan Jaminan Sosial Nasional, DJSN], BPJS-K, and MoH) could implement a ‘package of reforms’ on the revenue and expenditure side to make BPJS-K financially viable. The World Bank’s Public Expenditure Review39 for the MoF identifies such a package in detail, which is summarized as follows:
On the revenue side
1. Simplify the overall tobacco tax structure and increase tobacco excise taxes at the
38 Currently, there are only three ‘performance-based’ indicators: contact rate (150 contacts per 1,000 people per month); referral rate for services that could have been treated at puskesmas based on an agreed set of services (below 5 percent); and rate of visit of chronic disease patients (at least 50 percent of those enrolled to PROLANIS—at-risk chronic disease tagged patients—program visit regularly).
39 World Bank 2019.

35
On the expenditure side
1. Address open-ended hospital payments41 where most spending occurs by introducing a budget and/or volume ceiling. Options could include introducing global budgeting,42 base-rate-adjusted Diagnosis-related Groups (DRGs) payments,43 or spending caps.
2. Introduce an explicit benefit package44 commensurate with available resources. A transparent process as well as the use of an evidence-based approach through the use of JKN claims data and economic evaluations could help prioritize more cost-effective interventions. In addition, moving from a negative to a positive list could further help rationalize spending.
3. Strengthen the purchasing role of BPJS-K as discussed under constraint 4.3 in the following subsection.
national level, with potential earmarking to BPJS-K. A simulation suggests that an increase of tobacco tax by 12 percent will increase cigarette prices by an average of 5 percent, cut demand for cigarettes by nearly 2 percent, and raise government revenue by 6.4 percent (approximately IDR 11 trillion) with minimal impact on employment in the tobacco industry.40
2. Update JKN premiums based on actuarial analysis. Using actual claims data will allow for premiums to be set more accurately to reflect expanding coverage and growing utilization patterns.
3. Subsidize premiums for the informal sector to address adverse selection by attracting and retaining a larger pool of healthy members. This would drive down the cost per member per month among this subgroup, bring in additional resources to BPJS-K.
40 Araujo et al. (2018) shows that an increase in excise tax by 12 percent will result in increased cigarette prices in Indonesia by an average of 5 percent, lowered demand for cigarettes by 1.9 percent, and higher excise tax revenue by 6.41 percent, and an annual revenue gain of IDR 10.9 trillion. Under this scenario, the average excise tax burden on cigarettes would be just 49 percent of the retail price, still below the 57 percent legal limit and well below the 70 percent WHO recommendation.
41 While hospitals are reimbursed based on the Indonesia Case-based Grouping, there is no ceiling to the amount a hospital can claim.
42 Global budgeting is a fixed payment for all services and for the entire enrolled (or eligible) population for a given period.43 In base-rate-adjusted Indonesia case-mix based groups (INA-CBG), the payment is made up of a base rate multiplied by the
case group weight; if the volume goes up too much, the base rate is reduced to keep total hospital expenditure within the BPJS-K projected budget.
44 Moving to a positive list of services covered.

36
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Even though BPJS-K is the largest single purchaser of health services, its role has been more of a passive purchaser, making payments to providers and carrying out other administrative functions. This is in contrast with what BPJS-K should be doing as a strategic purchaser of health services that make it possible to create provider incentives for more effective and efficient service delivery, such as improving access, increasing quality of care, and reducing costs of services. This is in part due to the limited authority it has to do so, as most of the strategic purchasing functions (for example, deciding the benefit package, determining provider payment arrangements, and setting reimbursement rates) are housed within the MoH, although the original 2004 social security law allocated most of the key purchasing functions to BPJS-K.45
BPJS-K should strengthen its strategic purchasing function to improve quality of services and fill supply-side-gaps
An analysis of the supply side shows that improvements in service delivery after the introduction of JKN have been mixed. While there has been an overall improvement in service readiness between 2011 and 2016, the 2011 service readiness census of public sector health facilities,46 as well as the 2016 Quantitative Service Delivery Survey, revealed that not even one puskesmas met all the tracer service readiness indicators (Rajan et al. 2018). The main areas that still need improvement include availability of privacy for patients, health care waste management, availability of all basic equipment, drugs and diagnostic kits stock-outs, availability of clinical guidelines, and staff training. Private sector clinics lag puskesmas in terms of service readiness. There is significant variation across Indonesia with districts in eastern Indonesia being
45 Overview of Strategic Purchasing Functions Under JKN. 2018. Jakarta. World Bank46 The readiness to provide basic services was measured by a set of 38 tracer indicators that were collected as part of the 2011
Health Facility Census (Rifaskes) across five domains: basic amenities, basic equipment, standard precautions for infection prevention, diagnostic capacity, and essential medicines
Tabel 5 Responsibilities of JKN de jure and de facto
By Law By Regulation In practice
Premium settingPresident with inputs from MOF, BPJS-K, DJSN, and MOH
President with inputs from MOF, BPJS-K, DJSN, and MOH
President with inputs from MOF, BPJS-K, DJSN, and MOH
Determine the benefit package Unspecified MOH MOH
Develop provider payment systems BPJS-K BPJS-K/MOH MOH*
Set payment rates BPJS-K BPJS-K/MOH MOH
Contract with providers BPJS-K BPJS-K BPJS-K/MOH
Monitor quality BPJS-K BPJS-K/MOH BPJS-K/MOH
Source World Bank analysis 2018.

37
into account that puskesmas also receive other financing sources. This could help improve the overall system efficiency and quality of care.
Due to the acute shortage of specialized doctors across the market, if a doctor is well regarded and has a strong reputation in the market, he/she does not require referrals from external parties, BPJS-K included. There is also no obligation within private hospital groups that a reputable doctor is required to treat BPJS-K-referred patients. Since many upper- and middle-class patients pay for services out of pocket, the doctors themselves are generally not affected by delays in payments through or claims processing through the hospital system. For other providers though, the decision-making process for sending a patient with a specific medical case to a hospital remains opaque to the providers. One of Indonesia’s largest private hospital groups, HHG, explained that BPJS-K had informed them that there is a quota system for patient referrals to private hospitals, which takes into account the availability of the specialist doctor (or subspecialist) service, the geographic location of the hospital in relation to the patient, and the track record of the hospital in providing the required specialist treatment. The criteria under which a selected patient is sent to a specific hospital remains opaque to medical directors; however, they indicated that many of the patients that are referred by BPJS-K, particularly in the Greater Jakarta area, are sent based on geographic proximity to the respective hospital. The opaque nature of the referrals process, however, raises the possibility for rent-seeking by referees to send patients to specific hospitals. There is a regulation that gives some guidance on the current referral process, that is, for puskesmas or private clinics to refer patients to hospitals from a Class D to A, in a sequential manner. The logic of this is primarily from a cost-saving perspective, namely to let patients needing lower levels of care to attend lower levels of facilities. However, it is not entirely clear how this actually plays out in the provider setting as there is not much information on the readiness of these facilities. Based on some field visit interviews, it emerged that primary providers use their tacit knowledge of facilities that may be ready to provide
less supply-side ready than the national average. However, those private clinics empaneled by BPJS-K are more service ready than private clinics that were not, showing that the BPJS-K could be used as an effective lever to drive better service delivery through the public and private sectors. Interviews with leading providers mentioned the absence of the requirement to implement specific clinical pathways and the low capacity of BPJS-K to incorporate outcome-based measures of quality of care as factors that create incentives for providers to compromise on quality of care.
Compounding the low ability of private clinics to invest in their own supply-side readiness, they also tend to receive a lesser amount of overall BPJS-K capitation as a potential source of revenue for them to improve basic PHC services. The PHC service package covered under capitation includes 144 competencies or services that each primary care health facility that enrolls people for capitation payments is meant to perform. However, the package of services covered under JKN was never accurately costed nor was it based on whether facilities could actually provide all services. Instead, the capitation amount is determined based on the number of doctors and dentists in the facilities, and the number of beneficiaries assigned to facilities. This adversely affects remote areas where the costs of service delivery can be significantly higher, districts where disease burden is more pronounced, or facilities with a low provider to beneficiary ratio. In addition, the process of enrolment for capitation payments usually begins with the puskesmas, after which the person is free to change his/her own provider. There is a relatively low proportion of population enrolled for capitation under private providers compared to puskesmas.47 Hence, BPJS-K, could focus more resources and provide greater incentives for private providers to fill geographical gaps, including through the use of digital technologies. Similarly, it could also focus on strengthening private primary care providers by basing capitation payment amounts on actual cost of services rather than inputs only, taking
47 Purchasing of Primary Health Care Under JKN. 2018. Jakarta. World Bank.

38
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
such services to refer patients there, which may need exceptions. Patients may not be getting choice and may have to be referred more than once as the facilities may just not be ready at the lower levels. It is unclear whether the cost-saving objective of BPJS-K is being achieved; this may cause more hardship and OOP expenses to patients and create further complications or even mortality (in emergencies) due to such delays.
Leading private providers of diagnostics in Indonesia have largely been reluctant to have BPJS-K patients referred to their facilities for the reason of pricing. Diagnostics in emerging markets tends to be a volume-based business, which for common diagnostic tests generally rests on low margins. The real revenue is generated in higher-parameter tests, both for pathology and radiology, where specialist doctors are also required to provide a diagnosis for the test results.
Recommendations
1. Clarify roles of the MoH and BPJS-K to strengthen the purchasing role of BPJS-K. There needs to be clarity on who is responsible for selecting the benefit package, setting contribution rates and provider payment arrangements, and monitoring service delivery and quality standards. There are many different models followed, and most health insurance agencies have independence for many operational aspects of scheme implementation such as tariff-setting, contracting, provider payment methods, and, to a lesser extent, benefit package definition. However, provider accreditation and quality assurance are more commonly managed by the MoH.
2. BPJS-K, with the MoH, should strengthen performance-based capitation and hospital payments to incentivize broader health sector results. Moving beyond the current KBK performance indicators, indicators and verification systems should be introduced to incentivize providers to improve the quantity and quality of service delivery. In addition, primary care provision should be strengthened, and additional capitation should be explored after a through costing exercise, in addition to linking financing to performance.
3. The MoH, with BPJS-K, should target underserved areas and populations by introducing incentives. Using both demand-side financing through the JKN, and supply-side financing through the Special Allocation Fund (Dana Alokasi Khusus, DAK), incentives for investments to improve in areas that are underserved, such as in eastern Indonesia, should be introduced.
4. The MoH, with BPJS-K, should develop an effective referral process regulation, and modify/develop the necessary information systems to make this more patient centric, transparent, and driven by evidence of supply.
5. BPJS-K, with the MoH, should strengthen guidelines on quality of care by introducing clinical pathways, instituting clinical audits, strengthening monitoring of quality of care, and embedding quality-based criteria for reimbursement of providers.

