update on type 2 diabetes - psnc main...
TRANSCRIPT

Update on Type 2 Diabetes
North Staffs and Stoke LPC Keele Hall
17th June 2015
Karon Gilkes Senior Medical Liaison Manager
Boehringer Ingelheim

Content * Key facts and figures around Type 2 Diabetes
* Treatment Guidelines for T2D * Pros and Cons of different treatment classes
UK/EMP/00073 July 2014
References 1. Diabetes UK. Diabetes in the UK 2012. Available at: http://www.diabetes.org.uk/Documents/Reports/Diabetes-in-the-UK-2012.pdf (Accessed April 2014) 2. Diabetes UK. Diabetes: Facts and Stats (Version 3. Revised: March 2014). Available at: http://www.diabetes.org.uk/Documents/About%20Us/Statistics/Diabetes-key-stats-guidelines-April2014.pdf (Accessed June 2014) 3. Prevention and early diagnosis of type 2 diabetes. The NHS health check programme: let’s get it right. September 2012.
Available at: http://www.diabetes.org.uk/Documents/Reports/nhs-health-check-lets-get-it-right-0912.pdf (Accessed April 2014)
Diabetes is one of the biggest health challenges facing the UK1
● Currently 3.2 million people are living with the condition2
● About 630,000 people with diabetes remain undiagnosed2
● At diagnosis, half of the people with type 2 diabetes show signs of complications2
– Diabetes costs the NHS over £10 billion a year2
– This is approximately 10% of the NHS budget2
– 80% of these costs are spent on complications3

UK/EMP/00073 July 2014
Reference Diabetes UK. Diabetes: Facts and Stats (Version 3. Revised: March 2014). Available at: http://www.diabetes.org.uk/Documents/About%20Us/Statistics/Diabetes-key-stats-guidelines-April2014.pdf (Accessed June 2014)

UK/EMP/00073 July 2014
By 2025, it is estimated that five million people will have diabetes in the UK
UK/EMP/00073 June 2014
Reference Diabetes UK. Diabetes: Facts and Stats (Version 3. Revised: March 2014). Available at: http://www.diabetes.org.uk/Documents/About%20Us/Statistics/Diabetes-key-stats-guidelines-April2014.pdf (Accessed June 2014)
UK/EMP/00073 July 2014

UK/EMP/00073 July 2014
Reference Preventing type 2 diabetes: population and community-level interventions. NICE public health guideline 35. Available at: www.guidance.nice.org.uk/ph35 (Accessed June 2014)
Individual risk factors for type 2 diabetes
● Weight - a body mass index of 25 kg/m2 or more
● A large waist circumference
– more than 80 cm (31.5 in) in women
– more than 94 cm (37 in) in men
● Low physical activity levels
● A family history of type 2 diabetes
● A history of gestational diabetes
● Age
– being older than 40, or
– older than 25 for some black and minority ethnic groups
UK/EMP/00073 July 2014
References 1. Stratton IM et al. on behalf of the UK Prospective Diabetes Study Group. BMJ 2000;321:405–12; 2. Jeerakathil T et al. Stroke 2007;38(6):1739–1743. 3. World Heart Federation. Cardiovascular Risk Factors – Diabetes. Available at: www.worldheart.org/cardiovascular-health/cardiovascular-disease-risk-factors/diabetes/ (Accessed May 2010) 4. Hovind P et al. Kidney Int 2001;59(2):702–709; 5. Fong DS et al., Diabetes Care. 2004;27(10):2540–2553; 6. Deshpande AD et al. Phys Ther 2008;88:1254–1264. 7. Adler AI et al. on behalf of the UK Prospective Diabetes Study Group. BMJ 2000;321:412-9. 8. Peripheral artery disease. Available at: www.diabetes.co.uk/diabetes-complications/peripheral-artery-disease.html (Accessed June 2014) 9. Dang CN et al., Int J Low Extrem Wounds 2003;2(1):4-12.
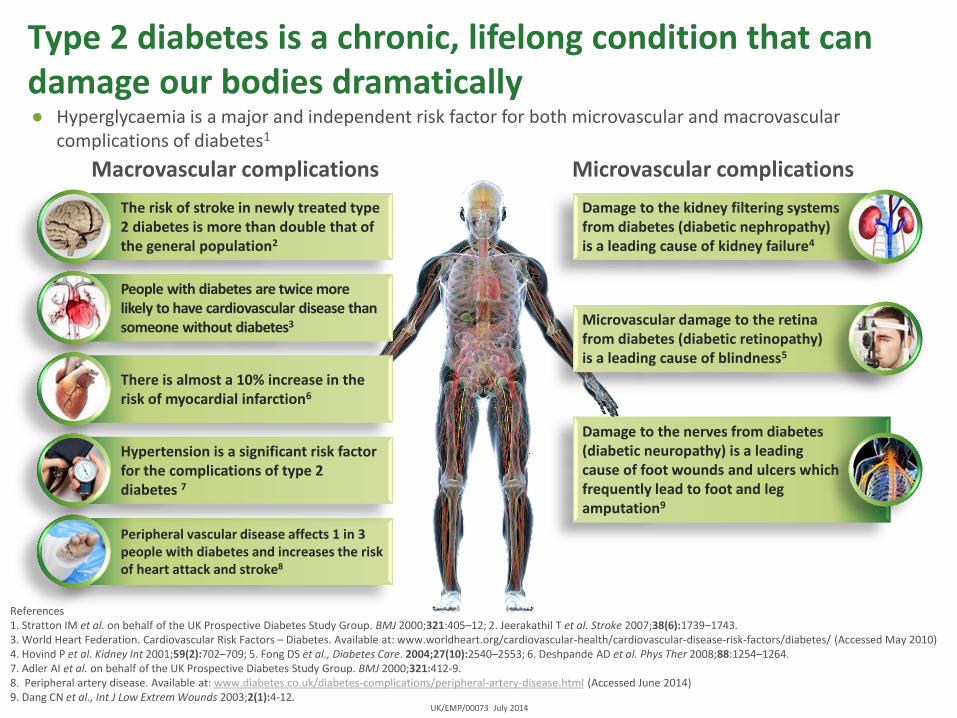
Type 2 diabetes is a chronic, lifelong condition that can damage our bodies dramatically ● Hyperglycaemia is a major and independent risk factor for both microvascular and macrovascular
complications of diabetes1
Macrovascular complications Microvascular complications
The risk of stroke in newly treated type 2 diabetes is more than double that of the general population2
Peripheral vascular disease affects 1 in 3 people with diabetes and increases the risk of heart attack and stroke8
Damage to the kidney filtering systems from diabetes (diabetic nephropathy) is a leading cause of kidney failure4
Microvascular damage to the retina from diabetes (diabetic retinopathy) is a leading cause of blindness5
Damage to the nerves from diabetes (diabetic neuropathy) is a leading cause of foot wounds and ulcers which frequently lead to foot and leg amputation9
People with diabetes are twice more likely to have cardiovascular disease than someone without diabetes3
There is almost a 10% increase in the risk of myocardial infarction6
Hypertension is a significant risk factor for the complications of type 2 diabetes 7

UK/EMP/00073 July 2014
Reference National Health and Nutrition Examination Surveys (NHANES), USA 1999-2004 Adapted from Deshpande AD et al. Phys Ther 2008;88:1254–1264.
Prevalence of diabetes-related complications among people with type 2 diabetes
Pe
rce
nta
ge w
ith
co
mp
licat
ion
s (%
)
UK/EMP/00073 July 2014
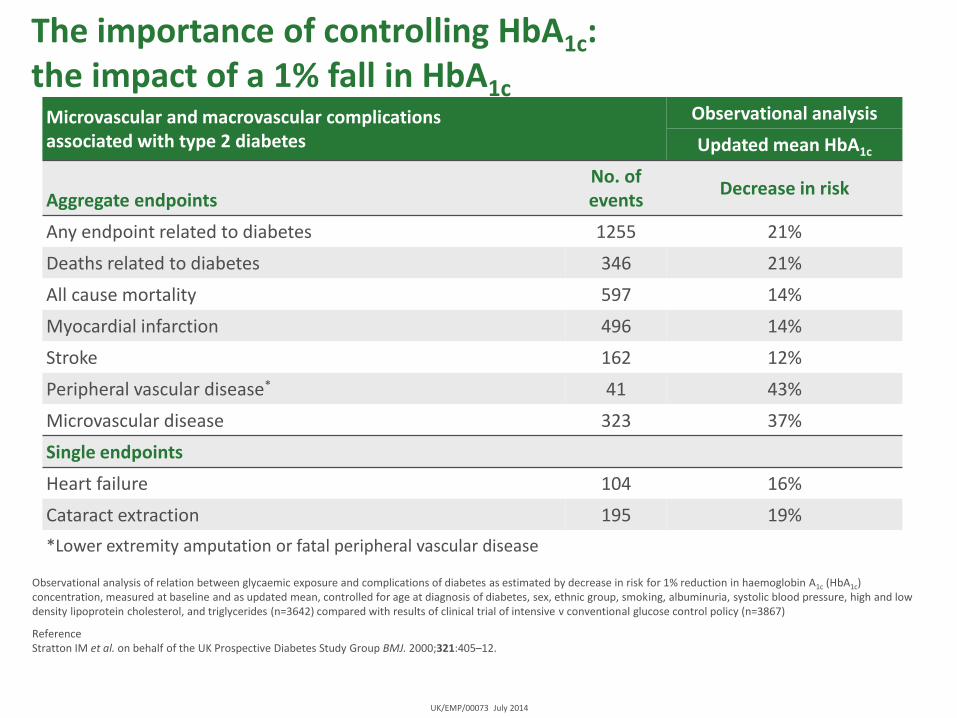
Microvascular and macrovascular complications associated with type 2 diabetes
Observational analysis
Updated mean HbA1c
Aggregate endpoints
No. of events
Decrease in risk
Any endpoint related to diabetes 1255 21%
Deaths related to diabetes 346 21%
All cause mortality 597 14%
Myocardial infarction 496 14%
Stroke 162 12%
Peripheral vascular disease* 41 43%
Microvascular disease 323 37%
Single endpoints
Heart failure 104 16%
Cataract extraction 195 19%
*Lower extremity amputation or fatal peripheral vascular disease
The importance of controlling HbA1c: the impact of a 1% fall in HbA1c
Observational analysis of relation between glycaemic exposure and complications of diabetes as estimated by decrease in risk for 1% reduction in haemoglobin A1c (HbA1c) concentration, measured at baseline and as updated mean, controlled for age at diagnosis of diabetes, sex, ethnic group, smoking, albuminuria, systolic blood pressure, high and low density lipoprotein cholesterol, and triglycerides (n=3642) compared with results of clinical trial of intensive v conventional glucose control policy (n=3867)
Reference Stratton IM et al. on behalf of the UK Prospective Diabetes Study Group BMJ. 2000;321:405–12.