39
The key requirements for a health system to function and grow is the availability of adequate health workers, which is an important concern in Indonesia. At 0.38 doctors per 1,000 people, the ratio of medical doctors to the population remains well below the WHO-recommended ratio of 1 doctor per 1,000 people. Indonesia has a significantly lower density of both physicians and nurses/midwives than countries at a similar level of income per capita (Figure 10). This scarcity of human resources has been amplified over time. Between 2006 and 2012, the density of physicians did not grow, while the density of nurses and midwives decreased in 2007–15, leaving Indonesia with densities on par with low-income countries. This makes it difficult for the system to cope with the increasing demand for health services.
The shortage of HRH is particularly acute for specialist doctors and nurses, which all private hospital groups interviewed for this report identified as the greatest challenge in expanding investment. Shortages are apparent in diverse areas as pathology, radiology, oncology, and cardiology. These shortages are particularly problematic also in light of the expected rise in chronic diseases such as cardiology, diabetes, stroke, and cancer. Newer private hospitals have focused on establishing specialist practices to draw a greater portion of their patients from BPJS-K, but they have to compete for the limited supply of specialist doctors with the more established private hospitals in Jakarta and other second-tier cities. The competition for human resources limits the ability of hospitals to expand specialist Centers of Excellence. The shortage
Reforms in health education and in recognition of qualifications are needed to expand the quantity and quality of HRH
of specific fields specialists has led to hospitals providing much higher salaries and incentives to specialists for them to practice exclusively at their hospitals. While this ensures the exclusive services of a specific doctor, higher specialist salaries can disrupt business models if they are unable to meet financial targets.
Compounding the issue of overall quantity of HRH are inequalities in the distribution of HRH between geographical regions and provinces and between urban and rural areas. For example, the physician-to-population ratio in Kalimantan and Maluku-NTT-Papua is, respectively, one-half and one-third of that in the Java-Bali region (Tandon et al. 2016). The geographic maldistribution for specialists is even worse than for physicians. Most specialist doctors are located on the islands of Java, South Sumatra, and Bali, with limited specialists elsewhere. This is primarily due to economic factors, with specialists preferring to practice in urban areas where hospitals can provide higher-value services. For example, an estimated 90 percent of the 105 endocrinologists practicing in Indonesia are located in the Greater Jakarta area, Bandung, and Surabaya.48 Across Indonesia there is also an acute shortage of nurses in puskesmas and hospitals compared to the MoH standards.49
Besides the shortages, it is also the quality of HRH—GPs—which appears concerning and deteriorating over time. Health care workers across Indonesia show a limited knowledge of the basic notions of curative care as Table 6 illustrates. The table presents the results of a test
48 Indonesian Society of Endocrinologists (PERKENI).49 The MoH standards require employment of six nurses for each regular puskesmas and 10 nurses for each puskesmas with
beds, while for Types A and B hospitals, the standard is one nurse for every bed and for Types C and D hospitals, two nurses for every three beds.

40
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Figure 10 Indonesia has a lower density of health workers than its income level suggests
Number of physicians per 1,000 people in 2006, 2009, and 2012 versus gross national income (GNI) per capita
Number of nurses and midwives per 1,000 people in 2007, 2010, and 2015 versus GNI per capita
Source World Development Indicators
IDN 2007
IDN 2010
IDN 2015
0
2
4
6
8
10
12
14
16
18
20
6 7 8 9 10 11 12
LOG GNI per capita ( Current US$ )
IDN 2006
IDN 2009 IDN 2012
0
1
2
3
4
5
6
7
8
6 7 8 9 10 11 12
WorldOECDASEANIndonesia

41
50 Table 6 includes a balanced panel data of individuals who are interviewed in each of the two waves thus ensuring full consistency of the samples.
carried out across two waves of the Indonesia Family Life Survey (IFLS), which suggest that as of 2014, the majority of Indonesian health care workers (physicians, midwives, paramedical nurses, and village midwives) are unable to follow the minimum required standards to deal with basic clinical cases of prenatal and adult curative care (see Box 1 for the methodology). Across the main regions surveyed, health workers in Sumatra
appear to perform particularly poorly. Worryingly, the quality appears to be deteriorating over time, with statistically significant drops in each of the measures of quality except for prenatal care in public facilities.50 The trend is common across the regions and the quality of responses appears to have deteriorated faster in private rather than public sector facilities.
Tabel 6 The quality of PHC workers is relatively low and deteriorating(Share of basic diagnostic and treatment procedures correctly identified by health care workers across three types of curative cares)
National Java-Bali
2007 2014 p-value (2007–14) No. 2007 2014 p-value (2007–14) No.
Prenatal Care
Public 46.30 45.10 0.145 487 47.48 46.44 0.234 336
Private 45.06 39.40 0.0001 210 45.40 40.14 0.004 134
Child Curative Care
Public 63.80 58.93 0.000 503 65.97 61.94 0.003 335
Private 62.69 51.99 0.000 268 62.85 53.08 0.000 181
Adult Curative Care
Public 55.51 48.19 0.000 502 58.26 50.85 0.000 335
Private 54.55 40.01 0.000 237 56.01 39.60 0.000 149
Sumatra Other
2007 2014 p-value (2007–14) No. 2007 2014 p-value (2007–14) No.
Prenatal Care
Public 40.48 41.24 0.364 97 49.42 43.66 0.038 54
Private 43.37 36.65 0.012 54 47.13 41.63 0.155 22
Child Curative Care
Public 57.33 52.58 0.039 100 62.62 53.43 0.002 68
Private 61.64 48.99 0.000 58 63.79 51.15 0.000 29
Adult Curative Care
Public 49.31 42.15 0.001 99 50.94 43.85 0.016 68
Private 50.72 36.68 0.000 57 54.55 48.09 0.084 31
Source Authors’ elaboration on IFLS data.Note The table reports the share of procedures correctly identified (that is, either mentioned spontaneously or when prompted) across PHC
workers interviewed in both waves of the survey (see Box 1 for the methodology); p-values indicate the level of statistical significance of the difference between the measures in 2007 and 2014 (from one-tail t-test); No. indicates the number of health care workers interviewed in each wave.

Box 1
Measuring diagnostic and treatment ability using IFLS vignettes
The ability of health providers to diagnose illness correctly is measured using community and health vignette questions from the IFLS (http://www.rand.org/labor/FLS/IFLS/) 2007 and 2014. The enumerator presents the health vignette or case to the health worker and asks how the worker would proceed. Three vignettes are conducted related to diagnosis and treatment of conditions common in prenatal, child, and adult care, respectively. For example, one vignette has a mother bringing in a child suffering from diarrhea for more than two days. Among the items that the interviewer records is an indication of whether the health provider takes the temperature of the patient and asks about frequency of diarrhea and about the nature of the stool. The health worker is then prompted to list the standard diagnostics and treatment procedures for each case. The enumerator then asks the respondent on whether each of the minimum standard procedures that he/she did
not mention spontaneously should be followed in each case. Table 6 and 7 reports the share of basic procedures (across all PHC workers interviewed) correctly identified (that is, either mentioned spontaneously or when prompted). These shares are computed out of a total of nine vignettes questions for adult curative care, 12 questions for child curative care, and 18 questions for prenatal care for each respondent.51
For the public sector, only puskesmas and auxiliary puskesmas (pustu) are included, whereas private practitioner ratings were obtained for nurses, midwives, and physicians. At public health facilities, the vignettes were conducted with the highest-level health worker present when the enumerator arrived to conduct the facility survey, and responses are used as the puskesmas or pustu score. In cases where no physician was present, the person questioned could have been a midwife, paramedic, or nurse, which is considered representative of the quality of care provided at that facility at that time.Source: Adapted from World Bank 2010.
Source: Bitran 2013; Missoni 2010.
42
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Tabel 7 The quality of PHC workers is worse in private than public sector(Share of basic questions on three types of curative cares answered correctly by health care workers)
National Java-Bali Sumatra Other
2007 2014 2007 2014 2007 2014 2007 2014
Prenatal Care
Public 45.64 44.04 47.05 47.14 38.98 39.93 49.09 35.67
Private 44.18 38.49 46.48 40.11 37.32 33.40 45.70 40.75
p-(Publ.-priv. diff.) 0.0301 0.0000 0.2833 0.0000 0.1244 0.0000 0.0301 0.0181
Child Curative Care
Public 63.59 58.40 65.50 61.94 56.18 51.06 65.24 52.90
Private 61.96 49.87 64.29 52.23 55.07 44.76 61.90 46.97
p-(Publ.-priv. diff.) 0.0266 0.0000 0.1233 0.0000 0.2660 0.0000 0.0625 0.0000
Adult Curative Care
Public 55.47 48.24 58.43 50.98 48.05 42.36 52.31 44.18
Private 53.10 39.26 56.15 41.68 46.54 33.77 51.13 38.22
p-(Publ.-priv. diff.) 0.0017 0.0000 0.0125 0.0000 0.1747 0.0000 0.2773 0.0026
Source Authors’ elaboration on IFLS data.Note The table reports the share of procedures correctly identified (that is, either mentioned spontaneously or when prompted) across all PHC
workers interviewed (see Box 1 for the methodology); p-values indicate the level of statistical significance of the difference between the measures in 2007 and 2014 (from one-tail t-test).
51 This analysis does not include all vignettes in the IFLS data

43
The quality of PHC workers is lower in private than public facilities, and the gap expanded between 2007 and 2014. Table 7 shows the differences in the health care quality test between private and public primary facilities in each year (for all health care workers). The scores of public health workers are marginally higher than those of private workers in 2007 although generally statistically significant. At the national level, the gap in 2007 was between 1.5 (for prenatal care) and 2.5 percentage points (for adult curative care), with similar differences across the country. This gap increased substantially in 2014 to between 5.5 (for prenatal care) and 9 percentage points (for child curative care). In Sumatra, for example, private health workers could correctly identify, on average, only a third of the basic procedures for prenatal and adult curative cares in 2014. The results indicate similar issues also for physicians in primary care facilities, with low and deteriorating quality particularly in the private sector. The results are shown in Tables A1 and A2 in Annex 1.
These severe shortages in skills point to an issue of undersupply of health professionals from tertiary education institutions. While there has been an increase in such a supply, mainly driven by private universities (Tandon et al. 2016), the production of HRH is still well below the needs of the system. At the same time, Indonesia has also made significant investments in improving the quality assurance system of health professional education by strengthening the school accreditation system and introducing nationally standardized competency testing for graduate certification. While this was much needed because of the rapidly growing number of health professional schools, especially private, it may have the effect of slowing the growth of medical schools—particularly the smaller ones—as it implies a higher level of requirements to establish each school (World Bank 2014). Since 2014, the GoI provides scholarships for postgraduate studies abroad, including for doctors, to specialize under the Indonesia Endowment Fund for Education (Lembaga Pengelola Dana Pendidikan, LPDP) scheme. The types of specialties are decided based on needs and can include obstetrics, gynecology, pediatrics, internists, radiology, clinical pathology, anesthesiologist, surgery, and medical rehabilitation/physiotherapy.
The lack of skilled health workers is also in part due to restrictions on the entry of foreign health professionals (FHPs) including doctors, dentists, and health practitioners. According to the MoH Decree No. 67/2013, FHPs can only work in Indonesia as long as there is a bilateral relationship with the origin country. The definition of ‘bilateral relationship’ is unclear. There are additional restrictions as follows:
1. The FHP can only provide the following services: health services, health education services, social activities, and health research. If the FHP aims to offer health services to patients, an Indonesian worker must be a mentee of the foreign worker during their tenure. The FHP can only be hired to provide health services if and only if there is a lack of supply of such skills or lack of resources.
2. The health institution (the user) employing the FHP should be a minimum Class A or Class B hospital (offering specialist services) and should have operated for a minimum of two years.
3. The user shall also provide financial evidence that show their ability to cover the FHP’s living costs for the next two years.
4. Doctors and dentists are required to have specialist degrees, while health practitioners must have at least a bachelor’s degree for health practitioners. In addition, the FHP must have ‘excellent’ Bahasa Indonesia skills that are proven with a certificate from the Center of Bahasa Indonesia.
5. The FHP should also take and pass a ‘competence certification test’ conducted by the Indonesian Doctors’ Council (Konsil Kedokteran Indonesia, KKI) or Indonesian Health Practitioners Assembly (Majelis Tenaga Kesehatan Indonesia or MTKI). This can only take place once the Ministry of Manpower receives and approves a work plan (RPTKA) from the user for the FHP, similar to conditions on foreign professors. Once the FHPs pass the test, they can obtain a temporary registration letter (Surat Tanda Registrasi Sementara) and SIP that is valid for only one year, subject to renewal only for the following year.