UK/EMP/00073 July 2014
NICE goals for effective management of type 2 diabetes and current treatment options

UK/EMP/00073 July 2014
Reference TYPE 2 DIABETES: National clinical guideline for management in primary and secondary care (update). Available at: http://www.nice.org.uk/nicemedia/live/11983/40803/40803.pdf (Accessed June 2014)
NICE goals of treatment
To manage type 2 diabetes through the effective control of:
● Blood glucose
– Initial HbA1c target: <6.5%
● Hypertension
– Target: <140/80 mmHg <130/80 mmHg if kidney, eye or cerebrovascular damage
● Blood lipids
– Target: <4.0 mmol/L TC <2.0 mmol/L LDL
● Antithrombotic therapy
– Offer low-dose aspirin (75 mg) to patients >50yrs if BP<145/90 mmHg or <50yrs with significant other CV risk

HbA1c target for people with type 2 diabetes recommended by NICE
• Individualised HbA1c target – may be above the general target of 48 mmol/mol (6.5%)
• HbA1c monitored every 2–6 months until stable on unchanging therapy
• HbA1c monitored every 6 months once blood glucose level and therapy are stable
NICE guideline on type 2 diabetes
• Personalised HbA1c target – usually between 48 mmol/mol and 58 mmol/mol (6.5% and 7.5%)
• Ongoing treatment review to minimise hypoglycaemia
NICE quality standard for diabetes
NICE (2009) Type 2 diabetes: The Management of Type 2 Diabetes. NICE Clinical Guidance 87. Available at: http://nice.org.uk/cg87 (accessed: 12.05.2015); NICE (2011) Diabetes in adults quality standard. Available at: http://bit.ly/1bbFunM (accessed 12.05.2015)
Job code: UK/DIA/00242i. Date of preparation: May 2015.
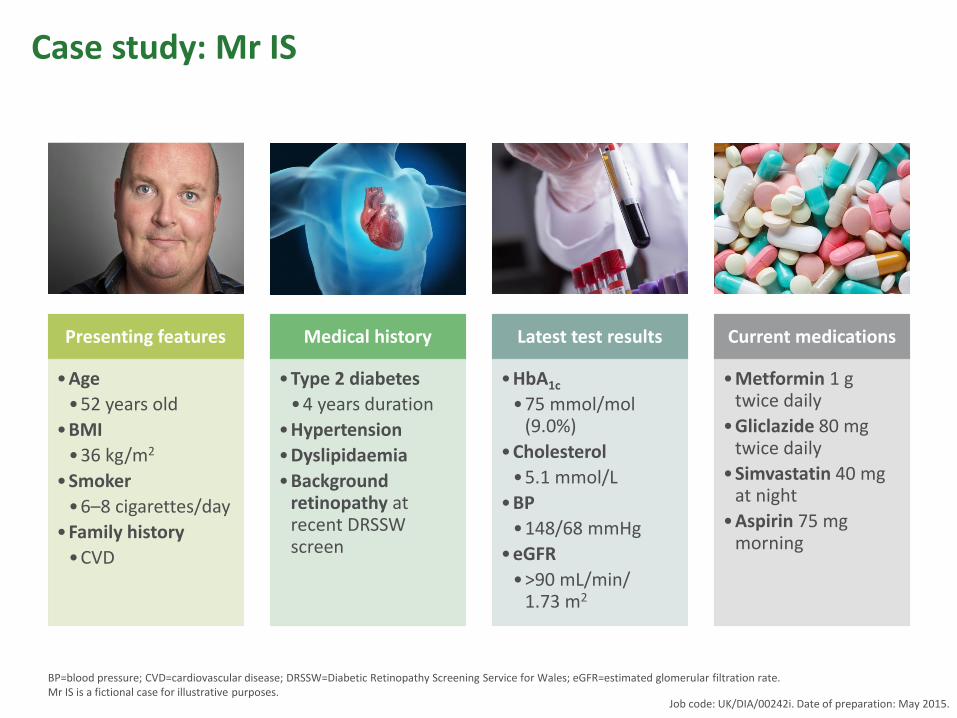
Case study: Mr IS
BP=blood pressure; CVD=cardiovascular disease; DRSSW=Diabetic Retinopathy Screening Service for Wales; eGFR=estimated glomerular filtration rate. Mr IS is a fictional case for illustrative purposes.
Presenting features
•Age
•52 years old
•BMI
•36 kg/m2
•Smoker
•6–8 cigarettes/day
•Family history
•CVD
Medical history
•Type 2 diabetes
•4 years duration
•Hypertension
•Dyslipidaemia
•Background retinopathy at recent DRSSW screen
Latest test results
•HbA1c
•75 mmol/mol (9.0%)
•Cholesterol
•5.1 mmol/L
•BP
•148/68 mmHg
•eGFR
•>90 mL/min/ 1.73 m2
Current medications
•Metformin 1 g twice daily
•Gliclazide 80 mg twice daily
•Simvastatin 40 mg at night
•Aspirin 75 mg morning
Job code: UK/DIA/00242i. Date of preparation: May 2015.

Achievement of therapeutic targets
• 2012/13 National Diabetes Audit
– 62.4% HbA1c <7.5%
– 76.2% Cholesterol <5mmol/l
– 69.0% BP <140/80
• What percentage of patients met all 3 of the above targets ?

Interventional relationships between cholesterol,
blood pressure and HbA1c with CVD events
119
44
34
0 50 100 150
0.9% reduction in HbA1c
1 mmol/L reduction in cholesterol
10/5 mmHg reduction in BP
NNT for 5 years in order to prevent 1 CVD event
For each variable, data shown are for a change corresponding to the mean change of the variable in intervention studies.
BP=blood pressure; CVD=cardiovascular disease; NNT=number needed to treat.
Adapted from Yudkin JS et al (2010) Diabetologia 53: 2079–85

Dat
e o
f p
rep
arat
ion
: May
20
15
UK
/DIA
/00
25
2h
Biosimilars
Exenatide
Repaglinide
▼Dapagliflozin
▼Liraglutide
▼Canagliflozin
▼Degludec
Insulin
Protamine Zn Insulin
Sulphonvlureas
Metformin
Biguanides Human Insulin
Metformin
Acarbose
Rosiglitazone Lantus (insulin glargine)
Insulin detemir
Exenatide
Pramlintide
Sitagliptin
Saxagliptin
Nu
mb
er o
f n
ew t
her
apie
s
1921 1932 1957 1952 1970 1983 1995 1999 2000 2002 2005 2006 2009 2010 2012 2014
▼Empagliflozin
▼Linagliptin
Limitations of older therapies
• Weight gain (SU1, TZD2, insulin3)
• Hypoglycaemia (SU1, insulin3)
• Concerns over CV safety (TZD2)
• Concerns over cancer risks (TZD2, some insulins3)
• Limited options in patients with renal disease4
• Natural history of disease not altered
1. Smith CJ, et al. Br J Cardiol 2010;17:279-82.; 2. McGrane D, et al. Br J Cardiol 2011;18:24–7.; 3. Barwell N, et al. Br J Cardiol 2010;18:224-8.-82;
4. Marshall SM. B J Renal Med 2011;16:28–31.