Figure 11 Indonesia has a much lower share of foreign medical practitioners than other countries in the region
Source Laporan KKI 2015, Malaysian Medical Council Annual Report, Thailand Medical Council (http://tmc.or.th/statistics.php), and Singapore Medical Council annual report 2016.
Note For Indonesia, the foreign doctors’ number is based on permits for technology transfer. For Malaysia, the cumulative number of arrivals is reported since 2000 until 2015, for full registration with a conditional permit. Data for Singapore is for 2016, while that for Indonesia and Malaysia is for 2015.
44
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
These conditions make the entry of the FHPs to Indonesia extremely cumbersome and time-consuming, both from the user and the FHP’s point of view. According to the MoH, it only received five applications from the FHPs requesting recommendations or renewals of permits to practice in 2017. Among 95,000 practicing doctors in 2015, only 41 were foreign, a much lower number than other smaller countries and with more advanced health systems in the region, including Singapore, Malaysia, and Thailand (Figure 11).
Restrictions on the entry of Indonesian doctors that receive specialist training abroad add to the problem of shortages. Currently, regulations (Indonesia Medical Council Regulation No. 41/2016) require that doctors who study their specialization abroad must undergo a domestic ‘adjustment period’ of 6–24 months during which they are required to take an equivalency exam and undergo residency training under the mentorship of a doctor in their field of specialization. These regulatory requirements mean that doctors
that are trained in their field of specialty are sometimes unable to practice as specialists for long periods. Anecdotally, in practice, this can take up to 9–24 months, and the period varies across medical schools in Indonesia. This policy can be a deterrent for specialists to return to Indonesia following their training, particularly when host countries such as the United States, Australia, Germany, and the United Kingdom provide opportunities to practice medicine in-country following their training. This ‘adjustment period’ is not unique to Indonesia, but with one of the lowest specialist-to-patient ratios globally, the policy deters Indonesian specialists from returning to practice in Indonesia.
Recommendations1. Increase the domestic production of quality
health professionals by expanding the capacity of the tertiary education sector. While this is a difficult undertaking, other countries in the region, such as Singapore, Thailand, and the Philippines, have managed to
0,02
7,05
0,45
15,73
0
2
4
6
8
10
12
14
16
18
Indonesia Malaysia Thailand Singapore
Share Foreign to Total (%) Foreign Doctors
Sh
are
Fo
reig
n t
o T
ota
l (%
)
Nu
mb
er
of
Fo
reig
n D
oct
ors
41
3726
247
2120
500
1000
1500
2000
2500
3000
3500
4000
0

Box 2
Duke-NUS cooperation to expand domestic supply of physicians in Singapore
One interesting aspect of Singapore’s health care system development is the effort to improve medical education. This case provides an illustration of the important links between the health and education sectors, which are examined in this report. Development in the education sector also helps resolve matters related to the capacity available in the health system.
One notable example is the cooperation between the National University of Singapore (NUS) and Duke University (USA). Together they established the Duke-NUS Medical School in 2005, which started to accept students in 2007. The school follows the American model of post-bachelor medical education (students can only do their medical studies after earning a bachelor’s degree). Successful completion of the four-year program will award the students a joint MD degree from both Duke University and NUS.
The curriculum follows that of Duke’s Medical School: the first year focuses on pre-clerkship, the second year is dedicated to clerkship, third-year students begin their research, and in the final year students are expected to participate in the advanced clinical rotations. The school also offers a doctoral degree in integrated biology and medicine, as well as an M.D.-PhD degree in which students can accelerate their studies to earn a PhD.
Research is an important component of the learning process and it receives a great amount of resources. By 2016, members of the school have made over 2,800 publications in refereed journals, 63 patents, and many other awards. The main research areas include neuroscience and behavioral disorders, cancer and stem cell biology, emerging infectious diseases, cardiovascular and metabolic disorders, and health services and systems. SingHealth, the largest health care group in Singapore, has partnered with the Duke-NUS School to promote clinical research at affiliated hospitals, clinics, and specific research locations.
Source: Presisi and University of Adelaide 2018.
45
expand domestic supply without compromising the quality of HRH. To that end, different countries have followed different routes, but one common trait has been the involvement of the private sector in providing health-related tertiary education. For example, Singapore has developed a successful model of cooperation with a foreign university enhancing the domestic curriculum and research capacity (Box 2). It would also be important to continue implementing reforms to regulate the quality of medical education that began in Indonesia.
2. Relax restrictions to the hiring of FHPs thus enabling the system to expand the stock of qualified HRH. To that end, Indonesia should increase the use of Mutual Recognition Arrangements (MRA) of qualifications for medical practitioners, which is currently a necessary requirement to employ foreign professionals. A starting point would be to use the existing Association of Southeast Asian Nations (ASEAN) framework, which aims at (i)
facilitating mobility of medical practitioners within ASEAN; (ii) exchanging information and enhancing cooperation in respect of mutual recognition of medical practitioners; (iii) promoting adoption of best practices on standards and qualifications; and (iv) providing opportunities for capacity building and training of medical practitioners, in the ASEAN region. In addition, Indonesia could consider relaxing other requirements to the hiring of foreign HRH in the MoH Decree No. 67/2013.
3. Reduce requirements to convert medical qualifications of Indonesian physicians who studied abroad. The current system of recognition of qualification could be made both less burdensome and less time-consuming. This could incentivize more qualified Indonesian health professionals to return and could also encourage more Indonesians to pursue medical studies abroad thus increasing the overall availability and quality of skills in the country.
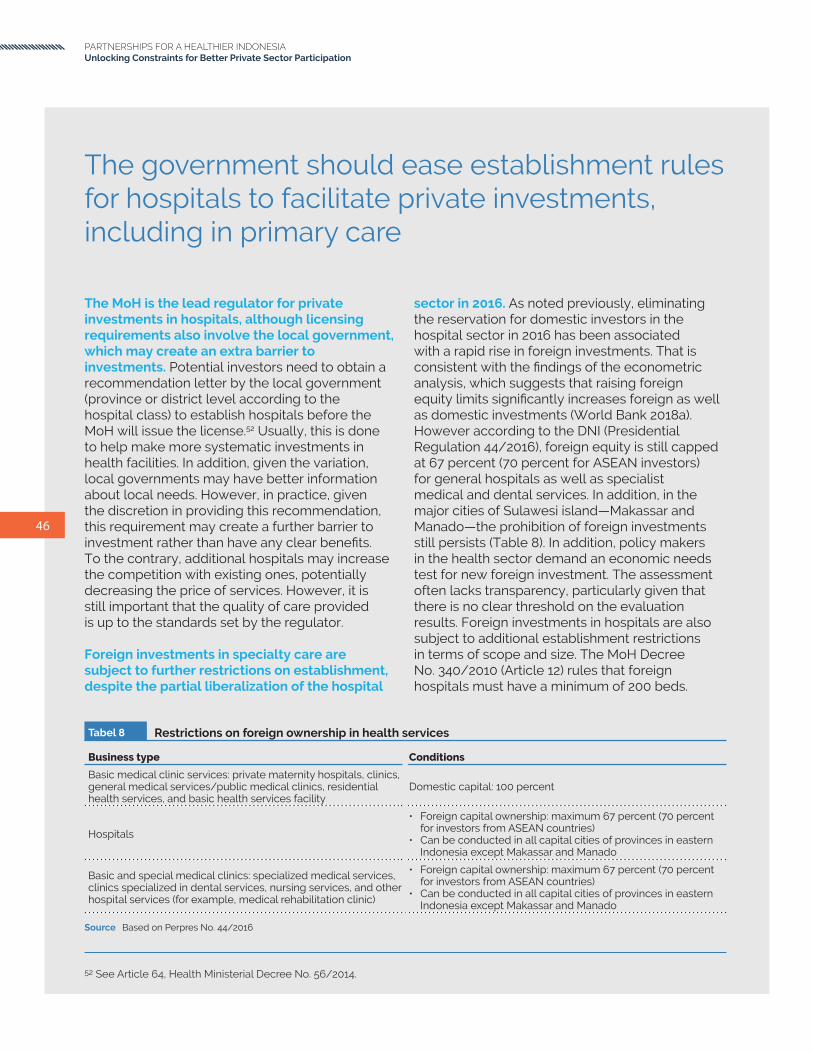
Tabel 8 Restrictions on foreign ownership in health services
Business type Conditions
Basic medical clinic services: private maternity hospitals, clinics, general medical services/public medical clinics, residential health services, and basic health services facility
Domestic capital: 100 percent
Hospitals
• Foreign capital ownership: maximum 67 percent (70 percent for investors from ASEAN countries)
• Can be conducted in all capital cities of provinces in eastern Indonesia except Makassar and Manado
Basic and special medical clinics: specialized medical services, clinics specialized in dental services, nursing services, and other hospital services (for example, medical rehabilitation clinic)
• Foreign capital ownership: maximum 67 percent (70 percent for investors from ASEAN countries)
• Can be conducted in all capital cities of provinces in eastern Indonesia except Makassar and Manado
Source Based on Perpres No. 44/2016
46
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
The MoH is the lead regulator for private investments in hospitals, although licensing requirements also involve the local government, which may create an extra barrier to investments. Potential investors need to obtain a recommendation letter by the local government (province or district level according to the hospital class) to establish hospitals before the MoH will issue the license.52 Usually, this is done to help make more systematic investments in health facilities. In addition, given the variation, local governments may have better information about local needs. However, in practice, given the discretion in providing this recommendation, this requirement may create a further barrier to investment rather than have any clear benefits. To the contrary, additional hospitals may increase the competition with existing ones, potentially decreasing the price of services. However, it is still important that the quality of care provided is up to the standards set by the regulator.
Foreign investments in specialty care are subject to further restrictions on establishment, despite the partial liberalization of the hospital
The government should ease establishment rules for hospitals to facilitate private investments, including in primary care
sector in 2016. As noted previously, eliminating the reservation for domestic investors in the hospital sector in 2016 has been associated with a rapid rise in foreign investments. That is consistent with the findings of the econometric analysis, which suggests that raising foreign equity limits significantly increases foreign as well as domestic investments (World Bank 2018a). However according to the DNI (Presidential Regulation 44/2016), foreign equity is still capped at 67 percent (70 percent for ASEAN investors) for general hospitals as well as specialist medical and dental services. In addition, in the major cities of Sulawesi island—Makassar and Manado—the prohibition of foreign investments still persists (Table 8). In addition, policy makers in the health sector demand an economic needs test for new foreign investment. The assessment often lacks transparency, particularly given that there is no clear threshold on the evaluation results. Foreign investments in hospitals are also subject to additional establishment restrictions in terms of scope and size. The MoH Decree No. 340/2010 (Article 12) rules that foreign hospitals must have a minimum of 200 beds.
52 See Article 64, Health Ministerial Decree No. 56/2014.