UK/EMP/00073 July 2014
References 1. Nathan DM et al. Diabetes Care 2009; 32:193–203. 2. Wulffele MG et al. J Intern Med 2004; 256: 1–14; 3. 3. Victoza (liraglutide) Summary of Product Characteristics. Available at: www.medicines.org.uk/emc (Accessed June 2014) 4. JARDIANCE (empagliflozin) Summary of Product Characteristics 5. Valentine V. Clinical Diabetes 2012 30:151–155. 6. Phillips P et al. Diabetes Care 2003;26:269–273. 7. Acarbose Summary of Product Characteristics. Available at: www.medicines.org.uk/emc (Accessed June 2014) 8. Kurukulasuriya LR, Sowers JR. Cardiovasc Diabetol 2010; 9:45. 9. The Cochrane Colloboration. Meglitinide analogues for type 2 diabetes mellitus (Review) 10. Prandin (replaginide) Summary of Product Characteristics. Available at: www.medicines.org.uk/emc (Accessed June 2014) 11. Inzucchi SE, McGuire DK. Circulation 2008; 117:574-84.
Treatment options in the management of type 2 diabetes
Class HbA1c
reduction
Increased risk of hypo-
glycaemia
Weight change
Systolic blood pressure change
Metformin 1.0 – 2.01 X1 Neutral1 Neutral2
Sulphonylurea 1.0 – 2.01
1 Gain1 Not reported
TZDs 0.5 – 1.41 X1 Gain1 Not reported
DPP-4 inhibitors 0.5 – 0.81 X1 Neutral1 Not reported
GLP-1 agonists 0.5 – 1.01 X1 Loss1 Reduction3
Long acting insulin 1.5 – 3.51
1 Gain1 Not reported
Rapid acting insulin 1.5 – 3.51 1 Gain1 Not reported
SGLT2 inhibitors 0.5 – 1.14 X4 Loss5 Reduction5
Acarbose 16 X7 Loss8 Not reported
Meglitinides 0.1 – 2.19
10 Gain11 Not reported
Adapted from: Nathan DM et al. Diabetes Care 2009 32:193–203

UK/EMP/00073a July 2014
Drug treatments for type 2 diabetes and their sites of action
DPP-4, dipeptidyl peptidase-4; GLP-1, glucagon-like peptide-1; SGLT2, sodium-glucose co-transporter 2
Reference Tahrani AA, et al. Lancet. 2011;378:182–197.
Hyperglycaemia
Increased glucose
production
Glucose absorption
Impaired insulin
secretion
Decreased glucose uptake
Increased glucose reabsorption
Acarbose
Metformin Pioglitazone Insulin
SGLT2 inhibitors Insulin Sulphonylureas
Meglitinides GLP-1 receptor agonists
DPP-4 inhibitors
Metformin GLP-1 receptor agonists
DPP-4 inhibitors Insulin

National Institute for Health and Clinical Excellence (NICE):
T2D treatment algorithm1
Consider substituting
DPP-4 or TZD for SU if:
• Risk of hypoglycaemia
or SU is
contraindicated or not
tolerated
Consider SU if:
• Not overweight
• MET not tolerated
• Rapid response
needed because of
hypoglycaemic
symptoms
1. Adapted from: National Institute for Health and Clinical Excellence. Clinical Guideline 87. Type 2 diabetes - newer
agents (a partial update of CG66): quick reference guide.
MET = metformin, SU = sulphonylureas, TZD = thiazolidinedione, DPP-4= dipeptidyl peptidase-4 inhibitor
Insulin + MET + SU
MET + SU + sitagliptin, or
MET + SU + TZD, or
MET + SU + exenatide
HbA1c
≥7.5%
HbA1c
≥7.5%
Consider adding sitagliptin
or TZD:
• Instead of insulin if insulin is
unacceptable
Consider adding exenatide
to MET and SU if
• BMI ≥35kg/m2 or BMI <35
kg/m2 and insulin
unacceptable
Start insulin
MET +
DPP-4 or TZD
MET
MET + SU
HbA1c
≥7.5%
HbA1c
≥6.5%
HbA1c ≥6.5% after
lifestyle intervention
SU
SU + DPP-4
or TZD
Consider adding
DPP-4 or TZD if: • MET not tolerated
or contraindicated
HbA1c
≥6.5%
HbA1c
≥7.5%
HbA1c
≥7.5%
Increase insulin dose and intensify regimen.
Consider adding pioglitazone if:
• A TZD has previously had marked effect or blood
glucose control is inadequate with high-dose insulin HbA1c
≥7.5%
20
2012: Updated joint 2012 position statement
from the ADA and EASD
• “…an update was deemed necessary because of contemporary information on the benefits/risks of glycemic control, recent evidence concerning efficacy and safety of several new drug classes, the withdrawal/restriction of others, and increasing calls for a move toward more patient-centered care.”
• “…individualization of treatment is the cornerstone of success.”
• “Our recommendations are less prescriptive than and not as algorithmic as prior guidelines. This follows from the general lack of comparative effectiveness research in this area.”
ADA=American Diabetes Association; EASD=European Association for the study of Diabetes.
Inzucchi SE et al (2012) Diabetes Care 35: 1364–79

ADA/EASD: Approach to the management
of hyperglycaemia
ADA=American Diabetes Association; EASD=European Association for the study of Diabetes.
Adapted from: Inzucchi SE et al (2012) Diabetes Care 35: 1364–79
More stringent Less stringent
Patient attitude and
expected treatment efforts
Risks potentially associated
with hypoglycaemia, other
adverse events
Disease duration
Life expectancy
Important comorbidities
Established vascular
complications
Resources, support system Readily available Limited
Severe
Severe
Short
Long-standing
High
Less motivated, non-adherent,
poor self-care capacities
Absent
Absent
Long
Newly diagnosed
Low
Highly motivated, adherent,
excellent self-care capacities

ADA/EASD: Antihyperglycaemic therapy in
type 2 diabetes – general recommendations
ADA=American Diabetes Association; DPP-4=dipeptidyl peptidase-4; EASD=European Association for the study of Diabetes; GLP-1=glucagon-
like peptide-1; SU=sulphonylurea; TZD=thiazolidinedione.
Inzucchi SE et al (2012) Diabetes Care 35: 1364–79

Weight gain with sulphonylureas, meglitinides, thiazolidinediones and insulin
● An increase in body weight was observed all second-line therapies except DPP-4 inhibitors, alpha-glucosidase inhibitors and GLP-1 analogues
CrI=credible interval; DPP-4=dipeptidyl peptidase-4; GLP-1=glucagon-like peptide-1. Mixed-treatment comparison (MTC) results showing the effect of adding second-line agents versus placebo in adults taking metformin on change from baseline in bodyweight (kg). MTC analysis based on 30 randomised controlled trials (n=15,265). Most trials were 6–12 months long. Overall, meta-regression and sensitivity analyses yielded minimal differences from the reference case. Adapted from: McIntosh B et al (2011) Open Medicine 5: E35–48
Sulphonylureas 2.01 (1.09, 2.94)
Meglitinides 1.80 (0.35, 3.29)
Thiazolidinediones 2.59 (1.66, 3.51)
DPP-4 inhibitors 0.57 (–0.45, 1.60)
Alpha-glucosidase inhibitors –0.92 (–2.35, 0.51)
GLP-1 analogues –1.79 (–3.43, –0.14)
Basal insulin 1.56 (–0.46, 3.63)
Biphasic insulin 2.96 (0.96, 5.00)
–5.0 –2.5 0 2.5 5.0
Treatment MTC estimate (95% CrI) Favours placebo Favours treatment
Difference in change from baseline in body weight kg (95% CI)
Job code: UK/DIA/00242i. Date of preparation: May 2015.
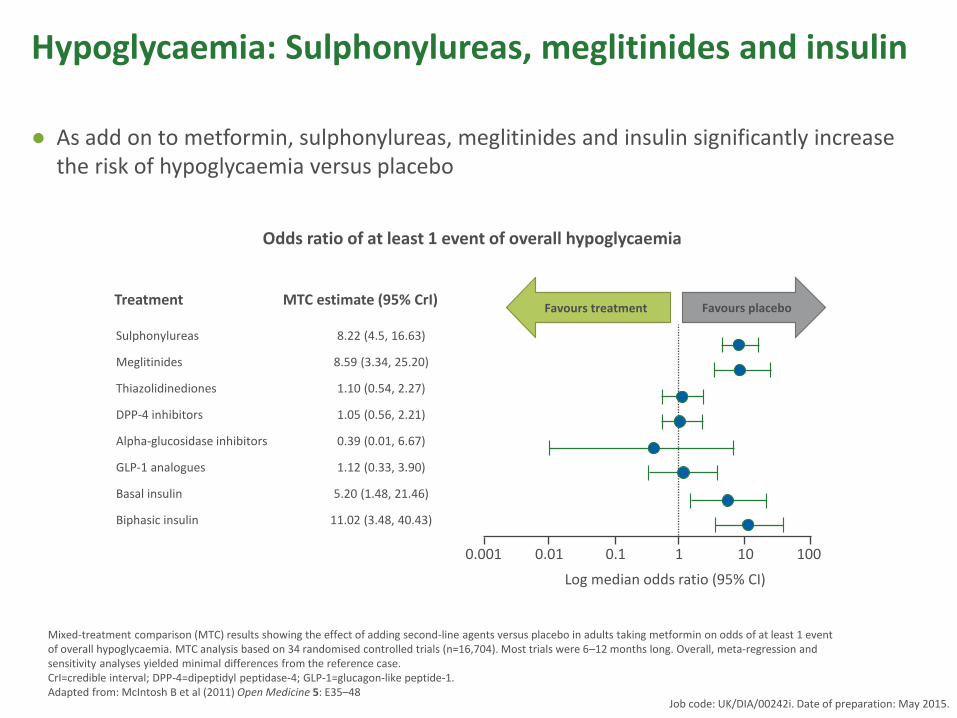
Hypoglycaemia: Sulphonylureas, meglitinides and insulin
● As add on to metformin, sulphonylureas, meglitinides and insulin significantly increase the risk of hypoglycaemia versus placebo
Mixed-treatment comparison (MTC) results showing the effect of adding second-line agents versus placebo in adults taking metformin on odds of at least 1 event of overall hypoglycaemia. MTC analysis based on 34 randomised controlled trials (n=16,704). Most trials were 6–12 months long. Overall, meta-regression and sensitivity analyses yielded minimal differences from the reference case. CrI=credible interval; DPP-4=dipeptidyl peptidase-4; GLP-1=glucagon-like peptide-1. Adapted from: McIntosh B et al (2011) Open Medicine 5: E35–48
Sulphonylureas 8.22 (4.5, 16.63)
Meglitinides 8.59 (3.34, 25.20)
Thiazolidinediones 1.10 (0.54, 2.27)
DPP-4 inhibitors 1.05 (0.56, 2.21)
Alpha-glucosidase inhibitors 0.39 (0.01, 6.67)
GLP-1 analogues 1.12 (0.33, 3.90)
Basal insulin 5.20 (1.48, 21.46)
Biphasic insulin 11.02 (3.48, 40.43)
0.001 0.01 0.1 1 10 100
Treatment MTC estimate (95% CrI) Favours placebo Favours treatment
Log median odds ratio (95% CI)
Odds ratio of at least 1 event of overall hypoglycaemia
Job code: UK/DIA/00242i. Date of preparation: May 2015.

ADA/EASD: Recommendations for antihyperglycaemic therapy
ADA=American Diabetes Association; DPP-4=dipeptidyl peptidase-4; EASD=European Association for the Study of Diabetes; GLP-1 RA=glucagon-like peptide-1 receptor agonist; SGLT2=sodium-glucose co-transporter-2; SU=sulphonylurea; TZD=thiazolidinedione. Adapted from: Inzucchi SE et al (2015) Diabetes Care 38: 140–9
Job code: UK/DIA/00242i. Date of preparation: May 2015.

Factors to be taken into consideration when
selecting an appropriate drug
Person with type 2
diabetes
Age
Occupation
Hobbies
Sex
Past medical history (e.g. haematuria/
cancer)
Renal function
Fasting
Live alone/nutritio
n
Driving
Liver function
BMI / body weight
Fracture risk
The series of considerations above was
generated by the programme committee.
Aims of treatment of
hyperglycaemia in
Type 2 Diabetes
Symptom control
Prognosis
Side effects
Adherence
The ideal diabetes drug?
• blood glucose • βcell function • insulin resistance • Without hypoglycaemia • Give durable control • Well tolerated • Convenient to take • Weight loss/no weight gain • Able to be used in
challenging patient populations eg elderly, renal and hepatic impairment, other co-morbidities
• blood pressure
• LDL cholesterol
• HDL and trigs
• Cheap
• Trialed and licensed for use with all other combinations of diabetes drugs
• Long term data showing improvements in clinical outcomes
Metformin: Advantages and disadvantages
Advantages
•Extensive clinical experience
•No weight gain
•Low inherent risk of hypoglycaemia
•Likely ↓ CVD events (UKPDS)
•Low unit cost
Disadvantages
•Gastrointestinal side-effects (diarrhoea, abdominal cramping)
•Lactic acidosis risk (rare)
•Vitamin B12 deficiency
•Multiple contraindications: CKD, acidosis, hypoxia, dehydration, etc.
CKD=chronic kidney disease; CVD=cardiovascular disease; UKPDS=UK Prospective Diabetes Study.
Adapted from Inzucchi SE et al (2012) Diabetes Care 35: 1364–79
Primary physiological action: ↓ Hepatic glucose production

SUs: Advantages and disadvantages
Advantages
• Extensive clinical experience
• ↓ Microvascular risk (UKPDS)
• Low unit cost
Disadvantages
• Hypoglycaemia
• Weight gain
• Blunts myocardial ischaemic preconditioning
• Low durability
SUs=sulphonylureas; UKPDS=United Kingdom Prospective Diabetes Study.
Adapted from Inzucchi SE et al (2012) Diabetes Care 35: 1364–79
1. British National Formulary (2012) 6.1.2.1 Sulfonylureas. Available at: www.bnf.org (accessed 19.09.2012)
Primary physiological action: ↑ Insulin secretion
Available agents1: glibenclamide, gliclazide, glimepiride, glipizide, tolbutamide

UK Hypoglycaemia Study: Prevalence of
self-reported hypoglycaemia with SU use
SU=sulphonylurea; T1D=type 1 diabetes; T2D=type 2 diabetes.
Adapted from: UK Hypoglycaemia Study Group (2007) Diabetologia 50: 1140–7
SU <2 yr >5 yr <5 yr >15 yr
T1D T2D
SU <2 yr >5 yr <5 yr >15 yr
T1D T2D
Severe hypoglycaemia Mild hypoglycaemia
Pro
po
rtio
n r
ep
ort
ing
at le
ast o
ne
hyp
og
lyca
em
ic e
pis
od
e
39% of patients
receiving an SU
reported mild
hypoglycaemia
7% of patients
receiving an SU
reported severe
hypoglycaemia
Driving and hypoglycaemia with SUs and
meglitinides: Updated DVLA medical rules
• Group 1 drivers:
– Must not have had more than one episode of
hypoglycaemia requiring the assistance of another
person within the preceding 12 months.
– It may be appropriate to monitor blood glucose
regularly and at times relevant to driving to enable
the detection of hypoglycaemia.
– Must be under regular medical review.
• Group 2 drivers: must satisfy the following criteria:
– No episode of hypoglycaemia requiring the
assistance of another person has occurred in the
preceding 12 months.
– Has full awareness of hypoglycaemia.
– Regularly monitors blood glucose at least twice daily
and at times relevant to driving.
– Must demonstrate an understanding of the risks of
hypoglycaemia.
– There are no other debarring complications of
diabetes such as a visual field defect.
The applicant or licence holder must notify DVLA unless stated otherwise in the text
0
DVLA=Driver and Vehicle Licensing Agency; SUs=sulphonylureas.
Drivers Medical Group (2012) At a Glance Guide to the Current Medical Standards of Fitness to Drive. Available at: http://bit.ly/lPWwxf
(accessed 08.08.2012)

This presentation has been developed by Boehringer Ingelheim Ltd. and Eli Lilly Company Ltd. UK/TRJ/00296c. October 2013.
Certain factors are associated with an
increased risk of hypoglycaemia
• Use of insulin secretagogues and insulin therapy
• Behavioural, physiological and therapeutic factors including:
– Missed or irregular meals
– Older age
– Longer duration of diabetes
– Presence of comorbidities
– Loss of residual insulin secretion
– Loss of awareness of hypoglycaemia
– Time of day (lowest plasma glucose of the day is just before the evening
meal and unsuspected hypoglycaemia can occur at this time once drug
therapy is started)
Amiel SA, et al. Diabet Med. 2008; 25(3):245–254.