Figure 12 Restriction index by selected individual components of four selected ASEAN countries
Source Presisi and University of Adelaide 2018.Note The Services Trade Restrictiveness Index (STRI) has been constructed on the basis of the analysis of regulations of the provision of health
services across following Dee (2009) and Organisation for Economic Co-operation and Development (OECD) STRI.
47
Moreover, foreign investors may only establish hospitals with specialty and subspecialty services (the MoH Decree No. 56/2014, Article 65).
Foreign investments are prohibited altogether in primary care, forgoing the opportunity of attracting a source of much-needed capital as well as expertise in the sector. According to the DNI, all types of basic medical clinic services, including maternity hospitals, clinics, general medical services/public medical clinics, residential health services, and basic health services facilities, are reserved to domestic investors. The rationale of this restriction is not compelling, as foreign primary care providers are not intrinsically more risky or problematic than private domestic providers. If anything, foreign providers may help expose the Indonesian health system to the global knowledge and best practices.
As a result of these restrictions, foreign investments in health services in Indonesia are more restricted than in comparator countries in the region. Figure 12 shows that the restrictiveness of Indonesia’s regulations in relation to foreign investments is considerably
higher than in Singapore, Malaysia, and Thailand. These comparator countries have the most advanced health systems in southeast Asia, which in fact attract large numbers of high-income Indonesian patients. This is consistent with the idea that openness to foreign private investments in health may not harm—and in fact may well benefit—the quality of the national health systems.
Recommendations1. The MoH could remove the need for
the recommendation letter from the local governments for the establishment of hospitals and have a transparent set of criteria for investment, endorsed by the local governments, to replace it.
2. The MoH could remove the restriction on the scope of services for foreign hospitals.
3. The President (through the decree on DNI) could expand foreign equity limits to 100 percent across all health services sectors. These measures could encourage investments in new hospital and PHC development, which are likely to boost competition, and improve the quality of and/or access to health services.
0,00
0,20
0,40
0,60
0,80
1,00
Commercial presence
Movement of peopleOther discriminatory
measures
Indonesia Malaysia Thailand Singapore
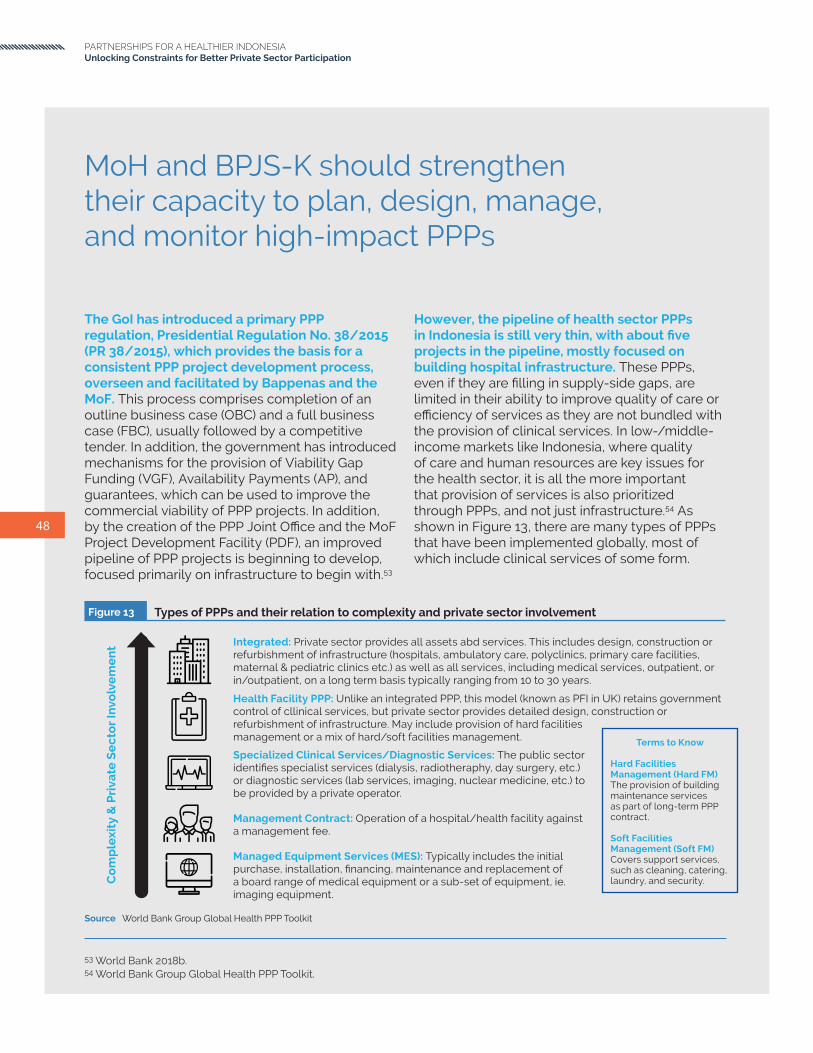
Figure 13 Types of PPPs and their relation to complexity and private sector involvement
Source World Bank Group Global Health PPP Toolkit
48
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
The GoI has introduced a primary PPP regulation, Presidential Regulation No. 38/2015 (PR 38/2015), which provides the basis for a consistent PPP project development process, overseen and facilitated by Bappenas and the MoF. This process comprises completion of an outline business case (OBC) and a full business case (FBC), usually followed by a competitive tender. In addition, the government has introduced mechanisms for the provision of Viability Gap Funding (VGF), Availability Payments (AP), and guarantees, which can be used to improve the commercial viability of PPP projects. In addition, by the creation of the PPP Joint Office and the MoF Project Development Facility (PDF), an improved pipeline of PPP projects is beginning to develop, focused primarily on infrastructure to begin with.53
MoH and BPJS-K should strengthen their capacity to plan, design, manage, and monitor high-impact PPPs
However, the pipeline of health sector PPPs in Indonesia is still very thin, with about five projects in the pipeline, mostly focused on building hospital infrastructure. These PPPs, even if they are filling in supply-side gaps, are limited in their ability to improve quality of care or efficiency of services as they are not bundled with the provision of clinical services. In low-/middle-income markets like Indonesia, where quality of care and human resources are key issues for the health sector, it is all the more important that provision of services is also prioritized through PPPs, and not just infrastructure.54 As shown in Figure 13, there are many types of PPPs that have been implemented globally, most of which include clinical services of some form.
53 World Bank 2018b.54 World Bank Group Global Health PPP Toolkit.
Terms to Know
Hard Facilities Management (Hard FM)The provision of building maintenance services as part of long-term PPP contract.
Soft Facilities Management (Soft FM)Covers support services, such as cleaning, catering, laundry, and security.C
om
ple
xity
& P
riva
te S
ec
tor
Invo
lve
me
nt
Health Facility PPP: Unlike an integrated PPP, this model (known as PFI in UK) retains government control of cllinical services, but private sector provides detailed design, construction or refurbishment of infrastructure. May include provision of hard facilities management or a mix of hard/soft facilities management.
Integrated: Private sector provides all assets abd services. This includes design, construction or refurbishment of infrastructure (hospitals, ambulatory care, polyclinics, primary care facilities, maternal & pediatric clinics etc.) as well as all services, including medical services, outpatient, or in/outpatient, on a long term basis typically ranging from 10 to 30 years.
Specialized Clinical Services/Diagnostic Services: The public sector identifies specialist services (dialysis, radiotheraphy, day surgery, etc.) or diagnostic services (lab services, imaging, nuclear medicine, etc.) to be provided by a private operator.
Management Contract: Operation of a hospital/health facility against a management fee.
Managed Equipment Services (MES): Typically includes the initial purchase, installation, financing, maintenance and replacement of a board range of medical equipment or a sub-set of equipment, ie. imaging equipment.