Acarbose
Advantages1 - Not associated with hypoglycaemia - ↓Postprandial glucose excursions
- Possible cardiovascular benefit - Non-systemic
Adverse effects of note*2 - Flatulence - Diarrhoea
- Gastrointestinal and abdominal pains
Cautions2 - Hypoglycaemia (may potentiate effects
of other antihyperglycaemic agents; episodes may be treated with glucose,
not sucrose) - Liver enzyme monitoring
Contraindications2 - Inflammatory bowel disease, colonic
ulceration, partial intestinal obstruction or in patients predisposed to intestinal
obstruction - Severe hepatic impairment
- Severe renal impairment
Acarbose Slows intestinal carbohydrate digestion and absorption (should be chewed with the first
mouthful of food, or swallowed directly before the meal2)
*Common or very common in summary of product characteristics 1. Inzucchi S et al (2015) Diabetes Care 38: 140–9; 2. Acarbose Summary of Product Characteristics. Available at: http://www.medicines.org.uk/emc (accessed 07.05.2015)
Job code: UK/DIA/00242i. Date of preparation: May 2015.
Meglitinides
Advantages1 - ↓Postprandial glucose excursions
- Dosing flexibility
Adverse effects of note*2
- Hypoglycaemia - Gastrointestinal disturbances
Cautions3 - Substitute insulin during intercurrent
illness and surgery - Debilitated and malnourished patients
- Renal and hepatic impairment
Contraindications3 - Ketoacidosis
- Severe hepatic impairment2
Repaglinide, nateglinide3 ↑Insulin secretion (rapid onset and short duration of action; taken with meals)1,3
*Listed as common in summaries of product characteristics 1. Inzucchi S et al (2015) Diabetes Care 38: 140–9; 2. Summaries of product characteristics for repaglinide and nateglinide, available from http://www.medicines.org.uk/emc (accessed 07.05.2015); 3. British National Formulary (2015) 6.1.2.3 Other antidiabetic drugs. Available at: http://bit.ly/1P3jlMM (accessed 07.05.2015)
Job code: UK/DIA/00242i. Date of preparation: May 2015.
Pioglitazone: Advantages and
disadvantages
Advantages
• Low inherent risk of hypoglycaemia
• Durable glucose lowering
• ↑ HDL-cholesterol
• ↓ Triglycerides
• ↓ CVD events (PROactive)
Disadvantages
• Weight gain
• Oedema/heart failure
• Bone fractures
• ? ↑ Bladder cancer
CVD=cardiovascular disease.
Adapted from Inzucchi SE et al (2012) Diabetes Care 35: 1364–79
Primary physiological action: ↑ Insulin sensitivity
DPP-4 inhibitors: Advantages and
disadvantages
Advantages
•Low inherent risk of hypoglycaemia
•Weight neutrality
•Well tolerated
•CVOT – SAVOR-TIMI, EXAMINE, TECOS
Disadvantages
•High unit cost
•Lack of long-term efficacy and tolerability data
•Concern regarding possible risk of pancreatitis, increased hospitalisations for heart failure
DPP-4=dipeptidyl peptidase-4.
Inzucchi SE et al (2012) Diabetes Care 35: 1364–79
1. British National Formulary (2012) 6.1.2.3 Other antidiabetic drugs. Available at: www.bnf.org (accessed 19.09.2012)
Primary physiological actions: ↑ Insulin secretion (glucose-dependent); ↓ glucagon
secretion (glucose-dependent)
Available agents1: linagliptin, saxagliptin, sitagliptin, vildagliptin

Are all DPP-4 inhibitors the same?
Drug Features Prescribing considerations
Sitagliptin1 Once daily, renal
excretion
Dose reduction in CKD
Vildagliptin2 Twice daily, renal
excretion, liver upset
described
Dose reduction in CKD, LFT
monitoring recommended
Saxagliptin3 Once daily, renal
excretion
Dose reduction in CKD
Linagliptin4 Once daily, biliary
excretion
No dose reduction in CKD
Alogliptin5 Once daily, renal
excretion
Dose reduction in CKD
References 1-5: Summary of Product Characteristics for sitagliptin, vildagliptin, saxagliptin, linagliptin, alogliptin.
Available at www.medicines.org.uk/emc (accessed October 2014)
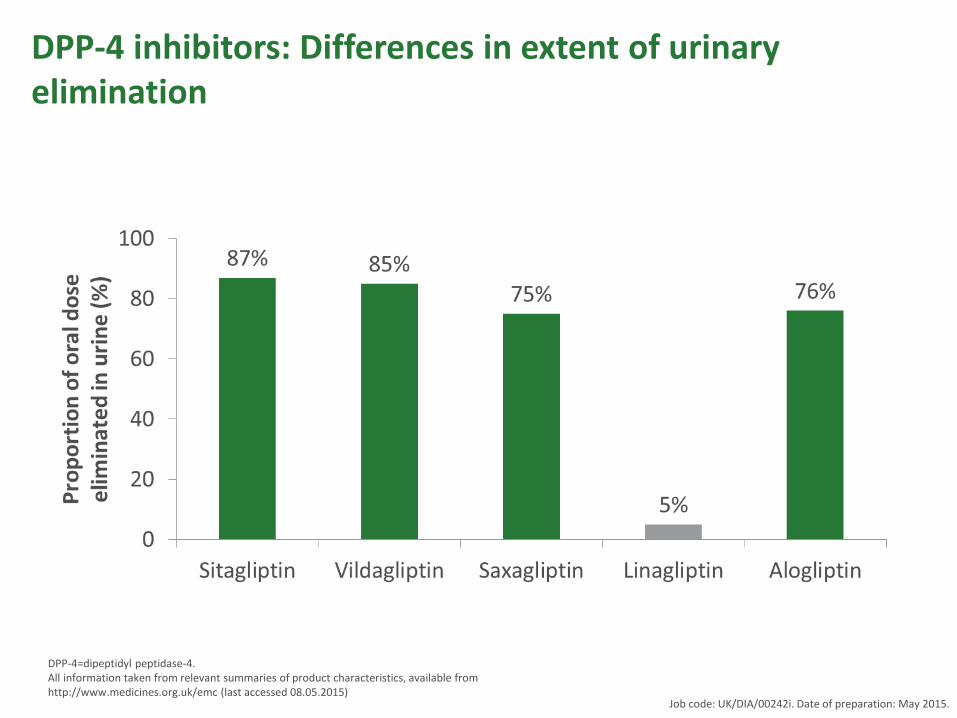
DPP-4 inhibitors: Differences in extent of urinary elimination
DPP-4=dipeptidyl peptidase-4. All information taken from relevant summaries of product characteristics, available from http://www.medicines.org.uk/emc (last accessed 08.05.2015)
Job code: UK/DIA/00242i. Date of preparation: May 2015.

Effect of renal impairment on DPP-4 inhibitor pharmacokinetics
*Estimated creatinine clearance values were calculated using the Cockcroft–Gault formula. ESRD=end-stage renal disease; DPP-4=dipeptidyl peptidase-4; HD=haemodialysis. Adapted from Graefe-Mody U et al (2011) Diab Obes Metab 13: 939–46. Alogliptin became available after this analysis was published and was therefore not included.
Two-fold increase in exposure
Normal n=6
Mild n=8
Moderate n=6
Severe n=6
ESRD n=6
1
2
3
4
5
6
7
Fold
incr
eas
e in
e
xpo
sure
re
lati
ve t
o
no
rmal
re
nal
fu
nct
ion
Linagliptin Sitagliptin
Normal n=6
Mild n=6
Moderate n=6
Severe n=6
ESRD n=6
1
2
3
4
5
6
7
Fold
incr
eas
e in
e
xpo
sure
re
lati
ve t
o
no
rmal
re
nal
fu
nct
ion
Normal n=8
Mild n=8
Moderate n=8
Severe n=7
ESRD n=8
1
2
3
4
5
6
7
Fold
incr
ease
in
exp
osu
re r
ela
tive
to
n
orm
al r
enal
fu
nct
ion
Saxagliptin (5-hydroxy saxagliptin metabolite)
Vildagliptin (LAY151 metabolite)
Normal Mild Moderate Severe ESRD
1
2
3
4
5
6
7
Fold
incr
ease
in
exp
osu
re r
elat
ive
to
no
rmal
re
nal
fu
nct
ion
Creatinine clearance >80 >50 to ≤80 >30 to ≤50 ≤30 ≤30 on HD (mL/min)
Creatinine clearance* >80 >50 to ≤80 >30 to ≤50 ≤30 ≤30 on HD (mL/min)
Creatinine clearance* >80 >50 to ≤80 >30 to ≤50 ≤30 ≤30 on HD (mL/min)
Job code: UK/DIA/00242i. Date of preparation: May 2015.
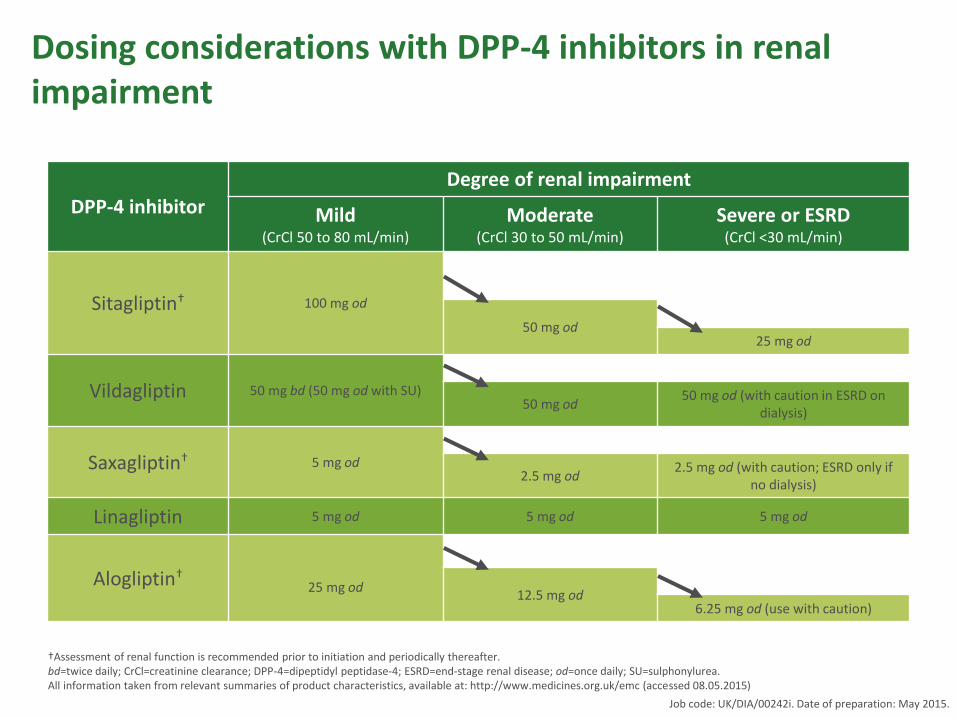
Dosing considerations with DPP-4 inhibitors in renal impairment
DPP-4 inhibitor
Degree of renal impairment
Mild (CrCl 50 to 80 mL/min)
Moderate (CrCl 30 to 50 mL/min)
Severe or ESRD (CrCl <30 mL/min)
Sitagliptin† 100 mg od
50 mg od 25 mg od
Vildagliptin 50 mg bd (50 mg od with SU) 50 mg od
50 mg od (with caution in ESRD on dialysis)
Saxagliptin† 5 mg od 2.5 mg od
2.5 mg od (with caution; ESRD only if no dialysis)
Linagliptin 5 mg od 5 mg od 5 mg od
Alogliptin† 25 mg od
12.5 mg od 6.25 mg od (use with caution)
†Assessment of renal function is recommended prior to initiation and periodically thereafter. bd=twice daily; CrCl=creatinine clearance; DPP-4=dipeptidyl peptidase-4; ESRD=end-stage renal disease; od=once daily; SU=sulphonylurea. All information taken from relevant summaries of product characteristics, available at: http://www.medicines.org.uk/emc (accessed 08.05.2015)
Job code: UK/DIA/00242i. Date of preparation: May 2015.