Box 3
Diagnostics PPP - Jakarta National Hospital (Rumah Sakit Cipto Mangkukusumo, RSCM), Jakarta
There is an existing PPP model in radiology at RSCM, where a private investor has placed Computerized Tomography Scan (CT Scan) units at the hospital in a revenue share agreement with the hospital. The operator also provides the technical assistance required to operate the units, and the hospital provides the space and the required permits to operate the unit.
The private investor has been in a working relationship with RSCM for the past six years, and before the introduction of BPJS-K referrals, it was receiving an average of 30 patients per day for diagnostic imaging. Following the introduction of BPJS-K referrals, it saw the numbers increase to 50–60 patients per day, which eventually led to a request from RSCM to invest in an additional CT Scan unit to account for the increased patient numbers. The investor was initially reluctant to invest in an additional CT Scan, as their projections found that the average number of patients requiring imaging would drop or remain the same, partly due to BPJS-K starting to restrict the number of services that were covered for BPJS-K patients. The private investor,
however, felt somewhat pressured by the hospital to invest in an additional CT Scan, while the number of patients requiring diagnostic imaging has remained the same at about 50–60 patients per day. The operator said that for the past 18 months, it noticed significant delays in accounts receivable (AR), with payment from BPJS-K delayed an average of 4–5 months. Unlike for private hospitals, there is no provision for a 1 percent interest payment for delays for public hospitals that have services agreements with private investors, so the private investor has to simply accept delayed payments as part of working with the leading public hospital.
The investor anticipates that the BPJS-K deficit problem will eventually be resolved; however, it said that public hospitals tend to have greater leverage over private investors because they are the first option for BPJS-K patient referrals, and since RSCM is affiliated with the University of Indonesia (UI) faculty of medicine, and is the teaching hospital for UI. The investor indicated that if private investors feel that PPPs are not a win-win proposition, the incentives to invest may dissipate. More importantly, if payment delays continue, they can eventually threaten to disrupt business operations, which can result in a losing proposition for the private investor. It would like to see a win-win proposition where both private investors can allocate capital for investment in services and human resources, and the hospital can improve its operational efficiency and improve the overall patient experience.
49
In addition, many of these PPPs can have a ‘high impact’, in terms of enabling access to a larger population group, increasing efficiency due to larger economies of scale as well as intervening at lower levels of care, improving quality by standardizing processes, and reaching out to underserved populations. These include PPPs such as expanding quality diagnostic services (radiology and pathology) using hub-and-spoke models, integrated provider networks of primary and hospital care, and specialist services (such as eye care); managing supply chains and managed equipment services; and potentially using digital health solutions (for data management and analytics as well as service delivery). Two examples of implementing a radiology PPP in Jakarta and one in Jharkhand, India, are provided in Box 3 and Box 4, respectively.
As a follow-up to the Presidential Regulation No. 38/2015, the MoH has developed an MoF decree PMK 40/2018, as a regulation for PPPs. This is a good first step as it indicates the government’s commitment to use private sector solutions or PPPs for improving the health sector. While the PMK 40/2018 has a strong infrastructure focus at the hospital level, it also includes other facilities (primary care clinics, laboratories, and health polytechnics) as well as services.
The types of PPPs as defined in the PMK 40/2018 are for infrastructure (Kerjasama Pemerintah Dengan Badan Usaha (KPBU) or Government Cooperation with Business Entities) services (contracting through BPJS-K), health information, advocacy and capacity building (Social Responsibility Partnership or CSR/

Box 4
Diagnostics imaging PPP - Jharkhand, India
The state of Jharkhand in India has a population of 30 million and an extreme shortage of specialists in the state. The critical need for diagnostic services and radiologists, particularly in rural areas, led to an 84 percent shortfall of radiologists in district and smaller hospitals. The Government of Jharkhand sought a PPP with a private sector provider to develop modern radiology services in all 24 district hospitals across the state, in a hub-and-spoke model.
The International Finance Corporation (IFC) assisted the Government of Jharkhand to structure and develop a model of radiology centers across the state, and the competitive bidding process was awarded to HealthMap, a diagnostics provider in Ranchi, Jharkhand. The company was a joint venture between
Manipal Hospitals and Philips, which provides lower-cost imaging devices such as MRIs and CT Scans.
A 10-year concession agreement was signed in November 2015 between HealthMap Diagnostic and the Government of Jharkhand. HealthMap as the operator will be responsible for the financing, operating, and maintenance of the radiological equipment placed at government hospitals. The government will channel the required volumes of patients to ensure that the radiology units are being utilized at an efficient capacity. The agreement also provides an annual review and followed by an overview of the services, which if satisfactory can be renewed for another 10-year term. The arrangement allows for public hospitals to tap into the network of radiologists that work in the private sector and improves accessibility for patients and timely analysis of diagnostic results. Installing standardized diagnostic units across all 24 state hospitals and imaging equipment allowed for greater reliability of results and lessened the need for additional testing thereby reducing costs for both the public hospitals and the operators.
Tabel 9 Different types of PPPs according to PMK 40/2018
KPBU KSO CSR/KTJS
ScopeBuildings, medical devices, and related services
Related medical devices and services
Health infrastructure and medical equipment grants, promotive and preventive activities, and capacity-building activities
PeriodLong (10–20 years) according to contract
Short (3–5 years) according to contract Occasional/one-off
Enterprises provisions
Private enterprises in the form of limited liability company, foreign legal entity, cooperative, BUMN, or Badan Usaha Milik Daerah (BUMD) or Provincial/Municipal-Owned Enterprises
Private enterprises in the form of limited liability company, foreign legal entity, cooperative, BUMN, or BUMD
Enterprises in the form of limited liability companies, foreign legal entities, cooperatives, foundations, forms of private enterprises that are not legal entities (individuals and firms), mass organizations, nongovernmental organizations, philanthropic organizations, universities, media, communities, and other organizations all of which have social responsibility in the field of health, BUMN, or BUMD
Profit value for enterprises Yes Yes No
Source Based on Perpres No. 44/2016
50
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation

51
KTJS), and for medical devices and services Kerjasama Operasi (KSO) or Operational Cooperation Contract. The differences in these types of PPPs are given in Table 9.
Under the KPBU type of PPP, the PMK has specified the following for hospitals and includes infrastructure and equipment provision as well as operational management, such as hospital management, provision of various services listed below, and human resources required for the same.
1. Medical services including emergency services, general medical services, basic specialist medical services, supporting specialist medical services, other specialist medical services, subspecialty medical services, and medical services for dental and oral specialists
2. Pharmaceutical services including the management of pharmaceutical preparations, medical devices and consumable medical materials, and clinical pharmacy services
3. Midwifery and nursing services including general nursing and specialist nursing care and midwifery care
4. Clinical supporting services including blood bank services, intensive care for all age groups and types of diseases, nutrition, instrument sterilization, and medical records
5. Nonclinical support services including laundry/linen services, catering/kitchen services, engineering and maintenance of facilities, waste management, warehouses, ambulances, information and communication systems, mortuary, fire management systems, medical gas management, and clean water management
The overall PMK 40/2018 looks broad enough to do various types of PPPs but has less clarity on nonhospital and service-oriented PPPs. For example, whether specific PPPs will be applied such as for laboratory networks, data management services, logistics and supply chain management, digital health services or an integrated network of hospitals and clinics is less clear. While there is scope to improve
aspects of the law to clarify some of these issues and make it more service oriented, the current regulation allows for the health sector to move forward with planning, designing, and implementing high-impact PPPs.
Box 5 illustrates a network PPP, consisting of both hospital and primary clinics, for both infrastructure upgrading and service delivery.
In addition to having an enabling law or regulatory framework, one of the key aspects that was found that determined success is the ability to plan, design, and manage PPPs, with a specific expertise in the health sector. A World Bank Group Independent Evaluation Group report on health PPPs in 2016 found that among World Bank Group projects that led to contract closure, the largest success factors are project design and government commitment. Project design factors were cited in 76 percent of the successful cases, followed by government commitment, found to be a success factor in 72 percent of the projects. An important aspect of success is the willingness or the capacity of governments to undertake PPPs. Similarly, lack of government capacity or commitment is the main reason PPPs do not pass from the options report stage to the bidding assistance stage. Other studies have also found that effectiveness is found to be dependent on a more active regulatory role from the government (Torchia, Calabro, and Morner 2013).
In Indonesia, as in most countries, the main PPP unit functions lie between the MoF and Bappenas level for broader PPP planning, design, and management.55 However, capacity in the MoH to take some important sectoral functions remains limited. There is a small team in the center for health financing that functions as the ‘health PPP team’ for the MoH and usually takes the lead on health PPP-related matters, including most recently the development of the PMK 40/2018. Similarly, in BPJS-K, there is some capacity in terms of engaging the private sector in the empanelment of providers and in entering into contracts or agreement for purchasing services. However, BPJS-K does not do many of
55 A recently concluded study by the World Bank (2018b) in Indonesia has already made recommendations on how these could be improved, and hence they are not covered in this report

Box 5
PPP - Bhubaneshwar health network
Odisha is a low-income state in India where the largest public hospital is in the state capital, Bhubaneshwar. Capital Hospital, the state’s main public hospital was overcrowded and ran above 100 percent capacity. These issues along with frequent downtime for essential equipment and the lack of medical staff led to inefficient services for patients. The state also operated five clinics in Bhubaneshwar; however, these were underperforming and underutilized. The state government has had difficulty in maintaining and expanding health facilities in Bhubaneshwar and sought private sector assistance to improve capacity.
In 2016, the Bhubaneswar Municipal Corporation (BMC) that operates Capital Hospital launched a bidding process to find a private partner to improve existing facilities and to build a new multispecialty hospital that would relieve the burden on Capital Hospital. In April 2017, Krishna Institute of Medical Science, a
Maharashtra-based medical institute and specialist hospital operator, was selected as the private partner.
The bidding process for the private partner was unique as the bidders were required to provide a minimum number of beds allocated within the hospital facilities for patients who fell below the poverty line. The key terms of the transaction ensured that there is bare minimum OOP expenditure for poor and underprivileged patients—zero consultation fees and inpatient costs and highly subsidized outpatient costs, with service fees being covered by social health insurance. Another requirement was for BMC to integrate its Hospital Management Information Systems, so that data required for public health statistics were directly transmitted to the MoH.
The government decided to upgrade the five clinics and to establish a greenfield multispecialty hospital that would have a total of 500 beds between the new hospital and the upgraded clinics. The private partner will lead the design, refurbishment, and upgrading of the clinics and develop the greenfield multispecialty hospital; procure and install equipment; and staff, maintain, and operate the network for a period of 34 years.
52
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
the upstream as well as downstream functions needed to plan, design, and manage PPPs. Many countries that have taken health PPPs forward, such as Australia, have good capacity on both the broader PPP unit as well as health sector capacity. Some of the key functions needed to be performed by the PPP team, in coordination with other units in the MoH, with BPJS-K and other relevant institutions, would include
1. Having data and information on demand patterns and supply-side readiness for better planning: identifying clear gaps based on demand patterns (population, disease burden, and utilization of services) as well as using available data on public and private sector provision, the services they provide, and their supply-side readiness;
2. Developing an umbrella public-private platform for the health sector as well as sub-sectoral fora and cross-government coordination mechanisms (MoH, BPJS-K, Bappenas, MoF, Indonesia Infrastructure Guarantee Fund (IIGF), and local governments) to discuss and resolve constraints as well as
identify a pipeline of ‘high-impact’ PPPs that helps fulfill supply-side needs and also ensures that these plans have private sector interest;
3. Developing capacity to design and manage the PPP transaction process, including hiring and managing transaction advisors;
4. Developing capacity for managing and monitoring PPPs post transaction completion in the MoH, BPJS-K, and involved local governments; and
5. Developing capacity to evaluate PPPs in terms of health sector goals of access, quality, efficiency, equity, or financial protection.
In terms of funding for PPPs, the government has supply-side financing mechanisms such as the provision of VGF, AP, and guarantees, which can be used to improve the commercial viability of PPP projects. At the same time, it envisages BPJS-K as the main purchaser of services, and hence, operational financing. There are some models of financing in the PMK 40/2018, but there may be more clarity required on how these both would work together as necessary to structure a deal where both infrastructure and

53
56 Referred under constraint #1 also..
services are envisaged, such as an integrated hospital and clinic network or building and operation of a network of diagnostic facilities.
Leading hospital groups have indicated that establishing PPPs with government providers in the specific areas of pathology and radiology are attractive due to the rapid increase in patient volumes due to BPJS-K referrals. In addition, many hospital providers have been told by BPJS-K that they would prefer them to invest in more remote or underserved regions. However, these providers also mention that to make more informed choices, they would be better placed if they get more information on the demand and utilization rates as well as have a platform where they could see how their investment risk could be mitigated. These structured platforms for discussing these issues and potential solutions for the health sector across various arms of government (MoH, BPJS-K, Bappenas, MoF, IIGF, and local governments) do not exist as of now.
Recommendations
1. The MoF and Bappenas, with the MoH and BPJS-K, should establish cross-government coordination mechanisms (also involving IIGF and local governments) and public-private platforms to identify a pipeline of high-impact PPPs that have private sector interest.
2. The MoH, with BPJS-K, should identify clear gaps which could be fulfilled by the private sector, including PPPs, based on demand patterns (population, disease burden, and utilization of services) as well as using available data on public and private sector provision.56
3. The MoH and BPJS-K, with the MoF and Bappenas, should develop capacity as well as identify clear roles and responsibilities to design and manage the PPP transaction process, manage and monitor PPPs, and evaluate PPP results.
54
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Indonesia has recently established KAFKTP, based on two decades of experience in hospital accreditation. Accreditation is a voluntary process that is followed by providers to improve quality of services by ensuring that not only the necessary inputs (such as infrastructure, equipment, and human resources) are in place but also that both clinical and managerial processes are improved. Accreditation involves a hands-on process of expert mentoring of facilities to improve their managerial processes, clinical care standards, and community health programs (in the case of PHC). Facilities are required to be reaccredited every three years to provide an incentive to maintain standards. While accreditation does not lead to improved clinical outcomes by itself, it is an important part of a ‘package’ of interventions that improve the performance of health facilities. In addition to building capacity, it also provides a governance framework for the sector, directing investments and signaling to beneficiaries and payors managerial and clinical competence.
The new policy of the MoH is to make accreditation of hospitals and PHC facilities a prerequisite for empanelment by Badan Penyelenggara Jaminan Sosial - Health (BPJS-Health) as a JKN provider, by 2019 and 2021, respectively. However, while most C-Class hospitals in the Jakarta area have been required to accept BPJS-K patients, there have been significant delays in uptake of patients as many private hospitals have not been accredited by KARS.57 As of December 2018, approximately 2,200 private hospitals have been empaneled by BPJS-K-signed contracts to provide services. However, only 1,759 private hospitals have
The government should strengthen hospital and primary care accreditation capacity to facilitate empanelment by BPJS-K
been accredited to date. The MoH said that 341 unaccredited hospitals have committed to finishing the accreditation process by June 30, 2019. A recent media report indicated that 19 hospitals in the Greater Jakarta area were taken off the BPJS-K referral hospital list as they were not accredited by KARS.58
Similarly, for primary care accreditation to work, the credibility of KAFKTP, and its processes, needs to be strengthened. Accreditation of PHC facilities began in 2015, with the enactment of the MoH Regulation No. 46/2015 and the establishment of KAFKTP. While the current capacity of KAFKTP is limited (owing to its nascent stage), the vision is to expand its capacity, become fully independent, cover both the public and private sectors, and eventually get accredited itself, by ISQua. At present, the KAFKTP covers only the public sector.
It is also important that KAFKTP develops credible quality assurance and validation mechanisms, as well as makes its standards and results transparent. There are four levels of accreditation for PHC facilities, namely dasar, madya, utama, and paripurna, based on the scores achieved across nine major standard areas. For the public sector, plans for accreditation of puskesmas include a staggered approach, where at least one puskesmas in 5,600 subdistricts is to be accredited by 2019. According to the MoH reports, 7,518 puskesmas have been accredited as of December 2018, of which 32 percent have received the basic level (dasar) accreditation, 56.5 percent mid-level (madya), 10.6 percent superior level (utama), and only 1 percent the
57 KARS was established by the MoH as a domestic equivalent to Joint Commission International, an international hospital accreditation body.
58 https://www.thejakartapost.com/news/2019/01/06/BPJS-K-kesehatan-terminates-contracts-with-dozens-of-hospitals.html.
55
highest level (paripurna).59 Once accredited, the status is retained for three years. While the MoH has been focused on increasing coverage, from 2018, it will shift attention to increasing the proportion of puskesmas that achieve higher levels of accreditation. This is very important as higher levels of accreditation require more stringent adherence to outreach, managerial, and clinical standards, which are challenging to reach. Though puskesmas accreditation has reached several districts/cities and all 34 provinces across Indonesia, the number of accredited puskesmas is much lower in eastern provinces such as Papua, Maluku, and NTT.
59 Indonesia Health Profile, MoH, 2018.
Recommendations
1. The MoH, and KAFKTP, should develop and implement a business plan that outlines the vision to expand its capacity (for facilitation and accreditation), become fully independent from the MoH (both financially and institutionally), and cover both the public and private sectors.
2. KARS should expand its capacity to cover the increased demand for hospital accreditation services.

56
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
The MoH is currently developing e-health regulations in collaboration with both traditional health care providers and digital health providers. The primary focus of e-health regulations from the MoH perspective is to safeguard patients’ medical records and data. The MoH is working closely with digital health providers to develop regulations on e-health, e-prescriptions, and telemedicine specifically for diagnostics. BPJS-K maintains a digital footprint for those patients that have downloaded and utilized their application, as well as patients that have been referred through BPJS-K to private providers for specialist treatment. Digital health providers see the potential in collecting patient data and extracting relevant information that could be monetized and be useful to health care providers, pharmaceutical companies, and medical device manufacturers. While digital health providers have confirmed that discussions are under way to develop data privacy standards for e-health, there was no indication as to when these regulations would be issued, stating that it is a work in progress.
The ability for digital health providers in Indonesia to integrate with private health care providers or BPJS-K has been limited due to the general lack of integrated hospital HISs and electronic medical records (EMRs), for both public and private health care providers. Many health care providers lack information technology (IT) systems due to financial considerations, as the solutions can be expensive. There has been progress however as Indonesia’s leading private hospital group, Siloam, recently implemented an EMR in 2018, and HHG and Mitra Keluarga recently implemented an HIS across all their hospitals. Until recently, hospital groups were unable to provide patient data from one hospital to another digitally. Digital health providers are now working
MoH should clarify and ease e-health regulations to foster digital health innovations
with hospitals, clinics, and insurance groups to digitize employee health benefits. Digital health providers will be leading this integration of ecosystems to bring together HISs, EMR, or IT solutions for finance and procurement. If digital health providers can integrate platforms by bringing together appointments, consultations, diagnostics, and pharmacies, it will lead to more efficient operations for health care providers and more efficient patient pathways. One of the constraints to this is a lack of clarity on data standards as well as standards of interoperability for the health sector that impedes development of such solutions on a larger scale.
The growth of e-commerce platforms in the last five years in Indonesia has also led to companies that provide the delivery of prescription and OTC drugs. The MoH expressed concerns over the legality of delivery services that seek to provide prescription drugs through digital health applications. While OTC drugs are allowed to be purchased online and delivered directly to the patient, concerns remain over prescription drugs. In particular, there are concerns over drugs that contain psychoactive substances, to ensure that digital platforms do not enable the abuse or unregulated purchasing of such drugs. Mobile applications can currently provide the delivery of prescription medications, and a physical prescription is required to purchase the medicine either at a hospital or pharmacy. The MoH is developing a draft legislation for an e-prescription regulation and is consulting with digital health providers and pharmacy groups to identify risks and potential mitigation measures. The MoH realizes the benefits and convenience to patients if they can have their medications delivered and prescriptions renewed utilizing digital platforms. A major constraint in developing e-prescriptions is that there are limited HISs and EMRs in place

57
across public and private hospitals, which are in turn connected with pharmacies and digital health applications. A universal basic data standard for IT systems at hospitals and diagnostic centers would allow easier collection of data and transfer of data between health care service providers and digital health applications.
Existing forms of digital health are already being used by Indonesia’s diagnostics providers (including hospitals) particularly since imaging or pathology tests can be sent through email or mobile devices or specialized digital platforms to be analyzed by specialist radiologists or pathologists. BPJS-K has also developed its own internal database that provides primary care physicians a database of hospitals for specialist referrals. Specialist doctors are normally only allowed three SIPs. However, at the discretion of DinKes, officials occasionally provide additional SIPs to specialists such as radiologists or pathologists to practice at hospitals that provide diagnostic services. Radiologists can work remotely or are based at one location where they can receive images and test results through digital means and can sign off on their analysis and diagnosis. A chief operating officer of Jakarta’s leading diagnostic provider has said that telemedicine could solve the problem in the near future with automated interpretation of diagnostic results. At present, regulations require that a laboratory or radiology result requires the sign-off from a qualified Indonesian pathologist or radiologist, in-country, for a patient to be treated. Telemedicine for diagnostics is already commonplace in the Philippines and India, and due to Indonesia’s specialist shortage, foreign joint ventures could address this shortage initially in the private health care market. It is unclear that these restrictions have much benefit, especially given the shortage of specialists in Indonesia.
Digital health providers face the same problems of health care service providers with the lack of human resources, specifically for specialist doctors. Patients in remote areas are at a minimum able to visit a GP at a puskesmas or primary care clinic. However, access to specialist doctors in remote areas is rare. The digital health platforms are aiming to address this lack of access to specialist doctors but are constrained by the same limit in
supply of specialist doctors. Many specialists tend to practice in urban areas where the flow of patients is higher and where hospitals will have equipment where they can provide higher-value services. In the cases of sub-specialists or surgeons, many are working over capacity as the demand for their services exceeds the supply of the specialists. As a result, many specialist doctors are working at full capacity, and are unable to add digital patients to their schedule. Digital health can provide a solution for access to primary care by providing for mobile consultations for patients that do not have access to health care facilities. With existing mobile infrastructure, doctors in second- or third-tier cities could provide mobile consultations with medical staff in the field where doctors are unable to reach. Based on tele-consultations, an assessment could be made by a doctor if the patient requires additional care or if the patient should come to the nearest hospital for further tests.
Despite having a relatively high penetration of mobile Internet, digital infrastructure remains a major challenge in Indonesia, which constrains digital health’s ability to provide health care access to patients. Indonesia’s Internet penetration is 50 percent, not far from southeast Asia average of 58 percent and below the global average of 53 percent (We Are Social 2018). However, the average quality of connections—as measured by download speed—is poor (Figure 14). This could make it difficult to use some of the e-health services such as video-based remote consultations. In addition, the quality of infrastructure is heterogenous across the archipelago, with sparsely populated remote regions—such as in Eastern Indonesia—that still have limited access to fast mobile broadband Internet (Figure 15). Telemedicine in Indonesia is an obvious solution to provide last-mile access, primarily due to the logistical difficulties in remote provinces. However, until data security and mobile infrastructure are not adequate, the implementation of these solutions will be limited.