SGLT2 inhibitors: Advantages and
disadvantages
Advantages
•Low risk of hypos
•Weight reduction
•Blood pressure lowering
•Effect independent of insulin
Disadvantages
•Bacterial urinary tract infections
•Fungal genital tract infections
•Dehydration/nocturia
•Renal function
•Cost
UKPDS=UK Prospective Diabetes Study.
1. British National Formulary (2012) 6.1.1 Insulins. Available at: www.bnf.org (accessed 19.09.2012)
Adapted from Inzucchi SE et al (2012) Diabetes Care 35: 1364–79
Primary physiological actions: decreased renal reuptake of glucose
Available agents1: Dapagliflozin, Canagliflozin, Empagliflozin

Date of preparation: September 2014. UK/EMP/xxxxxx
SGLT2 inhibitors: therapeutic indications
Empagliflozin1 Canagliflozin2 Dapagliflozin3
Monotherapy*
In combination with other
glucose-lowering products
including insulin
(except pioglitazone)
Available doses 10 mg od
25 mg od
100 mg od
300 mg od 10 mg od
References
1. Jardiance® (empagliflozin) Summary of product characteristics.
2. Invokana® (canagliflozin) Summary of Product Characteristics. Available at: http://www.medicines.org.uk/emc/medicine/28400 (accessed August 2014).
3. Forxiga® (dapagliflozin) Summary of Product Characteristics. Available at: http://www.medicines.org.uk/emc/medicine/27188 (accessed August 2014).
*When diet and exercise alone do not provide adequate glycaemic control in patients for whom use of
metformin is considered inappropriate due to intolerance.
Date of preparation: September 2014. UK/EMP/xxxxxx
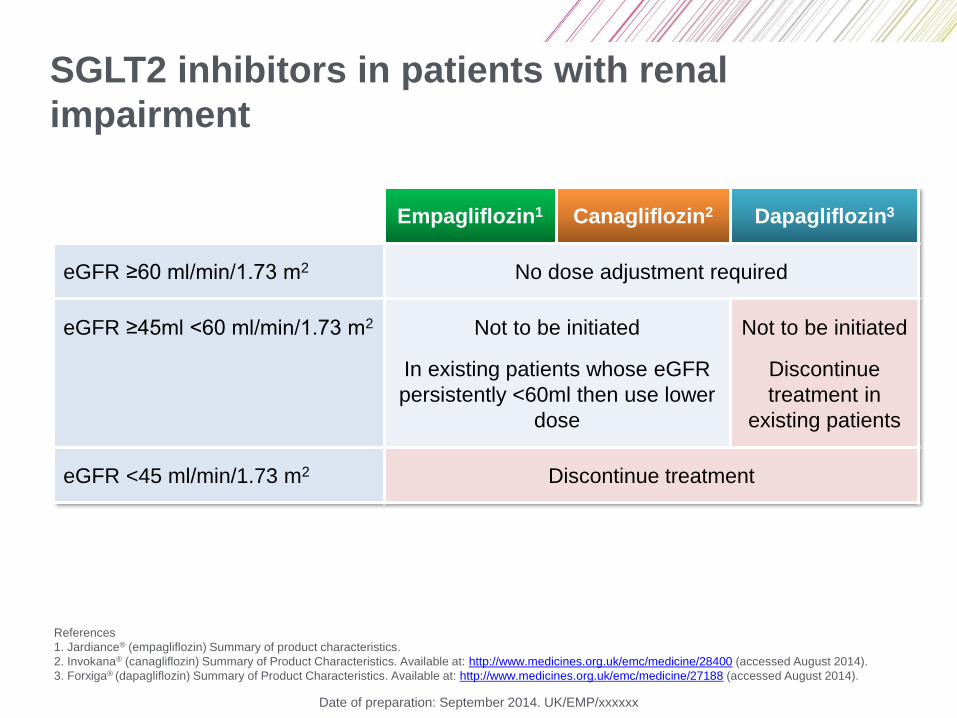
SGLT2 inhibitors in patients with renal
impairment
Empagliflozin1 Canagliflozin2 Dapagliflozin3
eGFR ≥60 ml/min/1.73 m2 No dose adjustment required
eGFR ≥45ml <60 ml/min/1.73 m2 Not to be initiated
In existing patients whose eGFR
persistently <60ml then use lower
dose
Not to be initiated
Discontinue
treatment in
existing patients
eGFR <45 ml/min/1.73 m2 Discontinue treatment
References
1. Jardiance® (empagliflozin) Summary of product characteristics.
2. Invokana® (canagliflozin) Summary of Product Characteristics. Available at: http://www.medicines.org.uk/emc/medicine/28400 (accessed August 2014).
3. Forxiga® (dapagliflozin) Summary of Product Characteristics. Available at: http://www.medicines.org.uk/emc/medicine/27188 (accessed August 2014).
Date of preparation: September 2014. UK/EMP/xxxxxx
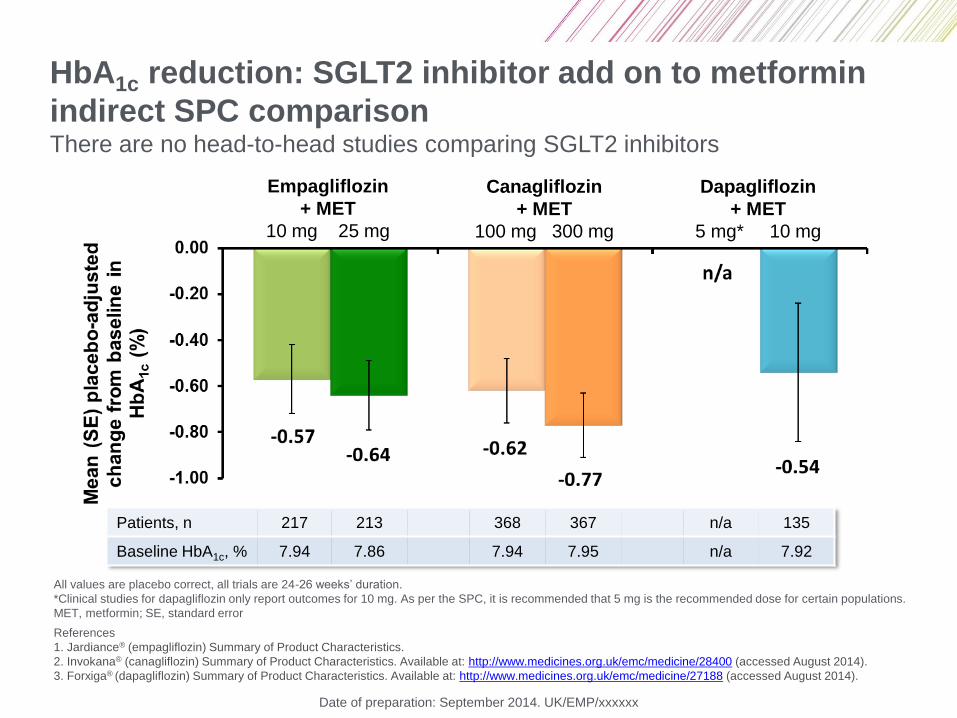
HbA1c reduction: SGLT2 inhibitor add on to metformin
indirect SPC comparison There are no head-to-head studies comparing SGLT2 inhibitors
Empagliflozin
+ MET
10 mg 25 mg
Canagliflozin
+ MET
100 mg 300 mg
Dapagliflozin
+ MET
5 mg* 10 mg
Patients, n 217 213 368 367 n/a 135
Baseline HbA1c, % 7.94 7.86 7.94 7.95 n/a 7.92
All values are placebo correct, all trials are 24-26 weeks’ duration.
*Clinical studies for dapagliflozin only report outcomes for 10 mg. As per the SPC, it is recommended that 5 mg is the recommended dose for certain populations.
MET, metformin; SE, standard error
References
1. Jardiance® (empagliflozin) Summary of Product Characteristics.
2. Invokana® (canagliflozin) Summary of Product Characteristics. Available at: http://www.medicines.org.uk/emc/medicine/28400 (accessed August 2014).
3. Forxiga® (dapagliflozin) Summary of Product Characteristics. Available at: http://www.medicines.org.uk/emc/medicine/27188 (accessed August 2014).