Figure 14 Digital infrastructure quality is poor in Indonesia
Source We Are Social 2018.Note Left hand side panel is average MBps for fixed Internet connections and right hand side panel is average MBps for mobile Internet
connections. Both the figures contain the three top-ranked countries followed by a selected sample of Asian countries.
0
20
40
60
80
100
120
140
160
180
Sin
gap
ore
Ho
ng
Ko
ng
So
uth
Ko
rea
Wo
rld
Th
aila
nd
Vie
tnam
Mal
aysi
a
Ph
ilip
pin
es
Ind
on
esi
a
0
10
20
30
40
50
60
Ne
the
rlan
ds
Sin
gap
ore
U.A
.E.
So
uth
Ko
rea
Ho
ng
Ko
ng
Wo
rld
Vie
tnam
Mal
aysi
a
Th
aila
nd
Ph
ilip
pin
es
Ind
on
esi
a
Average MBps for fixed Internet connections Average MBps for mobile Internet connections
58
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Figure 15 Download throughout Telkomsel long-term evolution (MBps)
Ace
h: B
and
a A
ceh
So
uth
Su
law
esi
: Mak
assa
r
Ria
u: B
en
gka
lis (P
alap
a R
ing
We
st)
So
uth
Eas
t S
ula
we
si: k
en
dar
i
Bal
i: D
en
pas
ar -
Nu
sa D
ua
Go
ron
talo
Nia
s: G
un
un
g S
ito
li
No
rth
Su
law
esi
: Man
ado
Eas
t Ja
va: R
ura
l, ar
ou
nd
Mad
iun
Jaka
rta
Ce
ntr
al S
ula
we
si: L
uw
uk
Ban
dar
Lam
pu
ng
: Ko
ta A
gu
ng
No
rth
Su
mat
era
: ou
tsid
e M
ed
an
Mal
uku
Uta
ra: T
ern
ate
No
rth
Su
law
esi
: ou
tsid
e M
anad
o
Be
ng
kulu
Mal
uku
: Tu
al
Ce
ntr
al K
alim
anta
n
Eas
t K
alim
anta
n: S
amar
ind
a
Su
mb
a: W
ain
gap
u
Pap
ua:
Jay
apu
ra
Pap
ua:
Me
rau
ke
Pap
ua
Bar
at: M
ano
kwar
i
Pap
ua:
Wam
en
a (s
ate
llite
)
Mal
uku
: Sau
mla
ki (s
ate
llite
)
0
5
10
15
20
25
30
35

59
Recommendations
1. The MoH and BPJS-K should develop data privacy standards as well as pass the necessary legislation in consultation with stakeholders, including health care service providers and digital health providers. Medical data are frequently the target of hackers, and BPJS-K should invest in IT security to prevent the disclosure of confidential medical records. As some digital platforms are already collecting their own data on their users, a timely issuance of protection of digital patient data would be beneficial to patients as well as would make clear the type of data private companies can collect on their users.
2. The MoH and BPJS-K should develop protocols for sharing of data with privacy protections and consider using digital health providers for data analytics and service delivery. This could enable the MoH and BPJS-K to use digital health providers that are strong in providing technology solutions that could assist BPJS-K in the development of applications with the data analytics and telemedicine that could improve access to health care, specifically in remote regions of the archipelago. In working with digital health providers, they can institute a nationwide standard of IT systems to integrate across health care service providers and ensure interoperability between the various stakeholders.
3. The MoH, with BPJS-K could develop legislation that focuses on e-prescriptions to improve access to prescription medications, while maintaining necessary safeguards. E-prescriptions can help increase patients access to appropriate medication and also potentially improve adherence through linked digital solutions. However, it would also be important to safeguard from abuse of prescription medication, and the MoH can require that e-prescriptions could be restricted to certain classes of drugs.
4. The MoH could lift restrictions on foreign telemedicine providers specifically in pathology and radiology. As these two specialist functions are non-patient facing, the doctors do not necessarily need to be in the country, and the additional specialist doctors can address the shortage of specialist doctors in the short term. Countries such as India and the Philippines that have an adequate supply of pathologists and radiologists can create joint ventures with both public and private providers, to alleviate some of the burden of the number of tests that Indonesian specialist doctors have to conduct. Providing doctors with a balanced workload will improve the analysis and provide for more accurate diagnostics, which in the end will benefit the patients. The MoH and BPJS-K would need to come up with revisions in the regulations for foreign doctors, and they could relax restrictions only in specialist areas that face an acute supply shortage.
5. The GoI should focus on the upgrading of mobile infrastructure in remote regions to improve access to 3G and the use of smartphones. The improvement in connectivity through smartphones can help in improving last-mile access to patients in regions where there is a limited number of health care workers. This would enable many digital health solutions to enable remote diagnostics and consultations, not to mention support for frontline community health workers.

60
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
The table below summarizes the recommendations for various constraints grouping them as regulatory reforms needed, institutional coordination mechanisms that need be set up, as well as capacity building that needs to be carried out to ensure better private sector participation to improve the health sector in Indonesia.
Summary Table of Recommendations
CONSTRAINTS RECOMMENDATIONS
Regulatory reforms
Lack of a clearly articulated strategy for private sector engagement
The MoH, with BPJS-K, and Bappenas, should prepare a private sector engagement strategy, with differential strategies for various subsectors, to fulfill supply-side gaps by improving access, quality, and efficiency.
Sustained and increasing financial deficit of BPJS-K
• Simplify the overall tobacco tax structure and increase tobacco excise taxes at the national level, with potential earmarking to BPJS-K.
• Update JKN premiums based on actuarial analysis.• Subsidize premiums for the informal sector to address adverse selection
by attracting and retaining a larger pool of healthy members.• Address open-ended hospital payments where most spending occurs by
introducing a budget and/or volume ceiling.• Introduce an explicit benefit package commensurate with available
resources.
Underutilization of the BPJS-K strategic purchasing function to drive improvements in service provision and quality
• The MoH, with BPJS-K, should target underserved areas and populations by introducing incentives.
• BPJS-K, with the MoH, should strengthen performance-based capitation and hospital payments to incentivize broader health sector results.
Inadequate availability of skilled health professionals
• Continue to implement reforms to improve quality of medical education.• Relax restrictions to the hiring of FHPs thus enabling the system to
expand the stock of qualified HRH.• Reduce requirements to convert medical qualifications of Indonesian
physicians who studied abroad.
Restrictive establishment rules for private sector players—foreign in particular
• The MoH could remove the need for the recommendation letter from the local governments for the establishment of hospitals and have a transparent set of criteria for investment, endorsed by the local governments, to replace it.
• The MoH could remove the restriction on the scope of services for foreign hospitals.
• The President (through the decree on DNI) could expand foreign equity limits to 100 percent across all health services sectors.
Unclear and at times overly restrictive e-health regulations
• The MoH and BPJS-K should develop data privacy standards as well as pass the necessary legislation in consultation with the stakeholders.
• The MoH and BPJS-K should develop protocols for sharing of data with privacy protections and consider using digital health providers for data analytics and service delivery.
• The MoH, with BPJS-K, could develop legislation that focuses on e-prescriptions to improve access to prescription medications, while maintaining necessary safeguards.
• The MoH could lift restrictions on foreign telemedicine providers specifically in pathology and radiology.

61
CONSTRAINTS RECOMMENDATIONS
Institutional coordination platforms
Lack of a clearly articulated strategy for private sector engagement
The MoH, with BPJS-K, should prepare a database of private (and public) providers using multiple information sources.
Underutilization of the BPJS-K strategic purchasing function to drive improvements in service provision and quality
Clarify roles of the MoH and BPJS-K to strengthen the purchasing role of BPJS-K.
Lack of an enabling government environment to design, manage, and monitor PPPs
• The MoF and Bappenas, with the MoH and BPJS-K, should establish a cross-government coordination mechanisms (also involving IIGF and local governments) and establish an umbrella public-private platform for the health sector as well as sub-sectoral fora to identify a pipeline of high-impact PPPs that have private sector interest.
• The MoH, with BPJS-K, should identify clear gaps which could be fulfilled by the private sector, including PPPs, based on demand patterns (population, disease burden, and utilization of services) as well as using available data on public and private sector provision.
Capacity building
Underutilization of the BPJS-K strategic purchasing function to drive improvements in service provision and quality
• The MoH, with BPJS-K, should develop an effective referral process regulation and modify/develop the necessary information systems to make this more patient centric, transparent, and driven by evidence of supply.
• BPJS-K, with the MoH, should strengthen guidelines on quality of care by introducing clinical pathways, instituting clinical audits, strengthening monitoring of quality of care, and embedding quality-based criteria for reimbursement of providers.
Inadequate availability of skilled health professionals
Increase the domestic production of quality health professionals by expanding the capacity of the tertiary education sector.
Lack of an enabling government environment to design, manage, and monitor PPPs
The MoH and BPJS-K, with the MoF and Bappenas, should develop capacity as well as identify clear roles and responsibilities to design and manage the PPP transaction process, manage and monitor PPPs, and evaluate PPP results.
Poor capacity of the hospital and primary care accreditation systems
• The MoH, and KAFKTP to (a) expand capacity (for facilitation and accreditation) and (b) become fully independent from the MoH (both financially and institutionally).
• KARS should expand its capacity to cover the increased demand for hospital accreditation services.
Unclear and at times overly restrictive e-health regulations
The GoI should focus on the upgrading of mobile infrastructure in remote regions to improve access to 3G and the use of smartphones.

62
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation

63
APPENDIXES
ANNEXES

64
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Annex 1HRH - Quality Assessment using Clinical Vignettes
Table A1 The quality of physicians in primary care is relatively low and deteriorating
(Share of basic diagnostic and treatment procedures correctly identified by physicians across three types of curative cares)
National Java-Bali
2007 2014 p-value (2007–14) No. 2007 2014 p-value (2007–14) No.
Prenatal Care
Public 47.59 46.68 0.239 361 48.36 47.45 0.288 249
Private 44.48 31.92 0.003 31 44.74 25.56 0.001 14
Child Curative Care
Public 66.30 60.66 0.000 361 67.91 62.92 0.002 247
Private 64.56 56.58 0.000 95 65.53 56.62 0.000 73
Adult Curative Care
Public 58.38 51.97 0.000 360 60.58 54.51 0.000 247
Private 57.45 44.73 0.000 100 58.13 43.66 0.000 76
Sumatra Other
2007 2014 p-value (2007–14) No. 2007 2014 p-value (2007–14) No.
Prenatal Care
Public 43.14 43.46 0.552 66 49.77 47.14 0.217 46
Private 42.86 37.97 0.272 14 50.88 33.33 0.121 3
Child Curative Care
Public 60.57 55.10 0.058 67 65.96 56.74 0.005 47
Private 60.00 55.00 0.1470 15 64.29 59.52 0.3091 7
Adult Curative Care
Public 53.44 45.87 0.006 66 53.77 47.20 0.055 47
Private 54.55 43.18 0.003 16 56.82 57.95 0.461 8
Source Authors’ elaboration on IFLS data.Note The table reports the share of procedures correctly identified (that is, either mentioned spontaneously or when prompted) across physicians
in PHC interviewed in both waves of the survey (see Box 1 for the methodology); p-values indicate the level of statistical significance of the difference between the measures in 2007 and 2014 (from one-tail t-test); No. indicates the number of physicians interviewed in each wave.

65
APPENDIXES
Table A2 The quality of PHC workers is worse in private than public sector
(Share of basic questions on three types of curative cares answered correctly by physicians in primary care facilities)
National Java-Bali Sumatra Other
2007 2014 2007 2014 2007 2014 2007 2014
Prenatal Care
Public 46.44 47.47 46.93 49.13 41.85 42.44 49.03 41.87
Private 44.39 34.30 44.44 33.65 42.48 32.83 48.61 46.05
p-(Publ.-priv. diff.) 0.0572 0.0000 0.0609 0.0000 0.4131 0.0003 0.4467 0.1294
Child Curative Care
Public 65.73 61.14 66.90 63.40 58.25 55.47 68.14 57.58
Private 65.45 55.35 66.07 55.87 59.29 50.73 69.81 60.16
p-(Publ.-priv. diff.) 0.4090 0.0000 0.2701 0.3682 0.3737 0.0615 0.3085 0.2477
Adult Curative Care
Public 57.65 52.29 59.70 54.41 51.90 47.13 54.07 48.66
Private 58.54 45.72 58.62 46.23 56.49 40.64 60.93 51.52
p-(Publ.-priv. diff.) 0.2151 0.0000 0.2114 0.0000 0.0489 0.0074 0.0174 0.2177
Source Authors’ elaboration on IFLS data.Note The table reports the share of procedures correctly identified (that is, either mentioned spontaneously or when prompted) across all primary
physicians interviewed in primary care facilities (see Box 1 for the methodology); p-values indicate the level of statistical significance of the difference between the measures in 2007 and 2014 (from one-tail t-test).

66
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Annex 2The main private sector associations in health services
THE INDONESIAN DOCTORS ASSOCIATION (IDI – IKATAN DOKTER INDONESIA)
IDI is Indonesia’s largest doctors association for GPs, specialist doctors, dentists, and dental surgeons. It advances public health and advocates for the interests and professional development of Indonesian physicians. It is the umbrella organization under which all specialist doctor associations come under (see Table A3).
IDI works closely with the MoH to coordinate public health policy and best practices, acting as the gatekeeper for labor policies that affect doctors specifically and health care workers. It also works closely with universities and shapes medical education guidelines and provides guidance and mentorship to junior doctors seeking further education and specialty studies. In recent years, IDI has pushed to improve medical competence with the emergence of new technologies and medical devices and holds regular seminars and conferences in conjunction with pharmaceutical companies, medical device manufacturers, and health care service providers.
PERSI
PERSI’s primary function is to assist and guide existing and new private hospitals in accreditation and hospital management, human resource guidance, and training in administration and operations. Since the implementation of JKN in 2014, PERSI has been working closely with KARS to advise hospitals on accreditation procedures and the integration of BPJS - K for qualified hospitals.
ASSRI
ASSRI encompasses all private sector hospitals and works with service providers to inform the public about the quality and excellent service of Indonesian private hospitals. Since the implementation of JKN, ASSRI has been guiding private hospitals to provide transparent information to the public about the services provided and coverage under BPJS. Due to the budgetary constraints facing BPJS – K over the past two years, ASSRI has shifted focus to assisting private hospitals in dealing with financial shortfalls stemming from delayed payments and also to encourage constructive dialogue between private providers that have so far remained reluctant to work with BPJS. Since the implementation of INA-CBG in November 2018, ASSRI has been working with private providers of specialist services to develop fee structures that are in line with the requirements of BPJS - K coverage, without adding to financial gaps in the costs that hospitals incur in providing these services.

67
APPENDIXES
Table A3 Specialist provider association groups
Association Name
PDPI The Indonesian Association of Pulmonologist
PDSRI The Indonesian Radiology Association
API The Indonesian Association of Pathologists
POGI The Indonesian Society of Obstetrics and Gynecology
PERHATI - KL The Indonesian Orthoinongological Society
PERDOSKI The Indonesian Society of Dermatology & Venereology
PAPDI The Indonesian Society of Internal Medicine
PERKI The Indonesian Heart Association
IDAI The Indonesian Society of Pediatricians
IAUI The Indonesian Urological Association
KABI The Indonesian Surgeon Association
PERDATIN The Indonesian Society of Anesthesiologists
PABOI The Indonesian Orthopedic Association
PERSPEBSI The Indonesian Association of Neurosurgeons
PERDOSSI The Indonesian Neurological Association
PERDOPSI The Indonesian Association of Aviation Medicine Specialists
PERDOSRI The Indonesian Physical Medicine and Rehabilitation Association
PERDOKLA The Association of Marine Doctors
PERAPI The Indonesian Association of Plastic Surgeons
PKNI The Indonesian Association of Nuclear Medicine
PAMKI The Indonesian Society of Clinical Microbiology
PDS PARKI The Indonesian Society for Medical Specialists in Clinical Parasitology
DFI The Indonesian Association of Forensic Medicine
PERDOKI The Indonesian Association of Occupational Medicine
PDS PATKLIN The Indonesian Association of Clinical Pathologist
PDGKI The Indonesian Association of Clinical Nutrition Doctors
PERDAFKI The Indonesian Clinical Pharmacology Association
PERSANDI The Indonesian Andrology Association
PERDAMI The Indonesian Ophthalmologist Association
PDSKJI The Indonesian Psychiatry Association
PDSKO The Indonesia Sports Medicine Association
PABI The Indonesian General Surgeons Society
PERBANI The Indonesian Society of Pediatric Surgeons
PORI The Indonesian Association of Radiology Oncologists

68
PARTNERSHIPS FOR A HEALTHIER INDONESIAUnlocking Constraints for Better Private Sector Participation
Afifi, N. H., R. Busse, and A. Harding. 2003. “Chapter 4: Regulation of Health Services.” In Private Participation in Health Services, edited by A. Harding and A. Preker. Washington, DC: World Bank.
Almuzaini, T., I. Choonara, and H. Sammons. 2013. “Substandard and Counterfeit Medicines: A Systematic Review of the Literature.” BMJ Open
Sahadewo, G. et. al. 2018. The Economics of Tobacco Taxation and Employment in Indonesia. Jakarta: World Bank.
Basu, S. et al. 2012. “Comparative Performance of Private and Public Healthcare Systems in Low and Middle Income Countries: A Systematic Review.” PlosMedicine 9 (6).
Berendes, S., P. Heywood, S. Oliver, and P. Garner. 2011. “Quality of Private and Public Ambulatory Health Care in Low and Middle Income Countries: Systematic Review of Comparative Studies.” PlosMed 8 (4).
Britton, K., S. Koseki, and A. Dutta. 2018. Expanding Markets while Improving Health in Indonesia: Private Health Sector Market in the JKN Era. Washington, DC: Palladium, Health Policy Plus and Jakarta, Indonesia: TNP2K.
Cali, M., and M. Stern. 2009. “Trade in health services and health systems: does regulation hinder or help? Some evidence from developing countries.” Overseas Development Insitute.
Chanda, R. 2002. “Trade in Health Services.” Bulletin of the World Health Organization 80:158–163.
References
Doherty, J., and D. McIntyre. 2013. “Addressing the Failings of Public Health Systems: Should the Private Sector be An Instrument of Choice?” In Social Policy in a Developing World. Cheltenham, edited by D. Surender and R. Walker. U.K.: Edward Elgar, 101–124.
Herrera, C., G. Rada, L. Kuhn-Barrientos, and X. Barrios. 2014. “Does Ownership Matter? An Overview of Systematic Reviews of the Performance of Private for-Profit, Private Not-for-Profit and Public Healthcare Providers.” PlosONE 9 (12).
Hidayat, B., N. J. Mundiharno, V. Rabovskaja, C. S. Rozanna, and J. Spatz. 2015. “Financial Sustainability of the National Health Insurance in Indonesia: A First Year Review.” Jakarta: Indonesian-German Social Protection Programme (SPP).
Lim, J., S. Sharma, T. Coyler, and S. Lee. 2018. The Future of The Indonesian Healthcare Ecosystem. Olivier Wyman.
Patouillard, E., C. Goodman, K. Hanson, and A. Mills. 2007. “Can Working with the Private for-Profit Sector Improve Utilization of Quality Health Services by the poor? A Systematic Review of the Literature.” International Journal for Equity in Health 6 (17).
Presisi and University of Adelaide. 2018. “Indonesia’s Education and Health Services: Policy and Performance.” Unpublished Report for the World Bank.

69
Rajan, V. S, A. Patil, E. S. Pambudi, and B. Junedi. 2018. Is Indonesia Ready to Serve?: An Analysis of Indonesia’s Primary Health Care Supply-Side Readiness (English). Washington, DC: World Bank Group.
Schoeps, A., S. Gabrysch, L. Niamba, A. Sié, and H. Becher. 2011. “The Effect of Distance to Health-Care Facilities on Childhood Mortality in Rural Burkina Faso.” American Journal of Epidemiology 173 (5): 492–498.
Tandon, A. et. al. 2016. Indonesia Health Financing Systems Assessment. Washington, DC: World Bank.
Torchia, M., A. Calabro, and M. Morner. 2013. “Public-Private Partnerships in the Health Care Sector: A Systematic Review of the Literature.” Public Management Review 14 (48).
Wadge, H., R. Roy, A. Sripathy, M. Prime, A. Carter, G. Fontana, J. Mart, and K. Chalkidou. 2017. Evaluating the impact of private providers on health and health systems. London, U.K.: Imperial College London.
West, D. 2015. Digital Divide: Improving Internet Access in the Developing World through Affordable Services and Diverse Content. Washington, DC: Brookings Institution.
WHO and MoH Indonesia, 2018. “Presentation on the Indonesia National TB program.” April 11.
World Bank. 2010. New Insights into the Provision of Health Services in Indonesia: A Health Workforce Study. Washington, DC: World Bank Group.
———. 2014. The Production, Distribution, and Performance of Physicians, Nurses and Midwives in Indonesia: An Update. Jakarta: World Bank.
———. 2016. Indonesia Health Financing System Assessment: Spend More, Spend Right, Spend Better. Jakarta: World Bank.
———. 2018a. Indonesia Economic Quarterly: Strengthening Competitiveness (English). Indonesia Economic Quarterly. Jakarta: World Bank.
———. 2018b. Infrastructure Sector Assessment Republic of Indonesia. Jakarta: World Bank.
———. 2018c. Overview of Strategic Purchasing Functions Under JKN. Jakarta. World Bank.
———. 2018d. Purchasing of Primary Health Care Under JKN. Jakarta. World Bank
———. 2019. Indonesia Public Expenditure Review.