GLP-1 receptor agonists: Advantages and
disadvantages
Advantages • Low inherent risk of hypoglycaemia
• Potential for weight reduction
• Potential for blood pressure reduction
Disadvantages • Gastrointestinal side effects (nausea/vomiting)
• Injectable
• Training requirements
• High unit cost
• Concerns regarding possible risk of pancreatitis
Adapted from Inzucchi SE et al (2012) Diabetes Care 35: 1364–79
1. British National Formulary (2012) 6.1.2.3 Other antidiabetic drugs. Available at: www.bnf.org (accessed 19.09.2012)
Primary physiological actions: ↑ insulin secretion (glucose-dependent); ↓ glucagon
secretion (glucose-dependent); slows gastric emptying; ↑ satiety
Available agents1: exenatide once weekly, exenatide twice daily, liraglutide

Insulin: Advantages and disadvantages
Advantages
• Universally effective
• Theoretically unlimited efficacy
• ↓ Microvascular risk (UKPDS)
Disadvantages
• Hypoglycaemia
• Weight gain
• Injectable
• Training requirements
• “Stigma” (for patients)
UKPDS=UK Prospective Diabetes Study.
1. British National Formulary (2012) 6.1.1 Insulins. Available at: www.bnf.org (accessed 19.09.2012)
Adapted from Inzucchi SE et al (2012) Diabetes Care 35: 1364–79
Primary physiological actions: ↑ Glucose disposal; ↓ hepatic glucose production
Available agents1: various short-acting, long-acting and premixed preparations, of human, animal or
analogue origin.
This presentation has been developed by Boehringer Ingelheim Ltd. and Eli Lilly Company Ltd. UK/TRJ/00125a. May 2012
Pre
va
len
ce
in
T2
D
po
pu
latio
n (
%)
0
20
30
40
27.5
2.7
6.3
24.8
2.5
0.2
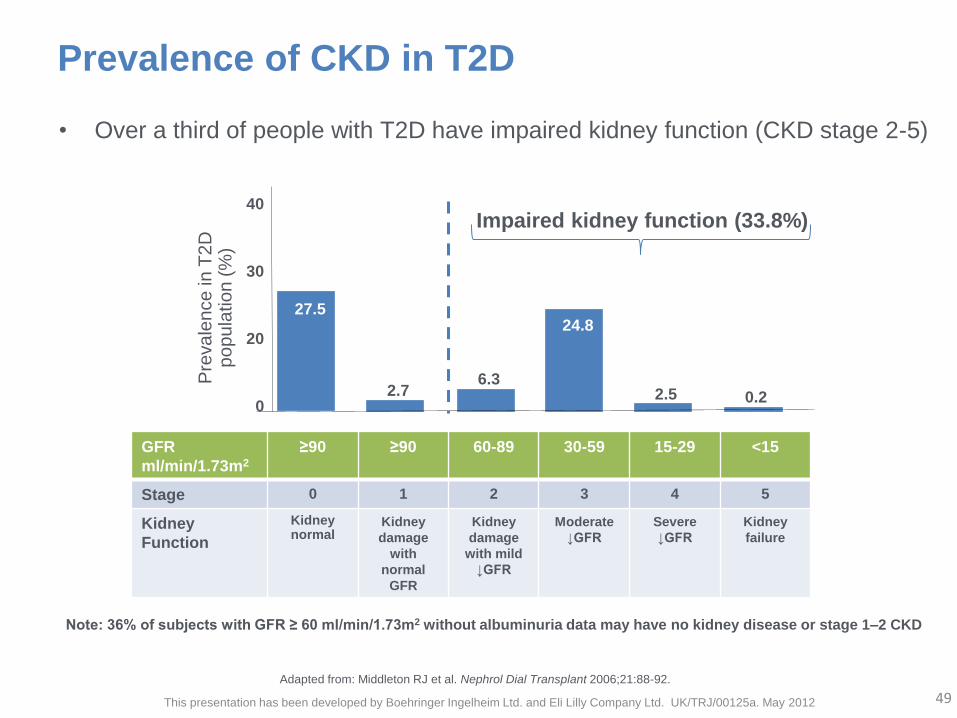
Adapted from: Middleton RJ et al. Nephrol Dial Transplant 2006;21:88-92.
Prevalence of CKD in T2D
GFR
ml/min/1.73m2
≥90
≥90
60-89
30-59 15-29
<15
Stage 0 1 2 3 4 5
Kidney
Function
Kidney normal
Kidney
damage
with
normal
GFR
Kidney
damage
with mild
↓GFR
Moderate
↓GFR
Severe
↓GFR
Kidney
failure
• Over a third of people with T2D have impaired kidney function (CKD stage 2-5)
Impaired kidney function (33.8%)
Note: 36% of subjects with GFR ≥ 60 ml/min/1.73m2 without albuminuria data may have no kidney disease or stage 1–2 CKD
49

Renal impairment and glucose-lowering drugs for type 2 diabetes
● Many of the glucose-lowering agents for type 2 diabetes require dose adjustment or additional monitoring as renal function declines
● The level of intervention required as renal function declines is dependent on the specific drug chosen
Job code: UK/DIA/00242i. Date of preparation: May 2015.
Prescribing considerations in
renal disease1
• Stop metformin when eGFR <45ml/min/1.73m2
• Caution with SUs as increased risk hypoglycemia1
• Pioglitazone can be used1
• Dose reduction required for gliptins except linagliptin1
• SGLT-2s become less effective in developing CKD1
1. Marshall SM. B J Renal Med 2011;16:28–31. 2. Medicines.org.uk accessed 21st January 2015
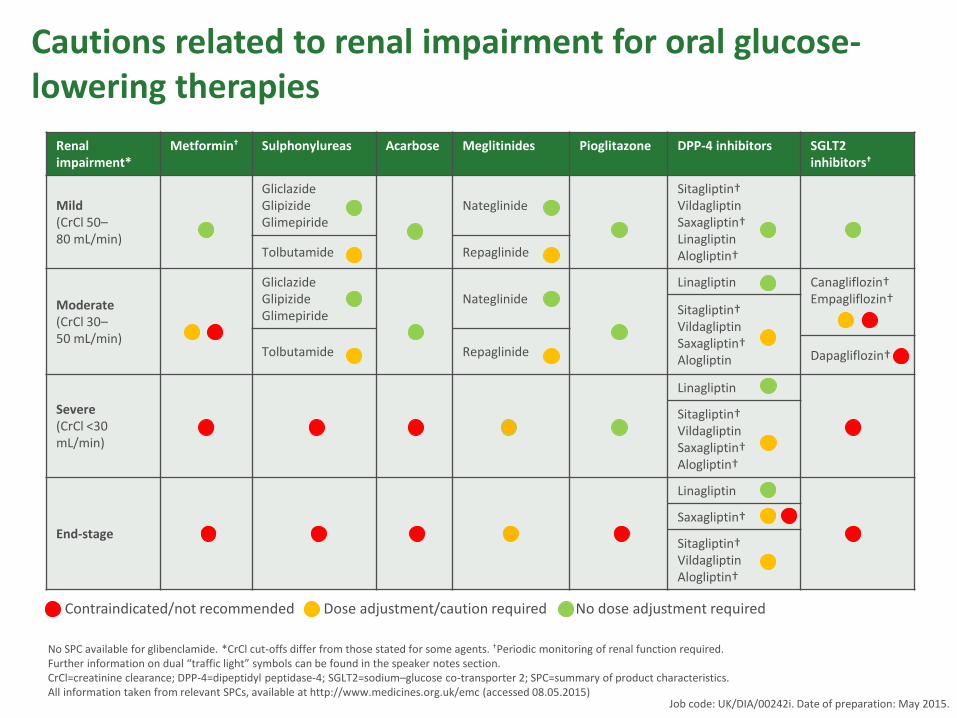
Cautions related to renal impairment for oral glucose-lowering therapies
Contraindicated/not recommended Dose adjustment/caution required No dose adjustment required
No SPC available for glibenclamide. *CrCl cut-offs differ from those stated for some agents. †Periodic monitoring of renal function required. Further information on dual “traffic light” symbols can be found in the speaker notes section. CrCl=creatinine clearance; DPP-4=dipeptidyl peptidase-4; SGLT2=sodium–glucose co-transporter 2; SPC=summary of product characteristics. All information taken from relevant SPCs, available at http://www.medicines.org.uk/emc (accessed 08.05.2015)
Renal impairment*
Metformin† Sulphonylureas Acarbose Meglitinides Pioglitazone DPP-4 inhibitors SGLT2 inhibitors†
Mild (CrCl 50– 80 mL/min)
Gliclazide Glipizide Glimepiride
Nateglinide Sitagliptin† Vildagliptin Saxagliptin† Linagliptin Alogliptin† Tolbutamide Repaglinide
Moderate (CrCl 30– 50 mL/min)
Gliclazide Glipizide Glimepiride
Nateglinide Linagliptin Canagliflozin†
Empagliflozin† Sitagliptin†
Vildagliptin Saxagliptin† Alogliptin
Tolbutamide Repaglinide Dapagliflozin†
Severe (CrCl <30 mL/min)
Linagliptin
Sitagliptin† Vildagliptin Saxagliptin† Alogliptin†
End-stage
Linagliptin
Saxagliptin†
Sitagliptin† Vildagliptin Alogliptin†
Job code: UK/DIA/00242i. Date of preparation: May 2015.

Cautions related to renal impairment for injectable glucose-lowering therapies
Renal impairment* Insulin Glucagon-like peptide-1 receptor agonists
Mild (CrCl 50–80 mL/min)
Liraglutide
Dulaglutide
Lixisenatide
Exenatide twice daily
Exenatide once weekly
Moderate (CrCl 30–50 mL/min)
Liraglutide
Dulaglutide
Lixisenatide
Exenatide twice daily
Exenatide once weekly
Severe (<30 mL/min)
Liraglutide
Dulaglutide
Lixisenatide
Exenatide twice daily
Exenatide once weekly
End-stage
Liraglutide
Dulaglutide
Lixisenatide
Exenatide twice daily
Exenatide once weekly
*CrCl cut-offs differ from those stated for some agents. CrCl=creatinine clearance. All information taken from relevant summaries of product characteristics, available at http://www.medicines.org.uk/emc (accessed 08.05.2015)
Contraindicated/not recommended Dose adjustment/caution required No dose adjustment required
Job code: UK/DIA/00242i. Date of preparation: May 2015.

Prescribing considerations in
heart failure
• May use metformin in chronic
heart failure, withhold during
acute episodes of failure1
• Avoid pioglitazone1
• DPP-4 inhibitors may increase
hospitalization for heart failure1
• Caution with SGLT2 inhibitors
in volume depleted patients1
1. White A, et al. Br J Cardiol 2012;19:85-9.
Prescribing considerations in
liver disease
• Most drugs not tested in
advanced liver disease
• Pioglitazone may reduce
steatosis1
• LFT monitoring recommended
for vildagliptin2
• Lower starting dose for
dapaglifozin in severe hepatic
impairment3
1. Musso G, et al. Diabetologia 2012;55:885-904.; 2. Vildaglitin Summary of Product Characteristics.
Available at www.medicines.org.uk/emc (accessed Oct 2014) 3. 3. Dapaglifozin Summary of Product Characteristics.
Available at www.medicines.org.uk/emc (accessed Oct 2014)

Prescribing considerations in the elderly1
• Co-morbidities -
polypharmacy with risk of
drug interactions1,2
• Increased likelihood of AEs
to drugs1,2
• Decrease in eGFR1,2
• Increased likelihood of
hypoglycaemia1,2
• Individualise therapy
balancing likely benefit with
potential risks1,2
Benefits
Risks
1. McLaren LA, et al. BMJ 2013;346:f2625.; 2. Kirkman MS, et al. Diabetes care 2012;35;2650-64
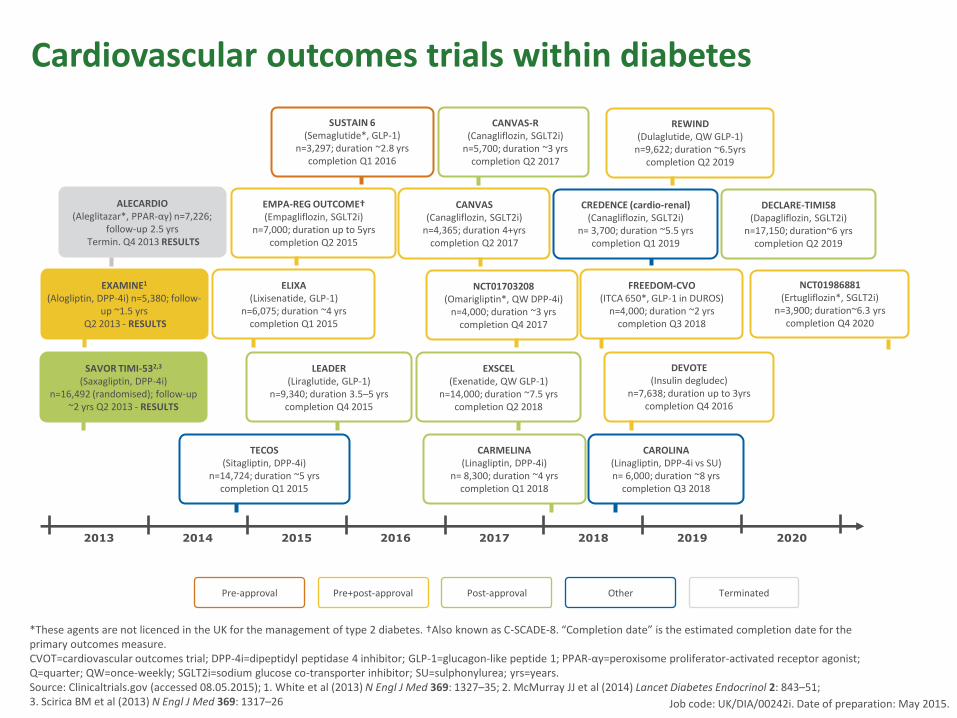
Cardiovascular outcomes trials within diabetes
2013 2014 2015 2016 2017 2018 2019 2020
Pre-approval Pre+post-approval Post-approval Other Terminated
TECOS (Sitagliptin, DPP-4i)
n=14,724; duration ~5 yrs completion Q1 2015
CARMELINA (Linagliptin, DPP-4i)
n= 8,300; duration ~4 yrs completion Q1 2018
CAROLINA (Linagliptin, DPP-4i vs SU) n= 6,000; duration ~8 yrs
completion Q3 2018
SAVOR TIMI-532,3 (Saxagliptin, DPP-4i)
n=16,492 (randomised); follow-up ~2 yrs Q2 2013 - RESULTS
EXAMINE1
(Alogliptin, DPP-4i) n=5,380; follow-up ~1.5 yrs
Q2 2013 - RESULTS
ALECARDIO (Aleglitazar*, PPAR-αγ) n=7,226;
follow-up 2.5 yrs Termin. Q4 2013 RESULTS
LEADER (Liraglutide, GLP-1)
n=9,340; duration 3.5–5 yrs completion Q4 2015
ELIXA (Lixisenatide, GLP-1)
n=6,075; duration ~4 yrs completion Q1 2015
EMPA-REG OUTCOME† (Empagliflozin, SGLT2i)
n=7,000; duration up to 5yrs completion Q2 2015
EXSCEL (Exenatide, QW GLP-1)
n=14,000; duration ~7.5 yrs completion Q2 2018
NCT01703208 (Omarigliptin*, QW DPP-4i)
n=4,000; duration ~3 yrs completion Q4 2017
CANVAS (Canagliflozin, SGLT2i)
n=4,365; duration 4+yrs completion Q2 2017
CANVAS-R (Canagliflozin, SGLT2i)
n=5,700; duration ~3 yrs completion Q2 2017
DEVOTE (Insulin degludec)
n=7,638; duration up to 3yrs completion Q4 2016
FREEDOM-CVO (ITCA 650*, GLP-1 in DUROS)
n=4,000; duration ~2 yrs completion Q3 2018
CREDENCE (cardio-renal) (Canagliflozin, SGLT2i)
n= 3,700; duration ~5.5 yrs completion Q1 2019
REWIND (Dulaglutide, QW GLP-1)
n=9,622; duration ~6.5yrs completion Q2 2019
DECLARE-TIMI58 (Dapagliflozin, SGLT2i)
n=17,150; duration~6 yrs completion Q2 2019
NCT01986881 (Ertugliflozin*, SGLT2i)
n=3,900; duration~6.3 yrs completion Q4 2020
*These agents are not licenced in the UK for the management of type 2 diabetes. †Also known as C-SCADE-8. “Completion date” is the estimated completion date for the primary outcomes measure. CVOT=cardiovascular outcomes trial; DPP-4i=dipeptidyl peptidase 4 inhibitor; GLP-1=glucagon-like peptide 1; PPAR-αγ=peroxisome proliferator-activated receptor agonist; Q=quarter; QW=once-weekly; SGLT2i=sodium glucose co-transporter inhibitor; SU=sulphonylurea; yrs=years. Source: Clinicaltrials.gov (accessed 08.05.2015); 1. White et al (2013) N Engl J Med 369: 1327–35; 2. McMurray JJ et al (2014) Lancet Diabetes Endocrinol 2: 843–51; 3. Scirica BM et al (2013) N Engl J Med 369: 1317–26
SUSTAIN 6 (Semaglutide*, GLP-1)
n=3,297; duration ~2.8 yrs completion Q1 2016
Job code: UK/DIA/00242i. Date of preparation: May 2015.
Conclusions
• Many different types of
patients with type 2
diabetes at different stages
of the disease
• Many different oral agents
available to choose from
• Guidelines may help
• Individualise therapy choice
• Regular follow up to monitor
therapeutic effectiveness is
essential.
Symptom control
Prognostic benefit
Side effects
Adherence